User login
Advocacy strategies: Leveraging patient testimonials, physician expertise, and Google
When an insurance coverage snafu threatened to take away a vital infusion drug for one of her patients, Julie Baak discovered that writing a letter wasn’t enough. Simponi Aria (golimumab) is the least expensive of all rheumatoid arthritis drugs for infusion, and at only six infusions a year offers a better experience for patients when compared with more expensive drugs like Humira (adalimumab), said Ms. Baak, practice manager at the Arthritis Center in St. Louis.

United Healthcare had drafted, then retracted, policy changes affecting and delaying access to RA drugs like Simponi Aria. Ms. Baak’s patient thrived on this drug after failing with others. UHC “kept pointing the finger at the employer, a self-funded plan,” she explained. Once correspondence efforts between the employer and payer fell through, she called a local news reporter, arranging an interview between Steven Baak, MD, the office’s medical director, and the patient, who was willing to go on the news. Through a 3-minute news segment, “we got that insurance company to allow us to get coverage for Simponi Aria on the medical side.”
Ms. Baak joined Karen Ferguson, Nilsa Cruz, and Madelaine A. Feldman, MD, at the Coalition of State Rheumatology Organizations 2020 State Society Advocacy Conference Virtual Meeting to discuss the power of advocacy in rheumatology, and impart strategies for enabling change. The Simponi Aria example underscores the importance of media and social media, Ms. Baak said. “When people do the wrong thing, you can bring light to others.”
The news spot on Dr. Baak and his patient mobilized Ms. Cruz to share it with others. “I took that interview and blasted it all over Wisconsin and to my colleagues because they needed to know what the options were for us in advocacy,” stressed Ms. Cruz, practice administrator of Milwaukee Rheumatology Center.

Rheumatologists are master problem solvers – the Sherlock Holmes’ of the medical industry, she continued. However, not many insurance companies understand the cognitive value of what they do. “There’s a lack of communication and education,” Ms. Cruz noted. Any advocacy measures calls for research on the topic, the panel stressed. It involves looking through medical and administrative insurance companies’ policies and using Google and social media, such as Twitter, to identify topics and key decision makers, a practice Ms. Cruz favors in particular.
Physicians as reliable sources
You need good documentation to support why you’re doing what you’re doing, advised Ms. Ferguson, practice administrator of Arthritis Northwest, Spokane, Wash. When an issue comes up, she always consults her doctors and her billing staff.

She recalled when biosimilars first came out, and one of them for Rituxan (rituximab) had not been indicated by the Food and Drug Administration for RA. “And yet, an insurance company was mandating that we use this nonindicated biosimilar,” said Ms. Ferguson, who learned about this from her billing staff. “I went immediately to the doctors and asked how they felt about this, and they said they were uncomfortable,” she continued. Ms. Ferguson found out that 45 states had legislation that prohibited interchangeability with non–FDA-indicated drugs. She was able to show this literature to the insurance company and get the mandate reversed. “One thing that’s so important is to be able to use your physicians’ knowledge and how they really feel and advocate based off of that,” using sound statutes to support your argument, she added.
“Ensuring that patients get the right medications that their physicians deem is important is critical for improved safety and efficacy,” Ms. Ferguson said. Yet, she acknowledged that facing off against an insurance company or a pharmacy benefit manager is often hard to do.
Many practices don’t have a Julie Baak or Karen Ferguson to fight on their behalf, Ms. Cruz noted. In this case, they should look within their state for high-profile advocates. “I guarantee you, every state has one. Practices should be able to reach out to those individuals, or respective state societies, or CSRO,” Ms. Cruz said. Best results are obtained when working through coalitions.
Patient testimony can make an impact
CSRO recently enacted a public relations campaign to shine a light on certain health plan policies that are harmful to patients. “We have been able to get the real impact of the policy on patients and their stories into the public eye,” Dr. Feldman, a rheumatologist in New Orleans and CSRO president, said in an interview. The group has spearheaded the effort to keep Stelara off of the Medicare self-administered drug list. CSRO has also built coalitions and provided testimony on several state step therapy and nonmedical switching bills. “When asked if these are pharma-backed bills, we say: ‘No, these are patient-backed bills,’ ” she added.

Patients act as powerful witnesses at hearings. “When legislation is being considered, it is important for both physicians and patients to be heard and to tell their stories,” Dr. Feldman said.
Ms. Cruz makes a point of getting involved with the payers themselves. As an example, she serves as a member on UHC’s National Steering Committee. “They know me to be very outspoken. Sometimes they listen, sometimes they don’t. Nevertheless, I consider it a compliment when they say they like that I hold them accountable. Every little thing that I can do to bring issues to the table,” filtering into their other divisions, is an accomplishment, she said.
When an insurance coverage snafu threatened to take away a vital infusion drug for one of her patients, Julie Baak discovered that writing a letter wasn’t enough. Simponi Aria (golimumab) is the least expensive of all rheumatoid arthritis drugs for infusion, and at only six infusions a year offers a better experience for patients when compared with more expensive drugs like Humira (adalimumab), said Ms. Baak, practice manager at the Arthritis Center in St. Louis.
United Healthcare had drafted, then retracted, policy changes affecting and delaying access to RA drugs like Simponi Aria. Ms. Baak’s patient thrived on this drug after failing with others. UHC “kept pointing the finger at the employer, a self-funded plan,” she explained. Once correspondence efforts between the employer and payer fell through, she called a local news reporter, arranging an interview between Steven Baak, MD, the office’s medical director, and the patient, who was willing to go on the news. Through a 3-minute news segment, “we got that insurance company to allow us to get coverage for Simponi Aria on the medical side.”
Ms. Baak joined Karen Ferguson, Nilsa Cruz, and Madelaine A. Feldman, MD, at the Coalition of State Rheumatology Organizations 2020 State Society Advocacy Conference Virtual Meeting to discuss the power of advocacy in rheumatology, and impart strategies for enabling change. The Simponi Aria example underscores the importance of media and social media, Ms. Baak said. “When people do the wrong thing, you can bring light to others.”
The news spot on Dr. Baak and his patient mobilized Ms. Cruz to share it with others. “I took that interview and blasted it all over Wisconsin and to my colleagues because they needed to know what the options were for us in advocacy,” stressed Ms. Cruz, practice administrator of Milwaukee Rheumatology Center.
Rheumatologists are master problem solvers – the Sherlock Holmes’ of the medical industry, she continued. However, not many insurance companies understand the cognitive value of what they do. “There’s a lack of communication and education,” Ms. Cruz noted. Any advocacy measures calls for research on the topic, the panel stressed. It involves looking through medical and administrative insurance companies’ policies and using Google and social media, such as Twitter, to identify topics and key decision makers, a practice Ms. Cruz favors in particular.
Physicians as reliable sources
You need good documentation to support why you’re doing what you’re doing, advised Ms. Ferguson, practice administrator of Arthritis Northwest, Spokane, Wash. When an issue comes up, she always consults her doctors and her billing staff.
She recalled when biosimilars first came out, and one of them for Rituxan (rituximab) had not been indicated by the Food and Drug Administration for RA. “And yet, an insurance company was mandating that we use this nonindicated biosimilar,” said Ms. Ferguson, who learned about this from her billing staff. “I went immediately to the doctors and asked how they felt about this, and they said they were uncomfortable,” she continued. Ms. Ferguson found out that 45 states had legislation that prohibited interchangeability with non–FDA-indicated drugs. She was able to show this literature to the insurance company and get the mandate reversed. “One thing that’s so important is to be able to use your physicians’ knowledge and how they really feel and advocate based off of that,” using sound statutes to support your argument, she added.
“Ensuring that patients get the right medications that their physicians deem is important is critical for improved safety and efficacy,” Ms. Ferguson said. Yet, she acknowledged that facing off against an insurance company or a pharmacy benefit manager is often hard to do.
Many practices don’t have a Julie Baak or Karen Ferguson to fight on their behalf, Ms. Cruz noted. In this case, they should look within their state for high-profile advocates. “I guarantee you, every state has one. Practices should be able to reach out to those individuals, or respective state societies, or CSRO,” Ms. Cruz said. Best results are obtained when working through coalitions.
Patient testimony can make an impact
CSRO recently enacted a public relations campaign to shine a light on certain health plan policies that are harmful to patients. “We have been able to get the real impact of the policy on patients and their stories into the public eye,” Dr. Feldman, a rheumatologist in New Orleans and CSRO president, said in an interview. The group has spearheaded the effort to keep Stelara off of the Medicare self-administered drug list. CSRO has also built coalitions and provided testimony on several state step therapy and nonmedical switching bills. “When asked if these are pharma-backed bills, we say: ‘No, these are patient-backed bills,’ ” she added.
Patients act as powerful witnesses at hearings. “When legislation is being considered, it is important for both physicians and patients to be heard and to tell their stories,” Dr. Feldman said.
Ms. Cruz makes a point of getting involved with the payers themselves. As an example, she serves as a member on UHC’s National Steering Committee. “They know me to be very outspoken. Sometimes they listen, sometimes they don’t. Nevertheless, I consider it a compliment when they say they like that I hold them accountable. Every little thing that I can do to bring issues to the table,” filtering into their other divisions, is an accomplishment, she said.
When an insurance coverage snafu threatened to take away a vital infusion drug for one of her patients, Julie Baak discovered that writing a letter wasn’t enough. Simponi Aria (golimumab) is the least expensive of all rheumatoid arthritis drugs for infusion, and at only six infusions a year offers a better experience for patients when compared with more expensive drugs like Humira (adalimumab), said Ms. Baak, practice manager at the Arthritis Center in St. Louis.
United Healthcare had drafted, then retracted, policy changes affecting and delaying access to RA drugs like Simponi Aria. Ms. Baak’s patient thrived on this drug after failing with others. UHC “kept pointing the finger at the employer, a self-funded plan,” she explained. Once correspondence efforts between the employer and payer fell through, she called a local news reporter, arranging an interview between Steven Baak, MD, the office’s medical director, and the patient, who was willing to go on the news. Through a 3-minute news segment, “we got that insurance company to allow us to get coverage for Simponi Aria on the medical side.”
Ms. Baak joined Karen Ferguson, Nilsa Cruz, and Madelaine A. Feldman, MD, at the Coalition of State Rheumatology Organizations 2020 State Society Advocacy Conference Virtual Meeting to discuss the power of advocacy in rheumatology, and impart strategies for enabling change. The Simponi Aria example underscores the importance of media and social media, Ms. Baak said. “When people do the wrong thing, you can bring light to others.”
The news spot on Dr. Baak and his patient mobilized Ms. Cruz to share it with others. “I took that interview and blasted it all over Wisconsin and to my colleagues because they needed to know what the options were for us in advocacy,” stressed Ms. Cruz, practice administrator of Milwaukee Rheumatology Center.
Rheumatologists are master problem solvers – the Sherlock Holmes’ of the medical industry, she continued. However, not many insurance companies understand the cognitive value of what they do. “There’s a lack of communication and education,” Ms. Cruz noted. Any advocacy measures calls for research on the topic, the panel stressed. It involves looking through medical and administrative insurance companies’ policies and using Google and social media, such as Twitter, to identify topics and key decision makers, a practice Ms. Cruz favors in particular.
Physicians as reliable sources
You need good documentation to support why you’re doing what you’re doing, advised Ms. Ferguson, practice administrator of Arthritis Northwest, Spokane, Wash. When an issue comes up, she always consults her doctors and her billing staff.
She recalled when biosimilars first came out, and one of them for Rituxan (rituximab) had not been indicated by the Food and Drug Administration for RA. “And yet, an insurance company was mandating that we use this nonindicated biosimilar,” said Ms. Ferguson, who learned about this from her billing staff. “I went immediately to the doctors and asked how they felt about this, and they said they were uncomfortable,” she continued. Ms. Ferguson found out that 45 states had legislation that prohibited interchangeability with non–FDA-indicated drugs. She was able to show this literature to the insurance company and get the mandate reversed. “One thing that’s so important is to be able to use your physicians’ knowledge and how they really feel and advocate based off of that,” using sound statutes to support your argument, she added.
“Ensuring that patients get the right medications that their physicians deem is important is critical for improved safety and efficacy,” Ms. Ferguson said. Yet, she acknowledged that facing off against an insurance company or a pharmacy benefit manager is often hard to do.
Many practices don’t have a Julie Baak or Karen Ferguson to fight on their behalf, Ms. Cruz noted. In this case, they should look within their state for high-profile advocates. “I guarantee you, every state has one. Practices should be able to reach out to those individuals, or respective state societies, or CSRO,” Ms. Cruz said. Best results are obtained when working through coalitions.
Patient testimony can make an impact
CSRO recently enacted a public relations campaign to shine a light on certain health plan policies that are harmful to patients. “We have been able to get the real impact of the policy on patients and their stories into the public eye,” Dr. Feldman, a rheumatologist in New Orleans and CSRO president, said in an interview. The group has spearheaded the effort to keep Stelara off of the Medicare self-administered drug list. CSRO has also built coalitions and provided testimony on several state step therapy and nonmedical switching bills. “When asked if these are pharma-backed bills, we say: ‘No, these are patient-backed bills,’ ” she added.
Patients act as powerful witnesses at hearings. “When legislation is being considered, it is important for both physicians and patients to be heard and to tell their stories,” Dr. Feldman said.
Ms. Cruz makes a point of getting involved with the payers themselves. As an example, she serves as a member on UHC’s National Steering Committee. “They know me to be very outspoken. Sometimes they listen, sometimes they don’t. Nevertheless, I consider it a compliment when they say they like that I hold them accountable. Every little thing that I can do to bring issues to the table,” filtering into their other divisions, is an accomplishment, she said.
FROM CSRO 2020
A young physician hopes to buck the status quo in Congress
On March 3 of this year, Bryant Cameron Webb, MD, JD, won two-thirds of the vote in Virginia’s Democratic primary race. In November, he’ll compete against Republican Bob Good to represent the state’s 5th Congressional District. If he succeeds, he will become the first Black physician ever elected to a seat in Congress.

