User login
OSA may provide cardioprotection
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in CHEST.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“These results suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury,” the authors said in the report. The findings “suggest that OSA has a protective effect in the context of MI,” they added.
Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed Inc., Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in CHEST.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“These results suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury,” the authors said in the report. The findings “suggest that OSA has a protective effect in the context of MI,” they added.
Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed Inc., Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in CHEST.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“These results suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury,” the authors said in the report. The findings “suggest that OSA has a protective effect in the context of MI,” they added.
Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed Inc., Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046
FROM CHEST
Key clinical point: Obstructive sleep apnea may have a protective effect in acute coronary syndromes.
Major finding: Median peak cTn-I value was significantly higher in patients without obstructive sleep apnea than in OSA patients (10.7, interquartile range: 1.78-40.1 vs. 3.79; IQR: 0.37-24.3 respectively; P = .04).
Data source: An observational study of 89 OSA and 38 non-OSA patients admitted for acute coronary syndromes.
Disclosures: The authors disclosed relationships with ResMed Inc., Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER.
Source: Sánchez-de-la-Torre, A et al. CHEST. 2018 Feb 5;153[2]:329-38.
This is what a flu pandemic looks like
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.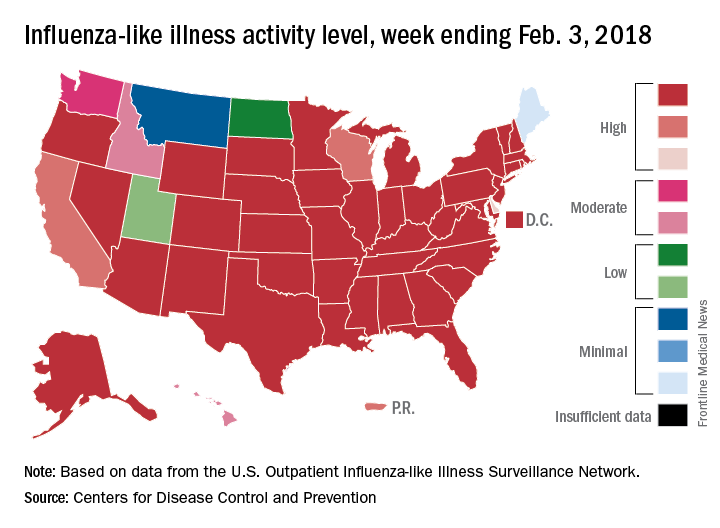
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
FROM A CDC TELECONFERENCE
HIV Treatment: OK to Take a Break?
Antiretroviral therapy (ART) keeps viral load of HIV at undetectable levels. The key is taking it daily. But it may be possible for patients to temporarily stop ART without long-lasting or irreversible damage to the immune system.
That approach is called analytical treatment interruption (ATI), and it is the subject of a study by NIH researchers at the National Institute of Allergy and Infectious Diseases. They analyzed blood samples from 10 volunteers who participated in a clinical trial that evaluated whether infusions of a broadly neutralizing antibody could control HIV in the absence of ART.
During the trial, participants temporarily stopped taking ART, resuming 22 to 115 days after stopping. In that hiatus, HIV reservoirs expanded and viral load increased. The researchers also observed abnormalities in the participants’ immune cells. However, 6 to 12 months after the participants resumed ART, the size of the HIV reservoirs and the immune parameters returned to the pre-ATI levels.
These findings support the use of ATI in clinical trials of therapeutic strategies aimed at achieving sustained ART-free remission, the researchers say. They are now conducting a clinical trial to monitor the impact of short-term ATI on a variety of parameters in people living with HIV.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-supports-use-short-term-hiv-treatment-interruption-clinical-trials. Published January 11, 2018. Accessed February 8, 2018.
Antiretroviral therapy (ART) keeps viral load of HIV at undetectable levels. The key is taking it daily. But it may be possible for patients to temporarily stop ART without long-lasting or irreversible damage to the immune system.
That approach is called analytical treatment interruption (ATI), and it is the subject of a study by NIH researchers at the National Institute of Allergy and Infectious Diseases. They analyzed blood samples from 10 volunteers who participated in a clinical trial that evaluated whether infusions of a broadly neutralizing antibody could control HIV in the absence of ART.
During the trial, participants temporarily stopped taking ART, resuming 22 to 115 days after stopping. In that hiatus, HIV reservoirs expanded and viral load increased. The researchers also observed abnormalities in the participants’ immune cells. However, 6 to 12 months after the participants resumed ART, the size of the HIV reservoirs and the immune parameters returned to the pre-ATI levels.
These findings support the use of ATI in clinical trials of therapeutic strategies aimed at achieving sustained ART-free remission, the researchers say. They are now conducting a clinical trial to monitor the impact of short-term ATI on a variety of parameters in people living with HIV.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-supports-use-short-term-hiv-treatment-interruption-clinical-trials. Published January 11, 2018. Accessed February 8, 2018.
Antiretroviral therapy (ART) keeps viral load of HIV at undetectable levels. The key is taking it daily. But it may be possible for patients to temporarily stop ART without long-lasting or irreversible damage to the immune system.
