User login
E-cigarette flavorings foster cardiovascular dysfunction
Flavored tobacco products are popular among current smokers, including youth, and the flavorings have been deemed ingestible, but their impact on heart health has not been studied, wrote Jennifer Fetterman, PhD, of Boston University, and her colleagues. The report was published in Arteriosclerosis, Thrombosis, and Vascular Biology.
The researchers studied nine types of flavorings used in alternative tobacco products to assess their impact on cardiovascular health.
The first part of the study comprised a population of nine nonsmokers, six nonmenthol cigarette smokers, and six menthol cigarette smokers without cardiovascular disease. The researchers isolated venous endothelial cells from each participant.
Overall, cells from both nonmenthol and menthol cigarette smokers had significantly lower nitric oxide production compared with nonsmokers (P = .003 and P = .012, respectively). In addition, the flavoring compounds menthol and eugenol impaired nitric oxide production in the cells of healthy individuals.
“Increased inflammation and a loss of nitric oxide are some of the first changes to occur leading up to cardiovascular disease and events like heart attacks and stroke, so they are considered early predictors of heart disease,” Dr. Fetterman said in a statement, adding that the “findings suggest that these flavoring additives may have serious health consequences.”
All nine flavorings induced cell death at the highest concentration tested, ranging from 10 to 100 mmol/L).
The study findings were limited by several factors, primarily a lack of data on how heating the flavorings in the in vitro part of the study might have affected toxicity in the body, the researchers noted.
“Future studies will focus on how the toxicity of the flavorings is altered with heating and characterization of the levels obtained in the circulation after use of an e-cigarette,” they said.
However, data support the need for regulation and limits on the level of flavorings used in e-cigarettes and other tobacco products, they emphasized.
“These findings suggest that flavoring compounds induce endothelial cell dysfunction in human cells similarly to the abnormal function in active cigarette smokers,” the researchers noted.
The study was funded by the National Heart, Lung, and Blood Institute; Food and Drug Administration Center for Tobacco Products; and the American Heart Association. The researchers had no financial conflicts to disclose.
SOURCE: Fetterman J et al. Arterioscler Thromb Vasc Biol. 2018. doi: 10.1161/ATVBAHA.118.311156.
Flavored tobacco products are popular among current smokers, including youth, and the flavorings have been deemed ingestible, but their impact on heart health has not been studied, wrote Jennifer Fetterman, PhD, of Boston University, and her colleagues. The report was published in Arteriosclerosis, Thrombosis, and Vascular Biology.
The researchers studied nine types of flavorings used in alternative tobacco products to assess their impact on cardiovascular health.
The first part of the study comprised a population of nine nonsmokers, six nonmenthol cigarette smokers, and six menthol cigarette smokers without cardiovascular disease. The researchers isolated venous endothelial cells from each participant.
Overall, cells from both nonmenthol and menthol cigarette smokers had significantly lower nitric oxide production compared with nonsmokers (P = .003 and P = .012, respectively). In addition, the flavoring compounds menthol and eugenol impaired nitric oxide production in the cells of healthy individuals.
“Increased inflammation and a loss of nitric oxide are some of the first changes to occur leading up to cardiovascular disease and events like heart attacks and stroke, so they are considered early predictors of heart disease,” Dr. Fetterman said in a statement, adding that the “findings suggest that these flavoring additives may have serious health consequences.”
All nine flavorings induced cell death at the highest concentration tested, ranging from 10 to 100 mmol/L).
The study findings were limited by several factors, primarily a lack of data on how heating the flavorings in the in vitro part of the study might have affected toxicity in the body, the researchers noted.
“Future studies will focus on how the toxicity of the flavorings is altered with heating and characterization of the levels obtained in the circulation after use of an e-cigarette,” they said.
However, data support the need for regulation and limits on the level of flavorings used in e-cigarettes and other tobacco products, they emphasized.
“These findings suggest that flavoring compounds induce endothelial cell dysfunction in human cells similarly to the abnormal function in active cigarette smokers,” the researchers noted.
The study was funded by the National Heart, Lung, and Blood Institute; Food and Drug Administration Center for Tobacco Products; and the American Heart Association. The researchers had no financial conflicts to disclose.
SOURCE: Fetterman J et al. Arterioscler Thromb Vasc Biol. 2018. doi: 10.1161/ATVBAHA.118.311156.
Flavored tobacco products are popular among current smokers, including youth, and the flavorings have been deemed ingestible, but their impact on heart health has not been studied, wrote Jennifer Fetterman, PhD, of Boston University, and her colleagues. The report was published in Arteriosclerosis, Thrombosis, and Vascular Biology.
The researchers studied nine types of flavorings used in alternative tobacco products to assess their impact on cardiovascular health.
The first part of the study comprised a population of nine nonsmokers, six nonmenthol cigarette smokers, and six menthol cigarette smokers without cardiovascular disease. The researchers isolated venous endothelial cells from each participant.
Overall, cells from both nonmenthol and menthol cigarette smokers had significantly lower nitric oxide production compared with nonsmokers (P = .003 and P = .012, respectively). In addition, the flavoring compounds menthol and eugenol impaired nitric oxide production in the cells of healthy individuals.
“Increased inflammation and a loss of nitric oxide are some of the first changes to occur leading up to cardiovascular disease and events like heart attacks and stroke, so they are considered early predictors of heart disease,” Dr. Fetterman said in a statement, adding that the “findings suggest that these flavoring additives may have serious health consequences.”
All nine flavorings induced cell death at the highest concentration tested, ranging from 10 to 100 mmol/L).
