User login
Health disparities in rural America: Chronic conditions
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
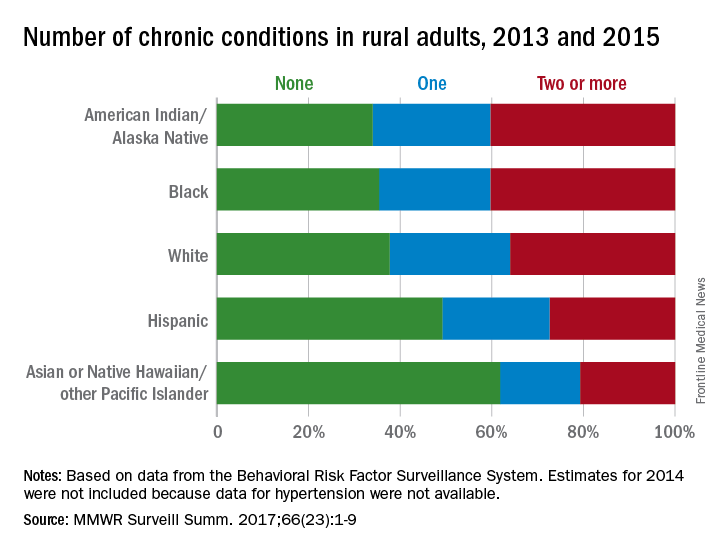
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
Among rural adults, multiple chronic health conditions are most common in non-Hispanic blacks and American Indians/Alaska Natives (AI/ANs) and least common among Asians and Native Hawaiians/other Pacific Islanders (NHOPIs), according to the Centers for Disease Control and Prevention.
The order was reversed for adults reporting no chronic conditions: Asians and NHOPIs at 61.8%, Hispanics at 49.2%, whites at 37.8%, blacks at 35.4%, and AI/ANs at 34.0%, the researchers said.
For the chronic health conditions included separately in the report, blacks had the highest rate (45.9%) and Asians and NHOPIs had the lowest rate (15.5%) of obesity; AI/ANs were most likely (23.2%) and Asians and NHOPIs were least likely (5.8%) to report depressive disorder. Other conditions considered in the estimates were myocardial infarction; coronary heart disease; stroke; hypertension; asthma; skin cancer; other types of cancer; chronic obstructive pulmonary disease; kidney disease; some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia; and diabetes. Estimates for 2014 were not included because data for hypertension were not available, the investigators noted.
Of the 3,143 counties categorized by the National Center for Health Statistics’ Urban-Rural Classification Scheme for Counties, a total of 1,325 were considered rural and included 6.1% of the U.S. population, they said.
FROM MMWR SURVEILLANCE SUMMARIES
Acute kidney injury linked with doubled inpatient VTEs
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.

He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.
He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Hospitalized patients with acute kidney injury had more than double the inpatient rate of venous thromboembolism as had patients without acute kidney injury in a prospective, observational study of more than 6,000 hospitalized U.S. soldiers.
He offered four possible mechanisms to explain a link between AKI and VTE:
- Patients with AKI are in a hypercoagulable state.
- AKI alters the pharmacodynamics or pharmacokinetics of VTE prophylactic treatments.
- AKI is a marker of an illness that causes VTE.
- VTE leads to an increased rate of AKI rather than the other way around.
Dr. McMahon’s analysis also revealed that two other clinical conditions that are generally believed to raise VTE risk – obesity and impaired overall renal function identified with stagnant measures – did not correspond with a significantly elevated VTE rate in this study.
The data came from 6,552 adults hospitalized for at least 2 days at Walter Reed between September 2009 and March 2011. The study excluded patients with VTE at the time of admission and also those who had been treated with an anticoagulant at the time of admission. The patients averaged 55 years of age and were hospitalized for a median of 4 days. About 22% of patients received VTE prophylaxis with unfractionated heparin, about 41% received prophylaxis with low-molecular-weight heparin, and about 39% received no VTE prophylaxis (percentages total 102% because of rounding).
About 16% of the patients had been diagnosed with AKI at the time of admission, and an additional 8% developed AKI while hospitalized, defined as an increase in serum creatinine during hospitalization of at least 50% above baseline levels or an increase of more than 0.3 mg/dL above the level at time of admission. During hospitalization, 160 patients (2%) developed a new onset VTE.
In an analysis that adjusted for baseline differences in type of surgery, body mass index, sex, age, and prior hospitalizations during the prior 90 days, the results showed that patients with preexisting or new onset AKI had a 2.2-fold higher rate of VTE, compared with patients without AKI, and this difference was statistically significant, Dr. McMahon reported.
The analysis also showed a significant 62% relatively higher rate of VTE among soldiers hospitalized for a deployment-related event, as well as a significant 63% relatively lower VTE rate among patients not receiving medical prophylaxis, compared with patients receiving an anticoagulant. Dr. McMahon suggested that this lower rate of VTEs among patients not on prophylaxis reflected success in identifying which patients had an increased risk for VTE and hence received prophylaxis.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Inpatients with AKI had an adjusted 2.2-fold higher rate of VTE, compared with other inpatients.
Data source: Prospective, observational data from 6,552 inpatients at a single U.S. military hospital.
Disclosures: Dr. McMahon had no disclosures.
Reducing the Stigma of HIV Testing With Online Support
Adolescents are one of the highest risk groups for HIV, but they often don’t want to talk about it. They also don’t want to get tested—of 40% of high school students who had had intercourse, only 10% had been tested, according to a CDC study.
Are online forums the solution? They offer anonymity along with information, and many adolescents—if not most—are used to getting information from social media. Researchers from University of California in Davis, say there’s a real need for a reliable source of advice on the subject for that audience. Most online forums for adolescent message boards and websites revolve around pregnancy and birth control rather than STDs.
The researchers noted that higher levels of stigma surrounding HIV correlate with lower levels of HIV testing. Even the testing is stigmatized, because many people feel just getting the test creates the impression that they are promiscuous, for instance. They also fear what the test may tell them and that it might be used against them in employment or health insurance.
The researchers analyzed 201 threads and 319 posts. Among 7 forums, 2 (POZ, MedHelp) were monitored by counselors, and 4 (DailyStrength, eHealth Forum, HealingWell, and HealthBoards) were monitored by members. One (The Body) was monitored by counselors and members.
In 13 threads, users displayed a “self-stigmatizing attitude” toward HIV testing, mainly because of the fear of being diagnosed. Others feared losing employment or having relationships affected. Notably, no adolescents asked about HIV testing in the forums targeted at their age groups. It is important to increase the visibility of HIV-related resources in adolescents’ forums, the researchers say; the lack of available information online may “perpetuate the taboo among this population by conveying a deeper stigma toward HIV.”
The study showed that the level of stigmatization differed significantly based on who monitored the session: The threads maintained by members had fewer stigmatized posts. The researchers suggest that if health care professionals get more involved by collaborating with forums to provide more content and framing HIV testing as a regular preventive checkup, they may reduce the stigma. Health care professionals also may be able to identify those who suspect they have HIV and encourage them to get tested. Health care professionals also can initiate threads that invite open discussion of HIV-related topics in sexual education forums devoted to adolescents. The researchers say breaking the online silence will lead more people to timely testing.
Source:
Ho CL, Pan W, Taylor LD. J Psychosoc Nurs Ment Health Serv. 2017;55(12):34-43.
doi: 10.3928/02793695-20170905-01.
Adolescents are one of the highest risk groups for HIV, but they often don’t want to talk about it. They also don’t want to get tested—of 40% of high school students who had had intercourse, only 10% had been tested, according to a CDC study.
