User login
Could High BMI Reduce Premenopausal Breast Cancer Risk?
Young women may not want to hear it, but fat could be their friend. Researchers from the Premenopausal Breast Cancer Collaborative Group have found that women aged 18 – 24 years with high body fat have a lower risk of developing breast cancer before menopause.
The researchers pooled data from 19 different studies, involving about 800,000 women from around the world. Overall, 1.7% of the women developed breast cancer. The researchers found that the relative risk of premenopausal breast cancer dropped 12% to 23% for each 5-unit increase in body mass index, depending on age. They saw the strongest effect at ages 18 – 24 years: Very obese women in this age group were 4.2 times less likely to develop premenopausal breast cancer than women with low body mass index (BMI) at the same age.
The researchers do not know why high BMI might protect against breast cancer in some women. Breast cancer is relatively rare before menopause, although previous studies have suggested that the risk factors might be different for younger vs older women, says Dale Sandler, PhD, co-author of the group and head of the Epidemiology Branch at the National Institute of Environmental Health Sciences. For instance, it is well known that women who gain weight, particularly after menopause, have a higher risk. The fact that this study found that the risk not only is not increased, but actually decreased, in younger women points to the possibility that different biologic mechanisms are at work, Sandler says.
Nonetheless, the researchers caution that young women should not intentionally gain weight to offset the risk.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-associates-obesity-lower-breast-cancer-risk-young-women. Published June 27, 2018. Accessed July 18, 2018.
Young women may not want to hear it, but fat could be their friend. Researchers from the Premenopausal Breast Cancer Collaborative Group have found that women aged 18 – 24 years with high body fat have a lower risk of developing breast cancer before menopause.
The researchers pooled data from 19 different studies, involving about 800,000 women from around the world. Overall, 1.7% of the women developed breast cancer. The researchers found that the relative risk of premenopausal breast cancer dropped 12% to 23% for each 5-unit increase in body mass index, depending on age. They saw the strongest effect at ages 18 – 24 years: Very obese women in this age group were 4.2 times less likely to develop premenopausal breast cancer than women with low body mass index (BMI) at the same age.
The researchers do not know why high BMI might protect against breast cancer in some women. Breast cancer is relatively rare before menopause, although previous studies have suggested that the risk factors might be different for younger vs older women, says Dale Sandler, PhD, co-author of the group and head of the Epidemiology Branch at the National Institute of Environmental Health Sciences. For instance, it is well known that women who gain weight, particularly after menopause, have a higher risk. The fact that this study found that the risk not only is not increased, but actually decreased, in younger women points to the possibility that different biologic mechanisms are at work, Sandler says.
Nonetheless, the researchers caution that young women should not intentionally gain weight to offset the risk.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-associates-obesity-lower-breast-cancer-risk-young-women. Published June 27, 2018. Accessed July 18, 2018.
Young women may not want to hear it, but fat could be their friend. Researchers from the Premenopausal Breast Cancer Collaborative Group have found that women aged 18 – 24 years with high body fat have a lower risk of developing breast cancer before menopause.
The researchers pooled data from 19 different studies, involving about 800,000 women from around the world. Overall, 1.7% of the women developed breast cancer. The researchers found that the relative risk of premenopausal breast cancer dropped 12% to 23% for each 5-unit increase in body mass index, depending on age. They saw the strongest effect at ages 18 – 24 years: Very obese women in this age group were 4.2 times less likely to develop premenopausal breast cancer than women with low body mass index (BMI) at the same age.
The researchers do not know why high BMI might protect against breast cancer in some women. Breast cancer is relatively rare before menopause, although previous studies have suggested that the risk factors might be different for younger vs older women, says Dale Sandler, PhD, co-author of the group and head of the Epidemiology Branch at the National Institute of Environmental Health Sciences. For instance, it is well known that women who gain weight, particularly after menopause, have a higher risk. The fact that this study found that the risk not only is not increased, but actually decreased, in younger women points to the possibility that different biologic mechanisms are at work, Sandler says.
Nonetheless, the researchers caution that young women should not intentionally gain weight to offset the risk.
Source:
National Institutes of Health. https://www.nih.gov/news-events/news-releases/nih-study-associates-obesity-lower-breast-cancer-risk-young-women. Published June 27, 2018. Accessed July 18, 2018.
Bug Bites More Than Just a Nuisance
As if it were not bad enough that illnesses from mosquito, tick, and flea bites tripled between 2004 and 2016, 9 new germs spread by mosquitoes and ticks were discovered or introduced into the US in the same 13 years.
According to the CDC’s first summary collectively examining data trends for all nationally notifiable diseases caused by the bite of an infected mosquito, tick, or flea, the most common tickborne diseases in 2016 were Lyme disease and ehrlichiosis/anaplasmosis. The most common mosquito-borne viruses were West Nile, dengue, and Zika.
The increase is due to many factors, the CDC says, but 1 issue is that mosquitoes and ticks are moving into new areas, putting more people at risk. The US is “not fully prepared” to meet the public health threat, the CDC warns: About 80% of vector control organizations lack critical prevention and control capacities. Reducing the spread of the diseases and responding effectively to outbreaks will require additional capacity at the state and local levels for tracking, diagnosing, and reporting cases.
As if it were not bad enough that illnesses from mosquito, tick, and flea bites tripled between 2004 and 2016, 9 new germs spread by mosquitoes and ticks were discovered or introduced into the US in the same 13 years.
According to the CDC’s first summary collectively examining data trends for all nationally notifiable diseases caused by the bite of an infected mosquito, tick, or flea, the most common tickborne diseases in 2016 were Lyme disease and ehrlichiosis/anaplasmosis. The most common mosquito-borne viruses were West Nile, dengue, and Zika.
The increase is due to many factors, the CDC says, but 1 issue is that mosquitoes and ticks are moving into new areas, putting more people at risk. The US is “not fully prepared” to meet the public health threat, the CDC warns: About 80% of vector control organizations lack critical prevention and control capacities. Reducing the spread of the diseases and responding effectively to outbreaks will require additional capacity at the state and local levels for tracking, diagnosing, and reporting cases.
As if it were not bad enough that illnesses from mosquito, tick, and flea bites tripled between 2004 and 2016, 9 new germs spread by mosquitoes and ticks were discovered or introduced into the US in the same 13 years.
According to the CDC’s first summary collectively examining data trends for all nationally notifiable diseases caused by the bite of an infected mosquito, tick, or flea, the most common tickborne diseases in 2016 were Lyme disease and ehrlichiosis/anaplasmosis. The most common mosquito-borne viruses were West Nile, dengue, and Zika.
The increase is due to many factors, the CDC says, but 1 issue is that mosquitoes and ticks are moving into new areas, putting more people at risk. The US is “not fully prepared” to meet the public health threat, the CDC warns: About 80% of vector control organizations lack critical prevention and control capacities. Reducing the spread of the diseases and responding effectively to outbreaks will require additional capacity at the state and local levels for tracking, diagnosing, and reporting cases.
Later diagnosis predicts poorer outcomes in adult-diagnosed cystic fibrosis
Older age at diagnosis, diabetes, and poorer lung function are all , new research suggests.
A growing number of people with cystic fibrosis are diagnosed in adulthood, partly because of increased awareness among physicians of variations in disease presentation, more accessible genotyping, and easier diagnostic criteria.
Adult-diagnosed cystic fibrosis patients generally have a milder form of the disease than that of those diagnosed in childhood; however, less is known about their prognosis and life expectancy.
Researchers reported the outcomes of a retrospective cohort study of 362 adults diagnosed with cystic fibrosis at age 18 years or older. The median age at diagnosis was 34.3 years, and 71% of patients presented with pulmonary and/or gastrointestinal symptoms. The study was published in Annals of the American Thoracic Society.
The patients were followed for a median of 7.7 years, during which time there were 15 lung transplants and 33 deaths without transplant. Overall, 10-year lung transplant–free survival was 87.7%, and 15-year survival was 86.1%.
Those who were diagnosed young and who had higher lung function had the best median survival times. For each 5-year increase in age at diagnosis, the risk of death or transplant increased by 24%, and for each 5% decrease in forced expiratory volume in one second (FEV1), the risk was 35% higher.
