User login
CPAP adherence linked to reduced readmissions
Hospitalized patients with obstructive sleep apnea (OSA) who were nonadherent to continuous positive airway pressure (CPAP) treatment were more than three times as likely to be readmitted for complications, according to a study.
Since preventable causes of readmission like congestive heart failure, obstructive lung disease, and diabetes are connected to OSA, boosting adherence rates to sleep apnea treatment could be an effective way to mitigate these risks.
Investigators gathered data for 345 hospitalized patients with OSA who were admitted to the VA Long Beach (Calif.) Healthcare System between January 2007 and December 2015.
Both the adherent and nonadherent groups were mostly white males. The 183 adherent patients were, on average, slightly older than the patients in the nonadherent group (66.3 vs. 62.3 years), while the nonadherent group had a larger proportion of African Americans (19.1%) than did the adherent group (10.4%).
In an analysis of both groups, 28% of nonadherent patients were readmitted within 30 days of discharge, compared with 10.2% of those in the adherent group (P less than .001). Readmission rates were significantly higher for nonadherent patients brought in for all-causes (adjusted odds ratio, 3.52; P less than .001), as were their rates of cardiovascular-related readmission (AOR, 2.31; P = .02).
The cardiovascular-related readmissions were most often caused by atrial fibrillation (29%), myocardial ischemia (22.5%), and congestive heart failure (19.3%) in the group who were not using CPAP. In this same group, urologic problems (10.7%), infections (8.0%), and psychiatric issues (5.3%) were the most common causes for hospital readmissions.
Investigators were surprised to find that the rate of pulmonary-related readmissions was not higher among nonadherent patients, considering the shared characteristics of OSA and COPD.
While nonadherent patients had an adjusted rate of pulmonary-related readmissions of 3.66, the difference between nonadherent and adherent patients was not significant.
“Those with OSA and COPD are considered to have overlap syndrome and, without CPAP therapy, are at higher risk for COPD exacerbation requiring hospitalization, pulmonary hypertension, and mortality,” according to Dr. Truong and her colleagues. “However, the number of patients with pulmonary readmissions was very small, and analysis did not reach statistical or clinical significance.”
Given the single-center nature of the study, these findings have limited generalizability. The study may also have been underpowered to uncover certain differences between the two groups because of the small population size.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: K. Truong et al. J Clin Sleep Med. 2018;14(2):183–9.
The comorbidities associated with obstructive sleep apnea (OSA), such as heart failure, coronary artery disease, diabetes, and stroke, can be detrimental to patients’ care and commonly lead to hospitalization. Not only are these diseases interfering with successful treatment, but financial penalties linked to 30-day readmissions have economic implications for hospitals as well. Increasing CPAP adherence, therefore, may be a low-cost tool to improve hospital outcomes. Dr. Truong and her colleagues find compelling data showing the association of CPAP adherence and reduced 30-day readmissions. However, more work is needed before we can fully back the idea that CPAP adherence will prevent readmissions. While many studies have shown associations between OSA and cardiovascular events, there are no large, randomized trials that show the cardiovascular benefit of CPAP. The current theory is that patients who are adherent to CPAP are more likely to be healthier individuals, which makes them less likely to exhibit the comorbidities that would cause readmissions. A large randomized trial is the next logical step, and with OSA costs estimated at $2,000 annually per patient, it is a step worth pursuing.
Lucas M. Donovan, MD, is a pulmonologist at the University of Washington, Seattle. Martha E. Billings, MD, is an assistant professor in the division of pulmonary and critical care medicine at the University of Washington, Seattle. They reported no conflicts of interest.
The comorbidities associated with obstructive sleep apnea (OSA), such as heart failure, coronary artery disease, diabetes, and stroke, can be detrimental to patients’ care and commonly lead to hospitalization. Not only are these diseases interfering with successful treatment, but financial penalties linked to 30-day readmissions have economic implications for hospitals as well. Increasing CPAP adherence, therefore, may be a low-cost tool to improve hospital outcomes. Dr. Truong and her colleagues find compelling data showing the association of CPAP adherence and reduced 30-day readmissions. However, more work is needed before we can fully back the idea that CPAP adherence will prevent readmissions. While many studies have shown associations between OSA and cardiovascular events, there are no large, randomized trials that show the cardiovascular benefit of CPAP. The current theory is that patients who are adherent to CPAP are more likely to be healthier individuals, which makes them less likely to exhibit the comorbidities that would cause readmissions. A large randomized trial is the next logical step, and with OSA costs estimated at $2,000 annually per patient, it is a step worth pursuing.
Lucas M. Donovan, MD, is a pulmonologist at the University of Washington, Seattle. Martha E. Billings, MD, is an assistant professor in the division of pulmonary and critical care medicine at the University of Washington, Seattle. They reported no conflicts of interest.
The comorbidities associated with obstructive sleep apnea (OSA), such as heart failure, coronary artery disease, diabetes, and stroke, can be detrimental to patients’ care and commonly lead to hospitalization. Not only are these diseases interfering with successful treatment, but financial penalties linked to 30-day readmissions have economic implications for hospitals as well. Increasing CPAP adherence, therefore, may be a low-cost tool to improve hospital outcomes. Dr. Truong and her colleagues find compelling data showing the association of CPAP adherence and reduced 30-day readmissions. However, more work is needed before we can fully back the idea that CPAP adherence will prevent readmissions. While many studies have shown associations between OSA and cardiovascular events, there are no large, randomized trials that show the cardiovascular benefit of CPAP. The current theory is that patients who are adherent to CPAP are more likely to be healthier individuals, which makes them less likely to exhibit the comorbidities that would cause readmissions. A large randomized trial is the next logical step, and with OSA costs estimated at $2,000 annually per patient, it is a step worth pursuing.
Lucas M. Donovan, MD, is a pulmonologist at the University of Washington, Seattle. Martha E. Billings, MD, is an assistant professor in the division of pulmonary and critical care medicine at the University of Washington, Seattle. They reported no conflicts of interest.
Hospitalized patients with obstructive sleep apnea (OSA) who were nonadherent to continuous positive airway pressure (CPAP) treatment were more than three times as likely to be readmitted for complications, according to a study.
Since preventable causes of readmission like congestive heart failure, obstructive lung disease, and diabetes are connected to OSA, boosting adherence rates to sleep apnea treatment could be an effective way to mitigate these risks.
Investigators gathered data for 345 hospitalized patients with OSA who were admitted to the VA Long Beach (Calif.) Healthcare System between January 2007 and December 2015.
Both the adherent and nonadherent groups were mostly white males. The 183 adherent patients were, on average, slightly older than the patients in the nonadherent group (66.3 vs. 62.3 years), while the nonadherent group had a larger proportion of African Americans (19.1%) than did the adherent group (10.4%).
In an analysis of both groups, 28% of nonadherent patients were readmitted within 30 days of discharge, compared with 10.2% of those in the adherent group (P less than .001). Readmission rates were significantly higher for nonadherent patients brought in for all-causes (adjusted odds ratio, 3.52; P less than .001), as were their rates of cardiovascular-related readmission (AOR, 2.31; P = .02).
The cardiovascular-related readmissions were most often caused by atrial fibrillation (29%), myocardial ischemia (22.5%), and congestive heart failure (19.3%) in the group who were not using CPAP. In this same group, urologic problems (10.7%), infections (8.0%), and psychiatric issues (5.3%) were the most common causes for hospital readmissions.
Investigators were surprised to find that the rate of pulmonary-related readmissions was not higher among nonadherent patients, considering the shared characteristics of OSA and COPD.
While nonadherent patients had an adjusted rate of pulmonary-related readmissions of 3.66, the difference between nonadherent and adherent patients was not significant.
“Those with OSA and COPD are considered to have overlap syndrome and, without CPAP therapy, are at higher risk for COPD exacerbation requiring hospitalization, pulmonary hypertension, and mortality,” according to Dr. Truong and her colleagues. “However, the number of patients with pulmonary readmissions was very small, and analysis did not reach statistical or clinical significance.”
Given the single-center nature of the study, these findings have limited generalizability. The study may also have been underpowered to uncover certain differences between the two groups because of the small population size.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: K. Truong et al. J Clin Sleep Med. 2018;14(2):183–9.
Hospitalized patients with obstructive sleep apnea (OSA) who were nonadherent to continuous positive airway pressure (CPAP) treatment were more than three times as likely to be readmitted for complications, according to a study.
Since preventable causes of readmission like congestive heart failure, obstructive lung disease, and diabetes are connected to OSA, boosting adherence rates to sleep apnea treatment could be an effective way to mitigate these risks.
