User login
High obesity rates in Southern states magnify COVID threats
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
In January, as Mississippi health officials planned for their incoming shipments of COVID-19 vaccine, they assessed the state’s most vulnerable: health care workers, of course, and elderly people in nursing homes. But among those who needed urgent protection from the virus ripping across the Magnolia State were 1 million Mississippians with obesity.
Obesity and weight-related illnesses have been deadly liabilities in the COVID era. A report released this month by the World Obesity Federation found that increased body weight is the second-greatest predictor of COVID-related hospitalization and death across the globe, trailing only old age as a risk factor.
As a fixture of life in the American South – home to 9 of the nation’s 12 heaviest states – obesity is playing a role not only in COVID outcomes, but in the calculus of the vaccination rollout. Mississippi was one of the first states to add a body mass index of 30 or more (a rough gauge of obesity tied to height and weight) to the list of qualifying medical conditions for a shot. About 40% of the state’s adults meet that definition, according to federal health survey data, and combined with the risk group already eligible for vaccination – residents 65 and older – that means fully half of Mississippi’s adults are entitled to vie for a restricted allotment of shots.
At least 29 states have green-lighted obesity for inclusion in the first phases of the vaccine rollout, according to KFF – a vast widening of eligibility that has the potential to overwhelm government efforts and heighten competition for scarce doses.
“We have a lifesaving intervention, and we don’t have enough of it,” said Jen Kates, PhD, director of global health and HIV policy for Kaiser Family Foundation. “Hard choices are being made about who should go first, and there is no right answer.”
The sheer prevalence of obesity in the nation – two in three Americans exceed what is considered a healthy weight – was a public health concern well before the pandemic. But COVID-19 dramatically fast-tracked the discussion from warnings about the long-term damage excess fat tissue can pose to heart, lung and metabolic functions to far more immediate threats.
In the United Kingdom, for example, overweight COVID patients were 67% more likely to require intensive care, and obese patients three times likelier, according to the World Obesity Federation report. A Centers for Disease Control and Prevention study released Monday found a similar trend among U.S. patients and noted that the risk of COVID-related hospitalization, ventilation and death increased with patients’ obesity level.
The counties that hug the southern Mississippi River are home to some of the most concentrated pockets of extreme obesity in the United States. Coronavirus infections began surging in Southern states early last summer, and hospitalizations rose in step.
Deaths in rural stretches of Arkansas, Louisiana, Mississippi, and Tennessee have been overshadowed by the sheer number of deaths in metropolitan areas like New York, Los Angeles, and Essex County, N.J. But as a share of the population, the coronavirus has been similarly unsparing in many Southern communities. In sparsely populated Claiborne County, Miss., on the floodplains of the Mississippi River, 30 residents – about 1 in 300 – had died as of early March. In East Feliciana Parish, La., north of Baton Rouge, with 106 deaths, about 1 in 180 had died by then.
“It’s just math. If the population is more obese and obesity clearly contributes to worse outcomes, then neighborhoods, cities, states and countries that are more obese will have a greater toll from COVID,” said Dr. James de Lemos, MD, a professor of internal medicine at UT Southwestern Medical Center in Dallas who led a study of hospitalized COVID patients published in the medical journal Circulation.
And, because in the U.S. obesity rates tend to be relatively high among African Americans and Latinos who are poor, with diminished access to health care, “it’s a triple whammy,” Dr. de Lemos said. “All these things intersect.”
Poverty and limited access to medical care are common features in the South, where residents like Michelle Antonyshyn, a former registered nurse and mother of seven in Salem, Ark., say they are afraid of the virus. Ms. Antonyshyn, 49, has obesity and debilitating pain in her knees and back, though she does not have high blood pressure or diabetes, two underlying conditions that federal health officials have determined are added risk factors for severe cases of COVID-19.
Still, she said, she “was very concerned just knowing that being obese puts you more at risk for bad outcomes such as being on a ventilator and death.” As a precaution, Ms. Antonyshyn said, she and her large brood locked down early and stopped attending church services in person, watching online instead.
“It’s not the same as having fellowship, but the risk for me was enough,” said Ms. Antonyshyn.
Governors throughout the South seem to recognize that weight can contribute to COVID-19 complications and have pushed for vaccine eligibility rules that prioritize obesity. But on the ground, local health officials are girding for having to tell newly eligible people who qualify as obese that there aren’t enough shots to go around.
In Port Gibson, Miss., Mheja Williams, MD, medical director of the Claiborne County Family Health Center, has been receiving barely enough doses to inoculate the health workers and oldest seniors in her county of 9,600. One week in early February, she received 100 doses.
Obesity and extreme obesity are endemic in Claiborne County, and health officials say the “normalization” of obesity means people often don’t register their weight as a risk factor, whether for COVID or other health issues. The risks are exacerbated by a general flouting of pandemic etiquette: Dr. Williams said that middle-aged and younger residents are not especially vigilant about physical distancing and that mask use is rare.
The rise of obesity in the United States is well documented over the past half-century, as the nation turned from a diet of fruits, vegetables and limited meats to one laden with ultra-processed foods and rich with salt, fat, sugar, and flavorings, along with copious amounts of meat, fast food, and soda. The U.S. has generally led the global obesity race, setting records as even toddlers and young children grew implausibly, dangerously overweight.
Well before COVID, obesity was a leading cause of preventable death in the United States. The National Institutes of Health declared it a disease in 1998, one that fosters heart disease, stroke, type 2 diabetes, and breast, colon, and other cancers.
Researchers say it is no coincidence that nations like the United States, the United Kingdom, and Italy, with relatively high obesity rates, have proved particularly vulnerable to the novel coronavirus.
They believe the virus may exploit underlying metabolic and physiological impairments that often exist in concert with obesity. Extra fat can lead to a cascade of metabolic disruptions, chronic systemic inflammation, and hormonal dysregulation that may thwart the body’s response to infection.
Other respiratory viruses, like influenza and SARS, which appeared in China in 2002, rely on cholesterol to spread enveloped RNA virus to neighboring cells, and researchers have proposed that a similar mechanism may play a role in the spread of the novel coronavirus.
There are also practical problems for coronavirus patients with obesity admitted to the hospital. They can be more difficult to intubate because of excess central weight pressing down on the diaphragm, making breathing with infected lungs even more difficult.
Physicians who specialize in treating patients with obesity say public health officials need to be more forthright and urgent in their messaging, telegraphing the risks of this COVID era.
“It should be explicit and direct,” said Fatima Stanford, MD, an obesity medicine specialist at Massachusetts General Hospital, Boston, and a Harvard Medical School instructor.
Dr. Stanford denounces the fat-shaming and bullying that people with obesity often experience. But telling patients – and the public – that obesity increases the risk of hospitalization and death is crucial, she said.
“I don’t think it’s stigmatizing,” she said. “If you tell them in that way, it’s not to scare you, it’s just giving information. Sometimes people are just unaware.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
FDA scrutinizes cancer therapies granted accelerated approval
U.S. regulators are stepping up scrutiny of therapies that were granted an accelerated approval to treat cancers on the basis of surrogate endpoints but have failed to show clinical or survival benefits upon more extensive testing.
At issue are a number of cancer indications for immunotherapies. Four have already been withdrawn (voluntarily by the manufacturer), and six more will be reviewed at an upcoming meeting.
In recent years, the US Food and Drug Administration has granted accelerated approvals to oncology medicines on the basis of evidence that suggests a benefit for patients. Examples of such evidence relate to response rates and estimates of tumor shrinkage. But these approvals are granted on the condition that the manufacturer conducts larger clinical trials that show clinical benefit, including benefit in overall survival.
Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, has argued that the point of these conditional approvals is to find acceptable surrogate markers to allow people with “desperate illnesses” to have access to potentially helpful drugs while work continues to determine the drug’s actual benefit to patients.
Oncologists are now questioning whether the FDA has become too lenient in its approach, Daniel A. Goldstein, MD, a senior physician in medical oncology and internal medicine at the Rabin Medical Center, Petah Tikva, Israel, told this news organization.
“The main two things you want from a cancer drug is to live longer and live a higher quality of life,” said Goldstein. “But these endpoints that they’ve been using over the past few years are not really giving us confidence that these drugs are actually going to help to live longer or better.”
Dr. Pazdur said the FDA will consider withdrawing its accelerated approvals when results of further studies do not confirm expected benefit for patients.
“This is like the pendulum has swung as far as it was going to swing and now is on the backswing,” said Dr. Goldstein, also of the department of health policy and management at the University of North Carolina at Chapel Hill. “You could call this a watershed moment.”
Although there’s near universal interest in allowing people with advanced cancer access to promising medicines, there’s also rising concern about exposing patients needlessly to costly drugs with potentially tough side effects. That may prompt a shift in the standards U.S. regulators apply to cancer medicines, Dr. Goldstein said.
Indications withdrawn and under review
In a meeting scheduled for April 27-29, the FDA’s Oncologic Drugs Advisory Committee will review indications granted through the accelerated approval process for three immunotherapies: pembrolizumab (Keytruda), atezolizumab (Tecentriq), and nivolumab (Opdivo).
It is part of an industry-wide evaluation of accelerated approvals for cancer indications in which confirmatory trials did not confirm clinical benefit, the FDA noted.
The process has already led to voluntary withdrawals of four cancer indications by the manufacturers, including one indication each for pembrolizumab, atezolizumab, and nivolumab, and one for durvalumab (Imfinzi).
All of these immunotherapies are approved for numerous cancer indications, and they all remain on the market. It is only the U.S. approvals for particular cancer indications that have been withdrawn.
In the past, olaratumab (Lartruvo) was withdrawn from the market altogether. The FDA granted accelerated approval of the drug for soft tissue sarcoma, but clinical benefit was not confirmed in a phase 3 trial.
Issue highlighted by Dr. Prasad and Dr. Gyawali
In recent years, much of the attention on accelerated approvals was spurred by the work of a few researchers, particularly Vinay Prasad, MD, MPH, associate professor in the department of epidemiology and biostatistics, University of California, San Francisco, and Bishal Gyawali, MD, PhD, from Queen’s University Cancer Research Institute, Kingston, Ont. (Both are regular contributors to the oncology section of this news organization.)
Dr. Goldstein made this point in a tweet about the FDA’s announcement of the April ODAC meetings:
“Well done to @oncology_bg and @VPrasadMDMPH among others for highlighting in their papers that the FDA wasn’t properly evaluating accelerated approval drugs.
FDA have listened.
And I thought that the impact of academia was limited!”
Dr. Prasad has made the case for closer scrutiny of accelerated approvals in a number of journal articles and in his 2020 book, “Malignant: How Bad Policy and Bad Evidence Harm People with Cancer,” published by Johns Hopkins University Press.
The book includes highlights of a 2016 article published in Mayo Clinic Proceedings that focused on surrogate endpoints used for FDA approvals. In the article, Dr. Prasad and his coauthor report that they did not find formal analyses of the strength of the surrogate-survival correlation in 14 of 25 cases of accelerated approvals (56%) and in 11 of 30 traditional approvals (37%).
“Our results were concerning. They imply that many surrogates are based on little more than a gut feeling. You might rationalize that and argue a gut feeling is the same as ‘reasonably likely to predict,’ but no reasonable person could think a gut feeling means established,” Dr. Prasad writes in his book. “Our result suggests the FDA is using surrogate endpoints far beyond what may be fair or reasonable.”
Dr. Gyawali has argued that the process by which the FDA assesses cancer drugs for approvals has undergone a profound shift. He has most recently remarked on this in an October 2020 commentary on Medscape.
“Until the recent floodgate of approvals based on response rates from single-arm trials, the majority of cancer therapy decisions were supported by evidence generated from randomized controlled trials (RCTs),” Dr. Gyawali wrote. “The evidence base to support clinical decisions in managing therapeutic side effects has been comparatively sparse.”
Accelerated approval to improve access
The FDA has struggled for about 2 decades with questions of where to set the bar on evidence for promising cancer drugs.
The agency’s accelerated approval program for drugs began in 1992. During the first decade, the focus was largely on medicines related to HIV.
In the early 2000s, oncology drugs began to dominate the program.
Dr. Pazdur has presided over the FDA’s marked changes regarding the use of surrogate markers when weighing whether to allow sales of cancer medicines. Formerly a professor at the University of Texas MD Anderson Cancer Center, Houston, Dr. Pazdur joined the FDA as director of the Division of Oncology Drug Products in 1999.
Soon after his appointment, he had to field inquiries from pharmaceutical companies about how much evidence they needed to receive accelerated approvals.
Early on, he publicly expressed impatience about the drugmakers’ approach. “The purpose of accelerated approval was not accelerated drug company profits,” Dr. Padzur said at a 2004 ODAC meeting.
Rather, the point is to allow access to potentially helpful drugs while work continues to determine their actual benefit to patients, he explained.
“It wasn’t a license to do less, less, less, and less to a point now that we may be getting companies that are coming in” intent on determining the minimum evidence the FDA will take, Dr. Pazdur said. “It shouldn’t be what is the lowest. It is what is a sufficient amount to give patients and physicians a real understanding of what their drug will do.”
In a 2016 interview with The New York Times, Dr. Pazdur said that his views on cancer drug approvals have evolved with time. He described himself as being “on a jihad to streamline the review process and get things out the door faster.”
“I have evolved from regulator to regulator-advocate,” Dr. Pazdur told the newspaper.
His attitude reflected his personal experience in losing his wife to ovarian cancer in 2015, as well as shifts in science and law. In 2012, Congress passed a law that gave the FDA new resources to speed medicines for life-threatening diseases to market. In addition, advances in genetics appeared to be making some medications more effective and easier to test, Dr. Pazdur said in The New York Times interview.
Withdrawals seen as sign of success
Since the program’s inception, only 6% of accelerated approvals for oncology indications have been withdrawn, the FDA said.
It would be a sign that the program is working if the April meetings lead to further withdrawals of indications that have been granted accelerated approval, Julie R. Gralow, MD, chief medical officer of the American Society of Clinical Oncology, said in an interview with this news organization.
“It shouldn’t be seen as a failure,” Dr. Gralow said.
In her own practice at the Fred Hutchinson Cancer Research Center, Seattle, she has seen the value of emerging therapies for patients fighting advanced cancers. During her 25 years of clinical practice in an academic setting, she has gained access to drugs through single-patient investigative new drug applications.
However, this path is not an option for many patients who undergo treatment in facilities other than academic centers, she commented. She noted that the accelerated approval process is a way to expand access to emerging medicines, but she sees a need for caution in the use of drugs that have been given only this conditional approval. She emphasizes that such drugs may be suitable only for certain patients.
“I would say that, for metastatic patients, patients with incurable disease, we are willing to take some risk,” Dr. Gralow said. “We don’t have other options. They can’t wait the years that it would take to get a drug approved.”