Individuals who had diabetes at baseline had a more than fourfold higher risk of death or transplant than did those without diabetes.
“While newborn screening programs will reduce the rate of missed diagnoses in the future, clinicians still need to consider CF as a possible diagnosis if individuals are presenting with suspicious CF symptoms (e.g. GI or pulmonary symptoms) during adulthood, particularly if born prior to the introduction of newborn screening in their jurisdiction,” wrote Sameer Desai, of the University of British Columbia, Vancouver, and his coauthors.
Commenting on the association with diabetes, the authors noted that this finding had some uncertainty but suggested the additional inflammatory burden could increase the risk of death in individuals with cystic fibrosis.
The authors highlighted that fewer than 5% of people with adult-diagnosed cystic fibrosis had two copies of the F508del mutation, which is associated with severe, early-onset disease. However, those who were homozygous for that mutation tended to be diagnosed at a younger adult age, had worse nutritional status and a lower FEV1 percent predicted, compared with the overall adult-diagnosed population.
“This finding suggests potential delays in CF diagnosis for these people leading to worse outcomes,” the authors wrote.
The researchers also identified 25 individuals who had a possible unconfirmed diagnosis based on the most recent cystic fibrosis diagnostic guidelines. These individuals were either asymptomatic or had unknown symptoms, had sweat chlorides at or below 60 mmol/L (where available), and either unknown or two non–cystic fibrosis–causing mutations. They were also more likely to be male, to be nonwhite, to have increased unknown mutations, and to be pancreatic sufficient, compared with individuals with a confirmed diagnosis.
The study looked at whether Pseudomonas aeruginosa and Burkholderia cepacia complex increased the risk of transplant or death, but found these did not significantly predict survival.
“Adult CF clinicians can use this information to educate newly diagnosed adults with CF about their prognosis and to guide treatment decisions, specifically those at high-risk for a worse prognosis,” the authors wrote.
The study was partly funded by the Rare Disease Foundation. Two authors declared support from Cystic Fibrosis Canada, but no other conflicts of interest were declared.
SOURCE: Desai A et al. Ann Am Thorac Soc. 2018 Jun 26. doi: 10.1513/AnnalsATS.201801-037OC.
Older age at diagnosis, diabetes, and poorer lung function are all , new research suggests.
A growing number of people with cystic fibrosis are diagnosed in adulthood, partly because of increased awareness among physicians of variations in disease presentation, more accessible genotyping, and easier diagnostic criteria.
Adult-diagnosed cystic fibrosis patients generally have a milder form of the disease than that of those diagnosed in childhood; however, less is known about their prognosis and life expectancy.
Researchers reported the outcomes of a retrospective cohort study of 362 adults diagnosed with cystic fibrosis at age 18 years or older. The median age at diagnosis was 34.3 years, and 71% of patients presented with pulmonary and/or gastrointestinal symptoms. The study was published in Annals of the American Thoracic Society.
The patients were followed for a median of 7.7 years, during which time there were 15 lung transplants and 33 deaths without transplant. Overall, 10-year lung transplant–free survival was 87.7%, and 15-year survival was 86.1%.
Those who were diagnosed young and who had higher lung function had the best median survival times. For each 5-year increase in age at diagnosis, the risk of death or transplant increased by 24%, and for each 5% decrease in forced expiratory volume in one second (FEV1), the risk was 35% higher.
Individuals who had diabetes at baseline had a more than fourfold higher risk of death or transplant than did those without diabetes.
“While newborn screening programs will reduce the rate of missed diagnoses in the future, clinicians still need to consider CF as a possible diagnosis if individuals are presenting with suspicious CF symptoms (e.g. GI or pulmonary symptoms) during adulthood, particularly if born prior to the introduction of newborn screening in their jurisdiction,” wrote Sameer Desai, of the University of British Columbia, Vancouver, and his coauthors.
Commenting on the association with diabetes, the authors noted that this finding had some uncertainty but suggested the additional inflammatory burden could increase the risk of death in individuals with cystic fibrosis.
The authors highlighted that fewer than 5% of people with adult-diagnosed cystic fibrosis had two copies of the F508del mutation, which is associated with severe, early-onset disease. However, those who were homozygous for that mutation tended to be diagnosed at a younger adult age, had worse nutritional status and a lower FEV1 percent predicted, compared with the overall adult-diagnosed population.
“This finding suggests potential delays in CF diagnosis for these people leading to worse outcomes,” the authors wrote.
The researchers also identified 25 individuals who had a possible unconfirmed diagnosis based on the most recent cystic fibrosis diagnostic guidelines. These individuals were either asymptomatic or had unknown symptoms, had sweat chlorides at or below 60 mmol/L (where available), and either unknown or two non–cystic fibrosis–causing mutations. They were also more likely to be male, to be nonwhite, to have increased unknown mutations, and to be pancreatic sufficient, compared with individuals with a confirmed diagnosis.
The study looked at whether Pseudomonas aeruginosa and Burkholderia cepacia complex increased the risk of transplant or death, but found these did not significantly predict survival.
“Adult CF clinicians can use this information to educate newly diagnosed adults with CF about their prognosis and to guide treatment decisions, specifically those at high-risk for a worse prognosis,” the authors wrote.
The study was partly funded by the Rare Disease Foundation. Two authors declared support from Cystic Fibrosis Canada, but no other conflicts of interest were declared.
SOURCE: Desai A et al. Ann Am Thorac Soc. 2018 Jun 26. doi: 10.1513/AnnalsATS.201801-037OC.
Older age at diagnosis, diabetes, and poorer lung function are all , new research suggests.
A growing number of people with cystic fibrosis are diagnosed in adulthood, partly because of increased awareness among physicians of variations in disease presentation, more accessible genotyping, and easier diagnostic criteria.
Adult-diagnosed cystic fibrosis patients generally have a milder form of the disease than that of those diagnosed in childhood; however, less is known about their prognosis and life expectancy.
Researchers reported the outcomes of a retrospective cohort study of 362 adults diagnosed with cystic fibrosis at age 18 years or older. The median age at diagnosis was 34.3 years, and 71% of patients presented with pulmonary and/or gastrointestinal symptoms. The study was published in Annals of the American Thoracic Society.
The patients were followed for a median of 7.7 years, during which time there were 15 lung transplants and 33 deaths without transplant. Overall, 10-year lung transplant–free survival was 87.7%, and 15-year survival was 86.1%.
Those who were diagnosed young and who had higher lung function had the best median survival times. For each 5-year increase in age at diagnosis, the risk of death or transplant increased by 24%, and for each 5% decrease in forced expiratory volume in one second (FEV1), the risk was 35% higher.
Individuals who had diabetes at baseline had a more than fourfold higher risk of death or transplant than did those without diabetes.
“While newborn screening programs will reduce the rate of missed diagnoses in the future, clinicians still need to consider CF as a possible diagnosis if individuals are presenting with suspicious CF symptoms (e.g. GI or pulmonary symptoms) during adulthood, particularly if born prior to the introduction of newborn screening in their jurisdiction,” wrote Sameer Desai, of the University of British Columbia, Vancouver, and his coauthors.
Commenting on the association with diabetes, the authors noted that this finding had some uncertainty but suggested the additional inflammatory burden could increase the risk of death in individuals with cystic fibrosis.
The authors highlighted that fewer than 5% of people with adult-diagnosed cystic fibrosis had two copies of the F508del mutation, which is associated with severe, early-onset disease. However, those who were homozygous for that mutation tended to be diagnosed at a younger adult age, had worse nutritional status and a lower FEV1 percent predicted, compared with the overall adult-diagnosed population.
“This finding suggests potential delays in CF diagnosis for these people leading to worse outcomes,” the authors wrote.
The researchers also identified 25 individuals who had a possible unconfirmed diagnosis based on the most recent cystic fibrosis diagnostic guidelines. These individuals were either asymptomatic or had unknown symptoms, had sweat chlorides at or below 60 mmol/L (where available), and either unknown or two non–cystic fibrosis–causing mutations. They were also more likely to be male, to be nonwhite, to have increased unknown mutations, and to be pancreatic sufficient, compared with individuals with a confirmed diagnosis.
