User login
New resilience center targets traumatized health care workers
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.

“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.

But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.

“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.

“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
What to keep in mind as 2021 begins
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice

Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice
Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
As 2020 comes to a close, most of us are looking forward to a (hopefully) brighter 2021. This year has been full of challenges and new experiences, but we have learned a lot. Pandemic or not, there are some things that you and your practice can do to ensure that you are prepared to make 2021 a success.
Tips for your practice
Assess staff morale: It seems simple but checking in with your staff can go a long way. Everyone is dealing with challenges both in and out of the workplace. Check in, show them you care, and think of ways that you can make their work a positive experience in the new year. During our May 2020 GI division chief townhall, John Inadomi, MD, gave a great presentation on the importance of staff morale during the pandemic.
Listen to colleagues: Find out about their experiences, challenges, and solutions. In October, the American Gastroenterological Association held a town hall with some great information and resources called “Adapting to Changing Practice Paradigms.” The agenda covered topics from telehealth to private equity and planning for the next potential wave of COVID-19.
Celebrate the wins: It can often feel like not much went right in 2020, but we did accomplish significant wins for GIs, including achieving payment parity for telephone evaluation and management (E/M) visits with video visits, increases in digestive disease and GI cancer research funding, and inclusion/expansion of GI cancers research opportunities. We couldn’t have done it without you, though, and we will continue to need your help to move important issues forward in 2021. Get involved today! Visit “Get Involved” under Advocacy and Policy on www.gastro.org.
Prepare for E/M changes: The Current Procedural Terminology (CPT) E/M for new and established patient office/outpatient codes (99201-99205, 99211-99215), guidelines, and Medicare payments will undergo major changes beginning Jan. 1, 2021. See the AGA’s coding and reimbursement experts’ article from the March 2020 issue of GI & Hepatology News, “Prepare for major changes to E/M coding starting in 2021,” to learn about the changes and get resources to help practices prepare.
Keep up with new Medicare payment rules: The release of the 2021 physician payments and rules for the Medicare program was delayed this year because of the COVID-19 public health emergency. We were dismayed to learn that Medicare did not make any changes that substantively mitigated the expected cuts to most specialties. Instead of a 5% cut for GI, the Centers for Medicare & Medicaid Services now projects GI will experience a 4% payment cut for 2021. AGA is calling on Congress to pass legislation to stop the cuts. This situation is evolving quickly. Watch for AGA member alerts for breaking news and resources, including the AGA’s “Medicare plans significant payment cuts for 2021.”
Stay current on telehealth and telephone E/M coverage: The commercial payer community came together to cover telehealth (video visits) and telephone E/M at the beginning of the COVID-19 pandemic but have since regularly teased the end of coverage only to extend it just before it expires. It’s impossible to predict what each payer will do, but you can use the following resources to keep current on most payers’ policies and correct coding/reporting for telehealth and telephone E/M:
- “Current State Laws & Reimbursement Policies ” from the Center for Connected Health.
- “Coding for Telehealth & Virtual Visits During COVID-19” from the AGA University.
Check to see if you can report on additional quality measures: AGA has expanded the Merit-Based Incentive Payment System (MIPS) measure portfolio by assuming ownership and stewardship of two hepatitis C virus (HCV) measures from PCPI, including annually checking for HCV in active injection drug users (measure 387) and performing a one-time screening for HCV among patients at risk (measure 400). As a result, gastroenterologists can now report on even more GI-specific measures. There have been the following two changes to GI-specific measures in 2021:
- Measure 275: “Inflammatory Bowel Disease (IBD): Assessment of Hepatitis B Virus (HBV) Status Before Initiating Anti-TNF (Tumor Necrosis Factor) Therapy” now includes coding to allow reporting for all age groups, including pediatric populations.
- Measure 439: “Age Appropriate Screening Colonoscopy” now includes all colonoscopies for patients 50 years and older; however, there’s an exclusion for those patients between the ages of 50 and 85 years.
These changes will help more gastroenterologists qualify for these measures.
Dates and deadlines to remember
January 2021
- Jan. 1 – MIPS Performance Year 2021 begins.
- Jan. 4 – Submission window opens for MIPS Performance Year 2020.
- Changes to Improvement Activity category go into effect (if approved in final rule).
March 2021
- March 31 – First snapshot for Qualifying Participant (QP) determinations and MIPS APM participation.
April 2021
- April 1 – Registration begins for CMS web interface and Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey.
June 2021
- June 30 – Second snapshot for QP determinations and MIPS APM participation.
- June 30 – Registration ends for CMS web interface and CAHPS for MIPS survey.
July 2021
- CMS publishes proposed reimbursement values for 2022 in the Medicare Physician Fee Schedule proposed rule.
- CMS “Targeted Review” opens once CMS makes your MIPS payment adjustment available.
- July 1 - MIPS Performance Feedback Available. CMS will provide you with performance feedback based on the data you submitted for Performance Year 2020. You can use this feedback to improve your care and optimize the payments you receive from CMS in the future.
August 2021
- Aug. 31 - Targeted Review period closes (appeals process).
September 2021
- AMA releases CPT 2022 book, including a new CPT code for Peroral Endoscopic Myotomy (POEM).
October 2021
- Oct. 3 - Last day to start a 90-day performance period for promoting Interoperability and Improvement Activities.
November 2021
- CMS finalizes reimbursement values for 2022 in the MPFS final rule. New payment rates take effect Jan. 1, 2022.
December 2021
- Dec. 31 – Quality Payment Program Exception Applications window closes.
- Dec. 31 – MIPS Performance year 2020 ends.
- Dec. 31 – Fourth snapshot for full TIN APMs (Medicare Shared Savings Program).
G. Anton Decker, MD, is chair of the AGA Practice Management and Economics Committee, Mayo Clinic International; Dawn Francis, MD, is chair-elect of the AGA Practice Management and Economics Committee, Mayo Clinic, Jacksonville, Fla.
They have no conflicts of interest.
CMS finalizes 2021 physician pay rule with E/M changes
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests. While gastroenterology is estimated to experience a 4% cut, other fields are expecting cuts up to 10%.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule takes effect on Jan. 1, 2021, within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%). The changes also would lead to an expected 4% decrease for gastroenterology. The GI societies are among the groups pressing Congress to intercede.
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’s planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Dr. Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Dr. Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on Jan. 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020. AGA has been advocating for passage of this bill before the end of the 116th Congress and urges GIs to contact their lawmakers to prevent these cuts to specialty care. While the GI societies are in support of the bill, they have expressed concerns regarding the financial cliff H.R. 8702 would create. With the payment cuts pushed to 2023, this financial cliff would require physicians to return to Congress to prevent future cuts once the 2-year delay is up.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a Nov. 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last-minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
Based on reporting from Medscape.com.
‘She’s not a real doctor, she’s a psych doctor’
During a particularly hectic day, Janeni Nayagan, MD, a first-year resident in the department of psychiatry and behavioral health at Cooper University Hospital, Camden, N.J., was taken aback – but not surprised – by a patient’s comment.

In the middle of an emergent situation, she overheard a patient say that Dr. Nayagan wasn’t a “real doctor, she’s a psych doctor.”
“When it happened, I wasn’t particularly angry. It was something I knew I would hear eventually because I’d heard of others experiencing it,” Dr. Nayagan said in an interview. “Psychiatry is one of the fields of medicine that is often questioned in terms of legitimacy, and I knew that when I applied for psych residency,” she said.
Nevertheless, she wrote a post about the incident on Twitter, and she discovered she was far from alone. She posted her original tweet at the start of a night shift and was surprised by the number of responses when she opened her account the next day.
So far, Dr. Nayagan’s initial tweet has garnered 86 replies, 960 likes, and 35 retweets. Some clinicians reported similar experiences from both patients and colleagues, and others offered advice on how to handle such slights.
“There were a lot from people within mental health, but I also received responses from pathologists, radiologists, and others. I didn’t realize how much this experience pervaded through medicine, where a certain specialty would be told: You’re not a real doctor. So it was nice having that support,” Dr. Nayagan said.
Dr. Nayagan noted that psychiatrists encounter “specialty bias” to a greater extent than other medical professionals, and it can be a deterrent for medical students when considering psychiatry as a career path.
“It is something that has been around for a while, but it’s surprising that it’s still prevalent in 2020,” Dr. Nayagan said.
‘Busting the myth’
This type of bias is real, agreed Kaz Nelson, MD, associate professor of psychiatry and behavioral sciences and vice chair for education at the University of Minnesota, Minneapolis, and former director of the psychiatry residency program at the school for 8 years.

She said there is “discrimination” toward psychiatrists, but noted that the problem is improving.
“I think we’re better now than 2 years or 5 years or 10 years ago, so we’re heading in the right direction. But ,” Dr. Nelson said in an interview.
“Psychiatrists have the same robust biomedical training as all specialties. They completed medical school and have this additional specialty and in some cases subspecialty training that is comprehensive of biology, psychology, and social components. We call that using a biopsychosocial model,” she said.
However, she noted that, when talking with students about the field of psychiatry, there’s an awareness “that perhaps we aren’t wearing a white coat” or a stethoscope around the neck.
“That gets translated as, You are giving up medicine – you got this medical training, and you’re not using it. And I have to bust that myth and convey that it really is a privilege to be able to integrate these aspects of knowledge and expertise. It’s in no way giving up medicine – we’re practicing medicine every single day,” said Dr. Nelson.
Remnants of stigma remain
Tristan Gorrindo, MD, deputy medical director and chief of the division of education at the American Psychiatric Association, noted “remnants of stigma” still occur.
“In my mind, it’s really a misunderstanding of the relationship between mental health and physical health,” Dr. Gorrindo said in an interview.
“There’s still this notion that holds over from an old belief that the mind and the body are separate. However, the contemporary thinking in most of modern medicine is that mental illness and physical illness are really one and the same, and they influence each other in a very dynamic way all the time,” he said.
“Psychiatrists stand in both worlds. They’re really the bridge to both the psychiatric and physical aspects,” he added.
Dr. Gorrindo agreed with Dr. Nelson that this understanding has become more prevalent during past few decades.
“Within society, it’s become much more acceptable for people to talk about their mental illness and seek treatment. In a way, shedding daylight on this issue has allowed psychiatry to step forward and demonstrate its value,” he said.
“I think over time we’re going to see that stigma or specialty bias become an anachronism that will fall by the wayside as we see psychiatry more broadly integrated and accepted within the entire house of medicine,” said Dr. Gorrindo.
Taking a toll
Although some responders on Twitter advised Dr. Nayagan and other psychiatrists to “educate with a smile” when faced with specialty discrimination, Dr. Nelson noted that it’s important to recognize that experiencing “microaggressions” takes a toll.
“Anytime you’re given a signal that you aren’t really a physician or you’re not doing a real job, whether it’s based on race, gender, ethnicity, or being a psychiatrist, there is a cost. I’d say, know what you’re doing and hold your head up high, but recognize that there’s a cost for which you may need community and support from colleagues,” she said.
“Together, our culture is changing, and the future is bright. But it’s a little bit of an oversimplification to say, ‘Just brush it off.’ We must recognize that there’s a burden that comes from those forms of exclusion,” Dr. Nelson concluded.
A version of this article first appeared on Medscape.com.
During a particularly hectic day, Janeni Nayagan, MD, a first-year resident in the department of psychiatry and behavioral health at Cooper University Hospital, Camden, N.J., was taken aback – but not surprised – by a patient’s comment.
In the middle of an emergent situation, she overheard a patient say that Dr. Nayagan wasn’t a “real doctor, she’s a psych doctor.”
“When it happened, I wasn’t particularly angry. It was something I knew I would hear eventually because I’d heard of others experiencing it,” Dr. Nayagan said in an interview. “Psychiatry is one of the fields of medicine that is often questioned in terms of legitimacy, and I knew that when I applied for psych residency,” she said.
