User login
Fluarix Quadrivalent effective in very young, simplifies flu shots for all ages
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”

The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
ilacy@frontlinemedcom.com
SOURCE: D-QIV-004.
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”
The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
ilacy@frontlinemedcom.com
SOURCE: D-QIV-004.
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”
The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
ilacy@frontlinemedcom.com
SOURCE: D-QIV-004.
FROM AN ACIP MEETING
Key clinical point: The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, as well as preventing moderate to severe influenza, reduced health care utilization by pediatric influenza patients.
Major finding: Fluarix Quadrivalent was effective against moderate to severe influenza in 63.2% and against any severity of influenza in 49.8% of children aged 6-35 months.
Study details: A phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months, in which the children were split into five cohorts, each in a different influenza season from October 2011 to December 2014.
Disclosures: No disclosures were reported.
Source: The D-QIV-004 study.
Dexmedetomidine: ‘Silver bullet’ for ventilator liberation?
SAN ANTONIO – Among medications to facilitate extubation, dexmedetomidine offers favorable attributes, but whether it’s the best choice for patients who have difficulty being liberated from the ventilator remains to be proven, said Gilles L. Fraser, BS Pharm, PharmD.
The current CHEST/ATS guidelines on liberation from mechanical ventilation in critically ill adults strongly suggest extubation to noninvasive mechanical ventilation in high-risk patients (Chest. 2017 Jan;151[1]:160-5. doi: 10.1016/j.chest.2016.10.037). Guideline authors also suggested protocols attempting to minimize sedation for acutely hospitalized patients ventilated for more than 24 hours, based on some evidence showing a trend toward shorter ventilation time and ICU stay, as well as lower short-term mortality.
, one of the coauthors of the guidelines, during his presentation at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
“I’ll leave you up to your own devices,” he told attendees at a session on conundrums in critical care that are not addressed in current guidelines. “We use it all the time, frankly, but I don’t have any firm data to support that contention.”
Despite best practices, extubation attempts are not always successful: “If you follow the rules of the road, success is going to occur about 85% of the time,” said Dr. Fraser, who is a clinical pharmacist at Maine Medical Center, Portland, and professor of medicine at Tufts University, Boston. “That means that about 15% of our patients have difficulties in being liberated from the ventilator.”
In terms of medications to facilitate ventilator liberation, benzodiazepines, dexmedetomidine, and propofol all have roles to play, according to Dr. Fraser. Clinicians have to consider agent-specific side effects, pharmacokinetics and dynamics, and “econotoxicity,” or the cost of care, he added.
Although there are few comparative data available to guide choice of medication, Dr. Fraser and his colleagues have published a systematic review and meta-analysis of randomized trials of benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adult patients (Crit Care Med. 2013 Sep;41[9 Suppl 1]:S30-8. doi: 10.1097/CCM.0b013e3182a16898).
They found that dexmedetomidine- or propofol-based sedation regimens appeared to reduce mechanical ventilation duration and length of ICU stay versus benzodiazepine-based sedation, but they stated that larger controlled studies would be needed to further define outcomes in this setting.
More recently, other investigators reported an evaluation of 9,603 consecutive mechanical ventilation episodes (Chest. 2016 Jun;149[6]:1373-9. doi: 10.1378/chest.15-1389). In this large, real-world experience, propofol and dexmedetomidine were both associated with less time to extubation versus benzodiazepines, and dexmedetomidine was associated with less time to extubation versus propofol.
Relatively few patients (about 12%), however, received dexmedetomidine in that large series, and that was mostly in the setting of cardiac surgery, Dr. Fraser noted. Moreover, the investigators reported finding no differences between any two agents in hospital discharge or mortality hazard ratio.
“We’re not suggesting the benzodiazepines as routine sedative agents in our patient populations,” Dr. Fraser said in his presentation. “The primary reason is that they result in a longer time on the vent, typically between 1 and 2 days.”
But this doesn’t mean that the benzodiazepines are the “devil’s handiwork,” he added, noting that they may be useful in patients with anxiety related to ventilator weaning and those recovering from hemodynamic instability or at risk for GABA-agonist withdrawal.
Dexmedetomidine is opioid sparing and has a minimal effect on respiratory drive, among other advantages; however, some potential drawbacks include its hemodynamic effects and its cost, according to Dr. Fraser.
Dr. Fraser said that his institution’s daily acquisition cost for dexmedetomidine is $500, compared with $120 for propofol and $40 for benzodiazepines, but some pharmacoeconomic evaluations suggest use of dexmedetomidine may actually save between $3,000 and $9,000 per ICU admission. “At least in our place, one day in the ICU costs about $5,000, so that all makes sense … and I can argue fairly effectively that dexmedetomidine really isn’t that expensive compared to midazolam,” he said.
Dr. Fraser said that he had no disclosures related to his presentation.
SAN ANTONIO – Among medications to facilitate extubation, dexmedetomidine offers favorable attributes, but whether it’s the best choice for patients who have difficulty being liberated from the ventilator remains to be proven, said Gilles L. Fraser, BS Pharm, PharmD.
The current CHEST/ATS guidelines on liberation from mechanical ventilation in critically ill adults strongly suggest extubation to noninvasive mechanical ventilation in high-risk patients (Chest. 2017 Jan;151[1]:160-5. doi: 10.1016/j.chest.2016.10.037). Guideline authors also suggested protocols attempting to minimize sedation for acutely hospitalized patients ventilated for more than 24 hours, based on some evidence showing a trend toward shorter ventilation time and ICU stay, as well as lower short-term mortality.
, one of the coauthors of the guidelines, during his presentation at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
“I’ll leave you up to your own devices,” he told attendees at a session on conundrums in critical care that are not addressed in current guidelines. “We use it all the time, frankly, but I don’t have any firm data to support that contention.”
Despite best practices, extubation attempts are not always successful: “If you follow the rules of the road, success is going to occur about 85% of the time,” said Dr. Fraser, who is a clinical pharmacist at Maine Medical Center, Portland, and professor of medicine at Tufts University, Boston. “That means that about 15% of our patients have difficulties in being liberated from the ventilator.”
In terms of medications to facilitate ventilator liberation, benzodiazepines, dexmedetomidine, and propofol all have roles to play, according to Dr. Fraser. Clinicians have to consider agent-specific side effects, pharmacokinetics and dynamics, and “econotoxicity,” or the cost of care, he added.
Although there are few comparative data available to guide choice of medication, Dr. Fraser and his colleagues have published a systematic review and meta-analysis of randomized trials of benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adult patients (Crit Care Med. 2013 Sep;41[9 Suppl 1]:S30-8. doi: 10.1097/CCM.0b013e3182a16898).
They found that dexmedetomidine- or propofol-based sedation regimens appeared to reduce mechanical ventilation duration and length of ICU stay versus benzodiazepine-based sedation, but they stated that larger controlled studies would be needed to further define outcomes in this setting.
More recently, other investigators reported an evaluation of 9,603 consecutive mechanical ventilation episodes (Chest. 2016 Jun;149[6]:1373-9. doi: 10.1378/chest.15-1389). In this large, real-world experience, propofol and dexmedetomidine were both associated with less time to extubation versus benzodiazepines, and dexmedetomidine was associated with less time to extubation versus propofol.
Relatively few patients (about 12%), however, received dexmedetomidine in that large series, and that was mostly in the setting of cardiac surgery, Dr. Fraser noted. Moreover, the investigators reported finding no differences between any two agents in hospital discharge or mortality hazard ratio.
“We’re not suggesting the benzodiazepines as routine sedative agents in our patient populations,” Dr. Fraser said in his presentation. “The primary reason is that they result in a longer time on the vent, typically between 1 and 2 days.”
But this doesn’t mean that the benzodiazepines are the “devil’s handiwork,” he added, noting that they may be useful in patients with anxiety related to ventilator weaning and those recovering from hemodynamic instability or at risk for GABA-agonist withdrawal.
Dexmedetomidine is opioid sparing and has a minimal effect on respiratory drive, among other advantages; however, some potential drawbacks include its hemodynamic effects and its cost, according to Dr. Fraser.
Dr. Fraser said that his institution’s daily acquisition cost for dexmedetomidine is $500, compared with $120 for propofol and $40 for benzodiazepines, but some pharmacoeconomic evaluations suggest use of dexmedetomidine may actually save between $3,000 and $9,000 per ICU admission. “At least in our place, one day in the ICU costs about $5,000, so that all makes sense … and I can argue fairly effectively that dexmedetomidine really isn’t that expensive compared to midazolam,” he said.
