User login
The Cost of Regulation
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?

The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
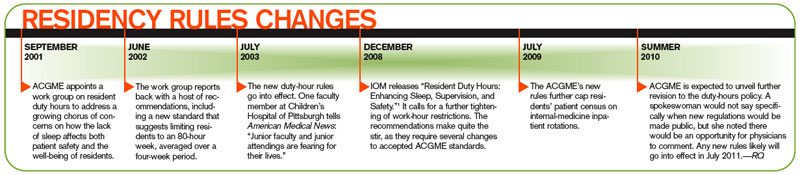
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.

At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
Spousal Consent
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
Discharge Services
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
The Humble Approach
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
The Earlier, the Better

Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Practice Management Session
PHYSICIAN ASSISTANTS (PAs) and nurse practitioners can do almost anything a physician can do, and many have skill sets physicians lack, according to David Friar, MD, FHM, president of Hospitalists of Northwest Michigan based in Traverse City.
“As we go forward, with continued physician shortages and with the growing responsibilities of the hospitalist movement, we are going to need more and more people with different skill sets,” Dr. Friar said during his presentation at HM10. “I think one of those important areas is nonphysician providers.”

A quick survey of the 300 or so hospitalists at the session showed most HM groups employ NPPs, but less than a third of those thought they were “using NPPs well.” Dr. Friar, who has worked with NPs and PAs for 14 years, said he has found NPPs “to be an integral part of our practice. They have become indispensable to us in the way we provide services to our hospitals and patients.”
Still, many hospitalist groups waste NPP potential, Dr. Friar explained. He suggested HM groups evaluate their NPP roster and duties, and make necessary changes. “Make sure you treat them as if they are part of the team. That is very important,” he said. “NPPs can and should take care of patients throughout all stages of the hospital stay, from admission to discharge.”
When hiring NPPs, look for team players who are flexible and willing to learn. Make sure the NPP knows their limits and is comfortable asking for help. Target local training programs or other departments in the hospital as fertile ground for new hires. But, most importantly, know what you are getting when you hire an NPP.
“Don’t underestimate the cost of the inexperienced NPP in terms of training. If you think it’s two weeks or two months, you are fooling yourself,” Dr. Friar emphasized, adding an inexperienced NPP could take from six months to two years to reach full competency in hospitalist service. “Know the tradeoffs,” he said. “It might be more important for you to hire the more experienced—and more costly—NPP so you don’t have to spend two years to get them up to speed.” HM10
PHYSICIAN ASSISTANTS (PAs) and nurse practitioners can do almost anything a physician can do, and many have skill sets physicians lack, according to David Friar, MD, FHM, president of Hospitalists of Northwest Michigan based in Traverse City.
“As we go forward, with continued physician shortages and with the growing responsibilities of the hospitalist movement, we are going to need more and more people with different skill sets,” Dr. Friar said during his presentation at HM10. “I think one of those important areas is nonphysician providers.”
A quick survey of the 300 or so hospitalists at the session showed most HM groups employ NPPs, but less than a third of those thought they were “using NPPs well.” Dr. Friar, who has worked with NPs and PAs for 14 years, said he has found NPPs “to be an integral part of our practice. They have become indispensable to us in the way we provide services to our hospitals and patients.”
Still, many hospitalist groups waste NPP potential, Dr. Friar explained. He suggested HM groups evaluate their NPP roster and duties, and make necessary changes. “Make sure you treat them as if they are part of the team. That is very important,” he said. “NPPs can and should take care of patients throughout all stages of the hospital stay, from admission to discharge.”
When hiring NPPs, look for team players who are flexible and willing to learn. Make sure the NPP knows their limits and is comfortable asking for help. Target local training programs or other departments in the hospital as fertile ground for new hires. But, most importantly, know what you are getting when you hire an NPP.
“Don’t underestimate the cost of the inexperienced NPP in terms of training. If you think it’s two weeks or two months, you are fooling yourself,” Dr. Friar emphasized, adding an inexperienced NPP could take from six months to two years to reach full competency in hospitalist service. “Know the tradeoffs,” he said. “It might be more important for you to hire the more experienced—and more costly—NPP so you don’t have to spend two years to get them up to speed.” HM10
PHYSICIAN ASSISTANTS (PAs) and nurse practitioners can do almost anything a physician can do, and many have skill sets physicians lack, according to David Friar, MD, FHM, president of Hospitalists of Northwest Michigan based in Traverse City.
“As we go forward, with continued physician shortages and with the growing responsibilities of the hospitalist movement, we are going to need more and more people with different skill sets,” Dr. Friar said during his presentation at HM10. “I think one of those important areas is nonphysician providers.”
A quick survey of the 300 or so hospitalists at the session showed most HM groups employ NPPs, but less than a third of those thought they were “using NPPs well.” Dr. Friar, who has worked with NPs and PAs for 14 years, said he has found NPPs “to be an integral part of our practice. They have become indispensable to us in the way we provide services to our hospitals and patients.”
Still, many hospitalist groups waste NPP potential, Dr. Friar explained. He suggested HM groups evaluate their NPP roster and duties, and make necessary changes. “Make sure you treat them as if they are part of the team. That is very important,” he said. “NPPs can and should take care of patients throughout all stages of the hospital stay, from admission to discharge.”
When hiring NPPs, look for team players who are flexible and willing to learn. Make sure the NPP knows their limits and is comfortable asking for help. Target local training programs or other departments in the hospital as fertile ground for new hires. But, most importantly, know what you are getting when you hire an NPP.