The study looked at whether Pseudomonas aeruginosa and Burkholderia cepacia complex increased the risk of transplant or death, but found these did not significantly predict survival.
“Adult CF clinicians can use this information to educate newly diagnosed adults with CF about their prognosis and to guide treatment decisions, specifically those at high-risk for a worse prognosis,” the authors wrote.
The study was partly funded by the Rare Disease Foundation. Two authors declared support from Cystic Fibrosis Canada, but no other conflicts of interest were declared.
SOURCE: Desai A et al. Ann Am Thorac Soc. 2018 Jun 26. doi: 10.1513/AnnalsATS.201801-037OC.
FROM ANNALS OF THE AMERICAN THORACIC SOCIETY
Key clinical point: Older age at diagnosis is a risk factor for death or transplant in adult-diagnosed cystic fibrosis.
Major finding: The risk of death or transplant increases by 24% per 5-year increase in age at diagnosis in adult-diagnosed cystic fibrosis.
Study details: A retrospective cohort study of 362 adults diagnosed with cystic fibrosis.
Disclosures: The study was partly funded by The Rare Disease Foundation. Two authors declared support from Cystic Fibrosis Canada, but no other conflicts of interest were declared.
Source: Desai A et al. Ann Am Thorac Soc. 2018 Jun 26. doi: 10.1513/AnnalsATS.201801-037OC.
Are We Beating Cancer—Finally?
Cancer death rates continue to decline in the US in all major racial and ethnic groups, according to the National Cancer Institute’s (NCI) latest Annual Report to the Nation on the Status of Cancer. The data are an “encouraging indicator of progress” in cancer research, says NCI Director Ned Sharpless, MD. “It’s clear that interventions are having an impact.”
Overall incidence, or rates of new cancers, dropped by 1.8% in men and 1.4% in women from 1999 to 2015. Between 2011 and 2015, death rates dropped for 11 of the 18 most common cancer types in men and 14 of the 20 most common types in women. The researchers say the “significant declines” also hold “significant differences” in rate by sex, race, and ethnicity. For example, black men and white women had the highest incidence rates, and black men and black women had the highest death rates.
However, over the same period, death rates for cancers of the liver, pancreas, and brain and nervous system rose in both men and women. Death rates for cancer of the uterus rose (the researchers say obesity is thought to be a contributing factor) and death rates for cancers of the oral cavity and pharynx and soft tissue increased in men, perhaps associated with human papillomavirus infection.
In a companion study, when researchers explored prostate cancer trends in more detail they found overall prostate cancer incidence rates declined an average of 6.5% each year between 2007 and 2014, from 163 new cases per 100,000 men to 104 new cases. Still, after a 2-decade steady decline, rates leveled off. Incidence of distant disease rose from 7.8 new cases per 100,000 to 9.2, but there was no increase in the rates of cases with aggressive histologic grade.
Interestingly, the researchers also report a decline in recent prostate-specific antigen screening between 2010 and 2013 national surveys. “The increase in late-stage disease and the flattening of the mortality trended occurred contemporaneously with the observed decrease in PSA screening,” said Serban Negoita, MD, DrPH, of NCI’s Surveillance Research Program. However, while “suggestive,” Negoita adds, their observation does not demonstrate causality: many factors contribute to incidence and mortality, such as improvements in staging and treating cancer.
Cancer death rates continue to decline in the US in all major racial and ethnic groups, according to the National Cancer Institute’s (NCI) latest Annual Report to the Nation on the Status of Cancer. The data are an “encouraging indicator of progress” in cancer research, says NCI Director Ned Sharpless, MD. “It’s clear that interventions are having an impact.”
Overall incidence, or rates of new cancers, dropped by 1.8% in men and 1.4% in women from 1999 to 2015. Between 2011 and 2015, death rates dropped for 11 of the 18 most common cancer types in men and 14 of the 20 most common types in women. The researchers say the “significant declines” also hold “significant differences” in rate by sex, race, and ethnicity. For example, black men and white women had the highest incidence rates, and black men and black women had the highest death rates.
However, over the same period, death rates for cancers of the liver, pancreas, and brain and nervous system rose in both men and women. Death rates for cancer of the uterus rose (the researchers say obesity is thought to be a contributing factor) and death rates for cancers of the oral cavity and pharynx and soft tissue increased in men, perhaps associated with human papillomavirus infection.
In a companion study, when researchers explored prostate cancer trends in more detail they found overall prostate cancer incidence rates declined an average of 6.5% each year between 2007 and 2014, from 163 new cases per 100,000 men to 104 new cases. Still, after a 2-decade steady decline, rates leveled off. Incidence of distant disease rose from 7.8 new cases per 100,000 to 9.2, but there was no increase in the rates of cases with aggressive histologic grade.
Interestingly, the researchers also report a decline in recent prostate-specific antigen screening between 2010 and 2013 national surveys. “The increase in late-stage disease and the flattening of the mortality trended occurred contemporaneously with the observed decrease in PSA screening,” said Serban Negoita, MD, DrPH, of NCI’s Surveillance Research Program. However, while “suggestive,” Negoita adds, their observation does not demonstrate causality: many factors contribute to incidence and mortality, such as improvements in staging and treating cancer.
Cancer death rates continue to decline in the US in all major racial and ethnic groups, according to the National Cancer Institute’s (NCI) latest Annual Report to the Nation on the Status of Cancer. The data are an “encouraging indicator of progress” in cancer research, says NCI Director Ned Sharpless, MD. “It’s clear that interventions are having an impact.”
Overall incidence, or rates of new cancers, dropped by 1.8% in men and 1.4% in women from 1999 to 2015. Between 2011 and 2015, death rates dropped for 11 of the 18 most common cancer types in men and 14 of the 20 most common types in women. The researchers say the “significant declines” also hold “significant differences” in rate by sex, race, and ethnicity. For example, black men and white women had the highest incidence rates, and black men and black women had the highest death rates.
However, over the same period, death rates for cancers of the liver, pancreas, and brain and nervous system rose in both men and women. Death rates for cancer of the uterus rose (the researchers say obesity is thought to be a contributing factor) and death rates for cancers of the oral cavity and pharynx and soft tissue increased in men, perhaps associated with human papillomavirus infection.
In a companion study, when researchers explored prostate cancer trends in more detail they found overall prostate cancer incidence rates declined an average of 6.5% each year between 2007 and 2014, from 163 new cases per 100,000 men to 104 new cases. Still, after a 2-decade steady decline, rates leveled off. Incidence of distant disease rose from 7.8 new cases per 100,000 to 9.2, but there was no increase in the rates of cases with aggressive histologic grade.
Interestingly, the researchers also report a decline in recent prostate-specific antigen screening between 2010 and 2013 national surveys. “The increase in late-stage disease and the flattening of the mortality trended occurred contemporaneously with the observed decrease in PSA screening,” said Serban Negoita, MD, DrPH, of NCI’s Surveillance Research Program. However, while “suggestive,” Negoita adds, their observation does not demonstrate causality: many factors contribute to incidence and mortality, such as improvements in staging and treating cancer.
Suicide Federal Health Data Trends (FULL)
Although rates of suicide have been increasing across the U.S., active-duty service members and veterans’ suicides have outpaced civilian rates. For many years, the military and VA struggled to quantify the number of suicides, but increasingly the DoD and VA have developed better reporting systems and have compiled more data to have a better understanding of this public health crisis.
For its 2016 report, VA examined more than 55 million records from 1979 to 2014 from all 50 states and 4 territories from veterans both inside and outside the VA health system. “Nothing is more important to me than making sure that we don’t lose any veterans to suicide,” VA Secretary David J. Shulkin, MD, said at a June 5, 2017, press conference. “As you know, 20 veterans a day are dying by suicide. That should be unacceptable to all of us. This is a national public health crisis, and it requires solutions that not only VA will work on but all of government and other partnerships in the private sector, nonprofit organizations.”
