User login
MD jailed for road rage, career spirals downhill
It was a 95° F day in July 2015, and emergency physician Martin Maag, MD, was driving down Bee Ridge Road, a busy seven-lane thoroughfare in Sarasota, Fla., on his way home from a family dinner. To distance himself from a truck blowing black smoke, Dr. Maag says he had just passed some vehicles, when a motorcycle flew past him in the turning lane and the passenger flipped him off.

“I started laughing because I knew we were coming up to a red light,” said Dr. Maag. “When we pulled up to the light, I put my window down and said: ‘Hey, you ought to be a little more careful about who you’re flipping off! You never know who it might be and what they might do.’ ”
The female passenger cursed at Dr. Maag, and the two traded profanities. The male driver then told Dr. Maag: “Get out of the car, old man,” according to Dr. Maag. Fuming, Dr. Maag got out of his black Tesla, and the two men met in the middle of the street.
“As soon as I got close enough to see him, I could tell he really looked young,” Dr. Maag recalls. “I said: ‘You’re like 12 years old. I’m going to end up beating your ass and then I’m going to go to jail. Go get on your bike, and ride home to your mom.’ I don’t remember what he said to me, but I spun around and said: ‘If you want to act like a man, meet me up the street in a parking lot and let’s have at it like men.’ ”
The motorcyclist got back on his white Suzuki and sped off, and Dr. Maag followed. Both vehicles went racing down the road, swerving between cars, and reaching speeds of 100 miles per hour, Dr. Maag said. At one point, Dr. Maag says he drove in front of the motorcyclist to slow him down, and the motorcycle clipped the back of his car. No one was seriously hurt, but soon Dr. Maag was in the back of a police cruiser headed to jail.
Dr. Maag wishes he could take back his actions that summer day 6 years ago. Those few minutes of fury have had lasting effects on the doctor’s life. The incident resulted in criminal charges, a jail sentence, thousands of dollars in legal fees, and a 3-year departure from emergency medicine. Although Dr. Maag did not lose his medical license as a result of the incident, the physician’s Medicare billing privileges were suspended because of a federal provision that ties some felonies to enrollment revocations.
“Every doctor, every health professional needs to know that there are a lot of consequences that go with our actions outside of work,” he said. “In my situation, what happened had nothing to do with medicine, it had nothing to do with patients, it had nothing to do my professional demeanor. But yet it affected my entire career, and I lost the ability to practice emergency medicine for 3 years. Three years for any doctor is a long time. Three years for emergency medicine is a lifetime.”
The physician ends up in jail
After the collision, Dr. Maag pulled over in a parking lot and dialed 911. Several passing motorists did the same. It appeared the biker was trying to get away, and Dr. Maag was concerned about the damage to his Tesla, he said.
When police arrived, they heard very different accounts of what happened. The motorcyclist and his girlfriend claimed Dr. Maag was the aggressor during the altercation, and that he deliberately tried to hit them with his vehicle. Two witnesses at the scene said they had watched Dr. Maag pursue the motorcycle in his vehicle, and that they believed he crossed into their lane intentionally to strike the motorcycle, according to police reports.
“[The motorcyclist] stated that the vehicle struck his right foot when it hit the motorcycle and that he was able to keep his balance and not lay the bike down,” Sarasota County Deputy C. Moore wrote in his report. “The motorcycle was damaged on the right side near [his] foot, verifying his story. Both victims were adamant that the defendant actually and intentionally struck the motorcycle with his car due to the previous altercation.”
Dr. Maag told officers the motorcyclist had initiated the confrontation. He acknowledged racing after the biker, but said it was the motorcyclist who hit his vehicle. In an interview, Dr. Maag disputed the witnesses’ accounts, saying that one of the witnesses was without a car and made claims to police that were impossible from her distance.
In the end, the officer believed the motorcyclist, writing in his report that the damage to the Tesla was consistent with the biker’s version of events. Dr. Maag was handcuffed and taken to the Sarasota County Jail.
“I was in shock,” he said. “When we got to the jail, they got me booked in and fingerprinted. I sat down and said [to an officer]: ‘So, when do I get to bond out?’ The guy started laughing and said: ‘You’re not going anywhere. You’re spending the night in jail, my friend.’ He said: ‘Your charge is one step below murder.’”
‘I like to drive fast’
Aside from speeding tickets, Dr. Maag said he had never been in serious trouble with the law before.
The husband and father of two has practiced emergency medicine for more 15 years, and his license has remained in good standing. Florida Department of Health records show Dr. Maag’s medical license as clear and active with no discipline cases or public complaints on file.
“I did my best for every patient that came through that door,” he said. “There were a lot of people who didn’t like my personality. I’ve said many times: ‘I’m not here to be liked. I’m here to take care of people and provide the best care possible.’ ”
Sarasota County records show that Dr. Maag has received traffic citations in the past for careless driving, unlawful speed, and failure to stop at a red light, among others. He admits to having a “lead foot,” but says he had never before been involved in a road rage incident.
“I’m not going to lie, I like to drive fast,” he said. “I like that feeling. It just seems to slow everything down for me, the faster I’m going.”
After being booked into jail that July evening in 2015, Dr. Maag called his wife to explain what happened.
“She said, ‘I can’t believe you’ve done this. I’ve told you a million times, don’t worry about how other people drive. Keep your mouth shut,’” he recalled. “I asked her to call my work and let them know I wouldn’t be coming in the next day. Until that happened, I had never missed a day of work since becoming a physician.”
After an anxious night in his jail cell, Dr. Maag lined up with the other inmates the next morning for his bond hearing. His charges included felony, aggravated battery, and felony aggravated assault with a deadly weapon. A prosecutor recommended Dr. Maag’s bond be set at $1 million, which a judge lowered to $500,000.
Michael Fayard, a criminal defense attorney who represented Dr. Maag in the case, said even with the reduction, $500,000 was an outrageous bond for such a case.
“The prosecutor’s arguments to the judge were that he was a physician driving a Tesla,” Mr. Fayard said. “That was his exact argument for charging him a higher bond. It shouldn’t have been that high. I argued he was not a flight risk. He didn’t even have a passport.”
The Florida State Attorney’s Office did not return messages seeking comment about the case.
Dr. Maag spent 2 more nights in jail while he and his wife came up with $50,000 in cash, in accordance with the 10% bond rule. In the meantime, the government put a lien on their house. A circuit court judge later agreed the bond was excessive, according to Mr. Fayard, but by that time, the $50,000 was paid and Dr. Maag was released.
New evidence lowers charges
Dr. Maag ultimately accepted a plea deal from the prosecutor’s office and pled no contest to one count of felony criminal mischief and one count of misdemeanor reckless driving. In return, the state dropped the two more serious felonies. A no-contest plea is not considered an admission of guilt.
Mr. Fayard said his investigation into the road rage victim unearthed evidence that poked holes in the motorcyclist’s credibility, and that contributed to the plea offer.
“We found tons of evidence about the kid being a hot-rodding rider on his motorcycle, videos of him traveling 140 miles an hour, popping wheelies, and darting in and out of traffic,” he said. “There was a lot of mitigation that came up during the course of the investigation.”
The plea deal was a favorable result for Dr. Maag considering his original charges, Mr. Fayard said. He added that the criminal case could have ended much differently.
“Given the facts of this case and given the fact that there were no serious injuries, we supported the state’s decision to accept our mitigation and come out with the sentence that they did,” Mr. Fayard said. “If there would have been injuries, the outcome would have likely been much worse for Dr. Maag.”
With the plea agreement reached, Dr. Maag faced his next consequence – jail time. He was sentenced to 60 days in jail, a $1,000 fine, 12 months of probation, and 8 months of house arrest. Unlike his first jail stay, Dr. Maag said the second, longer stint behind bars was more relaxing.
“It was the first time since I had become an emergency physician that I remember my dreams,” he recalled. “I had nothing to worry about, nothing to do. All I had to do was get up and eat. Every now and then, I would mop the floors because I’m kind of a clean freak, and I would talk to guys and that was it. It wasn’t bad at all.”
Dr. Maag told no one that he was a doctor because he didn’t want to be treated differently. The anonymity led to interesting tidbits from other inmates about the best pill mills in the area for example, how to make crack cocaine, and selling items for drugs. On his last day in jail, the other inmates learned from his discharge paperwork that Dr. Maag was a physician.
“One of the corrections officers said: ‘You’re a doctor? We’ve never had a doctor in here before!’” Dr. Maag remembers. “He said: ‘What did a doctor do to get into jail?’ I said: ‘Do you really want to know?’ ”
About the time that Dr. Maag was released from jail, the Florida Board of Medicine learned of his charges and began reviewing his case. Mr. Fayard presented the same facts to the board and argued for Dr. Maag to keep his license, emphasizing the offenses in which he was convicted were significantly less severe than the original felonies charged. The board agreed to dismiss the case.
“The probable cause panel for the board of medicine considered the complaint that has been filed against your client in the above referenced case,” Peter Delia, then-assistant general counsel for the Florida Department of Health, wrote in a letter dated April 27, 2016. “After careful review of all information and evidence obtained in this case, the panel determined that probable cause of a violation does not exist and directed this case to be closed.”
A short-lived celebration
Once home, Dr. Maag was on house arrest, but he was granted permission to travel for work. He continued to practice emergency medicine. After several months, authorities dropped the house arrest, and a judge canceled his probation early. It appeared the road rage incident was finally behind him.
But a year later, in 2018, the doctor received a letter from the Centers for Medicare & Medicaid Services informing him that because of his charges, his Medicare number had been revoked in November 2015.
“It took them 3 years to find me and tell me, even though I never moved,” he said. “Medicare said because I never reported this, they were hitting me up with falsification of documentation because I had signed other Medicare paperwork saying I had never been barred from Medicare, because I didn’t know that I was.”
Dr. Maag hired a different attorney to help him fight the 3-year enrollment ban. He requested reconsideration from CMS, but a hearing officer in October 2017 upheld the revocation. Because his privileges had been revoked in 2015, Dr. Maag’s practice group had to return all money billed by Dr. Maag to Medicare over the 3-year period, which totaled about $190,000.
A CMS spokeswoman declined to comment about Dr. Maag’s case, referring a reporter for this news organization to an administrative law judge’s decision that summarizes the agency’s findings.
According to the summary, in separate reconsidered determinations, the CMS hearing officer concluded that the revocation was proper under section 424.535(a)(3). The regulation, enacted in 2011, allows CMS to revoke billing privileges if a provider was convicted of a federal or state felony within the preceding 10 years that the agency determines is detrimental to the Medicare program and its beneficiaries.
The hearing officer reasoned that Dr. Maag “had been convicted of a felony that is akin to assault and, even if it were not, his actions showed a reckless disregard for the safety of others.” She concluded also that CMS could appropriately revoke Dr. Maag’s Medicare enrollment because he did not report his felony conviction within 30 days as required.
Dr. Maag went through several phases of fighting the revocation, including an appeal to the Department of Health & Human Services Departmental Appeals Board. He argued that his plea was a no-contest plea, which is not considered an admission of guilt. Dr. Maag and his attorney provided CMS a 15-page paper about his background, education, career accomplishments, and patient care history. They emphasized that Dr. Maag had never harmed or threatened a patient, and that his offense had nothing to do with his practice.
In February 2021, Judge Carolyn Cozad Hughes, an administrative law judge with CMS, upheld the 3-year revocation. In her decision, she wrote that for purposes of revocation under CMS law, “convicted” means that a judgment of conviction has been entered by a federal, state, or local court regardless of whether the judgment of conviction has been expunged or otherwise removed. She disagreed with Dr. Maag’s contention that his was a crime against property and, therefore, not akin to any of the felony offenses enumerated under the revocation section, which are crimes against persons.
“Even disregarding the allegations contained in the probable cause affidavit, Petitioner cannot escape the undisputed fact, established by his conviction and his own admissions, that the ‘property’ he so ‘willfully and maliciously’ damaged was a motorcycle traveling at a high rate of speed, and, that two young people were sitting atop that motorcycle,” Judge Hughes wrote. “Moreover, as part of the same conduct, he was charged – and convicted – of misdemeanor reckless driving with ‘willful and wanton disregard for the safety of persons or property.’ Thus, even accepting Petitioner’s description of the events, he unquestionably showed no regard for the safety of the young people on that motorcycle.”
Judge Hughes noted that, although Dr. Maag’s crimes may not be among those specified in the regulation, CMS has broad authority to determine which felonies are detrimental to the best interests of the program and its beneficiaries.
A new career path
Unable to practice emergency medicine and beset with debt, Dr. Maag spiraled into a dark depression. His family had to start using retirement money that he was saving for the future care of his son, who has autism.
“I was suicidal,” he said. “There were two times that I came very close to going out to the woods by my house and hanging myself. All I wanted was to have everything go away. My wife saved my life.”
Slowly, Dr. Maag climbed out of the despondency and began considering new career options. After working and training briefly in hair restoration, Dr. Maag became a hair transplant specialist and opened his own hair restoration practice. It was a way to practice and help patients without having to accept Medicare. Today, he is the founder of Honest Hair Restoration in Bradenton, Fla.
Hair restoration is not the type of medicine that he “was designed to do,” Dr. Maag said, but he has embraced its advantages, such as learning about the business aspects of medicine and having a slower-paced work life. The business, which opened in 2019, is doing well and growing steadily.
Earlier this month, Dr. Maag learned CMS had reinstated his Medicare billing privileges. If an opportunity arises to go back into emergency medicine or urgent care, he is open to the possibilities, he said, but he plans to continue hair restoration for now. He hopes the lessons learned from his road rage incident may help others in similar circumstances.
“If I could go back to that very moment, I would’ve just kept my window up and I wouldn’t have said anything,” Dr. Maag said. “I would’ve kept my mouth shut and gone on about my day. Would I have loved it to have never happened? Yeah, and I’d probably be starting my retirement now. Am I stronger now? Well, I’m probably a hell of a lot wiser. But when all is said and done, I don’t want anybody feeling sorry for me. It was all my doing and I have to live with the consequences.”
Mr. Fayard, the attorney, says the case is a cautionary tale for doctors.
“No one is really above the law,” he said. “There aren’t two legal systems. You can’t just pay a little money and be done. At every level, serious charges have serious ramifications for everyone involved. Law enforcement and judges are not going to care of you’re a physician and you commit a crime. But physicians have a lot more on the line than many others. They can lose their ability to practice.”
A version of this article first appeared on Medscape.com.
It was a 95° F day in July 2015, and emergency physician Martin Maag, MD, was driving down Bee Ridge Road, a busy seven-lane thoroughfare in Sarasota, Fla., on his way home from a family dinner. To distance himself from a truck blowing black smoke, Dr. Maag says he had just passed some vehicles, when a motorcycle flew past him in the turning lane and the passenger flipped him off.
“I started laughing because I knew we were coming up to a red light,” said Dr. Maag. “When we pulled up to the light, I put my window down and said: ‘Hey, you ought to be a little more careful about who you’re flipping off! You never know who it might be and what they might do.’ ”
The female passenger cursed at Dr. Maag, and the two traded profanities. The male driver then told Dr. Maag: “Get out of the car, old man,” according to Dr. Maag. Fuming, Dr. Maag got out of his black Tesla, and the two men met in the middle of the street.
“As soon as I got close enough to see him, I could tell he really looked young,” Dr. Maag recalls. “I said: ‘You’re like 12 years old. I’m going to end up beating your ass and then I’m going to go to jail. Go get on your bike, and ride home to your mom.’ I don’t remember what he said to me, but I spun around and said: ‘If you want to act like a man, meet me up the street in a parking lot and let’s have at it like men.’ ”
The motorcyclist got back on his white Suzuki and sped off, and Dr. Maag followed. Both vehicles went racing down the road, swerving between cars, and reaching speeds of 100 miles per hour, Dr. Maag said. At one point, Dr. Maag says he drove in front of the motorcyclist to slow him down, and the motorcycle clipped the back of his car. No one was seriously hurt, but soon Dr. Maag was in the back of a police cruiser headed to jail.
Dr. Maag wishes he could take back his actions that summer day 6 years ago. Those few minutes of fury have had lasting effects on the doctor’s life. The incident resulted in criminal charges, a jail sentence, thousands of dollars in legal fees, and a 3-year departure from emergency medicine. Although Dr. Maag did not lose his medical license as a result of the incident, the physician’s Medicare billing privileges were suspended because of a federal provision that ties some felonies to enrollment revocations.
“Every doctor, every health professional needs to know that there are a lot of consequences that go with our actions outside of work,” he said. “In my situation, what happened had nothing to do with medicine, it had nothing to do with patients, it had nothing to do my professional demeanor. But yet it affected my entire career, and I lost the ability to practice emergency medicine for 3 years. Three years for any doctor is a long time. Three years for emergency medicine is a lifetime.”
