User login
CLL drug in limited supply outside U.S.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Shorter walk test predicts IPF outcomes
, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.

, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.
, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.
FROM CHEST 2017
Analysis of Twitter lung cancer content reveals opportunity for clinicians
Social media communication around lung cancer is focused primarily on cancer treatment and use of pharmaceutical and research interventions, followed closely by awareness, prevention, and risk topics, according to an analysis of Twitter conversation over a 10-day period.
Although awareness and risk prevention tweets were likely to contain cues toward action, “messages focused on treatment, end of life ... were significantly less likely to integrate cues for personal activity,” the investigators wrote. The report was published in Journal of the American College of Radiology.
The investigators collected 1.3 million unique Twitter messages between Sept. 30 and Oct. 9, 2016, that contained at least one of six keywords commonly used to describe cancer: cancer, chemo, tumor, malignant, biopsy, and metastasis. They then drew a random, proportional stratified sample of 3,000 messages (12.5%) for manual coding from the 23,926 messages posted that included keywords related to lung cancer. Tweets were examined by user type (individuals, media, and organizations) to identify content and structural message features.
Message content was most frequently related to treatment (32.1%), followed by awareness (22.9%), end of life (15.5%), prevention and risk information (13.3%), active cancer-unknown phase (7.6%), diagnosis (6.1%), early detection (2.7%), and survivorship (1%), Dr. Sutton and her colleagues reported.
“The large volume of messages containing content about pharmaceuticals suggests that Twitter is also a forum for sharing information and discussing emerging treatments. Importantly, treatment messages were shared primarily by individuals, suggesting that this online user community jointly includes members of the public as well as medical practitioners and companies who have an awareness of emerging treatment approaches, suggesting an opportunity for online engagement between these various groups (e.g., Lung Cancer Social Media #LCSM community and related chats),” the investigators wrote.
The National Science Foundation supported parts of this research. None of the authors reported any conflicts of interest.
SOURCE: Sutton J. et al., J Am Coll Radiol. 2018 Jan. doi: 10.1016/j.jacr.2017.09.043
Social media communication around lung cancer is focused primarily on cancer treatment and use of pharmaceutical and research interventions, followed closely by awareness, prevention, and risk topics, according to an analysis of Twitter conversation over a 10-day period.
Although awareness and risk prevention tweets were likely to contain cues toward action, “messages focused on treatment, end of life ... were significantly less likely to integrate cues for personal activity,” the investigators wrote. The report was published in Journal of the American College of Radiology.
The investigators collected 1.3 million unique Twitter messages between Sept. 30 and Oct. 9, 2016, that contained at least one of six keywords commonly used to describe cancer: cancer, chemo, tumor, malignant, biopsy, and metastasis. They then drew a random, proportional stratified sample of 3,000 messages (12.5%) for manual coding from the 23,926 messages posted that included keywords related to lung cancer. Tweets were examined by user type (individuals, media, and organizations) to identify content and structural message features.
Message content was most frequently related to treatment (32.1%), followed by awareness (22.9%), end of life (15.5%), prevention and risk information (13.3%), active cancer-unknown phase (7.6%), diagnosis (6.1%), early detection (2.7%), and survivorship (1%), Dr. Sutton and her colleagues reported.
“The large volume of messages containing content about pharmaceuticals suggests that Twitter is also a forum for sharing information and discussing emerging treatments. Importantly, treatment messages were shared primarily by individuals, suggesting that this online user community jointly includes members of the public as well as medical practitioners and companies who have an awareness of emerging treatment approaches, suggesting an opportunity for online engagement between these various groups (e.g., Lung Cancer Social Media #LCSM community and related chats),” the investigators wrote.
The National Science Foundation supported parts of this research. None of the authors reported any conflicts of interest.
SOURCE: Sutton J. et al., J Am Coll Radiol. 2018 Jan. doi: 10.1016/j.jacr.2017.09.043
Social media communication around lung cancer is focused primarily on cancer treatment and use of pharmaceutical and research interventions, followed closely by awareness, prevention, and risk topics, according to an analysis of Twitter conversation over a 10-day period.
Although awareness and risk prevention tweets were likely to contain cues toward action, “messages focused on treatment, end of life ... were significantly less likely to integrate cues for personal activity,” the investigators wrote. The report was published in Journal of the American College of Radiology.
The investigators collected 1.3 million unique Twitter messages between Sept. 30 and Oct. 9, 2016, that contained at least one of six keywords commonly used to describe cancer: cancer, chemo, tumor, malignant, biopsy, and metastasis. They then drew a random, proportional stratified sample of 3,000 messages (12.5%) for manual coding from the 23,926 messages posted that included keywords related to lung cancer. Tweets were examined by user type (individuals, media, and organizations) to identify content and structural message features.
Message content was most frequently related to treatment (32.1%), followed by awareness (22.9%), end of life (15.5%), prevention and risk information (13.3%), active cancer-unknown phase (7.6%), diagnosis (6.1%), early detection (2.7%), and survivorship (1%), Dr. Sutton and her colleagues reported.
