User login
Long COVID seen in patients with severe and mild disease
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.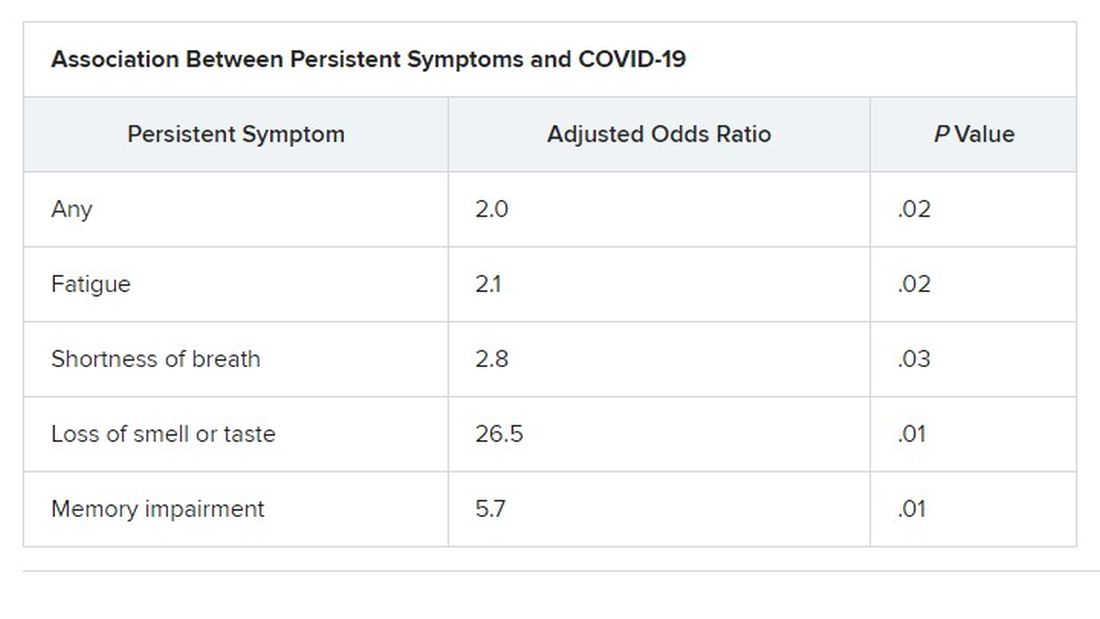
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Findings from the cohort, composed of 113 COVID-19 survivors who developed ARDS after admission to a single center before to April 16, 2020, were presented online at the 31st European Congress of Clinical Microbiology & Infectious Diseases by Judit Aranda, MD, from Complex Hospitalari Moisés Broggi in Barcelona.
Median age of the participants was 64 years, and 70% were male. At least one persistent symptom was experienced during follow-up by 81% of the cohort, with 45% reporting shortness of breath, 50% reporting muscle pain, 43% reporting memory impairment, and 46% reporting physical weakness of at least 5 on a 10-point scale.
Of the 104 participants who completed a 6-minute walk test, 30% had a decrease in oxygen saturation level of at least 4%, and 5% had an initial or final level below 88%. Of the 46 participants who underwent a pulmonary function test, 15% had a forced expiratory volume in 1 second below 70%.
And of the 49% of participants with pathologic findings on chest x-ray, most were bilateral interstitial infiltrates (88%).
In addition, more than 90% of participants developed depression, anxiety, or PTSD, Dr. Aranda reported.
Not the whole picture
This study shows that sicker people – “those in intensive care units with acute respiratory distress syndrome” – are “more likely to be struggling with more severe symptoms,” said Christopher Terndrup, MD, from the division of general internal medicine and geriatrics at Oregon Health & Science University, Portland.
But a Swiss study, also presented at the meeting, “shows how even mild COVID cases can lead to debilitating symptoms,” Dr. Terndrup said in an interview.
The investigation of long-term COVID symptoms in outpatients was presented online by Florian Desgranges, MD, from Lausanne (Switzerland) University Hospital. He and his colleagues found that more than half of those with a mild to moderate disease had persistent symptoms at least 3 months after diagnosis.
The prevalence of long COVID has varied in previous research, from 15% in a study of health care workers, to 46% in a study of patients with mild COVID, 52% in a study of young COVID outpatients, and 76% in a study of patients hospitalized with COVID.
Dr. Desgranges and colleagues evaluated patients seen in an ED or outpatient clinic from February to April 2020.
The 418 patients with a confirmed COVID-19 diagnosis were compared with a control group of 89 patients who presented to the same centers during the same time frame with similar symptoms – cough, shortness of breath, or fever – but had a negative SARS-CoV-2 test.
The number of patients with comorbidities was similar in the COVID and control groups (34% vs. 36%), as was median age (41 vs. 36 years) and the prevalence of women (62% vs 64%), but the proportion of health care workers was lower in the COVID group (64% vs 82%; P =.006).
Symptoms that persisted for at least 3 months were more common in the COVID than in the control group (53% vs. 37%). And patients in the COVID group reported more symptoms than those in the control group after adjustment for age, gender, smoking status, comorbidities, and timing of the survey phone call.
Levels of sleeping problems and headache were similar in the two groups.
“We have to remember that with COVID-19 came the psychosocial changes of the pandemic situation” Dr. Desgranges said.
This study suggests that some long-COVID symptoms – such as the fatigue, headache, and sleep disorders reported in the control group – could be related to the pandemic itself, which has caused psychosocial distress, Dr. Terndrup said.
Another study that looked at outpatients “has some fantastic long-term follow-up data, and shows that many patients are still engaging in rehabilitation programs nearly a year after their diagnosis,” he explained.
The COVID HOME study
That prospective longitudinal COVID HOME study, which assessed long-term symptoms in people who were never hospitalized for COVID, was presented online by Adriana Tami, MD, PhD, from the University Medical Center Groningen (the Netherlands).
The researchers visited the homes of patients to collect data, blood samples, and perform polymerase chain reaction (PCR) testing 1, 2, and 3 weeks after a diagnosis of COVID-19. If their PCR test was still positive, testing continued until week 6 or a negative test. In addition, participants completed questionnaires at week 2 and at months 3, 6 and 12 to assess fatigue, quality of life, and symptoms of depression and anxiety.
Three-month follow-up data were available for 134 of the 276 people initially enrolled in the study. Questionnaires were completed by 85 participants at 3 months, 62 participants at 6 months, and 10 participants at 12 months.
At least 40% of participants reported long-lasting symptoms at some point during follow-up, and at least 30% said they didn’t feel fully recovered at 12 months. The most common symptom was persistent fatigue, reported at 3, 6, and 12 months by at least 44% of participants. Other common symptoms – reported by at least 20% of respondents at 3, 6, and 12 months – were headache, mental or neurologic symptoms, and sleep disorders, shortness of breath, lack of smell or taste, and severe fatigue.
“We have a high proportion of nonhospitalized individuals who suffer from long COVID after more than 12 months,” Dr. Tami concluded, adding that the study is ongoing. “We have other variables that we want to look at, including duration viral shedding and serological results and variants.”
“These cohort studies are very helpful, but they can lead to inaccurate conclusions,” Dr. Terndrup cautioned.
They only provide pieces of the big picture, but they “do add to a growing body of knowledge about a significant portion of COVID patients still struggling with symptoms long after their initial infection. The symptoms can be quite variable but are dominated by both physical and mental fatigue, and tend to be worse in patients who were sicker at initial infection,” he said in an interview.
As a whole, these studies reinforce the need for treatment programs to help patients who suffer from long COVID, he added, but “I advise caution to folks suffering out there who seek ‘miracle cures’; across the world, we are collaborating to find solutions that are safe and effective.”
We are in desperate need of an equity lens in these studies.
“There is still a great deal to learn about long COVID,” said Dr. Terndrup. Data on underrepresented populations – such as Black, Indigenous, and people of color – are lacking from these and others studies, he explained. “We are in desperate need of an equity lens in these studies,” particularly in the United States, where there are “significant disparities” in the treatment of different populations.
However, “I do hope that this work can lead to a better understanding of how other viral infections can cause long-lasting symptoms,” said Dr. Terndrup.
“We have long proposed that after acute presentation, some microbes can cause chronic symptoms, like fatigue and widespread pain. Perhaps we can learn how to better care for these patients after learning from COVID’s significant impact on our societies across the globe.”
Dr. Aranda and Dr. Desgranges have disclosed no relevant financial relationships or study funding. The study by Dr. Tami’s team was funded by the University Medical Center Groningen Organization for Health Research and Development, and Connecting European Cohorts to Increase Common and Effective Response to SARS-CoV-2 Pandemic. Dr. Terndrup disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN CONGRESS OF CLINICAL MICROBIOLOGY & INFECTIOUS DISEASES
Recent trend: Melanoma mortality declining rapidly
according to an annual report by several national organizations.
