User login
Children and COVID: New cases increase for third straight week
There were almost 142,000 new cases reported during the week of Nov. 12-18, marking an increase of 16% over the previous week and the 15th straight week with a weekly total over 100,000, the American Academy of Pediatrics and the Children’s Hospital Association said.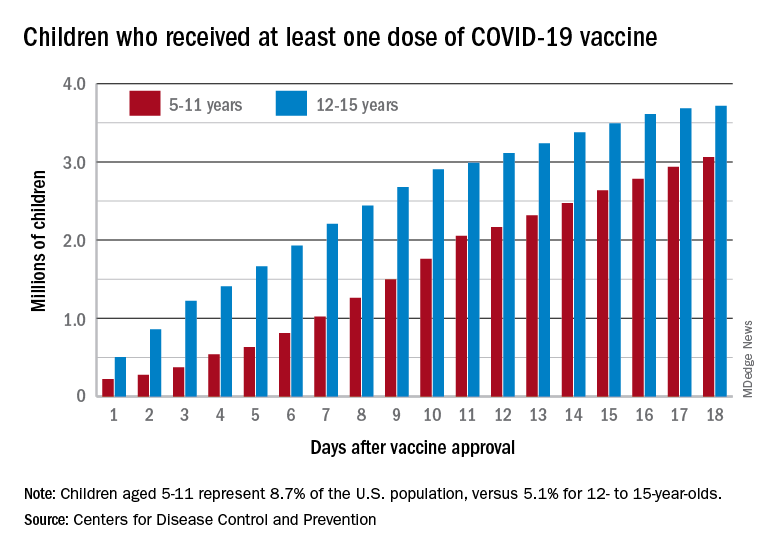
Regional data show that the Midwest has experienced the largest share of this latest surge, followed by the Northeast. Cases increased in the South during the week of Nov. 12-18 after holding steady over the previous 2 weeks, while new cases in the West dropped in the last week. At the state level, Maine, New Hampshire, and Vermont again reported the largest percent increases, with Michigan, Minnesota, and New Mexico also above average, the AAP and CHA said in their weekly COVID report.
Data from the Centers for Disease Control and Prevention show similar trends for both emergency department visits and hospital admissions, as both have risen in November after declines that began in late August and early September.
The cumulative number of pediatric cases is 6.77 million since the pandemic began, based on the AAP/CHA accounting of state cases, although Alabama, Nebraska, and Texas stopped reporting over the summer, suggesting the actual number is higher. The CDC puts the total number of COVID cases in children at 5.96 million, but there are age discrepancies between the CDC and the AAP/CHA’s state-based data.
The vaccine gap is closing
Vaccinations among the recently eligible 5- to 11-year-olds have steadily increased following a somewhat slow start. The initial pace was behind that of the 12- to 15-years-olds through the first postapproval week but has since closed the gap, based on data from the CDC’s COVID Data Tracker.
The tally of children who received at least one dose of the COVID vaccine among the 5- to 11-year-olds was behind the older group by almost 1.2 million on day 7 after the CDC’s Nov. 2 approval, but by day 18 the deficit was down to about 650,000, the CDC reported.
Altogether, just over 3 million children aged 5-11 have received at least one dose, which is 10.7% of that age group’s total population. Among children aged 12-17, the proportions are 60.7% with at least one dose and 51.1% at full vaccination. Children aged 5-11, who make up 8.7% of the total U.S. population, represented 42.8% of all vaccinations initiated over the 2 weeks ending Nov. 21, compared with 4.2% for those aged 12-17, the CDC said.
There were almost 142,000 new cases reported during the week of Nov. 12-18, marking an increase of 16% over the previous week and the 15th straight week with a weekly total over 100,000, the American Academy of Pediatrics and the Children’s Hospital Association said.
Regional data show that the Midwest has experienced the largest share of this latest surge, followed by the Northeast. Cases increased in the South during the week of Nov. 12-18 after holding steady over the previous 2 weeks, while new cases in the West dropped in the last week. At the state level, Maine, New Hampshire, and Vermont again reported the largest percent increases, with Michigan, Minnesota, and New Mexico also above average, the AAP and CHA said in their weekly COVID report.
Data from the Centers for Disease Control and Prevention show similar trends for both emergency department visits and hospital admissions, as both have risen in November after declines that began in late August and early September.
The cumulative number of pediatric cases is 6.77 million since the pandemic began, based on the AAP/CHA accounting of state cases, although Alabama, Nebraska, and Texas stopped reporting over the summer, suggesting the actual number is higher. The CDC puts the total number of COVID cases in children at 5.96 million, but there are age discrepancies between the CDC and the AAP/CHA’s state-based data.
The vaccine gap is closing
Vaccinations among the recently eligible 5- to 11-year-olds have steadily increased following a somewhat slow start. The initial pace was behind that of the 12- to 15-years-olds through the first postapproval week but has since closed the gap, based on data from the CDC’s COVID Data Tracker.
The tally of children who received at least one dose of the COVID vaccine among the 5- to 11-year-olds was behind the older group by almost 1.2 million on day 7 after the CDC’s Nov. 2 approval, but by day 18 the deficit was down to about 650,000, the CDC reported.
Altogether, just over 3 million children aged 5-11 have received at least one dose, which is 10.7% of that age group’s total population. Among children aged 12-17, the proportions are 60.7% with at least one dose and 51.1% at full vaccination. Children aged 5-11, who make up 8.7% of the total U.S. population, represented 42.8% of all vaccinations initiated over the 2 weeks ending Nov. 21, compared with 4.2% for those aged 12-17, the CDC said.
There were almost 142,000 new cases reported during the week of Nov. 12-18, marking an increase of 16% over the previous week and the 15th straight week with a weekly total over 100,000, the American Academy of Pediatrics and the Children’s Hospital Association said.
Regional data show that the Midwest has experienced the largest share of this latest surge, followed by the Northeast. Cases increased in the South during the week of Nov. 12-18 after holding steady over the previous 2 weeks, while new cases in the West dropped in the last week. At the state level, Maine, New Hampshire, and Vermont again reported the largest percent increases, with Michigan, Minnesota, and New Mexico also above average, the AAP and CHA said in their weekly COVID report.
Data from the Centers for Disease Control and Prevention show similar trends for both emergency department visits and hospital admissions, as both have risen in November after declines that began in late August and early September.
The cumulative number of pediatric cases is 6.77 million since the pandemic began, based on the AAP/CHA accounting of state cases, although Alabama, Nebraska, and Texas stopped reporting over the summer, suggesting the actual number is higher. The CDC puts the total number of COVID cases in children at 5.96 million, but there are age discrepancies between the CDC and the AAP/CHA’s state-based data.
The vaccine gap is closing
Vaccinations among the recently eligible 5- to 11-year-olds have steadily increased following a somewhat slow start. The initial pace was behind that of the 12- to 15-years-olds through the first postapproval week but has since closed the gap, based on data from the CDC’s COVID Data Tracker.
The tally of children who received at least one dose of the COVID vaccine among the 5- to 11-year-olds was behind the older group by almost 1.2 million on day 7 after the CDC’s Nov. 2 approval, but by day 18 the deficit was down to about 650,000, the CDC reported.
Altogether, just over 3 million children aged 5-11 have received at least one dose, which is 10.7% of that age group’s total population. Among children aged 12-17, the proportions are 60.7% with at least one dose and 51.1% at full vaccination. Children aged 5-11, who make up 8.7% of the total U.S. population, represented 42.8% of all vaccinations initiated over the 2 weeks ending Nov. 21, compared with 4.2% for those aged 12-17, the CDC said.
Short-acting opioids needed for withdrawal in U.S. hospitals, say experts
The commentary by Robert A. Kleinman, MD, with the Centre for Addiction and Mental Health, and department of psychiatry, University of Toronto, and Sarah E. Wakeman, MD, with the division of general internal medicine at Massachusetts General Hospital, and Harvard Medical School, Boston, was published in Annals of Internal Medicine.
Currently, short-acting opioids are not recommended in the United States for opioid withdrawal symptoms (OWS) management in the hospital, the authors wrote. Instead, withdrawal symptoms are typically treated, followed by methadone or buprenorphine or nonopioid medications, but many patients don’t get enough relief. Undertreated withdrawal can result in patients leaving the hospital against medical advice, which is linked with higher risk of death.
Addiction specialist Elisabeth Poorman, MD, of the University of Illinois Chicago, said in an interview that she agrees it’s time to start shifting the thinking on using short-acting opioids for OWS in hospitals. Use varies greatly by hospital and by clinician, she said.

“It’s time to let evidence guide us and to be flexible,” Dr. Poorman said.
The commentary authors noted that with methadone, patients must wait several hours for maximal symptom reduction, and the full benefits of methadone treatment are not realized until days after initiation.
Rapid initiation of methadone may be feasible in hospitals and has been proposed as an option, but further study is necessary before widespread use, the authors wrote.
Short-acting opioids may address limitations of other opioids
Lofexidine, an alpha-2-adrenergic agonist, is the only drug approved by the Food and Drug Administration specifically for OWS.
“However,” the authors said, “more than half of patients with OWS treated with lofexidine in phase 3 efficacy trials dropped out by day five. Clonidine, another alpha-2-agonist used off label to treat OWS, has similar effects to those of lofexidine. “
Therefore, short-acting opioids may complement methadone and buprenorphine in treating OWS in the hospital by addressing their limitations, the authors wrote.
Dr. Kleinman and Dr. Wakeman also say short-acting opioids may help with starting buprenorphine for patients exposed to fentanyl, because short-acting opioids can relieve withdrawal symptoms while fentanyl is metabolized and excreted.
Supplementation with short-acting opioids within the hospital can relieve withdrawal symptoms and help keep patients comfortable while methadone is titrated to more effective doses for long-term treatment, they wrote.
With short-acting opioids, patients may become more engaged in their care with, for example, a tamper-proof, patient-controlled analgesia pump, which would allow them to have more autonomy in administration of opioids to relieve pain and withdrawal symptoms, the authors wrote.
Dr. Kleinman and Dr. Wakeman noted that many patients who inject drugs already consume short-acting illicit drugs in the hospital, typically in washrooms and smoking areas, so supervised use of short-acting opioids helps eliminate the risk for unwitnessed overdoses.
Barriers to short-acting opioid use
Despite use of short-acting opioids internationally, barriers in the United States include limited prospective, randomized, controlled research on their benefits. There is limited institutional support for such approaches, and concerns and stigma around providing opioids to patients with OUD.
“[M]any institutions have insufficient numbers of providers who are both confident and competent with standard buprenorphine and methadone initiation approaches, a prerequisite before adopting more complex regimens,” the authors wrote.
Short-acting, full-agonist opioids, as a complement to methadone or buprenorphine, is already recommended for inpatients with OUD who are experiencing acute pain.
But the authors argue it should be an option when pain is not present, but methadone or buprenorphine have not provided enough OWS relief.
When short-acting opioids are helpful, according to outside expert
Dr. Poorman agrees and says she has found short-acting opioids simple to use in the hospital and very helpful in two situations.
One is when patients are very clear that they don’t want any medication for opioid use disorder, but they do want to be treated for their acute medical issue.
“I thought that was a fantastic tool to have to demonstrate we’re listening to them and weren’t trying to impose something on them and left the door open to come back when they did want treatment, which many of them did,” Dr. Poorman said.
The second situation is when the patient is uncertain about options but very afraid of precipitated withdrawal from buprenorphine.
She said she then found it easy to switch from those medications to buprenorphine and methadone.
Dr. Poorman described a situation she encountered previously where the patient was injecting heroin several times a day for 30-40 years. He was very clear he wasn’t going to stop injecting heroin, but he needed medical attention. He was willing to get medical attention, but he told his doctor he didn’t want to be uncomfortable while in the hospital.
It was very hard for his doctor to accept relieving his symptoms of withdrawal as part of her job, because she felt as though she was condoning his drug use, Dr. Poorman explained.
But Dr. Poorman said it’s not realistic to think that someone who clearly does not want to stop using is going to stop using because a doctor made that person go through painful withdrawal “that they’ve structured their whole life around avoiding.”
Take-home message
“We need to understand that addiction is very complex. A lot of times people come to us distressed, and it’s a great time to engage them in care but engaging them in care doesn’t mean imposing discomfort or pain on them,” Dr. Poorman noted. Instead, it means “listening to them, helping them be comfortable in a really stressful situation and then letting them know we are always there for them wherever they are on their disease process or recovery journey so that they can come back to us.”
Dr. Wakeman previously served on clinical advisory board for Celero Systems and receives textbook royalties from Springer and author payment from UpToDate. Dr. Kleinman and Dr. Poorman declared no relevant financial relationships.
The commentary by Robert A. Kleinman, MD, with the Centre for Addiction and Mental Health, and department of psychiatry, University of Toronto, and Sarah E. Wakeman, MD, with the division of general internal medicine at Massachusetts General Hospital, and Harvard Medical School, Boston, was published in Annals of Internal Medicine.
Currently, short-acting opioids are not recommended in the United States for opioid withdrawal symptoms (OWS) management in the hospital, the authors wrote. Instead, withdrawal symptoms are typically treated, followed by methadone or buprenorphine or nonopioid medications, but many patients don’t get enough relief. Undertreated withdrawal can result in patients leaving the hospital against medical advice, which is linked with higher risk of death.
Addiction specialist Elisabeth Poorman, MD, of the University of Illinois Chicago, said in an interview that she agrees it’s time to start shifting the thinking on using short-acting opioids for OWS in hospitals. Use varies greatly by hospital and by clinician, she said.
“It’s time to let evidence guide us and to be flexible,” Dr. Poorman said.
The commentary authors noted that with methadone, patients must wait several hours for maximal symptom reduction, and the full benefits of methadone treatment are not realized until days after initiation.
Rapid initiation of methadone may be feasible in hospitals and has been proposed as an option, but further study is necessary before widespread use, the authors wrote.
Short-acting opioids may address limitations of other opioids
Lofexidine, an alpha-2-adrenergic agonist, is the only drug approved by the Food and Drug Administration specifically for OWS.
“However,” the authors said, “more than half of patients with OWS treated with lofexidine in phase 3 efficacy trials dropped out by day five. Clonidine, another alpha-2-agonist used off label to treat OWS, has similar effects to those of lofexidine. “
Therefore, short-acting opioids may complement methadone and buprenorphine in treating OWS in the hospital by addressing their limitations, the authors wrote.
Dr. Kleinman and Dr. Wakeman also say short-acting opioids may help with starting buprenorphine for patients exposed to fentanyl, because short-acting opioids can relieve withdrawal symptoms while fentanyl is metabolized and excreted.
Supplementation with short-acting opioids within the hospital can relieve withdrawal symptoms and help keep patients comfortable while methadone is titrated to more effective doses for long-term treatment, they wrote.
With short-acting opioids, patients may become more engaged in their care with, for example, a tamper-proof, patient-controlled analgesia pump, which would allow them to have more autonomy in administration of opioids to relieve pain and withdrawal symptoms, the authors wrote.
Dr. Kleinman and Dr. Wakeman noted that many patients who inject drugs already consume short-acting illicit drugs in the hospital, typically in washrooms and smoking areas, so supervised use of short-acting opioids helps eliminate the risk for unwitnessed overdoses.
Barriers to short-acting opioid use
Despite use of short-acting opioids internationally, barriers in the United States include limited prospective, randomized, controlled research on their benefits. There is limited institutional support for such approaches, and concerns and stigma around providing opioids to patients with OUD.
“[M]any institutions have insufficient numbers of providers who are both confident and competent with standard buprenorphine and methadone initiation approaches, a prerequisite before adopting more complex regimens,” the authors wrote.
Short-acting, full-agonist opioids, as a complement to methadone or buprenorphine, is already recommended for inpatients with OUD who are experiencing acute pain.
But the authors argue it should be an option when pain is not present, but methadone or buprenorphine have not provided enough OWS relief.
When short-acting opioids are helpful, according to outside expert
Dr. Poorman agrees and says she has found short-acting opioids simple to use in the hospital and very helpful in two situations.
One is when patients are very clear that they don’t want any medication for opioid use disorder, but they do want to be treated for their acute medical issue.
“I thought that was a fantastic tool to have to demonstrate we’re listening to them and weren’t trying to impose something on them and left the door open to come back when they did want treatment, which many of them did,” Dr. Poorman said.
The second situation is when the patient is uncertain about options but very afraid of precipitated withdrawal from buprenorphine.
She said she then found it easy to switch from those medications to buprenorphine and methadone.
Dr. Poorman described a situation she encountered previously where the patient was injecting heroin several times a day for 30-40 years. He was very clear he wasn’t going to stop injecting heroin, but he needed medical attention. He was willing to get medical attention, but he told his doctor he didn’t want to be uncomfortable while in the hospital.
It was very hard for his doctor to accept relieving his symptoms of withdrawal as part of her job, because she felt as though she was condoning his drug use, Dr. Poorman explained.
But Dr. Poorman said it’s not realistic to think that someone who clearly does not want to stop using is going to stop using because a doctor made that person go through painful withdrawal “that they’ve structured their whole life around avoiding.”
Take-home message
“We need to understand that addiction is very complex. A lot of times people come to us distressed, and it’s a great time to engage them in care but engaging them in care doesn’t mean imposing discomfort or pain on them,” Dr. Poorman noted. Instead, it means “listening to them, helping them be comfortable in a really stressful situation and then letting them know we are always there for them wherever they are on their disease process or recovery journey so that they can come back to us.”