“Don’t underestimate the cost of the inexperienced NPP in terms of training. If you think it’s two weeks or two months, you are fooling yourself,” Dr. Friar emphasized, adding an inexperienced NPP could take from six months to two years to reach full competency in hospitalist service. “Know the tradeoffs,” he said. “It might be more important for you to hire the more experienced—and more costly—NPP so you don’t have to spend two years to get them up to speed.” HM10
Practice Management Session
IN THEORY, unit-based de-ployment of hospitalists is a perfect answer to the struggles of navigating, say, a 16-patient census that includes seven units on four floors. But in the real world, it’s not.
“Just placing hospitalists on a unit and giving them patients isn’t the answer,” said Russell L. Holman, MD, SFHM, chief operating officer for Cogent Healthcare in Brentwood, Tenn., and past president of SHM. “Structure has to support a deliberate strategy. Think of what your strategic goals are. … Don’t just implement a new structure and let that be the end.”

—Russell L. Holman, MD, SFHM, chief operating officer, Cogent Healthcare, Brentwood, Tenn., past president of SHM
Dr. Holman led a panel, “The Case for Unit-Based Hospitalists: Benefits and Challenges,” in which HM experts agreed that tracking the efficacy of the setup is key to success.
Although the benefits are usually clear—less time spent traveling from floor to floor and more direct communication between physicians and nonphysician providers (NPPs)—the challenges can be numerous, including:
- Fairness. The first complaint of most HM groups switching to a unit-based approach is that it unfairly distributes patient loads, leading to daytime shifts for which one physician starts with a patient census of eight, while a colleague starts with 15.
- Interunit transfers. By creating defined geographic areas, a patient’s movement from one unit to another becomes another transition of care and brings with it those issues.
- Buy-in from other stakeholders. Physician assistants (PA), nursing staff, and others are affected by geographic alignment. Make sure to pitch quantifiable goals—increased productivity, increased touch time with patients, reduced staff turnover—when instituting the new approach.
Kevin O’Leary, MD, MS, associate chief of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, urges physicians to be practical, and not to expect the unit-based approach to be a panacea. “This is really the first step,” he said. HM10
IN THEORY, unit-based de-ployment of hospitalists is a perfect answer to the struggles of navigating, say, a 16-patient census that includes seven units on four floors. But in the real world, it’s not.
“Just placing hospitalists on a unit and giving them patients isn’t the answer,” said Russell L. Holman, MD, SFHM, chief operating officer for Cogent Healthcare in Brentwood, Tenn., and past president of SHM. “Structure has to support a deliberate strategy. Think of what your strategic goals are. … Don’t just implement a new structure and let that be the end.”
—Russell L. Holman, MD, SFHM, chief operating officer, Cogent Healthcare, Brentwood, Tenn., past president of SHM
Dr. Holman led a panel, “The Case for Unit-Based Hospitalists: Benefits and Challenges,” in which HM experts agreed that tracking the efficacy of the setup is key to success.
Although the benefits are usually clear—less time spent traveling from floor to floor and more direct communication between physicians and nonphysician providers (NPPs)—the challenges can be numerous, including:
- Fairness. The first complaint of most HM groups switching to a unit-based approach is that it unfairly distributes patient loads, leading to daytime shifts for which one physician starts with a patient census of eight, while a colleague starts with 15.
- Interunit transfers. By creating defined geographic areas, a patient’s movement from one unit to another becomes another transition of care and brings with it those issues.
- Buy-in from other stakeholders. Physician assistants (PA), nursing staff, and others are affected by geographic alignment. Make sure to pitch quantifiable goals—increased productivity, increased touch time with patients, reduced staff turnover—when instituting the new approach.
Kevin O’Leary, MD, MS, associate chief of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, urges physicians to be practical, and not to expect the unit-based approach to be a panacea. “This is really the first step,” he said. HM10
IN THEORY, unit-based de-ployment of hospitalists is a perfect answer to the struggles of navigating, say, a 16-patient census that includes seven units on four floors. But in the real world, it’s not.
“Just placing hospitalists on a unit and giving them patients isn’t the answer,” said Russell L. Holman, MD, SFHM, chief operating officer for Cogent Healthcare in Brentwood, Tenn., and past president of SHM. “Structure has to support a deliberate strategy. Think of what your strategic goals are. … Don’t just implement a new structure and let that be the end.”
—Russell L. Holman, MD, SFHM, chief operating officer, Cogent Healthcare, Brentwood, Tenn., past president of SHM
Dr. Holman led a panel, “The Case for Unit-Based Hospitalists: Benefits and Challenges,” in which HM experts agreed that tracking the efficacy of the setup is key to success.
Although the benefits are usually clear—less time spent traveling from floor to floor and more direct communication between physicians and nonphysician providers (NPPs)—the challenges can be numerous, including:
- Fairness. The first complaint of most HM groups switching to a unit-based approach is that it unfairly distributes patient loads, leading to daytime shifts for which one physician starts with a patient census of eight, while a colleague starts with 15.
- Interunit transfers. By creating defined geographic areas, a patient’s movement from one unit to another becomes another transition of care and brings with it those issues.
- Buy-in from other stakeholders. Physician assistants (PA), nursing staff, and others are affected by geographic alignment. Make sure to pitch quantifiable goals—increased productivity, increased touch time with patients, reduced staff turnover—when instituting the new approach.
