User login
New pediatric therapies show promise for influenza, multidrug-resistant pathogens
ORLANDO – John S. Bradley, MD, said at the annual meeting of the American Academy of Pediatrics.
Dr. Bradley, director of the division of infectious diseases at Rady Children’s Hospital–San Diego, discussed a therapy for influenza, baloxavir, which was recently approved as a fast-acting single-dose medication and currently is under study in children. Also, a recent double-blind, phase 3 trial in the New England Journal of Medicine recruited patients as young as 12 years old. In the study, patients in the intervention group resolved their fever in median 25 hours, compared with 42 hours in the placebo group. Baloxavir better reduced viral load at day 2, compared with oseltamivir and placebo, but there was a similar alleviation of symptoms between both groups. There was a greater incidence of nausea and vomiting among the oseltamivir group, while the baloxavir group had a higher rate of diarrhea (N Engl J Med 2018;379:913-23).
However, Dr. Bradley noted baloxavir is much more expensive than oseltamivir, which may not justify the better tolerance of the drug for influenza treatment.
You don’t get better with it faster, so I’m not going to be recommending you all run to baloxavir this flu season for kids 12 years of age and older,” Dr. Bradley said. “I think oseltamivir is still fine, unless we end up with oseltamivir resistance.”
Solithromycin, an intravenous and oral fluoroketolide, has shown promising results against gram-positive and gram-negative pathogens for community-acquired pneumonia and other infections. During the drug’s study period, Cempra sold solithromycin to Melinta. However, one trial showed elevated liver functions in a higher number of patients than expected, and the Food and Drug Administration asked Melinta to conduct additional studies. Investigations on solithromycin have currently stopped until Melinta secures funding. “Until they get better resources, this particular drug is on hold, but you’ll see it again, I’m sure,” said Dr. Bradley, who also is professor and chief of the division of infectious diseases at the University of California, San Diego.
Dr. Bradley also discussed the efficacy of tedizolid, a protein synthesis inhibitor similar to linezolid approved in adults for the treatment of skin infections. He noted tedizolid is more active than linezolid, but the treatment course is a shorter dose for a shorter amount of time. Compared with linezolid, which can cause thrombocytopenia or neutropenia if taken for more than 10 days to 14 days, there also are fewer side effects.
“The tedizolid is much, much safer,” Dr. Bradley said, who added that trials for efficacy of tedizolid are currently underway in pediatric patients. “We’re hoping that will end up being the pediatric oxazolidinone.”
Other investigative therapies approved for adults and under study for use in children include ceftazidime/avibactam for treatment of urinary tract and complicated intra-abdominal infections, which is effective against meropenem-resistant Enterobacteriaceae and resistant Escherichia coli with extended-spectrum beta-lactamases (ESBL); ceftolozane/tazobactam has also been approved for adults, is pending approval in pediatric patients, and is active against ESBLs such as Pseudomonas; and meropenem/vaborbactam, which is active against Klebsiella pneumoniae carbapenemase (KPC)–producing isolates. Plazomicin, an aminoglycoside similar to gentamicin used to treat KPC-producing isolates, is stable against enzymes that degrade gentamicin and tobramycin.
Therapies currently under study for adults and being considered for children include imipenem/relebactam for treatment against E. coli, Enterobacter species, and KPC-producing isolates, and cefiderocol, a siderophore cephalosporin antibiotic – commonly described as a “Trojan horse” antibiotic because it binds to iron and is actively transported into the organism – is effective against Pseudomonas and has finished phase 2 trials in adults, with researchers looking to do single-dose trials in children, Dr. Bradley noted.
More experimentally, phage therapy for multidrug-resistant Acinetobacter baumannii proved effective in a 68-year-old patient with necrotizing pancreatitis who continued to deteriorate over a 4-month period despite multiple courses of antibiotics and attempted drainage of a pancreatic pseudocyst. Researchers selected a phage-specific bacterium with specificity for A. baumannii and cured him. “This is like science fiction,” Dr. Bradley said.
Dr. Bradley reported no relevant conflicts of interest.
ORLANDO – John S. Bradley, MD, said at the annual meeting of the American Academy of Pediatrics.
Dr. Bradley, director of the division of infectious diseases at Rady Children’s Hospital–San Diego, discussed a therapy for influenza, baloxavir, which was recently approved as a fast-acting single-dose medication and currently is under study in children. Also, a recent double-blind, phase 3 trial in the New England Journal of Medicine recruited patients as young as 12 years old. In the study, patients in the intervention group resolved their fever in median 25 hours, compared with 42 hours in the placebo group. Baloxavir better reduced viral load at day 2, compared with oseltamivir and placebo, but there was a similar alleviation of symptoms between both groups. There was a greater incidence of nausea and vomiting among the oseltamivir group, while the baloxavir group had a higher rate of diarrhea (N Engl J Med 2018;379:913-23).
However, Dr. Bradley noted baloxavir is much more expensive than oseltamivir, which may not justify the better tolerance of the drug for influenza treatment.
You don’t get better with it faster, so I’m not going to be recommending you all run to baloxavir this flu season for kids 12 years of age and older,” Dr. Bradley said. “I think oseltamivir is still fine, unless we end up with oseltamivir resistance.”
Solithromycin, an intravenous and oral fluoroketolide, has shown promising results against gram-positive and gram-negative pathogens for community-acquired pneumonia and other infections. During the drug’s study period, Cempra sold solithromycin to Melinta. However, one trial showed elevated liver functions in a higher number of patients than expected, and the Food and Drug Administration asked Melinta to conduct additional studies. Investigations on solithromycin have currently stopped until Melinta secures funding. “Until they get better resources, this particular drug is on hold, but you’ll see it again, I’m sure,” said Dr. Bradley, who also is professor and chief of the division of infectious diseases at the University of California, San Diego.
Dr. Bradley also discussed the efficacy of tedizolid, a protein synthesis inhibitor similar to linezolid approved in adults for the treatment of skin infections. He noted tedizolid is more active than linezolid, but the treatment course is a shorter dose for a shorter amount of time. Compared with linezolid, which can cause thrombocytopenia or neutropenia if taken for more than 10 days to 14 days, there also are fewer side effects.