The political and social unrest across the United States in recent months has resulted in millions of people becoming more proactive: from sports arenas to the halls of Congress, the rally cry of Black Lives Matter has echoed like never before after the killing of George Floyd and Breonna Taylor at the hands of law enforcement. Dr. Webb, a practicing internist and professor at the University of Virginia, Charlottesville, is among many physicians joining the cause. If elected, he hopes to bring a unique perspective to Washington and advocate for racial equity to help combat systemic racist policies that result in health disparities.
“For me as a professor at UVA in both public health sciences and in medicine, I have a lot to bring to this moment,” he commented, “real expertise on issues that are critical to the nation. Beyond my passion for health and wellness, I have a passion for justice.”
Dr. Webb also believes that serving in Congress is a way to help his patients. “I balance the work of direct patient care and patient advocacy in different spaces,” said the Spotsylvania County native. “Working in Congress is patient advocacy to me. It’s where I can be at my highest use to the people I take care of. It is different from direct patient care. I think this [unique] background that I have is needed in Congress.”
Dr. Webb has never held an elected office before, and he’s looking to get elected in a district that voted for President Trump in the past election. He knows challenges lie ahead.
A calling
The field of medicine called for Dr. Webb at an early age. He credits his family doctor, a Black man, for inspiring him. “With six kids in our family, we saw the doctor frequently. Dr. Yarboro was a young Black man just a few years out of residency. My mom had supreme confidence in him, and he made us feel at ease. So I wanted to be a doctor ever since I was 5 or 6 years old.”
Dr. Webb earned a bachelor’s degree from the University of Virginia in 2005. He entered medical school at Wake Forest University, Winston-Salem, N.C., the following year. Following his third year of medical training, he heeded another calling: He took time off to attend law school. He enrolled in Loyola University of Chicago School of Law and earned his juris doctorate in 2012.
The move may seem an unexpected turn. But Dr. Webb feels his law degree enhances his work. “I think that it’s because I’m so steeped in the legal resources that folks need to navigate. I think I am able to provide better care. ... It’s a complement and helpful to me professionally, whether it’s fighting with an insurance company or with a prescription drug company.”
After law school, Dr. Webb finished his medical training at Wake Forest and moved north, where he completed an internal medicine residency at New York–Presbyterian Hospital. Then came yet another twist in Dr. Webb’s unconventional career path: in 2016, he was selected by President Obama as a White House fellow. He spent the next 2 years in Washington, where he worked on Mr. Obama’s My Brother’s Keeper Task Force, an initiative that addresses opportunity gaps faced by boys and young men of color.
Adeze Enekwechi, MD, president of Impaq and associate professor at the George Washington University, Washington, worked with Dr. Webb at the White House. “This is the place where he will have the most impact. We’ve been talking and writing about health equity ever since our time [there]. Not everybody can speak that language.
Why here? Why now?
Dr. Webb sees patients 2-3 days a week on alternating weeks and knows well the concerns of people who struggle with health. Now he’s ready to have those conversations on a larger platform. “As a Black physician, it’s about bringing that healer mindset to these problems. It’s not about just going there to brow beat people or add to that divisive nature in Congress. You acknowledge that the problems exist, and then bridge,” he said, hoping that bridging party divides can be a catalyst for healing.
Carla Boutin-Foster, MD, associate dean, office of diversity education and research at the State University of New York, Brooklyn, has mentored Dr. Webb since 2013. With his credentials, confidence, and persistence, she believes, he will be a great representative of the medical community in D.C. “You need someone who respects the Constitution. When policy needs to be developed, you need a healer, someone who understands the science of vaccines. This is something Cam has been groomed for. It’s something he has been living and practicing for years.”
The killing of George Floyd and the uprising that ensued has opened the dialogue about racial inequality in America. Health care is not immune to racial bias, and the effects are palatable. One survey conducted by the Larry A. Green Center, in collaboration with the Primary Care Collaborative and 3rd Conversation, found that more than 40% of clinicians say Mr. Floyd’s demise has become a topic of concern among patients of all demographics.
When it comes to racism, Dr. Webb understands that he plays a critical role in moving America forward. “We have so many voices that are powerful and important in the highest level of legislation. We have to use those voices to root out the injustices in our society, like in the Breonna Taylor case. We have to do so because that is how you achieve the American dream,” he said.
The social determinants of health – or “ZIP-code risk” – has been proven to influence health outcomes, yet few physicians screen for them during patient visits. For Dr. Webb, discussing things like housing security and interpersonal violence are critical to providing care.
One of Dr. Webb’s biggest supporters is his wife of 11 years, Leigh Ann Webb, MD, MBA, an emergency medicine physician and assistant professor of emergency medicine at UVA. “He is an effective leader and a consensus builder,” she said of her husband, with whom she has two children. “There has always been something very unique and special about him and the way he engages the world. We need more thoughtful, intelligent people like him to help our country move forward.”
In addition to being the director of health policy and equity at UVA this fall, Dr. Webb plans to teach a course at UVA centered around the social determinants of health called Place Matters. “The focus is on understanding how education and housing and food insecurity all come together to cause illness,” he said. “Health doesn’t happen in hospitals and clinics. It happens in the community.”
A version of this article originally appeared on Medscape.com.
On March 3 of this year, Bryant Cameron Webb, MD, JD, won two-thirds of the vote in Virginia’s Democratic primary race. In November, he’ll compete against Republican Bob Good to represent the state’s 5th Congressional District. If he succeeds, he will become the first Black physician ever elected to a seat in Congress.
The political and social unrest across the United States in recent months has resulted in millions of people becoming more proactive: from sports arenas to the halls of Congress, the rally cry of Black Lives Matter has echoed like never before after the killing of George Floyd and Breonna Taylor at the hands of law enforcement. Dr. Webb, a practicing internist and professor at the University of Virginia, Charlottesville, is among many physicians joining the cause. If elected, he hopes to bring a unique perspective to Washington and advocate for racial equity to help combat systemic racist policies that result in health disparities.
“For me as a professor at UVA in both public health sciences and in medicine, I have a lot to bring to this moment,” he commented, “real expertise on issues that are critical to the nation. Beyond my passion for health and wellness, I have a passion for justice.”
Dr. Webb also believes that serving in Congress is a way to help his patients. “I balance the work of direct patient care and patient advocacy in different spaces,” said the Spotsylvania County native. “Working in Congress is patient advocacy to me. It’s where I can be at my highest use to the people I take care of. It is different from direct patient care. I think this [unique] background that I have is needed in Congress.”
Dr. Webb has never held an elected office before, and he’s looking to get elected in a district that voted for President Trump in the past election. He knows challenges lie ahead.
A calling
The field of medicine called for Dr. Webb at an early age. He credits his family doctor, a Black man, for inspiring him. “With six kids in our family, we saw the doctor frequently. Dr. Yarboro was a young Black man just a few years out of residency. My mom had supreme confidence in him, and he made us feel at ease. So I wanted to be a doctor ever since I was 5 or 6 years old.”
Dr. Webb earned a bachelor’s degree from the University of Virginia in 2005. He entered medical school at Wake Forest University, Winston-Salem, N.C., the following year. Following his third year of medical training, he heeded another calling: He took time off to attend law school. He enrolled in Loyola University of Chicago School of Law and earned his juris doctorate in 2012.
The move may seem an unexpected turn. But Dr. Webb feels his law degree enhances his work. “I think that it’s because I’m so steeped in the legal resources that folks need to navigate. I think I am able to provide better care. ... It’s a complement and helpful to me professionally, whether it’s fighting with an insurance company or with a prescription drug company.”
After law school, Dr. Webb finished his medical training at Wake Forest and moved north, where he completed an internal medicine residency at New York–Presbyterian Hospital. Then came yet another twist in Dr. Webb’s unconventional career path: in 2016, he was selected by President Obama as a White House fellow. He spent the next 2 years in Washington, where he worked on Mr. Obama’s My Brother’s Keeper Task Force, an initiative that addresses opportunity gaps faced by boys and young men of color.
Adeze Enekwechi, MD, president of Impaq and associate professor at the George Washington University, Washington, worked with Dr. Webb at the White House. “This is the place where he will have the most impact. We’ve been talking and writing about health equity ever since our time [there]. Not everybody can speak that language.
Why here? Why now?
Dr. Webb sees patients 2-3 days a week on alternating weeks and knows well the concerns of people who struggle with health. Now he’s ready to have those conversations on a larger platform. “As a Black physician, it’s about bringing that healer mindset to these problems. It’s not about just going there to brow beat people or add to that divisive nature in Congress. You acknowledge that the problems exist, and then bridge,” he said, hoping that bridging party divides can be a catalyst for healing.
Carla Boutin-Foster, MD, associate dean, office of diversity education and research at the State University of New York, Brooklyn, has mentored Dr. Webb since 2013. With his credentials, confidence, and persistence, she believes, he will be a great representative of the medical community in D.C. “You need someone who respects the Constitution. When policy needs to be developed, you need a healer, someone who understands the science of vaccines. This is something Cam has been groomed for. It’s something he has been living and practicing for years.”
The killing of George Floyd and the uprising that ensued has opened the dialogue about racial inequality in America. Health care is not immune to racial bias, and the effects are palatable. One survey conducted by the Larry A. Green Center, in collaboration with the Primary Care Collaborative and 3rd Conversation, found that more than 40% of clinicians say Mr. Floyd’s demise has become a topic of concern among patients of all demographics.
When it comes to racism, Dr. Webb understands that he plays a critical role in moving America forward. “We have so many voices that are powerful and important in the highest level of legislation. We have to use those voices to root out the injustices in our society, like in the Breonna Taylor case. We have to do so because that is how you achieve the American dream,” he said.
The social determinants of health – or “ZIP-code risk” – has been proven to influence health outcomes, yet few physicians screen for them during patient visits. For Dr. Webb, discussing things like housing security and interpersonal violence are critical to providing care.
One of Dr. Webb’s biggest supporters is his wife of 11 years, Leigh Ann Webb, MD, MBA, an emergency medicine physician and assistant professor of emergency medicine at UVA. “He is an effective leader and a consensus builder,” she said of her husband, with whom she has two children. “There has always been something very unique and special about him and the way he engages the world. We need more thoughtful, intelligent people like him to help our country move forward.”
In addition to being the director of health policy and equity at UVA this fall, Dr. Webb plans to teach a course at UVA centered around the social determinants of health called Place Matters. “The focus is on understanding how education and housing and food insecurity all come together to cause illness,” he said. “Health doesn’t happen in hospitals and clinics. It happens in the community.”
A version of this article originally appeared on Medscape.com.
On March 3 of this year, Bryant Cameron Webb, MD, JD, won two-thirds of the vote in Virginia’s Democratic primary race. In November, he’ll compete against Republican Bob Good to represent the state’s 5th Congressional District. If he succeeds, he will become the first Black physician ever elected to a seat in Congress.
The political and social unrest across the United States in recent months has resulted in millions of people becoming more proactive: from sports arenas to the halls of Congress, the rally cry of Black Lives Matter has echoed like never before after the killing of George Floyd and Breonna Taylor at the hands of law enforcement. Dr. Webb, a practicing internist and professor at the University of Virginia, Charlottesville, is among many physicians joining the cause. If elected, he hopes to bring a unique perspective to Washington and advocate for racial equity to help combat systemic racist policies that result in health disparities.
“For me as a professor at UVA in both public health sciences and in medicine, I have a lot to bring to this moment,” he commented, “real expertise on issues that are critical to the nation. Beyond my passion for health and wellness, I have a passion for justice.”
Dr. Webb also believes that serving in Congress is a way to help his patients. “I balance the work of direct patient care and patient advocacy in different spaces,” said the Spotsylvania County native. “Working in Congress is patient advocacy to me. It’s where I can be at my highest use to the people I take care of. It is different from direct patient care. I think this [unique] background that I have is needed in Congress.”
Dr. Webb has never held an elected office before, and he’s looking to get elected in a district that voted for President Trump in the past election. He knows challenges lie ahead.
A calling
The field of medicine called for Dr. Webb at an early age. He credits his family doctor, a Black man, for inspiring him. “With six kids in our family, we saw the doctor frequently. Dr. Yarboro was a young Black man just a few years out of residency. My mom had supreme confidence in him, and he made us feel at ease. So I wanted to be a doctor ever since I was 5 or 6 years old.”
Dr. Webb earned a bachelor’s degree from the University of Virginia in 2005. He entered medical school at Wake Forest University, Winston-Salem, N.C., the following year. Following his third year of medical training, he heeded another calling: He took time off to attend law school. He enrolled in Loyola University of Chicago School of Law and earned his juris doctorate in 2012.
The move may seem an unexpected turn. But Dr. Webb feels his law degree enhances his work. “I think that it’s because I’m so steeped in the legal resources that folks need to navigate. I think I am able to provide better care. ... It’s a complement and helpful to me professionally, whether it’s fighting with an insurance company or with a prescription drug company.”
After law school, Dr. Webb finished his medical training at Wake Forest and moved north, where he completed an internal medicine residency at New York–Presbyterian Hospital. Then came yet another twist in Dr. Webb’s unconventional career path: in 2016, he was selected by President Obama as a White House fellow. He spent the next 2 years in Washington, where he worked on Mr. Obama’s My Brother’s Keeper Task Force, an initiative that addresses opportunity gaps faced by boys and young men of color.
Adeze Enekwechi, MD, president of Impaq and associate professor at the George Washington University, Washington, worked with Dr. Webb at the White House. “This is the place where he will have the most impact. We’ve been talking and writing about health equity ever since our time [there]. Not everybody can speak that language.
Why here? Why now?
Dr. Webb sees patients 2-3 days a week on alternating weeks and knows well the concerns of people who struggle with health. Now he’s ready to have those conversations on a larger platform. “As a Black physician, it’s about bringing that healer mindset to these problems. It’s not about just going there to brow beat people or add to that divisive nature in Congress. You acknowledge that the problems exist, and then bridge,” he said, hoping that bridging party divides can be a catalyst for healing.
Carla Boutin-Foster, MD, associate dean, office of diversity education and research at the State University of New York, Brooklyn, has mentored Dr. Webb since 2013. With his credentials, confidence, and persistence, she believes, he will be a great representative of the medical community in D.C. “You need someone who respects the Constitution. When policy needs to be developed, you need a healer, someone who understands the science of vaccines. This is something Cam has been groomed for. It’s something he has been living and practicing for years.”
The killing of George Floyd and the uprising that ensued has opened the dialogue about racial inequality in America. Health care is not immune to racial bias, and the effects are palatable. One survey conducted by the Larry A. Green Center, in collaboration with the Primary Care Collaborative and 3rd Conversation, found that more than 40% of clinicians say Mr. Floyd’s demise has become a topic of concern among patients of all demographics.
When it comes to racism, Dr. Webb understands that he plays a critical role in moving America forward. “We have so many voices that are powerful and important in the highest level of legislation. We have to use those voices to root out the injustices in our society, like in the Breonna Taylor case. We have to do so because that is how you achieve the American dream,” he said.
The social determinants of health – or “ZIP-code risk” – has been proven to influence health outcomes, yet few physicians screen for them during patient visits. For Dr. Webb, discussing things like housing security and interpersonal violence are critical to providing care.
One of Dr. Webb’s biggest supporters is his wife of 11 years, Leigh Ann Webb, MD, MBA, an emergency medicine physician and assistant professor of emergency medicine at UVA. “He is an effective leader and a consensus builder,” she said of her husband, with whom she has two children. “There has always been something very unique and special about him and the way he engages the world. We need more thoughtful, intelligent people like him to help our country move forward.”
In addition to being the director of health policy and equity at UVA this fall, Dr. Webb plans to teach a course at UVA centered around the social determinants of health called Place Matters. “The focus is on understanding how education and housing and food insecurity all come together to cause illness,” he said. “Health doesn’t happen in hospitals and clinics. It happens in the community.”
A version of this article originally appeared on Medscape.com.
Rheumatology feels impact of COVID-19 telehealth boom
Rheumatologists are seeing the number of telehealth visits skyrocket in their practices as the COVID-19 pandemic rages on and patients seek out alternatives to in-person visits. Telemedicine makes it easier for patients to connect with physicians, but not all patients have access to a computer or device. It also limits what a physician can do. Rheumatologists often rely on physical exams to make diagnoses and treatment decisions – an obstacle if you’re looking at patients through a computer screen.

