User login
LAIV4 was less effective for children than IIV against influenza A/H1N1pdm09
The live attenuated influenza vaccine was less effective against the influenza A/H1N1pdm09 virus in children and adolescents across multiple influenza seasons between 2013 and 2016, compared with the inactivated influenza vaccine, according to research published in the journal Pediatrics.

Jessie R. Chung, MPH, from the influenza division at the Centers for Disease Control and Prevention in Atlanta, and her colleagues performed an analysis of five different studies where vaccine effectiveness (VE) was examined for quadrivalent live attenuated vaccine (LAIV4) and inactivated influenza vaccine (IIV) in children and adolescents aged 2-17 years from 42 states.
The analysis included data from the U.S. Influenza Vaccine Effectiveness Network (6,793 patients), a study from the Louisiana State University Health Sciences Center (3,822 patients), the Influenza Clinical Investigation for Children (3,521 patients), Department of Defense Global, Laboratory-based, Influenza Surveillance Program (1,935 patients), and the Influenza Incidence Surveillance Project (1,102 patients) between the periods of 2013-2014 and 2015-2016. The researchers sourced current and previous season vaccination history from electronic medical records and immunization registries.
Of patients who were vaccinated across all seasons, there was 67% effectiveness against influenza A/H1N1pdm09 (95% confidence interval, 62%-72%) for those who received the IIV and 20% (95% CI, −6%-39%) for LAIV4. Among patients who received the LAIV4 vaccination, there was a significantly higher likelihood of developing influenza A/H1N1pdm09 (odds ratio, 2.66; 95% CI, 2.06-3.44) compared with patients who received the IIV vaccination.
With regard to other strains, there was similar effectiveness against influenza A/H3N2 and influenza B with LAIV4 and IIV vaccinations.
“In contrast to findings of reduced LAIV4 effectiveness against influenza A/H1N1pdm09 viruses, our results suggest a possible but nonsignificant benefit of LAIV4 over IIV against influenza B viruses, which has been described previously,” the investigators wrote.
Limitations of the study included having data only one season prior to enrollment and little available demographic information beyond age, gender, and geographic location.
The Influenza Clinical Investigation for Children was funded by MedImmune, a member of the AstraZeneca Group. Two of the researchers are employees of AstraZeneca. The other authors reported having no conflicts of interest. The U.S. Influenza Vaccine Effectiveness Network was supported by the CDC through cooperative agreements with the University of Michigan, Kaiser Permanente Washington Health Research Institute, Marshfield Clinic Research Institute, University of Pittsburgh, and Baylor Scott & White Health. At the University of Pittsburgh, the project also was supported by the National Institutes of Health.
SOURCE: Chung JR et al. Pediatrics. 2018. doi: 10.1542/peds.2018-2094.
There are many explanations for the decline in effectiveness of the live attenuated influenza vaccine (LAIV4), but the data are complicated by conflicting information from studies outside the United States indicating “reasonable protection” against influenza A/H1N1pdm09, A/H3N2, and influenza B, compared with the inactivated influenza virus (IIV), Pedro A. Piedra, MD, wrote in an accompanying editorial.
In 2016, the World Health Organization met to discuss LAIV effectiveness and highlighted factors such as methodological study differences, inadequate vaccine handling at distribution centers, intrinsic virological differences of the A/H1N1pdm09 virus, and increased preexisting population immunity in the United States since 2010 as potential explanations. During the transition from LAIV3 to LAIV4 for the 2013-2014 influenza season, viral interference may have also occurred when the influenza B strain was introduced into the vaccine, he added.
According to the CDC’s Advisory Committee on Immunization Practices (ACIP), viral growth properties of A/H1N1pdm09 has improved in LAIV4, and viral shedding also has improved for children between 2 years and 4 years of age. Although effectiveness numbers were not available for the ACIP recommendation, an interim analysis from Public Health England for the 2017-2018 influenza season found a vaccine effectiveness of 90.3% (95% confidence interval, 16.4%-98.9%).
“This early result is encouraging and supports the reintroduction of LAIV4 in the United States as an option for the control of seasonal influenza,” he said. “It also highlights the need for annual influenza vaccine effectiveness estimates and the importance of the U.S. Influenza Vaccine Effectiveness Network in providing updated information for ACIP recommendations.”
Dr. Piedra is from the departments of molecular virology and microbiology and pediatrics, Baylor College of Medicine, Houston. He reports being a consultant for AstraZeneca, Sanofi Pasteur, GlaxoSmithKline, and Merck Sharp and Dohme, and he has received travel support to present at an influenza seminar supported by Seqirus. His comments are from an editorial accompanying the article by Chung and colleagues ( Pediatrics. 2019. doi: 10.1542/peds.2018- 3290 ).
There are many explanations for the decline in effectiveness of the live attenuated influenza vaccine (LAIV4), but the data are complicated by conflicting information from studies outside the United States indicating “reasonable protection” against influenza A/H1N1pdm09, A/H3N2, and influenza B, compared with the inactivated influenza virus (IIV), Pedro A. Piedra, MD, wrote in an accompanying editorial.
In 2016, the World Health Organization met to discuss LAIV effectiveness and highlighted factors such as methodological study differences, inadequate vaccine handling at distribution centers, intrinsic virological differences of the A/H1N1pdm09 virus, and increased preexisting population immunity in the United States since 2010 as potential explanations. During the transition from LAIV3 to LAIV4 for the 2013-2014 influenza season, viral interference may have also occurred when the influenza B strain was introduced into the vaccine, he added.
According to the CDC’s Advisory Committee on Immunization Practices (ACIP), viral growth properties of A/H1N1pdm09 has improved in LAIV4, and viral shedding also has improved for children between 2 years and 4 years of age. Although effectiveness numbers were not available for the ACIP recommendation, an interim analysis from Public Health England for the 2017-2018 influenza season found a vaccine effectiveness of 90.3% (95% confidence interval, 16.4%-98.9%).
“This early result is encouraging and supports the reintroduction of LAIV4 in the United States as an option for the control of seasonal influenza,” he said. “It also highlights the need for annual influenza vaccine effectiveness estimates and the importance of the U.S. Influenza Vaccine Effectiveness Network in providing updated information for ACIP recommendations.”
Dr. Piedra is from the departments of molecular virology and microbiology and pediatrics, Baylor College of Medicine, Houston. He reports being a consultant for AstraZeneca, Sanofi Pasteur, GlaxoSmithKline, and Merck Sharp and Dohme, and he has received travel support to present at an influenza seminar supported by Seqirus. His comments are from an editorial accompanying the article by Chung and colleagues ( Pediatrics. 2019. doi: 10.1542/peds.2018- 3290 ).
There are many explanations for the decline in effectiveness of the live attenuated influenza vaccine (LAIV4), but the data are complicated by conflicting information from studies outside the United States indicating “reasonable protection” against influenza A/H1N1pdm09, A/H3N2, and influenza B, compared with the inactivated influenza virus (IIV), Pedro A. Piedra, MD, wrote in an accompanying editorial.
In 2016, the World Health Organization met to discuss LAIV effectiveness and highlighted factors such as methodological study differences, inadequate vaccine handling at distribution centers, intrinsic virological differences of the A/H1N1pdm09 virus, and increased preexisting population immunity in the United States since 2010 as potential explanations. During the transition from LAIV3 to LAIV4 for the 2013-2014 influenza season, viral interference may have also occurred when the influenza B strain was introduced into the vaccine, he added.
According to the CDC’s Advisory Committee on Immunization Practices (ACIP), viral growth properties of A/H1N1pdm09 has improved in LAIV4, and viral shedding also has improved for children between 2 years and 4 years of age. Although effectiveness numbers were not available for the ACIP recommendation, an interim analysis from Public Health England for the 2017-2018 influenza season found a vaccine effectiveness of 90.3% (95% confidence interval, 16.4%-98.9%).
“This early result is encouraging and supports the reintroduction of LAIV4 in the United States as an option for the control of seasonal influenza,” he said. “It also highlights the need for annual influenza vaccine effectiveness estimates and the importance of the U.S. Influenza Vaccine Effectiveness Network in providing updated information for ACIP recommendations.”