“The large volume of messages containing content about pharmaceuticals suggests that Twitter is also a forum for sharing information and discussing emerging treatments. Importantly, treatment messages were shared primarily by individuals, suggesting that this online user community jointly includes members of the public as well as medical practitioners and companies who have an awareness of emerging treatment approaches, suggesting an opportunity for online engagement between these various groups (e.g., Lung Cancer Social Media #LCSM community and related chats),” the investigators wrote.
The National Science Foundation supported parts of this research. None of the authors reported any conflicts of interest.
SOURCE: Sutton J. et al., J Am Coll Radiol. 2018 Jan. doi: 10.1016/j.jacr.2017.09.043
FROM JOURNAL OF THE AMERICAN COLLEGE OF RADIOLOGY
Key clinical point: In a random sample of Twitter conversation related to lung cancer, message content was most frequently related to treatment.
Major finding: Majority of tweets evaluated focused on lung cancer treatment and the use of pharmaceutical and research interventions, followed by awareness, prevention, and risk topics.
Study details: Random sample of 3,000 tweets posted in a 10-day period between Sept. 30 and Oct. 9, 2016. Lung cancer–specific tweets by user type (individuals, media, and organizations) were examined to identify content and structural message features.
Disclosures: The National Science Foundation supported parts of this research. None of the authors reported any conflicts of interest.
Source: Sutton J. et al., J Am Coll Radiol. 2018 Jan. doi: 10.1016/j.jacr.2017.09.043.
Influenza: All that and MI too
Myocardial infarction admissions were six times more likely to occur in the week after a positive test for influenza than in the year before or the 51 weeks after the infection, according to analysis of a Canadian cohort that links laboratories with administrative databases.
The investigators used this cohort data to define definitions of “risk interval” – the first 7 days after flu detection – and a combined “control interval” – 52 weeks before the flu detection and 51 weeks after the end of the risk interval.
Among the total of 364 hospital admissions for MI in patients with confirmed influenza, 20 occurred during the defined 1-week risk interval (20 admissions/week) and 344 occurred during the control interval (3.3 admissions/week), giving an incidence ratio (IR) of 6.05, Jeffrey C. Kwong, MD, of the University of Toronto and his associates reported in the New England Journal of Medicine.
There was little difference between days 1 and 3 after flu confirmation (IR, 6.3) and days 4-7 (IR, 5.8), but risk dropped off quickly after that, with IRs of 0.6 at days 8-14 and 0.75 at days 15-28. Risk was increased for older adults, those with influenza B infection, and those who had their first MI, the investigators said.
MI incidence also was elevated after infection with noninfluenza respiratory viruses, although to a lesser extent than with influenza, which suggests that “influenza is illustrative of the role that acute respiratory infections have in precipitating acute myocardial infarction,” Dr. Kwong and his associates wrote.
The study was supported by the Canadian Institutes of Health Research, by Public Health Ontario, and by the Institute for Clinical Evaluative Sciences. Dr. Kwong reported grants from Canadian Institutes of Health Research during the conduct of the study, as well as grants from Canadian Institutes of Health Research and University of Toronto.
SOURCE: Kwong JC et al. N Engl J Med. 2018. 378(4):345-53. doi: 10.1056/NEJMoa1702090.
Myocardial infarction admissions were six times more likely to occur in the week after a positive test for influenza than in the year before or the 51 weeks after the infection, according to analysis of a Canadian cohort that links laboratories with administrative databases.
The investigators used this cohort data to define definitions of “risk interval” – the first 7 days after flu detection – and a combined “control interval” – 52 weeks before the flu detection and 51 weeks after the end of the risk interval.
Among the total of 364 hospital admissions for MI in patients with confirmed influenza, 20 occurred during the defined 1-week risk interval (20 admissions/week) and 344 occurred during the control interval (3.3 admissions/week), giving an incidence ratio (IR) of 6.05, Jeffrey C. Kwong, MD, of the University of Toronto and his associates reported in the New England Journal of Medicine.
There was little difference between days 1 and 3 after flu confirmation (IR, 6.3) and days 4-7 (IR, 5.8), but risk dropped off quickly after that, with IRs of 0.6 at days 8-14 and 0.75 at days 15-28. Risk was increased for older adults, those with influenza B infection, and those who had their first MI, the investigators said.
MI incidence also was elevated after infection with noninfluenza respiratory viruses, although to a lesser extent than with influenza, which suggests that “influenza is illustrative of the role that acute respiratory infections have in precipitating acute myocardial infarction,” Dr. Kwong and his associates wrote.
The study was supported by the Canadian Institutes of Health Research, by Public Health Ontario, and by the Institute for Clinical Evaluative Sciences. Dr. Kwong reported grants from Canadian Institutes of Health Research during the conduct of the study, as well as grants from Canadian Institutes of Health Research and University of Toronto.
