User login
Nap length linked to cognitive changes
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.

Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.

The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.

This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.
Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.
The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.
This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
No wonder we feel worse after naps
Some of us have hectic schedules that may make a nap feel more necessary. It’s common knowledge that naps shouldn’t be too long – maybe 20 minutes or so – but if you frequently take 3-hour naps and wake up thinking you’re late for school even though you’re 47 and have your PhD, this LOTME is for you.
Studies have shown that there is a link between napping during the day and Alzheimer’s/cognitive decline, but now we’ve got a double whammy for you: Longer and more frequent napping is linked to worse cognition after a year, and in turn, those with cognitive decline and Alzheimer’s are known to nap longer and more frequently during the day.
“We now know that the pathology related to cognitive decline can cause other changes in function,” he said. “It’s really a multisystem disorder, also including difficulty sleeping, changes in movement, changes in body composition, depression symptoms, behavioral changes, etc.,” coauthor Aron Buchman, MD, said in a statement from Rush University Medical Center.
The investigators monitored 1,400 patients over the course of 14 years with wrist bracelets that recorded when a person was not active during the day and considered that a nap.
At the beginning of the study, 75% of the study subjects had no cognitive impairment, 19.5% had some cognitive impairment, and approximately 4% had Alzheimer’s. Napping during the day only increased about 11 minutes a year for those with no signs of cognitive impairment, but those who showed significantly more signs of cognitive decline doubled their nap time and those actually diagnosed with Alzheimer’s tripled theirs.
The investigators did not imply that napping causes Alzheimer’s, but they noted that people who are older and nap more than an hour a day are 40% more likely to be at risk. It is something to consider and monitor.
Sometimes, after all, a nap seems like the best idea ever, but more often than not we wake up feeling 10 times worse. Our bodies may be giving us a heads up.
Pokemon Go away depression
The summer of 2016 was a great time if you happened to be a fan of Pokemon. Which is quite a lot of people. For almost 20 years millions have enjoyed the games and animated series, but Pokemon Go brought the thrill of catching Pokemon to life in a whole new way. For the first time, you could go out into the world and pretend you were a real Pokemon trainer, and everywhere you went, there would be others like you.
The ability to chase after Pikachu and Charizard in real life (well, augmented reality, but close enough) seemed to bring people a lot of joy, but seemed is never good enough for science. Can’t have anecdotes, we need data! So researchers at the London School of Economics and Political Science conducted a study into how Pokemon Go affected local Internet search rates of depression as the game was released slowly around the world.
Through analyzing Google Trend data of words like “depression,” “anxiety,” and “stress,” the researchers found that the release of Pokemon Go was significantly associated with a noticeable, though short-term, drop in depression-related Internet searches. Location-based augmented reality games may alleviate symptoms of mild depression, the researchers said, as they encourage physical activity, face-to-face socialization, and exposure to nature, though they added that simply going outside is likely not enough to combat clinical cases of severe depression.
Still, augmented reality games represent a viable target for public health investment, since they’re easy to use and inexpensive to make. That said, we’re not sure we want the FDA or CDC making a new Pokemon Go game. They’d probably end up filling the streets with Mr. Mime. And no one would leave their house for that.
And now a word from our sponsor
How many times has this happened to you? You need to repair a jet engine, inspect a nuclear reactor cooling system, AND perform bowel surgery, but you can’t carry around all the heavy, old-fashioned tools needed for those jobs.
Well, we’ve got one tool that can do it all! And that tool is a snake. No, it’s a robot.
It’s both! It’s the COntinuum roBot for Remote Applications. COBRA is the robot that looks like a snake! A snake that’s 5 meters long but only as thick as a pencil (about 9 mm in diameter). A robot with “extraordinary manoeuvrability and responsiveness due to … a compliant-joint structure and multiple continuous sections that enable it to bend at around 90 degrees,” according to the team at the University of Nottingham (England) that developed it.
COBRA comes equipped with a stereovision camera and a miniature cutting tool to perform complex industrial repair, but other devices can be interchanged for possible medical use.
COBRA and its joystick-like controller were designed to be easy to use. Dr. Oladejo Olaleye, the ear, nose, and throat and robotic surgeon at University Hospitals of Leicester who is directing its surgical development, was able to use COBRA on a dummy after just 5 minutes of training. He called it “the future of diagnostic endoscopy and therapeutic surgery.”
Don’t be the last aircraft engineer/nuclear technician/surgeon on your block to have this ultraslender, ultramaneuverable reptilian repair robot. Get your COBRA now! Operators are standing by.
Disclaimer: Robot is still under development and not yet on sale.
Rule, (worm) Britannia!
As long as there have been people, there have been parasitic worms living in their guts. Helminth infection is a continuing and largely ignored crisis in poor, tropical nations, though worm-based diseases have been basically eliminated from wealthier countries.
This wasn’t always the case, however, as a study published in PLOS Neglected Tropical Diseases (now there’s a specific topic) has found. The researchers detail the glorious history of helminth infestation in the United Kingdom from the Victorian era all the way back to prehistory, scouring hundreds of skeletons found in 17 sites across the country for eggs, which can remain intact for thousands of years.
The researchers found that two eras in particular had very high rates of infection. Unsurprisingly, the late medieval era was one of them, but the other is less obvious. The Romans were famous for their hygiene, their baths, and their plumbing, but maybe they also should be famous for the abundance of worms in their bellies. That doesn’t make sense at first: Shouldn’t good hygiene lower infection? The benefits of a good sewer system, however, are lessened when the waste containing said infectious organisms is used to fertilize crops. Recycling is generally a good thing, but less so when you’re recycling parasitic worms.
Curiously, of the three sites from the industrial age, only the one in London had high levels of worm infestation. Considering how dirty and cramped 19th-century British cities were, one might expect disease to run rampant (tuberculosis certainly did), but the sites in Oxford and Birmingham were almost devoid of worms. The researchers theorized that this was because of access to clean well water. Or maybe worms just have a thing for London. [Editor’s note: It’s probably not that.]
Will you have cardiac arrest? New tech may predict if and when
Deaths from COVID-19 may have caught more attention lately, but heart disease remains the leading cause of death in the United States.
More than 300,000 Americans will die this year of sudden cardiac arrest (also called sudden cardiac death, or SCD), when the heart abruptly stops working.
These events happen suddenly and often without warning, making them nearly impossible to predict. But that may be changing, thanks to 3D imaging and artificial intelligence (AI) technology under study at Johns Hopkins University, Baltimore.
There, researchers are working to create more accurate and personalized models of the heart – and not just any heart, your heart, if you have heart disease.
“Right now, a clinician can only say whether a patient is at risk or not at risk for sudden death,” says Dan Popescu, PhD, a Johns Hopkins research scientist and first author of a new study on AI’s ability to predict sudden cardiac arrest. “With this new technology, you can have much more nuanced predictions of probability of an event over time.”
Put another way: With AI, clinicians may be able not only to predict if someone is at risk for sudden cardiac arrest, but also when it is most likely to happen. They can do this using a much clearer and more personalized look at the electrical “wiring” of your heart.
Your heart, the conductor
Your heart isn’t just a metronome responsible for keeping a steady stream of blood pumping to tissues with every beat. It’s also a conductor through which vital energy flows.
To make the heart beat, electrical impulses flow from the top to the bottom of the organ. Healthy heart cells relay this electricity seamlessly. But in a heart damaged by inflammation or a past heart attack, scar tissue will block the energy flow.
When an electrical impulse encounters a scarred area, the signal can become erratic, disrupting the set top-to-bottom path and causing irregular heartbeats (arrhythmias), which increase someone’s danger of sudden cardiac death.
Seeing the heart in 3D
Today’s tests offer some insights into the heart’s makeup. For example, MRI scans can reveal damaged areas. PET scans can show inflammation. And EKGs can record the heart’s electrical signals from beat to beat.
But all these technologies offer only a snapshot, showing heart health at a moment in time. They can’t predict the future. That’s why scientists at Johns Hopkins are going further to develop 3D digital replicas of a person’s heart, known as computational heart models.
Computational models are computer-simulated replicas that combine mathematics, physics, and computer science. These models have been around for a long time and are used in many fields, ranging from manufacturing to economics.
In heart medicine, these models are populated with digital “cells,” which imitate living cells and can be programmed with different electrical properties, depending on whether they are healthy or diseased.
“Currently available imaging and testing (MRIs, PETs, EKGs) give some representation of the scarring, but you cannot translate that to what is going to happen over time,” says Natalia Trayanova, PhD, of the Johns Hopkins department of biomedical engineering.
“With computational heart models, we create a dynamic digital image of the heart. We can then give the digital image an electrical stimulus and assess how the heart is able to respond. Then you can better predict what is going to happen.”
The computerized 3D models also mean better, more accurate treatment for heart conditions.
For example, a common treatment for a type of arrhythmia known as atrial fibrillation is ablation, or burning some heart tissue. Ablation stops the erratic electrical impulses causing the arrhythmia, but it can also damage otherwise healthy heart cells.
A personalized computational heart model could allow doctors to see more accurately what areas should and shouldn’t be treated for a specific patient.
Using deep learning AI to predict health outcomes
Dr. Trayanova’s colleague Dr. Popescu is applying deep learning and AI to do more with computerized heart models to predict the future.
In a recent paper in Nature Cardiovascular Research, the research team showed their algorithm assessed the health of 269 patients and was able to predict the chance of sudden cardiac arrest up to 10 years in advance.
“This is really the first time ever, as far as we know, where deep learning technology has been proven to analyze scarring of the heart in a successful way,” Dr. Popescu says.
Dr. Popescu and Dr. Trayanova say the AI algorithm gathers information from the 3D computational heart models with patient data like MRIs, ethnicity, age, lifestyle, and other clinical information. Analyzing all these data can produce accurate and consistent estimates about how long patients might live if they are at risk for sudden death.
“You can’t afford to be wrong. If you are wrong, you can actually impact a patient’s quality of life dramatically,” Dr. Popescu says. “Having clinicians use this technology in the decision-making process will provide confidence in a better diagnosis and prognosis.”
While the current study was specifically about patients with a particular type of heart disease, Dr. Popescu says his algorithm can also be trained to assess other health conditions.
So when might you see this being used outside of a research study? Dr. Trayanova predicts 3D imaging of heart models could be available in 2 years, but first the technique must be tested in more clinical trials – some of which are happening right now.
Adding AI to the heart models will require more studies and Food and Drug Administration approval, so the timeline is less clear. But perhaps the biggest hurdle is that after approval the technologies would need to be adopted and used by clinicians and caregivers.
“The much harder question to answer is, ‘When will doctors be perfectly comfortable with AI tools?’ And I don’t know the answer,” Dr. Popescu says. “How to use AI as an aid in the decision-making process is something that’s not currently taught.”
A version of this article first appeared on WebMD.com.
Deaths from COVID-19 may have caught more attention lately, but heart disease remains the leading cause of death in the United States.
More than 300,000 Americans will die this year of sudden cardiac arrest (also called sudden cardiac death, or SCD), when the heart abruptly stops working.
These events happen suddenly and often without warning, making them nearly impossible to predict. But that may be changing, thanks to 3D imaging and artificial intelligence (AI) technology under study at Johns Hopkins University, Baltimore.