Are online forums the solution? They offer anonymity along with information, and many adolescents—if not most—are used to getting information from social media. Researchers from University of California in Davis, say there’s a real need for a reliable source of advice on the subject for that audience. Most online forums for adolescent message boards and websites revolve around pregnancy and birth control rather than STDs.
The researchers noted that higher levels of stigma surrounding HIV correlate with lower levels of HIV testing. Even the testing is stigmatized, because many people feel just getting the test creates the impression that they are promiscuous, for instance. They also fear what the test may tell them and that it might be used against them in employment or health insurance.
The researchers analyzed 201 threads and 319 posts. Among 7 forums, 2 (POZ, MedHelp) were monitored by counselors, and 4 (DailyStrength, eHealth Forum, HealingWell, and HealthBoards) were monitored by members. One (The Body) was monitored by counselors and members.
In 13 threads, users displayed a “self-stigmatizing attitude” toward HIV testing, mainly because of the fear of being diagnosed. Others feared losing employment or having relationships affected. Notably, no adolescents asked about HIV testing in the forums targeted at their age groups. It is important to increase the visibility of HIV-related resources in adolescents’ forums, the researchers say; the lack of available information online may “perpetuate the taboo among this population by conveying a deeper stigma toward HIV.”
The study showed that the level of stigmatization differed significantly based on who monitored the session: The threads maintained by members had fewer stigmatized posts. The researchers suggest that if health care professionals get more involved by collaborating with forums to provide more content and framing HIV testing as a regular preventive checkup, they may reduce the stigma. Health care professionals also may be able to identify those who suspect they have HIV and encourage them to get tested. Health care professionals also can initiate threads that invite open discussion of HIV-related topics in sexual education forums devoted to adolescents. The researchers say breaking the online silence will lead more people to timely testing.
Source:
Ho CL, Pan W, Taylor LD. J Psychosoc Nurs Ment Health Serv. 2017;55(12):34-43.
doi: 10.3928/02793695-20170905-01.
Adolescents are one of the highest risk groups for HIV, but they often don’t want to talk about it. They also don’t want to get tested—of 40% of high school students who had had intercourse, only 10% had been tested, according to a CDC study.
Are online forums the solution? They offer anonymity along with information, and many adolescents—if not most—are used to getting information from social media. Researchers from University of California in Davis, say there’s a real need for a reliable source of advice on the subject for that audience. Most online forums for adolescent message boards and websites revolve around pregnancy and birth control rather than STDs.
The researchers noted that higher levels of stigma surrounding HIV correlate with lower levels of HIV testing. Even the testing is stigmatized, because many people feel just getting the test creates the impression that they are promiscuous, for instance. They also fear what the test may tell them and that it might be used against them in employment or health insurance.
The researchers analyzed 201 threads and 319 posts. Among 7 forums, 2 (POZ, MedHelp) were monitored by counselors, and 4 (DailyStrength, eHealth Forum, HealingWell, and HealthBoards) were monitored by members. One (The Body) was monitored by counselors and members.
In 13 threads, users displayed a “self-stigmatizing attitude” toward HIV testing, mainly because of the fear of being diagnosed. Others feared losing employment or having relationships affected. Notably, no adolescents asked about HIV testing in the forums targeted at their age groups. It is important to increase the visibility of HIV-related resources in adolescents’ forums, the researchers say; the lack of available information online may “perpetuate the taboo among this population by conveying a deeper stigma toward HIV.”
The study showed that the level of stigmatization differed significantly based on who monitored the session: The threads maintained by members had fewer stigmatized posts. The researchers suggest that if health care professionals get more involved by collaborating with forums to provide more content and framing HIV testing as a regular preventive checkup, they may reduce the stigma. Health care professionals also may be able to identify those who suspect they have HIV and encourage them to get tested. Health care professionals also can initiate threads that invite open discussion of HIV-related topics in sexual education forums devoted to adolescents. The researchers say breaking the online silence will lead more people to timely testing.
Source:
Ho CL, Pan W, Taylor LD. J Psychosoc Nurs Ment Health Serv. 2017;55(12):34-43.
doi: 10.3928/02793695-20170905-01.
Attack on asthma: Scrubbing homes of allergens may tame disease and its costs
After years of studying the causes of asthma, a pediatrician-turned-public health sleuth thinks there’s a way to substantially reduce its impact.
But the approach faces a big hurdle: getting someone to pay for it, said Elizabeth C. Matsui, MD, a professor at Johns Hopkins University in Baltimore.
Dr. Matsui, who suffered from asthma as a child, has spent much of her career studying the link between poor housing and asthma in low-income neighborhoods. In particular, she’s looked at the effects of mouse allergens, typically found in high concentrations in urban homes.
Dr. Matsui cited a 2004 study in the New England Journal of Medicine that described measures to reduce home allergen levels and concluded that they were linked to reductions in asthma symptoms.
That research “was highly successful and impactful,” but the approach wasn’t widely adopted, according to Dr. Matsui.
“So here we have this trial that was published more than 10 years ago that shows [indoor allergen control] works,” said Dr. Matsui, who did not participate in the study. “But the families who need it most can’t afford to do these things, don’t have control oftentimes over their home environment, and insurance or other payers don’t cover these things.”
Dr. Matsui has proposed new incentives for hospitals to provide home intervention, including Medicaid waivers. But, she said, scientists can’t use research money for these programs. “Delivery of community health care programs would require a different type of funding.”
As a result, doctors and scientists doubted if a plan to control home allergens would scale up, and insurers questioned whether benefits to their bottom line would justify the added cost.
“We have this enormous public health problem in that there are housing conditions that directly affect allergen exposure in this population of kids,” Dr. Matsui said. “We have dedicated individuals and groups who are trying to solve the problem. But we don’t have a system that is able to solve the problem.”
A 2017 study by Dr. Matsui, published in JAMA, suggests that even without intensive professional cleaning services, families that receive some training can substantially reduce home allergens on their own.
That finding suggests health agencies should routinely offer to educate asthma-affected families in home allergen control. “There’s potentially a large benefit,” Dr. Matsui said.
In a separate study, Dr. Matsui’s group is following 200 Baltimore children to see if those in homes scrubbed of allergens need fewer treatments with rescue inhalers. If they do, that could give health insurers an incentive to pay for the approach.
There’s another incentive: Clearing the air in a child’s home may be critical in cases where medications alone don’t work. “We continue to see a lot of kids that, despite being on medication, don’t have well-controlled asthma,” Dr. Matsui said.
Asthma drugs can also have serious side effects, she said, especially at higher doses, and may suppress symptoms without halting lung damage.
Dr. Matsui’s work on asthma began while working as a pediatrician at Baltimore’s Franklin Square Hospital in 1998. As part of her job, she spent a half-day each week in a school health clinic in a low-income area.
Dr. Matsui was struck by the number of kids she saw with severe asthma, she said, and set up a home health visit program to help them. But she wasn’t certain the program was working, so she consulted with experts at Hopkins.
In 2004, she earned a master’s from the Johns Hopkins School of Public Health. Today, she is one of the nation’s leading asthma researchers.
Dr. Matsui said her career was shaped by her own struggle with childhood asthma. “I think that that probably played a role, consciously or unconsciously,” she said.
KHN’s coverage of health disparities in east Baltimore is supported by The Annie E. Casey Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Environment is certainly a factor in asthma control. We are lucky enough to have a network in our county that will take pediatric asthma cases to help with asthma education. The nurse will even accompany the child and parent to their outpatient visits to help advocate for help with their asthma management and go into the home to see if there is a cockroach problem or a dusty environment, for example. They will also help families learn how to better organize the child’s bedroom so there is less dust! Some Medicaid HMOs will pay for this care management plan but not all of the insurances in our area.