Dr. Wakeman previously served on clinical advisory board for Celero Systems and receives textbook royalties from Springer and author payment from UpToDate. Dr. Kleinman and Dr. Poorman declared no relevant financial relationships.
The commentary by Robert A. Kleinman, MD, with the Centre for Addiction and Mental Health, and department of psychiatry, University of Toronto, and Sarah E. Wakeman, MD, with the division of general internal medicine at Massachusetts General Hospital, and Harvard Medical School, Boston, was published in Annals of Internal Medicine.
Currently, short-acting opioids are not recommended in the United States for opioid withdrawal symptoms (OWS) management in the hospital, the authors wrote. Instead, withdrawal symptoms are typically treated, followed by methadone or buprenorphine or nonopioid medications, but many patients don’t get enough relief. Undertreated withdrawal can result in patients leaving the hospital against medical advice, which is linked with higher risk of death.
Addiction specialist Elisabeth Poorman, MD, of the University of Illinois Chicago, said in an interview that she agrees it’s time to start shifting the thinking on using short-acting opioids for OWS in hospitals. Use varies greatly by hospital and by clinician, she said.
“It’s time to let evidence guide us and to be flexible,” Dr. Poorman said.
The commentary authors noted that with methadone, patients must wait several hours for maximal symptom reduction, and the full benefits of methadone treatment are not realized until days after initiation.
Rapid initiation of methadone may be feasible in hospitals and has been proposed as an option, but further study is necessary before widespread use, the authors wrote.
Short-acting opioids may address limitations of other opioids
Lofexidine, an alpha-2-adrenergic agonist, is the only drug approved by the Food and Drug Administration specifically for OWS.
“However,” the authors said, “more than half of patients with OWS treated with lofexidine in phase 3 efficacy trials dropped out by day five. Clonidine, another alpha-2-agonist used off label to treat OWS, has similar effects to those of lofexidine. “
Therefore, short-acting opioids may complement methadone and buprenorphine in treating OWS in the hospital by addressing their limitations, the authors wrote.
Dr. Kleinman and Dr. Wakeman also say short-acting opioids may help with starting buprenorphine for patients exposed to fentanyl, because short-acting opioids can relieve withdrawal symptoms while fentanyl is metabolized and excreted.
Supplementation with short-acting opioids within the hospital can relieve withdrawal symptoms and help keep patients comfortable while methadone is titrated to more effective doses for long-term treatment, they wrote.
With short-acting opioids, patients may become more engaged in their care with, for example, a tamper-proof, patient-controlled analgesia pump, which would allow them to have more autonomy in administration of opioids to relieve pain and withdrawal symptoms, the authors wrote.
Dr. Kleinman and Dr. Wakeman noted that many patients who inject drugs already consume short-acting illicit drugs in the hospital, typically in washrooms and smoking areas, so supervised use of short-acting opioids helps eliminate the risk for unwitnessed overdoses.
Barriers to short-acting opioid use
Despite use of short-acting opioids internationally, barriers in the United States include limited prospective, randomized, controlled research on their benefits. There is limited institutional support for such approaches, and concerns and stigma around providing opioids to patients with OUD.
“[M]any institutions have insufficient numbers of providers who are both confident and competent with standard buprenorphine and methadone initiation approaches, a prerequisite before adopting more complex regimens,” the authors wrote.
Short-acting, full-agonist opioids, as a complement to methadone or buprenorphine, is already recommended for inpatients with OUD who are experiencing acute pain.
But the authors argue it should be an option when pain is not present, but methadone or buprenorphine have not provided enough OWS relief.
When short-acting opioids are helpful, according to outside expert
Dr. Poorman agrees and says she has found short-acting opioids simple to use in the hospital and very helpful in two situations.
One is when patients are very clear that they don’t want any medication for opioid use disorder, but they do want to be treated for their acute medical issue.
“I thought that was a fantastic tool to have to demonstrate we’re listening to them and weren’t trying to impose something on them and left the door open to come back when they did want treatment, which many of them did,” Dr. Poorman said.
The second situation is when the patient is uncertain about options but very afraid of precipitated withdrawal from buprenorphine.
She said she then found it easy to switch from those medications to buprenorphine and methadone.
Dr. Poorman described a situation she encountered previously where the patient was injecting heroin several times a day for 30-40 years. He was very clear he wasn’t going to stop injecting heroin, but he needed medical attention. He was willing to get medical attention, but he told his doctor he didn’t want to be uncomfortable while in the hospital.
It was very hard for his doctor to accept relieving his symptoms of withdrawal as part of her job, because she felt as though she was condoning his drug use, Dr. Poorman explained.
But Dr. Poorman said it’s not realistic to think that someone who clearly does not want to stop using is going to stop using because a doctor made that person go through painful withdrawal “that they’ve structured their whole life around avoiding.”
Take-home message
“We need to understand that addiction is very complex. A lot of times people come to us distressed, and it’s a great time to engage them in care but engaging them in care doesn’t mean imposing discomfort or pain on them,” Dr. Poorman noted. Instead, it means “listening to them, helping them be comfortable in a really stressful situation and then letting them know we are always there for them wherever they are on their disease process or recovery journey so that they can come back to us.”
Dr. Wakeman previously served on clinical advisory board for Celero Systems and receives textbook royalties from Springer and author payment from UpToDate. Dr. Kleinman and Dr. Poorman declared no relevant financial relationships.
FROM ANNALS OF INTERNAL MEDICINE
Inexplicably drunk: A case of an underdiagnosed condition?
A 46-year-old North Carolina man, who was pulled over on suspicion of drunk driving, vehemently denied consuming alcohol. When he refused to take a breathalyzer test, he was hospitalized and doctors confirmed what police suspected – his blood alcohol level was 0.20, two-and-a-half times the state’s legal limit – and he was charged with driving while intoxicated (DWI).
For an entire year after his arrest, the cause of his “intoxication” remained a mystery. It wasn’t until his aunt learned about a similar case that had been successfully treated at an Ohio clinic that he understood what was happening to him – he had auto brewery syndrome (ABS).
and suffer all the medical and social implications of alcoholism.
“ABS occurs when ingested carbohydrates are converted to alcohol by fungi in the gastrointestinal tract,” Fahad Malik, MD, who reported the case in BMJ Open Gastroenterology while a resident at Richmond University Medical Center in New York, told this news organization.
At the urging of his aunt, the patient attended the Ohio clinic where he underwent a complete blood count, comprehensive metabolic panel, immunology panel and urinalysis, all of which were normal.
However, stool testing revealed the presence of two strains of yeast – Saccharomyces cerevisiae, commonly used in winemaking, baking, and beer brewing, and Saccharomyces boulardii.
To confirm the ABS diagnosis, the patient received a carbohydrate meal and clinicians monitored his blood alcohol level, which, after 8 hours, reached 57 mg/dL. He was treated with antifungals for the Saccharomyces fungi in his stool and discharged on a strict carbohydrate-free diet along with special supplements, including multivitamins and probiotics, but no further antifungal therapy.
Probiotics, said Dr. Malik, competitively inhibit bad bacteria and fungi, but currently there is evidence to show they are useful for ABS.
Although the patient adhered to his prescribed treatment regimen, after a few weeks of no symptoms, intermittent “flares” returned. In one instance of inebriation, he fell and hit his head, resulting in intracranial bleeding that resulted in a transfer to a neurosurgical center. During his hospital stay, his blood alcohol levels ranged from 50 to 400 mg/dL.
Antibiotics the culprit?
Disheartened by the continuation of his symptoms, the patient sought support from an online forum. It was there he read about Dr. Malik and gastroenterologist Prasanna Wickremesinghe, MD (a colleague of Dr. Malik’s at Richmond MC), who had treated a complicated, very similar case of ABS. The patient made contact with the two physicians and they assessed him.
“We went from A to Z with the patient, because we were trying to look for similar things in the history – we wanted to know the exact point at which it started and understand when he started experiencing mental fog,” said Dr. Malik.
After speaking to the patient, Dr. Malik and Dr. Wickremesinghe traced his initial symptoms to a 2011 course of antibiotics (cephalexin 250 mg oral three times a day for 3 weeks) prescribed for a complicated traumatic thumb injury.
About a week after he finished the antibiotics, he experienced noticeable behavioral changes, including depression, brain fog, and aggressive outbursts, all of which were very uncharacteristic.
He visited his primary care physician in 2014 for treatment, which resulted in a referral to a psychiatrist, who treated him with lorazepam and fluoxetine. The patient noted that he was previously healthy, with no significant medical or psychiatric history.
Dr. Malik believes the antibiotics prescribed all those years ago is the culprit. “We were postulating that the antibiotics had changed the microbiome of his gut and allowed the fungi to develop,” he said.
Since there are no established diagnostic criteria or treatment regimen for ABS, Dr. Malik and Dr. Wickremesinghe developed their own.
Diagnosis consisted of a standardized carbohydrate challenge test vs. a carbohydrate meal, where they gave the patient 200 g of glucose by mouth after an overnight fast and drew blood at timed intervals of 0, 0.5, 1, 2, 4, 8, 16, and 24 hours to test for glucose and blood alcohol levels.
“After that we needed to isolate the fungi by examining the gut secretions through an upper and lower endoscopy,” said Dr. Wickremesinghe. Fungal cultures from the upper small gut and cecal secretions grew Candida albicans and C. parapsilosis.
Both fungi were sensitive to azoles and the physicians prescribed oral itraconazole 150 mg per day as an initial therapy. After 10 days, his symptoms did not improve so the dose was increased to 200 mg/day and the patient became “completely asymptomatic.”
“We had nothing to follow. We didn’t know how long to treat the patient, it was really just a process of trial and error,” said Dr. Malik. The physicians asked the patient to monitor his breath alcohol levels twice a day during treatment and immediately report any increases. Over time, he also received treatment with various probiotics to help normalize his gut flora.
Underdiagnosed condition?
At the time of the case study’s publication in the summer of 2019, the patient had been asymptomatic for 18 months and had been able to resume a normal diet, but still checks his breath alcohol levels from time to time.
“Before this patient’s case, I went all through the literature and found only a few cases of ABS,” said Dr. Malik.
However, he added, after this case study was published 10 other patients contacted him with a similar history of antibiotic use and the same symptoms. This, said Dr. Malik, is “significant” and suggests ABS is much more common than previously thought.
The clinicians also note that to the best of their knowledge this is the first report of antibiotic exposure initiating ABS.
“What we tried to do was set up a protocol by which to identify these patients, confirm a diagnosis, and treat them for a sufficient amount of time,” said Dr. Wickremesinghe. “We also wanted to inform other physicians that this may function as a standardized way of treating these patients, and may promote further study,” added Dr. Malik, who emphasized that the role of probiotics in ABS still needs to be studied.
Dr. Malik and Dr. Wickremesinghe note that physicians should be aware that mood changes, brain fog, and delirium in patients who deny alcohol ingestion may be the first symptoms of ABS.
Dr. Wickremesinghe said since the case study was published he and Dr. Malik have received queries from all over the world. “It’s unbelievable the amount of interest we have had in the paper, so if we have made the medical community and the general population aware of this condition and how to treat it, we have done a major thing for medicine,” he said.
A version of this article first appeared on Medscape.com.
A 46-year-old North Carolina man, who was pulled over on suspicion of drunk driving, vehemently denied consuming alcohol. When he refused to take a breathalyzer test, he was hospitalized and doctors confirmed what police suspected – his blood alcohol level was 0.20, two-and-a-half times the state’s legal limit – and he was charged with driving while intoxicated (DWI).
For an entire year after his arrest, the cause of his “intoxication” remained a mystery. It wasn’t until his aunt learned about a similar case that had been successfully treated at an Ohio clinic that he understood what was happening to him – he had auto brewery syndrome (ABS).
and suffer all the medical and social implications of alcoholism.
“ABS occurs when ingested carbohydrates are converted to alcohol by fungi in the gastrointestinal tract,” Fahad Malik, MD, who reported the case in BMJ Open Gastroenterology while a resident at Richmond University Medical Center in New York, told this news organization.
At the urging of his aunt, the patient attended the Ohio clinic where he underwent a complete blood count, comprehensive metabolic panel, immunology panel and urinalysis, all of which were normal.
However, stool testing revealed the presence of two strains of yeast – Saccharomyces cerevisiae, commonly used in winemaking, baking, and beer brewing, and Saccharomyces boulardii.
To confirm the ABS diagnosis, the patient received a carbohydrate meal and clinicians monitored his blood alcohol level, which, after 8 hours, reached 57 mg/dL. He was treated with antifungals for the Saccharomyces fungi in his stool and discharged on a strict carbohydrate-free diet along with special supplements, including multivitamins and probiotics, but no further antifungal therapy.
Probiotics, said Dr. Malik, competitively inhibit bad bacteria and fungi, but currently there is evidence to show they are useful for ABS.
Although the patient adhered to his prescribed treatment regimen, after a few weeks of no symptoms, intermittent “flares” returned. In one instance of inebriation, he fell and hit his head, resulting in intracranial bleeding that resulted in a transfer to a neurosurgical center. During his hospital stay, his blood alcohol levels ranged from 50 to 400 mg/dL.
Antibiotics the culprit?
Disheartened by the continuation of his symptoms, the patient sought support from an online forum. It was there he read about Dr. Malik and gastroenterologist Prasanna Wickremesinghe, MD (a colleague of Dr. Malik’s at Richmond MC), who had treated a complicated, very similar case of ABS. The patient made contact with the two physicians and they assessed him.
“We went from A to Z with the patient, because we were trying to look for similar things in the history – we wanted to know the exact point at which it started and understand when he started experiencing mental fog,” said Dr. Malik.
After speaking to the patient, Dr. Malik and Dr. Wickremesinghe traced his initial symptoms to a 2011 course of antibiotics (cephalexin 250 mg oral three times a day for 3 weeks) prescribed for a complicated traumatic thumb injury.
About a week after he finished the antibiotics, he experienced noticeable behavioral changes, including depression, brain fog, and aggressive outbursts, all of which were very uncharacteristic.
He visited his primary care physician in 2014 for treatment, which resulted in a referral to a psychiatrist, who treated him with lorazepam and fluoxetine. The patient noted that he was previously healthy, with no significant medical or psychiatric history.
Dr. Malik believes the antibiotics prescribed all those years ago is the culprit. “We were postulating that the antibiotics had changed the microbiome of his gut and allowed the fungi to develop,” he said.
Since there are no established diagnostic criteria or treatment regimen for ABS, Dr. Malik and Dr. Wickremesinghe developed their own.
Diagnosis consisted of a standardized carbohydrate challenge test vs. a carbohydrate meal, where they gave the patient 200 g of glucose by mouth after an overnight fast and drew blood at timed intervals of 0, 0.5, 1, 2, 4, 8, 16, and 24 hours to test for glucose and blood alcohol levels.
“After that we needed to isolate the fungi by examining the gut secretions through an upper and lower endoscopy,” said Dr. Wickremesinghe. Fungal cultures from the upper small gut and cecal secretions grew Candida albicans and C. parapsilosis.
Both fungi were sensitive to azoles and the physicians prescribed oral itraconazole 150 mg per day as an initial therapy. After 10 days, his symptoms did not improve so the dose was increased to 200 mg/day and the patient became “completely asymptomatic.”
“We had nothing to follow. We didn’t know how long to treat the patient, it was really just a process of trial and error,” said Dr. Malik. The physicians asked the patient to monitor his breath alcohol levels twice a day during treatment and immediately report any increases. Over time, he also received treatment with various probiotics to help normalize his gut flora.
Underdiagnosed condition?
At the time of the case study’s publication in the summer of 2019, the patient had been asymptomatic for 18 months and had been able to resume a normal diet, but still checks his breath alcohol levels from time to time.
“Before this patient’s case, I went all through the literature and found only a few cases of ABS,” said Dr. Malik.
However, he added, after this case study was published 10 other patients contacted him with a similar history of antibiotic use and the same symptoms. This, said Dr. Malik, is “significant” and suggests ABS is much more common than previously thought.
The clinicians also note that to the best of their knowledge this is the first report of antibiotic exposure initiating ABS.
“What we tried to do was set up a protocol by which to identify these patients, confirm a diagnosis, and treat them for a sufficient amount of time,” said Dr. Wickremesinghe. “We also wanted to inform other physicians that this may function as a standardized way of treating these patients, and may promote further study,” added Dr. Malik, who emphasized that the role of probiotics in ABS still needs to be studied.
Dr. Malik and Dr. Wickremesinghe note that physicians should be aware that mood changes, brain fog, and delirium in patients who deny alcohol ingestion may be the first symptoms of ABS.
Dr. Wickremesinghe said since the case study was published he and Dr. Malik have received queries from all over the world. “It’s unbelievable the amount of interest we have had in the paper, so if we have made the medical community and the general population aware of this condition and how to treat it, we have done a major thing for medicine,” he said.
A version of this article first appeared on Medscape.com.
A 46-year-old North Carolina man, who was pulled over on suspicion of drunk driving, vehemently denied consuming alcohol. When he refused to take a breathalyzer test, he was hospitalized and doctors confirmed what police suspected – his blood alcohol level was 0.20, two-and-a-half times the state’s legal limit – and he was charged with driving while intoxicated (DWI).