There, researchers are working to create more accurate and personalized models of the heart – and not just any heart, your heart, if you have heart disease.
“Right now, a clinician can only say whether a patient is at risk or not at risk for sudden death,” says Dan Popescu, PhD, a Johns Hopkins research scientist and first author of a new study on AI’s ability to predict sudden cardiac arrest. “With this new technology, you can have much more nuanced predictions of probability of an event over time.”
Put another way: With AI, clinicians may be able not only to predict if someone is at risk for sudden cardiac arrest, but also when it is most likely to happen. They can do this using a much clearer and more personalized look at the electrical “wiring” of your heart.
Your heart, the conductor
Your heart isn’t just a metronome responsible for keeping a steady stream of blood pumping to tissues with every beat. It’s also a conductor through which vital energy flows.
To make the heart beat, electrical impulses flow from the top to the bottom of the organ. Healthy heart cells relay this electricity seamlessly. But in a heart damaged by inflammation or a past heart attack, scar tissue will block the energy flow.
When an electrical impulse encounters a scarred area, the signal can become erratic, disrupting the set top-to-bottom path and causing irregular heartbeats (arrhythmias), which increase someone’s danger of sudden cardiac death.
Seeing the heart in 3D
Today’s tests offer some insights into the heart’s makeup. For example, MRI scans can reveal damaged areas. PET scans can show inflammation. And EKGs can record the heart’s electrical signals from beat to beat.
But all these technologies offer only a snapshot, showing heart health at a moment in time. They can’t predict the future. That’s why scientists at Johns Hopkins are going further to develop 3D digital replicas of a person’s heart, known as computational heart models.
Computational models are computer-simulated replicas that combine mathematics, physics, and computer science. These models have been around for a long time and are used in many fields, ranging from manufacturing to economics.
In heart medicine, these models are populated with digital “cells,” which imitate living cells and can be programmed with different electrical properties, depending on whether they are healthy or diseased.
“Currently available imaging and testing (MRIs, PETs, EKGs) give some representation of the scarring, but you cannot translate that to what is going to happen over time,” says Natalia Trayanova, PhD, of the Johns Hopkins department of biomedical engineering.
“With computational heart models, we create a dynamic digital image of the heart. We can then give the digital image an electrical stimulus and assess how the heart is able to respond. Then you can better predict what is going to happen.”
The computerized 3D models also mean better, more accurate treatment for heart conditions.
For example, a common treatment for a type of arrhythmia known as atrial fibrillation is ablation, or burning some heart tissue. Ablation stops the erratic electrical impulses causing the arrhythmia, but it can also damage otherwise healthy heart cells.
A personalized computational heart model could allow doctors to see more accurately what areas should and shouldn’t be treated for a specific patient.
Using deep learning AI to predict health outcomes
Dr. Trayanova’s colleague Dr. Popescu is applying deep learning and AI to do more with computerized heart models to predict the future.
In a recent paper in Nature Cardiovascular Research, the research team showed their algorithm assessed the health of 269 patients and was able to predict the chance of sudden cardiac arrest up to 10 years in advance.
“This is really the first time ever, as far as we know, where deep learning technology has been proven to analyze scarring of the heart in a successful way,” Dr. Popescu says.
Dr. Popescu and Dr. Trayanova say the AI algorithm gathers information from the 3D computational heart models with patient data like MRIs, ethnicity, age, lifestyle, and other clinical information. Analyzing all these data can produce accurate and consistent estimates about how long patients might live if they are at risk for sudden death.
“You can’t afford to be wrong. If you are wrong, you can actually impact a patient’s quality of life dramatically,” Dr. Popescu says. “Having clinicians use this technology in the decision-making process will provide confidence in a better diagnosis and prognosis.”
While the current study was specifically about patients with a particular type of heart disease, Dr. Popescu says his algorithm can also be trained to assess other health conditions.
So when might you see this being used outside of a research study? Dr. Trayanova predicts 3D imaging of heart models could be available in 2 years, but first the technique must be tested in more clinical trials – some of which are happening right now.
Adding AI to the heart models will require more studies and Food and Drug Administration approval, so the timeline is less clear. But perhaps the biggest hurdle is that after approval the technologies would need to be adopted and used by clinicians and caregivers.
“The much harder question to answer is, ‘When will doctors be perfectly comfortable with AI tools?’ And I don’t know the answer,” Dr. Popescu says. “How to use AI as an aid in the decision-making process is something that’s not currently taught.”
A version of this article first appeared on WebMD.com.
Deaths from COVID-19 may have caught more attention lately, but heart disease remains the leading cause of death in the United States.
More than 300,000 Americans will die this year of sudden cardiac arrest (also called sudden cardiac death, or SCD), when the heart abruptly stops working.
These events happen suddenly and often without warning, making them nearly impossible to predict. But that may be changing, thanks to 3D imaging and artificial intelligence (AI) technology under study at Johns Hopkins University, Baltimore.
There, researchers are working to create more accurate and personalized models of the heart – and not just any heart, your heart, if you have heart disease.
“Right now, a clinician can only say whether a patient is at risk or not at risk for sudden death,” says Dan Popescu, PhD, a Johns Hopkins research scientist and first author of a new study on AI’s ability to predict sudden cardiac arrest. “With this new technology, you can have much more nuanced predictions of probability of an event over time.”
Put another way: With AI, clinicians may be able not only to predict if someone is at risk for sudden cardiac arrest, but also when it is most likely to happen. They can do this using a much clearer and more personalized look at the electrical “wiring” of your heart.
Your heart, the conductor
Your heart isn’t just a metronome responsible for keeping a steady stream of blood pumping to tissues with every beat. It’s also a conductor through which vital energy flows.
To make the heart beat, electrical impulses flow from the top to the bottom of the organ. Healthy heart cells relay this electricity seamlessly. But in a heart damaged by inflammation or a past heart attack, scar tissue will block the energy flow.
When an electrical impulse encounters a scarred area, the signal can become erratic, disrupting the set top-to-bottom path and causing irregular heartbeats (arrhythmias), which increase someone’s danger of sudden cardiac death.
Seeing the heart in 3D
Today’s tests offer some insights into the heart’s makeup. For example, MRI scans can reveal damaged areas. PET scans can show inflammation. And EKGs can record the heart’s electrical signals from beat to beat.
But all these technologies offer only a snapshot, showing heart health at a moment in time. They can’t predict the future. That’s why scientists at Johns Hopkins are going further to develop 3D digital replicas of a person’s heart, known as computational heart models.
Computational models are computer-simulated replicas that combine mathematics, physics, and computer science. These models have been around for a long time and are used in many fields, ranging from manufacturing to economics.
In heart medicine, these models are populated with digital “cells,” which imitate living cells and can be programmed with different electrical properties, depending on whether they are healthy or diseased.
“Currently available imaging and testing (MRIs, PETs, EKGs) give some representation of the scarring, but you cannot translate that to what is going to happen over time,” says Natalia Trayanova, PhD, of the Johns Hopkins department of biomedical engineering.
“With computational heart models, we create a dynamic digital image of the heart. We can then give the digital image an electrical stimulus and assess how the heart is able to respond. Then you can better predict what is going to happen.”
The computerized 3D models also mean better, more accurate treatment for heart conditions.
For example, a common treatment for a type of arrhythmia known as atrial fibrillation is ablation, or burning some heart tissue. Ablation stops the erratic electrical impulses causing the arrhythmia, but it can also damage otherwise healthy heart cells.
A personalized computational heart model could allow doctors to see more accurately what areas should and shouldn’t be treated for a specific patient.
Using deep learning AI to predict health outcomes
Dr. Trayanova’s colleague Dr. Popescu is applying deep learning and AI to do more with computerized heart models to predict the future.
In a recent paper in Nature Cardiovascular Research, the research team showed their algorithm assessed the health of 269 patients and was able to predict the chance of sudden cardiac arrest up to 10 years in advance.
“This is really the first time ever, as far as we know, where deep learning technology has been proven to analyze scarring of the heart in a successful way,” Dr. Popescu says.
Dr. Popescu and Dr. Trayanova say the AI algorithm gathers information from the 3D computational heart models with patient data like MRIs, ethnicity, age, lifestyle, and other clinical information. Analyzing all these data can produce accurate and consistent estimates about how long patients might live if they are at risk for sudden death.
“You can’t afford to be wrong. If you are wrong, you can actually impact a patient’s quality of life dramatically,” Dr. Popescu says. “Having clinicians use this technology in the decision-making process will provide confidence in a better diagnosis and prognosis.”
While the current study was specifically about patients with a particular type of heart disease, Dr. Popescu says his algorithm can also be trained to assess other health conditions.
So when might you see this being used outside of a research study? Dr. Trayanova predicts 3D imaging of heart models could be available in 2 years, but first the technique must be tested in more clinical trials – some of which are happening right now.
Adding AI to the heart models will require more studies and Food and Drug Administration approval, so the timeline is less clear. But perhaps the biggest hurdle is that after approval the technologies would need to be adopted and used by clinicians and caregivers.
“The much harder question to answer is, ‘When will doctors be perfectly comfortable with AI tools?’ And I don’t know the answer,” Dr. Popescu says. “How to use AI as an aid in the decision-making process is something that’s not currently taught.”
A version of this article first appeared on WebMD.com.
Children and COVID: Weekly cases rise again, but more slowly
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.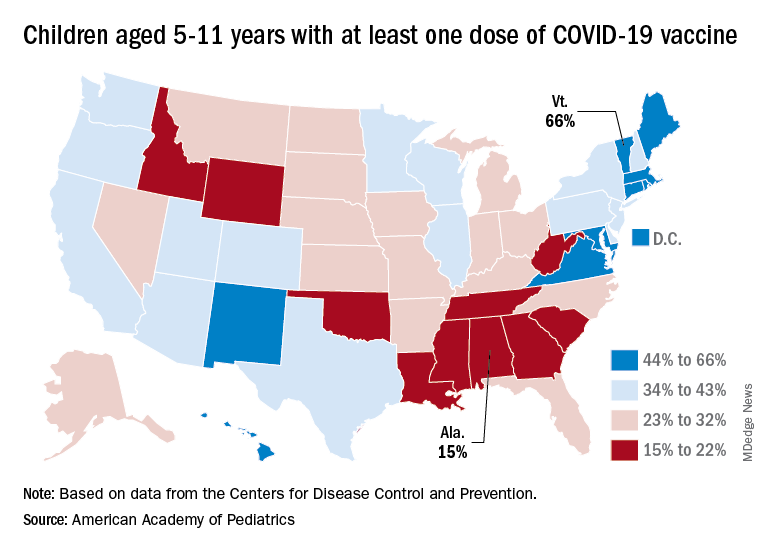
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
Experts decry CDC’s long pause on neglected tropical disease testing
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Internet intervention improved insomnia in Black women
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”

“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”
“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”
“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
FROM JAMA PSYCHIATRY
Are free lunches back? Docs start seeing drug reps again
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
The Empire strikes out against one physician’s homemade star fighter
The force is with Ukraine, always
Of all the things we could want from Star Wars, a lightsaber is at the top of the list. And someone is working on that. But second is probably the iconic X-wing. It was used to blow up the Death Star after all: Who wouldn’t want one?