The physician ends up in jail
After the collision, Dr. Maag pulled over in a parking lot and dialed 911. Several passing motorists did the same. It appeared the biker was trying to get away, and Dr. Maag was concerned about the damage to his Tesla, he said.
When police arrived, they heard very different accounts of what happened. The motorcyclist and his girlfriend claimed Dr. Maag was the aggressor during the altercation, and that he deliberately tried to hit them with his vehicle. Two witnesses at the scene said they had watched Dr. Maag pursue the motorcycle in his vehicle, and that they believed he crossed into their lane intentionally to strike the motorcycle, according to police reports.
“[The motorcyclist] stated that the vehicle struck his right foot when it hit the motorcycle and that he was able to keep his balance and not lay the bike down,” Sarasota County Deputy C. Moore wrote in his report. “The motorcycle was damaged on the right side near [his] foot, verifying his story. Both victims were adamant that the defendant actually and intentionally struck the motorcycle with his car due to the previous altercation.”
Dr. Maag told officers the motorcyclist had initiated the confrontation. He acknowledged racing after the biker, but said it was the motorcyclist who hit his vehicle. In an interview, Dr. Maag disputed the witnesses’ accounts, saying that one of the witnesses was without a car and made claims to police that were impossible from her distance.
In the end, the officer believed the motorcyclist, writing in his report that the damage to the Tesla was consistent with the biker’s version of events. Dr. Maag was handcuffed and taken to the Sarasota County Jail.
“I was in shock,” he said. “When we got to the jail, they got me booked in and fingerprinted. I sat down and said [to an officer]: ‘So, when do I get to bond out?’ The guy started laughing and said: ‘You’re not going anywhere. You’re spending the night in jail, my friend.’ He said: ‘Your charge is one step below murder.’”
‘I like to drive fast’
Aside from speeding tickets, Dr. Maag said he had never been in serious trouble with the law before.
The husband and father of two has practiced emergency medicine for more 15 years, and his license has remained in good standing. Florida Department of Health records show Dr. Maag’s medical license as clear and active with no discipline cases or public complaints on file.
“I did my best for every patient that came through that door,” he said. “There were a lot of people who didn’t like my personality. I’ve said many times: ‘I’m not here to be liked. I’m here to take care of people and provide the best care possible.’ ”
Sarasota County records show that Dr. Maag has received traffic citations in the past for careless driving, unlawful speed, and failure to stop at a red light, among others. He admits to having a “lead foot,” but says he had never before been involved in a road rage incident.
“I’m not going to lie, I like to drive fast,” he said. “I like that feeling. It just seems to slow everything down for me, the faster I’m going.”
After being booked into jail that July evening in 2015, Dr. Maag called his wife to explain what happened.
“She said, ‘I can’t believe you’ve done this. I’ve told you a million times, don’t worry about how other people drive. Keep your mouth shut,’” he recalled. “I asked her to call my work and let them know I wouldn’t be coming in the next day. Until that happened, I had never missed a day of work since becoming a physician.”
After an anxious night in his jail cell, Dr. Maag lined up with the other inmates the next morning for his bond hearing. His charges included felony, aggravated battery, and felony aggravated assault with a deadly weapon. A prosecutor recommended Dr. Maag’s bond be set at $1 million, which a judge lowered to $500,000.
Michael Fayard, a criminal defense attorney who represented Dr. Maag in the case, said even with the reduction, $500,000 was an outrageous bond for such a case.
“The prosecutor’s arguments to the judge were that he was a physician driving a Tesla,” Mr. Fayard said. “That was his exact argument for charging him a higher bond. It shouldn’t have been that high. I argued he was not a flight risk. He didn’t even have a passport.”
The Florida State Attorney’s Office did not return messages seeking comment about the case.
Dr. Maag spent 2 more nights in jail while he and his wife came up with $50,000 in cash, in accordance with the 10% bond rule. In the meantime, the government put a lien on their house. A circuit court judge later agreed the bond was excessive, according to Mr. Fayard, but by that time, the $50,000 was paid and Dr. Maag was released.
New evidence lowers charges
Dr. Maag ultimately accepted a plea deal from the prosecutor’s office and pled no contest to one count of felony criminal mischief and one count of misdemeanor reckless driving. In return, the state dropped the two more serious felonies. A no-contest plea is not considered an admission of guilt.
Mr. Fayard said his investigation into the road rage victim unearthed evidence that poked holes in the motorcyclist’s credibility, and that contributed to the plea offer.
“We found tons of evidence about the kid being a hot-rodding rider on his motorcycle, videos of him traveling 140 miles an hour, popping wheelies, and darting in and out of traffic,” he said. “There was a lot of mitigation that came up during the course of the investigation.”
The plea deal was a favorable result for Dr. Maag considering his original charges, Mr. Fayard said. He added that the criminal case could have ended much differently.
“Given the facts of this case and given the fact that there were no serious injuries, we supported the state’s decision to accept our mitigation and come out with the sentence that they did,” Mr. Fayard said. “If there would have been injuries, the outcome would have likely been much worse for Dr. Maag.”
With the plea agreement reached, Dr. Maag faced his next consequence – jail time. He was sentenced to 60 days in jail, a $1,000 fine, 12 months of probation, and 8 months of house arrest. Unlike his first jail stay, Dr. Maag said the second, longer stint behind bars was more relaxing.
“It was the first time since I had become an emergency physician that I remember my dreams,” he recalled. “I had nothing to worry about, nothing to do. All I had to do was get up and eat. Every now and then, I would mop the floors because I’m kind of a clean freak, and I would talk to guys and that was it. It wasn’t bad at all.”
Dr. Maag told no one that he was a doctor because he didn’t want to be treated differently. The anonymity led to interesting tidbits from other inmates about the best pill mills in the area for example, how to make crack cocaine, and selling items for drugs. On his last day in jail, the other inmates learned from his discharge paperwork that Dr. Maag was a physician.
“One of the corrections officers said: ‘You’re a doctor? We’ve never had a doctor in here before!’” Dr. Maag remembers. “He said: ‘What did a doctor do to get into jail?’ I said: ‘Do you really want to know?’ ”
About the time that Dr. Maag was released from jail, the Florida Board of Medicine learned of his charges and began reviewing his case. Mr. Fayard presented the same facts to the board and argued for Dr. Maag to keep his license, emphasizing the offenses in which he was convicted were significantly less severe than the original felonies charged. The board agreed to dismiss the case.
“The probable cause panel for the board of medicine considered the complaint that has been filed against your client in the above referenced case,” Peter Delia, then-assistant general counsel for the Florida Department of Health, wrote in a letter dated April 27, 2016. “After careful review of all information and evidence obtained in this case, the panel determined that probable cause of a violation does not exist and directed this case to be closed.”
A short-lived celebration
Once home, Dr. Maag was on house arrest, but he was granted permission to travel for work. He continued to practice emergency medicine. After several months, authorities dropped the house arrest, and a judge canceled his probation early. It appeared the road rage incident was finally behind him.
But a year later, in 2018, the doctor received a letter from the Centers for Medicare & Medicaid Services informing him that because of his charges, his Medicare number had been revoked in November 2015.
“It took them 3 years to find me and tell me, even though I never moved,” he said. “Medicare said because I never reported this, they were hitting me up with falsification of documentation because I had signed other Medicare paperwork saying I had never been barred from Medicare, because I didn’t know that I was.”
Dr. Maag hired a different attorney to help him fight the 3-year enrollment ban. He requested reconsideration from CMS, but a hearing officer in October 2017 upheld the revocation. Because his privileges had been revoked in 2015, Dr. Maag’s practice group had to return all money billed by Dr. Maag to Medicare over the 3-year period, which totaled about $190,000.
A CMS spokeswoman declined to comment about Dr. Maag’s case, referring a reporter for this news organization to an administrative law judge’s decision that summarizes the agency’s findings.
According to the summary, in separate reconsidered determinations, the CMS hearing officer concluded that the revocation was proper under section 424.535(a)(3). The regulation, enacted in 2011, allows CMS to revoke billing privileges if a provider was convicted of a federal or state felony within the preceding 10 years that the agency determines is detrimental to the Medicare program and its beneficiaries.
The hearing officer reasoned that Dr. Maag “had been convicted of a felony that is akin to assault and, even if it were not, his actions showed a reckless disregard for the safety of others.” She concluded also that CMS could appropriately revoke Dr. Maag’s Medicare enrollment because he did not report his felony conviction within 30 days as required.
Dr. Maag went through several phases of fighting the revocation, including an appeal to the Department of Health & Human Services Departmental Appeals Board. He argued that his plea was a no-contest plea, which is not considered an admission of guilt. Dr. Maag and his attorney provided CMS a 15-page paper about his background, education, career accomplishments, and patient care history. They emphasized that Dr. Maag had never harmed or threatened a patient, and that his offense had nothing to do with his practice.
In February 2021, Judge Carolyn Cozad Hughes, an administrative law judge with CMS, upheld the 3-year revocation. In her decision, she wrote that for purposes of revocation under CMS law, “convicted” means that a judgment of conviction has been entered by a federal, state, or local court regardless of whether the judgment of conviction has been expunged or otherwise removed. She disagreed with Dr. Maag’s contention that his was a crime against property and, therefore, not akin to any of the felony offenses enumerated under the revocation section, which are crimes against persons.
“Even disregarding the allegations contained in the probable cause affidavit, Petitioner cannot escape the undisputed fact, established by his conviction and his own admissions, that the ‘property’ he so ‘willfully and maliciously’ damaged was a motorcycle traveling at a high rate of speed, and, that two young people were sitting atop that motorcycle,” Judge Hughes wrote. “Moreover, as part of the same conduct, he was charged – and convicted – of misdemeanor reckless driving with ‘willful and wanton disregard for the safety of persons or property.’ Thus, even accepting Petitioner’s description of the events, he unquestionably showed no regard for the safety of the young people on that motorcycle.”
Judge Hughes noted that, although Dr. Maag’s crimes may not be among those specified in the regulation, CMS has broad authority to determine which felonies are detrimental to the best interests of the program and its beneficiaries.
A new career path
Unable to practice emergency medicine and beset with debt, Dr. Maag spiraled into a dark depression. His family had to start using retirement money that he was saving for the future care of his son, who has autism.
“I was suicidal,” he said. “There were two times that I came very close to going out to the woods by my house and hanging myself. All I wanted was to have everything go away. My wife saved my life.”
Slowly, Dr. Maag climbed out of the despondency and began considering new career options. After working and training briefly in hair restoration, Dr. Maag became a hair transplant specialist and opened his own hair restoration practice. It was a way to practice and help patients without having to accept Medicare. Today, he is the founder of Honest Hair Restoration in Bradenton, Fla.
Hair restoration is not the type of medicine that he “was designed to do,” Dr. Maag said, but he has embraced its advantages, such as learning about the business aspects of medicine and having a slower-paced work life. The business, which opened in 2019, is doing well and growing steadily.
Earlier this month, Dr. Maag learned CMS had reinstated his Medicare billing privileges. If an opportunity arises to go back into emergency medicine or urgent care, he is open to the possibilities, he said, but he plans to continue hair restoration for now. He hopes the lessons learned from his road rage incident may help others in similar circumstances.
“If I could go back to that very moment, I would’ve just kept my window up and I wouldn’t have said anything,” Dr. Maag said. “I would’ve kept my mouth shut and gone on about my day. Would I have loved it to have never happened? Yeah, and I’d probably be starting my retirement now. Am I stronger now? Well, I’m probably a hell of a lot wiser. But when all is said and done, I don’t want anybody feeling sorry for me. It was all my doing and I have to live with the consequences.”
Mr. Fayard, the attorney, says the case is a cautionary tale for doctors.
“No one is really above the law,” he said. “There aren’t two legal systems. You can’t just pay a little money and be done. At every level, serious charges have serious ramifications for everyone involved. Law enforcement and judges are not going to care of you’re a physician and you commit a crime. But physicians have a lot more on the line than many others. They can lose their ability to practice.”
A version of this article first appeared on Medscape.com.
It was a 95° F day in July 2015, and emergency physician Martin Maag, MD, was driving down Bee Ridge Road, a busy seven-lane thoroughfare in Sarasota, Fla., on his way home from a family dinner. To distance himself from a truck blowing black smoke, Dr. Maag says he had just passed some vehicles, when a motorcycle flew past him in the turning lane and the passenger flipped him off.
“I started laughing because I knew we were coming up to a red light,” said Dr. Maag. “When we pulled up to the light, I put my window down and said: ‘Hey, you ought to be a little more careful about who you’re flipping off! You never know who it might be and what they might do.’ ”
The female passenger cursed at Dr. Maag, and the two traded profanities. The male driver then told Dr. Maag: “Get out of the car, old man,” according to Dr. Maag. Fuming, Dr. Maag got out of his black Tesla, and the two men met in the middle of the street.
“As soon as I got close enough to see him, I could tell he really looked young,” Dr. Maag recalls. “I said: ‘You’re like 12 years old. I’m going to end up beating your ass and then I’m going to go to jail. Go get on your bike, and ride home to your mom.’ I don’t remember what he said to me, but I spun around and said: ‘If you want to act like a man, meet me up the street in a parking lot and let’s have at it like men.’ ”
The motorcyclist got back on his white Suzuki and sped off, and Dr. Maag followed. Both vehicles went racing down the road, swerving between cars, and reaching speeds of 100 miles per hour, Dr. Maag said. At one point, Dr. Maag says he drove in front of the motorcyclist to slow him down, and the motorcycle clipped the back of his car. No one was seriously hurt, but soon Dr. Maag was in the back of a police cruiser headed to jail.
Dr. Maag wishes he could take back his actions that summer day 6 years ago. Those few minutes of fury have had lasting effects on the doctor’s life. The incident resulted in criminal charges, a jail sentence, thousands of dollars in legal fees, and a 3-year departure from emergency medicine. Although Dr. Maag did not lose his medical license as a result of the incident, the physician’s Medicare billing privileges were suspended because of a federal provision that ties some felonies to enrollment revocations.
“Every doctor, every health professional needs to know that there are a lot of consequences that go with our actions outside of work,” he said. “In my situation, what happened had nothing to do with medicine, it had nothing to do with patients, it had nothing to do my professional demeanor. But yet it affected my entire career, and I lost the ability to practice emergency medicine for 3 years. Three years for any doctor is a long time. Three years for emergency medicine is a lifetime.”
The physician ends up in jail
After the collision, Dr. Maag pulled over in a parking lot and dialed 911. Several passing motorists did the same. It appeared the biker was trying to get away, and Dr. Maag was concerned about the damage to his Tesla, he said.
When police arrived, they heard very different accounts of what happened. The motorcyclist and his girlfriend claimed Dr. Maag was the aggressor during the altercation, and that he deliberately tried to hit them with his vehicle. Two witnesses at the scene said they had watched Dr. Maag pursue the motorcycle in his vehicle, and that they believed he crossed into their lane intentionally to strike the motorcycle, according to police reports.
“[The motorcyclist] stated that the vehicle struck his right foot when it hit the motorcycle and that he was able to keep his balance and not lay the bike down,” Sarasota County Deputy C. Moore wrote in his report. “The motorcycle was damaged on the right side near [his] foot, verifying his story. Both victims were adamant that the defendant actually and intentionally struck the motorcycle with his car due to the previous altercation.”
Dr. Maag told officers the motorcyclist had initiated the confrontation. He acknowledged racing after the biker, but said it was the motorcyclist who hit his vehicle. In an interview, Dr. Maag disputed the witnesses’ accounts, saying that one of the witnesses was without a car and made claims to police that were impossible from her distance.
In the end, the officer believed the motorcyclist, writing in his report that the damage to the Tesla was consistent with the biker’s version of events. Dr. Maag was handcuffed and taken to the Sarasota County Jail.
“I was in shock,” he said. “When we got to the jail, they got me booked in and fingerprinted. I sat down and said [to an officer]: ‘So, when do I get to bond out?’ The guy started laughing and said: ‘You’re not going anywhere. You’re spending the night in jail, my friend.’ He said: ‘Your charge is one step below murder.’”
‘I like to drive fast’
Aside from speeding tickets, Dr. Maag said he had never been in serious trouble with the law before.
The husband and father of two has practiced emergency medicine for more 15 years, and his license has remained in good standing. Florida Department of Health records show Dr. Maag’s medical license as clear and active with no discipline cases or public complaints on file.
“I did my best for every patient that came through that door,” he said. “There were a lot of people who didn’t like my personality. I’ve said many times: ‘I’m not here to be liked. I’m here to take care of people and provide the best care possible.’ ”
Sarasota County records show that Dr. Maag has received traffic citations in the past for careless driving, unlawful speed, and failure to stop at a red light, among others. He admits to having a “lead foot,” but says he had never before been involved in a road rage incident.
“I’m not going to lie, I like to drive fast,” he said. “I like that feeling. It just seems to slow everything down for me, the faster I’m going.”
After being booked into jail that July evening in 2015, Dr. Maag called his wife to explain what happened.