Environment is certainly a factor in asthma control. We are lucky enough to have a network in our county that will take pediatric asthma cases to help with asthma education. The nurse will even accompany the child and parent to their outpatient visits to help advocate for help with their asthma management and go into the home to see if there is a cockroach problem or a dusty environment, for example. They will also help families learn how to better organize the child’s bedroom so there is less dust! Some Medicaid HMOs will pay for this care management plan but not all of the insurances in our area.
Environment is certainly a factor in asthma control. We are lucky enough to have a network in our county that will take pediatric asthma cases to help with asthma education. The nurse will even accompany the child and parent to their outpatient visits to help advocate for help with their asthma management and go into the home to see if there is a cockroach problem or a dusty environment, for example. They will also help families learn how to better organize the child’s bedroom so there is less dust! Some Medicaid HMOs will pay for this care management plan but not all of the insurances in our area.
After years of studying the causes of asthma, a pediatrician-turned-public health sleuth thinks there’s a way to substantially reduce its impact.
But the approach faces a big hurdle: getting someone to pay for it, said Elizabeth C. Matsui, MD, a professor at Johns Hopkins University in Baltimore.
Dr. Matsui, who suffered from asthma as a child, has spent much of her career studying the link between poor housing and asthma in low-income neighborhoods. In particular, she’s looked at the effects of mouse allergens, typically found in high concentrations in urban homes.
Dr. Matsui cited a 2004 study in the New England Journal of Medicine that described measures to reduce home allergen levels and concluded that they were linked to reductions in asthma symptoms.
That research “was highly successful and impactful,” but the approach wasn’t widely adopted, according to Dr. Matsui.
“So here we have this trial that was published more than 10 years ago that shows [indoor allergen control] works,” said Dr. Matsui, who did not participate in the study. “But the families who need it most can’t afford to do these things, don’t have control oftentimes over their home environment, and insurance or other payers don’t cover these things.”
Dr. Matsui has proposed new incentives for hospitals to provide home intervention, including Medicaid waivers. But, she said, scientists can’t use research money for these programs. “Delivery of community health care programs would require a different type of funding.”
As a result, doctors and scientists doubted if a plan to control home allergens would scale up, and insurers questioned whether benefits to their bottom line would justify the added cost.
“We have this enormous public health problem in that there are housing conditions that directly affect allergen exposure in this population of kids,” Dr. Matsui said. “We have dedicated individuals and groups who are trying to solve the problem. But we don’t have a system that is able to solve the problem.”
A 2017 study by Dr. Matsui, published in JAMA, suggests that even without intensive professional cleaning services, families that receive some training can substantially reduce home allergens on their own.
That finding suggests health agencies should routinely offer to educate asthma-affected families in home allergen control. “There’s potentially a large benefit,” Dr. Matsui said.
In a separate study, Dr. Matsui’s group is following 200 Baltimore children to see if those in homes scrubbed of allergens need fewer treatments with rescue inhalers. If they do, that could give health insurers an incentive to pay for the approach.
There’s another incentive: Clearing the air in a child’s home may be critical in cases where medications alone don’t work. “We continue to see a lot of kids that, despite being on medication, don’t have well-controlled asthma,” Dr. Matsui said.
Asthma drugs can also have serious side effects, she said, especially at higher doses, and may suppress symptoms without halting lung damage.
Dr. Matsui’s work on asthma began while working as a pediatrician at Baltimore’s Franklin Square Hospital in 1998. As part of her job, she spent a half-day each week in a school health clinic in a low-income area.
Dr. Matsui was struck by the number of kids she saw with severe asthma, she said, and set up a home health visit program to help them. But she wasn’t certain the program was working, so she consulted with experts at Hopkins.
In 2004, she earned a master’s from the Johns Hopkins School of Public Health. Today, she is one of the nation’s leading asthma researchers.
Dr. Matsui said her career was shaped by her own struggle with childhood asthma. “I think that that probably played a role, consciously or unconsciously,” she said.
KHN’s coverage of health disparities in east Baltimore is supported by The Annie E. Casey Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
After years of studying the causes of asthma, a pediatrician-turned-public health sleuth thinks there’s a way to substantially reduce its impact.
But the approach faces a big hurdle: getting someone to pay for it, said Elizabeth C. Matsui, MD, a professor at Johns Hopkins University in Baltimore.
Dr. Matsui, who suffered from asthma as a child, has spent much of her career studying the link between poor housing and asthma in low-income neighborhoods. In particular, she’s looked at the effects of mouse allergens, typically found in high concentrations in urban homes.
Dr. Matsui cited a 2004 study in the New England Journal of Medicine that described measures to reduce home allergen levels and concluded that they were linked to reductions in asthma symptoms.
That research “was highly successful and impactful,” but the approach wasn’t widely adopted, according to Dr. Matsui.
“So here we have this trial that was published more than 10 years ago that shows [indoor allergen control] works,” said Dr. Matsui, who did not participate in the study. “But the families who need it most can’t afford to do these things, don’t have control oftentimes over their home environment, and insurance or other payers don’t cover these things.”
Dr. Matsui has proposed new incentives for hospitals to provide home intervention, including Medicaid waivers. But, she said, scientists can’t use research money for these programs. “Delivery of community health care programs would require a different type of funding.”
As a result, doctors and scientists doubted if a plan to control home allergens would scale up, and insurers questioned whether benefits to their bottom line would justify the added cost.
“We have this enormous public health problem in that there are housing conditions that directly affect allergen exposure in this population of kids,” Dr. Matsui said. “We have dedicated individuals and groups who are trying to solve the problem. But we don’t have a system that is able to solve the problem.”
A 2017 study by Dr. Matsui, published in JAMA, suggests that even without intensive professional cleaning services, families that receive some training can substantially reduce home allergens on their own.
That finding suggests health agencies should routinely offer to educate asthma-affected families in home allergen control. “There’s potentially a large benefit,” Dr. Matsui said.
In a separate study, Dr. Matsui’s group is following 200 Baltimore children to see if those in homes scrubbed of allergens need fewer treatments with rescue inhalers. If they do, that could give health insurers an incentive to pay for the approach.
There’s another incentive: Clearing the air in a child’s home may be critical in cases where medications alone don’t work. “We continue to see a lot of kids that, despite being on medication, don’t have well-controlled asthma,” Dr. Matsui said.
Asthma drugs can also have serious side effects, she said, especially at higher doses, and may suppress symptoms without halting lung damage.
Dr. Matsui’s work on asthma began while working as a pediatrician at Baltimore’s Franklin Square Hospital in 1998. As part of her job, she spent a half-day each week in a school health clinic in a low-income area.
Dr. Matsui was struck by the number of kids she saw with severe asthma, she said, and set up a home health visit program to help them. But she wasn’t certain the program was working, so she consulted with experts at Hopkins.
In 2004, she earned a master’s from the Johns Hopkins School of Public Health. Today, she is one of the nation’s leading asthma researchers.
Dr. Matsui said her career was shaped by her own struggle with childhood asthma. “I think that that probably played a role, consciously or unconsciously,” she said.
KHN’s coverage of health disparities in east Baltimore is supported by The Annie E. Casey Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
More states allowing pharmacists to administer vaccines to younger patients
.
Since the 1990s, states have made laws to increase access to immunization services by giving pharmacists authority to give vaccines, said Cason D. Schmit, JD, of Texas A&M University at College Station, and Matthew S. Penn, JD, director of the Public Health Law Program at the Centers for Disease Control and Prevention, Atlanta. This has the advantage of pharmacies being open longer hours than most physicians’ offices, in addition to the opportunities for immunizing people in rural locations as well as those people without a regular physician.