The study findings were limited by several factors, primarily a lack of data on how heating the flavorings in the in vitro part of the study might have affected toxicity in the body, the researchers noted.
“Future studies will focus on how the toxicity of the flavorings is altered with heating and characterization of the levels obtained in the circulation after use of an e-cigarette,” they said.
However, data support the need for regulation and limits on the level of flavorings used in e-cigarettes and other tobacco products, they emphasized.
“These findings suggest that flavoring compounds induce endothelial cell dysfunction in human cells similarly to the abnormal function in active cigarette smokers,” the researchers noted.
The study was funded by the National Heart, Lung, and Blood Institute; Food and Drug Administration Center for Tobacco Products; and the American Heart Association. The researchers had no financial conflicts to disclose.
SOURCE: Fetterman J et al. Arterioscler Thromb Vasc Biol. 2018. doi: 10.1161/ATVBAHA.118.311156.
FROM ARTERIOSCLEROSIS, THROMBOSIS, AND VASCULAR BIOLOGY
Key clinical point: Nitric oxide production was impaired in cells exposed to compounds used in alternative tobacco products.
Major finding: Nitric oxide products were significantly lower in nonmenthol and menthol cigarette smokers compared with nonsmokers (P = .003 and P = .012, respectively).
Study details: The data come from nine nonsmokers, six menthol cigarette smokers, and six nonmenthol cigarette smokers, plus in vitro cells.
Disclosures: The study was funded by the National Heart, Lung, and Blood Institute; Food and Drug Administration Center for Tobacco Products; and the American Heart Association. The researchers had no financial conflicts to disclose.
Source: Fetterman J et al. Arterioscler Thromb Vasc Biol. 2018. doi: 10.1161/ATVBAHA.118.311156.
Vaccine nonmedical exemptions creating metro ‘hotspots’
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.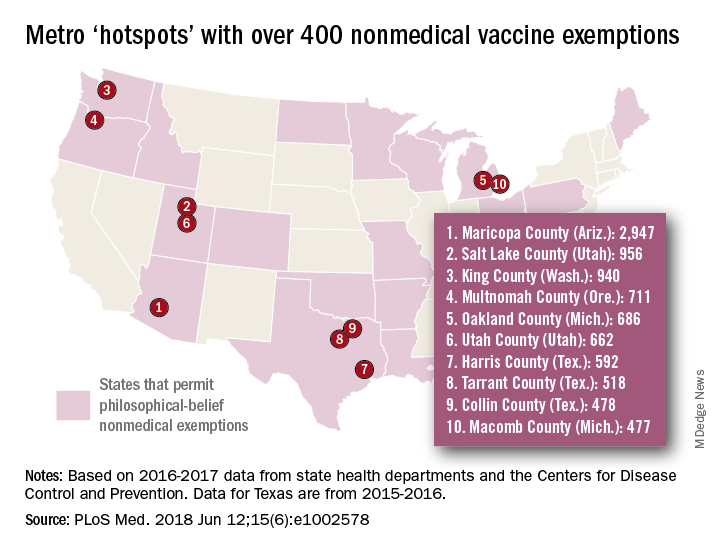
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
Recent increases in nonmedical exemptions (NMEs) to vaccination have created metropolitan “hotspots” with large numbers of unvaccinated children, according to a report published June 12 in PLoS Medicine.
although rates seem to have plateaued in some states since 2014. As a result of those increases, there were, during the 2016-2017 school year, 15 metro areas with kindergarten NME populations over 400, reported Jacqueline K. Olive, and her associates at Baylor College of Medicine. Their report was based on data from state health departments and the Centers for Disease Control and Prevention.
Leading the way was Maricopa County, Ariz., home of Phoenix and 2,947 unvaccinated kindergartners, which was more than triple the number in county/city No. 2, Salt Lake County/Salt Lake City (NME total: 956). Close behind in third was King County, Wash. (Seattle) at 940, followed by Multnomah County, Ore. (Portland) at 711 and Oakland County, Mich. (Troy) at 686, the investigators said.
[There was only room for 10 in the map, so here are hotspots 11-15: Wayne County, Mich. (Detroit); Allegheny County, Pa. (Pittsburgh); Travis County, Tex. (Austin); Jackson County, Mo. (Kansas City); and Spokane County, Wash. (Spokane).]
In addition to the large-population hotspots, there are also a number of mainly rural counties with smaller populations but high NME rates. Eight of the 10 highest such rates can be found in Idaho, and at the top of that list is Camas County, which had an NME rate of 27% in 2016-2017, the researchers reported.
Analysis of the relationship between NMEs and MMR vaccination showed that “states with more NME students exhibited lower MMR vaccination rates. In contrast, states that have banned NMEs – Mississippi, California, and West Virginia – exhibit the highest MMR vaccine uptake and lowest incidence of vaccine preventable diseases,” the investigators wrote.
Ms. Olive and her associates said that there was no specific funding for the study and that no conflicts of interest existed.
SOURCE: Olive JK et al. PLoS Med. 2018 Jun 12;15(6): e1002578. doi: 10.1371/journal.pmed.1002578.
FROM PLOS MEDICINE
More Smoke-Free Campuses, Not Enough Screening and Counseling
People with mental and/or substance abuse disorders are more than twice as likely to smoke cigarettes as people without those disorders, and are more likely to die of a smoking-related illness than from a behavioral health condition. Yet many people are not screened for tobacco use in behavioral health facilities. According to the Centers for Disease Control and Prevention (CDC) and Substance Abuse and Mental Health Services Administration (SAMHSA), in 2016, only half of mental health treatment facilities and 64% of substance abuse treatment facilities reported screening patients for tobacco use.