That approach is called analytical treatment interruption (ATI), and it is the subject of a study by NIH researchers at the National Institute of Allergy and Infectious Diseases. They analyzed blood samples from 10 volunteers who participated in a clinical trial that evaluated whether infusions of a broadly neutralizing antibody could control HIV in the absence of ART.
During the trial, participants temporarily stopped taking ART, resuming 22 to 115 days after stopping. In that hiatus, HIV reservoirs expanded and viral load increased. The researchers also observed abnormalities in the participants’ immune cells. However, 6 to 12 months after the participants resumed ART, the size of the HIV reservoirs and the immune parameters returned to the pre-ATI levels.
These findings support the use of ATI in clinical trials of therapeutic strategies aimed at achieving sustained ART-free remission, the researchers say. They are now conducting a clinical trial to monitor the impact of short-term ATI on a variety of parameters in people living with HIV.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-supports-use-short-term-hiv-treatment-interruption-clinical-trials. Published January 11, 2018. Accessed February 8, 2018.
Meningococcal Arthritis Masking as Possible Myeloma
For a group of clinicians in Australia, the diagnosis of meningococcal arthritis was “straightforward” except for abnormal serum total protein, anemia, and immunoglobulin results, which suggested their patient might have a hematological disorder such as myeloma.
The patient came to the hospital after 4 days of worsening knee and arm pain so severe he could not stand. His knees and both wrists showed swelling but no palpable lymphadenopathy or hepatosplenomegaly. The patient’s medical history showed he was taking no regular medications.
Joint aspiration grew Neisseria meningitidis. The patient’s blood tests showed hemoglobin 126 g/dL, white blood cell count 15.3 x 109/L, an unusually high total protein level (100 g/L), and an IgM kappa paraprotein band of 45 g/L on protein electrophoresis. A computed tomography scan showed widespread lymphadenopathy, hepatosplenomegaly, and multilevel thoracic vertebral collapse. A bone marrow biopsy showed evidence of a lymphocytic infiltrate, with lymphoplasmacytoid differentiation.
The histology best fitted a diagnosis of nodal marginal zone lymphoma with plasmacytic differentiation, the clinicians say. Having ruled out other possibilities, they settled on non-Hodgkin lymphoma.
Initially, the suspicion was that the patient had septic arthritis due to Staphylococcus aureus (the most common organism isolated in septic arthritis), and he was given piperacillin/tazobactam. That was changed to flucloxacillin and then to ceftriaxone after the result of N meningitidis. The patient also was treated with rituximab and bendamustine for the lymphoma with a complete remission.
Meningococcal infection presenting as septic arthritis in the case of invasive meningococcemia is rare, the clinicians say, but primary meningococcal arthritis is even rarer. The case highlights the important aspect that “diagnosis of one condition can lead to diagnosis of another”—in this case, the lymphoma-weakened immune system led to the symptoms of polyarthropathy and the diagnosis of primary meningococcal arthritis. The clinicians also cited a case of a patient who presented with meningococcal meningitis and arthritis who was found to have an underlying Waldenström disease, and a patient whose HIV was diagnosed again after the patient presented with meningococcal arthritis symptoms.
The clinicans say such cases underscore the importance of screening for an underlying impaired immune response in patients presenting with rare conditions such as meningococcal arthritis.
For a group of clinicians in Australia, the diagnosis of meningococcal arthritis was “straightforward” except for abnormal serum total protein, anemia, and immunoglobulin results, which suggested their patient might have a hematological disorder such as myeloma.
The patient came to the hospital after 4 days of worsening knee and arm pain so severe he could not stand. His knees and both wrists showed swelling but no palpable lymphadenopathy or hepatosplenomegaly. The patient’s medical history showed he was taking no regular medications.
Joint aspiration grew Neisseria meningitidis. The patient’s blood tests showed hemoglobin 126 g/dL, white blood cell count 15.3 x 109/L, an unusually high total protein level (100 g/L), and an IgM kappa paraprotein band of 45 g/L on protein electrophoresis. A computed tomography scan showed widespread lymphadenopathy, hepatosplenomegaly, and multilevel thoracic vertebral collapse. A bone marrow biopsy showed evidence of a lymphocytic infiltrate, with lymphoplasmacytoid differentiation.
The histology best fitted a diagnosis of nodal marginal zone lymphoma with plasmacytic differentiation, the clinicians say. Having ruled out other possibilities, they settled on non-Hodgkin lymphoma.
Initially, the suspicion was that the patient had septic arthritis due to Staphylococcus aureus (the most common organism isolated in septic arthritis), and he was given piperacillin/tazobactam. That was changed to flucloxacillin and then to ceftriaxone after the result of N meningitidis. The patient also was treated with rituximab and bendamustine for the lymphoma with a complete remission.
Meningococcal infection presenting as septic arthritis in the case of invasive meningococcemia is rare, the clinicians say, but primary meningococcal arthritis is even rarer. The case highlights the important aspect that “diagnosis of one condition can lead to diagnosis of another”—in this case, the lymphoma-weakened immune system led to the symptoms of polyarthropathy and the diagnosis of primary meningococcal arthritis. The clinicians also cited a case of a patient who presented with meningococcal meningitis and arthritis who was found to have an underlying Waldenström disease, and a patient whose HIV was diagnosed again after the patient presented with meningococcal arthritis symptoms.