Dr. Fraser said that he had no disclosures related to his presentation.
SAN ANTONIO – Among medications to facilitate extubation, dexmedetomidine offers favorable attributes, but whether it’s the best choice for patients who have difficulty being liberated from the ventilator remains to be proven, said Gilles L. Fraser, BS Pharm, PharmD.
The current CHEST/ATS guidelines on liberation from mechanical ventilation in critically ill adults strongly suggest extubation to noninvasive mechanical ventilation in high-risk patients (Chest. 2017 Jan;151[1]:160-5. doi: 10.1016/j.chest.2016.10.037). Guideline authors also suggested protocols attempting to minimize sedation for acutely hospitalized patients ventilated for more than 24 hours, based on some evidence showing a trend toward shorter ventilation time and ICU stay, as well as lower short-term mortality.
, one of the coauthors of the guidelines, during his presentation at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
“I’ll leave you up to your own devices,” he told attendees at a session on conundrums in critical care that are not addressed in current guidelines. “We use it all the time, frankly, but I don’t have any firm data to support that contention.”
Despite best practices, extubation attempts are not always successful: “If you follow the rules of the road, success is going to occur about 85% of the time,” said Dr. Fraser, who is a clinical pharmacist at Maine Medical Center, Portland, and professor of medicine at Tufts University, Boston. “That means that about 15% of our patients have difficulties in being liberated from the ventilator.”
In terms of medications to facilitate ventilator liberation, benzodiazepines, dexmedetomidine, and propofol all have roles to play, according to Dr. Fraser. Clinicians have to consider agent-specific side effects, pharmacokinetics and dynamics, and “econotoxicity,” or the cost of care, he added.
Although there are few comparative data available to guide choice of medication, Dr. Fraser and his colleagues have published a systematic review and meta-analysis of randomized trials of benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adult patients (Crit Care Med. 2013 Sep;41[9 Suppl 1]:S30-8. doi: 10.1097/CCM.0b013e3182a16898).
They found that dexmedetomidine- or propofol-based sedation regimens appeared to reduce mechanical ventilation duration and length of ICU stay versus benzodiazepine-based sedation, but they stated that larger controlled studies would be needed to further define outcomes in this setting.
More recently, other investigators reported an evaluation of 9,603 consecutive mechanical ventilation episodes (Chest. 2016 Jun;149[6]:1373-9. doi: 10.1378/chest.15-1389). In this large, real-world experience, propofol and dexmedetomidine were both associated with less time to extubation versus benzodiazepines, and dexmedetomidine was associated with less time to extubation versus propofol.
Relatively few patients (about 12%), however, received dexmedetomidine in that large series, and that was mostly in the setting of cardiac surgery, Dr. Fraser noted. Moreover, the investigators reported finding no differences between any two agents in hospital discharge or mortality hazard ratio.
“We’re not suggesting the benzodiazepines as routine sedative agents in our patient populations,” Dr. Fraser said in his presentation. “The primary reason is that they result in a longer time on the vent, typically between 1 and 2 days.”
But this doesn’t mean that the benzodiazepines are the “devil’s handiwork,” he added, noting that they may be useful in patients with anxiety related to ventilator weaning and those recovering from hemodynamic instability or at risk for GABA-agonist withdrawal.
Dexmedetomidine is opioid sparing and has a minimal effect on respiratory drive, among other advantages; however, some potential drawbacks include its hemodynamic effects and its cost, according to Dr. Fraser.
Dr. Fraser said that his institution’s daily acquisition cost for dexmedetomidine is $500, compared with $120 for propofol and $40 for benzodiazepines, but some pharmacoeconomic evaluations suggest use of dexmedetomidine may actually save between $3,000 and $9,000 per ICU admission. “At least in our place, one day in the ICU costs about $5,000, so that all makes sense … and I can argue fairly effectively that dexmedetomidine really isn’t that expensive compared to midazolam,” he said.
Dr. Fraser said that he had no disclosures related to his presentation.
EXPERT ANALYSIS FROM CCC47
Combo therapy does not improve outcomes for A. Baumannii
, based on data from 406 patients.
In a study published online in The Lancet Infectious Diseases, Mical Paul, MD, of Rambam Health Care Campus, Haifa, Israel, and colleagues randomized 198 patients to colistin alone and 208 to colistin plus meropenem (Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099[18]30099-9).
The demographics were similar between the groups and approximately 77% of patients in each group were infected with A. baumannii.
The results highlight “the necessity of assessing combination therapy in randomized trials before adopting it into clinical use,” the researchers said.
The study was not designed to examine the effect of the two types of therapy on bacteria other than A. baumannii, the researchers noted. However, based on the findings, “we recommend against the routine use of carbapenems for the treatment of carbapenem-resistant A. baumannii infections,” they said.
The study was supported by EU AIDA grant Health-F3-2011-278348. Dr. Paul had no financial conflicts to disclose.
SOURCE: Paul M et al. Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099(18)30099-9.
, based on data from 406 patients.
In a study published online in The Lancet Infectious Diseases, Mical Paul, MD, of Rambam Health Care Campus, Haifa, Israel, and colleagues randomized 198 patients to colistin alone and 208 to colistin plus meropenem (Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099[18]30099-9).
The demographics were similar between the groups and approximately 77% of patients in each group were infected with A. baumannii.
The results highlight “the necessity of assessing combination therapy in randomized trials before adopting it into clinical use,” the researchers said.
The study was not designed to examine the effect of the two types of therapy on bacteria other than A. baumannii, the researchers noted. However, based on the findings, “we recommend against the routine use of carbapenems for the treatment of carbapenem-resistant A. baumannii infections,” they said.
The study was supported by EU AIDA grant Health-F3-2011-278348. Dr. Paul had no financial conflicts to disclose.
SOURCE: Paul M et al. Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099(18)30099-9.
, based on data from 406 patients.
In a study published online in The Lancet Infectious Diseases, Mical Paul, MD, of Rambam Health Care Campus, Haifa, Israel, and colleagues randomized 198 patients to colistin alone and 208 to colistin plus meropenem (Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099[18]30099-9).
The demographics were similar between the groups and approximately 77% of patients in each group were infected with A. baumannii.
The results highlight “the necessity of assessing combination therapy in randomized trials before adopting it into clinical use,” the researchers said.
The study was not designed to examine the effect of the two types of therapy on bacteria other than A. baumannii, the researchers noted. However, based on the findings, “we recommend against the routine use of carbapenems for the treatment of carbapenem-resistant A. baumannii infections,” they said.
The study was supported by EU AIDA grant Health-F3-2011-278348. Dr. Paul had no financial conflicts to disclose.
SOURCE: Paul M et al. Lancet Infect Dis. 2018 Feb 15. doi: 10.1016/S1473-3099(18)30099-9.
FROM THE LANCET INFECTIOUS DISEASES
New device cuts postoperative pulmonary complications
SAN ANTONIO – according to results of a nonrandomized study including high-risk patients undergoing elective surgical procedures.
“For certain types of surgical procedures, this therapy (MetaNeb, Hill-Rom) may provide a benefit for high-risk patients in terms of reducing their pulmonary complications and their hospital stay,” said Toan Huynh, MD, lead investigator and director of trauma research at Carolinas HealthCare System, Charlotte, N.C., at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
Currently, aggressive management of high-risk patients with strategies such as optimal analgesia, early ambulation, secretion mobilization, and lung expansion are used to try to reduce the incidence of postoperative pulmonary complications, noted Dr. Huynh, in an interview.
In this study, Dr. Huynh and his colleagues from the University of Pennsylvania, Philadelphia, and the Lahey Hospital & Medical Center, Burlington, Mass., sought to evaluate the efficacy of the MetaNeb system, which delivers continuous high-frequency oscillation, continuous positive expiratory pressure, and in-line aerosol flow in one combined unit. To estimate usual postoperative pulmonary complication rates, they first queried CPT and ICD-9-CM codes to identify a total of 210 patients who had undergone thoracic, upper-abdominal, or aortic open surgical procedures. Then, in the second stage of the study, the investigators prospectively enrolled 209 subjects who underwent those types of surgery with the MetaNeb system in addition to a standard postoperative respiratory regimen. All patients were high risk as defined by having either an American Society of Anesthesiologists classification of at least 3 or an ASA classification of 2 along with one or more comorbidities, such as COPD or recent smoking history.