One such patient is David Mitchell, who serves as the consumer representative on ODAC. He told this news organization that he is taking three drugs for multiple myeloma that received accelerated approvals: pomalidomide, bortezomib, and daratumumab.
“I want the FDA to have the option to approve drugs in an accelerated pathway, because as a patient taking three drugs granted accelerated approval, I’m benefiting – I’ve lived the benefit,” Mr. Mitchell said, “and I want other patients to have the opportunity to have that benefit.”
He believes that the FDA’s approach regarding accelerated approvals serves to get potentially beneficial medicines to patients who have few options and also fulfills the FDA’s mandate to protect the public from treatments that have little benefit but can cause harm.
Accelerated approval also offers needed flexibility to drugmakers as they develop more specifically targeted drugs for diseases that affect relatively few people, such as multiple myeloma, he said. “As the targeting of your therapies gets tighter and for smaller groups of patients, you have a harder time following the traditional model,” such as conducting large, double-blind, placebo-controlled trials that may indicate increased overall survival, he said.
“To me, this is the way the FDA intended it to work,” he added. “It’s going to offer the accelerated approval based on a surrogate endpoint for a safe drug, but it’s going to require the confirmatory trial, and if the confirmatory trial fails, it will pull the drug off the market.”
Some medicines that have received accelerated approvals may ultimately be found not to benefit patients, Mr. Mitchell acknowledged. But people in his situation, whose disease has progressed despite treatments, may want to take that risk, he added.
Four cancer indications recently withdrawn voluntarily by the manufacturer
- December 2020: Nivolumab for the treatment of patients with metastatic small cell lung cancer with progression after platinum-based chemotherapy and at least one other line of therapy (Bristol Myers Squibb).
- February 2021: Durvalumab for the treatment of patients with locally advanced or metastatic urothelial carcinoma whose disease has progressed during or following platinum-based chemotherapy or within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy (AstraZeneca).
- March 2021: Pembrolizumab for the treatment of patients with metastatic small cell lung cancer with disease progression on or after platinum-based chemotherapy and at least one other prior line of therapy (Merck).
- March 2021: Atezolizumab for treatment of patients with locally advanced or metastatic urothelial carcinoma who experience disease progression during or following platinum-containing atezolizumab chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy (Genentech).
Six cancer indications under review at the April 2021 ODAC meeting
- Atezolizumab indicated in combination with protein-bound for the treatment of adults with unresectable locally advanced or metastatic triple-negative whose tumors express PD-L1 (PD-L1 stained tumor-infiltrating immune cells of any intensity covering ≥1% of the tumor area), as determined by an FDA-approved test.
- Atezolizumab indicated for patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma whose tumors express PD-L1 (Combined Positive Score ≥1), as determined by an FDA-approved test, with disease progression on or after two or more prior lines of therapy including fluoropyrimidine- and platinum-containing chemotherapy and if appropriate, HER2/neu-targeted therapy.
- Pembrolizumab indicated for the treatment of patients with who have been previously treated with .
- Nivolumab indicated as a single agent for the treatment of patients with hepatocellular carcinoma who have been previously treated with sorafenib.
A version of this article first appeared on Medscape.com.
U.S. regulators are stepping up scrutiny of therapies that were granted an accelerated approval to treat cancers on the basis of surrogate endpoints but have failed to show clinical or survival benefits upon more extensive testing.
At issue are a number of cancer indications for immunotherapies. Four have already been withdrawn (voluntarily by the manufacturer), and six more will be reviewed at an upcoming meeting.
In recent years, the US Food and Drug Administration has granted accelerated approvals to oncology medicines on the basis of evidence that suggests a benefit for patients. Examples of such evidence relate to response rates and estimates of tumor shrinkage. But these approvals are granted on the condition that the manufacturer conducts larger clinical trials that show clinical benefit, including benefit in overall survival.
Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, has argued that the point of these conditional approvals is to find acceptable surrogate markers to allow people with “desperate illnesses” to have access to potentially helpful drugs while work continues to determine the drug’s actual benefit to patients.
Oncologists are now questioning whether the FDA has become too lenient in its approach, Daniel A. Goldstein, MD, a senior physician in medical oncology and internal medicine at the Rabin Medical Center, Petah Tikva, Israel, told this news organization.
“The main two things you want from a cancer drug is to live longer and live a higher quality of life,” said Goldstein. “But these endpoints that they’ve been using over the past few years are not really giving us confidence that these drugs are actually going to help to live longer or better.”
Dr. Pazdur said the FDA will consider withdrawing its accelerated approvals when results of further studies do not confirm expected benefit for patients.
“This is like the pendulum has swung as far as it was going to swing and now is on the backswing,” said Dr. Goldstein, also of the department of health policy and management at the University of North Carolina at Chapel Hill. “You could call this a watershed moment.”
Although there’s near universal interest in allowing people with advanced cancer access to promising medicines, there’s also rising concern about exposing patients needlessly to costly drugs with potentially tough side effects. That may prompt a shift in the standards U.S. regulators apply to cancer medicines, Dr. Goldstein said.
Indications withdrawn and under review
In a meeting scheduled for April 27-29, the FDA’s Oncologic Drugs Advisory Committee will review indications granted through the accelerated approval process for three immunotherapies: pembrolizumab (Keytruda), atezolizumab (Tecentriq), and nivolumab (Opdivo).
It is part of an industry-wide evaluation of accelerated approvals for cancer indications in which confirmatory trials did not confirm clinical benefit, the FDA noted.
The process has already led to voluntary withdrawals of four cancer indications by the manufacturers, including one indication each for pembrolizumab, atezolizumab, and nivolumab, and one for durvalumab (Imfinzi).
All of these immunotherapies are approved for numerous cancer indications, and they all remain on the market. It is only the U.S. approvals for particular cancer indications that have been withdrawn.
In the past, olaratumab (Lartruvo) was withdrawn from the market altogether. The FDA granted accelerated approval of the drug for soft tissue sarcoma, but clinical benefit was not confirmed in a phase 3 trial.
Issue highlighted by Dr. Prasad and Dr. Gyawali
In recent years, much of the attention on accelerated approvals was spurred by the work of a few researchers, particularly Vinay Prasad, MD, MPH, associate professor in the department of epidemiology and biostatistics, University of California, San Francisco, and Bishal Gyawali, MD, PhD, from Queen’s University Cancer Research Institute, Kingston, Ont. (Both are regular contributors to the oncology section of this news organization.)
Dr. Goldstein made this point in a tweet about the FDA’s announcement of the April ODAC meetings:
“Well done to @oncology_bg and @VPrasadMDMPH among others for highlighting in their papers that the FDA wasn’t properly evaluating accelerated approval drugs.
FDA have listened.
And I thought that the impact of academia was limited!”
Dr. Prasad has made the case for closer scrutiny of accelerated approvals in a number of journal articles and in his 2020 book, “Malignant: How Bad Policy and Bad Evidence Harm People with Cancer,” published by Johns Hopkins University Press.
The book includes highlights of a 2016 article published in Mayo Clinic Proceedings that focused on surrogate endpoints used for FDA approvals. In the article, Dr. Prasad and his coauthor report that they did not find formal analyses of the strength of the surrogate-survival correlation in 14 of 25 cases of accelerated approvals (56%) and in 11 of 30 traditional approvals (37%).
“Our results were concerning. They imply that many surrogates are based on little more than a gut feeling. You might rationalize that and argue a gut feeling is the same as ‘reasonably likely to predict,’ but no reasonable person could think a gut feeling means established,” Dr. Prasad writes in his book. “Our result suggests the FDA is using surrogate endpoints far beyond what may be fair or reasonable.”
Dr. Gyawali has argued that the process by which the FDA assesses cancer drugs for approvals has undergone a profound shift. He has most recently remarked on this in an October 2020 commentary on Medscape.
“Until the recent floodgate of approvals based on response rates from single-arm trials, the majority of cancer therapy decisions were supported by evidence generated from randomized controlled trials (RCTs),” Dr. Gyawali wrote. “The evidence base to support clinical decisions in managing therapeutic side effects has been comparatively sparse.”
Accelerated approval to improve access
The FDA has struggled for about 2 decades with questions of where to set the bar on evidence for promising cancer drugs.
The agency’s accelerated approval program for drugs began in 1992. During the first decade, the focus was largely on medicines related to HIV.
In the early 2000s, oncology drugs began to dominate the program.
Dr. Pazdur has presided over the FDA’s marked changes regarding the use of surrogate markers when weighing whether to allow sales of cancer medicines. Formerly a professor at the University of Texas MD Anderson Cancer Center, Houston, Dr. Pazdur joined the FDA as director of the Division of Oncology Drug Products in 1999.
Soon after his appointment, he had to field inquiries from pharmaceutical companies about how much evidence they needed to receive accelerated approvals.
Early on, he publicly expressed impatience about the drugmakers’ approach. “The purpose of accelerated approval was not accelerated drug company profits,” Dr. Padzur said at a 2004 ODAC meeting.
Rather, the point is to allow access to potentially helpful drugs while work continues to determine their actual benefit to patients, he explained.
“It wasn’t a license to do less, less, less, and less to a point now that we may be getting companies that are coming in” intent on determining the minimum evidence the FDA will take, Dr. Pazdur said. “It shouldn’t be what is the lowest. It is what is a sufficient amount to give patients and physicians a real understanding of what their drug will do.”
In a 2016 interview with The New York Times, Dr. Pazdur said that his views on cancer drug approvals have evolved with time. He described himself as being “on a jihad to streamline the review process and get things out the door faster.”
“I have evolved from regulator to regulator-advocate,” Dr. Pazdur told the newspaper.
His attitude reflected his personal experience in losing his wife to ovarian cancer in 2015, as well as shifts in science and law. In 2012, Congress passed a law that gave the FDA new resources to speed medicines for life-threatening diseases to market. In addition, advances in genetics appeared to be making some medications more effective and easier to test, Dr. Pazdur said in The New York Times interview.
Withdrawals seen as sign of success
Since the program’s inception, only 6% of accelerated approvals for oncology indications have been withdrawn, the FDA said.
It would be a sign that the program is working if the April meetings lead to further withdrawals of indications that have been granted accelerated approval, Julie R. Gralow, MD, chief medical officer of the American Society of Clinical Oncology, said in an interview with this news organization.
“It shouldn’t be seen as a failure,” Dr. Gralow said.
In her own practice at the Fred Hutchinson Cancer Research Center, Seattle, she has seen the value of emerging therapies for patients fighting advanced cancers. During her 25 years of clinical practice in an academic setting, she has gained access to drugs through single-patient investigative new drug applications.
However, this path is not an option for many patients who undergo treatment in facilities other than academic centers, she commented. She noted that the accelerated approval process is a way to expand access to emerging medicines, but she sees a need for caution in the use of drugs that have been given only this conditional approval. She emphasizes that such drugs may be suitable only for certain patients.
“I would say that, for metastatic patients, patients with incurable disease, we are willing to take some risk,” Dr. Gralow said. “We don’t have other options. They can’t wait the years that it would take to get a drug approved.”
One such patient is David Mitchell, who serves as the consumer representative on ODAC. He told this news organization that he is taking three drugs for multiple myeloma that received accelerated approvals: pomalidomide, bortezomib, and daratumumab.
“I want the FDA to have the option to approve drugs in an accelerated pathway, because as a patient taking three drugs granted accelerated approval, I’m benefiting – I’ve lived the benefit,” Mr. Mitchell said, “and I want other patients to have the opportunity to have that benefit.”
He believes that the FDA’s approach regarding accelerated approvals serves to get potentially beneficial medicines to patients who have few options and also fulfills the FDA’s mandate to protect the public from treatments that have little benefit but can cause harm.
Accelerated approval also offers needed flexibility to drugmakers as they develop more specifically targeted drugs for diseases that affect relatively few people, such as multiple myeloma, he said. “As the targeting of your therapies gets tighter and for smaller groups of patients, you have a harder time following the traditional model,” such as conducting large, double-blind, placebo-controlled trials that may indicate increased overall survival, he said.
“To me, this is the way the FDA intended it to work,” he added. “It’s going to offer the accelerated approval based on a surrogate endpoint for a safe drug, but it’s going to require the confirmatory trial, and if the confirmatory trial fails, it will pull the drug off the market.”
Some medicines that have received accelerated approvals may ultimately be found not to benefit patients, Mr. Mitchell acknowledged. But people in his situation, whose disease has progressed despite treatments, may want to take that risk, he added.
Four cancer indications recently withdrawn voluntarily by the manufacturer
- December 2020: Nivolumab for the treatment of patients with metastatic small cell lung cancer with progression after platinum-based chemotherapy and at least one other line of therapy (Bristol Myers Squibb).
- February 2021: Durvalumab for the treatment of patients with locally advanced or metastatic urothelial carcinoma whose disease has progressed during or following platinum-based chemotherapy or within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy (AstraZeneca).
- March 2021: Pembrolizumab for the treatment of patients with metastatic small cell lung cancer with disease progression on or after platinum-based chemotherapy and at least one other prior line of therapy (Merck).
- March 2021: Atezolizumab for treatment of patients with locally advanced or metastatic urothelial carcinoma who experience disease progression during or following platinum-containing atezolizumab chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy (Genentech).
Six cancer indications under review at the April 2021 ODAC meeting
- Atezolizumab indicated in combination with protein-bound for the treatment of adults with unresectable locally advanced or metastatic triple-negative whose tumors express PD-L1 (PD-L1 stained tumor-infiltrating immune cells of any intensity covering ≥1% of the tumor area), as determined by an FDA-approved test.
- Atezolizumab indicated for patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma whose tumors express PD-L1 (Combined Positive Score ≥1), as determined by an FDA-approved test, with disease progression on or after two or more prior lines of therapy including fluoropyrimidine- and platinum-containing chemotherapy and if appropriate, HER2/neu-targeted therapy.
- Pembrolizumab indicated for the treatment of patients with who have been previously treated with .
- Nivolumab indicated as a single agent for the treatment of patients with hepatocellular carcinoma who have been previously treated with sorafenib.
A version of this article first appeared on Medscape.com.
U.S. regulators are stepping up scrutiny of therapies that were granted an accelerated approval to treat cancers on the basis of surrogate endpoints but have failed to show clinical or survival benefits upon more extensive testing.
At issue are a number of cancer indications for immunotherapies. Four have already been withdrawn (voluntarily by the manufacturer), and six more will be reviewed at an upcoming meeting.
In recent years, the US Food and Drug Administration has granted accelerated approvals to oncology medicines on the basis of evidence that suggests a benefit for patients. Examples of such evidence relate to response rates and estimates of tumor shrinkage. But these approvals are granted on the condition that the manufacturer conducts larger clinical trials that show clinical benefit, including benefit in overall survival.
Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, has argued that the point of these conditional approvals is to find acceptable surrogate markers to allow people with “desperate illnesses” to have access to potentially helpful drugs while work continues to determine the drug’s actual benefit to patients.
Oncologists are now questioning whether the FDA has become too lenient in its approach, Daniel A. Goldstein, MD, a senior physician in medical oncology and internal medicine at the Rabin Medical Center, Petah Tikva, Israel, told this news organization.
“The main two things you want from a cancer drug is to live longer and live a higher quality of life,” said Goldstein. “But these endpoints that they’ve been using over the past few years are not really giving us confidence that these drugs are actually going to help to live longer or better.”
Dr. Pazdur said the FDA will consider withdrawing its accelerated approvals when results of further studies do not confirm expected benefit for patients.
“This is like the pendulum has swung as far as it was going to swing and now is on the backswing,” said Dr. Goldstein, also of the department of health policy and management at the University of North Carolina at Chapel Hill. “You could call this a watershed moment.”
Although there’s near universal interest in allowing people with advanced cancer access to promising medicines, there’s also rising concern about exposing patients needlessly to costly drugs with potentially tough side effects. That may prompt a shift in the standards U.S. regulators apply to cancer medicines, Dr. Goldstein said.
Indications withdrawn and under review
In a meeting scheduled for April 27-29, the FDA’s Oncologic Drugs Advisory Committee will review indications granted through the accelerated approval process for three immunotherapies: pembrolizumab (Keytruda), atezolizumab (Tecentriq), and nivolumab (Opdivo).
It is part of an industry-wide evaluation of accelerated approvals for cancer indications in which confirmatory trials did not confirm clinical benefit, the FDA noted.
The process has already led to voluntary withdrawals of four cancer indications by the manufacturers, including one indication each for pembrolizumab, atezolizumab, and nivolumab, and one for durvalumab (Imfinzi).
All of these immunotherapies are approved for numerous cancer indications, and they all remain on the market. It is only the U.S. approvals for particular cancer indications that have been withdrawn.
In the past, olaratumab (Lartruvo) was withdrawn from the market altogether. The FDA granted accelerated approval of the drug for soft tissue sarcoma, but clinical benefit was not confirmed in a phase 3 trial.
Issue highlighted by Dr. Prasad and Dr. Gyawali
In recent years, much of the attention on accelerated approvals was spurred by the work of a few researchers, particularly Vinay Prasad, MD, MPH, associate professor in the department of epidemiology and biostatistics, University of California, San Francisco, and Bishal Gyawali, MD, PhD, from Queen’s University Cancer Research Institute, Kingston, Ont. (Both are regular contributors to the oncology section of this news organization.)
Dr. Goldstein made this point in a tweet about the FDA’s announcement of the April ODAC meetings:
“Well done to @oncology_bg and @VPrasadMDMPH among others for highlighting in their papers that the FDA wasn’t properly evaluating accelerated approval drugs.
FDA have listened.
And I thought that the impact of academia was limited!”
Dr. Prasad has made the case for closer scrutiny of accelerated approvals in a number of journal articles and in his 2020 book, “Malignant: How Bad Policy and Bad Evidence Harm People with Cancer,” published by Johns Hopkins University Press.
The book includes highlights of a 2016 article published in Mayo Clinic Proceedings that focused on surrogate endpoints used for FDA approvals. In the article, Dr. Prasad and his coauthor report that they did not find formal analyses of the strength of the surrogate-survival correlation in 14 of 25 cases of accelerated approvals (56%) and in 11 of 30 traditional approvals (37%).
“Our results were concerning. They imply that many surrogates are based on little more than a gut feeling. You might rationalize that and argue a gut feeling is the same as ‘reasonably likely to predict,’ but no reasonable person could think a gut feeling means established,” Dr. Prasad writes in his book. “Our result suggests the FDA is using surrogate endpoints far beyond what may be fair or reasonable.”
Dr. Gyawali has argued that the process by which the FDA assesses cancer drugs for approvals has undergone a profound shift. He has most recently remarked on this in an October 2020 commentary on Medscape.
“Until the recent floodgate of approvals based on response rates from single-arm trials, the majority of cancer therapy decisions were supported by evidence generated from randomized controlled trials (RCTs),” Dr. Gyawali wrote. “The evidence base to support clinical decisions in managing therapeutic side effects has been comparatively sparse.”
Accelerated approval to improve access
The FDA has struggled for about 2 decades with questions of where to set the bar on evidence for promising cancer drugs.
The agency’s accelerated approval program for drugs began in 1992. During the first decade, the focus was largely on medicines related to HIV.
In the early 2000s, oncology drugs began to dominate the program.
Dr. Pazdur has presided over the FDA’s marked changes regarding the use of surrogate markers when weighing whether to allow sales of cancer medicines. Formerly a professor at the University of Texas MD Anderson Cancer Center, Houston, Dr. Pazdur joined the FDA as director of the Division of Oncology Drug Products in 1999.
Soon after his appointment, he had to field inquiries from pharmaceutical companies about how much evidence they needed to receive accelerated approvals.
Early on, he publicly expressed impatience about the drugmakers’ approach. “The purpose of accelerated approval was not accelerated drug company profits,” Dr. Padzur said at a 2004 ODAC meeting.
Rather, the point is to allow access to potentially helpful drugs while work continues to determine their actual benefit to patients, he explained.
“It wasn’t a license to do less, less, less, and less to a point now that we may be getting companies that are coming in” intent on determining the minimum evidence the FDA will take, Dr. Pazdur said. “It shouldn’t be what is the lowest. It is what is a sufficient amount to give patients and physicians a real understanding of what their drug will do.”
In a 2016 interview with The New York Times, Dr. Pazdur said that his views on cancer drug approvals have evolved with time. He described himself as being “on a jihad to streamline the review process and get things out the door faster.”
“I have evolved from regulator to regulator-advocate,” Dr. Pazdur told the newspaper.
His attitude reflected his personal experience in losing his wife to ovarian cancer in 2015, as well as shifts in science and law. In 2012, Congress passed a law that gave the FDA new resources to speed medicines for life-threatening diseases to market. In addition, advances in genetics appeared to be making some medications more effective and easier to test, Dr. Pazdur said in The New York Times interview.
Withdrawals seen as sign of success
Since the program’s inception, only 6% of accelerated approvals for oncology indications have been withdrawn, the FDA said.
It would be a sign that the program is working if the April meetings lead to further withdrawals of indications that have been granted accelerated approval, Julie R. Gralow, MD, chief medical officer of the American Society of Clinical Oncology, said in an interview with this news organization.
“It shouldn’t be seen as a failure,” Dr. Gralow said.
In her own practice at the Fred Hutchinson Cancer Research Center, Seattle, she has seen the value of emerging therapies for patients fighting advanced cancers. During her 25 years of clinical practice in an academic setting, she has gained access to drugs through single-patient investigative new drug applications.
However, this path is not an option for many patients who undergo treatment in facilities other than academic centers, she commented. She noted that the accelerated approval process is a way to expand access to emerging medicines, but she sees a need for caution in the use of drugs that have been given only this conditional approval. She emphasizes that such drugs may be suitable only for certain patients.
“I would say that, for metastatic patients, patients with incurable disease, we are willing to take some risk,” Dr. Gralow said. “We don’t have other options. They can’t wait the years that it would take to get a drug approved.”
One such patient is David Mitchell, who serves as the consumer representative on ODAC. He told this news organization that he is taking three drugs for multiple myeloma that received accelerated approvals: pomalidomide, bortezomib, and daratumumab.
“I want the FDA to have the option to approve drugs in an accelerated pathway, because as a patient taking three drugs granted accelerated approval, I’m benefiting – I’ve lived the benefit,” Mr. Mitchell said, “and I want other patients to have the opportunity to have that benefit.”
He believes that the FDA’s approach regarding accelerated approvals serves to get potentially beneficial medicines to patients who have few options and also fulfills the FDA’s mandate to protect the public from treatments that have little benefit but can cause harm.
Accelerated approval also offers needed flexibility to drugmakers as they develop more specifically targeted drugs for diseases that affect relatively few people, such as multiple myeloma, he said. “As the targeting of your therapies gets tighter and for smaller groups of patients, you have a harder time following the traditional model,” such as conducting large, double-blind, placebo-controlled trials that may indicate increased overall survival, he said.
“To me, this is the way the FDA intended it to work,” he added. “It’s going to offer the accelerated approval based on a surrogate endpoint for a safe drug, but it’s going to require the confirmatory trial, and if the confirmatory trial fails, it will pull the drug off the market.”
Some medicines that have received accelerated approvals may ultimately be found not to benefit patients, Mr. Mitchell acknowledged. But people in his situation, whose disease has progressed despite treatments, may want to take that risk, he added.
Four cancer indications recently withdrawn voluntarily by the manufacturer
- December 2020: Nivolumab for the treatment of patients with metastatic small cell lung cancer with progression after platinum-based chemotherapy and at least one other line of therapy (Bristol Myers Squibb).
- February 2021: Durvalumab for the treatment of patients with locally advanced or metastatic urothelial carcinoma whose disease has progressed during or following platinum-based chemotherapy or within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy (AstraZeneca).
- March 2021: Pembrolizumab for the treatment of patients with metastatic small cell lung cancer with disease progression on or after platinum-based chemotherapy and at least one other prior line of therapy (Merck).
- March 2021: Atezolizumab for treatment of patients with locally advanced or metastatic urothelial carcinoma who experience disease progression during or following platinum-containing atezolizumab chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy (Genentech).
Six cancer indications under review at the April 2021 ODAC meeting
- Atezolizumab indicated in combination with protein-bound for the treatment of adults with unresectable locally advanced or metastatic triple-negative whose tumors express PD-L1 (PD-L1 stained tumor-infiltrating immune cells of any intensity covering ≥1% of the tumor area), as determined by an FDA-approved test.
- Atezolizumab indicated for patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy.
- Pembrolizumab indicated for the treatment of patients with recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma whose tumors express PD-L1 (Combined Positive Score ≥1), as determined by an FDA-approved test, with disease progression on or after two or more prior lines of therapy including fluoropyrimidine- and platinum-containing chemotherapy and if appropriate, HER2/neu-targeted therapy.
- Pembrolizumab indicated for the treatment of patients with who have been previously treated with .
- Nivolumab indicated as a single agent for the treatment of patients with hepatocellular carcinoma who have been previously treated with sorafenib.
A version of this article first appeared on Medscape.com.
Climate change: Dermatologists address impact on health, and mobilize to increase awareness
Climate change will increasingly affect the distribution and frequency of insect-borne diseases, cutaneous leishmaniasis, skin cancer, fungal diseases, and a host of other illnesses that have cutaneous manifestations or involve the skin – and dermatologists are being urged to be ready to diagnose clinical findings, counsel patients about risk mitigation, and decrease the carbon footprint of their practices and medical organizations.
“Climate change is not a far-off threat but an urgent health issue,” Misha Rosenbach, MD, associate professor of dermatology at the University of Pennsylvania, Philadelphia, wrote in an editorial with coauthor Mary Sun, a student at Icahn School of Medicine at Mount Sinai, New York. It was first published online in the British Journal of Dermatology last year, titled, “The climate emergency: Why should dermatologists care and how can they act?”.
. Some of the 150-plus members of the ERG have been writing about the dermatologic impacts of climate change – including content that filled the January issue of the International Journal of Women’s Dermatology – and speaking about the issues.
A session at the AAD’s virtual annual meeting in April will address climate change and dermatology – the second such session at an annual meeting – and the first two of three planned virtual symposia led by Dr. Rosenbach and his colleagues, have been hosted by the Association of Professors of Dermatology. The ERG encouraged the AAD’s adoption of a position statement in 2018 about climate change and dermatology and its membership in the Medical Society Consortium on Climate and Health.
“There’s been a lot of conversation in the medical community about the health effects of climate change, but most people leave out the skin,” said Mary L. Williams, MD, clinical professor of dermatology at the University of California, San Francisco, who is a cofounder and coleader with Dr. Rosenbach of the climate change ERG.
“That’s interesting because the skin is the most environmental of all our organs. Of course it will be impacted by all that’s going on,” she said. “We want to bring the dermatologic community and the wider medical community along with us [in appreciating and acting on this knowledge].”
Changing disease patterns
Dr. Rosenbach did not think much about how climate change could affect his patients and his clinical practice until he saw a severe case of hand, foot, and mouth disease in a hospitalized adult in Philadelphia about 10 years ago.

A presentation of the case at an infectious disease conference spurred discussion of how the preceding winters had been warmer and of correlations reported by researchers in China between the incidence of hand, foot, and mouth disease – historically a mild infection in children – and average temperature and other meteorological factors. “I knew about climate change, but I never knew we’d see different diseases in our clinical practice, or old diseases affecting new hosts,” Dr. Rosenbach said in an interview.
He pored over the literature to deepen his understanding of climate change science and the impact of climate change on medicine, and found an “emerging focus” on climate change in some medical journals, but “very little in dermatology.” In collaboration with Benjamin Kaffenberger, MD, a dermatologist at The Ohio State University, and colleagues, including an entomologist, Dr. Rosenbach wrote a review of publications relating to climate change and skin disease in North America.
Published in 2017 in the Journal of the American Academy of Dermatology, the review details how bacteria, viruses, fungi, and parasites are responding to changing weather patterns in North America, and why dermatologists should be able to recognize changing patterns of disease. Globalization plays a role in changing disease and vector patterns, but “climate change allows expansion of the natural range of pathogens, hosts, reservoirs, and vectors that allow diseases to appear in immunologically naive populations,” they wrote.
Patterns of infectious diseases with cutaneous manifestations are already changing. The geographic range of coccidioidomycosis, or valley fever, for instance, “has basically doubled in the Southwest U.S., extending up the entire West Coast,” Dr. Rosenbach said, as the result of longer dry seasons and more frequent wind storms that aerosolize the mycosis-causing, soil-dwelling fungal spores.
Lyme disease and associated tick-borne infections continue to expand northward as Ixodes tick vectors move and breed “exactly in sync with a warming world,” Dr. Rosenbach said. “We’re seeing Lyme in Philadelphia in February, whereas in the past we may not have seen it until May ... There are derms in Maine [whose patients have Lyme disease] who may never have seen a case before, and derms in Canada who are making diagnoses of Lyme [for the first time].”
And locally acquired cases of dengue are being reported in Hawaii, Texas, and Florida – and even North Carolina, according to a review of infectious diseases with cutaneous manifestations in the issue of the International Journal of Women’s Dermatology dedicated to climate change. As with Ixodes ticks, which transmit Lyme disease, rising temperatures lead to longer breeding seasons for Aedes mosquitoes, which transmit dengue. Increased endemicity of dengue is concerning because severe illness is significantly more likely in individuals previously infected with a different serotype.