“She said, ‘I can’t believe you’ve done this. I’ve told you a million times, don’t worry about how other people drive. Keep your mouth shut,’” he recalled. “I asked her to call my work and let them know I wouldn’t be coming in the next day. Until that happened, I had never missed a day of work since becoming a physician.”
After an anxious night in his jail cell, Dr. Maag lined up with the other inmates the next morning for his bond hearing. His charges included felony, aggravated battery, and felony aggravated assault with a deadly weapon. A prosecutor recommended Dr. Maag’s bond be set at $1 million, which a judge lowered to $500,000.
Michael Fayard, a criminal defense attorney who represented Dr. Maag in the case, said even with the reduction, $500,000 was an outrageous bond for such a case.
“The prosecutor’s arguments to the judge were that he was a physician driving a Tesla,” Mr. Fayard said. “That was his exact argument for charging him a higher bond. It shouldn’t have been that high. I argued he was not a flight risk. He didn’t even have a passport.”
The Florida State Attorney’s Office did not return messages seeking comment about the case.
Dr. Maag spent 2 more nights in jail while he and his wife came up with $50,000 in cash, in accordance with the 10% bond rule. In the meantime, the government put a lien on their house. A circuit court judge later agreed the bond was excessive, according to Mr. Fayard, but by that time, the $50,000 was paid and Dr. Maag was released.
New evidence lowers charges
Dr. Maag ultimately accepted a plea deal from the prosecutor’s office and pled no contest to one count of felony criminal mischief and one count of misdemeanor reckless driving. In return, the state dropped the two more serious felonies. A no-contest plea is not considered an admission of guilt.
Mr. Fayard said his investigation into the road rage victim unearthed evidence that poked holes in the motorcyclist’s credibility, and that contributed to the plea offer.
“We found tons of evidence about the kid being a hot-rodding rider on his motorcycle, videos of him traveling 140 miles an hour, popping wheelies, and darting in and out of traffic,” he said. “There was a lot of mitigation that came up during the course of the investigation.”
The plea deal was a favorable result for Dr. Maag considering his original charges, Mr. Fayard said. He added that the criminal case could have ended much differently.
“Given the facts of this case and given the fact that there were no serious injuries, we supported the state’s decision to accept our mitigation and come out with the sentence that they did,” Mr. Fayard said. “If there would have been injuries, the outcome would have likely been much worse for Dr. Maag.”
With the plea agreement reached, Dr. Maag faced his next consequence – jail time. He was sentenced to 60 days in jail, a $1,000 fine, 12 months of probation, and 8 months of house arrest. Unlike his first jail stay, Dr. Maag said the second, longer stint behind bars was more relaxing.
“It was the first time since I had become an emergency physician that I remember my dreams,” he recalled. “I had nothing to worry about, nothing to do. All I had to do was get up and eat. Every now and then, I would mop the floors because I’m kind of a clean freak, and I would talk to guys and that was it. It wasn’t bad at all.”
Dr. Maag told no one that he was a doctor because he didn’t want to be treated differently. The anonymity led to interesting tidbits from other inmates about the best pill mills in the area for example, how to make crack cocaine, and selling items for drugs. On his last day in jail, the other inmates learned from his discharge paperwork that Dr. Maag was a physician.
“One of the corrections officers said: ‘You’re a doctor? We’ve never had a doctor in here before!’” Dr. Maag remembers. “He said: ‘What did a doctor do to get into jail?’ I said: ‘Do you really want to know?’ ”
About the time that Dr. Maag was released from jail, the Florida Board of Medicine learned of his charges and began reviewing his case. Mr. Fayard presented the same facts to the board and argued for Dr. Maag to keep his license, emphasizing the offenses in which he was convicted were significantly less severe than the original felonies charged. The board agreed to dismiss the case.
“The probable cause panel for the board of medicine considered the complaint that has been filed against your client in the above referenced case,” Peter Delia, then-assistant general counsel for the Florida Department of Health, wrote in a letter dated April 27, 2016. “After careful review of all information and evidence obtained in this case, the panel determined that probable cause of a violation does not exist and directed this case to be closed.”
A short-lived celebration
Once home, Dr. Maag was on house arrest, but he was granted permission to travel for work. He continued to practice emergency medicine. After several months, authorities dropped the house arrest, and a judge canceled his probation early. It appeared the road rage incident was finally behind him.
But a year later, in 2018, the doctor received a letter from the Centers for Medicare & Medicaid Services informing him that because of his charges, his Medicare number had been revoked in November 2015.
“It took them 3 years to find me and tell me, even though I never moved,” he said. “Medicare said because I never reported this, they were hitting me up with falsification of documentation because I had signed other Medicare paperwork saying I had never been barred from Medicare, because I didn’t know that I was.”
Dr. Maag hired a different attorney to help him fight the 3-year enrollment ban. He requested reconsideration from CMS, but a hearing officer in October 2017 upheld the revocation. Because his privileges had been revoked in 2015, Dr. Maag’s practice group had to return all money billed by Dr. Maag to Medicare over the 3-year period, which totaled about $190,000.
A CMS spokeswoman declined to comment about Dr. Maag’s case, referring a reporter for this news organization to an administrative law judge’s decision that summarizes the agency’s findings.
According to the summary, in separate reconsidered determinations, the CMS hearing officer concluded that the revocation was proper under section 424.535(a)(3). The regulation, enacted in 2011, allows CMS to revoke billing privileges if a provider was convicted of a federal or state felony within the preceding 10 years that the agency determines is detrimental to the Medicare program and its beneficiaries.
The hearing officer reasoned that Dr. Maag “had been convicted of a felony that is akin to assault and, even if it were not, his actions showed a reckless disregard for the safety of others.” She concluded also that CMS could appropriately revoke Dr. Maag’s Medicare enrollment because he did not report his felony conviction within 30 days as required.
Dr. Maag went through several phases of fighting the revocation, including an appeal to the Department of Health & Human Services Departmental Appeals Board. He argued that his plea was a no-contest plea, which is not considered an admission of guilt. Dr. Maag and his attorney provided CMS a 15-page paper about his background, education, career accomplishments, and patient care history. They emphasized that Dr. Maag had never harmed or threatened a patient, and that his offense had nothing to do with his practice.
In February 2021, Judge Carolyn Cozad Hughes, an administrative law judge with CMS, upheld the 3-year revocation. In her decision, she wrote that for purposes of revocation under CMS law, “convicted” means that a judgment of conviction has been entered by a federal, state, or local court regardless of whether the judgment of conviction has been expunged or otherwise removed. She disagreed with Dr. Maag’s contention that his was a crime against property and, therefore, not akin to any of the felony offenses enumerated under the revocation section, which are crimes against persons.
“Even disregarding the allegations contained in the probable cause affidavit, Petitioner cannot escape the undisputed fact, established by his conviction and his own admissions, that the ‘property’ he so ‘willfully and maliciously’ damaged was a motorcycle traveling at a high rate of speed, and, that two young people were sitting atop that motorcycle,” Judge Hughes wrote. “Moreover, as part of the same conduct, he was charged – and convicted – of misdemeanor reckless driving with ‘willful and wanton disregard for the safety of persons or property.’ Thus, even accepting Petitioner’s description of the events, he unquestionably showed no regard for the safety of the young people on that motorcycle.”
Judge Hughes noted that, although Dr. Maag’s crimes may not be among those specified in the regulation, CMS has broad authority to determine which felonies are detrimental to the best interests of the program and its beneficiaries.
A new career path
Unable to practice emergency medicine and beset with debt, Dr. Maag spiraled into a dark depression. His family had to start using retirement money that he was saving for the future care of his son, who has autism.
“I was suicidal,” he said. “There were two times that I came very close to going out to the woods by my house and hanging myself. All I wanted was to have everything go away. My wife saved my life.”
Slowly, Dr. Maag climbed out of the despondency and began considering new career options. After working and training briefly in hair restoration, Dr. Maag became a hair transplant specialist and opened his own hair restoration practice. It was a way to practice and help patients without having to accept Medicare. Today, he is the founder of Honest Hair Restoration in Bradenton, Fla.
Hair restoration is not the type of medicine that he “was designed to do,” Dr. Maag said, but he has embraced its advantages, such as learning about the business aspects of medicine and having a slower-paced work life. The business, which opened in 2019, is doing well and growing steadily.
Earlier this month, Dr. Maag learned CMS had reinstated his Medicare billing privileges. If an opportunity arises to go back into emergency medicine or urgent care, he is open to the possibilities, he said, but he plans to continue hair restoration for now. He hopes the lessons learned from his road rage incident may help others in similar circumstances.
“If I could go back to that very moment, I would’ve just kept my window up and I wouldn’t have said anything,” Dr. Maag said. “I would’ve kept my mouth shut and gone on about my day. Would I have loved it to have never happened? Yeah, and I’d probably be starting my retirement now. Am I stronger now? Well, I’m probably a hell of a lot wiser. But when all is said and done, I don’t want anybody feeling sorry for me. It was all my doing and I have to live with the consequences.”
Mr. Fayard, the attorney, says the case is a cautionary tale for doctors.
“No one is really above the law,” he said. “There aren’t two legal systems. You can’t just pay a little money and be done. At every level, serious charges have serious ramifications for everyone involved. Law enforcement and judges are not going to care of you’re a physician and you commit a crime. But physicians have a lot more on the line than many others. They can lose their ability to practice.”
A version of this article first appeared on Medscape.com.
C. difficile guidelines offer new possibilities
The American College of Gastroenterology has issued new guidelines on management of Clostridioides difficile infection that now include roles for fecal microbial transplant (FMT), combination testing, and bezlotoxumab.

The ACG’s previous guidelines on the diagnosis, management, and treatment of what was then still called Clostridium difficile were published in 2013. Since then, the organism’s name changed to Clostridioides difficile, and that’s just the beginning of the changes reflected in the scientific literature, wrote lead author Colleen R. Kelly, MD, of Brown University, Providence, R.I., and colleagues.
“Other developments include the increased recognition of diagnostic challenges in the era of nucleic acid amplification–based testing, new therapeutic options for treatment and prevention of recurrence, and increasing evidence to support fecal microbiota transplantation (FMT) in recurrent and severe infection,” the authors said.
The guidelines, published in the American Journal of Gastroenterology, include 23 graded recommendations addressing issues of prevention, diagnosis, treatment, prevention of recurrence, and guidance for special populations in the management of C. difficile infection (CDI).
New faces among familiar ones
In terms of diagnosis, the new guidelines recommend using both a highly sensitive testing modality and a highly specific one to help distinguish colonization from active infection. Specifically, the authors recommend that stool is first tested using a highly sensitive test, either nucleic acid amplification testing or glutamate dehydrogenase, followed by an enzyme immunoassays for its high specificity.
Changes to treatment recommendations include the initial use of oral vancomycin or oral fidaxomicin for cases of nonsevere CDI. Oral metronidazole may be considered for initial nonsevere CDI in low-risk patients, the authors noted. The evidence is strong for the continued recommendations of vancomycin (125 mg four times daily for 10 days) and fidaxomicin (200 mg twice daily for 10 days) for patients with severe CDI. For patients with fulminant CDI, the recommendations call for medical therapy including volume resuscitation and oral vancomycin, although combination therapy with parenteral metronidazole may be considered despite the very low quality of evidence.
A notable update to the guidelines is the recommendation of fecal microbiota transplant (FMT) for both severe and fulminant CDI cases that are resistant to antibiotics and to prevent recurrence in at-risk patients. Although the quality of evidence is ranked as low, the recommendation is strong, the authors wrote. “Beyond improved cure rates, FMT may result in decreased rates of CDI-related colectomy and sepsis and may offer survival benefit in this critically ill patient population.” However, most patients in studies of FMT required multiple treatments in combination with anti-CDI antibiotics.
Other recommendations to prevent recurrence include oral vancomycin prophylaxis during the subsequent use of systemic antibiotics in patients with a history of CDI. The guidelines also recommend bezlotoxumab for prevention of CDI recurrence in high-risk patients, and advise against discontinuing antisecretory therapy in CDI patients if there is an appropriate indication for use.
Based on the lack of quality evidence, the guidelines recommend against the use of probiotics for preventing CDI in patients being treated with antibiotics and for prevention of recurrent infection.
Special populations
For patients with inflammatory bowel disease, the guidelines recommend C. difficile testing when these individuals present with acute flares and diarrhea, and the use of vancomycin for treatment. In addition, the authors strongly recommended FMT for recurrent CDI in these patients. For pregnant, postpartum, and breastfeeding patients with CDI, the guidelines recommend vancomycin, and either vancomycin or fidaxomicin may be used for treating CDI in immunocompromised patients, the authors noted.
The updated guidelines are designed to complement those issued by the Infections Disease Society of America and Society of Healthcare Epidemiologists of America, the researchers noted.
Reflecting the research
The previous guidelines for C. difficile were issued in 2013, and much has changed since then in terms of epidemiology, diagnosis, treatment, and infection control, Sahil Khanna, MBBS, MS, of the Mayo Clinic, Rochester, Minn., said in an interview.
Notably, diagnostic testing has “made leaps and bounds” and new treatments have become available that were not included in earlier guidelines, said Dr. Khanna. In particular, the new guidelines are recommending a two-step diagnostic assay; “the diagnostic algorithm has changed, and hopefully that will help us change practice” to identify active infection more quickly and efficiently.
Another important update is the recommendation of fidaxomicin as an option for initial nonfulminant CDI as an alternative to vancomycin, Dr. Khanna said, noting that metronidazole remains an option for low-risk patients. An additional change is the advice to use a different treatment for a second recurrent infection rather than repeating the initial treatment.
The recommendation of bezlotoxumab for prevention of CDI recurrence in patients who are at high risk of recurrence is the first time this drug has appeared in major guidelines, Dr. Khanna observed.
The recommendation in support of fecal microbiota transplant is a key update to the management of CDI, including the guidance that the procedure can be repeated if necessary, he said.
Looking ahead, “Additional research is needed to fully understand the best testing algorithms for CDI,” Dr. Khanna explained. “More studies also are needed to show how FMT fully fits into the picture, and some current studies are looking at its potential earlier in the course of infection.”
The guidelines were developed in collaboration with the Practice Parameters Committee of the American College of Gastroenterology and received no outside funding. Dr. Kelly disclosed serving as a site investigator of a clinical trial for Finch Therapeutics and is an unpaid clinical advisory board member for OpenBiome. Dr. Khanna has coauthored previous guidelines on C. difficile. He disclosed consulting relationships with Finch, GlaxoSmithKline, Jetson, ProbioTech, and Shire/Takeda, as well as research support from Rebiotix, Seres, and Vedanta.
The American College of Gastroenterology has issued new guidelines on management of Clostridioides difficile infection that now include roles for fecal microbial transplant (FMT), combination testing, and bezlotoxumab.
The ACG’s previous guidelines on the diagnosis, management, and treatment of what was then still called Clostridium difficile were published in 2013. Since then, the organism’s name changed to Clostridioides difficile, and that’s just the beginning of the changes reflected in the scientific literature, wrote lead author Colleen R. Kelly, MD, of Brown University, Providence, R.I., and colleagues.
“Other developments include the increased recognition of diagnostic challenges in the era of nucleic acid amplification–based testing, new therapeutic options for treatment and prevention of recurrence, and increasing evidence to support fecal microbiota transplantation (FMT) in recurrent and severe infection,” the authors said.
The guidelines, published in the American Journal of Gastroenterology, include 23 graded recommendations addressing issues of prevention, diagnosis, treatment, prevention of recurrence, and guidance for special populations in the management of C. difficile infection (CDI).
New faces among familiar ones
In terms of diagnosis, the new guidelines recommend using both a highly sensitive testing modality and a highly specific one to help distinguish colonization from active infection. Specifically, the authors recommend that stool is first tested using a highly sensitive test, either nucleic acid amplification testing or glutamate dehydrogenase, followed by an enzyme immunoassays for its high specificity.
Changes to treatment recommendations include the initial use of oral vancomycin or oral fidaxomicin for cases of nonsevere CDI. Oral metronidazole may be considered for initial nonsevere CDI in low-risk patients, the authors noted. The evidence is strong for the continued recommendations of vancomycin (125 mg four times daily for 10 days) and fidaxomicin (200 mg twice daily for 10 days) for patients with severe CDI. For patients with fulminant CDI, the recommendations call for medical therapy including volume resuscitation and oral vancomycin, although combination therapy with parenteral metronidazole may be considered despite the very low quality of evidence.
A notable update to the guidelines is the recommendation of fecal microbiota transplant (FMT) for both severe and fulminant CDI cases that are resistant to antibiotics and to prevent recurrence in at-risk patients. Although the quality of evidence is ranked as low, the recommendation is strong, the authors wrote. “Beyond improved cure rates, FMT may result in decreased rates of CDI-related colectomy and sepsis and may offer survival benefit in this critically ill patient population.” However, most patients in studies of FMT required multiple treatments in combination with anti-CDI antibiotics.