Kevin O’Leary, MD, MS, associate chief of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, urges physicians to be practical, and not to expect the unit-based approach to be a panacea. “This is really the first step,” he said. HM10
Professional Advice
NATIONAL HARBOR, Md.—;Amie Dlouhy, RN, BSN, hospitalist program manager with Saint Mary’s Health Care in Grand Rapids, Mich., couldn’t scribble notes furiously enough during the practice-management pre-course at HM10. Dlouhy was promoted to her new position as an administrator some six weeks before the annual meeting at the Gaylord National Resort & Convention Center in early April.
So the first-time meeting attendee decided she would jot down as many tips as she could. She quickly realized the trip was worth it, as she learned that a departmental dashboard is a relatively simple way to gather key information in one place. She also likes the idea of drawing up a brochure that tells patients what they can expect from their hospitalists—and perhaps vice versa. And what new HM group leader doesn’t want advice on building a schedule that adds individualized wrinkles to the “seven-on, seven-off” structure?

“It is a business and you need to treat it as if it’s a business,” Dlouhy said. “It’s an ongoing process, and you want to make sure you have a concrete foundation.”
The tidbits Dlouhy gleaned from her pre-course were among scores of nuggets discussed during eight of the accredited educational sessions. This year’s pre-courses boosted to a new high of 20 the number of Category 1 credits physicians could earn toward the American Medical Association’s (AMA) Physician Recognition Award. Last year, the total was 15.
Offering more classes—and more varied topics—worked pretty well, as this year’s slate of pre-courses was more popular than ever, according to SHM officials. At HM09 in Chicago, more than 800 attendees participated in six sessions. At HM10, the total attendance was roughly 10% higher.
A main driver of the growth was the addition of two new courses—“Essential Neurology for the Hospitalist” and “Early Career Hospitalist: Skills for Success.” Another was a packed room of hospitalists answering questions—some right, some wrong—and preparing for the new Focused Practice in Hospital Medicine (FPHM) via the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC). The learning session pre-course debuted last year, but the new HM pathway to board recertification helped push attendance higher this year.
“The nice thing about the audience-response system is that you can actually see that not everybody is always going straight to the right answer on all of the questions,” said Julius Yang, MD, PhD, a hospitalist at Beth Israel Deaconess Medical Center in Boston and the MOC course director. “It’s really serving as an important refresher of our medical knowledge base.”
Dr. Yang said the “mini-retreat” environment of an annual convention is the perfect place to focus on granular professional development. “Trying to do these types of MOCs when you’re working to keep current with all of your other duties, you don’t get as much out of it,” Dr. Yang said. “Here, you get it all.”
—Troy Ahlstrom, MD, FHM, Hospitalists of Northwest Michigan, Traverse City
He adds that those physicians who take the time and spend the money to travel for an educational session tend to be very focused on taking advantage of the program, not just showing up to be counted.
“All of these [questions] are very much directed at growing as a hospitalist,” Dr. Yang said. “It’s a different focus than the rest of the meeting. This is about every individual bringing something back to their institution.”
That’s what keeps bringing Troy Ahlstrom, MD, FHM, back. Dr. Ahlstrom, of Hos-pitalists of Northwest Michigan in Traverse City, has been to three annual meetings, and he said he tries to hit a pre-course every time. Last year, it was a session on how to more completely capture costs from billing and coding.
This year: “Comprehensive Critical Care in 2010: An Interactive Course.” The former appealed to him given that every HM group needs to capture as many of its charges as possible, and the latter because his group helps staff the critical-care units of three hospitals.
Several physicians noted that the critical-care pre-course was particularly appealing to attendees, as more hospitalists are handling those duties at their respective institutions. The format was popular, too, and was structured in the same way as the ABIM learning session, with course director David Schul-man, MD, MPH, chief of pulmonary and critical-care medicine at Emory University Hospital in Atlanta, leading a room full of hospitalists through a multiple-choice exam.

Dr. Ahlstrom and others noted that aside from the engagement in education that the daylong pre-courses offer, the sessions are set up with take-home guides, reference materials, and earnest pledges for mentoring from speakers and SHM staff.
“Most medical meetings have a scientific focus with a couple of practical aspects,” Dr. Ahlstrom said. “SHM’s meeting is very practical. It presents research, but it’s research you will use in your practice.”
Gerald Johnson, MD, a hospitalist at Texoma Medical Center in Denison, Texas, signed up for the “Best Practices in Managing a Hospital Medicine Program” pre-course during his first visit to an SHM meeting. A hospitalist for about four years, Dr. Johnson decided to take the pre-course at the urging of senior colleagues. He said the most helpful lessons he gleaned were about compensation plans, scheduling, and staffing.
“It’s not one person getting up there and presenting ‘This is how it needs to be done,’ ” Dr. Johnson said. “They present you with several ways. It really gives you something to adapt to your personal environment.”
Dr. Johnson, who gushed about “the gurus” of HM leading his session, also likes the fact that people with both a financial pedigree and a background in clinical work present the information. In fact, several attendees of the best-practices session noted that the attention to both medicine and management helps fill in the gaps between being a clinician and being a businessman.
“You’ve got to do both well,” Dr. Ahlstrom said. “You’ve got to take good care of patients. But in order to take good care of patients, you have to run a good business model, too.” HM10
Richard Quinn is a freelance writer based in New Jersey.
NATIONAL HARBOR, Md.—;Amie Dlouhy, RN, BSN, hospitalist program manager with Saint Mary’s Health Care in Grand Rapids, Mich., couldn’t scribble notes furiously enough during the practice-management pre-course at HM10. Dlouhy was promoted to her new position as an administrator some six weeks before the annual meeting at the Gaylord National Resort & Convention Center in early April.