Presenters at the 2020 Coalition of State Rheumatology Organizations’ state advocacy conference discussed the benefits and challenges of this mode of care in early September. Within weeks, the U.S. health system eliminated almost half of all medical care as the pandemic ramped up and things went virtual, said Larry Van Horn, PhD, MPH, a speaker at the CSRO conference. Still, “we are in uncharted territory with respect to how telehealth is being used. ... It’s being deployed everywhere, but it’s too early to tell how it’s affecting patient outcomes,” said Dr. Van Horn, founder and director of the Center of Health Care Market Innovation at Vanderbilt University, Nashville, Tenn.
Patients seem to like using telemedicine, observed New Jersey state Sen. Herb Conaway, MD, another presenter. “I think it’s here to stay, and it’s likely to expand going forward. But physicians and others are going to want to make sure it’s used appropriately.”
Some payers feel that telemedicine should be billed differently than brick and mortar visits, Dr. Conaway said. “Physicians feel differently about that, and so we’ll see how this goes, moving forward.”
Lately, there have been discussions of liability concerns associated with telemedicine, said CSRO President Madelaine A. Feldman, MD, who practices in New Orleans. “There are some things you can miss with virtual visits. Certain new patient visits may need to be done in person.”
The landscape of telehealth in rheumatology
Telehealth has directly affected the way rheumatologists do business. In a national survey of more than 1,100 adult patients, the American College of Rheumatology found that 66% are choosing telehealth for rheumatology visits, mainly to avoid exposure to the SARS-CoV-2 virus. This contrasts with a 52% decline in the percentage of patients who are currently seeing a rheumatologist since 2019. “The pandemic has altered almost every aspect of our rheumatology practices,” said ACR President Ellen Gravallese, MD in a statement. “It has impacted our patients’ lives significantly and required us to create new ways of delivering care through improved telehealth and other adaptations.”
While many rheumatologists have resumed in-person visits, “others, like myself, are doing a hybrid,” Dr. Feldman said.

At the height of the pandemic in New York City, Elana J. Bernstein, MD’s practice relied entirely on telehealth visits. “We weren’t seeing any patients in the office for a couple of months. Now that things have reopened here, we’ve resumed face-to-face visits,” keeping some telehealth visits for patients who are still uncomfortable with in-person visits or who live far away, Dr. Bernstein, director of the scleroderma program at Columbia University, New York, said in an interview. She estimates that telehealth represents about 20%-30% of her practice right now.
Advantages, drawbacks of telehealth
For patients in underserved or geographically distant areas, telehealth means access to care, Kanika Monga, MD, of the University of Texas Health Science Center, Houston, said in an interview. During the COVID-19 public health crisis, “it has allowed the most vulnerable patient populations to continue receiving care at the click of a button.”

Virtual visits also improve patient care by improving follow-up and compliance, Dr. Monga continued. “For example, in our patient population, mobility can be a major issue because of the underlying disease. Telemedicine improves care for patients who struggle to make it to appointments.” It’s also more convenient for patients in her county that depend on arranged and/or public transportation and have to request a portion of their day off work for a doctor’s appointment.
But the virtual visit has its drawbacks. Different available platforms and their usability create challenges, Dr. Monga said. “Although some patients are tech-savvy, some are not. This is a challenge, especially when using platforms that have many steps involved.” Telemedicine also highlights general health inequities that already exist in some populations. Patients who are older, live in rural areas, are less educated, or are from a lower socioeconomic household might not have the technology or Internet connection available to enable telemedicine visits.
Telemedicine also complicates the physical examination, which is a central part of the diagnostic process, Dr. Bernstein said. Some components of the physical exam lend themselves to a video visit, such as evaluating for facial rashes or examining a patient’s digital ulcers. “But if you suspect the patient has rheumatoid arthritis, for example, you can’t examine the joints for swelling.” When seeing scleroderma patients over telemedicine, “I can’t perform the modified Rodnan skin score to assess for skin thickening, or auscultate the lungs for crackles. It’s also hard to assess a patient’s response to therapy over telemedicine,” Dr. Feldman added.
Some rheumatologists have sought out multiple pathways on telemedicine to provide more options for patients.
Christine Peoples, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center, uses several telehealth options to reach patients that live in the largely rural area she serves. For her, telemedicine isn’t a novel concept. “I’ve been providing care through telemedicine for 6 years,” she said in an interview. Prior to COVID-19, her patients had gone to teleconsult centers for a telemedicine visit. With the onset of the COVID-19 pandemic, she expanded telehealth services to include more home video visits through the practice’s online medical record.