Other recommendations to prevent recurrence include oral vancomycin prophylaxis during the subsequent use of systemic antibiotics in patients with a history of CDI. The guidelines also recommend bezlotoxumab for prevention of CDI recurrence in high-risk patients, and advise against discontinuing antisecretory therapy in CDI patients if there is an appropriate indication for use.
Based on the lack of quality evidence, the guidelines recommend against the use of probiotics for preventing CDI in patients being treated with antibiotics and for prevention of recurrent infection.
Special populations
For patients with inflammatory bowel disease, the guidelines recommend C. difficile testing when these individuals present with acute flares and diarrhea, and the use of vancomycin for treatment. In addition, the authors strongly recommended FMT for recurrent CDI in these patients. For pregnant, postpartum, and breastfeeding patients with CDI, the guidelines recommend vancomycin, and either vancomycin or fidaxomicin may be used for treating CDI in immunocompromised patients, the authors noted.
The updated guidelines are designed to complement those issued by the Infections Disease Society of America and Society of Healthcare Epidemiologists of America, the researchers noted.
Reflecting the research
The previous guidelines for C. difficile were issued in 2013, and much has changed since then in terms of epidemiology, diagnosis, treatment, and infection control, Sahil Khanna, MBBS, MS, of the Mayo Clinic, Rochester, Minn., said in an interview.
Notably, diagnostic testing has “made leaps and bounds” and new treatments have become available that were not included in earlier guidelines, said Dr. Khanna. In particular, the new guidelines are recommending a two-step diagnostic assay; “the diagnostic algorithm has changed, and hopefully that will help us change practice” to identify active infection more quickly and efficiently.
Another important update is the recommendation of fidaxomicin as an option for initial nonfulminant CDI as an alternative to vancomycin, Dr. Khanna said, noting that metronidazole remains an option for low-risk patients. An additional change is the advice to use a different treatment for a second recurrent infection rather than repeating the initial treatment.
The recommendation of bezlotoxumab for prevention of CDI recurrence in patients who are at high risk of recurrence is the first time this drug has appeared in major guidelines, Dr. Khanna observed.
The recommendation in support of fecal microbiota transplant is a key update to the management of CDI, including the guidance that the procedure can be repeated if necessary, he said.
Looking ahead, “Additional research is needed to fully understand the best testing algorithms for CDI,” Dr. Khanna explained. “More studies also are needed to show how FMT fully fits into the picture, and some current studies are looking at its potential earlier in the course of infection.”
The guidelines were developed in collaboration with the Practice Parameters Committee of the American College of Gastroenterology and received no outside funding. Dr. Kelly disclosed serving as a site investigator of a clinical trial for Finch Therapeutics and is an unpaid clinical advisory board member for OpenBiome. Dr. Khanna has coauthored previous guidelines on C. difficile. He disclosed consulting relationships with Finch, GlaxoSmithKline, Jetson, ProbioTech, and Shire/Takeda, as well as research support from Rebiotix, Seres, and Vedanta.
The American College of Gastroenterology has issued new guidelines on management of Clostridioides difficile infection that now include roles for fecal microbial transplant (FMT), combination testing, and bezlotoxumab.
The ACG’s previous guidelines on the diagnosis, management, and treatment of what was then still called Clostridium difficile were published in 2013. Since then, the organism’s name changed to Clostridioides difficile, and that’s just the beginning of the changes reflected in the scientific literature, wrote lead author Colleen R. Kelly, MD, of Brown University, Providence, R.I., and colleagues.
“Other developments include the increased recognition of diagnostic challenges in the era of nucleic acid amplification–based testing, new therapeutic options for treatment and prevention of recurrence, and increasing evidence to support fecal microbiota transplantation (FMT) in recurrent and severe infection,” the authors said.
The guidelines, published in the American Journal of Gastroenterology, include 23 graded recommendations addressing issues of prevention, diagnosis, treatment, prevention of recurrence, and guidance for special populations in the management of C. difficile infection (CDI).
New faces among familiar ones
In terms of diagnosis, the new guidelines recommend using both a highly sensitive testing modality and a highly specific one to help distinguish colonization from active infection. Specifically, the authors recommend that stool is first tested using a highly sensitive test, either nucleic acid amplification testing or glutamate dehydrogenase, followed by an enzyme immunoassays for its high specificity.
Changes to treatment recommendations include the initial use of oral vancomycin or oral fidaxomicin for cases of nonsevere CDI. Oral metronidazole may be considered for initial nonsevere CDI in low-risk patients, the authors noted. The evidence is strong for the continued recommendations of vancomycin (125 mg four times daily for 10 days) and fidaxomicin (200 mg twice daily for 10 days) for patients with severe CDI. For patients with fulminant CDI, the recommendations call for medical therapy including volume resuscitation and oral vancomycin, although combination therapy with parenteral metronidazole may be considered despite the very low quality of evidence.
A notable update to the guidelines is the recommendation of fecal microbiota transplant (FMT) for both severe and fulminant CDI cases that are resistant to antibiotics and to prevent recurrence in at-risk patients. Although the quality of evidence is ranked as low, the recommendation is strong, the authors wrote. “Beyond improved cure rates, FMT may result in decreased rates of CDI-related colectomy and sepsis and may offer survival benefit in this critically ill patient population.” However, most patients in studies of FMT required multiple treatments in combination with anti-CDI antibiotics.
Other recommendations to prevent recurrence include oral vancomycin prophylaxis during the subsequent use of systemic antibiotics in patients with a history of CDI. The guidelines also recommend bezlotoxumab for prevention of CDI recurrence in high-risk patients, and advise against discontinuing antisecretory therapy in CDI patients if there is an appropriate indication for use.
Based on the lack of quality evidence, the guidelines recommend against the use of probiotics for preventing CDI in patients being treated with antibiotics and for prevention of recurrent infection.
Special populations
For patients with inflammatory bowel disease, the guidelines recommend C. difficile testing when these individuals present with acute flares and diarrhea, and the use of vancomycin for treatment. In addition, the authors strongly recommended FMT for recurrent CDI in these patients. For pregnant, postpartum, and breastfeeding patients with CDI, the guidelines recommend vancomycin, and either vancomycin or fidaxomicin may be used for treating CDI in immunocompromised patients, the authors noted.
The updated guidelines are designed to complement those issued by the Infections Disease Society of America and Society of Healthcare Epidemiologists of America, the researchers noted.
Reflecting the research
The previous guidelines for C. difficile were issued in 2013, and much has changed since then in terms of epidemiology, diagnosis, treatment, and infection control, Sahil Khanna, MBBS, MS, of the Mayo Clinic, Rochester, Minn., said in an interview.
Notably, diagnostic testing has “made leaps and bounds” and new treatments have become available that were not included in earlier guidelines, said Dr. Khanna. In particular, the new guidelines are recommending a two-step diagnostic assay; “the diagnostic algorithm has changed, and hopefully that will help us change practice” to identify active infection more quickly and efficiently.
Another important update is the recommendation of fidaxomicin as an option for initial nonfulminant CDI as an alternative to vancomycin, Dr. Khanna said, noting that metronidazole remains an option for low-risk patients. An additional change is the advice to use a different treatment for a second recurrent infection rather than repeating the initial treatment.
The recommendation of bezlotoxumab for prevention of CDI recurrence in patients who are at high risk of recurrence is the first time this drug has appeared in major guidelines, Dr. Khanna observed.
The recommendation in support of fecal microbiota transplant is a key update to the management of CDI, including the guidance that the procedure can be repeated if necessary, he said.
Looking ahead, “Additional research is needed to fully understand the best testing algorithms for CDI,” Dr. Khanna explained. “More studies also are needed to show how FMT fully fits into the picture, and some current studies are looking at its potential earlier in the course of infection.”
The guidelines were developed in collaboration with the Practice Parameters Committee of the American College of Gastroenterology and received no outside funding. Dr. Kelly disclosed serving as a site investigator of a clinical trial for Finch Therapeutics and is an unpaid clinical advisory board member for OpenBiome. Dr. Khanna has coauthored previous guidelines on C. difficile. He disclosed consulting relationships with Finch, GlaxoSmithKline, Jetson, ProbioTech, and Shire/Takeda, as well as research support from Rebiotix, Seres, and Vedanta.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
FDA to add myocarditis warning to mRNA COVID-19 vaccines
The Food and Drug Administration is adding a warning to mRNA COVID-19 vaccines’ fact sheets as medical experts continue to investigate cases of heart inflammation, which are rare but are more likely to occur in young men and teen boys.
Doran Fink, MD, PhD, deputy director of the FDA’s division of vaccines and related products applications, told a Centers for Disease Control and Prevention expert panel on June 23 that the FDA is finalizing language on a warning statement for health care providers, vaccine recipients, and parents or caregivers of teens.
The incidents are more likely to follow the second dose of the Pfizer or Moderna vaccine, with chest pain and other symptoms occurring within several days to a week, the warning will note.
“Based on limited follow-up, most cases appear to have been associated with resolution of symptoms, but limited information is available about potential long-term sequelae,” Dr. Fink said, describing the statement to the Advisory Committee on Immunization Practices, independent experts who advise the CDC.
“Symptoms suggestive of myocarditis or pericarditis should result in vaccine recipients seeking medical attention,” he said.
Benefits outweigh risks
Although no formal vote occurred after the meeting, the ACIP members delivered a strong endorsement for continuing to vaccinate 12- to 29-year-olds with the Pfizer and Moderna vaccines despite the warning.
“To me it’s clear, based on current information, that the benefits of vaccine clearly outweigh the risks,” said ACIP member Veronica McNally, president and CEO of the Franny Strong Foundation in Bloomfield, Mich., a sentiment echoed by other members.
As ACIP was meeting, leaders of the nation’s major physician, nurse, and public health associations issued a statement supporting continued vaccination: “The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination.
“Importantly, for the young people who do, most cases are mild, and individuals recover often on their own or with minimal treatment. In addition, we know that myocarditis and pericarditis are much more common if you get COVID-19, and the risks to the heart from COVID-19 infection can be more severe.”
ACIP heard the evidence behind that claim. According to the Vaccine Safety Datalink, which contains data from more than 12 million medical records, myocarditis or pericarditis occurs in 12- to 39-year-olds at a rate of 8 per 1 million after the second Pfizer dose and 19.8 per 1 million after the second Moderna dose.
The CDC continues to investigate the link between the mRNA vaccines and heart inflammation, including any differences between the vaccines.
Most of the symptoms resolved quickly, said Tom Shimabukuro, deputy director of CDC’s Immunization Safety Office. Of 323 cases analyzed by the CDC, 309 were hospitalized, 295 were discharged, and 218, or 79%, had recovered from symptoms.
“Most postvaccine myocarditis has been responding to minimal treatment,” pediatric cardiologist Matthew Oster, MD, MPH, from Children’s Healthcare of Atlanta, told the panel.
COVID ‘risks are higher’
Overall, the CDC has reported 2,767 COVID-19 deaths among people aged 12-29 years, and there have been 4,018 reported cases of the COVID-linked inflammatory disorder MIS-C since the beginning of the pandemic.
That amounts to 1 MIS-C case in every 3,200 COVID infections – 36% of them among teens aged 12-20 years and 62% among children who are Hispanic or Black and non-Hispanic, according to a CDC presentation.
The CDC estimated that every 1 million second-dose COVID vaccines administered to 12- to 17-year-old boys could prevent 5,700 cases of COVID-19, 215 hospitalizations, 71 ICU admissions, and 2 deaths. There could also be 56-69 myocarditis cases.
The emergence of new variants in the United States and the skewed pattern of vaccination around the country also may increase the risk to unvaccinated young people, noted Grace Lee, MD, MPH, chair of the ACIP’s COVID-19 Vaccine Safety Technical Subgroup and a pediatric infectious disease physician at Stanford (Calif.) Children’s Health.
“If you’re in an area with low vaccination, the risks are higher,” she said. “The benefits [of the vaccine] are going to be far, far greater than any risk.”
Individuals, parents, and their clinicians should consider the full scope of risk when making decisions about vaccination, she said.
As the pandemic evolves, medical experts have to balance the known risks and benefits while they gather more information, said William Schaffner, MD, an infectious disease physician at Vanderbilt University, Nashville, Tenn., and medical director of the National Foundation for Infectious Diseases.
“The story is not over,” Dr. Schaffner said in an interview. “Clearly, we are still working in the face of a pandemic, so there’s urgency to continue vaccinating. But they would like to know more about the long-term consequences of the myocarditis.”
Booster possibilities
Meanwhile, ACIP began conversations on the parameters for a possible vaccine booster. For now, there are simply questions: Would a third vaccine help the immunocompromised gain protection? Should people get a different type of vaccine – mRNA versus adenovirus vector – for their booster? Most important, how long do antibodies last?
“Prior to going around giving everyone boosters, we really need to improve the overall vaccination coverage,” said Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University. “That will protect everyone.”
A version of this article first appeared on Medscape.com.
The Food and Drug Administration is adding a warning to mRNA COVID-19 vaccines’ fact sheets as medical experts continue to investigate cases of heart inflammation, which are rare but are more likely to occur in young men and teen boys.
Doran Fink, MD, PhD, deputy director of the FDA’s division of vaccines and related products applications, told a Centers for Disease Control and Prevention expert panel on June 23 that the FDA is finalizing language on a warning statement for health care providers, vaccine recipients, and parents or caregivers of teens.
The incidents are more likely to follow the second dose of the Pfizer or Moderna vaccine, with chest pain and other symptoms occurring within several days to a week, the warning will note.
“Based on limited follow-up, most cases appear to have been associated with resolution of symptoms, but limited information is available about potential long-term sequelae,” Dr. Fink said, describing the statement to the Advisory Committee on Immunization Practices, independent experts who advise the CDC.
“Symptoms suggestive of myocarditis or pericarditis should result in vaccine recipients seeking medical attention,” he said.
Benefits outweigh risks
Although no formal vote occurred after the meeting, the ACIP members delivered a strong endorsement for continuing to vaccinate 12- to 29-year-olds with the Pfizer and Moderna vaccines despite the warning.
“To me it’s clear, based on current information, that the benefits of vaccine clearly outweigh the risks,” said ACIP member Veronica McNally, president and CEO of the Franny Strong Foundation in Bloomfield, Mich., a sentiment echoed by other members.
As ACIP was meeting, leaders of the nation’s major physician, nurse, and public health associations issued a statement supporting continued vaccination: “The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination.
“Importantly, for the young people who do, most cases are mild, and individuals recover often on their own or with minimal treatment. In addition, we know that myocarditis and pericarditis are much more common if you get COVID-19, and the risks to the heart from COVID-19 infection can be more severe.”
ACIP heard the evidence behind that claim. According to the Vaccine Safety Datalink, which contains data from more than 12 million medical records, myocarditis or pericarditis occurs in 12- to 39-year-olds at a rate of 8 per 1 million after the second Pfizer dose and 19.8 per 1 million after the second Moderna dose.
The CDC continues to investigate the link between the mRNA vaccines and heart inflammation, including any differences between the vaccines.
Most of the symptoms resolved quickly, said Tom Shimabukuro, deputy director of CDC’s Immunization Safety Office. Of 323 cases analyzed by the CDC, 309 were hospitalized, 295 were discharged, and 218, or 79%, had recovered from symptoms.
“Most postvaccine myocarditis has been responding to minimal treatment,” pediatric cardiologist Matthew Oster, MD, MPH, from Children’s Healthcare of Atlanta, told the panel.
COVID ‘risks are higher’
Overall, the CDC has reported 2,767 COVID-19 deaths among people aged 12-29 years, and there have been 4,018 reported cases of the COVID-linked inflammatory disorder MIS-C since the beginning of the pandemic.
That amounts to 1 MIS-C case in every 3,200 COVID infections – 36% of them among teens aged 12-20 years and 62% among children who are Hispanic or Black and non-Hispanic, according to a CDC presentation.
The CDC estimated that every 1 million second-dose COVID vaccines administered to 12- to 17-year-old boys could prevent 5,700 cases of COVID-19, 215 hospitalizations, 71 ICU admissions, and 2 deaths. There could also be 56-69 myocarditis cases.
The emergence of new variants in the United States and the skewed pattern of vaccination around the country also may increase the risk to unvaccinated young people, noted Grace Lee, MD, MPH, chair of the ACIP’s COVID-19 Vaccine Safety Technical Subgroup and a pediatric infectious disease physician at Stanford (Calif.) Children’s Health.
“If you’re in an area with low vaccination, the risks are higher,” she said. “The benefits [of the vaccine] are going to be far, far greater than any risk.”
Individuals, parents, and their clinicians should consider the full scope of risk when making decisions about vaccination, she said.