SOURCE: Kwong JC et al. N Engl J Med. 2018. 378(4):345-53. doi: 10.1056/NEJMoa1702090.
Myocardial infarction admissions were six times more likely to occur in the week after a positive test for influenza than in the year before or the 51 weeks after the infection, according to analysis of a Canadian cohort that links laboratories with administrative databases.
The investigators used this cohort data to define definitions of “risk interval” – the first 7 days after flu detection – and a combined “control interval” – 52 weeks before the flu detection and 51 weeks after the end of the risk interval.
Among the total of 364 hospital admissions for MI in patients with confirmed influenza, 20 occurred during the defined 1-week risk interval (20 admissions/week) and 344 occurred during the control interval (3.3 admissions/week), giving an incidence ratio (IR) of 6.05, Jeffrey C. Kwong, MD, of the University of Toronto and his associates reported in the New England Journal of Medicine.
There was little difference between days 1 and 3 after flu confirmation (IR, 6.3) and days 4-7 (IR, 5.8), but risk dropped off quickly after that, with IRs of 0.6 at days 8-14 and 0.75 at days 15-28. Risk was increased for older adults, those with influenza B infection, and those who had their first MI, the investigators said.
MI incidence also was elevated after infection with noninfluenza respiratory viruses, although to a lesser extent than with influenza, which suggests that “influenza is illustrative of the role that acute respiratory infections have in precipitating acute myocardial infarction,” Dr. Kwong and his associates wrote.
The study was supported by the Canadian Institutes of Health Research, by Public Health Ontario, and by the Institute for Clinical Evaluative Sciences. Dr. Kwong reported grants from Canadian Institutes of Health Research during the conduct of the study, as well as grants from Canadian Institutes of Health Research and University of Toronto.
SOURCE: Kwong JC et al. N Engl J Med. 2018. 378(4):345-53. doi: 10.1056/NEJMoa1702090.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
FDA Pledges Faster Updates for Antibiotics
The FDA is launching a new website to get critical updates about antibiotics and antifungals out faster to health care professionals to help them make more informed prescribing decisions. The site will provide “direct and timely access” to information about when bacterial or fungal infections are likely to respond to a specific drug.
“When you are treating critically ill patients, you want as much information as possible about the pathogen…and the susceptibility of that pathogen to various treatment,” said FDA Commissioner Scott Gottlieb, MD. Under the old approach, he said, updating each drug’s individual labeling took too long. Only after the revised drug labeling was approved could a drug or device manufacturer update testing criteria and labeling for the latest antimicrobial susceptibility test results. Each drug and device labeling had to be updated whenever criteria changed.
The new tool will allow the FDA to simultaneously provide updates multiple drugs that have the same active ingredient and share that information transparently via a dedicated web page.
The FDA is launching a new website to get critical updates about antibiotics and antifungals out faster to health care professionals to help them make more informed prescribing decisions. The site will provide “direct and timely access” to information about when bacterial or fungal infections are likely to respond to a specific drug.
“When you are treating critically ill patients, you want as much information as possible about the pathogen…and the susceptibility of that pathogen to various treatment,” said FDA Commissioner Scott Gottlieb, MD. Under the old approach, he said, updating each drug’s individual labeling took too long. Only after the revised drug labeling was approved could a drug or device manufacturer update testing criteria and labeling for the latest antimicrobial susceptibility test results. Each drug and device labeling had to be updated whenever criteria changed.
The new tool will allow the FDA to simultaneously provide updates multiple drugs that have the same active ingredient and share that information transparently via a dedicated web page.
The FDA is launching a new website to get critical updates about antibiotics and antifungals out faster to health care professionals to help them make more informed prescribing decisions. The site will provide “direct and timely access” to information about when bacterial or fungal infections are likely to respond to a specific drug.
“When you are treating critically ill patients, you want as much information as possible about the pathogen…and the susceptibility of that pathogen to various treatment,” said FDA Commissioner Scott Gottlieb, MD. Under the old approach, he said, updating each drug’s individual labeling took too long. Only after the revised drug labeling was approved could a drug or device manufacturer update testing criteria and labeling for the latest antimicrobial susceptibility test results. Each drug and device labeling had to be updated whenever criteria changed.
The new tool will allow the FDA to simultaneously provide updates multiple drugs that have the same active ingredient and share that information transparently via a dedicated web page.
Checkpoint inhibitors look safe in rheumatology patients
People with rheumatologic diseases and cancer appear to be at no higher risk of having an adverse event or disease flare if they receive checkpoint inhibitor therapy, compared with the general population, experience from the Mayo Clinic suggests.
In a brief report published in Arthritis and Rheumatology, a team from the Mayo Clinic in Rochester, Minn., reported on 16 patients with rheumatologic diseases who received cancer immunotherapy. They found that only a minority experienced a flare of their disease or another immune-related event.