For care that can’t take place online, Dr. Peoples said she works with colleagues in orthopedics, which have far greater numbers than rheumatologists in Pennsylvania, to provide injections to patients. All of the teleconference centers are at local hospitals or outpatient community centers. Patients can go there to get an injection from another doctor, she said. Additionally, all of her practice’s locations at UPMC hospitals have infusion centers.
Adopting a ‘computer-side’ manner
Any practice offering telemedicine should be training their staff, as virtual meetings require certain skills, Dr. Peoples stressed. “You have to have experience as a rheumatologist, but you also have to have experience in telemedicine. Then it’s about merging those two skills.” Physicians need to be familiar with the technology and equipment. “I have a Bluetooth stethoscope that hears the heart and the lungs” of a patient during a virtual visit, she said.
Most importantly, physicians need to adopt a “computer-side” manner. “Make sure you have good eye contact on the screen, that you’re maintaining a good, professional relationship with the patient.” Training nurses to assist doctors during a telehealth visit is also key.
Dr. Peoples said UPMC has been training its fellows in telemedicine to adopt these skills.
Efforts to pay doctors for telehealth
As rheumatologists navigate the growing market for telehealth, questions remain about the long term payment outlook for these services.
For now, there appears to be reimbursement parity for telehealth visits, Dr. Feldman said. COVID-19’s public health emergency put into place certain flexibilities for telehealth. But some concerns remain about the commercial insurance sector. Whether private payers will continue paying the same amount as they do for in-person visits once the pandemic is over is unknown, Dr. Feldman added. “Insurance companies have had a boom in profits and should not be able to use ‘losses’ from COVID as an excuse for stopping pay parity for telehealth visits.”
David Allen, spokesperson for America’s Health Insurance Plans, said some plans are voluntarily offering telehealth payment parity during the public health emergency. “However, as a policy, AHIP does not support mandating that clinicians be paid the same amount for telehealth and in-person care,” Mr. Allen said, adding that AHIP hasn’t tallied how many insurance companies offer payment parity. “Too many variances exist between plans to make any kind of declarative statement on this.”
For her telemedicine visits at teleconsult centers, Dr. Peoples said compensation is comparable with traditional in-person visits. “Compensation is different for video visits where the patient is at home. However, these video visits are still reimbursed by most insurance plans.”
Federal payers and many states have taken actions on parity. Telehealth is seeing major legislative action at the state level, Kelly Hughes, a program director for the National Conference of State Legislatures, said during the CSRO meeting. All 50 states, the District of Columbia, and Puerto Rico have made revisions to telehealth policies during the COVID-19 pandemic to maintain access to health care services and to minimize potential exposure. Most of these are temporary modifications to address the pandemic, but some states are either adopting permanent changes or mulling over permanent changes to telehealth, Ms. Hughes said.
Modifications vary widely by state, but the top three trends include allowing reimbursement for phone calls (not requiring video), expanding the types of providers authorized to provide telehealth services, and allowing a relationship between a patient and provider to begin with a telehealth visit.
The Commonwealth Fund reports that at least 13 states have enacted payment parity laws in response to COVID-19. Another four had parity laws in place prior to the pandemic. “Many states have taken direct action via Medicaid policy; all but two issued specific guidance on the expansion or reimbursement of Medicaid-based telehealth services,” according to the Commonwealth Fund.
In Texas, where Dr. Monga practices. Gov. Greg Abbott (R) has temporarily waived regulations to lift certain telehealth restrictions. The Texas Department of Insurance under an emergency rule is directing state-regulated health plans to cover telemedicine visits at the same rate as in-person visits during the COVID-19 emergency declaration. “This has helped expand our telehealth options in Texas,” Dr. Monga said.
Medicare has also boosted coverage of telehealth services. “I appreciate that the Centers for Medicare & Medicaid Services has acknowledged the value of telehealth services by reimbursing for audio-only visits at the same rate as audiovisual and in-person evaluations during the public health emergency,” Dr. Monga said.
CMS has also proposed to expand telehealth access in its CY 2021 Physician Fee Schedule Proposed Rule. Additionally, the Department of Health & Human Services Office of Rights will not be penalizing physicians for HIPAA noncompliance for conducting visits through technologies such as FaceTime or Skype during COVID-19, she added.
While telehealth can’t replace all in-person visits in rheumatology, “it can certainly provide us with support during certain circumstances, as we have learned during the current health emergency,” Dr. Monga said. “I hope that even after this crisis has passed that parity for telehealth will be maintained and we can make permanent some of the current updates.”
Rheumatologists are seeing the number of telehealth visits skyrocket in their practices as the COVID-19 pandemic rages on and patients seek out alternatives to in-person visits. Telemedicine makes it easier for patients to connect with physicians, but not all patients have access to a computer or device. It also limits what a physician can do. Rheumatologists often rely on physical exams to make diagnoses and treatment decisions – an obstacle if you’re looking at patients through a computer screen.
Presenters at the 2020 Coalition of State Rheumatology Organizations’ state advocacy conference discussed the benefits and challenges of this mode of care in early September. Within weeks, the U.S. health system eliminated almost half of all medical care as the pandemic ramped up and things went virtual, said Larry Van Horn, PhD, MPH, a speaker at the CSRO conference. Still, “we are in uncharted territory with respect to how telehealth is being used. ... It’s being deployed everywhere, but it’s too early to tell how it’s affecting patient outcomes,” said Dr. Van Horn, founder and director of the Center of Health Care Market Innovation at Vanderbilt University, Nashville, Tenn.
Patients seem to like using telemedicine, observed New Jersey state Sen. Herb Conaway, MD, another presenter. “I think it’s here to stay, and it’s likely to expand going forward. But physicians and others are going to want to make sure it’s used appropriately.”
Some payers feel that telemedicine should be billed differently than brick and mortar visits, Dr. Conaway said. “Physicians feel differently about that, and so we’ll see how this goes, moving forward.”
Lately, there have been discussions of liability concerns associated with telemedicine, said CSRO President Madelaine A. Feldman, MD, who practices in New Orleans. “There are some things you can miss with virtual visits. Certain new patient visits may need to be done in person.”
The landscape of telehealth in rheumatology
Telehealth has directly affected the way rheumatologists do business. In a national survey of more than 1,100 adult patients, the American College of Rheumatology found that 66% are choosing telehealth for rheumatology visits, mainly to avoid exposure to the SARS-CoV-2 virus. This contrasts with a 52% decline in the percentage of patients who are currently seeing a rheumatologist since 2019. “The pandemic has altered almost every aspect of our rheumatology practices,” said ACR President Ellen Gravallese, MD in a statement. “It has impacted our patients’ lives significantly and required us to create new ways of delivering care through improved telehealth and other adaptations.”
While many rheumatologists have resumed in-person visits, “others, like myself, are doing a hybrid,” Dr. Feldman said.
At the height of the pandemic in New York City, Elana J. Bernstein, MD’s practice relied entirely on telehealth visits. “We weren’t seeing any patients in the office for a couple of months. Now that things have reopened here, we’ve resumed face-to-face visits,” keeping some telehealth visits for patients who are still uncomfortable with in-person visits or who live far away, Dr. Bernstein, director of the scleroderma program at Columbia University, New York, said in an interview. She estimates that telehealth represents about 20%-30% of her practice right now.
Advantages, drawbacks of telehealth
For patients in underserved or geographically distant areas, telehealth means access to care, Kanika Monga, MD, of the University of Texas Health Science Center, Houston, said in an interview. During the COVID-19 public health crisis, “it has allowed the most vulnerable patient populations to continue receiving care at the click of a button.”
Virtual visits also improve patient care by improving follow-up and compliance, Dr. Monga continued. “For example, in our patient population, mobility can be a major issue because of the underlying disease. Telemedicine improves care for patients who struggle to make it to appointments.” It’s also more convenient for patients in her county that depend on arranged and/or public transportation and have to request a portion of their day off work for a doctor’s appointment.
But the virtual visit has its drawbacks. Different available platforms and their usability create challenges, Dr. Monga said. “Although some patients are tech-savvy, some are not. This is a challenge, especially when using platforms that have many steps involved.” Telemedicine also highlights general health inequities that already exist in some populations. Patients who are older, live in rural areas, are less educated, or are from a lower socioeconomic household might not have the technology or Internet connection available to enable telemedicine visits.
Telemedicine also complicates the physical examination, which is a central part of the diagnostic process, Dr. Bernstein said. Some components of the physical exam lend themselves to a video visit, such as evaluating for facial rashes or examining a patient’s digital ulcers. “But if you suspect the patient has rheumatoid arthritis, for example, you can’t examine the joints for swelling.” When seeing scleroderma patients over telemedicine, “I can’t perform the modified Rodnan skin score to assess for skin thickening, or auscultate the lungs for crackles. It’s also hard to assess a patient’s response to therapy over telemedicine,” Dr. Feldman added.
Some rheumatologists have sought out multiple pathways on telemedicine to provide more options for patients.
Christine Peoples, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center, uses several telehealth options to reach patients that live in the largely rural area she serves. For her, telemedicine isn’t a novel concept. “I’ve been providing care through telemedicine for 6 years,” she said in an interview. Prior to COVID-19, her patients had gone to teleconsult centers for a telemedicine visit. With the onset of the COVID-19 pandemic, she expanded telehealth services to include more home video visits through the practice’s online medical record.
For care that can’t take place online, Dr. Peoples said she works with colleagues in orthopedics, which have far greater numbers than rheumatologists in Pennsylvania, to provide injections to patients. All of the teleconference centers are at local hospitals or outpatient community centers. Patients can go there to get an injection from another doctor, she said. Additionally, all of her practice’s locations at UPMC hospitals have infusion centers.
Adopting a ‘computer-side’ manner
Any practice offering telemedicine should be training their staff, as virtual meetings require certain skills, Dr. Peoples stressed. “You have to have experience as a rheumatologist, but you also have to have experience in telemedicine. Then it’s about merging those two skills.” Physicians need to be familiar with the technology and equipment. “I have a Bluetooth stethoscope that hears the heart and the lungs” of a patient during a virtual visit, she said.
Most importantly, physicians need to adopt a “computer-side” manner. “Make sure you have good eye contact on the screen, that you’re maintaining a good, professional relationship with the patient.” Training nurses to assist doctors during a telehealth visit is also key.
Dr. Peoples said UPMC has been training its fellows in telemedicine to adopt these skills.
Efforts to pay doctors for telehealth
As rheumatologists navigate the growing market for telehealth, questions remain about the long term payment outlook for these services.
For now, there appears to be reimbursement parity for telehealth visits, Dr. Feldman said. COVID-19’s public health emergency put into place certain flexibilities for telehealth. But some concerns remain about the commercial insurance sector. Whether private payers will continue paying the same amount as they do for in-person visits once the pandemic is over is unknown, Dr. Feldman added. “Insurance companies have had a boom in profits and should not be able to use ‘losses’ from COVID as an excuse for stopping pay parity for telehealth visits.”
David Allen, spokesperson for America’s Health Insurance Plans, said some plans are voluntarily offering telehealth payment parity during the public health emergency. “However, as a policy, AHIP does not support mandating that clinicians be paid the same amount for telehealth and in-person care,” Mr. Allen said, adding that AHIP hasn’t tallied how many insurance companies offer payment parity. “Too many variances exist between plans to make any kind of declarative statement on this.”
For her telemedicine visits at teleconsult centers, Dr. Peoples said compensation is comparable with traditional in-person visits. “Compensation is different for video visits where the patient is at home. However, these video visits are still reimbursed by most insurance plans.”
Federal payers and many states have taken actions on parity. Telehealth is seeing major legislative action at the state level, Kelly Hughes, a program director for the National Conference of State Legislatures, said during the CSRO meeting. All 50 states, the District of Columbia, and Puerto Rico have made revisions to telehealth policies during the COVID-19 pandemic to maintain access to health care services and to minimize potential exposure. Most of these are temporary modifications to address the pandemic, but some states are either adopting permanent changes or mulling over permanent changes to telehealth, Ms. Hughes said.
Modifications vary widely by state, but the top three trends include allowing reimbursement for phone calls (not requiring video), expanding the types of providers authorized to provide telehealth services, and allowing a relationship between a patient and provider to begin with a telehealth visit.
The Commonwealth Fund reports that at least 13 states have enacted payment parity laws in response to COVID-19. Another four had parity laws in place prior to the pandemic. “Many states have taken direct action via Medicaid policy; all but two issued specific guidance on the expansion or reimbursement of Medicaid-based telehealth services,” according to the Commonwealth Fund.
In Texas, where Dr. Monga practices. Gov. Greg Abbott (R) has temporarily waived regulations to lift certain telehealth restrictions. The Texas Department of Insurance under an emergency rule is directing state-regulated health plans to cover telemedicine visits at the same rate as in-person visits during the COVID-19 emergency declaration. “This has helped expand our telehealth options in Texas,” Dr. Monga said.
Medicare has also boosted coverage of telehealth services. “I appreciate that the Centers for Medicare & Medicaid Services has acknowledged the value of telehealth services by reimbursing for audio-only visits at the same rate as audiovisual and in-person evaluations during the public health emergency,” Dr. Monga said.
CMS has also proposed to expand telehealth access in its CY 2021 Physician Fee Schedule Proposed Rule. Additionally, the Department of Health & Human Services Office of Rights will not be penalizing physicians for HIPAA noncompliance for conducting visits through technologies such as FaceTime or Skype during COVID-19, she added.
While telehealth can’t replace all in-person visits in rheumatology, “it can certainly provide us with support during certain circumstances, as we have learned during the current health emergency,” Dr. Monga said. “I hope that even after this crisis has passed that parity for telehealth will be maintained and we can make permanent some of the current updates.”
Rheumatologists are seeing the number of telehealth visits skyrocket in their practices as the COVID-19 pandemic rages on and patients seek out alternatives to in-person visits. Telemedicine makes it easier for patients to connect with physicians, but not all patients have access to a computer or device. It also limits what a physician can do. Rheumatologists often rely on physical exams to make diagnoses and treatment decisions – an obstacle if you’re looking at patients through a computer screen.
Presenters at the 2020 Coalition of State Rheumatology Organizations’ state advocacy conference discussed the benefits and challenges of this mode of care in early September. Within weeks, the U.S. health system eliminated almost half of all medical care as the pandemic ramped up and things went virtual, said Larry Van Horn, PhD, MPH, a speaker at the CSRO conference. Still, “we are in uncharted territory with respect to how telehealth is being used. ... It’s being deployed everywhere, but it’s too early to tell how it’s affecting patient outcomes,” said Dr. Van Horn, founder and director of the Center of Health Care Market Innovation at Vanderbilt University, Nashville, Tenn.
Patients seem to like using telemedicine, observed New Jersey state Sen. Herb Conaway, MD, another presenter. “I think it’s here to stay, and it’s likely to expand going forward. But physicians and others are going to want to make sure it’s used appropriately.”
Some payers feel that telemedicine should be billed differently than brick and mortar visits, Dr. Conaway said. “Physicians feel differently about that, and so we’ll see how this goes, moving forward.”
Lately, there have been discussions of liability concerns associated with telemedicine, said CSRO President Madelaine A. Feldman, MD, who practices in New Orleans. “There are some things you can miss with virtual visits. Certain new patient visits may need to be done in person.”
The landscape of telehealth in rheumatology
Telehealth has directly affected the way rheumatologists do business. In a national survey of more than 1,100 adult patients, the American College of Rheumatology found that 66% are choosing telehealth for rheumatology visits, mainly to avoid exposure to the SARS-CoV-2 virus. This contrasts with a 52% decline in the percentage of patients who are currently seeing a rheumatologist since 2019. “The pandemic has altered almost every aspect of our rheumatology practices,” said ACR President Ellen Gravallese, MD in a statement. “It has impacted our patients’ lives significantly and required us to create new ways of delivering care through improved telehealth and other adaptations.”
While many rheumatologists have resumed in-person visits, “others, like myself, are doing a hybrid,” Dr. Feldman said.
At the height of the pandemic in New York City, Elana J. Bernstein, MD’s practice relied entirely on telehealth visits. “We weren’t seeing any patients in the office for a couple of months. Now that things have reopened here, we’ve resumed face-to-face visits,” keeping some telehealth visits for patients who are still uncomfortable with in-person visits or who live far away, Dr. Bernstein, director of the scleroderma program at Columbia University, New York, said in an interview. She estimates that telehealth represents about 20%-30% of her practice right now.
Advantages, drawbacks of telehealth
For patients in underserved or geographically distant areas, telehealth means access to care, Kanika Monga, MD, of the University of Texas Health Science Center, Houston, said in an interview. During the COVID-19 public health crisis, “it has allowed the most vulnerable patient populations to continue receiving care at the click of a button.”
Virtual visits also improve patient care by improving follow-up and compliance, Dr. Monga continued. “For example, in our patient population, mobility can be a major issue because of the underlying disease. Telemedicine improves care for patients who struggle to make it to appointments.” It’s also more convenient for patients in her county that depend on arranged and/or public transportation and have to request a portion of their day off work for a doctor’s appointment.
But the virtual visit has its drawbacks. Different available platforms and their usability create challenges, Dr. Monga said. “Although some patients are tech-savvy, some are not. This is a challenge, especially when using platforms that have many steps involved.” Telemedicine also highlights general health inequities that already exist in some populations. Patients who are older, live in rural areas, are less educated, or are from a lower socioeconomic household might not have the technology or Internet connection available to enable telemedicine visits.
Telemedicine also complicates the physical examination, which is a central part of the diagnostic process, Dr. Bernstein said. Some components of the physical exam lend themselves to a video visit, such as evaluating for facial rashes or examining a patient’s digital ulcers. “But if you suspect the patient has rheumatoid arthritis, for example, you can’t examine the joints for swelling.” When seeing scleroderma patients over telemedicine, “I can’t perform the modified Rodnan skin score to assess for skin thickening, or auscultate the lungs for crackles. It’s also hard to assess a patient’s response to therapy over telemedicine,” Dr. Feldman added.
Some rheumatologists have sought out multiple pathways on telemedicine to provide more options for patients.
Christine Peoples, MD, clinical assistant professor of medicine at the University of Pittsburgh Medical Center, uses several telehealth options to reach patients that live in the largely rural area she serves. For her, telemedicine isn’t a novel concept. “I’ve been providing care through telemedicine for 6 years,” she said in an interview. Prior to COVID-19, her patients had gone to teleconsult centers for a telemedicine visit. With the onset of the COVID-19 pandemic, she expanded telehealth services to include more home video visits through the practice’s online medical record.
For care that can’t take place online, Dr. Peoples said she works with colleagues in orthopedics, which have far greater numbers than rheumatologists in Pennsylvania, to provide injections to patients. All of the teleconference centers are at local hospitals or outpatient community centers. Patients can go there to get an injection from another doctor, she said. Additionally, all of her practice’s locations at UPMC hospitals have infusion centers.
Adopting a ‘computer-side’ manner
Any practice offering telemedicine should be training their staff, as virtual meetings require certain skills, Dr. Peoples stressed. “You have to have experience as a rheumatologist, but you also have to have experience in telemedicine. Then it’s about merging those two skills.” Physicians need to be familiar with the technology and equipment. “I have a Bluetooth stethoscope that hears the heart and the lungs” of a patient during a virtual visit, she said.
Most importantly, physicians need to adopt a “computer-side” manner. “Make sure you have good eye contact on the screen, that you’re maintaining a good, professional relationship with the patient.” Training nurses to assist doctors during a telehealth visit is also key.
Dr. Peoples said UPMC has been training its fellows in telemedicine to adopt these skills.
Efforts to pay doctors for telehealth
As rheumatologists navigate the growing market for telehealth, questions remain about the long term payment outlook for these services.
For now, there appears to be reimbursement parity for telehealth visits, Dr. Feldman said. COVID-19’s public health emergency put into place certain flexibilities for telehealth. But some concerns remain about the commercial insurance sector. Whether private payers will continue paying the same amount as they do for in-person visits once the pandemic is over is unknown, Dr. Feldman added. “Insurance companies have had a boom in profits and should not be able to use ‘losses’ from COVID as an excuse for stopping pay parity for telehealth visits.”
David Allen, spokesperson for America’s Health Insurance Plans, said some plans are voluntarily offering telehealth payment parity during the public health emergency. “However, as a policy, AHIP does not support mandating that clinicians be paid the same amount for telehealth and in-person care,” Mr. Allen said, adding that AHIP hasn’t tallied how many insurance companies offer payment parity. “Too many variances exist between plans to make any kind of declarative statement on this.”
For her telemedicine visits at teleconsult centers, Dr. Peoples said compensation is comparable with traditional in-person visits. “Compensation is different for video visits where the patient is at home. However, these video visits are still reimbursed by most insurance plans.”
Federal payers and many states have taken actions on parity. Telehealth is seeing major legislative action at the state level, Kelly Hughes, a program director for the National Conference of State Legislatures, said during the CSRO meeting. All 50 states, the District of Columbia, and Puerto Rico have made revisions to telehealth policies during the COVID-19 pandemic to maintain access to health care services and to minimize potential exposure. Most of these are temporary modifications to address the pandemic, but some states are either adopting permanent changes or mulling over permanent changes to telehealth, Ms. Hughes said.
Modifications vary widely by state, but the top three trends include allowing reimbursement for phone calls (not requiring video), expanding the types of providers authorized to provide telehealth services, and allowing a relationship between a patient and provider to begin with a telehealth visit.
The Commonwealth Fund reports that at least 13 states have enacted payment parity laws in response to COVID-19. Another four had parity laws in place prior to the pandemic. “Many states have taken direct action via Medicaid policy; all but two issued specific guidance on the expansion or reimbursement of Medicaid-based telehealth services,” according to the Commonwealth Fund.
In Texas, where Dr. Monga practices. Gov. Greg Abbott (R) has temporarily waived regulations to lift certain telehealth restrictions. The Texas Department of Insurance under an emergency rule is directing state-regulated health plans to cover telemedicine visits at the same rate as in-person visits during the COVID-19 emergency declaration. “This has helped expand our telehealth options in Texas,” Dr. Monga said.
Medicare has also boosted coverage of telehealth services. “I appreciate that the Centers for Medicare & Medicaid Services has acknowledged the value of telehealth services by reimbursing for audio-only visits at the same rate as audiovisual and in-person evaluations during the public health emergency,” Dr. Monga said.
CMS has also proposed to expand telehealth access in its CY 2021 Physician Fee Schedule Proposed Rule. Additionally, the Department of Health & Human Services Office of Rights will not be penalizing physicians for HIPAA noncompliance for conducting visits through technologies such as FaceTime or Skype during COVID-19, she added.
While telehealth can’t replace all in-person visits in rheumatology, “it can certainly provide us with support during certain circumstances, as we have learned during the current health emergency,” Dr. Monga said. “I hope that even after this crisis has passed that parity for telehealth will be maintained and we can make permanent some of the current updates.”
Wildfires’ toxic air leaves damage long after the smoke clears
When researchers arrived in Seeley Lake, Mont., a town tucked in the northern Rockies, 3 years ago, they could still smell the smoke a day after it cleared from devastating wildfires. Their plan was to chart how long it took for people to recover from living for 7 weeks surrounded by relentless smoke.