Even fewer facilities provide counseling and treatments. Only 38% of mental health facilities offer tobacco cessation counseling, 25% offer nicotine replacement therapy (NRT), and 22% offer non-nicotine cessation medications. Of substance abuse treatment facilities, 47% offer tobacco cessation counseling, 26% offer NRT, and 20% offer non-nicotine cessation medications. Oklahoma and New York had the highest percentage of programs.
On the other hand, 49% of mental health and 33% of substance abuse treatment facilities now have smoke-free campuses in the 50 states, Washington DC, and Puerto Rico. That number varies by state, ranging from 20% of mental health facilities in Idaho to 78% in Oklahoma, and 10% of substance abuse treatment facilities in Idaho to 83% in New York.
Practical steps can boost the availability of smoking cessation screening and programs. The CDC recommends integrating screening and treatment protocols into workflows and electronic health record systems. The CDC also advises providing outreach to behavioral health providers who reinforce the message that patients can benefit from evidence-based cessation treatment.
The report is based on data from the 2016 National Mental Health Services Survey and the 2016 National Survey of Substance Abuse Treatment Services.
People with mental and/or substance abuse disorders are more than twice as likely to smoke cigarettes as people without those disorders, and are more likely to die of a smoking-related illness than from a behavioral health condition. Yet many people are not screened for tobacco use in behavioral health facilities. According to the Centers for Disease Control and Prevention (CDC) and Substance Abuse and Mental Health Services Administration (SAMHSA), in 2016, only half of mental health treatment facilities and 64% of substance abuse treatment facilities reported screening patients for tobacco use.
Even fewer facilities provide counseling and treatments. Only 38% of mental health facilities offer tobacco cessation counseling, 25% offer nicotine replacement therapy (NRT), and 22% offer non-nicotine cessation medications. Of substance abuse treatment facilities, 47% offer tobacco cessation counseling, 26% offer NRT, and 20% offer non-nicotine cessation medications. Oklahoma and New York had the highest percentage of programs.
On the other hand, 49% of mental health and 33% of substance abuse treatment facilities now have smoke-free campuses in the 50 states, Washington DC, and Puerto Rico. That number varies by state, ranging from 20% of mental health facilities in Idaho to 78% in Oklahoma, and 10% of substance abuse treatment facilities in Idaho to 83% in New York.
Practical steps can boost the availability of smoking cessation screening and programs. The CDC recommends integrating screening and treatment protocols into workflows and electronic health record systems. The CDC also advises providing outreach to behavioral health providers who reinforce the message that patients can benefit from evidence-based cessation treatment.
The report is based on data from the 2016 National Mental Health Services Survey and the 2016 National Survey of Substance Abuse Treatment Services.
People with mental and/or substance abuse disorders are more than twice as likely to smoke cigarettes as people without those disorders, and are more likely to die of a smoking-related illness than from a behavioral health condition. Yet many people are not screened for tobacco use in behavioral health facilities. According to the Centers for Disease Control and Prevention (CDC) and Substance Abuse and Mental Health Services Administration (SAMHSA), in 2016, only half of mental health treatment facilities and 64% of substance abuse treatment facilities reported screening patients for tobacco use.
Even fewer facilities provide counseling and treatments. Only 38% of mental health facilities offer tobacco cessation counseling, 25% offer nicotine replacement therapy (NRT), and 22% offer non-nicotine cessation medications. Of substance abuse treatment facilities, 47% offer tobacco cessation counseling, 26% offer NRT, and 20% offer non-nicotine cessation medications. Oklahoma and New York had the highest percentage of programs.
On the other hand, 49% of mental health and 33% of substance abuse treatment facilities now have smoke-free campuses in the 50 states, Washington DC, and Puerto Rico. That number varies by state, ranging from 20% of mental health facilities in Idaho to 78% in Oklahoma, and 10% of substance abuse treatment facilities in Idaho to 83% in New York.
Practical steps can boost the availability of smoking cessation screening and programs. The CDC recommends integrating screening and treatment protocols into workflows and electronic health record systems. The CDC also advises providing outreach to behavioral health providers who reinforce the message that patients can benefit from evidence-based cessation treatment.
The report is based on data from the 2016 National Mental Health Services Survey and the 2016 National Survey of Substance Abuse Treatment Services.
Hepatitis A Outbreak in a Childcare Facility
In young children, hepatitis A is usually asymptomatic. So a childcare facility (CCF) in Ireland surprised by an outbreak of hepatitis A that infected 7 adults and 5 children, hospitalizing 6 of the adults. By the time the investigation and interventions were over, > 554 contacts had been followed up, and it had all cost > €45,000 ($53,000).
The outbreak was traced to a man with hepatitis A whose child had been unwell for 3 weeks with fever, fatigue, abdominal pain, diarrhea, pale stools, and possible jaundice. The child (and an infected cousin) attended a local CCF but because several other cases seemed to be limited to the family and their friends, no one immediately considered the CCF as a possible source of infection. However, approximately 10 days after the first 2 cases were reported, an outbreak was officially declared.
At the time, 93 children were attending the CCF. All 7 adults were household contacts of children in the CCF. None of the 23-member CCF staff developed symptoms of hepatitis A.
As many as 70% of infections are asymptomatic in children under age 6, the researchers note, but that group is often a source of transmission due to suboptimal hygiene. Transmission is usually fecal-oral and person-to-person. Although the initial source of outbreak was not identified, the subsequent transmission suggested person-to-person spread. The researchers say the distribution of cases suggests that the transmission probably happened in the school, with asymptomatic children infecting their families, highlighting the fact that symptomatic cases of hepatitis A only represent a portion of the cases in an outbreak.