Nevertheless, she wrote a post about the incident on Twitter, and she discovered she was far from alone. She posted her original tweet at the start of a night shift and was surprised by the number of responses when she opened her account the next day.
So far, Dr. Nayagan’s initial tweet has garnered 86 replies, 960 likes, and 35 retweets. Some clinicians reported similar experiences from both patients and colleagues, and others offered advice on how to handle such slights.
“There were a lot from people within mental health, but I also received responses from pathologists, radiologists, and others. I didn’t realize how much this experience pervaded through medicine, where a certain specialty would be told: You’re not a real doctor. So it was nice having that support,” Dr. Nayagan said.
Dr. Nayagan noted that psychiatrists encounter “specialty bias” to a greater extent than other medical professionals, and it can be a deterrent for medical students when considering psychiatry as a career path.
“It is something that has been around for a while, but it’s surprising that it’s still prevalent in 2020,” Dr. Nayagan said.
‘Busting the myth’
This type of bias is real, agreed Kaz Nelson, MD, associate professor of psychiatry and behavioral sciences and vice chair for education at the University of Minnesota, Minneapolis, and former director of the psychiatry residency program at the school for 8 years.
She said there is “discrimination” toward psychiatrists, but noted that the problem is improving.
“I think we’re better now than 2 years or 5 years or 10 years ago, so we’re heading in the right direction. But ,” Dr. Nelson said in an interview.
“Psychiatrists have the same robust biomedical training as all specialties. They completed medical school and have this additional specialty and in some cases subspecialty training that is comprehensive of biology, psychology, and social components. We call that using a biopsychosocial model,” she said.
However, she noted that, when talking with students about the field of psychiatry, there’s an awareness “that perhaps we aren’t wearing a white coat” or a stethoscope around the neck.
“That gets translated as, You are giving up medicine – you got this medical training, and you’re not using it. And I have to bust that myth and convey that it really is a privilege to be able to integrate these aspects of knowledge and expertise. It’s in no way giving up medicine – we’re practicing medicine every single day,” said Dr. Nelson.
Remnants of stigma remain
Tristan Gorrindo, MD, deputy medical director and chief of the division of education at the American Psychiatric Association, noted “remnants of stigma” still occur.
“In my mind, it’s really a misunderstanding of the relationship between mental health and physical health,” Dr. Gorrindo said in an interview.
“There’s still this notion that holds over from an old belief that the mind and the body are separate. However, the contemporary thinking in most of modern medicine is that mental illness and physical illness are really one and the same, and they influence each other in a very dynamic way all the time,” he said.
“Psychiatrists stand in both worlds. They’re really the bridge to both the psychiatric and physical aspects,” he added.
Dr. Gorrindo agreed with Dr. Nelson that this understanding has become more prevalent during past few decades.
“Within society, it’s become much more acceptable for people to talk about their mental illness and seek treatment. In a way, shedding daylight on this issue has allowed psychiatry to step forward and demonstrate its value,” he said.
“I think over time we’re going to see that stigma or specialty bias become an anachronism that will fall by the wayside as we see psychiatry more broadly integrated and accepted within the entire house of medicine,” said Dr. Gorrindo.
Taking a toll
Although some responders on Twitter advised Dr. Nayagan and other psychiatrists to “educate with a smile” when faced with specialty discrimination, Dr. Nelson noted that it’s important to recognize that experiencing “microaggressions” takes a toll.
“Anytime you’re given a signal that you aren’t really a physician or you’re not doing a real job, whether it’s based on race, gender, ethnicity, or being a psychiatrist, there is a cost. I’d say, know what you’re doing and hold your head up high, but recognize that there’s a cost for which you may need community and support from colleagues,” she said.
“Together, our culture is changing, and the future is bright. But it’s a little bit of an oversimplification to say, ‘Just brush it off.’ We must recognize that there’s a burden that comes from those forms of exclusion,” Dr. Nelson concluded.
A version of this article first appeared on Medscape.com.
During a particularly hectic day, Janeni Nayagan, MD, a first-year resident in the department of psychiatry and behavioral health at Cooper University Hospital, Camden, N.J., was taken aback – but not surprised – by a patient’s comment.
In the middle of an emergent situation, she overheard a patient say that Dr. Nayagan wasn’t a “real doctor, she’s a psych doctor.”
“When it happened, I wasn’t particularly angry. It was something I knew I would hear eventually because I’d heard of others experiencing it,” Dr. Nayagan said in an interview. “Psychiatry is one of the fields of medicine that is often questioned in terms of legitimacy, and I knew that when I applied for psych residency,” she said.
Nevertheless, she wrote a post about the incident on Twitter, and she discovered she was far from alone. She posted her original tweet at the start of a night shift and was surprised by the number of responses when she opened her account the next day.
So far, Dr. Nayagan’s initial tweet has garnered 86 replies, 960 likes, and 35 retweets. Some clinicians reported similar experiences from both patients and colleagues, and others offered advice on how to handle such slights.
“There were a lot from people within mental health, but I also received responses from pathologists, radiologists, and others. I didn’t realize how much this experience pervaded through medicine, where a certain specialty would be told: You’re not a real doctor. So it was nice having that support,” Dr. Nayagan said.
Dr. Nayagan noted that psychiatrists encounter “specialty bias” to a greater extent than other medical professionals, and it can be a deterrent for medical students when considering psychiatry as a career path.
“It is something that has been around for a while, but it’s surprising that it’s still prevalent in 2020,” Dr. Nayagan said.
‘Busting the myth’
This type of bias is real, agreed Kaz Nelson, MD, associate professor of psychiatry and behavioral sciences and vice chair for education at the University of Minnesota, Minneapolis, and former director of the psychiatry residency program at the school for 8 years.
She said there is “discrimination” toward psychiatrists, but noted that the problem is improving.
“I think we’re better now than 2 years or 5 years or 10 years ago, so we’re heading in the right direction. But ,” Dr. Nelson said in an interview.
“Psychiatrists have the same robust biomedical training as all specialties. They completed medical school and have this additional specialty and in some cases subspecialty training that is comprehensive of biology, psychology, and social components. We call that using a biopsychosocial model,” she said.
However, she noted that, when talking with students about the field of psychiatry, there’s an awareness “that perhaps we aren’t wearing a white coat” or a stethoscope around the neck.
“That gets translated as, You are giving up medicine – you got this medical training, and you’re not using it. And I have to bust that myth and convey that it really is a privilege to be able to integrate these aspects of knowledge and expertise. It’s in no way giving up medicine – we’re practicing medicine every single day,” said Dr. Nelson.
Remnants of stigma remain
Tristan Gorrindo, MD, deputy medical director and chief of the division of education at the American Psychiatric Association, noted “remnants of stigma” still occur.
“In my mind, it’s really a misunderstanding of the relationship between mental health and physical health,” Dr. Gorrindo said in an interview.
“There’s still this notion that holds over from an old belief that the mind and the body are separate. However, the contemporary thinking in most of modern medicine is that mental illness and physical illness are really one and the same, and they influence each other in a very dynamic way all the time,” he said.
“Psychiatrists stand in both worlds. They’re really the bridge to both the psychiatric and physical aspects,” he added.
Dr. Gorrindo agreed with Dr. Nelson that this understanding has become more prevalent during past few decades.
“Within society, it’s become much more acceptable for people to talk about their mental illness and seek treatment. In a way, shedding daylight on this issue has allowed psychiatry to step forward and demonstrate its value,” he said.
“I think over time we’re going to see that stigma or specialty bias become an anachronism that will fall by the wayside as we see psychiatry more broadly integrated and accepted within the entire house of medicine,” said Dr. Gorrindo.
Taking a toll
Although some responders on Twitter advised Dr. Nayagan and other psychiatrists to “educate with a smile” when faced with specialty discrimination, Dr. Nelson noted that it’s important to recognize that experiencing “microaggressions” takes a toll.
“Anytime you’re given a signal that you aren’t really a physician or you’re not doing a real job, whether it’s based on race, gender, ethnicity, or being a psychiatrist, there is a cost. I’d say, know what you’re doing and hold your head up high, but recognize that there’s a cost for which you may need community and support from colleagues,” she said.
“Together, our culture is changing, and the future is bright. But it’s a little bit of an oversimplification to say, ‘Just brush it off.’ We must recognize that there’s a burden that comes from those forms of exclusion,” Dr. Nelson concluded.
A version of this article first appeared on Medscape.com.
Pregnant women should be offered COVID-19 vaccine, experts agree
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.

Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.
Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
according to guidance from the Centers for Disease Control and Prevention, the American College of Obstetricians and Gynecologists, and the Society for Maternal-Fetal Medicine.
Pregnant women who opt not to receive the vaccine should be supported in that decision as well, a practice advisory from ACOG recommends.
“Pregnant women who experience fever following vaccination should be counseled to take acetaminophen,” the advisory notes.
In addition, women do not need to avoid pregnancy after receiving the Pfizer-BioNTech COVID-19 vaccine, according to the CDC’s interim clinical considerations for its use. The U.S. Food and Drug Administration issued an emergency use authorization for the vaccine on Dec. 11.
Although investigators excluded pregnant women from clinical trials, experts believe that mRNA vaccines, which are not live vaccines, “are unlikely to pose a risk for people who are pregnant” and “are not thought to be a risk to the breastfeeding infant,” the CDC notes.
Meanwhile, women who are pregnant may be at greater risk of severe COVID-19, even though the absolute risk of severe illness is low. COVID-19 also may increase the risk of adverse pregnancy outcomes, such as preterm birth, although the data have been mixed with some studies finding an association and others not.
“If pregnant people are part of a group that is recommended to receive a COVID-19 vaccine (e.g., health care personnel), they may choose to be vaccinated,” the CDC advises. “A conversation between the patient and their clinical team may assist with decisions regarding the use of vaccines approved under EUA for the prevention of COVID-19. While a conversation with a health care provider may be helpful, it is not required prior to vaccination.”
Acknowledging side effects and uncertainty
ACOG’s advisory reiterates that approach. The group notes that, based on the mRNA vaccine’s mechanism of action and its safety and efficacy in clinical trials, “it is expected that the safety and efficacy profile of the vaccine for pregnant individuals would be similar to that observed in nonpregnant individuals ... That said, there are no safety data specific to mRNA vaccine use in pregnant or lactating individuals and the potential risks to a pregnant individual and the fetus are unknown.”
In clinical trials, most participants experienced mild influenza-like symptoms following vaccination, including injection site reactions, fatigue, chills, muscle and joint pain, and headache. Among participants aged 18-55 years, fever greater than 38°C occurred in 3.7% of participants after the first dose and in 15.8% after the second dose. Most symptoms resolved within a few days.
Women who are pregnant should treat fever with acetaminophen because “fever has been associated with adverse pregnancy outcomes,” according to the ACOG guidance. “Acetaminophen has been proven to be safe for use in pregnancy and does not appear to impact antibody response to COVID-19 vaccines.” Patients may treat other vaccine side effects, such as injection-site soreness with acetaminophen as well.
When counseling patients, clinicians should explain that side effects are a normal part of developing antibodies to protect against COVID-19. “Regardless of their decision,” the group says, “these conversations provide an opportunity to remind patients about the importance of other prevention measures such as hand washing, physical distancing, and wearing a mask.”
More data expected
Data from developmental and reproductive toxicity studies in animals are expected soon, the CDC said. In addition, the manufacturer is following clinical trial participants who became pregnant during the study.
Women who are pregnant and their physicians should weigh factors such as the extent of COVID-19 transmission in the community, the patient’s risk of contracting COVID-19, risks of COVID-19 to the patient and fetus, vaccine efficacy and side effects, and the lack of data about COVID-19 vaccination during pregnancy.
The Society for Maternal-Fetal Medicine recommends that pregnant and lactating women have access to COVID-19 vaccines in general and has advocated for the inclusion of women who are pregnant or lactating in vaccine trials. The society has suggested that health care professionals “counsel their patients that the theoretical risk of fetal harm from mRNA vaccines is very low.” It published resources this week for physicians and patients focused on COVID-19 vaccination and pregnancy.