They still don’t know, because most residents haven’t recovered. In fact, they’ve gotten worse.
Forest fires had funneled hazardous air into Seeley Lake, a town of fewer than 2,000 people, for 49 days. The air quality was so bad that on some days the monitoring stations couldn’t measure the extent of the pollution. The intensity of the smoke and the length of time residents had been trapped in it were unprecedented, prompting county officials to issue their first evacuation orders because of smoke, not fire risk.
Many people stayed. That made Seeley Lake an ideal place to track the long-term health of people inundated by wildfire pollution.
So far, researchers have found that people’s lung capacity declined in the first 2 years after the smoke cleared. Chris Migliaccio, PhD, an immunologist with the University of Montana, Missoula, and associates found the percentage of residents whose lung function sank below normal thresholds more than doubled in the first year after the fire and remained low a year after that.
“There’s something wrong there,” Dr. Migliaccio said.
While it’s long been known that smoke can be dangerous when in the thick of it – triggering asthma attacks, cardiac arrests, hospitalizations and more – the Seeley Lake research confirmed what public health experts feared: Wildfire haze can have consequences long after it’s gone.
That doesn’t bode well for the 78 million people in the western United States now confronting historic wildfires.
Toxic air from fires has blanketed California and the Pacific Northwest for weeks now, causing some of the world’s worst air quality. California fires have burned roughly 2.3 million acres so far this year, and the wildfire season isn’t over yet. Oregon estimates 500,000 people in the state have been under a notice to either prepare to evacuate or leave. Smoke from the West Coast blazes has drifted as far away as Europe.
Extreme wildfires are predicted to become a regular occurrence because of climate change. And, as more people increasingly settle in fire-prone places, the risks increase. That’s shifted wildfires from being a perennial reality for rural mountain towns to becoming an annual threat for areas across the West.
Perry Hystad, PhD, an associate professor at Oregon State University, Corvallis, said the Seeley Lake research offers unique insights into wildfire smoke’s impact, which until recently had largely been unexplored. He said similar studies are likely to follow because of this fire season.
“This is the question that everybody is asking,” Dr. Hystad said. “‘I’ve been sitting in smoke for 2 weeks, how concerned should I be?’”
Dr. Migliaccio wants to know whether the lung damage he saw in Seeley Lake is reversible – or even treatable. (Think of an inhaler for asthma or other medication that prevents swollen airways.)
But those discoveries will have to wait. The team hasn’t been able to return to Seeley Lake this year because of the coronavirus pandemic.
Dr. Migliaccio said more research is needed on whether wildfire smoke damages organs besides the lungs, and whether routine exposure makes people more susceptible to diseases.
The combination of the fire season and the pandemic has spurred other questions as well, like whether heavy smoke exposure could lead to more COVID-19 deaths. A recent study showed a spike in influenza cases following major fire seasons.
“Now you have the combination of flu season and COVID and the wildfires,” Dr. Migliaccio said. “How are all these things going to interact come late fall or winter?”
A case study
Seeley Lake has long known smoke. It sits in a narrow valley between vast stretches of thick forests.
On a recent September day, Boyd Gossard stood on his back porch and pointed toward the mountains that were ablaze in 2017.
Mr. Gossard, 80, expects to have some summer days veiled in haze. But that year, he said, he could hardly see his neighbor’s house a few hundred feet away.
“I’ve seen a lot of smoke in my career,” said Mr. Gossard, who worked in timber management and served as a wildland firefighter. “But having to just live in it like this was very different. It got to you after a while.”
When Missoula County health officials urged people to leave town and flee the hazardous smoke, many residents stayed close to home. Some said their jobs wouldn’t let them leave. Others didn’t have a place to go – or the money to get there.
Health officials warned those who stayed to avoid exercising and breathing too hard, to remain inside, and to follow steps to make their homes as smoke free as possible. The health department also worked to get air filters to those who needed them most.
But when flames got too close, some people had to sleep outside in campsites on the other side of town.
Understanding the science of smoke
One of the known dangers of smoke is particulate matter. Smaller than the width of a human hair, it can bypass a body’s defenses, lodging deep into lungs. Lu Hu, PhD, an atmospheric chemist with the University of Montana, said air quality reports are based on how much of that pollution is in the air.
“It’s like lead; there’s no safe level, but still we have a safety measure for what’s allowable,” Dr. Hu said. “Some things kill you fast and some things kill you slowly.”
While air quality measurements can gauge the overall amount of pollution, they can’t assess which specific toxins people are inhaling. Dr. Hu is collaborating with other scientists to better predict how smoke travels and what pollutants people actually breathe.
He said smoke’s chemistry changes based on how far it travels and what’s burning, among other factors.
Over the past few years, teams of researchers drove trucks along fire lines to collect smoke samples. Other scientists boarded cargo planes and flew into smoke plumes to take samples right from a fire’s source. Still others stationed at a mountain lookout captured smoke drifting in from nearby fires. And ground-level machines at a Missoula site logged data over 2 summers.
Bob Yokelson, PhD, a longtime smoke researcher with the University of Montana, said scientists are getting closer to understanding its contents. And, he said, “it’s not all bad news.”
Temperature and sunlight can change some pollutants over time. Some dangerous particles seem to disappear. But others, such as ozone, can increase as smoke ages.
Dr. Yokelson said scientists are still a long way from determining a safe level of exposure to the hundred-odd pollutants in smoke.
“We can complete the circle by measuring not only what’s in smoke, but measuring what’s happening to the people who breathe it,” Dr. Yokelson said. “That’s where the future of health research on smoke is going to go.”
Coping with nowhere to flee
In the meantime, those studying wildland smoke hope what they’ve learned so far can better prepare people to live in the haze when evacuation isn’t an option.
Joan Wollan, 82, was one of the Seeley Lake study participants. She stayed put during the 2017 fire because her house at the time sat on a border of the evacuation zone. The air made her eyes burn and her husband cough. She ordered air filters to create cleaner air inside her home, which helped.
On a recent day, the air in Mrs. Wollan’s new neighborhood in Missoula turned that familiar gray-orange as traces of fires from elsewhere appeared. Local health officials warned that western Montana could get hit by some of the worst air quality the state had seen since those 2017 fires.
If it got bad enough, Mrs. Wollan said, she’d get the filters out of storage or look for a way to get to cleaner air – “if there is someplace in Montana that isn’t smoky.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
When researchers arrived in Seeley Lake, Mont., a town tucked in the northern Rockies, 3 years ago, they could still smell the smoke a day after it cleared from devastating wildfires. Their plan was to chart how long it took for people to recover from living for 7 weeks surrounded by relentless smoke.
They still don’t know, because most residents haven’t recovered. In fact, they’ve gotten worse.
Forest fires had funneled hazardous air into Seeley Lake, a town of fewer than 2,000 people, for 49 days. The air quality was so bad that on some days the monitoring stations couldn’t measure the extent of the pollution. The intensity of the smoke and the length of time residents had been trapped in it were unprecedented, prompting county officials to issue their first evacuation orders because of smoke, not fire risk.
Many people stayed. That made Seeley Lake an ideal place to track the long-term health of people inundated by wildfire pollution.
So far, researchers have found that people’s lung capacity declined in the first 2 years after the smoke cleared. Chris Migliaccio, PhD, an immunologist with the University of Montana, Missoula, and associates found the percentage of residents whose lung function sank below normal thresholds more than doubled in the first year after the fire and remained low a year after that.
“There’s something wrong there,” Dr. Migliaccio said.
While it’s long been known that smoke can be dangerous when in the thick of it – triggering asthma attacks, cardiac arrests, hospitalizations and more – the Seeley Lake research confirmed what public health experts feared: Wildfire haze can have consequences long after it’s gone.
That doesn’t bode well for the 78 million people in the western United States now confronting historic wildfires.
Toxic air from fires has blanketed California and the Pacific Northwest for weeks now, causing some of the world’s worst air quality. California fires have burned roughly 2.3 million acres so far this year, and the wildfire season isn’t over yet. Oregon estimates 500,000 people in the state have been under a notice to either prepare to evacuate or leave. Smoke from the West Coast blazes has drifted as far away as Europe.
Extreme wildfires are predicted to become a regular occurrence because of climate change. And, as more people increasingly settle in fire-prone places, the risks increase. That’s shifted wildfires from being a perennial reality for rural mountain towns to becoming an annual threat for areas across the West.
Perry Hystad, PhD, an associate professor at Oregon State University, Corvallis, said the Seeley Lake research offers unique insights into wildfire smoke’s impact, which until recently had largely been unexplored. He said similar studies are likely to follow because of this fire season.
“This is the question that everybody is asking,” Dr. Hystad said. “‘I’ve been sitting in smoke for 2 weeks, how concerned should I be?’”
Dr. Migliaccio wants to know whether the lung damage he saw in Seeley Lake is reversible – or even treatable. (Think of an inhaler for asthma or other medication that prevents swollen airways.)
But those discoveries will have to wait. The team hasn’t been able to return to Seeley Lake this year because of the coronavirus pandemic.
Dr. Migliaccio said more research is needed on whether wildfire smoke damages organs besides the lungs, and whether routine exposure makes people more susceptible to diseases.
The combination of the fire season and the pandemic has spurred other questions as well, like whether heavy smoke exposure could lead to more COVID-19 deaths. A recent study showed a spike in influenza cases following major fire seasons.
“Now you have the combination of flu season and COVID and the wildfires,” Dr. Migliaccio said. “How are all these things going to interact come late fall or winter?”
A case study
Seeley Lake has long known smoke. It sits in a narrow valley between vast stretches of thick forests.
On a recent September day, Boyd Gossard stood on his back porch and pointed toward the mountains that were ablaze in 2017.
Mr. Gossard, 80, expects to have some summer days veiled in haze. But that year, he said, he could hardly see his neighbor’s house a few hundred feet away.
“I’ve seen a lot of smoke in my career,” said Mr. Gossard, who worked in timber management and served as a wildland firefighter. “But having to just live in it like this was very different. It got to you after a while.”
When Missoula County health officials urged people to leave town and flee the hazardous smoke, many residents stayed close to home. Some said their jobs wouldn’t let them leave. Others didn’t have a place to go – or the money to get there.
Health officials warned those who stayed to avoid exercising and breathing too hard, to remain inside, and to follow steps to make their homes as smoke free as possible. The health department also worked to get air filters to those who needed them most.
But when flames got too close, some people had to sleep outside in campsites on the other side of town.
Understanding the science of smoke
One of the known dangers of smoke is particulate matter. Smaller than the width of a human hair, it can bypass a body’s defenses, lodging deep into lungs. Lu Hu, PhD, an atmospheric chemist with the University of Montana, said air quality reports are based on how much of that pollution is in the air.
“It’s like lead; there’s no safe level, but still we have a safety measure for what’s allowable,” Dr. Hu said. “Some things kill you fast and some things kill you slowly.”
While air quality measurements can gauge the overall amount of pollution, they can’t assess which specific toxins people are inhaling. Dr. Hu is collaborating with other scientists to better predict how smoke travels and what pollutants people actually breathe.
He said smoke’s chemistry changes based on how far it travels and what’s burning, among other factors.
Over the past few years, teams of researchers drove trucks along fire lines to collect smoke samples. Other scientists boarded cargo planes and flew into smoke plumes to take samples right from a fire’s source. Still others stationed at a mountain lookout captured smoke drifting in from nearby fires. And ground-level machines at a Missoula site logged data over 2 summers.
Bob Yokelson, PhD, a longtime smoke researcher with the University of Montana, said scientists are getting closer to understanding its contents. And, he said, “it’s not all bad news.”
Temperature and sunlight can change some pollutants over time. Some dangerous particles seem to disappear. But others, such as ozone, can increase as smoke ages.
Dr. Yokelson said scientists are still a long way from determining a safe level of exposure to the hundred-odd pollutants in smoke.
“We can complete the circle by measuring not only what’s in smoke, but measuring what’s happening to the people who breathe it,” Dr. Yokelson said. “That’s where the future of health research on smoke is going to go.”
Coping with nowhere to flee
In the meantime, those studying wildland smoke hope what they’ve learned so far can better prepare people to live in the haze when evacuation isn’t an option.
Joan Wollan, 82, was one of the Seeley Lake study participants. She stayed put during the 2017 fire because her house at the time sat on a border of the evacuation zone. The air made her eyes burn and her husband cough. She ordered air filters to create cleaner air inside her home, which helped.
On a recent day, the air in Mrs. Wollan’s new neighborhood in Missoula turned that familiar gray-orange as traces of fires from elsewhere appeared. Local health officials warned that western Montana could get hit by some of the worst air quality the state had seen since those 2017 fires.
If it got bad enough, Mrs. Wollan said, she’d get the filters out of storage or look for a way to get to cleaner air – “if there is someplace in Montana that isn’t smoky.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
When researchers arrived in Seeley Lake, Mont., a town tucked in the northern Rockies, 3 years ago, they could still smell the smoke a day after it cleared from devastating wildfires. Their plan was to chart how long it took for people to recover from living for 7 weeks surrounded by relentless smoke.
They still don’t know, because most residents haven’t recovered. In fact, they’ve gotten worse.
Forest fires had funneled hazardous air into Seeley Lake, a town of fewer than 2,000 people, for 49 days. The air quality was so bad that on some days the monitoring stations couldn’t measure the extent of the pollution. The intensity of the smoke and the length of time residents had been trapped in it were unprecedented, prompting county officials to issue their first evacuation orders because of smoke, not fire risk.
Many people stayed. That made Seeley Lake an ideal place to track the long-term health of people inundated by wildfire pollution.
So far, researchers have found that people’s lung capacity declined in the first 2 years after the smoke cleared. Chris Migliaccio, PhD, an immunologist with the University of Montana, Missoula, and associates found the percentage of residents whose lung function sank below normal thresholds more than doubled in the first year after the fire and remained low a year after that.
“There’s something wrong there,” Dr. Migliaccio said.
While it’s long been known that smoke can be dangerous when in the thick of it – triggering asthma attacks, cardiac arrests, hospitalizations and more – the Seeley Lake research confirmed what public health experts feared: Wildfire haze can have consequences long after it’s gone.
That doesn’t bode well for the 78 million people in the western United States now confronting historic wildfires.
Toxic air from fires has blanketed California and the Pacific Northwest for weeks now, causing some of the world’s worst air quality. California fires have burned roughly 2.3 million acres so far this year, and the wildfire season isn’t over yet. Oregon estimates 500,000 people in the state have been under a notice to either prepare to evacuate or leave. Smoke from the West Coast blazes has drifted as far away as Europe.
Extreme wildfires are predicted to become a regular occurrence because of climate change. And, as more people increasingly settle in fire-prone places, the risks increase. That’s shifted wildfires from being a perennial reality for rural mountain towns to becoming an annual threat for areas across the West.
Perry Hystad, PhD, an associate professor at Oregon State University, Corvallis, said the Seeley Lake research offers unique insights into wildfire smoke’s impact, which until recently had largely been unexplored. He said similar studies are likely to follow because of this fire season.
“This is the question that everybody is asking,” Dr. Hystad said. “‘I’ve been sitting in smoke for 2 weeks, how concerned should I be?’”
Dr. Migliaccio wants to know whether the lung damage he saw in Seeley Lake is reversible – or even treatable. (Think of an inhaler for asthma or other medication that prevents swollen airways.)
But those discoveries will have to wait. The team hasn’t been able to return to Seeley Lake this year because of the coronavirus pandemic.
Dr. Migliaccio said more research is needed on whether wildfire smoke damages organs besides the lungs, and whether routine exposure makes people more susceptible to diseases.
The combination of the fire season and the pandemic has spurred other questions as well, like whether heavy smoke exposure could lead to more COVID-19 deaths. A recent study showed a spike in influenza cases following major fire seasons.
“Now you have the combination of flu season and COVID and the wildfires,” Dr. Migliaccio said. “How are all these things going to interact come late fall or winter?”
A case study
Seeley Lake has long known smoke. It sits in a narrow valley between vast stretches of thick forests.
On a recent September day, Boyd Gossard stood on his back porch and pointed toward the mountains that were ablaze in 2017.
Mr. Gossard, 80, expects to have some summer days veiled in haze. But that year, he said, he could hardly see his neighbor’s house a few hundred feet away.
“I’ve seen a lot of smoke in my career,” said Mr. Gossard, who worked in timber management and served as a wildland firefighter. “But having to just live in it like this was very different. It got to you after a while.”
When Missoula County health officials urged people to leave town and flee the hazardous smoke, many residents stayed close to home. Some said their jobs wouldn’t let them leave. Others didn’t have a place to go – or the money to get there.
Health officials warned those who stayed to avoid exercising and breathing too hard, to remain inside, and to follow steps to make their homes as smoke free as possible. The health department also worked to get air filters to those who needed them most.
But when flames got too close, some people had to sleep outside in campsites on the other side of town.
Understanding the science of smoke
One of the known dangers of smoke is particulate matter. Smaller than the width of a human hair, it can bypass a body’s defenses, lodging deep into lungs. Lu Hu, PhD, an atmospheric chemist with the University of Montana, said air quality reports are based on how much of that pollution is in the air.
“It’s like lead; there’s no safe level, but still we have a safety measure for what’s allowable,” Dr. Hu said. “Some things kill you fast and some things kill you slowly.”
While air quality measurements can gauge the overall amount of pollution, they can’t assess which specific toxins people are inhaling. Dr. Hu is collaborating with other scientists to better predict how smoke travels and what pollutants people actually breathe.
He said smoke’s chemistry changes based on how far it travels and what’s burning, among other factors.
Over the past few years, teams of researchers drove trucks along fire lines to collect smoke samples. Other scientists boarded cargo planes and flew into smoke plumes to take samples right from a fire’s source. Still others stationed at a mountain lookout captured smoke drifting in from nearby fires. And ground-level machines at a Missoula site logged data over 2 summers.
Bob Yokelson, PhD, a longtime smoke researcher with the University of Montana, said scientists are getting closer to understanding its contents. And, he said, “it’s not all bad news.”
Temperature and sunlight can change some pollutants over time. Some dangerous particles seem to disappear. But others, such as ozone, can increase as smoke ages.
Dr. Yokelson said scientists are still a long way from determining a safe level of exposure to the hundred-odd pollutants in smoke.
“We can complete the circle by measuring not only what’s in smoke, but measuring what’s happening to the people who breathe it,” Dr. Yokelson said. “That’s where the future of health research on smoke is going to go.”
Coping with nowhere to flee
In the meantime, those studying wildland smoke hope what they’ve learned so far can better prepare people to live in the haze when evacuation isn’t an option.
Joan Wollan, 82, was one of the Seeley Lake study participants. She stayed put during the 2017 fire because her house at the time sat on a border of the evacuation zone. The air made her eyes burn and her husband cough. She ordered air filters to create cleaner air inside her home, which helped.
On a recent day, the air in Mrs. Wollan’s new neighborhood in Missoula turned that familiar gray-orange as traces of fires from elsewhere appeared. Local health officials warned that western Montana could get hit by some of the worst air quality the state had seen since those 2017 fires.
If it got bad enough, Mrs. Wollan said, she’d get the filters out of storage or look for a way to get to cleaner air – “if there is someplace in Montana that isn’t smoky.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Many Americans still concerned about access to health care
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
Children and COVID-19: New cases may be leveling off
Growth in new pediatric COVID-19 cases has evened out in recent weeks, but children now represent 10% of all COVID-19 cases in the United States, and that measurement has been rising throughout the pandemic, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
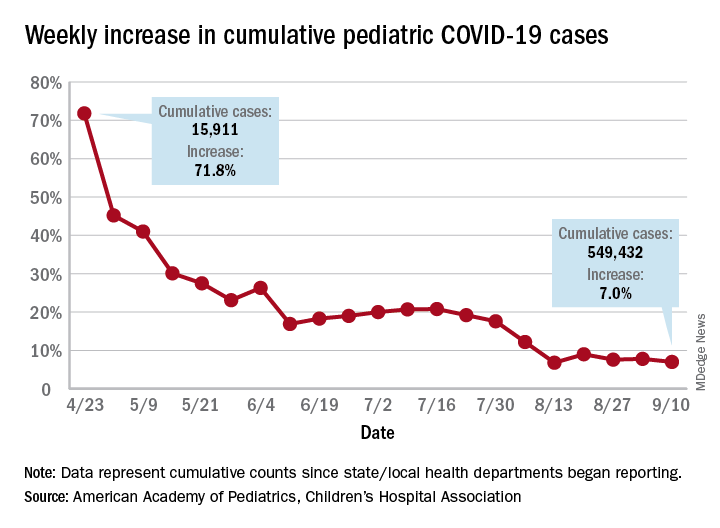
the AAP and the CHA said in the report, based on data from 49 states (New York City is included but not New York state), the District of Columbia, Puerto Rico, and Guam.
The weekly percentage of increase in the number of new cases has not reached double digits since early August and has been no higher than 7.8% over the last 3 weeks. The number of child COVID-19 cases, however, has finally reached 10% of the total for Americans of all ages, which stands at 5.49 million in the jurisdictions included in the report, the AHA and CHA reported.
Measures, however, continue to show low levels of severe illness in children, they noted, including the following:
- Child cases as a proportion of all COVID-19 hospitalizations: 1.7%.
- Hospitalization rate for children: 1.8%.
- Child deaths as a proportion of all deaths: 0.07%.
- Percent of child cases resulting in death: 0.01%.
The number of cumulative cases per 100,000 children is now up to 728.5 nationally, with a range by state that goes from 154.0 in Vermont to 1,670.3 in Tennessee, which is one of only two states reporting cases in those aged 0-20 years as children (the other is South Carolina). The age range for children is 0-17 or 0-19 for most other states, although Florida uses a range of 0-14, the report notes.
Other than Tennessee, there are 10 states with overall rates higher than 1,000 COVID-19 cases per 100,000 children, and there are nine states with cumulative totals over 15,000 cases (California is the highest with just over 75,000), according to the report.
Growth in new pediatric COVID-19 cases has evened out in recent weeks, but children now represent 10% of all COVID-19 cases in the United States, and that measurement has been rising throughout the pandemic, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and the CHA said in the report, based on data from 49 states (New York City is included but not New York state), the District of Columbia, Puerto Rico, and Guam.
The weekly percentage of increase in the number of new cases has not reached double digits since early August and has been no higher than 7.8% over the last 3 weeks. The number of child COVID-19 cases, however, has finally reached 10% of the total for Americans of all ages, which stands at 5.49 million in the jurisdictions included in the report, the AHA and CHA reported.
Measures, however, continue to show low levels of severe illness in children, they noted, including the following:
- Child cases as a proportion of all COVID-19 hospitalizations: 1.7%.
- Hospitalization rate for children: 1.8%.
- Child deaths as a proportion of all deaths: 0.07%.
- Percent of child cases resulting in death: 0.01%.
The number of cumulative cases per 100,000 children is now up to 728.5 nationally, with a range by state that goes from 154.0 in Vermont to 1,670.3 in Tennessee, which is one of only two states reporting cases in those aged 0-20 years as children (the other is South Carolina). The age range for children is 0-17 or 0-19 for most other states, although Florida uses a range of 0-14, the report notes.
Other than Tennessee, there are 10 states with overall rates higher than 1,000 COVID-19 cases per 100,000 children, and there are nine states with cumulative totals over 15,000 cases (California is the highest with just over 75,000), according to the report.
Growth in new pediatric COVID-19 cases has evened out in recent weeks, but children now represent 10% of all COVID-19 cases in the United States, and that measurement has been rising throughout the pandemic, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and the CHA said in the report, based on data from 49 states (New York City is included but not New York state), the District of Columbia, Puerto Rico, and Guam.
The weekly percentage of increase in the number of new cases has not reached double digits since early August and has been no higher than 7.8% over the last 3 weeks. The number of child COVID-19 cases, however, has finally reached 10% of the total for Americans of all ages, which stands at 5.49 million in the jurisdictions included in the report, the AHA and CHA reported.
Measures, however, continue to show low levels of severe illness in children, they noted, including the following:
- Child cases as a proportion of all COVID-19 hospitalizations: 1.7%.
- Hospitalization rate for children: 1.8%.
- Child deaths as a proportion of all deaths: 0.07%.
- Percent of child cases resulting in death: 0.01%.
The number of cumulative cases per 100,000 children is now up to 728.5 nationally, with a range by state that goes from 154.0 in Vermont to 1,670.3 in Tennessee, which is one of only two states reporting cases in those aged 0-20 years as children (the other is South Carolina). The age range for children is 0-17 or 0-19 for most other states, although Florida uses a range of 0-14, the report notes.
Other than Tennessee, there are 10 states with overall rates higher than 1,000 COVID-19 cases per 100,000 children, and there are nine states with cumulative totals over 15,000 cases (California is the highest with just over 75,000), according to the report.
Physician income drops, burnout spikes globally in pandemic
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
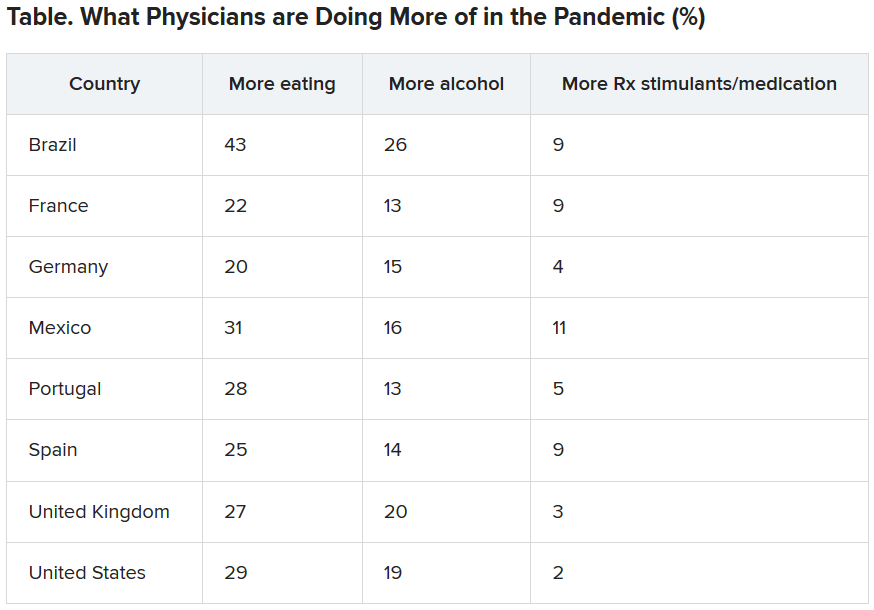
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
Rural areas with local obstetrical care have better perinatal outcomes
according to a retrospective study using county-level data from the Alabama Department of Public Health.

Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.

The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
according to a retrospective study using county-level data from the Alabama Department of Public Health.
Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.
The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
according to a retrospective study using county-level data from the Alabama Department of Public Health.
Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.
The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
FROM ANNALS OF FAMILY MEDICINE
Key clinical point: The absence of labor and delivery (L&D) services in rural counties predicts adverse outcomes, including higher child mortality.
Major finding: In the absence of L&D units, the risk of perinatal mortality per 1,000 live births is 19% higher (5.67 vs. 4.74; P = .0034).
Data Source: Retrospective cohort study.
Disclosures: Potential conflicts of interest involving this topic were not reported.
Source: Waits JB et al. Ann Fam Med. 2020;18:446-51.
Innovator banks on ‘truly smart’ robotic lasers in dermatology

Dr. Anderson, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, conceived and developed many of the nonscarring laser treatments now widely used in dermatology. These include selective photothermolysis for birthmarks, microvascular and pigmented lesions, and tattoo and permanent hair removal. He also contributed to laser lithotripsy, laser angioplasty, photodynamic therapy, and optical diagnostics. The highest-resolution imaging device approved for human use, an infrared confocal microscope, came from his laboratory. Dr. Anderson has also contributed to basic knowledge of human photobiology, drug photosensitization mechanisms, tissue optics and laser-tissue interactions. In this Q&A with Doug Brunk, he reflects on his achievements and on the future of lasers in dermatology.
In published interviews you have described yourself as more of a problem solver than an inventor. How did your upbringing foster your affinity for problem solving?
I grew up in Central Illinois during the 1950s and early 1960s, an area known for corn, soybeans, and hogs. At an early age I learned to be interested in other things because it’s possible to die of boredom there. By the time I was 12 years old, I was an amateur radio operator, and I was building rockets to see how high they would go.
Problem solving comes naturally to me. I enjoy very much finding a problem that is worth solving, which means getting passionate about it and brainstorming. Half the time you don’t come up with a potential route to solve the problem. I attended the Massachusetts Institute of Technology at the age of 17, which was a real eye-opener. I had never been east of the Wabash River prior to that. I studied physics for a while, then decided to flip into biology. That combination has served me well. My special sauce is to have some intuitive and academic rigorous feeling for physical processes. But we physicians have a front row seat to nature’s human drama. There is no lack of problems to solve. I can sit around and obsess about things theoretically, but at the end of the day I want to work on things that ultimately benefit people.
What inspired you most early in your career as a physician scientist?
After I made a commitment to medicine, Dr. John A. Parrish, and Dr. Thomas B. Fitzpatrick were key mentors to me. I was 30 years old when I started medical school, but they took me under their wing even before that. I took a part-time, temporary job with them, which turned into a permanent job. That turned into a love for the work they did. Instead of going into a graduate program in a laboratory and studying bacteria and genetics, the whole idea of working with people and on people was awesome. Dr. Parrish really mentored me. I won a lifetime achievement award from the American Academy of Dermatology a few years ago. I found myself on stage and it rolled out of my mouth that John Parrish believed in me before I believed in myself. It’s really true. He somehow recognized that I had some talents. I was very young and a combination of naive and humble, I guess.
What was the initial genesis for your idea of selective photothermolysis?
I was interested in going to medical school and working with Dr. Fitzpatrick and Dr. Parrish on things related to light. They were mostly interested in PUVA and UVB; it was the heyday of modern phototherapy. I attended a lecture at the Beth Israel Hospital in Boston given by a plastic surgeon, Dr. Joel Mark Noe. He was talking about using lasers to treat port-wine stains in children. The gist of the talk was that argon lasers were being used, and that the results were sometimes decent, but not great. Often children would have burn scars after the treatment. Dr. Noe was talking about how you had to choose the color of the wavelength of the laser to be absorbed by hemoglobin, but he wasn’t talking about what happens to the heat once it’s created. My background in physics led me to recognize that he wasn’t capturing the full picture. Selective disruption of a target in the skin by light is half of the story. The confinement of heat in the target is the other half of the story. Literally on a bus on the way home from that lecture to my apartment in Cambridge, I hatched the idea for selective photothermolysis and wrote down some equations. I also wrote down the ideal wavelength region, how much energy was needed, and what the pulse duration would have to be like to damage target vessels that small. I showed John Parrish what I had written. He took me seriously and said, “Let’s see if we can find a light source that can accomplish this.” We traveled around the country looking at various lasers, but we wound up building the first pulsed dye laser for treating port-wine stains. To me, the surprise was that we didn’t kill the skin. If you treat an area of skin with a laser and hurt all the blood vessels, you think, “Wait a minute. Are we going to kill the skin because it has no blood supply?” The questions of the day were so basic, and we just got lucky. It took 6-8 years before we ramped up the clinical studies showing efficacy and safety of this technology.
I presume that you experimented on your own skin while developing some of the nonscarring laser treatments now widely used in dermatology. What “war story” stands out to you most from that part of your work?
I’m right handed, so I’d grab a laser with my right hand and treat my left arm, so that arm sports a bit of history. In 1994, while working with Dr. Melanie Grossman on the development of laser hair removal, I used a ruby laser to self-treat a patch of hair on my left arm. I still have the world’s oldest laser-induced bald spot on that arm. It’s been 26 years now. I still look at it and count the hairs, because one of the big questions is, is laser hair removal permanent? In all these years I have grown two hairs.
What technology that you conceived of or developed has most surprised you, in term of its ultimate clinical impact?
I would say confocal microscopy. In the mid-1990s I worked with a physicist named Robert H. Webb, who invented an imaging system for the retina. We got together, noodled about it, and decided we would modify his ophthalmoscope system to see if we could get images from inside the skin. It worked pretty well. It was truly surprising from many points of view. First, it wasn’t clear at all that we’d get any images this way. Now, reflectance confocal microscopy is a standard tool in both clinical and research dermatology. But there were odd discoveries early on. For example, the darker your skin, the brighter it appeared in the microscope. You might think that melanin absorbs light and that you would get poor images in dark skin. It was the exact opposite; melanin acts as a natural contrast agent.
We worked with a small company to make the first confocal microscope. Initially, it had no clinical applications but what was fascinating to me was the incredible value of being able to see inside human skin harmlessly, and just see what’s going on. It became a potent research tool, and recently CPT codes were established for its use in evaluating skin cancer margins. I wouldn’t be surprised if 30 years from now, taking a skin biopsy is seemingly barbaric. A forerunner of all these new imaging tools for the skin was the confocal microscope developed in my lab in 1994.
During a 2011 TED talk, you said that nevus of Ota is your favorite thing to treat, because the outcome is usually perfect skin. Are there other technologies or devices you played a role in developing that make you proud at this stage in your career?
The reason I love treating nevus of Ota is that you have a lifelong facial disfigurement, and the only treatment for it is a laser we came up with, and it always works. How perfect could it be? The flip side of the same coin is, there are lesions of the skin that just don’t respond. One of the things we don’t know enough about is the connection between the biologic aspects of repair of various lesions and the treatments that we come up with. The most recent example of selective photothermolysis is a new laser we’re building right now for acne that is based on sebaceous gland injury. You’ll see this coming out in the next year or two. My heart goes out to people with nodular cystic acne. For young men it’s highly associated with suicide. So, I’m excited about optimizing and learning what happens when we target sebaceous glands.
One of the other big stories in laser dermatology is the fractional laser. I developed this with Dr. Dieter Manstein when he was a postdoc in my lab. One of the most pleasing things from this technology is how well you can rehabilitate scars, particularly burn scars in children. Over the last few years, I have trained plastic surgeons at the Shriners Hospital for Children in Boston on how to use fractional lasers to improve the lives of these kids. Another technology I developed with Dr. Manstein is cryolipolysis, which is removing fat from the body by cooling it. There are no lasers involved with this technology. I like to say that I’ve spent most of my career studying light and heat, and now we’ve come up with something that’s cold in the dark. We are now working on derivatives of cryolipolysis, to determine if what we’ve learned about targeting fat that might be applicable elsewhere.
Who inspires you most in your work today?
In addition to Dr. John Parrish and Dr. Thomas Fitzpatrick, the late Dr. Albert M. Kligman also influenced me. He never accepted dogma and he loved to ask questions, like, “What if?” as opposed to just accumulating a fund of knowledge. Understanding things is not just based on how much you know. It’s based on critical thinking and the ability to question. I also admire Albert Einstein, his ability to sit down with nothing more than pencil and paper and change our view of the universe. I love physics because it’s the science of everything. I also love poetry. My favorite poet is Stanley Kunitz. He had amazing insight and was named United States Poet Laureate in 1974 and in 2000. I have plenty of antiheroes as well, mostly politicians.
I understand that you play the banjo. How long have you been playing, and what do you enjoy about it?
You cannot sit down and play the banjo and have your mind on much else. It’s a wonderful moving meditation. Before my medical career, I was a schoolteacher in Vermont. There was a guy on the staff there who played banjo. He came from a small town in Georgia. I just picked it up and started plunking. It’s a happy instrument. It’s awfully hard to make the banjo sound melancholy.
What novel use of lasers and light in dermatology are you most excited about in the next 5 years?
The marriage of therapeutic devices with diagnostic and imaging devices has not happened yet. They are not even in the honeymoon moment. But I think that having truly smart robotic systems in our hands for treating patients will become a reality. These days, dermatologists have to buy a certain type of laser to treat a certain type of lesion. For example, the Q-switched alexandrite laser you buy for treating Nevus of Ota won’t do anything for a port-wine stain; it’s the wrong pulse duration. This means that clinicians who practice a lot of laser dermatology end up with a dozen lasers in their practice. In the future, I think it will be possible to have a software laser, so when you want to acquire another target, you load an App as opposed to buying a new laser. This means that you would have software programmable targeting, and you would not have the requirement of having selective absorption. So, I’m excited by the idea of guided fractional lasers. None of them exist now. We have to start from scratch.
Dr. Anderson, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, conceived and developed many of the nonscarring laser treatments now widely used in dermatology. These include selective photothermolysis for birthmarks, microvascular and pigmented lesions, and tattoo and permanent hair removal. He also contributed to laser lithotripsy, laser angioplasty, photodynamic therapy, and optical diagnostics. The highest-resolution imaging device approved for human use, an infrared confocal microscope, came from his laboratory. Dr. Anderson has also contributed to basic knowledge of human photobiology, drug photosensitization mechanisms, tissue optics and laser-tissue interactions. In this Q&A with Doug Brunk, he reflects on his achievements and on the future of lasers in dermatology.
In published interviews you have described yourself as more of a problem solver than an inventor. How did your upbringing foster your affinity for problem solving?
I grew up in Central Illinois during the 1950s and early 1960s, an area known for corn, soybeans, and hogs. At an early age I learned to be interested in other things because it’s possible to die of boredom there. By the time I was 12 years old, I was an amateur radio operator, and I was building rockets to see how high they would go.
Problem solving comes naturally to me. I enjoy very much finding a problem that is worth solving, which means getting passionate about it and brainstorming. Half the time you don’t come up with a potential route to solve the problem. I attended the Massachusetts Institute of Technology at the age of 17, which was a real eye-opener. I had never been east of the Wabash River prior to that. I studied physics for a while, then decided to flip into biology. That combination has served me well. My special sauce is to have some intuitive and academic rigorous feeling for physical processes. But we physicians have a front row seat to nature’s human drama. There is no lack of problems to solve. I can sit around and obsess about things theoretically, but at the end of the day I want to work on things that ultimately benefit people.
What inspired you most early in your career as a physician scientist?
After I made a commitment to medicine, Dr. John A. Parrish, and Dr. Thomas B. Fitzpatrick were key mentors to me. I was 30 years old when I started medical school, but they took me under their wing even before that. I took a part-time, temporary job with them, which turned into a permanent job. That turned into a love for the work they did. Instead of going into a graduate program in a laboratory and studying bacteria and genetics, the whole idea of working with people and on people was awesome. Dr. Parrish really mentored me. I won a lifetime achievement award from the American Academy of Dermatology a few years ago. I found myself on stage and it rolled out of my mouth that John Parrish believed in me before I believed in myself. It’s really true. He somehow recognized that I had some talents. I was very young and a combination of naive and humble, I guess.
What was the initial genesis for your idea of selective photothermolysis?
I was interested in going to medical school and working with Dr. Fitzpatrick and Dr. Parrish on things related to light. They were mostly interested in PUVA and UVB; it was the heyday of modern phototherapy. I attended a lecture at the Beth Israel Hospital in Boston given by a plastic surgeon, Dr. Joel Mark Noe. He was talking about using lasers to treat port-wine stains in children. The gist of the talk was that argon lasers were being used, and that the results were sometimes decent, but not great. Often children would have burn scars after the treatment. Dr. Noe was talking about how you had to choose the color of the wavelength of the laser to be absorbed by hemoglobin, but he wasn’t talking about what happens to the heat once it’s created. My background in physics led me to recognize that he wasn’t capturing the full picture. Selective disruption of a target in the skin by light is half of the story. The confinement of heat in the target is the other half of the story. Literally on a bus on the way home from that lecture to my apartment in Cambridge, I hatched the idea for selective photothermolysis and wrote down some equations. I also wrote down the ideal wavelength region, how much energy was needed, and what the pulse duration would have to be like to damage target vessels that small. I showed John Parrish what I had written. He took me seriously and said, “Let’s see if we can find a light source that can accomplish this.” We traveled around the country looking at various lasers, but we wound up building the first pulsed dye laser for treating port-wine stains. To me, the surprise was that we didn’t kill the skin. If you treat an area of skin with a laser and hurt all the blood vessels, you think, “Wait a minute. Are we going to kill the skin because it has no blood supply?” The questions of the day were so basic, and we just got lucky. It took 6-8 years before we ramped up the clinical studies showing efficacy and safety of this technology.
I presume that you experimented on your own skin while developing some of the nonscarring laser treatments now widely used in dermatology. What “war story” stands out to you most from that part of your work?