“Death rates for cutaneous melanoma have declined rapidly in recent years following introduction of new therapies, including targeted and immune checkpoint inhibitors, the first of which was approved by the [Food and Drug Administration] in early 2011,” Farhad Islami, MD, PhD, of the American Cancer Society, and associates wrote in the Journal of the National Cancer Institute.
The American Cancer Society, along with the Centers for Disease Control and Prevention, the National Cancer Institute, and the North American Association of Central Cancer Registries, issue a joint report each year to update the incidence and mortality of the most common cancers and analyze short- and long-term trends since 2001.
Long-term melanoma mortality gets divided into two trends: First a slow decline over about a decade, then an accelerated decline until the end of the study period, although the timing is slightly different between males and females. For men, the death rate fell by an average of 0.9% a year from 2001 to 2009, compared with 5.7% per year in 2013-2018. For women, the average annual change went from –0.3% for 2001-2012 to –4.4% in 2012-2018.
The incidence of melanoma, however, headed in the opposite direction, rising 1.9% per year for females and 2.2% for males from 2001 to 2017, without the notable change in trend seen with death rates, Dr. Islami and associates said.
Incidence by race/ethnicity, reported for 2013-2017, shows that melanoma is much more common among white non-Hispanics: 37.4 per 100,000 standard population for males and 24.5 for females. Non-Hispanic American Indians/Alaska Natives were next at 10.8 (men) and 6.7 (women), followed by Hispanics (5.1/4.5), non-Hispanic Asians/Pacific Islanders (1.6/1.3), and non-Hispanic Blacks (1.2/1.0), they reported.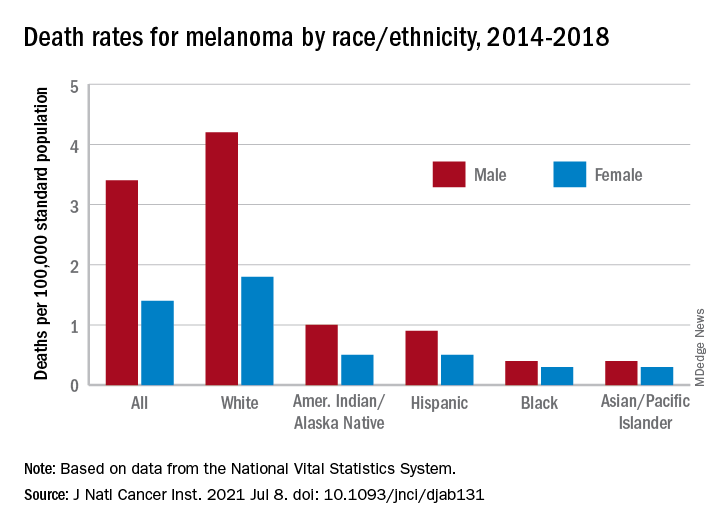
Death rates for melanoma, reported for 2014-2018, follow a similar pattern. White males (4.2 per 100,000) and females (1.8 per 100,000) had the highest mortality, then American Indians/Alaska Natives (1.0/0.5) and Hispanics (0.9/0.5), but rates were the same for Blacks and Asians/Pacific Islanders (0.4/0.3), the investigators said.
The accelerated decline in death rates in more recent years reflects “a substantial increase in survival for metastatic melanoma,” the participating organizations noted in a joint statement.
Increases in 2-year survival in distant-stage disease averaged 3.1% per year for those diagnosed during 2009-2014, which “slightly preceded the FDA approval of new therapies, likely because of the administration of these therapies through clinical trials and the FDA expanded access programs prior to the approval,” Dr. Islami and associates wrote.
The 2-year relative survival for those with nonmetastatic melanoma also improved over the study period, but the increases were much smaller: 0.4% per year for regional-stage disease and just 0.03% localized-stage cases diagnosed in 2001-2014, they reported.
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
according to an annual report by several national organizations.
“Death rates for cutaneous melanoma have declined rapidly in recent years following introduction of new therapies, including targeted and immune checkpoint inhibitors, the first of which was approved by the [Food and Drug Administration] in early 2011,” Farhad Islami, MD, PhD, of the American Cancer Society, and associates wrote in the Journal of the National Cancer Institute.
The American Cancer Society, along with the Centers for Disease Control and Prevention, the National Cancer Institute, and the North American Association of Central Cancer Registries, issue a joint report each year to update the incidence and mortality of the most common cancers and analyze short- and long-term trends since 2001.
Long-term melanoma mortality gets divided into two trends: First a slow decline over about a decade, then an accelerated decline until the end of the study period, although the timing is slightly different between males and females. For men, the death rate fell by an average of 0.9% a year from 2001 to 2009, compared with 5.7% per year in 2013-2018. For women, the average annual change went from –0.3% for 2001-2012 to –4.4% in 2012-2018.
The incidence of melanoma, however, headed in the opposite direction, rising 1.9% per year for females and 2.2% for males from 2001 to 2017, without the notable change in trend seen with death rates, Dr. Islami and associates said.
Incidence by race/ethnicity, reported for 2013-2017, shows that melanoma is much more common among white non-Hispanics: 37.4 per 100,000 standard population for males and 24.5 for females. Non-Hispanic American Indians/Alaska Natives were next at 10.8 (men) and 6.7 (women), followed by Hispanics (5.1/4.5), non-Hispanic Asians/Pacific Islanders (1.6/1.3), and non-Hispanic Blacks (1.2/1.0), they reported.
Death rates for melanoma, reported for 2014-2018, follow a similar pattern. White males (4.2 per 100,000) and females (1.8 per 100,000) had the highest mortality, then American Indians/Alaska Natives (1.0/0.5) and Hispanics (0.9/0.5), but rates were the same for Blacks and Asians/Pacific Islanders (0.4/0.3), the investigators said.
The accelerated decline in death rates in more recent years reflects “a substantial increase in survival for metastatic melanoma,” the participating organizations noted in a joint statement.
Increases in 2-year survival in distant-stage disease averaged 3.1% per year for those diagnosed during 2009-2014, which “slightly preceded the FDA approval of new therapies, likely because of the administration of these therapies through clinical trials and the FDA expanded access programs prior to the approval,” Dr. Islami and associates wrote.
The 2-year relative survival for those with nonmetastatic melanoma also improved over the study period, but the increases were much smaller: 0.4% per year for regional-stage disease and just 0.03% localized-stage cases diagnosed in 2001-2014, they reported.
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
according to an annual report by several national organizations.
“Death rates for cutaneous melanoma have declined rapidly in recent years following introduction of new therapies, including targeted and immune checkpoint inhibitors, the first of which was approved by the [Food and Drug Administration] in early 2011,” Farhad Islami, MD, PhD, of the American Cancer Society, and associates wrote in the Journal of the National Cancer Institute.
The American Cancer Society, along with the Centers for Disease Control and Prevention, the National Cancer Institute, and the North American Association of Central Cancer Registries, issue a joint report each year to update the incidence and mortality of the most common cancers and analyze short- and long-term trends since 2001.
Long-term melanoma mortality gets divided into two trends: First a slow decline over about a decade, then an accelerated decline until the end of the study period, although the timing is slightly different between males and females. For men, the death rate fell by an average of 0.9% a year from 2001 to 2009, compared with 5.7% per year in 2013-2018. For women, the average annual change went from –0.3% for 2001-2012 to –4.4% in 2012-2018.
The incidence of melanoma, however, headed in the opposite direction, rising 1.9% per year for females and 2.2% for males from 2001 to 2017, without the notable change in trend seen with death rates, Dr. Islami and associates said.
Incidence by race/ethnicity, reported for 2013-2017, shows that melanoma is much more common among white non-Hispanics: 37.4 per 100,000 standard population for males and 24.5 for females. Non-Hispanic American Indians/Alaska Natives were next at 10.8 (men) and 6.7 (women), followed by Hispanics (5.1/4.5), non-Hispanic Asians/Pacific Islanders (1.6/1.3), and non-Hispanic Blacks (1.2/1.0), they reported.
Death rates for melanoma, reported for 2014-2018, follow a similar pattern. White males (4.2 per 100,000) and females (1.8 per 100,000) had the highest mortality, then American Indians/Alaska Natives (1.0/0.5) and Hispanics (0.9/0.5), but rates were the same for Blacks and Asians/Pacific Islanders (0.4/0.3), the investigators said.
The accelerated decline in death rates in more recent years reflects “a substantial increase in survival for metastatic melanoma,” the participating organizations noted in a joint statement.