“The tedizolid is much, much safer,” Dr. Bradley said, who added that trials for efficacy of tedizolid are currently underway in pediatric patients. “We’re hoping that will end up being the pediatric oxazolidinone.”
Other investigative therapies approved for adults and under study for use in children include ceftazidime/avibactam for treatment of urinary tract and complicated intra-abdominal infections, which is effective against meropenem-resistant Enterobacteriaceae and resistant Escherichia coli with extended-spectrum beta-lactamases (ESBL); ceftolozane/tazobactam has also been approved for adults, is pending approval in pediatric patients, and is active against ESBLs such as Pseudomonas; and meropenem/vaborbactam, which is active against Klebsiella pneumoniae carbapenemase (KPC)–producing isolates. Plazomicin, an aminoglycoside similar to gentamicin used to treat KPC-producing isolates, is stable against enzymes that degrade gentamicin and tobramycin.
Therapies currently under study for adults and being considered for children include imipenem/relebactam for treatment against E. coli, Enterobacter species, and KPC-producing isolates, and cefiderocol, a siderophore cephalosporin antibiotic – commonly described as a “Trojan horse” antibiotic because it binds to iron and is actively transported into the organism – is effective against Pseudomonas and has finished phase 2 trials in adults, with researchers looking to do single-dose trials in children, Dr. Bradley noted.
More experimentally, phage therapy for multidrug-resistant Acinetobacter baumannii proved effective in a 68-year-old patient with necrotizing pancreatitis who continued to deteriorate over a 4-month period despite multiple courses of antibiotics and attempted drainage of a pancreatic pseudocyst. Researchers selected a phage-specific bacterium with specificity for A. baumannii and cured him. “This is like science fiction,” Dr. Bradley said.
Dr. Bradley reported no relevant conflicts of interest.
ORLANDO – John S. Bradley, MD, said at the annual meeting of the American Academy of Pediatrics.
Dr. Bradley, director of the division of infectious diseases at Rady Children’s Hospital–San Diego, discussed a therapy for influenza, baloxavir, which was recently approved as a fast-acting single-dose medication and currently is under study in children. Also, a recent double-blind, phase 3 trial in the New England Journal of Medicine recruited patients as young as 12 years old. In the study, patients in the intervention group resolved their fever in median 25 hours, compared with 42 hours in the placebo group. Baloxavir better reduced viral load at day 2, compared with oseltamivir and placebo, but there was a similar alleviation of symptoms between both groups. There was a greater incidence of nausea and vomiting among the oseltamivir group, while the baloxavir group had a higher rate of diarrhea (N Engl J Med 2018;379:913-23).
However, Dr. Bradley noted baloxavir is much more expensive than oseltamivir, which may not justify the better tolerance of the drug for influenza treatment.
You don’t get better with it faster, so I’m not going to be recommending you all run to baloxavir this flu season for kids 12 years of age and older,” Dr. Bradley said. “I think oseltamivir is still fine, unless we end up with oseltamivir resistance.”
Solithromycin, an intravenous and oral fluoroketolide, has shown promising results against gram-positive and gram-negative pathogens for community-acquired pneumonia and other infections. During the drug’s study period, Cempra sold solithromycin to Melinta. However, one trial showed elevated liver functions in a higher number of patients than expected, and the Food and Drug Administration asked Melinta to conduct additional studies. Investigations on solithromycin have currently stopped until Melinta secures funding. “Until they get better resources, this particular drug is on hold, but you’ll see it again, I’m sure,” said Dr. Bradley, who also is professor and chief of the division of infectious diseases at the University of California, San Diego.
Dr. Bradley also discussed the efficacy of tedizolid, a protein synthesis inhibitor similar to linezolid approved in adults for the treatment of skin infections. He noted tedizolid is more active than linezolid, but the treatment course is a shorter dose for a shorter amount of time. Compared with linezolid, which can cause thrombocytopenia or neutropenia if taken for more than 10 days to 14 days, there also are fewer side effects.
“The tedizolid is much, much safer,” Dr. Bradley said, who added that trials for efficacy of tedizolid are currently underway in pediatric patients. “We’re hoping that will end up being the pediatric oxazolidinone.”
Other investigative therapies approved for adults and under study for use in children include ceftazidime/avibactam for treatment of urinary tract and complicated intra-abdominal infections, which is effective against meropenem-resistant Enterobacteriaceae and resistant Escherichia coli with extended-spectrum beta-lactamases (ESBL); ceftolozane/tazobactam has also been approved for adults, is pending approval in pediatric patients, and is active against ESBLs such as Pseudomonas; and meropenem/vaborbactam, which is active against Klebsiella pneumoniae carbapenemase (KPC)–producing isolates. Plazomicin, an aminoglycoside similar to gentamicin used to treat KPC-producing isolates, is stable against enzymes that degrade gentamicin and tobramycin.
Therapies currently under study for adults and being considered for children include imipenem/relebactam for treatment against E. coli, Enterobacter species, and KPC-producing isolates, and cefiderocol, a siderophore cephalosporin antibiotic – commonly described as a “Trojan horse” antibiotic because it binds to iron and is actively transported into the organism – is effective against Pseudomonas and has finished phase 2 trials in adults, with researchers looking to do single-dose trials in children, Dr. Bradley noted.
More experimentally, phage therapy for multidrug-resistant Acinetobacter baumannii proved effective in a 68-year-old patient with necrotizing pancreatitis who continued to deteriorate over a 4-month period despite multiple courses of antibiotics and attempted drainage of a pancreatic pseudocyst. Researchers selected a phage-specific bacterium with specificity for A. baumannii and cured him. “This is like science fiction,” Dr. Bradley said.
Dr. Bradley reported no relevant conflicts of interest.
EXPERT ANALYSIS FROM AAP 18
Investigation Into New Antimalarial Drug Begins
In 2016, a staggering 216 million people developed malaria, and 445,000 died—primarily children in sub-Saharan Africa. But a new first-in-human study sponsored by the National Institute of Allergy and Infectious Disease may help reduce the numbers of future victims.
Enrollment has begun in a phase I trial to test the safety of DM1157, an investigational modified form of chloroquine. Many strains of Plasmodium falciparum are now resistant to chloroquine. In fact, the parasites can expel the drug before it can affect them. Like chloroquine, DM1157 interferes with the parasite’s metabolism, but it also inhibits the parasite’s ability to expel the drug.