“Dermatologists should be ready to identify and diagnose these mosquito-borne diseases that we think of as occurring in Central America or tropical regions,” Dr. Rosenbach said. “In my children’s lifetime there will be tropical diseases in New York, Philadelphia, Boston and other such places.”
In his articles and talks, Dr. Rosenbach lays out the science of climate change – for instance, the change in average global temperatures above preindustrial levels (an approximate 1° C rise) , the threshold beyond which the Earth will become less hospitable (1.5° C of warming according to United Nation’s Intergovernmental Panel on Climate Change), the current projections for future warming (an increase of about 3° Celsius by 2100), and the “gold-standard” level of scientific certainty that climate change is human-caused.
Mathematical climate modeling, he emphasized in the interview, can accurately project changes in infection rates. Researchers predicted 10 years ago in a published paper, for instance, that based on global warming patterns, the sand fly vector responsible for cutaneous leishmaniasis would live in the Southern United States and cause endemic infections within 10 years.
And in 2018, Dr. Rosenbach said, a paper in JAMA Dermatology described how more than half – 59% – of the cases of cutaneous leishmaniasis diagnosed in Texas were endemic, all occurring in people with no prior travel outside the United States.
Dr. Williams’ devotion to climate change and dermatology and to the climate change ERG was inspired in large part by Dr. Rosenbach’s 2017 paper in JAAD. She had long been concerned about climate change, she said, but “the review article was really the impetus for me to think, this is really within my specialty.”
Extreme weather events, and the climate-driven migration expected to increasingly occur, have clear relevance to dermatology, Dr. Williams said. “Often, the most vexing problems that people have when they’re forced out of their homes ... are dermatologic,” she said, like infections from contaminated waters after flooding and the spread of scabies and other communicable diseases due to crowding and unsanitary conditions.
But there are other less obvious ramifications of a changing climate that affect dermatology. Dr. Williams has delved into the literature on heat-related illness, for instance, and found that most research has been in the realm of sports medicine and military health. “Most of us don’t treat serious heat-related illnesses, but our skin is responsible for keeping us cool and there’s an important role for dermatologists to play in knowing how the skin does that and who is at risk for heat illness because the skin is unable to do the full job,” she said.
Research is needed to identify which medications can interfere with the skin’s thermoregulatory responses and put patients at risk, she noted. “And a lot of the work on sweat gland physiology is probably 30 years old now. We should bring to bear contemporary research techniques.”
Dermatology is also “in the early stages of understanding the role that air pollution plays in skin disease,” Dr. Williams said. “Most of the medical literature focuses on the effects of pollution on the lungs and in cardiovascular disease.”
There is evidence linking small particulate matter found in wood smoke and other air pollutants to exacerbations of atopic dermatitis and other inflammatory skin conditions, she noted, but mechanisms need to be explored and health disparities examined. “While we know that there are health disparities in terms of [exposure to] pollution and respiratory illness, we have no idea if this is the case with our skin diseases like atopic dermatitis,” said Dr. Williams.
In general, according to the AAD position statement, low-income and minority communities, in addition to the very young and the very old, “are and will continue to be disproportionately affected by climate change.”
Education and the carbon footprint
Viewing climate change as a social determinant of health (SDH ) – and integrating it into medical training as such – is a topic of active discussion. At UCSF, Sarah J. Coates, MD, a fellow in pediatric dermatology, is working with colleagues to integrate climate change into formal resident education. “We know that climate change affects housing, food security, migration ... and certain populations are and will be especially vulnerable,” she said in an interview. “The effects of climate change fit squarely into the social determinant of health curriculum that we’re building here.”

Dr. Coates began to appreciate the link between climate and infectious diseases – a topic she now writes and speaks about – when she saw several patients with coccidioidomycosis as a dermatology resident at UCSF and learned that the cases represented an epidemic in the Central Valley “resulting from several years of drought.”
Her medical school and residency training were otherwise devoid of any discussion of climate change. At UCSF and nearby Stanford (Calif.) University, this is no longer the case, she and Dr. Williams said. “The medical students here have been quite active and are requesting education,” noted Dr. Williams. “The desire to know more is coming from the bottom.”
Mary E. Maloney, MD, professor of medicine and director of dermatologic surgery at the University of Massachusetts, Worcester, sees the same interest from physicians-in-training in the Boston area. They want education about climate science, the impact of climate changes on health and risk mitigation, and ways to reduce medicine’s carbon footprint. “We need to teach them and charge them to lead in their communities,” she said in an interview.

Dr. Maloney joined the AAD’s climate change resource group soon after its inception, having realized the urgency of climate change and feeling that she needed “to get passionate and not just do small things.” As a Mohs surgeon, she expects an “explosion” of skin cancer as temperatures and sun exposure continue to increase.
She urges dermatologists to work to decrease the carbon footprint of their practices and to advocate for local hospitals and other clinical institutions to do so. On the AAD website, members now have free access to tools provided by the nonprofit organization My Green Doctor for outpatient offices to lighten their carbon footprints in a cost-effective – or even cost-saving – manner.
Dr. Maloney’s institution has moved to automated lighting systems and the use of LED lights, she said, and has encouraged ride sharing (prior to the pandemic) and computer switch-offs at night. And in her practice, she and a colleague have been working to reduce the purchasing and use of disposable plastics.
Educating patients about the effects of climate change on the health of their skin is another of the missions listed in the AAD’s position statement, and it’s something that Dr. Coates is currently researching. “It seems similar to talking about other social determinants of health,” she said. “Saying to a patient, for instance, ‘we’ve had some really terrible wildfires lately. They’re getting worse as the seasons go on and we know that’s because of climate change. How do you think your current rash relates to the current air quality? How you think the air quality affects your skin?’ ”
Dr. Rosenbach emphasizes that physicians are a broadly trusted group. “I’d tell a patient, ‘you’re the fourth patient I’ve seen with Lyme – we think that’s because it’s been a warmer year due to climate change,’” he said. “I don’t think that bringing up climate change has ever been a source of friction.”
Climate change will increasingly affect the distribution and frequency of insect-borne diseases, cutaneous leishmaniasis, skin cancer, fungal diseases, and a host of other illnesses that have cutaneous manifestations or involve the skin – and dermatologists are being urged to be ready to diagnose clinical findings, counsel patients about risk mitigation, and decrease the carbon footprint of their practices and medical organizations.
“Climate change is not a far-off threat but an urgent health issue,” Misha Rosenbach, MD, associate professor of dermatology at the University of Pennsylvania, Philadelphia, wrote in an editorial with coauthor Mary Sun, a student at Icahn School of Medicine at Mount Sinai, New York. It was first published online in the British Journal of Dermatology last year, titled, “The climate emergency: Why should dermatologists care and how can they act?”.
. Some of the 150-plus members of the ERG have been writing about the dermatologic impacts of climate change – including content that filled the January issue of the International Journal of Women’s Dermatology – and speaking about the issues.
A session at the AAD’s virtual annual meeting in April will address climate change and dermatology – the second such session at an annual meeting – and the first two of three planned virtual symposia led by Dr. Rosenbach and his colleagues, have been hosted by the Association of Professors of Dermatology. The ERG encouraged the AAD’s adoption of a position statement in 2018 about climate change and dermatology and its membership in the Medical Society Consortium on Climate and Health.
“There’s been a lot of conversation in the medical community about the health effects of climate change, but most people leave out the skin,” said Mary L. Williams, MD, clinical professor of dermatology at the University of California, San Francisco, who is a cofounder and coleader with Dr. Rosenbach of the climate change ERG.
“That’s interesting because the skin is the most environmental of all our organs. Of course it will be impacted by all that’s going on,” she said. “We want to bring the dermatologic community and the wider medical community along with us [in appreciating and acting on this knowledge].”
Changing disease patterns
Dr. Rosenbach did not think much about how climate change could affect his patients and his clinical practice until he saw a severe case of hand, foot, and mouth disease in a hospitalized adult in Philadelphia about 10 years ago.
A presentation of the case at an infectious disease conference spurred discussion of how the preceding winters had been warmer and of correlations reported by researchers in China between the incidence of hand, foot, and mouth disease – historically a mild infection in children – and average temperature and other meteorological factors. “I knew about climate change, but I never knew we’d see different diseases in our clinical practice, or old diseases affecting new hosts,” Dr. Rosenbach said in an interview.
He pored over the literature to deepen his understanding of climate change science and the impact of climate change on medicine, and found an “emerging focus” on climate change in some medical journals, but “very little in dermatology.” In collaboration with Benjamin Kaffenberger, MD, a dermatologist at The Ohio State University, and colleagues, including an entomologist, Dr. Rosenbach wrote a review of publications relating to climate change and skin disease in North America.
Published in 2017 in the Journal of the American Academy of Dermatology, the review details how bacteria, viruses, fungi, and parasites are responding to changing weather patterns in North America, and why dermatologists should be able to recognize changing patterns of disease. Globalization plays a role in changing disease and vector patterns, but “climate change allows expansion of the natural range of pathogens, hosts, reservoirs, and vectors that allow diseases to appear in immunologically naive populations,” they wrote.
Patterns of infectious diseases with cutaneous manifestations are already changing. The geographic range of coccidioidomycosis, or valley fever, for instance, “has basically doubled in the Southwest U.S., extending up the entire West Coast,” Dr. Rosenbach said, as the result of longer dry seasons and more frequent wind storms that aerosolize the mycosis-causing, soil-dwelling fungal spores.
Lyme disease and associated tick-borne infections continue to expand northward as Ixodes tick vectors move and breed “exactly in sync with a warming world,” Dr. Rosenbach said. “We’re seeing Lyme in Philadelphia in February, whereas in the past we may not have seen it until May ... There are derms in Maine [whose patients have Lyme disease] who may never have seen a case before, and derms in Canada who are making diagnoses of Lyme [for the first time].”
And locally acquired cases of dengue are being reported in Hawaii, Texas, and Florida – and even North Carolina, according to a review of infectious diseases with cutaneous manifestations in the issue of the International Journal of Women’s Dermatology dedicated to climate change. As with Ixodes ticks, which transmit Lyme disease, rising temperatures lead to longer breeding seasons for Aedes mosquitoes, which transmit dengue. Increased endemicity of dengue is concerning because severe illness is significantly more likely in individuals previously infected with a different serotype.
“Dermatologists should be ready to identify and diagnose these mosquito-borne diseases that we think of as occurring in Central America or tropical regions,” Dr. Rosenbach said. “In my children’s lifetime there will be tropical diseases in New York, Philadelphia, Boston and other such places.”
In his articles and talks, Dr. Rosenbach lays out the science of climate change – for instance, the change in average global temperatures above preindustrial levels (an approximate 1° C rise) , the threshold beyond which the Earth will become less hospitable (1.5° C of warming according to United Nation’s Intergovernmental Panel on Climate Change), the current projections for future warming (an increase of about 3° Celsius by 2100), and the “gold-standard” level of scientific certainty that climate change is human-caused.
Mathematical climate modeling, he emphasized in the interview, can accurately project changes in infection rates. Researchers predicted 10 years ago in a published paper, for instance, that based on global warming patterns, the sand fly vector responsible for cutaneous leishmaniasis would live in the Southern United States and cause endemic infections within 10 years.
And in 2018, Dr. Rosenbach said, a paper in JAMA Dermatology described how more than half – 59% – of the cases of cutaneous leishmaniasis diagnosed in Texas were endemic, all occurring in people with no prior travel outside the United States.
Dr. Williams’ devotion to climate change and dermatology and to the climate change ERG was inspired in large part by Dr. Rosenbach’s 2017 paper in JAAD. She had long been concerned about climate change, she said, but “the review article was really the impetus for me to think, this is really within my specialty.”
Extreme weather events, and the climate-driven migration expected to increasingly occur, have clear relevance to dermatology, Dr. Williams said. “Often, the most vexing problems that people have when they’re forced out of their homes ... are dermatologic,” she said, like infections from contaminated waters after flooding and the spread of scabies and other communicable diseases due to crowding and unsanitary conditions.
But there are other less obvious ramifications of a changing climate that affect dermatology. Dr. Williams has delved into the literature on heat-related illness, for instance, and found that most research has been in the realm of sports medicine and military health. “Most of us don’t treat serious heat-related illnesses, but our skin is responsible for keeping us cool and there’s an important role for dermatologists to play in knowing how the skin does that and who is at risk for heat illness because the skin is unable to do the full job,” she said.
Research is needed to identify which medications can interfere with the skin’s thermoregulatory responses and put patients at risk, she noted. “And a lot of the work on sweat gland physiology is probably 30 years old now. We should bring to bear contemporary research techniques.”
Dermatology is also “in the early stages of understanding the role that air pollution plays in skin disease,” Dr. Williams said. “Most of the medical literature focuses on the effects of pollution on the lungs and in cardiovascular disease.”
There is evidence linking small particulate matter found in wood smoke and other air pollutants to exacerbations of atopic dermatitis and other inflammatory skin conditions, she noted, but mechanisms need to be explored and health disparities examined. “While we know that there are health disparities in terms of [exposure to] pollution and respiratory illness, we have no idea if this is the case with our skin diseases like atopic dermatitis,” said Dr. Williams.
In general, according to the AAD position statement, low-income and minority communities, in addition to the very young and the very old, “are and will continue to be disproportionately affected by climate change.”
Education and the carbon footprint
Viewing climate change as a social determinant of health (SDH ) – and integrating it into medical training as such – is a topic of active discussion. At UCSF, Sarah J. Coates, MD, a fellow in pediatric dermatology, is working with colleagues to integrate climate change into formal resident education. “We know that climate change affects housing, food security, migration ... and certain populations are and will be especially vulnerable,” she said in an interview. “The effects of climate change fit squarely into the social determinant of health curriculum that we’re building here.”
Dr. Coates began to appreciate the link between climate and infectious diseases – a topic she now writes and speaks about – when she saw several patients with coccidioidomycosis as a dermatology resident at UCSF and learned that the cases represented an epidemic in the Central Valley “resulting from several years of drought.”
Her medical school and residency training were otherwise devoid of any discussion of climate change. At UCSF and nearby Stanford (Calif.) University, this is no longer the case, she and Dr. Williams said. “The medical students here have been quite active and are requesting education,” noted Dr. Williams. “The desire to know more is coming from the bottom.”
Mary E. Maloney, MD, professor of medicine and director of dermatologic surgery at the University of Massachusetts, Worcester, sees the same interest from physicians-in-training in the Boston area. They want education about climate science, the impact of climate changes on health and risk mitigation, and ways to reduce medicine’s carbon footprint. “We need to teach them and charge them to lead in their communities,” she said in an interview.