As the pandemic evolves, medical experts have to balance the known risks and benefits while they gather more information, said William Schaffner, MD, an infectious disease physician at Vanderbilt University, Nashville, Tenn., and medical director of the National Foundation for Infectious Diseases.
“The story is not over,” Dr. Schaffner said in an interview. “Clearly, we are still working in the face of a pandemic, so there’s urgency to continue vaccinating. But they would like to know more about the long-term consequences of the myocarditis.”
Booster possibilities
Meanwhile, ACIP began conversations on the parameters for a possible vaccine booster. For now, there are simply questions: Would a third vaccine help the immunocompromised gain protection? Should people get a different type of vaccine – mRNA versus adenovirus vector – for their booster? Most important, how long do antibodies last?
“Prior to going around giving everyone boosters, we really need to improve the overall vaccination coverage,” said Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University. “That will protect everyone.”
A version of this article first appeared on Medscape.com.
The Food and Drug Administration is adding a warning to mRNA COVID-19 vaccines’ fact sheets as medical experts continue to investigate cases of heart inflammation, which are rare but are more likely to occur in young men and teen boys.
Doran Fink, MD, PhD, deputy director of the FDA’s division of vaccines and related products applications, told a Centers for Disease Control and Prevention expert panel on June 23 that the FDA is finalizing language on a warning statement for health care providers, vaccine recipients, and parents or caregivers of teens.
The incidents are more likely to follow the second dose of the Pfizer or Moderna vaccine, with chest pain and other symptoms occurring within several days to a week, the warning will note.
“Based on limited follow-up, most cases appear to have been associated with resolution of symptoms, but limited information is available about potential long-term sequelae,” Dr. Fink said, describing the statement to the Advisory Committee on Immunization Practices, independent experts who advise the CDC.
“Symptoms suggestive of myocarditis or pericarditis should result in vaccine recipients seeking medical attention,” he said.
Benefits outweigh risks
Although no formal vote occurred after the meeting, the ACIP members delivered a strong endorsement for continuing to vaccinate 12- to 29-year-olds with the Pfizer and Moderna vaccines despite the warning.
“To me it’s clear, based on current information, that the benefits of vaccine clearly outweigh the risks,” said ACIP member Veronica McNally, president and CEO of the Franny Strong Foundation in Bloomfield, Mich., a sentiment echoed by other members.
As ACIP was meeting, leaders of the nation’s major physician, nurse, and public health associations issued a statement supporting continued vaccination: “The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination.
“Importantly, for the young people who do, most cases are mild, and individuals recover often on their own or with minimal treatment. In addition, we know that myocarditis and pericarditis are much more common if you get COVID-19, and the risks to the heart from COVID-19 infection can be more severe.”
ACIP heard the evidence behind that claim. According to the Vaccine Safety Datalink, which contains data from more than 12 million medical records, myocarditis or pericarditis occurs in 12- to 39-year-olds at a rate of 8 per 1 million after the second Pfizer dose and 19.8 per 1 million after the second Moderna dose.
The CDC continues to investigate the link between the mRNA vaccines and heart inflammation, including any differences between the vaccines.
Most of the symptoms resolved quickly, said Tom Shimabukuro, deputy director of CDC’s Immunization Safety Office. Of 323 cases analyzed by the CDC, 309 were hospitalized, 295 were discharged, and 218, or 79%, had recovered from symptoms.
“Most postvaccine myocarditis has been responding to minimal treatment,” pediatric cardiologist Matthew Oster, MD, MPH, from Children’s Healthcare of Atlanta, told the panel.
COVID ‘risks are higher’
Overall, the CDC has reported 2,767 COVID-19 deaths among people aged 12-29 years, and there have been 4,018 reported cases of the COVID-linked inflammatory disorder MIS-C since the beginning of the pandemic.
That amounts to 1 MIS-C case in every 3,200 COVID infections – 36% of them among teens aged 12-20 years and 62% among children who are Hispanic or Black and non-Hispanic, according to a CDC presentation.
The CDC estimated that every 1 million second-dose COVID vaccines administered to 12- to 17-year-old boys could prevent 5,700 cases of COVID-19, 215 hospitalizations, 71 ICU admissions, and 2 deaths. There could also be 56-69 myocarditis cases.
The emergence of new variants in the United States and the skewed pattern of vaccination around the country also may increase the risk to unvaccinated young people, noted Grace Lee, MD, MPH, chair of the ACIP’s COVID-19 Vaccine Safety Technical Subgroup and a pediatric infectious disease physician at Stanford (Calif.) Children’s Health.
“If you’re in an area with low vaccination, the risks are higher,” she said. “The benefits [of the vaccine] are going to be far, far greater than any risk.”
Individuals, parents, and their clinicians should consider the full scope of risk when making decisions about vaccination, she said.
As the pandemic evolves, medical experts have to balance the known risks and benefits while they gather more information, said William Schaffner, MD, an infectious disease physician at Vanderbilt University, Nashville, Tenn., and medical director of the National Foundation for Infectious Diseases.
“The story is not over,” Dr. Schaffner said in an interview. “Clearly, we are still working in the face of a pandemic, so there’s urgency to continue vaccinating. But they would like to know more about the long-term consequences of the myocarditis.”
Booster possibilities
Meanwhile, ACIP began conversations on the parameters for a possible vaccine booster. For now, there are simply questions: Would a third vaccine help the immunocompromised gain protection? Should people get a different type of vaccine – mRNA versus adenovirus vector – for their booster? Most important, how long do antibodies last?
“Prior to going around giving everyone boosters, we really need to improve the overall vaccination coverage,” said Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University. “That will protect everyone.”
A version of this article first appeared on Medscape.com.
‘Dreck’ to drama: How the media handled, and got handled by, COVID
For well over a year, the COVID-19 pandemic has been the biggest story in the world, costing millions of lives, impacting a presidential election, and quaking economies around the world.
But as vaccination rates increase and restrictions relax across the United States, relief is beginning to mix with reflection. Part of that contemplation means grappling with how the media depicted the crisis – in ways that were helpful, harmful, and somewhere in between.
“This story was so overwhelming, and the amount of journalism done about it was also overwhelming, and it’s going to be a while before we can do any kind of comprehensive overview of how journalism really performed,” said Maryn McKenna, an independent journalist and journalism professor at Emory University, Atlanta, who specializes in public and global health.
Some ‘heroically good’ reporting
The pandemic hit at a time when journalism was under a lot of pressure from external forces – undermined by politics, swimming through a sea of misinformation, and pressed by financial pressure to produce more stories more quickly, said Emily Bell, founding director of the Tow Center for Digital Journalism at Columbia University, New York.
The pandemic drove enormous audiences to news outlets, as people searched for reliable information, and increased the appreciation many people felt for the work of journalists, she said.
“I think there’s been some heroically good reporting and some really empathetic reporting as well,” said Ms. Bell. She cites The New York Times stories honoring the nearly 100,000 people lost to COVID-19 in May 2020 and The Atlantic’s COVID Tracking Project as exceptionally good examples.
Journalism is part of a complex, and evolving, information ecosystem characterized by “traditional” television, radio, and newspapers but also social media, search engine results, niche online news outlets, and clickbait sites.
On the one hand, social media provided a way for physicians, nurses, and scientists to speak directly to the world about their experiences and research. On the other hand, it’s challenging to elevate the really good work of traditional media over all of the bad or unhelpful signals, said Ms. Bell.
But, at the end of the day, much of journalism is a business. There are incentives in the market for tabloids to do sensational coverage and for outlets to push misleading, clickbait headlines, Ms. Bell said.
“Sometimes we’ll criticize journalists for ‘getting it wrong,’ but they might be getting it right in their business model but getting it wrong in terms of what it’s doing for society,” she said.
“We need to do a self-examination, when or if the dust from this ever settles, [on] how much of the past year was viewed as a business opportunity and did that get in the way of informing the public adequately,” Ms. McKenna said.
Digital platforms and journalists also need to reflect on how narratives build on one another, particularly online, said Ms. Bell. If you search for side effects of the Johnson & Johnson vaccine, for example, you will see a list of dozens of headlines that might give you the impression this is a major problem without the context that these effects are exceedingly rare, she notes.
There was also a personnel problem. Shrinking newsrooms over the last decade meant many outlets didn’t have dedicated science and health reporting, or very few staffers, if any. During the pandemic, suddenly general assignment and politics reporters had to be science and health reporters, too.
“You have a hard enough time with these issues if you’re a fairly seasoned science journalist,” said Gary Schwitzer, a former head of the health care news unit for CNN, journalism professor at the University of Minnesota, and founder of the watchdog site HealthNewsReview.org.
And outlets that had the staffing didn’t always put science reporters to full use, Ms. McKenna said. In March and April of 2020, major media outlets should have sent science reporters, not politics reporters, to President Donald Trump’s White House press briefings, which often included incorrect statements about COVID-19 science.
“I just don’t feel that the big outlets understood that that expertise would have made a difference,” she said.
New challenges, old problems
Some of the science journalism done during the pandemic has been some of the best ever seen in this country, said Mr. Schwitzer. But between the peaks of excellence, there is “the daily drumbeat coverage of dreck,” he added.
Many of the issues with this dreck coverage aren’t new or unique to the pandemic. For example, over the last year there have been far too many news stories based solely on weak information sources, like a drug company press release or a not-yet-peer-reviewed preprint article that hasn’t been put into proper context, said Mr. Schwitzer.
A quality science story should always include an independent perspective, he said, but many COVID-19 stories missed that perspective. This isn’t a new issue for science coverage – at Health News Review, Mr. Schwitzer and his colleagues saw stories without appropriate independent sources every day for 15 years.
It’s also challenging to write about uncertainty without over- or underselling what scientists know about a particular phenomenon. “We know that the media in general tends to portray science as more certain than it is,” said Dominique Brossard, PhD, professor and department chair at the University of Wisconsin–Madison and an expert on the intersection between science, media, and policy. This can lead to confusion when the science, and the advice based on that science, changes.
“The public has a really difficult time understanding what uncertainty means within science,” said Todd P. Newman, PhD, assistant professor at the University of Wisconsin–Madison who studies strategic communication within the context of science, technology, and the environment.
“I think the media generally has been good on the subject,” said Paul Offit, MD, director of the Vaccine Education Center, attending physician in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, and a prominent expert voice throughout the pandemic. “I think where they’ve been imperfect is they tend to be a little more dramatic in terms of how we’re doing.”
Dr. Offit isn’t the only expert to point to the drama of COVID-19 coverage. A study published in March 2021 by the National Bureau of Economic Research found 87% of stories by major U.S. media outlets leaned negative in the tone of their COVID-19 reporting, compared with 50% of stories from non-U.S. major outlets and 64% of articles in scientific journals. The negative emphasis persists even around positive developments, like vaccine trials and school re-openings.
John Whyte, MD, chief medical officer for WebMD, said he is very proud of the way WebMD and Medscape ramped up production of video series and other content to give health care providers the most up-to-date guidance on a rapidly evolving medical situation.
“But I think as [we] started to make progress – especially in the last 6 months – the coverage was never balanced enough; any positive news was immediately proceeded by negative,” he said.
“You want to be honest, but you also don’t want to be alarmist – and that’s where I think the challenge is at times in the media,” said Dr. Whyte. “We didn’t put enough optimism in at times, especially in recent months.”
“Any good coverage on vaccines immediately [was] covered by ‘[we] might need boosters in the fall.’ Why can’t [we] have an opportunity to breathe for a little while and see the good news?” he asked.
Variants or scariants?
Negativity and fear shaped much of the coverage around variants and vaccines earlier this year. In February 2021, Zeynep Tufekci, PhD, a sociologist at the University of North Carolina at Chapel Hill school of information and library science, wrote in The Atlantic about how much reporting has not reflected “the truly amazing reality of these vaccines,” and has instead highlighted “a chorus of relentless pessimism.”
This felt especially true earlier in 2021, when lots of coverage repeatedly emphasized what vaccinated people still could not do.
Eric Topol, MD, editor-in-chief of Medscape and executive vice president of Scripps Research in La Jolla, California, said New York Times editors told him earlier in the pandemic that he couldn’t use the word “scariant” in an opinion piece about the media’s overly fearful and sometimes inaccurate reporting around COVID-19 variants because they worried it would seem like the Times was coming after other media outlets.
“A variant is innocent until proven guilty,” said Dr. Topol. Had journalists approached the subject from that point of view, he said we would have seen “much more faithful reporting.”
Dr. Brossard and Dr. Newman worry that focusing on uncommon negative behavior, like people who break social distancing and mask rules by gathering at the beach or the bar, makes those actions seem more common than they actually are.
The evidence suggests that “if you show these kinds of things to people, you encourage them to do the same behavior,” said Dr. Brossard.
There have been other mistakes along the way, too. Early in the pandemic, many outlets pointed viewers to official government sources of information, some of which, like the White House press briefings in March and April of 2020, ended up being some of the most virulent spreaders of misinformation, said Ms. Bell.
Before that, a handful of journalists like Roxanne Khamsi were the few pushing back against the dominant media narrative in early 2020 that the novel coronavirus was less concerning than the seasonal flu.
“Science journalists have always been writing about studies that sometimes contradict each other, and what’s happened is that has only been condensed in time,” said Ms. Khamsi, a health care reporter for outlets like WIRED magazine and The New York Times and a former chief news editor for Nature Medicine.
Politics and misinformation
It’s impossible to talk about media coverage of COVID-19 without touching on politics and misinformation.
Coverage of the pandemic was politicized and polarized from the very beginning, said Sedona Chinn, PhD, an assistant professor at the University of Wisconsin–Madison who researches the prevalence and effects of scientific disagreements in media.
By looking at network news transcripts and articles from national outlets like the Washington Post and The New York Times, Dr. Chinn and her colleagues were able to determine politicization of coverage by counting the mentions of politicians versus scientists in COVID-19 coverage and polarization by looking at how different or similar the language was surrounding mentions of Republicans and Democrats.
If the two parties were working together or on the same page, they reasoned, the language would be similar.
From mid-March through May 2020, Dr. Chinn and fellow researchers found politicians were featured more often than scientists in newspaper coverage and as frequently as scientists in network news coverage. They also found polarized language around Republicans and Democrats, particularly in stories describing duels between the (at the time) Republican national government and Democratic state and local leaders.
It’s possible that polarization in news coverage helped contribute to polarized attitudes around the virus, the authors write in the study, which was published in August 2020 in the journal Science Communication.
The politicization and polarization of the issue is mirrored in our fractured media environment, where people tend to read, listen, and watch outlets that align with their political leanings. If that trusted outlet features misinformation, the people who follow it are more likely to accept that false information as truth, said Matt Motta, PhD, a political scientist at Oklahoma State University whose research includes public opinion and science communication.
This is true across the political spectrum, he said. When it comes to COVID-19, however, right-wing media outlets like Fox News and Breitbart are more likely to promote conspiratorial tropes and misinformation about the pandemic, according to Dr. Motta and his collaborator Dominik Stecula, PhD, a political scientist at Colorado State University who studies the news media environment and its effects on society.
Across the media ecosystem, reporting on the “infodemic” accompanying the pandemic – the rapid spread of misinformation and disinformation about the virus – has been a major challenge. Outlets may not be creating the misinformation, but they are the ones choosing to give it a platform, said Dr. Motta.
By repeating a false idea, even with the goal of debunking it, you can unintentionally cause the information to stick in people’s minds, said Dr. Brossard.
“Just because something is controversial doesn’t mean it’s worth covering,” said Dr. Motta. Using vaccines as an example, he said many reporters and scientists alike assume that if people have all the facts, they’ll land on the side of science.
“That is just fundamentally not how people think about the decision to get vaccinated,” he said. Instead, the choice is wrapped up with cultural factors, religious beliefs, political identity, and more.
The factors and challenges that shaped the media’s coverage of the pandemic aren’t going anywhere. Improving science and medical coverage in the future is a collective project for journalists, scientists, and everyone in between, said Dr. Newman.
“I call on scientists, too, to think really deeply about how they’re communicating – and especially how they’re communicating what they know and don’t know,” he said.
A version of this article first appeared on Medscape.com.
For well over a year, the COVID-19 pandemic has been the biggest story in the world, costing millions of lives, impacting a presidential election, and quaking economies around the world.
But as vaccination rates increase and restrictions relax across the United States, relief is beginning to mix with reflection. Part of that contemplation means grappling with how the media depicted the crisis – in ways that were helpful, harmful, and somewhere in between.
“This story was so overwhelming, and the amount of journalism done about it was also overwhelming, and it’s going to be a while before we can do any kind of comprehensive overview of how journalism really performed,” said Maryn McKenna, an independent journalist and journalism professor at Emory University, Atlanta, who specializes in public and global health.
Some ‘heroically good’ reporting
The pandemic hit at a time when journalism was under a lot of pressure from external forces – undermined by politics, swimming through a sea of misinformation, and pressed by financial pressure to produce more stories more quickly, said Emily Bell, founding director of the Tow Center for Digital Journalism at Columbia University, New York.