The study will enroll up to 104 healthy volunteers aged 18-45 years. One group will fast overnight and then receive either a single dose of the experimental drug at 1 of 7 dosage levels or a placebo. A second group also will fast and receive 1 dose at 1 of 4 dosage levels and repeat the routine for 2 more consecutive days. A third group will be given either a single 300-mg dose or placebo after eating a high-fat meal.
The study is expected to be completed by June 2019.
In 2016, a staggering 216 million people developed malaria, and 445,000 died—primarily children in sub-Saharan Africa. But a new first-in-human study sponsored by the National Institute of Allergy and Infectious Disease may help reduce the numbers of future victims.
Enrollment has begun in a phase I trial to test the safety of DM1157, an investigational modified form of chloroquine. Many strains of Plasmodium falciparum are now resistant to chloroquine. In fact, the parasites can expel the drug before it can affect them. Like chloroquine, DM1157 interferes with the parasite’s metabolism, but it also inhibits the parasite’s ability to expel the drug.
The study will enroll up to 104 healthy volunteers aged 18-45 years. One group will fast overnight and then receive either a single dose of the experimental drug at 1 of 7 dosage levels or a placebo. A second group also will fast and receive 1 dose at 1 of 4 dosage levels and repeat the routine for 2 more consecutive days. A third group will be given either a single 300-mg dose or placebo after eating a high-fat meal.
The study is expected to be completed by June 2019.
In 2016, a staggering 216 million people developed malaria, and 445,000 died—primarily children in sub-Saharan Africa. But a new first-in-human study sponsored by the National Institute of Allergy and Infectious Disease may help reduce the numbers of future victims.
Enrollment has begun in a phase I trial to test the safety of DM1157, an investigational modified form of chloroquine. Many strains of Plasmodium falciparum are now resistant to chloroquine. In fact, the parasites can expel the drug before it can affect them. Like chloroquine, DM1157 interferes with the parasite’s metabolism, but it also inhibits the parasite’s ability to expel the drug.
The study will enroll up to 104 healthy volunteers aged 18-45 years. One group will fast overnight and then receive either a single dose of the experimental drug at 1 of 7 dosage levels or a placebo. A second group also will fast and receive 1 dose at 1 of 4 dosage levels and repeat the routine for 2 more consecutive days. A third group will be given either a single 300-mg dose or placebo after eating a high-fat meal.
The study is expected to be completed by June 2019.
More acute flaccid myelitis cases confirmed by CDC
Acute flaccid myelitis (AFM) has stricken 90 patients in the United States this year and another 252 cases are being investigated, according to new data from the Centers for Disease Control and Prevention.

The number of confirmed cases is triple that seen in 2017.
Nearly all of the patients (90%) were children aged 2-8 years, and 99% experienced a fever and /or respiratory illness 7-10 days before the onset of symptoms. But although the prodrome and seasonality of AFM suggest an infective process, only 54% of the patients tested positive for the virus, Nancy Messonnier, MD, said during a briefing held by CDC officials. The most common findings were the enteroviruses EV-A71 (29%) and EV-D68 (37%); other viruses were recovered in the remaining pathogen-positive cases.
It’s not at all clear that these were causative agents, said Dr. Messonnier, director of the National Center for Immunization and Respiratory Diseases.
“At this time of year lots of children have a fever and respiratory infections,” she said. AFM may be caused by one of the identified viruses, a still-undetected pathogen, or a pathogen hiding in untested tissue. “Or, it could be an infection that’s kicking off an immune process,” attacking gray matter in the spinal cord.
The reported increase in cases must be viewed cautiously, Dr. Messonnier said. Physicians are becoming more aware of AFM, so the spike could represent an increase in reporting as well as actual incidence.
It’s not clear why the disease manifests almost exclusively in children, Dr. Messonnier said. Nor do health officials have much of a grasp on AFM’s long-term sequelae.
“We know that patients can recover fully, but at least half don’t, and some of those have serious sequelae. Unfortunately, we have not been following every patient, so this is a gap in our knowledge.”
A newly created national task force will examine AFM’s long-term effects, Dr. Messonnier said. The task force will also look at mortality; health departments across the country will examine mortality records to identify any past deaths preceded by AFM-like symptoms.
“One of the reasons we have convened this task force is to think about this hypothesis [of an autoimmune syndrome]. We have not backed off on the idea of an infectious organism causing it, but we are thinking more broadly,” Dr. Messonnier said.
Some anti-immunization groups are blaming vaccines for the disease, noting that several childhood vaccines list encephalomyelitis and transverse myelitis as possible adverse events.
“We are investigating every one of the cases in this and prior years and have a list of hypotheses based on the epidemiology,” Dr. Messonnier said. “I would say toxins are low on that list. Many of the children may have been vaccinated [before developing AFM] and that is something we will look at, but for now we recommend that all children should be vaccinated” according to the recommended schedule.
Additional details were published on 80 of the cases. Patients’ mean age was 4 years; 59% were male. Symptoms suggesting a viral illness occurred in 99%; these included fever (81%), cough, rhinorrhea, and congestion (78%), and vomiting and diarrhea (38%).
AFM symptoms varied; 47% had only upper limb involvement, 9% only lower limb, 15% two or three upper, and 29% all four limbs. All the patients with confirmed AFM were hospitalized, and 59% treated in intensive care units. There were no deaths (MMWR. 2018;ePub:13 November. DOI: http://dx.doi.org/10.15585/mmwr.mm6745e1).
AFM remains extremely rare, Dr. Messonnier said. But physicians should be alert for any signs of sudden limb weakness in children and report those immediately. The workup should include questions about recent fever with or without respiratory or gastrointestinal symptoms. Prompt collection of viral testing samples (cerebrospinal fluid, serum, respiratory, and stool specimens) is critical.
Additional information for health care professionals is available on the CDC AFM web page.
Acute flaccid myelitis (AFM) has stricken 90 patients in the United States this year and another 252 cases are being investigated, according to new data from the Centers for Disease Control and Prevention.
The number of confirmed cases is triple that seen in 2017.