Dr. Piedra is from the departments of molecular virology and microbiology and pediatrics, Baylor College of Medicine, Houston. He reports being a consultant for AstraZeneca, Sanofi Pasteur, GlaxoSmithKline, and Merck Sharp and Dohme, and he has received travel support to present at an influenza seminar supported by Seqirus. His comments are from an editorial accompanying the article by Chung and colleagues ( Pediatrics. 2019. doi: 10.1542/peds.2018- 3290 ).
The live attenuated influenza vaccine was less effective against the influenza A/H1N1pdm09 virus in children and adolescents across multiple influenza seasons between 2013 and 2016, compared with the inactivated influenza vaccine, according to research published in the journal Pediatrics.
Jessie R. Chung, MPH, from the influenza division at the Centers for Disease Control and Prevention in Atlanta, and her colleagues performed an analysis of five different studies where vaccine effectiveness (VE) was examined for quadrivalent live attenuated vaccine (LAIV4) and inactivated influenza vaccine (IIV) in children and adolescents aged 2-17 years from 42 states.
The analysis included data from the U.S. Influenza Vaccine Effectiveness Network (6,793 patients), a study from the Louisiana State University Health Sciences Center (3,822 patients), the Influenza Clinical Investigation for Children (3,521 patients), Department of Defense Global, Laboratory-based, Influenza Surveillance Program (1,935 patients), and the Influenza Incidence Surveillance Project (1,102 patients) between the periods of 2013-2014 and 2015-2016. The researchers sourced current and previous season vaccination history from electronic medical records and immunization registries.
Of patients who were vaccinated across all seasons, there was 67% effectiveness against influenza A/H1N1pdm09 (95% confidence interval, 62%-72%) for those who received the IIV and 20% (95% CI, −6%-39%) for LAIV4. Among patients who received the LAIV4 vaccination, there was a significantly higher likelihood of developing influenza A/H1N1pdm09 (odds ratio, 2.66; 95% CI, 2.06-3.44) compared with patients who received the IIV vaccination.
With regard to other strains, there was similar effectiveness against influenza A/H3N2 and influenza B with LAIV4 and IIV vaccinations.
“In contrast to findings of reduced LAIV4 effectiveness against influenza A/H1N1pdm09 viruses, our results suggest a possible but nonsignificant benefit of LAIV4 over IIV against influenza B viruses, which has been described previously,” the investigators wrote.
Limitations of the study included having data only one season prior to enrollment and little available demographic information beyond age, gender, and geographic location.
The Influenza Clinical Investigation for Children was funded by MedImmune, a member of the AstraZeneca Group. Two of the researchers are employees of AstraZeneca. The other authors reported having no conflicts of interest. The U.S. Influenza Vaccine Effectiveness Network was supported by the CDC through cooperative agreements with the University of Michigan, Kaiser Permanente Washington Health Research Institute, Marshfield Clinic Research Institute, University of Pittsburgh, and Baylor Scott & White Health. At the University of Pittsburgh, the project also was supported by the National Institutes of Health.
SOURCE: Chung JR et al. Pediatrics. 2018. doi: 10.1542/peds.2018-2094.
The live attenuated influenza vaccine was less effective against the influenza A/H1N1pdm09 virus in children and adolescents across multiple influenza seasons between 2013 and 2016, compared with the inactivated influenza vaccine, according to research published in the journal Pediatrics.
Jessie R. Chung, MPH, from the influenza division at the Centers for Disease Control and Prevention in Atlanta, and her colleagues performed an analysis of five different studies where vaccine effectiveness (VE) was examined for quadrivalent live attenuated vaccine (LAIV4) and inactivated influenza vaccine (IIV) in children and adolescents aged 2-17 years from 42 states.
The analysis included data from the U.S. Influenza Vaccine Effectiveness Network (6,793 patients), a study from the Louisiana State University Health Sciences Center (3,822 patients), the Influenza Clinical Investigation for Children (3,521 patients), Department of Defense Global, Laboratory-based, Influenza Surveillance Program (1,935 patients), and the Influenza Incidence Surveillance Project (1,102 patients) between the periods of 2013-2014 and 2015-2016. The researchers sourced current and previous season vaccination history from electronic medical records and immunization registries.
Of patients who were vaccinated across all seasons, there was 67% effectiveness against influenza A/H1N1pdm09 (95% confidence interval, 62%-72%) for those who received the IIV and 20% (95% CI, −6%-39%) for LAIV4. Among patients who received the LAIV4 vaccination, there was a significantly higher likelihood of developing influenza A/H1N1pdm09 (odds ratio, 2.66; 95% CI, 2.06-3.44) compared with patients who received the IIV vaccination.
With regard to other strains, there was similar effectiveness against influenza A/H3N2 and influenza B with LAIV4 and IIV vaccinations.
“In contrast to findings of reduced LAIV4 effectiveness against influenza A/H1N1pdm09 viruses, our results suggest a possible but nonsignificant benefit of LAIV4 over IIV against influenza B viruses, which has been described previously,” the investigators wrote.
Limitations of the study included having data only one season prior to enrollment and little available demographic information beyond age, gender, and geographic location.
The Influenza Clinical Investigation for Children was funded by MedImmune, a member of the AstraZeneca Group. Two of the researchers are employees of AstraZeneca. The other authors reported having no conflicts of interest. The U.S. Influenza Vaccine Effectiveness Network was supported by the CDC through cooperative agreements with the University of Michigan, Kaiser Permanente Washington Health Research Institute, Marshfield Clinic Research Institute, University of Pittsburgh, and Baylor Scott & White Health. At the University of Pittsburgh, the project also was supported by the National Institutes of Health.
SOURCE: Chung JR et al. Pediatrics. 2018. doi: 10.1542/peds.2018-2094.
FROM PEDIATRICS
Key clinical point: The live attenuated influenza vaccine (LAIV4) was significantly less effective than was the inactivated influenza vaccine (IIV) for children against the influenza A/H1N1pdm09 virus across multiple flu seasons.
Major finding:
Study details: A combined analysis of five studies in the United States between the periods of 2013-2014 and 2015-2016 from the U.S. Influenza Vaccine Effectiveness Network.
Disclosures: The Influenza Clinical Investigation for Children was funded by MedImmune, a member of the AstraZeneca Group. Two of the researchers are employees of AstraZeneca. The other authors reported having no conflicts of interest. The U.S. Influenza Vaccine Effectiveness Network was supported by the CDC through cooperative agreements with the University of Michigan, Kaiser Permanente Washington Health Research Institute, Marshfield Clinic Research Institute, University of Pittsburgh, and Baylor Scott & White Health. At the University of Pittsburgh, the project also was supported by the National Institutes of Health.
Source: Chung JR et al. Pediatrics. 2018. doi: 10.1542/peds.2018-2094.
Surgeon General: Public Health Investment is key to Economic Security
In December 2018, Federal Practitioner sat down with Surgeon General VADM Jerome M. Adams, MD, MPH to discuss recent initiatives to combat the opioid epidemic and to improve health care engagement and delivery in this exclusive video interview. During 2018, the Office of the Surgeon General took a number of steps to address the ongoing opioid crisis, releasing a public health advisory to urge increased use of naloxone, which can reverse the effects of an opioid overdose. In addition, the office of the Surgeon General released a postcard with 5 actions every person can take to address the opioid epidemic.
Increasing Health Care Engagement

Next: Community health and economic prosperity, What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
Community Health and Economic Prosperity

Next: What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
What Health Care Providers Can Do for Prevention

Next: Expanding the PHS mission, the Surgeon General's challenge on opioids
Expanding the PHS Mission

Next: The Surgeon General's challenge on opioids
The Surgeon General's Challenge on Opioids

{kind=link}
In December 2018, Federal Practitioner sat down with Surgeon General VADM Jerome M. Adams, MD, MPH to discuss recent initiatives to combat the opioid epidemic and to improve health care engagement and delivery in this exclusive video interview. During 2018, the Office of the Surgeon General took a number of steps to address the ongoing opioid crisis, releasing a public health advisory to urge increased use of naloxone, which can reverse the effects of an opioid overdose. In addition, the office of the Surgeon General released a postcard with 5 actions every person can take to address the opioid epidemic.
