User login
Psoriasis, Etanercept, and Myelodysplasia: Looking for Connections
Physicians from Menoufia University and Cairo University in Egypt, and Al Hada Armed Forces Hospital in Saudi Arabia report on a patient who developed myelodysplasia with excess blasts 1 year after he started on the tumor necrosis factor-alpha blocker etanercept for psoriasis. The patient, a 76-year-old man, arrived at the emergency department (ED) with ecchymosis and recurrent epistaxis. He had a critically low platelet count, anemia, and normal leukocyte count. The reticulocyte index, serum ferritin, and folate levels indicated ineffective erythropoiesis. Bone marrow aspirate and biopsy confirmed a diagnosis of myelodysplastic syndrome.
The physicians stopped the etanercept and administered 2 cycles of azacitidine and folic acid supplementation, but the response was minima,l and the patient platelet count worsened. While waiting for the third cycle, the patient was readmitted to the ED with lower gastrointestinal bleeding, epistaxis, and shock. He died of cardiopulmonary arrest.
The physicians note that immune dysregulation and altered T-cell hemostasis are essential to the development of myelodysplastic syndrome. They also note that nonspecific activation and proliferation of T lymphocytes has been documented as promoting epidermal growth in genetically susceptible psoriasis patients.
Myelodysplastic syndrome has been associated with psoriasis in about 7% of cases, and researchers have found a higher incidence of leukemia and laryngeal cancer in families of psoriasis patients. There also have been reports of leukemia in psoriasis patients on systemic immunosuppressives. Etanercept has various hematologic adverse effects, including pancytopenia and aplastic anemia.
However, only 4 cases (including this one) have been reported of myelodysplastic syndrome in psoriasis patients. Taken together, the cases add to the growing evidence that suggests a link between myelodysplastic syndrome and etanercept treatment for psoriasis. Those patients, the physicians caution, should be considered at dual risk from treatment and disease. The physicians also recommend regular routine blood counts and discontinuing etanercept at onset of any cytopenias.
Source:
Dawoud NM, Ayoub OH, Essa ES, Dawoud DM. Indian J Dermatol Venereol Leprol. 2018;84(4):463-465.
doi: 10.4103/ijdvl.IJDVL_463_17
Physicians from Menoufia University and Cairo University in Egypt, and Al Hada Armed Forces Hospital in Saudi Arabia report on a patient who developed myelodysplasia with excess blasts 1 year after he started on the tumor necrosis factor-alpha blocker etanercept for psoriasis. The patient, a 76-year-old man, arrived at the emergency department (ED) with ecchymosis and recurrent epistaxis. He had a critically low platelet count, anemia, and normal leukocyte count. The reticulocyte index, serum ferritin, and folate levels indicated ineffective erythropoiesis. Bone marrow aspirate and biopsy confirmed a diagnosis of myelodysplastic syndrome.
The physicians stopped the etanercept and administered 2 cycles of azacitidine and folic acid supplementation, but the response was minima,l and the patient platelet count worsened. While waiting for the third cycle, the patient was readmitted to the ED with lower gastrointestinal bleeding, epistaxis, and shock. He died of cardiopulmonary arrest.
The physicians note that immune dysregulation and altered T-cell hemostasis are essential to the development of myelodysplastic syndrome. They also note that nonspecific activation and proliferation of T lymphocytes has been documented as promoting epidermal growth in genetically susceptible psoriasis patients.
Myelodysplastic syndrome has been associated with psoriasis in about 7% of cases, and researchers have found a higher incidence of leukemia and laryngeal cancer in families of psoriasis patients. There also have been reports of leukemia in psoriasis patients on systemic immunosuppressives. Etanercept has various hematologic adverse effects, including pancytopenia and aplastic anemia.
However, only 4 cases (including this one) have been reported of myelodysplastic syndrome in psoriasis patients. Taken together, the cases add to the growing evidence that suggests a link between myelodysplastic syndrome and etanercept treatment for psoriasis. Those patients, the physicians caution, should be considered at dual risk from treatment and disease. The physicians also recommend regular routine blood counts and discontinuing etanercept at onset of any cytopenias.
Source:
Dawoud NM, Ayoub OH, Essa ES, Dawoud DM. Indian J Dermatol Venereol Leprol. 2018;84(4):463-465.
doi: 10.4103/ijdvl.IJDVL_463_17
Physicians from Menoufia University and Cairo University in Egypt, and Al Hada Armed Forces Hospital in Saudi Arabia report on a patient who developed myelodysplasia with excess blasts 1 year after he started on the tumor necrosis factor-alpha blocker etanercept for psoriasis. The patient, a 76-year-old man, arrived at the emergency department (ED) with ecchymosis and recurrent epistaxis. He had a critically low platelet count, anemia, and normal leukocyte count. The reticulocyte index, serum ferritin, and folate levels indicated ineffective erythropoiesis. Bone marrow aspirate and biopsy confirmed a diagnosis of myelodysplastic syndrome.
The physicians stopped the etanercept and administered 2 cycles of azacitidine and folic acid supplementation, but the response was minima,l and the patient platelet count worsened. While waiting for the third cycle, the patient was readmitted to the ED with lower gastrointestinal bleeding, epistaxis, and shock. He died of cardiopulmonary arrest.
The physicians note that immune dysregulation and altered T-cell hemostasis are essential to the development of myelodysplastic syndrome. They also note that nonspecific activation and proliferation of T lymphocytes has been documented as promoting epidermal growth in genetically susceptible psoriasis patients.
Myelodysplastic syndrome has been associated with psoriasis in about 7% of cases, and researchers have found a higher incidence of leukemia and laryngeal cancer in families of psoriasis patients. There also have been reports of leukemia in psoriasis patients on systemic immunosuppressives. Etanercept has various hematologic adverse effects, including pancytopenia and aplastic anemia.
However, only 4 cases (including this one) have been reported of myelodysplastic syndrome in psoriasis patients. Taken together, the cases add to the growing evidence that suggests a link between myelodysplastic syndrome and etanercept treatment for psoriasis. Those patients, the physicians caution, should be considered at dual risk from treatment and disease. The physicians also recommend regular routine blood counts and discontinuing etanercept at onset of any cytopenias.
Source:
Dawoud NM, Ayoub OH, Essa ES, Dawoud DM. Indian J Dermatol Venereol Leprol. 2018;84(4):463-465.
doi: 10.4103/ijdvl.IJDVL_463_17
VA Funds Intimate Partner Violence Programs
In the US, 36% of women and 29% of men have experienced rape, physical violence, or stalking by an intimate partner. Research suggests that veterans may be at greater risk for intimate partner violence than civilian counterparts, given the unique stressors posed by military life, such as military deployments that result in family separation, reintegration issues, and combat-related health issues, including PTSD and TBI. According to the VA’s Domestic Violence Task Force, the overall 12-month prevalence of inmate partner violence (IPV) perpetration among active duty service members was 22%, and victimization was 30%.
To help address this problem, the VA launched the IPV Assistance Program in 2014 and has since established coordinators at more than 115 facilities. The program coordinators use resources from mental health, primary care, women’s health, veterans’ justice outreach, and employee occupational health and assistance programs. The program also offers intervention through VA and community partnerships that address housing, education, and employment needs.
The program takes a holistic approach, focusing on developing a culture of safety, the VA says, with the goal of understanding, recognizing and responding to the effects of all types of trauma, including physical, sexual, and psychological. “We are giving careful attention to this program,” says Acting VA Secretary Peter O’Rourke, “ensuring it is integrated into clinical care and workplace safety.”
In the US, 36% of women and 29% of men have experienced rape, physical violence, or stalking by an intimate partner. Research suggests that veterans may be at greater risk for intimate partner violence than civilian counterparts, given the unique stressors posed by military life, such as military deployments that result in family separation, reintegration issues, and combat-related health issues, including PTSD and TBI. According to the VA’s Domestic Violence Task Force, the overall 12-month prevalence of inmate partner violence (IPV) perpetration among active duty service members was 22%, and victimization was 30%.
To help address this problem, the VA launched the IPV Assistance Program in 2014 and has since established coordinators at more than 115 facilities. The program coordinators use resources from mental health, primary care, women’s health, veterans’ justice outreach, and employee occupational health and assistance programs. The program also offers intervention through VA and community partnerships that address housing, education, and employment needs.
The program takes a holistic approach, focusing on developing a culture of safety, the VA says, with the goal of understanding, recognizing and responding to the effects of all types of trauma, including physical, sexual, and psychological. “We are giving careful attention to this program,” says Acting VA Secretary Peter O’Rourke, “ensuring it is integrated into clinical care and workplace safety.”