Among the patients managed with MetaNeb, 33 (15.8%) experienced one or more pulmonary complications, compared with 48 (22.9%) in the retrospective cohort (P = 0.06). For intubated patients, at least one complication was seen in 22 patients (36.7%) in the MetaNeb group, compared with 37 (69.8%) in the comparison group (P less than .05). Time on mechanical ventilation was 8.5 hours in the MetaNeb group versus 23.7 hours in the comparison group (P less than .05).
Use of the device was also associated with decreased length of hospital stay, but the difference between lengths of stay was not statistically significant. Hospital length of stay was 6.8 days in the MetaNeb versus 8.4 days in the comparison groups.“In the current day and age of value-based health care, I think any kind of reduction in expenditure related to health care costs would be compelling for clinicians,” Dr. Huynh said in the interview.
Further study may be needed to better define the role of the combined modality system in clinical practice, according to Dr. Huynh.
“This is sort of a ‘before and after’ nonrandomized trial,” Dr. Huynh explained. “I think, ideally, if we can do a truly controlled, randomized trial, that will be much more powerful.”
The study was sponsored by Hill-Rom, which manufactures the device under study. Dr. Huynh said he and coinvestigators had no financial conflicts related to the research.
SOURCE: Huynh T et al. Critical Care Congress, Abstract 17.
SAN ANTONIO – according to results of a nonrandomized study including high-risk patients undergoing elective surgical procedures.
“For certain types of surgical procedures, this therapy (MetaNeb, Hill-Rom) may provide a benefit for high-risk patients in terms of reducing their pulmonary complications and their hospital stay,” said Toan Huynh, MD, lead investigator and director of trauma research at Carolinas HealthCare System, Charlotte, N.C., at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
Currently, aggressive management of high-risk patients with strategies such as optimal analgesia, early ambulation, secretion mobilization, and lung expansion are used to try to reduce the incidence of postoperative pulmonary complications, noted Dr. Huynh, in an interview.
In this study, Dr. Huynh and his colleagues from the University of Pennsylvania, Philadelphia, and the Lahey Hospital & Medical Center, Burlington, Mass., sought to evaluate the efficacy of the MetaNeb system, which delivers continuous high-frequency oscillation, continuous positive expiratory pressure, and in-line aerosol flow in one combined unit. To estimate usual postoperative pulmonary complication rates, they first queried CPT and ICD-9-CM codes to identify a total of 210 patients who had undergone thoracic, upper-abdominal, or aortic open surgical procedures. Then, in the second stage of the study, the investigators prospectively enrolled 209 subjects who underwent those types of surgery with the MetaNeb system in addition to a standard postoperative respiratory regimen. All patients were high risk as defined by having either an American Society of Anesthesiologists classification of at least 3 or an ASA classification of 2 along with one or more comorbidities, such as COPD or recent smoking history.
Among the patients managed with MetaNeb, 33 (15.8%) experienced one or more pulmonary complications, compared with 48 (22.9%) in the retrospective cohort (P = 0.06). For intubated patients, at least one complication was seen in 22 patients (36.7%) in the MetaNeb group, compared with 37 (69.8%) in the comparison group (P less than .05). Time on mechanical ventilation was 8.5 hours in the MetaNeb group versus 23.7 hours in the comparison group (P less than .05).
Use of the device was also associated with decreased length of hospital stay, but the difference between lengths of stay was not statistically significant. Hospital length of stay was 6.8 days in the MetaNeb versus 8.4 days in the comparison groups.“In the current day and age of value-based health care, I think any kind of reduction in expenditure related to health care costs would be compelling for clinicians,” Dr. Huynh said in the interview.
Further study may be needed to better define the role of the combined modality system in clinical practice, according to Dr. Huynh.
“This is sort of a ‘before and after’ nonrandomized trial,” Dr. Huynh explained. “I think, ideally, if we can do a truly controlled, randomized trial, that will be much more powerful.”
The study was sponsored by Hill-Rom, which manufactures the device under study. Dr. Huynh said he and coinvestigators had no financial conflicts related to the research.
SOURCE: Huynh T et al. Critical Care Congress, Abstract 17.
SAN ANTONIO – according to results of a nonrandomized study including high-risk patients undergoing elective surgical procedures.
“For certain types of surgical procedures, this therapy (MetaNeb, Hill-Rom) may provide a benefit for high-risk patients in terms of reducing their pulmonary complications and their hospital stay,” said Toan Huynh, MD, lead investigator and director of trauma research at Carolinas HealthCare System, Charlotte, N.C., at the Critical Care Congress sponsored by the Society for Critical Care Medicine.
Currently, aggressive management of high-risk patients with strategies such as optimal analgesia, early ambulation, secretion mobilization, and lung expansion are used to try to reduce the incidence of postoperative pulmonary complications, noted Dr. Huynh, in an interview.
In this study, Dr. Huynh and his colleagues from the University of Pennsylvania, Philadelphia, and the Lahey Hospital & Medical Center, Burlington, Mass., sought to evaluate the efficacy of the MetaNeb system, which delivers continuous high-frequency oscillation, continuous positive expiratory pressure, and in-line aerosol flow in one combined unit. To estimate usual postoperative pulmonary complication rates, they first queried CPT and ICD-9-CM codes to identify a total of 210 patients who had undergone thoracic, upper-abdominal, or aortic open surgical procedures. Then, in the second stage of the study, the investigators prospectively enrolled 209 subjects who underwent those types of surgery with the MetaNeb system in addition to a standard postoperative respiratory regimen. All patients were high risk as defined by having either an American Society of Anesthesiologists classification of at least 3 or an ASA classification of 2 along with one or more comorbidities, such as COPD or recent smoking history.
Among the patients managed with MetaNeb, 33 (15.8%) experienced one or more pulmonary complications, compared with 48 (22.9%) in the retrospective cohort (P = 0.06). For intubated patients, at least one complication was seen in 22 patients (36.7%) in the MetaNeb group, compared with 37 (69.8%) in the comparison group (P less than .05). Time on mechanical ventilation was 8.5 hours in the MetaNeb group versus 23.7 hours in the comparison group (P less than .05).
Use of the device was also associated with decreased length of hospital stay, but the difference between lengths of stay was not statistically significant. Hospital length of stay was 6.8 days in the MetaNeb versus 8.4 days in the comparison groups.“In the current day and age of value-based health care, I think any kind of reduction in expenditure related to health care costs would be compelling for clinicians,” Dr. Huynh said in the interview.
Further study may be needed to better define the role of the combined modality system in clinical practice, according to Dr. Huynh.
“This is sort of a ‘before and after’ nonrandomized trial,” Dr. Huynh explained. “I think, ideally, if we can do a truly controlled, randomized trial, that will be much more powerful.”
The study was sponsored by Hill-Rom, which manufactures the device under study. Dr. Huynh said he and coinvestigators had no financial conflicts related to the research.
SOURCE: Huynh T et al. Critical Care Congress, Abstract 17.
AT THE CRITICAL CARE CONGRESS
Key clinical point: A device that combines lung expansion, secretion clearance, and aerosol delivery (MetaNeb) appears to reduce postoperative pulmonary complications and resource use.Major finding: Pulmonary complications occurred in 36.7% of intubated patients, compared with 69.8% for a prospectively evaluated reference population (P less than 0.05).
Data source: A prospective, nonrandomized, two-stage study including 417 subjects who underwent thoracic, upper-abdominal, or aortic open surgical procedure at one of three centers.
Disclosures: The study was sponsored by Hill-Rom, which manufactures the MetaNeb device. Investigators had no financial conflicts related to the study.
Source: Huynh T et al. Critical Care Congress, Abstract 17.
Adenotonsillectomy reduced hypertension in OSA subgroup
after surgery, according to a retrospective analysis.
This is one of the few studies to have ever examined whether adenotonsillectomy for children with OSA had any effects on blood pressure (BP) and was based on “one of the largest cohorts for evaluating postoperative BP changes in nonobese children with OSA,” noted Cho-Hsueh Lee, MD, and colleagues. The report was published in JAMA Otolaryngology–Head & Neck Surgery. Among the previous studies that evaluated BP in children with OSA before and after having this surgery, the results varied, they added.
The researchers analyzed the medical records of 240 nonobese children with clinical symptoms and polysomnography-confirmed OSA (having an apnea-hypopnea index of greater than 1) who underwent adenotonsillectomy. Prior to surgery, 169 patients (70.4%) of the patients were classified as nonhypertensive, while 71 (29.6%) were classified as hypertensive. The children had a mean age of 7.3 years, and 160 were males.