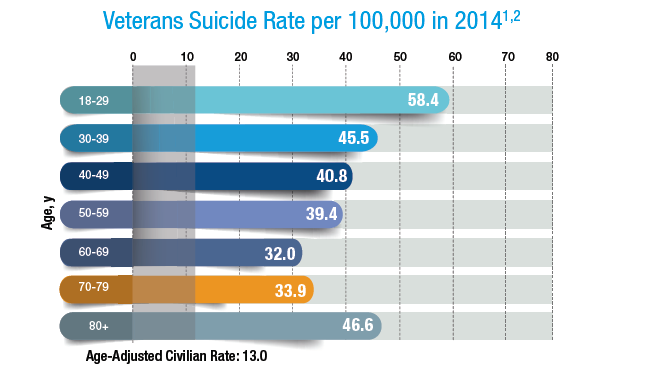
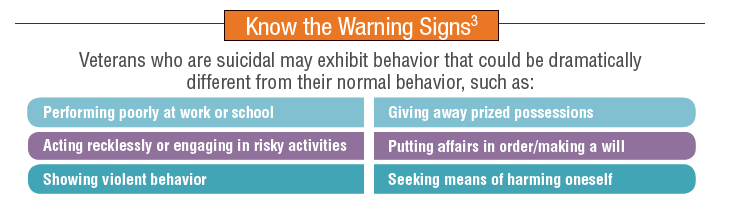
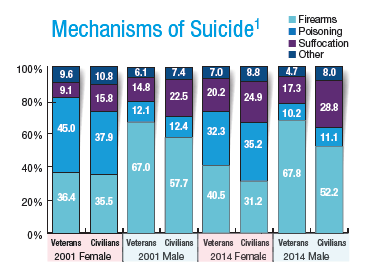
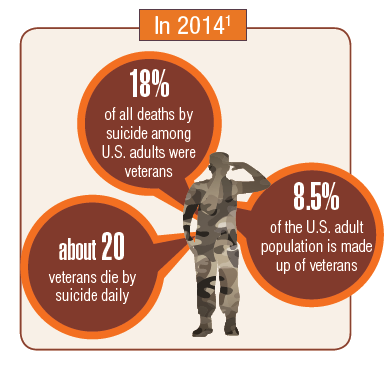
Much of the data from the VA report are startling. An average of 20 veterans die by suicide each day, and 14 of those veterans did not access VA health care services. Despite being just 8.5% of the U.S. population, veterans account for 18% of all deaths by suicide. In 2014, about 67% of all veteran deaths by suicide were the result of firearm injuries. Suicide impacts just about every veteran demographic: 65% of all veterans who died by suicide were aged 50 years or older. Women veterans were 2.4 times more likely to die by suicide than were nonveteran women.
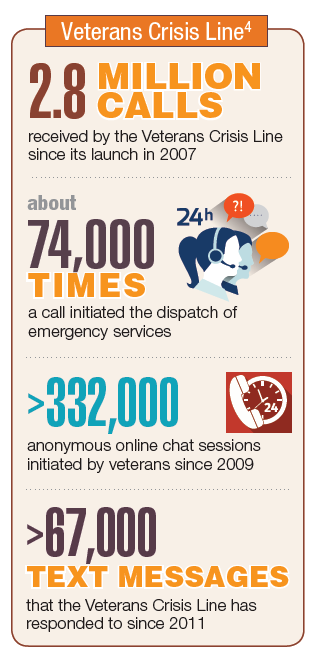
In response, the VA has refocused its efforts in a number of directions. Secretary Shulkin has announced that veterans with other-than-honorable discharges will now be permitted to access VA mental health services. Since its launch in 2007, The Veterans Crisis Line has answered nearly 3 million calls.
Click here to read the digital edition.
Although rates of suicide have been increasing across the U.S., active-duty service members and veterans’ suicides have outpaced civilian rates. For many years, the military and VA struggled to quantify the number of suicides, but increasingly the DoD and VA have developed better reporting systems and have compiled more data to have a better understanding of this public health crisis.
For its 2016 report, VA examined more than 55 million records from 1979 to 2014 from all 50 states and 4 territories from veterans both inside and outside the VA health system. “Nothing is more important to me than making sure that we don’t lose any veterans to suicide,” VA Secretary David J. Shulkin, MD, said at a June 5, 2017, press conference. “As you know, 20 veterans a day are dying by suicide. That should be unacceptable to all of us. This is a national public health crisis, and it requires solutions that not only VA will work on but all of government and other partnerships in the private sector, nonprofit organizations.”
Much of the data from the VA report are startling. An average of 20 veterans die by suicide each day, and 14 of those veterans did not access VA health care services. Despite being just 8.5% of the U.S. population, veterans account for 18% of all deaths by suicide. In 2014, about 67% of all veteran deaths by suicide were the result of firearm injuries. Suicide impacts just about every veteran demographic: 65% of all veterans who died by suicide were aged 50 years or older. Women veterans were 2.4 times more likely to die by suicide than were nonveteran women.
In response, the VA has refocused its efforts in a number of directions. Secretary Shulkin has announced that veterans with other-than-honorable discharges will now be permitted to access VA mental health services. Since its launch in 2007, The Veterans Crisis Line has answered nearly 3 million calls.
Click here to read the digital edition.
Although rates of suicide have been increasing across the U.S., active-duty service members and veterans’ suicides have outpaced civilian rates. For many years, the military and VA struggled to quantify the number of suicides, but increasingly the DoD and VA have developed better reporting systems and have compiled more data to have a better understanding of this public health crisis.
For its 2016 report, VA examined more than 55 million records from 1979 to 2014 from all 50 states and 4 territories from veterans both inside and outside the VA health system. “Nothing is more important to me than making sure that we don’t lose any veterans to suicide,” VA Secretary David J. Shulkin, MD, said at a June 5, 2017, press conference. “As you know, 20 veterans a day are dying by suicide. That should be unacceptable to all of us. This is a national public health crisis, and it requires solutions that not only VA will work on but all of government and other partnerships in the private sector, nonprofit organizations.”
Much of the data from the VA report are startling. An average of 20 veterans die by suicide each day, and 14 of those veterans did not access VA health care services. Despite being just 8.5% of the U.S. population, veterans account for 18% of all deaths by suicide. In 2014, about 67% of all veteran deaths by suicide were the result of firearm injuries. Suicide impacts just about every veteran demographic: 65% of all veterans who died by suicide were aged 50 years or older. Women veterans were 2.4 times more likely to die by suicide than were nonveteran women.
In response, the VA has refocused its efforts in a number of directions. Secretary Shulkin has announced that veterans with other-than-honorable discharges will now be permitted to access VA mental health services. Since its launch in 2007, The Veterans Crisis Line has answered nearly 3 million calls.
Click here to read the digital edition.
Chronic Pain Federal Health Data Trends (FULL)
Chronic pain is a major public health problem that affects more than 100 million people in the U.S. and is even more prevalent among active-duty service members and veterans. According to the National Institutes of Health, the prevalence of persistent pain is expected to rise in the near future, as the incidence of associated diseases (including diabetes mellitus, obesity, cardiovascular disorders, arthritis, and cancer) increases in the aging U.S. population.
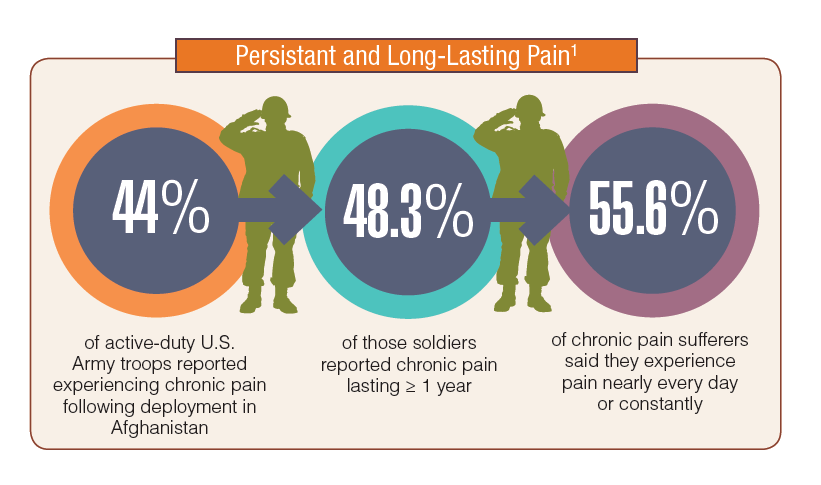
Perhaps no other health care problem is more persistent and more vexing than pain for the VA and DoD health care systems. Close to half of the soldiers who served in Afghanistan and nearly two-thirds of veterans reported chronic pain. Headaches and severe pain in the jaw, neck, and back are the most commonly reported locations. Veterans were far more likely than nonveterans were to experience severe pain in each of those locations.