In a review published online Dec. 10 in the American Journal of Obstetrics & Gynecology MFM, Amanda M. Craig, MD, of Duke University Health System in Durham, N.C., and coauthors note that there “is a theoretical risk for fetal harm from any untested medical intervention and this is no different for COVID-19 vaccines.”
“Pregnant individuals should be given the opportunity, along with their obstetric provider, to weigh the potential risk of severe maternal disease against the unknown risk of fetal exposure, and make an autonomous decision about whether or not to accept vaccine until pregnancy safety data are available,” they write.
A version of this article first appeared on Medscape.com.
Experts offer roadmap for treating CLL during the pandemic
COVID-19 has thrown a wrench in standard treatment protocols for patients with chronic lymphocytic leukemia (CLL). These patients already face a greater risk of dying from infections, and recent research suggests they tend to have risk factors that increase their likelihood of complications and death from COVID-19.
In August, a group of oncologists from the United States and Europe published a literature-informed expert opinion to help their colleagues navigate this new CLL treatment landscape. It offers a roadmap for balancing patients’ therapeutic needs against their risk for viral infection and outlines the safest course of action for patients who test positive for COVID-19.
Mazyar Shadman, MD, MPH, an associate professor in the Clinical Research Division of the Fred Hutchinson Cancer Research Center and the Division of Medical Oncology at the University of Washington School of Medicine, in Seattle, Washington, was contacted for comment to break down what clinicians need to know about treating CLL during the pandemic. This interview has been edited for length and clarity.
Question: What prompted you and colleagues from the United States and Europe to write these recommendations?
Dr. Shadman: When we began the collaboration earlier this year, our colleagues in Italy and the rest of Europe had more experience with COVID-19, so they led the effort. We wanted to help oncologists manage their patients with CLL during the pandemic based on the evidence we had at the time and the unknowns we faced.
What’s an example of how the available evidence informed your recommendations?
At the time, we didn’t know whether patients with CLL were more likely to get COVID-19, compared to the general population, but we did have evidence already that cancer increases patients’ risk of bad outcomes and death from COVID-19. CLL, for example, can increase risk factors for infection, including hypogammaglobulinemia, innate immune dysfunction, and neutropenia, which may be exacerbated by anticancer treatments. Patients’ existing immune suppression might prevent or delay their ability to react to or cope with the virus. And many patients with CLL have other conditions that increase their risk of a severe response to COVID-19, including older age (70% of CLL patients are older than 65 years), hypertension (21%), and diabetes (26%).
These factors informed our recommendations to limit patients’ exposure to COVID-19 by reducing or postponing the number of in-person visits and routine in-hospital follow-ups, especially if they could be substituted with virtual check-ins.
The expert opinion recommendations are divided into three main categories: patients who are newly diagnosed with CLL but have not begun receiving therapy, those already receiving therapy but are free of COVID-19, and those who test positive for COVID-19. Let’s start with the first category. What do the recommendations say about waiting versus proceeding for newly diagnosed patients?
Our priority was balancing the negative impacts of getting COVID-19 with the negative impacts of postponing cancer treatment. We suggested taking each new CLL case on a patient-by-patient basis to determine who needed treatment tomorrow and who could wait a few weeks or months. Fortunately, CLL rarely requires immediate therapy, so the preference was to postpone treatment a few weeks, depending on the local COVID-19 outbreak situation.
In my practice, for instance, we tried to postpone visits as much as we could. Before the pandemic, patients with CLL in the watch-and-wait phase – those diagnosed but who don’t require treatment immediately – would come in for bloodwork and exams every 3-6 months. But when the pandemic hit, we skipped 3-month visits for patients with stable lab results and switched to telehealth visits instead. For those who needed blood draws, we used local labs closer to the patient’s home to minimize their exposure and transportation requirements.
When treatment cannot be deferred, we’ve recommended starting patients on therapies that require fewer in-person visits and are less immune suppressive. We recommended oncologists consider Bruton tyrosine kinase (BTK) inhibitors, such as ibrutinib and acalabrutinib, as well as venetoclax. Some research suggests these inhibitors may be protective against COVID-19 by blunting a patient’s hyperinflammatory response to the virus. These drugs also require minimal routine treatment and lab visits, which helps limit patients’ potential exposure to COVID-19.
But there are risks to waiting. Even during the peak of the pandemic here in Seattle, if patients needed treatment immediately, we did not delay. Patients with significant drops in their platelet or neutrophil count or those with bulky disease, for instance, do require therapy.
It’s important to mention that we did have bad experiences with patients who needed immediate treatment and their treating physicians decided to wait because of COVID-19 risks. These patients who came in with aggressive CLL and experienced delays in care had much more complicated CLL treatment than if they had started treatment earlier.
When organ function became abnormal, for example, some patients could no longer receive certain therapies. If someone’s kidney function becomes abnormal, I wouldn’t recommend giving a drug like venetoclax. Although rare, some patients on venetoclax develop tumor lysis syndrome, which can lead to kidney failure.
Bottom line: Don’t just assume it’s a low-grade disease and that you can wait.
What about patients already receiving treatment for CLL who are free of COVID-19?
For patients on active treatment, we suggested stopping or holding treatment with monoclonal antibodies, such as rituximab and obinutuzumab, and chemotherapy regimens, such as idelalisib plus rituximab and duvelisib, when possible. We recommended oncologists consider continuing treatment for patients on BTK inhibitors.
What happens if a patient with CLL tests positive for COVID-19?
If a patient tests positive for COVID-19 but is not yet on CLL treatment, we recommend postponing CLL care until they’ve recovered from the infection. If a patient is already receiving treatment, the recommendations are similar to those above for COVID-19–negative patients: Delay care for those on chemotherapy and monoclonal antibodies, but consider continuing treatment for patients on BTK inhibitors.
The expert opinion was submitted in May and ultimately published in August. How has our understanding of treating CLL during the pandemic changed since then? Would you change any recommendations?
When we published this paper, it was still early on in the pandemic, and we didn’t know as much about COVID-19 and CLL as we do now. Since we published the recommendations, we have received confirmation from several studies that patients with cancer have a more complicated course of COVID-19 and have worse outcomes. But I believe the recommendations we devised early in the pandemic still hold now. Decisions about delivering treatment should be influenced by the local COVID-19 numbers and hospital resources as well as the patient’s specific situation – whether they have more stable disease and can delay or postpone care or whether they need more immediate attention.
With a further surge in cases predicted as we move even deeper into flu season, what would you recommend for initiating treatment in newly diagnosed patients?
The pandemic has created a very fluid situation for treating CLL. What’s happening now in Seattle may not be the same story in New York, California, or elsewhere. In early November [when Dr. Shadman was first contacted], in Seattle, we were not postponing care because our COVID-19 numbers were fairly good. But, as of mid December, that is starting to change as the COVID-19 numbers fluctuate.
If we do experience a second peak of COVID-19 cases, we would need to modify our practice as we did during the initial surge earlier this year. That would mean avoiding treatment with monoclonal antibodies and chemotherapy, as well as minimizing blood draws and drugs that require frequent in-person visits.
How important is it for patients to be vaccinated against COVID-19?
There are two key things to consider about a vaccine. Is the vaccine safe from the general safety standpoint that everyone is worried about? And if the vaccine is not harmful, will it work in patients will CLL?
Because we don’t yet know the complete side-effect profile of a COVID-19 vaccine, we would need to assess each patient’s condition to limit adverse reactions and to see whether the vaccine alters a patient’s immune response to the CLL drug they’re taking.
At the University of Washington, Seattle, we have a plan to start studying the effectiveness of the Pfizer and Moderna vaccines in patients with CLL – carefully assessing patients’ response to the vaccine in terms of antibody response. We already know, based on small studies, that the antibody response to the flu vaccine, for instance, is not as strong in patients with CLL, compared to those without. But, overall, as long as the vaccine won’t cause harm, I would recommend my patients get it.
Dr. Shadman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 has thrown a wrench in standard treatment protocols for patients with chronic lymphocytic leukemia (CLL). These patients already face a greater risk of dying from infections, and recent research suggests they tend to have risk factors that increase their likelihood of complications and death from COVID-19.
In August, a group of oncologists from the United States and Europe published a literature-informed expert opinion to help their colleagues navigate this new CLL treatment landscape. It offers a roadmap for balancing patients’ therapeutic needs against their risk for viral infection and outlines the safest course of action for patients who test positive for COVID-19.
Mazyar Shadman, MD, MPH, an associate professor in the Clinical Research Division of the Fred Hutchinson Cancer Research Center and the Division of Medical Oncology at the University of Washington School of Medicine, in Seattle, Washington, was contacted for comment to break down what clinicians need to know about treating CLL during the pandemic. This interview has been edited for length and clarity.
Question: What prompted you and colleagues from the United States and Europe to write these recommendations?
Dr. Shadman: When we began the collaboration earlier this year, our colleagues in Italy and the rest of Europe had more experience with COVID-19, so they led the effort. We wanted to help oncologists manage their patients with CLL during the pandemic based on the evidence we had at the time and the unknowns we faced.
What’s an example of how the available evidence informed your recommendations?
At the time, we didn’t know whether patients with CLL were more likely to get COVID-19, compared to the general population, but we did have evidence already that cancer increases patients’ risk of bad outcomes and death from COVID-19. CLL, for example, can increase risk factors for infection, including hypogammaglobulinemia, innate immune dysfunction, and neutropenia, which may be exacerbated by anticancer treatments. Patients’ existing immune suppression might prevent or delay their ability to react to or cope with the virus. And many patients with CLL have other conditions that increase their risk of a severe response to COVID-19, including older age (70% of CLL patients are older than 65 years), hypertension (21%), and diabetes (26%).
These factors informed our recommendations to limit patients’ exposure to COVID-19 by reducing or postponing the number of in-person visits and routine in-hospital follow-ups, especially if they could be substituted with virtual check-ins.
The expert opinion recommendations are divided into three main categories: patients who are newly diagnosed with CLL but have not begun receiving therapy, those already receiving therapy but are free of COVID-19, and those who test positive for COVID-19. Let’s start with the first category. What do the recommendations say about waiting versus proceeding for newly diagnosed patients?
Our priority was balancing the negative impacts of getting COVID-19 with the negative impacts of postponing cancer treatment. We suggested taking each new CLL case on a patient-by-patient basis to determine who needed treatment tomorrow and who could wait a few weeks or months. Fortunately, CLL rarely requires immediate therapy, so the preference was to postpone treatment a few weeks, depending on the local COVID-19 outbreak situation.
In my practice, for instance, we tried to postpone visits as much as we could. Before the pandemic, patients with CLL in the watch-and-wait phase – those diagnosed but who don’t require treatment immediately – would come in for bloodwork and exams every 3-6 months. But when the pandemic hit, we skipped 3-month visits for patients with stable lab results and switched to telehealth visits instead. For those who needed blood draws, we used local labs closer to the patient’s home to minimize their exposure and transportation requirements.
When treatment cannot be deferred, we’ve recommended starting patients on therapies that require fewer in-person visits and are less immune suppressive. We recommended oncologists consider Bruton tyrosine kinase (BTK) inhibitors, such as ibrutinib and acalabrutinib, as well as venetoclax. Some research suggests these inhibitors may be protective against COVID-19 by blunting a patient’s hyperinflammatory response to the virus. These drugs also require minimal routine treatment and lab visits, which helps limit patients’ potential exposure to COVID-19.
But there are risks to waiting. Even during the peak of the pandemic here in Seattle, if patients needed treatment immediately, we did not delay. Patients with significant drops in their platelet or neutrophil count or those with bulky disease, for instance, do require therapy.
It’s important to mention that we did have bad experiences with patients who needed immediate treatment and their treating physicians decided to wait because of COVID-19 risks. These patients who came in with aggressive CLL and experienced delays in care had much more complicated CLL treatment than if they had started treatment earlier.