The clinicans say such cases underscore the importance of screening for an underlying impaired immune response in patients presenting with rare conditions such as meningococcal arthritis.
For a group of clinicians in Australia, the diagnosis of meningococcal arthritis was “straightforward” except for abnormal serum total protein, anemia, and immunoglobulin results, which suggested their patient might have a hematological disorder such as myeloma.
The patient came to the hospital after 4 days of worsening knee and arm pain so severe he could not stand. His knees and both wrists showed swelling but no palpable lymphadenopathy or hepatosplenomegaly. The patient’s medical history showed he was taking no regular medications.
Joint aspiration grew Neisseria meningitidis. The patient’s blood tests showed hemoglobin 126 g/dL, white blood cell count 15.3 x 109/L, an unusually high total protein level (100 g/L), and an IgM kappa paraprotein band of 45 g/L on protein electrophoresis. A computed tomography scan showed widespread lymphadenopathy, hepatosplenomegaly, and multilevel thoracic vertebral collapse. A bone marrow biopsy showed evidence of a lymphocytic infiltrate, with lymphoplasmacytoid differentiation.
The histology best fitted a diagnosis of nodal marginal zone lymphoma with plasmacytic differentiation, the clinicians say. Having ruled out other possibilities, they settled on non-Hodgkin lymphoma.
Initially, the suspicion was that the patient had septic arthritis due to Staphylococcus aureus (the most common organism isolated in septic arthritis), and he was given piperacillin/tazobactam. That was changed to flucloxacillin and then to ceftriaxone after the result of N meningitidis. The patient also was treated with rituximab and bendamustine for the lymphoma with a complete remission.
Meningococcal infection presenting as septic arthritis in the case of invasive meningococcemia is rare, the clinicians say, but primary meningococcal arthritis is even rarer. The case highlights the important aspect that “diagnosis of one condition can lead to diagnosis of another”—in this case, the lymphoma-weakened immune system led to the symptoms of polyarthropathy and the diagnosis of primary meningococcal arthritis. The clinicians also cited a case of a patient who presented with meningococcal meningitis and arthritis who was found to have an underlying Waldenström disease, and a patient whose HIV was diagnosed again after the patient presented with meningococcal arthritis symptoms.
The clinicans say such cases underscore the importance of screening for an underlying impaired immune response in patients presenting with rare conditions such as meningococcal arthritis.
Why Fruit Flies (and People) Sleep Differently
Why do some people need more—or less—sleep than others do? Scientists from the National Heart, Lung, and Blood Institute say they have identified a group of genes that might help answer that question.
Using 13 generations of fruit flies bred to be long sleepers (18 hours a day) or short sleepers (3 hours a day), the researchers compared genetic data and identified 126 differences among 80 genes that seem to be associated with sleep duration. According to the researchers, the genetic differences were tied to several important developmental and cell signaling pathways, and some had known functions in brain development, learning, and memory.
The lifespans of the 2 groups of long and short sleepers did not differ from those of the flies with normal sleeping patterns. That suggests, the researchers say, that there are few physiologic consequences of being an extremely long or short sleeper.
The study is “an important step toward solving one of the biggest mysteries in biology: the need to sleep,” says study leader Susan Harbison, PhD. “The involvement of highly diverse biologic processes in sleep duration may help explain why the purpose of sleep has been so elusive.”
Why do some people need more—or less—sleep than others do? Scientists from the National Heart, Lung, and Blood Institute say they have identified a group of genes that might help answer that question.
Using 13 generations of fruit flies bred to be long sleepers (18 hours a day) or short sleepers (3 hours a day), the researchers compared genetic data and identified 126 differences among 80 genes that seem to be associated with sleep duration. According to the researchers, the genetic differences were tied to several important developmental and cell signaling pathways, and some had known functions in brain development, learning, and memory.
The lifespans of the 2 groups of long and short sleepers did not differ from those of the flies with normal sleeping patterns. That suggests, the researchers say, that there are few physiologic consequences of being an extremely long or short sleeper.
The study is “an important step toward solving one of the biggest mysteries in biology: the need to sleep,” says study leader Susan Harbison, PhD. “The involvement of highly diverse biologic processes in sleep duration may help explain why the purpose of sleep has been so elusive.”
Why do some people need more—or less—sleep than others do? Scientists from the National Heart, Lung, and Blood Institute say they have identified a group of genes that might help answer that question.
Using 13 generations of fruit flies bred to be long sleepers (18 hours a day) or short sleepers (3 hours a day), the researchers compared genetic data and identified 126 differences among 80 genes that seem to be associated with sleep duration. According to the researchers, the genetic differences were tied to several important developmental and cell signaling pathways, and some had known functions in brain development, learning, and memory.
The lifespans of the 2 groups of long and short sleepers did not differ from those of the flies with normal sleeping patterns. That suggests, the researchers say, that there are few physiologic consequences of being an extremely long or short sleeper.
The study is “an important step toward solving one of the biggest mysteries in biology: the need to sleep,” says study leader Susan Harbison, PhD. “The involvement of highly diverse biologic processes in sleep duration may help explain why the purpose of sleep has been so elusive.”