Both the VA and DoD have recognized the dangers posed by high-levels of opioid prescriptions. While only 23% of veterans reported using opioid prescriptions for managing their chronic pain, the VA and DoD have actively sought to reduce the morphine equivalent daily doses for patients on opioids or to eliminate the prescriptions altogether. Through Centers of Excellence, such as the Defense & Veterans Center for Integrative Pain Management, the DoD and VA also have explored alternatives to opioids for pain management. In addition, the VA has used shared medical appointments and conjoint sessions with pharmacists and health psychologists to find alternative treatments and to educate patients about the dangers of opioid therapies for chronic pain.



Click here to read the digital edition.
Chronic pain is a major public health problem that affects more than 100 million people in the U.S. and is even more prevalent among active-duty service members and veterans. According to the National Institutes of Health, the prevalence of persistent pain is expected to rise in the near future, as the incidence of associated diseases (including diabetes mellitus, obesity, cardiovascular disorders, arthritis, and cancer) increases in the aging U.S. population.
Perhaps no other health care problem is more persistent and more vexing than pain for the VA and DoD health care systems. Close to half of the soldiers who served in Afghanistan and nearly two-thirds of veterans reported chronic pain. Headaches and severe pain in the jaw, neck, and back are the most commonly reported locations. Veterans were far more likely than nonveterans were to experience severe pain in each of those locations.
Both the VA and DoD have recognized the dangers posed by high-levels of opioid prescriptions. While only 23% of veterans reported using opioid prescriptions for managing their chronic pain, the VA and DoD have actively sought to reduce the morphine equivalent daily doses for patients on opioids or to eliminate the prescriptions altogether. Through Centers of Excellence, such as the Defense & Veterans Center for Integrative Pain Management, the DoD and VA also have explored alternatives to opioids for pain management. In addition, the VA has used shared medical appointments and conjoint sessions with pharmacists and health psychologists to find alternative treatments and to educate patients about the dangers of opioid therapies for chronic pain.
Click here to read the digital edition.
Chronic pain is a major public health problem that affects more than 100 million people in the U.S. and is even more prevalent among active-duty service members and veterans. According to the National Institutes of Health, the prevalence of persistent pain is expected to rise in the near future, as the incidence of associated diseases (including diabetes mellitus, obesity, cardiovascular disorders, arthritis, and cancer) increases in the aging U.S. population.
Perhaps no other health care problem is more persistent and more vexing than pain for the VA and DoD health care systems. Close to half of the soldiers who served in Afghanistan and nearly two-thirds of veterans reported chronic pain. Headaches and severe pain in the jaw, neck, and back are the most commonly reported locations. Veterans were far more likely than nonveterans were to experience severe pain in each of those locations.
Both the VA and DoD have recognized the dangers posed by high-levels of opioid prescriptions. While only 23% of veterans reported using opioid prescriptions for managing their chronic pain, the VA and DoD have actively sought to reduce the morphine equivalent daily doses for patients on opioids or to eliminate the prescriptions altogether. Through Centers of Excellence, such as the Defense & Veterans Center for Integrative Pain Management, the DoD and VA also have explored alternatives to opioids for pain management. In addition, the VA has used shared medical appointments and conjoint sessions with pharmacists and health psychologists to find alternative treatments and to educate patients about the dangers of opioid therapies for chronic pain.
Click here to read the digital edition.
Sleep Disorder Federal Health Data Trends (FULL)
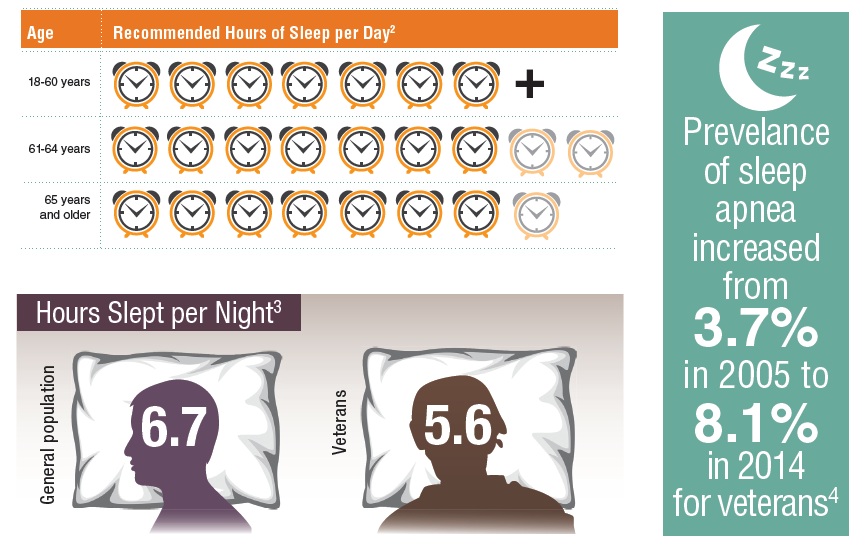
Sleep is an essential need, and insufficient sleep is associated with a wide range of adverse outcomes. Service members are especially at risk for acquiring sleep disorders due in part to the sometimes austere living conditions and the irregularity of active-duty sleep/wake schedules. For both active-duty service members and veterans, posttraumatic stress disorder or other mental health diagnoses can further exacerbate poor sleep hygiene and sleep disorders. Poor sleep hygiene and sleep disorders have been shown to be related to other health care problems, including obesity, hypertension, diabetes mellitus, cardiovascular disease, and stroke.
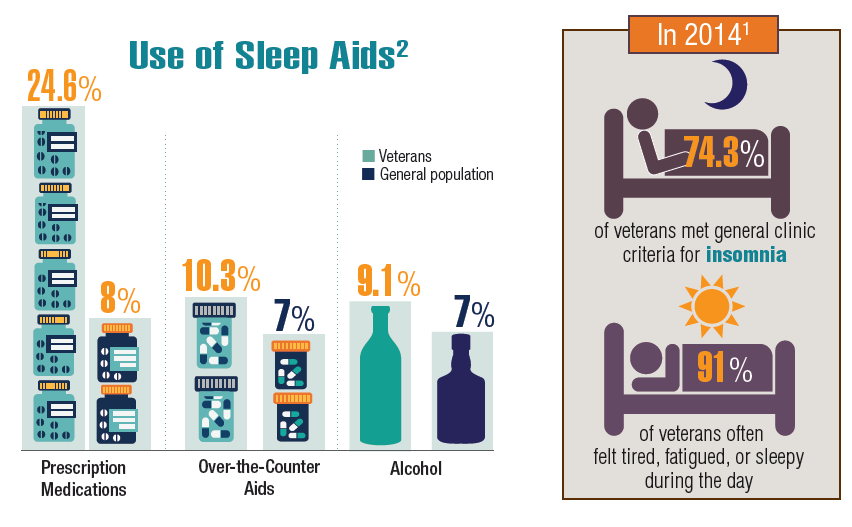
Nearly half of veterans in one study were diagnosed with sleep apnea, and more than one-fourth had insomnia. According to the National Veteran Sleep Survey, three-quarters of veterans may meet the clinical criteria for insomnia: “difficulty falling or staying asleep, 3 or more nights per week for at least a month with at least some significant sleep related daytime symptoms.”1 Fortunately, the National Veteran Sleep Survey found that veterans who participated expressed “a clear interest in behavioral sleep coaching to combat serious sleep deficits,” and the overwhelming majority were interested in sleep-tracking to help improve the
quality of their sleep.1
Veterans use a variety of aids to help them sleep. Nearly 25% use prescription medications. Troublingly, 10% of veterans use over-thecounter (OTC) products, and 9% report using alcohol, even though frequent use of alcohol can have a negative impact on health and may contribute to sleep disturbance.2 Moreover, there are little data on OTC sleep medications, and many have high rates of daytime sedation as an adverse effect.