Nearly all of the patients (90%) were children aged 2-8 years, and 99% experienced a fever and /or respiratory illness 7-10 days before the onset of symptoms. But although the prodrome and seasonality of AFM suggest an infective process, only 54% of the patients tested positive for the virus, Nancy Messonnier, MD, said during a briefing held by CDC officials. The most common findings were the enteroviruses EV-A71 (29%) and EV-D68 (37%); other viruses were recovered in the remaining pathogen-positive cases.
It’s not at all clear that these were causative agents, said Dr. Messonnier, director of the National Center for Immunization and Respiratory Diseases.
“At this time of year lots of children have a fever and respiratory infections,” she said. AFM may be caused by one of the identified viruses, a still-undetected pathogen, or a pathogen hiding in untested tissue. “Or, it could be an infection that’s kicking off an immune process,” attacking gray matter in the spinal cord.
The reported increase in cases must be viewed cautiously, Dr. Messonnier said. Physicians are becoming more aware of AFM, so the spike could represent an increase in reporting as well as actual incidence.
It’s not clear why the disease manifests almost exclusively in children, Dr. Messonnier said. Nor do health officials have much of a grasp on AFM’s long-term sequelae.
“We know that patients can recover fully, but at least half don’t, and some of those have serious sequelae. Unfortunately, we have not been following every patient, so this is a gap in our knowledge.”
A newly created national task force will examine AFM’s long-term effects, Dr. Messonnier said. The task force will also look at mortality; health departments across the country will examine mortality records to identify any past deaths preceded by AFM-like symptoms.
“One of the reasons we have convened this task force is to think about this hypothesis [of an autoimmune syndrome]. We have not backed off on the idea of an infectious organism causing it, but we are thinking more broadly,” Dr. Messonnier said.
Some anti-immunization groups are blaming vaccines for the disease, noting that several childhood vaccines list encephalomyelitis and transverse myelitis as possible adverse events.
“We are investigating every one of the cases in this and prior years and have a list of hypotheses based on the epidemiology,” Dr. Messonnier said. “I would say toxins are low on that list. Many of the children may have been vaccinated [before developing AFM] and that is something we will look at, but for now we recommend that all children should be vaccinated” according to the recommended schedule.
Additional details were published on 80 of the cases. Patients’ mean age was 4 years; 59% were male. Symptoms suggesting a viral illness occurred in 99%; these included fever (81%), cough, rhinorrhea, and congestion (78%), and vomiting and diarrhea (38%).
AFM symptoms varied; 47% had only upper limb involvement, 9% only lower limb, 15% two or three upper, and 29% all four limbs. All the patients with confirmed AFM were hospitalized, and 59% treated in intensive care units. There were no deaths (MMWR. 2018;ePub:13 November. DOI: http://dx.doi.org/10.15585/mmwr.mm6745e1).
AFM remains extremely rare, Dr. Messonnier said. But physicians should be alert for any signs of sudden limb weakness in children and report those immediately. The workup should include questions about recent fever with or without respiratory or gastrointestinal symptoms. Prompt collection of viral testing samples (cerebrospinal fluid, serum, respiratory, and stool specimens) is critical.
Additional information for health care professionals is available on the CDC AFM web page.
Acute flaccid myelitis (AFM) has stricken 90 patients in the United States this year and another 252 cases are being investigated, according to new data from the Centers for Disease Control and Prevention.
The number of confirmed cases is triple that seen in 2017.
Nearly all of the patients (90%) were children aged 2-8 years, and 99% experienced a fever and /or respiratory illness 7-10 days before the onset of symptoms. But although the prodrome and seasonality of AFM suggest an infective process, only 54% of the patients tested positive for the virus, Nancy Messonnier, MD, said during a briefing held by CDC officials. The most common findings were the enteroviruses EV-A71 (29%) and EV-D68 (37%); other viruses were recovered in the remaining pathogen-positive cases.
It’s not at all clear that these were causative agents, said Dr. Messonnier, director of the National Center for Immunization and Respiratory Diseases.
“At this time of year lots of children have a fever and respiratory infections,” she said. AFM may be caused by one of the identified viruses, a still-undetected pathogen, or a pathogen hiding in untested tissue. “Or, it could be an infection that’s kicking off an immune process,” attacking gray matter in the spinal cord.
The reported increase in cases must be viewed cautiously, Dr. Messonnier said. Physicians are becoming more aware of AFM, so the spike could represent an increase in reporting as well as actual incidence.
It’s not clear why the disease manifests almost exclusively in children, Dr. Messonnier said. Nor do health officials have much of a grasp on AFM’s long-term sequelae.
“We know that patients can recover fully, but at least half don’t, and some of those have serious sequelae. Unfortunately, we have not been following every patient, so this is a gap in our knowledge.”
A newly created national task force will examine AFM’s long-term effects, Dr. Messonnier said. The task force will also look at mortality; health departments across the country will examine mortality records to identify any past deaths preceded by AFM-like symptoms.
“One of the reasons we have convened this task force is to think about this hypothesis [of an autoimmune syndrome]. We have not backed off on the idea of an infectious organism causing it, but we are thinking more broadly,” Dr. Messonnier said.
Some anti-immunization groups are blaming vaccines for the disease, noting that several childhood vaccines list encephalomyelitis and transverse myelitis as possible adverse events.
“We are investigating every one of the cases in this and prior years and have a list of hypotheses based on the epidemiology,” Dr. Messonnier said. “I would say toxins are low on that list. Many of the children may have been vaccinated [before developing AFM] and that is something we will look at, but for now we recommend that all children should be vaccinated” according to the recommended schedule.
Additional details were published on 80 of the cases. Patients’ mean age was 4 years; 59% were male. Symptoms suggesting a viral illness occurred in 99%; these included fever (81%), cough, rhinorrhea, and congestion (78%), and vomiting and diarrhea (38%).
AFM symptoms varied; 47% had only upper limb involvement, 9% only lower limb, 15% two or three upper, and 29% all four limbs. All the patients with confirmed AFM were hospitalized, and 59% treated in intensive care units. There were no deaths (MMWR. 2018;ePub:13 November. DOI: http://dx.doi.org/10.15585/mmwr.mm6745e1).
AFM remains extremely rare, Dr. Messonnier said. But physicians should be alert for any signs of sudden limb weakness in children and report those immediately. The workup should include questions about recent fever with or without respiratory or gastrointestinal symptoms. Prompt collection of viral testing samples (cerebrospinal fluid, serum, respiratory, and stool specimens) is critical.