A preschool inspection report that preceded the outbreak highlighted deficiencies in the staff’s handwashing practices. An infection control audit undertaken because of the outbreak found a number of deficits, including lack of foot-operated bins and the use of cloth covers on furnishings rather than waterproof material. Medical expenses, including hospitalization, serology, and vaccine, cost between €43,400 - €47, 400 ($51,000 - $56,000).
The researchers say the delayed notification to public health of the first case probably contributed to the extent of the outbreak. Medical professionals, they note, should be aware that although uncommon, hepatitis A still occurs. Prompt recognition and notification can mitigate the significant morbidity associated with the infection.
Source:
O'Connor L, McGovern E, O'Meara M, et al. Epidemiol Infect. 2018;146(6):705-711.
In young children, hepatitis A is usually asymptomatic. So a childcare facility (CCF) in Ireland surprised by an outbreak of hepatitis A that infected 7 adults and 5 children, hospitalizing 6 of the adults. By the time the investigation and interventions were over, > 554 contacts had been followed up, and it had all cost > €45,000 ($53,000).
The outbreak was traced to a man with hepatitis A whose child had been unwell for 3 weeks with fever, fatigue, abdominal pain, diarrhea, pale stools, and possible jaundice. The child (and an infected cousin) attended a local CCF but because several other cases seemed to be limited to the family and their friends, no one immediately considered the CCF as a possible source of infection. However, approximately 10 days after the first 2 cases were reported, an outbreak was officially declared.
At the time, 93 children were attending the CCF. All 7 adults were household contacts of children in the CCF. None of the 23-member CCF staff developed symptoms of hepatitis A.
As many as 70% of infections are asymptomatic in children under age 6, the researchers note, but that group is often a source of transmission due to suboptimal hygiene. Transmission is usually fecal-oral and person-to-person. Although the initial source of outbreak was not identified, the subsequent transmission suggested person-to-person spread. The researchers say the distribution of cases suggests that the transmission probably happened in the school, with asymptomatic children infecting their families, highlighting the fact that symptomatic cases of hepatitis A only represent a portion of the cases in an outbreak.
A preschool inspection report that preceded the outbreak highlighted deficiencies in the staff’s handwashing practices. An infection control audit undertaken because of the outbreak found a number of deficits, including lack of foot-operated bins and the use of cloth covers on furnishings rather than waterproof material. Medical expenses, including hospitalization, serology, and vaccine, cost between €43,400 - €47, 400 ($51,000 - $56,000).
The researchers say the delayed notification to public health of the first case probably contributed to the extent of the outbreak. Medical professionals, they note, should be aware that although uncommon, hepatitis A still occurs. Prompt recognition and notification can mitigate the significant morbidity associated with the infection.
Source:
O'Connor L, McGovern E, O'Meara M, et al. Epidemiol Infect. 2018;146(6):705-711.
In young children, hepatitis A is usually asymptomatic. So a childcare facility (CCF) in Ireland surprised by an outbreak of hepatitis A that infected 7 adults and 5 children, hospitalizing 6 of the adults. By the time the investigation and interventions were over, > 554 contacts had been followed up, and it had all cost > €45,000 ($53,000).
The outbreak was traced to a man with hepatitis A whose child had been unwell for 3 weeks with fever, fatigue, abdominal pain, diarrhea, pale stools, and possible jaundice. The child (and an infected cousin) attended a local CCF but because several other cases seemed to be limited to the family and their friends, no one immediately considered the CCF as a possible source of infection. However, approximately 10 days after the first 2 cases were reported, an outbreak was officially declared.
At the time, 93 children were attending the CCF. All 7 adults were household contacts of children in the CCF. None of the 23-member CCF staff developed symptoms of hepatitis A.
As many as 70% of infections are asymptomatic in children under age 6, the researchers note, but that group is often a source of transmission due to suboptimal hygiene. Transmission is usually fecal-oral and person-to-person. Although the initial source of outbreak was not identified, the subsequent transmission suggested person-to-person spread. The researchers say the distribution of cases suggests that the transmission probably happened in the school, with asymptomatic children infecting their families, highlighting the fact that symptomatic cases of hepatitis A only represent a portion of the cases in an outbreak.
A preschool inspection report that preceded the outbreak highlighted deficiencies in the staff’s handwashing practices. An infection control audit undertaken because of the outbreak found a number of deficits, including lack of foot-operated bins and the use of cloth covers on furnishings rather than waterproof material. Medical expenses, including hospitalization, serology, and vaccine, cost between €43,400 - €47, 400 ($51,000 - $56,000).
The researchers say the delayed notification to public health of the first case probably contributed to the extent of the outbreak. Medical professionals, they note, should be aware that although uncommon, hepatitis A still occurs. Prompt recognition and notification can mitigate the significant morbidity associated with the infection.
Source:
O'Connor L, McGovern E, O'Meara M, et al. Epidemiol Infect. 2018;146(6):705-711.
Aclidinium bromide for COPD: No impact on MACE
SAN DIEGO – The use of aclidinium bromide 400 mcg b.i.d. did not increase the risk of major adverse cardiac events or mortality in patients with moderate to very severe , compared with placebo.