In the US, 36% of women and 29% of men have experienced rape, physical violence, or stalking by an intimate partner. Research suggests that veterans may be at greater risk for intimate partner violence than civilian counterparts, given the unique stressors posed by military life, such as military deployments that result in family separation, reintegration issues, and combat-related health issues, including PTSD and TBI. According to the VA’s Domestic Violence Task Force, the overall 12-month prevalence of inmate partner violence (IPV) perpetration among active duty service members was 22%, and victimization was 30%.
To help address this problem, the VA launched the IPV Assistance Program in 2014 and has since established coordinators at more than 115 facilities. The program coordinators use resources from mental health, primary care, women’s health, veterans’ justice outreach, and employee occupational health and assistance programs. The program also offers intervention through VA and community partnerships that address housing, education, and employment needs.
The program takes a holistic approach, focusing on developing a culture of safety, the VA says, with the goal of understanding, recognizing and responding to the effects of all types of trauma, including physical, sexual, and psychological. “We are giving careful attention to this program,” says Acting VA Secretary Peter O’Rourke, “ensuring it is integrated into clinical care and workplace safety.”
Rituximab reduces risk of follicular lymphoma transformation
Rituximab-based chemotherapy can significantly reduce the risk of transformation of follicular lymphoma (FL) from an indolent to an aggressive histology, such as diffuse large B-cell lymphoma, results of a retrospective pooled analysis have suggested.

“Despite the intrinsic limitations related to the retrospective nature of our study, we confirmed that the cumulative hazard of histological transformation as a first event in follicular lymphoma can be reduced significantly by introducing rituximab to a backbone therapy. Moreover, our data also confirm that histological transformation still has an adverse effect on patient outcome, although it is less catastrophic than the pre-rituximab regimens,” they wrote in the Lancet Haematology.
These investigators, from 11 cooperative groups or institutions across Europe, pooled data on patients aged 18 years and older who had a histologically confirmed diagnosis of grade 1, 2, or 3a FL between Jan. 2, 1997, and Dec. 20, 2013.
They defined histologic transformation as a biopsy-proven aggressive lymphoma that occurred as a first event after first-line therapy.
Data on a total of 8,116 patients were available for analysis; 509 of these patients had had histologic transformations. After a median follow-up of 87 months, the 10-year cumulative hazard for all patients was 7.7%. The 10-year cumulative hazard – one of two primary endpoints – was 5.2% for patients who had received any rituximab versus 8.7% for those who did not, which translated into a hazard ratio of 0.73 (P = .004).
Among patients who received rituximab during induction only, the 10-year cumulative hazard was 5.9%, and it was 3.6% among those who received rituximab during induction and maintenance phases of treatment. This difference translated into a HR of 0.55 (P = .003).
The benefit of rituximab induction and maintenance – compared with induction only – held up in a multivariate analysis controlling for age at diagnosis, sex, FLIPI (Follicular Lymphoma International Prognostic Index) score, active surveillance vs. treatment, and FL grade (HR, 0.55; P = .016).
There were 287 deaths among the 509 patients with transformation, resulting in a 10-year survival after transformation of 32%.
The 5-year survival after transformation was 38% for patients who were not exposed to rituximab, 42% for patients who received induction rituximab, and 43% for those who received both induction and maintenance rituximab, but the differences between the three groups were not statistically significant.
“More comprehensive knowledge of the biological risk factors for follicular lymphoma transformation and the molecular pathways involved is likely to help clinicians make more accurate prognostic assessments and also inform the potential usefulness of novel drugs for the treatment of follicular lymphoma,” the researchers wrote.
The study was funded by the European Lymphoma Institute and other research groups. The researchers reported having no financial disclosures.
SOURCE: Federico M et al. Lancet Haematol. 2018 Jul 4. doi: 10.1016/S2352-3026(18)30090-5.
Rituximab-based chemotherapy can significantly reduce the risk of transformation of follicular lymphoma (FL) from an indolent to an aggressive histology, such as diffuse large B-cell lymphoma, results of a retrospective pooled analysis have suggested.
“Despite the intrinsic limitations related to the retrospective nature of our study, we confirmed that the cumulative hazard of histological transformation as a first event in follicular lymphoma can be reduced significantly by introducing rituximab to a backbone therapy. Moreover, our data also confirm that histological transformation still has an adverse effect on patient outcome, although it is less catastrophic than the pre-rituximab regimens,” they wrote in the Lancet Haematology.
These investigators, from 11 cooperative groups or institutions across Europe, pooled data on patients aged 18 years and older who had a histologically confirmed diagnosis of grade 1, 2, or 3a FL between Jan. 2, 1997, and Dec. 20, 2013.
They defined histologic transformation as a biopsy-proven aggressive lymphoma that occurred as a first event after first-line therapy.
Data on a total of 8,116 patients were available for analysis; 509 of these patients had had histologic transformations. After a median follow-up of 87 months, the 10-year cumulative hazard for all patients was 7.7%. The 10-year cumulative hazard – one of two primary endpoints – was 5.2% for patients who had received any rituximab versus 8.7% for those who did not, which translated into a hazard ratio of 0.73 (P = .004).
Among patients who received rituximab during induction only, the 10-year cumulative hazard was 5.9%, and it was 3.6% among those who received rituximab during induction and maintenance phases of treatment. This difference translated into a HR of 0.55 (P = .003).
The benefit of rituximab induction and maintenance – compared with induction only – held up in a multivariate analysis controlling for age at diagnosis, sex, FLIPI (Follicular Lymphoma International Prognostic Index) score, active surveillance vs. treatment, and FL grade (HR, 0.55; P = .016).
There were 287 deaths among the 509 patients with transformation, resulting in a 10-year survival after transformation of 32%.
The 5-year survival after transformation was 38% for patients who were not exposed to rituximab, 42% for patients who received induction rituximab, and 43% for those who received both induction and maintenance rituximab, but the differences between the three groups were not statistically significant.
“More comprehensive knowledge of the biological risk factors for follicular lymphoma transformation and the molecular pathways involved is likely to help clinicians make more accurate prognostic assessments and also inform the potential usefulness of novel drugs for the treatment of follicular lymphoma,” the researchers wrote.
The study was funded by the European Lymphoma Institute and other research groups. The researchers reported having no financial disclosures.
SOURCE: Federico M et al. Lancet Haematol. 2018 Jul 4. doi: 10.1016/S2352-3026(18)30090-5.
Rituximab-based chemotherapy can significantly reduce the risk of transformation of follicular lymphoma (FL) from an indolent to an aggressive histology, such as diffuse large B-cell lymphoma, results of a retrospective pooled analysis have suggested.
“Despite the intrinsic limitations related to the retrospective nature of our study, we confirmed that the cumulative hazard of histological transformation as a first event in follicular lymphoma can be reduced significantly by introducing rituximab to a backbone therapy. Moreover, our data also confirm that histological transformation still has an adverse effect on patient outcome, although it is less catastrophic than the pre-rituximab regimens,” they wrote in the Lancet Haematology.
These investigators, from 11 cooperative groups or institutions across Europe, pooled data on patients aged 18 years and older who had a histologically confirmed diagnosis of grade 1, 2, or 3a FL between Jan. 2, 1997, and Dec. 20, 2013.
They defined histologic transformation as a biopsy-proven aggressive lymphoma that occurred as a first event after first-line therapy.
Data on a total of 8,116 patients were available for analysis; 509 of these patients had had histologic transformations. After a median follow-up of 87 months, the 10-year cumulative hazard for all patients was 7.7%. The 10-year cumulative hazard – one of two primary endpoints – was 5.2% for patients who had received any rituximab versus 8.7% for those who did not, which translated into a hazard ratio of 0.73 (P = .004).
Among patients who received rituximab during induction only, the 10-year cumulative hazard was 5.9%, and it was 3.6% among those who received rituximab during induction and maintenance phases of treatment. This difference translated into a HR of 0.55 (P = .003).
The benefit of rituximab induction and maintenance – compared with induction only – held up in a multivariate analysis controlling for age at diagnosis, sex, FLIPI (Follicular Lymphoma International Prognostic Index) score, active surveillance vs. treatment, and FL grade (HR, 0.55; P = .016).
There were 287 deaths among the 509 patients with transformation, resulting in a 10-year survival after transformation of 32%.
The 5-year survival after transformation was 38% for patients who were not exposed to rituximab, 42% for patients who received induction rituximab, and 43% for those who received both induction and maintenance rituximab, but the differences between the three groups were not statistically significant.
“More comprehensive knowledge of the biological risk factors for follicular lymphoma transformation and the molecular pathways involved is likely to help clinicians make more accurate prognostic assessments and also inform the potential usefulness of novel drugs for the treatment of follicular lymphoma,” the researchers wrote.
The study was funded by the European Lymphoma Institute and other research groups. The researchers reported having no financial disclosures.