Patients participated in full-night polysomnography (PSG) before surgery and at 3-6 months after adenotonsillectomy in the National Taiwan University Hospital Sleep Center. Apnea episodes were defined as a 90% decrease in airflow for two consecutive breaths. Sleep center staff measured the study participants’ systolic and diastolic BP in a sleep center using an electronic sphygmomanometer, in the evening, prior to the PSG study, and in the morning. Pediatric hypertension was based on the nocturnal BP measurement and was defined as having mean systolic and diastolic BP greater or equal to the 95th percentile for age, sex, and height.
“Postoperatively, hypertensive children had a significant decrease in all BP measures, including nocturnal and morning [systolic] BP ... A total of 47 hypertensive patients (66.2%) became nonhypertensive after surgery,” the researchers said.
For patients who were hypertensive before surgery, the average nocturnal (before PSG) preop systolic BP was 114.3 mm Hg, versus 107.5 mm Hg after surgery. The mean nocturnal diastolic BP for this same group of patients decreased to 65.1 mm Hg from 74.3 mm Hg. Similarly, the average morning (after PSG) systolic BP and diastolic BP were 106.0 mm Hg and 64.4 mm Hg after these patients underwent adenotonsillectomy, compared with 111.8 mm Hg and 71.7 mm Hg prior to surgery, respectively.
The adenotonsillectomy didn’t improve all patients’ BP. For some who were nonhypertensive before surgery, blood pressure increased, with 36 (21.3%) of this group having become hypersensitive after surgery, the researchers acknowledged.
Overall, the cohort experienced significant improvements in several PSG measures, including the average apnea-hypopnea index, which decreased from 12.1 events per hour to 1.7. The total arousal index also declined, going from 6.1 events per hour to 4.2. In addition, the mean oxygen saturation improved from 96.8% to 97.7%.
The investigators described several limitations of the study, including their inability to collect patients’ arterial stiffness, carotid intima thickness, and other cardiovascular measures beyond BP.
They recommended a follow-up study. “Although we observed improvements in BP measures within 6 months after surgery for hypertensive children with OSA, the long-term effects of surgery on BP remain uncertain,” they explained.
The study was supported by grants from the Ministry of Science and Technology, Republic of China (Taiwan). The researchers disclosed no potential conflicts of interest.
SOURCE: Lee, C-H et al. JAMA Otolaryngol Head Neck Surg. 2018 Feb 15. doi: 10.1001/jamaoto.2017.3127.

after surgery, according to a retrospective analysis.
This is one of the few studies to have ever examined whether adenotonsillectomy for children with OSA had any effects on blood pressure (BP) and was based on “one of the largest cohorts for evaluating postoperative BP changes in nonobese children with OSA,” noted Cho-Hsueh Lee, MD, and colleagues. The report was published in JAMA Otolaryngology–Head & Neck Surgery. Among the previous studies that evaluated BP in children with OSA before and after having this surgery, the results varied, they added.
The researchers analyzed the medical records of 240 nonobese children with clinical symptoms and polysomnography-confirmed OSA (having an apnea-hypopnea index of greater than 1) who underwent adenotonsillectomy. Prior to surgery, 169 patients (70.4%) of the patients were classified as nonhypertensive, while 71 (29.6%) were classified as hypertensive. The children had a mean age of 7.3 years, and 160 were males.
Patients participated in full-night polysomnography (PSG) before surgery and at 3-6 months after adenotonsillectomy in the National Taiwan University Hospital Sleep Center. Apnea episodes were defined as a 90% decrease in airflow for two consecutive breaths. Sleep center staff measured the study participants’ systolic and diastolic BP in a sleep center using an electronic sphygmomanometer, in the evening, prior to the PSG study, and in the morning. Pediatric hypertension was based on the nocturnal BP measurement and was defined as having mean systolic and diastolic BP greater or equal to the 95th percentile for age, sex, and height.
“Postoperatively, hypertensive children had a significant decrease in all BP measures, including nocturnal and morning [systolic] BP ... A total of 47 hypertensive patients (66.2%) became nonhypertensive after surgery,” the researchers said.
For patients who were hypertensive before surgery, the average nocturnal (before PSG) preop systolic BP was 114.3 mm Hg, versus 107.5 mm Hg after surgery. The mean nocturnal diastolic BP for this same group of patients decreased to 65.1 mm Hg from 74.3 mm Hg. Similarly, the average morning (after PSG) systolic BP and diastolic BP were 106.0 mm Hg and 64.4 mm Hg after these patients underwent adenotonsillectomy, compared with 111.8 mm Hg and 71.7 mm Hg prior to surgery, respectively.
The adenotonsillectomy didn’t improve all patients’ BP. For some who were nonhypertensive before surgery, blood pressure increased, with 36 (21.3%) of this group having become hypersensitive after surgery, the researchers acknowledged.
Overall, the cohort experienced significant improvements in several PSG measures, including the average apnea-hypopnea index, which decreased from 12.1 events per hour to 1.7. The total arousal index also declined, going from 6.1 events per hour to 4.2. In addition, the mean oxygen saturation improved from 96.8% to 97.7%.
The investigators described several limitations of the study, including their inability to collect patients’ arterial stiffness, carotid intima thickness, and other cardiovascular measures beyond BP.
They recommended a follow-up study. “Although we observed improvements in BP measures within 6 months after surgery for hypertensive children with OSA, the long-term effects of surgery on BP remain uncertain,” they explained.
The study was supported by grants from the Ministry of Science and Technology, Republic of China (Taiwan). The researchers disclosed no potential conflicts of interest.
SOURCE: Lee, C-H et al. JAMA Otolaryngol Head Neck Surg. 2018 Feb 15. doi: 10.1001/jamaoto.2017.3127.
after surgery, according to a retrospective analysis.
This is one of the few studies to have ever examined whether adenotonsillectomy for children with OSA had any effects on blood pressure (BP) and was based on “one of the largest cohorts for evaluating postoperative BP changes in nonobese children with OSA,” noted Cho-Hsueh Lee, MD, and colleagues. The report was published in JAMA Otolaryngology–Head & Neck Surgery. Among the previous studies that evaluated BP in children with OSA before and after having this surgery, the results varied, they added.
The researchers analyzed the medical records of 240 nonobese children with clinical symptoms and polysomnography-confirmed OSA (having an apnea-hypopnea index of greater than 1) who underwent adenotonsillectomy. Prior to surgery, 169 patients (70.4%) of the patients were classified as nonhypertensive, while 71 (29.6%) were classified as hypertensive. The children had a mean age of 7.3 years, and 160 were males.
Patients participated in full-night polysomnography (PSG) before surgery and at 3-6 months after adenotonsillectomy in the National Taiwan University Hospital Sleep Center. Apnea episodes were defined as a 90% decrease in airflow for two consecutive breaths. Sleep center staff measured the study participants’ systolic and diastolic BP in a sleep center using an electronic sphygmomanometer, in the evening, prior to the PSG study, and in the morning. Pediatric hypertension was based on the nocturnal BP measurement and was defined as having mean systolic and diastolic BP greater or equal to the 95th percentile for age, sex, and height.
“Postoperatively, hypertensive children had a significant decrease in all BP measures, including nocturnal and morning [systolic] BP ... A total of 47 hypertensive patients (66.2%) became nonhypertensive after surgery,” the researchers said.
For patients who were hypertensive before surgery, the average nocturnal (before PSG) preop systolic BP was 114.3 mm Hg, versus 107.5 mm Hg after surgery. The mean nocturnal diastolic BP for this same group of patients decreased to 65.1 mm Hg from 74.3 mm Hg. Similarly, the average morning (after PSG) systolic BP and diastolic BP were 106.0 mm Hg and 64.4 mm Hg after these patients underwent adenotonsillectomy, compared with 111.8 mm Hg and 71.7 mm Hg prior to surgery, respectively.
The adenotonsillectomy didn’t improve all patients’ BP. For some who were nonhypertensive before surgery, blood pressure increased, with 36 (21.3%) of this group having become hypersensitive after surgery, the researchers acknowledged.
Overall, the cohort experienced significant improvements in several PSG measures, including the average apnea-hypopnea index, which decreased from 12.1 events per hour to 1.7. The total arousal index also declined, going from 6.1 events per hour to 4.2. In addition, the mean oxygen saturation improved from 96.8% to 97.7%.
The investigators described several limitations of the study, including their inability to collect patients’ arterial stiffness, carotid intima thickness, and other cardiovascular measures beyond BP.
They recommended a follow-up study. “Although we observed improvements in BP measures within 6 months after surgery for hypertensive children with OSA, the long-term effects of surgery on BP remain uncertain,” they explained.