The rate of severe immune-related adverse effects (IRAEs) with a single immune checkpoint inhibitor (ICI) has been reported to be less than 2% among the average population. However, less is known about patients with underlying rheumatologic disease, largely because initial trials of ICIs had excluded patients with autoimmune diseases for fear the treatment would induce a disease flare, the researchers noted.
Small studies have suggested that people with inflammatory arthritis or connective tissue diseases have higher rates of IRAEs with immunotherapy, but it is unclear how often these events represented flares of their disease or new autoimmune events, and whether the events had any predictive significance for cancer survival.
In this study, researchers performed a retrospective review of medical records and identified 16 patients with rheumatologic diseases who had received checkpoint inhibitor therapy at the Mayo Clinic between 2011 and 2016.
The most common rheumatologic diseases among the 16 patients were rheumatoid arthritis, polymyalgia rheumatica, Sjögren’s syndrome, and systemic lupus erythematosus, and the most common cancers were malignant melanoma, pulmonary malignancies, and non-Hodgkin lymphoma. Seven of the patients were receiving immunosuppressive therapy or glucocorticoids for their rheumatologic disease upon initiation of a checkpoint inhibitor.
Ten patients had received a prior disease-modifying antirheumatic drug, but only two patients were still taking this at the time of ICI initiation.
Results showed that six of the patients (38%) had an IRAE or flare of their rheumatologic disease, two were graded as mild. All of the patients responded well to glucocorticoids and discontinuation of therapy. The most common event was colitis and just one patient had a flare of rheumatologic disease.
“This is consistent with what is currently known about the management of IRAEs,” the research team wrote. “This study adds further support to the emerging notion that the rate of IRAEs is not necessarily higher in this group compared to the general population.”
The type and severity of rheumatologic disease may play an important role in both the risk of disease flare and IRAEs, a factor that they were unable to assess in the current study, the researchers wrote.
“Further large, prospective studies are needed to address the link between the type, severity, and concurrent rheumatologic disease activity on the risk of flare and IRAE. It is possible that patients with more severe or active disease are at higher risk for these complications,” they wrote.
While patients in the study did not appear to have significantly increased incidence or severity of adverse effects, the research team advised that “treatment decisions must factor in clinical judgement.”
They noted that some studies had proposed predictive biomarkers, pretreatment workup, and monitoring, but this advice was based on a small body of evidence.
“Larger, prospective studies will be necessary to validate these findings and establish evidence-based guidelines for appropriate identification and rating of the rheumatologic IRAEs as well as their treatment, such that patients can continue to receive potentially life-saving cancer treatments,” they wrote.
One of the researchers reported advisory board membership with Bristol-Myers Squibb.
SOURCE: Richter M et al. Arthritis Rheumatol. 2018 Jan 24. doi: 10.1002/art.40397.
People with rheumatologic diseases and cancer appear to be at no higher risk of having an adverse event or disease flare if they receive checkpoint inhibitor therapy, compared with the general population, experience from the Mayo Clinic suggests.
In a brief report published in Arthritis and Rheumatology, a team from the Mayo Clinic in Rochester, Minn., reported on 16 patients with rheumatologic diseases who received cancer immunotherapy. They found that only a minority experienced a flare of their disease or another immune-related event.
The rate of severe immune-related adverse effects (IRAEs) with a single immune checkpoint inhibitor (ICI) has been reported to be less than 2% among the average population. However, less is known about patients with underlying rheumatologic disease, largely because initial trials of ICIs had excluded patients with autoimmune diseases for fear the treatment would induce a disease flare, the researchers noted.
Small studies have suggested that people with inflammatory arthritis or connective tissue diseases have higher rates of IRAEs with immunotherapy, but it is unclear how often these events represented flares of their disease or new autoimmune events, and whether the events had any predictive significance for cancer survival.
In this study, researchers performed a retrospective review of medical records and identified 16 patients with rheumatologic diseases who had received checkpoint inhibitor therapy at the Mayo Clinic between 2011 and 2016.
The most common rheumatologic diseases among the 16 patients were rheumatoid arthritis, polymyalgia rheumatica, Sjögren’s syndrome, and systemic lupus erythematosus, and the most common cancers were malignant melanoma, pulmonary malignancies, and non-Hodgkin lymphoma. Seven of the patients were receiving immunosuppressive therapy or glucocorticoids for their rheumatologic disease upon initiation of a checkpoint inhibitor.
Ten patients had received a prior disease-modifying antirheumatic drug, but only two patients were still taking this at the time of ICI initiation.
Results showed that six of the patients (38%) had an IRAE or flare of their rheumatologic disease, two were graded as mild. All of the patients responded well to glucocorticoids and discontinuation of therapy. The most common event was colitis and just one patient had a flare of rheumatologic disease.
“This is consistent with what is currently known about the management of IRAEs,” the research team wrote. “This study adds further support to the emerging notion that the rate of IRAEs is not necessarily higher in this group compared to the general population.”
The type and severity of rheumatologic disease may play an important role in both the risk of disease flare and IRAEs, a factor that they were unable to assess in the current study, the researchers wrote.