SOURCE: Federico M et al. Lancet Haematol. 2018 Jul 4. doi: 10.1016/S2352-3026(18)30090-5.
FROM THE LANCET HAEMATOLOGY
Key clinical point:
Major finding: The 10-year cumulative hazard of histologic transformation was 5.2% for patients who had received rituximab and 8.7% for those who had not.
Study details: Retrospective pooled analysis of 8,116 patients with FL, 509 of whom had transformation over a 10-year period.
Disclosures: The study was funded by Associazione Angela Serra per la Ricerca sul Cancro, European Lymphoma Institute, European Hematology Association Lymphoma Group, Fondazione Italiana Linfomi, and the Spanish Group of Lymphoma and Bone Marrow Transplantation. The researchers reported having no financial disclosures.
Source: Federico M et al. Lancet Haematol. 2018 Jul 4. doi: 10.1016/S2352-3026(18)30090-5.
New guidance offered for managing poorly controlled asthma in children
published in the Annals of Allergy, Asthma & Immunology.

“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.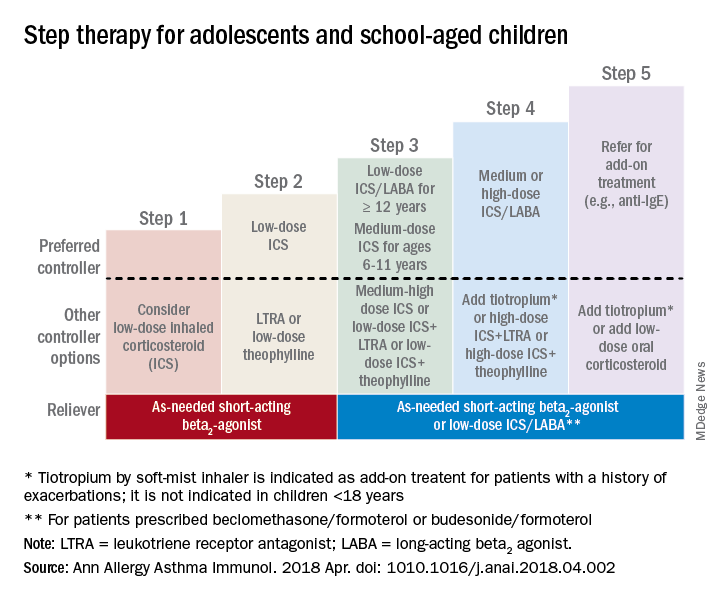
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger

In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider

Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
published in the Annals of Allergy, Asthma & Immunology.
“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger
In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider
Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
published in the Annals of Allergy, Asthma & Immunology.
“Although many children with asthma achieve symptom control with appropriate management, a substantial subset does not,” Bradley E. Chipps, MD, from the Capital Allergy & Respiratory Disease Center in Sacramento, Calif., and his colleagues wrote in the recommendations sponsored by the American College of Allergy, Asthma, and Immunology. “These children should undergo a step-up in care, but when and how to do that is not always straightforward. The Pediatric Asthma Yardstick is a practical resource for starting or adjusting controller therapy based on the options that are currently available for children, from infants to 18 years of age.”
In their recommendations, the authors grouped patients into age ranges of adolescent (12-18 years), school aged (6-11 years), and young children (5 years and under) as well as severity classifications.
Adolescents and school-aged children
For adolescents and school-aged children, step 1 was classified as intermittent asthma that can be controlled with low-dose inhaled corticosteroids (ICS) with short-acting beta2-agonist (SABA) for as-needed relief. Children considered for stepping up to the next therapy should show symptoms of mild persistent asthma that the authors recommended controlling with low-dose ICS, leukotriene receptor antagonist (LTRA), or low-dose theophylline with as-needed SABA.
In children 12-18 years with moderate persistent asthma (step 3), the authors recommended a combination of low-dose ICA and a long-acting beta2-agonist (LABA), while children 6-11 years should receive a medium dose of ICS; other considerations for school-aged children include a medium-high dose of ICS, a low-dose combination of ICS and LTRA, or low-dose ICS together with theophylline.
Adolescent or school-aged children with severe persistent asthma (step 4) should take a medium or high dose of ICS together with LABA, with the authors recommending adding tiotropium to a soft mist inhaler, combination high-dose ICS and LTRA, or a combination high-dose ICS and theophylline.
Dr. Chipps and his coauthors recommended children stepping up therapy beyond severe persistent asthma (step 5) should add on treatment such as low-dose oral corticosteroids, anti-immunoglobulin E therapy, and adding tiotropium to a soft-mist inhaler.
For adolescent and school-aged children going to steps 3-5, Dr. Chipps and his coauthors recommended prescribing as needed a short-acting beta2 agonist or low-dose ICS/LABA.
Children 5 years and younger
In children 5 years and younger, intermittent asthma (step 1) should be considered if the child has infrequent or viral wheezing but few or no symptoms in the interim that can be controlled with as-needed SABA. These young children who show symptoms of mild persistent asthma (step 2) can be treated with daily low-dose ICS, with other controller options of LTRA or intermittent ICS.
Stepping up therapy from mild to moderate persistent asthma (step 3), young children should receive double the daily dose of low-dose ICS from the previous step or use the low-dose ICS together with LTRA; if children show symptoms of severe persistent asthma (step 4), they should continue their daily controller and be referred to a specialist; other considerations for controllers at this step included adding LTRA, adding intermittent ICS, or increasing ICS frequency.
Other factors to consider
Inconsistencies in response to medication can occur because of comorbid conditions such as obesity, rhinosinusitis, respiratory infection or gastroesophageal reflux; suboptimal inhaled drug delivery; or failure to comply with treatment because of not wanting to take medication (common in adolescents), belief that even controller medicine can be taken intermittently, family stress, cost including lack of insurance or medication not covered by insurance. “Before adjusting therapy, it is important to ensure that the child’s change in symptoms is due to asthma and not to any of these factors that need to be addressed,” Dr. Chipps and his colleagues wrote.
Collaboration among children, their parents, and clinicians is needed to achieve good asthma control because of the “variable presentation within individuals and within the population of children affected” with asthma, they wrote.
The article summarizing the guidelines was sponsored by the American College of Allergy, Asthma, and Immunology. Most of the authors report various financial relationships with companies including AstraZeneca, Aerocrine, Aviragen, Boehringer Ingelheim, Cephalon, Circassia, Commense, Genentech, GlaxoSmithKline, Greer, Meda, Merck, Mylan, Novartis, Patara, Regeneron, Sanofi, TEVA, Theravance, and Vectura Group. Dr. Farrar and Dr. Szefler had no financial interests to disclose.
SOURCE: Chipps BE et al. Ann Allergy Asthma Immunol. 2018 Apr. doi: 1010.1016/j.anai.2018.04.002.
FROM ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Pros and Cons of Telemental Health Care
When telemental health care (TMH) works, it works well, the research agrees. For rural patients who often do not have easy access to health care TMH can be a lifesaver. The VA uses TMH to deliver care to veterans in rural VA medical centers, community-based outpatient clinics, and residential areas. However, TMH is still relatively new in many rural communities, say researchers from University of Mississippi in Oxford and Augusta University in Georgia, and few studies have examined the delivery tool from an administrative standpoint. The literature suggests TMH will save money—the exploratory study, however, suggests otherwise.
The researchers interviewed 6 providers selected from the 15 community mental health (MH) centers (CMHCs) in rural Mississippi as well as an independent MH counselor who develops policy for the Mississippi Counselors Association. They asked respondents about the feasibility of TMH in the Mississippi Delta; in particular, the benefits, the costs, and the role of the state in facilitating the service. The researchers also collected data from a grant-funded pilot project conducted in the Mississippi Delta region by the Delta Health Alliance, a nonprofit organization in partnership with the University of Mississippi Medical Center, which ran from 2008 to 2011. Telepsychiatry sessions are not currently being used in the region, but before the project ended, it was responsible for > 1,000 videoconferencing clinical sessions.
The initial counseling sessions were “awkward” for some patients, the interviewees said, and some clients felt the consultation was “less personal.” Getting used to the technology may take some time. Once clients acclimated the feedback was positive.
The health care providers were concerned by not being able to observe in-person nonverbal clues, such as poor hygiene, that would normally help them evaluate the client’s health. The nurse at the CMHC helped fill a gap, the researchers say, created by technology.
The researchers determined that the benefit side was weighty: For instance, patients had better access to well-trained MH professionals and to the state hospital, and family could visit inpatients via videoconferencing. Staff had better access to professional development and training.
However, cost issues were a definite concern. The project would not have been feasible without grant funding, the researchers say. Medicaid reimburses for TMH services but not for technology setup costs and maintenance. Moreover, the interviews with administrators, the researchers say, indicated that TMH did not save the organization money. Costs for the equipment, installation, rent, and other supplies were prohibitive.