Pulmonary Fibrosis Foundation offers trial-finding app
The Pulmonary Fibrosis Foundation (PFF) has begun offering a tool to help patients navigate through more than 100 clinical trials aimed at advancing the treatment of pulmonary fibrosis, according to a statement from the Foundation.
The platform includes trials for patients with idiopathic pulmonary fibrosis.
“Before this, it was pretty impossible to search for clinical trials,” noted Bill Burke, a PF patient and support group leader from Williamsburg, Va., in the statement.
The tool, which is available both on the PFF website and as a free app, draws on information from ClinicalTrials.gov.
The Foundation intends for the new tool to give patients “a voice in their care process,” according to the statement.
“We want to empower patients to actively participate in identifying clinical trials,” said Harold R. Collard, MD, senior medical adviser of research and development for the Pulmonary Fibrosis Foundation.
More information about the trial finder is available on the PFF’s website.
The Pulmonary Fibrosis Foundation (PFF) has begun offering a tool to help patients navigate through more than 100 clinical trials aimed at advancing the treatment of pulmonary fibrosis, according to a statement from the Foundation.
The platform includes trials for patients with idiopathic pulmonary fibrosis.
“Before this, it was pretty impossible to search for clinical trials,” noted Bill Burke, a PF patient and support group leader from Williamsburg, Va., in the statement.
The tool, which is available both on the PFF website and as a free app, draws on information from ClinicalTrials.gov.
The Foundation intends for the new tool to give patients “a voice in their care process,” according to the statement.
“We want to empower patients to actively participate in identifying clinical trials,” said Harold R. Collard, MD, senior medical adviser of research and development for the Pulmonary Fibrosis Foundation.
More information about the trial finder is available on the PFF’s website.
The Pulmonary Fibrosis Foundation (PFF) has begun offering a tool to help patients navigate through more than 100 clinical trials aimed at advancing the treatment of pulmonary fibrosis, according to a statement from the Foundation.
The platform includes trials for patients with idiopathic pulmonary fibrosis.
“Before this, it was pretty impossible to search for clinical trials,” noted Bill Burke, a PF patient and support group leader from Williamsburg, Va., in the statement.
The tool, which is available both on the PFF website and as a free app, draws on information from ClinicalTrials.gov.
The Foundation intends for the new tool to give patients “a voice in their care process,” according to the statement.
“We want to empower patients to actively participate in identifying clinical trials,” said Harold R. Collard, MD, senior medical adviser of research and development for the Pulmonary Fibrosis Foundation.
More information about the trial finder is available on the PFF’s website.
Decline in non-Hodgkin lymphoma deaths to continue in 2018
Mortality from non-Hodgkin lymphoma is expected to be about 6.1 per 100,000 population in 2018, with the highest rate in Maine and West Virginia and the lowest in Utah.
in its Cancer Facts & Figures 2018, based on analysis of 2001-2015 data from the National Center for Health Statistics. That figure is down from the 20,140 predicted for 2017, as the trend in the death rate since 2006 has been a decline of about 2% per year.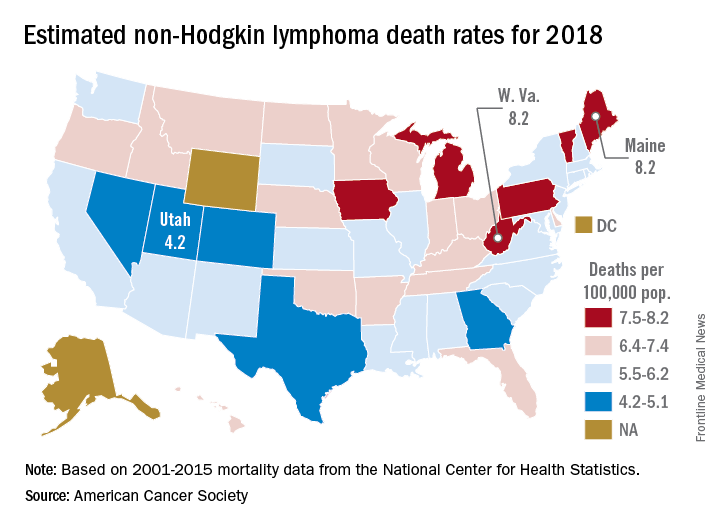
Nationally, death rates for NHL were 7.4 per 100,000 for males and 4.5 for females for 2011-2015, and incidence rates were 22.9 per 100,000 for males and 15.8 for females for 2010-2014, the ACS reported.
Over time, the relative survival rate for NHL has gone from 47% in 1975-1977 to 51% in 1987-1989 to 73% in 2007-2013, although there is some disparity between whites, whose respective rates are 47%, 51%, and 74%, and blacks, who have rates of 49%, 46%, and 67%, respectively, the ACS said.
Mortality from non-Hodgkin lymphoma is expected to be about 6.1 per 100,000 population in 2018, with the highest rate in Maine and West Virginia and the lowest in Utah.
in its Cancer Facts & Figures 2018, based on analysis of 2001-2015 data from the National Center for Health Statistics. That figure is down from the 20,140 predicted for 2017, as the trend in the death rate since 2006 has been a decline of about 2% per year.