Dr. Maloney joined the AAD’s climate change resource group soon after its inception, having realized the urgency of climate change and feeling that she needed “to get passionate and not just do small things.” As a Mohs surgeon, she expects an “explosion” of skin cancer as temperatures and sun exposure continue to increase.
She urges dermatologists to work to decrease the carbon footprint of their practices and to advocate for local hospitals and other clinical institutions to do so. On the AAD website, members now have free access to tools provided by the nonprofit organization My Green Doctor for outpatient offices to lighten their carbon footprints in a cost-effective – or even cost-saving – manner.
Dr. Maloney’s institution has moved to automated lighting systems and the use of LED lights, she said, and has encouraged ride sharing (prior to the pandemic) and computer switch-offs at night. And in her practice, she and a colleague have been working to reduce the purchasing and use of disposable plastics.
Educating patients about the effects of climate change on the health of their skin is another of the missions listed in the AAD’s position statement, and it’s something that Dr. Coates is currently researching. “It seems similar to talking about other social determinants of health,” she said. “Saying to a patient, for instance, ‘we’ve had some really terrible wildfires lately. They’re getting worse as the seasons go on and we know that’s because of climate change. How do you think your current rash relates to the current air quality? How you think the air quality affects your skin?’ ”
Dr. Rosenbach emphasizes that physicians are a broadly trusted group. “I’d tell a patient, ‘you’re the fourth patient I’ve seen with Lyme – we think that’s because it’s been a warmer year due to climate change,’” he said. “I don’t think that bringing up climate change has ever been a source of friction.”
Climate change will increasingly affect the distribution and frequency of insect-borne diseases, cutaneous leishmaniasis, skin cancer, fungal diseases, and a host of other illnesses that have cutaneous manifestations or involve the skin – and dermatologists are being urged to be ready to diagnose clinical findings, counsel patients about risk mitigation, and decrease the carbon footprint of their practices and medical organizations.
“Climate change is not a far-off threat but an urgent health issue,” Misha Rosenbach, MD, associate professor of dermatology at the University of Pennsylvania, Philadelphia, wrote in an editorial with coauthor Mary Sun, a student at Icahn School of Medicine at Mount Sinai, New York. It was first published online in the British Journal of Dermatology last year, titled, “The climate emergency: Why should dermatologists care and how can they act?”.
. Some of the 150-plus members of the ERG have been writing about the dermatologic impacts of climate change – including content that filled the January issue of the International Journal of Women’s Dermatology – and speaking about the issues.
A session at the AAD’s virtual annual meeting in April will address climate change and dermatology – the second such session at an annual meeting – and the first two of three planned virtual symposia led by Dr. Rosenbach and his colleagues, have been hosted by the Association of Professors of Dermatology. The ERG encouraged the AAD’s adoption of a position statement in 2018 about climate change and dermatology and its membership in the Medical Society Consortium on Climate and Health.
“There’s been a lot of conversation in the medical community about the health effects of climate change, but most people leave out the skin,” said Mary L. Williams, MD, clinical professor of dermatology at the University of California, San Francisco, who is a cofounder and coleader with Dr. Rosenbach of the climate change ERG.
“That’s interesting because the skin is the most environmental of all our organs. Of course it will be impacted by all that’s going on,” she said. “We want to bring the dermatologic community and the wider medical community along with us [in appreciating and acting on this knowledge].”
Changing disease patterns
Dr. Rosenbach did not think much about how climate change could affect his patients and his clinical practice until he saw a severe case of hand, foot, and mouth disease in a hospitalized adult in Philadelphia about 10 years ago.
A presentation of the case at an infectious disease conference spurred discussion of how the preceding winters had been warmer and of correlations reported by researchers in China between the incidence of hand, foot, and mouth disease – historically a mild infection in children – and average temperature and other meteorological factors. “I knew about climate change, but I never knew we’d see different diseases in our clinical practice, or old diseases affecting new hosts,” Dr. Rosenbach said in an interview.
He pored over the literature to deepen his understanding of climate change science and the impact of climate change on medicine, and found an “emerging focus” on climate change in some medical journals, but “very little in dermatology.” In collaboration with Benjamin Kaffenberger, MD, a dermatologist at The Ohio State University, and colleagues, including an entomologist, Dr. Rosenbach wrote a review of publications relating to climate change and skin disease in North America.
Published in 2017 in the Journal of the American Academy of Dermatology, the review details how bacteria, viruses, fungi, and parasites are responding to changing weather patterns in North America, and why dermatologists should be able to recognize changing patterns of disease. Globalization plays a role in changing disease and vector patterns, but “climate change allows expansion of the natural range of pathogens, hosts, reservoirs, and vectors that allow diseases to appear in immunologically naive populations,” they wrote.
Patterns of infectious diseases with cutaneous manifestations are already changing. The geographic range of coccidioidomycosis, or valley fever, for instance, “has basically doubled in the Southwest U.S., extending up the entire West Coast,” Dr. Rosenbach said, as the result of longer dry seasons and more frequent wind storms that aerosolize the mycosis-causing, soil-dwelling fungal spores.
Lyme disease and associated tick-borne infections continue to expand northward as Ixodes tick vectors move and breed “exactly in sync with a warming world,” Dr. Rosenbach said. “We’re seeing Lyme in Philadelphia in February, whereas in the past we may not have seen it until May ... There are derms in Maine [whose patients have Lyme disease] who may never have seen a case before, and derms in Canada who are making diagnoses of Lyme [for the first time].”
And locally acquired cases of dengue are being reported in Hawaii, Texas, and Florida – and even North Carolina, according to a review of infectious diseases with cutaneous manifestations in the issue of the International Journal of Women’s Dermatology dedicated to climate change. As with Ixodes ticks, which transmit Lyme disease, rising temperatures lead to longer breeding seasons for Aedes mosquitoes, which transmit dengue. Increased endemicity of dengue is concerning because severe illness is significantly more likely in individuals previously infected with a different serotype.
“Dermatologists should be ready to identify and diagnose these mosquito-borne diseases that we think of as occurring in Central America or tropical regions,” Dr. Rosenbach said. “In my children’s lifetime there will be tropical diseases in New York, Philadelphia, Boston and other such places.”
In his articles and talks, Dr. Rosenbach lays out the science of climate change – for instance, the change in average global temperatures above preindustrial levels (an approximate 1° C rise) , the threshold beyond which the Earth will become less hospitable (1.5° C of warming according to United Nation’s Intergovernmental Panel on Climate Change), the current projections for future warming (an increase of about 3° Celsius by 2100), and the “gold-standard” level of scientific certainty that climate change is human-caused.
Mathematical climate modeling, he emphasized in the interview, can accurately project changes in infection rates. Researchers predicted 10 years ago in a published paper, for instance, that based on global warming patterns, the sand fly vector responsible for cutaneous leishmaniasis would live in the Southern United States and cause endemic infections within 10 years.
And in 2018, Dr. Rosenbach said, a paper in JAMA Dermatology described how more than half – 59% – of the cases of cutaneous leishmaniasis diagnosed in Texas were endemic, all occurring in people with no prior travel outside the United States.
Dr. Williams’ devotion to climate change and dermatology and to the climate change ERG was inspired in large part by Dr. Rosenbach’s 2017 paper in JAAD. She had long been concerned about climate change, she said, but “the review article was really the impetus for me to think, this is really within my specialty.”
Extreme weather events, and the climate-driven migration expected to increasingly occur, have clear relevance to dermatology, Dr. Williams said. “Often, the most vexing problems that people have when they’re forced out of their homes ... are dermatologic,” she said, like infections from contaminated waters after flooding and the spread of scabies and other communicable diseases due to crowding and unsanitary conditions.
But there are other less obvious ramifications of a changing climate that affect dermatology. Dr. Williams has delved into the literature on heat-related illness, for instance, and found that most research has been in the realm of sports medicine and military health. “Most of us don’t treat serious heat-related illnesses, but our skin is responsible for keeping us cool and there’s an important role for dermatologists to play in knowing how the skin does that and who is at risk for heat illness because the skin is unable to do the full job,” she said.
Research is needed to identify which medications can interfere with the skin’s thermoregulatory responses and put patients at risk, she noted. “And a lot of the work on sweat gland physiology is probably 30 years old now. We should bring to bear contemporary research techniques.”
Dermatology is also “in the early stages of understanding the role that air pollution plays in skin disease,” Dr. Williams said. “Most of the medical literature focuses on the effects of pollution on the lungs and in cardiovascular disease.”
There is evidence linking small particulate matter found in wood smoke and other air pollutants to exacerbations of atopic dermatitis and other inflammatory skin conditions, she noted, but mechanisms need to be explored and health disparities examined. “While we know that there are health disparities in terms of [exposure to] pollution and respiratory illness, we have no idea if this is the case with our skin diseases like atopic dermatitis,” said Dr. Williams.
In general, according to the AAD position statement, low-income and minority communities, in addition to the very young and the very old, “are and will continue to be disproportionately affected by climate change.”
Education and the carbon footprint
Viewing climate change as a social determinant of health (SDH ) – and integrating it into medical training as such – is a topic of active discussion. At UCSF, Sarah J. Coates, MD, a fellow in pediatric dermatology, is working with colleagues to integrate climate change into formal resident education. “We know that climate change affects housing, food security, migration ... and certain populations are and will be especially vulnerable,” she said in an interview. “The effects of climate change fit squarely into the social determinant of health curriculum that we’re building here.”
Dr. Coates began to appreciate the link between climate and infectious diseases – a topic she now writes and speaks about – when she saw several patients with coccidioidomycosis as a dermatology resident at UCSF and learned that the cases represented an epidemic in the Central Valley “resulting from several years of drought.”
Her medical school and residency training were otherwise devoid of any discussion of climate change. At UCSF and nearby Stanford (Calif.) University, this is no longer the case, she and Dr. Williams said. “The medical students here have been quite active and are requesting education,” noted Dr. Williams. “The desire to know more is coming from the bottom.”
Mary E. Maloney, MD, professor of medicine and director of dermatologic surgery at the University of Massachusetts, Worcester, sees the same interest from physicians-in-training in the Boston area. They want education about climate science, the impact of climate changes on health and risk mitigation, and ways to reduce medicine’s carbon footprint. “We need to teach them and charge them to lead in their communities,” she said in an interview.
Dr. Maloney joined the AAD’s climate change resource group soon after its inception, having realized the urgency of climate change and feeling that she needed “to get passionate and not just do small things.” As a Mohs surgeon, she expects an “explosion” of skin cancer as temperatures and sun exposure continue to increase.
She urges dermatologists to work to decrease the carbon footprint of their practices and to advocate for local hospitals and other clinical institutions to do so. On the AAD website, members now have free access to tools provided by the nonprofit organization My Green Doctor for outpatient offices to lighten their carbon footprints in a cost-effective – or even cost-saving – manner.
Dr. Maloney’s institution has moved to automated lighting systems and the use of LED lights, she said, and has encouraged ride sharing (prior to the pandemic) and computer switch-offs at night. And in her practice, she and a colleague have been working to reduce the purchasing and use of disposable plastics.
Educating patients about the effects of climate change on the health of their skin is another of the missions listed in the AAD’s position statement, and it’s something that Dr. Coates is currently researching. “It seems similar to talking about other social determinants of health,” she said. “Saying to a patient, for instance, ‘we’ve had some really terrible wildfires lately. They’re getting worse as the seasons go on and we know that’s because of climate change. How do you think your current rash relates to the current air quality? How you think the air quality affects your skin?’ ”
Dr. Rosenbach emphasizes that physicians are a broadly trusted group. “I’d tell a patient, ‘you’re the fourth patient I’ve seen with Lyme – we think that’s because it’s been a warmer year due to climate change,’” he said. “I don’t think that bringing up climate change has ever been a source of friction.”
Survey explores impact of pandemic on dermatologist happiness, burnout
, according to Medscape’s 2021 Dermatologist Lifestyle, Happiness & Burnout Report.
In addition, 15% reported being burned out, and 3% reported being depressed, yet about half reported being too busy to seek help for burnout and/or depression.
Those are among the key findings from the Medscape report, which was published online on Feb. 19, 2021. More than 12,000 physicians from 29 specialties, including dermatology, participated in the survey, which explores how physicians are coping with burnout, maintaining their personal wellness, and viewing their workplaces and futures amid the COVID-19 pandemic.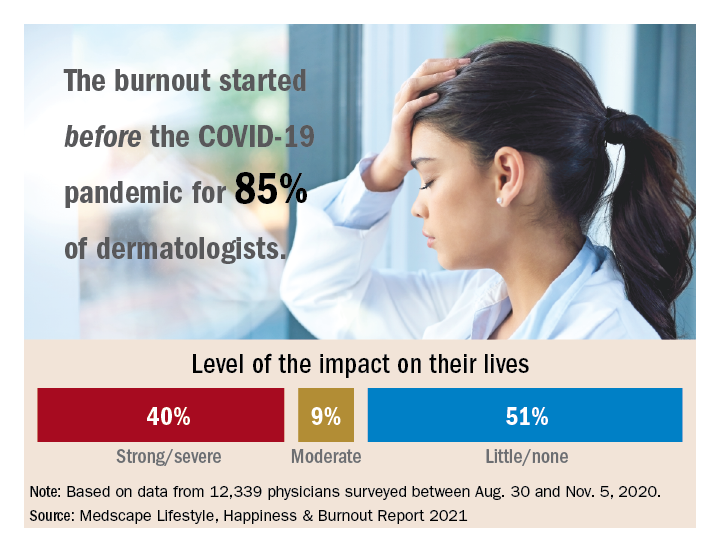
Among dermatologists who reported burnout, 85% said that it started prior to the pandemic, but 15% said it began with the pandemic. That finding resonates with Diane L. Whitaker-Worth, MD, a dermatologist with the University of Connecticut Health Center, Farmington. “A lot of dermatology practices closed down for a while, which was a huge economic hit,” she said in an interview. “I work for a university, so the stress wasn’t quite as bad. We shut down for about a week, but we canceled a lot of visits. We ramped up quickly, and I would say by the summer more people were coming in. Then we got backlogged. We’re still drowning in the number of patients who want to get in sooner, who can’t get an appointment, who need to be seen. It’s unbelievable, and it’s unrelenting.”
Dermatology trainees were also upended, with many residency programs going virtual. “We had to quickly figure out how to continue educating our residents,” said Dr. Whitaker-Worth, who also directs the university’s dermatology residency program. “What’s reasonable to expect them to be doing in clinic? There were fears about becoming infected [with the] virus. Every week, I had double the amount of work in the bureaucratic realm, trying to figure out how we run our clinic and keep our residents safe but learning. That was hard and the residents were really stressed. They were afraid they were going to get pulled to the ICUs. At that time, we didn’t have adequate PPE, and patients and doctors were dying.”