“Further large, prospective studies are needed to address the link between the type, severity, and concurrent rheumatologic disease activity on the risk of flare and IRAE. It is possible that patients with more severe or active disease are at higher risk for these complications,” they wrote.
While patients in the study did not appear to have significantly increased incidence or severity of adverse effects, the research team advised that “treatment decisions must factor in clinical judgement.”
They noted that some studies had proposed predictive biomarkers, pretreatment workup, and monitoring, but this advice was based on a small body of evidence.
“Larger, prospective studies will be necessary to validate these findings and establish evidence-based guidelines for appropriate identification and rating of the rheumatologic IRAEs as well as their treatment, such that patients can continue to receive potentially life-saving cancer treatments,” they wrote.
One of the researchers reported advisory board membership with Bristol-Myers Squibb.
SOURCE: Richter M et al. Arthritis Rheumatol. 2018 Jan 24. doi: 10.1002/art.40397.
People with rheumatologic diseases and cancer appear to be at no higher risk of having an adverse event or disease flare if they receive checkpoint inhibitor therapy, compared with the general population, experience from the Mayo Clinic suggests.
In a brief report published in Arthritis and Rheumatology, a team from the Mayo Clinic in Rochester, Minn., reported on 16 patients with rheumatologic diseases who received cancer immunotherapy. They found that only a minority experienced a flare of their disease or another immune-related event.
The rate of severe immune-related adverse effects (IRAEs) with a single immune checkpoint inhibitor (ICI) has been reported to be less than 2% among the average population. However, less is known about patients with underlying rheumatologic disease, largely because initial trials of ICIs had excluded patients with autoimmune diseases for fear the treatment would induce a disease flare, the researchers noted.
Small studies have suggested that people with inflammatory arthritis or connective tissue diseases have higher rates of IRAEs with immunotherapy, but it is unclear how often these events represented flares of their disease or new autoimmune events, and whether the events had any predictive significance for cancer survival.
In this study, researchers performed a retrospective review of medical records and identified 16 patients with rheumatologic diseases who had received checkpoint inhibitor therapy at the Mayo Clinic between 2011 and 2016.
The most common rheumatologic diseases among the 16 patients were rheumatoid arthritis, polymyalgia rheumatica, Sjögren’s syndrome, and systemic lupus erythematosus, and the most common cancers were malignant melanoma, pulmonary malignancies, and non-Hodgkin lymphoma. Seven of the patients were receiving immunosuppressive therapy or glucocorticoids for their rheumatologic disease upon initiation of a checkpoint inhibitor.
Ten patients had received a prior disease-modifying antirheumatic drug, but only two patients were still taking this at the time of ICI initiation.
Results showed that six of the patients (38%) had an IRAE or flare of their rheumatologic disease, two were graded as mild. All of the patients responded well to glucocorticoids and discontinuation of therapy. The most common event was colitis and just one patient had a flare of rheumatologic disease.
“This is consistent with what is currently known about the management of IRAEs,” the research team wrote. “This study adds further support to the emerging notion that the rate of IRAEs is not necessarily higher in this group compared to the general population.”
The type and severity of rheumatologic disease may play an important role in both the risk of disease flare and IRAEs, a factor that they were unable to assess in the current study, the researchers wrote.
“Further large, prospective studies are needed to address the link between the type, severity, and concurrent rheumatologic disease activity on the risk of flare and IRAE. It is possible that patients with more severe or active disease are at higher risk for these complications,” they wrote.
While patients in the study did not appear to have significantly increased incidence or severity of adverse effects, the research team advised that “treatment decisions must factor in clinical judgement.”
They noted that some studies had proposed predictive biomarkers, pretreatment workup, and monitoring, but this advice was based on a small body of evidence.
“Larger, prospective studies will be necessary to validate these findings and establish evidence-based guidelines for appropriate identification and rating of the rheumatologic IRAEs as well as their treatment, such that patients can continue to receive potentially life-saving cancer treatments,” they wrote.
One of the researchers reported advisory board membership with Bristol-Myers Squibb.
SOURCE: Richter M et al. Arthritis Rheumatol. 2018 Jan 24. doi: 10.1002/art.40397.
FROM ARTHRITIS AND RHEUMATOLOGY
Key clinical point:
Major finding: Six of 16 patients (38%) with rheumatologic disease and cancer had an IRAE or flare of their rheumatologic disease.
Study details: A single-center, retrospective records review to identify patients with rheumatologic diseases who had received checkpoint inhibitor therapy at Mayo Clinic between 2011 and 2016.
Disclosures: One of the authors reported advisory board membership with Bristol-Myers Squibb.
Source: Richter M et al. Arthritis Rheumatol. 2018 Jan 24. doi: 10.1002/art.40397.
Sharing Our Homes With Allergens
No shocker here: > 90% of American homes have ≥ 3 detectable allergens, and 73% have at least 1 allergen at elevated levels, acceding to the largest U.S. indoor allergen study to date.