Nationally, death rates for NHL were 7.4 per 100,000 for males and 4.5 for females for 2011-2015, and incidence rates were 22.9 per 100,000 for males and 15.8 for females for 2010-2014, the ACS reported.
Over time, the relative survival rate for NHL has gone from 47% in 1975-1977 to 51% in 1987-1989 to 73% in 2007-2013, although there is some disparity between whites, whose respective rates are 47%, 51%, and 74%, and blacks, who have rates of 49%, 46%, and 67%, respectively, the ACS said.
Mortality from non-Hodgkin lymphoma is expected to be about 6.1 per 100,000 population in 2018, with the highest rate in Maine and West Virginia and the lowest in Utah.
in its Cancer Facts & Figures 2018, based on analysis of 2001-2015 data from the National Center for Health Statistics. That figure is down from the 20,140 predicted for 2017, as the trend in the death rate since 2006 has been a decline of about 2% per year.
Nationally, death rates for NHL were 7.4 per 100,000 for males and 4.5 for females for 2011-2015, and incidence rates were 22.9 per 100,000 for males and 15.8 for females for 2010-2014, the ACS reported.
Over time, the relative survival rate for NHL has gone from 47% in 1975-1977 to 51% in 1987-1989 to 73% in 2007-2013, although there is some disparity between whites, whose respective rates are 47%, 51%, and 74%, and blacks, who have rates of 49%, 46%, and 67%, respectively, the ACS said.
FDA’s standards for approving generics are questioned
TORONTO – The Food and Drug Administration’s standards for demonstrating pharmacokinetic bioequivalence between two inhaled products, which allow for single batch comparisons of approved and generic candidate products, need to be revised to address batch to batch variability, suggested a presenter at the CHEST annual meeting.
Marketing approval of a new generic drug in the United States, including orally inhaled products, generally requires a demonstration of pharmacokinetic bioequivalence to a reference listed product. The standard criterion for statistical bioequivalence applied by the FDA requires the pharmacokinetics of the generic to be within about 10% of the branded product.
In early pharmacokinetic bioequivalence studies, Elise Burmeister Getz, PhD, and her colleagues compared single batches of their generic candidate OT329 Solis 100/50 to single batches of Advair Diskus 100/50 in five individual studies and single batches of Advair Diskus 100/50 to single batches of the same drug. They also found Advair Diskus 100/50 batches that were more than 30% different from each other.

“When patients differ from one another, we put many patients in the trial. And when batches differ from one another, we should be putting many batches in the trial,” Dr. Burmeister Getz, director of clinical pharmacology at Oriel Therapeutics, said at the CHEST meeting. “If we want a robust assessment of bioequivalence and not just a check the box exercise, we really need to have product sampling that’s aligned with product variability.”
When the researchers combined the data in a meta-analysis, bioequivalence was demonstrated, but the pooled analysis could not be used for FDA registration because of its retrospective nature.
They later conducted a prospective study with multiple batches of both the generic and branded drugs. This multiple-batch bioequivalence study involved 96 healthy subjects using 16 batches each of Advair Diskus and Oriel’s OT329 Solis 100/50. A single inhalation was administered to healthy adult subjects in a randomized crossover design and blood samples were collected pre dose and up to 48 hours after inhalation.
With the FDA’s definition of bioequivalence, the generic candidate fell within the bioequivalence goalposts, Dr. Burmeister Getz noted.
The issue of pharmacokinetic variance is not unique to Advair Diskus, but she and her colleagues don’t understand why different batches show such wide variability, Dr. Burmeister Getz noted.
“The advantage of this multibatch approach is that the results of the bioequivalence assessment aren’t dependent on the single batch that happened to be chosen for the study. They are generalizable to the product because the product has been robustly represented in the study,” Dr. Burmeister Getz told attendees.
Oriel makes OT329 Solis 100/50, a fully substitutable generic to Advair Diskus 100/50, which is indicated for treating asthma. Both are multidose dry powder oral inhalation products containing fluticasone propionate, to reduce inflammation in the lungs, and salmeterol, to relax muscles in the airways, for the maintenance treatment of asthma. Advair Diskus at higher doses is indicated for asthma and COPD.
An FDA response?
Asked what the FDA makes of the batch-to-batch variability data, Dr. Burmeister Getz answered simply, “We don’t know.” Before she and her colleagues ran the 16 batch per product study, they submitted their protocol to the FDA for review, but 1 year later, they still hadn’t heard any response.
“Sponsors are apparently allowed to simply pick their batch in a careful and, dare I say manipulative way, to gain the result they want. With a single batch study the selection of batch will absolutely determine the outcome of the study.”
In vitro bioequivalence studies are already required to use multiple batches, she noted.
This research was funded by Oriel Therapeutics, an indirect wholly-owned subsidiary of Novartis AG.
TORONTO – The Food and Drug Administration’s standards for demonstrating pharmacokinetic bioequivalence between two inhaled products, which allow for single batch comparisons of approved and generic candidate products, need to be revised to address batch to batch variability, suggested a presenter at the CHEST annual meeting.
Marketing approval of a new generic drug in the United States, including orally inhaled products, generally requires a demonstration of pharmacokinetic bioequivalence to a reference listed product. The standard criterion for statistical bioequivalence applied by the FDA requires the pharmacokinetics of the generic to be within about 10% of the branded product.