Increases in 2-year survival in distant-stage disease averaged 3.1% per year for those diagnosed during 2009-2014, which “slightly preceded the FDA approval of new therapies, likely because of the administration of these therapies through clinical trials and the FDA expanded access programs prior to the approval,” Dr. Islami and associates wrote.
The 2-year relative survival for those with nonmetastatic melanoma also improved over the study period, but the increases were much smaller: 0.4% per year for regional-stage disease and just 0.03% localized-stage cases diagnosed in 2001-2014, they reported.
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Drinking coffee not linked to increased arrhythmia risk in new study
In fact, an adjusted analysis found that “each additional cup of coffee intake was associated with a 3% lower risk of incident arrhythmia,” Eun-jeong Kim, MD, of the division of cardiology at the University of California, San Francisco, and colleagues reported in JAMA Internal Medicine.
In addition, genetic differences that affect caffeine metabolism did not significantly influence the odds of arrhythmias, the researchers found.
Still, these findings should not necessarily encourage people to start drinking coffee if they don’t already, or to guzzle additional cups with abandon, they said.

“We certainly don’t want to say drink coffee and it will reduce your risk of arrhythmias,” study author Gregory M. Marcus, MD, MAS, associate chief of cardiology for research at UCSF Health, said in an interview. “But rather, we think the main point is that a blanket prohibition against coffee or caffeine to reduce the risk of arrhythmias among patients who have a diagnosis of arrhythmias is likely unwarranted. And given some evidence that coffee consumption may actually have other benefits regarding diabetes, mood, and perhaps overall mortality, it may be problematic to admonish patients to avoid coffee or caffeine when it is not really warranted.”
Methods and results
The conventional wisdom that caffeine increases arrhythmic risk has not been well substantiated. To further examine whether moderate, habitual coffee drinking relates to arrhythmia risk, and whether certain genetic variants influence the association, Dr. Kim and colleagues analyzed data from the UK Biobank. They focused on longitudinal data collected between 2006 and 2018 from 386,258 people who did not have a prior diagnosis of arrhythmia.
Participants had an average age of 56 years, and about 52% were female. They provided information about their coffee consumption, and the researchers grouped the participants into eight categories based on their daily coffee intake: 0, less than 1, 1, 2, 3, 4, 5, and 6 or more cups per day.
Over an average follow-up of 4.5 years, 16,979 participants developed an incident arrhythmia. After adjusting for demographic characteristics, comorbid conditions, and lifestyle habits, the decreased risk with each cup of coffee was similar for atrial fibrillation or flutter (hazard ratio, 0.97) and supraventricular tachycardia (HR, 0.96).
Taking into account genetic variations that relate to caffeine metabolism did not modify the findings. Mendelian randomization analyses that used a polygenic score of inherited caffeine metabolism patterns “failed to provide evidence that caffeine consumption leads to a greater risk of arrhythmias,” the researchers said.
Professional society guidelines have suggested staying away from caffeinated products to reduce the risk of arrhythmia, but this guidance has “relied on assumed mechanisms and a small observational study from 1980,” the authors wrote. Subsequent research has indicated that coffee’s reputation of increasing the risk of arrhythmia may be undeserved.
“The investigators should be commended on performing a high-quality observational study to try to further understand the association between coffee consumption and arrhythmias, or the lack of one,” commented Zachary D. Goldberger, MD, MS, with the division of cardiovascular medicine at the University of Wisconsin–Madison, who was not involved in the study. “This is not a randomized, controlled trial, and coffee consumption was self-reported, but the methods employed are rigorous, despite these and other important limitations. However, we need to be extremely cautious in how we interpret these findings, and not use these data as a prescription for more coffee. It’s important to recognize that this study is not telling us to drink more coffee, or start drinking coffee, to protect against developing arrhythmias. However, it should offer more reassurance that moderate coffee consumption is not necessarily harmful, and will not always lead to arrhythmias. This is important, given the widespread notion that coffee is universally proarrhythmic.”
A call for personalized guidance
“As the investigators note, there are definitely biologically plausible reasons how coffee and caffeine may not cause arrhythmias, and may be possibly protective in some, despite being a stimulant,” Dr. Goldberger said. “However, if your patient is reporting palpitations or symptoms of an arrhythmia, and feels they be related to coffee or caffeine, we should not use this study to tell them that coffee may not be the culprit. We need to listen to our patients, and the decision to reduce coffee consumption to reduce these symptoms needs to be personalized.”
The effect size was small, and only about 4% of the participants developed an arrhythmia, Dr. Goldberger and Rodney A. Hayward, MD, wrote in an invited commentary on the study in JAMA Internal Medicine. Dr. Hayward is a professor of public health and internal medicine at the University of Michigan, Ann Arbor, and a senior investigator at the Ann Arbor Veterans Affairs Center for Clinical Management Research.
“Unfortunately, coffee consumption was self-reported at a single time point. Not only can this lead to recall bias, but subsequent and substantial changes in coffee consumption are also possible, including reductions due to new signs or symptoms,” they said.
No evidence that coffee ups risk for developing arrhythmias
Another recent study suggests that people may alter their coffee consumption depending on their baseline cardiovascular health, according to the commentary.
Overall, the results “strengthen the evidence that caffeine is not proarrhythmic, but they should not be taken as proving that coffee is an antiarrhythmic—this distinction is of paramount importance,” Dr. Goldberger and Dr. Hayward wrote. “Health care professionals can reassure patients that there is no evidence that drinking coffee increases the risk for developing arrhythmias. This is particularly important for the many patients with benign palpitations who are devastated when they think, or are told, that they have to stop drinking coffee. Given current evidence, this is entirely a patient-preference decision, not a medical one.”
Dr. Marcus, a cardiac electrophysiologist, sees patients with arrhythmias all the time. They tend to “come in fairly convinced that caffeine is to be avoided when they have arrhythmias,” he said. “Often, they been told by their primary care physician or their general cardiologist to avoid caffeine because they have an arrhythmia.
“What I suggest to my patients is that they feel free to go ahead and experiment and try coffee,” Dr. Marcus said.
Still, Dr. Marcus suspects that there are some individuals in whom caffeine is a trigger for the arrhythmia. But evidence indicates these cases likely are rare, and avoiding caffeine need not apply to the general population, particularly “given the potential health benefits of benefits of coffee and also, frankly, just the enhanced quality of life that people can enjoy drinking a good cup of coffee.”
The research was conducted using the UK Biobank resource, which was established by the Wellcome Trust, the Medical Research Council, the U.K. Department of Health, and the Scottish government. The UK Biobank has received funding from other agencies and foundations as well. Dr. Marcus disclosed grants from Baylis, Medtronic, and Eight Sleep outside the submitted work. In addition, he reported consulting for Johnson & Johnson and InCarda, and holding equity in InCarda. A coauthor received salary support from the National Institutes of Health during the study. Dr. Goldberger and Dr. Hayward disclosed no conflicts of interest.
In fact, an adjusted analysis found that “each additional cup of coffee intake was associated with a 3% lower risk of incident arrhythmia,” Eun-jeong Kim, MD, of the division of cardiology at the University of California, San Francisco, and colleagues reported in JAMA Internal Medicine.
In addition, genetic differences that affect caffeine metabolism did not significantly influence the odds of arrhythmias, the researchers found.
Still, these findings should not necessarily encourage people to start drinking coffee if they don’t already, or to guzzle additional cups with abandon, they said.
“We certainly don’t want to say drink coffee and it will reduce your risk of arrhythmias,” study author Gregory M. Marcus, MD, MAS, associate chief of cardiology for research at UCSF Health, said in an interview. “But rather, we think the main point is that a blanket prohibition against coffee or caffeine to reduce the risk of arrhythmias among patients who have a diagnosis of arrhythmias is likely unwarranted. And given some evidence that coffee consumption may actually have other benefits regarding diabetes, mood, and perhaps overall mortality, it may be problematic to admonish patients to avoid coffee or caffeine when it is not really warranted.”
Methods and results
The conventional wisdom that caffeine increases arrhythmic risk has not been well substantiated. To further examine whether moderate, habitual coffee drinking relates to arrhythmia risk, and whether certain genetic variants influence the association, Dr. Kim and colleagues analyzed data from the UK Biobank. They focused on longitudinal data collected between 2006 and 2018 from 386,258 people who did not have a prior diagnosis of arrhythmia.
Participants had an average age of 56 years, and about 52% were female. They provided information about their coffee consumption, and the researchers grouped the participants into eight categories based on their daily coffee intake: 0, less than 1, 1, 2, 3, 4, 5, and 6 or more cups per day.
Over an average follow-up of 4.5 years, 16,979 participants developed an incident arrhythmia. After adjusting for demographic characteristics, comorbid conditions, and lifestyle habits, the decreased risk with each cup of coffee was similar for atrial fibrillation or flutter (hazard ratio, 0.97) and supraventricular tachycardia (HR, 0.96).