A real-life star fighter may be outside our technological capabilities, but Dr. Akaki Lekiachvili of Atlanta has done the next best thing and constructed a two-thirds scale model to encourage kids to enter the sciences and, with the advent of the war in Ukraine, raise money for medical supplies to assist doctors in the embattled country. Perhaps unsurprisingly, Dr. Lekiachvili, originally from Georgia (the country, former Soviet republic, and previous target of Russian aggression in 2008), takes a dim view toward the invasion of Ukraine: “Russia is like the Evil Empire and Ukraine the Rebel Alliance.”
It’s been a long road finishing the X-Wing, as Dr. Lekiachvili started the project in 2016 and spent $60,000 on it, posting numerous updates on social media over that time, even attracting the attention of Luke Skywalker himself, actor Mark Hamill. Now that he’s done, he’s brought his model out to the public multiple times, delighting kids and adults alike. It can’t fly, but it has an engine and wheels so it can move, the wings can lock into attack position, the thrusters light up, and the voices of Obi-Wan Kenobi and R2-D2 guide children along as they sit in the cockpit.
Dr. Lekiachvili hopes to auction off his creation to a collector and donate the proceeds to Ukrainian charities, and we’re sure he’ll receive far more than the $60,000 he spent building his masterpiece. Now, if you’ll excuse us, we’re off to raid our bank accounts. We have a Death Star to destroy.
I’m a doctor, not a hologram
Telemedicine got a big boost during the early phase of the pandemic when hospitals and medical offices were off limits to anyone without COVID-19, but things have cooled off, telemedically speaking, since then. Well, NASA may have heated them up again. Or maybe it was Starfleet. Hmm, wait a second while we check. … No, it was NASA.

The space agency used the Microsoft Hololens Kinect camera and a personal computer with custom software from Aexa Aerospace to “holoport” NASA flight surgeon Josef Schmid up to the International Space Station, where he had a conversation with European Space Agency astronaut Thomas Pesquet, who wore an augmented reality headset that allowed him to see, hear, and interact with a 3D representation of the earthbound medical provider.
“Holoportation has been in use since at least 2016 by Microsoft, but this is the first use in such an extreme and remote environment such as space,” NASA said in a recent written statement, noting that the extreme house call took place on Oct. 8, 2021.
They seem to be forgetting about Star Trek, but we’ll let them slide on that one. Anyway, NASA didn’t share any details of the medical holoconversation – which may have strained the limits of HIPAA’s portability provisions – but Dr. Schmid described it as “a brand-new way of human exploration, where our human entity is able to travel off the planet. Our physical body is not there, but our human entity absolutely is there.”
Boldly doctoring where no doctor has gone before, you might say. You also might notice from the photo that Dr. Schmid went full Trekkie with a genuine Vulcan salute. Live long and prosper, Dr. Schmid. Live long and prosper.
Add electricity for umami
Salt makes everything taste better. Unfortunately, excess salt can cause problems for our bodies down the line, starting with high blood pressure and continuing on to heart disease and strokes. So how do we enjoy our deliciously salty foods without putting ourselves at risk? One answer may be electricity.

Researchers at Meiji University in Tokyo partnered with food and beverage maker Kirin to develop a set of electric chopsticks to boost the taste of salt in foods without the extra sodium. According to codeveloper and Meiji University professor Homei Miyashita, the device, worn like a watch with a wire attached to one of the chopsticks, “uses a weak electrical current to transmit sodium ions from food, through the chopsticks, to the mouth where they create a sense of saltines,” Reuters said.
In a country like Japan, where a lot of food is made with heavily sodium-based ingredients like miso and soy sauce, the average adult consumes 10 g of salt a day. That’s twice the recommended amount proposed by the World Health Organization. To not sacrifice bland food for better health, this device, which enhances the saltiness of the food consumed by 1.5 times, offers a fairly easy solution to a big public health crisis.
The chopsticks were tested by giving participants reduced-sodium miso soup. They told the researchers that the food was improved in “richness, sweetness, and overall tastiness,” the Guardian said.
Worried about having something electric in your mouth? Don’t worry. Kirin said in a statement that the electricity is very weak and not enough to affect the body.
The chopsticks are still in a prototype stage, but you may be able to get your pair as soon as next year. Until then, maybe be a little mindful of the salt.
Pet poop works in mysterious ways
We usually see it as a burden when our pets poop and pee in the house, but those bodily excretions may be able to tell us something about cancer-causing toxins running rampant in our homes.

Those toxins, known as aromatic amines, can be found in tobacco smoke and dyes used in make-up, textiles, and plastics. “Our findings suggest that pets are coming into contact with aromatic amines that leach from products in their household environment,” lead author Sridhar Chinthakindi, PhD, of NYU Langone Health, said in a statement from the university. “As these substances have been tied to bladder, colorectal, and other forms of cancer, our results may help explain why so many dogs and cats develop such diseases.”
Tobacco smoke was not the main source of the aromatic amines found in the poop and urine, but 70% of dogs and 80% of cats had these chemicals in their waste. The researchers looked for 30 types of aromatic amines plus nicotine in the sample and found 8. The chemical concentrations were much higher in cats than in dogs, possibly because of differences in exposure and metabolism between the two species, they suggested.
“If [pets] are getting exposed to toxins in our homes, then we had better take a closer look at our own exposure,” said senior author Kurunthachalam Kannan, PhD, of NYU Langone.
So the next time your pet poops or pees in the house, don’t get mad. Maybe they’re just trying to help you out by supplying some easy-to-collect samples.
The force is with Ukraine, always
Of all the things we could want from Star Wars, a lightsaber is at the top of the list. And someone is working on that. But second is probably the iconic X-wing. It was used to blow up the Death Star after all: Who wouldn’t want one?
A real-life star fighter may be outside our technological capabilities, but Dr. Akaki Lekiachvili of Atlanta has done the next best thing and constructed a two-thirds scale model to encourage kids to enter the sciences and, with the advent of the war in Ukraine, raise money for medical supplies to assist doctors in the embattled country. Perhaps unsurprisingly, Dr. Lekiachvili, originally from Georgia (the country, former Soviet republic, and previous target of Russian aggression in 2008), takes a dim view toward the invasion of Ukraine: “Russia is like the Evil Empire and Ukraine the Rebel Alliance.”
It’s been a long road finishing the X-Wing, as Dr. Lekiachvili started the project in 2016 and spent $60,000 on it, posting numerous updates on social media over that time, even attracting the attention of Luke Skywalker himself, actor Mark Hamill. Now that he’s done, he’s brought his model out to the public multiple times, delighting kids and adults alike. It can’t fly, but it has an engine and wheels so it can move, the wings can lock into attack position, the thrusters light up, and the voices of Obi-Wan Kenobi and R2-D2 guide children along as they sit in the cockpit.
Dr. Lekiachvili hopes to auction off his creation to a collector and donate the proceeds to Ukrainian charities, and we’re sure he’ll receive far more than the $60,000 he spent building his masterpiece. Now, if you’ll excuse us, we’re off to raid our bank accounts. We have a Death Star to destroy.
I’m a doctor, not a hologram
Telemedicine got a big boost during the early phase of the pandemic when hospitals and medical offices were off limits to anyone without COVID-19, but things have cooled off, telemedically speaking, since then. Well, NASA may have heated them up again. Or maybe it was Starfleet. Hmm, wait a second while we check. … No, it was NASA.
The space agency used the Microsoft Hololens Kinect camera and a personal computer with custom software from Aexa Aerospace to “holoport” NASA flight surgeon Josef Schmid up to the International Space Station, where he had a conversation with European Space Agency astronaut Thomas Pesquet, who wore an augmented reality headset that allowed him to see, hear, and interact with a 3D representation of the earthbound medical provider.
“Holoportation has been in use since at least 2016 by Microsoft, but this is the first use in such an extreme and remote environment such as space,” NASA said in a recent written statement, noting that the extreme house call took place on Oct. 8, 2021.
They seem to be forgetting about Star Trek, but we’ll let them slide on that one. Anyway, NASA didn’t share any details of the medical holoconversation – which may have strained the limits of HIPAA’s portability provisions – but Dr. Schmid described it as “a brand-new way of human exploration, where our human entity is able to travel off the planet. Our physical body is not there, but our human entity absolutely is there.”
Boldly doctoring where no doctor has gone before, you might say. You also might notice from the photo that Dr. Schmid went full Trekkie with a genuine Vulcan salute. Live long and prosper, Dr. Schmid. Live long and prosper.
Add electricity for umami
Salt makes everything taste better. Unfortunately, excess salt can cause problems for our bodies down the line, starting with high blood pressure and continuing on to heart disease and strokes. So how do we enjoy our deliciously salty foods without putting ourselves at risk? One answer may be electricity.
Researchers at Meiji University in Tokyo partnered with food and beverage maker Kirin to develop a set of electric chopsticks to boost the taste of salt in foods without the extra sodium. According to codeveloper and Meiji University professor Homei Miyashita, the device, worn like a watch with a wire attached to one of the chopsticks, “uses a weak electrical current to transmit sodium ions from food, through the chopsticks, to the mouth where they create a sense of saltines,” Reuters said.
In a country like Japan, where a lot of food is made with heavily sodium-based ingredients like miso and soy sauce, the average adult consumes 10 g of salt a day. That’s twice the recommended amount proposed by the World Health Organization. To not sacrifice bland food for better health, this device, which enhances the saltiness of the food consumed by 1.5 times, offers a fairly easy solution to a big public health crisis.
The chopsticks were tested by giving participants reduced-sodium miso soup. They told the researchers that the food was improved in “richness, sweetness, and overall tastiness,” the Guardian said.
Worried about having something electric in your mouth? Don’t worry. Kirin said in a statement that the electricity is very weak and not enough to affect the body.
The chopsticks are still in a prototype stage, but you may be able to get your pair as soon as next year. Until then, maybe be a little mindful of the salt.
Pet poop works in mysterious ways
We usually see it as a burden when our pets poop and pee in the house, but those bodily excretions may be able to tell us something about cancer-causing toxins running rampant in our homes.
Those toxins, known as aromatic amines, can be found in tobacco smoke and dyes used in make-up, textiles, and plastics. “Our findings suggest that pets are coming into contact with aromatic amines that leach from products in their household environment,” lead author Sridhar Chinthakindi, PhD, of NYU Langone Health, said in a statement from the university. “As these substances have been tied to bladder, colorectal, and other forms of cancer, our results may help explain why so many dogs and cats develop such diseases.”
Tobacco smoke was not the main source of the aromatic amines found in the poop and urine, but 70% of dogs and 80% of cats had these chemicals in their waste. The researchers looked for 30 types of aromatic amines plus nicotine in the sample and found 8. The chemical concentrations were much higher in cats than in dogs, possibly because of differences in exposure and metabolism between the two species, they suggested.
“If [pets] are getting exposed to toxins in our homes, then we had better take a closer look at our own exposure,” said senior author Kurunthachalam Kannan, PhD, of NYU Langone.