Increasing Health Care Engagement
Next: Community health and economic prosperity, What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
Community Health and Economic Prosperity
Next: What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
What Health Care Providers Can Do for Prevention
Next: Expanding the PHS mission, the Surgeon General's challenge on opioids
Expanding the PHS Mission
Next: The Surgeon General's challenge on opioids
The Surgeon General's Challenge on Opioids
In December 2018, Federal Practitioner sat down with Surgeon General VADM Jerome M. Adams, MD, MPH to discuss recent initiatives to combat the opioid epidemic and to improve health care engagement and delivery in this exclusive video interview. During 2018, the Office of the Surgeon General took a number of steps to address the ongoing opioid crisis, releasing a public health advisory to urge increased use of naloxone, which can reverse the effects of an opioid overdose. In addition, the office of the Surgeon General released a postcard with 5 actions every person can take to address the opioid epidemic.
Increasing Health Care Engagement
Next: Community health and economic prosperity, What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
Community Health and Economic Prosperity
Next: What health care providers can do for prevention, expanding the PHS mission, the Surgeon General's challenge on opioids
What Health Care Providers Can Do for Prevention
Next: Expanding the PHS mission, the Surgeon General's challenge on opioids
Expanding the PHS Mission
Next: The Surgeon General's challenge on opioids
The Surgeon General's Challenge on Opioids
Flu season intensifies: High activity now in 19 states
The effects of the flu became much more widespread in the last full week of 2018 as the number of states with a high level of influenza activity more than doubled from the week before, according to the Centers for Disease Control and Prevention.
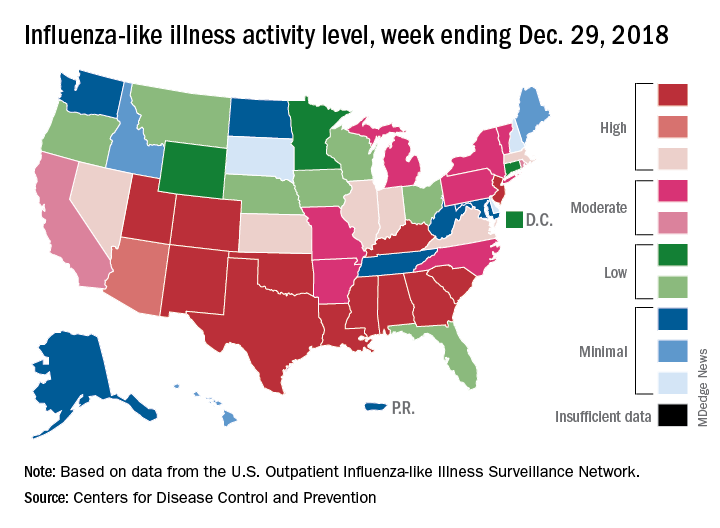
A total of 19 states were in the high range (8-10) on the CDC’s 1-10 scale of influenza-like illness (ILI) activity for the week ending Dec. 29, compared with 9 states the week before, the CDC’s influenza division reported Jan. 4. Of those 19 most-affected states, 12 were at level 10, 1 was at level 9, and 6 were at level 8. Geographic distribution of the virus was reported to be widespread in 24 states, the CDC said.
The proportion of outpatient visits for ILI – defined as fever (temperature of 100° F or greater) and cough and/or sore throat – rose to 4.1% for the week, which was up from 3.3% the previous week and well above the national baseline of 2.2%.
“The increase in the percentage of patient visits for ILI may be influenced in part by a reduction in routine health care visits during the winter holidays,” the report noted. There were 38 influenza deaths reported for the most recent week with available data (the week ending Dec. 22), although reporting for that week was just over 54% complete as of Jan. 4. For the previous weeks, 39 flu-related deaths occurred during the week ending Dec. 15 (reporting 84% complete) and 43 deaths during the week ending Dec. 8 (reporting 94% complete). For the respective weeks of last year’s flu season, total deaths were 359, 165, and 118, CDC data show.
For the week ending Dec. 29, two pediatric deaths were reported, one of which occurred the week before. For the 2018-2019 season so far, 13 flu-related pediatric deaths have been reported, the CDC said.
The effects of the flu became much more widespread in the last full week of 2018 as the number of states with a high level of influenza activity more than doubled from the week before, according to the Centers for Disease Control and Prevention.
A total of 19 states were in the high range (8-10) on the CDC’s 1-10 scale of influenza-like illness (ILI) activity for the week ending Dec. 29, compared with 9 states the week before, the CDC’s influenza division reported Jan. 4. Of those 19 most-affected states, 12 were at level 10, 1 was at level 9, and 6 were at level 8. Geographic distribution of the virus was reported to be widespread in 24 states, the CDC said.
The proportion of outpatient visits for ILI – defined as fever (temperature of 100° F or greater) and cough and/or sore throat – rose to 4.1% for the week, which was up from 3.3% the previous week and well above the national baseline of 2.2%.
“The increase in the percentage of patient visits for ILI may be influenced in part by a reduction in routine health care visits during the winter holidays,” the report noted. There were 38 influenza deaths reported for the most recent week with available data (the week ending Dec. 22), although reporting for that week was just over 54% complete as of Jan. 4. For the previous weeks, 39 flu-related deaths occurred during the week ending Dec. 15 (reporting 84% complete) and 43 deaths during the week ending Dec. 8 (reporting 94% complete). For the respective weeks of last year’s flu season, total deaths were 359, 165, and 118, CDC data show.
For the week ending Dec. 29, two pediatric deaths were reported, one of which occurred the week before. For the 2018-2019 season so far, 13 flu-related pediatric deaths have been reported, the CDC said.
The effects of the flu became much more widespread in the last full week of 2018 as the number of states with a high level of influenza activity more than doubled from the week before, according to the Centers for Disease Control and Prevention.
A total of 19 states were in the high range (8-10) on the CDC’s 1-10 scale of influenza-like illness (ILI) activity for the week ending Dec. 29, compared with 9 states the week before, the CDC’s influenza division reported Jan. 4. Of those 19 most-affected states, 12 were at level 10, 1 was at level 9, and 6 were at level 8. Geographic distribution of the virus was reported to be widespread in 24 states, the CDC said.
The proportion of outpatient visits for ILI – defined as fever (temperature of 100° F or greater) and cough and/or sore throat – rose to 4.1% for the week, which was up from 3.3% the previous week and well above the national baseline of 2.2%.
“The increase in the percentage of patient visits for ILI may be influenced in part by a reduction in routine health care visits during the winter holidays,” the report noted. There were 38 influenza deaths reported for the most recent week with available data (the week ending Dec. 22), although reporting for that week was just over 54% complete as of Jan. 4. For the previous weeks, 39 flu-related deaths occurred during the week ending Dec. 15 (reporting 84% complete) and 43 deaths during the week ending Dec. 8 (reporting 94% complete). For the respective weeks of last year’s flu season, total deaths were 359, 165, and 118, CDC data show.
For the week ending Dec. 29, two pediatric deaths were reported, one of which occurred the week before. For the 2018-2019 season so far, 13 flu-related pediatric deaths have been reported, the CDC said.
Hospital Readmissions Reduction Program may be doing more harm than good
A Medicare program aimed at lowering readmissions to hospitals could be having an adverse effect on mortality.

Results from a retrospective cohort study of hospitalizations for heart failure, acute myocardial infarction, and pneumonia among Medicare beneficiaries aged 65 years and older between April 1, 2005 and March 31, 2015 (covering the period before and after the Medicare Hospital Readmissions Reduction Program was announced in April 2010 and implemented in October 2012) found a significant increase in 30-day post discharge mortality among heart failure and pneumonia patients.
“Most concerning, however, is the possibility that the relationship between the HRRP and postdischarge mortality for heart failure and pneumonia is causal, indicating that the HRRP led to changes in quality of care that adversely affected patients,” Rishi Wadhera, MD, Harvard Medical School, Boston, and his colleagues wrote in a report published Dec. 25, 2018, in JAMA.