The pandemic drove enormous audiences to news outlets, as people searched for reliable information, and increased the appreciation many people felt for the work of journalists, she said.
“I think there’s been some heroically good reporting and some really empathetic reporting as well,” said Ms. Bell. She cites The New York Times stories honoring the nearly 100,000 people lost to COVID-19 in May 2020 and The Atlantic’s COVID Tracking Project as exceptionally good examples.
Journalism is part of a complex, and evolving, information ecosystem characterized by “traditional” television, radio, and newspapers but also social media, search engine results, niche online news outlets, and clickbait sites.
On the one hand, social media provided a way for physicians, nurses, and scientists to speak directly to the world about their experiences and research. On the other hand, it’s challenging to elevate the really good work of traditional media over all of the bad or unhelpful signals, said Ms. Bell.
But, at the end of the day, much of journalism is a business. There are incentives in the market for tabloids to do sensational coverage and for outlets to push misleading, clickbait headlines, Ms. Bell said.
“Sometimes we’ll criticize journalists for ‘getting it wrong,’ but they might be getting it right in their business model but getting it wrong in terms of what it’s doing for society,” she said.
“We need to do a self-examination, when or if the dust from this ever settles, [on] how much of the past year was viewed as a business opportunity and did that get in the way of informing the public adequately,” Ms. McKenna said.
Digital platforms and journalists also need to reflect on how narratives build on one another, particularly online, said Ms. Bell. If you search for side effects of the Johnson & Johnson vaccine, for example, you will see a list of dozens of headlines that might give you the impression this is a major problem without the context that these effects are exceedingly rare, she notes.
There was also a personnel problem. Shrinking newsrooms over the last decade meant many outlets didn’t have dedicated science and health reporting, or very few staffers, if any. During the pandemic, suddenly general assignment and politics reporters had to be science and health reporters, too.
“You have a hard enough time with these issues if you’re a fairly seasoned science journalist,” said Gary Schwitzer, a former head of the health care news unit for CNN, journalism professor at the University of Minnesota, and founder of the watchdog site HealthNewsReview.org.
And outlets that had the staffing didn’t always put science reporters to full use, Ms. McKenna said. In March and April of 2020, major media outlets should have sent science reporters, not politics reporters, to President Donald Trump’s White House press briefings, which often included incorrect statements about COVID-19 science.
“I just don’t feel that the big outlets understood that that expertise would have made a difference,” she said.
New challenges, old problems
Some of the science journalism done during the pandemic has been some of the best ever seen in this country, said Mr. Schwitzer. But between the peaks of excellence, there is “the daily drumbeat coverage of dreck,” he added.
Many of the issues with this dreck coverage aren’t new or unique to the pandemic. For example, over the last year there have been far too many news stories based solely on weak information sources, like a drug company press release or a not-yet-peer-reviewed preprint article that hasn’t been put into proper context, said Mr. Schwitzer.
A quality science story should always include an independent perspective, he said, but many COVID-19 stories missed that perspective. This isn’t a new issue for science coverage – at Health News Review, Mr. Schwitzer and his colleagues saw stories without appropriate independent sources every day for 15 years.
It’s also challenging to write about uncertainty without over- or underselling what scientists know about a particular phenomenon. “We know that the media in general tends to portray science as more certain than it is,” said Dominique Brossard, PhD, professor and department chair at the University of Wisconsin–Madison and an expert on the intersection between science, media, and policy. This can lead to confusion when the science, and the advice based on that science, changes.
“The public has a really difficult time understanding what uncertainty means within science,” said Todd P. Newman, PhD, assistant professor at the University of Wisconsin–Madison who studies strategic communication within the context of science, technology, and the environment.
“I think the media generally has been good on the subject,” said Paul Offit, MD, director of the Vaccine Education Center, attending physician in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, and a prominent expert voice throughout the pandemic. “I think where they’ve been imperfect is they tend to be a little more dramatic in terms of how we’re doing.”
Dr. Offit isn’t the only expert to point to the drama of COVID-19 coverage. A study published in March 2021 by the National Bureau of Economic Research found 87% of stories by major U.S. media outlets leaned negative in the tone of their COVID-19 reporting, compared with 50% of stories from non-U.S. major outlets and 64% of articles in scientific journals. The negative emphasis persists even around positive developments, like vaccine trials and school re-openings.
John Whyte, MD, chief medical officer for WebMD, said he is very proud of the way WebMD and Medscape ramped up production of video series and other content to give health care providers the most up-to-date guidance on a rapidly evolving medical situation.
“But I think as [we] started to make progress – especially in the last 6 months – the coverage was never balanced enough; any positive news was immediately proceeded by negative,” he said.
“You want to be honest, but you also don’t want to be alarmist – and that’s where I think the challenge is at times in the media,” said Dr. Whyte. “We didn’t put enough optimism in at times, especially in recent months.”
“Any good coverage on vaccines immediately [was] covered by ‘[we] might need boosters in the fall.’ Why can’t [we] have an opportunity to breathe for a little while and see the good news?” he asked.
Variants or scariants?
Negativity and fear shaped much of the coverage around variants and vaccines earlier this year. In February 2021, Zeynep Tufekci, PhD, a sociologist at the University of North Carolina at Chapel Hill school of information and library science, wrote in The Atlantic about how much reporting has not reflected “the truly amazing reality of these vaccines,” and has instead highlighted “a chorus of relentless pessimism.”
This felt especially true earlier in 2021, when lots of coverage repeatedly emphasized what vaccinated people still could not do.
Eric Topol, MD, editor-in-chief of Medscape and executive vice president of Scripps Research in La Jolla, California, said New York Times editors told him earlier in the pandemic that he couldn’t use the word “scariant” in an opinion piece about the media’s overly fearful and sometimes inaccurate reporting around COVID-19 variants because they worried it would seem like the Times was coming after other media outlets.
“A variant is innocent until proven guilty,” said Dr. Topol. Had journalists approached the subject from that point of view, he said we would have seen “much more faithful reporting.”
Dr. Brossard and Dr. Newman worry that focusing on uncommon negative behavior, like people who break social distancing and mask rules by gathering at the beach or the bar, makes those actions seem more common than they actually are.
The evidence suggests that “if you show these kinds of things to people, you encourage them to do the same behavior,” said Dr. Brossard.
There have been other mistakes along the way, too. Early in the pandemic, many outlets pointed viewers to official government sources of information, some of which, like the White House press briefings in March and April of 2020, ended up being some of the most virulent spreaders of misinformation, said Ms. Bell.
Before that, a handful of journalists like Roxanne Khamsi were the few pushing back against the dominant media narrative in early 2020 that the novel coronavirus was less concerning than the seasonal flu.
“Science journalists have always been writing about studies that sometimes contradict each other, and what’s happened is that has only been condensed in time,” said Ms. Khamsi, a health care reporter for outlets like WIRED magazine and The New York Times and a former chief news editor for Nature Medicine.
Politics and misinformation
It’s impossible to talk about media coverage of COVID-19 without touching on politics and misinformation.
Coverage of the pandemic was politicized and polarized from the very beginning, said Sedona Chinn, PhD, an assistant professor at the University of Wisconsin–Madison who researches the prevalence and effects of scientific disagreements in media.
By looking at network news transcripts and articles from national outlets like the Washington Post and The New York Times, Dr. Chinn and her colleagues were able to determine politicization of coverage by counting the mentions of politicians versus scientists in COVID-19 coverage and polarization by looking at how different or similar the language was surrounding mentions of Republicans and Democrats.
If the two parties were working together or on the same page, they reasoned, the language would be similar.
From mid-March through May 2020, Dr. Chinn and fellow researchers found politicians were featured more often than scientists in newspaper coverage and as frequently as scientists in network news coverage. They also found polarized language around Republicans and Democrats, particularly in stories describing duels between the (at the time) Republican national government and Democratic state and local leaders.
It’s possible that polarization in news coverage helped contribute to polarized attitudes around the virus, the authors write in the study, which was published in August 2020 in the journal Science Communication.
The politicization and polarization of the issue is mirrored in our fractured media environment, where people tend to read, listen, and watch outlets that align with their political leanings. If that trusted outlet features misinformation, the people who follow it are more likely to accept that false information as truth, said Matt Motta, PhD, a political scientist at Oklahoma State University whose research includes public opinion and science communication.
This is true across the political spectrum, he said. When it comes to COVID-19, however, right-wing media outlets like Fox News and Breitbart are more likely to promote conspiratorial tropes and misinformation about the pandemic, according to Dr. Motta and his collaborator Dominik Stecula, PhD, a political scientist at Colorado State University who studies the news media environment and its effects on society.
Across the media ecosystem, reporting on the “infodemic” accompanying the pandemic – the rapid spread of misinformation and disinformation about the virus – has been a major challenge. Outlets may not be creating the misinformation, but they are the ones choosing to give it a platform, said Dr. Motta.
By repeating a false idea, even with the goal of debunking it, you can unintentionally cause the information to stick in people’s minds, said Dr. Brossard.
“Just because something is controversial doesn’t mean it’s worth covering,” said Dr. Motta. Using vaccines as an example, he said many reporters and scientists alike assume that if people have all the facts, they’ll land on the side of science.
“That is just fundamentally not how people think about the decision to get vaccinated,” he said. Instead, the choice is wrapped up with cultural factors, religious beliefs, political identity, and more.
The factors and challenges that shaped the media’s coverage of the pandemic aren’t going anywhere. Improving science and medical coverage in the future is a collective project for journalists, scientists, and everyone in between, said Dr. Newman.
“I call on scientists, too, to think really deeply about how they’re communicating – and especially how they’re communicating what they know and don’t know,” he said.
A version of this article first appeared on Medscape.com.
For well over a year, the COVID-19 pandemic has been the biggest story in the world, costing millions of lives, impacting a presidential election, and quaking economies around the world.
But as vaccination rates increase and restrictions relax across the United States, relief is beginning to mix with reflection. Part of that contemplation means grappling with how the media depicted the crisis – in ways that were helpful, harmful, and somewhere in between.
“This story was so overwhelming, and the amount of journalism done about it was also overwhelming, and it’s going to be a while before we can do any kind of comprehensive overview of how journalism really performed,” said Maryn McKenna, an independent journalist and journalism professor at Emory University, Atlanta, who specializes in public and global health.
Some ‘heroically good’ reporting
The pandemic hit at a time when journalism was under a lot of pressure from external forces – undermined by politics, swimming through a sea of misinformation, and pressed by financial pressure to produce more stories more quickly, said Emily Bell, founding director of the Tow Center for Digital Journalism at Columbia University, New York.
The pandemic drove enormous audiences to news outlets, as people searched for reliable information, and increased the appreciation many people felt for the work of journalists, she said.
“I think there’s been some heroically good reporting and some really empathetic reporting as well,” said Ms. Bell. She cites The New York Times stories honoring the nearly 100,000 people lost to COVID-19 in May 2020 and The Atlantic’s COVID Tracking Project as exceptionally good examples.
Journalism is part of a complex, and evolving, information ecosystem characterized by “traditional” television, radio, and newspapers but also social media, search engine results, niche online news outlets, and clickbait sites.
On the one hand, social media provided a way for physicians, nurses, and scientists to speak directly to the world about their experiences and research. On the other hand, it’s challenging to elevate the really good work of traditional media over all of the bad or unhelpful signals, said Ms. Bell.
But, at the end of the day, much of journalism is a business. There are incentives in the market for tabloids to do sensational coverage and for outlets to push misleading, clickbait headlines, Ms. Bell said.
“Sometimes we’ll criticize journalists for ‘getting it wrong,’ but they might be getting it right in their business model but getting it wrong in terms of what it’s doing for society,” she said.
“We need to do a self-examination, when or if the dust from this ever settles, [on] how much of the past year was viewed as a business opportunity and did that get in the way of informing the public adequately,” Ms. McKenna said.
Digital platforms and journalists also need to reflect on how narratives build on one another, particularly online, said Ms. Bell. If you search for side effects of the Johnson & Johnson vaccine, for example, you will see a list of dozens of headlines that might give you the impression this is a major problem without the context that these effects are exceedingly rare, she notes.
There was also a personnel problem. Shrinking newsrooms over the last decade meant many outlets didn’t have dedicated science and health reporting, or very few staffers, if any. During the pandemic, suddenly general assignment and politics reporters had to be science and health reporters, too.
“You have a hard enough time with these issues if you’re a fairly seasoned science journalist,” said Gary Schwitzer, a former head of the health care news unit for CNN, journalism professor at the University of Minnesota, and founder of the watchdog site HealthNewsReview.org.
And outlets that had the staffing didn’t always put science reporters to full use, Ms. McKenna said. In March and April of 2020, major media outlets should have sent science reporters, not politics reporters, to President Donald Trump’s White House press briefings, which often included incorrect statements about COVID-19 science.
“I just don’t feel that the big outlets understood that that expertise would have made a difference,” she said.
New challenges, old problems
Some of the science journalism done during the pandemic has been some of the best ever seen in this country, said Mr. Schwitzer. But between the peaks of excellence, there is “the daily drumbeat coverage of dreck,” he added.
Many of the issues with this dreck coverage aren’t new or unique to the pandemic. For example, over the last year there have been far too many news stories based solely on weak information sources, like a drug company press release or a not-yet-peer-reviewed preprint article that hasn’t been put into proper context, said Mr. Schwitzer.
A quality science story should always include an independent perspective, he said, but many COVID-19 stories missed that perspective. This isn’t a new issue for science coverage – at Health News Review, Mr. Schwitzer and his colleagues saw stories without appropriate independent sources every day for 15 years.
It’s also challenging to write about uncertainty without over- or underselling what scientists know about a particular phenomenon. “We know that the media in general tends to portray science as more certain than it is,” said Dominique Brossard, PhD, professor and department chair at the University of Wisconsin–Madison and an expert on the intersection between science, media, and policy. This can lead to confusion when the science, and the advice based on that science, changes.
“The public has a really difficult time understanding what uncertainty means within science,” said Todd P. Newman, PhD, assistant professor at the University of Wisconsin–Madison who studies strategic communication within the context of science, technology, and the environment.
“I think the media generally has been good on the subject,” said Paul Offit, MD, director of the Vaccine Education Center, attending physician in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia, and a prominent expert voice throughout the pandemic. “I think where they’ve been imperfect is they tend to be a little more dramatic in terms of how we’re doing.”
Dr. Offit isn’t the only expert to point to the drama of COVID-19 coverage. A study published in March 2021 by the National Bureau of Economic Research found 87% of stories by major U.S. media outlets leaned negative in the tone of their COVID-19 reporting, compared with 50% of stories from non-U.S. major outlets and 64% of articles in scientific journals. The negative emphasis persists even around positive developments, like vaccine trials and school re-openings.
John Whyte, MD, chief medical officer for WebMD, said he is very proud of the way WebMD and Medscape ramped up production of video series and other content to give health care providers the most up-to-date guidance on a rapidly evolving medical situation.
“But I think as [we] started to make progress – especially in the last 6 months – the coverage was never balanced enough; any positive news was immediately proceeded by negative,” he said.
“You want to be honest, but you also don’t want to be alarmist – and that’s where I think the challenge is at times in the media,” said Dr. Whyte. “We didn’t put enough optimism in at times, especially in recent months.”
“Any good coverage on vaccines immediately [was] covered by ‘[we] might need boosters in the fall.’ Why can’t [we] have an opportunity to breathe for a little while and see the good news?” he asked.
Variants or scariants?
Negativity and fear shaped much of the coverage around variants and vaccines earlier this year. In February 2021, Zeynep Tufekci, PhD, a sociologist at the University of North Carolina at Chapel Hill school of information and library science, wrote in The Atlantic about how much reporting has not reflected “the truly amazing reality of these vaccines,” and has instead highlighted “a chorus of relentless pessimism.”
This felt especially true earlier in 2021, when lots of coverage repeatedly emphasized what vaccinated people still could not do.
Eric Topol, MD, editor-in-chief of Medscape and executive vice president of Scripps Research in La Jolla, California, said New York Times editors told him earlier in the pandemic that he couldn’t use the word “scariant” in an opinion piece about the media’s overly fearful and sometimes inaccurate reporting around COVID-19 variants because they worried it would seem like the Times was coming after other media outlets.
“A variant is innocent until proven guilty,” said Dr. Topol. Had journalists approached the subject from that point of view, he said we would have seen “much more faithful reporting.”
Dr. Brossard and Dr. Newman worry that focusing on uncommon negative behavior, like people who break social distancing and mask rules by gathering at the beach or the bar, makes those actions seem more common than they actually are.
The evidence suggests that “if you show these kinds of things to people, you encourage them to do the same behavior,” said Dr. Brossard.
There have been other mistakes along the way, too. Early in the pandemic, many outlets pointed viewers to official government sources of information, some of which, like the White House press briefings in March and April of 2020, ended up being some of the most virulent spreaders of misinformation, said Ms. Bell.