So the first-time meeting attendee decided she would jot down as many tips as she could. She quickly realized the trip was worth it, as she learned that a departmental dashboard is a relatively simple way to gather key information in one place. She also likes the idea of drawing up a brochure that tells patients what they can expect from their hospitalists—and perhaps vice versa. And what new HM group leader doesn’t want advice on building a schedule that adds individualized wrinkles to the “seven-on, seven-off” structure?
“It is a business and you need to treat it as if it’s a business,” Dlouhy said. “It’s an ongoing process, and you want to make sure you have a concrete foundation.”
The tidbits Dlouhy gleaned from her pre-course were among scores of nuggets discussed during eight of the accredited educational sessions. This year’s pre-courses boosted to a new high of 20 the number of Category 1 credits physicians could earn toward the American Medical Association’s (AMA) Physician Recognition Award. Last year, the total was 15.
Offering more classes—and more varied topics—worked pretty well, as this year’s slate of pre-courses was more popular than ever, according to SHM officials. At HM09 in Chicago, more than 800 attendees participated in six sessions. At HM10, the total attendance was roughly 10% higher.
A main driver of the growth was the addition of two new courses—“Essential Neurology for the Hospitalist” and “Early Career Hospitalist: Skills for Success.” Another was a packed room of hospitalists answering questions—some right, some wrong—and preparing for the new Focused Practice in Hospital Medicine (FPHM) via the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC). The learning session pre-course debuted last year, but the new HM pathway to board recertification helped push attendance higher this year.
“The nice thing about the audience-response system is that you can actually see that not everybody is always going straight to the right answer on all of the questions,” said Julius Yang, MD, PhD, a hospitalist at Beth Israel Deaconess Medical Center in Boston and the MOC course director. “It’s really serving as an important refresher of our medical knowledge base.”
Dr. Yang said the “mini-retreat” environment of an annual convention is the perfect place to focus on granular professional development. “Trying to do these types of MOCs when you’re working to keep current with all of your other duties, you don’t get as much out of it,” Dr. Yang said. “Here, you get it all.”
—Troy Ahlstrom, MD, FHM, Hospitalists of Northwest Michigan, Traverse City
He adds that those physicians who take the time and spend the money to travel for an educational session tend to be very focused on taking advantage of the program, not just showing up to be counted.
“All of these [questions] are very much directed at growing as a hospitalist,” Dr. Yang said. “It’s a different focus than the rest of the meeting. This is about every individual bringing something back to their institution.”
That’s what keeps bringing Troy Ahlstrom, MD, FHM, back. Dr. Ahlstrom, of Hos-pitalists of Northwest Michigan in Traverse City, has been to three annual meetings, and he said he tries to hit a pre-course every time. Last year, it was a session on how to more completely capture costs from billing and coding.
This year: “Comprehensive Critical Care in 2010: An Interactive Course.” The former appealed to him given that every HM group needs to capture as many of its charges as possible, and the latter because his group helps staff the critical-care units of three hospitals.
Several physicians noted that the critical-care pre-course was particularly appealing to attendees, as more hospitalists are handling those duties at their respective institutions. The format was popular, too, and was structured in the same way as the ABIM learning session, with course director David Schul-man, MD, MPH, chief of pulmonary and critical-care medicine at Emory University Hospital in Atlanta, leading a room full of hospitalists through a multiple-choice exam.
Dr. Ahlstrom and others noted that aside from the engagement in education that the daylong pre-courses offer, the sessions are set up with take-home guides, reference materials, and earnest pledges for mentoring from speakers and SHM staff.
“Most medical meetings have a scientific focus with a couple of practical aspects,” Dr. Ahlstrom said. “SHM’s meeting is very practical. It presents research, but it’s research you will use in your practice.”
Gerald Johnson, MD, a hospitalist at Texoma Medical Center in Denison, Texas, signed up for the “Best Practices in Managing a Hospital Medicine Program” pre-course during his first visit to an SHM meeting. A hospitalist for about four years, Dr. Johnson decided to take the pre-course at the urging of senior colleagues. He said the most helpful lessons he gleaned were about compensation plans, scheduling, and staffing.
“It’s not one person getting up there and presenting ‘This is how it needs to be done,’ ” Dr. Johnson said. “They present you with several ways. It really gives you something to adapt to your personal environment.”
Dr. Johnson, who gushed about “the gurus” of HM leading his session, also likes the fact that people with both a financial pedigree and a background in clinical work present the information. In fact, several attendees of the best-practices session noted that the attention to both medicine and management helps fill in the gaps between being a clinician and being a businessman.
“You’ve got to do both well,” Dr. Ahlstrom said. “You’ve got to take good care of patients. But in order to take good care of patients, you have to run a good business model, too.” HM10
Richard Quinn is a freelance writer based in New Jersey.
NATIONAL HARBOR, Md.—;Amie Dlouhy, RN, BSN, hospitalist program manager with Saint Mary’s Health Care in Grand Rapids, Mich., couldn’t scribble notes furiously enough during the practice-management pre-course at HM10. Dlouhy was promoted to her new position as an administrator some six weeks before the annual meeting at the Gaylord National Resort & Convention Center in early April.
So the first-time meeting attendee decided she would jot down as many tips as she could. She quickly realized the trip was worth it, as she learned that a departmental dashboard is a relatively simple way to gather key information in one place. She also likes the idea of drawing up a brochure that tells patients what they can expect from their hospitalists—and perhaps vice versa. And what new HM group leader doesn’t want advice on building a schedule that adds individualized wrinkles to the “seven-on, seven-off” structure?