They looked at 8.3 million hospitalizations for heart failure, acute MI, and pneumonia, among whom 7.9 million were alive at the time of discharge. There were roughly 270,000 deaths within 30 days of discharge for heart failure; 128,000 for acute MI; and 246,000 for pneumonia.
To examine trends, the timing was divided into four periods: two prior to the announcement of the HRRP (April 2005–September 2007 and October 2007–March 2010); a third covering the time when the HRRP was announced (April 2010–September 2012); and the fourth when HRRP was implemented (October 2012–March 2015).
They found that among patients discharged with heart failure, 30-day mortality was rising even before the announcement of the HRRP, by 0.27% from the first period to the second period. That baseline trend continued when the HRRP was announced, by 0.49%, from second period to third. The difference in change between those periods was 0.22%. After implementation, 30-day mortality increased by 0.52%, with a difference in change from the third period of 0.25%. Both changes were statistically significant.
Among pneumonia patients, postdischarge mortality was stable before HRRP, but significantly increased after HRRP announcement, by 0.26%, with a difference in change from the second period to the third period of 0.22%. After implementation, the 30-day postdischarge mortality was 0.44%, with a significant difference in change of 0.40%.
Acute MI was a different story. Postdischarge mortality decreased significantly after the implementation of the HRRP, by 0.22%. The difference in change was –0.26%.
The authors suggested that “some hospitals may have focused more resources and efforts on reducing or avoiding readmissions than on prioritizing survival.” They add that the increases in heart failure morbidity could be related to patients with more severe heart conditions.
They noted that “although hospitals that reduce readmissions also appear to reduce mortality, this hospital-level concordance does not reflect the change in readmissions and mortality at the level of the patient population, which is arguably of greater importance to individual patients and to public health.”
Further research is needed to understand whether the increase in 30-day postdischarge mortality is a result of the HRRP, the authors concluded.
SOURCE: Wadhera R et al. JAMA. 2018 Dec 25. doi: 10.1001/jama.2018.19232.
Evidence in this study shows that while the Hospital Readmissions Reduction Program my be succeeding in reducing hospital admissions, little evidence is available to show that it is having a positive effect on patient outcomes.
The Centers for Medicare & Medicaid Services needs to reexamine the program and find alternative methods that are both effective at reducing hospital readmissions while at the same time protect patients from unintentional harm, including death.
Gregg C. Fonarow, MD , University of California Medical Center, Los Angeles, in an editorial published in JAMA, Dec. 25, 2018. doi:10.1001/jama.2018.19325 .
Evidence in this study shows that while the Hospital Readmissions Reduction Program my be succeeding in reducing hospital admissions, little evidence is available to show that it is having a positive effect on patient outcomes.
The Centers for Medicare & Medicaid Services needs to reexamine the program and find alternative methods that are both effective at reducing hospital readmissions while at the same time protect patients from unintentional harm, including death.
Gregg C. Fonarow, MD , University of California Medical Center, Los Angeles, in an editorial published in JAMA, Dec. 25, 2018. doi:10.1001/jama.2018.19325 .
Evidence in this study shows that while the Hospital Readmissions Reduction Program my be succeeding in reducing hospital admissions, little evidence is available to show that it is having a positive effect on patient outcomes.
The Centers for Medicare & Medicaid Services needs to reexamine the program and find alternative methods that are both effective at reducing hospital readmissions while at the same time protect patients from unintentional harm, including death.
Gregg C. Fonarow, MD , University of California Medical Center, Los Angeles, in an editorial published in JAMA, Dec. 25, 2018. doi:10.1001/jama.2018.19325 .
A Medicare program aimed at lowering readmissions to hospitals could be having an adverse effect on mortality.
Results from a retrospective cohort study of hospitalizations for heart failure, acute myocardial infarction, and pneumonia among Medicare beneficiaries aged 65 years and older between April 1, 2005 and March 31, 2015 (covering the period before and after the Medicare Hospital Readmissions Reduction Program was announced in April 2010 and implemented in October 2012) found a significant increase in 30-day post discharge mortality among heart failure and pneumonia patients.
“Most concerning, however, is the possibility that the relationship between the HRRP and postdischarge mortality for heart failure and pneumonia is causal, indicating that the HRRP led to changes in quality of care that adversely affected patients,” Rishi Wadhera, MD, Harvard Medical School, Boston, and his colleagues wrote in a report published Dec. 25, 2018, in JAMA.
They looked at 8.3 million hospitalizations for heart failure, acute MI, and pneumonia, among whom 7.9 million were alive at the time of discharge. There were roughly 270,000 deaths within 30 days of discharge for heart failure; 128,000 for acute MI; and 246,000 for pneumonia.
To examine trends, the timing was divided into four periods: two prior to the announcement of the HRRP (April 2005–September 2007 and October 2007–March 2010); a third covering the time when the HRRP was announced (April 2010–September 2012); and the fourth when HRRP was implemented (October 2012–March 2015).
They found that among patients discharged with heart failure, 30-day mortality was rising even before the announcement of the HRRP, by 0.27% from the first period to the second period. That baseline trend continued when the HRRP was announced, by 0.49%, from second period to third. The difference in change between those periods was 0.22%. After implementation, 30-day mortality increased by 0.52%, with a difference in change from the third period of 0.25%. Both changes were statistically significant.
Among pneumonia patients, postdischarge mortality was stable before HRRP, but significantly increased after HRRP announcement, by 0.26%, with a difference in change from the second period to the third period of 0.22%. After implementation, the 30-day postdischarge mortality was 0.44%, with a significant difference in change of 0.40%.
Acute MI was a different story. Postdischarge mortality decreased significantly after the implementation of the HRRP, by 0.22%. The difference in change was –0.26%.
The authors suggested that “some hospitals may have focused more resources and efforts on reducing or avoiding readmissions than on prioritizing survival.” They add that the increases in heart failure morbidity could be related to patients with more severe heart conditions.
They noted that “although hospitals that reduce readmissions also appear to reduce mortality, this hospital-level concordance does not reflect the change in readmissions and mortality at the level of the patient population, which is arguably of greater importance to individual patients and to public health.”
Further research is needed to understand whether the increase in 30-day postdischarge mortality is a result of the HRRP, the authors concluded.
SOURCE: Wadhera R et al. JAMA. 2018 Dec 25. doi: 10.1001/jama.2018.19232.
A Medicare program aimed at lowering readmissions to hospitals could be having an adverse effect on mortality.
Results from a retrospective cohort study of hospitalizations for heart failure, acute myocardial infarction, and pneumonia among Medicare beneficiaries aged 65 years and older between April 1, 2005 and March 31, 2015 (covering the period before and after the Medicare Hospital Readmissions Reduction Program was announced in April 2010 and implemented in October 2012) found a significant increase in 30-day post discharge mortality among heart failure and pneumonia patients.
“Most concerning, however, is the possibility that the relationship between the HRRP and postdischarge mortality for heart failure and pneumonia is causal, indicating that the HRRP led to changes in quality of care that adversely affected patients,” Rishi Wadhera, MD, Harvard Medical School, Boston, and his colleagues wrote in a report published Dec. 25, 2018, in JAMA.
They looked at 8.3 million hospitalizations for heart failure, acute MI, and pneumonia, among whom 7.9 million were alive at the time of discharge. There were roughly 270,000 deaths within 30 days of discharge for heart failure; 128,000 for acute MI; and 246,000 for pneumonia.
To examine trends, the timing was divided into four periods: two prior to the announcement of the HRRP (April 2005–September 2007 and October 2007–March 2010); a third covering the time when the HRRP was announced (April 2010–September 2012); and the fourth when HRRP was implemented (October 2012–March 2015).
They found that among patients discharged with heart failure, 30-day mortality was rising even before the announcement of the HRRP, by 0.27% from the first period to the second period. That baseline trend continued when the HRRP was announced, by 0.49%, from second period to third. The difference in change between those periods was 0.22%. After implementation, 30-day mortality increased by 0.52%, with a difference in change from the third period of 0.25%. Both changes were statistically significant.
Among pneumonia patients, postdischarge mortality was stable before HRRP, but significantly increased after HRRP announcement, by 0.26%, with a difference in change from the second period to the third period of 0.22%. After implementation, the 30-day postdischarge mortality was 0.44%, with a significant difference in change of 0.40%.