Investigators gathered data for 345 hospitalized patients with OSA who were admitted to the VA Long Beach (Calif.) Healthcare System between January 2007 and December 2015.
Both the adherent and nonadherent groups were mostly white males. The 183 adherent patients were, on average, slightly older than the patients in the nonadherent group (66.3 vs. 62.3 years), while the nonadherent group had a larger proportion of African Americans (19.1%) than did the adherent group (10.4%).
In an analysis of both groups, 28% of nonadherent patients were readmitted within 30 days of discharge, compared with 10.2% of those in the adherent group (P less than .001). Readmission rates were significantly higher for nonadherent patients brought in for all-causes (adjusted odds ratio, 3.52; P less than .001), as were their rates of cardiovascular-related readmission (AOR, 2.31; P = .02).
The cardiovascular-related readmissions were most often caused by atrial fibrillation (29%), myocardial ischemia (22.5%), and congestive heart failure (19.3%) in the group who were not using CPAP. In this same group, urologic problems (10.7%), infections (8.0%), and psychiatric issues (5.3%) were the most common causes for hospital readmissions.
Investigators were surprised to find that the rate of pulmonary-related readmissions was not higher among nonadherent patients, considering the shared characteristics of OSA and COPD.
While nonadherent patients had an adjusted rate of pulmonary-related readmissions of 3.66, the difference between nonadherent and adherent patients was not significant.
“Those with OSA and COPD are considered to have overlap syndrome and, without CPAP therapy, are at higher risk for COPD exacerbation requiring hospitalization, pulmonary hypertension, and mortality,” according to Dr. Truong and her colleagues. “However, the number of patients with pulmonary readmissions was very small, and analysis did not reach statistical or clinical significance.”
Given the single-center nature of the study, these findings have limited generalizability. The study may also have been underpowered to uncover certain differences between the two groups because of the small population size.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
SOURCE: K. Truong et al. J Clin Sleep Med. 2018;14(2):183–9.
FROM THE JOURNAL OF CLINICAL SLEEP MEDICINE
Key clinical point:
Major finding: CPAP-nonadherent patients were 3.5 times more likely to be readmitted within 30 days.
Study details: A retrospective study of 345 patients with obstructive sleep apnea who were hospitalized at a Veterans Affairs hospital between Jan. 1, 2007, and Dec. 31, 2015.
Disclosures: Investigators reported no relevant financial disclosures.
Source: K. Truong et al. J Clin Sleep Med. 2018;14(2):183-9.
Novel Treatment Helps Heal Diabetic Foot Ulcers
About 30 million people in the U.S. have diabetes, and about 25% of those will have a foot ulcer at some point. When circulation is so poor that the ulcer does not heal, or when treatment cannot stop infection, amputation may be necessary. Diabetes is the leading cause of lower limb amputations.
The FDA has approved a new treatment to help heal diabetic foot ulcers. The Dermapace System (Sanuwave, Inc., Suwanee, GA) sends shock waves to mechanically stimulate the wound. The treatment is intended for adult patients with chronic foot ulcers with wound areas no larger than 16 cm2, extending through the epidermis, dermis, tendon, or capsule, but without bone exposure. It is used along with standard diabetic ulcer care.
In 2 multicenter studies of 336 patients, patients were given 1 to 7 treatments over 24 weeks. The shock wave systems increased wound healing by 44%. The patients treated with a sham shock wave therapy had a 30% wound closure rate.
About 30 million people in the U.S. have diabetes, and about 25% of those will have a foot ulcer at some point. When circulation is so poor that the ulcer does not heal, or when treatment cannot stop infection, amputation may be necessary. Diabetes is the leading cause of lower limb amputations.
The FDA has approved a new treatment to help heal diabetic foot ulcers. The Dermapace System (Sanuwave, Inc., Suwanee, GA) sends shock waves to mechanically stimulate the wound. The treatment is intended for adult patients with chronic foot ulcers with wound areas no larger than 16 cm2, extending through the epidermis, dermis, tendon, or capsule, but without bone exposure. It is used along with standard diabetic ulcer care.
In 2 multicenter studies of 336 patients, patients were given 1 to 7 treatments over 24 weeks. The shock wave systems increased wound healing by 44%. The patients treated with a sham shock wave therapy had a 30% wound closure rate.
About 30 million people in the U.S. have diabetes, and about 25% of those will have a foot ulcer at some point. When circulation is so poor that the ulcer does not heal, or when treatment cannot stop infection, amputation may be necessary. Diabetes is the leading cause of lower limb amputations.
The FDA has approved a new treatment to help heal diabetic foot ulcers. The Dermapace System (Sanuwave, Inc., Suwanee, GA) sends shock waves to mechanically stimulate the wound. The treatment is intended for adult patients with chronic foot ulcers with wound areas no larger than 16 cm2, extending through the epidermis, dermis, tendon, or capsule, but without bone exposure. It is used along with standard diabetic ulcer care.
In 2 multicenter studies of 336 patients, patients were given 1 to 7 treatments over 24 weeks. The shock wave systems increased wound healing by 44%. The patients treated with a sham shock wave therapy had a 30% wound closure rate.
NF-kappaB pathway could help solve resistance problem in mantle cell lymphoma
B-cell receptor (BCR) resistance is a significant treatment obstacle in mantle cell lymphoma (MCL), but a new study highlights the potential protective role for cells expressing specific ligands.
Hilka Rauert-Wunderlich, of the University of Würzburg and Comprehensive Cancer Center, Germany, and her colleagues stimulated the REC-1, MAVER-1, and L-929 cell lines to show the role of the alternative nuclear factor-kappa B (NF-kappaB) pathway and the tumor necrosis factor ligand CD40L.
Viability assays showed a protective effect of CD40L prestimulation on BCR inhibitor treatment. The effect was detectable and significant in the REC-1 cell line for both ibrutinib and sotrastaurin at “clinically relevant concentrations” and in the resistant MAVER-1 cell line at “nonphysiologically high” sotrastaurin concentrations. CD40L stimulation also induced alternative NF-kappaB pathway signaling in both REC-1 and MAVER-1 cell lines.
“The data presented in this study argue for the protective potential of microenvironmentally mediated activation of the alternative [NF-kappaB] pathway in MCL cell against BCR signaling-associated drugs, which might represent a physiologic niche for MCL relapse. Additionally, these data provide evidence for the potential of the alternative [NF-kappaB] pathway as a possible therapeutic target in MCL,” the researchers wrote in Cell Death & Disease.
The researchers reported having no conflicts of interest.
SOURCE: Rauert-Wunderlich H et al. Cell Death Dis. 2018 Jan 24. doi: 10.1038/s41419-017-0157-6.
B-cell receptor (BCR) resistance is a significant treatment obstacle in mantle cell lymphoma (MCL), but a new study highlights the potential protective role for cells expressing specific ligands.
Hilka Rauert-Wunderlich, of the University of Würzburg and Comprehensive Cancer Center, Germany, and her colleagues stimulated the REC-1, MAVER-1, and L-929 cell lines to show the role of the alternative nuclear factor-kappa B (NF-kappaB) pathway and the tumor necrosis factor ligand CD40L.
Viability assays showed a protective effect of CD40L prestimulation on BCR inhibitor treatment. The effect was detectable and significant in the REC-1 cell line for both ibrutinib and sotrastaurin at “clinically relevant concentrations” and in the resistant MAVER-1 cell line at “nonphysiologically high” sotrastaurin concentrations. CD40L stimulation also induced alternative NF-kappaB pathway signaling in both REC-1 and MAVER-1 cell lines.
“The data presented in this study argue for the protective potential of microenvironmentally mediated activation of the alternative [NF-kappaB] pathway in MCL cell against BCR signaling-associated drugs, which might represent a physiologic niche for MCL relapse. Additionally, these data provide evidence for the potential of the alternative [NF-kappaB] pathway as a possible therapeutic target in MCL,” the researchers wrote in Cell Death & Disease.
The researchers reported having no conflicts of interest.
SOURCE: Rauert-Wunderlich H et al. Cell Death Dis. 2018 Jan 24. doi: 10.1038/s41419-017-0157-6.
B-cell receptor (BCR) resistance is a significant treatment obstacle in mantle cell lymphoma (MCL), but a new study highlights the potential protective role for cells expressing specific ligands.
Hilka Rauert-Wunderlich, of the University of Würzburg and Comprehensive Cancer Center, Germany, and her colleagues stimulated the REC-1, MAVER-1, and L-929 cell lines to show the role of the alternative nuclear factor-kappa B (NF-kappaB) pathway and the tumor necrosis factor ligand CD40L.