I’m right handed, so I’d grab a laser with my right hand and treat my left arm, so that arm sports a bit of history. In 1994, while working with Dr. Melanie Grossman on the development of laser hair removal, I used a ruby laser to self-treat a patch of hair on my left arm. I still have the world’s oldest laser-induced bald spot on that arm. It’s been 26 years now. I still look at it and count the hairs, because one of the big questions is, is laser hair removal permanent? In all these years I have grown two hairs.
What technology that you conceived of or developed has most surprised you, in term of its ultimate clinical impact?
I would say confocal microscopy. In the mid-1990s I worked with a physicist named Robert H. Webb, who invented an imaging system for the retina. We got together, noodled about it, and decided we would modify his ophthalmoscope system to see if we could get images from inside the skin. It worked pretty well. It was truly surprising from many points of view. First, it wasn’t clear at all that we’d get any images this way. Now, reflectance confocal microscopy is a standard tool in both clinical and research dermatology. But there were odd discoveries early on. For example, the darker your skin, the brighter it appeared in the microscope. You might think that melanin absorbs light and that you would get poor images in dark skin. It was the exact opposite; melanin acts as a natural contrast agent.
We worked with a small company to make the first confocal microscope. Initially, it had no clinical applications but what was fascinating to me was the incredible value of being able to see inside human skin harmlessly, and just see what’s going on. It became a potent research tool, and recently CPT codes were established for its use in evaluating skin cancer margins. I wouldn’t be surprised if 30 years from now, taking a skin biopsy is seemingly barbaric. A forerunner of all these new imaging tools for the skin was the confocal microscope developed in my lab in 1994.
During a 2011 TED talk, you said that nevus of Ota is your favorite thing to treat, because the outcome is usually perfect skin. Are there other technologies or devices you played a role in developing that make you proud at this stage in your career?
The reason I love treating nevus of Ota is that you have a lifelong facial disfigurement, and the only treatment for it is a laser we came up with, and it always works. How perfect could it be? The flip side of the same coin is, there are lesions of the skin that just don’t respond. One of the things we don’t know enough about is the connection between the biologic aspects of repair of various lesions and the treatments that we come up with. The most recent example of selective photothermolysis is a new laser we’re building right now for acne that is based on sebaceous gland injury. You’ll see this coming out in the next year or two. My heart goes out to people with nodular cystic acne. For young men it’s highly associated with suicide. So, I’m excited about optimizing and learning what happens when we target sebaceous glands.
One of the other big stories in laser dermatology is the fractional laser. I developed this with Dr. Dieter Manstein when he was a postdoc in my lab. One of the most pleasing things from this technology is how well you can rehabilitate scars, particularly burn scars in children. Over the last few years, I have trained plastic surgeons at the Shriners Hospital for Children in Boston on how to use fractional lasers to improve the lives of these kids. Another technology I developed with Dr. Manstein is cryolipolysis, which is removing fat from the body by cooling it. There are no lasers involved with this technology. I like to say that I’ve spent most of my career studying light and heat, and now we’ve come up with something that’s cold in the dark. We are now working on derivatives of cryolipolysis, to determine if what we’ve learned about targeting fat that might be applicable elsewhere.
Who inspires you most in your work today?
In addition to Dr. John Parrish and Dr. Thomas Fitzpatrick, the late Dr. Albert M. Kligman also influenced me. He never accepted dogma and he loved to ask questions, like, “What if?” as opposed to just accumulating a fund of knowledge. Understanding things is not just based on how much you know. It’s based on critical thinking and the ability to question. I also admire Albert Einstein, his ability to sit down with nothing more than pencil and paper and change our view of the universe. I love physics because it’s the science of everything. I also love poetry. My favorite poet is Stanley Kunitz. He had amazing insight and was named United States Poet Laureate in 1974 and in 2000. I have plenty of antiheroes as well, mostly politicians.
I understand that you play the banjo. How long have you been playing, and what do you enjoy about it?
You cannot sit down and play the banjo and have your mind on much else. It’s a wonderful moving meditation. Before my medical career, I was a schoolteacher in Vermont. There was a guy on the staff there who played banjo. He came from a small town in Georgia. I just picked it up and started plunking. It’s a happy instrument. It’s awfully hard to make the banjo sound melancholy.
What novel use of lasers and light in dermatology are you most excited about in the next 5 years?
The marriage of therapeutic devices with diagnostic and imaging devices has not happened yet. They are not even in the honeymoon moment. But I think that having truly smart robotic systems in our hands for treating patients will become a reality. These days, dermatologists have to buy a certain type of laser to treat a certain type of lesion. For example, the Q-switched alexandrite laser you buy for treating Nevus of Ota won’t do anything for a port-wine stain; it’s the wrong pulse duration. This means that clinicians who practice a lot of laser dermatology end up with a dozen lasers in their practice. In the future, I think it will be possible to have a software laser, so when you want to acquire another target, you load an App as opposed to buying a new laser. This means that you would have software programmable targeting, and you would not have the requirement of having selective absorption. So, I’m excited by the idea of guided fractional lasers. None of them exist now. We have to start from scratch.
Dr. Anderson, director of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston, conceived and developed many of the nonscarring laser treatments now widely used in dermatology. These include selective photothermolysis for birthmarks, microvascular and pigmented lesions, and tattoo and permanent hair removal. He also contributed to laser lithotripsy, laser angioplasty, photodynamic therapy, and optical diagnostics. The highest-resolution imaging device approved for human use, an infrared confocal microscope, came from his laboratory. Dr. Anderson has also contributed to basic knowledge of human photobiology, drug photosensitization mechanisms, tissue optics and laser-tissue interactions. In this Q&A with Doug Brunk, he reflects on his achievements and on the future of lasers in dermatology.
In published interviews you have described yourself as more of a problem solver than an inventor. How did your upbringing foster your affinity for problem solving?
I grew up in Central Illinois during the 1950s and early 1960s, an area known for corn, soybeans, and hogs. At an early age I learned to be interested in other things because it’s possible to die of boredom there. By the time I was 12 years old, I was an amateur radio operator, and I was building rockets to see how high they would go.
Problem solving comes naturally to me. I enjoy very much finding a problem that is worth solving, which means getting passionate about it and brainstorming. Half the time you don’t come up with a potential route to solve the problem. I attended the Massachusetts Institute of Technology at the age of 17, which was a real eye-opener. I had never been east of the Wabash River prior to that. I studied physics for a while, then decided to flip into biology. That combination has served me well. My special sauce is to have some intuitive and academic rigorous feeling for physical processes. But we physicians have a front row seat to nature’s human drama. There is no lack of problems to solve. I can sit around and obsess about things theoretically, but at the end of the day I want to work on things that ultimately benefit people.
What inspired you most early in your career as a physician scientist?
After I made a commitment to medicine, Dr. John A. Parrish, and Dr. Thomas B. Fitzpatrick were key mentors to me. I was 30 years old when I started medical school, but they took me under their wing even before that. I took a part-time, temporary job with them, which turned into a permanent job. That turned into a love for the work they did. Instead of going into a graduate program in a laboratory and studying bacteria and genetics, the whole idea of working with people and on people was awesome. Dr. Parrish really mentored me. I won a lifetime achievement award from the American Academy of Dermatology a few years ago. I found myself on stage and it rolled out of my mouth that John Parrish believed in me before I believed in myself. It’s really true. He somehow recognized that I had some talents. I was very young and a combination of naive and humble, I guess.
What was the initial genesis for your idea of selective photothermolysis?
I was interested in going to medical school and working with Dr. Fitzpatrick and Dr. Parrish on things related to light. They were mostly interested in PUVA and UVB; it was the heyday of modern phototherapy. I attended a lecture at the Beth Israel Hospital in Boston given by a plastic surgeon, Dr. Joel Mark Noe. He was talking about using lasers to treat port-wine stains in children. The gist of the talk was that argon lasers were being used, and that the results were sometimes decent, but not great. Often children would have burn scars after the treatment. Dr. Noe was talking about how you had to choose the color of the wavelength of the laser to be absorbed by hemoglobin, but he wasn’t talking about what happens to the heat once it’s created. My background in physics led me to recognize that he wasn’t capturing the full picture. Selective disruption of a target in the skin by light is half of the story. The confinement of heat in the target is the other half of the story. Literally on a bus on the way home from that lecture to my apartment in Cambridge, I hatched the idea for selective photothermolysis and wrote down some equations. I also wrote down the ideal wavelength region, how much energy was needed, and what the pulse duration would have to be like to damage target vessels that small. I showed John Parrish what I had written. He took me seriously and said, “Let’s see if we can find a light source that can accomplish this.” We traveled around the country looking at various lasers, but we wound up building the first pulsed dye laser for treating port-wine stains. To me, the surprise was that we didn’t kill the skin. If you treat an area of skin with a laser and hurt all the blood vessels, you think, “Wait a minute. Are we going to kill the skin because it has no blood supply?” The questions of the day were so basic, and we just got lucky. It took 6-8 years before we ramped up the clinical studies showing efficacy and safety of this technology.
I presume that you experimented on your own skin while developing some of the nonscarring laser treatments now widely used in dermatology. What “war story” stands out to you most from that part of your work?
I’m right handed, so I’d grab a laser with my right hand and treat my left arm, so that arm sports a bit of history. In 1994, while working with Dr. Melanie Grossman on the development of laser hair removal, I used a ruby laser to self-treat a patch of hair on my left arm. I still have the world’s oldest laser-induced bald spot on that arm. It’s been 26 years now. I still look at it and count the hairs, because one of the big questions is, is laser hair removal permanent? In all these years I have grown two hairs.
What technology that you conceived of or developed has most surprised you, in term of its ultimate clinical impact?
I would say confocal microscopy. In the mid-1990s I worked with a physicist named Robert H. Webb, who invented an imaging system for the retina. We got together, noodled about it, and decided we would modify his ophthalmoscope system to see if we could get images from inside the skin. It worked pretty well. It was truly surprising from many points of view. First, it wasn’t clear at all that we’d get any images this way. Now, reflectance confocal microscopy is a standard tool in both clinical and research dermatology. But there were odd discoveries early on. For example, the darker your skin, the brighter it appeared in the microscope. You might think that melanin absorbs light and that you would get poor images in dark skin. It was the exact opposite; melanin acts as a natural contrast agent.
We worked with a small company to make the first confocal microscope. Initially, it had no clinical applications but what was fascinating to me was the incredible value of being able to see inside human skin harmlessly, and just see what’s going on. It became a potent research tool, and recently CPT codes were established for its use in evaluating skin cancer margins. I wouldn’t be surprised if 30 years from now, taking a skin biopsy is seemingly barbaric. A forerunner of all these new imaging tools for the skin was the confocal microscope developed in my lab in 1994.
During a 2011 TED talk, you said that nevus of Ota is your favorite thing to treat, because the outcome is usually perfect skin. Are there other technologies or devices you played a role in developing that make you proud at this stage in your career?
The reason I love treating nevus of Ota is that you have a lifelong facial disfigurement, and the only treatment for it is a laser we came up with, and it always works. How perfect could it be? The flip side of the same coin is, there are lesions of the skin that just don’t respond. One of the things we don’t know enough about is the connection between the biologic aspects of repair of various lesions and the treatments that we come up with. The most recent example of selective photothermolysis is a new laser we’re building right now for acne that is based on sebaceous gland injury. You’ll see this coming out in the next year or two. My heart goes out to people with nodular cystic acne. For young men it’s highly associated with suicide. So, I’m excited about optimizing and learning what happens when we target sebaceous glands.
One of the other big stories in laser dermatology is the fractional laser. I developed this with Dr. Dieter Manstein when he was a postdoc in my lab. One of the most pleasing things from this technology is how well you can rehabilitate scars, particularly burn scars in children. Over the last few years, I have trained plastic surgeons at the Shriners Hospital for Children in Boston on how to use fractional lasers to improve the lives of these kids. Another technology I developed with Dr. Manstein is cryolipolysis, which is removing fat from the body by cooling it. There are no lasers involved with this technology. I like to say that I’ve spent most of my career studying light and heat, and now we’ve come up with something that’s cold in the dark. We are now working on derivatives of cryolipolysis, to determine if what we’ve learned about targeting fat that might be applicable elsewhere.
Who inspires you most in your work today?
In addition to Dr. John Parrish and Dr. Thomas Fitzpatrick, the late Dr. Albert M. Kligman also influenced me. He never accepted dogma and he loved to ask questions, like, “What if?” as opposed to just accumulating a fund of knowledge. Understanding things is not just based on how much you know. It’s based on critical thinking and the ability to question. I also admire Albert Einstein, his ability to sit down with nothing more than pencil and paper and change our view of the universe. I love physics because it’s the science of everything. I also love poetry. My favorite poet is Stanley Kunitz. He had amazing insight and was named United States Poet Laureate in 1974 and in 2000. I have plenty of antiheroes as well, mostly politicians.
I understand that you play the banjo. How long have you been playing, and what do you enjoy about it?
You cannot sit down and play the banjo and have your mind on much else. It’s a wonderful moving meditation. Before my medical career, I was a schoolteacher in Vermont. There was a guy on the staff there who played banjo. He came from a small town in Georgia. I just picked it up and started plunking. It’s a happy instrument. It’s awfully hard to make the banjo sound melancholy.
What novel use of lasers and light in dermatology are you most excited about in the next 5 years?
The marriage of therapeutic devices with diagnostic and imaging devices has not happened yet. They are not even in the honeymoon moment. But I think that having truly smart robotic systems in our hands for treating patients will become a reality. These days, dermatologists have to buy a certain type of laser to treat a certain type of lesion. For example, the Q-switched alexandrite laser you buy for treating Nevus of Ota won’t do anything for a port-wine stain; it’s the wrong pulse duration. This means that clinicians who practice a lot of laser dermatology end up with a dozen lasers in their practice. In the future, I think it will be possible to have a software laser, so when you want to acquire another target, you load an App as opposed to buying a new laser. This means that you would have software programmable targeting, and you would not have the requirement of having selective absorption. So, I’m excited by the idea of guided fractional lasers. None of them exist now. We have to start from scratch.
Visionary reflects on the importance of teamwork in advancing technology
When John A. Parrish, MD, worked with R. Rox Anderson, MD, and a team of clinicians and scientists in the early 1980s to develop the first pulsed dye laser for dermatologic use, it became clear that the Food and Drug Administration required convincing that their prototype would be safe.