Although start-up costs are high, overall systematic costs go down, with savings on travel-related costs, including fewer missed appointments. Broadband technology, videoconferencing software, webcams, and education all take money. “If policymakers are serious” about TMH, the researchers conclude, they should allocate appropriate funding and resources.
Source:
Holland J, Hatcher W, Meares WL. J Health Hum Serv Adm. 2018;41(1):52-86.
When telemental health care (TMH) works, it works well, the research agrees. For rural patients who often do not have easy access to health care TMH can be a lifesaver. The VA uses TMH to deliver care to veterans in rural VA medical centers, community-based outpatient clinics, and residential areas. However, TMH is still relatively new in many rural communities, say researchers from University of Mississippi in Oxford and Augusta University in Georgia, and few studies have examined the delivery tool from an administrative standpoint. The literature suggests TMH will save money—the exploratory study, however, suggests otherwise.
The researchers interviewed 6 providers selected from the 15 community mental health (MH) centers (CMHCs) in rural Mississippi as well as an independent MH counselor who develops policy for the Mississippi Counselors Association. They asked respondents about the feasibility of TMH in the Mississippi Delta; in particular, the benefits, the costs, and the role of the state in facilitating the service. The researchers also collected data from a grant-funded pilot project conducted in the Mississippi Delta region by the Delta Health Alliance, a nonprofit organization in partnership with the University of Mississippi Medical Center, which ran from 2008 to 2011. Telepsychiatry sessions are not currently being used in the region, but before the project ended, it was responsible for > 1,000 videoconferencing clinical sessions.
The initial counseling sessions were “awkward” for some patients, the interviewees said, and some clients felt the consultation was “less personal.” Getting used to the technology may take some time. Once clients acclimated the feedback was positive.
The health care providers were concerned by not being able to observe in-person nonverbal clues, such as poor hygiene, that would normally help them evaluate the client’s health. The nurse at the CMHC helped fill a gap, the researchers say, created by technology.
The researchers determined that the benefit side was weighty: For instance, patients had better access to well-trained MH professionals and to the state hospital, and family could visit inpatients via videoconferencing. Staff had better access to professional development and training.
However, cost issues were a definite concern. The project would not have been feasible without grant funding, the researchers say. Medicaid reimburses for TMH services but not for technology setup costs and maintenance. Moreover, the interviews with administrators, the researchers say, indicated that TMH did not save the organization money. Costs for the equipment, installation, rent, and other supplies were prohibitive.
Although start-up costs are high, overall systematic costs go down, with savings on travel-related costs, including fewer missed appointments. Broadband technology, videoconferencing software, webcams, and education all take money. “If policymakers are serious” about TMH, the researchers conclude, they should allocate appropriate funding and resources.
Source:
Holland J, Hatcher W, Meares WL. J Health Hum Serv Adm. 2018;41(1):52-86.
When telemental health care (TMH) works, it works well, the research agrees. For rural patients who often do not have easy access to health care TMH can be a lifesaver. The VA uses TMH to deliver care to veterans in rural VA medical centers, community-based outpatient clinics, and residential areas. However, TMH is still relatively new in many rural communities, say researchers from University of Mississippi in Oxford and Augusta University in Georgia, and few studies have examined the delivery tool from an administrative standpoint. The literature suggests TMH will save money—the exploratory study, however, suggests otherwise.
The researchers interviewed 6 providers selected from the 15 community mental health (MH) centers (CMHCs) in rural Mississippi as well as an independent MH counselor who develops policy for the Mississippi Counselors Association. They asked respondents about the feasibility of TMH in the Mississippi Delta; in particular, the benefits, the costs, and the role of the state in facilitating the service. The researchers also collected data from a grant-funded pilot project conducted in the Mississippi Delta region by the Delta Health Alliance, a nonprofit organization in partnership with the University of Mississippi Medical Center, which ran from 2008 to 2011. Telepsychiatry sessions are not currently being used in the region, but before the project ended, it was responsible for > 1,000 videoconferencing clinical sessions.
The initial counseling sessions were “awkward” for some patients, the interviewees said, and some clients felt the consultation was “less personal.” Getting used to the technology may take some time. Once clients acclimated the feedback was positive.
The health care providers were concerned by not being able to observe in-person nonverbal clues, such as poor hygiene, that would normally help them evaluate the client’s health. The nurse at the CMHC helped fill a gap, the researchers say, created by technology.
The researchers determined that the benefit side was weighty: For instance, patients had better access to well-trained MH professionals and to the state hospital, and family could visit inpatients via videoconferencing. Staff had better access to professional development and training.
However, cost issues were a definite concern. The project would not have been feasible without grant funding, the researchers say. Medicaid reimburses for TMH services but not for technology setup costs and maintenance. Moreover, the interviews with administrators, the researchers say, indicated that TMH did not save the organization money. Costs for the equipment, installation, rent, and other supplies were prohibitive.
Although start-up costs are high, overall systematic costs go down, with savings on travel-related costs, including fewer missed appointments. Broadband technology, videoconferencing software, webcams, and education all take money. “If policymakers are serious” about TMH, the researchers conclude, they should allocate appropriate funding and resources.
Source:
Holland J, Hatcher W, Meares WL. J Health Hum Serv Adm. 2018;41(1):52-86.
Neurology Federal Health Data Trends (FULL)
Neurologic disorders seem to impact veterans disproportionately. Multiple sclerosis, Parkinson disease, dementia, epilepsy, and other less common neurologic disorders require a high-level of care for veterans.
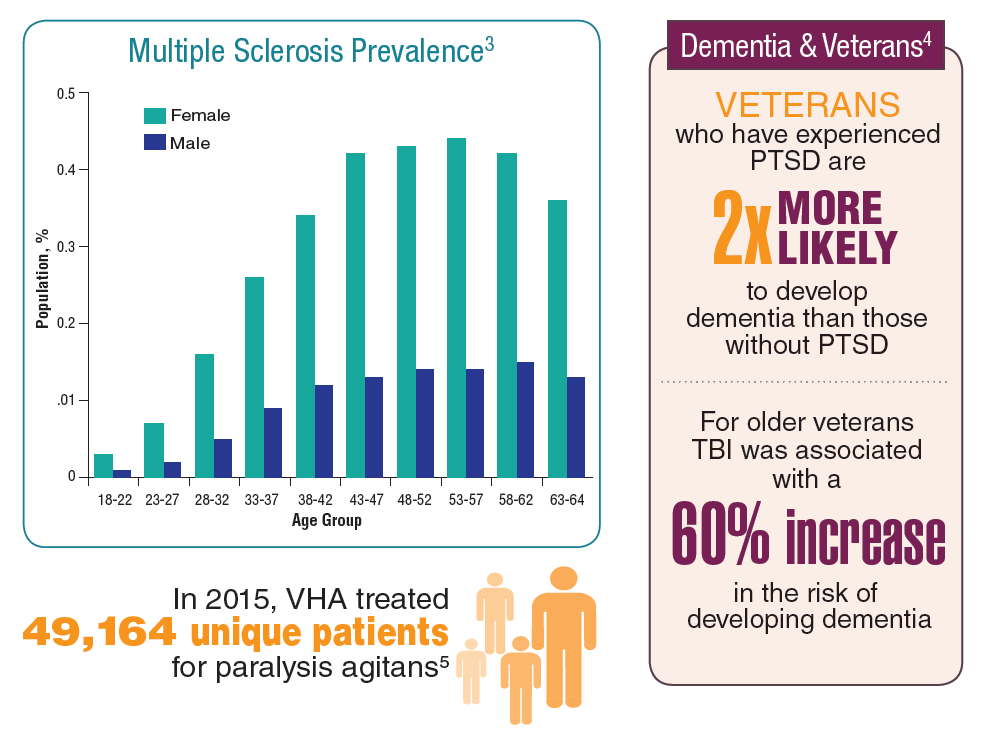
Multiple sclerosis is often diagnosed when patients are in their 20s or 30s. Typically, MS affects women more than men at a rate up to 3 times higher, and studies have shown that race and geography also may play a role in the risk of acquiring MS. Rates of MS in Vietnam era veterans were higher than those of veterans of World War II and the Korean War. That trend continued for Army and Air Force Gulf War veterans.