For an entire year after his arrest, the cause of his “intoxication” remained a mystery. It wasn’t until his aunt learned about a similar case that had been successfully treated at an Ohio clinic that he understood what was happening to him – he had auto brewery syndrome (ABS).
and suffer all the medical and social implications of alcoholism.
“ABS occurs when ingested carbohydrates are converted to alcohol by fungi in the gastrointestinal tract,” Fahad Malik, MD, who reported the case in BMJ Open Gastroenterology while a resident at Richmond University Medical Center in New York, told this news organization.
At the urging of his aunt, the patient attended the Ohio clinic where he underwent a complete blood count, comprehensive metabolic panel, immunology panel and urinalysis, all of which were normal.
However, stool testing revealed the presence of two strains of yeast – Saccharomyces cerevisiae, commonly used in winemaking, baking, and beer brewing, and Saccharomyces boulardii.
To confirm the ABS diagnosis, the patient received a carbohydrate meal and clinicians monitored his blood alcohol level, which, after 8 hours, reached 57 mg/dL. He was treated with antifungals for the Saccharomyces fungi in his stool and discharged on a strict carbohydrate-free diet along with special supplements, including multivitamins and probiotics, but no further antifungal therapy.
Probiotics, said Dr. Malik, competitively inhibit bad bacteria and fungi, but currently there is evidence to show they are useful for ABS.
Although the patient adhered to his prescribed treatment regimen, after a few weeks of no symptoms, intermittent “flares” returned. In one instance of inebriation, he fell and hit his head, resulting in intracranial bleeding that resulted in a transfer to a neurosurgical center. During his hospital stay, his blood alcohol levels ranged from 50 to 400 mg/dL.
Antibiotics the culprit?
Disheartened by the continuation of his symptoms, the patient sought support from an online forum. It was there he read about Dr. Malik and gastroenterologist Prasanna Wickremesinghe, MD (a colleague of Dr. Malik’s at Richmond MC), who had treated a complicated, very similar case of ABS. The patient made contact with the two physicians and they assessed him.
“We went from A to Z with the patient, because we were trying to look for similar things in the history – we wanted to know the exact point at which it started and understand when he started experiencing mental fog,” said Dr. Malik.
After speaking to the patient, Dr. Malik and Dr. Wickremesinghe traced his initial symptoms to a 2011 course of antibiotics (cephalexin 250 mg oral three times a day for 3 weeks) prescribed for a complicated traumatic thumb injury.
About a week after he finished the antibiotics, he experienced noticeable behavioral changes, including depression, brain fog, and aggressive outbursts, all of which were very uncharacteristic.
He visited his primary care physician in 2014 for treatment, which resulted in a referral to a psychiatrist, who treated him with lorazepam and fluoxetine. The patient noted that he was previously healthy, with no significant medical or psychiatric history.
Dr. Malik believes the antibiotics prescribed all those years ago is the culprit. “We were postulating that the antibiotics had changed the microbiome of his gut and allowed the fungi to develop,” he said.
Since there are no established diagnostic criteria or treatment regimen for ABS, Dr. Malik and Dr. Wickremesinghe developed their own.
Diagnosis consisted of a standardized carbohydrate challenge test vs. a carbohydrate meal, where they gave the patient 200 g of glucose by mouth after an overnight fast and drew blood at timed intervals of 0, 0.5, 1, 2, 4, 8, 16, and 24 hours to test for glucose and blood alcohol levels.
“After that we needed to isolate the fungi by examining the gut secretions through an upper and lower endoscopy,” said Dr. Wickremesinghe. Fungal cultures from the upper small gut and cecal secretions grew Candida albicans and C. parapsilosis.
Both fungi were sensitive to azoles and the physicians prescribed oral itraconazole 150 mg per day as an initial therapy. After 10 days, his symptoms did not improve so the dose was increased to 200 mg/day and the patient became “completely asymptomatic.”
“We had nothing to follow. We didn’t know how long to treat the patient, it was really just a process of trial and error,” said Dr. Malik. The physicians asked the patient to monitor his breath alcohol levels twice a day during treatment and immediately report any increases. Over time, he also received treatment with various probiotics to help normalize his gut flora.
Underdiagnosed condition?
At the time of the case study’s publication in the summer of 2019, the patient had been asymptomatic for 18 months and had been able to resume a normal diet, but still checks his breath alcohol levels from time to time.
“Before this patient’s case, I went all through the literature and found only a few cases of ABS,” said Dr. Malik.
However, he added, after this case study was published 10 other patients contacted him with a similar history of antibiotic use and the same symptoms. This, said Dr. Malik, is “significant” and suggests ABS is much more common than previously thought.
The clinicians also note that to the best of their knowledge this is the first report of antibiotic exposure initiating ABS.
“What we tried to do was set up a protocol by which to identify these patients, confirm a diagnosis, and treat them for a sufficient amount of time,” said Dr. Wickremesinghe. “We also wanted to inform other physicians that this may function as a standardized way of treating these patients, and may promote further study,” added Dr. Malik, who emphasized that the role of probiotics in ABS still needs to be studied.
Dr. Malik and Dr. Wickremesinghe note that physicians should be aware that mood changes, brain fog, and delirium in patients who deny alcohol ingestion may be the first symptoms of ABS.
Dr. Wickremesinghe said since the case study was published he and Dr. Malik have received queries from all over the world. “It’s unbelievable the amount of interest we have had in the paper, so if we have made the medical community and the general population aware of this condition and how to treat it, we have done a major thing for medicine,” he said.
A version of this article first appeared on Medscape.com.
TikTok trends: Scalp popping, EpiPen tutorial, and plant juice
With the holidays just around the corner (how did that happen?), it’s a good time to remind yourself of the things you’re grateful for.
Perhaps you’re grateful for spending chilly evenings under a warm blanket binge-watching your favorite shows or being able to safely gather with loved ones. If you’re William Shatner, maybe you’re grateful for that quick trip to space (because apparently, that’s a thing now) and the poetic tweets it induced. Down here on earth, TikTok has surpassed 1 billion users, and while we’re not grateful, necessarily, we are entertained.
Here are the latest ugly, good, and bad TikToks that have been trending lately.
The Ugly: Scalp popping
Warning: Don’t watch this if you’re easily freaked out by weird body sounds. It’s like cracking your knuckles but way, way worse.
This TikTok from @asmr.barber has 1.7 million likes, and lots of people are trying it out for themselves. The viral video features the (disturbed) art of scalp popping, also known as hair cracking. It features what is assumed to be some sort of barber or professional (here’s hoping) twisting a client’s hair around his fingers and then yanking, creating an audible popping sound. Many are posting their own hair-cracking attempts on the platform. It’s unclear if this is supposed to feel good or just be grossly satisfying, though some users claim it helps with migraines.
But it turns out this might be more than kind of gross; it can be dangerous, too.
Anthony Youn, MD, a board-certified plastic surgeon, comments on the trend with concern: “What the hell is going on here?” Not something you want to hear from a doctor. Dr. Youn explained that the popping sound comes from the galea aponeurotica, a fibrous sheet of connective tissue under your scalp, being pulled off the skull.
In a comment, Dr. Youn continued to warn people of replicating this trend: “It can tear the inside of the scalp, which can bleed a ton on the inside. Think boxer or MMA fighter with scalp hematoma.”
Let’s keep our scalps attached to our skulls, people. If I never have to hear that sound again, I’ll be eternally grateful.
The Good: Doctor demonstrates correct EpiPen use
This reaction TikTok from medical student Mutahir Farhan (aka @madmedicine) has over 252,000 likes and hundreds of comments. In it, Ms. Farhan watches a video of a young woman attempting to administer an EpiPen to her friend, with the caption “How NOT to use an EpiPen” over it (in bright red, of course).
The woman in the video is using the wrong end of the EpiPen against her friend’s leg, so it isn’t working. When she uses her thumb to press down and help, her thumb is actually pressed against the needle end and the EpiPen sticks her instead of her friend. Ouch!
Ms. Farhan goes on to explain the anatomy of the EpiPen and shows his audience of 1.1 million followers where to inject it.
“You gotta remember that the orange tip is where the needle comes out. Otherwise, you’re going to end up stabbing yourself with epinephrine, like that girl in the video,” Ms. Farhan says. He goes on to instruct the important, but often overlooked, follow-up: “After you stab someone with epinephrine, call 911 or go to the ER, so that we can make sure they’re actually okay and good to go.”
The Bad: Liquid chlorophyll
Here is another one of those tricky trends that are so widespread and popular that it’s hard to find exactly where it originated from. A video from @lenamaiah has over 5 million views and 800,000 likes, which even by TikTok standards, is a lot. TikTok is rife with similar videos, which feature drops of liquid chlorophyll being added to water and smoothies.
The pretty emerald hue is mesmerizing and it’s hard to resist trying it out when it’s being peddled by seemingly every pretty, smooth-skinned pseudo-model on the platform. In this video, Lena says drinking a glass of water with a few drops of chlorophyll can reduce inflammation, get rid of eye bags, boost your vitamin levels, reduce free radical damage, detoxify your system, and file your taxes. Okay, I made that last one up, but it follows, doesn’t it? This stuff sounds pretty good. Maybe too good.
Chlorophyll, if you skipped biology class (somehow, I doubt you did), is what makes plants green. Medscape has a detailed explanation of chlorophyll, but all you really need to know is that it’s the secret to that cool thing plants do: photosynthesis, or turning sunlight into energy. Scientists have been trying to find uses for it in people since the 1940s. Unfortunately, studies never found much that it can do for us, aside from being kind of deodorizing. So, while it’s been historically marketed as toothpaste and deodorant, the new TikTok claims of it being a cure-all or the next big skincare supplement are not widely substantiated by scientific studies. The only real evidence of it being effective is word of mouth from those who claim to like the way they look or feel since taking it, which isn’t enough for doctors to recommend it.
TikTok’s resident dermatologist, Muneeb Shah, DO, stitched a TikTok from another user, with his captions explaining, “[There’s] no scientific evidence for liquid chlorophyll [helping] rosacea or acne.”
His advice: “Chlorophyll is great, but just eat more veggies.”
A version of this article first appeared on Medscape.com.
With the holidays just around the corner (how did that happen?), it’s a good time to remind yourself of the things you’re grateful for.
Perhaps you’re grateful for spending chilly evenings under a warm blanket binge-watching your favorite shows or being able to safely gather with loved ones. If you’re William Shatner, maybe you’re grateful for that quick trip to space (because apparently, that’s a thing now) and the poetic tweets it induced. Down here on earth, TikTok has surpassed 1 billion users, and while we’re not grateful, necessarily, we are entertained.
Here are the latest ugly, good, and bad TikToks that have been trending lately.
The Ugly: Scalp popping
Warning: Don’t watch this if you’re easily freaked out by weird body sounds. It’s like cracking your knuckles but way, way worse.
This TikTok from @asmr.barber has 1.7 million likes, and lots of people are trying it out for themselves. The viral video features the (disturbed) art of scalp popping, also known as hair cracking. It features what is assumed to be some sort of barber or professional (here’s hoping) twisting a client’s hair around his fingers and then yanking, creating an audible popping sound. Many are posting their own hair-cracking attempts on the platform. It’s unclear if this is supposed to feel good or just be grossly satisfying, though some users claim it helps with migraines.
But it turns out this might be more than kind of gross; it can be dangerous, too.
Anthony Youn, MD, a board-certified plastic surgeon, comments on the trend with concern: “What the hell is going on here?” Not something you want to hear from a doctor. Dr. Youn explained that the popping sound comes from the galea aponeurotica, a fibrous sheet of connective tissue under your scalp, being pulled off the skull.
In a comment, Dr. Youn continued to warn people of replicating this trend: “It can tear the inside of the scalp, which can bleed a ton on the inside. Think boxer or MMA fighter with scalp hematoma.”
Let’s keep our scalps attached to our skulls, people. If I never have to hear that sound again, I’ll be eternally grateful.
The Good: Doctor demonstrates correct EpiPen use
This reaction TikTok from medical student Mutahir Farhan (aka @madmedicine) has over 252,000 likes and hundreds of comments. In it, Ms. Farhan watches a video of a young woman attempting to administer an EpiPen to her friend, with the caption “How NOT to use an EpiPen” over it (in bright red, of course).
The woman in the video is using the wrong end of the EpiPen against her friend’s leg, so it isn’t working. When she uses her thumb to press down and help, her thumb is actually pressed against the needle end and the EpiPen sticks her instead of her friend. Ouch!
Ms. Farhan goes on to explain the anatomy of the EpiPen and shows his audience of 1.1 million followers where to inject it.
“You gotta remember that the orange tip is where the needle comes out. Otherwise, you’re going to end up stabbing yourself with epinephrine, like that girl in the video,” Ms. Farhan says. He goes on to instruct the important, but often overlooked, follow-up: “After you stab someone with epinephrine, call 911 or go to the ER, so that we can make sure they’re actually okay and good to go.”
The Bad: Liquid chlorophyll
Here is another one of those tricky trends that are so widespread and popular that it’s hard to find exactly where it originated from. A video from @lenamaiah has over 5 million views and 800,000 likes, which even by TikTok standards, is a lot. TikTok is rife with similar videos, which feature drops of liquid chlorophyll being added to water and smoothies.
The pretty emerald hue is mesmerizing and it’s hard to resist trying it out when it’s being peddled by seemingly every pretty, smooth-skinned pseudo-model on the platform. In this video, Lena says drinking a glass of water with a few drops of chlorophyll can reduce inflammation, get rid of eye bags, boost your vitamin levels, reduce free radical damage, detoxify your system, and file your taxes. Okay, I made that last one up, but it follows, doesn’t it? This stuff sounds pretty good. Maybe too good.
Chlorophyll, if you skipped biology class (somehow, I doubt you did), is what makes plants green. Medscape has a detailed explanation of chlorophyll, but all you really need to know is that it’s the secret to that cool thing plants do: photosynthesis, or turning sunlight into energy. Scientists have been trying to find uses for it in people since the 1940s. Unfortunately, studies never found much that it can do for us, aside from being kind of deodorizing. So, while it’s been historically marketed as toothpaste and deodorant, the new TikTok claims of it being a cure-all or the next big skincare supplement are not widely substantiated by scientific studies. The only real evidence of it being effective is word of mouth from those who claim to like the way they look or feel since taking it, which isn’t enough for doctors to recommend it.
TikTok’s resident dermatologist, Muneeb Shah, DO, stitched a TikTok from another user, with his captions explaining, “[There’s] no scientific evidence for liquid chlorophyll [helping] rosacea or acne.”
His advice: “Chlorophyll is great, but just eat more veggies.”
A version of this article first appeared on Medscape.com.
With the holidays just around the corner (how did that happen?), it’s a good time to remind yourself of the things you’re grateful for.
Perhaps you’re grateful for spending chilly evenings under a warm blanket binge-watching your favorite shows or being able to safely gather with loved ones. If you’re William Shatner, maybe you’re grateful for that quick trip to space (because apparently, that’s a thing now) and the poetic tweets it induced. Down here on earth, TikTok has surpassed 1 billion users, and while we’re not grateful, necessarily, we are entertained.
Here are the latest ugly, good, and bad TikToks that have been trending lately.
The Ugly: Scalp popping
Warning: Don’t watch this if you’re easily freaked out by weird body sounds. It’s like cracking your knuckles but way, way worse.
This TikTok from @asmr.barber has 1.7 million likes, and lots of people are trying it out for themselves. The viral video features the (disturbed) art of scalp popping, also known as hair cracking. It features what is assumed to be some sort of barber or professional (here’s hoping) twisting a client’s hair around his fingers and then yanking, creating an audible popping sound. Many are posting their own hair-cracking attempts on the platform. It’s unclear if this is supposed to feel good or just be grossly satisfying, though some users claim it helps with migraines.
But it turns out this might be more than kind of gross; it can be dangerous, too.
Anthony Youn, MD, a board-certified plastic surgeon, comments on the trend with concern: “What the hell is going on here?” Not something you want to hear from a doctor. Dr. Youn explained that the popping sound comes from the galea aponeurotica, a fibrous sheet of connective tissue under your scalp, being pulled off the skull.
In a comment, Dr. Youn continued to warn people of replicating this trend: “It can tear the inside of the scalp, which can bleed a ton on the inside. Think boxer or MMA fighter with scalp hematoma.”
Let’s keep our scalps attached to our skulls, people. If I never have to hear that sound again, I’ll be eternally grateful.
The Good: Doctor demonstrates correct EpiPen use
This reaction TikTok from medical student Mutahir Farhan (aka @madmedicine) has over 252,000 likes and hundreds of comments. In it, Ms. Farhan watches a video of a young woman attempting to administer an EpiPen to her friend, with the caption “How NOT to use an EpiPen” over it (in bright red, of course).
The woman in the video is using the wrong end of the EpiPen against her friend’s leg, so it isn’t working. When she uses her thumb to press down and help, her thumb is actually pressed against the needle end and the EpiPen sticks her instead of her friend. Ouch!
Ms. Farhan goes on to explain the anatomy of the EpiPen and shows his audience of 1.1 million followers where to inject it.
“You gotta remember that the orange tip is where the needle comes out. Otherwise, you’re going to end up stabbing yourself with epinephrine, like that girl in the video,” Ms. Farhan says. He goes on to instruct the important, but often overlooked, follow-up: “After you stab someone with epinephrine, call 911 or go to the ER, so that we can make sure they’re actually okay and good to go.”