Using data from National Institute of Environmental Health Sciences (NHANES) 2005-2006, researchers studied levels of 8 common allergens (cat, dog, cockroach, mouse, rat, mold, and 2 types of dust mite allergens) in nearly 7,000 homes.
Mobile homes, older homes, rental homes, and rural homes were more likely to have higher amounts of indoor allergens, as were homes with pets and pests.
Elevated levels of dust mites were more common in the South and Northeast and humid regions. Cat and dust mite allergens were more common in rural settings compared with urban.
The NHANES 2005-2006 data allowed national comparisons for the first time of exposure and sensitization. Men and non-Hispanic blacks were less likely to be exposed to multiple allergens, and sensitization was more common in those groups compared with women and other racial groups, respectively. Exposure to several elevated allergens was most prevalent in rural areas. Sensitization rates were higher in urban areas.
The researchers emphasize that the relationships between allergen exposures, allergic sensitization, and disease are complex. They also note that studies are still investigating how allergen exposures interact with other environmental and genetic factors in asthma and allergies. However, among the tips they offer: vacuum every week, wash sheets and blankets in hot water every week, and lower indoor humidity levels below 50%.
No shocker here: > 90% of American homes have ≥ 3 detectable allergens, and 73% have at least 1 allergen at elevated levels, acceding to the largest U.S. indoor allergen study to date.
Using data from National Institute of Environmental Health Sciences (NHANES) 2005-2006, researchers studied levels of 8 common allergens (cat, dog, cockroach, mouse, rat, mold, and 2 types of dust mite allergens) in nearly 7,000 homes.
Mobile homes, older homes, rental homes, and rural homes were more likely to have higher amounts of indoor allergens, as were homes with pets and pests.
Elevated levels of dust mites were more common in the South and Northeast and humid regions. Cat and dust mite allergens were more common in rural settings compared with urban.
The NHANES 2005-2006 data allowed national comparisons for the first time of exposure and sensitization. Men and non-Hispanic blacks were less likely to be exposed to multiple allergens, and sensitization was more common in those groups compared with women and other racial groups, respectively. Exposure to several elevated allergens was most prevalent in rural areas. Sensitization rates were higher in urban areas.
The researchers emphasize that the relationships between allergen exposures, allergic sensitization, and disease are complex. They also note that studies are still investigating how allergen exposures interact with other environmental and genetic factors in asthma and allergies. However, among the tips they offer: vacuum every week, wash sheets and blankets in hot water every week, and lower indoor humidity levels below 50%.
No shocker here: > 90% of American homes have ≥ 3 detectable allergens, and 73% have at least 1 allergen at elevated levels, acceding to the largest U.S. indoor allergen study to date.
Using data from National Institute of Environmental Health Sciences (NHANES) 2005-2006, researchers studied levels of 8 common allergens (cat, dog, cockroach, mouse, rat, mold, and 2 types of dust mite allergens) in nearly 7,000 homes.
Mobile homes, older homes, rental homes, and rural homes were more likely to have higher amounts of indoor allergens, as were homes with pets and pests.
Elevated levels of dust mites were more common in the South and Northeast and humid regions. Cat and dust mite allergens were more common in rural settings compared with urban.
The NHANES 2005-2006 data allowed national comparisons for the first time of exposure and sensitization. Men and non-Hispanic blacks were less likely to be exposed to multiple allergens, and sensitization was more common in those groups compared with women and other racial groups, respectively. Exposure to several elevated allergens was most prevalent in rural areas. Sensitization rates were higher in urban areas.
The researchers emphasize that the relationships between allergen exposures, allergic sensitization, and disease are complex. They also note that studies are still investigating how allergen exposures interact with other environmental and genetic factors in asthma and allergies. However, among the tips they offer: vacuum every week, wash sheets and blankets in hot water every week, and lower indoor humidity levels below 50%.