Viability assays showed a protective effect of CD40L prestimulation on BCR inhibitor treatment. The effect was detectable and significant in the REC-1 cell line for both ibrutinib and sotrastaurin at “clinically relevant concentrations” and in the resistant MAVER-1 cell line at “nonphysiologically high” sotrastaurin concentrations. CD40L stimulation also induced alternative NF-kappaB pathway signaling in both REC-1 and MAVER-1 cell lines.
“The data presented in this study argue for the protective potential of microenvironmentally mediated activation of the alternative [NF-kappaB] pathway in MCL cell against BCR signaling-associated drugs, which might represent a physiologic niche for MCL relapse. Additionally, these data provide evidence for the potential of the alternative [NF-kappaB] pathway as a possible therapeutic target in MCL,” the researchers wrote in Cell Death & Disease.
The researchers reported having no conflicts of interest.
SOURCE: Rauert-Wunderlich H et al. Cell Death Dis. 2018 Jan 24. doi: 10.1038/s41419-017-0157-6.
FROM CELL DEATH & DISEASE
Flu increase may be slowing
A bit of revisionist history has outpatient influenza activity at a lower level than was reported last week, even though it hasn’t dropped.
The proportion of outpatient visits for influenza-like illness (ILI) for the week ending Feb. 10 was 7.5%, according to the Centers for Disease Control. That is lower than the 7.7% previously reported for the week ending Feb. 3, which would seem to be a drop, but the CDC also has revised that earlier number to 7.5%, so there is no change. (This is not the first time an earlier ILI level has been retroactively lowered: The figure reported for the week ending Jan. 13 was revised in the following report from 6.3% down to 6.0%.)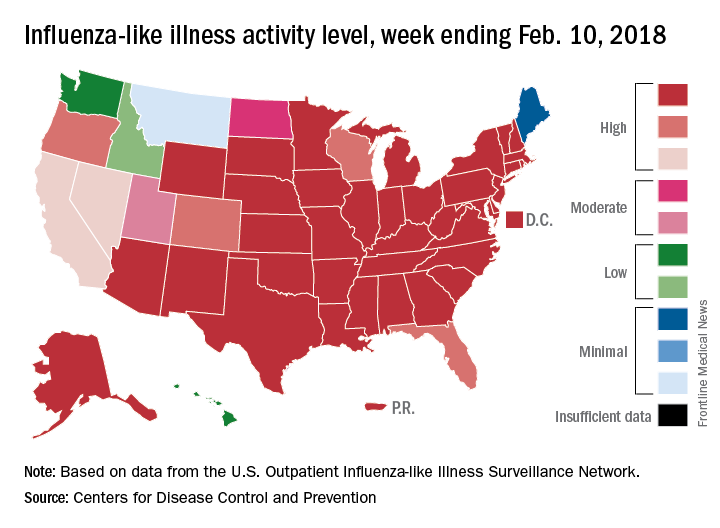
Hospital visits, however, continue to rise at record levels. The cumulative rate for the week ending Feb. 10 was 67.9 visits per 100,000 population, which is higher than the same week for the 2014-2015 (52.9 per 100,000) when flu hospitalizations for the season hit a high of 710,000. Flu-related pediatric deaths also went up, with 22 new reports; this brings the total to 84 for the 2017-2018 season.
A bit of revisionist history has outpatient influenza activity at a lower level than was reported last week, even though it hasn’t dropped.
The proportion of outpatient visits for influenza-like illness (ILI) for the week ending Feb. 10 was 7.5%, according to the Centers for Disease Control. That is lower than the 7.7% previously reported for the week ending Feb. 3, which would seem to be a drop, but the CDC also has revised that earlier number to 7.5%, so there is no change. (This is not the first time an earlier ILI level has been retroactively lowered: The figure reported for the week ending Jan. 13 was revised in the following report from 6.3% down to 6.0%.)
Hospital visits, however, continue to rise at record levels. The cumulative rate for the week ending Feb. 10 was 67.9 visits per 100,000 population, which is higher than the same week for the 2014-2015 (52.9 per 100,000) when flu hospitalizations for the season hit a high of 710,000. Flu-related pediatric deaths also went up, with 22 new reports; this brings the total to 84 for the 2017-2018 season.
A bit of revisionist history has outpatient influenza activity at a lower level than was reported last week, even though it hasn’t dropped.
The proportion of outpatient visits for influenza-like illness (ILI) for the week ending Feb. 10 was 7.5%, according to the Centers for Disease Control. That is lower than the 7.7% previously reported for the week ending Feb. 3, which would seem to be a drop, but the CDC also has revised that earlier number to 7.5%, so there is no change. (This is not the first time an earlier ILI level has been retroactively lowered: The figure reported for the week ending Jan. 13 was revised in the following report from 6.3% down to 6.0%.)
Hospital visits, however, continue to rise at record levels. The cumulative rate for the week ending Feb. 10 was 67.9 visits per 100,000 population, which is higher than the same week for the 2014-2015 (52.9 per 100,000) when flu hospitalizations for the season hit a high of 710,000. Flu-related pediatric deaths also went up, with 22 new reports; this brings the total to 84 for the 2017-2018 season.
FROM THE CDC WEEKLY U.S. INFLUENZA SURVEILLANCE REPORT
Helping Veterans Stop Smoking
Three in 10 U.S. veterans used some form of tobacco during 2010-2015—a higher number than among nonveterans across all age groups except men aged ≥ 50 years, according to a CDC analysis of data from the National Survey on Drug Use and Health. More than one-third of the veterans surveyed started smoking after enlisting.
The analysis also found that > 60% of the veterans who used tobacco products had no health insurance, more than half were living in poverty, and 48% reported serious psychological distress.
The toll is significant not only for the smokers and their families, but also for the health care system. The researchers estimate that during 2010, VHA spent nearly $3 billion on smoking-related ambulatory care, prescription drugs, hospitalization, and home health care.
“VA has more tobacco use treatment options available than ever,” said Kim Hamlett-Berry, PhD, program director of VA Tobacco and Health Policy, and that has led to declines in rates of smoking. She notes that the 2015 VA Survey of Enrollees reported that 16.8% of veterans enrolled for health care in VA identified as a current smoker.
In addition to the quit lines already available (800-QUIT-VET, 800-QUIT-NOW, and https://smokefree.gov/VET), veterans can access quit services through TRICARE. VA treatment centers also have integrated smoking cessation programs into treatment for PTSD and other disorders. Smokers with psychiatric illness are more likely to die of smoking-related diseases than of complications from their mental illness or substance use disorders, Hamlett-Berry said at an American Psychological Association conference in 2013. She added that people with alcohol dependence and other substance use disorders smoke at higher rates. Research shows that combining smoking cessation with substance use treatment increase patients’ likelihood of success.
The CDC says more can be done. Strategies could include promoting cessation to current military personnel and veterans, implementing tobacco-free policies at military installations and VA medical centers and clinics, increasing the age requirement to buy tobacco on military bases to 21, and eliminating tobacco product discounts through military retailers.
Three in 10 U.S. veterans used some form of tobacco during 2010-2015—a higher number than among nonveterans across all age groups except men aged ≥ 50 years, according to a CDC analysis of data from the National Survey on Drug Use and Health. More than one-third of the veterans surveyed started smoking after enlisting.
The analysis also found that > 60% of the veterans who used tobacco products had no health insurance, more than half were living in poverty, and 48% reported serious psychological distress.
The toll is significant not only for the smokers and their families, but also for the health care system. The researchers estimate that during 2010, VHA spent nearly $3 billion on smoking-related ambulatory care, prescription drugs, hospitalization, and home health care.
“VA has more tobacco use treatment options available than ever,” said Kim Hamlett-Berry, PhD, program director of VA Tobacco and Health Policy, and that has led to declines in rates of smoking. She notes that the 2015 VA Survey of Enrollees reported that 16.8% of veterans enrolled for health care in VA identified as a current smoker.
In addition to the quit lines already available (800-QUIT-VET, 800-QUIT-NOW, and https://smokefree.gov/VET), veterans can access quit services through TRICARE. VA treatment centers also have integrated smoking cessation programs into treatment for PTSD and other disorders. Smokers with psychiatric illness are more likely to die of smoking-related diseases than of complications from their mental illness or substance use disorders, Hamlett-Berry said at an American Psychological Association conference in 2013. She added that people with alcohol dependence and other substance use disorders smoke at higher rates. Research shows that combining smoking cessation with substance use treatment increase patients’ likelihood of success.
The CDC says more can be done. Strategies could include promoting cessation to current military personnel and veterans, implementing tobacco-free policies at military installations and VA medical centers and clinics, increasing the age requirement to buy tobacco on military bases to 21, and eliminating tobacco product discounts through military retailers.