The Bad: Liquid chlorophyll
Here is another one of those tricky trends that are so widespread and popular that it’s hard to find exactly where it originated from. A video from @lenamaiah has over 5 million views and 800,000 likes, which even by TikTok standards, is a lot. TikTok is rife with similar videos, which feature drops of liquid chlorophyll being added to water and smoothies.
The pretty emerald hue is mesmerizing and it’s hard to resist trying it out when it’s being peddled by seemingly every pretty, smooth-skinned pseudo-model on the platform. In this video, Lena says drinking a glass of water with a few drops of chlorophyll can reduce inflammation, get rid of eye bags, boost your vitamin levels, reduce free radical damage, detoxify your system, and file your taxes. Okay, I made that last one up, but it follows, doesn’t it? This stuff sounds pretty good. Maybe too good.
Chlorophyll, if you skipped biology class (somehow, I doubt you did), is what makes plants green. Medscape has a detailed explanation of chlorophyll, but all you really need to know is that it’s the secret to that cool thing plants do: photosynthesis, or turning sunlight into energy. Scientists have been trying to find uses for it in people since the 1940s. Unfortunately, studies never found much that it can do for us, aside from being kind of deodorizing. So, while it’s been historically marketed as toothpaste and deodorant, the new TikTok claims of it being a cure-all or the next big skincare supplement are not widely substantiated by scientific studies. The only real evidence of it being effective is word of mouth from those who claim to like the way they look or feel since taking it, which isn’t enough for doctors to recommend it.
TikTok’s resident dermatologist, Muneeb Shah, DO, stitched a TikTok from another user, with his captions explaining, “[There’s] no scientific evidence for liquid chlorophyll [helping] rosacea or acne.”
His advice: “Chlorophyll is great, but just eat more veggies.”
A version of this article first appeared on Medscape.com.
Social media use associated with depression in adults
Use of social media has been linked to increased anxiety and depression, as well as reduced well-being in adolescents and young adults, but similar associations in older adults have not been well studied, and longitudinal data are lacking, Ron H. Perlis, MD, of Massachusetts General Hospital, Boston, and colleagues wrote in their paper, which was published in JAMA Network Open.
To examine the association between social media use and depressive symptoms in older adults, the researchers reviewed data from 13 waves of an internet survey conducted each month between May 2020 and May 2021. The survey respondents included individuals aged 18 years and older, with a mean age of 56 years.
In the study the researchers analyzed responses from 5,395 individuals aged 18 years and older, with a mean age of 56 years. The study participants had minimal or no depressive symptoms at baseline, according to scores on the nine-item Patient Health Questionnaire (PHQ-9).
Overall, 8.9% of the respondents reported a worsening of 5 points or more on the PHQ-9 score on a follow-up survey, which was the primary outcome. Participants who reported using social media platforms Snapchat, Facebook, or TikTok were significantly more likely to report increased depressive symptoms, compared with those who did not report use of social media. The fully adjusted odds ratio was largest for Snapchat (aOR, 1.53), followed by Facebook (aOR, 1.42), and TikTok (aOR, 1.39).
Incorporating recent television and internet news terms, such as COVID-19, changed the association for Snapchat, for which the aOR decreased from 1.53 to 1.12 when news source terms were included in the survey. TikTok and Facebook associations remained similar.
When the results were further stratified by age, use of TikTok and Snapchat was associated with depressive symptoms in those aged 35 years and older, but not in those younger than 35 years. However, the opposite pattern emerged for Facebook; use was associated with depressive symptoms for individuals younger than 35 years, but not in those aged 35 years and older (aOR, 2.60 vs. aOR, 1.12).
The association between increased self-reported depressive symptoms and use of certain social media platforms was not impacted by baseline social support or face-to-face interactions, the researchers noted.
Family physician was surprised results weren’t more significant
In the current study, “I was honestly surprised the results weren’t more significant,” Mary Ann Dakkak, MD, of Boston University said in an interview. “That said, social media uses during the COVID pandemic may have been a necessary social outlet and form of connection for many people who were otherwise isolated.”
To still see a significant increase in depression when social media could have been a positive force may suggest a heavier impact during “normal” times, she added.
“It is not surprising that what we see in youth is shown among adults,” noted Dr. Dakkak, who was not involved with this study. “I always tell my patients that what is good for their children is good for the adults too, and vice versa.
“We expect to see outcomes of this on youth and adults who have been more isolated, who have used more screen time for learning, work, connection and boredom, in the near future,” she said. “The complex nature of why social media may have been used more heavily for connection during a time when in-person meetings were not possible may be a heavy confounder as the typical profile of heavy social media users may have differed during the COVID shutdowns.”
Psychiatrist: Balance benefits of social media with mental health risks
The current study was likely conducted before the recent news on “hidden” Facebook data and the implications that Facebook knew it was contributing to worsened mental health in teens, particularly around self-esteem, Jessica “Jessi” Gold, MD, a psychiatrist at Washington University, St. Louis, said in an interview.
“If you look more specifically at other studies, however, the data around social media and mental health is constantly varied, with some showing benefits and some showing negatives, and none conclusively suggesting either way,” said Dr. Gold, who also was not involved with the new research. “More data are needed, especially longitudinally and on a broader age group, to understand social media’s impact on mental health over time.
“It is also even more important in the wake of COVID-19, as so many people have turned to social media as a primary source of social support and connection, and are using it even more than before,” she emphasized.
In the current study, “I think the most interesting information is that, for TikTok and Snapchat, the effects seemed to be more pronounced in those older than 35 years who used social media,” said Dr. Gold.
What this study leaves unanswered is “whether people who might develop depression are simply more prone to use social media in the first place, such as to seek out social support,” Dr. Gold said. “Also, we don’t know anything about how long they are using social media or what they are using it for, which to me is important for understanding more about the nuance of the relationship with mental health and social media.”
Experts advise clinicians to discuss social media with patients
This new research suggests that clinicians should be talking to their patients about how social media impacts their emotional reactions, as well as their sleep, Dr. Gold said.
“Patients should be asking themselves how they are feeling when they are on social media and not using it before sleep. They should also be considering time limits and how to effectively use social media while taking care of their mental health,” she said. This conversation between clinician and patient should be had with any patient of any age, who uses social media, not only with teenagers.
“This is also a conversation about moderation, and knowing that individuals may feel they benefit from social media, that they should balance these benefits with potential mental health risks,” she said.
“Studies such as this one shed light onto why social media consumption should be at least a point of discussion with our patients,” said Dr. Dakkak.
She advised clinicians to ask and listen to patients and their families when it comes to screen time habits. “Whenever I see a patient with mood symptoms, I ask about their habits – eating, sleeping, socializing, screen time – including phone time. I ask about the family dynamics around screen time.
“I’ve added screen time to my adolescent assessment. Discussing safe use of cell phones and social media can have a significant impact on adolescent behavior and wellbeing, and parents are very thankful for the help,” she said. “This study encourages us to add screen time to the assessments we do at all adult ages, especially if mood symptoms exist,” Dr. Dakkak emphasized.
Suggestions for future research
Dr. Dakkak added that more areas for research include the differences in the impact of social media use on content creators versus content consumers. Also, “I would like to see research using the real data of use, the times of use, interruptions in sleep and use, possible confounding variables to include exercise, presence of intimate relationship and school/job performance.”
Given the many confounding variables, more controlled studies are needed to examine mental health outcomes in use, how long people use social media, and the impact of interventions such as time limits, Dr. Gold said.
“We can’t ignore the benefits of social media, such as helping those with social anxiety, finding peer support, and normalizing mental health, and those factors need to be studied and measured more effectively as well, she said.
Take-home message
It is important to recognize that the current study represents a correlation, not causality, said Dr. Gold. In addressing the issues of how social media impact mental health, “as always, the hardest thing is that many people get their news from social media, and often get social support from social media, so there has to be a balance of not removing social media completely, but of helping people see how it affects their mental health and how to find balance.”
The study findings were limited by several factors, including the inability to control for all potential confounders, the inability to assess the nature of social media use, and the lack of dose-response data, the researchers noted. Although the surveys in the current study were not specific to COVID-19, the effects of social media on depression may be specific to the content, and the findings may not generalize beyond the COVID-19 pandemic period.
Approximately two-thirds (66%) of the study participants identified as female, and 76% as White; 11% as Black; 6% as Asian; 5% as Hispanic; and 2% as American Indian or Alaska Native, Pacific Islander or Native Hawaiian, or other.
The National Institute of Mental Health provided a grant for the study to Dr. Pelis, who disclosed consulting fees from various companies and equity in Psy Therapeutics. The study’s lead author also serves as associate editor for JAMA Network Open, but was not involved in the decision process for publication of this study. Dr. Gold disclosed conducting a conference for Johnson & Johnson about social media and health care workers, and was on the advisory council.
Use of social media has been linked to increased anxiety and depression, as well as reduced well-being in adolescents and young adults, but similar associations in older adults have not been well studied, and longitudinal data are lacking, Ron H. Perlis, MD, of Massachusetts General Hospital, Boston, and colleagues wrote in their paper, which was published in JAMA Network Open.
To examine the association between social media use and depressive symptoms in older adults, the researchers reviewed data from 13 waves of an internet survey conducted each month between May 2020 and May 2021. The survey respondents included individuals aged 18 years and older, with a mean age of 56 years.
In the study the researchers analyzed responses from 5,395 individuals aged 18 years and older, with a mean age of 56 years. The study participants had minimal or no depressive symptoms at baseline, according to scores on the nine-item Patient Health Questionnaire (PHQ-9).
Overall, 8.9% of the respondents reported a worsening of 5 points or more on the PHQ-9 score on a follow-up survey, which was the primary outcome. Participants who reported using social media platforms Snapchat, Facebook, or TikTok were significantly more likely to report increased depressive symptoms, compared with those who did not report use of social media. The fully adjusted odds ratio was largest for Snapchat (aOR, 1.53), followed by Facebook (aOR, 1.42), and TikTok (aOR, 1.39).
Incorporating recent television and internet news terms, such as COVID-19, changed the association for Snapchat, for which the aOR decreased from 1.53 to 1.12 when news source terms were included in the survey. TikTok and Facebook associations remained similar.
When the results were further stratified by age, use of TikTok and Snapchat was associated with depressive symptoms in those aged 35 years and older, but not in those younger than 35 years. However, the opposite pattern emerged for Facebook; use was associated with depressive symptoms for individuals younger than 35 years, but not in those aged 35 years and older (aOR, 2.60 vs. aOR, 1.12).
The association between increased self-reported depressive symptoms and use of certain social media platforms was not impacted by baseline social support or face-to-face interactions, the researchers noted.
Family physician was surprised results weren’t more significant
In the current study, “I was honestly surprised the results weren’t more significant,” Mary Ann Dakkak, MD, of Boston University said in an interview. “That said, social media uses during the COVID pandemic may have been a necessary social outlet and form of connection for many people who were otherwise isolated.”
To still see a significant increase in depression when social media could have been a positive force may suggest a heavier impact during “normal” times, she added.
“It is not surprising that what we see in youth is shown among adults,” noted Dr. Dakkak, who was not involved with this study. “I always tell my patients that what is good for their children is good for the adults too, and vice versa.
“We expect to see outcomes of this on youth and adults who have been more isolated, who have used more screen time for learning, work, connection and boredom, in the near future,” she said. “The complex nature of why social media may have been used more heavily for connection during a time when in-person meetings were not possible may be a heavy confounder as the typical profile of heavy social media users may have differed during the COVID shutdowns.”
Psychiatrist: Balance benefits of social media with mental health risks
The current study was likely conducted before the recent news on “hidden” Facebook data and the implications that Facebook knew it was contributing to worsened mental health in teens, particularly around self-esteem, Jessica “Jessi” Gold, MD, a psychiatrist at Washington University, St. Louis, said in an interview.
“If you look more specifically at other studies, however, the data around social media and mental health is constantly varied, with some showing benefits and some showing negatives, and none conclusively suggesting either way,” said Dr. Gold, who also was not involved with the new research. “More data are needed, especially longitudinally and on a broader age group, to understand social media’s impact on mental health over time.
“It is also even more important in the wake of COVID-19, as so many people have turned to social media as a primary source of social support and connection, and are using it even more than before,” she emphasized.
In the current study, “I think the most interesting information is that, for TikTok and Snapchat, the effects seemed to be more pronounced in those older than 35 years who used social media,” said Dr. Gold.
What this study leaves unanswered is “whether people who might develop depression are simply more prone to use social media in the first place, such as to seek out social support,” Dr. Gold said. “Also, we don’t know anything about how long they are using social media or what they are using it for, which to me is important for understanding more about the nuance of the relationship with mental health and social media.”
Experts advise clinicians to discuss social media with patients
This new research suggests that clinicians should be talking to their patients about how social media impacts their emotional reactions, as well as their sleep, Dr. Gold said.
“Patients should be asking themselves how they are feeling when they are on social media and not using it before sleep. They should also be considering time limits and how to effectively use social media while taking care of their mental health,” she said. This conversation between clinician and patient should be had with any patient of any age, who uses social media, not only with teenagers.
“This is also a conversation about moderation, and knowing that individuals may feel they benefit from social media, that they should balance these benefits with potential mental health risks,” she said.
“Studies such as this one shed light onto why social media consumption should be at least a point of discussion with our patients,” said Dr. Dakkak.
She advised clinicians to ask and listen to patients and their families when it comes to screen time habits. “Whenever I see a patient with mood symptoms, I ask about their habits – eating, sleeping, socializing, screen time – including phone time. I ask about the family dynamics around screen time.
“I’ve added screen time to my adolescent assessment. Discussing safe use of cell phones and social media can have a significant impact on adolescent behavior and wellbeing, and parents are very thankful for the help,” she said. “This study encourages us to add screen time to the assessments we do at all adult ages, especially if mood symptoms exist,” Dr. Dakkak emphasized.
Suggestions for future research
Dr. Dakkak added that more areas for research include the differences in the impact of social media use on content creators versus content consumers. Also, “I would like to see research using the real data of use, the times of use, interruptions in sleep and use, possible confounding variables to include exercise, presence of intimate relationship and school/job performance.”
Given the many confounding variables, more controlled studies are needed to examine mental health outcomes in use, how long people use social media, and the impact of interventions such as time limits, Dr. Gold said.
“We can’t ignore the benefits of social media, such as helping those with social anxiety, finding peer support, and normalizing mental health, and those factors need to be studied and measured more effectively as well, she said.
Take-home message
It is important to recognize that the current study represents a correlation, not causality, said Dr. Gold. In addressing the issues of how social media impact mental health, “as always, the hardest thing is that many people get their news from social media, and often get social support from social media, so there has to be a balance of not removing social media completely, but of helping people see how it affects their mental health and how to find balance.”
The study findings were limited by several factors, including the inability to control for all potential confounders, the inability to assess the nature of social media use, and the lack of dose-response data, the researchers noted. Although the surveys in the current study were not specific to COVID-19, the effects of social media on depression may be specific to the content, and the findings may not generalize beyond the COVID-19 pandemic period.
Approximately two-thirds (66%) of the study participants identified as female, and 76% as White; 11% as Black; 6% as Asian; 5% as Hispanic; and 2% as American Indian or Alaska Native, Pacific Islander or Native Hawaiian, or other.
The National Institute of Mental Health provided a grant for the study to Dr. Pelis, who disclosed consulting fees from various companies and equity in Psy Therapeutics. The study’s lead author also serves as associate editor for JAMA Network Open, but was not involved in the decision process for publication of this study. Dr. Gold disclosed conducting a conference for Johnson & Johnson about social media and health care workers, and was on the advisory council.
Use of social media has been linked to increased anxiety and depression, as well as reduced well-being in adolescents and young adults, but similar associations in older adults have not been well studied, and longitudinal data are lacking, Ron H. Perlis, MD, of Massachusetts General Hospital, Boston, and colleagues wrote in their paper, which was published in JAMA Network Open.
To examine the association between social media use and depressive symptoms in older adults, the researchers reviewed data from 13 waves of an internet survey conducted each month between May 2020 and May 2021. The survey respondents included individuals aged 18 years and older, with a mean age of 56 years.
In the study the researchers analyzed responses from 5,395 individuals aged 18 years and older, with a mean age of 56 years. The study participants had minimal or no depressive symptoms at baseline, according to scores on the nine-item Patient Health Questionnaire (PHQ-9).
Overall, 8.9% of the respondents reported a worsening of 5 points or more on the PHQ-9 score on a follow-up survey, which was the primary outcome. Participants who reported using social media platforms Snapchat, Facebook, or TikTok were significantly more likely to report increased depressive symptoms, compared with those who did not report use of social media. The fully adjusted odds ratio was largest for Snapchat (aOR, 1.53), followed by Facebook (aOR, 1.42), and TikTok (aOR, 1.39).
Incorporating recent television and internet news terms, such as COVID-19, changed the association for Snapchat, for which the aOR decreased from 1.53 to 1.12 when news source terms were included in the survey. TikTok and Facebook associations remained similar.
When the results were further stratified by age, use of TikTok and Snapchat was associated with depressive symptoms in those aged 35 years and older, but not in those younger than 35 years. However, the opposite pattern emerged for Facebook; use was associated with depressive symptoms for individuals younger than 35 years, but not in those aged 35 years and older (aOR, 2.60 vs. aOR, 1.12).
The association between increased self-reported depressive symptoms and use of certain social media platforms was not impacted by baseline social support or face-to-face interactions, the researchers noted.