Acute MI was a different story. Postdischarge mortality decreased significantly after the implementation of the HRRP, by 0.22%. The difference in change was –0.26%.
The authors suggested that “some hospitals may have focused more resources and efforts on reducing or avoiding readmissions than on prioritizing survival.” They add that the increases in heart failure morbidity could be related to patients with more severe heart conditions.
They noted that “although hospitals that reduce readmissions also appear to reduce mortality, this hospital-level concordance does not reflect the change in readmissions and mortality at the level of the patient population, which is arguably of greater importance to individual patients and to public health.”
Further research is needed to understand whether the increase in 30-day postdischarge mortality is a result of the HRRP, the authors concluded.
SOURCE: Wadhera R et al. JAMA. 2018 Dec 25. doi: 10.1001/jama.2018.19232.
FROM JAMA
Key clinical point:
Major finding: Heart failure patients saw mortality increase 0.52% after HRRP launched.
Study details: A retrospective cohort study across 10 years, including time before and after the implementation of the HRRP.
Disclosures: The Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology funded the study. No relevant conflicts of interest were disclosed.
Source: Wadhera R et al. JAMA 2018 Dec 25. doi: 10.1001/jama.2018.19232.
VHA Suicide Prevention Media Outreach Is Falling Short—But Not for Lack of Money
The VHA’s suicide prevention media outreach activities—including social media postings, public service announcements, paid media, and Suicide Prevention Month activities—shrank markedly in fiscal years 2017 and 2018, according to the Government Accountability Office (GAO).
Since 2010, the primary focus of the outreach campaign has been to raise awareness of the Veterans Crisis Line (VCL), with output falling into 2 main categories: unpaid (eg, social media, public service announcements [PSAs], website) and paid (digital media, such as online keyword searches, and “out-of-home” media, such as billboards).
But between 2016 and the first 10 months of 2018, social media content dropped from 339 pieces to only 47. VHA also had not aired a suicide prevention PSA in more than 1 year, the first time there has been a gap of more than 1 month since June 2012.
In 2015, with a budget of > $4 million, VHA ran 58 advertisements on Google, Bing, and Facebook; 30 billboards; 180 bus advertisements; > 19,000 radio advertisements; 252 print advertisements; and 39 movie theater placements across the US. Fiscal years 2013, 2014, and 2016 were similarly productive.
Meanwhile, in FY 2017, the VHA spent < 10% of its approximately $1.7 million on paid ads on Google and Bing. And as of September 2018, VHA said it had spent only $57,000 of its $6.2 million paid media budget.
The waning outreach is “inconsistent with VA’s strategic goals,” the GAO says, which identify suicide prevention as the agency’s top clinical priority for FY 2018 through 2024.
VHA officials said they had not spent all the available funds due to changes in leadership and organizational realignment of the suicide prevention program. The position of National Director for Suicide Prevention position, for example, was vacant from July 2017 to April 2018. It was filled temporarily for 6 months; the interim director was then hired permanently in April 2018.
Since 2016, the VHA says, the plan has been to have a national strategy for preventing veteran suicides—an average of 20 per day, according to the VA—using a public health approach, focusing less on raising awareness of the VCL and more on reaching veterans before the point of crisis. However, in May 2018, VHA officials told the GAO that they “were just beginning to conceptualize what the suicide prevention outreach campaign should look like moving forward.”
One problem, the GAO says, is that the VHA has not established targets for the majority of the metrics it uses to help gauge the effectiveness of the outreach campaign. As a result, the VHA does not have the information it needs for a full evaluation. The only target the VHA has set is for each PSA to rank in the top 10% of the Nielsen ratings because, it says, that is the only meaningful target available that is accepted industry-wide. (The GAO notes, however: “VHA could use information about how its metrics performed in the past to develop reasonable and meaningful targets for future performance.”)
The GAO has made 2 recommendations to the VA based on its audit:
- The Under Secretary for Health should establish an approach for overseeing its suicide prevention media outreach efforts that includes “clear delineation of roles and responsibilities for those in leadership and contract oversight roles, including during periods of staff turnover or program changes.”
- Officials within the Office of Mental Health and Suicide Prevention (OMHSP) must establish targets for the metrics used to evaluate the campaign’s effectiveness.
In written comments, the VA concurred with the GAO recommendations and provided a time line for addressing them. VA said OMHSP has made organizational improvements, including creating a new organizational structure. It also has plans to work with communications experts to develop metrics, targets, and an evaluation strategy, expected to be completed by April 2019.
The VHA’s suicide prevention media outreach activities—including social media postings, public service announcements, paid media, and Suicide Prevention Month activities—shrank markedly in fiscal years 2017 and 2018, according to the Government Accountability Office (GAO).
Since 2010, the primary focus of the outreach campaign has been to raise awareness of the Veterans Crisis Line (VCL), with output falling into 2 main categories: unpaid (eg, social media, public service announcements [PSAs], website) and paid (digital media, such as online keyword searches, and “out-of-home” media, such as billboards).
But between 2016 and the first 10 months of 2018, social media content dropped from 339 pieces to only 47. VHA also had not aired a suicide prevention PSA in more than 1 year, the first time there has been a gap of more than 1 month since June 2012.
In 2015, with a budget of > $4 million, VHA ran 58 advertisements on Google, Bing, and Facebook; 30 billboards; 180 bus advertisements; > 19,000 radio advertisements; 252 print advertisements; and 39 movie theater placements across the US. Fiscal years 2013, 2014, and 2016 were similarly productive.
Meanwhile, in FY 2017, the VHA spent < 10% of its approximately $1.7 million on paid ads on Google and Bing. And as of September 2018, VHA said it had spent only $57,000 of its $6.2 million paid media budget.
The waning outreach is “inconsistent with VA’s strategic goals,” the GAO says, which identify suicide prevention as the agency’s top clinical priority for FY 2018 through 2024.
VHA officials said they had not spent all the available funds due to changes in leadership and organizational realignment of the suicide prevention program. The position of National Director for Suicide Prevention position, for example, was vacant from July 2017 to April 2018. It was filled temporarily for 6 months; the interim director was then hired permanently in April 2018.
Since 2016, the VHA says, the plan has been to have a national strategy for preventing veteran suicides—an average of 20 per day, according to the VA—using a public health approach, focusing less on raising awareness of the VCL and more on reaching veterans before the point of crisis. However, in May 2018, VHA officials told the GAO that they “were just beginning to conceptualize what the suicide prevention outreach campaign should look like moving forward.”
One problem, the GAO says, is that the VHA has not established targets for the majority of the metrics it uses to help gauge the effectiveness of the outreach campaign. As a result, the VHA does not have the information it needs for a full evaluation. The only target the VHA has set is for each PSA to rank in the top 10% of the Nielsen ratings because, it says, that is the only meaningful target available that is accepted industry-wide. (The GAO notes, however: “VHA could use information about how its metrics performed in the past to develop reasonable and meaningful targets for future performance.”)
The GAO has made 2 recommendations to the VA based on its audit:
- The Under Secretary for Health should establish an approach for overseeing its suicide prevention media outreach efforts that includes “clear delineation of roles and responsibilities for those in leadership and contract oversight roles, including during periods of staff turnover or program changes.”
- Officials within the Office of Mental Health and Suicide Prevention (OMHSP) must establish targets for the metrics used to evaluate the campaign’s effectiveness.
In written comments, the VA concurred with the GAO recommendations and provided a time line for addressing them. VA said OMHSP has made organizational improvements, including creating a new organizational structure. It also has plans to work with communications experts to develop metrics, targets, and an evaluation strategy, expected to be completed by April 2019.
The VHA’s suicide prevention media outreach activities—including social media postings, public service announcements, paid media, and Suicide Prevention Month activities—shrank markedly in fiscal years 2017 and 2018, according to the Government Accountability Office (GAO).
Since 2010, the primary focus of the outreach campaign has been to raise awareness of the Veterans Crisis Line (VCL), with output falling into 2 main categories: unpaid (eg, social media, public service announcements [PSAs], website) and paid (digital media, such as online keyword searches, and “out-of-home” media, such as billboards).