Three in 10 U.S. veterans used some form of tobacco during 2010-2015—a higher number than among nonveterans across all age groups except men aged ≥ 50 years, according to a CDC analysis of data from the National Survey on Drug Use and Health. More than one-third of the veterans surveyed started smoking after enlisting.
The analysis also found that > 60% of the veterans who used tobacco products had no health insurance, more than half were living in poverty, and 48% reported serious psychological distress.
The toll is significant not only for the smokers and their families, but also for the health care system. The researchers estimate that during 2010, VHA spent nearly $3 billion on smoking-related ambulatory care, prescription drugs, hospitalization, and home health care.
“VA has more tobacco use treatment options available than ever,” said Kim Hamlett-Berry, PhD, program director of VA Tobacco and Health Policy, and that has led to declines in rates of smoking. She notes that the 2015 VA Survey of Enrollees reported that 16.8% of veterans enrolled for health care in VA identified as a current smoker.
In addition to the quit lines already available (800-QUIT-VET, 800-QUIT-NOW, and https://smokefree.gov/VET), veterans can access quit services through TRICARE. VA treatment centers also have integrated smoking cessation programs into treatment for PTSD and other disorders. Smokers with psychiatric illness are more likely to die of smoking-related diseases than of complications from their mental illness or substance use disorders, Hamlett-Berry said at an American Psychological Association conference in 2013. She added that people with alcohol dependence and other substance use disorders smoke at higher rates. Research shows that combining smoking cessation with substance use treatment increase patients’ likelihood of success.
The CDC says more can be done. Strategies could include promoting cessation to current military personnel and veterans, implementing tobacco-free policies at military installations and VA medical centers and clinics, increasing the age requirement to buy tobacco on military bases to 21, and eliminating tobacco product discounts through military retailers.
Treating Cancer Fatigue With Placebo
Cancer-related fatigue can linger long after treatments are ended, making daily activities harder and diminishing quality of life (QOL). But researchers from University of Alabama in Birmingham and Harvard Medical School in Boston suggest a nonpharmaceutical way to help patients feel better: placebo.
They compared an open-label placebo with treatment as usual in patients with cancer-related fatigue in a 21-day controlled trial. The patients had completed cancer treatment 6 months to 10 years prior to enrollment. Of 74 patients, 28 reported a moderate level of fatigue and 46 reported a severe level. The mean fatigue scores at baseline were similar for both groups.
The participants randomly assigned to placebo took 2 placebo pills twice a day. At 21 days, the average difference in scores was statistically significant. The placebo group reported a 29% improvement in fatigue severity and a 39% improvement in fatigue-disrupted QOL. Put another way, 76% of the placebo group had a change score above the mean change score of the usual-treatment group. The results were clinically meaningful, the researchers say. Moreover, there were no reported adverse events or adverse effects.
After that main study, the researchers also conducted a 21-day exploratory crossover extension, which began 1 week later. Their findings supported the main study results, with the same magnitude of improvement. The usual-treatment patients who chose to try the placebo also reported a similar magnitude of reductions in fatigue severity (23%) and fatigue-disrupted QOL (35%).
Interestingly, the effects seemed to be sustained, the researchers say. At day 48, there was no significant change in fatigue scores compared with day 21, an “exciting” preliminary finding they say that needs further exploration.
Source:
Hoenemeyer TW, Kaptchuk TJ, Mehta TS, Fontaine KR. Scientific Reports. 2018;8:2784.
doi:10.1038/s41598-018-20993-y.
Cancer-related fatigue can linger long after treatments are ended, making daily activities harder and diminishing quality of life (QOL). But researchers from University of Alabama in Birmingham and Harvard Medical School in Boston suggest a nonpharmaceutical way to help patients feel better: placebo.
They compared an open-label placebo with treatment as usual in patients with cancer-related fatigue in a 21-day controlled trial. The patients had completed cancer treatment 6 months to 10 years prior to enrollment. Of 74 patients, 28 reported a moderate level of fatigue and 46 reported a severe level. The mean fatigue scores at baseline were similar for both groups.
The participants randomly assigned to placebo took 2 placebo pills twice a day. At 21 days, the average difference in scores was statistically significant. The placebo group reported a 29% improvement in fatigue severity and a 39% improvement in fatigue-disrupted QOL. Put another way, 76% of the placebo group had a change score above the mean change score of the usual-treatment group. The results were clinically meaningful, the researchers say. Moreover, there were no reported adverse events or adverse effects.
After that main study, the researchers also conducted a 21-day exploratory crossover extension, which began 1 week later. Their findings supported the main study results, with the same magnitude of improvement. The usual-treatment patients who chose to try the placebo also reported a similar magnitude of reductions in fatigue severity (23%) and fatigue-disrupted QOL (35%).
Interestingly, the effects seemed to be sustained, the researchers say. At day 48, there was no significant change in fatigue scores compared with day 21, an “exciting” preliminary finding they say that needs further exploration.
Source:
Hoenemeyer TW, Kaptchuk TJ, Mehta TS, Fontaine KR. Scientific Reports. 2018;8:2784.
doi:10.1038/s41598-018-20993-y.
Cancer-related fatigue can linger long after treatments are ended, making daily activities harder and diminishing quality of life (QOL). But researchers from University of Alabama in Birmingham and Harvard Medical School in Boston suggest a nonpharmaceutical way to help patients feel better: placebo.
They compared an open-label placebo with treatment as usual in patients with cancer-related fatigue in a 21-day controlled trial. The patients had completed cancer treatment 6 months to 10 years prior to enrollment. Of 74 patients, 28 reported a moderate level of fatigue and 46 reported a severe level. The mean fatigue scores at baseline were similar for both groups.
The participants randomly assigned to placebo took 2 placebo pills twice a day. At 21 days, the average difference in scores was statistically significant. The placebo group reported a 29% improvement in fatigue severity and a 39% improvement in fatigue-disrupted QOL. Put another way, 76% of the placebo group had a change score above the mean change score of the usual-treatment group. The results were clinically meaningful, the researchers say. Moreover, there were no reported adverse events or adverse effects.
After that main study, the researchers also conducted a 21-day exploratory crossover extension, which began 1 week later. Their findings supported the main study results, with the same magnitude of improvement. The usual-treatment patients who chose to try the placebo also reported a similar magnitude of reductions in fatigue severity (23%) and fatigue-disrupted QOL (35%).
Interestingly, the effects seemed to be sustained, the researchers say. At day 48, there was no significant change in fatigue scores compared with day 21, an “exciting” preliminary finding they say that needs further exploration.
Source:
Hoenemeyer TW, Kaptchuk TJ, Mehta TS, Fontaine KR. Scientific Reports. 2018;8:2784.
doi:10.1038/s41598-018-20993-y.
At Some Veterans Homes, Aid-In-Dying Is Not An Option
California voters passed a law two years ago that allows terminally ill people to take lethal drugs to end their lives, but controversy is growing over a newer rule that effectively bans that option in the state’s eight veterans homes.
Proponents of medical aid-in-dying and residents of the Veterans Home of California-Yountville — the largest in the nation — are protesting a regulation passed last year by the California Department of Veterans Affairs, or CalVet, that requires that anyone living in the facilities must be discharged if they intend to use the law.
That’s a position shared by most — but not all — states where aid-in-dying is allowed. As more U.S. jurisdictions consider whether to legalize the practice, the status of terminally ill veterans living in state-run homes will loom large.
“It would be a terrible hardship, because I have no place to go,” said Bob Sloan, 73, who suffers from congestive heart failure and other serious cardiac problems. He said he intends to seek medical aid-in-dying if doctors certify he has six months or less to live.
“I’m not going to be a vegetable,” said Sloan, a Vietnam War-era veteran who moved into the Yountville center five years ago. “I’m not going to end up living in so much pain it’s unbearable.”
A CalVet official said the agency adopted the rule to avoid violating a federal statute that prohibits using U.S. government resources for physician-assisted death. Otherwise, the agency would jeopardize nearly $68 million in federal funds that helps run the facilities, said June Iljana, CalVet’s deputy secretary of communications.
California is not alone. Three other states where aid-in-dying is legal — Oregon, Colorado and Vermont — all prohibit use of lethal medications in state-run veterans homes.
In Montana, where aid-in-dying is allowed under a state Supreme Court ruling, officials didn’t respond to multiple requests about whether veterans would be able to use the law in the residences. However, Dr. Eric Kress, a Missoula physician who prescribes the lethal medication, says he has transferred patients to hospice, to relatives’ homes, even to extended-stay hotels to avoid conflict.