Additional information for health care professionals is available on the CDC AFM web page.
FROM A CDC BRIEFING
Can Probiotics Beat MRSA?
An unexpected finding in a study by National Institute of Health (NIH) researchers suggests that a “good” bacterium commonly found in probiotic digestive supplements works against Staphylococcus aureus (S aureus).
The researchers recruited 200 volunteers in Thailand for the study. They speculated that Thais would not be as affected by food sterilization or antibiotics as people in highly developed urban areas. The researchers analyzed fecal samples from each participant for bacteria correlated with the absence of S aureus. They found 101 samples positive for bacillus, primarily Bacillus subtilis (B subtilis), which is often mixed with other bacteria in probiotic products. The researchers then sampled for S aureus and found 25 positive gut samples and 26 positive nose samples. Strikingly, the researchers say, they found no S aureus in any of the samples that contained bacillus.
Using chromatography and mass spectrometry, the study team identified fengycins—a class of lipopeptides—as the specific bacillus substance that inhibited the S aureus sensing system. Other tests showed that fengycins had the same effect on several different strains of S aureus, including high-risk USA300 methicillin-resistant S aureus (MRSA).
To further validate their findings, the researchers colonized the gut of mice with S aureus and fed them B subtilis spores. Probiotic bacillus given every 2 days eliminated S aureus. The same test using bacillus where fengycin production had been removed had no effect: S aureus grew as expected.
An unexpected finding in a study by National Institute of Health (NIH) researchers suggests that a “good” bacterium commonly found in probiotic digestive supplements works against Staphylococcus aureus (S aureus).
The researchers recruited 200 volunteers in Thailand for the study. They speculated that Thais would not be as affected by food sterilization or antibiotics as people in highly developed urban areas. The researchers analyzed fecal samples from each participant for bacteria correlated with the absence of S aureus. They found 101 samples positive for bacillus, primarily Bacillus subtilis (B subtilis), which is often mixed with other bacteria in probiotic products. The researchers then sampled for S aureus and found 25 positive gut samples and 26 positive nose samples. Strikingly, the researchers say, they found no S aureus in any of the samples that contained bacillus.
Using chromatography and mass spectrometry, the study team identified fengycins—a class of lipopeptides—as the specific bacillus substance that inhibited the S aureus sensing system. Other tests showed that fengycins had the same effect on several different strains of S aureus, including high-risk USA300 methicillin-resistant S aureus (MRSA).
To further validate their findings, the researchers colonized the gut of mice with S aureus and fed them B subtilis spores. Probiotic bacillus given every 2 days eliminated S aureus. The same test using bacillus where fengycin production had been removed had no effect: S aureus grew as expected.
An unexpected finding in a study by National Institute of Health (NIH) researchers suggests that a “good” bacterium commonly found in probiotic digestive supplements works against Staphylococcus aureus (S aureus).
The researchers recruited 200 volunteers in Thailand for the study. They speculated that Thais would not be as affected by food sterilization or antibiotics as people in highly developed urban areas. The researchers analyzed fecal samples from each participant for bacteria correlated with the absence of S aureus. They found 101 samples positive for bacillus, primarily Bacillus subtilis (B subtilis), which is often mixed with other bacteria in probiotic products. The researchers then sampled for S aureus and found 25 positive gut samples and 26 positive nose samples. Strikingly, the researchers say, they found no S aureus in any of the samples that contained bacillus.
Using chromatography and mass spectrometry, the study team identified fengycins—a class of lipopeptides—as the specific bacillus substance that inhibited the S aureus sensing system. Other tests showed that fengycins had the same effect on several different strains of S aureus, including high-risk USA300 methicillin-resistant S aureus (MRSA).
To further validate their findings, the researchers colonized the gut of mice with S aureus and fed them B subtilis spores. Probiotic bacillus given every 2 days eliminated S aureus. The same test using bacillus where fengycin production had been removed had no effect: S aureus grew as expected.
FDA puts selinexor on fast track for DLBCL
The Food and Drug Administration has granted fast track designation to selinexor for the treatment of diffuse large B-cell lymphoma (DLBCL).

The designation is for selinexor to treat DLBCL patients who have received at least two prior therapies and who are not eligible for high-dose chemotherapy with stem cell rescue or chimeric antigen receptor (CAR) T-cell therapy.
Selinexor is being studied in the phase 2b SADAL trial (NCT02227251), which is enrolling patients with relapsed or refractory DLBCL who have received two to five prior therapies and are not eligible for stem cell transplant.
Top-line results from this trial are scheduled to be presented at the 2018 ASH Annual Meeting (Abstract 1677).
Selinexor is an oral selective inhibitor of nuclear export compound being developed by Karyopharm Therapeutics.
The company previously received fast track designation for selinexor to treat patients with penta-refractory multiple myeloma who have received at least three prior lines of therapy.
The FDA’s fast track program is designed to facilitate the development and expedite the review of products that are intended to treat serious conditions and have the potential to address unmet medical needs. Fast track designation provides developers with greater access to the FDA as well as eligibility for accelerated approval, priority review, and rolling review.
“Pending positive results from the phase 2b SADAL study, we plan to submit a second NDA [new drug application] to the FDA in the first half of 2019, with a request for accelerated approval, for oral selinexor as a potential new treatment for patients with relapsed or refractory DLBCL,” Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm, said in a statement.
In October, the FDA accepted an NDA for selinexor as a treatment for penta-refractory multiple myeloma. The agency granted the application priority review and set an action date of April 6, 2019.
The Food and Drug Administration has granted fast track designation to selinexor for the treatment of diffuse large B-cell lymphoma (DLBCL).
The designation is for selinexor to treat DLBCL patients who have received at least two prior therapies and who are not eligible for high-dose chemotherapy with stem cell rescue or chimeric antigen receptor (CAR) T-cell therapy.
Selinexor is being studied in the phase 2b SADAL trial (NCT02227251), which is enrolling patients with relapsed or refractory DLBCL who have received two to five prior therapies and are not eligible for stem cell transplant.
Top-line results from this trial are scheduled to be presented at the 2018 ASH Annual Meeting (Abstract 1677).
Selinexor is an oral selective inhibitor of nuclear export compound being developed by Karyopharm Therapeutics.