Those are two key findings from the ASCENT COPD trial presented by Robert A. Wise, MD, at an international conference of the American Thoracic Society. “Cardiovascular risk factors and comorbidities are prevalent in patients with COPD, and about 30% of COPD patients die of cardiovascular disease,” said Dr. Wise, who serves as director of research for the division of pulmonary and critical care medicine at the Johns Hopkins University School of Medicine, Baltimore. “However, patients who have cardiovascular disease are often excluded from, or not enrolled in, COPD clinical trials. Moreover, there has been controversy as to whether or not treatment with a long-acting muscarinic antagonist is associated with an increased risk of cardiovascular events. That’s been seen in randomized trials, meta-analyses, as well as in observational studies.”
Aclidinium bromide 400 mcg b.i.d., administered by the Pressair inhaler, is approved as a maintenance treatment for patients with COPD. However, during the registration studies, there were not an adequate number of cardiovascular events in order to ascertain clearly whether or not the drug was associated with increased risk, Dr. Wise said. Therefore, he and his associates in the ASCENT COPD study set out to assess the long-term cardiovascular safety profile of aclidinium 400 mcg b.i.d. in patients with moderate to very severe COPD at risk of major adverse cardiovascular events (MACE) for up to 3 years (Chronic Obstr Pulm Dis. 2018;5[1]:5-15). For the randomized, placebo-controlled, parallel-group study, patients received treatment with aclidinium bromide or a placebo inhaler of similar appearance. The study was designed to be terminated when at least 122 patients experienced an adjudicated MACE. The primary safety endpoint was time to first MACE during follow-up of up to 3 years, while the primary efficacy endpoint was the rate of moderate to severe exacerbations per patient per year during the first year of treatment.
To be included in the study, patients had to be at least 40 years of age with moderate to very severe stable COPD, have a smoking history of at least 10 pack-years, and have at least one of the following significant risk factors: cerebrovascular disease; coronary artery disease; peripheral vascular disease, or history of claudication; or at least two atherothrombotic risk factors (male at least 65 years of age, female at least 70 years of age; waist circumference of at least 40 inches among males or at least 38 inches among females; an estimated glomerular filtration rate of less than 60 mL/min and microalbuminuria; dyslipidemia; or hypertension).
The researchers randomized 1,791 patients to the aclidinium group and 1,798 to the placebo group. Their mean age was 67 years, and about 60% of patients had an exacerbation in the preceding year. Nearly two-thirds of patients (63%) were receiving concomitant long-acting beta 2-agonists (LABA) or LABA/inhaled corticosteroid therapy. In addition, 44% of patients entered the study with a history of a prior cardiovascular event plus at least two atherothrombotic risk factors, 52% reported at least two atherothrombotic risk factors without any prior cardiovascular events, and 4% had a history of a prior cardiovascular event only.
Dr. Wise reported that aclidinium did not increase the risk of MACE in patients with moderate to very severe COPD with significant cardiovascular risk factors, compared with placebo (hazard ratio 0.89; P = .469); non-inferiority was concluded as the upper bound of the 95% confidence interval was less than 1.8). In terms of all-cause mortality, aclidinium did not increase the risk of death, compared with placebo (HR 0.99; P = .929).
During the first year of treatment, Dr. Wise and his associates also observed a 22% reduction in COPD exacerbation rate for aclidinium vs. placebo groups (HR 0.44 vs. 0.57, respectively; P less than .001), and a 35% reduction in the rate of COPD exacerbations leading to hospitalizations (HR 0.07 vs. 0.10; P = .006). “The reduction in exacerbation risk was similar, whether or not patients had an exacerbation in the past year,” Dr. Wise said. He reported being a consultant to, and receiving research support from, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and ContraFect.
dbrunk@mdedge.com
SOURCE: Wise, R., et al., Abstract 7711, ATS 2018.
SAN DIEGO – The use of aclidinium bromide 400 mcg b.i.d. did not increase the risk of major adverse cardiac events or mortality in patients with moderate to very severe , compared with placebo.
Those are two key findings from the ASCENT COPD trial presented by Robert A. Wise, MD, at an international conference of the American Thoracic Society. “Cardiovascular risk factors and comorbidities are prevalent in patients with COPD, and about 30% of COPD patients die of cardiovascular disease,” said Dr. Wise, who serves as director of research for the division of pulmonary and critical care medicine at the Johns Hopkins University School of Medicine, Baltimore. “However, patients who have cardiovascular disease are often excluded from, or not enrolled in, COPD clinical trials. Moreover, there has been controversy as to whether or not treatment with a long-acting muscarinic antagonist is associated with an increased risk of cardiovascular events. That’s been seen in randomized trials, meta-analyses, as well as in observational studies.”
Aclidinium bromide 400 mcg b.i.d., administered by the Pressair inhaler, is approved as a maintenance treatment for patients with COPD. However, during the registration studies, there were not an adequate number of cardiovascular events in order to ascertain clearly whether or not the drug was associated with increased risk, Dr. Wise said. Therefore, he and his associates in the ASCENT COPD study set out to assess the long-term cardiovascular safety profile of aclidinium 400 mcg b.i.d. in patients with moderate to very severe COPD at risk of major adverse cardiovascular events (MACE) for up to 3 years (Chronic Obstr Pulm Dis. 2018;5[1]:5-15). For the randomized, placebo-controlled, parallel-group study, patients received treatment with aclidinium bromide or a placebo inhaler of similar appearance. The study was designed to be terminated when at least 122 patients experienced an adjudicated MACE. The primary safety endpoint was time to first MACE during follow-up of up to 3 years, while the primary efficacy endpoint was the rate of moderate to severe exacerbations per patient per year during the first year of treatment.