The study was supported by grants from the Ministry of Science and Technology, Republic of China (Taiwan). The researchers disclosed no potential conflicts of interest.
SOURCE: Lee, C-H et al. JAMA Otolaryngol Head Neck Surg. 2018 Feb 15. doi: 10.1001/jamaoto.2017.3127.
FROM JAMA OTOLARYNGOLOGY-HEAD & NECK SURGERY
Key clinical point: Hypertensive children with obstructive sleep apnea (OSA) who had an adenotonsillectomy experienced significant improvements in their blood pressure after surgery.
Major finding: Sixty-six percent of hypertensive patients with OSA became nonhypertensive after adenotonsillectomy.
Study details: A retrospective analysis of 240 nonobese children with OSA who underwent adenotonsillectomy.
Disclosures: The study was supported by grants from the Ministry of Science and Technology, Republic of China (Taiwan). The researchers disclosed no potential conflicts of interest.
Source: Lee, C-H et al. JAMA Otolaryngol Head Neck Surg. 2018 Feb 15. doi: 10.1001/jamaoto.2017.3127.
VA is Trying New Ways to Treat TBI and PTSD
The VA is examining two alternative treatments for TBI and PTSD: a light-emitting diode (LED) treatment for mild to moderate TBI and stellate ganglion block (SGB) for PTSD.
In the LED treatment, which takes about 30 minutes, a lightweight LED-lined helmet is placed on the patient’s head, and more diodes are placed inside the nose to deliver photons to the deeper parts of the brain. The light is painless and generates no heat.
Although it is considered investigational, LED therapy is available at the VAHS Boston, as well as for veterans to use at home. Dr. Margaret Naeser, a professor of neurology at Boston University School of Medicine and lead investigator of the Boston study team, interviewed in VA Research Currents, says the technology has been around a while, but it was previously used on the body for wound healing and pain. Using it on the brain is new. The LED light has been shown to boost the output of nitric oxide, improving blood flow. Studies have shown that LED improves brain function, including attention and memory, emotions, and sleep.
Naeser says most of the TBI and PTSD cases helped so far with LEDs on the head included cognitive rehabilitation therapy. The patients showed additional progress after the LED treatments. A combination of both treatments would likely produce the best results, she says.
Providers at the Long Beach VAMC have been using SGB, commonly used in pain management with ropivacaine or bupivacaine, to reduce the symptoms of PTSD. According to the VA Evidence-based Synthesis Program (ESP), SGB may ease anxiety and the alert response by inhibiting connections between the peripheral sympathetic nerve system and regions of the cerebral cortex, such as the amygdala, thought to be abnormally activated in PTSD. Stellate ganglion block also has been associated with biologic markers of sedation.
The ESP experts say there is insufficient information to determine which veterans are most likely to benefit from SGB for PTSD, but an uncontrolled, unblinded case series of 30 active duty service members with combat-related PTSD suggests that those with predominantly hyperarousal and avoidance symptoms might be the best candidates. Patients who have undergone SGB have found it highly acceptable, although the invasive nature of SGB may be a barrier for some. Findings from the first randomized controlled trial of SGB for PTSD were inconclusive, the panel said; further research is warranted.
The VA is examining two alternative treatments for TBI and PTSD: a light-emitting diode (LED) treatment for mild to moderate TBI and stellate ganglion block (SGB) for PTSD.
In the LED treatment, which takes about 30 minutes, a lightweight LED-lined helmet is placed on the patient’s head, and more diodes are placed inside the nose to deliver photons to the deeper parts of the brain. The light is painless and generates no heat.
Although it is considered investigational, LED therapy is available at the VAHS Boston, as well as for veterans to use at home. Dr. Margaret Naeser, a professor of neurology at Boston University School of Medicine and lead investigator of the Boston study team, interviewed in VA Research Currents, says the technology has been around a while, but it was previously used on the body for wound healing and pain. Using it on the brain is new. The LED light has been shown to boost the output of nitric oxide, improving blood flow. Studies have shown that LED improves brain function, including attention and memory, emotions, and sleep.
Naeser says most of the TBI and PTSD cases helped so far with LEDs on the head included cognitive rehabilitation therapy. The patients showed additional progress after the LED treatments. A combination of both treatments would likely produce the best results, she says.
Providers at the Long Beach VAMC have been using SGB, commonly used in pain management with ropivacaine or bupivacaine, to reduce the symptoms of PTSD. According to the VA Evidence-based Synthesis Program (ESP), SGB may ease anxiety and the alert response by inhibiting connections between the peripheral sympathetic nerve system and regions of the cerebral cortex, such as the amygdala, thought to be abnormally activated in PTSD. Stellate ganglion block also has been associated with biologic markers of sedation.
The ESP experts say there is insufficient information to determine which veterans are most likely to benefit from SGB for PTSD, but an uncontrolled, unblinded case series of 30 active duty service members with combat-related PTSD suggests that those with predominantly hyperarousal and avoidance symptoms might be the best candidates. Patients who have undergone SGB have found it highly acceptable, although the invasive nature of SGB may be a barrier for some. Findings from the first randomized controlled trial of SGB for PTSD were inconclusive, the panel said; further research is warranted.
The VA is examining two alternative treatments for TBI and PTSD: a light-emitting diode (LED) treatment for mild to moderate TBI and stellate ganglion block (SGB) for PTSD.
In the LED treatment, which takes about 30 minutes, a lightweight LED-lined helmet is placed on the patient’s head, and more diodes are placed inside the nose to deliver photons to the deeper parts of the brain. The light is painless and generates no heat.
Although it is considered investigational, LED therapy is available at the VAHS Boston, as well as for veterans to use at home. Dr. Margaret Naeser, a professor of neurology at Boston University School of Medicine and lead investigator of the Boston study team, interviewed in VA Research Currents, says the technology has been around a while, but it was previously used on the body for wound healing and pain. Using it on the brain is new. The LED light has been shown to boost the output of nitric oxide, improving blood flow. Studies have shown that LED improves brain function, including attention and memory, emotions, and sleep.
Naeser says most of the TBI and PTSD cases helped so far with LEDs on the head included cognitive rehabilitation therapy. The patients showed additional progress after the LED treatments. A combination of both treatments would likely produce the best results, she says.
Providers at the Long Beach VAMC have been using SGB, commonly used in pain management with ropivacaine or bupivacaine, to reduce the symptoms of PTSD. According to the VA Evidence-based Synthesis Program (ESP), SGB may ease anxiety and the alert response by inhibiting connections between the peripheral sympathetic nerve system and regions of the cerebral cortex, such as the amygdala, thought to be abnormally activated in PTSD. Stellate ganglion block also has been associated with biologic markers of sedation.
The ESP experts say there is insufficient information to determine which veterans are most likely to benefit from SGB for PTSD, but an uncontrolled, unblinded case series of 30 active duty service members with combat-related PTSD suggests that those with predominantly hyperarousal and avoidance symptoms might be the best candidates. Patients who have undergone SGB have found it highly acceptable, although the invasive nature of SGB may be a barrier for some. Findings from the first randomized controlled trial of SGB for PTSD were inconclusive, the panel said; further research is warranted.
Perfusion-only scan rules out PE in pregnancy
For pregnant women with suspected pulmonary embolism (PE), (CTPA), according to authors of a recent retrospective study.
Pulmonary embolism causes 9% of maternal deaths in the United States, according to the authors of the study, which was published online in the journal CHEST®. While it’s clear that perfusion scans yield lower radiation exposure than CTPA, to date, there has only been limited study of its diagnostic performance in women with suspected PE.
The low-dose perfusion scan offered comparable diagnostic efficacy while potentially limiting radiation exposure, according to the single-center cohort study.
The retrospective study included pregnant women (mean age, 27.3 years) who underwent imaging for pulmonary embolism at Montefiore Medical Center, New York, between 2008 and 2013. A total of 225 women underwent perfusion-only scans, while 97 underwent CTPA.
Chest pain and dyspnea were the most common symptoms for patients in both groups: 136 of the patients (60.4%) in the low-dose perfusion group reported chest pain versus 40 patients (41.2%) in the CTPA group. About half of the patients in both groups had dyspnea.
Tachycardia was found in 43 of patients (44.3%) who underwent CTPA, compared with 77 of patients (34.2% ) who underwent the diagnostic test involving less radiation exposure.
Imaging was negative for PE in 198 of the patients (88.0%) who were scanned with low-dose perfusion, while 84 of patients (86.6%) who had CTPAs were negative for PE. For both groups of patients, the percentage who had indeterminate imaging was 9.3%. Only one study participant had a deep vein thrombosis at the time she presented with PE symptoms.