When organ function became abnormal, for example, some patients could no longer receive certain therapies. If someone’s kidney function becomes abnormal, I wouldn’t recommend giving a drug like venetoclax. Although rare, some patients on venetoclax develop tumor lysis syndrome, which can lead to kidney failure.
Bottom line: Don’t just assume it’s a low-grade disease and that you can wait.
What about patients already receiving treatment for CLL who are free of COVID-19?
For patients on active treatment, we suggested stopping or holding treatment with monoclonal antibodies, such as rituximab and obinutuzumab, and chemotherapy regimens, such as idelalisib plus rituximab and duvelisib, when possible. We recommended oncologists consider continuing treatment for patients on BTK inhibitors.
What happens if a patient with CLL tests positive for COVID-19?
If a patient tests positive for COVID-19 but is not yet on CLL treatment, we recommend postponing CLL care until they’ve recovered from the infection. If a patient is already receiving treatment, the recommendations are similar to those above for COVID-19–negative patients: Delay care for those on chemotherapy and monoclonal antibodies, but consider continuing treatment for patients on BTK inhibitors.
The expert opinion was submitted in May and ultimately published in August. How has our understanding of treating CLL during the pandemic changed since then? Would you change any recommendations?
When we published this paper, it was still early on in the pandemic, and we didn’t know as much about COVID-19 and CLL as we do now. Since we published the recommendations, we have received confirmation from several studies that patients with cancer have a more complicated course of COVID-19 and have worse outcomes. But I believe the recommendations we devised early in the pandemic still hold now. Decisions about delivering treatment should be influenced by the local COVID-19 numbers and hospital resources as well as the patient’s specific situation – whether they have more stable disease and can delay or postpone care or whether they need more immediate attention.
With a further surge in cases predicted as we move even deeper into flu season, what would you recommend for initiating treatment in newly diagnosed patients?
The pandemic has created a very fluid situation for treating CLL. What’s happening now in Seattle may not be the same story in New York, California, or elsewhere. In early November [when Dr. Shadman was first contacted], in Seattle, we were not postponing care because our COVID-19 numbers were fairly good. But, as of mid December, that is starting to change as the COVID-19 numbers fluctuate.
If we do experience a second peak of COVID-19 cases, we would need to modify our practice as we did during the initial surge earlier this year. That would mean avoiding treatment with monoclonal antibodies and chemotherapy, as well as minimizing blood draws and drugs that require frequent in-person visits.
How important is it for patients to be vaccinated against COVID-19?
There are two key things to consider about a vaccine. Is the vaccine safe from the general safety standpoint that everyone is worried about? And if the vaccine is not harmful, will it work in patients will CLL?
Because we don’t yet know the complete side-effect profile of a COVID-19 vaccine, we would need to assess each patient’s condition to limit adverse reactions and to see whether the vaccine alters a patient’s immune response to the CLL drug they’re taking.
At the University of Washington, Seattle, we have a plan to start studying the effectiveness of the Pfizer and Moderna vaccines in patients with CLL – carefully assessing patients’ response to the vaccine in terms of antibody response. We already know, based on small studies, that the antibody response to the flu vaccine, for instance, is not as strong in patients with CLL, compared to those without. But, overall, as long as the vaccine won’t cause harm, I would recommend my patients get it.
Dr. Shadman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 has thrown a wrench in standard treatment protocols for patients with chronic lymphocytic leukemia (CLL). These patients already face a greater risk of dying from infections, and recent research suggests they tend to have risk factors that increase their likelihood of complications and death from COVID-19.
In August, a group of oncologists from the United States and Europe published a literature-informed expert opinion to help their colleagues navigate this new CLL treatment landscape. It offers a roadmap for balancing patients’ therapeutic needs against their risk for viral infection and outlines the safest course of action for patients who test positive for COVID-19.
Mazyar Shadman, MD, MPH, an associate professor in the Clinical Research Division of the Fred Hutchinson Cancer Research Center and the Division of Medical Oncology at the University of Washington School of Medicine, in Seattle, Washington, was contacted for comment to break down what clinicians need to know about treating CLL during the pandemic. This interview has been edited for length and clarity.
Question: What prompted you and colleagues from the United States and Europe to write these recommendations?
Dr. Shadman: When we began the collaboration earlier this year, our colleagues in Italy and the rest of Europe had more experience with COVID-19, so they led the effort. We wanted to help oncologists manage their patients with CLL during the pandemic based on the evidence we had at the time and the unknowns we faced.
What’s an example of how the available evidence informed your recommendations?
At the time, we didn’t know whether patients with CLL were more likely to get COVID-19, compared to the general population, but we did have evidence already that cancer increases patients’ risk of bad outcomes and death from COVID-19. CLL, for example, can increase risk factors for infection, including hypogammaglobulinemia, innate immune dysfunction, and neutropenia, which may be exacerbated by anticancer treatments. Patients’ existing immune suppression might prevent or delay their ability to react to or cope with the virus. And many patients with CLL have other conditions that increase their risk of a severe response to COVID-19, including older age (70% of CLL patients are older than 65 years), hypertension (21%), and diabetes (26%).
These factors informed our recommendations to limit patients’ exposure to COVID-19 by reducing or postponing the number of in-person visits and routine in-hospital follow-ups, especially if they could be substituted with virtual check-ins.
The expert opinion recommendations are divided into three main categories: patients who are newly diagnosed with CLL but have not begun receiving therapy, those already receiving therapy but are free of COVID-19, and those who test positive for COVID-19. Let’s start with the first category. What do the recommendations say about waiting versus proceeding for newly diagnosed patients?
Our priority was balancing the negative impacts of getting COVID-19 with the negative impacts of postponing cancer treatment. We suggested taking each new CLL case on a patient-by-patient basis to determine who needed treatment tomorrow and who could wait a few weeks or months. Fortunately, CLL rarely requires immediate therapy, so the preference was to postpone treatment a few weeks, depending on the local COVID-19 outbreak situation.
In my practice, for instance, we tried to postpone visits as much as we could. Before the pandemic, patients with CLL in the watch-and-wait phase – those diagnosed but who don’t require treatment immediately – would come in for bloodwork and exams every 3-6 months. But when the pandemic hit, we skipped 3-month visits for patients with stable lab results and switched to telehealth visits instead. For those who needed blood draws, we used local labs closer to the patient’s home to minimize their exposure and transportation requirements.
When treatment cannot be deferred, we’ve recommended starting patients on therapies that require fewer in-person visits and are less immune suppressive. We recommended oncologists consider Bruton tyrosine kinase (BTK) inhibitors, such as ibrutinib and acalabrutinib, as well as venetoclax. Some research suggests these inhibitors may be protective against COVID-19 by blunting a patient’s hyperinflammatory response to the virus. These drugs also require minimal routine treatment and lab visits, which helps limit patients’ potential exposure to COVID-19.
But there are risks to waiting. Even during the peak of the pandemic here in Seattle, if patients needed treatment immediately, we did not delay. Patients with significant drops in their platelet or neutrophil count or those with bulky disease, for instance, do require therapy.
It’s important to mention that we did have bad experiences with patients who needed immediate treatment and their treating physicians decided to wait because of COVID-19 risks. These patients who came in with aggressive CLL and experienced delays in care had much more complicated CLL treatment than if they had started treatment earlier.
When organ function became abnormal, for example, some patients could no longer receive certain therapies. If someone’s kidney function becomes abnormal, I wouldn’t recommend giving a drug like venetoclax. Although rare, some patients on venetoclax develop tumor lysis syndrome, which can lead to kidney failure.
Bottom line: Don’t just assume it’s a low-grade disease and that you can wait.
What about patients already receiving treatment for CLL who are free of COVID-19?
For patients on active treatment, we suggested stopping or holding treatment with monoclonal antibodies, such as rituximab and obinutuzumab, and chemotherapy regimens, such as idelalisib plus rituximab and duvelisib, when possible. We recommended oncologists consider continuing treatment for patients on BTK inhibitors.
What happens if a patient with CLL tests positive for COVID-19?
If a patient tests positive for COVID-19 but is not yet on CLL treatment, we recommend postponing CLL care until they’ve recovered from the infection. If a patient is already receiving treatment, the recommendations are similar to those above for COVID-19–negative patients: Delay care for those on chemotherapy and monoclonal antibodies, but consider continuing treatment for patients on BTK inhibitors.
The expert opinion was submitted in May and ultimately published in August. How has our understanding of treating CLL during the pandemic changed since then? Would you change any recommendations?
When we published this paper, it was still early on in the pandemic, and we didn’t know as much about COVID-19 and CLL as we do now. Since we published the recommendations, we have received confirmation from several studies that patients with cancer have a more complicated course of COVID-19 and have worse outcomes. But I believe the recommendations we devised early in the pandemic still hold now. Decisions about delivering treatment should be influenced by the local COVID-19 numbers and hospital resources as well as the patient’s specific situation – whether they have more stable disease and can delay or postpone care or whether they need more immediate attention.
With a further surge in cases predicted as we move even deeper into flu season, what would you recommend for initiating treatment in newly diagnosed patients?
The pandemic has created a very fluid situation for treating CLL. What’s happening now in Seattle may not be the same story in New York, California, or elsewhere. In early November [when Dr. Shadman was first contacted], in Seattle, we were not postponing care because our COVID-19 numbers were fairly good. But, as of mid December, that is starting to change as the COVID-19 numbers fluctuate.
If we do experience a second peak of COVID-19 cases, we would need to modify our practice as we did during the initial surge earlier this year. That would mean avoiding treatment with monoclonal antibodies and chemotherapy, as well as minimizing blood draws and drugs that require frequent in-person visits.
How important is it for patients to be vaccinated against COVID-19?
There are two key things to consider about a vaccine. Is the vaccine safe from the general safety standpoint that everyone is worried about? And if the vaccine is not harmful, will it work in patients will CLL?
Because we don’t yet know the complete side-effect profile of a COVID-19 vaccine, we would need to assess each patient’s condition to limit adverse reactions and to see whether the vaccine alters a patient’s immune response to the CLL drug they’re taking.
At the University of Washington, Seattle, we have a plan to start studying the effectiveness of the Pfizer and Moderna vaccines in patients with CLL – carefully assessing patients’ response to the vaccine in terms of antibody response. We already know, based on small studies, that the antibody response to the flu vaccine, for instance, is not as strong in patients with CLL, compared to those without. But, overall, as long as the vaccine won’t cause harm, I would recommend my patients get it.
Dr. Shadman has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Call to arms: vaccinating the health workforce of 21 million strong
As the first American health care workers rolled up their sleeves for a COVID-19 vaccine, the images were instantly frozen in history, marking the triumph of scientific know-how and ingenuity. Cameras captured the first trucks pulling out of a warehouse in Portage, Mich., to the applause of workers and area residents. A day later, Boston Medical Center employees – some dressed in scrubs and wearing masks, face shields, and protective gowns – literally danced on the sidewalk when doses arrived. Some have photographed themselves getting the vaccine and posted it on social media, tagging it #MyCOVIDVax.
But the real story of the debut of COVID-19 vaccination is more methodical than monumental, a celebration of teamwork rather than of conquest. As hospitals waited for their first allotment, they reviewed their carefully drafted plans. They relied on each other, reaching across the usual divisions of competition and working collaboratively to share the limited supply. Their priority lists for the first vaccinations included environmental services workers who clean patient rooms and the critical care physicians who work to save lives.
“Health care workers have pulled together throughout this pandemic,” said Melanie Swift, MD, cochair of the COVID-19 Vaccine Allocation and Distribution Work Group at Mayo Clinic in Rochester, Minn. “We’ve gone through the darkest of years relying so heavily on each other,” she said. “Now we’re pulling together to get out of it.”