In Washington, D.C., where an aid-in-dying law took effect last summer, the Armed Forces Retirement Home won’t assist patients in any way. Those who wish to use the law would be referred to an ethics committee for individual consideration, spokesman Christopher Kelly said in an email.
Only Washington state has a policy that allows veterans to remain in government-run residences if they intend to ingest lethal medications.. At least one veteran has died in a state-run home using that law, said Heidi Audette, a spokeswoman for the state’s Department of Veterans Affairs.
Paul Sherbo, a spokesman for the U.S. Department of Veterans Affairs, said the choice is up to the states.
“VA does not mandate how states comply with federal law,” Sherbo said in an email. “There are a number of ways individual states can choose to handle such situations and still be in compliance.”
To date, none of the 2,400 residents of California’s veterans homes has formally requested medical aid-in-dying, said Iljana. That includes the more than 900 residents of the Yountville center, located about 60 miles north of San Francisco.
“We would respectfully and compassionately assist them in transferring to a hospice, family home or other location,” Iljana said in an email. “We will readmit them immediately if they change their minds.”
But Kathryn Tucker, executive director of the End of Life Liberty Project, an advocacy group that supports aid-in-dying, said that CalVet is interpreting the federal regulations too broadly and denying terminally ill veterans the right to choose a “peaceful death” through medical assistance.
“Nothing exists in the federal statute’s language that would prohibit a resident from receiving aid-in-dying services at state homes, so long as they are not provided using federal funds or employees,” she said.
Ed Warren, head of the Allied Council, a group representing veterans at the Yountville site, co-signed a letter to CalVet officials protesting the ruling.
“My point of view is that it is inhumane to expect people in the last stages of dying to go through the hullabaloo of leaving their homes,” he said.
In Washington state, a 60-year-old man diagnosed with terminal chronic obstructive pulmonary disease, or COPD, died in June 2015 after ingesting lethal drugs at the Washington Soldiers Home in Orting, where he lived.
“It was all done very much in the open,” said Chris Fruitrich, a volunteer with the group End of Life Washington, which assisted the man.
There has been no indication that the policy jeopardizes the nearly $47 million the agency receives each year in federal funds, said Audette, the state VA spokeswoman.
In California, additional protests have centered on allegations that CalVet suppressed information about the aid-in-dying law.
Critics at the Yountville home contend that CalVet passed the discharge rule quietly, with little public input. Then the agency refused to broadcast a public meeting about medical aid-in-dying on KVET, the center’s state-run, closed-circuit television station.
Iljana said the Aug. 21 meeting, led by Tucker and Dr. Robert Brody, also a supporter of aid-in-dying, violated state rules that prohibit using public resources to promote political causes.
“Free speech is great and criticizing the government is great, but not using the government’s own resources and paid staff to advocate for a change in the law,” Iljana wrote in an email to prohibit the broadcast.
That decision, however, prompted Jac Warren, 81, who has been KVET’s station manager for eight years, to resign last month in protest, citing censorship.
“What is at issue is whether a state may completely suppress the dissemination of concededly truthful information about entirely lawful activity,” Warren wrote in an email to CalVet.
The hour-long meeting, attended by about 50 people, was not propaganda, Tucker said, but “an educational event with information provided by an attorney and a physician who both specialize in their respective fields in end-of-life care.”
Bob Sloan, who works as an engineer at KVET for a $400 monthly stipend, disagreed with the decision not to broadcast the meeting on the system that serves residents of the Yountville home.
Sloan said he knows other residents who would like to be able to use California’s aid-in-dying law if their illnesses progress.
“The only other option that people have in this state is committing suicide,” he said. “If I can’t find some way of doing it legally, I’ll do it illegally.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
California voters passed a law two years ago that allows terminally ill people to take lethal drugs to end their lives, but controversy is growing over a newer rule that effectively bans that option in the state’s eight veterans homes.
Proponents of medical aid-in-dying and residents of the Veterans Home of California-Yountville — the largest in the nation — are protesting a regulation passed last year by the California Department of Veterans Affairs, or CalVet, that requires that anyone living in the facilities must be discharged if they intend to use the law.
That’s a position shared by most — but not all — states where aid-in-dying is allowed. As more U.S. jurisdictions consider whether to legalize the practice, the status of terminally ill veterans living in state-run homes will loom large.
“It would be a terrible hardship, because I have no place to go,” said Bob Sloan, 73, who suffers from congestive heart failure and other serious cardiac problems. He said he intends to seek medical aid-in-dying if doctors certify he has six months or less to live.
“I’m not going to be a vegetable,” said Sloan, a Vietnam War-era veteran who moved into the Yountville center five years ago. “I’m not going to end up living in so much pain it’s unbearable.”
A CalVet official said the agency adopted the rule to avoid violating a federal statute that prohibits using U.S. government resources for physician-assisted death. Otherwise, the agency would jeopardize nearly $68 million in federal funds that helps run the facilities, said June Iljana, CalVet’s deputy secretary of communications.
California is not alone. Three other states where aid-in-dying is legal — Oregon, Colorado and Vermont — all prohibit use of lethal medications in state-run veterans homes.
In Montana, where aid-in-dying is allowed under a state Supreme Court ruling, officials didn’t respond to multiple requests about whether veterans would be able to use the law in the residences. However, Dr. Eric Kress, a Missoula physician who prescribes the lethal medication, says he has transferred patients to hospice, to relatives’ homes, even to extended-stay hotels to avoid conflict.
In Washington, D.C., where an aid-in-dying law took effect last summer, the Armed Forces Retirement Home won’t assist patients in any way. Those who wish to use the law would be referred to an ethics committee for individual consideration, spokesman Christopher Kelly said in an email.
Only Washington state has a policy that allows veterans to remain in government-run residences if they intend to ingest lethal medications.. At least one veteran has died in a state-run home using that law, said Heidi Audette, a spokeswoman for the state’s Department of Veterans Affairs.
Paul Sherbo, a spokesman for the U.S. Department of Veterans Affairs, said the choice is up to the states.
“VA does not mandate how states comply with federal law,” Sherbo said in an email. “There are a number of ways individual states can choose to handle such situations and still be in compliance.”
To date, none of the 2,400 residents of California’s veterans homes has formally requested medical aid-in-dying, said Iljana. That includes the more than 900 residents of the Yountville center, located about 60 miles north of San Francisco.
“We would respectfully and compassionately assist them in transferring to a hospice, family home or other location,” Iljana said in an email. “We will readmit them immediately if they change their minds.”
But Kathryn Tucker, executive director of the End of Life Liberty Project, an advocacy group that supports aid-in-dying, said that CalVet is interpreting the federal regulations too broadly and denying terminally ill veterans the right to choose a “peaceful death” through medical assistance.
“Nothing exists in the federal statute’s language that would prohibit a resident from receiving aid-in-dying services at state homes, so long as they are not provided using federal funds or employees,” she said.
Ed Warren, head of the Allied Council, a group representing veterans at the Yountville site, co-signed a letter to CalVet officials protesting the ruling.
“My point of view is that it is inhumane to expect people in the last stages of dying to go through the hullabaloo of leaving their homes,” he said.
In Washington state, a 60-year-old man diagnosed with terminal chronic obstructive pulmonary disease, or COPD, died in June 2015 after ingesting lethal drugs at the Washington Soldiers Home in Orting, where he lived.
“It was all done very much in the open,” said Chris Fruitrich, a volunteer with the group End of Life Washington, which assisted the man.
There has been no indication that the policy jeopardizes the nearly $47 million the agency receives each year in federal funds, said Audette, the state VA spokeswoman.
In California, additional protests have centered on allegations that CalVet suppressed information about the aid-in-dying law.
Critics at the Yountville home contend that CalVet passed the discharge rule quietly, with little public input. Then the agency refused to broadcast a public meeting about medical aid-in-dying on KVET, the center’s state-run, closed-circuit television station.
Iljana said the Aug. 21 meeting, led by Tucker and Dr. Robert Brody, also a supporter of aid-in-dying, violated state rules that prohibit using public resources to promote political causes.
“Free speech is great and criticizing the government is great, but not using the government’s own resources and paid staff to advocate for a change in the law,” Iljana wrote in an email to prohibit the broadcast.
That decision, however, prompted Jac Warren, 81, who has been KVET’s station manager for eight years, to resign last month in protest, citing censorship.
“What is at issue is whether a state may completely suppress the dissemination of concededly truthful information about entirely lawful activity,” Warren wrote in an email to CalVet.
The hour-long meeting, attended by about 50 people, was not propaganda, Tucker said, but “an educational event with information provided by an attorney and a physician who both specialize in their respective fields in end-of-life care.”