Taking into account genetic variations that relate to caffeine metabolism did not modify the findings. Mendelian randomization analyses that used a polygenic score of inherited caffeine metabolism patterns “failed to provide evidence that caffeine consumption leads to a greater risk of arrhythmias,” the researchers said.
Professional society guidelines have suggested staying away from caffeinated products to reduce the risk of arrhythmia, but this guidance has “relied on assumed mechanisms and a small observational study from 1980,” the authors wrote. Subsequent research has indicated that coffee’s reputation of increasing the risk of arrhythmia may be undeserved.
“The investigators should be commended on performing a high-quality observational study to try to further understand the association between coffee consumption and arrhythmias, or the lack of one,” commented Zachary D. Goldberger, MD, MS, with the division of cardiovascular medicine at the University of Wisconsin–Madison, who was not involved in the study. “This is not a randomized, controlled trial, and coffee consumption was self-reported, but the methods employed are rigorous, despite these and other important limitations. However, we need to be extremely cautious in how we interpret these findings, and not use these data as a prescription for more coffee. It’s important to recognize that this study is not telling us to drink more coffee, or start drinking coffee, to protect against developing arrhythmias. However, it should offer more reassurance that moderate coffee consumption is not necessarily harmful, and will not always lead to arrhythmias. This is important, given the widespread notion that coffee is universally proarrhythmic.”
A call for personalized guidance
“As the investigators note, there are definitely biologically plausible reasons how coffee and caffeine may not cause arrhythmias, and may be possibly protective in some, despite being a stimulant,” Dr. Goldberger said. “However, if your patient is reporting palpitations or symptoms of an arrhythmia, and feels they be related to coffee or caffeine, we should not use this study to tell them that coffee may not be the culprit. We need to listen to our patients, and the decision to reduce coffee consumption to reduce these symptoms needs to be personalized.”
The effect size was small, and only about 4% of the participants developed an arrhythmia, Dr. Goldberger and Rodney A. Hayward, MD, wrote in an invited commentary on the study in JAMA Internal Medicine. Dr. Hayward is a professor of public health and internal medicine at the University of Michigan, Ann Arbor, and a senior investigator at the Ann Arbor Veterans Affairs Center for Clinical Management Research.
“Unfortunately, coffee consumption was self-reported at a single time point. Not only can this lead to recall bias, but subsequent and substantial changes in coffee consumption are also possible, including reductions due to new signs or symptoms,” they said.
No evidence that coffee ups risk for developing arrhythmias
Another recent study suggests that people may alter their coffee consumption depending on their baseline cardiovascular health, according to the commentary.
Overall, the results “strengthen the evidence that caffeine is not proarrhythmic, but they should not be taken as proving that coffee is an antiarrhythmic—this distinction is of paramount importance,” Dr. Goldberger and Dr. Hayward wrote. “Health care professionals can reassure patients that there is no evidence that drinking coffee increases the risk for developing arrhythmias. This is particularly important for the many patients with benign palpitations who are devastated when they think, or are told, that they have to stop drinking coffee. Given current evidence, this is entirely a patient-preference decision, not a medical one.”
Dr. Marcus, a cardiac electrophysiologist, sees patients with arrhythmias all the time. They tend to “come in fairly convinced that caffeine is to be avoided when they have arrhythmias,” he said. “Often, they been told by their primary care physician or their general cardiologist to avoid caffeine because they have an arrhythmia.
“What I suggest to my patients is that they feel free to go ahead and experiment and try coffee,” Dr. Marcus said.
Still, Dr. Marcus suspects that there are some individuals in whom caffeine is a trigger for the arrhythmia. But evidence indicates these cases likely are rare, and avoiding caffeine need not apply to the general population, particularly “given the potential health benefits of benefits of coffee and also, frankly, just the enhanced quality of life that people can enjoy drinking a good cup of coffee.”
The research was conducted using the UK Biobank resource, which was established by the Wellcome Trust, the Medical Research Council, the U.K. Department of Health, and the Scottish government. The UK Biobank has received funding from other agencies and foundations as well. Dr. Marcus disclosed grants from Baylis, Medtronic, and Eight Sleep outside the submitted work. In addition, he reported consulting for Johnson & Johnson and InCarda, and holding equity in InCarda. A coauthor received salary support from the National Institutes of Health during the study. Dr. Goldberger and Dr. Hayward disclosed no conflicts of interest.
In fact, an adjusted analysis found that “each additional cup of coffee intake was associated with a 3% lower risk of incident arrhythmia,” Eun-jeong Kim, MD, of the division of cardiology at the University of California, San Francisco, and colleagues reported in JAMA Internal Medicine.
In addition, genetic differences that affect caffeine metabolism did not significantly influence the odds of arrhythmias, the researchers found.
Still, these findings should not necessarily encourage people to start drinking coffee if they don’t already, or to guzzle additional cups with abandon, they said.
“We certainly don’t want to say drink coffee and it will reduce your risk of arrhythmias,” study author Gregory M. Marcus, MD, MAS, associate chief of cardiology for research at UCSF Health, said in an interview. “But rather, we think the main point is that a blanket prohibition against coffee or caffeine to reduce the risk of arrhythmias among patients who have a diagnosis of arrhythmias is likely unwarranted. And given some evidence that coffee consumption may actually have other benefits regarding diabetes, mood, and perhaps overall mortality, it may be problematic to admonish patients to avoid coffee or caffeine when it is not really warranted.”
Methods and results
The conventional wisdom that caffeine increases arrhythmic risk has not been well substantiated. To further examine whether moderate, habitual coffee drinking relates to arrhythmia risk, and whether certain genetic variants influence the association, Dr. Kim and colleagues analyzed data from the UK Biobank. They focused on longitudinal data collected between 2006 and 2018 from 386,258 people who did not have a prior diagnosis of arrhythmia.
Participants had an average age of 56 years, and about 52% were female. They provided information about their coffee consumption, and the researchers grouped the participants into eight categories based on their daily coffee intake: 0, less than 1, 1, 2, 3, 4, 5, and 6 or more cups per day.
Over an average follow-up of 4.5 years, 16,979 participants developed an incident arrhythmia. After adjusting for demographic characteristics, comorbid conditions, and lifestyle habits, the decreased risk with each cup of coffee was similar for atrial fibrillation or flutter (hazard ratio, 0.97) and supraventricular tachycardia (HR, 0.96).
Taking into account genetic variations that relate to caffeine metabolism did not modify the findings. Mendelian randomization analyses that used a polygenic score of inherited caffeine metabolism patterns “failed to provide evidence that caffeine consumption leads to a greater risk of arrhythmias,” the researchers said.
Professional society guidelines have suggested staying away from caffeinated products to reduce the risk of arrhythmia, but this guidance has “relied on assumed mechanisms and a small observational study from 1980,” the authors wrote. Subsequent research has indicated that coffee’s reputation of increasing the risk of arrhythmia may be undeserved.
“The investigators should be commended on performing a high-quality observational study to try to further understand the association between coffee consumption and arrhythmias, or the lack of one,” commented Zachary D. Goldberger, MD, MS, with the division of cardiovascular medicine at the University of Wisconsin–Madison, who was not involved in the study. “This is not a randomized, controlled trial, and coffee consumption was self-reported, but the methods employed are rigorous, despite these and other important limitations. However, we need to be extremely cautious in how we interpret these findings, and not use these data as a prescription for more coffee. It’s important to recognize that this study is not telling us to drink more coffee, or start drinking coffee, to protect against developing arrhythmias. However, it should offer more reassurance that moderate coffee consumption is not necessarily harmful, and will not always lead to arrhythmias. This is important, given the widespread notion that coffee is universally proarrhythmic.”
A call for personalized guidance
“As the investigators note, there are definitely biologically plausible reasons how coffee and caffeine may not cause arrhythmias, and may be possibly protective in some, despite being a stimulant,” Dr. Goldberger said. “However, if your patient is reporting palpitations or symptoms of an arrhythmia, and feels they be related to coffee or caffeine, we should not use this study to tell them that coffee may not be the culprit. We need to listen to our patients, and the decision to reduce coffee consumption to reduce these symptoms needs to be personalized.”
The effect size was small, and only about 4% of the participants developed an arrhythmia, Dr. Goldberger and Rodney A. Hayward, MD, wrote in an invited commentary on the study in JAMA Internal Medicine. Dr. Hayward is a professor of public health and internal medicine at the University of Michigan, Ann Arbor, and a senior investigator at the Ann Arbor Veterans Affairs Center for Clinical Management Research.