According to the dermatologists who responded to the Medscape survey and reported burnout, the seven chief contributors to burnout were too many bureaucratic tasks (70%); increasing computerization of practice (47%); insufficient compensation/reimbursement (31%); lack of respect from patients (27%); government regulations (26%); lack of respect from administrators/employers, colleagues, or staff (23%); and stress from social distancing/societal issues related to COVID-19 (15%).
“Even though dermatologists seemingly have such a nice schedule, compared to a lot of other doctors, it’s still a very stressful occupation,” said Dr. Whitaker-Worth, who coauthored a study on the topic of burnout among female dermatologists. “It is harder to practice now because there are so many people telling us how we have to do things. That will burn you out over time, when control is taken away, when tasks are handed to you randomly by different entities – insurance companies, the government, the electronic medical record.”
Among dermatologists who self-reported burnout on the survey, 51% said it had no impact on their life, 9% said the impact was moderate, while 40% indicated that it had a strong/severe impact. About half (49%) use exercise to cope with burnout, while other key coping strategies include talking with family members/close friends (40%), playing or listening to music (39%), isolating themselves from others (35%), eating junk food (35%), and drinking alcohol (30%). At the same time, only 6% indicated that they are currently seeking professional health for their burnout and/or depression, and 3% indicated that they are planning to seek professional help. When asked why they hadn’t sought help for their burnout and/or depression, 51% of respondents said they were too busy and 36% said their symptoms weren’t severe enough.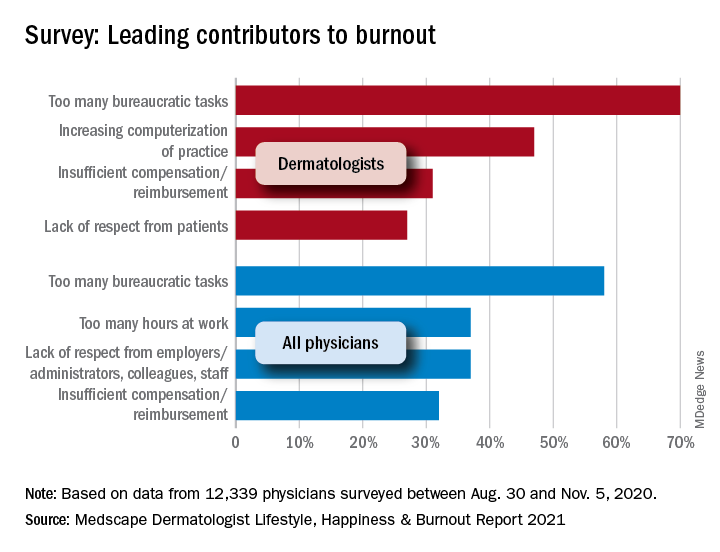
Dr. Whitaker-Worth characterized bureaucratic tasks as “a huge cause” of her burnout, but the larger contributor, she said, is managing her role as wife and mother of four children who are currently at home attending online school classes or working remotely, while she juggles her own work responsibilities. “They were stressed,” she said of her children. “The whole world was stressed. There are exceptions, but I still think that women are mostly shouldering the tasks at home. Even if they’re not doing them, they’re still feeling responsible for them. During the pandemic, every aspect of life became harder. Work was harder. Getting kids focused on school was harder. Doing basic tasks like errands was harder.”
Despite the stress and uncertainty generated by the pandemic, Dr. Whitaker-Worth considers dermatology as one of the happier specialties in medicine. “We still have a little more control of our time,” she said. “We are lucky in that we have reasonable hours, not as much in-house call, and a little more control over our day. I think work-life balance is the main thing that drives burnout – over bureaucracy, over everything.”
, according to Medscape’s 2021 Dermatologist Lifestyle, Happiness & Burnout Report.
In addition, 15% reported being burned out, and 3% reported being depressed, yet about half reported being too busy to seek help for burnout and/or depression.
Those are among the key findings from the Medscape report, which was published online on Feb. 19, 2021. More than 12,000 physicians from 29 specialties, including dermatology, participated in the survey, which explores how physicians are coping with burnout, maintaining their personal wellness, and viewing their workplaces and futures amid the COVID-19 pandemic.
Among dermatologists who reported burnout, 85% said that it started prior to the pandemic, but 15% said it began with the pandemic. That finding resonates with Diane L. Whitaker-Worth, MD, a dermatologist with the University of Connecticut Health Center, Farmington. “A lot of dermatology practices closed down for a while, which was a huge economic hit,” she said in an interview. “I work for a university, so the stress wasn’t quite as bad. We shut down for about a week, but we canceled a lot of visits. We ramped up quickly, and I would say by the summer more people were coming in. Then we got backlogged. We’re still drowning in the number of patients who want to get in sooner, who can’t get an appointment, who need to be seen. It’s unbelievable, and it’s unrelenting.”
Dermatology trainees were also upended, with many residency programs going virtual. “We had to quickly figure out how to continue educating our residents,” said Dr. Whitaker-Worth, who also directs the university’s dermatology residency program. “What’s reasonable to expect them to be doing in clinic? There were fears about becoming infected [with the] virus. Every week, I had double the amount of work in the bureaucratic realm, trying to figure out how we run our clinic and keep our residents safe but learning. That was hard and the residents were really stressed. They were afraid they were going to get pulled to the ICUs. At that time, we didn’t have adequate PPE, and patients and doctors were dying.”
According to the dermatologists who responded to the Medscape survey and reported burnout, the seven chief contributors to burnout were too many bureaucratic tasks (70%); increasing computerization of practice (47%); insufficient compensation/reimbursement (31%); lack of respect from patients (27%); government regulations (26%); lack of respect from administrators/employers, colleagues, or staff (23%); and stress from social distancing/societal issues related to COVID-19 (15%).
“Even though dermatologists seemingly have such a nice schedule, compared to a lot of other doctors, it’s still a very stressful occupation,” said Dr. Whitaker-Worth, who coauthored a study on the topic of burnout among female dermatologists. “It is harder to practice now because there are so many people telling us how we have to do things. That will burn you out over time, when control is taken away, when tasks are handed to you randomly by different entities – insurance companies, the government, the electronic medical record.”
Among dermatologists who self-reported burnout on the survey, 51% said it had no impact on their life, 9% said the impact was moderate, while 40% indicated that it had a strong/severe impact. About half (49%) use exercise to cope with burnout, while other key coping strategies include talking with family members/close friends (40%), playing or listening to music (39%), isolating themselves from others (35%), eating junk food (35%), and drinking alcohol (30%). At the same time, only 6% indicated that they are currently seeking professional health for their burnout and/or depression, and 3% indicated that they are planning to seek professional help. When asked why they hadn’t sought help for their burnout and/or depression, 51% of respondents said they were too busy and 36% said their symptoms weren’t severe enough.
Dr. Whitaker-Worth characterized bureaucratic tasks as “a huge cause” of her burnout, but the larger contributor, she said, is managing her role as wife and mother of four children who are currently at home attending online school classes or working remotely, while she juggles her own work responsibilities. “They were stressed,” she said of her children. “The whole world was stressed. There are exceptions, but I still think that women are mostly shouldering the tasks at home. Even if they’re not doing them, they’re still feeling responsible for them. During the pandemic, every aspect of life became harder. Work was harder. Getting kids focused on school was harder. Doing basic tasks like errands was harder.”
Despite the stress and uncertainty generated by the pandemic, Dr. Whitaker-Worth considers dermatology as one of the happier specialties in medicine. “We still have a little more control of our time,” she said. “We are lucky in that we have reasonable hours, not as much in-house call, and a little more control over our day. I think work-life balance is the main thing that drives burnout – over bureaucracy, over everything.”
, according to Medscape’s 2021 Dermatologist Lifestyle, Happiness & Burnout Report.
In addition, 15% reported being burned out, and 3% reported being depressed, yet about half reported being too busy to seek help for burnout and/or depression.
Those are among the key findings from the Medscape report, which was published online on Feb. 19, 2021. More than 12,000 physicians from 29 specialties, including dermatology, participated in the survey, which explores how physicians are coping with burnout, maintaining their personal wellness, and viewing their workplaces and futures amid the COVID-19 pandemic.
Among dermatologists who reported burnout, 85% said that it started prior to the pandemic, but 15% said it began with the pandemic. That finding resonates with Diane L. Whitaker-Worth, MD, a dermatologist with the University of Connecticut Health Center, Farmington. “A lot of dermatology practices closed down for a while, which was a huge economic hit,” she said in an interview. “I work for a university, so the stress wasn’t quite as bad. We shut down for about a week, but we canceled a lot of visits. We ramped up quickly, and I would say by the summer more people were coming in. Then we got backlogged. We’re still drowning in the number of patients who want to get in sooner, who can’t get an appointment, who need to be seen. It’s unbelievable, and it’s unrelenting.”
Dermatology trainees were also upended, with many residency programs going virtual. “We had to quickly figure out how to continue educating our residents,” said Dr. Whitaker-Worth, who also directs the university’s dermatology residency program. “What’s reasonable to expect them to be doing in clinic? There were fears about becoming infected [with the] virus. Every week, I had double the amount of work in the bureaucratic realm, trying to figure out how we run our clinic and keep our residents safe but learning. That was hard and the residents were really stressed. They were afraid they were going to get pulled to the ICUs. At that time, we didn’t have adequate PPE, and patients and doctors were dying.”
According to the dermatologists who responded to the Medscape survey and reported burnout, the seven chief contributors to burnout were too many bureaucratic tasks (70%); increasing computerization of practice (47%); insufficient compensation/reimbursement (31%); lack of respect from patients (27%); government regulations (26%); lack of respect from administrators/employers, colleagues, or staff (23%); and stress from social distancing/societal issues related to COVID-19 (15%).
“Even though dermatologists seemingly have such a nice schedule, compared to a lot of other doctors, it’s still a very stressful occupation,” said Dr. Whitaker-Worth, who coauthored a study on the topic of burnout among female dermatologists. “It is harder to practice now because there are so many people telling us how we have to do things. That will burn you out over time, when control is taken away, when tasks are handed to you randomly by different entities – insurance companies, the government, the electronic medical record.”
Among dermatologists who self-reported burnout on the survey, 51% said it had no impact on their life, 9% said the impact was moderate, while 40% indicated that it had a strong/severe impact. About half (49%) use exercise to cope with burnout, while other key coping strategies include talking with family members/close friends (40%), playing or listening to music (39%), isolating themselves from others (35%), eating junk food (35%), and drinking alcohol (30%). At the same time, only 6% indicated that they are currently seeking professional health for their burnout and/or depression, and 3% indicated that they are planning to seek professional help. When asked why they hadn’t sought help for their burnout and/or depression, 51% of respondents said they were too busy and 36% said their symptoms weren’t severe enough.
Dr. Whitaker-Worth characterized bureaucratic tasks as “a huge cause” of her burnout, but the larger contributor, she said, is managing her role as wife and mother of four children who are currently at home attending online school classes or working remotely, while she juggles her own work responsibilities. “They were stressed,” she said of her children. “The whole world was stressed. There are exceptions, but I still think that women are mostly shouldering the tasks at home. Even if they’re not doing them, they’re still feeling responsible for them. During the pandemic, every aspect of life became harder. Work was harder. Getting kids focused on school was harder. Doing basic tasks like errands was harder.”
Despite the stress and uncertainty generated by the pandemic, Dr. Whitaker-Worth considers dermatology as one of the happier specialties in medicine. “We still have a little more control of our time,” she said. “We are lucky in that we have reasonable hours, not as much in-house call, and a little more control over our day. I think work-life balance is the main thing that drives burnout – over bureaucracy, over everything.”
Fauci worries about possible post–COVID-19 ‘mental health pandemic’
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.

Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.
Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
Anthony Fauci, MD, says he’s concerned about how Americans will react once the coronavirus pandemic is brought under control, CBS News reports.
Noting that an American Psychological Association survey showed people reporting high stress levels because of the pandemic, CBS’s Norah O’Donnell asked if Dr. Fauci was concerned about a possible “mental health pandemic.”
“Very much so,” Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases and a top White House coronavirus adviser, replied.
“That’s the reason why I want to get the virological aspect of this pandemic behind us as quickly as we possibly can because the long-term ravages of this are so multifaceted,” Dr. Fauci said.
, he said.
“And then the other things: Not only the mental health effects, but many people have put off routine types of medical examinations that they normally would have done,” Dr. Fauci said.
“I hope we don’t see an increase in some preventable situations that would not have happened if people had the normal access to medical care, which clearly was interrupted by the shutdown associated with COVID-19,” he added.
The American Psychological Association released the survey results March 11 in what many people consider the 1-year anniversary of the start of the coronavirus pandemic.
“The prolonged stress experienced by adults, especially the high levels of stress reported by Americans directly linked to the pandemic, is seriously affecting mental and physical health, including changes to weight, sleep and alcohol use,” the APA said in a news release.
Some of the key findings of the survey include:
- 61% of respondents reported experiencing undesired weight changes since the start of the pandemic.
- 67% said their sleep habits changed, with 35% saying they slept more and 31% less.
- 23% reported drinking more alcohol to cope with stress.
- 47% said they delayed or canceled health care services because of the pandemic.
- 48% said their stress levels had increased.
A version of this article first appeared on Medscape.com.
Decline in child COVID-19 cases picks up after 2-week slowdown
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.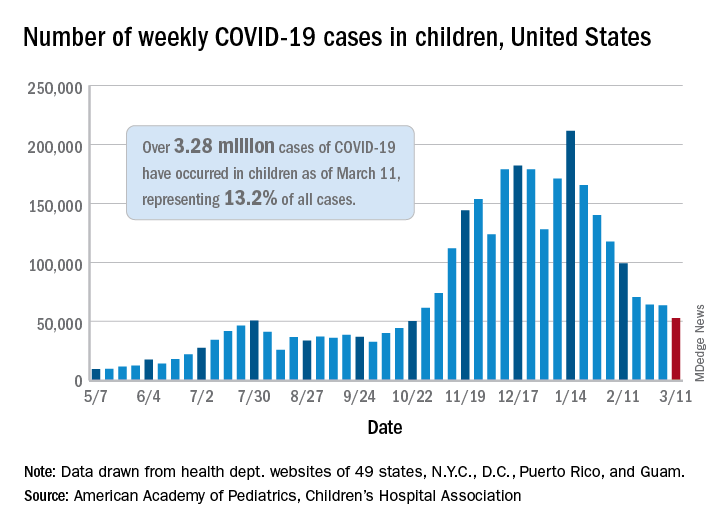
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
Blood cancer patients, survivors hesitate over COVID-19 vaccine
Nearly one in three patients with blood cancer, and survivors, say they are unlikely to get a COVID-19 vaccine or unsure about getting it if one were available. The findings come from a nationwide survey by The Leukemia & Lymphoma Society, which collected 6,517 responses.