Yet barriers to pharmacists’ providing immunization services remain because of some state laws. Laws in nine states that prevent pharmacists from vaccinating patients younger than age 18 years keep pharmacists from administering any of the vaccines listed in the 2016 Advisory Committee of Immunization Practices child immunization schedule. The two states in which pharmacists can vaccinate patients as young as 14 years allow the pharmacists to administer only the recommended booster for meningococcal vaccine and annual influenza vaccines for children. And the 15 states with minimum patient age restrictions for 7- to 12-year-oldss allow pharmacists to administer only the four vaccines ACIP recommends on the 2016 schedule for children (meningococcal, Tdap, human papillomavirus, and annual influenza vaccines).
Read more in the Journal of the American Pharmacists Association (2017 Nov-Dec;57[6]:661-9).
.
Since the 1990s, states have made laws to increase access to immunization services by giving pharmacists authority to give vaccines, said Cason D. Schmit, JD, of Texas A&M University at College Station, and Matthew S. Penn, JD, director of the Public Health Law Program at the Centers for Disease Control and Prevention, Atlanta. This has the advantage of pharmacies being open longer hours than most physicians’ offices, in addition to the opportunities for immunizing people in rural locations as well as those people without a regular physician.
Yet barriers to pharmacists’ providing immunization services remain because of some state laws. Laws in nine states that prevent pharmacists from vaccinating patients younger than age 18 years keep pharmacists from administering any of the vaccines listed in the 2016 Advisory Committee of Immunization Practices child immunization schedule. The two states in which pharmacists can vaccinate patients as young as 14 years allow the pharmacists to administer only the recommended booster for meningococcal vaccine and annual influenza vaccines for children. And the 15 states with minimum patient age restrictions for 7- to 12-year-oldss allow pharmacists to administer only the four vaccines ACIP recommends on the 2016 schedule for children (meningococcal, Tdap, human papillomavirus, and annual influenza vaccines).
Read more in the Journal of the American Pharmacists Association (2017 Nov-Dec;57[6]:661-9).
.
Since the 1990s, states have made laws to increase access to immunization services by giving pharmacists authority to give vaccines, said Cason D. Schmit, JD, of Texas A&M University at College Station, and Matthew S. Penn, JD, director of the Public Health Law Program at the Centers for Disease Control and Prevention, Atlanta. This has the advantage of pharmacies being open longer hours than most physicians’ offices, in addition to the opportunities for immunizing people in rural locations as well as those people without a regular physician.
Yet barriers to pharmacists’ providing immunization services remain because of some state laws. Laws in nine states that prevent pharmacists from vaccinating patients younger than age 18 years keep pharmacists from administering any of the vaccines listed in the 2016 Advisory Committee of Immunization Practices child immunization schedule. The two states in which pharmacists can vaccinate patients as young as 14 years allow the pharmacists to administer only the recommended booster for meningococcal vaccine and annual influenza vaccines for children. And the 15 states with minimum patient age restrictions for 7- to 12-year-oldss allow pharmacists to administer only the four vaccines ACIP recommends on the 2016 schedule for children (meningococcal, Tdap, human papillomavirus, and annual influenza vaccines).
Read more in the Journal of the American Pharmacists Association (2017 Nov-Dec;57[6]:661-9).
FROM THE JOURNAL OF THE AMERICAN PHARMACISTS ASSOCIATION
Pulmonary hypertension treatment gets under the skin
Pulmonary arterial hypertension (PAH) patients with moderate, stable disease can benefit from an implantable drug delivery system, based on data from a review of 60 adults with successful implantations. The findings were published in the December issue of CHEST.
“A fully implanted system offers patients the hope of returning to more normal activities such as bathing, swimming, and reduced risk of infections from externalized central venous catheter contamination or reduced subcutaneous pain from subcutaneous infusion,” wrote Aaron B. Waxman, MD, PhD, of Brigham and Women’s Hospital, Boston, and his colleagues (Chest. 2017 June 3. doi: 10.1016/j.chest.2017.04.188).
In the DelIVery Trial, clinicians at 10 locations in the United States placed a fully implantable delivery system in adults aged 18 years and older with stable PAH who were previously receiving treprostinil via an external pump at an average dose of 71 ng/kg per min.
All 60 patients were successfully implanted with a system consisting of a drug infusion pump placed in an abdominal pocket and an intravascular catheter linking the implanted pump to the superior vena cava.
“The location of the pump pocket was determined in partnership with the patient and was based on consideration of clothing styles, belt line and subcutaneous fat depth,” the researchers noted.
Procedure-related complications deemed clinically significant included one atrial fibrillation, two incidences of pneumothorax, two infections unrelated to catheter placement, and three catheter dislocations (two in the same patient). The most common patient complaints were expected implant site pain in 83% and bruising in 17%.
The findings were limited by the small number of patients, but the researchers identified several factors that contributed to the success of the procedure, including selecting patients who have shown response to treprostinil and are motivated to comply with pump refill visits, performing the procedure at centers with a high volume of PAH patients, keeping the procedure consistent for each patient, and using the same implant team in each case. “The implant procedure was successfully performed with a low complication rate by clinicians with a diverse range of specialty training,” the researchers added.
Patients reported satisfaction with the implant system at 6 weeks and 6 months, and said they spent an average of 75% less time managing their delivery system, according to previously published data on the patients’ perspective (CHEST 2016;150[1]:27-34).
Medtronic sponsored the study. The lead author, Dr. Waxman, had no financial conflicts to disclose; several coauthors reported relationships with companies including Medtronic, Actelion, Bayer, Gilead, Merck, and United Therapeutics.
The development of an implantable therapy for pulmonary hypertension could expand the use of treprostinil, a demonstrated effective treatment for PAH that has been limited in its use because of a range of side effects when given intravenously, orally, subcutaneously, or by inhalation, Joel A. Wirth, MD, FCCP, and Harold I. Palevsky, MD, FCCP, wrote in an editorial.
The use of an intravenous pump and catheter infusion system for stable PAH patients could help them return more quickly to normal activities and curb the risk of catheter-related infections, they said. “Having the potential to remove some of the burden and risk incumbent with an external delivery system may reduce several of the overall barriers to continuous intravenous prostanoid acceptance by both patients and providers,” they noted (Chest. 2017 Dec 6. doi: 10.1016/j.chest.2017.07.006).
Clinicians must be educated to perform the implant procedure itself, and care centers must be trained in identifying patient management issues and refilling the pump reservoir as needed, Dr. Wirth and Dr. Palevsky emphasized. Patients must be educated in what to expect, including how to monitor the pump and track the need for refills, they said. Although the pump is not appropriate for patients with severe PAH, “a planned staged approach of transitioning PAH patients from IV therapy to a less complex system could lend itself to employing prostanoid use earlier and for less severely affected PAH patients,” they said.
Dr. Wirth is affiliated with Tufts University, Boston. Dr. Palevsky is affiliated with the University of Pennsylvania, Philadelphia. Both Dr. Wirth and Dr. Palevsky disclosed serving as consultants and as principal investigators for United Therapeutics.
The development of an implantable therapy for pulmonary hypertension could expand the use of treprostinil, a demonstrated effective treatment for PAH that has been limited in its use because of a range of side effects when given intravenously, orally, subcutaneously, or by inhalation, Joel A. Wirth, MD, FCCP, and Harold I. Palevsky, MD, FCCP, wrote in an editorial.
The use of an intravenous pump and catheter infusion system for stable PAH patients could help them return more quickly to normal activities and curb the risk of catheter-related infections, they said. “Having the potential to remove some of the burden and risk incumbent with an external delivery system may reduce several of the overall barriers to continuous intravenous prostanoid acceptance by both patients and providers,” they noted (Chest. 2017 Dec 6. doi: 10.1016/j.chest.2017.07.006).