“Unfortunately, coffee consumption was self-reported at a single time point. Not only can this lead to recall bias, but subsequent and substantial changes in coffee consumption are also possible, including reductions due to new signs or symptoms,” they said.
No evidence that coffee ups risk for developing arrhythmias
Another recent study suggests that people may alter their coffee consumption depending on their baseline cardiovascular health, according to the commentary.
Overall, the results “strengthen the evidence that caffeine is not proarrhythmic, but they should not be taken as proving that coffee is an antiarrhythmic—this distinction is of paramount importance,” Dr. Goldberger and Dr. Hayward wrote. “Health care professionals can reassure patients that there is no evidence that drinking coffee increases the risk for developing arrhythmias. This is particularly important for the many patients with benign palpitations who are devastated when they think, or are told, that they have to stop drinking coffee. Given current evidence, this is entirely a patient-preference decision, not a medical one.”
Dr. Marcus, a cardiac electrophysiologist, sees patients with arrhythmias all the time. They tend to “come in fairly convinced that caffeine is to be avoided when they have arrhythmias,” he said. “Often, they been told by their primary care physician or their general cardiologist to avoid caffeine because they have an arrhythmia.
“What I suggest to my patients is that they feel free to go ahead and experiment and try coffee,” Dr. Marcus said.
Still, Dr. Marcus suspects that there are some individuals in whom caffeine is a trigger for the arrhythmia. But evidence indicates these cases likely are rare, and avoiding caffeine need not apply to the general population, particularly “given the potential health benefits of benefits of coffee and also, frankly, just the enhanced quality of life that people can enjoy drinking a good cup of coffee.”
The research was conducted using the UK Biobank resource, which was established by the Wellcome Trust, the Medical Research Council, the U.K. Department of Health, and the Scottish government. The UK Biobank has received funding from other agencies and foundations as well. Dr. Marcus disclosed grants from Baylis, Medtronic, and Eight Sleep outside the submitted work. In addition, he reported consulting for Johnson & Johnson and InCarda, and holding equity in InCarda. A coauthor received salary support from the National Institutes of Health during the study. Dr. Goldberger and Dr. Hayward disclosed no conflicts of interest.
FROM JAMA INTERNAL MEDICINE
Homeopath arrested for fake COVID immunization, vaccine card scheme
A homeopathic doctor licensed in California was arrested July 14 and charged with a scheme to sell homeoprophylaxis immunization pellets and to falsify COVID-19 vaccination cards by making it appear that her customers had received the Moderna vaccine, according to the U.S. Department of Justice.
Juli A. Mazi, 41, of Napa, is charged with one count of wire fraud and one count of false statements related to health care matters. The case is the first federal criminal fraud prosecution related to homeoprophylaxis immunizations and fraudulent vaccination record cards, the DOJ said in a news release.
In April, according to federal authorities, an individual submitted a complaint to the Department of Health and Human Services Office of Inspector General, stating that family members had purchased the immunization pellets from Ms. Mazi. The complainant stated that the family members had told her/him that Ms. Mazi had said the pellets contained the COVID-19 virus and would create an antibody response in the immune system.
The affidavit noted that none of the family members had received injections of any of the COVID-19 vaccines authorized by the Food and Drug Administration.
However, the complainant said, Ms. Mazi sent COVID-19 vaccination cards listing Moderna to the complainant family. Ms. Mazi allegedly instructed the family members to mark the cards to falsely state that they had received the Moderna vaccine on the date that they ingested the homeoprophylaxis immunization pellets.
She also allegedly provided instructions on how to fraudulently complete the cards to make it appear that a customer had received two doses of the Moderna vaccine. She even supplied Moderna lot numbers to enter on the cards.
In addition, Ms. Mazi allegedly offered homeoprophylaxis immunizations for childhood illnesses that she falsely claimed would satisfy the immunization requirements for California schools, and falsified immunization cards that were submitted by parents to California schools.
Ms. Mazi further stated that her customers could provide the pellets to children for COVID-19 immunity, and that “the dose is actually the same for babies,” the news release said.
Ms. Mazi is alleged to have falsely claimed that ingesting the pellets would result in full lifelong immunity from COVID-19. In addition, she exploited the disinformation and fear surrounding COVID-19 vaccination by falsely claiming that the FDA-authorized vaccines contain “toxic ingredients,” the DOJ said.
Homeopathic preparations
According to the DOJ, “Homeophrophylaxis involves the exposure of an individual to dilute amounts of a disease, purportedly to stimulate the immune system and confer immunity.”
According to Australia’s National Centre for Immunisation Research & Surveillance (NCIRS), a private organization funded by the Australian and New South Wales governments, there is no high-quality research showing that homeopathic preparations are effective in preventing infectious disease.
Typical homeopathic preparations dilute a disease, tissue, or plant extract in water “to the point where none of the original material is contained within the preparation by the end of the process,” an NCIRS fact sheet says.
Referring to Ms. Mazi, Deputy Attorney General Lisa Monaco said in the news release, “This defendant allegedly defrauded and endangered the public by preying on fears and spreading misinformation about FDA-authorized vaccinations, while also peddling fake treatments that put people’s lives at risk.
“Even worse, the defendant allegedly created counterfeit COVID-19 vaccination cards and instructed her customers to falsely mark that they had received a vaccine, allowing them to circumvent efforts to contain the spread of the disease.”
The case against Ms. Mazi was brought in coordination with the DOJ Health Care Fraud Unit’s COVID-19 Interagency Working Group, which organizes efforts to address illegal activity involving health care programs during the pandemic.
The fraud unit leads the department’s Health Care Fraud Strike Force, which has existed since 2007. In May, U.S. Attorney General Merrick Garland established the COVID-19 Fraud Enforcement Task Force in partnership with other government agencies to combat and prevent pandemic-related fraud.
A version of this article first appeared on Medscape.com.
A homeopathic doctor licensed in California was arrested July 14 and charged with a scheme to sell homeoprophylaxis immunization pellets and to falsify COVID-19 vaccination cards by making it appear that her customers had received the Moderna vaccine, according to the U.S. Department of Justice.
Juli A. Mazi, 41, of Napa, is charged with one count of wire fraud and one count of false statements related to health care matters. The case is the first federal criminal fraud prosecution related to homeoprophylaxis immunizations and fraudulent vaccination record cards, the DOJ said in a news release.
In April, according to federal authorities, an individual submitted a complaint to the Department of Health and Human Services Office of Inspector General, stating that family members had purchased the immunization pellets from Ms. Mazi. The complainant stated that the family members had told her/him that Ms. Mazi had said the pellets contained the COVID-19 virus and would create an antibody response in the immune system.
The affidavit noted that none of the family members had received injections of any of the COVID-19 vaccines authorized by the Food and Drug Administration.
However, the complainant said, Ms. Mazi sent COVID-19 vaccination cards listing Moderna to the complainant family. Ms. Mazi allegedly instructed the family members to mark the cards to falsely state that they had received the Moderna vaccine on the date that they ingested the homeoprophylaxis immunization pellets.
She also allegedly provided instructions on how to fraudulently complete the cards to make it appear that a customer had received two doses of the Moderna vaccine. She even supplied Moderna lot numbers to enter on the cards.
In addition, Ms. Mazi allegedly offered homeoprophylaxis immunizations for childhood illnesses that she falsely claimed would satisfy the immunization requirements for California schools, and falsified immunization cards that were submitted by parents to California schools.
Ms. Mazi further stated that her customers could provide the pellets to children for COVID-19 immunity, and that “the dose is actually the same for babies,” the news release said.
Ms. Mazi is alleged to have falsely claimed that ingesting the pellets would result in full lifelong immunity from COVID-19. In addition, she exploited the disinformation and fear surrounding COVID-19 vaccination by falsely claiming that the FDA-authorized vaccines contain “toxic ingredients,” the DOJ said.
Homeopathic preparations
According to the DOJ, “Homeophrophylaxis involves the exposure of an individual to dilute amounts of a disease, purportedly to stimulate the immune system and confer immunity.”
According to Australia’s National Centre for Immunisation Research & Surveillance (NCIRS), a private organization funded by the Australian and New South Wales governments, there is no high-quality research showing that homeopathic preparations are effective in preventing infectious disease.
Typical homeopathic preparations dilute a disease, tissue, or plant extract in water “to the point where none of the original material is contained within the preparation by the end of the process,” an NCIRS fact sheet says.
Referring to Ms. Mazi, Deputy Attorney General Lisa Monaco said in the news release, “This defendant allegedly defrauded and endangered the public by preying on fears and spreading misinformation about FDA-authorized vaccinations, while also peddling fake treatments that put people’s lives at risk.