But between 2016 and the first 10 months of 2018, social media content dropped from 339 pieces to only 47. VHA also had not aired a suicide prevention PSA in more than 1 year, the first time there has been a gap of more than 1 month since June 2012.
In 2015, with a budget of > $4 million, VHA ran 58 advertisements on Google, Bing, and Facebook; 30 billboards; 180 bus advertisements; > 19,000 radio advertisements; 252 print advertisements; and 39 movie theater placements across the US. Fiscal years 2013, 2014, and 2016 were similarly productive.
Meanwhile, in FY 2017, the VHA spent < 10% of its approximately $1.7 million on paid ads on Google and Bing. And as of September 2018, VHA said it had spent only $57,000 of its $6.2 million paid media budget.
The waning outreach is “inconsistent with VA’s strategic goals,” the GAO says, which identify suicide prevention as the agency’s top clinical priority for FY 2018 through 2024.
VHA officials said they had not spent all the available funds due to changes in leadership and organizational realignment of the suicide prevention program. The position of National Director for Suicide Prevention position, for example, was vacant from July 2017 to April 2018. It was filled temporarily for 6 months; the interim director was then hired permanently in April 2018.
Since 2016, the VHA says, the plan has been to have a national strategy for preventing veteran suicides—an average of 20 per day, according to the VA—using a public health approach, focusing less on raising awareness of the VCL and more on reaching veterans before the point of crisis. However, in May 2018, VHA officials told the GAO that they “were just beginning to conceptualize what the suicide prevention outreach campaign should look like moving forward.”
One problem, the GAO says, is that the VHA has not established targets for the majority of the metrics it uses to help gauge the effectiveness of the outreach campaign. As a result, the VHA does not have the information it needs for a full evaluation. The only target the VHA has set is for each PSA to rank in the top 10% of the Nielsen ratings because, it says, that is the only meaningful target available that is accepted industry-wide. (The GAO notes, however: “VHA could use information about how its metrics performed in the past to develop reasonable and meaningful targets for future performance.”)
The GAO has made 2 recommendations to the VA based on its audit:
- The Under Secretary for Health should establish an approach for overseeing its suicide prevention media outreach efforts that includes “clear delineation of roles and responsibilities for those in leadership and contract oversight roles, including during periods of staff turnover or program changes.”
- Officials within the Office of Mental Health and Suicide Prevention (OMHSP) must establish targets for the metrics used to evaluate the campaign’s effectiveness.
In written comments, the VA concurred with the GAO recommendations and provided a time line for addressing them. VA said OMHSP has made organizational improvements, including creating a new organizational structure. It also has plans to work with communications experts to develop metrics, targets, and an evaluation strategy, expected to be completed by April 2019.
Biomarkers predict asthma/COPD risk in 9/11 first responders
Elevated eosinophil levels and interleukin-4 (IL-4) levels were significantly associated with an increased risk of overlapping asthma and chronic obstructive pulmonary disease (COPD) in firefighters exposed to toxins at the World Trade Center on Sept. 11, 2001.

Patients with asthma/COPD overlap experience decreased quality of life and increased mortality, compared with patients who have either isolated COPD or isolated asthma, and longitudinal data on risk factors for the overlapping condition are lacking, wrote Ankura Singh, MPH, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in CHEST, the researchers reviewed data from 2,137 firefighters exposed to toxins at the World Trade Center on 9/11. The study participants underwent a bronchodilator pulmonary function test between Sept. 9, 2001, and Sept. 10, 2017, and at least three routine monitoring pulmonary function tests between these two dates.
In a multivariate analysis, eosinophil concentration of at least 300 cells/mcL was a significant predictor of asthma/COPD overlap. Serum IL-4 levels also were significant predictors of asthma/COPD overlap (hazard ratio, 1.51).
In addition, a greater concentration of IL-21 was associated with both isolated asthma and isolated COPD, but not with the overlap.
The study results were strengthened by the availability of pre-exposure medical data for the firefighters and the close follow-up, although limitations included the mostly white male population and a limited definition of asthma, the researchers noted.
However, the findings suggest that “high eosinophil concentrations, uniquely associated with asthma/COPD overlap in this population, may reflect biological pathways that predispose one to exaggerated inflammation and/or poor counterregulatory responses to inflammation, leading to reversible and fixed airflow obstruction,” they wrote. Consequently, early interventions targeting specific inflammatory pathways may improve lung function outcomes.
The study was supported in part by the National Institute of Occupational Safety and Health and the National Institutes of Health.
SOURCE: Singh A et al. CHEST. 2018 Dec;154;1301-10.
Elevated eosinophil levels and interleukin-4 (IL-4) levels were significantly associated with an increased risk of overlapping asthma and chronic obstructive pulmonary disease (COPD) in firefighters exposed to toxins at the World Trade Center on Sept. 11, 2001.
Patients with asthma/COPD overlap experience decreased quality of life and increased mortality, compared with patients who have either isolated COPD or isolated asthma, and longitudinal data on risk factors for the overlapping condition are lacking, wrote Ankura Singh, MPH, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in CHEST, the researchers reviewed data from 2,137 firefighters exposed to toxins at the World Trade Center on 9/11. The study participants underwent a bronchodilator pulmonary function test between Sept. 9, 2001, and Sept. 10, 2017, and at least three routine monitoring pulmonary function tests between these two dates.
In a multivariate analysis, eosinophil concentration of at least 300 cells/mcL was a significant predictor of asthma/COPD overlap. Serum IL-4 levels also were significant predictors of asthma/COPD overlap (hazard ratio, 1.51).
In addition, a greater concentration of IL-21 was associated with both isolated asthma and isolated COPD, but not with the overlap.
The study results were strengthened by the availability of pre-exposure medical data for the firefighters and the close follow-up, although limitations included the mostly white male population and a limited definition of asthma, the researchers noted.
However, the findings suggest that “high eosinophil concentrations, uniquely associated with asthma/COPD overlap in this population, may reflect biological pathways that predispose one to exaggerated inflammation and/or poor counterregulatory responses to inflammation, leading to reversible and fixed airflow obstruction,” they wrote. Consequently, early interventions targeting specific inflammatory pathways may improve lung function outcomes.
The study was supported in part by the National Institute of Occupational Safety and Health and the National Institutes of Health.
SOURCE: Singh A et al. CHEST. 2018 Dec;154;1301-10.
Elevated eosinophil levels and interleukin-4 (IL-4) levels were significantly associated with an increased risk of overlapping asthma and chronic obstructive pulmonary disease (COPD) in firefighters exposed to toxins at the World Trade Center on Sept. 11, 2001.
Patients with asthma/COPD overlap experience decreased quality of life and increased mortality, compared with patients who have either isolated COPD or isolated asthma, and longitudinal data on risk factors for the overlapping condition are lacking, wrote Ankura Singh, MPH, of Albert Einstein College of Medicine, New York, and colleagues.
In a study published in CHEST, the researchers reviewed data from 2,137 firefighters exposed to toxins at the World Trade Center on 9/11. The study participants underwent a bronchodilator pulmonary function test between Sept. 9, 2001, and Sept. 10, 2017, and at least three routine monitoring pulmonary function tests between these two dates.
In a multivariate analysis, eosinophil concentration of at least 300 cells/mcL was a significant predictor of asthma/COPD overlap. Serum IL-4 levels also were significant predictors of asthma/COPD overlap (hazard ratio, 1.51).
In addition, a greater concentration of IL-21 was associated with both isolated asthma and isolated COPD, but not with the overlap.
The study results were strengthened by the availability of pre-exposure medical data for the firefighters and the close follow-up, although limitations included the mostly white male population and a limited definition of asthma, the researchers noted.
However, the findings suggest that “high eosinophil concentrations, uniquely associated with asthma/COPD overlap in this population, may reflect biological pathways that predispose one to exaggerated inflammation and/or poor counterregulatory responses to inflammation, leading to reversible and fixed airflow obstruction,” they wrote. Consequently, early interventions targeting specific inflammatory pathways may improve lung function outcomes.
