User login
Productivity Capacity

The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
Surge Protection

Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Penetrating Head Injury...
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Dr. Hospitalist

I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
Cases That Have Gone to Trial
Observation Care
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
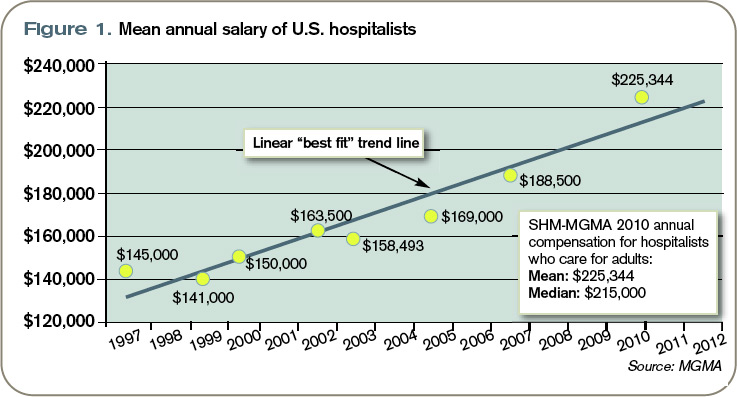
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
Transitions Telethon

The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.