In early pharmacokinetic bioequivalence studies, Elise Burmeister Getz, PhD, and her colleagues compared single batches of their generic candidate OT329 Solis 100/50 to single batches of Advair Diskus 100/50 in five individual studies and single batches of Advair Diskus 100/50 to single batches of the same drug. They also found Advair Diskus 100/50 batches that were more than 30% different from each other.
“When patients differ from one another, we put many patients in the trial. And when batches differ from one another, we should be putting many batches in the trial,” Dr. Burmeister Getz, director of clinical pharmacology at Oriel Therapeutics, said at the CHEST meeting. “If we want a robust assessment of bioequivalence and not just a check the box exercise, we really need to have product sampling that’s aligned with product variability.”
When the researchers combined the data in a meta-analysis, bioequivalence was demonstrated, but the pooled analysis could not be used for FDA registration because of its retrospective nature.
They later conducted a prospective study with multiple batches of both the generic and branded drugs. This multiple-batch bioequivalence study involved 96 healthy subjects using 16 batches each of Advair Diskus and Oriel’s OT329 Solis 100/50. A single inhalation was administered to healthy adult subjects in a randomized crossover design and blood samples were collected pre dose and up to 48 hours after inhalation.
With the FDA’s definition of bioequivalence, the generic candidate fell within the bioequivalence goalposts, Dr. Burmeister Getz noted.
The issue of pharmacokinetic variance is not unique to Advair Diskus, but she and her colleagues don’t understand why different batches show such wide variability, Dr. Burmeister Getz noted.
“The advantage of this multibatch approach is that the results of the bioequivalence assessment aren’t dependent on the single batch that happened to be chosen for the study. They are generalizable to the product because the product has been robustly represented in the study,” Dr. Burmeister Getz told attendees.
Oriel makes OT329 Solis 100/50, a fully substitutable generic to Advair Diskus 100/50, which is indicated for treating asthma. Both are multidose dry powder oral inhalation products containing fluticasone propionate, to reduce inflammation in the lungs, and salmeterol, to relax muscles in the airways, for the maintenance treatment of asthma. Advair Diskus at higher doses is indicated for asthma and COPD.
An FDA response?
Asked what the FDA makes of the batch-to-batch variability data, Dr. Burmeister Getz answered simply, “We don’t know.” Before she and her colleagues ran the 16 batch per product study, they submitted their protocol to the FDA for review, but 1 year later, they still hadn’t heard any response.
“Sponsors are apparently allowed to simply pick their batch in a careful and, dare I say manipulative way, to gain the result they want. With a single batch study the selection of batch will absolutely determine the outcome of the study.”
In vitro bioequivalence studies are already required to use multiple batches, she noted.
This research was funded by Oriel Therapeutics, an indirect wholly-owned subsidiary of Novartis AG.
TORONTO – The Food and Drug Administration’s standards for demonstrating pharmacokinetic bioequivalence between two inhaled products, which allow for single batch comparisons of approved and generic candidate products, need to be revised to address batch to batch variability, suggested a presenter at the CHEST annual meeting.
Marketing approval of a new generic drug in the United States, including orally inhaled products, generally requires a demonstration of pharmacokinetic bioequivalence to a reference listed product. The standard criterion for statistical bioequivalence applied by the FDA requires the pharmacokinetics of the generic to be within about 10% of the branded product.
In early pharmacokinetic bioequivalence studies, Elise Burmeister Getz, PhD, and her colleagues compared single batches of their generic candidate OT329 Solis 100/50 to single batches of Advair Diskus 100/50 in five individual studies and single batches of Advair Diskus 100/50 to single batches of the same drug. They also found Advair Diskus 100/50 batches that were more than 30% different from each other.
“When patients differ from one another, we put many patients in the trial. And when batches differ from one another, we should be putting many batches in the trial,” Dr. Burmeister Getz, director of clinical pharmacology at Oriel Therapeutics, said at the CHEST meeting. “If we want a robust assessment of bioequivalence and not just a check the box exercise, we really need to have product sampling that’s aligned with product variability.”
When the researchers combined the data in a meta-analysis, bioequivalence was demonstrated, but the pooled analysis could not be used for FDA registration because of its retrospective nature.
They later conducted a prospective study with multiple batches of both the generic and branded drugs. This multiple-batch bioequivalence study involved 96 healthy subjects using 16 batches each of Advair Diskus and Oriel’s OT329 Solis 100/50. A single inhalation was administered to healthy adult subjects in a randomized crossover design and blood samples were collected pre dose and up to 48 hours after inhalation.
With the FDA’s definition of bioequivalence, the generic candidate fell within the bioequivalence goalposts, Dr. Burmeister Getz noted.
The issue of pharmacokinetic variance is not unique to Advair Diskus, but she and her colleagues don’t understand why different batches show such wide variability, Dr. Burmeister Getz noted.
“The advantage of this multibatch approach is that the results of the bioequivalence assessment aren’t dependent on the single batch that happened to be chosen for the study. They are generalizable to the product because the product has been robustly represented in the study,” Dr. Burmeister Getz told attendees.