To be included in the study, patients had to be at least 40 years of age with moderate to very severe stable COPD, have a smoking history of at least 10 pack-years, and have at least one of the following significant risk factors: cerebrovascular disease; coronary artery disease; peripheral vascular disease, or history of claudication; or at least two atherothrombotic risk factors (male at least 65 years of age, female at least 70 years of age; waist circumference of at least 40 inches among males or at least 38 inches among females; an estimated glomerular filtration rate of less than 60 mL/min and microalbuminuria; dyslipidemia; or hypertension).
The researchers randomized 1,791 patients to the aclidinium group and 1,798 to the placebo group. Their mean age was 67 years, and about 60% of patients had an exacerbation in the preceding year. Nearly two-thirds of patients (63%) were receiving concomitant long-acting beta 2-agonists (LABA) or LABA/inhaled corticosteroid therapy. In addition, 44% of patients entered the study with a history of a prior cardiovascular event plus at least two atherothrombotic risk factors, 52% reported at least two atherothrombotic risk factors without any prior cardiovascular events, and 4% had a history of a prior cardiovascular event only.
Dr. Wise reported that aclidinium did not increase the risk of MACE in patients with moderate to very severe COPD with significant cardiovascular risk factors, compared with placebo (hazard ratio 0.89; P = .469); non-inferiority was concluded as the upper bound of the 95% confidence interval was less than 1.8). In terms of all-cause mortality, aclidinium did not increase the risk of death, compared with placebo (HR 0.99; P = .929).
During the first year of treatment, Dr. Wise and his associates also observed a 22% reduction in COPD exacerbation rate for aclidinium vs. placebo groups (HR 0.44 vs. 0.57, respectively; P less than .001), and a 35% reduction in the rate of COPD exacerbations leading to hospitalizations (HR 0.07 vs. 0.10; P = .006). “The reduction in exacerbation risk was similar, whether or not patients had an exacerbation in the past year,” Dr. Wise said. He reported being a consultant to, and receiving research support from, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and ContraFect.
dbrunk@mdedge.com
SOURCE: Wise, R., et al., Abstract 7711, ATS 2018.
SAN DIEGO – The use of aclidinium bromide 400 mcg b.i.d. did not increase the risk of major adverse cardiac events or mortality in patients with moderate to very severe , compared with placebo.
Those are two key findings from the ASCENT COPD trial presented by Robert A. Wise, MD, at an international conference of the American Thoracic Society. “Cardiovascular risk factors and comorbidities are prevalent in patients with COPD, and about 30% of COPD patients die of cardiovascular disease,” said Dr. Wise, who serves as director of research for the division of pulmonary and critical care medicine at the Johns Hopkins University School of Medicine, Baltimore. “However, patients who have cardiovascular disease are often excluded from, or not enrolled in, COPD clinical trials. Moreover, there has been controversy as to whether or not treatment with a long-acting muscarinic antagonist is associated with an increased risk of cardiovascular events. That’s been seen in randomized trials, meta-analyses, as well as in observational studies.”
Aclidinium bromide 400 mcg b.i.d., administered by the Pressair inhaler, is approved as a maintenance treatment for patients with COPD. However, during the registration studies, there were not an adequate number of cardiovascular events in order to ascertain clearly whether or not the drug was associated with increased risk, Dr. Wise said. Therefore, he and his associates in the ASCENT COPD study set out to assess the long-term cardiovascular safety profile of aclidinium 400 mcg b.i.d. in patients with moderate to very severe COPD at risk of major adverse cardiovascular events (MACE) for up to 3 years (Chronic Obstr Pulm Dis. 2018;5[1]:5-15). For the randomized, placebo-controlled, parallel-group study, patients received treatment with aclidinium bromide or a placebo inhaler of similar appearance. The study was designed to be terminated when at least 122 patients experienced an adjudicated MACE. The primary safety endpoint was time to first MACE during follow-up of up to 3 years, while the primary efficacy endpoint was the rate of moderate to severe exacerbations per patient per year during the first year of treatment.
To be included in the study, patients had to be at least 40 years of age with moderate to very severe stable COPD, have a smoking history of at least 10 pack-years, and have at least one of the following significant risk factors: cerebrovascular disease; coronary artery disease; peripheral vascular disease, or history of claudication; or at least two atherothrombotic risk factors (male at least 65 years of age, female at least 70 years of age; waist circumference of at least 40 inches among males or at least 38 inches among females; an estimated glomerular filtration rate of less than 60 mL/min and microalbuminuria; dyslipidemia; or hypertension).
The researchers randomized 1,791 patients to the aclidinium group and 1,798 to the placebo group. Their mean age was 67 years, and about 60% of patients had an exacerbation in the preceding year. Nearly two-thirds of patients (63%) were receiving concomitant long-acting beta 2-agonists (LABA) or LABA/inhaled corticosteroid therapy. In addition, 44% of patients entered the study with a history of a prior cardiovascular event plus at least two atherothrombotic risk factors, 52% reported at least two atherothrombotic risk factors without any prior cardiovascular events, and 4% had a history of a prior cardiovascular event only.
Dr. Wise reported that aclidinium did not increase the risk of MACE in patients with moderate to very severe COPD with significant cardiovascular risk factors, compared with placebo (hazard ratio 0.89; P = .469); non-inferiority was concluded as the upper bound of the 95% confidence interval was less than 1.8). In terms of all-cause mortality, aclidinium did not increase the risk of death, compared with placebo (HR 0.99; P = .929).