“It is a business and you need to treat it as if it’s a business,” Dlouhy said. “It’s an ongoing process, and you want to make sure you have a concrete foundation.”
The tidbits Dlouhy gleaned from her pre-course were among scores of nuggets discussed during eight of the accredited educational sessions. This year’s pre-courses boosted to a new high of 20 the number of Category 1 credits physicians could earn toward the American Medical Association’s (AMA) Physician Recognition Award. Last year, the total was 15.
Offering more classes—and more varied topics—worked pretty well, as this year’s slate of pre-courses was more popular than ever, according to SHM officials. At HM09 in Chicago, more than 800 attendees participated in six sessions. At HM10, the total attendance was roughly 10% higher.
A main driver of the growth was the addition of two new courses—“Essential Neurology for the Hospitalist” and “Early Career Hospitalist: Skills for Success.” Another was a packed room of hospitalists answering questions—some right, some wrong—and preparing for the new Focused Practice in Hospital Medicine (FPHM) via the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC). The learning session pre-course debuted last year, but the new HM pathway to board recertification helped push attendance higher this year.
“The nice thing about the audience-response system is that you can actually see that not everybody is always going straight to the right answer on all of the questions,” said Julius Yang, MD, PhD, a hospitalist at Beth Israel Deaconess Medical Center in Boston and the MOC course director. “It’s really serving as an important refresher of our medical knowledge base.”
Dr. Yang said the “mini-retreat” environment of an annual convention is the perfect place to focus on granular professional development. “Trying to do these types of MOCs when you’re working to keep current with all of your other duties, you don’t get as much out of it,” Dr. Yang said. “Here, you get it all.”
—Troy Ahlstrom, MD, FHM, Hospitalists of Northwest Michigan, Traverse City
He adds that those physicians who take the time and spend the money to travel for an educational session tend to be very focused on taking advantage of the program, not just showing up to be counted.
“All of these [questions] are very much directed at growing as a hospitalist,” Dr. Yang said. “It’s a different focus than the rest of the meeting. This is about every individual bringing something back to their institution.”
That’s what keeps bringing Troy Ahlstrom, MD, FHM, back. Dr. Ahlstrom, of Hos-pitalists of Northwest Michigan in Traverse City, has been to three annual meetings, and he said he tries to hit a pre-course every time. Last year, it was a session on how to more completely capture costs from billing and coding.
This year: “Comprehensive Critical Care in 2010: An Interactive Course.” The former appealed to him given that every HM group needs to capture as many of its charges as possible, and the latter because his group helps staff the critical-care units of three hospitals.
Several physicians noted that the critical-care pre-course was particularly appealing to attendees, as more hospitalists are handling those duties at their respective institutions. The format was popular, too, and was structured in the same way as the ABIM learning session, with course director David Schul-man, MD, MPH, chief of pulmonary and critical-care medicine at Emory University Hospital in Atlanta, leading a room full of hospitalists through a multiple-choice exam.
Dr. Ahlstrom and others noted that aside from the engagement in education that the daylong pre-courses offer, the sessions are set up with take-home guides, reference materials, and earnest pledges for mentoring from speakers and SHM staff.
“Most medical meetings have a scientific focus with a couple of practical aspects,” Dr. Ahlstrom said. “SHM’s meeting is very practical. It presents research, but it’s research you will use in your practice.”
Gerald Johnson, MD, a hospitalist at Texoma Medical Center in Denison, Texas, signed up for the “Best Practices in Managing a Hospital Medicine Program” pre-course during his first visit to an SHM meeting. A hospitalist for about four years, Dr. Johnson decided to take the pre-course at the urging of senior colleagues. He said the most helpful lessons he gleaned were about compensation plans, scheduling, and staffing.
“It’s not one person getting up there and presenting ‘This is how it needs to be done,’ ” Dr. Johnson said. “They present you with several ways. It really gives you something to adapt to your personal environment.”
Dr. Johnson, who gushed about “the gurus” of HM leading his session, also likes the fact that people with both a financial pedigree and a background in clinical work present the information. In fact, several attendees of the best-practices session noted that the attention to both medicine and management helps fill in the gaps between being a clinician and being a businessman.
“You’ve got to do both well,” Dr. Ahlstrom said. “You’ve got to take good care of patients. But in order to take good care of patients, you have to run a good business model, too.” HM10
Richard Quinn is a freelance writer based in New Jersey.
Continuity Conundrum

Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.

Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.
Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.
Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
New Referral Distribution

Editor’s note: Second of a three-part series.
As I mentioned last month, there isn’t a proven best method to use when distributing new referrals among your group’s providers. The popular methods fall along a continuum of being focused on daily, or continuous, leveling of patient loads between providers (“load leveling”) at one end; at the other end of the continuum is having a doctor be “on” for all new referrals for a predetermined time period, and accepting that patient volumes might be uneven day to day but tend to even out over long periods.
There might not be any reason to change your group’s approach to patient assignment, but you should always be thinking about how your own methods might be changed or improved. I have shared (“Bigger Isn’t Always Better,” June 2009, p. 46) my concern that some groups invest far too much time in a morning load-leveling and handoff conference. Make sure your group is using only as much time as needed.