The primary end point of the study, negative predictive value, was 100% for the perfusion-only group and 97.5% for CTPA, according to the report. It was determined by a diagnosis of venous thromboembolism within 90 days of evaluation.
Those “indistinguishable” negative predictive values suggest that low-dose perfusion scintigraphy performs comparably to CTPA, making it an appropriate first diagnostic modality for pregnant women who are suspected of having pulmonary embolism, Dr. Sheen and her colleagues wrote.
The negative predictive value was a particularly important endpoint to evaluate because pulmonary embolism is rare among pregnant women and most perfusion-only imaging is negative, the authors stated.
Of the women in the study, 252 (89%) of those who tested negative for PE – either by a low-dose perfusion scan or a CTPA – returned to the medical center for follow-up 90 days later. Thromboembolic events occurred in two of the women who previously had a negative CTPA, but none occurred in patients who had been tested for PE with low-dose perfusion scan. The two thromboembolic events were detected in women who were no longer pregnant.
Ten patients in the study (3.1%) were treated for pulmonary embolism, the authors reported. The PE diagnoses were based on four positive low-dose perfusion scans and six positive CTPAs “in conjunction with clinical suspicion.” These patients’ most common symptoms were chest pain and dyspnea, and one of these patients had recently been diagnosed with a deep vein thrombosis.
When perfusion defects are found, they should be interpreted cautiously, particularly in asthmatic patients, according to authors: “Segmental perfusion defects secondary to abnormal ventilation cannot be distinguished from PE without a ventilation scan,”they noted.
Three of the patients diagnosed with a PE had asthma. In a subanalysis of the 77 patients with asthma who participated in this study, the negative predictive values were 100% for both those who received a low-dose perfusion scan and those who received a CTPA. For patients in this subgroup, the negative rates of PE from low-dose perfusion scan and CTPA were 74.1% and 87.1%, respectively.
“Maternal-fetal radiation exposure should be of utmost importance when considering the choice of diagnostic test,” the authors wrote. “When available, [a low-dose perfusion scan] is a reasonable first choice modality for suspected pulmonary embolism in pregnant women with a negative chest radiograph.”
One study coauthor is on an advisory panel for Jubilant DraxImage, and another has a spouse who is a board member of Kyron Pharma Consulting. The remaining authors, including Dr. Sheen,reported no conflicts of interest.
SOURCE: Sheen JJ et al. Chest. 2018 Feb. doi: 10.1016/j.chest.2017.08.005.
Nirmal Sharma, MD, comments: During pregnancy, all radiation is bad radiation, but when it was really needed, we did use this low-radiation perfusion scan quite a bit at my past institution. This article definitely shines light on the utility/validity of this technique because most centers still use a computed tomographic pulmonary angiography study in pregnant females (with shielding methods) if suspicion of pulmonary embolism is high. The downside to low-dose perfusion scintigraphy is that it cannot be used in patients with grossly abnormal chest x-rays.

Nirmal Sharma, MD, comments: During pregnancy, all radiation is bad radiation, but when it was really needed, we did use this low-radiation perfusion scan quite a bit at my past institution. This article definitely shines light on the utility/validity of this technique because most centers still use a computed tomographic pulmonary angiography study in pregnant females (with shielding methods) if suspicion of pulmonary embolism is high. The downside to low-dose perfusion scintigraphy is that it cannot be used in patients with grossly abnormal chest x-rays.
Nirmal Sharma, MD, comments: During pregnancy, all radiation is bad radiation, but when it was really needed, we did use this low-radiation perfusion scan quite a bit at my past institution. This article definitely shines light on the utility/validity of this technique because most centers still use a computed tomographic pulmonary angiography study in pregnant females (with shielding methods) if suspicion of pulmonary embolism is high. The downside to low-dose perfusion scintigraphy is that it cannot be used in patients with grossly abnormal chest x-rays.
For pregnant women with suspected pulmonary embolism (PE), (CTPA), according to authors of a recent retrospective study.
Pulmonary embolism causes 9% of maternal deaths in the United States, according to the authors of the study, which was published online in the journal CHEST®. While it’s clear that perfusion scans yield lower radiation exposure than CTPA, to date, there has only been limited study of its diagnostic performance in women with suspected PE.
The low-dose perfusion scan offered comparable diagnostic efficacy while potentially limiting radiation exposure, according to the single-center cohort study.
The retrospective study included pregnant women (mean age, 27.3 years) who underwent imaging for pulmonary embolism at Montefiore Medical Center, New York, between 2008 and 2013. A total of 225 women underwent perfusion-only scans, while 97 underwent CTPA.
Chest pain and dyspnea were the most common symptoms for patients in both groups: 136 of the patients (60.4%) in the low-dose perfusion group reported chest pain versus 40 patients (41.2%) in the CTPA group. About half of the patients in both groups had dyspnea.
Tachycardia was found in 43 of patients (44.3%) who underwent CTPA, compared with 77 of patients (34.2% ) who underwent the diagnostic test involving less radiation exposure.
Imaging was negative for PE in 198 of the patients (88.0%) who were scanned with low-dose perfusion, while 84 of patients (86.6%) who had CTPAs were negative for PE. For both groups of patients, the percentage who had indeterminate imaging was 9.3%. Only one study participant had a deep vein thrombosis at the time she presented with PE symptoms.
The primary end point of the study, negative predictive value, was 100% for the perfusion-only group and 97.5% for CTPA, according to the report. It was determined by a diagnosis of venous thromboembolism within 90 days of evaluation.
Those “indistinguishable” negative predictive values suggest that low-dose perfusion scintigraphy performs comparably to CTPA, making it an appropriate first diagnostic modality for pregnant women who are suspected of having pulmonary embolism, Dr. Sheen and her colleagues wrote.
The negative predictive value was a particularly important endpoint to evaluate because pulmonary embolism is rare among pregnant women and most perfusion-only imaging is negative, the authors stated.
Of the women in the study, 252 (89%) of those who tested negative for PE – either by a low-dose perfusion scan or a CTPA – returned to the medical center for follow-up 90 days later. Thromboembolic events occurred in two of the women who previously had a negative CTPA, but none occurred in patients who had been tested for PE with low-dose perfusion scan. The two thromboembolic events were detected in women who were no longer pregnant.
Ten patients in the study (3.1%) were treated for pulmonary embolism, the authors reported. The PE diagnoses were based on four positive low-dose perfusion scans and six positive CTPAs “in conjunction with clinical suspicion.” These patients’ most common symptoms were chest pain and dyspnea, and one of these patients had recently been diagnosed with a deep vein thrombosis.
When perfusion defects are found, they should be interpreted cautiously, particularly in asthmatic patients, according to authors: “Segmental perfusion defects secondary to abnormal ventilation cannot be distinguished from PE without a ventilation scan,”they noted.
Three of the patients diagnosed with a PE had asthma. In a subanalysis of the 77 patients with asthma who participated in this study, the negative predictive values were 100% for both those who received a low-dose perfusion scan and those who received a CTPA. For patients in this subgroup, the negative rates of PE from low-dose perfusion scan and CTPA were 74.1% and 87.1%, respectively.
“Maternal-fetal radiation exposure should be of utmost importance when considering the choice of diagnostic test,” the authors wrote. “When available, [a low-dose perfusion scan] is a reasonable first choice modality for suspected pulmonary embolism in pregnant women with a negative chest radiograph.”
One study coauthor is on an advisory panel for Jubilant DraxImage, and another has a spouse who is a board member of Kyron Pharma Consulting. The remaining authors, including Dr. Sheen,reported no conflicts of interest.
SOURCE: Sheen JJ et al. Chest. 2018 Feb. doi: 10.1016/j.chest.2017.08.005.
For pregnant women with suspected pulmonary embolism (PE), (CTPA), according to authors of a recent retrospective study.
Pulmonary embolism causes 9% of maternal deaths in the United States, according to the authors of the study, which was published online in the journal CHEST®. While it’s clear that perfusion scans yield lower radiation exposure than CTPA, to date, there has only been limited study of its diagnostic performance in women with suspected PE.
The low-dose perfusion scan offered comparable diagnostic efficacy while potentially limiting radiation exposure, according to the single-center cohort study.
The retrospective study included pregnant women (mean age, 27.3 years) who underwent imaging for pulmonary embolism at Montefiore Medical Center, New York, between 2008 and 2013. A total of 225 women underwent perfusion-only scans, while 97 underwent CTPA.