Family physician was surprised results weren’t more significant
In the current study, “I was honestly surprised the results weren’t more significant,” Mary Ann Dakkak, MD, of Boston University said in an interview. “That said, social media uses during the COVID pandemic may have been a necessary social outlet and form of connection for many people who were otherwise isolated.”
To still see a significant increase in depression when social media could have been a positive force may suggest a heavier impact during “normal” times, she added.
“It is not surprising that what we see in youth is shown among adults,” noted Dr. Dakkak, who was not involved with this study. “I always tell my patients that what is good for their children is good for the adults too, and vice versa.
“We expect to see outcomes of this on youth and adults who have been more isolated, who have used more screen time for learning, work, connection and boredom, in the near future,” she said. “The complex nature of why social media may have been used more heavily for connection during a time when in-person meetings were not possible may be a heavy confounder as the typical profile of heavy social media users may have differed during the COVID shutdowns.”
Psychiatrist: Balance benefits of social media with mental health risks
The current study was likely conducted before the recent news on “hidden” Facebook data and the implications that Facebook knew it was contributing to worsened mental health in teens, particularly around self-esteem, Jessica “Jessi” Gold, MD, a psychiatrist at Washington University, St. Louis, said in an interview.
“If you look more specifically at other studies, however, the data around social media and mental health is constantly varied, with some showing benefits and some showing negatives, and none conclusively suggesting either way,” said Dr. Gold, who also was not involved with the new research. “More data are needed, especially longitudinally and on a broader age group, to understand social media’s impact on mental health over time.
“It is also even more important in the wake of COVID-19, as so many people have turned to social media as a primary source of social support and connection, and are using it even more than before,” she emphasized.
In the current study, “I think the most interesting information is that, for TikTok and Snapchat, the effects seemed to be more pronounced in those older than 35 years who used social media,” said Dr. Gold.
What this study leaves unanswered is “whether people who might develop depression are simply more prone to use social media in the first place, such as to seek out social support,” Dr. Gold said. “Also, we don’t know anything about how long they are using social media or what they are using it for, which to me is important for understanding more about the nuance of the relationship with mental health and social media.”
Experts advise clinicians to discuss social media with patients
This new research suggests that clinicians should be talking to their patients about how social media impacts their emotional reactions, as well as their sleep, Dr. Gold said.
“Patients should be asking themselves how they are feeling when they are on social media and not using it before sleep. They should also be considering time limits and how to effectively use social media while taking care of their mental health,” she said. This conversation between clinician and patient should be had with any patient of any age, who uses social media, not only with teenagers.
“This is also a conversation about moderation, and knowing that individuals may feel they benefit from social media, that they should balance these benefits with potential mental health risks,” she said.
“Studies such as this one shed light onto why social media consumption should be at least a point of discussion with our patients,” said Dr. Dakkak.
She advised clinicians to ask and listen to patients and their families when it comes to screen time habits. “Whenever I see a patient with mood symptoms, I ask about their habits – eating, sleeping, socializing, screen time – including phone time. I ask about the family dynamics around screen time.
“I’ve added screen time to my adolescent assessment. Discussing safe use of cell phones and social media can have a significant impact on adolescent behavior and wellbeing, and parents are very thankful for the help,” she said. “This study encourages us to add screen time to the assessments we do at all adult ages, especially if mood symptoms exist,” Dr. Dakkak emphasized.
Suggestions for future research
Dr. Dakkak added that more areas for research include the differences in the impact of social media use on content creators versus content consumers. Also, “I would like to see research using the real data of use, the times of use, interruptions in sleep and use, possible confounding variables to include exercise, presence of intimate relationship and school/job performance.”
Given the many confounding variables, more controlled studies are needed to examine mental health outcomes in use, how long people use social media, and the impact of interventions such as time limits, Dr. Gold said.
“We can’t ignore the benefits of social media, such as helping those with social anxiety, finding peer support, and normalizing mental health, and those factors need to be studied and measured more effectively as well, she said.
Take-home message
It is important to recognize that the current study represents a correlation, not causality, said Dr. Gold. In addressing the issues of how social media impact mental health, “as always, the hardest thing is that many people get their news from social media, and often get social support from social media, so there has to be a balance of not removing social media completely, but of helping people see how it affects their mental health and how to find balance.”
The study findings were limited by several factors, including the inability to control for all potential confounders, the inability to assess the nature of social media use, and the lack of dose-response data, the researchers noted. Although the surveys in the current study were not specific to COVID-19, the effects of social media on depression may be specific to the content, and the findings may not generalize beyond the COVID-19 pandemic period.
Approximately two-thirds (66%) of the study participants identified as female, and 76% as White; 11% as Black; 6% as Asian; 5% as Hispanic; and 2% as American Indian or Alaska Native, Pacific Islander or Native Hawaiian, or other.
The National Institute of Mental Health provided a grant for the study to Dr. Pelis, who disclosed consulting fees from various companies and equity in Psy Therapeutics. The study’s lead author also serves as associate editor for JAMA Network Open, but was not involved in the decision process for publication of this study. Dr. Gold disclosed conducting a conference for Johnson & Johnson about social media and health care workers, and was on the advisory council.
FROM JAMA NETWORK OPEN
Schools, pediatricians look to make up lost ground on non–COVID-19 vaccinations
WESTMINSTER, COLO. – Melissa Blatzer was determined to get her three children caught up on their routine immunizations on a recent Saturday morning at a walk-in clinic in this Denver suburb. It had been about a year since the kids’ last shots, a delay Ms. Blatzer chalked up to the pandemic.
Two-year-old Lincoln Blatzer, in his fleece dinosaur pajamas, waited anxiously in line for his hepatitis A vaccine. His siblings, 14-year-old Nyla Kusumah and 11-year-old Nevan Kusumah, were there for their TDAP, HPV and meningococcal vaccines, plus a COVID-19 shot for Nyla.
“You don’t have to make an appointment and you can take all three at once,” said Ms. Blatzer, who lives several miles away in Commerce City. That convenience outweighed the difficulty of getting everyone up early on a weekend.
Child health experts hope community clinics like this – along with the return to in-person classes, more well-child visits, and the rollout of COVID shots for younger children – can help boost routine childhood immunizations, which dropped during the pandemic. Despite a rebound, immunization rates are still lower than in 2019, and disparities in rates between racial and economic groups, particularly for Black children, have been exacerbated.
“We’re still not back to where we need to be,” said Sean O’Leary, MD, a pediatric infectious disease doctor at Children’s Hospital Colorado and a professor of pediatrics at the University of Colorado at Denver, Aurora.
Routine immunizations protect children against 16 infectious diseases, including measles, diphtheria and chickenpox, and inhibit transmission to the community.
The rollout of COVID shots for younger kids is an opportunity to catch up on routine vaccinations, said Dr. O’Leary, adding that children can receive these vaccines together. Primary care practices, where many children are likely to receive the COVID shots, usually have other childhood vaccines on hand.
“It’s really important that parents and health care providers work together so that all children are up to date on these recommended vaccines,” said Malini DeSilva, MD, an internist and pediatrician at HealthPartners in the Minneapolis–St. Paul area. “Not only for the child’s health but for our community’s health.”
People were reluctant to come out for routine immunizations at the height of the pandemic, said Karen Miller, an immunization nurse manager for the Denver area’s Tri-County Health Department, which ran the Westminster clinic. National and global data confirm what Ms. Miller saw on the ground.
Global vaccine coverage in children fell from 2019 to 2020, according to a recent study by scientists at the Centers for Disease Control and Prevention, the World Health Organization, and UNICEF. Reasons included reduced access, lack of transportation, worries about COVID exposure and supply chain interruptions, the study said.
Third doses of the DTP vaccine and of the polio vaccine decreased from 86% of all eligible children in 2019 to 83% in 2020, according to the study. Worldwide, 22.7 million children had not had their third dose of DTP in 2020, compared with 19 million in 2019. Three doses are far more effective than one or two at protecting children and communities.
In the United States, researchers who studied 2019 and 2020 data on routine vaccinations in California, Colorado, Minnesota, Oregon, Washington, and Wisconsin found substantial disruptions in vaccination rates during the pandemic that continued into September 2020. For example, the percentage of 7-month-old babies who were up to date on vaccinations decreased from 81% in September 2019 to 74% a year later.
The proportion of Black children up to date on immunizations in almost all age groups was lower than that of children in other racial and ethnic groups. This was most pronounced in those turning 18 months old: Only 41% of Black children that age were caught up on vaccinations in September 2020, compared with 57% of all children at 18 months, said Dr. DeSilva, who led that study.
A CDC study of data from the National Immunization Surveys found that race and ethnicity, poverty, and lack of insurance created the greatest disparities in vaccination rates, and the authors noted that extra efforts are needed to counter the pandemic’s disruptions.
In addition to the problems caused by COVID, Ms. Miller said, competing life priorities like work and school impede families from keeping up with shots. Weekend vaccination clinics can help working parents get their children caught up on routine immunizations while they get a flu or COVID shot. Ms. Miller and O’Leary also said reminders via phone, text or email can boost immunizations.
“Vaccines are so effective that I think it’s easy for families to put immunizations on the back burner because we don’t often hear about these diseases,” she said.
It’s a long and nasty list that includes hepatitis A and B, measles, mumps, whooping cough, polio, rubella, rotavirus, pneumococcus, tetanus, diphtheria, human papillomavirus, and meningococcal disease, among others. Even small drops in vaccination coverage can lead to outbreaks. And measles is the perfect example that worries experts, particularly as international travel opens up.
“Measles is among the most contagious diseases known to humankind, meaning that we have to keep very high vaccination coverage to keep it from spreading,” said Dr. O’Leary.
In 2019, 22 measles outbreaks occurred in 17 states in mostly unvaccinated children and adults. Dr. O’Leary said outbreaks in New York City were contained because surrounding areas had high vaccination coverage. But an outbreak in an undervaccinated community still could spread beyond its borders.
In some states a significant number of parents were opposed to routine childhood vaccines even before the pandemic for religious or personal reasons, posing another challenge for health professionals. For example, 87% of Colorado kindergartners were vaccinated against measles, mumps, and rubella during the 2018-19 school year, one of the nation’s lowest rates.
Those rates bumped up to 91% in 2019-20 but are still below the CDC’s target of 95%.
Dr. O’Leary said he does not see the same level of hesitancy for routine immunizations as for COVID. “There has always been vaccine hesitancy and vaccine refusers. But we’ve maintained vaccination rates north of 90% for all routine childhood vaccines for a long time now,” he said.
Dr. DeSilva said the “ripple effects” of missed vaccinations earlier in the pandemic continued into 2021. As children returned to in-person learning this fall, schools may have been the first place families heard about missed vaccinations. Individual states set vaccination requirements, and allowable exemptions, for entry at schools and child care facilities. In 2020, Colorado passed a school entry immunization law that tightened allowable exemptions.
“Schools, where vaccination requirements are generally enforced, are stretched thin for a variety of reasons, including COVID,” said Dr. O’Leary, adding that managing vaccine requirements may be more difficult for some, but not all, schools.
Anayeli Dominguez, 13, was at the Westminster clinic for a Tdap vaccine because her middle school had noticed she was not up to date.
“School nurses play an important role in helping identify students in need of immunizations, and also by connecting families to resources both within the district and in the larger community,” said Denver Public Schools spokesperson Will Jones.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
WESTMINSTER, COLO. – Melissa Blatzer was determined to get her three children caught up on their routine immunizations on a recent Saturday morning at a walk-in clinic in this Denver suburb. It had been about a year since the kids’ last shots, a delay Ms. Blatzer chalked up to the pandemic.
Two-year-old Lincoln Blatzer, in his fleece dinosaur pajamas, waited anxiously in line for his hepatitis A vaccine. His siblings, 14-year-old Nyla Kusumah and 11-year-old Nevan Kusumah, were there for their TDAP, HPV and meningococcal vaccines, plus a COVID-19 shot for Nyla.
“You don’t have to make an appointment and you can take all three at once,” said Ms. Blatzer, who lives several miles away in Commerce City. That convenience outweighed the difficulty of getting everyone up early on a weekend.
Child health experts hope community clinics like this – along with the return to in-person classes, more well-child visits, and the rollout of COVID shots for younger children – can help boost routine childhood immunizations, which dropped during the pandemic. Despite a rebound, immunization rates are still lower than in 2019, and disparities in rates between racial and economic groups, particularly for Black children, have been exacerbated.
“We’re still not back to where we need to be,” said Sean O’Leary, MD, a pediatric infectious disease doctor at Children’s Hospital Colorado and a professor of pediatrics at the University of Colorado at Denver, Aurora.
Routine immunizations protect children against 16 infectious diseases, including measles, diphtheria and chickenpox, and inhibit transmission to the community.
The rollout of COVID shots for younger kids is an opportunity to catch up on routine vaccinations, said Dr. O’Leary, adding that children can receive these vaccines together. Primary care practices, where many children are likely to receive the COVID shots, usually have other childhood vaccines on hand.
“It’s really important that parents and health care providers work together so that all children are up to date on these recommended vaccines,” said Malini DeSilva, MD, an internist and pediatrician at HealthPartners in the Minneapolis–St. Paul area. “Not only for the child’s health but for our community’s health.”
People were reluctant to come out for routine immunizations at the height of the pandemic, said Karen Miller, an immunization nurse manager for the Denver area’s Tri-County Health Department, which ran the Westminster clinic. National and global data confirm what Ms. Miller saw on the ground.
Global vaccine coverage in children fell from 2019 to 2020, according to a recent study by scientists at the Centers for Disease Control and Prevention, the World Health Organization, and UNICEF. Reasons included reduced access, lack of transportation, worries about COVID exposure and supply chain interruptions, the study said.
Third doses of the DTP vaccine and of the polio vaccine decreased from 86% of all eligible children in 2019 to 83% in 2020, according to the study. Worldwide, 22.7 million children had not had their third dose of DTP in 2020, compared with 19 million in 2019. Three doses are far more effective than one or two at protecting children and communities.
In the United States, researchers who studied 2019 and 2020 data on routine vaccinations in California, Colorado, Minnesota, Oregon, Washington, and Wisconsin found substantial disruptions in vaccination rates during the pandemic that continued into September 2020. For example, the percentage of 7-month-old babies who were up to date on vaccinations decreased from 81% in September 2019 to 74% a year later.
The proportion of Black children up to date on immunizations in almost all age groups was lower than that of children in other racial and ethnic groups. This was most pronounced in those turning 18 months old: Only 41% of Black children that age were caught up on vaccinations in September 2020, compared with 57% of all children at 18 months, said Dr. DeSilva, who led that study.
A CDC study of data from the National Immunization Surveys found that race and ethnicity, poverty, and lack of insurance created the greatest disparities in vaccination rates, and the authors noted that extra efforts are needed to counter the pandemic’s disruptions.
In addition to the problems caused by COVID, Ms. Miller said, competing life priorities like work and school impede families from keeping up with shots. Weekend vaccination clinics can help working parents get their children caught up on routine immunizations while they get a flu or COVID shot. Ms. Miller and O’Leary also said reminders via phone, text or email can boost immunizations.
“Vaccines are so effective that I think it’s easy for families to put immunizations on the back burner because we don’t often hear about these diseases,” she said.
It’s a long and nasty list that includes hepatitis A and B, measles, mumps, whooping cough, polio, rubella, rotavirus, pneumococcus, tetanus, diphtheria, human papillomavirus, and meningococcal disease, among others. Even small drops in vaccination coverage can lead to outbreaks. And measles is the perfect example that worries experts, particularly as international travel opens up.
“Measles is among the most contagious diseases known to humankind, meaning that we have to keep very high vaccination coverage to keep it from spreading,” said Dr. O’Leary.
In 2019, 22 measles outbreaks occurred in 17 states in mostly unvaccinated children and adults. Dr. O’Leary said outbreaks in New York City were contained because surrounding areas had high vaccination coverage. But an outbreak in an undervaccinated community still could spread beyond its borders.
In some states a significant number of parents were opposed to routine childhood vaccines even before the pandemic for religious or personal reasons, posing another challenge for health professionals. For example, 87% of Colorado kindergartners were vaccinated against measles, mumps, and rubella during the 2018-19 school year, one of the nation’s lowest rates.
Those rates bumped up to 91% in 2019-20 but are still below the CDC’s target of 95%.
Dr. O’Leary said he does not see the same level of hesitancy for routine immunizations as for COVID. “There has always been vaccine hesitancy and vaccine refusers. But we’ve maintained vaccination rates north of 90% for all routine childhood vaccines for a long time now,” he said.
Dr. DeSilva said the “ripple effects” of missed vaccinations earlier in the pandemic continued into 2021. As children returned to in-person learning this fall, schools may have been the first place families heard about missed vaccinations. Individual states set vaccination requirements, and allowable exemptions, for entry at schools and child care facilities. In 2020, Colorado passed a school entry immunization law that tightened allowable exemptions.
“Schools, where vaccination requirements are generally enforced, are stretched thin for a variety of reasons, including COVID,” said Dr. O’Leary, adding that managing vaccine requirements may be more difficult for some, but not all, schools.
Anayeli Dominguez, 13, was at the Westminster clinic for a Tdap vaccine because her middle school had noticed she was not up to date.