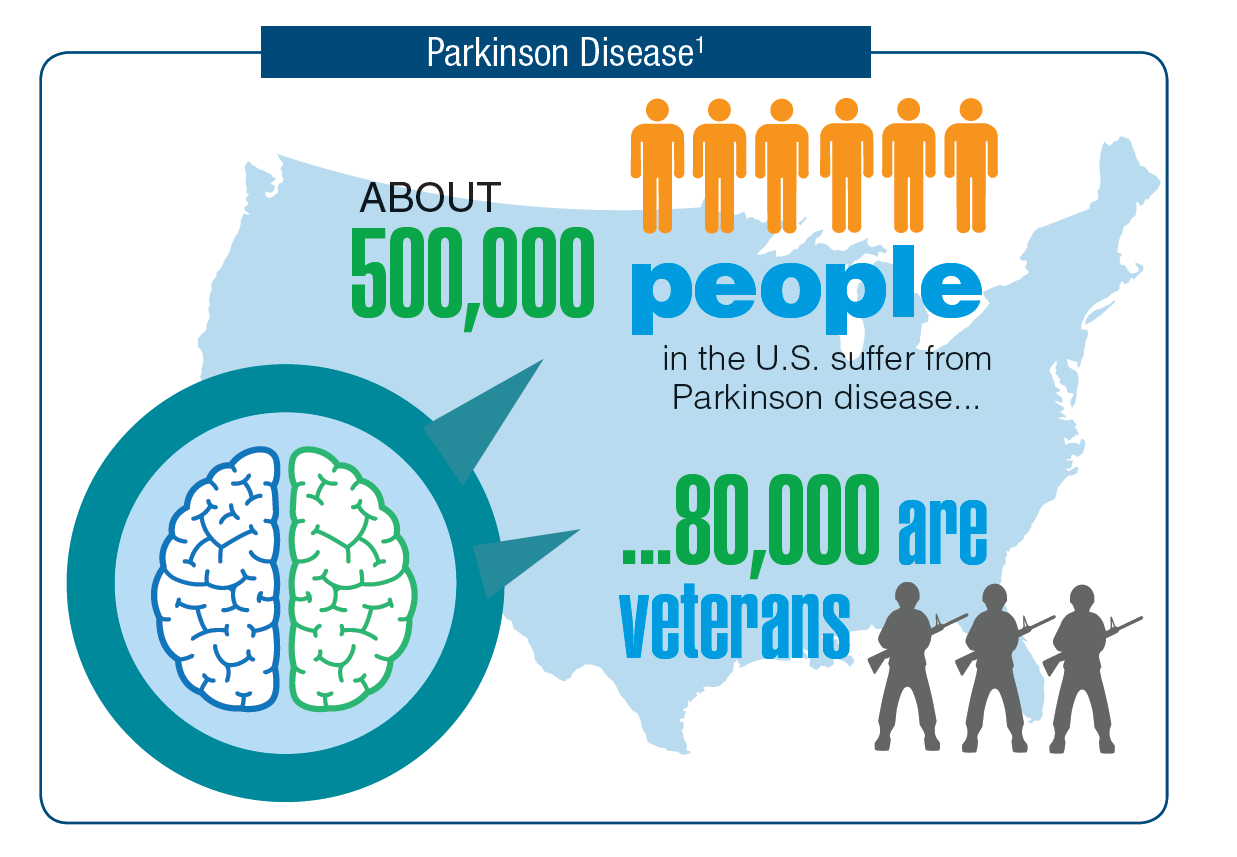
Veterans who were exposed to Agent Orange and go on to develop Parkinson disease are eligible for benefits without proving service connection. About 16% of the half million Americans with Parkinson disease are veterans.
Veterans also face increased risk of dementia. There is evidence that Parkinson disease, posttraumatic stress disorder, and traumatic brain injuries are all risk factors for developing dementia.

Click here to read the digital edition.
Neurologic disorders seem to impact veterans disproportionately. Multiple sclerosis, Parkinson disease, dementia, epilepsy, and other less common neurologic disorders require a high-level of care for veterans.
Multiple sclerosis is often diagnosed when patients are in their 20s or 30s. Typically, MS affects women more than men at a rate up to 3 times higher, and studies have shown that race and geography also may play a role in the risk of acquiring MS. Rates of MS in Vietnam era veterans were higher than those of veterans of World War II and the Korean War. That trend continued for Army and Air Force Gulf War veterans.
Veterans who were exposed to Agent Orange and go on to develop Parkinson disease are eligible for benefits without proving service connection. About 16% of the half million Americans with Parkinson disease are veterans.
Veterans also face increased risk of dementia. There is evidence that Parkinson disease, posttraumatic stress disorder, and traumatic brain injuries are all risk factors for developing dementia.
Click here to read the digital edition.
Neurologic disorders seem to impact veterans disproportionately. Multiple sclerosis, Parkinson disease, dementia, epilepsy, and other less common neurologic disorders require a high-level of care for veterans.
Multiple sclerosis is often diagnosed when patients are in their 20s or 30s. Typically, MS affects women more than men at a rate up to 3 times higher, and studies have shown that race and geography also may play a role in the risk of acquiring MS. Rates of MS in Vietnam era veterans were higher than those of veterans of World War II and the Korean War. That trend continued for Army and Air Force Gulf War veterans.
Veterans who were exposed to Agent Orange and go on to develop Parkinson disease are eligible for benefits without proving service connection. About 16% of the half million Americans with Parkinson disease are veterans.
Veterans also face increased risk of dementia. There is evidence that Parkinson disease, posttraumatic stress disorder, and traumatic brain injuries are all risk factors for developing dementia.
Click here to read the digital edition.
Traumatic Brain Injury Federal Health Data Trends (FULL)
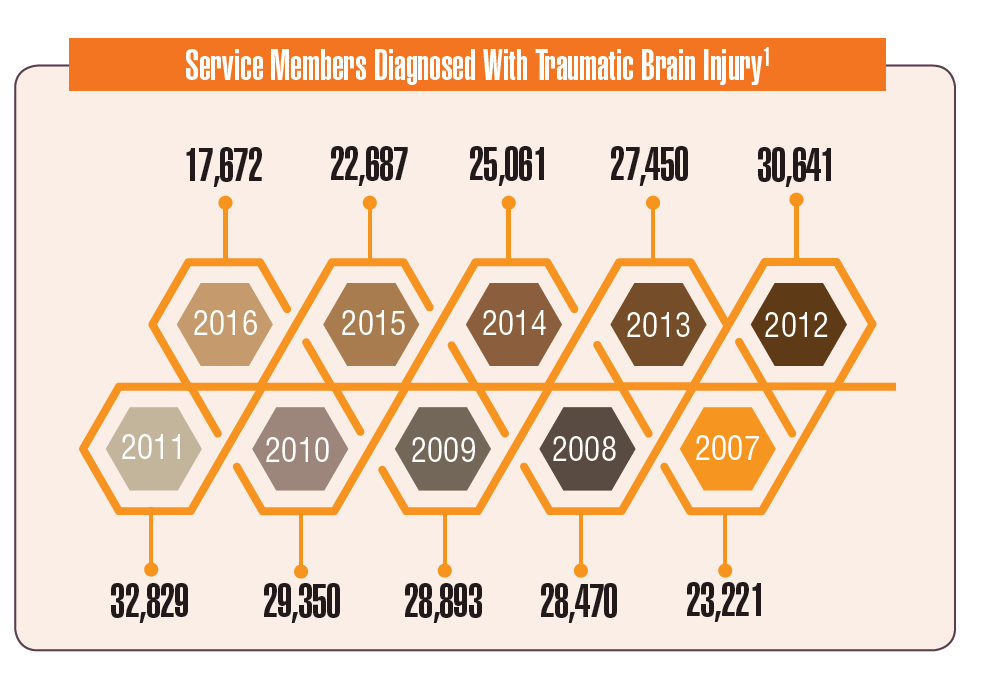
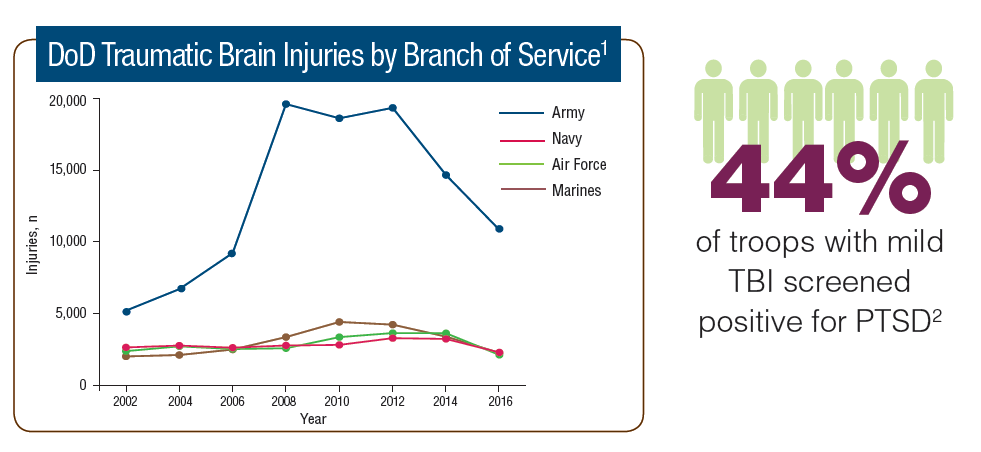
Traumatic brain injury (TBI) is now recognized as a significant health issue that impacts both activeduty service members and veterans. Blast injuries sustained in operations in Iraq and Afghanistan have led to a rising incidence of TBI in the DoD and VA patient populations.