Still, a rollout of this magnitude has hitches. Stanford issued an apology Dec. 18 after its medical residents protested a vaccine distribution plan that left out nearly all of its residents and fellows, many of whom regularly treat patients with COVID-19.
There have already been more than 287,000 COVID-19 cases and 953 deaths among health care workers, according to the Centers for Disease Control and Prevention. In its guidance, the agency pointed out that the “continued protection of them at work, at home, and in the community remains a national priority.” That means vaccinating a workforce of about 21 million people, often the largest group of employees in a community.
“It collectively takes all of us to vaccinate our teams to maintain that stability in our health care infrastructure across the metro Atlanta area,” Christy Norman, PharmD, vice president of pharmacy services at Emory Healthcare, told reporters in a briefing as the health system awaited its first delivery.
Don’t waste a dose
One overriding imperative prevails: Hospitals don’t want to waste any doses. The storage requirements of the Pfizer vaccine make that tricky.
Once vials are removed from the pizza-box-shaped containers in ultracold storage and placed in a refrigerator, they must be used within 5 days. Thawed five-dose vials must be brought to room temperature before they are diluted, and they can remain at room temperature for no more than 2 hours. Once they are diluted with 1.8 mL of a 0.9% sodium chloride injection, the vials must be used within 6 hours.
COVID-19 precautions require employees to stay physically distant while they wait their turn for vaccination, which means the process can’t mirror typical large-scale flu immunization programs.
To prioritize groups, the vaccination planners at Mayo conducted a thorough risk stratification, considering each employee’s duties. Do they work in a dedicated COVID-19 unit? Do they handle lab tests or collect swabs? Do they work in the ICU or emergency department?
“We have applied some principles to make sure that as we roll it out, we prioritize people who are at greatest risk of ongoing exposure and who are really critical to maintaining the COVID response and other essential health services,” said Dr. Swift, associate medical director of Mayo’s occupational health service.
Mayo employees who are eligible for the first doses can sign up for appointments through the medical record system. If it seems likely that some doses will be left over at the end of the vaccination period – perhaps because of missed appointments – supervisors in high-risk areas can refer other health care workers. Mayo gave its first vaccines on Dec. 18, but the vaccination program began in earnest the following week. With the pleasant surprise that each five-dose vial actually provides six doses, 474 vials will allow for the vaccination of 2,844 employees in the top-priority group. “It’s going to expand each week or few days as we get more and more vaccine,” Dr. Swift said.
Sharing vials with small rural hospitals
Minnesota is using a hub-and-spoke system to give small rural hospitals access to the Pfizer vaccine, even though they lack ultracold storage and can’t use a minimum order of 975 doses. Large hospitals, acting as hubs, are sharing their orders. (The minimum order for Moderna is 100 doses.)
In south-central Minnesota, for example, two hub hospitals each have six spoke hospitals. Five of the 14 hospitals are independent, and the rest are part of large hospital systems, but affiliation doesn’t matter, said Eric Weller, regional health care preparedness coordinator for the South Central Healthcare Coalition. “We are all working together. It doesn’t matter what system you’re from,” he said. “We’re working for the good of the community.”
Each hospital designed a process to provide vaccine education, prioritize groups, allocate appointments, register people for vaccination, obtain signed consent forms, administer vaccines in a COVID-safe way, and provide follow-up appointments for the second dose. “We’re using some of the lessons we learned during H1N1,” said Mr. Weller, referring to immunization during the 2009 influenza pandemic. “The difference is that during H1N1, you could have lines of people.”
Coordinating the appointments will be more important than ever. “One of the vaccination strategies is to get people in groups of five, so you use one vial on those five people and don’t waste it,” he said.
Logistics are somewhat different for the Moderna vaccine, which will come in 10-dose vials that can be refrigerated for up to 30 days.
Both vaccines may produce mild flulike symptoms, such as fatigue, headache, or muscle pain, particularly after the second dose. That’s a sign that the immune system is reacting to the vaccine, but it’s also another consideration in the vaccination plans, because health care workers might take a day or two off work. “We’re not going to vaccinate a whole department at one time. It will be staggered,” said Kevin Smith, MD, medical director of the occupational medicine program at ProMedica, a health care system based in Toledo, Ohio.
Dr. Smith said he plans to encourage employees to use V-Safe, an app created by the CDC to track adverse effects in people who receive the vaccine. He pointed out that a day or two of achiness will be better than coping with the symptoms of COVID-19. Some employees who recovered from the infection still feel fatigued or haven’t regained their sense of taste and smell. “We are still monitoring quite a few employees to make sure they get back to 100%,” he said.
Hope for ending the pandemic
Public health officials have worried about vaccine hesitancy, even among health care workers, but so far, that concern seems overshadowed by enthusiasm. Dr. Smith said his department has been fielding calls from employees who want to know when they will be able to get the vaccine. “I think everyone feels relief,” he said. “We’re at the beginning of the end.”
At Mayo, Dr. Swift is surveying staff to gauge the willingness to get the vaccine, but she already senses excitement among employees. “No doubt there are still people who are hesitant, but I’m feeling a shift,” she said. “I’m feeling this momentum building of health care workers coming on board and wanting to take this vaccine, which is good, because they will set an example for their patients.”
For Colleen Kelley, MD, an infectious disease physician at Emory University in Atlanta who was principal investigator for an Emory-affiliated Moderna clinical trial site, it has been an emotional time. “Things were looking very bleak and dark for a time, and then we started to get these efficacy results that were greater than anyone imagined,” she said.
Dr. Kelley spends time talking to journalists and educating physician colleagues and hospital employees about how the vaccine was developed so quickly and how it works. “Everyone asks me, ‘Should I get it? Are you going to get it?’ My answer is ‘yes’ and ‘yes,’ “ she said. “I am 1,000% confident that the benefits of widespread vaccination outweigh the risks of continued COVID and a continued pandemic.”
A version of this article first appeared on Medscape.com.
As the first American health care workers rolled up their sleeves for a COVID-19 vaccine, the images were instantly frozen in history, marking the triumph of scientific know-how and ingenuity. Cameras captured the first trucks pulling out of a warehouse in Portage, Mich., to the applause of workers and area residents. A day later, Boston Medical Center employees – some dressed in scrubs and wearing masks, face shields, and protective gowns – literally danced on the sidewalk when doses arrived. Some have photographed themselves getting the vaccine and posted it on social media, tagging it #MyCOVIDVax.
But the real story of the debut of COVID-19 vaccination is more methodical than monumental, a celebration of teamwork rather than of conquest. As hospitals waited for their first allotment, they reviewed their carefully drafted plans. They relied on each other, reaching across the usual divisions of competition and working collaboratively to share the limited supply. Their priority lists for the first vaccinations included environmental services workers who clean patient rooms and the critical care physicians who work to save lives.
“Health care workers have pulled together throughout this pandemic,” said Melanie Swift, MD, cochair of the COVID-19 Vaccine Allocation and Distribution Work Group at Mayo Clinic in Rochester, Minn. “We’ve gone through the darkest of years relying so heavily on each other,” she said. “Now we’re pulling together to get out of it.”
Still, a rollout of this magnitude has hitches. Stanford issued an apology Dec. 18 after its medical residents protested a vaccine distribution plan that left out nearly all of its residents and fellows, many of whom regularly treat patients with COVID-19.
There have already been more than 287,000 COVID-19 cases and 953 deaths among health care workers, according to the Centers for Disease Control and Prevention. In its guidance, the agency pointed out that the “continued protection of them at work, at home, and in the community remains a national priority.” That means vaccinating a workforce of about 21 million people, often the largest group of employees in a community.
“It collectively takes all of us to vaccinate our teams to maintain that stability in our health care infrastructure across the metro Atlanta area,” Christy Norman, PharmD, vice president of pharmacy services at Emory Healthcare, told reporters in a briefing as the health system awaited its first delivery.
Don’t waste a dose
One overriding imperative prevails: Hospitals don’t want to waste any doses. The storage requirements of the Pfizer vaccine make that tricky.
Once vials are removed from the pizza-box-shaped containers in ultracold storage and placed in a refrigerator, they must be used within 5 days. Thawed five-dose vials must be brought to room temperature before they are diluted, and they can remain at room temperature for no more than 2 hours. Once they are diluted with 1.8 mL of a 0.9% sodium chloride injection, the vials must be used within 6 hours.
COVID-19 precautions require employees to stay physically distant while they wait their turn for vaccination, which means the process can’t mirror typical large-scale flu immunization programs.
To prioritize groups, the vaccination planners at Mayo conducted a thorough risk stratification, considering each employee’s duties. Do they work in a dedicated COVID-19 unit? Do they handle lab tests or collect swabs? Do they work in the ICU or emergency department?
“We have applied some principles to make sure that as we roll it out, we prioritize people who are at greatest risk of ongoing exposure and who are really critical to maintaining the COVID response and other essential health services,” said Dr. Swift, associate medical director of Mayo’s occupational health service.
Mayo employees who are eligible for the first doses can sign up for appointments through the medical record system. If it seems likely that some doses will be left over at the end of the vaccination period – perhaps because of missed appointments – supervisors in high-risk areas can refer other health care workers. Mayo gave its first vaccines on Dec. 18, but the vaccination program began in earnest the following week. With the pleasant surprise that each five-dose vial actually provides six doses, 474 vials will allow for the vaccination of 2,844 employees in the top-priority group. “It’s going to expand each week or few days as we get more and more vaccine,” Dr. Swift said.
Sharing vials with small rural hospitals
Minnesota is using a hub-and-spoke system to give small rural hospitals access to the Pfizer vaccine, even though they lack ultracold storage and can’t use a minimum order of 975 doses. Large hospitals, acting as hubs, are sharing their orders. (The minimum order for Moderna is 100 doses.)
In south-central Minnesota, for example, two hub hospitals each have six spoke hospitals. Five of the 14 hospitals are independent, and the rest are part of large hospital systems, but affiliation doesn’t matter, said Eric Weller, regional health care preparedness coordinator for the South Central Healthcare Coalition. “We are all working together. It doesn’t matter what system you’re from,” he said. “We’re working for the good of the community.”
Each hospital designed a process to provide vaccine education, prioritize groups, allocate appointments, register people for vaccination, obtain signed consent forms, administer vaccines in a COVID-safe way, and provide follow-up appointments for the second dose. “We’re using some of the lessons we learned during H1N1,” said Mr. Weller, referring to immunization during the 2009 influenza pandemic. “The difference is that during H1N1, you could have lines of people.”
Coordinating the appointments will be more important than ever. “One of the vaccination strategies is to get people in groups of five, so you use one vial on those five people and don’t waste it,” he said.
Logistics are somewhat different for the Moderna vaccine, which will come in 10-dose vials that can be refrigerated for up to 30 days.
Both vaccines may produce mild flulike symptoms, such as fatigue, headache, or muscle pain, particularly after the second dose. That’s a sign that the immune system is reacting to the vaccine, but it’s also another consideration in the vaccination plans, because health care workers might take a day or two off work. “We’re not going to vaccinate a whole department at one time. It will be staggered,” said Kevin Smith, MD, medical director of the occupational medicine program at ProMedica, a health care system based in Toledo, Ohio.
Dr. Smith said he plans to encourage employees to use V-Safe, an app created by the CDC to track adverse effects in people who receive the vaccine. He pointed out that a day or two of achiness will be better than coping with the symptoms of COVID-19. Some employees who recovered from the infection still feel fatigued or haven’t regained their sense of taste and smell. “We are still monitoring quite a few employees to make sure they get back to 100%,” he said.
Hope for ending the pandemic
Public health officials have worried about vaccine hesitancy, even among health care workers, but so far, that concern seems overshadowed by enthusiasm. Dr. Smith said his department has been fielding calls from employees who want to know when they will be able to get the vaccine. “I think everyone feels relief,” he said. “We’re at the beginning of the end.”