Bob Sloan, who works as an engineer at KVET for a $400 monthly stipend, disagreed with the decision not to broadcast the meeting on the system that serves residents of the Yountville home.
Sloan said he knows other residents who would like to be able to use California’s aid-in-dying law if their illnesses progress.
“The only other option that people have in this state is committing suicide,” he said. “If I can’t find some way of doing it legally, I’ll do it illegally.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
California voters passed a law two years ago that allows terminally ill people to take lethal drugs to end their lives, but controversy is growing over a newer rule that effectively bans that option in the state’s eight veterans homes.
Proponents of medical aid-in-dying and residents of the Veterans Home of California-Yountville — the largest in the nation — are protesting a regulation passed last year by the California Department of Veterans Affairs, or CalVet, that requires that anyone living in the facilities must be discharged if they intend to use the law.
That’s a position shared by most — but not all — states where aid-in-dying is allowed. As more U.S. jurisdictions consider whether to legalize the practice, the status of terminally ill veterans living in state-run homes will loom large.
“It would be a terrible hardship, because I have no place to go,” said Bob Sloan, 73, who suffers from congestive heart failure and other serious cardiac problems. He said he intends to seek medical aid-in-dying if doctors certify he has six months or less to live.
“I’m not going to be a vegetable,” said Sloan, a Vietnam War-era veteran who moved into the Yountville center five years ago. “I’m not going to end up living in so much pain it’s unbearable.”
A CalVet official said the agency adopted the rule to avoid violating a federal statute that prohibits using U.S. government resources for physician-assisted death. Otherwise, the agency would jeopardize nearly $68 million in federal funds that helps run the facilities, said June Iljana, CalVet’s deputy secretary of communications.
California is not alone. Three other states where aid-in-dying is legal — Oregon, Colorado and Vermont — all prohibit use of lethal medications in state-run veterans homes.
In Montana, where aid-in-dying is allowed under a state Supreme Court ruling, officials didn’t respond to multiple requests about whether veterans would be able to use the law in the residences. However, Dr. Eric Kress, a Missoula physician who prescribes the lethal medication, says he has transferred patients to hospice, to relatives’ homes, even to extended-stay hotels to avoid conflict.
In Washington, D.C., where an aid-in-dying law took effect last summer, the Armed Forces Retirement Home won’t assist patients in any way. Those who wish to use the law would be referred to an ethics committee for individual consideration, spokesman Christopher Kelly said in an email.
Only Washington state has a policy that allows veterans to remain in government-run residences if they intend to ingest lethal medications.. At least one veteran has died in a state-run home using that law, said Heidi Audette, a spokeswoman for the state’s Department of Veterans Affairs.
Paul Sherbo, a spokesman for the U.S. Department of Veterans Affairs, said the choice is up to the states.
“VA does not mandate how states comply with federal law,” Sherbo said in an email. “There are a number of ways individual states can choose to handle such situations and still be in compliance.”
To date, none of the 2,400 residents of California’s veterans homes has formally requested medical aid-in-dying, said Iljana. That includes the more than 900 residents of the Yountville center, located about 60 miles north of San Francisco.
“We would respectfully and compassionately assist them in transferring to a hospice, family home or other location,” Iljana said in an email. “We will readmit them immediately if they change their minds.”
But Kathryn Tucker, executive director of the End of Life Liberty Project, an advocacy group that supports aid-in-dying, said that CalVet is interpreting the federal regulations too broadly and denying terminally ill veterans the right to choose a “peaceful death” through medical assistance.
“Nothing exists in the federal statute’s language that would prohibit a resident from receiving aid-in-dying services at state homes, so long as they are not provided using federal funds or employees,” she said.
Ed Warren, head of the Allied Council, a group representing veterans at the Yountville site, co-signed a letter to CalVet officials protesting the ruling.
“My point of view is that it is inhumane to expect people in the last stages of dying to go through the hullabaloo of leaving their homes,” he said.
In Washington state, a 60-year-old man diagnosed with terminal chronic obstructive pulmonary disease, or COPD, died in June 2015 after ingesting lethal drugs at the Washington Soldiers Home in Orting, where he lived.
“It was all done very much in the open,” said Chris Fruitrich, a volunteer with the group End of Life Washington, which assisted the man.
There has been no indication that the policy jeopardizes the nearly $47 million the agency receives each year in federal funds, said Audette, the state VA spokeswoman.
In California, additional protests have centered on allegations that CalVet suppressed information about the aid-in-dying law.
Critics at the Yountville home contend that CalVet passed the discharge rule quietly, with little public input. Then the agency refused to broadcast a public meeting about medical aid-in-dying on KVET, the center’s state-run, closed-circuit television station.
Iljana said the Aug. 21 meeting, led by Tucker and Dr. Robert Brody, also a supporter of aid-in-dying, violated state rules that prohibit using public resources to promote political causes.
“Free speech is great and criticizing the government is great, but not using the government’s own resources and paid staff to advocate for a change in the law,” Iljana wrote in an email to prohibit the broadcast.
That decision, however, prompted Jac Warren, 81, who has been KVET’s station manager for eight years, to resign last month in protest, citing censorship.
“What is at issue is whether a state may completely suppress the dissemination of concededly truthful information about entirely lawful activity,” Warren wrote in an email to CalVet.
The hour-long meeting, attended by about 50 people, was not propaganda, Tucker said, but “an educational event with information provided by an attorney and a physician who both specialize in their respective fields in end-of-life care.”
Bob Sloan, who works as an engineer at KVET for a $400 monthly stipend, disagreed with the decision not to broadcast the meeting on the system that serves residents of the Yountville home.
Sloan said he knows other residents who would like to be able to use California’s aid-in-dying law if their illnesses progress.
“The only other option that people have in this state is committing suicide,” he said. “If I can’t find some way of doing it legally, I’ll do it illegally.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
Early Intervention for Mental Health Pays Off Later
The facts are dire: In 2014, people diagnosed with schizophrenia or mood disorders made 10.8 million visits to emergency departments (EDs). Between 2006 and 2014, the rate of ED visits related to mental health/substance abuse jumped 44%. The suicide rate among people with serious emotional disturbances (SEDs) is 25 times higher than that in the general population. Two million people with serious mental illness (SMI) are jailed annually, but only about 1 in 3 is currently receiving any treatment.
However, early intervention for SMI can help many people stay out of EDs and jails. That is the focus of The Way Forward: Federal Action for a System That Works for All People Living With SMI and SED and Their Families and Caregivers, a report recently released by the Substance Abuse and Mental Health Services Administration (SAMHSA).
“The emergency room is not a place for people that are experiencing exacerbations of mental health conditions,” says Elinore McCance-Katz, MD, PhD, assistant secretary for mental health and substance use at SAMHSA and chair of the Interdepartmental Serious Mental Illness Coordinating Committee, which produced the report.
In the report, the committee cited the 2003 President’s New Freedom Commission on Mental Health, which concluded that America’s mental health service delivery system was “in shambles,” with “fragmented, disconnected and often inadequate” mental health services and supports. Yet a number of the commission’s recommendations still have not been implemented or only “partially realized,” the committee notes.
In an interview with MedPageToday.com, McCance-Katz says the solution is a “national system of crisis intervention services”—a continuum of care with outpatient services as alternatives to inpatient care. Most states report insufficient psychiatric crisis response capacity, as well as insufficient numbers of inpatient psychiatric hospital beds. If the right system, one that includes community interventions and adequate resources, were in place, McCance-Katz says, “we might not need so many beds.”
The facts are dire: In 2014, people diagnosed with schizophrenia or mood disorders made 10.8 million visits to emergency departments (EDs). Between 2006 and 2014, the rate of ED visits related to mental health/substance abuse jumped 44%. The suicide rate among people with serious emotional disturbances (SEDs) is 25 times higher than that in the general population. Two million people with serious mental illness (SMI) are jailed annually, but only about 1 in 3 is currently receiving any treatment.
However, early intervention for SMI can help many people stay out of EDs and jails. That is the focus of The Way Forward: Federal Action for a System That Works for All People Living With SMI and SED and Their Families and Caregivers, a report recently released by the Substance Abuse and Mental Health Services Administration (SAMHSA).
“The emergency room is not a place for people that are experiencing exacerbations of mental health conditions,” says Elinore McCance-Katz, MD, PhD, assistant secretary for mental health and substance use at SAMHSA and chair of the Interdepartmental Serious Mental Illness Coordinating Committee, which produced the report.
In the report, the committee cited the 2003 President’s New Freedom Commission on Mental Health, which concluded that America’s mental health service delivery system was “in shambles,” with “fragmented, disconnected and often inadequate” mental health services and supports. Yet a number of the commission’s recommendations still have not been implemented or only “partially realized,” the committee notes.