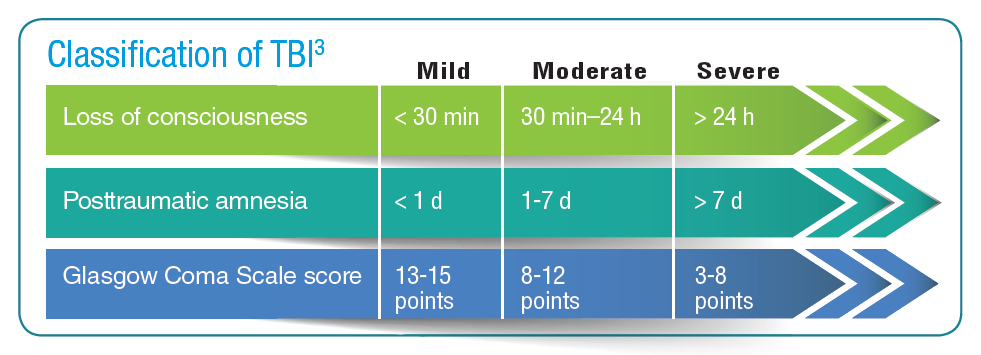
A TBI can result from a significant injury or even during day-to-day activities. Mild TBIs, also known as a concussion, typically result in short-term impacts. However, increasing evidence suggests that multiple mild TBIs can have a cumulative effect and longer term impact on patients. Moderate, severe, and penetrating TBIs can have a more serious impact on the patient.
Active-duty and reserve service members are at increased risk for TBI compared with civilians. Not only do combat operations increase the chance of blast-related injuries, but active-duty service members are often drawn from at-risk populations: men between the ages of 18 to 24 years are at greatest risk for TBI. Studies have suggested that between 10% and 20% of post-9/11 veterans experienced a mild-to-moderate TBI.
Posttraumatic stress disorder (PTSD) and TBI are closely linked. Nearly half of the active-duty service members with mild TBI also screen positive for PTSD. For clinicians, diagnosis remains a challenge because of an overlap in symptoms.

Click here to read the digital edition.
Traumatic brain injury (TBI) is now recognized as a significant health issue that impacts both activeduty service members and veterans. Blast injuries sustained in operations in Iraq and Afghanistan have led to a rising incidence of TBI in the DoD and VA patient populations.
A TBI can result from a significant injury or even during day-to-day activities. Mild TBIs, also known as a concussion, typically result in short-term impacts. However, increasing evidence suggests that multiple mild TBIs can have a cumulative effect and longer term impact on patients. Moderate, severe, and penetrating TBIs can have a more serious impact on the patient.
Active-duty and reserve service members are at increased risk for TBI compared with civilians. Not only do combat operations increase the chance of blast-related injuries, but active-duty service members are often drawn from at-risk populations: men between the ages of 18 to 24 years are at greatest risk for TBI. Studies have suggested that between 10% and 20% of post-9/11 veterans experienced a mild-to-moderate TBI.
Posttraumatic stress disorder (PTSD) and TBI are closely linked. Nearly half of the active-duty service members with mild TBI also screen positive for PTSD. For clinicians, diagnosis remains a challenge because of an overlap in symptoms.
Click here to read the digital edition.
Traumatic brain injury (TBI) is now recognized as a significant health issue that impacts both activeduty service members and veterans. Blast injuries sustained in operations in Iraq and Afghanistan have led to a rising incidence of TBI in the DoD and VA patient populations.
A TBI can result from a significant injury or even during day-to-day activities. Mild TBIs, also known as a concussion, typically result in short-term impacts. However, increasing evidence suggests that multiple mild TBIs can have a cumulative effect and longer term impact on patients. Moderate, severe, and penetrating TBIs can have a more serious impact on the patient.
Active-duty and reserve service members are at increased risk for TBI compared with civilians. Not only do combat operations increase the chance of blast-related injuries, but active-duty service members are often drawn from at-risk populations: men between the ages of 18 to 24 years are at greatest risk for TBI. Studies have suggested that between 10% and 20% of post-9/11 veterans experienced a mild-to-moderate TBI.
Posttraumatic stress disorder (PTSD) and TBI are closely linked. Nearly half of the active-duty service members with mild TBI also screen positive for PTSD. For clinicians, diagnosis remains a challenge because of an overlap in symptoms.
Click here to read the digital edition.
Women’s Health Federal Health Data Trends (FULL)
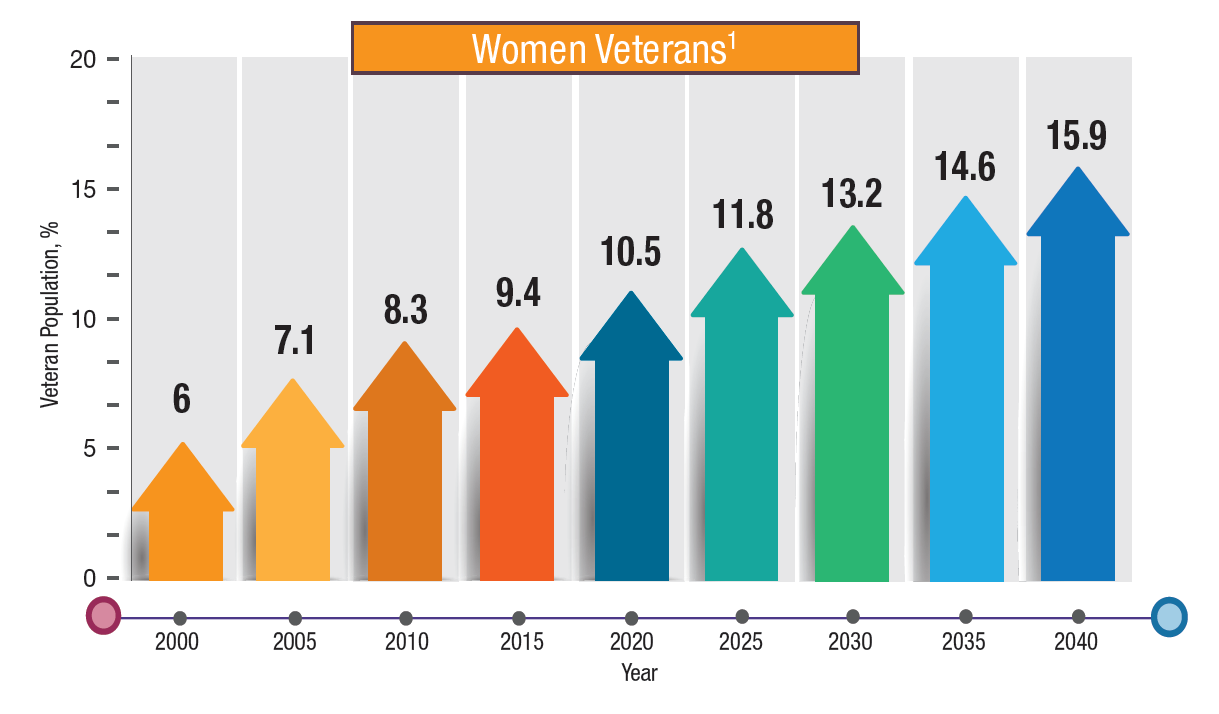
The number and impact of active-duty and veteran women continue to grow, as do their health care needs. For many years, the health care needs of women received little attention in the DoD and VA, but that is finally changing. Women now make up nearly 10% of the veteran population, a rise of more than 80% since 2005. By 2043, the VA projects that women will make up 16.3% of all veterans. The total population of women veterans is expected to continue to increase by about 18,000 women per year over the next 10 years.
The demographics of women veterans differ from that of their male counterparts in important ways. For example, 25% of women veterans served only during peace times, while 56% served during the post-9/11 era. Not surprisingly then, women veterans are much younger than male veterans, with a median age of 49 years. Nineteen percent of women veterans were African American, which is much higher than the percentage for male veterans. However Hispanic and Asian women are underrepresented when compared with men. Women veterans were more likely to have ever married than nonveteran women: 84% were currently married, divorced, widowed, or separated compared with 72% of nonveteran women.