“School nurses play an important role in helping identify students in need of immunizations, and also by connecting families to resources both within the district and in the larger community,” said Denver Public Schools spokesperson Will Jones.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
WESTMINSTER, COLO. – Melissa Blatzer was determined to get her three children caught up on their routine immunizations on a recent Saturday morning at a walk-in clinic in this Denver suburb. It had been about a year since the kids’ last shots, a delay Ms. Blatzer chalked up to the pandemic.
Two-year-old Lincoln Blatzer, in his fleece dinosaur pajamas, waited anxiously in line for his hepatitis A vaccine. His siblings, 14-year-old Nyla Kusumah and 11-year-old Nevan Kusumah, were there for their TDAP, HPV and meningococcal vaccines, plus a COVID-19 shot for Nyla.
“You don’t have to make an appointment and you can take all three at once,” said Ms. Blatzer, who lives several miles away in Commerce City. That convenience outweighed the difficulty of getting everyone up early on a weekend.
Child health experts hope community clinics like this – along with the return to in-person classes, more well-child visits, and the rollout of COVID shots for younger children – can help boost routine childhood immunizations, which dropped during the pandemic. Despite a rebound, immunization rates are still lower than in 2019, and disparities in rates between racial and economic groups, particularly for Black children, have been exacerbated.
“We’re still not back to where we need to be,” said Sean O’Leary, MD, a pediatric infectious disease doctor at Children’s Hospital Colorado and a professor of pediatrics at the University of Colorado at Denver, Aurora.
Routine immunizations protect children against 16 infectious diseases, including measles, diphtheria and chickenpox, and inhibit transmission to the community.
The rollout of COVID shots for younger kids is an opportunity to catch up on routine vaccinations, said Dr. O’Leary, adding that children can receive these vaccines together. Primary care practices, where many children are likely to receive the COVID shots, usually have other childhood vaccines on hand.
“It’s really important that parents and health care providers work together so that all children are up to date on these recommended vaccines,” said Malini DeSilva, MD, an internist and pediatrician at HealthPartners in the Minneapolis–St. Paul area. “Not only for the child’s health but for our community’s health.”
People were reluctant to come out for routine immunizations at the height of the pandemic, said Karen Miller, an immunization nurse manager for the Denver area’s Tri-County Health Department, which ran the Westminster clinic. National and global data confirm what Ms. Miller saw on the ground.
Global vaccine coverage in children fell from 2019 to 2020, according to a recent study by scientists at the Centers for Disease Control and Prevention, the World Health Organization, and UNICEF. Reasons included reduced access, lack of transportation, worries about COVID exposure and supply chain interruptions, the study said.
Third doses of the DTP vaccine and of the polio vaccine decreased from 86% of all eligible children in 2019 to 83% in 2020, according to the study. Worldwide, 22.7 million children had not had their third dose of DTP in 2020, compared with 19 million in 2019. Three doses are far more effective than one or two at protecting children and communities.
In the United States, researchers who studied 2019 and 2020 data on routine vaccinations in California, Colorado, Minnesota, Oregon, Washington, and Wisconsin found substantial disruptions in vaccination rates during the pandemic that continued into September 2020. For example, the percentage of 7-month-old babies who were up to date on vaccinations decreased from 81% in September 2019 to 74% a year later.
The proportion of Black children up to date on immunizations in almost all age groups was lower than that of children in other racial and ethnic groups. This was most pronounced in those turning 18 months old: Only 41% of Black children that age were caught up on vaccinations in September 2020, compared with 57% of all children at 18 months, said Dr. DeSilva, who led that study.
A CDC study of data from the National Immunization Surveys found that race and ethnicity, poverty, and lack of insurance created the greatest disparities in vaccination rates, and the authors noted that extra efforts are needed to counter the pandemic’s disruptions.
In addition to the problems caused by COVID, Ms. Miller said, competing life priorities like work and school impede families from keeping up with shots. Weekend vaccination clinics can help working parents get their children caught up on routine immunizations while they get a flu or COVID shot. Ms. Miller and O’Leary also said reminders via phone, text or email can boost immunizations.
“Vaccines are so effective that I think it’s easy for families to put immunizations on the back burner because we don’t often hear about these diseases,” she said.
It’s a long and nasty list that includes hepatitis A and B, measles, mumps, whooping cough, polio, rubella, rotavirus, pneumococcus, tetanus, diphtheria, human papillomavirus, and meningococcal disease, among others. Even small drops in vaccination coverage can lead to outbreaks. And measles is the perfect example that worries experts, particularly as international travel opens up.
“Measles is among the most contagious diseases known to humankind, meaning that we have to keep very high vaccination coverage to keep it from spreading,” said Dr. O’Leary.
In 2019, 22 measles outbreaks occurred in 17 states in mostly unvaccinated children and adults. Dr. O’Leary said outbreaks in New York City were contained because surrounding areas had high vaccination coverage. But an outbreak in an undervaccinated community still could spread beyond its borders.
In some states a significant number of parents were opposed to routine childhood vaccines even before the pandemic for religious or personal reasons, posing another challenge for health professionals. For example, 87% of Colorado kindergartners were vaccinated against measles, mumps, and rubella during the 2018-19 school year, one of the nation’s lowest rates.
Those rates bumped up to 91% in 2019-20 but are still below the CDC’s target of 95%.
Dr. O’Leary said he does not see the same level of hesitancy for routine immunizations as for COVID. “There has always been vaccine hesitancy and vaccine refusers. But we’ve maintained vaccination rates north of 90% for all routine childhood vaccines for a long time now,” he said.
Dr. DeSilva said the “ripple effects” of missed vaccinations earlier in the pandemic continued into 2021. As children returned to in-person learning this fall, schools may have been the first place families heard about missed vaccinations. Individual states set vaccination requirements, and allowable exemptions, for entry at schools and child care facilities. In 2020, Colorado passed a school entry immunization law that tightened allowable exemptions.
“Schools, where vaccination requirements are generally enforced, are stretched thin for a variety of reasons, including COVID,” said Dr. O’Leary, adding that managing vaccine requirements may be more difficult for some, but not all, schools.
Anayeli Dominguez, 13, was at the Westminster clinic for a Tdap vaccine because her middle school had noticed she was not up to date.
“School nurses play an important role in helping identify students in need of immunizations, and also by connecting families to resources both within the district and in the larger community,” said Denver Public Schools spokesperson Will Jones.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Beware of private equity–owned nursing homes: study
When you have to help a parent choose a nursing home or you need nursing home care yourself, you can consult a health care professional, talk to friends, or look at the Nursing Home Compare website of the Centers for Medicare and Medicaid Services (CMS). The CMS website includes star ratings for each nursing home, both overall and on health inspections, staffing and certain quality measures.
But what you might not know is what financial incentives a particular nursing home might have to provide high-quality care, depending on what kind of entity owns the facility.
According to the study, you can expect a somewhat lower level of quality in a PE-owned nursing home than in other for-profit facilities.
The researchers compared CMS data on 302 nursing homes owned by 79 PE firms to data on 9,562 for-profit facilities not owned by such companies from 2013 to 2017. Among fee-for-service Medicare patients in long-term care, private equity acquisitions of nursing homes were associated with an 11.1% increase in ambulatory-care-sensitive (ACS) visits to the emergency department (ED) and an 8.7% increase in ACS hospitalizations per quarter, compared to the changes that occurred in the non-PE-owned facilities, they found.
What’s more, Medicare costs per beneficiary increased 3.9% more – or about $1,000 a year – in the PE-owned nursing homes than they did in the other cohort during the study period.
And when the acquired nursing homes were compared to the nursing homes prior to their acquisition by PE firms, there were no statistically significant differences in unadjusted outcomes, the researchers found. That means the two cohorts were broadly comparable.
The researchers adjusted the numbers in their study for various characteristics of the facilities and their residents. For example, the PE-acquired nursing homes were likely to have a higher percentage of patients covered by Medicare and a lower percentage covered by Medicaid than their non-PE counterparts.
The mean percentages of Black residents, female residents, and residents aged 85 or older were 12.4%, 65.4%, and 36.2%, respectively, for the PE-owned nursing homes and 15.7%, 67.8%, and 39%, respectively, for the non–PE-owned facilities.
Less than optimal outcomes
On average, the residents of non–PE-owned nursing homes had better outcomes than did the patients in the PE-owned facilities. But that doesn’t mean that the average for-profit nursing home had terrific outcomes.
For all the nursing homes in the study, the mean quarterly rate of ACS emergency department visits was 14.1%, and the mean quarterly rate of ACS hospitalizations was 17.3%.
“These events should be largely, although not completely, preventable with appropriate care,” the researchers pointed out.
To date, PE firms have invested about $750 billion in U.S. health care, with nursing homes being a major target of these companies, which currently own 5% of skilled nursing facilities, per the study. PE companies seek annual returns of 20% or more, the paper says, and thus feel pressure to generate high short-term profits. That could lead to reduced staffing, services, supplies, or equipment in their facilities.
Some nursing homes purchased by PE firms may be responsible for the debt incurred in their own leveraged buyouts, the researchers noted. There is also concern that PE firms may focus their properties disproportionately on short-term post-acute care, which is reimbursed at a higher rate than long-term care, the study says.
For all these reasons, some health policy makers are concerned about the long-term impact of private-equity nursing home acquisitions, according to the study.
A version of this article first appeared on WebMD.com.
When you have to help a parent choose a nursing home or you need nursing home care yourself, you can consult a health care professional, talk to friends, or look at the Nursing Home Compare website of the Centers for Medicare and Medicaid Services (CMS). The CMS website includes star ratings for each nursing home, both overall and on health inspections, staffing and certain quality measures.
But what you might not know is what financial incentives a particular nursing home might have to provide high-quality care, depending on what kind of entity owns the facility.
According to the study, you can expect a somewhat lower level of quality in a PE-owned nursing home than in other for-profit facilities.
The researchers compared CMS data on 302 nursing homes owned by 79 PE firms to data on 9,562 for-profit facilities not owned by such companies from 2013 to 2017. Among fee-for-service Medicare patients in long-term care, private equity acquisitions of nursing homes were associated with an 11.1% increase in ambulatory-care-sensitive (ACS) visits to the emergency department (ED) and an 8.7% increase in ACS hospitalizations per quarter, compared to the changes that occurred in the non-PE-owned facilities, they found.
What’s more, Medicare costs per beneficiary increased 3.9% more – or about $1,000 a year – in the PE-owned nursing homes than they did in the other cohort during the study period.
And when the acquired nursing homes were compared to the nursing homes prior to their acquisition by PE firms, there were no statistically significant differences in unadjusted outcomes, the researchers found. That means the two cohorts were broadly comparable.
The researchers adjusted the numbers in their study for various characteristics of the facilities and their residents. For example, the PE-acquired nursing homes were likely to have a higher percentage of patients covered by Medicare and a lower percentage covered by Medicaid than their non-PE counterparts.
The mean percentages of Black residents, female residents, and residents aged 85 or older were 12.4%, 65.4%, and 36.2%, respectively, for the PE-owned nursing homes and 15.7%, 67.8%, and 39%, respectively, for the non–PE-owned facilities.
Less than optimal outcomes
On average, the residents of non–PE-owned nursing homes had better outcomes than did the patients in the PE-owned facilities. But that doesn’t mean that the average for-profit nursing home had terrific outcomes.
For all the nursing homes in the study, the mean quarterly rate of ACS emergency department visits was 14.1%, and the mean quarterly rate of ACS hospitalizations was 17.3%.
“These events should be largely, although not completely, preventable with appropriate care,” the researchers pointed out.
To date, PE firms have invested about $750 billion in U.S. health care, with nursing homes being a major target of these companies, which currently own 5% of skilled nursing facilities, per the study. PE companies seek annual returns of 20% or more, the paper says, and thus feel pressure to generate high short-term profits. That could lead to reduced staffing, services, supplies, or equipment in their facilities.
Some nursing homes purchased by PE firms may be responsible for the debt incurred in their own leveraged buyouts, the researchers noted. There is also concern that PE firms may focus their properties disproportionately on short-term post-acute care, which is reimbursed at a higher rate than long-term care, the study says.
For all these reasons, some health policy makers are concerned about the long-term impact of private-equity nursing home acquisitions, according to the study.
A version of this article first appeared on WebMD.com.
When you have to help a parent choose a nursing home or you need nursing home care yourself, you can consult a health care professional, talk to friends, or look at the Nursing Home Compare website of the Centers for Medicare and Medicaid Services (CMS). The CMS website includes star ratings for each nursing home, both overall and on health inspections, staffing and certain quality measures.
But what you might not know is what financial incentives a particular nursing home might have to provide high-quality care, depending on what kind of entity owns the facility.
According to the study, you can expect a somewhat lower level of quality in a PE-owned nursing home than in other for-profit facilities.
The researchers compared CMS data on 302 nursing homes owned by 79 PE firms to data on 9,562 for-profit facilities not owned by such companies from 2013 to 2017. Among fee-for-service Medicare patients in long-term care, private equity acquisitions of nursing homes were associated with an 11.1% increase in ambulatory-care-sensitive (ACS) visits to the emergency department (ED) and an 8.7% increase in ACS hospitalizations per quarter, compared to the changes that occurred in the non-PE-owned facilities, they found.
What’s more, Medicare costs per beneficiary increased 3.9% more – or about $1,000 a year – in the PE-owned nursing homes than they did in the other cohort during the study period.
And when the acquired nursing homes were compared to the nursing homes prior to their acquisition by PE firms, there were no statistically significant differences in unadjusted outcomes, the researchers found. That means the two cohorts were broadly comparable.
The researchers adjusted the numbers in their study for various characteristics of the facilities and their residents. For example, the PE-acquired nursing homes were likely to have a higher percentage of patients covered by Medicare and a lower percentage covered by Medicaid than their non-PE counterparts.
The mean percentages of Black residents, female residents, and residents aged 85 or older were 12.4%, 65.4%, and 36.2%, respectively, for the PE-owned nursing homes and 15.7%, 67.8%, and 39%, respectively, for the non–PE-owned facilities.
Less than optimal outcomes
On average, the residents of non–PE-owned nursing homes had better outcomes than did the patients in the PE-owned facilities. But that doesn’t mean that the average for-profit nursing home had terrific outcomes.
For all the nursing homes in the study, the mean quarterly rate of ACS emergency department visits was 14.1%, and the mean quarterly rate of ACS hospitalizations was 17.3%.
“These events should be largely, although not completely, preventable with appropriate care,” the researchers pointed out.
To date, PE firms have invested about $750 billion in U.S. health care, with nursing homes being a major target of these companies, which currently own 5% of skilled nursing facilities, per the study. PE companies seek annual returns of 20% or more, the paper says, and thus feel pressure to generate high short-term profits. That could lead to reduced staffing, services, supplies, or equipment in their facilities.
Some nursing homes purchased by PE firms may be responsible for the debt incurred in their own leveraged buyouts, the researchers noted. There is also concern that PE firms may focus their properties disproportionately on short-term post-acute care, which is reimbursed at a higher rate than long-term care, the study says.
For all these reasons, some health policy makers are concerned about the long-term impact of private-equity nursing home acquisitions, according to the study.
A version of this article first appeared on WebMD.com.
Black young adults: Remember this when facing discrimination
Joel Bervell recalls leaving his hometown of Seattle for the East Coast after being accepted into Yale University.
Still getting accustomed to the big move, Mr. Bervell, who had breezed through high school with straight As, went to see his chemistry professor for advice after getting a low grade on a test.
“He took one look at me and said, ‘Oh, if you’re on the football team, you don’t need to worry about it. So many people from the football team come into the class and end up dropping out, so if you need to drop this class, you can,’ ” Mr. Bervell says.
Mr. Bervell, who is Black, was not on the football team, nor did he receive a sports scholarship of any kind.
“For that professor to make an assumption of me, which to me felt like it was based on my race, made me less likely to want to go into a science field, where I felt like I was being judged before I even had a chance to prove myself,” Mr. Bervell says.
.
Researchers studied health data on 1,834 Americans ages 18-28 over a 10-year span. Findings show that the more instances of discrimination they experienced – including ageism, sexism, and racism – the more likely they were to face mental and behavioral struggles, like mental illness, drug use, severe psychological distress, and poor overall health.
Mr. Bervell, now 26, says he feels lucky that growing up, he was taught healthy ways to process his feelings and emotions.
“Instead of taking that and internalizing it, I said, ‘how can I use this to prove him wrong?’” he says. “Does that mean I need to work harder or does that mean I need to find a different mentor? Surround myself with different people?”
Mr. Bervell is currently a 3rd-year medical student at Washington State University.
When he’s not at the hospital seeing patients, you can find him educating his nearly 340,000 TikTok followers on topics like racial bias in medicine.
Acknowledge the impact
Most Black people don’t tie psychological distress to acts of racism, according to Rheeda Walker, PhD, psychology professor at the University of Houston and author of “The Unapologetic Guide to Black Mental Health” (Oakland, Calif.: New Harbinger Publications, 2020).
Many Black people even normalize it.
“Individuals deal with it [racism] as just another thing, like paying bills, going to work, and studying for class and not as the overwhelming psychological burden that it is,” says Dr. Walker.
And despite what some may say, racial discrimination is not merely “a thing of the past,” Dr. Walker says.
“Instead, discrimination has shifted form from more overt forms of discrimination to less obvious microaggression,” she says.
It’s also critical that young adults are taught how to deal with racism to avoid the risk of “internalizing that they deserve to be mistreated, and/or that they have to work twice as hard to overcome racism,” says Dr. Walker.