So the next time your pet poops or pees in the house, don’t get mad. Maybe they’re just trying to help you out by supplying some easy-to-collect samples.
The force is with Ukraine, always
Of all the things we could want from Star Wars, a lightsaber is at the top of the list. And someone is working on that. But second is probably the iconic X-wing. It was used to blow up the Death Star after all: Who wouldn’t want one?
A real-life star fighter may be outside our technological capabilities, but Dr. Akaki Lekiachvili of Atlanta has done the next best thing and constructed a two-thirds scale model to encourage kids to enter the sciences and, with the advent of the war in Ukraine, raise money for medical supplies to assist doctors in the embattled country. Perhaps unsurprisingly, Dr. Lekiachvili, originally from Georgia (the country, former Soviet republic, and previous target of Russian aggression in 2008), takes a dim view toward the invasion of Ukraine: “Russia is like the Evil Empire and Ukraine the Rebel Alliance.”
It’s been a long road finishing the X-Wing, as Dr. Lekiachvili started the project in 2016 and spent $60,000 on it, posting numerous updates on social media over that time, even attracting the attention of Luke Skywalker himself, actor Mark Hamill. Now that he’s done, he’s brought his model out to the public multiple times, delighting kids and adults alike. It can’t fly, but it has an engine and wheels so it can move, the wings can lock into attack position, the thrusters light up, and the voices of Obi-Wan Kenobi and R2-D2 guide children along as they sit in the cockpit.
Dr. Lekiachvili hopes to auction off his creation to a collector and donate the proceeds to Ukrainian charities, and we’re sure he’ll receive far more than the $60,000 he spent building his masterpiece. Now, if you’ll excuse us, we’re off to raid our bank accounts. We have a Death Star to destroy.
I’m a doctor, not a hologram
Telemedicine got a big boost during the early phase of the pandemic when hospitals and medical offices were off limits to anyone without COVID-19, but things have cooled off, telemedically speaking, since then. Well, NASA may have heated them up again. Or maybe it was Starfleet. Hmm, wait a second while we check. … No, it was NASA.
The space agency used the Microsoft Hololens Kinect camera and a personal computer with custom software from Aexa Aerospace to “holoport” NASA flight surgeon Josef Schmid up to the International Space Station, where he had a conversation with European Space Agency astronaut Thomas Pesquet, who wore an augmented reality headset that allowed him to see, hear, and interact with a 3D representation of the earthbound medical provider.
“Holoportation has been in use since at least 2016 by Microsoft, but this is the first use in such an extreme and remote environment such as space,” NASA said in a recent written statement, noting that the extreme house call took place on Oct. 8, 2021.
They seem to be forgetting about Star Trek, but we’ll let them slide on that one. Anyway, NASA didn’t share any details of the medical holoconversation – which may have strained the limits of HIPAA’s portability provisions – but Dr. Schmid described it as “a brand-new way of human exploration, where our human entity is able to travel off the planet. Our physical body is not there, but our human entity absolutely is there.”
Boldly doctoring where no doctor has gone before, you might say. You also might notice from the photo that Dr. Schmid went full Trekkie with a genuine Vulcan salute. Live long and prosper, Dr. Schmid. Live long and prosper.
Add electricity for umami
Salt makes everything taste better. Unfortunately, excess salt can cause problems for our bodies down the line, starting with high blood pressure and continuing on to heart disease and strokes. So how do we enjoy our deliciously salty foods without putting ourselves at risk? One answer may be electricity.
Researchers at Meiji University in Tokyo partnered with food and beverage maker Kirin to develop a set of electric chopsticks to boost the taste of salt in foods without the extra sodium. According to codeveloper and Meiji University professor Homei Miyashita, the device, worn like a watch with a wire attached to one of the chopsticks, “uses a weak electrical current to transmit sodium ions from food, through the chopsticks, to the mouth where they create a sense of saltines,” Reuters said.
In a country like Japan, where a lot of food is made with heavily sodium-based ingredients like miso and soy sauce, the average adult consumes 10 g of salt a day. That’s twice the recommended amount proposed by the World Health Organization. To not sacrifice bland food for better health, this device, which enhances the saltiness of the food consumed by 1.5 times, offers a fairly easy solution to a big public health crisis.
The chopsticks were tested by giving participants reduced-sodium miso soup. They told the researchers that the food was improved in “richness, sweetness, and overall tastiness,” the Guardian said.
Worried about having something electric in your mouth? Don’t worry. Kirin said in a statement that the electricity is very weak and not enough to affect the body.
The chopsticks are still in a prototype stage, but you may be able to get your pair as soon as next year. Until then, maybe be a little mindful of the salt.
Pet poop works in mysterious ways
We usually see it as a burden when our pets poop and pee in the house, but those bodily excretions may be able to tell us something about cancer-causing toxins running rampant in our homes.
Those toxins, known as aromatic amines, can be found in tobacco smoke and dyes used in make-up, textiles, and plastics. “Our findings suggest that pets are coming into contact with aromatic amines that leach from products in their household environment,” lead author Sridhar Chinthakindi, PhD, of NYU Langone Health, said in a statement from the university. “As these substances have been tied to bladder, colorectal, and other forms of cancer, our results may help explain why so many dogs and cats develop such diseases.”
Tobacco smoke was not the main source of the aromatic amines found in the poop and urine, but 70% of dogs and 80% of cats had these chemicals in their waste. The researchers looked for 30 types of aromatic amines plus nicotine in the sample and found 8. The chemical concentrations were much higher in cats than in dogs, possibly because of differences in exposure and metabolism between the two species, they suggested.
“If [pets] are getting exposed to toxins in our homes, then we had better take a closer look at our own exposure,” said senior author Kurunthachalam Kannan, PhD, of NYU Langone.
So the next time your pet poops or pees in the house, don’t get mad. Maybe they’re just trying to help you out by supplying some easy-to-collect samples.
Study: Fasting plus calorie counting offered no weight-loss benefit over calorie counting alone
Not so fast!
Over the course of a year, study participants who ate only from 8:00 a.m. to 4:00 p.m. did not lose significantly more weight than individuals who ate whenever they wanted, nor did they achieve significantly greater improvements in other obesity-related health measures like body mass index (BMI) or metabolic risk, reported lead author Deying Liu, MD, of Nanfang Hospital, Southern Medical University, Guangzhou, China, and colleagues.
“[Daily fasting] has gained popularity because it is a weight-loss strategy that is simple to follow, which may enhance adherence,” Dr. Liu and colleagues wrote in the New England Journal of Medicine. However, “the long-term efficacy and safety of time-restricted eating as a weight-loss strategy are still uncertain, and the long-term effects on weight loss of time-restricted eating as compared with daily calorie restriction alone have not been fully explored.”
To learn more, Dr. Liu and colleagues recruited 139 adult patients with BMIs between 28 and 45. Individuals with serious medical conditions, such as malignant tumors, diabetes, chronic kidney disease, and others were excluded. Other exclusion criteria included smoking, ongoing participation in a weight-loss program, GI surgery within the prior year, use of medications that impact energy balance and weight, and planned or current pregnancy.
All participants were advised to eat calorie-restricted diets, with ranges of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women. To determine the added impact of fasting, participants were randomized in a 1:1 ratio into time-restricted (fasting) or non–time-restricted (nonfasting) groups, in which fasting participants ate only during an 8-hour window from 8:00 a.m. to 4:00 p.m., whereas nonfasting participants ate whenever they wanted.
At 6 months and 12 months, participants were re-evaluated for changes in weight, body fat, BMI, blood pressure, lean body mass, and metabolic risk factors, including glucose level, triglycerides, blood pressure, and others.
Caloric intake restriction seems to explain most of beneficial effects
At one-year follow-up, 118 participants (84.9%) remained in the study. Although members of the fasting group lost slightly more weight on average than those in the non-fasting group (mean, 8.0 kg vs. 6.3 kg), the difference between groups was not statistically significant (95% confidence interval, −4.0 to 0.4; P = .11).
Most of the other obesity-related health measures also trended toward favoring the fasting group, but again, none of these improvements was statistically significant. Weight circumference at 1 year, for example, decreased by a mean of 9.4 cm in the fasting group versus 8.8 cm in the nonfasting group, a net difference of 1.8 cm (95% CI, –4.0 to 0.5).
“We found that the two weight-loss regimens that we evaluated had similar success in patients with obesity, regardless of whether they reduced their calorie consumption through time-restricted eating or through calorie restriction alone,” Dr. Liu and colleagues concluded.
Principal investigator Huijie Zhang MD, PhD, professor, chief physician, and deputy director of the department of endocrinology and metabolism at Nafang Hospital, noted that their findings are “consistent with the findings in previous studies.”
“Our data suggest that caloric intake restriction explained most of the beneficial effects of a time-restricted eating regimen,” Dr. Zhang said.
Still, Dr. Zhang called time-restricted eating “a viable and sustainable approach for a person who wants to lose weight.”
More work is needed, Dr. Zhang said, to uncover the impact of fasting in “diverse groups,” including patients with chronic disease like diabetes and cardiovascular disease. Investigators should also conduct studies to compare outcomes between men and women, and evaluate the effects of other fasting durations.
Can trial be applied to a wider population?
According to Blandine Laferrère, MD, PhD, and Satchidananda Panda, PhD, of Columbia University Irving Medical Center, New York, and the Salk Institute for Biological Studies, La Jolla, Calif., respectively, “the results of the trial suggest that calorie restriction combined with time restriction, when delivered with intensive coaching and monitoring, is an approach that is as safe, sustainable, and effective for weight loss as calorie restriction alone.”
Yet Dr. Laferrère and Dr. Panda also expressed skepticism about broader implementation of a similar regime.
“The applicability of this trial to wider populations is debatable,” they wrote in an accompanying editorial. “The short time period for eating at baseline may be specific to the population studied, since investigators outside China have reported longer time windows. The rigorous coaching and monitoring by trial staff also leaves open the question of whether time-restricted eating is easier to adhere to than intentional calorie restriction. Such cost-benefit analyses are important for the assessment of the scalability of a lifestyle intervention.”
Duration is trial’s greatest strength
Kristina Varady, PhD, professor of nutrition in the department of kinesiology and nutrition at the University of Illinois at Chicago, said the “key strength” of the trial was its duration, at 12 months, making it the longest time-restricted eating trial to date”; however, she was critical of the design.
“Quite frankly, I’m surprised this study got into such a high-caliber medical journal,” Dr. Varady said in a written comment. “It doesn’t even have a control group! It goes to show how popular these diets are and how much people want to know about them.”
She also noted that “the study was flawed in that it didn’t really look at the effects of true time-restricted eating.” According to Dr. Varady, combining calorie restriction with time-restricted eating “kind of defeats the purpose” of a time-restricted diet.
“The main benefit of time-restricted eating is that you don’t need to count calories in order to lose weight,” Dr. Varady said, citing two of her own studies from 2018 and 2020. “Just by limiting the eating window to 8 hours per day, people naturally cut out 300-500 calories per day. That’s why people like [time-restricted eating] so much.”