The study was supported in part by the National Institute of Occupational Safety and Health and the National Institutes of Health.
SOURCE: Singh A et al. CHEST. 2018 Dec;154;1301-10.
FROM CHEST
Key clinical point: Firefighters exposed to toxins at the World Trade Center on 9/11 who demonstrated elevated blood eosinophils and IL-4 levels were at increased risk for subsequent asthma/chronic obstructive pulmonary disease overlap.
Major finding: Increased eosinophils (300 cells/mcL or higher) was significantly associated with asthma/chronic obstructive pulmonary disease overlap (hazard ratio, 1.85).
Study details: The data come from 2,137 firefighters exposed to toxins at the World Trade Center in New York on 9/11.
Disclosures: The study was supported in part by the National Institute of Occupational Safety and Health and the National Institutes of Health.
Source: Singh A et al. CHEST. 2018 Dec; 154;1301-10.
CDC: Flu activity ‘high’ in nine states
according to the Centers for Disease Control and Prevention.
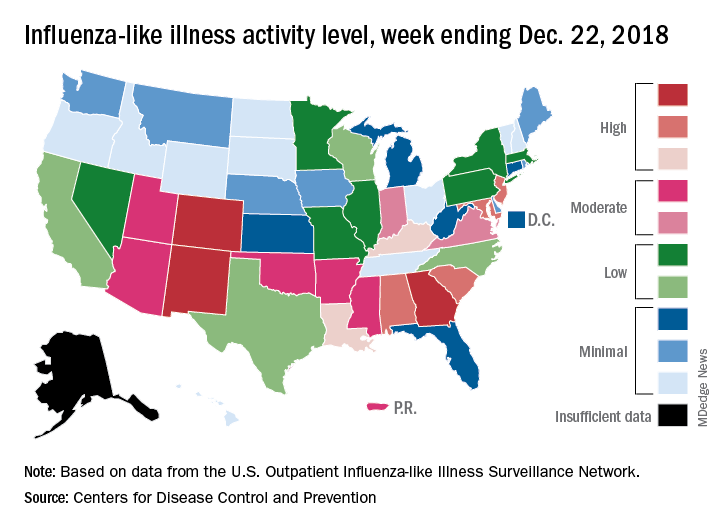
Patients with ILI made up an estimated 3.3% of outpatient visits for the week, which is up from 2.7% the previous week and well above the baseline rate of 2.2%, which the 2018-2019 flu season has now exceeded for the past 3 weeks, the CDC reported Dec. 28. ILI is defined “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Three states – Colorado, Georgia, and New Mexico – are now at the highest level of flu activity on the CDC’s 1-10 scale, and nine states are in the “high” range (8-10), compared with two states in high range (both at level 10) for the week ending Dec. 15. Another seven states and Puerto Rico are now in the “moderate” range of 6-7, data from the CDC’s Outpatient ILI Surveillance Network show.
Four flu-related deaths in children were reported during the week ending Dec. 22, two of which occurred in previous weeks, which brings the total to 11 for the 2018-2019 season, the CDC reported.
according to the Centers for Disease Control and Prevention.
Patients with ILI made up an estimated 3.3% of outpatient visits for the week, which is up from 2.7% the previous week and well above the baseline rate of 2.2%, which the 2018-2019 flu season has now exceeded for the past 3 weeks, the CDC reported Dec. 28. ILI is defined “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Three states – Colorado, Georgia, and New Mexico – are now at the highest level of flu activity on the CDC’s 1-10 scale, and nine states are in the “high” range (8-10), compared with two states in high range (both at level 10) for the week ending Dec. 15. Another seven states and Puerto Rico are now in the “moderate” range of 6-7, data from the CDC’s Outpatient ILI Surveillance Network show.
Four flu-related deaths in children were reported during the week ending Dec. 22, two of which occurred in previous weeks, which brings the total to 11 for the 2018-2019 season, the CDC reported.
according to the Centers for Disease Control and Prevention.
Patients with ILI made up an estimated 3.3% of outpatient visits for the week, which is up from 2.7% the previous week and well above the baseline rate of 2.2%, which the 2018-2019 flu season has now exceeded for the past 3 weeks, the CDC reported Dec. 28. ILI is defined “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Three states – Colorado, Georgia, and New Mexico – are now at the highest level of flu activity on the CDC’s 1-10 scale, and nine states are in the “high” range (8-10), compared with two states in high range (both at level 10) for the week ending Dec. 15. Another seven states and Puerto Rico are now in the “moderate” range of 6-7, data from the CDC’s Outpatient ILI Surveillance Network show.
Four flu-related deaths in children were reported during the week ending Dec. 22, two of which occurred in previous weeks, which brings the total to 11 for the 2018-2019 season, the CDC reported.
Guideline-concordant treatment still unlikely in nonchildren’s hospitals for pediatric CAP
according to new research.

“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
according to new research.
“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
according to new research.
“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
FROM JAMA PEDIATRICS
Pregnant women commonly refuse the influenza vaccine
Pregnant women commonly refuse vaccines, and refusal of influenza vaccine is more common than refusal of Tdap vaccine, according to a nationally representative survey of obstetrician/gynecologists.

“It appears vaccine refusal among pregnant women may be more common than parental refusal of childhood vaccines,” Sean T. O’Leary, MD, MPH, director of the Colorado Children’s Outcomes Network at the University of Colorado in Aurora, and his coauthors wrote in Obstetrics & Gynecology.
The survey was sent to 477 ob.gyns. via both email and mail between March and June 2016. The response rate was 69%, and almost all respondents reported recommending both influenza (97%) and Tdap (95%) vaccines to pregnant women.
However, respondents also reported that refusal of both vaccines was common, with more refusals of influenza vaccine than Tdap vaccine. Of ob.gyns. who responded, 62% reported that 10% or greater of their pregnant patients refused the influenza vaccine, compared with 32% reporting this for Tdap vaccine (P greater than .001; x2, less than 10% vs. 10% or greater). Of those refusing the vaccine, 48% believed influenza vaccine would make them sick; 38% felt they were unlikely to get a vaccine-preventable disease; and 32% had general worries about vaccines overall. In addition, the only strategy perceived as “very effective” in convincing a vaccine refuser to choose otherwise was “explaining that not getting the vaccine puts the fetus or newborn at risk.”
The authors shared potential limitations of their study, including the fact that they examined reported practices and perceptions, not observed practices, along with the potential that the attitudes and practices of respondents may differ from those of nonrespondents. However, they noted that this is unlikely given prior work and that next steps should consider responses to refusal while also sympathizing with the patients’ concerns. “Future work should focus on testing evidence-based strategies for addressing vaccine refusal in the obstetric setting and understanding how the unique concerns of pregnant women influence the effectiveness of such strategies,” they wrote.
The study was funded by the Centers for Disease Control and Prevention. No conflicts of interest were reported.
SOURCE: O’Leary ST et al. Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003005.
Pregnant women make up 1% of the population but accounted for 5% of all influenza deaths during the 2009 H1N1 pandemic, which makes the common vaccine refusals reported by the nation’s ob.gyns. all the more serious, according to Sonja A. Rasmussen, MD, MS, of the University of Florida in Gainesville and Denise J. Jamieson, MD, MPH, of Emory University in Atlanta.
After the 2009 pandemic, vaccination coverage for pregnant woman during flu season leapt from less than 30% to 54%, according to data from a 2016-2017 Internet panel survey. This was in large part because of the committed work of the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists, who emphasized the importance of the influenza vaccine. But coverage rates have stagnated since then, and these two coauthors wrote that “the 2017-2018 severe influenza season was a stern reminder that influenza should not be underestimated.”
These last 2 years saw the highest-documented rate of hospitalizations for influenza since 2005-2006, but given that there’s been very little specific information available on hospitalizations of pregnant women, Dr. Rasmussen and Dr. Jamieson fear the onset of “complacency among health care providers, pregnant women, and the general public” when it comes to the effects of influenza.
They insisted that, as 2009 drifts even further into memory, “obstetric providers should not become complacent regarding influenza.” Strategies to improve coverage are necessary to break that 50% barrier, and “pregnant women and their infants deserve our best efforts to protect them from influenza.”