“Even worse, the defendant allegedly created counterfeit COVID-19 vaccination cards and instructed her customers to falsely mark that they had received a vaccine, allowing them to circumvent efforts to contain the spread of the disease.”
The case against Ms. Mazi was brought in coordination with the DOJ Health Care Fraud Unit’s COVID-19 Interagency Working Group, which organizes efforts to address illegal activity involving health care programs during the pandemic.
The fraud unit leads the department’s Health Care Fraud Strike Force, which has existed since 2007. In May, U.S. Attorney General Merrick Garland established the COVID-19 Fraud Enforcement Task Force in partnership with other government agencies to combat and prevent pandemic-related fraud.
A version of this article first appeared on Medscape.com.
A homeopathic doctor licensed in California was arrested July 14 and charged with a scheme to sell homeoprophylaxis immunization pellets and to falsify COVID-19 vaccination cards by making it appear that her customers had received the Moderna vaccine, according to the U.S. Department of Justice.
Juli A. Mazi, 41, of Napa, is charged with one count of wire fraud and one count of false statements related to health care matters. The case is the first federal criminal fraud prosecution related to homeoprophylaxis immunizations and fraudulent vaccination record cards, the DOJ said in a news release.
In April, according to federal authorities, an individual submitted a complaint to the Department of Health and Human Services Office of Inspector General, stating that family members had purchased the immunization pellets from Ms. Mazi. The complainant stated that the family members had told her/him that Ms. Mazi had said the pellets contained the COVID-19 virus and would create an antibody response in the immune system.
The affidavit noted that none of the family members had received injections of any of the COVID-19 vaccines authorized by the Food and Drug Administration.
However, the complainant said, Ms. Mazi sent COVID-19 vaccination cards listing Moderna to the complainant family. Ms. Mazi allegedly instructed the family members to mark the cards to falsely state that they had received the Moderna vaccine on the date that they ingested the homeoprophylaxis immunization pellets.
She also allegedly provided instructions on how to fraudulently complete the cards to make it appear that a customer had received two doses of the Moderna vaccine. She even supplied Moderna lot numbers to enter on the cards.
In addition, Ms. Mazi allegedly offered homeoprophylaxis immunizations for childhood illnesses that she falsely claimed would satisfy the immunization requirements for California schools, and falsified immunization cards that were submitted by parents to California schools.
Ms. Mazi further stated that her customers could provide the pellets to children for COVID-19 immunity, and that “the dose is actually the same for babies,” the news release said.
Ms. Mazi is alleged to have falsely claimed that ingesting the pellets would result in full lifelong immunity from COVID-19. In addition, she exploited the disinformation and fear surrounding COVID-19 vaccination by falsely claiming that the FDA-authorized vaccines contain “toxic ingredients,” the DOJ said.
Homeopathic preparations
According to the DOJ, “Homeophrophylaxis involves the exposure of an individual to dilute amounts of a disease, purportedly to stimulate the immune system and confer immunity.”
According to Australia’s National Centre for Immunisation Research & Surveillance (NCIRS), a private organization funded by the Australian and New South Wales governments, there is no high-quality research showing that homeopathic preparations are effective in preventing infectious disease.
Typical homeopathic preparations dilute a disease, tissue, or plant extract in water “to the point where none of the original material is contained within the preparation by the end of the process,” an NCIRS fact sheet says.
Referring to Ms. Mazi, Deputy Attorney General Lisa Monaco said in the news release, “This defendant allegedly defrauded and endangered the public by preying on fears and spreading misinformation about FDA-authorized vaccinations, while also peddling fake treatments that put people’s lives at risk.
“Even worse, the defendant allegedly created counterfeit COVID-19 vaccination cards and instructed her customers to falsely mark that they had received a vaccine, allowing them to circumvent efforts to contain the spread of the disease.”
The case against Ms. Mazi was brought in coordination with the DOJ Health Care Fraud Unit’s COVID-19 Interagency Working Group, which organizes efforts to address illegal activity involving health care programs during the pandemic.
The fraud unit leads the department’s Health Care Fraud Strike Force, which has existed since 2007. In May, U.S. Attorney General Merrick Garland established the COVID-19 Fraud Enforcement Task Force in partnership with other government agencies to combat and prevent pandemic-related fraud.
A version of this article first appeared on Medscape.com.
Sen. Schumer backs federal decriminalization of marijuana
U.S. Sen. Chuck Schumer, the Senate majority leader, is cosponsoring legislation that would decriminalize marijuana at the federal level.

The Cannabis Administration & Opportunity Act would allow the federal government to regulate and tax marijuana sales for the first time and would stop the federal prosecution of people for possessing and selling the drug, The New York Times reported. States could still make their own marijuana laws, however.
The bill calls for using money raised by taxing marijuana to help poor people and communities of color that have been unduly affected by marijuana laws.
Arrests and convictions for nonviolent marijuana offenses would be automatically expunged, The New York Times reported.
“The War on Drugs has been a war on people – particularly people of color,” a draft of the bill said, adding that the bill “aims to end the decades of harm inflicted on communities of color by removing cannabis from the federal list of controlled substances and empowering states to implement their own cannabis laws.”
But passage of the bill is highly uncertain because of strong Republican opposition in the Senate, where Democrats hold a narrow majority, according to The New York Times.
Sen. Schumer signaled his intentions when he spoke on April 20, the unofficial holiday for marijuana smokers.
“Hopefully, the next time this unofficial holiday of 4/20 rolls around, our country will have made progress in addressing the massive overcriminalization of marijuana in a meaningful and comprehensive way,” he said at the time, the newspaper reported.
Cosponsors were U.S. Sen. Cory Booker of New Jersey and U.S. Sen. Ron Wyden of Oregon, chairman of the Senate Finance Committee.
A version of this article first appeared on WebMD.com.
U.S. Sen. Chuck Schumer, the Senate majority leader, is cosponsoring legislation that would decriminalize marijuana at the federal level.
The Cannabis Administration & Opportunity Act would allow the federal government to regulate and tax marijuana sales for the first time and would stop the federal prosecution of people for possessing and selling the drug, The New York Times reported. States could still make their own marijuana laws, however.
The bill calls for using money raised by taxing marijuana to help poor people and communities of color that have been unduly affected by marijuana laws.
Arrests and convictions for nonviolent marijuana offenses would be automatically expunged, The New York Times reported.
“The War on Drugs has been a war on people – particularly people of color,” a draft of the bill said, adding that the bill “aims to end the decades of harm inflicted on communities of color by removing cannabis from the federal list of controlled substances and empowering states to implement their own cannabis laws.”
But passage of the bill is highly uncertain because of strong Republican opposition in the Senate, where Democrats hold a narrow majority, according to The New York Times.
Sen. Schumer signaled his intentions when he spoke on April 20, the unofficial holiday for marijuana smokers.
“Hopefully, the next time this unofficial holiday of 4/20 rolls around, our country will have made progress in addressing the massive overcriminalization of marijuana in a meaningful and comprehensive way,” he said at the time, the newspaper reported.
Cosponsors were U.S. Sen. Cory Booker of New Jersey and U.S. Sen. Ron Wyden of Oregon, chairman of the Senate Finance Committee.
A version of this article first appeared on WebMD.com.
U.S. Sen. Chuck Schumer, the Senate majority leader, is cosponsoring legislation that would decriminalize marijuana at the federal level.
The Cannabis Administration & Opportunity Act would allow the federal government to regulate and tax marijuana sales for the first time and would stop the federal prosecution of people for possessing and selling the drug, The New York Times reported. States could still make their own marijuana laws, however.
The bill calls for using money raised by taxing marijuana to help poor people and communities of color that have been unduly affected by marijuana laws.
Arrests and convictions for nonviolent marijuana offenses would be automatically expunged, The New York Times reported.
“The War on Drugs has been a war on people – particularly people of color,” a draft of the bill said, adding that the bill “aims to end the decades of harm inflicted on communities of color by removing cannabis from the federal list of controlled substances and empowering states to implement their own cannabis laws.”
But passage of the bill is highly uncertain because of strong Republican opposition in the Senate, where Democrats hold a narrow majority, according to The New York Times.
Sen. Schumer signaled his intentions when he spoke on April 20, the unofficial holiday for marijuana smokers.
“Hopefully, the next time this unofficial holiday of 4/20 rolls around, our country will have made progress in addressing the massive overcriminalization of marijuana in a meaningful and comprehensive way,” he said at the time, the newspaper reported.
Cosponsors were U.S. Sen. Cory Booker of New Jersey and U.S. Sen. Ron Wyden of Oregon, chairman of the Senate Finance Committee.
A version of this article first appeared on WebMD.com.