“These findings are worrisome, to say the least,” Gwen Nichols, MD, chief medical officer of the society, said in a statement.
“We know cancer patients – and blood cancer patients in particular – are susceptible to the worst effects of the virus [and] all of us in the medical community need to help cancer patients understand the importance of getting vaccinated,” she added.
The survey – the largest ever done in which cancer patients and survivors were asked about their attitudes toward COVID-19 vaccines – was published online March 8 by The Leukemia & Lymphoma Society.
Survey sample
The survey asked patients with blood cancer, and survivors, about their attitudes regarding COVID-19 and COVID-19 vaccines.
“The main outcome [was] vaccine attitudes,” noted the authors, headed by Rena Conti, PhD, dean’s research scholar, Boston University.
Respondents were asked: “How likely are you to choose to get the vaccine?” Participants could indicate they were very unlikely, unlikely, neither likely nor unlikely, likely, or very likely to get vaccinated.
“We found that 17% of respondents indicate[d] that they [were] unlikely or very unlikely to take a vaccine,” Dr. Conti and colleagues observed.
Among the 17% – deemed to be “vaccine hesitant” – slightly over half (54%) stated they had concerns about the side effects associated with COVID-19 vaccination and believed neither of the two newly approved vaccines had been or would ever be tested properly.
The survey authors noted that there is no reason to believe COVID-19 vaccines are any less safe in patients with blood cancers, but concerns have been expressed that patients with some forms of blood cancer or those undergoing certain treatments may not achieve the same immune response to the vaccine as would noncancer controls.
Importantly, the survey was conducted Dec. 1-21, 2020, and responses differed depending on whether respondents answered the survey before or after the Pfizer-BioNTech and Moderna vaccines had been given emergency use authorization by the Food and Drug Administration starting Dec. 10, 2020.
There was a slight increase in positive responses after the vaccines were granted regulatory approval. (One-third of those who responded to the survey after the approval were 3.7% more likely to indicate they would get vaccinated). “This suggests that hesitancy may be influenced by emerging information dissemination, government action, and vaccine availability, transforming the hypothetical opportunity of vaccination to a real one,” the survey authors speculated.
Survey respondents who were vaccine hesitant were also over 14% more likely to indicate that they didn’t think they would require hospitalization should they contract COVID-19. But clinical data have suggested that approximately half of patients with a hematological malignancy who required hospitalization for COVID-19 die from the infection, the authors noted.
“Vaccine hesitant respondents [were] also significantly less likely to engage in protective health behaviors,” the survey authors pointed out. For example, they were almost 4% less likely to have worn a face mask and 1.6% less likely to have taken other protective measures to guard against COVID-19 infection.
Need for clear messaging
To counter vaccine hesitancy, the authors suggest there is a need for clear, consistent messaging targeting patients with cancer that emphasize the risks of COVID-19 and underscore vaccine benefits.
Dr. Conti pointed out that patients with blood cancer are, in fact, being given preferential access to vaccines in many communities, although this clearly doesn’t mean patients are willing to get vaccinated, as she also noted.
“We need both adequate supply and strong demand to keep this vulnerable population safe,” Dr. Conti emphasized.
The Leukemia & Lymphoma Society plans to repeat the survey in the near future to assess patients’ and survivors’ access to vaccines as well as their willingness to get vaccinated.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nearly one in three patients with blood cancer, and survivors, say they are unlikely to get a COVID-19 vaccine or unsure about getting it if one were available. The findings come from a nationwide survey by The Leukemia & Lymphoma Society, which collected 6,517 responses.
“These findings are worrisome, to say the least,” Gwen Nichols, MD, chief medical officer of the society, said in a statement.
“We know cancer patients – and blood cancer patients in particular – are susceptible to the worst effects of the virus [and] all of us in the medical community need to help cancer patients understand the importance of getting vaccinated,” she added.
The survey – the largest ever done in which cancer patients and survivors were asked about their attitudes toward COVID-19 vaccines – was published online March 8 by The Leukemia & Lymphoma Society.
Survey sample
The survey asked patients with blood cancer, and survivors, about their attitudes regarding COVID-19 and COVID-19 vaccines.
“The main outcome [was] vaccine attitudes,” noted the authors, headed by Rena Conti, PhD, dean’s research scholar, Boston University.
Respondents were asked: “How likely are you to choose to get the vaccine?” Participants could indicate they were very unlikely, unlikely, neither likely nor unlikely, likely, or very likely to get vaccinated.
“We found that 17% of respondents indicate[d] that they [were] unlikely or very unlikely to take a vaccine,” Dr. Conti and colleagues observed.
Among the 17% – deemed to be “vaccine hesitant” – slightly over half (54%) stated they had concerns about the side effects associated with COVID-19 vaccination and believed neither of the two newly approved vaccines had been or would ever be tested properly.
The survey authors noted that there is no reason to believe COVID-19 vaccines are any less safe in patients with blood cancers, but concerns have been expressed that patients with some forms of blood cancer or those undergoing certain treatments may not achieve the same immune response to the vaccine as would noncancer controls.
Importantly, the survey was conducted Dec. 1-21, 2020, and responses differed depending on whether respondents answered the survey before or after the Pfizer-BioNTech and Moderna vaccines had been given emergency use authorization by the Food and Drug Administration starting Dec. 10, 2020.
There was a slight increase in positive responses after the vaccines were granted regulatory approval. (One-third of those who responded to the survey after the approval were 3.7% more likely to indicate they would get vaccinated). “This suggests that hesitancy may be influenced by emerging information dissemination, government action, and vaccine availability, transforming the hypothetical opportunity of vaccination to a real one,” the survey authors speculated.
Survey respondents who were vaccine hesitant were also over 14% more likely to indicate that they didn’t think they would require hospitalization should they contract COVID-19. But clinical data have suggested that approximately half of patients with a hematological malignancy who required hospitalization for COVID-19 die from the infection, the authors noted.
“Vaccine hesitant respondents [were] also significantly less likely to engage in protective health behaviors,” the survey authors pointed out. For example, they were almost 4% less likely to have worn a face mask and 1.6% less likely to have taken other protective measures to guard against COVID-19 infection.
Need for clear messaging
To counter vaccine hesitancy, the authors suggest there is a need for clear, consistent messaging targeting patients with cancer that emphasize the risks of COVID-19 and underscore vaccine benefits.
Dr. Conti pointed out that patients with blood cancer are, in fact, being given preferential access to vaccines in many communities, although this clearly doesn’t mean patients are willing to get vaccinated, as she also noted.
“We need both adequate supply and strong demand to keep this vulnerable population safe,” Dr. Conti emphasized.
The Leukemia & Lymphoma Society plans to repeat the survey in the near future to assess patients’ and survivors’ access to vaccines as well as their willingness to get vaccinated.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nearly one in three patients with blood cancer, and survivors, say they are unlikely to get a COVID-19 vaccine or unsure about getting it if one were available. The findings come from a nationwide survey by The Leukemia & Lymphoma Society, which collected 6,517 responses.
“These findings are worrisome, to say the least,” Gwen Nichols, MD, chief medical officer of the society, said in a statement.
“We know cancer patients – and blood cancer patients in particular – are susceptible to the worst effects of the virus [and] all of us in the medical community need to help cancer patients understand the importance of getting vaccinated,” she added.
The survey – the largest ever done in which cancer patients and survivors were asked about their attitudes toward COVID-19 vaccines – was published online March 8 by The Leukemia & Lymphoma Society.
Survey sample
The survey asked patients with blood cancer, and survivors, about their attitudes regarding COVID-19 and COVID-19 vaccines.
“The main outcome [was] vaccine attitudes,” noted the authors, headed by Rena Conti, PhD, dean’s research scholar, Boston University.
Respondents were asked: “How likely are you to choose to get the vaccine?” Participants could indicate they were very unlikely, unlikely, neither likely nor unlikely, likely, or very likely to get vaccinated.
“We found that 17% of respondents indicate[d] that they [were] unlikely or very unlikely to take a vaccine,” Dr. Conti and colleagues observed.
Among the 17% – deemed to be “vaccine hesitant” – slightly over half (54%) stated they had concerns about the side effects associated with COVID-19 vaccination and believed neither of the two newly approved vaccines had been or would ever be tested properly.
The survey authors noted that there is no reason to believe COVID-19 vaccines are any less safe in patients with blood cancers, but concerns have been expressed that patients with some forms of blood cancer or those undergoing certain treatments may not achieve the same immune response to the vaccine as would noncancer controls.
Importantly, the survey was conducted Dec. 1-21, 2020, and responses differed depending on whether respondents answered the survey before or after the Pfizer-BioNTech and Moderna vaccines had been given emergency use authorization by the Food and Drug Administration starting Dec. 10, 2020.
There was a slight increase in positive responses after the vaccines were granted regulatory approval. (One-third of those who responded to the survey after the approval were 3.7% more likely to indicate they would get vaccinated). “This suggests that hesitancy may be influenced by emerging information dissemination, government action, and vaccine availability, transforming the hypothetical opportunity of vaccination to a real one,” the survey authors speculated.
Survey respondents who were vaccine hesitant were also over 14% more likely to indicate that they didn’t think they would require hospitalization should they contract COVID-19. But clinical data have suggested that approximately half of patients with a hematological malignancy who required hospitalization for COVID-19 die from the infection, the authors noted.
“Vaccine hesitant respondents [were] also significantly less likely to engage in protective health behaviors,” the survey authors pointed out. For example, they were almost 4% less likely to have worn a face mask and 1.6% less likely to have taken other protective measures to guard against COVID-19 infection.
Need for clear messaging
To counter vaccine hesitancy, the authors suggest there is a need for clear, consistent messaging targeting patients with cancer that emphasize the risks of COVID-19 and underscore vaccine benefits.
Dr. Conti pointed out that patients with blood cancer are, in fact, being given preferential access to vaccines in many communities, although this clearly doesn’t mean patients are willing to get vaccinated, as she also noted.
“We need both adequate supply and strong demand to keep this vulnerable population safe,” Dr. Conti emphasized.
The Leukemia & Lymphoma Society plans to repeat the survey in the near future to assess patients’ and survivors’ access to vaccines as well as their willingness to get vaccinated.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
First pill for COVID-19 could be ready by year’s end
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.

Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
Meghan Markle interview resurfaces suicidality screening debate
An eye-opening moment during March 7’s Meghan Markle/Prince Harry interview with Oprah Winfrey was Markle’s admission that, before the royal couple moved from the U.K., she was suicidal and had nowhere to turn for help.

For health care practitioners, this has resurfaced the debate over universal suicidality screening and discussion about what should happen when patients screen positive.
The American Psychiatric Association reports suicide is the 10th leading cause of death in the United States, but the second leading cause of death in people age 10-34 years old.
The latest data from the Centers for Disease Control and Prevention show that, in 2019, suicide rates dropped for the first time in 14 years. However, it is widely expected that, in the face of the COVID-19 pandemic and its associated isolation, loneliness, and stress, the next round of data will show a surge in suicide deaths.
, chair of the APA’s Committee on Women’s Mental Health.
“I can see it in my office. People who didn’t necessarily complain about anxiety and depression before or who had been stable for many years are decompensating now,” Dr. De Faria said in an interview.
Although other parts of the interview may have been controversial, said Dr. De Faria, Markle’s disclosure has opened up a much-needed discussion.
“I’m all for people talking about mental health, and I commend [Markle] for sharing her struggle and putting it out there,” she added.
In a perfect world, she noted, there would be universal suicide screening by all medical professionals.
However, Dr. De Faria, associate clinical professor of psychiatry, University of Florida, Gainesville, acknowledged that from a resource standpoint this is not a pragmatic solution.
Primary care physicians are often the frontline defense for suicide prevention, noted Mona Masood, DO, a Philadelphia-area psychiatrist and founder and chief organizer of the Physician Support Line, a free mental health hotline exclusively for doctors staffed by volunteer psychiatrists.

“I believe our general practitioner colleagues, our family medicine colleagues are the ones who are going to be seeing the majority of mental health concerns or illnesses because of the stigma that is often there from seeing a psychiatrist,” Dr. Masood said in an interview.
Dr. De Faria noted that the Patient Health Questionnaire-2 (PHQ-2) for mental health offers a simple screen that includes two key questions. It asks: Over the last 2 weeks, how often have you been bothered by the following problems?
- Little interest or pleasure in doing things.
- Feeling down, depressed, or hopeless.
However, both Dr. De Faria and Dr. Masood emphasized that individualized follow-up questions and follow-up care are equally important.
Unlike Dr. De Faria, who prefers universal screening but understands the challenges of implementing it, Dr. Masood favors targeted screening.
“For physicians, the whole point of what we do is to save lives. To talk to somebody about the complete opposite and to ask, ‘Are you planning on ending your life?’ is very jarring. But for the patient, that may be their only outlet. A primary care provider may be the only professional that they talk to about their mental health,” said Dr. Masood.
Patients can easily say “no” to suicidal ideation questions from a general screen, but targeted, probing questions let patients know that they’re being heard and seen beyond their physical examination, she added.
She also suggested that clinicians ask open-ended questions of those patients who are struggling.
Dr. Masood noted that having a plan in place before screening a patient is especially key.
“I’d argue that one of the subconscious reasons why so many doctors do not ask the question [about suicidality] is because if you ask it, you have to be ready for the answer and to know what you’d do,” she said.
All primary care physicians should have “mental health professionals as resources in your back pocket” in order to have a referral ready to give to patients in need, she said.
“Outside of your clinic time, have a rapport with your local psychiatrist or therapist and know where to send someone who is suicidal,” Dr. Masood said. “Know what is in your local area so you’ll already know how to implement your plan.”
Dr. Masood also recommended:
- Informing staff about protocols for patients with suicidal thoughts who need to go to the hospital for evaluation.
- Creating a safe space in the clinic/office, such as an unused exam room, where patients can wait for next steps.
- Having staff inform a patient’s emergency contact about the situation.
- Trying for a “warm handoff,” where the emergency contact takes the patient to the nearest crisis center and having staff call ahead to let them know to expect the patient.
- If the patient has no emergency contact, following your state’s involuntary crisis response protocol, which involves calling 911 for emergency services.
In addition, the APA’s suicide prevention page includes a long list of helpful resources for patients, families, and physicians.
A version of this article first appeared on Medscape.com.
An eye-opening moment during March 7’s Meghan Markle/Prince Harry interview with Oprah Winfrey was Markle’s admission that, before the royal couple moved from the U.K., she was suicidal and had nowhere to turn for help.
For health care practitioners, this has resurfaced the debate over universal suicidality screening and discussion about what should happen when patients screen positive.