Click here to read the digital edition.
Sleep is an essential need, and insufficient sleep is associated with a wide range of adverse outcomes. Service members are especially at risk for acquiring sleep disorders due in part to the sometimes austere living conditions and the irregularity of active-duty sleep/wake schedules. For both active-duty service members and veterans, posttraumatic stress disorder or other mental health diagnoses can further exacerbate poor sleep hygiene and sleep disorders. Poor sleep hygiene and sleep disorders have been shown to be related to other health care problems, including obesity, hypertension, diabetes mellitus, cardiovascular disease, and stroke.
Nearly half of veterans in one study were diagnosed with sleep apnea, and more than one-fourth had insomnia. According to the National Veteran Sleep Survey, three-quarters of veterans may meet the clinical criteria for insomnia: “difficulty falling or staying asleep, 3 or more nights per week for at least a month with at least some significant sleep related daytime symptoms.”1 Fortunately, the National Veteran Sleep Survey found that veterans who participated expressed “a clear interest in behavioral sleep coaching to combat serious sleep deficits,” and the overwhelming majority were interested in sleep-tracking to help improve the
quality of their sleep.1
Veterans use a variety of aids to help them sleep. Nearly 25% use prescription medications. Troublingly, 10% of veterans use over-thecounter (OTC) products, and 9% report using alcohol, even though frequent use of alcohol can have a negative impact on health and may contribute to sleep disturbance.2 Moreover, there are little data on OTC sleep medications, and many have high rates of daytime sedation as an adverse effect.
Click here to read the digital edition.
Sleep is an essential need, and insufficient sleep is associated with a wide range of adverse outcomes. Service members are especially at risk for acquiring sleep disorders due in part to the sometimes austere living conditions and the irregularity of active-duty sleep/wake schedules. For both active-duty service members and veterans, posttraumatic stress disorder or other mental health diagnoses can further exacerbate poor sleep hygiene and sleep disorders. Poor sleep hygiene and sleep disorders have been shown to be related to other health care problems, including obesity, hypertension, diabetes mellitus, cardiovascular disease, and stroke.
Nearly half of veterans in one study were diagnosed with sleep apnea, and more than one-fourth had insomnia. According to the National Veteran Sleep Survey, three-quarters of veterans may meet the clinical criteria for insomnia: “difficulty falling or staying asleep, 3 or more nights per week for at least a month with at least some significant sleep related daytime symptoms.”1 Fortunately, the National Veteran Sleep Survey found that veterans who participated expressed “a clear interest in behavioral sleep coaching to combat serious sleep deficits,” and the overwhelming majority were interested in sleep-tracking to help improve the
quality of their sleep.1
Veterans use a variety of aids to help them sleep. Nearly 25% use prescription medications. Troublingly, 10% of veterans use over-thecounter (OTC) products, and 9% report using alcohol, even though frequent use of alcohol can have a negative impact on health and may contribute to sleep disturbance.2 Moreover, there are little data on OTC sleep medications, and many have high rates of daytime sedation as an adverse effect.
Click here to read the digital edition.
Respiratory Disease Federal Health Data Trends (FULL)
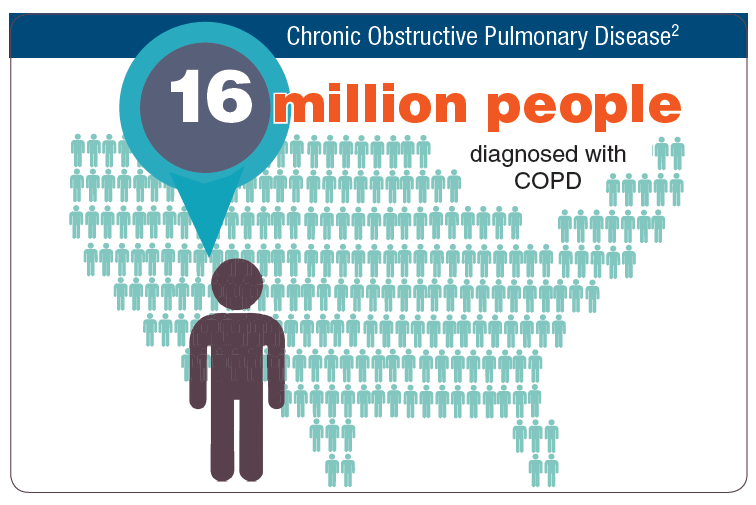
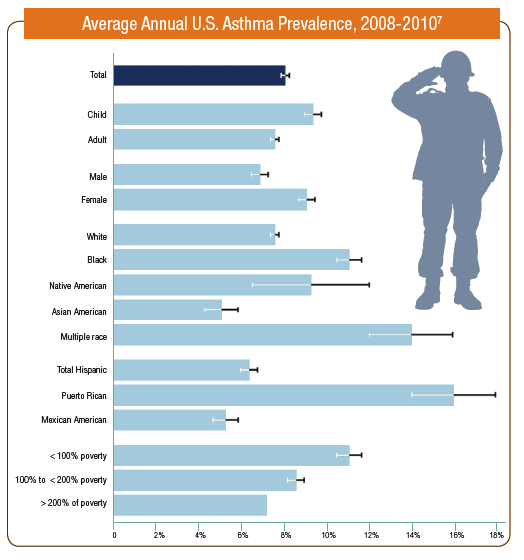
Nearly 25 million Americans (7.8%) have asthma, and just under 16 million (6.4%) have been diagnosed with chronic obstructive pulmonary disease (COPD). By all indications, the burden is even higher among active-duty service members and veterans, and the prevalence is expected to increase in those populations.
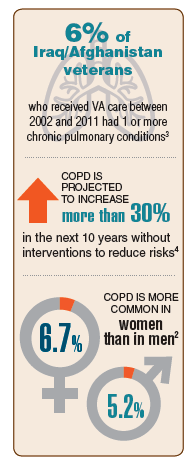
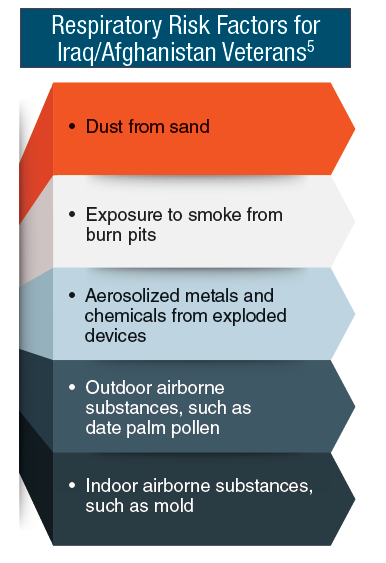
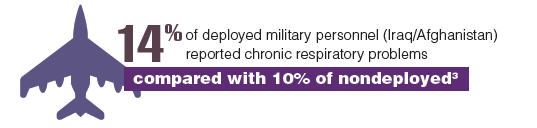
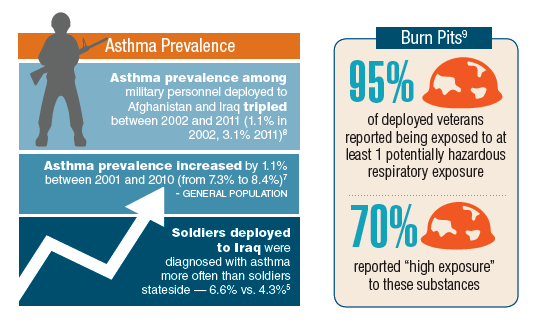
Exposure to irritants and hazardous materials during service seems to be a contributing factor. High rates of tobacco use in both activity-duty service members and veterans remain a significant factor. In addition, soldiers who deployed to Iraq were diagnosed with asthma more often than soldiers who stayed in the U.S., and the asthma prevalence among military personnel deployed to Afghanistan and Iraq tripled between 2002 and 2011. One in 7 deployed military personnel reported chronic respiratory problems compared with 10% of nondeployed service members, and 95% of deployed veterans reported at least 1 potentially hazardous exposure. It’s little wonder that 6% of Iraq/Afghanistan veterans who received VA care between 2002 and 2011 had 1 or more chronic pulmonary conditions.