“Both scenarios can escalate hopelessness and worry, psychological features of depression and anxiety, respectively,” Dr. Walker says.
Embrace your emotions
Known around the office as “a big teddy bear,” Frederick Herman, a mortgage loan originator based in Charlotte, Va., was coaching a newer employee on how to make sales calls, a common practice in his line of work.
He says a day or 2 days later, his manager let him know that he had made an employee “very uncomfortable” by intimidating them while they were on the phone. Mr. Herman, 29, was told to watch his “aggressive” behavior.
“I’m a bigger Black man. I’m like 6’2, 300 lbs., somewhat muscular. So, if me talking or trying to coach her came off as intimidating, then there’s nothing that I could do or say differently than I was already doing to make her not feel intimidated,” Mr. Herman says.
“If a big teddy bear is now intimidating to you, that just tells me everything I need to know.”
This wasn’t the first time Mr. Herman had been reprimanded for being “too aggressive” or “showing off” when trying to help colleagues at work.
“I’ve had other experiences at work where I may not share my ideas, or I may get super anxious,” says Mr. Herman, a Black man of Haitian descent.
It’s important to allow yourself to feel your emotions after facing acts of discrimination, says Ebony Butler, PhD, a licensed psychologist and creator of My Therapy Cards, a card deck tailored for men, women, and teens of color, with self-care and reflection prompts.
This is a practice called “self-validation” and can reduce the tendency to blame oneself for the mistreatment, says Dr. Butler.
Mr. Herman, 29, says that he recently signed up for therapy to work through his struggles with anxiety.
Relaxation techniques, like grounding and mindfulness, can also be helpful, says Dr. Butler.
“Some example ways to practice grounding are immersing oneself in nature, walking bare feet on the ground, lying on the floor, practicing slow, deep breathing, or engaging the senses,” she says.
“When we are grounded and present, we can better manage our responses and plan our action steps.”
Utilize unique
If you find yourself in a racially charged school or workplace setting, don’t be intimidated, says Wendy Osefo, PhD, education professor at Johns Hopkins University, Baltimore, political commentator, and television personality.
Dr. Osefo made history in 2016 as the first Black woman to earn a PhD in public affairs/community development from Rutgers University.
“Your attitude should be that, no matter how different you might be, you belong, and you earned the right to occupy this space. You’re not less qualified than others who surround you,” she says.
Dr. Ofeso is also CEO of The 1954 Equity Project, an organization that gives minority students tools to succeed in higher education – like mentorships, peer support groups, and other resources and services – all while remaining their authentic selves.
No matter how uncomfortable it might be, staying true to who you are vs. conforming to the masses pays off, says Dr. Osefo.
“Being different is unique and allows you to bring a new and fresh perspective into an environment,” she says.
“Leaning into this uniqueness builds a level of confidence that will aid in your ability to be successful.”
A version of this article first appeared on WebMD.com.
Joel Bervell recalls leaving his hometown of Seattle for the East Coast after being accepted into Yale University.
Still getting accustomed to the big move, Mr. Bervell, who had breezed through high school with straight As, went to see his chemistry professor for advice after getting a low grade on a test.
“He took one look at me and said, ‘Oh, if you’re on the football team, you don’t need to worry about it. So many people from the football team come into the class and end up dropping out, so if you need to drop this class, you can,’ ” Mr. Bervell says.
Mr. Bervell, who is Black, was not on the football team, nor did he receive a sports scholarship of any kind.
“For that professor to make an assumption of me, which to me felt like it was based on my race, made me less likely to want to go into a science field, where I felt like I was being judged before I even had a chance to prove myself,” Mr. Bervell says.
.
Researchers studied health data on 1,834 Americans ages 18-28 over a 10-year span. Findings show that the more instances of discrimination they experienced – including ageism, sexism, and racism – the more likely they were to face mental and behavioral struggles, like mental illness, drug use, severe psychological distress, and poor overall health.
Mr. Bervell, now 26, says he feels lucky that growing up, he was taught healthy ways to process his feelings and emotions.
“Instead of taking that and internalizing it, I said, ‘how can I use this to prove him wrong?’” he says. “Does that mean I need to work harder or does that mean I need to find a different mentor? Surround myself with different people?”
Mr. Bervell is currently a 3rd-year medical student at Washington State University.
When he’s not at the hospital seeing patients, you can find him educating his nearly 340,000 TikTok followers on topics like racial bias in medicine.
Acknowledge the impact
Most Black people don’t tie psychological distress to acts of racism, according to Rheeda Walker, PhD, psychology professor at the University of Houston and author of “The Unapologetic Guide to Black Mental Health” (Oakland, Calif.: New Harbinger Publications, 2020).
Many Black people even normalize it.
“Individuals deal with it [racism] as just another thing, like paying bills, going to work, and studying for class and not as the overwhelming psychological burden that it is,” says Dr. Walker.
And despite what some may say, racial discrimination is not merely “a thing of the past,” Dr. Walker says.
“Instead, discrimination has shifted form from more overt forms of discrimination to less obvious microaggression,” she says.
It’s also critical that young adults are taught how to deal with racism to avoid the risk of “internalizing that they deserve to be mistreated, and/or that they have to work twice as hard to overcome racism,” says Dr. Walker.
“Both scenarios can escalate hopelessness and worry, psychological features of depression and anxiety, respectively,” Dr. Walker says.
Embrace your emotions
Known around the office as “a big teddy bear,” Frederick Herman, a mortgage loan originator based in Charlotte, Va., was coaching a newer employee on how to make sales calls, a common practice in his line of work.
He says a day or 2 days later, his manager let him know that he had made an employee “very uncomfortable” by intimidating them while they were on the phone. Mr. Herman, 29, was told to watch his “aggressive” behavior.
“I’m a bigger Black man. I’m like 6’2, 300 lbs., somewhat muscular. So, if me talking or trying to coach her came off as intimidating, then there’s nothing that I could do or say differently than I was already doing to make her not feel intimidated,” Mr. Herman says.
“If a big teddy bear is now intimidating to you, that just tells me everything I need to know.”
This wasn’t the first time Mr. Herman had been reprimanded for being “too aggressive” or “showing off” when trying to help colleagues at work.
“I’ve had other experiences at work where I may not share my ideas, or I may get super anxious,” says Mr. Herman, a Black man of Haitian descent.
It’s important to allow yourself to feel your emotions after facing acts of discrimination, says Ebony Butler, PhD, a licensed psychologist and creator of My Therapy Cards, a card deck tailored for men, women, and teens of color, with self-care and reflection prompts.
This is a practice called “self-validation” and can reduce the tendency to blame oneself for the mistreatment, says Dr. Butler.
Mr. Herman, 29, says that he recently signed up for therapy to work through his struggles with anxiety.
Relaxation techniques, like grounding and mindfulness, can also be helpful, says Dr. Butler.
“Some example ways to practice grounding are immersing oneself in nature, walking bare feet on the ground, lying on the floor, practicing slow, deep breathing, or engaging the senses,” she says.
“When we are grounded and present, we can better manage our responses and plan our action steps.”
Utilize unique
If you find yourself in a racially charged school or workplace setting, don’t be intimidated, says Wendy Osefo, PhD, education professor at Johns Hopkins University, Baltimore, political commentator, and television personality.
Dr. Osefo made history in 2016 as the first Black woman to earn a PhD in public affairs/community development from Rutgers University.
“Your attitude should be that, no matter how different you might be, you belong, and you earned the right to occupy this space. You’re not less qualified than others who surround you,” she says.
Dr. Ofeso is also CEO of The 1954 Equity Project, an organization that gives minority students tools to succeed in higher education – like mentorships, peer support groups, and other resources and services – all while remaining their authentic selves.
No matter how uncomfortable it might be, staying true to who you are vs. conforming to the masses pays off, says Dr. Osefo.
“Being different is unique and allows you to bring a new and fresh perspective into an environment,” she says.
“Leaning into this uniqueness builds a level of confidence that will aid in your ability to be successful.”
A version of this article first appeared on WebMD.com.
Joel Bervell recalls leaving his hometown of Seattle for the East Coast after being accepted into Yale University.
Still getting accustomed to the big move, Mr. Bervell, who had breezed through high school with straight As, went to see his chemistry professor for advice after getting a low grade on a test.
“He took one look at me and said, ‘Oh, if you’re on the football team, you don’t need to worry about it. So many people from the football team come into the class and end up dropping out, so if you need to drop this class, you can,’ ” Mr. Bervell says.
Mr. Bervell, who is Black, was not on the football team, nor did he receive a sports scholarship of any kind.
“For that professor to make an assumption of me, which to me felt like it was based on my race, made me less likely to want to go into a science field, where I felt like I was being judged before I even had a chance to prove myself,” Mr. Bervell says.
.
Researchers studied health data on 1,834 Americans ages 18-28 over a 10-year span. Findings show that the more instances of discrimination they experienced – including ageism, sexism, and racism – the more likely they were to face mental and behavioral struggles, like mental illness, drug use, severe psychological distress, and poor overall health.
Mr. Bervell, now 26, says he feels lucky that growing up, he was taught healthy ways to process his feelings and emotions.
“Instead of taking that and internalizing it, I said, ‘how can I use this to prove him wrong?’” he says. “Does that mean I need to work harder or does that mean I need to find a different mentor? Surround myself with different people?”
Mr. Bervell is currently a 3rd-year medical student at Washington State University.
When he’s not at the hospital seeing patients, you can find him educating his nearly 340,000 TikTok followers on topics like racial bias in medicine.
Acknowledge the impact
Most Black people don’t tie psychological distress to acts of racism, according to Rheeda Walker, PhD, psychology professor at the University of Houston and author of “The Unapologetic Guide to Black Mental Health” (Oakland, Calif.: New Harbinger Publications, 2020).
Many Black people even normalize it.
“Individuals deal with it [racism] as just another thing, like paying bills, going to work, and studying for class and not as the overwhelming psychological burden that it is,” says Dr. Walker.
And despite what some may say, racial discrimination is not merely “a thing of the past,” Dr. Walker says.
“Instead, discrimination has shifted form from more overt forms of discrimination to less obvious microaggression,” she says.
It’s also critical that young adults are taught how to deal with racism to avoid the risk of “internalizing that they deserve to be mistreated, and/or that they have to work twice as hard to overcome racism,” says Dr. Walker.
“Both scenarios can escalate hopelessness and worry, psychological features of depression and anxiety, respectively,” Dr. Walker says.
Embrace your emotions
Known around the office as “a big teddy bear,” Frederick Herman, a mortgage loan originator based in Charlotte, Va., was coaching a newer employee on how to make sales calls, a common practice in his line of work.
He says a day or 2 days later, his manager let him know that he had made an employee “very uncomfortable” by intimidating them while they were on the phone. Mr. Herman, 29, was told to watch his “aggressive” behavior.
“I’m a bigger Black man. I’m like 6’2, 300 lbs., somewhat muscular. So, if me talking or trying to coach her came off as intimidating, then there’s nothing that I could do or say differently than I was already doing to make her not feel intimidated,” Mr. Herman says.
“If a big teddy bear is now intimidating to you, that just tells me everything I need to know.”
This wasn’t the first time Mr. Herman had been reprimanded for being “too aggressive” or “showing off” when trying to help colleagues at work.
“I’ve had other experiences at work where I may not share my ideas, or I may get super anxious,” says Mr. Herman, a Black man of Haitian descent.
It’s important to allow yourself to feel your emotions after facing acts of discrimination, says Ebony Butler, PhD, a licensed psychologist and creator of My Therapy Cards, a card deck tailored for men, women, and teens of color, with self-care and reflection prompts.
This is a practice called “self-validation” and can reduce the tendency to blame oneself for the mistreatment, says Dr. Butler.
Mr. Herman, 29, says that he recently signed up for therapy to work through his struggles with anxiety.
Relaxation techniques, like grounding and mindfulness, can also be helpful, says Dr. Butler.
“Some example ways to practice grounding are immersing oneself in nature, walking bare feet on the ground, lying on the floor, practicing slow, deep breathing, or engaging the senses,” she says.
“When we are grounded and present, we can better manage our responses and plan our action steps.”
Utilize unique
If you find yourself in a racially charged school or workplace setting, don’t be intimidated, says Wendy Osefo, PhD, education professor at Johns Hopkins University, Baltimore, political commentator, and television personality.
Dr. Osefo made history in 2016 as the first Black woman to earn a PhD in public affairs/community development from Rutgers University.
“Your attitude should be that, no matter how different you might be, you belong, and you earned the right to occupy this space. You’re not less qualified than others who surround you,” she says.
Dr. Ofeso is also CEO of The 1954 Equity Project, an organization that gives minority students tools to succeed in higher education – like mentorships, peer support groups, and other resources and services – all while remaining their authentic selves.
No matter how uncomfortable it might be, staying true to who you are vs. conforming to the masses pays off, says Dr. Osefo.
“Being different is unique and allows you to bring a new and fresh perspective into an environment,” she says.
“Leaning into this uniqueness builds a level of confidence that will aid in your ability to be successful.”
A version of this article first appeared on WebMD.com.
California plans for a post-Roe world as abortion access shrinks elsewhere
SACRAMENTO – With access to abortion at stake across America, California is preparing to become the nation’s abortion provider.
Democratic Gov. Gavin Newsom and legislative leaders have asked a group of reproductive health experts to propose policies to bolster the state’s abortion infrastructure and ready it for more patients. Lawmakers plan to begin debating the ideas when they reconvene in January.
Abortion clinics are already girding themselves for a surge in demand.
Janet Jacobson, MD, medical director of Planned Parenthood of Orange and San Bernardino Counties, said three or four out-of-state patients visit her clinics each day – about double the number that sought treatment before a near-total ban on abortion took effect in Texas in September.
While the nine clinics can absorb that slow trickle, they expect up to 50 out-of-state patients a week if the U.S. Supreme Court’s conservative majority guts abortion rights nationally, Dr. Jacobson said. She bases her estimate on new data from the Guttmacher Institute, a research organization that supports abortion and reproductive health rights.
She is adding staff members and appointment capacity, hoping to accommodate everyone.
“We have to make sure we can still continue to care for all of our California patients,” Dr. Jacobson said. “We don’t want them getting squeezed out” of appointments.
The Texas law banned nearly all abortions after about 6 weeks of pregnancy and empowered private citizens to sue anyone who performs or “aids and abets” an abortion after that time. The Supreme Court heard arguments in that case on Nov. 1 and is expected to announce a ruling on its constitutionality in June. Nonetheless, Florida and Ohio have announced plans for copycat laws.
Next month the high court will hear another abortion case with even broader implications, Dobbs v. Jackson Women’s Health Organization, a lawsuit challenging the constitutionality of a 2018 Mississippi law that prohibited abortion after 15 weeks. If the court sides with Mississippi, its decision could overturn existing abortion rights set by the landmark Roe v. Wade case.
Should that happen, reproductive rights experts predict, 26 states will ban the procedure altogether, and states with stronger protections for abortion, like California, will draw even more patients. There could be up to a 3,000% increase in people who “may drive to California for abortion care” each year, according to the Guttmacher data.
In 2017, the most recent year for which data are available from Guttmacher, California – by far the nation’s most populous state – had more abortion providers than any other state, with 419 hospitals, clinics, or doctors’ offices performing the procedure. The next highest were New York, with 252, and Florida, with 85. Neighboring Arizona and Nevada each had 11. Of the 862,320 abortions performed in the United States that year, 132.680, about 15% were in California.
Planned Parenthood clinics in California say they already serve about 7,000 out-of-state patients a year and are expecting a surge of new ones, especially in travel hubs like the Los Angeles area.
In September, Planned Parenthood and groups such as Black Women for Wellness convened the California Future of Abortion Council with backing from influential Democratic leaders including Gov. Newsom, state Senate leader Toni Atkins, and Assembly Speaker Anthony Rendon.
Ms. Atkins, who was the director of a San Diego women’s health clinic in the 1980s, said she spent time with women from states where it was hard to get an abortion. She said California is committed to ensuring abortion access in the state and beyond.
The council is focused on increasing funding for abortion services, providing logistical and financial help for women who need to travel, increasing the number of health care providers who perform abortions, and strengthening legal protections for them.
Increasing capacity could mean licensing more practitioners to provide abortions or pumping more resources into telehealth so people can see a doctor online to prescribe pills for a medical abortion – a service California doctors currently can provide to patients only in California.
The most important thing the state should do is fix its shortage of providers, especially those who perform second-trimester abortions, which are more expensive and complicated than first-trimester abortions, said council member Daniel Grossman, MD, director of the Advancing New Standards in Reproductive Health program at the University of California, San Francisco.
It’s not feasible to place an abortion provider in every corner of the state, Dr. Grossman said. Instead, the council should focus on creating “hubs that can provide abortion care for large numbers of people” in easy-to-get-to locations.
California already struggles to provide abortions to all who seek them, especially low-income women covered by Medi-Cal, California’s Medicaid program. For example, 28 counties – home to 10% of Medi-Cal recipients of childbearing age – don’t have facilities that provide abortions to Medi-Cal patients.
A medical abortion, in which pills are used to terminate a pregnancy, costs California patients an average of $306 out-of-pocket, according to an analysis by the California Health Benefits Review Program, but isn’t available after 10 weeks. After that, the only option is a surgical abortion, which costs an average of $887 out-of-pocket in California.