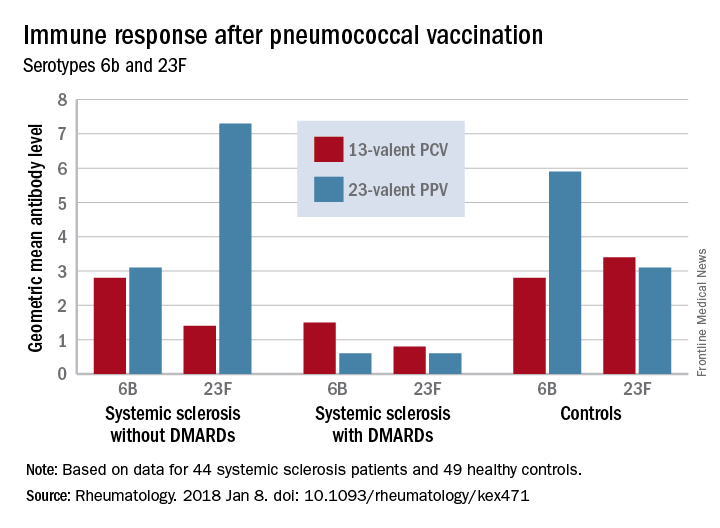
DMARDs may hamper pneumococcal vaccine response in systemic sclerosis patients
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.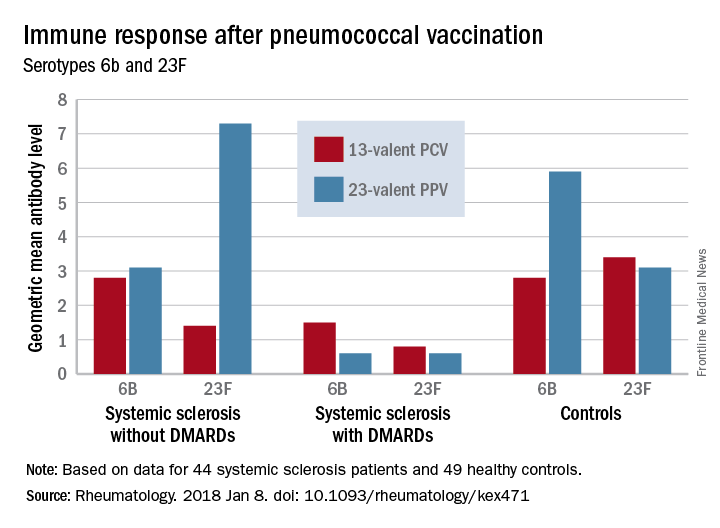
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
FROM RHEUMATOLOGY
Key clinical point:
Major finding: An increase in prevaccination antibody levels of at least twofold occurred in significantly fewer patients taking DMARDs than in patients not taking DMARDs and controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
Study details: The prospective study comprised 44 systemic sclerosis patients and 49 healthy controls.
Disclosures: None of the authors had conflicts of interest to disclose.
Source: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471
NIOSH Survey: Adherence to Best Practices is Falling Short
The health care industry sees more nonfatal occupational injury and illness than other industry sectors. One reason may be that employers and employees are not adhering to health and safety best practices, according to a recent National Institute for Occupational Safety and Health (NIOSH) survey of nearly 11,000 workers in a wide range of professional, technical, and support occupations.
The survey—the largest federally sponsored survey addressing chemical hazards in health care—found lapses everywhere. For instance, when administering aerosolized pentamidine, 69% of health care workers did not always wear protective gowns, 49% did not always wear respiratory protection, and 22% did not always wear protective gloves.
When NIOSH compared responses from respondents who administered pentamidine versus those who administered antibiotics, it found that those who administered pentamidine were more likely to be trained, familiar with employer standard procedures, and use eye/face protection and respirators. The major barrier to using personal protective equipment for those who administered either pentamidine or antibiotics include “the perception that aerosolized medications are not as dangerous as other chemicals.” Moreover, NIOSH concluded that there was “a belief” that employers do not fully appreciate the potential adverse health effects associated with exposure to the drugs, and thus do not prioritize adherence.
The survey also revealed that best practices to minimize exposure to high-level disinfectants are not universally implemented: 17% of respondents said they never received training. Of those who received training, 42% said it was > 12 months before, and 19% said employer safe handling procedures were unavailable. Nearly half of respondents did not always wear a protective gown when handling the products; 9% did not always wear protective gloves.
Among other findings: use of anesthesia machines with scavenging systems was “nearly universal.” However, adherence to other best practices was lacking. For instance, one third of health care workers who administered anesthetic gases to children and 14% of those with adult patients started the anesthetic gas flow before the delivery mask or airway mask was applied to the patient. And, 18% of respondents said they never received training. Of those who did receive training, 81% said it had been > 12 months before. Not surprisingly, NIOSH concludes that findings from the survey show that best practices have not been implemented and adherence is “not universal.”
The health care industry sees more nonfatal occupational injury and illness than other industry sectors. One reason may be that employers and employees are not adhering to health and safety best practices, according to a recent National Institute for Occupational Safety and Health (NIOSH) survey of nearly 11,000 workers in a wide range of professional, technical, and support occupations.
The survey—the largest federally sponsored survey addressing chemical hazards in health care—found lapses everywhere. For instance, when administering aerosolized pentamidine, 69% of health care workers did not always wear protective gowns, 49% did not always wear respiratory protection, and 22% did not always wear protective gloves.
When NIOSH compared responses from respondents who administered pentamidine versus those who administered antibiotics, it found that those who administered pentamidine were more likely to be trained, familiar with employer standard procedures, and use eye/face protection and respirators. The major barrier to using personal protective equipment for those who administered either pentamidine or antibiotics include “the perception that aerosolized medications are not as dangerous as other chemicals.” Moreover, NIOSH concluded that there was “a belief” that employers do not fully appreciate the potential adverse health effects associated with exposure to the drugs, and thus do not prioritize adherence.