Although preventable and treatable, worldwide COPD mortality is increasing. Moreover, prevalence of COPD is projected to increase more than 30% in the next 10 years without interventions to reduce risks. The Global Initiative for Chronic Obstructive Lung Disease now recommends that any patient with dyspnea, chronic cough, sputum production, or other risks factors should be examined for a potential COPD diagnosis.
Click here to read the digital edition.
Nearly 25 million Americans (7.8%) have asthma, and just under 16 million (6.4%) have been diagnosed with chronic obstructive pulmonary disease (COPD). By all indications, the burden is even higher among active-duty service members and veterans, and the prevalence is expected to increase in those populations.
Exposure to irritants and hazardous materials during service seems to be a contributing factor. High rates of tobacco use in both activity-duty service members and veterans remain a significant factor. In addition, soldiers who deployed to Iraq were diagnosed with asthma more often than soldiers who stayed in the U.S., and the asthma prevalence among military personnel deployed to Afghanistan and Iraq tripled between 2002 and 2011. One in 7 deployed military personnel reported chronic respiratory problems compared with 10% of nondeployed service members, and 95% of deployed veterans reported at least 1 potentially hazardous exposure. It’s little wonder that 6% of Iraq/Afghanistan veterans who received VA care between 2002 and 2011 had 1 or more chronic pulmonary conditions.
Although preventable and treatable, worldwide COPD mortality is increasing. Moreover, prevalence of COPD is projected to increase more than 30% in the next 10 years without interventions to reduce risks. The Global Initiative for Chronic Obstructive Lung Disease now recommends that any patient with dyspnea, chronic cough, sputum production, or other risks factors should be examined for a potential COPD diagnosis.
Click here to read the digital edition.
Nearly 25 million Americans (7.8%) have asthma, and just under 16 million (6.4%) have been diagnosed with chronic obstructive pulmonary disease (COPD). By all indications, the burden is even higher among active-duty service members and veterans, and the prevalence is expected to increase in those populations.
Exposure to irritants and hazardous materials during service seems to be a contributing factor. High rates of tobacco use in both activity-duty service members and veterans remain a significant factor. In addition, soldiers who deployed to Iraq were diagnosed with asthma more often than soldiers who stayed in the U.S., and the asthma prevalence among military personnel deployed to Afghanistan and Iraq tripled between 2002 and 2011. One in 7 deployed military personnel reported chronic respiratory problems compared with 10% of nondeployed service members, and 95% of deployed veterans reported at least 1 potentially hazardous exposure. It’s little wonder that 6% of Iraq/Afghanistan veterans who received VA care between 2002 and 2011 had 1 or more chronic pulmonary conditions.
Although preventable and treatable, worldwide COPD mortality is increasing. Moreover, prevalence of COPD is projected to increase more than 30% in the next 10 years without interventions to reduce risks. The Global Initiative for Chronic Obstructive Lung Disease now recommends that any patient with dyspnea, chronic cough, sputum production, or other risks factors should be examined for a potential COPD diagnosis.
Click here to read the digital edition.
Cardiovascular Disease Federal Health Data Trends (Full)
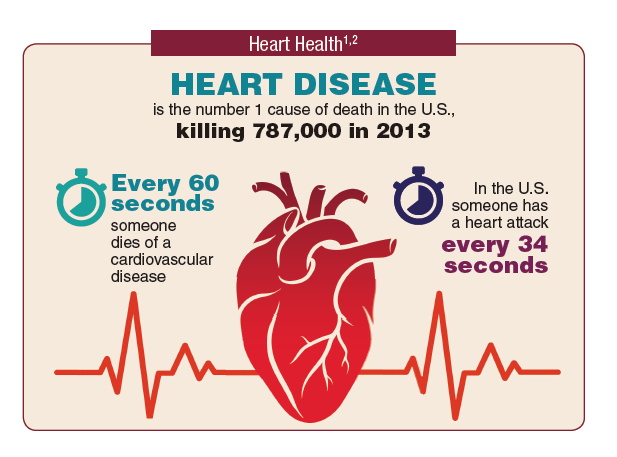
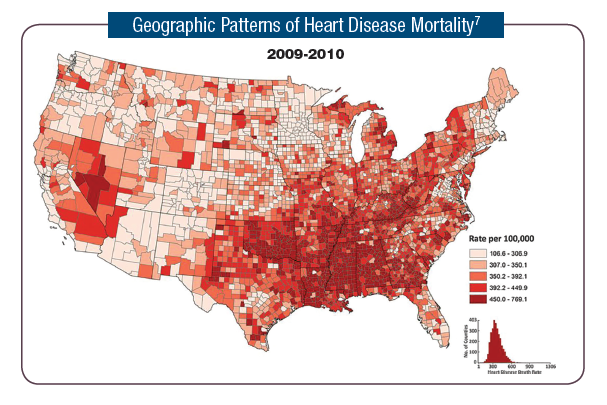
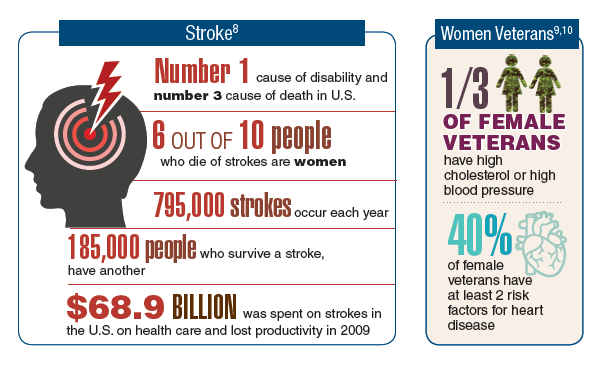
Cardiovascular disease is the leading cause of death in the U.S. and one of the leading causes of hospitalization and disability in the VA. It also is associated with other comorbid conditions that impact veterans, such as diabetes mellitus (DM), spinal cord injuries, and posttraumatic stress disorder. Most heart attacks are due to smoking, high cholesterol, high blood pressure, obesity, DM, diet, lack of exercise, high alcohol use, and stress. Many of these risk factors trend higher for veterans. Some veterans also are at higher risk due to exposure to hazardous materials. For example, veterans with ischemic heart disease who were exposed to Agent Orange or other herbicides during military service do not have to prove a service connection.
Currently the VA Office of Research and Development is sponsoring more than 70 clinical trials covering cardiovascular disease, ranging from using veteran peer coaches who promote cardiac health to robotic training for stroke neurorehabilitation.




Click here to read the digital edition.
Cardiovascular disease is the leading cause of death in the U.S. and one of the leading causes of hospitalization and disability in the VA. It also is associated with other comorbid conditions that impact veterans, such as diabetes mellitus (DM), spinal cord injuries, and posttraumatic stress disorder. Most heart attacks are due to smoking, high cholesterol, high blood pressure, obesity, DM, diet, lack of exercise, high alcohol use, and stress. Many of these risk factors trend higher for veterans. Some veterans also are at higher risk due to exposure to hazardous materials. For example, veterans with ischemic heart disease who were exposed to Agent Orange or other herbicides during military service do not have to prove a service connection.
Currently the VA Office of Research and Development is sponsoring more than 70 clinical trials covering cardiovascular disease, ranging from using veteran peer coaches who promote cardiac health to robotic training for stroke neurorehabilitation.
Click here to read the digital edition.