Dr. Varady was also “very surprised” at the adherence data. At 1 year, approximately 85% of the patients were still following the protocol, a notably higher rate than most dietary intervention studies, which typically report adherence rates of 50-60%, she said. The high adherence rate was particularly unexpected because of the 8:00 a.m.–4:00 p.m. eating window, Dr. Varady added, since that meant skipping “the family/social meal every evening over 1 whole year!”
The study was funded by the National Key Research and Development Project and others. The study investigators reported no conflicts of interest. Dr. Varady disclosed author fees from the Hachette Book group for her book “The Every Other Day Diet.”
Not so fast!
Over the course of a year, study participants who ate only from 8:00 a.m. to 4:00 p.m. did not lose significantly more weight than individuals who ate whenever they wanted, nor did they achieve significantly greater improvements in other obesity-related health measures like body mass index (BMI) or metabolic risk, reported lead author Deying Liu, MD, of Nanfang Hospital, Southern Medical University, Guangzhou, China, and colleagues.
“[Daily fasting] has gained popularity because it is a weight-loss strategy that is simple to follow, which may enhance adherence,” Dr. Liu and colleagues wrote in the New England Journal of Medicine. However, “the long-term efficacy and safety of time-restricted eating as a weight-loss strategy are still uncertain, and the long-term effects on weight loss of time-restricted eating as compared with daily calorie restriction alone have not been fully explored.”
To learn more, Dr. Liu and colleagues recruited 139 adult patients with BMIs between 28 and 45. Individuals with serious medical conditions, such as malignant tumors, diabetes, chronic kidney disease, and others were excluded. Other exclusion criteria included smoking, ongoing participation in a weight-loss program, GI surgery within the prior year, use of medications that impact energy balance and weight, and planned or current pregnancy.
All participants were advised to eat calorie-restricted diets, with ranges of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women. To determine the added impact of fasting, participants were randomized in a 1:1 ratio into time-restricted (fasting) or non–time-restricted (nonfasting) groups, in which fasting participants ate only during an 8-hour window from 8:00 a.m. to 4:00 p.m., whereas nonfasting participants ate whenever they wanted.
At 6 months and 12 months, participants were re-evaluated for changes in weight, body fat, BMI, blood pressure, lean body mass, and metabolic risk factors, including glucose level, triglycerides, blood pressure, and others.
Caloric intake restriction seems to explain most of beneficial effects
At one-year follow-up, 118 participants (84.9%) remained in the study. Although members of the fasting group lost slightly more weight on average than those in the non-fasting group (mean, 8.0 kg vs. 6.3 kg), the difference between groups was not statistically significant (95% confidence interval, −4.0 to 0.4; P = .11).
Most of the other obesity-related health measures also trended toward favoring the fasting group, but again, none of these improvements was statistically significant. Weight circumference at 1 year, for example, decreased by a mean of 9.4 cm in the fasting group versus 8.8 cm in the nonfasting group, a net difference of 1.8 cm (95% CI, –4.0 to 0.5).
“We found that the two weight-loss regimens that we evaluated had similar success in patients with obesity, regardless of whether they reduced their calorie consumption through time-restricted eating or through calorie restriction alone,” Dr. Liu and colleagues concluded.
Principal investigator Huijie Zhang MD, PhD, professor, chief physician, and deputy director of the department of endocrinology and metabolism at Nafang Hospital, noted that their findings are “consistent with the findings in previous studies.”
“Our data suggest that caloric intake restriction explained most of the beneficial effects of a time-restricted eating regimen,” Dr. Zhang said.
Still, Dr. Zhang called time-restricted eating “a viable and sustainable approach for a person who wants to lose weight.”
More work is needed, Dr. Zhang said, to uncover the impact of fasting in “diverse groups,” including patients with chronic disease like diabetes and cardiovascular disease. Investigators should also conduct studies to compare outcomes between men and women, and evaluate the effects of other fasting durations.
Can trial be applied to a wider population?
According to Blandine Laferrère, MD, PhD, and Satchidananda Panda, PhD, of Columbia University Irving Medical Center, New York, and the Salk Institute for Biological Studies, La Jolla, Calif., respectively, “the results of the trial suggest that calorie restriction combined with time restriction, when delivered with intensive coaching and monitoring, is an approach that is as safe, sustainable, and effective for weight loss as calorie restriction alone.”
Yet Dr. Laferrère and Dr. Panda also expressed skepticism about broader implementation of a similar regime.
“The applicability of this trial to wider populations is debatable,” they wrote in an accompanying editorial. “The short time period for eating at baseline may be specific to the population studied, since investigators outside China have reported longer time windows. The rigorous coaching and monitoring by trial staff also leaves open the question of whether time-restricted eating is easier to adhere to than intentional calorie restriction. Such cost-benefit analyses are important for the assessment of the scalability of a lifestyle intervention.”
Duration is trial’s greatest strength
Kristina Varady, PhD, professor of nutrition in the department of kinesiology and nutrition at the University of Illinois at Chicago, said the “key strength” of the trial was its duration, at 12 months, making it the longest time-restricted eating trial to date”; however, she was critical of the design.
“Quite frankly, I’m surprised this study got into such a high-caliber medical journal,” Dr. Varady said in a written comment. “It doesn’t even have a control group! It goes to show how popular these diets are and how much people want to know about them.”
She also noted that “the study was flawed in that it didn’t really look at the effects of true time-restricted eating.” According to Dr. Varady, combining calorie restriction with time-restricted eating “kind of defeats the purpose” of a time-restricted diet.
“The main benefit of time-restricted eating is that you don’t need to count calories in order to lose weight,” Dr. Varady said, citing two of her own studies from 2018 and 2020. “Just by limiting the eating window to 8 hours per day, people naturally cut out 300-500 calories per day. That’s why people like [time-restricted eating] so much.”
Dr. Varady was also “very surprised” at the adherence data. At 1 year, approximately 85% of the patients were still following the protocol, a notably higher rate than most dietary intervention studies, which typically report adherence rates of 50-60%, she said. The high adherence rate was particularly unexpected because of the 8:00 a.m.–4:00 p.m. eating window, Dr. Varady added, since that meant skipping “the family/social meal every evening over 1 whole year!”
The study was funded by the National Key Research and Development Project and others. The study investigators reported no conflicts of interest. Dr. Varady disclosed author fees from the Hachette Book group for her book “The Every Other Day Diet.”
Not so fast!
Over the course of a year, study participants who ate only from 8:00 a.m. to 4:00 p.m. did not lose significantly more weight than individuals who ate whenever they wanted, nor did they achieve significantly greater improvements in other obesity-related health measures like body mass index (BMI) or metabolic risk, reported lead author Deying Liu, MD, of Nanfang Hospital, Southern Medical University, Guangzhou, China, and colleagues.
“[Daily fasting] has gained popularity because it is a weight-loss strategy that is simple to follow, which may enhance adherence,” Dr. Liu and colleagues wrote in the New England Journal of Medicine. However, “the long-term efficacy and safety of time-restricted eating as a weight-loss strategy are still uncertain, and the long-term effects on weight loss of time-restricted eating as compared with daily calorie restriction alone have not been fully explored.”
To learn more, Dr. Liu and colleagues recruited 139 adult patients with BMIs between 28 and 45. Individuals with serious medical conditions, such as malignant tumors, diabetes, chronic kidney disease, and others were excluded. Other exclusion criteria included smoking, ongoing participation in a weight-loss program, GI surgery within the prior year, use of medications that impact energy balance and weight, and planned or current pregnancy.
All participants were advised to eat calorie-restricted diets, with ranges of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women. To determine the added impact of fasting, participants were randomized in a 1:1 ratio into time-restricted (fasting) or non–time-restricted (nonfasting) groups, in which fasting participants ate only during an 8-hour window from 8:00 a.m. to 4:00 p.m., whereas nonfasting participants ate whenever they wanted.
At 6 months and 12 months, participants were re-evaluated for changes in weight, body fat, BMI, blood pressure, lean body mass, and metabolic risk factors, including glucose level, triglycerides, blood pressure, and others.
Caloric intake restriction seems to explain most of beneficial effects
At one-year follow-up, 118 participants (84.9%) remained in the study. Although members of the fasting group lost slightly more weight on average than those in the non-fasting group (mean, 8.0 kg vs. 6.3 kg), the difference between groups was not statistically significant (95% confidence interval, −4.0 to 0.4; P = .11).
Most of the other obesity-related health measures also trended toward favoring the fasting group, but again, none of these improvements was statistically significant. Weight circumference at 1 year, for example, decreased by a mean of 9.4 cm in the fasting group versus 8.8 cm in the nonfasting group, a net difference of 1.8 cm (95% CI, –4.0 to 0.5).
“We found that the two weight-loss regimens that we evaluated had similar success in patients with obesity, regardless of whether they reduced their calorie consumption through time-restricted eating or through calorie restriction alone,” Dr. Liu and colleagues concluded.
Principal investigator Huijie Zhang MD, PhD, professor, chief physician, and deputy director of the department of endocrinology and metabolism at Nafang Hospital, noted that their findings are “consistent with the findings in previous studies.”
“Our data suggest that caloric intake restriction explained most of the beneficial effects of a time-restricted eating regimen,” Dr. Zhang said.
Still, Dr. Zhang called time-restricted eating “a viable and sustainable approach for a person who wants to lose weight.”
More work is needed, Dr. Zhang said, to uncover the impact of fasting in “diverse groups,” including patients with chronic disease like diabetes and cardiovascular disease. Investigators should also conduct studies to compare outcomes between men and women, and evaluate the effects of other fasting durations.
Can trial be applied to a wider population?
According to Blandine Laferrère, MD, PhD, and Satchidananda Panda, PhD, of Columbia University Irving Medical Center, New York, and the Salk Institute for Biological Studies, La Jolla, Calif., respectively, “the results of the trial suggest that calorie restriction combined with time restriction, when delivered with intensive coaching and monitoring, is an approach that is as safe, sustainable, and effective for weight loss as calorie restriction alone.”
Yet Dr. Laferrère and Dr. Panda also expressed skepticism about broader implementation of a similar regime.
“The applicability of this trial to wider populations is debatable,” they wrote in an accompanying editorial. “The short time period for eating at baseline may be specific to the population studied, since investigators outside China have reported longer time windows. The rigorous coaching and monitoring by trial staff also leaves open the question of whether time-restricted eating is easier to adhere to than intentional calorie restriction. Such cost-benefit analyses are important for the assessment of the scalability of a lifestyle intervention.”
Duration is trial’s greatest strength
Kristina Varady, PhD, professor of nutrition in the department of kinesiology and nutrition at the University of Illinois at Chicago, said the “key strength” of the trial was its duration, at 12 months, making it the longest time-restricted eating trial to date”; however, she was critical of the design.
“Quite frankly, I’m surprised this study got into such a high-caliber medical journal,” Dr. Varady said in a written comment. “It doesn’t even have a control group! It goes to show how popular these diets are and how much people want to know about them.”
She also noted that “the study was flawed in that it didn’t really look at the effects of true time-restricted eating.” According to Dr. Varady, combining calorie restriction with time-restricted eating “kind of defeats the purpose” of a time-restricted diet.
“The main benefit of time-restricted eating is that you don’t need to count calories in order to lose weight,” Dr. Varady said, citing two of her own studies from 2018 and 2020. “Just by limiting the eating window to 8 hours per day, people naturally cut out 300-500 calories per day. That’s why people like [time-restricted eating] so much.”