Clinicians must be educated to perform the implant procedure itself, and care centers must be trained in identifying patient management issues and refilling the pump reservoir as needed, Dr. Wirth and Dr. Palevsky emphasized. Patients must be educated in what to expect, including how to monitor the pump and track the need for refills, they said. Although the pump is not appropriate for patients with severe PAH, “a planned staged approach of transitioning PAH patients from IV therapy to a less complex system could lend itself to employing prostanoid use earlier and for less severely affected PAH patients,” they said.
Dr. Wirth is affiliated with Tufts University, Boston. Dr. Palevsky is affiliated with the University of Pennsylvania, Philadelphia. Both Dr. Wirth and Dr. Palevsky disclosed serving as consultants and as principal investigators for United Therapeutics.
The development of an implantable therapy for pulmonary hypertension could expand the use of treprostinil, a demonstrated effective treatment for PAH that has been limited in its use because of a range of side effects when given intravenously, orally, subcutaneously, or by inhalation, Joel A. Wirth, MD, FCCP, and Harold I. Palevsky, MD, FCCP, wrote in an editorial.
The use of an intravenous pump and catheter infusion system for stable PAH patients could help them return more quickly to normal activities and curb the risk of catheter-related infections, they said. “Having the potential to remove some of the burden and risk incumbent with an external delivery system may reduce several of the overall barriers to continuous intravenous prostanoid acceptance by both patients and providers,” they noted (Chest. 2017 Dec 6. doi: 10.1016/j.chest.2017.07.006).
Clinicians must be educated to perform the implant procedure itself, and care centers must be trained in identifying patient management issues and refilling the pump reservoir as needed, Dr. Wirth and Dr. Palevsky emphasized. Patients must be educated in what to expect, including how to monitor the pump and track the need for refills, they said. Although the pump is not appropriate for patients with severe PAH, “a planned staged approach of transitioning PAH patients from IV therapy to a less complex system could lend itself to employing prostanoid use earlier and for less severely affected PAH patients,” they said.
Dr. Wirth is affiliated with Tufts University, Boston. Dr. Palevsky is affiliated with the University of Pennsylvania, Philadelphia. Both Dr. Wirth and Dr. Palevsky disclosed serving as consultants and as principal investigators for United Therapeutics.
Pulmonary arterial hypertension (PAH) patients with moderate, stable disease can benefit from an implantable drug delivery system, based on data from a review of 60 adults with successful implantations. The findings were published in the December issue of CHEST.
“A fully implanted system offers patients the hope of returning to more normal activities such as bathing, swimming, and reduced risk of infections from externalized central venous catheter contamination or reduced subcutaneous pain from subcutaneous infusion,” wrote Aaron B. Waxman, MD, PhD, of Brigham and Women’s Hospital, Boston, and his colleagues (Chest. 2017 June 3. doi: 10.1016/j.chest.2017.04.188).
In the DelIVery Trial, clinicians at 10 locations in the United States placed a fully implantable delivery system in adults aged 18 years and older with stable PAH who were previously receiving treprostinil via an external pump at an average dose of 71 ng/kg per min.
All 60 patients were successfully implanted with a system consisting of a drug infusion pump placed in an abdominal pocket and an intravascular catheter linking the implanted pump to the superior vena cava.
“The location of the pump pocket was determined in partnership with the patient and was based on consideration of clothing styles, belt line and subcutaneous fat depth,” the researchers noted.
Procedure-related complications deemed clinically significant included one atrial fibrillation, two incidences of pneumothorax, two infections unrelated to catheter placement, and three catheter dislocations (two in the same patient). The most common patient complaints were expected implant site pain in 83% and bruising in 17%.
The findings were limited by the small number of patients, but the researchers identified several factors that contributed to the success of the procedure, including selecting patients who have shown response to treprostinil and are motivated to comply with pump refill visits, performing the procedure at centers with a high volume of PAH patients, keeping the procedure consistent for each patient, and using the same implant team in each case. “The implant procedure was successfully performed with a low complication rate by clinicians with a diverse range of specialty training,” the researchers added.
Patients reported satisfaction with the implant system at 6 weeks and 6 months, and said they spent an average of 75% less time managing their delivery system, according to previously published data on the patients’ perspective (CHEST 2016;150[1]:27-34).
Medtronic sponsored the study. The lead author, Dr. Waxman, had no financial conflicts to disclose; several coauthors reported relationships with companies including Medtronic, Actelion, Bayer, Gilead, Merck, and United Therapeutics.
Pulmonary arterial hypertension (PAH) patients with moderate, stable disease can benefit from an implantable drug delivery system, based on data from a review of 60 adults with successful implantations. The findings were published in the December issue of CHEST.
“A fully implanted system offers patients the hope of returning to more normal activities such as bathing, swimming, and reduced risk of infections from externalized central venous catheter contamination or reduced subcutaneous pain from subcutaneous infusion,” wrote Aaron B. Waxman, MD, PhD, of Brigham and Women’s Hospital, Boston, and his colleagues (Chest. 2017 June 3. doi: 10.1016/j.chest.2017.04.188).
In the DelIVery Trial, clinicians at 10 locations in the United States placed a fully implantable delivery system in adults aged 18 years and older with stable PAH who were previously receiving treprostinil via an external pump at an average dose of 71 ng/kg per min.
All 60 patients were successfully implanted with a system consisting of a drug infusion pump placed in an abdominal pocket and an intravascular catheter linking the implanted pump to the superior vena cava.
“The location of the pump pocket was determined in partnership with the patient and was based on consideration of clothing styles, belt line and subcutaneous fat depth,” the researchers noted.
Procedure-related complications deemed clinically significant included one atrial fibrillation, two incidences of pneumothorax, two infections unrelated to catheter placement, and three catheter dislocations (two in the same patient). The most common patient complaints were expected implant site pain in 83% and bruising in 17%.
The findings were limited by the small number of patients, but the researchers identified several factors that contributed to the success of the procedure, including selecting patients who have shown response to treprostinil and are motivated to comply with pump refill visits, performing the procedure at centers with a high volume of PAH patients, keeping the procedure consistent for each patient, and using the same implant team in each case. “The implant procedure was successfully performed with a low complication rate by clinicians with a diverse range of specialty training,” the researchers added.
Patients reported satisfaction with the implant system at 6 weeks and 6 months, and said they spent an average of 75% less time managing their delivery system, according to previously published data on the patients’ perspective (CHEST 2016;150[1]:27-34).
Medtronic sponsored the study. The lead author, Dr. Waxman, had no financial conflicts to disclose; several coauthors reported relationships with companies including Medtronic, Actelion, Bayer, Gilead, Merck, and United Therapeutics.
FROM CHEST
Key clinical point: An implantable drug delivery system was successfully placed in 100% of adult PAH patients with no serious complications.
Major finding: The most common complaints among patients who received an implant system to deliver treprostinil were implant site pain (83%) and bruising (17%).
Data source: A multicenter, prospective study of 60 adults with pulmonary arterial hypertension who received implantable pumps to deliver treprostinil.
Disclosures: Medtronic sponsored the study. The lead author, Dr. Waxman, had no financial conflicts to disclose; several coauthors reported relationships with companies including Medtronic, Actelion, Bayer, Gilead, Merck, and United Therapeutics.
Suboxone vs Vivitrol: Similar Outcomes
Two medicines used to treat opioid use disorder—buprenorphine/naloxone (Suboxone) and extended-release naltrexone (Vivitrol)—have similar outcomes if the patient adheres to the treatment, according to a 24-week study of 570 opioid-dependent adults.