The American Psychiatric Association reports suicide is the 10th leading cause of death in the United States, but the second leading cause of death in people age 10-34 years old.
The latest data from the Centers for Disease Control and Prevention show that, in 2019, suicide rates dropped for the first time in 14 years. However, it is widely expected that, in the face of the COVID-19 pandemic and its associated isolation, loneliness, and stress, the next round of data will show a surge in suicide deaths.
, chair of the APA’s Committee on Women’s Mental Health.
“I can see it in my office. People who didn’t necessarily complain about anxiety and depression before or who had been stable for many years are decompensating now,” Dr. De Faria said in an interview.
Although other parts of the interview may have been controversial, said Dr. De Faria, Markle’s disclosure has opened up a much-needed discussion.
“I’m all for people talking about mental health, and I commend [Markle] for sharing her struggle and putting it out there,” she added.
In a perfect world, she noted, there would be universal suicide screening by all medical professionals.
However, Dr. De Faria, associate clinical professor of psychiatry, University of Florida, Gainesville, acknowledged that from a resource standpoint this is not a pragmatic solution.
Primary care physicians are often the frontline defense for suicide prevention, noted Mona Masood, DO, a Philadelphia-area psychiatrist and founder and chief organizer of the Physician Support Line, a free mental health hotline exclusively for doctors staffed by volunteer psychiatrists.
“I believe our general practitioner colleagues, our family medicine colleagues are the ones who are going to be seeing the majority of mental health concerns or illnesses because of the stigma that is often there from seeing a psychiatrist,” Dr. Masood said in an interview.
Dr. De Faria noted that the Patient Health Questionnaire-2 (PHQ-2) for mental health offers a simple screen that includes two key questions. It asks: Over the last 2 weeks, how often have you been bothered by the following problems?
- Little interest or pleasure in doing things.
- Feeling down, depressed, or hopeless.
However, both Dr. De Faria and Dr. Masood emphasized that individualized follow-up questions and follow-up care are equally important.
Unlike Dr. De Faria, who prefers universal screening but understands the challenges of implementing it, Dr. Masood favors targeted screening.
“For physicians, the whole point of what we do is to save lives. To talk to somebody about the complete opposite and to ask, ‘Are you planning on ending your life?’ is very jarring. But for the patient, that may be their only outlet. A primary care provider may be the only professional that they talk to about their mental health,” said Dr. Masood.
Patients can easily say “no” to suicidal ideation questions from a general screen, but targeted, probing questions let patients know that they’re being heard and seen beyond their physical examination, she added.
She also suggested that clinicians ask open-ended questions of those patients who are struggling.
Dr. Masood noted that having a plan in place before screening a patient is especially key.
“I’d argue that one of the subconscious reasons why so many doctors do not ask the question [about suicidality] is because if you ask it, you have to be ready for the answer and to know what you’d do,” she said.
All primary care physicians should have “mental health professionals as resources in your back pocket” in order to have a referral ready to give to patients in need, she said.
“Outside of your clinic time, have a rapport with your local psychiatrist or therapist and know where to send someone who is suicidal,” Dr. Masood said. “Know what is in your local area so you’ll already know how to implement your plan.”
Dr. Masood also recommended:
- Informing staff about protocols for patients with suicidal thoughts who need to go to the hospital for evaluation.
- Creating a safe space in the clinic/office, such as an unused exam room, where patients can wait for next steps.
- Having staff inform a patient’s emergency contact about the situation.
- Trying for a “warm handoff,” where the emergency contact takes the patient to the nearest crisis center and having staff call ahead to let them know to expect the patient.
- If the patient has no emergency contact, following your state’s involuntary crisis response protocol, which involves calling 911 for emergency services.
In addition, the APA’s suicide prevention page includes a long list of helpful resources for patients, families, and physicians.
A version of this article first appeared on Medscape.com.
An eye-opening moment during March 7’s Meghan Markle/Prince Harry interview with Oprah Winfrey was Markle’s admission that, before the royal couple moved from the U.K., she was suicidal and had nowhere to turn for help.
For health care practitioners, this has resurfaced the debate over universal suicidality screening and discussion about what should happen when patients screen positive.
The American Psychiatric Association reports suicide is the 10th leading cause of death in the United States, but the second leading cause of death in people age 10-34 years old.
The latest data from the Centers for Disease Control and Prevention show that, in 2019, suicide rates dropped for the first time in 14 years. However, it is widely expected that, in the face of the COVID-19 pandemic and its associated isolation, loneliness, and stress, the next round of data will show a surge in suicide deaths.
, chair of the APA’s Committee on Women’s Mental Health.
“I can see it in my office. People who didn’t necessarily complain about anxiety and depression before or who had been stable for many years are decompensating now,” Dr. De Faria said in an interview.
Although other parts of the interview may have been controversial, said Dr. De Faria, Markle’s disclosure has opened up a much-needed discussion.
“I’m all for people talking about mental health, and I commend [Markle] for sharing her struggle and putting it out there,” she added.
In a perfect world, she noted, there would be universal suicide screening by all medical professionals.
However, Dr. De Faria, associate clinical professor of psychiatry, University of Florida, Gainesville, acknowledged that from a resource standpoint this is not a pragmatic solution.
Primary care physicians are often the frontline defense for suicide prevention, noted Mona Masood, DO, a Philadelphia-area psychiatrist and founder and chief organizer of the Physician Support Line, a free mental health hotline exclusively for doctors staffed by volunteer psychiatrists.
“I believe our general practitioner colleagues, our family medicine colleagues are the ones who are going to be seeing the majority of mental health concerns or illnesses because of the stigma that is often there from seeing a psychiatrist,” Dr. Masood said in an interview.
Dr. De Faria noted that the Patient Health Questionnaire-2 (PHQ-2) for mental health offers a simple screen that includes two key questions. It asks: Over the last 2 weeks, how often have you been bothered by the following problems?
- Little interest or pleasure in doing things.
- Feeling down, depressed, or hopeless.
However, both Dr. De Faria and Dr. Masood emphasized that individualized follow-up questions and follow-up care are equally important.
Unlike Dr. De Faria, who prefers universal screening but understands the challenges of implementing it, Dr. Masood favors targeted screening.
“For physicians, the whole point of what we do is to save lives. To talk to somebody about the complete opposite and to ask, ‘Are you planning on ending your life?’ is very jarring. But for the patient, that may be their only outlet. A primary care provider may be the only professional that they talk to about their mental health,” said Dr. Masood.
Patients can easily say “no” to suicidal ideation questions from a general screen, but targeted, probing questions let patients know that they’re being heard and seen beyond their physical examination, she added.
She also suggested that clinicians ask open-ended questions of those patients who are struggling.
Dr. Masood noted that having a plan in place before screening a patient is especially key.
“I’d argue that one of the subconscious reasons why so many doctors do not ask the question [about suicidality] is because if you ask it, you have to be ready for the answer and to know what you’d do,” she said.
All primary care physicians should have “mental health professionals as resources in your back pocket” in order to have a referral ready to give to patients in need, she said.
“Outside of your clinic time, have a rapport with your local psychiatrist or therapist and know where to send someone who is suicidal,” Dr. Masood said. “Know what is in your local area so you’ll already know how to implement your plan.”
Dr. Masood also recommended:
- Informing staff about protocols for patients with suicidal thoughts who need to go to the hospital for evaluation.
- Creating a safe space in the clinic/office, such as an unused exam room, where patients can wait for next steps.
- Having staff inform a patient’s emergency contact about the situation.
- Trying for a “warm handoff,” where the emergency contact takes the patient to the nearest crisis center and having staff call ahead to let them know to expect the patient.
- If the patient has no emergency contact, following your state’s involuntary crisis response protocol, which involves calling 911 for emergency services.
In addition, the APA’s suicide prevention page includes a long list of helpful resources for patients, families, and physicians.
A version of this article first appeared on Medscape.com.

Swallowable capsule-camera may reveal GI cancers, diseases
A miniature camera the size of a capsule that is swallowed and then transmits images of the inside of the gut can reveal cancer and gastrointestinal diseases. The device, which will be studied in a trial conducted by the National Health Service in England, is used by patients at home as a substitute for endoscopy.
“What sounds like sci-fi is now becoming a reality,” said Sir Simon Stevens, chief executive of NHS England. “These minute cameras pass through your body. They take two pictures per second, checking for signs of cancer and other conditions like Crohn’s disease.”
The trial, announced on March 11, 2021, will initially involve 11,000 patients from 40 regions in England. Participants will be sent the colon capsule endoscopy to use at home.
The capsule typically takes 5-8 hours to pass through the digestive system. As the capsule passes through the bowel, images are sent to a data recorder in a shoulder bag.
The trial is being conducted by the University College London Hospitals NHS Foundation Trust. The investigators have created a guide on using the device at home.
“Not only does colon capsule increase our diagnostic capacity, because it doesn’t require the resources of a dedicated hospital space to do the examination, it also allows us to do the examination in the patient’s home, so patients who may be shielding or cautious about going to a hospital can perform the procedure in the comfort of their own homes,” commented Ed Seward, MD, PhD, endoscopy lead at UCL.
The move is in response to a surge in patients coming forward for cancer checks after the slowdown in cancer services caused by the COVID-19 pandemic. In December 2020, more than 200,000 people came forward, an increase of 13,000 over the same month the previous year.
Traditional endoscopy services are still being offered, although endoscopies take longer to conduct because of infection control measures that must be employed to ensure that patients who undergo endoscopies do not develop COVID-19. This, in turn, means fewer people can undergo endoscopies over a given period.
“We welcome any initiative that seeks to simplify and improve the early diagnosis of gastrointestinal disease and, in particular, colorectal cancer, which unfortunately is still responsible for many avoidable deaths,” said Alastair McKinlay, MD, president of the British Society of Gastroenterology.
“Colon capsule is a promising new technology that may offer a real advantage for some patients. For this reason, we welcome the opportunity for a proper service evaluation so that both the limitations and advantages of this technique can be properly assessed,” he said.
“This has the potential to make a huge difference for people with bowel cancer symptoms and could help the NHS to prioritize those who urgently need further tests,” added Genevieve Edwards, chief executive at Bowel Cancer UK.
No funding for the study has been disclosed. No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
A miniature camera the size of a capsule that is swallowed and then transmits images of the inside of the gut can reveal cancer and gastrointestinal diseases. The device, which will be studied in a trial conducted by the National Health Service in England, is used by patients at home as a substitute for endoscopy.
“What sounds like sci-fi is now becoming a reality,” said Sir Simon Stevens, chief executive of NHS England. “These minute cameras pass through your body. They take two pictures per second, checking for signs of cancer and other conditions like Crohn’s disease.”
The trial, announced on March 11, 2021, will initially involve 11,000 patients from 40 regions in England. Participants will be sent the colon capsule endoscopy to use at home.
The capsule typically takes 5-8 hours to pass through the digestive system. As the capsule passes through the bowel, images are sent to a data recorder in a shoulder bag.
The trial is being conducted by the University College London Hospitals NHS Foundation Trust. The investigators have created a guide on using the device at home.
“Not only does colon capsule increase our diagnostic capacity, because it doesn’t require the resources of a dedicated hospital space to do the examination, it also allows us to do the examination in the patient’s home, so patients who may be shielding or cautious about going to a hospital can perform the procedure in the comfort of their own homes,” commented Ed Seward, MD, PhD, endoscopy lead at UCL.
The move is in response to a surge in patients coming forward for cancer checks after the slowdown in cancer services caused by the COVID-19 pandemic. In December 2020, more than 200,000 people came forward, an increase of 13,000 over the same month the previous year.
Traditional endoscopy services are still being offered, although endoscopies take longer to conduct because of infection control measures that must be employed to ensure that patients who undergo endoscopies do not develop COVID-19. This, in turn, means fewer people can undergo endoscopies over a given period.
“We welcome any initiative that seeks to simplify and improve the early diagnosis of gastrointestinal disease and, in particular, colorectal cancer, which unfortunately is still responsible for many avoidable deaths,” said Alastair McKinlay, MD, president of the British Society of Gastroenterology.
“Colon capsule is a promising new technology that may offer a real advantage for some patients. For this reason, we welcome the opportunity for a proper service evaluation so that both the limitations and advantages of this technique can be properly assessed,” he said.
“This has the potential to make a huge difference for people with bowel cancer symptoms and could help the NHS to prioritize those who urgently need further tests,” added Genevieve Edwards, chief executive at Bowel Cancer UK.
No funding for the study has been disclosed. No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
A miniature camera the size of a capsule that is swallowed and then transmits images of the inside of the gut can reveal cancer and gastrointestinal diseases. The device, which will be studied in a trial conducted by the National Health Service in England, is used by patients at home as a substitute for endoscopy.
“What sounds like sci-fi is now becoming a reality,” said Sir Simon Stevens, chief executive of NHS England. “These minute cameras pass through your body. They take two pictures per second, checking for signs of cancer and other conditions like Crohn’s disease.”
The trial, announced on March 11, 2021, will initially involve 11,000 patients from 40 regions in England. Participants will be sent the colon capsule endoscopy to use at home.
The capsule typically takes 5-8 hours to pass through the digestive system. As the capsule passes through the bowel, images are sent to a data recorder in a shoulder bag.
The trial is being conducted by the University College London Hospitals NHS Foundation Trust. The investigators have created a guide on using the device at home.
“Not only does colon capsule increase our diagnostic capacity, because it doesn’t require the resources of a dedicated hospital space to do the examination, it also allows us to do the examination in the patient’s home, so patients who may be shielding or cautious about going to a hospital can perform the procedure in the comfort of their own homes,” commented Ed Seward, MD, PhD, endoscopy lead at UCL.
The move is in response to a surge in patients coming forward for cancer checks after the slowdown in cancer services caused by the COVID-19 pandemic. In December 2020, more than 200,000 people came forward, an increase of 13,000 over the same month the previous year.
Traditional endoscopy services are still being offered, although endoscopies take longer to conduct because of infection control measures that must be employed to ensure that patients who undergo endoscopies do not develop COVID-19. This, in turn, means fewer people can undergo endoscopies over a given period.
“We welcome any initiative that seeks to simplify and improve the early diagnosis of gastrointestinal disease and, in particular, colorectal cancer, which unfortunately is still responsible for many avoidable deaths,” said Alastair McKinlay, MD, president of the British Society of Gastroenterology.
“Colon capsule is a promising new technology that may offer a real advantage for some patients. For this reason, we welcome the opportunity for a proper service evaluation so that both the limitations and advantages of this technique can be properly assessed,” he said.
“This has the potential to make a huge difference for people with bowel cancer symptoms and could help the NHS to prioritize those who urgently need further tests,” added Genevieve Edwards, chief executive at Bowel Cancer UK.
No funding for the study has been disclosed. No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.