During the first year of treatment, Dr. Wise and his associates also observed a 22% reduction in COPD exacerbation rate for aclidinium vs. placebo groups (HR 0.44 vs. 0.57, respectively; P less than .001), and a 35% reduction in the rate of COPD exacerbations leading to hospitalizations (HR 0.07 vs. 0.10; P = .006). “The reduction in exacerbation risk was similar, whether or not patients had an exacerbation in the past year,” Dr. Wise said. He reported being a consultant to, and receiving research support from, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and ContraFect.
dbrunk@mdedge.com
SOURCE: Wise, R., et al., Abstract 7711, ATS 2018.
AT ATS 2018
Key clinical point: Researchers found no increased risk of MACE in at-risk patients with COPD receiving aclidinium.
Major finding: MACE risk and mortality in COPD patients with significant cardiovascular risk given aclidinium bromide had a hazard ratio 0.89 (P = .469), compared to placebo.
Study details: A randomized, placebo-controlled, parallel-group study of 3,589 patients with moderate to very severe COPD at risk of major adverse cardiovascular events.
Disclosures: Dr. Wise reported being a consultant to, and receiving research support from, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and ContraFect.
Source: Wise, R. et al, ATS 2018, Abstract 7711.
Education sessions upped COPD patients’ knowledge of their disease
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
FROM CHEST
Key clinical point: Two 30-minute education sessions improved patients’ disease-specific knowledge for an acute exacerbation of COPD.
Major finding: Mean change on the Bristol COPD Knowledge Questionnaire (BCKQ) was 8 points for the educational intervention, and 3.4 for controls.
Study details: A pilot randomized controlled trial of 31 patients admitted to a community hospital.
Disclosures: Authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
Source: Janaudis-Ferreira T, et al. Chest 2018 Jun 4.
The IHS Helps Youth Transition Safely Back to the Community
When young people successfully complete an Indian Health Service (IHS) Youth Regional Treatment Center (YRTC) program, they often leave the structured environment to return to a community and family that cannot provide them with the necessary aftercare. The IHS has launched the YRTC Aftercare Pilot Project to fill that gap.
The 12 federal and tribal YRTCs provide a range of clinical services “rooted in culturally relevant, holistic models of care” to American Indian and Alaska Native (AI/AN) adolescents who abuse alcohol or drugs. But without aftercare and case management, the young people are at risk for falling back into old ways.
The YRTC project will identify transitional services that can be culturally adapted to meet the needs of AI/AN youth to support resiliency and coping skills and provide support systems. The project developers aim to establish community-based approaches to reduce relapse and encourage reintegration.
The IHS has awarded $1.62 million for YRTC Aftercare Pilot Projects to Healing Lodge of the Seven Nations in Spokane Valley, Washington, and Desert Sage Youth Wellness Center in Hemet, California. The awards are for 3 years. Both sites will develop innovative, collaborative strategies to improve the health of Native youth as they transition back to their communities.
When young people successfully complete an Indian Health Service (IHS) Youth Regional Treatment Center (YRTC) program, they often leave the structured environment to return to a community and family that cannot provide them with the necessary aftercare. The IHS has launched the YRTC Aftercare Pilot Project to fill that gap.
The 12 federal and tribal YRTCs provide a range of clinical services “rooted in culturally relevant, holistic models of care” to American Indian and Alaska Native (AI/AN) adolescents who abuse alcohol or drugs. But without aftercare and case management, the young people are at risk for falling back into old ways.
The YRTC project will identify transitional services that can be culturally adapted to meet the needs of AI/AN youth to support resiliency and coping skills and provide support systems. The project developers aim to establish community-based approaches to reduce relapse and encourage reintegration.
The IHS has awarded $1.62 million for YRTC Aftercare Pilot Projects to Healing Lodge of the Seven Nations in Spokane Valley, Washington, and Desert Sage Youth Wellness Center in Hemet, California. The awards are for 3 years. Both sites will develop innovative, collaborative strategies to improve the health of Native youth as they transition back to their communities.
When young people successfully complete an Indian Health Service (IHS) Youth Regional Treatment Center (YRTC) program, they often leave the structured environment to return to a community and family that cannot provide them with the necessary aftercare. The IHS has launched the YRTC Aftercare Pilot Project to fill that gap.
The 12 federal and tribal YRTCs provide a range of clinical services “rooted in culturally relevant, holistic models of care” to American Indian and Alaska Native (AI/AN) adolescents who abuse alcohol or drugs. But without aftercare and case management, the young people are at risk for falling back into old ways.
The YRTC project will identify transitional services that can be culturally adapted to meet the needs of AI/AN youth to support resiliency and coping skills and provide support systems. The project developers aim to establish community-based approaches to reduce relapse and encourage reintegration.
The IHS has awarded $1.62 million for YRTC Aftercare Pilot Projects to Healing Lodge of the Seven Nations in Spokane Valley, Washington, and Desert Sage Youth Wellness Center in Hemet, California. The awards are for 3 years. Both sites will develop innovative, collaborative strategies to improve the health of Native youth as they transition back to their communities.
FDA grants regular approval to venetoclax for CLL/SLL
Venetoclax (Venclexta) has received regular approval from the Food and Drug Administration for the treatment of patients with chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), with or without 17p deletion, who have received at least one prior therapy.
The approval was based results from the MURANO trial of 389 patients, which was a randomized, multicenter, open-label trial of venetoclax plus rituximab versus bendamustine plus rituximab.
Neutropenia, diarrhea, upper respiratory tract infection, fatigue, cough, and nausea were the most common adverse events seen in the venetoclax arm. Grade 3 or 4 neutropenia developed in 64% of those patients, and grade 4 in 31%. The most common infection in venetoclax patients was pneumonia, but overall, 21% of patients in that arm experienced some kind of infection.