These comments are adapted from an accompanying editorial (Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003040). No conflicts of interest were reported.
Pregnant women make up 1% of the population but accounted for 5% of all influenza deaths during the 2009 H1N1 pandemic, which makes the common vaccine refusals reported by the nation’s ob.gyns. all the more serious, according to Sonja A. Rasmussen, MD, MS, of the University of Florida in Gainesville and Denise J. Jamieson, MD, MPH, of Emory University in Atlanta.
After the 2009 pandemic, vaccination coverage for pregnant woman during flu season leapt from less than 30% to 54%, according to data from a 2016-2017 Internet panel survey. This was in large part because of the committed work of the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists, who emphasized the importance of the influenza vaccine. But coverage rates have stagnated since then, and these two coauthors wrote that “the 2017-2018 severe influenza season was a stern reminder that influenza should not be underestimated.”
These last 2 years saw the highest-documented rate of hospitalizations for influenza since 2005-2006, but given that there’s been very little specific information available on hospitalizations of pregnant women, Dr. Rasmussen and Dr. Jamieson fear the onset of “complacency among health care providers, pregnant women, and the general public” when it comes to the effects of influenza.
They insisted that, as 2009 drifts even further into memory, “obstetric providers should not become complacent regarding influenza.” Strategies to improve coverage are necessary to break that 50% barrier, and “pregnant women and their infants deserve our best efforts to protect them from influenza.”
These comments are adapted from an accompanying editorial (Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003040). No conflicts of interest were reported.
Pregnant women make up 1% of the population but accounted for 5% of all influenza deaths during the 2009 H1N1 pandemic, which makes the common vaccine refusals reported by the nation’s ob.gyns. all the more serious, according to Sonja A. Rasmussen, MD, MS, of the University of Florida in Gainesville and Denise J. Jamieson, MD, MPH, of Emory University in Atlanta.
After the 2009 pandemic, vaccination coverage for pregnant woman during flu season leapt from less than 30% to 54%, according to data from a 2016-2017 Internet panel survey. This was in large part because of the committed work of the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists, who emphasized the importance of the influenza vaccine. But coverage rates have stagnated since then, and these two coauthors wrote that “the 2017-2018 severe influenza season was a stern reminder that influenza should not be underestimated.”
These last 2 years saw the highest-documented rate of hospitalizations for influenza since 2005-2006, but given that there’s been very little specific information available on hospitalizations of pregnant women, Dr. Rasmussen and Dr. Jamieson fear the onset of “complacency among health care providers, pregnant women, and the general public” when it comes to the effects of influenza.
They insisted that, as 2009 drifts even further into memory, “obstetric providers should not become complacent regarding influenza.” Strategies to improve coverage are necessary to break that 50% barrier, and “pregnant women and their infants deserve our best efforts to protect them from influenza.”
These comments are adapted from an accompanying editorial (Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003040). No conflicts of interest were reported.
Pregnant women commonly refuse vaccines, and refusal of influenza vaccine is more common than refusal of Tdap vaccine, according to a nationally representative survey of obstetrician/gynecologists.
“It appears vaccine refusal among pregnant women may be more common than parental refusal of childhood vaccines,” Sean T. O’Leary, MD, MPH, director of the Colorado Children’s Outcomes Network at the University of Colorado in Aurora, and his coauthors wrote in Obstetrics & Gynecology.
The survey was sent to 477 ob.gyns. via both email and mail between March and June 2016. The response rate was 69%, and almost all respondents reported recommending both influenza (97%) and Tdap (95%) vaccines to pregnant women.
However, respondents also reported that refusal of both vaccines was common, with more refusals of influenza vaccine than Tdap vaccine. Of ob.gyns. who responded, 62% reported that 10% or greater of their pregnant patients refused the influenza vaccine, compared with 32% reporting this for Tdap vaccine (P greater than .001; x2, less than 10% vs. 10% or greater). Of those refusing the vaccine, 48% believed influenza vaccine would make them sick; 38% felt they were unlikely to get a vaccine-preventable disease; and 32% had general worries about vaccines overall. In addition, the only strategy perceived as “very effective” in convincing a vaccine refuser to choose otherwise was “explaining that not getting the vaccine puts the fetus or newborn at risk.”
The authors shared potential limitations of their study, including the fact that they examined reported practices and perceptions, not observed practices, along with the potential that the attitudes and practices of respondents may differ from those of nonrespondents. However, they noted that this is unlikely given prior work and that next steps should consider responses to refusal while also sympathizing with the patients’ concerns. “Future work should focus on testing evidence-based strategies for addressing vaccine refusal in the obstetric setting and understanding how the unique concerns of pregnant women influence the effectiveness of such strategies,” they wrote.
The study was funded by the Centers for Disease Control and Prevention. No conflicts of interest were reported.
SOURCE: O’Leary ST et al. Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003005.
Pregnant women commonly refuse vaccines, and refusal of influenza vaccine is more common than refusal of Tdap vaccine, according to a nationally representative survey of obstetrician/gynecologists.
“It appears vaccine refusal among pregnant women may be more common than parental refusal of childhood vaccines,” Sean T. O’Leary, MD, MPH, director of the Colorado Children’s Outcomes Network at the University of Colorado in Aurora, and his coauthors wrote in Obstetrics & Gynecology.
The survey was sent to 477 ob.gyns. via both email and mail between March and June 2016. The response rate was 69%, and almost all respondents reported recommending both influenza (97%) and Tdap (95%) vaccines to pregnant women.
However, respondents also reported that refusal of both vaccines was common, with more refusals of influenza vaccine than Tdap vaccine. Of ob.gyns. who responded, 62% reported that 10% or greater of their pregnant patients refused the influenza vaccine, compared with 32% reporting this for Tdap vaccine (P greater than .001; x2, less than 10% vs. 10% or greater). Of those refusing the vaccine, 48% believed influenza vaccine would make them sick; 38% felt they were unlikely to get a vaccine-preventable disease; and 32% had general worries about vaccines overall. In addition, the only strategy perceived as “very effective” in convincing a vaccine refuser to choose otherwise was “explaining that not getting the vaccine puts the fetus or newborn at risk.”
The authors shared potential limitations of their study, including the fact that they examined reported practices and perceptions, not observed practices, along with the potential that the attitudes and practices of respondents may differ from those of nonrespondents. However, they noted that this is unlikely given prior work and that next steps should consider responses to refusal while also sympathizing with the patients’ concerns. “Future work should focus on testing evidence-based strategies for addressing vaccine refusal in the obstetric setting and understanding how the unique concerns of pregnant women influence the effectiveness of such strategies,” they wrote.
The study was funded by the Centers for Disease Control and Prevention. No conflicts of interest were reported.
SOURCE: O’Leary ST et al. Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003005.
FROM OBSTETRICS & GYNECOLOGY
Key clinical point: Although almost all ob.gyns. recommend the influenza and Tdap vaccines for pregnant women, both commonly are refused.
Major finding: A total of 62% of ob.gyns. reported that 10% or greater of their pregnant patients refused the influenza vaccine; 32% reported this for Tdap vaccine.
Study details: An email and mail survey sent to a national network of ob.gyns. between March and June 2016.
Disclosures: The study was funded by the Centers for Disease Control and Prevention. No conflicts of interest were reported.
Source: O’Leary ST et al. Obstet Gynecol. 2018 Dec. doi: 10.1097/AOG.0000000000003005.
New insight gained into natural history of interstitial pneumonia with autoimmune features
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.

“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.
“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.
“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
REPORTING FROM the ACR ANNUAL MEETING
Key clinical point: The adjusted risk of progression to a systemic autoimmune rheumatic disease is 14.1 times greater in interstitial pneumonia with autoimmune features than in idiopathic interstitial lung disease without such features.
Major finding: A total of 16% of patients with interstitial pneumonia with autoimmune features progressed to a systemic autoimmune rheumatic disease during follow-up, compared with 1.6% of patients with idiopathic interstitial lung disease without such features.
Study details: This retrospective, single-center study included 174 patients with idiopathic interstitial lung disease followed for a median of 5.2 years.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was conducted free of commercial support.
Source: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.