At Mayo, Dr. Swift is surveying staff to gauge the willingness to get the vaccine, but she already senses excitement among employees. “No doubt there are still people who are hesitant, but I’m feeling a shift,” she said. “I’m feeling this momentum building of health care workers coming on board and wanting to take this vaccine, which is good, because they will set an example for their patients.”
For Colleen Kelley, MD, an infectious disease physician at Emory University in Atlanta who was principal investigator for an Emory-affiliated Moderna clinical trial site, it has been an emotional time. “Things were looking very bleak and dark for a time, and then we started to get these efficacy results that were greater than anyone imagined,” she said.
Dr. Kelley spends time talking to journalists and educating physician colleagues and hospital employees about how the vaccine was developed so quickly and how it works. “Everyone asks me, ‘Should I get it? Are you going to get it?’ My answer is ‘yes’ and ‘yes,’ “ she said. “I am 1,000% confident that the benefits of widespread vaccination outweigh the risks of continued COVID and a continued pandemic.”
A version of this article first appeared on Medscape.com.
As the first American health care workers rolled up their sleeves for a COVID-19 vaccine, the images were instantly frozen in history, marking the triumph of scientific know-how and ingenuity. Cameras captured the first trucks pulling out of a warehouse in Portage, Mich., to the applause of workers and area residents. A day later, Boston Medical Center employees – some dressed in scrubs and wearing masks, face shields, and protective gowns – literally danced on the sidewalk when doses arrived. Some have photographed themselves getting the vaccine and posted it on social media, tagging it #MyCOVIDVax.
But the real story of the debut of COVID-19 vaccination is more methodical than monumental, a celebration of teamwork rather than of conquest. As hospitals waited for their first allotment, they reviewed their carefully drafted plans. They relied on each other, reaching across the usual divisions of competition and working collaboratively to share the limited supply. Their priority lists for the first vaccinations included environmental services workers who clean patient rooms and the critical care physicians who work to save lives.
“Health care workers have pulled together throughout this pandemic,” said Melanie Swift, MD, cochair of the COVID-19 Vaccine Allocation and Distribution Work Group at Mayo Clinic in Rochester, Minn. “We’ve gone through the darkest of years relying so heavily on each other,” she said. “Now we’re pulling together to get out of it.”
Still, a rollout of this magnitude has hitches. Stanford issued an apology Dec. 18 after its medical residents protested a vaccine distribution plan that left out nearly all of its residents and fellows, many of whom regularly treat patients with COVID-19.
There have already been more than 287,000 COVID-19 cases and 953 deaths among health care workers, according to the Centers for Disease Control and Prevention. In its guidance, the agency pointed out that the “continued protection of them at work, at home, and in the community remains a national priority.” That means vaccinating a workforce of about 21 million people, often the largest group of employees in a community.
“It collectively takes all of us to vaccinate our teams to maintain that stability in our health care infrastructure across the metro Atlanta area,” Christy Norman, PharmD, vice president of pharmacy services at Emory Healthcare, told reporters in a briefing as the health system awaited its first delivery.
Don’t waste a dose
One overriding imperative prevails: Hospitals don’t want to waste any doses. The storage requirements of the Pfizer vaccine make that tricky.
Once vials are removed from the pizza-box-shaped containers in ultracold storage and placed in a refrigerator, they must be used within 5 days. Thawed five-dose vials must be brought to room temperature before they are diluted, and they can remain at room temperature for no more than 2 hours. Once they are diluted with 1.8 mL of a 0.9% sodium chloride injection, the vials must be used within 6 hours.
COVID-19 precautions require employees to stay physically distant while they wait their turn for vaccination, which means the process can’t mirror typical large-scale flu immunization programs.
To prioritize groups, the vaccination planners at Mayo conducted a thorough risk stratification, considering each employee’s duties. Do they work in a dedicated COVID-19 unit? Do they handle lab tests or collect swabs? Do they work in the ICU or emergency department?
“We have applied some principles to make sure that as we roll it out, we prioritize people who are at greatest risk of ongoing exposure and who are really critical to maintaining the COVID response and other essential health services,” said Dr. Swift, associate medical director of Mayo’s occupational health service.
Mayo employees who are eligible for the first doses can sign up for appointments through the medical record system. If it seems likely that some doses will be left over at the end of the vaccination period – perhaps because of missed appointments – supervisors in high-risk areas can refer other health care workers. Mayo gave its first vaccines on Dec. 18, but the vaccination program began in earnest the following week. With the pleasant surprise that each five-dose vial actually provides six doses, 474 vials will allow for the vaccination of 2,844 employees in the top-priority group. “It’s going to expand each week or few days as we get more and more vaccine,” Dr. Swift said.
Sharing vials with small rural hospitals
Minnesota is using a hub-and-spoke system to give small rural hospitals access to the Pfizer vaccine, even though they lack ultracold storage and can’t use a minimum order of 975 doses. Large hospitals, acting as hubs, are sharing their orders. (The minimum order for Moderna is 100 doses.)
In south-central Minnesota, for example, two hub hospitals each have six spoke hospitals. Five of the 14 hospitals are independent, and the rest are part of large hospital systems, but affiliation doesn’t matter, said Eric Weller, regional health care preparedness coordinator for the South Central Healthcare Coalition. “We are all working together. It doesn’t matter what system you’re from,” he said. “We’re working for the good of the community.”
Each hospital designed a process to provide vaccine education, prioritize groups, allocate appointments, register people for vaccination, obtain signed consent forms, administer vaccines in a COVID-safe way, and provide follow-up appointments for the second dose. “We’re using some of the lessons we learned during H1N1,” said Mr. Weller, referring to immunization during the 2009 influenza pandemic. “The difference is that during H1N1, you could have lines of people.”
Coordinating the appointments will be more important than ever. “One of the vaccination strategies is to get people in groups of five, so you use one vial on those five people and don’t waste it,” he said.
Logistics are somewhat different for the Moderna vaccine, which will come in 10-dose vials that can be refrigerated for up to 30 days.
Both vaccines may produce mild flulike symptoms, such as fatigue, headache, or muscle pain, particularly after the second dose. That’s a sign that the immune system is reacting to the vaccine, but it’s also another consideration in the vaccination plans, because health care workers might take a day or two off work. “We’re not going to vaccinate a whole department at one time. It will be staggered,” said Kevin Smith, MD, medical director of the occupational medicine program at ProMedica, a health care system based in Toledo, Ohio.
Dr. Smith said he plans to encourage employees to use V-Safe, an app created by the CDC to track adverse effects in people who receive the vaccine. He pointed out that a day or two of achiness will be better than coping with the symptoms of COVID-19. Some employees who recovered from the infection still feel fatigued or haven’t regained their sense of taste and smell. “We are still monitoring quite a few employees to make sure they get back to 100%,” he said.
Hope for ending the pandemic
Public health officials have worried about vaccine hesitancy, even among health care workers, but so far, that concern seems overshadowed by enthusiasm. Dr. Smith said his department has been fielding calls from employees who want to know when they will be able to get the vaccine. “I think everyone feels relief,” he said. “We’re at the beginning of the end.”
At Mayo, Dr. Swift is surveying staff to gauge the willingness to get the vaccine, but she already senses excitement among employees. “No doubt there are still people who are hesitant, but I’m feeling a shift,” she said. “I’m feeling this momentum building of health care workers coming on board and wanting to take this vaccine, which is good, because they will set an example for their patients.”
For Colleen Kelley, MD, an infectious disease physician at Emory University in Atlanta who was principal investigator for an Emory-affiliated Moderna clinical trial site, it has been an emotional time. “Things were looking very bleak and dark for a time, and then we started to get these efficacy results that were greater than anyone imagined,” she said.
Dr. Kelley spends time talking to journalists and educating physician colleagues and hospital employees about how the vaccine was developed so quickly and how it works. “Everyone asks me, ‘Should I get it? Are you going to get it?’ My answer is ‘yes’ and ‘yes,’ “ she said. “I am 1,000% confident that the benefits of widespread vaccination outweigh the risks of continued COVID and a continued pandemic.”
A version of this article first appeared on Medscape.com.
COVID-19 anticoagulation trials ‘paused’ for futility, safety
Parts of three linked studies investigating increased levels of anticoagulation in hospitalized COVID-19 patients have been “paused” because of futility and safety concerns, a statement from the U.S. National Heart, Lung, and Blood Institute (NHLBI) confirms.
The trials involved are the REMAP-CAP, ACTIV-4, and ATTACC studies.
The statement also says that a potential for harm in this subgroup could not be excluded, noting that increased bleeding is a known complication of full-dose anticoagulation. The trials are working urgently to undertake additional analyses, which will be made available as soon as possible.
The three clinical trial platforms are working together to test the effects of full therapeutic doses of anticoagulants vs. lower prophylactic doses in COVID-19 patients.
Informed by the deliberations of the data safety monitoring boards of these trials, all of the trial sites have paused enrollment of the most critically ill hospitalized patients with COVID-19.
Enrollment continues in the trials for moderately ill hospitalized COVID-19 patients, the statement notes.
“Whether the use of full-dose compared to low-dose anticoagulants leads to better outcomes in hospitalized patients with less COVID-19 severe disease remains a very important question,” the NHLBI statement says.
Patients who require full dose anticoagulants for another medical indication are not included in these trials.
The statement explains that COVID-19 is associated with significant inflammation and clinical and pathologic evidence of widespread blood clots. These trials were launched because clinicians have observed that many patients ill with COVID-19, including those who have died from the disease, formed blood clots throughout their bodies, even in their smallest blood vessels. This unusual clotting can cause multiple health complications, including lung failure, myocardial infarction, and stroke.
The three trials are the result of a collaboration between major international partners. The trials include: the Randomized, Embedded, Multi-factorial Adaptive Platform Trial for Community-Acquired Pneumonia (REMAP-CAP) Therapeutic Anticoagulation; Accelerating COVID-19 Therapeutic Interventions and Vaccines-4 (ACTIV-4) Antithrombotics Inpatient; and Antithrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC).
The trials, which span four continents, have the common goal of assessing the benefit of full doses of anticoagulants to treat moderately ill or critically ill adults hospitalized for COVID-19, compared with a lower dose often used to prevent blood clots in hospitalized patients.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The trials are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (UK), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this story first appeared on Medscape.com.
Parts of three linked studies investigating increased levels of anticoagulation in hospitalized COVID-19 patients have been “paused” because of futility and safety concerns, a statement from the U.S. National Heart, Lung, and Blood Institute (NHLBI) confirms.
The trials involved are the REMAP-CAP, ACTIV-4, and ATTACC studies.
The statement also says that a potential for harm in this subgroup could not be excluded, noting that increased bleeding is a known complication of full-dose anticoagulation. The trials are working urgently to undertake additional analyses, which will be made available as soon as possible.
The three clinical trial platforms are working together to test the effects of full therapeutic doses of anticoagulants vs. lower prophylactic doses in COVID-19 patients.
Informed by the deliberations of the data safety monitoring boards of these trials, all of the trial sites have paused enrollment of the most critically ill hospitalized patients with COVID-19.
Enrollment continues in the trials for moderately ill hospitalized COVID-19 patients, the statement notes.
“Whether the use of full-dose compared to low-dose anticoagulants leads to better outcomes in hospitalized patients with less COVID-19 severe disease remains a very important question,” the NHLBI statement says.
Patients who require full dose anticoagulants for another medical indication are not included in these trials.
The statement explains that COVID-19 is associated with significant inflammation and clinical and pathologic evidence of widespread blood clots. These trials were launched because clinicians have observed that many patients ill with COVID-19, including those who have died from the disease, formed blood clots throughout their bodies, even in their smallest blood vessels. This unusual clotting can cause multiple health complications, including lung failure, myocardial infarction, and stroke.
The three trials are the result of a collaboration between major international partners. The trials include: the Randomized, Embedded, Multi-factorial Adaptive Platform Trial for Community-Acquired Pneumonia (REMAP-CAP) Therapeutic Anticoagulation; Accelerating COVID-19 Therapeutic Interventions and Vaccines-4 (ACTIV-4) Antithrombotics Inpatient; and Antithrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC).