Early heparin treatment linked to lower COVID-19 mortality
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
The latest on HIV care, cure, and PrEP
The COVID-19 pandemic has overshadowed innovations in HIV care and prevention, says Tonia Poteat, PhD, MPH, PA-C, a primary HIV care and HIV pre-exposure prophylaxis (PrEP) clinician and associate professor of social medicine at the University of North Carolina at Chapel Hill. Therefore, even though the U.S. Food and Drug Administration approved monthly injections of cabotegravir/rilpivirine (Cabenuva) in January, none of her patients are taking it.
“We moved our clinic three times during the pandemic,” Dr. Poteat said. “I’m really interested in how on earth we’re going to integrate injectable products into our workflow. We don’t have systems set up yet, so we’re in the process of figuring out what the structure is going to be like. We have people who are interested on a wait list.”
Indeed, in an HIV world still reeling from the dual impact of HIV and COVID-19, the International AIDS Society Conference on HIV Science (IAS 2021) will bring a more coherent narrative on the future of HIV treatment and prevention. That narrative involves long-acting treatment and setting up the systems to make it available to everyone. And IAS offers data showing exactly how much people living with HIV risk poor COVID-19 outcomes.
The conference will be online for the second year in a row and, unlike in 2020, the focus will be much more on HIV treatment and prevention than on that other big infectious disease making news these days.
There will be new data on long-acting forms of prevention, such as the intravaginal ring and monthly PrEP pills. There will be new data on PrEP on demand (2-1-1 PrEP) and the results of a large trial looking at breakthrough HIV infections among those taking daily oral PrEP.
On the treatment side, trial results will be announced on cabotegravir/rilpivirine and islatravir long-acting treatment, as well as additional data on the effectiveness of two-drug antiretrovial therapy dolutegravir/lamivudine (Dovato) and bictegravir/emtricitabine/tenofovir alafenamide (Biktarvy), specifically in Black participants.
On the cure front, intriguing animal studies and ex vivo studies look into the use of cancer immunotherapies for an HIV functional cure, as well as the use of CAR-T to stop HIV replication in the absence of daily medication.
Dr. Poteat is not alone in being interested specifically in the PrEP and long-acting studies. Jonathan Baker, a PA in private practice in New York City, also wants to see the data on the ring and other expanded PrEP options.
But “a prevention method can only work when people are able to use it,” he said. “So [the session] ‘Reducing Barriers to PrEP’ is really relevant as we see inequitable intake failing the populations who need PrEP most.”
This is a concern Dr. Poteat has too. That’s why she’s glad to see there will be sessions on systemic inequities, particularly around what it will take to address those inequities in the U.S. by 2030 in line with “Ending the HIV Epidemic: A Plan for America.” She’s looking forward to sessions on novel service-delivery models with low thresholds of entry for people experiencing homelessness or people who inject drugs; on access to affordable medications; on trans-led care for transgender women in the global South; and on the comorbidities of aging that are keeping her patients sick these days.
To that end, there are sessions on common comorbidities with HIV, such as reinfection with hepatitis C, sexually transmitted infections, heart disease, and weight gain as a result of newer drug options, as well as drug-drug interactions between HIV medications and those used in gender-affirming care for transgender adults.
“I can count on one hand the number of people for whom the issue is finding the right antiretroviral,” she said. “That’s rarely the issue. The issue is often how do we manage their other comorbid conditions, and what about drug-drug interactions with those conditions? HIV is not the only condition many of them have.”
Mr. Baker reports that his clinic receives funding from Merck, Innovio, and Antiva. Dr. Poteat is a consultant for ViiV Healthcare and serves on a study advisory board for Merck.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has overshadowed innovations in HIV care and prevention, says Tonia Poteat, PhD, MPH, PA-C, a primary HIV care and HIV pre-exposure prophylaxis (PrEP) clinician and associate professor of social medicine at the University of North Carolina at Chapel Hill. Therefore, even though the U.S. Food and Drug Administration approved monthly injections of cabotegravir/rilpivirine (Cabenuva) in January, none of her patients are taking it.
“We moved our clinic three times during the pandemic,” Dr. Poteat said. “I’m really interested in how on earth we’re going to integrate injectable products into our workflow. We don’t have systems set up yet, so we’re in the process of figuring out what the structure is going to be like. We have people who are interested on a wait list.”
Indeed, in an HIV world still reeling from the dual impact of HIV and COVID-19, the International AIDS Society Conference on HIV Science (IAS 2021) will bring a more coherent narrative on the future of HIV treatment and prevention. That narrative involves long-acting treatment and setting up the systems to make it available to everyone. And IAS offers data showing exactly how much people living with HIV risk poor COVID-19 outcomes.
The conference will be online for the second year in a row and, unlike in 2020, the focus will be much more on HIV treatment and prevention than on that other big infectious disease making news these days.
There will be new data on long-acting forms of prevention, such as the intravaginal ring and monthly PrEP pills. There will be new data on PrEP on demand (2-1-1 PrEP) and the results of a large trial looking at breakthrough HIV infections among those taking daily oral PrEP.
On the treatment side, trial results will be announced on cabotegravir/rilpivirine and islatravir long-acting treatment, as well as additional data on the effectiveness of two-drug antiretrovial therapy dolutegravir/lamivudine (Dovato) and bictegravir/emtricitabine/tenofovir alafenamide (Biktarvy), specifically in Black participants.
On the cure front, intriguing animal studies and ex vivo studies look into the use of cancer immunotherapies for an HIV functional cure, as well as the use of CAR-T to stop HIV replication in the absence of daily medication.
Dr. Poteat is not alone in being interested specifically in the PrEP and long-acting studies. Jonathan Baker, a PA in private practice in New York City, also wants to see the data on the ring and other expanded PrEP options.
But “a prevention method can only work when people are able to use it,” he said. “So [the session] ‘Reducing Barriers to PrEP’ is really relevant as we see inequitable intake failing the populations who need PrEP most.”
This is a concern Dr. Poteat has too. That’s why she’s glad to see there will be sessions on systemic inequities, particularly around what it will take to address those inequities in the U.S. by 2030 in line with “Ending the HIV Epidemic: A Plan for America.” She’s looking forward to sessions on novel service-delivery models with low thresholds of entry for people experiencing homelessness or people who inject drugs; on access to affordable medications; on trans-led care for transgender women in the global South; and on the comorbidities of aging that are keeping her patients sick these days.
To that end, there are sessions on common comorbidities with HIV, such as reinfection with hepatitis C, sexually transmitted infections, heart disease, and weight gain as a result of newer drug options, as well as drug-drug interactions between HIV medications and those used in gender-affirming care for transgender adults.
“I can count on one hand the number of people for whom the issue is finding the right antiretroviral,” she said. “That’s rarely the issue. The issue is often how do we manage their other comorbid conditions, and what about drug-drug interactions with those conditions? HIV is not the only condition many of them have.”
Mr. Baker reports that his clinic receives funding from Merck, Innovio, and Antiva. Dr. Poteat is a consultant for ViiV Healthcare and serves on a study advisory board for Merck.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has overshadowed innovations in HIV care and prevention, says Tonia Poteat, PhD, MPH, PA-C, a primary HIV care and HIV pre-exposure prophylaxis (PrEP) clinician and associate professor of social medicine at the University of North Carolina at Chapel Hill. Therefore, even though the U.S. Food and Drug Administration approved monthly injections of cabotegravir/rilpivirine (Cabenuva) in January, none of her patients are taking it.
“We moved our clinic three times during the pandemic,” Dr. Poteat said. “I’m really interested in how on earth we’re going to integrate injectable products into our workflow. We don’t have systems set up yet, so we’re in the process of figuring out what the structure is going to be like. We have people who are interested on a wait list.”
Indeed, in an HIV world still reeling from the dual impact of HIV and COVID-19, the International AIDS Society Conference on HIV Science (IAS 2021) will bring a more coherent narrative on the future of HIV treatment and prevention. That narrative involves long-acting treatment and setting up the systems to make it available to everyone. And IAS offers data showing exactly how much people living with HIV risk poor COVID-19 outcomes.
The conference will be online for the second year in a row and, unlike in 2020, the focus will be much more on HIV treatment and prevention than on that other big infectious disease making news these days.
There will be new data on long-acting forms of prevention, such as the intravaginal ring and monthly PrEP pills. There will be new data on PrEP on demand (2-1-1 PrEP) and the results of a large trial looking at breakthrough HIV infections among those taking daily oral PrEP.
On the treatment side, trial results will be announced on cabotegravir/rilpivirine and islatravir long-acting treatment, as well as additional data on the effectiveness of two-drug antiretrovial therapy dolutegravir/lamivudine (Dovato) and bictegravir/emtricitabine/tenofovir alafenamide (Biktarvy), specifically in Black participants.