Before that, a handful of journalists like Roxanne Khamsi were the few pushing back against the dominant media narrative in early 2020 that the novel coronavirus was less concerning than the seasonal flu.
“Science journalists have always been writing about studies that sometimes contradict each other, and what’s happened is that has only been condensed in time,” said Ms. Khamsi, a health care reporter for outlets like WIRED magazine and The New York Times and a former chief news editor for Nature Medicine.
Politics and misinformation
It’s impossible to talk about media coverage of COVID-19 without touching on politics and misinformation.
Coverage of the pandemic was politicized and polarized from the very beginning, said Sedona Chinn, PhD, an assistant professor at the University of Wisconsin–Madison who researches the prevalence and effects of scientific disagreements in media.
By looking at network news transcripts and articles from national outlets like the Washington Post and The New York Times, Dr. Chinn and her colleagues were able to determine politicization of coverage by counting the mentions of politicians versus scientists in COVID-19 coverage and polarization by looking at how different or similar the language was surrounding mentions of Republicans and Democrats.
If the two parties were working together or on the same page, they reasoned, the language would be similar.
From mid-March through May 2020, Dr. Chinn and fellow researchers found politicians were featured more often than scientists in newspaper coverage and as frequently as scientists in network news coverage. They also found polarized language around Republicans and Democrats, particularly in stories describing duels between the (at the time) Republican national government and Democratic state and local leaders.
It’s possible that polarization in news coverage helped contribute to polarized attitudes around the virus, the authors write in the study, which was published in August 2020 in the journal Science Communication.
The politicization and polarization of the issue is mirrored in our fractured media environment, where people tend to read, listen, and watch outlets that align with their political leanings. If that trusted outlet features misinformation, the people who follow it are more likely to accept that false information as truth, said Matt Motta, PhD, a political scientist at Oklahoma State University whose research includes public opinion and science communication.
This is true across the political spectrum, he said. When it comes to COVID-19, however, right-wing media outlets like Fox News and Breitbart are more likely to promote conspiratorial tropes and misinformation about the pandemic, according to Dr. Motta and his collaborator Dominik Stecula, PhD, a political scientist at Colorado State University who studies the news media environment and its effects on society.
Across the media ecosystem, reporting on the “infodemic” accompanying the pandemic – the rapid spread of misinformation and disinformation about the virus – has been a major challenge. Outlets may not be creating the misinformation, but they are the ones choosing to give it a platform, said Dr. Motta.
By repeating a false idea, even with the goal of debunking it, you can unintentionally cause the information to stick in people’s minds, said Dr. Brossard.
“Just because something is controversial doesn’t mean it’s worth covering,” said Dr. Motta. Using vaccines as an example, he said many reporters and scientists alike assume that if people have all the facts, they’ll land on the side of science.
“That is just fundamentally not how people think about the decision to get vaccinated,” he said. Instead, the choice is wrapped up with cultural factors, religious beliefs, political identity, and more.
The factors and challenges that shaped the media’s coverage of the pandemic aren’t going anywhere. Improving science and medical coverage in the future is a collective project for journalists, scientists, and everyone in between, said Dr. Newman.
“I call on scientists, too, to think really deeply about how they’re communicating – and especially how they’re communicating what they know and don’t know,” he said.
A version of this article first appeared on Medscape.com.
Children and COVID: Vaccination trends beginning to diverge
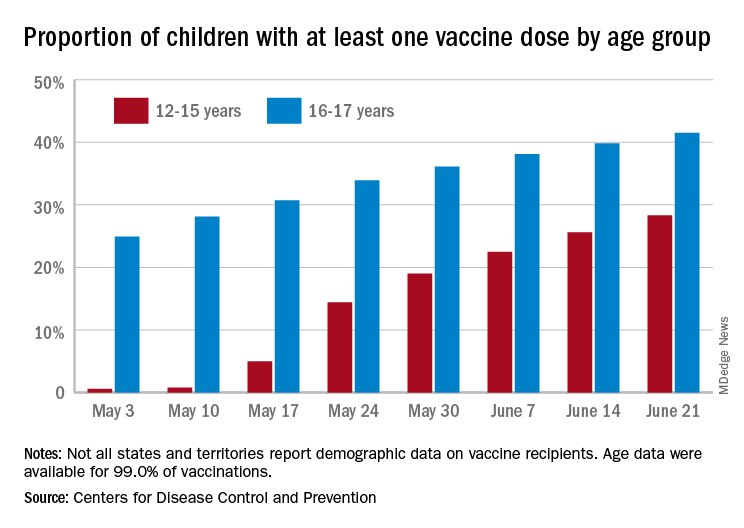
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
New data on COVID-19’s cognitive fallout
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
FDA approves OTC antihistamine nasal spray
, making it the first nasal antihistamine available over the counter in the United States.

The 0.15% strength of azelastine hydrochloride nasal spray is now approved for nonprescription treatment of seasonal and perennial allergic rhinitis in adults and children 6 years of age or older, the agency said. The 0.1% strength remains a prescription product that is indicated in younger children.
The “approval provides individuals an option for a safe and effective nasal antihistamine without requiring the assistance of a health care provider,” Theresa M. Michele, MD, director of the office of nonprescription drugs in the FDA’s Center for Drug Evaluation and Research, said in a prepared statement.
The FDA granted the nonprescription approval to Bayer Healthcare LLC, which said in a press release that the nasal spray would be available in national mass retail locations starting in the first quarter of 2022.
Oral antihistamines such as cetirizine (Zyrtec), loratadine (Claritin), and fexofenadine (Allegra) have been on store shelves for years. Azelastine 0.15% will be the first and only over-the-counter antihistamine for indoor and outdoor allergy relief in a nasal formulation, Bayer said.
An over-the-counter nasal antihistamine could be a better option for some allergy sufferers when compared with what is already over the counter, said Tracy Prematta, MD, a private practice allergist in Havertown, Pa.
“In general, I like the nasal antihistamines,” Dr. Prematta said in an interview. “They work quickly, whereas the nasal steroids don’t, and I think a lot of people who go to the drugstore looking for allergy relief are actually looking for something quick-acting.”
However, the cost of the over-the-counter azelastine may play a big role in whether patients go with the prescription or nonprescription option, according to Dr. Prematta.
Bayer has not yet set the price for nonprescription azelastine, a company spokesperson told this news organization.
The change in azelastine approval status happened through a regulatory process called an Rx-to-OTC switch. According to the FDA, products switched to nonprescription status need to have data demonstrating that they are safe and effective as self-medication when used as directed.
The product manufacturer has to show that consumers know how to use the drug safely and effectively without a health care professional supervising them, the FDA said.
The FDA considers the change in status for azelastine a partial Rx-to-OTC switch, since the 0.15% strength is now over the counter and the 0.1% strength remains a prescription product.
The 0.1% strength is indicated for perennial allergies in children 6 months to 6 years old, and seasonal allergies for children 2-6 years old, according to the FDA.
Drowsiness is a side effect of azelastine, the FDA said. According to prescribing information, consumers using the nasal spray need to be careful when driving or operating machinery, and should avoid alcohol.
Using the product with alcohol, sedatives, or tranquilizers may increase drowsiness, the agency added.
Sedation is also common with the oral antihistamines people take to treat their allergies, said Dr. Prematta, who added that patients may also complain of dry mouth, nose, or throat.
Although some allergy sufferers dislike the taste of antihistamine nasal spray, they can try to overcome that issue by tilting the head forward, pointing the tip of the nozzle toward the outside of the nose, and sniffing gently, Dr. Prematta said.
“That really minimizes what gets in the back of your throat, so taste becomes less of a problem,” she explained.
Dr. Prematta has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, making it the first nasal antihistamine available over the counter in the United States.
The 0.15% strength of azelastine hydrochloride nasal spray is now approved for nonprescription treatment of seasonal and perennial allergic rhinitis in adults and children 6 years of age or older, the agency said. The 0.1% strength remains a prescription product that is indicated in younger children.
The “approval provides individuals an option for a safe and effective nasal antihistamine without requiring the assistance of a health care provider,” Theresa M. Michele, MD, director of the office of nonprescription drugs in the FDA’s Center for Drug Evaluation and Research, said in a prepared statement.
The FDA granted the nonprescription approval to Bayer Healthcare LLC, which said in a press release that the nasal spray would be available in national mass retail locations starting in the first quarter of 2022.
Oral antihistamines such as cetirizine (Zyrtec), loratadine (Claritin), and fexofenadine (Allegra) have been on store shelves for years. Azelastine 0.15% will be the first and only over-the-counter antihistamine for indoor and outdoor allergy relief in a nasal formulation, Bayer said.
An over-the-counter nasal antihistamine could be a better option for some allergy sufferers when compared with what is already over the counter, said Tracy Prematta, MD, a private practice allergist in Havertown, Pa.
“In general, I like the nasal antihistamines,” Dr. Prematta said in an interview. “They work quickly, whereas the nasal steroids don’t, and I think a lot of people who go to the drugstore looking for allergy relief are actually looking for something quick-acting.”
However, the cost of the over-the-counter azelastine may play a big role in whether patients go with the prescription or nonprescription option, according to Dr. Prematta.
Bayer has not yet set the price for nonprescription azelastine, a company spokesperson told this news organization.
The change in azelastine approval status happened through a regulatory process called an Rx-to-OTC switch. According to the FDA, products switched to nonprescription status need to have data demonstrating that they are safe and effective as self-medication when used as directed.
The product manufacturer has to show that consumers know how to use the drug safely and effectively without a health care professional supervising them, the FDA said.
The FDA considers the change in status for azelastine a partial Rx-to-OTC switch, since the 0.15% strength is now over the counter and the 0.1% strength remains a prescription product.
The 0.1% strength is indicated for perennial allergies in children 6 months to 6 years old, and seasonal allergies for children 2-6 years old, according to the FDA.
Drowsiness is a side effect of azelastine, the FDA said. According to prescribing information, consumers using the nasal spray need to be careful when driving or operating machinery, and should avoid alcohol.
Using the product with alcohol, sedatives, or tranquilizers may increase drowsiness, the agency added.
Sedation is also common with the oral antihistamines people take to treat their allergies, said Dr. Prematta, who added that patients may also complain of dry mouth, nose, or throat.
Although some allergy sufferers dislike the taste of antihistamine nasal spray, they can try to overcome that issue by tilting the head forward, pointing the tip of the nozzle toward the outside of the nose, and sniffing gently, Dr. Prematta said.
“That really minimizes what gets in the back of your throat, so taste becomes less of a problem,” she explained.
Dr. Prematta has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, making it the first nasal antihistamine available over the counter in the United States.
The 0.15% strength of azelastine hydrochloride nasal spray is now approved for nonprescription treatment of seasonal and perennial allergic rhinitis in adults and children 6 years of age or older, the agency said. The 0.1% strength remains a prescription product that is indicated in younger children.
The “approval provides individuals an option for a safe and effective nasal antihistamine without requiring the assistance of a health care provider,” Theresa M. Michele, MD, director of the office of nonprescription drugs in the FDA’s Center for Drug Evaluation and Research, said in a prepared statement.
The FDA granted the nonprescription approval to Bayer Healthcare LLC, which said in a press release that the nasal spray would be available in national mass retail locations starting in the first quarter of 2022.
Oral antihistamines such as cetirizine (Zyrtec), loratadine (Claritin), and fexofenadine (Allegra) have been on store shelves for years. Azelastine 0.15% will be the first and only over-the-counter antihistamine for indoor and outdoor allergy relief in a nasal formulation, Bayer said.
An over-the-counter nasal antihistamine could be a better option for some allergy sufferers when compared with what is already over the counter, said Tracy Prematta, MD, a private practice allergist in Havertown, Pa.
“In general, I like the nasal antihistamines,” Dr. Prematta said in an interview. “They work quickly, whereas the nasal steroids don’t, and I think a lot of people who go to the drugstore looking for allergy relief are actually looking for something quick-acting.”
However, the cost of the over-the-counter azelastine may play a big role in whether patients go with the prescription or nonprescription option, according to Dr. Prematta.
Bayer has not yet set the price for nonprescription azelastine, a company spokesperson told this news organization.
The change in azelastine approval status happened through a regulatory process called an Rx-to-OTC switch. According to the FDA, products switched to nonprescription status need to have data demonstrating that they are safe and effective as self-medication when used as directed.
The product manufacturer has to show that consumers know how to use the drug safely and effectively without a health care professional supervising them, the FDA said.
The FDA considers the change in status for azelastine a partial Rx-to-OTC switch, since the 0.15% strength is now over the counter and the 0.1% strength remains a prescription product.
The 0.1% strength is indicated for perennial allergies in children 6 months to 6 years old, and seasonal allergies for children 2-6 years old, according to the FDA.
Drowsiness is a side effect of azelastine, the FDA said. According to prescribing information, consumers using the nasal spray need to be careful when driving or operating machinery, and should avoid alcohol.
Using the product with alcohol, sedatives, or tranquilizers may increase drowsiness, the agency added.
Sedation is also common with the oral antihistamines people take to treat their allergies, said Dr. Prematta, who added that patients may also complain of dry mouth, nose, or throat.
Although some allergy sufferers dislike the taste of antihistamine nasal spray, they can try to overcome that issue by tilting the head forward, pointing the tip of the nozzle toward the outside of the nose, and sniffing gently, Dr. Prematta said.
“That really minimizes what gets in the back of your throat, so taste becomes less of a problem,” she explained.
Dr. Prematta has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
High rates of work-related trauma, PTSD in intern physicians
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.

Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”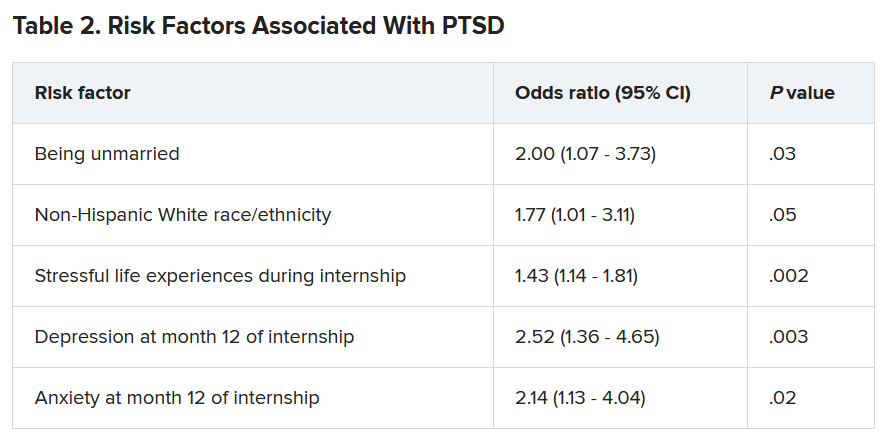
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Americans’ sun protection practices fall short of intentions
commissioned by the American Academy of Dermatology.
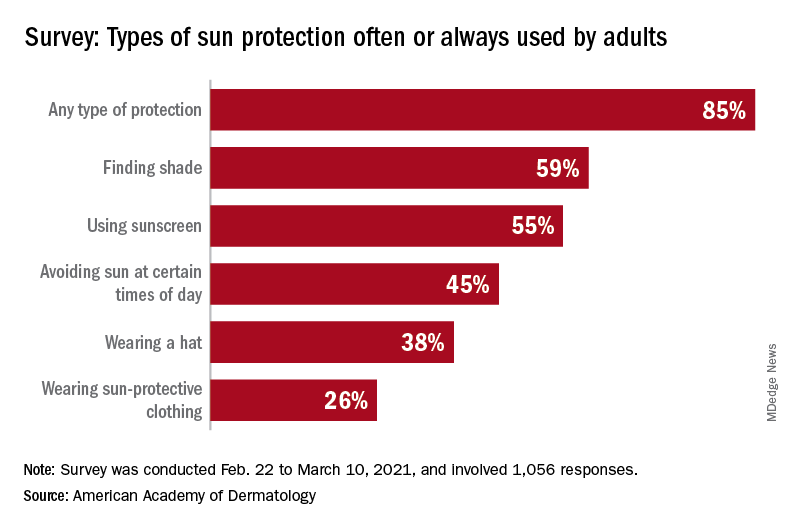
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
commissioned by the American Academy of Dermatology.
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
commissioned by the American Academy of Dermatology.
With the pandemic seemingly behind it, the United States enters the summer months facing the paradox of sun protection. Four out of five adults know that sunscreen should be reapplied every 2 hours when they’re outdoors, but only one in three make the actual effort, and 77% are likely to use sunscreen at the beach or a pool, compared with 41% when they’re gardening or working outside on their homes, the AAD reported.
“These findings are surprising and seem to suggest that many people do not take skin cancer seriously or perhaps believe skin cancer won’t happen to them,” Robert T. Brodell, MD, professor of dermatology at the University of Mississippi Medical Center, Jackson, said in a written statement from the AAD, adding that “unprotected exposure to ultraviolet rays is the most preventable risk factor for skin cancer, including melanoma.”