The survey also revealed that best practices to minimize exposure to high-level disinfectants are not universally implemented: 17% of respondents said they never received training. Of those who received training, 42% said it was > 12 months before, and 19% said employer safe handling procedures were unavailable. Nearly half of respondents did not always wear a protective gown when handling the products; 9% did not always wear protective gloves.
Among other findings: use of anesthesia machines with scavenging systems was “nearly universal.” However, adherence to other best practices was lacking. For instance, one third of health care workers who administered anesthetic gases to children and 14% of those with adult patients started the anesthetic gas flow before the delivery mask or airway mask was applied to the patient. And, 18% of respondents said they never received training. Of those who did receive training, 81% said it had been > 12 months before. Not surprisingly, NIOSH concludes that findings from the survey show that best practices have not been implemented and adherence is “not universal.”
The health care industry sees more nonfatal occupational injury and illness than other industry sectors. One reason may be that employers and employees are not adhering to health and safety best practices, according to a recent National Institute for Occupational Safety and Health (NIOSH) survey of nearly 11,000 workers in a wide range of professional, technical, and support occupations.
The survey—the largest federally sponsored survey addressing chemical hazards in health care—found lapses everywhere. For instance, when administering aerosolized pentamidine, 69% of health care workers did not always wear protective gowns, 49% did not always wear respiratory protection, and 22% did not always wear protective gloves.
When NIOSH compared responses from respondents who administered pentamidine versus those who administered antibiotics, it found that those who administered pentamidine were more likely to be trained, familiar with employer standard procedures, and use eye/face protection and respirators. The major barrier to using personal protective equipment for those who administered either pentamidine or antibiotics include “the perception that aerosolized medications are not as dangerous as other chemicals.” Moreover, NIOSH concluded that there was “a belief” that employers do not fully appreciate the potential adverse health effects associated with exposure to the drugs, and thus do not prioritize adherence.
The survey also revealed that best practices to minimize exposure to high-level disinfectants are not universally implemented: 17% of respondents said they never received training. Of those who received training, 42% said it was > 12 months before, and 19% said employer safe handling procedures were unavailable. Nearly half of respondents did not always wear a protective gown when handling the products; 9% did not always wear protective gloves.
Among other findings: use of anesthesia machines with scavenging systems was “nearly universal.” However, adherence to other best practices was lacking. For instance, one third of health care workers who administered anesthetic gases to children and 14% of those with adult patients started the anesthetic gas flow before the delivery mask or airway mask was applied to the patient. And, 18% of respondents said they never received training. Of those who did receive training, 81% said it had been > 12 months before. Not surprisingly, NIOSH concludes that findings from the survey show that best practices have not been implemented and adherence is “not universal.”
FDA grants priority review to CAR T-cell therapy for DLBCL
The Food and Drug Administration has granted a priority review for the CAR T-cell therapy tisagenlecleucel suspension, formerly CTL019, for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma who are ineligible for or relapsed after autologous stem cell transplant.

The current application is based on a 6-month primary analysis from the single-arm, phase 2 JULIET clinical trial in adult patients with relapsed or refractory diffuse large B-cell lymphoma. According to results presented at ASH 2017, among 81 patients followed for at least 3 months before data cutoff, best overall response rate was 53%, and 40% had a complete response. Cytokine release syndrome (all grades) occurred in 58% of infused patients. Other grade 3 or 4 adverse events included neurologic toxicities, cytopenias lasting more than 28 days, infections, and febrile neutropenia.
Tisagenlecleucel suspension is marketed as Kymriah by Novartis.
The Food and Drug Administration has granted a priority review for the CAR T-cell therapy tisagenlecleucel suspension, formerly CTL019, for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma who are ineligible for or relapsed after autologous stem cell transplant.
The current application is based on a 6-month primary analysis from the single-arm, phase 2 JULIET clinical trial in adult patients with relapsed or refractory diffuse large B-cell lymphoma. According to results presented at ASH 2017, among 81 patients followed for at least 3 months before data cutoff, best overall response rate was 53%, and 40% had a complete response. Cytokine release syndrome (all grades) occurred in 58% of infused patients. Other grade 3 or 4 adverse events included neurologic toxicities, cytopenias lasting more than 28 days, infections, and febrile neutropenia.
Tisagenlecleucel suspension is marketed as Kymriah by Novartis.
The Food and Drug Administration has granted a priority review for the CAR T-cell therapy tisagenlecleucel suspension, formerly CTL019, for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma who are ineligible for or relapsed after autologous stem cell transplant.
The current application is based on a 6-month primary analysis from the single-arm, phase 2 JULIET clinical trial in adult patients with relapsed or refractory diffuse large B-cell lymphoma. According to results presented at ASH 2017, among 81 patients followed for at least 3 months before data cutoff, best overall response rate was 53%, and 40% had a complete response. Cytokine release syndrome (all grades) occurred in 58% of infused patients. Other grade 3 or 4 adverse events included neurologic toxicities, cytopenias lasting more than 28 days, infections, and febrile neutropenia.
Tisagenlecleucel suspension is marketed as Kymriah by Novartis.