Air-Traffic Controllers
Many large groups (e.g., more than 15 full-time equivalents) that assign patients to providers in sequence, like dealing a deck of cards, have a designated provider who holds the triage pager and serves as “air-traffic controller.” This person typically takes incoming calls about all new referrals, jots down the relevant clinical data, keeps track of which hospitalist is due to take the next patient, pages that person, and repeats the clinical information. As I’ve written before (“How to Hire and Use Clerical Staff,” June 2007, p. 73), many practices have found that during business hours, they can hand this role to a clerical person who simply takes down the name and phone number of the doctor making the referral, then pages that information to the hospitalist due to get the next patient. The hospitalist then calls and speaks directly with the referring doctor.
Small- to medium-sized groups can eliminate entirely the need for any such “air-traffic control” function if they assign all new referrals to a single doctor for specified periods of time. For example, from 7 a.m. to 3 p.m. today, all new referrals go to Dr. Glass, and from 3 p.m. to 11 p.m., they go to Dr. Cage.
Admitter-Rounder Duties
Many—maybe most?—large groups separate daytime admitter and rounder functions so that on any given day, a hospitalist does one but not both. The principal advantages of this approach are reducing the stress on, and possibly increasing the efficiency of, rounding doctors by shielding them from the unpredictable and time-consuming interruption of needing to admit a new patient. And a daytime doctor who only does admissions might be able to start seeing a patient in the ED more quickly than one who is busy making rounds.
Any increased availability of admitters to the ED could be offset by their lack of surge capacity leading to a bottleneck in ED throughput when there are many patients to admit at the same time and a limited number of admitters (often only one). Such a bottleneck would be much less likely if all daytime doctors (i.e., the rounders) were available to see admissions rather than just admitters.
Continuity of care suffers when a group has separate admitters and rounders, because no patients will be seen by the same doctor on the day of admission and the day following. This method requires a handoff from the day of admission to the next day. Such a handoff might be unavoidable for patients admitted during the night, but this doesn’t have to occur when patients are admitted during the daytime.
Who’s Seeing this Patient?
It seems to make sense to wait until each morning to distribute patients. That allows the practice to know just how many new patients there are, and they can be distributed according to complexity and whether a hospitalist has formed a previous relationship with that patient. But it means that no one at the hospital will know which hospitalist is caring for the patient until later in the morning. For example, if the radiologist is over-reading a study done during the night and finds something worthy of a phone call to the hospitalist, no one is sure who should get the call. A patient might develop hypoglycemia shortly after the hospitalist night shift is over, but the nurse doesn’t know which hospitalist to call.
And, perhaps most importantly, if patients aren’t distributed until the start of the day shift, the night hospitalist can’t tell the patient and family which hospitalist to expect the next morning. To test the significance of this issue, I conducted an experiment while working our group’s late-evening admitter shift. I concluded my visit with each admitted patient by explaining, “I am on-call for our group tonight, so I will be off recovering tomorrow. Therefore, I won’t see you again, but one of my partners will take over in the morning. Do you have any questions for me?” Every patient I admitted had the same question. “What is that doctor’s name?”
How does your group answer a patient who asks which hospitalist will be in the next day? If your method is load-leveling in the morning, then the best answer your night admitting doctor can give is probably to say: “I don’t know which of my partners will be in. There are several working tomorrow, and at the start of the day, they will divide up the patients who come in tonight depending on how busy each of them is. But all the doctors in our group are terrific and will take good care of you.”
I’m told the same thing when I get my hair cut: You’ll get whichever “hair artist” is up next. I put up with it at the hair place because it costs less than $15. But I still find it a little irritating. I’m sure all the barbers aren’t equally skilled or diligent, and I want the best one. (Maybe I shouldn’t care since there isn’t much that can be done with my hair.) I’m pretty sure patients feel the same way about which doctor they get. The public is convinced there is a wide variety in the quality of doctors, and they want a good one. If you have to tell them theirs is being assigned by lottery, they won’t be as happy than if you can provide the name and a little information about the doctor they can expect to see the next day.
When the patients I admit late last evening ask who would see them the next day, I’m glad when I can provide a name and a little more information. I say something like, “I won’t see you after tonight, but my partner, Dr. Shawn Lee, will be instead. That means you’re getting an upgrade! Not only is he a really nice guy, he’s voted one of Seattle’s best doctors every year. He’ll do a great job for you.”
To make this communication effective, the night doctor has to know which hospitalist takes over the next morning and has a list indicating which day doctor will get the first, second, third new patient, and so on, admitted during the night. This is possible if patients are assigned by a predetermined algorithm, or if the day doctors have their load-leveling meeting at the end of each day shift, rather than in the morning, to create a list telling the night doctor which day hospitalist he should admit the first and subsequent patents to. That way, the night doctor can write in the admitting orders at 1 a.m. “admit to Dr. X.” This eliminates confusion on the part of other hospital staff who need to know who to call about a patient after the start of the day shift.
Next month I will look at special circumstances, and some pros and cons of having an individual hospitalist take on the care of more patients at the beginning of consecutive day shifts, and exempting them from taking on new patients on the last day or two before rotating off. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Second of a three-part series.
As I mentioned last month, there isn’t a proven best method to use when distributing new referrals among your group’s providers. The popular methods fall along a continuum of being focused on daily, or continuous, leveling of patient loads between providers (“load leveling”) at one end; at the other end of the continuum is having a doctor be “on” for all new referrals for a predetermined time period, and accepting that patient volumes might be uneven day to day but tend to even out over long periods.
There might not be any reason to change your group’s approach to patient assignment, but you should always be thinking about how your own methods might be changed or improved. I have shared (“Bigger Isn’t Always Better,” June 2009, p. 46) my concern that some groups invest far too much time in a morning load-leveling and handoff conference. Make sure your group is using only as much time as needed.