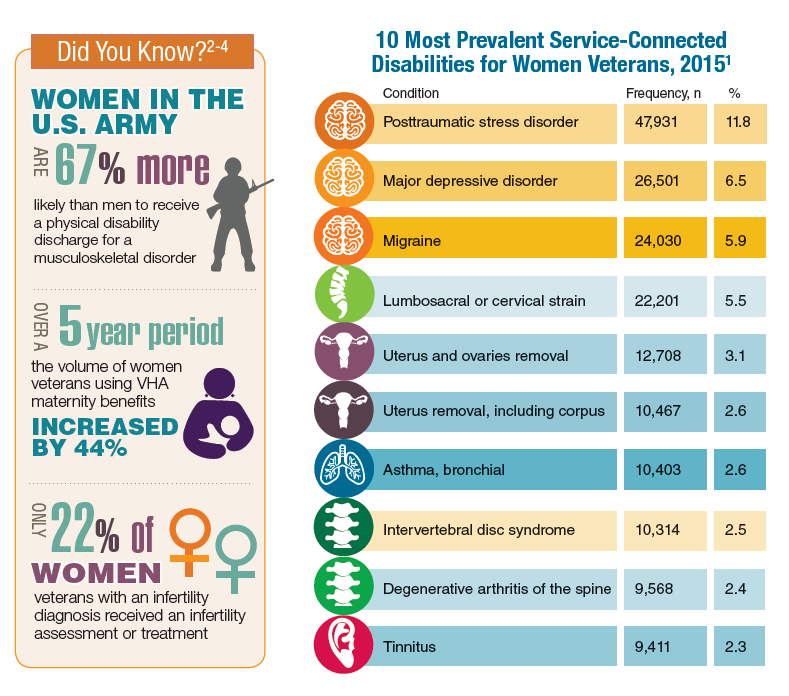
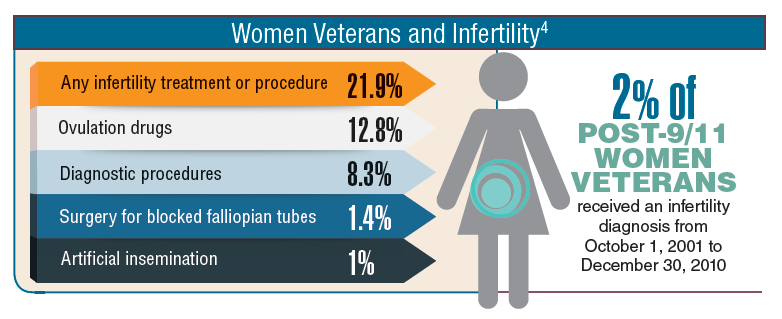
Many of the health care needs of women veterans mirror that of their male counterparts. The most common service-connected disabilities for women are posttraumatic stress disorder, depression, and musculoskeletal pain. However, the VHA and DoD are moving to provide maternity and infertility treatment to active-duty and veteran women.
Click here to read the digital edition.
The number and impact of active-duty and veteran women continue to grow, as do their health care needs. For many years, the health care needs of women received little attention in the DoD and VA, but that is finally changing. Women now make up nearly 10% of the veteran population, a rise of more than 80% since 2005. By 2043, the VA projects that women will make up 16.3% of all veterans. The total population of women veterans is expected to continue to increase by about 18,000 women per year over the next 10 years.
The demographics of women veterans differ from that of their male counterparts in important ways. For example, 25% of women veterans served only during peace times, while 56% served during the post-9/11 era. Not surprisingly then, women veterans are much younger than male veterans, with a median age of 49 years. Nineteen percent of women veterans were African American, which is much higher than the percentage for male veterans. However Hispanic and Asian women are underrepresented when compared with men. Women veterans were more likely to have ever married than nonveteran women: 84% were currently married, divorced, widowed, or separated compared with 72% of nonveteran women.
Many of the health care needs of women veterans mirror that of their male counterparts. The most common service-connected disabilities for women are posttraumatic stress disorder, depression, and musculoskeletal pain. However, the VHA and DoD are moving to provide maternity and infertility treatment to active-duty and veteran women.
Click here to read the digital edition.
The number and impact of active-duty and veteran women continue to grow, as do their health care needs. For many years, the health care needs of women received little attention in the DoD and VA, but that is finally changing. Women now make up nearly 10% of the veteran population, a rise of more than 80% since 2005. By 2043, the VA projects that women will make up 16.3% of all veterans. The total population of women veterans is expected to continue to increase by about 18,000 women per year over the next 10 years.
The demographics of women veterans differ from that of their male counterparts in important ways. For example, 25% of women veterans served only during peace times, while 56% served during the post-9/11 era. Not surprisingly then, women veterans are much younger than male veterans, with a median age of 49 years. Nineteen percent of women veterans were African American, which is much higher than the percentage for male veterans. However Hispanic and Asian women are underrepresented when compared with men. Women veterans were more likely to have ever married than nonveteran women: 84% were currently married, divorced, widowed, or separated compared with 72% of nonveteran women.
Many of the health care needs of women veterans mirror that of their male counterparts. The most common service-connected disabilities for women are posttraumatic stress disorder, depression, and musculoskeletal pain. However, the VHA and DoD are moving to provide maternity and infertility treatment to active-duty and veteran women.
Click here to read the digital edition.
How to “Nudge” Patients to Screen for HIV
What’s the best way to encourage patients to get screened for HIV? Money is a time-honored effective incentive, but researchers from University of California say the default option may be even better. They conducted, to their knowledge, the first head-to-head study of 2 types of behavioral economics interventions (cash incentives vs opt-out) in any health behavior context. The working hypothesis was based on “nudge theory,” a concept in behavioral science, political theory, and economics that says using positive reinforcement and indirect suggestions can influence behavior and decision making.
In the study, patients aged 13 to 64 years were told the emergency department was offering rapid screening HIV tests, with results available within 2 hours. Then each patient was given a test offer: opt-in (“You can let me, your nurse, or your doctor know if you’d like a test today”); active choice (“Would you like a test today?”); or opt-out (“You will be tested unless you decline.”) Patients assigned to a positive monetary incentive were told “To encourage testing today we are offering a $1 (or $5 or $10) cash incentive.”
Of 8,715 patients, 4,831 (55%) accepted an HIV test. Those offered no monetary incentive accepted 52% of test offers. The $1 offer did not increase test acceptance, but the $5 and $10 offers increased acceptance rates by 10.5 and 15 percentage points, respectively. Active-choice increased acceptance by 11.5 percentage points compared with that of opt-in offers.
However, opt-out testing—essentially a default option—had the largest effect, increasing acceptance by 24 percentage points. The next most effective was the $10 incentive.
The researchers say the effects were consistent across all levels of patient risk of infection, although the effects were somewhat attenuated when defaults and incentives were used together. In general, higher risk patients tested at higher rates than did lower risk patients.
Defaults have been “understudied in medicine,” the researchers say. The study not only reaffirms that behavioral economics “nudges” work, but also that “small interventions can have significant effects.” Moreover, the finding that moving from opt-in to opt-out testing influenced behavior more than even the largest incentive reinforces the notion that “medicine is not just a transaction, and what we say to patients matters.”
Source:
Montoy JCC, Dow WH, Kaplan BC. PLoS One. 2018;13(7):e0199833.
doi: 10.1371/journal.pone.0199833.
What’s the best way to encourage patients to get screened for HIV? Money is a time-honored effective incentive, but researchers from University of California say the default option may be even better. They conducted, to their knowledge, the first head-to-head study of 2 types of behavioral economics interventions (cash incentives vs opt-out) in any health behavior context. The working hypothesis was based on “nudge theory,” a concept in behavioral science, political theory, and economics that says using positive reinforcement and indirect suggestions can influence behavior and decision making.
In the study, patients aged 13 to 64 years were told the emergency department was offering rapid screening HIV tests, with results available within 2 hours. Then each patient was given a test offer: opt-in (“You can let me, your nurse, or your doctor know if you’d like a test today”); active choice (“Would you like a test today?”); or opt-out (“You will be tested unless you decline.”) Patients assigned to a positive monetary incentive were told “To encourage testing today we are offering a $1 (or $5 or $10) cash incentive.”
Of 8,715 patients, 4,831 (55%) accepted an HIV test. Those offered no monetary incentive accepted 52% of test offers. The $1 offer did not increase test acceptance, but the $5 and $10 offers increased acceptance rates by 10.5 and 15 percentage points, respectively. Active-choice increased acceptance by 11.5 percentage points compared with that of opt-in offers.
However, opt-out testing—essentially a default option—had the largest effect, increasing acceptance by 24 percentage points. The next most effective was the $10 incentive.
The researchers say the effects were consistent across all levels of patient risk of infection, although the effects were somewhat attenuated when defaults and incentives were used together. In general, higher risk patients tested at higher rates than did lower risk patients.