Dr. Varady was also “very surprised” at the adherence data. At 1 year, approximately 85% of the patients were still following the protocol, a notably higher rate than most dietary intervention studies, which typically report adherence rates of 50-60%, she said. The high adherence rate was particularly unexpected because of the 8:00 a.m.–4:00 p.m. eating window, Dr. Varady added, since that meant skipping “the family/social meal every evening over 1 whole year!”
The study was funded by the National Key Research and Development Project and others. The study investigators reported no conflicts of interest. Dr. Varady disclosed author fees from the Hachette Book group for her book “The Every Other Day Diet.”
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Cheap and noninvasive: Detecting HPV in sanitary pads
A cell phone rings in a red-brick bungalow in a village in India. A woman on the other end of the phone tells Ms. SK, a community health worker, that menstruation has started. Ms. SK guns her scooter through the dusty streets for 15 minutes in 30° C (86° F) heat.
A 32-year-old woman, waiting in the shade of a blue corrugated-iron roof, hands over a green polythene bag. Ms. SK whisks the package to the local health center and tucks it into a –20° C freezer. The following week, it will ride in dry ice to the National Institute for Research in Reproductive and Child Health Laboratory in Mumbai for human papillomavirus (HPV) testing.
This moment in rural India at first glance appears to have little relevance to wealthy countries such as the United States.
However, public health officials in both countries are trying to solve the same problem: how to prevent unnecessary deaths from cervical cancer by reaching women who have never or rarely been screened.
The United States has more in common with India than it may care to admit.
“In the U.S., we still have pockets of disparities that actually have incidence rates [of cervical cancer] comparable to many low- and middle-income countries,” said Vikrant Sahasrabuddhe, MBBS, DrPh, MPH, of the National Cancer Institute, where he heads the HPV and cervical cancer prevention clinical research program for the National Institutes of Health.
The incidence of cervical cancer in India is approximately 19 per 100,000 women. For the past 15 years incidence in the United States has stalled at approximately 7 per 100,000.
In India, there are no organized screening programs and most cervical cancer is regional or distant metastatic at diagnosis.
In the United States, 52% of new cases are advanced, and half of these are among women who have never or rarely been screened.
“There is a critical need for new strategies to reach this population,” Dr. Sahasrabuddhe said. “We absolutely have to do something out of the box creatively.”
Almost all cervical cancers are triggered by HPV, most commonly high-risk HPV-16 and HPV-18, although there are more than 200 types. HPV testing is taking over from cytology (Papanicolaou test) for secondary prevention of cervical cancer.
The trial of screening for HPV in menstrual pads that is ongoing in India was the brainchild of Atul Budukh, PhD, a government public health researcher and professor at the Centre for Cancer Epidemiology, Tata Memorial Centre, Mumbai.
Dr. Budukh’s eyes were opened to the scale of the problem when he participated in a cluster-randomized trial funded by the Bill and Melinda Gates Foundation. The study, published in 2009 in the New England Journal of Medicine, involved 131,746 rural women in the Osmanabad district of India.
A team of researchers from India and France compared outcomes for women over 8 years after cervical screening by HPV, cytology, or visual inspection with acetic acid. The control group was usual care, where women were advised how to seek screening at local hospitals. Women who screened positive were referred for colposcopy, biopsy, and treatment.
Over the 8-year follow-up, advanced cervical cancer was found in twice as many women left to their own devices, compared with women who had HPV testing during the study (82 vs. 39; hazard ratio for HPV, 0.47; 95% confidence interval, 0.32-0.69).
Similarly, cervical cancer deaths in the control group were nearly two times higher than among the women who were screened for HPV in the study (64 vs. 34; HR for HPV, 0.52; 95% CI, 0.33-0.83).
The study proved that rural Indian women were dying unnecessarily because they weren’t seeking cervical screening. And education wasn’t the problem.
“When we go and educate [a rural woman] about ... risk factors and the need to undergo screening, she understands it very well,” said Dr. Budukh. “She is ready to come but her priority is her bread and butter – she will lose her daily wages.”
Dr. Budukh and his team negotiated with local employers so that women could come to screening clinics, but they soon realized this wasn’t scalable.
One year after the NEJM publication, Dr. Budukh found what he was looking for.
A team of Hong Kong clinicians, headed by Sze Chuen Cesar Wong of the Hong Kong Cancer Institute, published a paper in 2010 in the Journal of Clinical Microbiology showing that menstrual pads provide reliable HPV results in women with and without cervical disease.
The Hong Kong team tested sanitary napkins for HPV from 235 of their patients with cervical intraepithelial neoplasia or condyloma acuminatum before and after treatment. Samples were compared with those from 323 women without cervical disease; for HPV in sanitary napkins the sensitivity was 82.8%, specificity was 93.1%, and positive and negative predictive values were 90% and 87.9%, respectively.
The authors pointed out that menstrual pad testing was the only truly noninvasive approach to HPV screening versus the other self-sampling methods such as tampons and cytobrushes. Also, these self-sampling tests require specialized liquid-based transport media. A menstrual pad needs only a plastic bag.
Dr. Budukh had his at-home solution for the hard-working rural women of India.
With funding from the Indian government, Dr. Budukh’s team put together a validation trial that ran from 2013 to 2016 in 18 rural villages in two separate districts: Ahmednagar and Pune.
Local health workers went house to house to recruit women and get family buy-in for this culturally delicate project. Participants were instructed to use their regular sanitary protection – most commonly a washable cloth – and told to call the health worker on the first day of menstruation. Health workers gave each woman a Ziploc bag for the pad and, for privacy, an outer polythene sac.
In Ahmednagar, all women who provided their pad also got screened with Hybrid Capture 2 (HC2; Qiagen) by a mobile screening unit. In Pune, only the positive cases underwent HC2. Screening was also extended to anyone who requested it, but these people were not included in the final analysis.
Genomic DNA was extracted from three 5 mm–sized punches in the pad using a commercial kit, QIAamp DNA Micro, and the quality and purity of the DNA checked by Implen NanoPhotometer.
The team followed the same protocol for PCR HPV assay as the team from Hong Kong.
The results were published in the European Journal of Cancer Prevention in 2018.
The concordance rate for a positive result between the menstrual pad sample and conventional HPV sampling was 98.8% for Ahmednagar and 95.2% for samples from Pune. The sensitivity for the first study was 83% and the specificity 99% – similar to that for the women in Hong Kong. The second study had lower sensitivity and specificity (67% and 88%), partly because of poor storage as a result of frequent power cuts.
The total cost per woman was $30.78.
“I was very excited when we saw the results,” Dr. Budukh recalled. “That day I couldn’t sleep ... such a wonderful result! I was excited to start the next phase immediately.”
Dr. Budukh has applied to the Indian government for funding for a larger trial involving 3,000 women. If successful, he hopes such evidence would be sufficient to convince the Indian government to make menstrual pad screening standard procedure for the 390 million women who live in India’s countryside.
Testing never-screened women for cervical cancer using menstrual pads appears to be relatively reliable, convenient, private, noninvasive, and incredibly cheap.
So who else has tried it?
The first published account of HPV in menstrual blood was a 2003 study by Tommy Tong and colleagues at the Princess Margaret Hospital in Hong Kong. The authors heralded, with lamentable optimism, “a new paradigm in cervical cancer screening.”
In the following 20 years, just six more studies appeared: two from Dr. Budukh’s field trial in India and four from hospital-based pilot studies in Hong Kong (in 2010 and 2018), South Korea (in 2016), and mainland China (in 2021). All these studies, although small, were published in top-flight journals and demonstrate high concordance between conventional high-risk HPV testing and menstrual-blood tests.
This news organization tried to find a U.S. thought-leader who had heard of the approach.
Elizabeth Fontham, MPH, DrPh, is the founding dean of the school of public health at Louisiana State University Health Center in New Orleans, and president of the American Cancer Society. Dr. Fontham said in an email that she had “no plans to evaluate the impact related to menstrual pads, but perhaps others have looked into that.”
Joy Melnikow, MD, MPH, was first author on the evidence synthesis driving the current cervical cancer screening recommendations from the U.S. Preventive Services Task Force. When asked about menstrual pad testing for HPV, she said she had “not heard of it before.”
The USPSTF guidelines don’t mention sanitary pads but acknowledge that “self-collection may be one strategy for increasing screening rates among populations where they are currently low.”
The USPSTF methodology excludes data from countries that don’t match the United States on the Human Development Index “or [are] not applicable to U.S. clinical settings or populations.” (Presumably, data from Hong Kong and South Korea would qualify; Indian data would not.)
Dr. Sahasrabuddhe of the NCI hadn’t heard of menstrual pad testing either, but he has a different explanation for lack of interest in this approach – or, indeed, any form of self-sampling for cervical cancer screening – in the United States.
“We have not seen movement happen in this space for years. ... If there is one intervention that we can simplify, that still has not been made widely available, it is self-sampling ... [but] we don’t have [Food and Drug Administration] approval for it,” Dr. Sahasrabuddhe said.
“Our system, at least in the U.S., is based on industry manufacturers seeking an approval for a particular way of collection and then clinicians and clinical-guideline bodies signing on. ... For a lot of reasons industry has shied away over the past several years, so far, at least, on seeking approval for self-sampling-based approaches,” he commented.
Dr. Sahasrabuddhe aims to change that. He heads a new NCI-led initiative called “The Last Mile,” a nationwide clinical trial supported by federal agencies, industry partners, and professional societies. The goal is to validate self-sampled HPV testing as non-inferior to specimens collected by providers. The team is currently finalizing the methodology of the study, so Dr. Sahasrabuddhe could not share the self-sampling methods that will be on trial, nor the industry partners who have signed up.
The following tests are approved in the United States for physician-collected HPV screening: Hybrid Capture 2, used in the Indian studies (Qiagen); cobas HPV (Roche); Aptima (Hologic); Cervista (Hologic); and Onclarity (Becton Dickinson).
Dr. Sahasrabuddhe said that, while a sanitary pad in a Ziploc bag is unlikely to make the grade for The Last Mile study, he doesn’t totally dismiss their potential and said the NCI is always open to new ideas.
“We are not supporting anybody specifically for menstrual pad-based collection device development,” Dr. Sahasrabuddhe said, “But if they fulfill other criteria for a small business–based grant application, they absolutely are welcome to apply for NCI funding for this.”
Said Dr. Melnikow: “Pre-COVID, the head of [the World Health Organization] said that we could eliminate cervical cancer from the globe and that we have the tools to do that now. And he’s right.”
Dr. Budukh, Dr. Melnikow, and Dr. Sahasrabuddhe disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A cell phone rings in a red-brick bungalow in a village in India. A woman on the other end of the phone tells Ms. SK, a community health worker, that menstruation has started. Ms. SK guns her scooter through the dusty streets for 15 minutes in 30° C (86° F) heat.
A 32-year-old woman, waiting in the shade of a blue corrugated-iron roof, hands over a green polythene bag. Ms. SK whisks the package to the local health center and tucks it into a –20° C freezer. The following week, it will ride in dry ice to the National Institute for Research in Reproductive and Child Health Laboratory in Mumbai for human papillomavirus (HPV) testing.