On the cure front, intriguing animal studies and ex vivo studies look into the use of cancer immunotherapies for an HIV functional cure, as well as the use of CAR-T to stop HIV replication in the absence of daily medication.
Dr. Poteat is not alone in being interested specifically in the PrEP and long-acting studies. Jonathan Baker, a PA in private practice in New York City, also wants to see the data on the ring and other expanded PrEP options.
But “a prevention method can only work when people are able to use it,” he said. “So [the session] ‘Reducing Barriers to PrEP’ is really relevant as we see inequitable intake failing the populations who need PrEP most.”
This is a concern Dr. Poteat has too. That’s why she’s glad to see there will be sessions on systemic inequities, particularly around what it will take to address those inequities in the U.S. by 2030 in line with “Ending the HIV Epidemic: A Plan for America.” She’s looking forward to sessions on novel service-delivery models with low thresholds of entry for people experiencing homelessness or people who inject drugs; on access to affordable medications; on trans-led care for transgender women in the global South; and on the comorbidities of aging that are keeping her patients sick these days.
To that end, there are sessions on common comorbidities with HIV, such as reinfection with hepatitis C, sexually transmitted infections, heart disease, and weight gain as a result of newer drug options, as well as drug-drug interactions between HIV medications and those used in gender-affirming care for transgender adults.
“I can count on one hand the number of people for whom the issue is finding the right antiretroviral,” she said. “That’s rarely the issue. The issue is often how do we manage their other comorbid conditions, and what about drug-drug interactions with those conditions? HIV is not the only condition many of them have.”
Mr. Baker reports that his clinic receives funding from Merck, Innovio, and Antiva. Dr. Poteat is a consultant for ViiV Healthcare and serves on a study advisory board for Merck.
A version of this article first appeared on Medscape.com.
Health anxiety common as COVID restrictions loosen
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
Florida-based doctor arrested in Haiti president’s assassination
About two dozen people have been arrested as suspects, the newspaper reported, though police believe Christian Emmanuel Sanon, 63, was plotting to become president.
“He arrived by private plane in June with political objectives and contacted a private security firm to recruit the people who committed this act,” Léon Charles, Haiti’s national police chief, said during a news conference on July 11.
The firm, called CTU Security, is a Venezuelan company based in Miami, Mr. Charles said. During a raid at Mr. Sanon’s home in Port-au-Prince, police found six rifles, 20 boxes of bullets, 24 unused shooting targets, pistol holsters, and a hat with a U.S. Drug Enforcement Agency logo.
“This initial mission that was given to these assailants was to protect the individual named Emmanuel Sanon, but afterwards, the mission changed,” Mr. Charles said.
The new “mission” was to arrest President Moïse and install Mr. Sanon as president, The New York Times reported, though Mr. Charles didn’t explain when the mission changed to assassination or how Mr. Sanon could have taken control of the government.
President Moïse was shot to death on July 7 at his home in Port-au-Prince by a “team of commandos,” according to The Washington Post. On July 9, Haiti asked the U.S. to send troops to the country to protect its airport and key infrastructure.
The announcement of Mr. Sanon’s arrest came hours after FBI and Department of Homeland Security officials arrived in Haiti on July 11 to discuss how the U.S. can offer assistance, the newspaper reported.
Mr. Sanon has a YouTube channel with three political campaign videos from 2011, which include discussions about Haitian politics, according to Forbes. In one of the videos, titled “Dr. Christian Sanon – Leadership for Haiti,” Mr. Sanon talks about corruption in the country and presents himself as a potential leader.
Mr. Sanon lived in Florida for more than 20 years, ranging from the Tampa Bay area to South Florida, according to the Miami Herald. Public records show that he had more than a dozen businesses registered in the state, including medical services and real estate, though most are inactive.
Mr. Sanon is the third person with links to the U.S. who has been arrested in connection with the assassination, the Miami Herald reported. Two Haitian-Americans from southern Florida – James Solages, 35, and Joseph G. Vincent, 55 – were arrested by local police. They claimed they were working as translators for the assassins.
The first lady, Martine Moïse, was wounded in the attack and is now receiving treatment at a hospital in Miami, the newspaper reported.
A version of this article first appeared on WebMD.com.
About two dozen people have been arrested as suspects, the newspaper reported, though police believe Christian Emmanuel Sanon, 63, was plotting to become president.
“He arrived by private plane in June with political objectives and contacted a private security firm to recruit the people who committed this act,” Léon Charles, Haiti’s national police chief, said during a news conference on July 11.
The firm, called CTU Security, is a Venezuelan company based in Miami, Mr. Charles said. During a raid at Mr. Sanon’s home in Port-au-Prince, police found six rifles, 20 boxes of bullets, 24 unused shooting targets, pistol holsters, and a hat with a U.S. Drug Enforcement Agency logo.
“This initial mission that was given to these assailants was to protect the individual named Emmanuel Sanon, but afterwards, the mission changed,” Mr. Charles said.
The new “mission” was to arrest President Moïse and install Mr. Sanon as president, The New York Times reported, though Mr. Charles didn’t explain when the mission changed to assassination or how Mr. Sanon could have taken control of the government.
President Moïse was shot to death on July 7 at his home in Port-au-Prince by a “team of commandos,” according to The Washington Post. On July 9, Haiti asked the U.S. to send troops to the country to protect its airport and key infrastructure.
The announcement of Mr. Sanon’s arrest came hours after FBI and Department of Homeland Security officials arrived in Haiti on July 11 to discuss how the U.S. can offer assistance, the newspaper reported.
Mr. Sanon has a YouTube channel with three political campaign videos from 2011, which include discussions about Haitian politics, according to Forbes. In one of the videos, titled “Dr. Christian Sanon – Leadership for Haiti,” Mr. Sanon talks about corruption in the country and presents himself as a potential leader.
Mr. Sanon lived in Florida for more than 20 years, ranging from the Tampa Bay area to South Florida, according to the Miami Herald. Public records show that he had more than a dozen businesses registered in the state, including medical services and real estate, though most are inactive.
Mr. Sanon is the third person with links to the U.S. who has been arrested in connection with the assassination, the Miami Herald reported. Two Haitian-Americans from southern Florida – James Solages, 35, and Joseph G. Vincent, 55 – were arrested by local police. They claimed they were working as translators for the assassins.
The first lady, Martine Moïse, was wounded in the attack and is now receiving treatment at a hospital in Miami, the newspaper reported.
A version of this article first appeared on WebMD.com.
About two dozen people have been arrested as suspects, the newspaper reported, though police believe Christian Emmanuel Sanon, 63, was plotting to become president.
“He arrived by private plane in June with political objectives and contacted a private security firm to recruit the people who committed this act,” Léon Charles, Haiti’s national police chief, said during a news conference on July 11.
The firm, called CTU Security, is a Venezuelan company based in Miami, Mr. Charles said. During a raid at Mr. Sanon’s home in Port-au-Prince, police found six rifles, 20 boxes of bullets, 24 unused shooting targets, pistol holsters, and a hat with a U.S. Drug Enforcement Agency logo.
“This initial mission that was given to these assailants was to protect the individual named Emmanuel Sanon, but afterwards, the mission changed,” Mr. Charles said.
The new “mission” was to arrest President Moïse and install Mr. Sanon as president, The New York Times reported, though Mr. Charles didn’t explain when the mission changed to assassination or how Mr. Sanon could have taken control of the government.
President Moïse was shot to death on July 7 at his home in Port-au-Prince by a “team of commandos,” according to The Washington Post. On July 9, Haiti asked the U.S. to send troops to the country to protect its airport and key infrastructure.
The announcement of Mr. Sanon’s arrest came hours after FBI and Department of Homeland Security officials arrived in Haiti on July 11 to discuss how the U.S. can offer assistance, the newspaper reported.
Mr. Sanon has a YouTube channel with three political campaign videos from 2011, which include discussions about Haitian politics, according to Forbes. In one of the videos, titled “Dr. Christian Sanon – Leadership for Haiti,” Mr. Sanon talks about corruption in the country and presents himself as a potential leader.
Mr. Sanon lived in Florida for more than 20 years, ranging from the Tampa Bay area to South Florida, according to the Miami Herald. Public records show that he had more than a dozen businesses registered in the state, including medical services and real estate, though most are inactive.
Mr. Sanon is the third person with links to the U.S. who has been arrested in connection with the assassination, the Miami Herald reported. Two Haitian-Americans from southern Florida – James Solages, 35, and Joseph G. Vincent, 55 – were arrested by local police. They claimed they were working as translators for the assassins.
The first lady, Martine Moïse, was wounded in the attack and is now receiving treatment at a hospital in Miami, the newspaper reported.
A version of this article first appeared on WebMD.com.
Talking about guns: Website helps physicians follow through on pledge
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.