Air-Traffic Controllers
Many large groups (e.g., more than 15 full-time equivalents) that assign patients to providers in sequence, like dealing a deck of cards, have a designated provider who holds the triage pager and serves as “air-traffic controller.” This person typically takes incoming calls about all new referrals, jots down the relevant clinical data, keeps track of which hospitalist is due to take the next patient, pages that person, and repeats the clinical information. As I’ve written before (“How to Hire and Use Clerical Staff,” June 2007, p. 73), many practices have found that during business hours, they can hand this role to a clerical person who simply takes down the name and phone number of the doctor making the referral, then pages that information to the hospitalist due to get the next patient. The hospitalist then calls and speaks directly with the referring doctor.
Small- to medium-sized groups can eliminate entirely the need for any such “air-traffic control” function if they assign all new referrals to a single doctor for specified periods of time. For example, from 7 a.m. to 3 p.m. today, all new referrals go to Dr. Glass, and from 3 p.m. to 11 p.m., they go to Dr. Cage.
Admitter-Rounder Duties
Many—maybe most?—large groups separate daytime admitter and rounder functions so that on any given day, a hospitalist does one but not both. The principal advantages of this approach are reducing the stress on, and possibly increasing the efficiency of, rounding doctors by shielding them from the unpredictable and time-consuming interruption of needing to admit a new patient. And a daytime doctor who only does admissions might be able to start seeing a patient in the ED more quickly than one who is busy making rounds.
Any increased availability of admitters to the ED could be offset by their lack of surge capacity leading to a bottleneck in ED throughput when there are many patients to admit at the same time and a limited number of admitters (often only one). Such a bottleneck would be much less likely if all daytime doctors (i.e., the rounders) were available to see admissions rather than just admitters.
Continuity of care suffers when a group has separate admitters and rounders, because no patients will be seen by the same doctor on the day of admission and the day following. This method requires a handoff from the day of admission to the next day. Such a handoff might be unavoidable for patients admitted during the night, but this doesn’t have to occur when patients are admitted during the daytime.
Who’s Seeing this Patient?
It seems to make sense to wait until each morning to distribute patients. That allows the practice to know just how many new patients there are, and they can be distributed according to complexity and whether a hospitalist has formed a previous relationship with that patient. But it means that no one at the hospital will know which hospitalist is caring for the patient until later in the morning. For example, if the radiologist is over-reading a study done during the night and finds something worthy of a phone call to the hospitalist, no one is sure who should get the call. A patient might develop hypoglycemia shortly after the hospitalist night shift is over, but the nurse doesn’t know which hospitalist to call.
And, perhaps most importantly, if patients aren’t distributed until the start of the day shift, the night hospitalist can’t tell the patient and family which hospitalist to expect the next morning. To test the significance of this issue, I conducted an experiment while working our group’s late-evening admitter shift. I concluded my visit with each admitted patient by explaining, “I am on-call for our group tonight, so I will be off recovering tomorrow. Therefore, I won’t see you again, but one of my partners will take over in the morning. Do you have any questions for me?” Every patient I admitted had the same question. “What is that doctor’s name?”
How does your group answer a patient who asks which hospitalist will be in the next day? If your method is load-leveling in the morning, then the best answer your night admitting doctor can give is probably to say: “I don’t know which of my partners will be in. There are several working tomorrow, and at the start of the day, they will divide up the patients who come in tonight depending on how busy each of them is. But all the doctors in our group are terrific and will take good care of you.”
I’m told the same thing when I get my hair cut: You’ll get whichever “hair artist” is up next. I put up with it at the hair place because it costs less than $15. But I still find it a little irritating. I’m sure all the barbers aren’t equally skilled or diligent, and I want the best one. (Maybe I shouldn’t care since there isn’t much that can be done with my hair.) I’m pretty sure patients feel the same way about which doctor they get. The public is convinced there is a wide variety in the quality of doctors, and they want a good one. If you have to tell them theirs is being assigned by lottery, they won’t be as happy than if you can provide the name and a little information about the doctor they can expect to see the next day.
When the patients I admit late last evening ask who would see them the next day, I’m glad when I can provide a name and a little more information. I say something like, “I won’t see you after tonight, but my partner, Dr. Shawn Lee, will be instead. That means you’re getting an upgrade! Not only is he a really nice guy, he’s voted one of Seattle’s best doctors every year. He’ll do a great job for you.”
To make this communication effective, the night doctor has to know which hospitalist takes over the next morning and has a list indicating which day doctor will get the first, second, third new patient, and so on, admitted during the night. This is possible if patients are assigned by a predetermined algorithm, or if the day doctors have their load-leveling meeting at the end of each day shift, rather than in the morning, to create a list telling the night doctor which day hospitalist he should admit the first and subsequent patents to. That way, the night doctor can write in the admitting orders at 1 a.m. “admit to Dr. X.” This eliminates confusion on the part of other hospital staff who need to know who to call about a patient after the start of the day shift.
Next month I will look at special circumstances, and some pros and cons of having an individual hospitalist take on the care of more patients at the beginning of consecutive day shifts, and exempting them from taking on new patients on the last day or two before rotating off. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Second of a three-part series.
As I mentioned last month, there isn’t a proven best method to use when distributing new referrals among your group’s providers. The popular methods fall along a continuum of being focused on daily, or continuous, leveling of patient loads between providers (“load leveling”) at one end; at the other end of the continuum is having a doctor be “on” for all new referrals for a predetermined time period, and accepting that patient volumes might be uneven day to day but tend to even out over long periods.