The company previously received fast track designation for selinexor to treat patients with penta-refractory multiple myeloma who have received at least three prior lines of therapy.
The FDA’s fast track program is designed to facilitate the development and expedite the review of products that are intended to treat serious conditions and have the potential to address unmet medical needs. Fast track designation provides developers with greater access to the FDA as well as eligibility for accelerated approval, priority review, and rolling review.
“Pending positive results from the phase 2b SADAL study, we plan to submit a second NDA [new drug application] to the FDA in the first half of 2019, with a request for accelerated approval, for oral selinexor as a potential new treatment for patients with relapsed or refractory DLBCL,” Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm, said in a statement.
In October, the FDA accepted an NDA for selinexor as a treatment for penta-refractory multiple myeloma. The agency granted the application priority review and set an action date of April 6, 2019.
The Food and Drug Administration has granted fast track designation to selinexor for the treatment of diffuse large B-cell lymphoma (DLBCL).
The designation is for selinexor to treat DLBCL patients who have received at least two prior therapies and who are not eligible for high-dose chemotherapy with stem cell rescue or chimeric antigen receptor (CAR) T-cell therapy.
Selinexor is being studied in the phase 2b SADAL trial (NCT02227251), which is enrolling patients with relapsed or refractory DLBCL who have received two to five prior therapies and are not eligible for stem cell transplant.
Top-line results from this trial are scheduled to be presented at the 2018 ASH Annual Meeting (Abstract 1677).
Selinexor is an oral selective inhibitor of nuclear export compound being developed by Karyopharm Therapeutics.
The company previously received fast track designation for selinexor to treat patients with penta-refractory multiple myeloma who have received at least three prior lines of therapy.
The FDA’s fast track program is designed to facilitate the development and expedite the review of products that are intended to treat serious conditions and have the potential to address unmet medical needs. Fast track designation provides developers with greater access to the FDA as well as eligibility for accelerated approval, priority review, and rolling review.
“Pending positive results from the phase 2b SADAL study, we plan to submit a second NDA [new drug application] to the FDA in the first half of 2019, with a request for accelerated approval, for oral selinexor as a potential new treatment for patients with relapsed or refractory DLBCL,” Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm, said in a statement.
In October, the FDA accepted an NDA for selinexor as a treatment for penta-refractory multiple myeloma. The agency granted the application priority review and set an action date of April 6, 2019.
What’s the Impact of Osteoporosis in Multiple Myeloma?
Osteoporosis is common among patients with multiple myeloma (MM), in part because both largely affect older adults. And more than half of MM patients will have MM skeletal-related events, which are painful, and can lead to complications (such as spinal cord compression) and death.
But how does pre-existing bone disease contribute to clinical outcomes in MM? Osteoporosis is a “silent condition” and very little is known about its role in MM, say researchers from The Ohio State University in Columbus and University of Massachusetts in Worcester. The standard diagnostic evaluation for MM does not include dual-energy x-ray absorptiometry, therefore assessments of underlying osteoporosis are not routine. Moreover, it is a challenge to distinguish osteoporotic fragility fractures from pathologic MM-induced fractures. Skeletal surveys underestimate bone involvement by about 40%, the researchers note, and are even less specific for distinguishing myeloma-related secondary osteoporosis from primary osteoporosis.
The researchers examined the relationship between the Fracture Risk Assessment Tool (FRAX) and the risk of death in women who developed MM. They analyzed data from 161,808 women in the Women’s Health Initiative (WHI). Of those, 409 developed MM; 362 had no history of cancer.
At baseline, 98 (27%) women had high FRAX scores, and 264 (73%) had low scores. The median follow-up period was 10.5 years from enrollment and 7.2 years from the time of MM diagnosis. Of the patients with MM, 226 died during the follow-up period, including 71 with high FRAX scores and 155 with low scores. MM mortality was higher among women with high FRAX scores: 72%, vs 59% of those with low scores. Poor bone health was associated with greater MM mortality but was not related to delay in time to diagnosis.
During the evaluation, 57 fractures were reported, 65% before MM diagnosis. Fewer than half of the women had a first fracture after diagnosis. The probability of fracture was similar among the women, regardless of FRAX score. Not surprisingly, older women with lower BMI were most at risk.
The WHI does not include information on staging, chemotherapy, or use of bisphosphonates. Therefore, the impact of bisphosphonates could not be determined in this study. The researchers also did not know how many patients might have had pre-existing monoclonal gammopathy of undetermined significance, a disorder in about 3% of the aging population that progresses to MM in 1% per year.
Source:
Rosko AE, Hade EM, Li W, et al. Clin Lymphoma Myeloma Leuk. 2018;18(9):597-602.
Osteoporosis is common among patients with multiple myeloma (MM), in part because both largely affect older adults. And more than half of MM patients will have MM skeletal-related events, which are painful, and can lead to complications (such as spinal cord compression) and death.
But how does pre-existing bone disease contribute to clinical outcomes in MM? Osteoporosis is a “silent condition” and very little is known about its role in MM, say researchers from The Ohio State University in Columbus and University of Massachusetts in Worcester. The standard diagnostic evaluation for MM does not include dual-energy x-ray absorptiometry, therefore assessments of underlying osteoporosis are not routine. Moreover, it is a challenge to distinguish osteoporotic fragility fractures from pathologic MM-induced fractures. Skeletal surveys underestimate bone involvement by about 40%, the researchers note, and are even less specific for distinguishing myeloma-related secondary osteoporosis from primary osteoporosis.
The researchers examined the relationship between the Fracture Risk Assessment Tool (FRAX) and the risk of death in women who developed MM. They analyzed data from 161,808 women in the Women’s Health Initiative (WHI). Of those, 409 developed MM; 362 had no history of cancer.
At baseline, 98 (27%) women had high FRAX scores, and 264 (73%) had low scores. The median follow-up period was 10.5 years from enrollment and 7.2 years from the time of MM diagnosis. Of the patients with MM, 226 died during the follow-up period, including 71 with high FRAX scores and 155 with low scores. MM mortality was higher among women with high FRAX scores: 72%, vs 59% of those with low scores. Poor bone health was associated with greater MM mortality but was not related to delay in time to diagnosis.