Defaults have been “understudied in medicine,” the researchers say. The study not only reaffirms that behavioral economics “nudges” work, but also that “small interventions can have significant effects.” Moreover, the finding that moving from opt-in to opt-out testing influenced behavior more than even the largest incentive reinforces the notion that “medicine is not just a transaction, and what we say to patients matters.”
Source:
Montoy JCC, Dow WH, Kaplan BC. PLoS One. 2018;13(7):e0199833.
doi: 10.1371/journal.pone.0199833.
What’s the best way to encourage patients to get screened for HIV? Money is a time-honored effective incentive, but researchers from University of California say the default option may be even better. They conducted, to their knowledge, the first head-to-head study of 2 types of behavioral economics interventions (cash incentives vs opt-out) in any health behavior context. The working hypothesis was based on “nudge theory,” a concept in behavioral science, political theory, and economics that says using positive reinforcement and indirect suggestions can influence behavior and decision making.
In the study, patients aged 13 to 64 years were told the emergency department was offering rapid screening HIV tests, with results available within 2 hours. Then each patient was given a test offer: opt-in (“You can let me, your nurse, or your doctor know if you’d like a test today”); active choice (“Would you like a test today?”); or opt-out (“You will be tested unless you decline.”) Patients assigned to a positive monetary incentive were told “To encourage testing today we are offering a $1 (or $5 or $10) cash incentive.”
Of 8,715 patients, 4,831 (55%) accepted an HIV test. Those offered no monetary incentive accepted 52% of test offers. The $1 offer did not increase test acceptance, but the $5 and $10 offers increased acceptance rates by 10.5 and 15 percentage points, respectively. Active-choice increased acceptance by 11.5 percentage points compared with that of opt-in offers.
However, opt-out testing—essentially a default option—had the largest effect, increasing acceptance by 24 percentage points. The next most effective was the $10 incentive.
The researchers say the effects were consistent across all levels of patient risk of infection, although the effects were somewhat attenuated when defaults and incentives were used together. In general, higher risk patients tested at higher rates than did lower risk patients.
Defaults have been “understudied in medicine,” the researchers say. The study not only reaffirms that behavioral economics “nudges” work, but also that “small interventions can have significant effects.” Moreover, the finding that moving from opt-in to opt-out testing influenced behavior more than even the largest incentive reinforces the notion that “medicine is not just a transaction, and what we say to patients matters.”
Source:
Montoy JCC, Dow WH, Kaplan BC. PLoS One. 2018;13(7):e0199833.
doi: 10.1371/journal.pone.0199833.
Respiratory illness is the most common pediatric emergency in ambulatory settings
followed by psychiatric and behavioral illness, seizures, and syncope, according to results published July 20 in Pediatrics.
Investigators conducted a retrospective observational study of data from the Indianapolis emergency medical services (EMS) system between Jan. 1, 2012, and Dec. 31, 2014. All patients younger than 18 years were eligible.
Of 38,841 pediatric EMS transports in the Indianapolis metropolitan area during the 3-year period, fewer than 1% (322) were verified as originating from an ambulatory practice, reported Matthew L. Yuknis, MD, and his coauthors at Indiana University, Indianapolis. Respiratory distress was the most common emergency (58%), followed by psychiatric and behavioral illness (6%), seizure (6%), and syncope (5%).
The most common interventions were use of supplemental oxygen (27%), albuterol (26%), and intravascular access (11%). The most common critical care interventions were administration of fluid bolus (2%), benzodiazepine (2%), or racemic or intramuscular epinephrine (1%). None required use of an artificial airway, cardiopulmonary resuscitation, intraosseous access, or bag mask ventilation, Dr. Yuknis and his colleagues said.
The average time from call to on-scene arrival was 6 minutes (ranging from less than 1 to 15 minutes). The average patient transport time was 13 minutes (ranging from less than 1 to 38 minutes). The average annual frequency of pediatric outpatient emergencies was 42 emergencies per 100,000 people under 18 years of age. Lower socioeconomic status was correlated with increased frequency of emergencies in ambulatory settings, the authors reported.
“These findings update and clarify existing literature with regard to the frequency of pediatric emergencies in the ambulatory setting, the conditions these patients present with, and the use of EMS data to define these events,” the authors wrote. Additionally, the findings can be used to “inform future decisions regarding necessary equipment and procedures.”
No relevant financial disclosures were reported. There was no external funding.
SOURCE: Yuknis M et al. Pediatrics. 2018. doi: 10.1542/peds.2017-3082.
followed by psychiatric and behavioral illness, seizures, and syncope, according to results published July 20 in Pediatrics.
Investigators conducted a retrospective observational study of data from the Indianapolis emergency medical services (EMS) system between Jan. 1, 2012, and Dec. 31, 2014. All patients younger than 18 years were eligible.
Of 38,841 pediatric EMS transports in the Indianapolis metropolitan area during the 3-year period, fewer than 1% (322) were verified as originating from an ambulatory practice, reported Matthew L. Yuknis, MD, and his coauthors at Indiana University, Indianapolis. Respiratory distress was the most common emergency (58%), followed by psychiatric and behavioral illness (6%), seizure (6%), and syncope (5%).
The most common interventions were use of supplemental oxygen (27%), albuterol (26%), and intravascular access (11%). The most common critical care interventions were administration of fluid bolus (2%), benzodiazepine (2%), or racemic or intramuscular epinephrine (1%). None required use of an artificial airway, cardiopulmonary resuscitation, intraosseous access, or bag mask ventilation, Dr. Yuknis and his colleagues said.
The average time from call to on-scene arrival was 6 minutes (ranging from less than 1 to 15 minutes). The average patient transport time was 13 minutes (ranging from less than 1 to 38 minutes). The average annual frequency of pediatric outpatient emergencies was 42 emergencies per 100,000 people under 18 years of age. Lower socioeconomic status was correlated with increased frequency of emergencies in ambulatory settings, the authors reported.
“These findings update and clarify existing literature with regard to the frequency of pediatric emergencies in the ambulatory setting, the conditions these patients present with, and the use of EMS data to define these events,” the authors wrote. Additionally, the findings can be used to “inform future decisions regarding necessary equipment and procedures.”
No relevant financial disclosures were reported. There was no external funding.
SOURCE: Yuknis M et al. Pediatrics. 2018. doi: 10.1542/peds.2017-3082.
followed by psychiatric and behavioral illness, seizures, and syncope, according to results published July 20 in Pediatrics.
Investigators conducted a retrospective observational study of data from the Indianapolis emergency medical services (EMS) system between Jan. 1, 2012, and Dec. 31, 2014. All patients younger than 18 years were eligible.
Of 38,841 pediatric EMS transports in the Indianapolis metropolitan area during the 3-year period, fewer than 1% (322) were verified as originating from an ambulatory practice, reported Matthew L. Yuknis, MD, and his coauthors at Indiana University, Indianapolis. Respiratory distress was the most common emergency (58%), followed by psychiatric and behavioral illness (6%), seizure (6%), and syncope (5%).
The most common interventions were use of supplemental oxygen (27%), albuterol (26%), and intravascular access (11%). The most common critical care interventions were administration of fluid bolus (2%), benzodiazepine (2%), or racemic or intramuscular epinephrine (1%). None required use of an artificial airway, cardiopulmonary resuscitation, intraosseous access, or bag mask ventilation, Dr. Yuknis and his colleagues said.
The average time from call to on-scene arrival was 6 minutes (ranging from less than 1 to 15 minutes). The average patient transport time was 13 minutes (ranging from less than 1 to 38 minutes). The average annual frequency of pediatric outpatient emergencies was 42 emergencies per 100,000 people under 18 years of age. Lower socioeconomic status was correlated with increased frequency of emergencies in ambulatory settings, the authors reported.
“These findings update and clarify existing literature with regard to the frequency of pediatric emergencies in the ambulatory setting, the conditions these patients present with, and the use of EMS data to define these events,” the authors wrote. Additionally, the findings can be used to “inform future decisions regarding necessary equipment and procedures.”
No relevant financial disclosures were reported. There was no external funding.
SOURCE: Yuknis M et al. Pediatrics. 2018. doi: 10.1542/peds.2017-3082.
FROM PEDIATRICS
Key clinical point: Respiratory illness was the most common pediatric emergency in ambulatory settings.
Major finding: Among pediatric emergency medical services from ambulatory settings, 58% were caused by respiratory illness.
Study details: A retrospective observational study of 38,841 EMS transports in the Indianapolis metropolitan area over 3 years.
Disclosures: No relevant financial disclosures were reported. There was no external funding.
Source: Yuknis M et al. Pediatrics. 2018. doi: 10.1542/peds.2017-3082.