Chest pain and dyspnea were the most common symptoms for patients in both groups: 136 of the patients (60.4%) in the low-dose perfusion group reported chest pain versus 40 patients (41.2%) in the CTPA group. About half of the patients in both groups had dyspnea.
Tachycardia was found in 43 of patients (44.3%) who underwent CTPA, compared with 77 of patients (34.2% ) who underwent the diagnostic test involving less radiation exposure.
Imaging was negative for PE in 198 of the patients (88.0%) who were scanned with low-dose perfusion, while 84 of patients (86.6%) who had CTPAs were negative for PE. For both groups of patients, the percentage who had indeterminate imaging was 9.3%. Only one study participant had a deep vein thrombosis at the time she presented with PE symptoms.
The primary end point of the study, negative predictive value, was 100% for the perfusion-only group and 97.5% for CTPA, according to the report. It was determined by a diagnosis of venous thromboembolism within 90 days of evaluation.
Those “indistinguishable” negative predictive values suggest that low-dose perfusion scintigraphy performs comparably to CTPA, making it an appropriate first diagnostic modality for pregnant women who are suspected of having pulmonary embolism, Dr. Sheen and her colleagues wrote.
The negative predictive value was a particularly important endpoint to evaluate because pulmonary embolism is rare among pregnant women and most perfusion-only imaging is negative, the authors stated.
Of the women in the study, 252 (89%) of those who tested negative for PE – either by a low-dose perfusion scan or a CTPA – returned to the medical center for follow-up 90 days later. Thromboembolic events occurred in two of the women who previously had a negative CTPA, but none occurred in patients who had been tested for PE with low-dose perfusion scan. The two thromboembolic events were detected in women who were no longer pregnant.
Ten patients in the study (3.1%) were treated for pulmonary embolism, the authors reported. The PE diagnoses were based on four positive low-dose perfusion scans and six positive CTPAs “in conjunction with clinical suspicion.” These patients’ most common symptoms were chest pain and dyspnea, and one of these patients had recently been diagnosed with a deep vein thrombosis.
When perfusion defects are found, they should be interpreted cautiously, particularly in asthmatic patients, according to authors: “Segmental perfusion defects secondary to abnormal ventilation cannot be distinguished from PE without a ventilation scan,”they noted.
Three of the patients diagnosed with a PE had asthma. In a subanalysis of the 77 patients with asthma who participated in this study, the negative predictive values were 100% for both those who received a low-dose perfusion scan and those who received a CTPA. For patients in this subgroup, the negative rates of PE from low-dose perfusion scan and CTPA were 74.1% and 87.1%, respectively.
“Maternal-fetal radiation exposure should be of utmost importance when considering the choice of diagnostic test,” the authors wrote. “When available, [a low-dose perfusion scan] is a reasonable first choice modality for suspected pulmonary embolism in pregnant women with a negative chest radiograph.”
One study coauthor is on an advisory panel for Jubilant DraxImage, and another has a spouse who is a board member of Kyron Pharma Consulting. The remaining authors, including Dr. Sheen,reported no conflicts of interest.
SOURCE: Sheen JJ et al. Chest. 2018 Feb. doi: 10.1016/j.chest.2017.08.005.
FROM CHEST®
Key clinical point: In the evaluation of pregnant women with suspected pulmonary embolism, low-dose perfusion scintigraphy may offer diagnostic performance that’s comparable to CTPA.
Major finding: The negative predictive value of a pulmonary embolism was 100% for the low dose perfusion scan, compared with 97.5% for CTPA.
Study details: A retrospective, single-center cohort study including 322 pregnant women who underwent imaging studies for suspected pulmonary embolism.
Disclosures: One study coauthor is on an advisory panel for Jubilant DraxImage, and another has a spouse who is a board member of Kyron Pharma Consulting. The remaining authors, including Dr. Sheen,reported no conflicts of interest.
Source: Sheen JJ et al. Chest. 2018 Feb. doi: 10.1016/j.chest.2017.08.005.
Flu season shows signs of slowing
Flu-related outpatient activity dropped for the second week in a row as the cumulative hospitalization rate continues to rise, according to data from the Centers for Disease Control and Prevention.
For the week ending Feb. 17, the proportion of outpatient visits for influenza-like illness (ILI) was 6.4%, which was down from 7.4% the previous week (Feb. 10) and down from the seasonal high of 7.5% set 2 weeks earlier, the CDC said in its weekly flu surveillance report. The rate for the week ending Feb. 10 was reported last week as 7.5%, but it has been revised downward.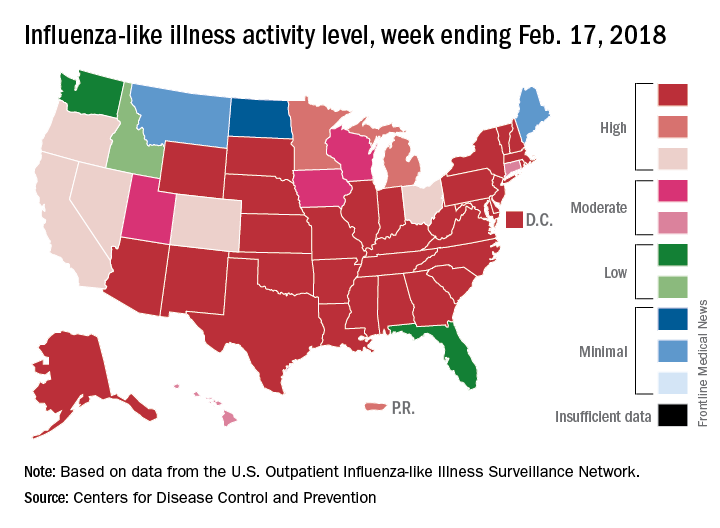
State reports of ILI activity support the decreases seen in the national outpatient rate. There were 33 states at level 10 on the CDC’s 1-10 scale for the week ending Feb. 17 – down from 39 the week before – and a total of 41 states in the “high” range from levels 8-10, compared with 45 the previous week, CDC’s FluView website shows.
Reports of flu-related pediatric deaths continued: 13 deaths were reported during the week, although 9 occurred in previous weeks. The total for the 2017-2018 season is now 97. There were 110 pediatric deaths in the entire 2016-2017 season, 93 during the 2015-2016 season, and 149 in 2014-2015, the CDC said.
Flu-related outpatient activity dropped for the second week in a row as the cumulative hospitalization rate continues to rise, according to data from the Centers for Disease Control and Prevention.
For the week ending Feb. 17, the proportion of outpatient visits for influenza-like illness (ILI) was 6.4%, which was down from 7.4% the previous week (Feb. 10) and down from the seasonal high of 7.5% set 2 weeks earlier, the CDC said in its weekly flu surveillance report. The rate for the week ending Feb. 10 was reported last week as 7.5%, but it has been revised downward.
State reports of ILI activity support the decreases seen in the national outpatient rate. There were 33 states at level 10 on the CDC’s 1-10 scale for the week ending Feb. 17 – down from 39 the week before – and a total of 41 states in the “high” range from levels 8-10, compared with 45 the previous week, CDC’s FluView website shows.
Reports of flu-related pediatric deaths continued: 13 deaths were reported during the week, although 9 occurred in previous weeks. The total for the 2017-2018 season is now 97. There were 110 pediatric deaths in the entire 2016-2017 season, 93 during the 2015-2016 season, and 149 in 2014-2015, the CDC said.
Flu-related outpatient activity dropped for the second week in a row as the cumulative hospitalization rate continues to rise, according to data from the Centers for Disease Control and Prevention.
For the week ending Feb. 17, the proportion of outpatient visits for influenza-like illness (ILI) was 6.4%, which was down from 7.4% the previous week (Feb. 10) and down from the seasonal high of 7.5% set 2 weeks earlier, the CDC said in its weekly flu surveillance report. The rate for the week ending Feb. 10 was reported last week as 7.5%, but it has been revised downward.
State reports of ILI activity support the decreases seen in the national outpatient rate. There were 33 states at level 10 on the CDC’s 1-10 scale for the week ending Feb. 17 – down from 39 the week before – and a total of 41 states in the “high” range from levels 8-10, compared with 45 the previous week, CDC’s FluView website shows.
Reports of flu-related pediatric deaths continued: 13 deaths were reported during the week, although 9 occurred in previous weeks. The total for the 2017-2018 season is now 97. There were 110 pediatric deaths in the entire 2016-2017 season, 93 during the 2015-2016 season, and 149 in 2014-2015, the CDC said.