During the evaluation, 57 fractures were reported, 65% before MM diagnosis. Fewer than half of the women had a first fracture after diagnosis. The probability of fracture was similar among the women, regardless of FRAX score. Not surprisingly, older women with lower BMI were most at risk.
The WHI does not include information on staging, chemotherapy, or use of bisphosphonates. Therefore, the impact of bisphosphonates could not be determined in this study. The researchers also did not know how many patients might have had pre-existing monoclonal gammopathy of undetermined significance, a disorder in about 3% of the aging population that progresses to MM in 1% per year.
Source:
Rosko AE, Hade EM, Li W, et al. Clin Lymphoma Myeloma Leuk. 2018;18(9):597-602.
Osteoporosis is common among patients with multiple myeloma (MM), in part because both largely affect older adults. And more than half of MM patients will have MM skeletal-related events, which are painful, and can lead to complications (such as spinal cord compression) and death.
But how does pre-existing bone disease contribute to clinical outcomes in MM? Osteoporosis is a “silent condition” and very little is known about its role in MM, say researchers from The Ohio State University in Columbus and University of Massachusetts in Worcester. The standard diagnostic evaluation for MM does not include dual-energy x-ray absorptiometry, therefore assessments of underlying osteoporosis are not routine. Moreover, it is a challenge to distinguish osteoporotic fragility fractures from pathologic MM-induced fractures. Skeletal surveys underestimate bone involvement by about 40%, the researchers note, and are even less specific for distinguishing myeloma-related secondary osteoporosis from primary osteoporosis.
The researchers examined the relationship between the Fracture Risk Assessment Tool (FRAX) and the risk of death in women who developed MM. They analyzed data from 161,808 women in the Women’s Health Initiative (WHI). Of those, 409 developed MM; 362 had no history of cancer.
At baseline, 98 (27%) women had high FRAX scores, and 264 (73%) had low scores. The median follow-up period was 10.5 years from enrollment and 7.2 years from the time of MM diagnosis. Of the patients with MM, 226 died during the follow-up period, including 71 with high FRAX scores and 155 with low scores. MM mortality was higher among women with high FRAX scores: 72%, vs 59% of those with low scores. Poor bone health was associated with greater MM mortality but was not related to delay in time to diagnosis.
During the evaluation, 57 fractures were reported, 65% before MM diagnosis. Fewer than half of the women had a first fracture after diagnosis. The probability of fracture was similar among the women, regardless of FRAX score. Not surprisingly, older women with lower BMI were most at risk.
The WHI does not include information on staging, chemotherapy, or use of bisphosphonates. Therefore, the impact of bisphosphonates could not be determined in this study. The researchers also did not know how many patients might have had pre-existing monoclonal gammopathy of undetermined significance, a disorder in about 3% of the aging population that progresses to MM in 1% per year.
Source:
Rosko AE, Hade EM, Li W, et al. Clin Lymphoma Myeloma Leuk. 2018;18(9):597-602.
Cigarette smoking at lowest level ever
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
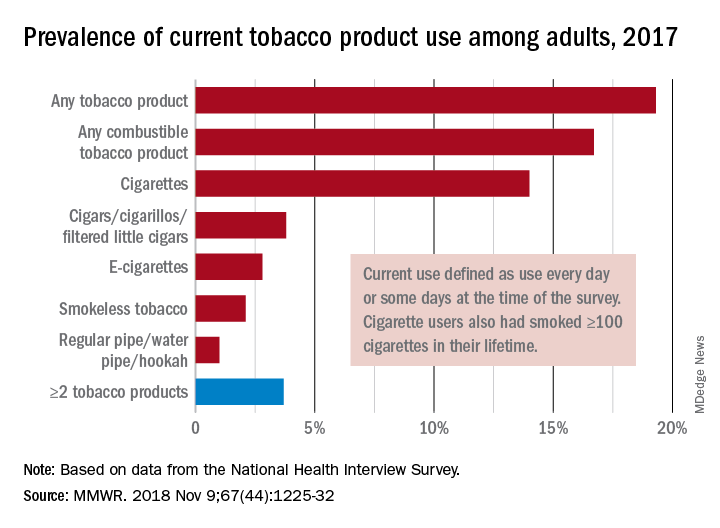
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
FROM MMWR
Gastric Banding vs Metformin
Gastric banding was just as successful as metformin alone in stabilizing prediabetes or new-onset type 2 diabetes in the Beta Cell Restoration through Fat Mitigation study (BetaFat), an NIH-supported study.
The study is part of the Restoring Insulin Secretion (RISE) study, a set of 3 clinical trials designed to find ways to reverse or slow the loss of insulin production and release in people at risk for type 2 diabetes.
In this study, 44 patients were randomly assigned to have a gastric banding procedure, and 44 were taking metformin. After 2 years, people in the gastric banding group had lost an average of 23 lb , vs 4 lb in the metformin group. Insulin sensitivity improved similarly in both groups, as did function of insulin-producing cells. Both groups showed small improvements in blood glucose levels.
Gastric banding was just as successful as metformin alone in stabilizing prediabetes or new-onset type 2 diabetes in the Beta Cell Restoration through Fat Mitigation study (BetaFat), an NIH-supported study.
The study is part of the Restoring Insulin Secretion (RISE) study, a set of 3 clinical trials designed to find ways to reverse or slow the loss of insulin production and release in people at risk for type 2 diabetes.
In this study, 44 patients were randomly assigned to have a gastric banding procedure, and 44 were taking metformin. After 2 years, people in the gastric banding group had lost an average of 23 lb , vs 4 lb in the metformin group. Insulin sensitivity improved similarly in both groups, as did function of insulin-producing cells. Both groups showed small improvements in blood glucose levels.
Gastric banding was just as successful as metformin alone in stabilizing prediabetes or new-onset type 2 diabetes in the Beta Cell Restoration through Fat Mitigation study (BetaFat), an NIH-supported study.
The study is part of the Restoring Insulin Secretion (RISE) study, a set of 3 clinical trials designed to find ways to reverse or slow the loss of insulin production and release in people at risk for type 2 diabetes.
In this study, 44 patients were randomly assigned to have a gastric banding procedure, and 44 were taking metformin. After 2 years, people in the gastric banding group had lost an average of 23 lb , vs 4 lb in the metformin group. Insulin sensitivity improved similarly in both groups, as did function of insulin-producing cells. Both groups showed small improvements in blood glucose levels.