“Laser medicine was new, and lasers had some specific frightening risks like blindness and bleeding from laser suturing,” recalled Dr. Parrish, founder of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “The main issue was eye risk. Because the operator and the patient were at risk for eye injury, the FDA was reluctant to press on with laser treatments of skin.”
To make the FDA more comfortable with their efforts, Dr. Parrish and his colleagues drew from the published work of ophthalmologists, who were ahead of dermatologists in the clinical use of lasers. “A lot of the animal experiments and the human understanding of laser-tissue interactions came from ophthalmologists,” he said. “We worked with a fellow named David H. Sliney, PhD. He was very interested in laser safety of the eye, so we worked closely with him to measure the boundary conditions that could be used without injuring the eye.”
To Dr. Parrish, forging that partnership illustrated a key principle in developing novel diagnostics and therapeutics that use lasers and light: You need a multidisciplinary team. “You need a pathologist, clinicians, physicists, technologists, and engineers, because all of the barriers to figure out how to deliver a new treatment safely often don’t rest in one person’s mind, so early on we had to be very collaborative and find experts who would help us solve problems,” he said. “That’s how the Wellman Labs got started. All of the new treatments were explored by multidisciplinary teams so that we didn’t have to hope that the expertise to get past all the barriers was in one person’s mind. That was often not the case.”
Dr. Parrish credits his mentor, the late Thomas B. Fitzpatrick, MD, PhD, who in 1975 devised the Fitzpatrick scale of skin phototypes, with inspiring his career path. Dr. Fitzpatrick, who is widely considered the father of modern academic dermatology, was professor and chief of dermatology at Harvard Medical School when Dr. Parrish began his dermatology training there. “He was a great clinician who loved patient care and he was a very curious investigator,” said Dr. Parrish, who cofounded the Consortia for Improving Medicine with Innovation and Technology (CIMIT). “He not only trained me, but I became his collaborator during my early faculty time. What I learned most from him was the joy of work, curiosity, and serious commitment to patient care. It was almost contagious.”

Of all the devices he’s played a role in developing in the past 50 years, Dr. Parrish said that he remains most surprised by the impact of pulsed lasers in dermatology. “It took us a while to understand the capabilities of pulsed lasers in that they could confine injury to small spots and treat multiple areas at once,” he said. “A lot of that did not come because we were so wise to think about that, but we did a lot of work in the early days with a free-electron laser, a pulsed laser which had a tunable wavelength and a tunable pulse duration. That gave us the capability of looking at very specific injuries and the host responses that heal without scarring.”
Dr. Parrish’s interest in dermatology was piqued in 1968, when he was assigned to Oak Knoll Naval Hospital in Oakland, Calif., after a year of serving in the U.S. Marine Corps as a battlefield doctor in Vietnam. (He wrote about his wartime experience in two books, most recently “Autopsy of War: A Personal History” [New York: Thomas Dunne Books, 2012].) Prior to serving in Vietnam he had completed early internal medicine training, but once at Oak Knoll he discovered that he had a propensity for diagnosing and treating disorders of the skin. “When I came back to resume my residency, I asked if I could train in dermatology,” he said. “It was by happenstance. I felt like I could understand skin disease and that I could make a difference. In internal medicine you often change blood pressure medicines around. I felt like I was a better diagnostician than in internal medicine and that I could most often make a difference. I liked seeing all ages of patients, and most of them got better, so it was more fun.”
When John A. Parrish, MD, worked with R. Rox Anderson, MD, and a team of clinicians and scientists in the early 1980s to develop the first pulsed dye laser for dermatologic use, it became clear that the Food and Drug Administration required convincing that their prototype would be safe.
“Laser medicine was new, and lasers had some specific frightening risks like blindness and bleeding from laser suturing,” recalled Dr. Parrish, founder of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “The main issue was eye risk. Because the operator and the patient were at risk for eye injury, the FDA was reluctant to press on with laser treatments of skin.”
To make the FDA more comfortable with their efforts, Dr. Parrish and his colleagues drew from the published work of ophthalmologists, who were ahead of dermatologists in the clinical use of lasers. “A lot of the animal experiments and the human understanding of laser-tissue interactions came from ophthalmologists,” he said. “We worked with a fellow named David H. Sliney, PhD. He was very interested in laser safety of the eye, so we worked closely with him to measure the boundary conditions that could be used without injuring the eye.”
To Dr. Parrish, forging that partnership illustrated a key principle in developing novel diagnostics and therapeutics that use lasers and light: You need a multidisciplinary team. “You need a pathologist, clinicians, physicists, technologists, and engineers, because all of the barriers to figure out how to deliver a new treatment safely often don’t rest in one person’s mind, so early on we had to be very collaborative and find experts who would help us solve problems,” he said. “That’s how the Wellman Labs got started. All of the new treatments were explored by multidisciplinary teams so that we didn’t have to hope that the expertise to get past all the barriers was in one person’s mind. That was often not the case.”
Dr. Parrish credits his mentor, the late Thomas B. Fitzpatrick, MD, PhD, who in 1975 devised the Fitzpatrick scale of skin phototypes, with inspiring his career path. Dr. Fitzpatrick, who is widely considered the father of modern academic dermatology, was professor and chief of dermatology at Harvard Medical School when Dr. Parrish began his dermatology training there. “He was a great clinician who loved patient care and he was a very curious investigator,” said Dr. Parrish, who cofounded the Consortia for Improving Medicine with Innovation and Technology (CIMIT). “He not only trained me, but I became his collaborator during my early faculty time. What I learned most from him was the joy of work, curiosity, and serious commitment to patient care. It was almost contagious.”
Of all the devices he’s played a role in developing in the past 50 years, Dr. Parrish said that he remains most surprised by the impact of pulsed lasers in dermatology. “It took us a while to understand the capabilities of pulsed lasers in that they could confine injury to small spots and treat multiple areas at once,” he said. “A lot of that did not come because we were so wise to think about that, but we did a lot of work in the early days with a free-electron laser, a pulsed laser which had a tunable wavelength and a tunable pulse duration. That gave us the capability of looking at very specific injuries and the host responses that heal without scarring.”
Dr. Parrish’s interest in dermatology was piqued in 1968, when he was assigned to Oak Knoll Naval Hospital in Oakland, Calif., after a year of serving in the U.S. Marine Corps as a battlefield doctor in Vietnam. (He wrote about his wartime experience in two books, most recently “Autopsy of War: A Personal History” [New York: Thomas Dunne Books, 2012].) Prior to serving in Vietnam he had completed early internal medicine training, but once at Oak Knoll he discovered that he had a propensity for diagnosing and treating disorders of the skin. “When I came back to resume my residency, I asked if I could train in dermatology,” he said. “It was by happenstance. I felt like I could understand skin disease and that I could make a difference. In internal medicine you often change blood pressure medicines around. I felt like I was a better diagnostician than in internal medicine and that I could most often make a difference. I liked seeing all ages of patients, and most of them got better, so it was more fun.”
When John A. Parrish, MD, worked with R. Rox Anderson, MD, and a team of clinicians and scientists in the early 1980s to develop the first pulsed dye laser for dermatologic use, it became clear that the Food and Drug Administration required convincing that their prototype would be safe.
“Laser medicine was new, and lasers had some specific frightening risks like blindness and bleeding from laser suturing,” recalled Dr. Parrish, founder of the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “The main issue was eye risk. Because the operator and the patient were at risk for eye injury, the FDA was reluctant to press on with laser treatments of skin.”
To make the FDA more comfortable with their efforts, Dr. Parrish and his colleagues drew from the published work of ophthalmologists, who were ahead of dermatologists in the clinical use of lasers. “A lot of the animal experiments and the human understanding of laser-tissue interactions came from ophthalmologists,” he said. “We worked with a fellow named David H. Sliney, PhD. He was very interested in laser safety of the eye, so we worked closely with him to measure the boundary conditions that could be used without injuring the eye.”
To Dr. Parrish, forging that partnership illustrated a key principle in developing novel diagnostics and therapeutics that use lasers and light: You need a multidisciplinary team. “You need a pathologist, clinicians, physicists, technologists, and engineers, because all of the barriers to figure out how to deliver a new treatment safely often don’t rest in one person’s mind, so early on we had to be very collaborative and find experts who would help us solve problems,” he said. “That’s how the Wellman Labs got started. All of the new treatments were explored by multidisciplinary teams so that we didn’t have to hope that the expertise to get past all the barriers was in one person’s mind. That was often not the case.”
Dr. Parrish credits his mentor, the late Thomas B. Fitzpatrick, MD, PhD, who in 1975 devised the Fitzpatrick scale of skin phototypes, with inspiring his career path. Dr. Fitzpatrick, who is widely considered the father of modern academic dermatology, was professor and chief of dermatology at Harvard Medical School when Dr. Parrish began his dermatology training there. “He was a great clinician who loved patient care and he was a very curious investigator,” said Dr. Parrish, who cofounded the Consortia for Improving Medicine with Innovation and Technology (CIMIT). “He not only trained me, but I became his collaborator during my early faculty time. What I learned most from him was the joy of work, curiosity, and serious commitment to patient care. It was almost contagious.”
Of all the devices he’s played a role in developing in the past 50 years, Dr. Parrish said that he remains most surprised by the impact of pulsed lasers in dermatology. “It took us a while to understand the capabilities of pulsed lasers in that they could confine injury to small spots and treat multiple areas at once,” he said. “A lot of that did not come because we were so wise to think about that, but we did a lot of work in the early days with a free-electron laser, a pulsed laser which had a tunable wavelength and a tunable pulse duration. That gave us the capability of looking at very specific injuries and the host responses that heal without scarring.”
Dr. Parrish’s interest in dermatology was piqued in 1968, when he was assigned to Oak Knoll Naval Hospital in Oakland, Calif., after a year of serving in the U.S. Marine Corps as a battlefield doctor in Vietnam. (He wrote about his wartime experience in two books, most recently “Autopsy of War: A Personal History” [New York: Thomas Dunne Books, 2012].) Prior to serving in Vietnam he had completed early internal medicine training, but once at Oak Knoll he discovered that he had a propensity for diagnosing and treating disorders of the skin. “When I came back to resume my residency, I asked if I could train in dermatology,” he said. “It was by happenstance. I felt like I could understand skin disease and that I could make a difference. In internal medicine you often change blood pressure medicines around. I felt like I was a better diagnostician than in internal medicine and that I could most often make a difference. I liked seeing all ages of patients, and most of them got better, so it was more fun.”