One of the council’s recommendations will likely be to increase the rate Medi-Cal payments for abortions so more providers will perform them, said council member Fabiola Carrión, interim director for reproductive and sexual health at the National Health Law Program.
Medi-Cal pays $354.43 for a second-trimester abortion. A 2020 study in the journal Contraception found that states paid between $79 and $626 for a second-trimester abortion in 2017.
Increasing Medi-Cal rates won’t help patients traveling from outside California. Generally, private insurance doesn’t cover out-of-state abortions, so most women will be on the hook for the full cost, and those enrolled in other states’ Medicaid programs must pay out-of-pocket, too.
The council hopes to reduce costs for state residents and visitors, said Brandon Richards, director of communications for Planned Parenthood Affiliates of California. “It’s about making it easy for people to access abortion in California, whether they reside here or are coming in from out of state,” he said.
One way to target costs is by funding the practical support, like helping to pay for transportation, child care, hotels, or time off work, said council member Jessica Pinckney, executive director of Access Reproductive Justice, a fund that helps people pay for abortions.
Ms. Pinckney said she’s working with Los Angeles County to set up a public abortion fund to cover some of those costs for anyone seeking an abortion in the county. It would be modeled after similar pots maintained by the cities of New York; Austin, Tex.; and Portland, Ore., and could eventually be a template for the first statewide fund, Ms. Pinckney said.
Most Texans seeking abortions since that state’s law took effect are going to nearby states like Colorado, New Mexico, and Oklahoma, said Sierra Harris, deputy director of network strategies for the National Network of Abortion Funds. Women in those states, in turn, are having trouble getting care and are looking to California for appointments.
Practical support is important for out-of-state patients, said Alissa Perrucci, PhD, MPH, operations manager at the Women’s Options Center at Zuckerberg San Francisco General Hospital, one of five abortion clinics inside California hospitals.
Dr. Perrucci’s clinic is focusing on telemedicine, phone counseling, and other ways to save time so it can add appointments for out-of-state patients if necessary.
But more slots are useless if women can’t make it to California. The clinic has booked about 10 appointments for Texans since the state’s ban went into effect, but only half have shown up, mostly women with family connections in California.
“Most people just don’t have the money to get here,” she said. “If the burden of abortion was borne predominantly by the wealthy, yeah, they’d just fly here.”
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
SACRAMENTO – With access to abortion at stake across America, California is preparing to become the nation’s abortion provider.
Democratic Gov. Gavin Newsom and legislative leaders have asked a group of reproductive health experts to propose policies to bolster the state’s abortion infrastructure and ready it for more patients. Lawmakers plan to begin debating the ideas when they reconvene in January.
Abortion clinics are already girding themselves for a surge in demand.
Janet Jacobson, MD, medical director of Planned Parenthood of Orange and San Bernardino Counties, said three or four out-of-state patients visit her clinics each day – about double the number that sought treatment before a near-total ban on abortion took effect in Texas in September.
While the nine clinics can absorb that slow trickle, they expect up to 50 out-of-state patients a week if the U.S. Supreme Court’s conservative majority guts abortion rights nationally, Dr. Jacobson said. She bases her estimate on new data from the Guttmacher Institute, a research organization that supports abortion and reproductive health rights.
She is adding staff members and appointment capacity, hoping to accommodate everyone.
“We have to make sure we can still continue to care for all of our California patients,” Dr. Jacobson said. “We don’t want them getting squeezed out” of appointments.
The Texas law banned nearly all abortions after about 6 weeks of pregnancy and empowered private citizens to sue anyone who performs or “aids and abets” an abortion after that time. The Supreme Court heard arguments in that case on Nov. 1 and is expected to announce a ruling on its constitutionality in June. Nonetheless, Florida and Ohio have announced plans for copycat laws.
Next month the high court will hear another abortion case with even broader implications, Dobbs v. Jackson Women’s Health Organization, a lawsuit challenging the constitutionality of a 2018 Mississippi law that prohibited abortion after 15 weeks. If the court sides with Mississippi, its decision could overturn existing abortion rights set by the landmark Roe v. Wade case.
Should that happen, reproductive rights experts predict, 26 states will ban the procedure altogether, and states with stronger protections for abortion, like California, will draw even more patients. There could be up to a 3,000% increase in people who “may drive to California for abortion care” each year, according to the Guttmacher data.
In 2017, the most recent year for which data are available from Guttmacher, California – by far the nation’s most populous state – had more abortion providers than any other state, with 419 hospitals, clinics, or doctors’ offices performing the procedure. The next highest were New York, with 252, and Florida, with 85. Neighboring Arizona and Nevada each had 11. Of the 862,320 abortions performed in the United States that year, 132.680, about 15% were in California.
Planned Parenthood clinics in California say they already serve about 7,000 out-of-state patients a year and are expecting a surge of new ones, especially in travel hubs like the Los Angeles area.
In September, Planned Parenthood and groups such as Black Women for Wellness convened the California Future of Abortion Council with backing from influential Democratic leaders including Gov. Newsom, state Senate leader Toni Atkins, and Assembly Speaker Anthony Rendon.
Ms. Atkins, who was the director of a San Diego women’s health clinic in the 1980s, said she spent time with women from states where it was hard to get an abortion. She said California is committed to ensuring abortion access in the state and beyond.
The council is focused on increasing funding for abortion services, providing logistical and financial help for women who need to travel, increasing the number of health care providers who perform abortions, and strengthening legal protections for them.
Increasing capacity could mean licensing more practitioners to provide abortions or pumping more resources into telehealth so people can see a doctor online to prescribe pills for a medical abortion – a service California doctors currently can provide to patients only in California.
The most important thing the state should do is fix its shortage of providers, especially those who perform second-trimester abortions, which are more expensive and complicated than first-trimester abortions, said council member Daniel Grossman, MD, director of the Advancing New Standards in Reproductive Health program at the University of California, San Francisco.
It’s not feasible to place an abortion provider in every corner of the state, Dr. Grossman said. Instead, the council should focus on creating “hubs that can provide abortion care for large numbers of people” in easy-to-get-to locations.
California already struggles to provide abortions to all who seek them, especially low-income women covered by Medi-Cal, California’s Medicaid program. For example, 28 counties – home to 10% of Medi-Cal recipients of childbearing age – don’t have facilities that provide abortions to Medi-Cal patients.
A medical abortion, in which pills are used to terminate a pregnancy, costs California patients an average of $306 out-of-pocket, according to an analysis by the California Health Benefits Review Program, but isn’t available after 10 weeks. After that, the only option is a surgical abortion, which costs an average of $887 out-of-pocket in California.
One of the council’s recommendations will likely be to increase the rate Medi-Cal payments for abortions so more providers will perform them, said council member Fabiola Carrión, interim director for reproductive and sexual health at the National Health Law Program.
Medi-Cal pays $354.43 for a second-trimester abortion. A 2020 study in the journal Contraception found that states paid between $79 and $626 for a second-trimester abortion in 2017.
Increasing Medi-Cal rates won’t help patients traveling from outside California. Generally, private insurance doesn’t cover out-of-state abortions, so most women will be on the hook for the full cost, and those enrolled in other states’ Medicaid programs must pay out-of-pocket, too.
The council hopes to reduce costs for state residents and visitors, said Brandon Richards, director of communications for Planned Parenthood Affiliates of California. “It’s about making it easy for people to access abortion in California, whether they reside here or are coming in from out of state,” he said.
One way to target costs is by funding the practical support, like helping to pay for transportation, child care, hotels, or time off work, said council member Jessica Pinckney, executive director of Access Reproductive Justice, a fund that helps people pay for abortions.
Ms. Pinckney said she’s working with Los Angeles County to set up a public abortion fund to cover some of those costs for anyone seeking an abortion in the county. It would be modeled after similar pots maintained by the cities of New York; Austin, Tex.; and Portland, Ore., and could eventually be a template for the first statewide fund, Ms. Pinckney said.
Most Texans seeking abortions since that state’s law took effect are going to nearby states like Colorado, New Mexico, and Oklahoma, said Sierra Harris, deputy director of network strategies for the National Network of Abortion Funds. Women in those states, in turn, are having trouble getting care and are looking to California for appointments.
Practical support is important for out-of-state patients, said Alissa Perrucci, PhD, MPH, operations manager at the Women’s Options Center at Zuckerberg San Francisco General Hospital, one of five abortion clinics inside California hospitals.
Dr. Perrucci’s clinic is focusing on telemedicine, phone counseling, and other ways to save time so it can add appointments for out-of-state patients if necessary.
But more slots are useless if women can’t make it to California. The clinic has booked about 10 appointments for Texans since the state’s ban went into effect, but only half have shown up, mostly women with family connections in California.
“Most people just don’t have the money to get here,” she said. “If the burden of abortion was borne predominantly by the wealthy, yeah, they’d just fly here.”
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
SACRAMENTO – With access to abortion at stake across America, California is preparing to become the nation’s abortion provider.
Democratic Gov. Gavin Newsom and legislative leaders have asked a group of reproductive health experts to propose policies to bolster the state’s abortion infrastructure and ready it for more patients. Lawmakers plan to begin debating the ideas when they reconvene in January.
Abortion clinics are already girding themselves for a surge in demand.
Janet Jacobson, MD, medical director of Planned Parenthood of Orange and San Bernardino Counties, said three or four out-of-state patients visit her clinics each day – about double the number that sought treatment before a near-total ban on abortion took effect in Texas in September.
While the nine clinics can absorb that slow trickle, they expect up to 50 out-of-state patients a week if the U.S. Supreme Court’s conservative majority guts abortion rights nationally, Dr. Jacobson said. She bases her estimate on new data from the Guttmacher Institute, a research organization that supports abortion and reproductive health rights.
She is adding staff members and appointment capacity, hoping to accommodate everyone.
“We have to make sure we can still continue to care for all of our California patients,” Dr. Jacobson said. “We don’t want them getting squeezed out” of appointments.
The Texas law banned nearly all abortions after about 6 weeks of pregnancy and empowered private citizens to sue anyone who performs or “aids and abets” an abortion after that time. The Supreme Court heard arguments in that case on Nov. 1 and is expected to announce a ruling on its constitutionality in June. Nonetheless, Florida and Ohio have announced plans for copycat laws.
Next month the high court will hear another abortion case with even broader implications, Dobbs v. Jackson Women’s Health Organization, a lawsuit challenging the constitutionality of a 2018 Mississippi law that prohibited abortion after 15 weeks. If the court sides with Mississippi, its decision could overturn existing abortion rights set by the landmark Roe v. Wade case.
Should that happen, reproductive rights experts predict, 26 states will ban the procedure altogether, and states with stronger protections for abortion, like California, will draw even more patients. There could be up to a 3,000% increase in people who “may drive to California for abortion care” each year, according to the Guttmacher data.
In 2017, the most recent year for which data are available from Guttmacher, California – by far the nation’s most populous state – had more abortion providers than any other state, with 419 hospitals, clinics, or doctors’ offices performing the procedure. The next highest were New York, with 252, and Florida, with 85. Neighboring Arizona and Nevada each had 11. Of the 862,320 abortions performed in the United States that year, 132.680, about 15% were in California.
Planned Parenthood clinics in California say they already serve about 7,000 out-of-state patients a year and are expecting a surge of new ones, especially in travel hubs like the Los Angeles area.
In September, Planned Parenthood and groups such as Black Women for Wellness convened the California Future of Abortion Council with backing from influential Democratic leaders including Gov. Newsom, state Senate leader Toni Atkins, and Assembly Speaker Anthony Rendon.
Ms. Atkins, who was the director of a San Diego women’s health clinic in the 1980s, said she spent time with women from states where it was hard to get an abortion. She said California is committed to ensuring abortion access in the state and beyond.
The council is focused on increasing funding for abortion services, providing logistical and financial help for women who need to travel, increasing the number of health care providers who perform abortions, and strengthening legal protections for them.
Increasing capacity could mean licensing more practitioners to provide abortions or pumping more resources into telehealth so people can see a doctor online to prescribe pills for a medical abortion – a service California doctors currently can provide to patients only in California.
The most important thing the state should do is fix its shortage of providers, especially those who perform second-trimester abortions, which are more expensive and complicated than first-trimester abortions, said council member Daniel Grossman, MD, director of the Advancing New Standards in Reproductive Health program at the University of California, San Francisco.
It’s not feasible to place an abortion provider in every corner of the state, Dr. Grossman said. Instead, the council should focus on creating “hubs that can provide abortion care for large numbers of people” in easy-to-get-to locations.
California already struggles to provide abortions to all who seek them, especially low-income women covered by Medi-Cal, California’s Medicaid program. For example, 28 counties – home to 10% of Medi-Cal recipients of childbearing age – don’t have facilities that provide abortions to Medi-Cal patients.
A medical abortion, in which pills are used to terminate a pregnancy, costs California patients an average of $306 out-of-pocket, according to an analysis by the California Health Benefits Review Program, but isn’t available after 10 weeks. After that, the only option is a surgical abortion, which costs an average of $887 out-of-pocket in California.
One of the council’s recommendations will likely be to increase the rate Medi-Cal payments for abortions so more providers will perform them, said council member Fabiola Carrión, interim director for reproductive and sexual health at the National Health Law Program.
Medi-Cal pays $354.43 for a second-trimester abortion. A 2020 study in the journal Contraception found that states paid between $79 and $626 for a second-trimester abortion in 2017.
Increasing Medi-Cal rates won’t help patients traveling from outside California. Generally, private insurance doesn’t cover out-of-state abortions, so most women will be on the hook for the full cost, and those enrolled in other states’ Medicaid programs must pay out-of-pocket, too.
The council hopes to reduce costs for state residents and visitors, said Brandon Richards, director of communications for Planned Parenthood Affiliates of California. “It’s about making it easy for people to access abortion in California, whether they reside here or are coming in from out of state,” he said.
One way to target costs is by funding the practical support, like helping to pay for transportation, child care, hotels, or time off work, said council member Jessica Pinckney, executive director of Access Reproductive Justice, a fund that helps people pay for abortions.
Ms. Pinckney said she’s working with Los Angeles County to set up a public abortion fund to cover some of those costs for anyone seeking an abortion in the county. It would be modeled after similar pots maintained by the cities of New York; Austin, Tex.; and Portland, Ore., and could eventually be a template for the first statewide fund, Ms. Pinckney said.
Most Texans seeking abortions since that state’s law took effect are going to nearby states like Colorado, New Mexico, and Oklahoma, said Sierra Harris, deputy director of network strategies for the National Network of Abortion Funds. Women in those states, in turn, are having trouble getting care and are looking to California for appointments.
Practical support is important for out-of-state patients, said Alissa Perrucci, PhD, MPH, operations manager at the Women’s Options Center at Zuckerberg San Francisco General Hospital, one of five abortion clinics inside California hospitals.
Dr. Perrucci’s clinic is focusing on telemedicine, phone counseling, and other ways to save time so it can add appointments for out-of-state patients if necessary.
But more slots are useless if women can’t make it to California. The clinic has booked about 10 appointments for Texans since the state’s ban went into effect, but only half have shown up, mostly women with family connections in California.
“Most people just don’t have the money to get here,” she said. “If the burden of abortion was borne predominantly by the wealthy, yeah, they’d just fly here.”
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Mask-wearing cuts new COVID-19 cases by 53%, study says
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
Social distancing and handwashing were also effective at lowering the number of cases, but wearing masks was the most effective tool against the coronavirus.
“Personal and social measures, including handwashing, mask wearing, and physical distancing are effective at reducing the incidence of COVID-19,” the study authors wrote.
The research team, which included public health and infectious disease specialists in Australia, China, and the U.K., evaluated 72 studies of COVID-19 precautions during the pandemic. They later looked at eight studies that focused on handwashing, mask wearing, and physical distancing.
Among six studies that looked at mask wearing, the researchers found a 53% reduction in COVID-19 cases. In the broader analysis with additional studies, wearing a mask reduced coronavirus transmission, cases, and deaths.
In one study across 200 countries, mandatory mask wearing resulted in nearly 46% fewer negative outcomes from COVID-19. In another study in the U.S., coronavirus transmission was reduced 29% in states where masks were mandatory.
But the research team couldn’t analyze the impact of the type of face mask used, the frequency of mask wearing, or the overall compliance with wearing face masks.
Among five studies that looked at physical distancing, the researchers found a 25% reduction in the rate of COVID-19. A study in the U.S. showed a 12% decrease in coronavirus transmission, while another study in Iran reported a reduction in COVID-19 mortality.
Handwashing interventions also suggested a substantial reduction of COVID-19 cases up to 53%, the researchers wrote. But in adjusted models, the results weren’t statistically significant due to the small number of studies included.
Other studies found significant decreases related to other public health measures, such as quarantines, broad lockdowns, border closures, school closures, business closures, and travel restrictions. Still, the research team couldn’t analyze the overall effectiveness of these measures due to the different ways the studies were conducted.
The study lines up with other research conducted so far during the pandemic, the research team wrote, which indicates that wearing masks and physical distancing can reduce transmission, cases, and deaths.
That said, more studies are needed, particularly now that vaccinations are available and contagious coronavirus variants have become prevalent.
“Further research is needed to assess the effectiveness of public health measures after adequate vaccination coverage has been achieved,” they wrote.
“It is likely that further control of the COVID-19 pandemic depends not only on high vaccination coverage and its effectiveness but also on ongoing adherence to effective and sustainable public health measures,” they concluded.
A version of this article first appeared on WebMD.com.
FROM THE BMJ