Many teens don’t know e-cigarettes contain nicotine
ORLANDO – Flavoring and lack of Food and Drug Administration regulation of e-cigarettes has led to more children and adolescents using these devices, according to American Academy of Pediatrics President Colleen A. Kraft, MD.
In an interview, Dr. Kraft said the FDA should regulate these products and limit their purchase to adults who are at least 21 years old. E-cigarettes were initially intended as an aid for adults to reduce their cigarette use, but the addition of flavoring has attracted children and adolescents to the devices, Dr. Kraft noted.
“When you have these devices that have flavors like gummy bear and cotton candy and bubblegum, you are marketing to children, and we are calling out the FDA because they could actually stop this today,” she said. In fact, Dr. Kraft added, many children and adolescents don’t even realize that e-cigarettes contain nicotine.
Dr. Kraft reported no relevant conflicts of interest.
ORLANDO – Flavoring and lack of Food and Drug Administration regulation of e-cigarettes has led to more children and adolescents using these devices, according to American Academy of Pediatrics President Colleen A. Kraft, MD.
In an interview, Dr. Kraft said the FDA should regulate these products and limit their purchase to adults who are at least 21 years old. E-cigarettes were initially intended as an aid for adults to reduce their cigarette use, but the addition of flavoring has attracted children and adolescents to the devices, Dr. Kraft noted.
“When you have these devices that have flavors like gummy bear and cotton candy and bubblegum, you are marketing to children, and we are calling out the FDA because they could actually stop this today,” she said. In fact, Dr. Kraft added, many children and adolescents don’t even realize that e-cigarettes contain nicotine.
Dr. Kraft reported no relevant conflicts of interest.
ORLANDO – Flavoring and lack of Food and Drug Administration regulation of e-cigarettes has led to more children and adolescents using these devices, according to American Academy of Pediatrics President Colleen A. Kraft, MD.
In an interview, Dr. Kraft said the FDA should regulate these products and limit their purchase to adults who are at least 21 years old. E-cigarettes were initially intended as an aid for adults to reduce their cigarette use, but the addition of flavoring has attracted children and adolescents to the devices, Dr. Kraft noted.
“When you have these devices that have flavors like gummy bear and cotton candy and bubblegum, you are marketing to children, and we are calling out the FDA because they could actually stop this today,” she said. In fact, Dr. Kraft added, many children and adolescents don’t even realize that e-cigarettes contain nicotine.
Dr. Kraft reported no relevant conflicts of interest.
REPORTING FROM AAP 2018

Testing the Limits of Low-Dose Aspirin
Unless someone has already had a heart attack or other cardiovascular event, daily low-dose aspirin does not prolong healthy independent living, according to the ASPirin in Reducing Events in the Elderly (ASPREE) trial.
The study began in 2010, enrolling 19,114 adults aged ≥ 65 years. The participants were treated with 100 mg/d of aspirin or placebo and followed for an average of 4.7 years. Of participants randomly assigned aspirin, 90.3% were still alive at the end of the treatment without persistent physical disability or dementia, as were 90.5% of those on placebo. Rates of dementia were almost identical in both groups. Major cardiovascular events were similar: 448 in the aspirin group and 474 in the placebo group.
The aspirin group had a slightly higher risk of death (5.9% vs 5.2%). The researchers advise interpreting this cautiously: Most of the deaths were due to cancer. A small increase in new cases of cancer was reported for the aspirin group but may have been due to chance. Heart disease accounted for 19% of deaths and major bleeding for 5%. People taking aspirin were more likely to have significant bleeding (3.8% vs 2.7%).
The researchers emphasize that, study findings notwithstanding, older adults should follow their physician’s advice about daily aspirin use. The new findings do not apply to people with an indication for aspirin, including stroke, heart attack, or other cardiovascular disease.
Unless someone has already had a heart attack or other cardiovascular event, daily low-dose aspirin does not prolong healthy independent living, according to the ASPirin in Reducing Events in the Elderly (ASPREE) trial.
The study began in 2010, enrolling 19,114 adults aged ≥ 65 years. The participants were treated with 100 mg/d of aspirin or placebo and followed for an average of 4.7 years. Of participants randomly assigned aspirin, 90.3% were still alive at the end of the treatment without persistent physical disability or dementia, as were 90.5% of those on placebo. Rates of dementia were almost identical in both groups. Major cardiovascular events were similar: 448 in the aspirin group and 474 in the placebo group.
The aspirin group had a slightly higher risk of death (5.9% vs 5.2%). The researchers advise interpreting this cautiously: Most of the deaths were due to cancer. A small increase in new cases of cancer was reported for the aspirin group but may have been due to chance. Heart disease accounted for 19% of deaths and major bleeding for 5%. People taking aspirin were more likely to have significant bleeding (3.8% vs 2.7%).
The researchers emphasize that, study findings notwithstanding, older adults should follow their physician’s advice about daily aspirin use. The new findings do not apply to people with an indication for aspirin, including stroke, heart attack, or other cardiovascular disease.
Unless someone has already had a heart attack or other cardiovascular event, daily low-dose aspirin does not prolong healthy independent living, according to the ASPirin in Reducing Events in the Elderly (ASPREE) trial.
The study began in 2010, enrolling 19,114 adults aged ≥ 65 years. The participants were treated with 100 mg/d of aspirin or placebo and followed for an average of 4.7 years. Of participants randomly assigned aspirin, 90.3% were still alive at the end of the treatment without persistent physical disability or dementia, as were 90.5% of those on placebo. Rates of dementia were almost identical in both groups. Major cardiovascular events were similar: 448 in the aspirin group and 474 in the placebo group.
The aspirin group had a slightly higher risk of death (5.9% vs 5.2%). The researchers advise interpreting this cautiously: Most of the deaths were due to cancer. A small increase in new cases of cancer was reported for the aspirin group but may have been due to chance. Heart disease accounted for 19% of deaths and major bleeding for 5%. People taking aspirin were more likely to have significant bleeding (3.8% vs 2.7%).
The researchers emphasize that, study findings notwithstanding, older adults should follow their physician’s advice about daily aspirin use. The new findings do not apply to people with an indication for aspirin, including stroke, heart attack, or other cardiovascular disease.