In an interview with MedPageToday.com, McCance-Katz says the solution is a “national system of crisis intervention services”—a continuum of care with outpatient services as alternatives to inpatient care. Most states report insufficient psychiatric crisis response capacity, as well as insufficient numbers of inpatient psychiatric hospital beds. If the right system, one that includes community interventions and adequate resources, were in place, McCance-Katz says, “we might not need so many beds.”
The facts are dire: In 2014, people diagnosed with schizophrenia or mood disorders made 10.8 million visits to emergency departments (EDs). Between 2006 and 2014, the rate of ED visits related to mental health/substance abuse jumped 44%. The suicide rate among people with serious emotional disturbances (SEDs) is 25 times higher than that in the general population. Two million people with serious mental illness (SMI) are jailed annually, but only about 1 in 3 is currently receiving any treatment.
However, early intervention for SMI can help many people stay out of EDs and jails. That is the focus of The Way Forward: Federal Action for a System That Works for All People Living With SMI and SED and Their Families and Caregivers, a report recently released by the Substance Abuse and Mental Health Services Administration (SAMHSA).
“The emergency room is not a place for people that are experiencing exacerbations of mental health conditions,” says Elinore McCance-Katz, MD, PhD, assistant secretary for mental health and substance use at SAMHSA and chair of the Interdepartmental Serious Mental Illness Coordinating Committee, which produced the report.
In the report, the committee cited the 2003 President’s New Freedom Commission on Mental Health, which concluded that America’s mental health service delivery system was “in shambles,” with “fragmented, disconnected and often inadequate” mental health services and supports. Yet a number of the commission’s recommendations still have not been implemented or only “partially realized,” the committee notes.
In an interview with MedPageToday.com, McCance-Katz says the solution is a “national system of crisis intervention services”—a continuum of care with outpatient services as alternatives to inpatient care. Most states report insufficient psychiatric crisis response capacity, as well as insufficient numbers of inpatient psychiatric hospital beds. If the right system, one that includes community interventions and adequate resources, were in place, McCance-Katz says, “we might not need so many beds.”
OSA patients report sleeping better with dronabinol
in a new study.
A paper published in the January edition of Sleep presents data from a phase 2, blinded, randomized controlled trial of the nonselective cannabinoid 1 and cannabinoid 2 receptor agonist, dronabinol, in 73 adults with moderate or severe obstructive sleep apnea (OSA). No approved drug treatments for OSA exist, and this study provides results “from the largest and longest randomized controlled trial to date of any putative drug treatment for OSA,” the researchers wrote.
Patients were randomized to 2.5 mg dronabinol or 10 mg dronabinol daily for up to 6 weeks, or placebo. At the end of treatment, researchers saw significant increases in the apnea-hypopnea index among the patients on placebo, while those who received dronabinol showed decreases in the number of apnea and hypopnea events per hour. Patients given the 2.5-mg dose of dronabinol had a mean decrease of 10.7 events per hour, and those on the 10-mg dose had a mean decrease of 12.9 events per hour compared with placebo.
The difference between the placebo and treatment arms was significant for both dosages, and the apnea-hypopnea index decreases were similar between the two dosages of dronabinol.
These effects were largely due to reductions in apnea events; the largest reduction was seen in the REM apnea index in patients treated with the 10-mg dose of dronabinol. However, there were few effects on the expression of hypopneas, except in the higher-dose group.
After adjustment for age, race, ethnicity, and baseline apnea-hypopnea index, the increases seen in the placebo group were no longer significant, but the decreases from baseline seen in the treatment arms were greater.
Dronabinol treatment was also associated with significant decreases, compared with placebo, in non-REM apnea-hypopnea index and REM apnea-hypopnea index.
Patients’ self-reported daytime sleepiness, measured by the Epworth Sleepiness Scale, remained similar compared with baseline in those who received placebo and the 2.5-mg/day dose of dronabinol, but decreased significantly by a mean of −2.3 points compared with placebo in those on the higher dose of dronabinol.
There were no significant changes from baseline in objective sleepiness, as measured by the maintenance of wakefulness test, in any of the study groups. Researchers also saw no significant changes in sleep architecture, oxygenation, or the duration of supine sleep in any of the study groups, although the patients on the higher dose of dronabinol showed a slight increase in REM sleep and those on placebo showed a slight decrease.
Younger patients and those with a greater preponderance of REM-related apnea/hypopnea, and shorter average event duration were both more likely to respond to treatment, but apart from these factors there were no other influences on likelihood of patients responding to dronabinol.
David W. Carley, PhD, of the University of Illinois at Chicago, and his coauthors noted that there was a great need for pharmacological treatments for obstructive sleep apnea because positive airway pressure – while effective – has poor long-term adherence rates.
“Based on a series of animal investigations, we proposed that drugs which dampen afferent vagal feedback to the medulla may be effective in stabilizing respiratory pattern generation and increasing activation of upper airway dilating muscles during sleep,” they wrote.
One patient experienced diarrhea and vomiting that required admission to hospital, and which was judged as possibly related to the study medication. There were six other withdrawals due to adverse events including dizziness and vision changes, vertigo, ECG arrhythmias, and headache with dizziness and vomiting. Overall, nearly 90% of patients reported at least one adverse event, but the rates did not differ significantly between the treatment and placebo arms.
The researchers noted that significantly higher satisfaction scores were seen among patients receiving the higher dose of dronabinol.
“All of these observations argue that dronabinol, at doses from 2.5 to 10 mg/day, is safe for use by medically stable patients with moderate or severe OSA,” the authors wrote. “Participants also tolerated and adhered well to daily self-administration of dronabinol.”
The National Institutes of Health, National Heart, Lung, and Blood Institute, and National Center for Advancing Translational Sciences funded the study. One author declared grants from the National Institutes of Health for the study, and patents related to treatment of sleep-related breathing disorders by cannabinoid drugs. He also holds stock in RespireRx Pharmaceuticals, which holds an exclusive license to these and other related patents.
SOURCE: Carley D, et al. Sleep. 2018 Jan 1. doi: 10.1093/sleep/zsx184
This study has found a small overall effect on the apnea-hypopnea index with treatment, but a strong beneficial effect on subjective sleepiness. In addition, participants who received the higher dose of the drug showed significant satisfaction with their therapy. It is therefore intriguing that there was no impact on objective wakefulness or sleep architecture with this treatment.
This suggests that perhaps sleepiness and subjective wellbeing may be improved without necessarily seeing major improvements in the apnea-hypopnea index, which calls into question our use of this index as a primary end-point.
Sigrid C. Veasey, MD, is with the Center for Sleep and Circadian Neurobiology at the Perelman School of Medicine, University of Pennsylvania, Philadelphia. These comments are taken from an accompanying (Sleep 2018 Jan 1. doi: 10.1093/sleep/zsy014). No conflicts of interest were declared.
This study has found a small overall effect on the apnea-hypopnea index with treatment, but a strong beneficial effect on subjective sleepiness. In addition, participants who received the higher dose of the drug showed significant satisfaction with their therapy. It is therefore intriguing that there was no impact on objective wakefulness or sleep architecture with this treatment.
This suggests that perhaps sleepiness and subjective wellbeing may be improved without necessarily seeing major improvements in the apnea-hypopnea index, which calls into question our use of this index as a primary end-point.
Sigrid C. Veasey, MD, is with the Center for Sleep and Circadian Neurobiology at the Perelman School of Medicine, University of Pennsylvania, Philadelphia. These comments are taken from an accompanying (Sleep 2018 Jan 1. doi: 10.1093/sleep/zsy014). No conflicts of interest were declared.
This study has found a small overall effect on the apnea-hypopnea index with treatment, but a strong beneficial effect on subjective sleepiness. In addition, participants who received the higher dose of the drug showed significant satisfaction with their therapy. It is therefore intriguing that there was no impact on objective wakefulness or sleep architecture with this treatment.
This suggests that perhaps sleepiness and subjective wellbeing may be improved without necessarily seeing major improvements in the apnea-hypopnea index, which calls into question our use of this index as a primary end-point.
Sigrid C. Veasey, MD, is with the Center for Sleep and Circadian Neurobiology at the Perelman School of Medicine, University of Pennsylvania, Philadelphia. These comments are taken from an accompanying (Sleep 2018 Jan 1. doi: 10.1093/sleep/zsy014). No conflicts of interest were declared.
in a new study.