Shock Treatment When It’s Needed Most
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
When blood pressure drops dangerously low, organ failure and death are real possibilities. Most deaths from trauma-related shock happen within 24 hours. But not all critically ill hypotensive patients respond to available therapies. A newly approved injectable drug could be a lifesaver for those patients.
Giapreza (angiotensin II/La Jolla Pharmaceutical, San Diego, CA) injection for intravenous infusion has been approved to increase blood pressure in cases of septic or other distributive shock. In a clinical trial of 321 patients with shock and critically low blood pressure, significantly more responded to treatment with Giapreza, compared with placebo. Giapreza effectively raised blood pressure when added to conventional treatments.
Giapreza can cause dangerous blood clots, including deep vein thrombosis. The FDA advises prophylactic treatment for blood clots.
House cleaning linked to lung function decline
that has found accelerated decline in lung function among women regularly engaged in cleaning activities.
The longitudinal population-based cohort study, published online Feb. 16 in the American Journal of Respiratory and Critical Care Medicine, looked at the lung health of 6,230 people who were followed for more than 20 years as part of the European Community Respiratory Health Survey.
Analysis based on questionnaires about cleaning practices revealed that women who were responsible for cleaning at home or who worked as professional cleaners showed significantly greater declines in maximum forced vital capacity (FVC) and maximum forced expiratory volume in 1 second (FEV1), compared with women who said they did not regularly clean.
However, there was no association between cleaning practices in men – either professional or domestic – and accelerated lung function decline. The authors suggested that the exposures experienced by men who worked as cleaners may have been different from the exposures experienced by women. They also noted that the small numbers of male cleaners meant the study wasn’t powered to pick up greater declines in lung function.
The study also showed a significant association between use of cleaning products and decline in lung function. Women who used sprays or other cleaning agents at least once a week showed significantly greater declines in FEV1 and FVC, compared with women who didn’t use cleaning products. Again, this effect was not significant in men.
“One possible mechanism for the accelerated decline in cleaners is the repetitive exposure to low-grade irritative cleaning agents over time, thereby causing persistent changes in the airways,” the authors wrote. “Repeated exposure could lead to remodelling of the airways, thereby over time causing an accelerated decline in FVC and FEV1.”
The analysis found no significant increases in the incidence of chronic airway obstruction among regular cleaners, nor among those who used cleaning products. The authors noted that while previous studies had suggested an increase in chronic obstructive pulmonary disease among occupational cleaners, their study reported relatively few cases of COPD.
While the prevalence of asthma was slightly higher in the two groups of women exposed to regular cleaning (12.3% and 13.7%, versus 9.6%), adjustment for asthma in the analysis did not change the associations. This suggests that the declines in lung function seen in regular cleaners were not mediated by cleaning-related asthma, the researchers noted.
They also noted that the women who reported not engaging in any cleaning may represent a particular socioeconomic group, but adjustment for socioeconomic status did not alter the associations.
The European Community Respiratory Health Survey is supported by the European Union, the European Commission, and the Medical Research Council. No conflicts of interest were reported.
SOURCE: Svanes Ø et al. Am J Resp Crit Care Med. 2018 Feb 16. doi: 10.1164/rccm.201706-1311OC.
that has found accelerated decline in lung function among women regularly engaged in cleaning activities.
The longitudinal population-based cohort study, published online Feb. 16 in the American Journal of Respiratory and Critical Care Medicine, looked at the lung health of 6,230 people who were followed for more than 20 years as part of the European Community Respiratory Health Survey.
Analysis based on questionnaires about cleaning practices revealed that women who were responsible for cleaning at home or who worked as professional cleaners showed significantly greater declines in maximum forced vital capacity (FVC) and maximum forced expiratory volume in 1 second (FEV1), compared with women who said they did not regularly clean.
However, there was no association between cleaning practices in men – either professional or domestic – and accelerated lung function decline. The authors suggested that the exposures experienced by men who worked as cleaners may have been different from the exposures experienced by women. They also noted that the small numbers of male cleaners meant the study wasn’t powered to pick up greater declines in lung function.
The study also showed a significant association between use of cleaning products and decline in lung function. Women who used sprays or other cleaning agents at least once a week showed significantly greater declines in FEV1 and FVC, compared with women who didn’t use cleaning products. Again, this effect was not significant in men.
“One possible mechanism for the accelerated decline in cleaners is the repetitive exposure to low-grade irritative cleaning agents over time, thereby causing persistent changes in the airways,” the authors wrote. “Repeated exposure could lead to remodelling of the airways, thereby over time causing an accelerated decline in FVC and FEV1.”
The analysis found no significant increases in the incidence of chronic airway obstruction among regular cleaners, nor among those who used cleaning products. The authors noted that while previous studies had suggested an increase in chronic obstructive pulmonary disease among occupational cleaners, their study reported relatively few cases of COPD.
While the prevalence of asthma was slightly higher in the two groups of women exposed to regular cleaning (12.3% and 13.7%, versus 9.6%), adjustment for asthma in the analysis did not change the associations. This suggests that the declines in lung function seen in regular cleaners were not mediated by cleaning-related asthma, the researchers noted.
They also noted that the women who reported not engaging in any cleaning may represent a particular socioeconomic group, but adjustment for socioeconomic status did not alter the associations.
The European Community Respiratory Health Survey is supported by the European Union, the European Commission, and the Medical Research Council. No conflicts of interest were reported.
SOURCE: Svanes Ø et al. Am J Resp Crit Care Med. 2018 Feb 16. doi: 10.1164/rccm.201706-1311OC.
that has found accelerated decline in lung function among women regularly engaged in cleaning activities.
The longitudinal population-based cohort study, published online Feb. 16 in the American Journal of Respiratory and Critical Care Medicine, looked at the lung health of 6,230 people who were followed for more than 20 years as part of the European Community Respiratory Health Survey.
Analysis based on questionnaires about cleaning practices revealed that women who were responsible for cleaning at home or who worked as professional cleaners showed significantly greater declines in maximum forced vital capacity (FVC) and maximum forced expiratory volume in 1 second (FEV1), compared with women who said they did not regularly clean.
However, there was no association between cleaning practices in men – either professional or domestic – and accelerated lung function decline. The authors suggested that the exposures experienced by men who worked as cleaners may have been different from the exposures experienced by women. They also noted that the small numbers of male cleaners meant the study wasn’t powered to pick up greater declines in lung function.
The study also showed a significant association between use of cleaning products and decline in lung function. Women who used sprays or other cleaning agents at least once a week showed significantly greater declines in FEV1 and FVC, compared with women who didn’t use cleaning products. Again, this effect was not significant in men.
“One possible mechanism for the accelerated decline in cleaners is the repetitive exposure to low-grade irritative cleaning agents over time, thereby causing persistent changes in the airways,” the authors wrote. “Repeated exposure could lead to remodelling of the airways, thereby over time causing an accelerated decline in FVC and FEV1.”
The analysis found no significant increases in the incidence of chronic airway obstruction among regular cleaners, nor among those who used cleaning products. The authors noted that while previous studies had suggested an increase in chronic obstructive pulmonary disease among occupational cleaners, their study reported relatively few cases of COPD.
While the prevalence of asthma was slightly higher in the two groups of women exposed to regular cleaning (12.3% and 13.7%, versus 9.6%), adjustment for asthma in the analysis did not change the associations. This suggests that the declines in lung function seen in regular cleaners were not mediated by cleaning-related asthma, the researchers noted.
They also noted that the women who reported not engaging in any cleaning may represent a particular socioeconomic group, but adjustment for socioeconomic status did not alter the associations.
The European Community Respiratory Health Survey is supported by the European Union, the European Commission, and the Medical Research Council. No conflicts of interest were reported.
SOURCE: Svanes Ø et al. Am J Resp Crit Care Med. 2018 Feb 16. doi: 10.1164/rccm.201706-1311OC.
FROM AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Key clinical point: Women – but not men – who regularly clean homes either domestically or professionally show accelerated declines in lung function.
Major finding: Women who work as cleaners or clean their own homes regularly show greater declines in FEV1 and FVC, compared with women who do not clean regularly.
Data source: Longitudinal cohort study of 6,230 individuals in the European Community Respiratory Health Survey.
Disclosures: The European Community Respiratory Health Survey is supported by the European Union, the European Commission, and the Medical Research Council. No conflicts of interest were provided.
Source: Svanes Ø et al. Am J Resp Crit Care Med. 2018 Feb. 16. doi: 10.1164/rccm.201706-1311OC.