Because of the rapid reduction in tumor size, tumor lysis syndrome is possible with venetoclax treatment, the FDA noted.
In 2016, the FDA granted accelerated approval to venetoclax for treatment of patients with CLL with 17d deletion who had received at least one prior line of therapy.
Venetoclax (Venclexta) has received regular approval from the Food and Drug Administration for the treatment of patients with chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), with or without 17p deletion, who have received at least one prior therapy.
The approval was based results from the MURANO trial of 389 patients, which was a randomized, multicenter, open-label trial of venetoclax plus rituximab versus bendamustine plus rituximab.
Neutropenia, diarrhea, upper respiratory tract infection, fatigue, cough, and nausea were the most common adverse events seen in the venetoclax arm. Grade 3 or 4 neutropenia developed in 64% of those patients, and grade 4 in 31%. The most common infection in venetoclax patients was pneumonia, but overall, 21% of patients in that arm experienced some kind of infection.
Because of the rapid reduction in tumor size, tumor lysis syndrome is possible with venetoclax treatment, the FDA noted.
In 2016, the FDA granted accelerated approval to venetoclax for treatment of patients with CLL with 17d deletion who had received at least one prior line of therapy.
Venetoclax (Venclexta) has received regular approval from the Food and Drug Administration for the treatment of patients with chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), with or without 17p deletion, who have received at least one prior therapy.
The approval was based results from the MURANO trial of 389 patients, which was a randomized, multicenter, open-label trial of venetoclax plus rituximab versus bendamustine plus rituximab.
Neutropenia, diarrhea, upper respiratory tract infection, fatigue, cough, and nausea were the most common adverse events seen in the venetoclax arm. Grade 3 or 4 neutropenia developed in 64% of those patients, and grade 4 in 31%. The most common infection in venetoclax patients was pneumonia, but overall, 21% of patients in that arm experienced some kind of infection.
Because of the rapid reduction in tumor size, tumor lysis syndrome is possible with venetoclax treatment, the FDA noted.
In 2016, the FDA granted accelerated approval to venetoclax for treatment of patients with CLL with 17d deletion who had received at least one prior line of therapy.
Sleep apnea treatment may not prevent sleepiness
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.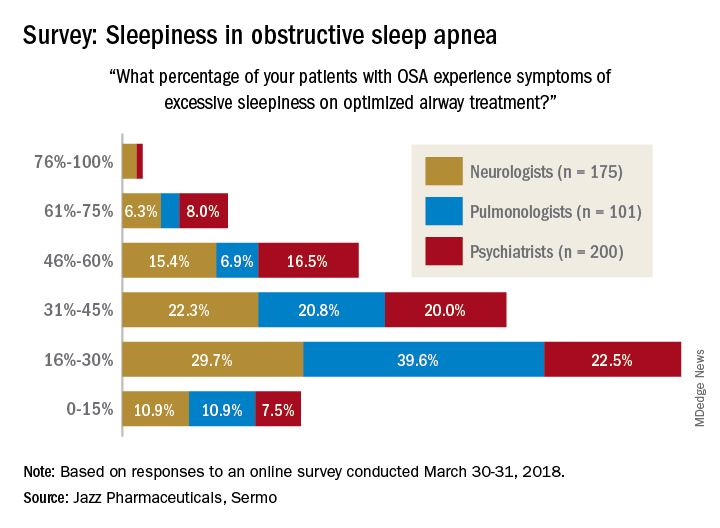
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Youth tobacco use shows ‘promising declines’
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
according to the Centers for Disease Control and Prevention.
The prevalence of current tobacco use – defined as use on 1 or more days in the past 30 days – among high schoolers fell from 24.2% in 2011 to 19.6% in 2017, and middle school use decreased from 7.5% to 5.6% over that same time. That means the number of youth tobacco users went from almost 4.6 million in 2011 to slightly more than 3.6 million in 2017, Teresa W. Wang, PhD, and her associates said in the Morbidity and Mortality Weekly Report.
Almost half (47%) of the high school students who used tobacco in 2017 used two or more products, as did two out of five (42%) middle schoolers. That year, black high school students were less likely to use any tobacco product (14.2%) than were whites (22.7%) and Hispanics (16.7%). E-cigarettes were the most popular form of tobacco among white and Hispanic high schoolers, while cigars were the most commonly used form among blacks, they reported based on data from the National Youth Tobacco Surveys, which had sample sizes of 18,766 in 2011 and 17,872 in 2017.
“Despite promising declines in tobacco use, far too many young people continue to use tobacco products, including e-cigarettes,” CDC Director Robert R. Redfield, MD, said in a written statement accompanying the report. “Comprehensive, sustained strategies can help prevent and reduce tobacco use and protect our nation’s youth from this preventable health risk.”
In a separate statement, FDA Commissioner Scott Gottlieb, MD, said, “We are working hard to develop a pathway to put products like e-cigarettes through an appropriate series of regulatory gates to properly evaluate them as an alternative for adults who still want to get access to satisfying levels of nicotine, without all the risks associated with lighting tobacco on fire. And we will continue to encourage the development of potentially less harmful forms of nicotine delivery for currently addicted adult smokers. … But these public health opportunities are put at risk if all we do is hook another generation of kids on nicotine and tobacco products through alternatives like e-cigarettes.”
SOURCE: Wang TW et al. MMWR. 2018;67(22):629-33.
FROM MMWR