Cardiovascular disease is the leading cause of death in the U.S. and one of the leading causes of hospitalization and disability in the VA. It also is associated with other comorbid conditions that impact veterans, such as diabetes mellitus (DM), spinal cord injuries, and posttraumatic stress disorder. Most heart attacks are due to smoking, high cholesterol, high blood pressure, obesity, DM, diet, lack of exercise, high alcohol use, and stress. Many of these risk factors trend higher for veterans. Some veterans also are at higher risk due to exposure to hazardous materials. For example, veterans with ischemic heart disease who were exposed to Agent Orange or other herbicides during military service do not have to prove a service connection.
Currently the VA Office of Research and Development is sponsoring more than 70 clinical trials covering cardiovascular disease, ranging from using veteran peer coaches who promote cardiac health to robotic training for stroke neurorehabilitation.
Click here to read the digital edition.
For smokers, the ends may not justify the ENDS
Smokers who used e-cigarettes and other electronic nicotine delivery systems (ENDS) were less likely to quit than were those who did not use such products, according to a 2015 survey and a follow-up conducted a year later.
“Under ‘real world’ use and conditions [ENDS] may have suppressed or delayed quitting among some adult smokers,” Scott R. Weaver, PhD, and his associates at Georgia State University, Atlanta, wrote in PLoS One. The original survey, conducted in August and September of 2015, involved 1,284 U.S. adult smokers from the GfK KnowledgePanel, of whom 858 completed the follow-up survey in September 2016.
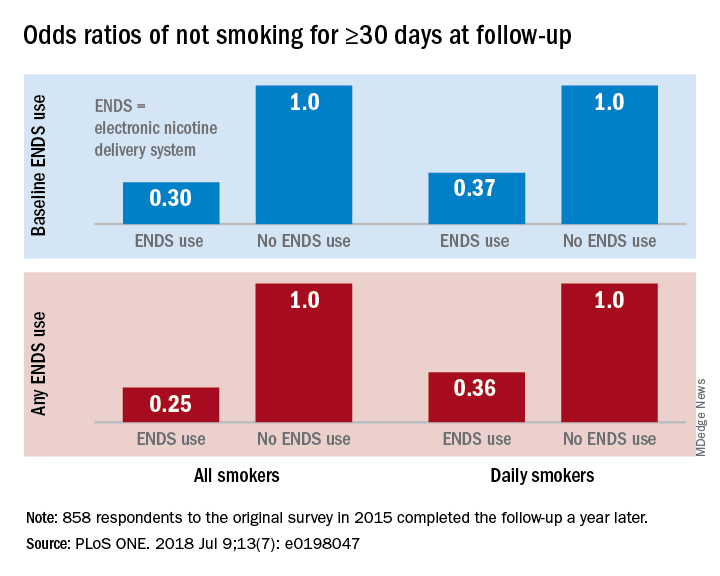
Smokers who used ENDS at baseline were slightly more likely to attempt to quit (53.7%) than were those who did not (48.6%) but were much less likely to have quit (defined as no smoking for at least 30 days at the time of follow-up): 9.4% vs. 18.9%, for an adjusted odds ratio of 0.30. Those who used ENDS at any time during the study were much more likely than were non-ENDS users to make an attempt (58.5% vs. 44.4%), but they were, again, much less likely to succeed (7.7% vs. 22.2%; AOR, 0.25), the investigators reported.
The results were similar for the subset of respondents who smoked every day: ENDS users were more likely to attempt to quit but less likely to succeed. Odds ratios for quitting were 0.37 for those using ENDS at baseline and 0.36 for those who used ENDS at any time since the first survey, Dr. Weaver and his associates said.
“Use of current ENDS products in real world conditions [does] not seem to improve the chances of quitting for smokers, and, under the current landscape, may not be the disruptive technology that increases the population quit rate and reduces the harm of combustibles,” they wrote.
The study was supported by the National Institute of Drug Abuse and the Food and Drug Administration’s Center for Tobacco Products. One of the investigators has received funding in the form of grant funding from Pfizer and the National Institutes of Health and another has served as a paid consultant to the Centers for Disease Control and Prevention.
SOURCE: Weaver SR et al. PLoS ONE. 2018 Jul 9;13(7): e0198047. doi: 10.1371/journal.pone.0198047.
Smokers who used e-cigarettes and other electronic nicotine delivery systems (ENDS) were less likely to quit than were those who did not use such products, according to a 2015 survey and a follow-up conducted a year later.
“Under ‘real world’ use and conditions [ENDS] may have suppressed or delayed quitting among some adult smokers,” Scott R. Weaver, PhD, and his associates at Georgia State University, Atlanta, wrote in PLoS One. The original survey, conducted in August and September of 2015, involved 1,284 U.S. adult smokers from the GfK KnowledgePanel, of whom 858 completed the follow-up survey in September 2016.
Smokers who used ENDS at baseline were slightly more likely to attempt to quit (53.7%) than were those who did not (48.6%) but were much less likely to have quit (defined as no smoking for at least 30 days at the time of follow-up): 9.4% vs. 18.9%, for an adjusted odds ratio of 0.30. Those who used ENDS at any time during the study were much more likely than were non-ENDS users to make an attempt (58.5% vs. 44.4%), but they were, again, much less likely to succeed (7.7% vs. 22.2%; AOR, 0.25), the investigators reported.
The results were similar for the subset of respondents who smoked every day: ENDS users were more likely to attempt to quit but less likely to succeed. Odds ratios for quitting were 0.37 for those using ENDS at baseline and 0.36 for those who used ENDS at any time since the first survey, Dr. Weaver and his associates said.
“Use of current ENDS products in real world conditions [does] not seem to improve the chances of quitting for smokers, and, under the current landscape, may not be the disruptive technology that increases the population quit rate and reduces the harm of combustibles,” they wrote.
The study was supported by the National Institute of Drug Abuse and the Food and Drug Administration’s Center for Tobacco Products. One of the investigators has received funding in the form of grant funding from Pfizer and the National Institutes of Health and another has served as a paid consultant to the Centers for Disease Control and Prevention.
SOURCE: Weaver SR et al. PLoS ONE. 2018 Jul 9;13(7): e0198047. doi: 10.1371/journal.pone.0198047.
Smokers who used e-cigarettes and other electronic nicotine delivery systems (ENDS) were less likely to quit than were those who did not use such products, according to a 2015 survey and a follow-up conducted a year later.
“Under ‘real world’ use and conditions [ENDS] may have suppressed or delayed quitting among some adult smokers,” Scott R. Weaver, PhD, and his associates at Georgia State University, Atlanta, wrote in PLoS One. The original survey, conducted in August and September of 2015, involved 1,284 U.S. adult smokers from the GfK KnowledgePanel, of whom 858 completed the follow-up survey in September 2016.
Smokers who used ENDS at baseline were slightly more likely to attempt to quit (53.7%) than were those who did not (48.6%) but were much less likely to have quit (defined as no smoking for at least 30 days at the time of follow-up): 9.4% vs. 18.9%, for an adjusted odds ratio of 0.30. Those who used ENDS at any time during the study were much more likely than were non-ENDS users to make an attempt (58.5% vs. 44.4%), but they were, again, much less likely to succeed (7.7% vs. 22.2%; AOR, 0.25), the investigators reported.
The results were similar for the subset of respondents who smoked every day: ENDS users were more likely to attempt to quit but less likely to succeed. Odds ratios for quitting were 0.37 for those using ENDS at baseline and 0.36 for those who used ENDS at any time since the first survey, Dr. Weaver and his associates said.
“Use of current ENDS products in real world conditions [does] not seem to improve the chances of quitting for smokers, and, under the current landscape, may not be the disruptive technology that increases the population quit rate and reduces the harm of combustibles,” they wrote.
The study was supported by the National Institute of Drug Abuse and the Food and Drug Administration’s Center for Tobacco Products. One of the investigators has received funding in the form of grant funding from Pfizer and the National Institutes of Health and another has served as a paid consultant to the Centers for Disease Control and Prevention.
SOURCE: Weaver SR et al. PLoS ONE. 2018 Jul 9;13(7): e0198047. doi: 10.1371/journal.pone.0198047.
FROM PLOS ONE