This moment in rural India at first glance appears to have little relevance to wealthy countries such as the United States.
However, public health officials in both countries are trying to solve the same problem: how to prevent unnecessary deaths from cervical cancer by reaching women who have never or rarely been screened.
The United States has more in common with India than it may care to admit.
“In the U.S., we still have pockets of disparities that actually have incidence rates [of cervical cancer] comparable to many low- and middle-income countries,” said Vikrant Sahasrabuddhe, MBBS, DrPh, MPH, of the National Cancer Institute, where he heads the HPV and cervical cancer prevention clinical research program for the National Institutes of Health.
The incidence of cervical cancer in India is approximately 19 per 100,000 women. For the past 15 years incidence in the United States has stalled at approximately 7 per 100,000.
In India, there are no organized screening programs and most cervical cancer is regional or distant metastatic at diagnosis.
In the United States, 52% of new cases are advanced, and half of these are among women who have never or rarely been screened.
“There is a critical need for new strategies to reach this population,” Dr. Sahasrabuddhe said. “We absolutely have to do something out of the box creatively.”
Almost all cervical cancers are triggered by HPV, most commonly high-risk HPV-16 and HPV-18, although there are more than 200 types. HPV testing is taking over from cytology (Papanicolaou test) for secondary prevention of cervical cancer.
The trial of screening for HPV in menstrual pads that is ongoing in India was the brainchild of Atul Budukh, PhD, a government public health researcher and professor at the Centre for Cancer Epidemiology, Tata Memorial Centre, Mumbai.
Dr. Budukh’s eyes were opened to the scale of the problem when he participated in a cluster-randomized trial funded by the Bill and Melinda Gates Foundation. The study, published in 2009 in the New England Journal of Medicine, involved 131,746 rural women in the Osmanabad district of India.
A team of researchers from India and France compared outcomes for women over 8 years after cervical screening by HPV, cytology, or visual inspection with acetic acid. The control group was usual care, where women were advised how to seek screening at local hospitals. Women who screened positive were referred for colposcopy, biopsy, and treatment.
Over the 8-year follow-up, advanced cervical cancer was found in twice as many women left to their own devices, compared with women who had HPV testing during the study (82 vs. 39; hazard ratio for HPV, 0.47; 95% confidence interval, 0.32-0.69).
Similarly, cervical cancer deaths in the control group were nearly two times higher than among the women who were screened for HPV in the study (64 vs. 34; HR for HPV, 0.52; 95% CI, 0.33-0.83).
The study proved that rural Indian women were dying unnecessarily because they weren’t seeking cervical screening. And education wasn’t the problem.
“When we go and educate [a rural woman] about ... risk factors and the need to undergo screening, she understands it very well,” said Dr. Budukh. “She is ready to come but her priority is her bread and butter – she will lose her daily wages.”
Dr. Budukh and his team negotiated with local employers so that women could come to screening clinics, but they soon realized this wasn’t scalable.
One year after the NEJM publication, Dr. Budukh found what he was looking for.
A team of Hong Kong clinicians, headed by Sze Chuen Cesar Wong of the Hong Kong Cancer Institute, published a paper in 2010 in the Journal of Clinical Microbiology showing that menstrual pads provide reliable HPV results in women with and without cervical disease.
The Hong Kong team tested sanitary napkins for HPV from 235 of their patients with cervical intraepithelial neoplasia or condyloma acuminatum before and after treatment. Samples were compared with those from 323 women without cervical disease; for HPV in sanitary napkins the sensitivity was 82.8%, specificity was 93.1%, and positive and negative predictive values were 90% and 87.9%, respectively.
The authors pointed out that menstrual pad testing was the only truly noninvasive approach to HPV screening versus the other self-sampling methods such as tampons and cytobrushes. Also, these self-sampling tests require specialized liquid-based transport media. A menstrual pad needs only a plastic bag.
Dr. Budukh had his at-home solution for the hard-working rural women of India.
With funding from the Indian government, Dr. Budukh’s team put together a validation trial that ran from 2013 to 2016 in 18 rural villages in two separate districts: Ahmednagar and Pune.
Local health workers went house to house to recruit women and get family buy-in for this culturally delicate project. Participants were instructed to use their regular sanitary protection – most commonly a washable cloth – and told to call the health worker on the first day of menstruation. Health workers gave each woman a Ziploc bag for the pad and, for privacy, an outer polythene sac.
In Ahmednagar, all women who provided their pad also got screened with Hybrid Capture 2 (HC2; Qiagen) by a mobile screening unit. In Pune, only the positive cases underwent HC2. Screening was also extended to anyone who requested it, but these people were not included in the final analysis.
Genomic DNA was extracted from three 5 mm–sized punches in the pad using a commercial kit, QIAamp DNA Micro, and the quality and purity of the DNA checked by Implen NanoPhotometer.
The team followed the same protocol for PCR HPV assay as the team from Hong Kong.
The results were published in the European Journal of Cancer Prevention in 2018.
The concordance rate for a positive result between the menstrual pad sample and conventional HPV sampling was 98.8% for Ahmednagar and 95.2% for samples from Pune. The sensitivity for the first study was 83% and the specificity 99% – similar to that for the women in Hong Kong. The second study had lower sensitivity and specificity (67% and 88%), partly because of poor storage as a result of frequent power cuts.
The total cost per woman was $30.78.
“I was very excited when we saw the results,” Dr. Budukh recalled. “That day I couldn’t sleep ... such a wonderful result! I was excited to start the next phase immediately.”
Dr. Budukh has applied to the Indian government for funding for a larger trial involving 3,000 women. If successful, he hopes such evidence would be sufficient to convince the Indian government to make menstrual pad screening standard procedure for the 390 million women who live in India’s countryside.
Testing never-screened women for cervical cancer using menstrual pads appears to be relatively reliable, convenient, private, noninvasive, and incredibly cheap.
So who else has tried it?
The first published account of HPV in menstrual blood was a 2003 study by Tommy Tong and colleagues at the Princess Margaret Hospital in Hong Kong. The authors heralded, with lamentable optimism, “a new paradigm in cervical cancer screening.”
In the following 20 years, just six more studies appeared: two from Dr. Budukh’s field trial in India and four from hospital-based pilot studies in Hong Kong (in 2010 and 2018), South Korea (in 2016), and mainland China (in 2021). All these studies, although small, were published in top-flight journals and demonstrate high concordance between conventional high-risk HPV testing and menstrual-blood tests.
This news organization tried to find a U.S. thought-leader who had heard of the approach.
Elizabeth Fontham, MPH, DrPh, is the founding dean of the school of public health at Louisiana State University Health Center in New Orleans, and president of the American Cancer Society. Dr. Fontham said in an email that she had “no plans to evaluate the impact related to menstrual pads, but perhaps others have looked into that.”
Joy Melnikow, MD, MPH, was first author on the evidence synthesis driving the current cervical cancer screening recommendations from the U.S. Preventive Services Task Force. When asked about menstrual pad testing for HPV, she said she had “not heard of it before.”
The USPSTF guidelines don’t mention sanitary pads but acknowledge that “self-collection may be one strategy for increasing screening rates among populations where they are currently low.”
The USPSTF methodology excludes data from countries that don’t match the United States on the Human Development Index “or [are] not applicable to U.S. clinical settings or populations.” (Presumably, data from Hong Kong and South Korea would qualify; Indian data would not.)
Dr. Sahasrabuddhe of the NCI hadn’t heard of menstrual pad testing either, but he has a different explanation for lack of interest in this approach – or, indeed, any form of self-sampling for cervical cancer screening – in the United States.
“We have not seen movement happen in this space for years. ... If there is one intervention that we can simplify, that still has not been made widely available, it is self-sampling ... [but] we don’t have [Food and Drug Administration] approval for it,” Dr. Sahasrabuddhe said.
“Our system, at least in the U.S., is based on industry manufacturers seeking an approval for a particular way of collection and then clinicians and clinical-guideline bodies signing on. ... For a lot of reasons industry has shied away over the past several years, so far, at least, on seeking approval for self-sampling-based approaches,” he commented.
Dr. Sahasrabuddhe aims to change that. He heads a new NCI-led initiative called “The Last Mile,” a nationwide clinical trial supported by federal agencies, industry partners, and professional societies. The goal is to validate self-sampled HPV testing as non-inferior to specimens collected by providers. The team is currently finalizing the methodology of the study, so Dr. Sahasrabuddhe could not share the self-sampling methods that will be on trial, nor the industry partners who have signed up.
The following tests are approved in the United States for physician-collected HPV screening: Hybrid Capture 2, used in the Indian studies (Qiagen); cobas HPV (Roche); Aptima (Hologic); Cervista (Hologic); and Onclarity (Becton Dickinson).
Dr. Sahasrabuddhe said that, while a sanitary pad in a Ziploc bag is unlikely to make the grade for The Last Mile study, he doesn’t totally dismiss their potential and said the NCI is always open to new ideas.
“We are not supporting anybody specifically for menstrual pad-based collection device development,” Dr. Sahasrabuddhe said, “But if they fulfill other criteria for a small business–based grant application, they absolutely are welcome to apply for NCI funding for this.”
Said Dr. Melnikow: “Pre-COVID, the head of [the World Health Organization] said that we could eliminate cervical cancer from the globe and that we have the tools to do that now. And he’s right.”
Dr. Budukh, Dr. Melnikow, and Dr. Sahasrabuddhe disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A cell phone rings in a red-brick bungalow in a village in India. A woman on the other end of the phone tells Ms. SK, a community health worker, that menstruation has started. Ms. SK guns her scooter through the dusty streets for 15 minutes in 30° C (86° F) heat.
A 32-year-old woman, waiting in the shade of a blue corrugated-iron roof, hands over a green polythene bag. Ms. SK whisks the package to the local health center and tucks it into a –20° C freezer. The following week, it will ride in dry ice to the National Institute for Research in Reproductive and Child Health Laboratory in Mumbai for human papillomavirus (HPV) testing.
This moment in rural India at first glance appears to have little relevance to wealthy countries such as the United States.
However, public health officials in both countries are trying to solve the same problem: how to prevent unnecessary deaths from cervical cancer by reaching women who have never or rarely been screened.
The United States has more in common with India than it may care to admit.
“In the U.S., we still have pockets of disparities that actually have incidence rates [of cervical cancer] comparable to many low- and middle-income countries,” said Vikrant Sahasrabuddhe, MBBS, DrPh, MPH, of the National Cancer Institute, where he heads the HPV and cervical cancer prevention clinical research program for the National Institutes of Health.
The incidence of cervical cancer in India is approximately 19 per 100,000 women. For the past 15 years incidence in the United States has stalled at approximately 7 per 100,000.
In India, there are no organized screening programs and most cervical cancer is regional or distant metastatic at diagnosis.
In the United States, 52% of new cases are advanced, and half of these are among women who have never or rarely been screened.
“There is a critical need for new strategies to reach this population,” Dr. Sahasrabuddhe said. “We absolutely have to do something out of the box creatively.”