The researchers expected that it would be more difficult to initiate treatment with naltrexone because it requires full detoxification, and patients often drop out of the process. And indeed, fewer patients successfully initiated naltrexone, compared with buprenorphine/naloxone (72% vs 94%). The 24-week relapse rates were slightly higher for naltrexone: 65%, compared with 57% for buprenorphine/naloxone, mainly due to early relapse in the naltrexone group.
But among the 474 patients who successfully started on medication, the relapse rates were similar: 52% for naltrexone vs 56% for buprenorphine/naloxone.
Other outcomes among patients who began treatment—days abstinent, negative urine tests, and time to relapse—generally favored buprenorphine/naloxone in the full group, the researchers say. When only those who initiated treatment were considered, the outcomes slightly favored naltrexone.
During the study, 5 people had fatal overdoses: 3 in the buprenorphine/naloxone group and 2 in the naltrexone group. However, overall overdose rates, including nonfatal overdose, were low compared with what would be expected in this population, the researchers say. Their findings “strongly support” the conclusion that medication protects against overdose.
“Studies show that people with opioid dependence who follow detoxification with no medication are very likely to return to drug use,” said Nora Volkow, MD, director of the National Institute on Drug Abuse. “Yet many treatment programs have been slow to accept medications that have proven to be safe and effective. These findings should encourage clinicians to use medication protocols.”
Two medicines used to treat opioid use disorder—buprenorphine/naloxone (Suboxone) and extended-release naltrexone (Vivitrol)—have similar outcomes if the patient adheres to the treatment, according to a 24-week study of 570 opioid-dependent adults.
The researchers expected that it would be more difficult to initiate treatment with naltrexone because it requires full detoxification, and patients often drop out of the process. And indeed, fewer patients successfully initiated naltrexone, compared with buprenorphine/naloxone (72% vs 94%). The 24-week relapse rates were slightly higher for naltrexone: 65%, compared with 57% for buprenorphine/naloxone, mainly due to early relapse in the naltrexone group.
But among the 474 patients who successfully started on medication, the relapse rates were similar: 52% for naltrexone vs 56% for buprenorphine/naloxone.
Other outcomes among patients who began treatment—days abstinent, negative urine tests, and time to relapse—generally favored buprenorphine/naloxone in the full group, the researchers say. When only those who initiated treatment were considered, the outcomes slightly favored naltrexone.
During the study, 5 people had fatal overdoses: 3 in the buprenorphine/naloxone group and 2 in the naltrexone group. However, overall overdose rates, including nonfatal overdose, were low compared with what would be expected in this population, the researchers say. Their findings “strongly support” the conclusion that medication protects against overdose.
“Studies show that people with opioid dependence who follow detoxification with no medication are very likely to return to drug use,” said Nora Volkow, MD, director of the National Institute on Drug Abuse. “Yet many treatment programs have been slow to accept medications that have proven to be safe and effective. These findings should encourage clinicians to use medication protocols.”
Two medicines used to treat opioid use disorder—buprenorphine/naloxone (Suboxone) and extended-release naltrexone (Vivitrol)—have similar outcomes if the patient adheres to the treatment, according to a 24-week study of 570 opioid-dependent adults.
The researchers expected that it would be more difficult to initiate treatment with naltrexone because it requires full detoxification, and patients often drop out of the process. And indeed, fewer patients successfully initiated naltrexone, compared with buprenorphine/naloxone (72% vs 94%). The 24-week relapse rates were slightly higher for naltrexone: 65%, compared with 57% for buprenorphine/naloxone, mainly due to early relapse in the naltrexone group.
But among the 474 patients who successfully started on medication, the relapse rates were similar: 52% for naltrexone vs 56% for buprenorphine/naloxone.
Other outcomes among patients who began treatment—days abstinent, negative urine tests, and time to relapse—generally favored buprenorphine/naloxone in the full group, the researchers say. When only those who initiated treatment were considered, the outcomes slightly favored naltrexone.
During the study, 5 people had fatal overdoses: 3 in the buprenorphine/naloxone group and 2 in the naltrexone group. However, overall overdose rates, including nonfatal overdose, were low compared with what would be expected in this population, the researchers say. Their findings “strongly support” the conclusion that medication protects against overdose.
“Studies show that people with opioid dependence who follow detoxification with no medication are very likely to return to drug use,” said Nora Volkow, MD, director of the National Institute on Drug Abuse. “Yet many treatment programs have been slow to accept medications that have proven to be safe and effective. These findings should encourage clinicians to use medication protocols.”
New Weapon Against Malaria
Malaria is a major challenge in more than 100 countries. In 2015, nearly half the countries in the world had ongoing malaria transmission, according to Dr. Eileen Villasante, head of the Malaria Department at the Naval Medical Research Center (NMRC). But NMRC researchers may have found a new way to meet that challenge. They identified a novel highly protective malaria antigen, Plasmodium yoelii E140.
E140 is found in multiple stages of the life cycle of the malaria parasite, including sporozoites, liver stages, and blood stages, Villasante said. The researchers found that E140 induced up to 100% sterile protection, persisting for at least 3 months. They are now at work on a vaccine with the antigen.
Malaria is a major challenge in more than 100 countries. In 2015, nearly half the countries in the world had ongoing malaria transmission, according to Dr. Eileen Villasante, head of the Malaria Department at the Naval Medical Research Center (NMRC). But NMRC researchers may have found a new way to meet that challenge. They identified a novel highly protective malaria antigen, Plasmodium yoelii E140.
E140 is found in multiple stages of the life cycle of the malaria parasite, including sporozoites, liver stages, and blood stages, Villasante said. The researchers found that E140 induced up to 100% sterile protection, persisting for at least 3 months. They are now at work on a vaccine with the antigen.
Malaria is a major challenge in more than 100 countries. In 2015, nearly half the countries in the world had ongoing malaria transmission, according to Dr. Eileen Villasante, head of the Malaria Department at the Naval Medical Research Center (NMRC). But NMRC researchers may have found a new way to meet that challenge. They identified a novel highly protective malaria antigen, Plasmodium yoelii E140.
E140 is found in multiple stages of the life cycle of the malaria parasite, including sporozoites, liver stages, and blood stages, Villasante said. The researchers found that E140 induced up to 100% sterile protection, persisting for at least 3 months. They are now at work on a vaccine with the antigen.
Adolescents with chronic health conditions often undervaccinated
said Annika M. Hofstetter, MD, PhD, of Columbia University, New York, and her associates.
The National Health Interview Survey on Disability in 1994-1995 estimated that chronic conditions of any type affected 15%-18% of U.S. children and adolescents. The Advisory Committee on Immunization Practices recommends that all adolescents, whether or not they have chronic medical condition, be vaccinated with human papillomavirus (HPV), Tdap, meningococcal, and flu vaccines.

Fewer adolescents with CMCs had received one more doses of HPV (81%), than did those without CMCs (85%; P less than .01). Fewer adolescents with epilepsy (63%), mental retardation (58%), cerebral palsy (54%), and autism spectrum disorder (46%) had started HPV vaccination, compared with those without each of these conditions (84%; all comparisons, P less than .001). No differences were seen for asthma or congenital heart disease, the investigators said.
More adolescents with CMCs had gotten their flu shot than did those without CMCs during the 2011-2012 season (67% vs. 50%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). More adolescents with asthma got their flu shot than did those without asthma during the 2011-2012 season (69% vs. 51%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). No differences were seen for the other common CMCs.
Nonetheless, the mean number of missed opportunities was significantly higher among unvaccinated adolescents with CMCs, compared with those without CMCs, for the first HPV vaccination, meningococcal vaccination, and influenza vaccination in both seasons measured (P less than .001 for all).
“Missed opportunities for the third HPV vaccine dose or Tdap did not differ by CMC status,” Dr. Hofstetter and her associates said.