The trials, which span four continents, have the common goal of assessing the benefit of full doses of anticoagulants to treat moderately ill or critically ill adults hospitalized for COVID-19, compared with a lower dose often used to prevent blood clots in hospitalized patients.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The trials are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (UK), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this story first appeared on Medscape.com.
Parts of three linked studies investigating increased levels of anticoagulation in hospitalized COVID-19 patients have been “paused” because of futility and safety concerns, a statement from the U.S. National Heart, Lung, and Blood Institute (NHLBI) confirms.
The trials involved are the REMAP-CAP, ACTIV-4, and ATTACC studies.
The statement also says that a potential for harm in this subgroup could not be excluded, noting that increased bleeding is a known complication of full-dose anticoagulation. The trials are working urgently to undertake additional analyses, which will be made available as soon as possible.
The three clinical trial platforms are working together to test the effects of full therapeutic doses of anticoagulants vs. lower prophylactic doses in COVID-19 patients.
Informed by the deliberations of the data safety monitoring boards of these trials, all of the trial sites have paused enrollment of the most critically ill hospitalized patients with COVID-19.
Enrollment continues in the trials for moderately ill hospitalized COVID-19 patients, the statement notes.
“Whether the use of full-dose compared to low-dose anticoagulants leads to better outcomes in hospitalized patients with less COVID-19 severe disease remains a very important question,” the NHLBI statement says.
Patients who require full dose anticoagulants for another medical indication are not included in these trials.
The statement explains that COVID-19 is associated with significant inflammation and clinical and pathologic evidence of widespread blood clots. These trials were launched because clinicians have observed that many patients ill with COVID-19, including those who have died from the disease, formed blood clots throughout their bodies, even in their smallest blood vessels. This unusual clotting can cause multiple health complications, including lung failure, myocardial infarction, and stroke.
The three trials are the result of a collaboration between major international partners. The trials include: the Randomized, Embedded, Multi-factorial Adaptive Platform Trial for Community-Acquired Pneumonia (REMAP-CAP) Therapeutic Anticoagulation; Accelerating COVID-19 Therapeutic Interventions and Vaccines-4 (ACTIV-4) Antithrombotics Inpatient; and Antithrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC).
The trials, which span four continents, have the common goal of assessing the benefit of full doses of anticoagulants to treat moderately ill or critically ill adults hospitalized for COVID-19, compared with a lower dose often used to prevent blood clots in hospitalized patients.
In the United States, the ACTIV-4 trial is being led by a collaborative effort involving a number of universities, including the University of Pittsburgh and New York University.
The trials are supported by multiple international funding organizations including the National Institutes of Health, Canadian Institutes of Health Research, the National Institute for Health Research (UK), the National Health and Medical Research Council (Australia), and the PREPARE and RECOVER consortia (European Union).
A version of this story first appeared on Medscape.com.
Latest rise in child COVID-19 cases is relatively small
For the seventh week out of the last eight, more new cases of COVID-19 in children were reported in the United States than any week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
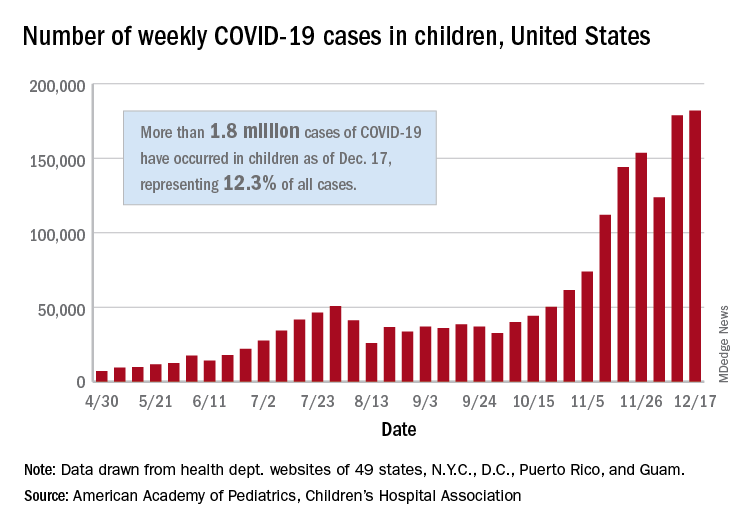
There were just over 182,000 new cases of COVID-19 in children during the week ending Dec. 17, topping the previous high of almost 179,000 set the previous week. – a stretch of 11 weeks that has produced only one decline, based on data from the latest AAP/CHA weekly report.
As of Dec. 17, there had been over 1.8 million cases of COVID-19 in children, which represents 12.3% of all U.S. cases. For the week, 14% of all cases occurred in children, which was up slightly from 13.8% the week before (Dec. 10). The overall rate of coronavirus infection is now 2,420 cases per 100,000 children in the population, the AAP and CHA said.
A total of 30 states are above that national rate, with North Dakota the highest at 7,515 cases per 100,000 children, followed by South Dakota (5,618), Wyoming (5,157), Wisconsin (5,106), and Tennessee (4,994). Wyoming has the highest proportion of cases occurring in children at 20.8%, but that is down from 23.4% in mid-November, based on data collected by the AAP and CHA from the health department websites of 49 states (New York does not provide age distributions), the District of Columbia, New York City, Puerto Rico, and Guam.
In the last 2 weeks, however, the largest percent increases in new cases came in states with low-to-average rates of cumulative child infection. California, Connecticut, Delaware, Maine, Maryland, New Hampshire, and Vermont all saw increases of over 35% from Dec. 3 to Dec. 17, while the smallest increases occurred in Hawaii, North Dakota, and Wyoming, the AAP and CHA reported.
For the seventh week out of the last eight, more new cases of COVID-19 in children were reported in the United States than any week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There were just over 182,000 new cases of COVID-19 in children during the week ending Dec. 17, topping the previous high of almost 179,000 set the previous week. – a stretch of 11 weeks that has produced only one decline, based on data from the latest AAP/CHA weekly report.
As of Dec. 17, there had been over 1.8 million cases of COVID-19 in children, which represents 12.3% of all U.S. cases. For the week, 14% of all cases occurred in children, which was up slightly from 13.8% the week before (Dec. 10). The overall rate of coronavirus infection is now 2,420 cases per 100,000 children in the population, the AAP and CHA said.
A total of 30 states are above that national rate, with North Dakota the highest at 7,515 cases per 100,000 children, followed by South Dakota (5,618), Wyoming (5,157), Wisconsin (5,106), and Tennessee (4,994). Wyoming has the highest proportion of cases occurring in children at 20.8%, but that is down from 23.4% in mid-November, based on data collected by the AAP and CHA from the health department websites of 49 states (New York does not provide age distributions), the District of Columbia, New York City, Puerto Rico, and Guam.
In the last 2 weeks, however, the largest percent increases in new cases came in states with low-to-average rates of cumulative child infection. California, Connecticut, Delaware, Maine, Maryland, New Hampshire, and Vermont all saw increases of over 35% from Dec. 3 to Dec. 17, while the smallest increases occurred in Hawaii, North Dakota, and Wyoming, the AAP and CHA reported.
For the seventh week out of the last eight, more new cases of COVID-19 in children were reported in the United States than any week before, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There were just over 182,000 new cases of COVID-19 in children during the week ending Dec. 17, topping the previous high of almost 179,000 set the previous week. – a stretch of 11 weeks that has produced only one decline, based on data from the latest AAP/CHA weekly report.
As of Dec. 17, there had been over 1.8 million cases of COVID-19 in children, which represents 12.3% of all U.S. cases. For the week, 14% of all cases occurred in children, which was up slightly from 13.8% the week before (Dec. 10). The overall rate of coronavirus infection is now 2,420 cases per 100,000 children in the population, the AAP and CHA said.
A total of 30 states are above that national rate, with North Dakota the highest at 7,515 cases per 100,000 children, followed by South Dakota (5,618), Wyoming (5,157), Wisconsin (5,106), and Tennessee (4,994). Wyoming has the highest proportion of cases occurring in children at 20.8%, but that is down from 23.4% in mid-November, based on data collected by the AAP and CHA from the health department websites of 49 states (New York does not provide age distributions), the District of Columbia, New York City, Puerto Rico, and Guam.
In the last 2 weeks, however, the largest percent increases in new cases came in states with low-to-average rates of cumulative child infection. California, Connecticut, Delaware, Maine, Maryland, New Hampshire, and Vermont all saw increases of over 35% from Dec. 3 to Dec. 17, while the smallest increases occurred in Hawaii, North Dakota, and Wyoming, the AAP and CHA reported.
Strategies for tracking SARS-CoV-2 could help detect next pandemic
Two recently published studies indicate that COVID-19 infections were already circulating in the United States in December 2019. The question is whether these methodologies that could be applied to track the next pandemic.
One study evaluating blood donations found antibodies on the West coast as early as Dec. 13, 2019, and in blood donated on the East Coast by early January 2020 (Clin Infect Dis. 2020; Nov 30. doi: 10.1093/cid/ciaa1785). Both preceded the first documented COVID-19 infection in the United States, which has been widely reported as occurring on Jan. 19, 2020, in a traveler returning from China.
The other study, utilizing electronic medical record (EMR) analytics, demonstrated a spike in visits or hospitalizations for cough, a trend that persisted from Dec. 22, 2019, onward, exceeding norms for seasonal flu ( J Med Internet Res. 2020;22:e21562). This spike was interpreted as evidence that the SARS-CoV-2 pandemic was already underway before the first case was established.
While the ongoing serologic testing of blood donations for viral antibodies “will advance understanding of the epidemiology” for SARS-CoV-2 and “inform allocation of resources and public health prevention interventions to mitigate morbidity and mortality,” it might also be a strategy for disease surveillance in the next pandemic, according to a team led by investigators at the Centers for Disease Control and Prevention.
Blood donation surveillance is not now used routinely to monitor for population-based health threats, but it is not a new idea, according to the lead author of the study, Sridhar V. Basavaraju, MD, of Emory University and director of the CDC’s Office of Blood, Organ, and Other Tissue Safety, Atlanta, and his coinvestigators. Most recently, blood donation surveillance was used in the United States to track the penetration of the Zika virus.
For early detection of respiratory infections, blood donations might have unique advantages over alternatives, such as surveillance of respiratory specimens from symptomatic patients. Not least, blood donation surveillance captures individuals who are not seeking medical care, according to the investigators.
EMR surveillance might also have unique advantages for population-based monitoring of health threats. For one, aggregate data from large EMR systems have the potential to reveal symptom patterns before they become apparent at level of clinical care, according to a team of collaborating investigators from the University of California, Los Angeles, and the University of Washington, Seattle.
Emphasizing an urgent need for “agile healthcare analytics” to enable “disease surveillance in real time,” the first author of the EMR study, Joann G. Elmore, MD, professor in the department of health policy and management at the University of California, Los Angeles, expressed the hope that the approach will “lead to better preparation and the ability to quickly provide warnings and track the next pandemic.”

In the blood donation surveillance study, the goal was simply to determine whether SARS-CoV-2 reactive antibodies could be found in blood donations before the first case was identified. Of the 7,389 archived blood samples tested between Dec. 13, 2019, and Jan. 17, 2020, 106 (1.4%) were reactive.
These were not true positives, acknowledged the investigators. True positives would require reactive antibodies in the context of a positive molecular diagnostic test or paired acute convalescent sera with rising titers. The investigators also cautioned that false positives could not be completely ruled out, particularly in light of cross-reactivity that has been reported with other human coronaviruses.
Nevertheless, the monitoring of blood donations offers substantial promise for “understanding the dynamics of SARS-CoV-2 pandemic from early introduction,” and the CDC is now collaborating on ongoing surveillance with the goal of contributing information that could be applied “to mitigate morbidity and mortality.”
Lessons learned from this pandemic are potentially relevant to the next.