A paper published in the January edition of Sleep presents data from a phase 2, blinded, randomized controlled trial of the nonselective cannabinoid 1 and cannabinoid 2 receptor agonist, dronabinol, in 73 adults with moderate or severe obstructive sleep apnea (OSA). No approved drug treatments for OSA exist, and this study provides results “from the largest and longest randomized controlled trial to date of any putative drug treatment for OSA,” the researchers wrote.
Patients were randomized to 2.5 mg dronabinol or 10 mg dronabinol daily for up to 6 weeks, or placebo. At the end of treatment, researchers saw significant increases in the apnea-hypopnea index among the patients on placebo, while those who received dronabinol showed decreases in the number of apnea and hypopnea events per hour. Patients given the 2.5-mg dose of dronabinol had a mean decrease of 10.7 events per hour, and those on the 10-mg dose had a mean decrease of 12.9 events per hour compared with placebo.
The difference between the placebo and treatment arms was significant for both dosages, and the apnea-hypopnea index decreases were similar between the two dosages of dronabinol.
These effects were largely due to reductions in apnea events; the largest reduction was seen in the REM apnea index in patients treated with the 10-mg dose of dronabinol. However, there were few effects on the expression of hypopneas, except in the higher-dose group.
After adjustment for age, race, ethnicity, and baseline apnea-hypopnea index, the increases seen in the placebo group were no longer significant, but the decreases from baseline seen in the treatment arms were greater.
Dronabinol treatment was also associated with significant decreases, compared with placebo, in non-REM apnea-hypopnea index and REM apnea-hypopnea index.
Patients’ self-reported daytime sleepiness, measured by the Epworth Sleepiness Scale, remained similar compared with baseline in those who received placebo and the 2.5-mg/day dose of dronabinol, but decreased significantly by a mean of −2.3 points compared with placebo in those on the higher dose of dronabinol.
There were no significant changes from baseline in objective sleepiness, as measured by the maintenance of wakefulness test, in any of the study groups. Researchers also saw no significant changes in sleep architecture, oxygenation, or the duration of supine sleep in any of the study groups, although the patients on the higher dose of dronabinol showed a slight increase in REM sleep and those on placebo showed a slight decrease.
Younger patients and those with a greater preponderance of REM-related apnea/hypopnea, and shorter average event duration were both more likely to respond to treatment, but apart from these factors there were no other influences on likelihood of patients responding to dronabinol.
David W. Carley, PhD, of the University of Illinois at Chicago, and his coauthors noted that there was a great need for pharmacological treatments for obstructive sleep apnea because positive airway pressure – while effective – has poor long-term adherence rates.
“Based on a series of animal investigations, we proposed that drugs which dampen afferent vagal feedback to the medulla may be effective in stabilizing respiratory pattern generation and increasing activation of upper airway dilating muscles during sleep,” they wrote.
One patient experienced diarrhea and vomiting that required admission to hospital, and which was judged as possibly related to the study medication. There were six other withdrawals due to adverse events including dizziness and vision changes, vertigo, ECG arrhythmias, and headache with dizziness and vomiting. Overall, nearly 90% of patients reported at least one adverse event, but the rates did not differ significantly between the treatment and placebo arms.
The researchers noted that significantly higher satisfaction scores were seen among patients receiving the higher dose of dronabinol.
“All of these observations argue that dronabinol, at doses from 2.5 to 10 mg/day, is safe for use by medically stable patients with moderate or severe OSA,” the authors wrote. “Participants also tolerated and adhered well to daily self-administration of dronabinol.”
The National Institutes of Health, National Heart, Lung, and Blood Institute, and National Center for Advancing Translational Sciences funded the study. One author declared grants from the National Institutes of Health for the study, and patents related to treatment of sleep-related breathing disorders by cannabinoid drugs. He also holds stock in RespireRx Pharmaceuticals, which holds an exclusive license to these and other related patents.
SOURCE: Carley D, et al. Sleep. 2018 Jan 1. doi: 10.1093/sleep/zsx184
in a new study.
A paper published in the January edition of Sleep presents data from a phase 2, blinded, randomized controlled trial of the nonselective cannabinoid 1 and cannabinoid 2 receptor agonist, dronabinol, in 73 adults with moderate or severe obstructive sleep apnea (OSA). No approved drug treatments for OSA exist, and this study provides results “from the largest and longest randomized controlled trial to date of any putative drug treatment for OSA,” the researchers wrote.
Patients were randomized to 2.5 mg dronabinol or 10 mg dronabinol daily for up to 6 weeks, or placebo. At the end of treatment, researchers saw significant increases in the apnea-hypopnea index among the patients on placebo, while those who received dronabinol showed decreases in the number of apnea and hypopnea events per hour. Patients given the 2.5-mg dose of dronabinol had a mean decrease of 10.7 events per hour, and those on the 10-mg dose had a mean decrease of 12.9 events per hour compared with placebo.
The difference between the placebo and treatment arms was significant for both dosages, and the apnea-hypopnea index decreases were similar between the two dosages of dronabinol.
These effects were largely due to reductions in apnea events; the largest reduction was seen in the REM apnea index in patients treated with the 10-mg dose of dronabinol. However, there were few effects on the expression of hypopneas, except in the higher-dose group.
After adjustment for age, race, ethnicity, and baseline apnea-hypopnea index, the increases seen in the placebo group were no longer significant, but the decreases from baseline seen in the treatment arms were greater.
Dronabinol treatment was also associated with significant decreases, compared with placebo, in non-REM apnea-hypopnea index and REM apnea-hypopnea index.
Patients’ self-reported daytime sleepiness, measured by the Epworth Sleepiness Scale, remained similar compared with baseline in those who received placebo and the 2.5-mg/day dose of dronabinol, but decreased significantly by a mean of −2.3 points compared with placebo in those on the higher dose of dronabinol.
There were no significant changes from baseline in objective sleepiness, as measured by the maintenance of wakefulness test, in any of the study groups. Researchers also saw no significant changes in sleep architecture, oxygenation, or the duration of supine sleep in any of the study groups, although the patients on the higher dose of dronabinol showed a slight increase in REM sleep and those on placebo showed a slight decrease.
Younger patients and those with a greater preponderance of REM-related apnea/hypopnea, and shorter average event duration were both more likely to respond to treatment, but apart from these factors there were no other influences on likelihood of patients responding to dronabinol.
David W. Carley, PhD, of the University of Illinois at Chicago, and his coauthors noted that there was a great need for pharmacological treatments for obstructive sleep apnea because positive airway pressure – while effective – has poor long-term adherence rates.
“Based on a series of animal investigations, we proposed that drugs which dampen afferent vagal feedback to the medulla may be effective in stabilizing respiratory pattern generation and increasing activation of upper airway dilating muscles during sleep,” they wrote.
One patient experienced diarrhea and vomiting that required admission to hospital, and which was judged as possibly related to the study medication. There were six other withdrawals due to adverse events including dizziness and vision changes, vertigo, ECG arrhythmias, and headache with dizziness and vomiting. Overall, nearly 90% of patients reported at least one adverse event, but the rates did not differ significantly between the treatment and placebo arms.
The researchers noted that significantly higher satisfaction scores were seen among patients receiving the higher dose of dronabinol.
“All of these observations argue that dronabinol, at doses from 2.5 to 10 mg/day, is safe for use by medically stable patients with moderate or severe OSA,” the authors wrote. “Participants also tolerated and adhered well to daily self-administration of dronabinol.”
The National Institutes of Health, National Heart, Lung, and Blood Institute, and National Center for Advancing Translational Sciences funded the study. One author declared grants from the National Institutes of Health for the study, and patents related to treatment of sleep-related breathing disorders by cannabinoid drugs. He also holds stock in RespireRx Pharmaceuticals, which holds an exclusive license to these and other related patents.
SOURCE: Carley D, et al. Sleep. 2018 Jan 1. doi: 10.1093/sleep/zsx184
FROM SLEEP
Key clinical point: A cannabinoid receptor agonist may significantly reduce apnea and hypopnea events in patients with obstructive sleep apnea.
Major finding: Patients who received either low dose or high-dose dronabinol showed significant decreases in apnea and hypopnea events compared to those on placebo.
Data source: Randomized controlled, blinded phase II trial in 73 patients with obstructive sleep apnea.
Disclosures: The National Institutes of Health, National Heart Lung and Blood Institute, and National Center for Advancing Translational Sciences funded the study. One author declared grants from the National Institutes of Health for the study, and patents related to treatment of sleep-related breathing disorders by cannabinoid drugs. He also holds stock in RespireRx Pharmaceuticals, which holds an exclusive license to these and other related patents.
Source: Carley D, et al. Sleep. 2018 Jan 1. doi: 10.1093/sleep/zsx184.
Self-Reported Cognitive Impairment Is Rising
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.