Read more in the American Journal of Preventive Medicine (2017 Nov;53[5]:680-8).
said Annika M. Hofstetter, MD, PhD, of Columbia University, New York, and her associates.
The National Health Interview Survey on Disability in 1994-1995 estimated that chronic conditions of any type affected 15%-18% of U.S. children and adolescents. The Advisory Committee on Immunization Practices recommends that all adolescents, whether or not they have chronic medical condition, be vaccinated with human papillomavirus (HPV), Tdap, meningococcal, and flu vaccines.
Fewer adolescents with CMCs had received one more doses of HPV (81%), than did those without CMCs (85%; P less than .01). Fewer adolescents with epilepsy (63%), mental retardation (58%), cerebral palsy (54%), and autism spectrum disorder (46%) had started HPV vaccination, compared with those without each of these conditions (84%; all comparisons, P less than .001). No differences were seen for asthma or congenital heart disease, the investigators said.
More adolescents with CMCs had gotten their flu shot than did those without CMCs during the 2011-2012 season (67% vs. 50%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). More adolescents with asthma got their flu shot than did those without asthma during the 2011-2012 season (69% vs. 51%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). No differences were seen for the other common CMCs.
Nonetheless, the mean number of missed opportunities was significantly higher among unvaccinated adolescents with CMCs, compared with those without CMCs, for the first HPV vaccination, meningococcal vaccination, and influenza vaccination in both seasons measured (P less than .001 for all).
“Missed opportunities for the third HPV vaccine dose or Tdap did not differ by CMC status,” Dr. Hofstetter and her associates said.
Read more in the American Journal of Preventive Medicine (2017 Nov;53[5]:680-8).
said Annika M. Hofstetter, MD, PhD, of Columbia University, New York, and her associates.
The National Health Interview Survey on Disability in 1994-1995 estimated that chronic conditions of any type affected 15%-18% of U.S. children and adolescents. The Advisory Committee on Immunization Practices recommends that all adolescents, whether or not they have chronic medical condition, be vaccinated with human papillomavirus (HPV), Tdap, meningococcal, and flu vaccines.
Fewer adolescents with CMCs had received one more doses of HPV (81%), than did those without CMCs (85%; P less than .01). Fewer adolescents with epilepsy (63%), mental retardation (58%), cerebral palsy (54%), and autism spectrum disorder (46%) had started HPV vaccination, compared with those without each of these conditions (84%; all comparisons, P less than .001). No differences were seen for asthma or congenital heart disease, the investigators said.
More adolescents with CMCs had gotten their flu shot than did those without CMCs during the 2011-2012 season (67% vs. 50%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). More adolescents with asthma got their flu shot than did those without asthma during the 2011-2012 season (69% vs. 51%; P less than .001) or during the 2012-2013 season (74% vs. 65%; P less than .001). No differences were seen for the other common CMCs.
Nonetheless, the mean number of missed opportunities was significantly higher among unvaccinated adolescents with CMCs, compared with those without CMCs, for the first HPV vaccination, meningococcal vaccination, and influenza vaccination in both seasons measured (P less than .001 for all).
“Missed opportunities for the third HPV vaccine dose or Tdap did not differ by CMC status,” Dr. Hofstetter and her associates said.
Read more in the American Journal of Preventive Medicine (2017 Nov;53[5]:680-8).
FROM THE AMERICAN JOURNAL OF PREVENTIVE MEDICINE
Ultrathin bronchoscopy plus radial EBUS unreliable at making diagnoses
TORONTO – Ultrathin bronchoscopy plus radial endobronchial ultrasound is not a great method for determining whether a suspicious lesion is cancerous or benign, suggests new research.
In this study of patients with CT-detected solid lung lesions, the researchers were able to make a diagnosis for only 49% of those whose nodules were evaluated using ultrathin bronchoscopy plus radial endobronchial ultrasound (EBUS).

“When you do CT-guided biopsies of lung lesions, the [diagnostic] yield is about 94%. So do the math” by comparing it to the roughly 50% yield from ultrathin bronchoscopy plus radial EBUS to decide whether the latter procedure is worth doing, she noted.
The study Dr. Tanner and her associates designed compared the diagnostic yield of ultrathin bronchoscopy plus radial EBUS with standard bronchoscopy and fluoroscopy in patients with CT-detected solid lung lesions 1.5-5.0 cm in size. It ran at five U.S. centers and randomized 221 patients: 85 evaluable patients were tested using the standard methods, and 112 evaluable patients were tested using ultrathin bronchoscopy plus radial EBUS. Patients averaged 65-68 years of age and were divided evenly between women and men. Their lesions averaged slightly more than 3 cm. The ultrathin device had a 4 mm wide diameter and had a 2 mm working channel.
The diagnostic yield was 38% among patients who underwent standard bronchoscopy and fluoroscopy, and 49% among those biopsied using ultrathin bronchoscopy and radial EBUS, Dr. Tanner reported. The between-group difference in yield fell short of being statistically significant.
Forty-six of the 53 patients who were not diagnosable using standard bronchoscopy and fluoroscopy crossed over to the investigational method, which produced a diagnosis for an additional seven patients (15% of the biopsied crossover patients).
The results showed that standard bronchoscopy plus fluoroscopy is “very poor” for distinguishing cancerous and benign pulmonary lesions, Dr. Tanner concluded. The yield from ultrathin bronchoscopy plus radial EBUS in her study was similar to the diagnostic yields reported in prior studies of guided bronchoscopy, even when also using radial EBUS, she added.
Given the limitations of ultrathin bronchoscopy plus radial EBUS, Dr. Tanner suggested that the best scenario for using this diagnostic method would be in patients who need a linear EBUS procedure for mediastinal lymph node staging. Such staging often requires a biopsy of the primary tumor to make a cancer diagnosis, and in such cases, “while you’re in the neighborhood, you could do bronchoscopy with an ultrathin scope,” she suggested.
The potential also exists to augment the diagnostic yield of ultrathin bronchoscopy by applying a navigational software platform and needle biopsy, two methods not included in the study, Dr. Tanner noted. “More studies should be done using this combination,” she said.
The study was funded by Olympus. Dr. Tanner has been a consultant to and has received research funding from Olympus. She has also been a consultant to Cook Medical, Integrated Diagnostics, Oncocyte, Veracyte, and Veran Medical Technologies, and she has also received research funding from Cook, Integrated Diagnostics, Oncocyte, Oncimmune, and Veracyte.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Although bronchoscopic tools are safe and accurate to evaluate both central and peripheral lung lesions, the diagnostic yield of the different available techniques is variable. In this study, a diagnostic yield of only 49% was achieved when ultrathin bronchoscopy with radial EBUS was performed for diagnosis of solid nodules. This yield is not much better than that obtained from conventional bronchoscopy with fluoroscopic guidance and much lower than the diagnostic yield from transthoracic needle biopsy. While there is no doubt that the advances in minimally invasive technologies for diagnosing lung nodules and diagnosing and staging lung cancer have revolutionized clinical practice, pulmonologists and thoracic surgeons need to recognize not only the utility but also the limitations of the available diagnostic procedures (as well as the cost). These technologies are complimentary and multidisciplinary discussions should facilitate selection of the best procedure for each individual case.

Although bronchoscopic tools are safe and accurate to evaluate both central and peripheral lung lesions, the diagnostic yield of the different available techniques is variable. In this study, a diagnostic yield of only 49% was achieved when ultrathin bronchoscopy with radial EBUS was performed for diagnosis of solid nodules. This yield is not much better than that obtained from conventional bronchoscopy with fluoroscopic guidance and much lower than the diagnostic yield from transthoracic needle biopsy. While there is no doubt that the advances in minimally invasive technologies for diagnosing lung nodules and diagnosing and staging lung cancer have revolutionized clinical practice, pulmonologists and thoracic surgeons need to recognize not only the utility but also the limitations of the available diagnostic procedures (as well as the cost). These technologies are complimentary and multidisciplinary discussions should facilitate selection of the best procedure for each individual case.