Oriel makes OT329 Solis 100/50, a fully substitutable generic to Advair Diskus 100/50, which is indicated for treating asthma. Both are multidose dry powder oral inhalation products containing fluticasone propionate, to reduce inflammation in the lungs, and salmeterol, to relax muscles in the airways, for the maintenance treatment of asthma. Advair Diskus at higher doses is indicated for asthma and COPD.
An FDA response?
Asked what the FDA makes of the batch-to-batch variability data, Dr. Burmeister Getz answered simply, “We don’t know.” Before she and her colleagues ran the 16 batch per product study, they submitted their protocol to the FDA for review, but 1 year later, they still hadn’t heard any response.
“Sponsors are apparently allowed to simply pick their batch in a careful and, dare I say manipulative way, to gain the result they want. With a single batch study the selection of batch will absolutely determine the outcome of the study.”
In vitro bioequivalence studies are already required to use multiple batches, she noted.
This research was funded by Oriel Therapeutics, an indirect wholly-owned subsidiary of Novartis AG.
AT CHEST 2017
Key clinical point: The FDA’s standards for demonstrating pharmacokinetic bioequivalence between two inhaled products need to be revised to address batch to batch variability.
Major finding: Investigators found Advair Diskus 100/50 batches that were more than 30% different from each other.
Data source: Pharmacokinetic bioequivalence studies comparing batches of Advair Diskus 100/50 to each other, and to batches of the generic candidate OT329 Solis 100/50.
Disclosures: This research was funded by Oriel Therapeutics, an indirect wholly-owned subsidiary of Novartis AG. Dr. Burmeister Getz is director of clinical pharmacology at Oriel Therapeutics.

Omalizumab Helps Relieve Food Allergies
More than 80% of children who were given omalizumab with oral immunotherapy (OIT) for 36 weeks could safely consume portions of at least 2 foods they were causing an allergic reaction, according to findings from a phase 2 study funded by the National Institute of Allergy and Infectious Diseases. Omalizumab, an injectable antibody drug approved for moderate-to-severe allergic asthma, blocks the activity of IgE.
Researchers from Stanford University School of Medicine in California enrolled 48 children aged 4 years to 15 years with confirmed allergy to multiple foods, such as milk, egg, wheat, soy, sesame seeds, peanuts, and tree nuts. The children received omalizumab or placebo injections for the first 16 weeks. At week 8, all participants began eating small, gradually increasing amounts of an allergenic food. They continued OIT until week 36, when they underwent an oral food challenge.
Of the 36 children who received omalizumab, 30 were able to eat at least 2 grams of ≥ 2 allergenic foods, compared with that of only 4 of 12 children (33%) who received placebo. Children who received omalizumab also had fewer adverse events from OIT
More than 80% of children who were given omalizumab with oral immunotherapy (OIT) for 36 weeks could safely consume portions of at least 2 foods they were causing an allergic reaction, according to findings from a phase 2 study funded by the National Institute of Allergy and Infectious Diseases. Omalizumab, an injectable antibody drug approved for moderate-to-severe allergic asthma, blocks the activity of IgE.
Researchers from Stanford University School of Medicine in California enrolled 48 children aged 4 years to 15 years with confirmed allergy to multiple foods, such as milk, egg, wheat, soy, sesame seeds, peanuts, and tree nuts. The children received omalizumab or placebo injections for the first 16 weeks. At week 8, all participants began eating small, gradually increasing amounts of an allergenic food. They continued OIT until week 36, when they underwent an oral food challenge.
Of the 36 children who received omalizumab, 30 were able to eat at least 2 grams of ≥ 2 allergenic foods, compared with that of only 4 of 12 children (33%) who received placebo. Children who received omalizumab also had fewer adverse events from OIT
More than 80% of children who were given omalizumab with oral immunotherapy (OIT) for 36 weeks could safely consume portions of at least 2 foods they were causing an allergic reaction, according to findings from a phase 2 study funded by the National Institute of Allergy and Infectious Diseases. Omalizumab, an injectable antibody drug approved for moderate-to-severe allergic asthma, blocks the activity of IgE.
Researchers from Stanford University School of Medicine in California enrolled 48 children aged 4 years to 15 years with confirmed allergy to multiple foods, such as milk, egg, wheat, soy, sesame seeds, peanuts, and tree nuts. The children received omalizumab or placebo injections for the first 16 weeks. At week 8, all participants began eating small, gradually increasing amounts of an allergenic food. They continued OIT until week 36, when they underwent an oral food challenge.
Of the 36 children who received omalizumab, 30 were able to eat at least 2 grams of ≥ 2 allergenic foods, compared with that of only 4 of 12 children (33%) who received placebo. Children who received omalizumab also had fewer adverse events from OIT
Triple therapy ups response in refractory mantle cell lymphoma
A combination of ibrutinib, lenalidomide, and rituximab produced an overall response rate of 76% at 17.8 months median follow-up among 50 adults with relapsed or refractory mantle cell lymphoma, according to an open-label, single-arm, phase 2 trial.
There were complete responses in 28 patients (56%) and partial responses in 10 (20%). Median progression-free survival was 16 months and median overall survival was 22 months. Similar proportions of patients, with and without TP53 mutations, had overall and complete responses, suggesting that triple therapy might be particularly useful in patients with high-risk genetic features.