There might not be any reason to change your group’s approach to patient assignment, but you should always be thinking about how your own methods might be changed or improved. I have shared (“Bigger Isn’t Always Better,” June 2009, p. 46) my concern that some groups invest far too much time in a morning load-leveling and handoff conference. Make sure your group is using only as much time as needed.
Air-Traffic Controllers
Many large groups (e.g., more than 15 full-time equivalents) that assign patients to providers in sequence, like dealing a deck of cards, have a designated provider who holds the triage pager and serves as “air-traffic controller.” This person typically takes incoming calls about all new referrals, jots down the relevant clinical data, keeps track of which hospitalist is due to take the next patient, pages that person, and repeats the clinical information. As I’ve written before (“How to Hire and Use Clerical Staff,” June 2007, p. 73), many practices have found that during business hours, they can hand this role to a clerical person who simply takes down the name and phone number of the doctor making the referral, then pages that information to the hospitalist due to get the next patient. The hospitalist then calls and speaks directly with the referring doctor.
Small- to medium-sized groups can eliminate entirely the need for any such “air-traffic control” function if they assign all new referrals to a single doctor for specified periods of time. For example, from 7 a.m. to 3 p.m. today, all new referrals go to Dr. Glass, and from 3 p.m. to 11 p.m., they go to Dr. Cage.
Admitter-Rounder Duties
Many—maybe most?—large groups separate daytime admitter and rounder functions so that on any given day, a hospitalist does one but not both. The principal advantages of this approach are reducing the stress on, and possibly increasing the efficiency of, rounding doctors by shielding them from the unpredictable and time-consuming interruption of needing to admit a new patient. And a daytime doctor who only does admissions might be able to start seeing a patient in the ED more quickly than one who is busy making rounds.
Any increased availability of admitters to the ED could be offset by their lack of surge capacity leading to a bottleneck in ED throughput when there are many patients to admit at the same time and a limited number of admitters (often only one). Such a bottleneck would be much less likely if all daytime doctors (i.e., the rounders) were available to see admissions rather than just admitters.
Continuity of care suffers when a group has separate admitters and rounders, because no patients will be seen by the same doctor on the day of admission and the day following. This method requires a handoff from the day of admission to the next day. Such a handoff might be unavoidable for patients admitted during the night, but this doesn’t have to occur when patients are admitted during the daytime.
Who’s Seeing this Patient?
It seems to make sense to wait until each morning to distribute patients. That allows the practice to know just how many new patients there are, and they can be distributed according to complexity and whether a hospitalist has formed a previous relationship with that patient. But it means that no one at the hospital will know which hospitalist is caring for the patient until later in the morning. For example, if the radiologist is over-reading a study done during the night and finds something worthy of a phone call to the hospitalist, no one is sure who should get the call. A patient might develop hypoglycemia shortly after the hospitalist night shift is over, but the nurse doesn’t know which hospitalist to call.
And, perhaps most importantly, if patients aren’t distributed until the start of the day shift, the night hospitalist can’t tell the patient and family which hospitalist to expect the next morning. To test the significance of this issue, I conducted an experiment while working our group’s late-evening admitter shift. I concluded my visit with each admitted patient by explaining, “I am on-call for our group tonight, so I will be off recovering tomorrow. Therefore, I won’t see you again, but one of my partners will take over in the morning. Do you have any questions for me?” Every patient I admitted had the same question. “What is that doctor’s name?”
How does your group answer a patient who asks which hospitalist will be in the next day? If your method is load-leveling in the morning, then the best answer your night admitting doctor can give is probably to say: “I don’t know which of my partners will be in. There are several working tomorrow, and at the start of the day, they will divide up the patients who come in tonight depending on how busy each of them is. But all the doctors in our group are terrific and will take good care of you.”
I’m told the same thing when I get my hair cut: You’ll get whichever “hair artist” is up next. I put up with it at the hair place because it costs less than $15. But I still find it a little irritating. I’m sure all the barbers aren’t equally skilled or diligent, and I want the best one. (Maybe I shouldn’t care since there isn’t much that can be done with my hair.) I’m pretty sure patients feel the same way about which doctor they get. The public is convinced there is a wide variety in the quality of doctors, and they want a good one. If you have to tell them theirs is being assigned by lottery, they won’t be as happy than if you can provide the name and a little information about the doctor they can expect to see the next day.
When the patients I admit late last evening ask who would see them the next day, I’m glad when I can provide a name and a little more information. I say something like, “I won’t see you after tonight, but my partner, Dr. Shawn Lee, will be instead. That means you’re getting an upgrade! Not only is he a really nice guy, he’s voted one of Seattle’s best doctors every year. He’ll do a great job for you.”
To make this communication effective, the night doctor has to know which hospitalist takes over the next morning and has a list indicating which day doctor will get the first, second, third new patient, and so on, admitted during the night. This is possible if patients are assigned by a predetermined algorithm, or if the day doctors have their load-leveling meeting at the end of each day shift, rather than in the morning, to create a list telling the night doctor which day hospitalist he should admit the first and subsequent patents to. That way, the night doctor can write in the admitting orders at 1 a.m. “admit to Dr. X.” This eliminates confusion on the part of other hospital staff who need to know who to call about a patient after the start of the day shift.
Next month I will look at special circumstances, and some pros and cons of having an individual hospitalist take on the care of more patients at the beginning of consecutive day shifts, and exempting them from taking on new patients on the last day or two before rotating off. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.