Although bronchoscopic tools are safe and accurate to evaluate both central and peripheral lung lesions, the diagnostic yield of the different available techniques is variable. In this study, a diagnostic yield of only 49% was achieved when ultrathin bronchoscopy with radial EBUS was performed for diagnosis of solid nodules. This yield is not much better than that obtained from conventional bronchoscopy with fluoroscopic guidance and much lower than the diagnostic yield from transthoracic needle biopsy. While there is no doubt that the advances in minimally invasive technologies for diagnosing lung nodules and diagnosing and staging lung cancer have revolutionized clinical practice, pulmonologists and thoracic surgeons need to recognize not only the utility but also the limitations of the available diagnostic procedures (as well as the cost). These technologies are complimentary and multidisciplinary discussions should facilitate selection of the best procedure for each individual case.
TORONTO – Ultrathin bronchoscopy plus radial endobronchial ultrasound is not a great method for determining whether a suspicious lesion is cancerous or benign, suggests new research.
In this study of patients with CT-detected solid lung lesions, the researchers were able to make a diagnosis for only 49% of those whose nodules were evaluated using ultrathin bronchoscopy plus radial endobronchial ultrasound (EBUS).
“When you do CT-guided biopsies of lung lesions, the [diagnostic] yield is about 94%. So do the math” by comparing it to the roughly 50% yield from ultrathin bronchoscopy plus radial EBUS to decide whether the latter procedure is worth doing, she noted.
The study Dr. Tanner and her associates designed compared the diagnostic yield of ultrathin bronchoscopy plus radial EBUS with standard bronchoscopy and fluoroscopy in patients with CT-detected solid lung lesions 1.5-5.0 cm in size. It ran at five U.S. centers and randomized 221 patients: 85 evaluable patients were tested using the standard methods, and 112 evaluable patients were tested using ultrathin bronchoscopy plus radial EBUS. Patients averaged 65-68 years of age and were divided evenly between women and men. Their lesions averaged slightly more than 3 cm. The ultrathin device had a 4 mm wide diameter and had a 2 mm working channel.
The diagnostic yield was 38% among patients who underwent standard bronchoscopy and fluoroscopy, and 49% among those biopsied using ultrathin bronchoscopy and radial EBUS, Dr. Tanner reported. The between-group difference in yield fell short of being statistically significant.
Forty-six of the 53 patients who were not diagnosable using standard bronchoscopy and fluoroscopy crossed over to the investigational method, which produced a diagnosis for an additional seven patients (15% of the biopsied crossover patients).
The results showed that standard bronchoscopy plus fluoroscopy is “very poor” for distinguishing cancerous and benign pulmonary lesions, Dr. Tanner concluded. The yield from ultrathin bronchoscopy plus radial EBUS in her study was similar to the diagnostic yields reported in prior studies of guided bronchoscopy, even when also using radial EBUS, she added.
Given the limitations of ultrathin bronchoscopy plus radial EBUS, Dr. Tanner suggested that the best scenario for using this diagnostic method would be in patients who need a linear EBUS procedure for mediastinal lymph node staging. Such staging often requires a biopsy of the primary tumor to make a cancer diagnosis, and in such cases, “while you’re in the neighborhood, you could do bronchoscopy with an ultrathin scope,” she suggested.
The potential also exists to augment the diagnostic yield of ultrathin bronchoscopy by applying a navigational software platform and needle biopsy, two methods not included in the study, Dr. Tanner noted. “More studies should be done using this combination,” she said.
The study was funded by Olympus. Dr. Tanner has been a consultant to and has received research funding from Olympus. She has also been a consultant to Cook Medical, Integrated Diagnostics, Oncocyte, Veracyte, and Veran Medical Technologies, and she has also received research funding from Cook, Integrated Diagnostics, Oncocyte, Oncimmune, and Veracyte.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Ultrathin bronchoscopy plus radial endobronchial ultrasound is not a great method for determining whether a suspicious lesion is cancerous or benign, suggests new research.
In this study of patients with CT-detected solid lung lesions, the researchers were able to make a diagnosis for only 49% of those whose nodules were evaluated using ultrathin bronchoscopy plus radial endobronchial ultrasound (EBUS).
“When you do CT-guided biopsies of lung lesions, the [diagnostic] yield is about 94%. So do the math” by comparing it to the roughly 50% yield from ultrathin bronchoscopy plus radial EBUS to decide whether the latter procedure is worth doing, she noted.
The study Dr. Tanner and her associates designed compared the diagnostic yield of ultrathin bronchoscopy plus radial EBUS with standard bronchoscopy and fluoroscopy in patients with CT-detected solid lung lesions 1.5-5.0 cm in size. It ran at five U.S. centers and randomized 221 patients: 85 evaluable patients were tested using the standard methods, and 112 evaluable patients were tested using ultrathin bronchoscopy plus radial EBUS. Patients averaged 65-68 years of age and were divided evenly between women and men. Their lesions averaged slightly more than 3 cm. The ultrathin device had a 4 mm wide diameter and had a 2 mm working channel.
The diagnostic yield was 38% among patients who underwent standard bronchoscopy and fluoroscopy, and 49% among those biopsied using ultrathin bronchoscopy and radial EBUS, Dr. Tanner reported. The between-group difference in yield fell short of being statistically significant.
Forty-six of the 53 patients who were not diagnosable using standard bronchoscopy and fluoroscopy crossed over to the investigational method, which produced a diagnosis for an additional seven patients (15% of the biopsied crossover patients).
The results showed that standard bronchoscopy plus fluoroscopy is “very poor” for distinguishing cancerous and benign pulmonary lesions, Dr. Tanner concluded. The yield from ultrathin bronchoscopy plus radial EBUS in her study was similar to the diagnostic yields reported in prior studies of guided bronchoscopy, even when also using radial EBUS, she added.
Given the limitations of ultrathin bronchoscopy plus radial EBUS, Dr. Tanner suggested that the best scenario for using this diagnostic method would be in patients who need a linear EBUS procedure for mediastinal lymph node staging. Such staging often requires a biopsy of the primary tumor to make a cancer diagnosis, and in such cases, “while you’re in the neighborhood, you could do bronchoscopy with an ultrathin scope,” she suggested.
The potential also exists to augment the diagnostic yield of ultrathin bronchoscopy by applying a navigational software platform and needle biopsy, two methods not included in the study, Dr. Tanner noted. “More studies should be done using this combination,” she said.
The study was funded by Olympus. Dr. Tanner has been a consultant to and has received research funding from Olympus. She has also been a consultant to Cook Medical, Integrated Diagnostics, Oncocyte, Veracyte, and Veran Medical Technologies, and she has also received research funding from Cook, Integrated Diagnostics, Oncocyte, Oncimmune, and Veracyte.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: The diagnostic yield using ultrathin bronchoscopy with radial EBUS was 49%, while standard bronchoscopy had a 38% yield.
Data source: Multicenter, randomized study with 221 total patients and 197 evaluable patients.
Disclosures: The study was funded by Olympus. Dr. Tanner has been a consultant to and has received research funding from Olympus. She has also been a consultant to Cook Medical, Integrated Diagnostics, Oncocyte, Veracyte, and Veran Medical Technologies, and she has also received research funding from Cook, Integrated Diagnostics, Oncocyte, Oncimmune, and Veracyte.