“Our results provide preliminary evidence that the triplet combination of ibrutinib, lenalidomide, and rituximab is an active regimen in patients with relapsed or refractory mantle cell lymphoma, and should be evaluated in a prospective randomized controlled trial,” wrote Mats Jerkeman, MD, of Lund University, Sweden, and colleagues. The report was published in The Lancet Haematology.
“Addition of lenalidomide to ibrutinib and rituximab might increase the proportion of patients who have complete remission ... Previous studies reported complete responses in 44% of patients on ibrutinib and rituximab, in 36% of patients on rituximab and lenalidomide, and in 19% of patients on ibrutinib alone,” they wrote.

Treatment was divided into an induction phase of 12 cycles of 28 days with all three drugs and a maintenance phase with ibrutinib and rituximab only, given until disease progression or unacceptable toxicity. All the patients had previously been treated with at least one rituximab-containing regimen.
Janssen and Celgene funded the work. Dr. Jerkeman reported ties to Janssen and Celgene, as well as AbbVie and Gilead.
SOURCE: Jerkeman M et al. Lancet Haematol. 2018 Jan 29. doi: 10.1016/S2352-3026(18)30018-8.
A combination of ibrutinib, lenalidomide, and rituximab produced an overall response rate of 76% at 17.8 months median follow-up among 50 adults with relapsed or refractory mantle cell lymphoma, according to an open-label, single-arm, phase 2 trial.
There were complete responses in 28 patients (56%) and partial responses in 10 (20%). Median progression-free survival was 16 months and median overall survival was 22 months. Similar proportions of patients, with and without TP53 mutations, had overall and complete responses, suggesting that triple therapy might be particularly useful in patients with high-risk genetic features.
“Our results provide preliminary evidence that the triplet combination of ibrutinib, lenalidomide, and rituximab is an active regimen in patients with relapsed or refractory mantle cell lymphoma, and should be evaluated in a prospective randomized controlled trial,” wrote Mats Jerkeman, MD, of Lund University, Sweden, and colleagues. The report was published in The Lancet Haematology.
“Addition of lenalidomide to ibrutinib and rituximab might increase the proportion of patients who have complete remission ... Previous studies reported complete responses in 44% of patients on ibrutinib and rituximab, in 36% of patients on rituximab and lenalidomide, and in 19% of patients on ibrutinib alone,” they wrote.
Treatment was divided into an induction phase of 12 cycles of 28 days with all three drugs and a maintenance phase with ibrutinib and rituximab only, given until disease progression or unacceptable toxicity. All the patients had previously been treated with at least one rituximab-containing regimen.
Janssen and Celgene funded the work. Dr. Jerkeman reported ties to Janssen and Celgene, as well as AbbVie and Gilead.
SOURCE: Jerkeman M et al. Lancet Haematol. 2018 Jan 29. doi: 10.1016/S2352-3026(18)30018-8.
A combination of ibrutinib, lenalidomide, and rituximab produced an overall response rate of 76% at 17.8 months median follow-up among 50 adults with relapsed or refractory mantle cell lymphoma, according to an open-label, single-arm, phase 2 trial.
There were complete responses in 28 patients (56%) and partial responses in 10 (20%). Median progression-free survival was 16 months and median overall survival was 22 months. Similar proportions of patients, with and without TP53 mutations, had overall and complete responses, suggesting that triple therapy might be particularly useful in patients with high-risk genetic features.
“Our results provide preliminary evidence that the triplet combination of ibrutinib, lenalidomide, and rituximab is an active regimen in patients with relapsed or refractory mantle cell lymphoma, and should be evaluated in a prospective randomized controlled trial,” wrote Mats Jerkeman, MD, of Lund University, Sweden, and colleagues. The report was published in The Lancet Haematology.
“Addition of lenalidomide to ibrutinib and rituximab might increase the proportion of patients who have complete remission ... Previous studies reported complete responses in 44% of patients on ibrutinib and rituximab, in 36% of patients on rituximab and lenalidomide, and in 19% of patients on ibrutinib alone,” they wrote.
Treatment was divided into an induction phase of 12 cycles of 28 days with all three drugs and a maintenance phase with ibrutinib and rituximab only, given until disease progression or unacceptable toxicity. All the patients had previously been treated with at least one rituximab-containing regimen.
Janssen and Celgene funded the work. Dr. Jerkeman reported ties to Janssen and Celgene, as well as AbbVie and Gilead.
SOURCE: Jerkeman M et al. Lancet Haematol. 2018 Jan 29. doi: 10.1016/S2352-3026(18)30018-8.
FROM THE LANCET HAEMATOLOGY
Key clinical point:
Major finding: The overall response from for the combination of the three drugs was 76% at 17.8 months median follow-up.
Study details: An open-label, single-arm, phase 2 trial of 50 adults with relapsed/refractory MCL.
Disclosures: Janssen and Celgene funded the work. Dr. Jerkeman reported ties to Janssen and Celgene, as well as AbbVie and Gilead.
Source: Jerkeman M et al. Lancet Haematol. 2018 Jan 29. doi: 10.1016/S2352-3026(18)30018-8.