A quarter of all survey respondents reported getting sunburned in 2020, with the youngest adults most likely to feel the wrath of the sun. Sunburn was reported by 43% of those aged 18-23 years, 37% of those aged 24-39, 25% of the 40- to 55-year-olds, 12% of the 56- to 74-year-olds, and 7% of those aged 75 and older. More than a quarter of those who got sunburned said that it was bad enough to make their clothes feel uncomfortable, the academy said.
“Americans see the damaging effects of the sun on their skin as they get older, and two out of three look back and wish they had been more careful. But when it comes to cancer, specifically, most feel unconcerned in spite of their own risk,” according to a statement from Versta Research, which conducted the poll on behalf of the AAD. The survey was conducted from Feb. 22 to March 10, 2021, and involved 1,056 respondents, with a ±3% margin of error.
The lack of concern for skin cancer looks like this: More than two-thirds of the respondents (69%) have at least one possible risk factor – lighter skin tone, blue or green eyes, more than 50 moles, family history – but only 36% expressed concern about developing it. “Indeed, half of survey respondents (49%) say they are more worried about avoiding sunburn than they are about preventing skin cancer, and a third (32%) are more worried about avoiding premature wrinkles than they are about preventing cancer,” the AAD said.
The AAD is considering the creation of a social media quiz or interactive tool, and if the results of this survey were recast as a potential “Knowledge and Awareness Quiz” and graded with a traditional scheme (A = 90%-100%, B = 80%-89%, etc.), then 34% of the respondents would have failed, 15% would have gotten a D, and only 5% would have earned an A, the academy noted.
Prophylactic anticoagulation tied to lower death rate in COVID
Prophylactic anticoagulation to prevent venous thromboembolism (VTE) was associated with reduced 60-day mortality in patients with COVID-19 who were ill enough to require hospitalization, a new report shows.
In a cohort study of more than 1,300 hospitalized patients with COVID-19 infection across 30 hospitals in Michigan, both prophylactic- and therapeutic-dose anticoagulation were associated with reduced in-hospital mortality; however, at 60 days, only prophylactic-dose anticoagulation remained associated with lower mortality.
And adherence was key; nonadherence, or missing 2 days or more of anticoagulation, was linked to more deaths at 60 days.
The findings, which were published online June 11 in JAMA Network Open, are final proof that a prophylactic anticoagulation strategy for the hospitalized COVID population is, indeed, the right one, Valerie M. Vaughn, MD, director of hospital medicine research at the University of Utah, Salt Lake City, said in an interview.
“We’ve probably always known that patients with COVID need prophylaxis for VTE, but we found that early on, unfortunately, that wasn’t being done,” Dr. Vaughn said.
“Now, we see that prophylactic rates have increased. We always knew to use anticoagulation prophylactically in patients who were hospitalized with infection because of their risk for VTE, so this study just drives home that proper adherence to an anticoagulation protocol improves mortality,” she said.
Dr. Vaughn was on the front lines when COVID-19 came to Michigan, where the research was conducted.
“We probably should have been anticoagulating from the get-go, but you have to remember that in the early days of COVID, the hospitals in Michigan were being overwhelmed. They didn’t have PPE. They were taking care of patients outside of their typical hospital beds or setting up field hospitals,” she said. “It was not quite as bad as New York, but at the University of Michigan, we set up four or five ICUs outside of our normal care.”
They also converted the top floor of their pediatric hospital into an ICU to take care of patients with COVID during the first surge, she added. “We didn’t know much about this disease, but faced with this influx of patients, many of whom were dying with blood clots, we had to do something.”
Some hospitals began prophylactically anticoagulating their patients, but others hesitated before adopting the strategy. “But now we feel confident that prophylactic anticoagulation, done according to the right protocol, with no interruptions in the treatment, is beneficial,” Dr. Vaughn said.
The best medication choice is enoxaparin (Lovenox), which can be given once a day, as opposed to heparin, which needs to be given via injection three times a day, she said.
“Prophylactic dose anticoagulation is typically given by an injection under the skin, but a lot of times, I’ve had patients tell me they feel like a human pin cushion and have all these bruises from being stuck with needles every day, which I can totally relate to,” she said.
“It is important for us as clinicians to explain that we’re having to poke our patients because it is good for them and will help them fight COVID,” she added. “Also having the once-a-day option is going to be a lot better for adherence, and adherence to the protocol, not missing any days, is key to the better outcome.”
Dr. Vaughn and her team reviewed the charts of 1,351 patients (48% women, 49% Black, median age 64 [range 52-75]) who were hospitalized throughout Michigan during the first several months of the COVID-19 pandemic, from March to June 2020.
Only 18 patients (1.3%) had a confirmed VTE and 219 patients (16.2%) received treatment-dose anticoagulation.
The researchers noted that use of treatment-dose anticoagulation without imaging ranged from 0% to 29% across hospitals and increased significantly over time.
Of the 1,127 patients who received anticoagulation, 392 (34.8%) missed 2 days or more of prophylaxis.
In addition, there were varying rates of missed prophylaxis among the hospitals, from 11% to 61%, but these rates decreased markedly over time.
Missed doses were associated with a higher 60-day mortality (adjusted hazard ratio, 1.31; 95% confidence interval, 1.03-1.67), but not in-hospital mortality (aHR, 0.97; 95% CI, 0.91-1.03).
Compared with no anticoagulation, receiving any dose of anticoagulation was associated with lower in-hospital mortality.
However, only prophylactic-dose anticoagulation remained associated with lower mortality at 60 days. The adjusted hazard ratio for prophylactic-dose anticoagulation was 0.71 (95% CI, 0.51-0.90), compared with 0.92 (95% CI, 0.63-1.35) for treatment-dose anticoagulation.
Study boosts confidence
Despite its limitations, the study should make clinicians more confident that the use of prophylactic anticoagulation is warranted for hospitalized patients with COVID-19, write Andrew B. Dicks, MD, and Ido Weinberg, MD, from Massachusetts General Hospital, Boston, in an invited commentary.
“Practically, we still lack the granular data we need to help guide us in patient-by-patient decision-making – such as anticoagulation agent choice, dosage, and duration of therapy – especially as dictated by acuity of patient illness,” Dr. Dicks and Dr. Weinberg note.
“While we still await the data from randomized controlled trials to guide the optimal anticoagulation dose and duration, this study adds significant merit to the previously published recommendations from several different medical organizations regarding the use of prophylactic anticoagulation in hospitalized patients with COVID-19,” Dr. Dicks told this news organization.
The study was supported by Blue Cross and Blue Shield of Michigan and Blue Care Network as part of their Value Partnerships program. Dr. Vaughn has reported receiving speaking fees from Thermo Fisher Scientific. Dr. Dicks and Dr. Weinberg have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prophylactic anticoagulation to prevent venous thromboembolism (VTE) was associated with reduced 60-day mortality in patients with COVID-19 who were ill enough to require hospitalization, a new report shows.
In a cohort study of more than 1,300 hospitalized patients with COVID-19 infection across 30 hospitals in Michigan, both prophylactic- and therapeutic-dose anticoagulation were associated with reduced in-hospital mortality; however, at 60 days, only prophylactic-dose anticoagulation remained associated with lower mortality.
And adherence was key; nonadherence, or missing 2 days or more of anticoagulation, was linked to more deaths at 60 days.
The findings, which were published online June 11 in JAMA Network Open, are final proof that a prophylactic anticoagulation strategy for the hospitalized COVID population is, indeed, the right one, Valerie M. Vaughn, MD, director of hospital medicine research at the University of Utah, Salt Lake City, said in an interview.
“We’ve probably always known that patients with COVID need prophylaxis for VTE, but we found that early on, unfortunately, that wasn’t being done,” Dr. Vaughn said.
“Now, we see that prophylactic rates have increased. We always knew to use anticoagulation prophylactically in patients who were hospitalized with infection because of their risk for VTE, so this study just drives home that proper adherence to an anticoagulation protocol improves mortality,” she said.
Dr. Vaughn was on the front lines when COVID-19 came to Michigan, where the research was conducted.
“We probably should have been anticoagulating from the get-go, but you have to remember that in the early days of COVID, the hospitals in Michigan were being overwhelmed. They didn’t have PPE. They were taking care of patients outside of their typical hospital beds or setting up field hospitals,” she said. “It was not quite as bad as New York, but at the University of Michigan, we set up four or five ICUs outside of our normal care.”
They also converted the top floor of their pediatric hospital into an ICU to take care of patients with COVID during the first surge, she added. “We didn’t know much about this disease, but faced with this influx of patients, many of whom were dying with blood clots, we had to do something.”
Some hospitals began prophylactically anticoagulating their patients, but others hesitated before adopting the strategy. “But now we feel confident that prophylactic anticoagulation, done according to the right protocol, with no interruptions in the treatment, is beneficial,” Dr. Vaughn said.
The best medication choice is enoxaparin (Lovenox), which can be given once a day, as opposed to heparin, which needs to be given via injection three times a day, she said.
“Prophylactic dose anticoagulation is typically given by an injection under the skin, but a lot of times, I’ve had patients tell me they feel like a human pin cushion and have all these bruises from being stuck with needles every day, which I can totally relate to,” she said.
“It is important for us as clinicians to explain that we’re having to poke our patients because it is good for them and will help them fight COVID,” she added. “Also having the once-a-day option is going to be a lot better for adherence, and adherence to the protocol, not missing any days, is key to the better outcome.”
Dr. Vaughn and her team reviewed the charts of 1,351 patients (48% women, 49% Black, median age 64 [range 52-75]) who were hospitalized throughout Michigan during the first several months of the COVID-19 pandemic, from March to June 2020.
Only 18 patients (1.3%) had a confirmed VTE and 219 patients (16.2%) received treatment-dose anticoagulation.
The researchers noted that use of treatment-dose anticoagulation without imaging ranged from 0% to 29% across hospitals and increased significantly over time.
Of the 1,127 patients who received anticoagulation, 392 (34.8%) missed 2 days or more of prophylaxis.
In addition, there were varying rates of missed prophylaxis among the hospitals, from 11% to 61%, but these rates decreased markedly over time.
Missed doses were associated with a higher 60-day mortality (adjusted hazard ratio, 1.31; 95% confidence interval, 1.03-1.67), but not in-hospital mortality (aHR, 0.97; 95% CI, 0.91-1.03).
Compared with no anticoagulation, receiving any dose of anticoagulation was associated with lower in-hospital mortality.
However, only prophylactic-dose anticoagulation remained associated with lower mortality at 60 days. The adjusted hazard ratio for prophylactic-dose anticoagulation was 0.71 (95% CI, 0.51-0.90), compared with 0.92 (95% CI, 0.63-1.35) for treatment-dose anticoagulation.
Study boosts confidence
Despite its limitations, the study should make clinicians more confident that the use of prophylactic anticoagulation is warranted for hospitalized patients with COVID-19, write Andrew B. Dicks, MD, and Ido Weinberg, MD, from Massachusetts General Hospital, Boston, in an invited commentary.
“Practically, we still lack the granular data we need to help guide us in patient-by-patient decision-making – such as anticoagulation agent choice, dosage, and duration of therapy – especially as dictated by acuity of patient illness,” Dr. Dicks and Dr. Weinberg note.
“While we still await the data from randomized controlled trials to guide the optimal anticoagulation dose and duration, this study adds significant merit to the previously published recommendations from several different medical organizations regarding the use of prophylactic anticoagulation in hospitalized patients with COVID-19,” Dr. Dicks told this news organization.
The study was supported by Blue Cross and Blue Shield of Michigan and Blue Care Network as part of their Value Partnerships program. Dr. Vaughn has reported receiving speaking fees from Thermo Fisher Scientific. Dr. Dicks and Dr. Weinberg have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prophylactic anticoagulation to prevent venous thromboembolism (VTE) was associated with reduced 60-day mortality in patients with COVID-19 who were ill enough to require hospitalization, a new report shows.
In a cohort study of more than 1,300 hospitalized patients with COVID-19 infection across 30 hospitals in Michigan, both prophylactic- and therapeutic-dose anticoagulation were associated with reduced in-hospital mortality; however, at 60 days, only prophylactic-dose anticoagulation remained associated with lower mortality.
And adherence was key; nonadherence, or missing 2 days or more of anticoagulation, was linked to more deaths at 60 days.
The findings, which were published online June 11 in JAMA Network Open, are final proof that a prophylactic anticoagulation strategy for the hospitalized COVID population is, indeed, the right one, Valerie M. Vaughn, MD, director of hospital medicine research at the University of Utah, Salt Lake City, said in an interview.
“We’ve probably always known that patients with COVID need prophylaxis for VTE, but we found that early on, unfortunately, that wasn’t being done,” Dr. Vaughn said.
“Now, we see that prophylactic rates have increased. We always knew to use anticoagulation prophylactically in patients who were hospitalized with infection because of their risk for VTE, so this study just drives home that proper adherence to an anticoagulation protocol improves mortality,” she said.
Dr. Vaughn was on the front lines when COVID-19 came to Michigan, where the research was conducted.
“We probably should have been anticoagulating from the get-go, but you have to remember that in the early days of COVID, the hospitals in Michigan were being overwhelmed. They didn’t have PPE. They were taking care of patients outside of their typical hospital beds or setting up field hospitals,” she said. “It was not quite as bad as New York, but at the University of Michigan, we set up four or five ICUs outside of our normal care.”
They also converted the top floor of their pediatric hospital into an ICU to take care of patients with COVID during the first surge, she added. “We didn’t know much about this disease, but faced with this influx of patients, many of whom were dying with blood clots, we had to do something.”
Some hospitals began prophylactically anticoagulating their patients, but others hesitated before adopting the strategy. “But now we feel confident that prophylactic anticoagulation, done according to the right protocol, with no interruptions in the treatment, is beneficial,” Dr. Vaughn said.
The best medication choice is enoxaparin (Lovenox), which can be given once a day, as opposed to heparin, which needs to be given via injection three times a day, she said.
“Prophylactic dose anticoagulation is typically given by an injection under the skin, but a lot of times, I’ve had patients tell me they feel like a human pin cushion and have all these bruises from being stuck with needles every day, which I can totally relate to,” she said.
“It is important for us as clinicians to explain that we’re having to poke our patients because it is good for them and will help them fight COVID,” she added. “Also having the once-a-day option is going to be a lot better for adherence, and adherence to the protocol, not missing any days, is key to the better outcome.”
Dr. Vaughn and her team reviewed the charts of 1,351 patients (48% women, 49% Black, median age 64 [range 52-75]) who were hospitalized throughout Michigan during the first several months of the COVID-19 pandemic, from March to June 2020.
Only 18 patients (1.3%) had a confirmed VTE and 219 patients (16.2%) received treatment-dose anticoagulation.
The researchers noted that use of treatment-dose anticoagulation without imaging ranged from 0% to 29% across hospitals and increased significantly over time.
Of the 1,127 patients who received anticoagulation, 392 (34.8%) missed 2 days or more of prophylaxis.
In addition, there were varying rates of missed prophylaxis among the hospitals, from 11% to 61%, but these rates decreased markedly over time.
Missed doses were associated with a higher 60-day mortality (adjusted hazard ratio, 1.31; 95% confidence interval, 1.03-1.67), but not in-hospital mortality (aHR, 0.97; 95% CI, 0.91-1.03).
Compared with no anticoagulation, receiving any dose of anticoagulation was associated with lower in-hospital mortality.
However, only prophylactic-dose anticoagulation remained associated with lower mortality at 60 days. The adjusted hazard ratio for prophylactic-dose anticoagulation was 0.71 (95% CI, 0.51-0.90), compared with 0.92 (95% CI, 0.63-1.35) for treatment-dose anticoagulation.
Study boosts confidence
Despite its limitations, the study should make clinicians more confident that the use of prophylactic anticoagulation is warranted for hospitalized patients with COVID-19, write Andrew B. Dicks, MD, and Ido Weinberg, MD, from Massachusetts General Hospital, Boston, in an invited commentary.
“Practically, we still lack the granular data we need to help guide us in patient-by-patient decision-making – such as anticoagulation agent choice, dosage, and duration of therapy – especially as dictated by acuity of patient illness,” Dr. Dicks and Dr. Weinberg note.
“While we still await the data from randomized controlled trials to guide the optimal anticoagulation dose and duration, this study adds significant merit to the previously published recommendations from several different medical organizations regarding the use of prophylactic anticoagulation in hospitalized patients with COVID-19,” Dr. Dicks told this news organization.
The study was supported by Blue Cross and Blue Shield of Michigan and Blue Care Network as part of their Value Partnerships program. Dr. Vaughn has reported receiving speaking fees from Thermo Fisher Scientific. Dr. Dicks and Dr. Weinberg have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.