The EMR study simply looked at whether the word “cough” was included more often in the notes from visits or hospitalizations between December 2019 and February 2020 relative to the preceding 5 years. The investigators drew on data from three hospitals and more than 180 clinics.
From Dec. 22, 2019, onward, cough was noted above the 95% prediction interval for all 10 weeks of the study. The excess was seen in the outpatient setting and among hospitalized patients. There was also significant excess in the number of patients hospitalized with acute respiratory failure during the study period.
“Our approach to analyzing electronic records could be helpful in the future as we included consideration of data from the outpatient clinics in addition to the emergency departments and inpatient settings,” Dr. Elmore reported.
Surveillance of influenza and influenza-like infections has been undertaken in the United States for more than 20 years, but Dr. Elmore contends that EMR data, particularly data from outpatient clinics are “usually a harbinger of what is to come” for emergency department visits and, ultimately, hospitalizations. She thinks that this is a resource not yet fully exploited.
“There are always opportunities to better harness EMR data,” Dr. Elmore said.
These are intriguing studies and “useful” for reconsidering when SARS-CoV-2 was introduced in the United States, according to Janet G. Basemen, PhD, a professor of epidemiology and the associate dean of the University of Washington School of Public Health, Seattle. However, she noted that the task of translating data like these into actionable public health strategies has proven difficult in the past.
Symptom-based surveillance systems “have mostly served as situational awareness rather than early detection tools,” Dr. Baseman said. The problem is timely interpretation of a given signal.
Not that she doubts such tools “would be an incredible resource for humanity” if the current limitations can be resolved or that technological advances will lead to better methods of detecting and monitoring pandemics “at some point.” Rather, “we’re just not there yet,” she said.
SOURCE: Basavaraju SV et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1785); Elmore JG et al. J Med Internet Res. 2020;22:e21562).
Two recently published studies indicate that COVID-19 infections were already circulating in the United States in December 2019. The question is whether these methodologies that could be applied to track the next pandemic.
One study evaluating blood donations found antibodies on the West coast as early as Dec. 13, 2019, and in blood donated on the East Coast by early January 2020 (Clin Infect Dis. 2020; Nov 30. doi: 10.1093/cid/ciaa1785). Both preceded the first documented COVID-19 infection in the United States, which has been widely reported as occurring on Jan. 19, 2020, in a traveler returning from China.
The other study, utilizing electronic medical record (EMR) analytics, demonstrated a spike in visits or hospitalizations for cough, a trend that persisted from Dec. 22, 2019, onward, exceeding norms for seasonal flu ( J Med Internet Res. 2020;22:e21562). This spike was interpreted as evidence that the SARS-CoV-2 pandemic was already underway before the first case was established.
While the ongoing serologic testing of blood donations for viral antibodies “will advance understanding of the epidemiology” for SARS-CoV-2 and “inform allocation of resources and public health prevention interventions to mitigate morbidity and mortality,” it might also be a strategy for disease surveillance in the next pandemic, according to a team led by investigators at the Centers for Disease Control and Prevention.
Blood donation surveillance is not now used routinely to monitor for population-based health threats, but it is not a new idea, according to the lead author of the study, Sridhar V. Basavaraju, MD, of Emory University and director of the CDC’s Office of Blood, Organ, and Other Tissue Safety, Atlanta, and his coinvestigators. Most recently, blood donation surveillance was used in the United States to track the penetration of the Zika virus.
For early detection of respiratory infections, blood donations might have unique advantages over alternatives, such as surveillance of respiratory specimens from symptomatic patients. Not least, blood donation surveillance captures individuals who are not seeking medical care, according to the investigators.
EMR surveillance might also have unique advantages for population-based monitoring of health threats. For one, aggregate data from large EMR systems have the potential to reveal symptom patterns before they become apparent at level of clinical care, according to a team of collaborating investigators from the University of California, Los Angeles, and the University of Washington, Seattle.
Emphasizing an urgent need for “agile healthcare analytics” to enable “disease surveillance in real time,” the first author of the EMR study, Joann G. Elmore, MD, professor in the department of health policy and management at the University of California, Los Angeles, expressed the hope that the approach will “lead to better preparation and the ability to quickly provide warnings and track the next pandemic.”
In the blood donation surveillance study, the goal was simply to determine whether SARS-CoV-2 reactive antibodies could be found in blood donations before the first case was identified. Of the 7,389 archived blood samples tested between Dec. 13, 2019, and Jan. 17, 2020, 106 (1.4%) were reactive.
These were not true positives, acknowledged the investigators. True positives would require reactive antibodies in the context of a positive molecular diagnostic test or paired acute convalescent sera with rising titers. The investigators also cautioned that false positives could not be completely ruled out, particularly in light of cross-reactivity that has been reported with other human coronaviruses.
Nevertheless, the monitoring of blood donations offers substantial promise for “understanding the dynamics of SARS-CoV-2 pandemic from early introduction,” and the CDC is now collaborating on ongoing surveillance with the goal of contributing information that could be applied “to mitigate morbidity and mortality.”
Lessons learned from this pandemic are potentially relevant to the next.
The EMR study simply looked at whether the word “cough” was included more often in the notes from visits or hospitalizations between December 2019 and February 2020 relative to the preceding 5 years. The investigators drew on data from three hospitals and more than 180 clinics.
From Dec. 22, 2019, onward, cough was noted above the 95% prediction interval for all 10 weeks of the study. The excess was seen in the outpatient setting and among hospitalized patients. There was also significant excess in the number of patients hospitalized with acute respiratory failure during the study period.
“Our approach to analyzing electronic records could be helpful in the future as we included consideration of data from the outpatient clinics in addition to the emergency departments and inpatient settings,” Dr. Elmore reported.
Surveillance of influenza and influenza-like infections has been undertaken in the United States for more than 20 years, but Dr. Elmore contends that EMR data, particularly data from outpatient clinics are “usually a harbinger of what is to come” for emergency department visits and, ultimately, hospitalizations. She thinks that this is a resource not yet fully exploited.
“There are always opportunities to better harness EMR data,” Dr. Elmore said.
These are intriguing studies and “useful” for reconsidering when SARS-CoV-2 was introduced in the United States, according to Janet G. Basemen, PhD, a professor of epidemiology and the associate dean of the University of Washington School of Public Health, Seattle. However, she noted that the task of translating data like these into actionable public health strategies has proven difficult in the past.
Symptom-based surveillance systems “have mostly served as situational awareness rather than early detection tools,” Dr. Baseman said. The problem is timely interpretation of a given signal.
Not that she doubts such tools “would be an incredible resource for humanity” if the current limitations can be resolved or that technological advances will lead to better methods of detecting and monitoring pandemics “at some point.” Rather, “we’re just not there yet,” she said.
SOURCE: Basavaraju SV et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1785); Elmore JG et al. J Med Internet Res. 2020;22:e21562).
Two recently published studies indicate that COVID-19 infections were already circulating in the United States in December 2019. The question is whether these methodologies that could be applied to track the next pandemic.
One study evaluating blood donations found antibodies on the West coast as early as Dec. 13, 2019, and in blood donated on the East Coast by early January 2020 (Clin Infect Dis. 2020; Nov 30. doi: 10.1093/cid/ciaa1785). Both preceded the first documented COVID-19 infection in the United States, which has been widely reported as occurring on Jan. 19, 2020, in a traveler returning from China.
The other study, utilizing electronic medical record (EMR) analytics, demonstrated a spike in visits or hospitalizations for cough, a trend that persisted from Dec. 22, 2019, onward, exceeding norms for seasonal flu ( J Med Internet Res. 2020;22:e21562). This spike was interpreted as evidence that the SARS-CoV-2 pandemic was already underway before the first case was established.
While the ongoing serologic testing of blood donations for viral antibodies “will advance understanding of the epidemiology” for SARS-CoV-2 and “inform allocation of resources and public health prevention interventions to mitigate morbidity and mortality,” it might also be a strategy for disease surveillance in the next pandemic, according to a team led by investigators at the Centers for Disease Control and Prevention.
Blood donation surveillance is not now used routinely to monitor for population-based health threats, but it is not a new idea, according to the lead author of the study, Sridhar V. Basavaraju, MD, of Emory University and director of the CDC’s Office of Blood, Organ, and Other Tissue Safety, Atlanta, and his coinvestigators. Most recently, blood donation surveillance was used in the United States to track the penetration of the Zika virus.
For early detection of respiratory infections, blood donations might have unique advantages over alternatives, such as surveillance of respiratory specimens from symptomatic patients. Not least, blood donation surveillance captures individuals who are not seeking medical care, according to the investigators.
EMR surveillance might also have unique advantages for population-based monitoring of health threats. For one, aggregate data from large EMR systems have the potential to reveal symptom patterns before they become apparent at level of clinical care, according to a team of collaborating investigators from the University of California, Los Angeles, and the University of Washington, Seattle.
Emphasizing an urgent need for “agile healthcare analytics” to enable “disease surveillance in real time,” the first author of the EMR study, Joann G. Elmore, MD, professor in the department of health policy and management at the University of California, Los Angeles, expressed the hope that the approach will “lead to better preparation and the ability to quickly provide warnings and track the next pandemic.”
In the blood donation surveillance study, the goal was simply to determine whether SARS-CoV-2 reactive antibodies could be found in blood donations before the first case was identified. Of the 7,389 archived blood samples tested between Dec. 13, 2019, and Jan. 17, 2020, 106 (1.4%) were reactive.
These were not true positives, acknowledged the investigators. True positives would require reactive antibodies in the context of a positive molecular diagnostic test or paired acute convalescent sera with rising titers. The investigators also cautioned that false positives could not be completely ruled out, particularly in light of cross-reactivity that has been reported with other human coronaviruses.
Nevertheless, the monitoring of blood donations offers substantial promise for “understanding the dynamics of SARS-CoV-2 pandemic from early introduction,” and the CDC is now collaborating on ongoing surveillance with the goal of contributing information that could be applied “to mitigate morbidity and mortality.”
Lessons learned from this pandemic are potentially relevant to the next.
The EMR study simply looked at whether the word “cough” was included more often in the notes from visits or hospitalizations between December 2019 and February 2020 relative to the preceding 5 years. The investigators drew on data from three hospitals and more than 180 clinics.
From Dec. 22, 2019, onward, cough was noted above the 95% prediction interval for all 10 weeks of the study. The excess was seen in the outpatient setting and among hospitalized patients. There was also significant excess in the number of patients hospitalized with acute respiratory failure during the study period.
“Our approach to analyzing electronic records could be helpful in the future as we included consideration of data from the outpatient clinics in addition to the emergency departments and inpatient settings,” Dr. Elmore reported.
Surveillance of influenza and influenza-like infections has been undertaken in the United States for more than 20 years, but Dr. Elmore contends that EMR data, particularly data from outpatient clinics are “usually a harbinger of what is to come” for emergency department visits and, ultimately, hospitalizations. She thinks that this is a resource not yet fully exploited.
“There are always opportunities to better harness EMR data,” Dr. Elmore said.
These are intriguing studies and “useful” for reconsidering when SARS-CoV-2 was introduced in the United States, according to Janet G. Basemen, PhD, a professor of epidemiology and the associate dean of the University of Washington School of Public Health, Seattle. However, she noted that the task of translating data like these into actionable public health strategies has proven difficult in the past.
Symptom-based surveillance systems “have mostly served as situational awareness rather than early detection tools,” Dr. Baseman said. The problem is timely interpretation of a given signal.
Not that she doubts such tools “would be an incredible resource for humanity” if the current limitations can be resolved or that technological advances will lead to better methods of detecting and monitoring pandemics “at some point.” Rather, “we’re just not there yet,” she said.
SOURCE: Basavaraju SV et al. Clin Infect Dis. 2020 Nov 30. doi: 10.1093/cid/ciaa1785); Elmore JG et al. J Med Internet Res. 2020;22:e21562).