Almost all cervical cancers are triggered by HPV, most commonly high-risk HPV-16 and HPV-18, although there are more than 200 types. HPV testing is taking over from cytology (Papanicolaou test) for secondary prevention of cervical cancer.
The trial of screening for HPV in menstrual pads that is ongoing in India was the brainchild of Atul Budukh, PhD, a government public health researcher and professor at the Centre for Cancer Epidemiology, Tata Memorial Centre, Mumbai.
Dr. Budukh’s eyes were opened to the scale of the problem when he participated in a cluster-randomized trial funded by the Bill and Melinda Gates Foundation. The study, published in 2009 in the New England Journal of Medicine, involved 131,746 rural women in the Osmanabad district of India.
A team of researchers from India and France compared outcomes for women over 8 years after cervical screening by HPV, cytology, or visual inspection with acetic acid. The control group was usual care, where women were advised how to seek screening at local hospitals. Women who screened positive were referred for colposcopy, biopsy, and treatment.
Over the 8-year follow-up, advanced cervical cancer was found in twice as many women left to their own devices, compared with women who had HPV testing during the study (82 vs. 39; hazard ratio for HPV, 0.47; 95% confidence interval, 0.32-0.69).
Similarly, cervical cancer deaths in the control group were nearly two times higher than among the women who were screened for HPV in the study (64 vs. 34; HR for HPV, 0.52; 95% CI, 0.33-0.83).
The study proved that rural Indian women were dying unnecessarily because they weren’t seeking cervical screening. And education wasn’t the problem.
“When we go and educate [a rural woman] about ... risk factors and the need to undergo screening, she understands it very well,” said Dr. Budukh. “She is ready to come but her priority is her bread and butter – she will lose her daily wages.”
Dr. Budukh and his team negotiated with local employers so that women could come to screening clinics, but they soon realized this wasn’t scalable.
One year after the NEJM publication, Dr. Budukh found what he was looking for.
A team of Hong Kong clinicians, headed by Sze Chuen Cesar Wong of the Hong Kong Cancer Institute, published a paper in 2010 in the Journal of Clinical Microbiology showing that menstrual pads provide reliable HPV results in women with and without cervical disease.
The Hong Kong team tested sanitary napkins for HPV from 235 of their patients with cervical intraepithelial neoplasia or condyloma acuminatum before and after treatment. Samples were compared with those from 323 women without cervical disease; for HPV in sanitary napkins the sensitivity was 82.8%, specificity was 93.1%, and positive and negative predictive values were 90% and 87.9%, respectively.
The authors pointed out that menstrual pad testing was the only truly noninvasive approach to HPV screening versus the other self-sampling methods such as tampons and cytobrushes. Also, these self-sampling tests require specialized liquid-based transport media. A menstrual pad needs only a plastic bag.
Dr. Budukh had his at-home solution for the hard-working rural women of India.
With funding from the Indian government, Dr. Budukh’s team put together a validation trial that ran from 2013 to 2016 in 18 rural villages in two separate districts: Ahmednagar and Pune.
Local health workers went house to house to recruit women and get family buy-in for this culturally delicate project. Participants were instructed to use their regular sanitary protection – most commonly a washable cloth – and told to call the health worker on the first day of menstruation. Health workers gave each woman a Ziploc bag for the pad and, for privacy, an outer polythene sac.
In Ahmednagar, all women who provided their pad also got screened with Hybrid Capture 2 (HC2; Qiagen) by a mobile screening unit. In Pune, only the positive cases underwent HC2. Screening was also extended to anyone who requested it, but these people were not included in the final analysis.
Genomic DNA was extracted from three 5 mm–sized punches in the pad using a commercial kit, QIAamp DNA Micro, and the quality and purity of the DNA checked by Implen NanoPhotometer.
The team followed the same protocol for PCR HPV assay as the team from Hong Kong.
The results were published in the European Journal of Cancer Prevention in 2018.
The concordance rate for a positive result between the menstrual pad sample and conventional HPV sampling was 98.8% for Ahmednagar and 95.2% for samples from Pune. The sensitivity for the first study was 83% and the specificity 99% – similar to that for the women in Hong Kong. The second study had lower sensitivity and specificity (67% and 88%), partly because of poor storage as a result of frequent power cuts.
The total cost per woman was $30.78.
“I was very excited when we saw the results,” Dr. Budukh recalled. “That day I couldn’t sleep ... such a wonderful result! I was excited to start the next phase immediately.”
Dr. Budukh has applied to the Indian government for funding for a larger trial involving 3,000 women. If successful, he hopes such evidence would be sufficient to convince the Indian government to make menstrual pad screening standard procedure for the 390 million women who live in India’s countryside.
Testing never-screened women for cervical cancer using menstrual pads appears to be relatively reliable, convenient, private, noninvasive, and incredibly cheap.
So who else has tried it?
The first published account of HPV in menstrual blood was a 2003 study by Tommy Tong and colleagues at the Princess Margaret Hospital in Hong Kong. The authors heralded, with lamentable optimism, “a new paradigm in cervical cancer screening.”
In the following 20 years, just six more studies appeared: two from Dr. Budukh’s field trial in India and four from hospital-based pilot studies in Hong Kong (in 2010 and 2018), South Korea (in 2016), and mainland China (in 2021). All these studies, although small, were published in top-flight journals and demonstrate high concordance between conventional high-risk HPV testing and menstrual-blood tests.
This news organization tried to find a U.S. thought-leader who had heard of the approach.
Elizabeth Fontham, MPH, DrPh, is the founding dean of the school of public health at Louisiana State University Health Center in New Orleans, and president of the American Cancer Society. Dr. Fontham said in an email that she had “no plans to evaluate the impact related to menstrual pads, but perhaps others have looked into that.”
Joy Melnikow, MD, MPH, was first author on the evidence synthesis driving the current cervical cancer screening recommendations from the U.S. Preventive Services Task Force. When asked about menstrual pad testing for HPV, she said she had “not heard of it before.”
The USPSTF guidelines don’t mention sanitary pads but acknowledge that “self-collection may be one strategy for increasing screening rates among populations where they are currently low.”
The USPSTF methodology excludes data from countries that don’t match the United States on the Human Development Index “or [are] not applicable to U.S. clinical settings or populations.” (Presumably, data from Hong Kong and South Korea would qualify; Indian data would not.)
Dr. Sahasrabuddhe of the NCI hadn’t heard of menstrual pad testing either, but he has a different explanation for lack of interest in this approach – or, indeed, any form of self-sampling for cervical cancer screening – in the United States.
“We have not seen movement happen in this space for years. ... If there is one intervention that we can simplify, that still has not been made widely available, it is self-sampling ... [but] we don’t have [Food and Drug Administration] approval for it,” Dr. Sahasrabuddhe said.
“Our system, at least in the U.S., is based on industry manufacturers seeking an approval for a particular way of collection and then clinicians and clinical-guideline bodies signing on. ... For a lot of reasons industry has shied away over the past several years, so far, at least, on seeking approval for self-sampling-based approaches,” he commented.
Dr. Sahasrabuddhe aims to change that. He heads a new NCI-led initiative called “The Last Mile,” a nationwide clinical trial supported by federal agencies, industry partners, and professional societies. The goal is to validate self-sampled HPV testing as non-inferior to specimens collected by providers. The team is currently finalizing the methodology of the study, so Dr. Sahasrabuddhe could not share the self-sampling methods that will be on trial, nor the industry partners who have signed up.
The following tests are approved in the United States for physician-collected HPV screening: Hybrid Capture 2, used in the Indian studies (Qiagen); cobas HPV (Roche); Aptima (Hologic); Cervista (Hologic); and Onclarity (Becton Dickinson).
Dr. Sahasrabuddhe said that, while a sanitary pad in a Ziploc bag is unlikely to make the grade for The Last Mile study, he doesn’t totally dismiss their potential and said the NCI is always open to new ideas.
“We are not supporting anybody specifically for menstrual pad-based collection device development,” Dr. Sahasrabuddhe said, “But if they fulfill other criteria for a small business–based grant application, they absolutely are welcome to apply for NCI funding for this.”
Said Dr. Melnikow: “Pre-COVID, the head of [the World Health Organization] said that we could eliminate cervical cancer from the globe and that we have the tools to do that now. And he’s right.”
Dr. Budukh, Dr. Melnikow, and Dr. Sahasrabuddhe disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and COVID: Decline in new cases comes to an end
It was a good run while it lasted.
according to the American Academy of Pediatrics and the Children’s Hospital Association.
The number of reported pediatric cases for the week was 33,146, and the actual increase from the previous week was just 7,231 cases, the AAP and CHA said, but some reports suggest that the new COVID variants and subvariants are starting to have an effect on incidence in some areas while mask mandates continue to fall.
Data from the Centers for Disease Control and Prevention show that, over the last week or two, the 7-day average for percentage of emergency department visits with diagnosed COVID has risen from 0.5% to 0.6% in children aged 0-11 years, from 0.3% to 0.5% among 12- to 15-year-olds, and from 0.3% to 0.4% in 16- and 17-year-olds. Small increases, to be sure, but increases nonetheless.
A somewhat similar scenario is playing out for new admissions of children aged 0-17, which have leveled out after dropping from a high of 1.25 per 100,000 population in mid-January to 0.13 per 100,000 in early April. Over the last 2 weeks, the rate has been alternating between 0.13 and 0.14 per 100,000, the CDC said on its COVID Data Tracker.
The latest news on the vaccination front came from Pfizer and BIoNTech, which announced that a third dose of its COVID-19 vaccine boosted immune protection in children aged 5-11 years in a phase 2/3 trial. Protection against the Omicron strain was 36 times higher than the two previous doses, the companies said, adding that they plan to submit a request for emergency use authorization of a booster dose in the near future.
The ongoing vaccination effort, however, produced mixed results in the last week. Initial vaccinations among children aged 5-11 years fell 14.5% to another new low while initial doses were up 9.3% for those aged 12-17, the AAP said. Overall, just 28.2% of the country’s 5- to 11-year-olds are fully vaccinated, compared with 58.7% of those aged 12-17, the CDC reported.
It was a good run while it lasted.
according to the American Academy of Pediatrics and the Children’s Hospital Association.
The number of reported pediatric cases for the week was 33,146, and the actual increase from the previous week was just 7,231 cases, the AAP and CHA said, but some reports suggest that the new COVID variants and subvariants are starting to have an effect on incidence in some areas while mask mandates continue to fall.
Data from the Centers for Disease Control and Prevention show that, over the last week or two, the 7-day average for percentage of emergency department visits with diagnosed COVID has risen from 0.5% to 0.6% in children aged 0-11 years, from 0.3% to 0.5% among 12- to 15-year-olds, and from 0.3% to 0.4% in 16- and 17-year-olds. Small increases, to be sure, but increases nonetheless.
A somewhat similar scenario is playing out for new admissions of children aged 0-17, which have leveled out after dropping from a high of 1.25 per 100,000 population in mid-January to 0.13 per 100,000 in early April. Over the last 2 weeks, the rate has been alternating between 0.13 and 0.14 per 100,000, the CDC said on its COVID Data Tracker.
The latest news on the vaccination front came from Pfizer and BIoNTech, which announced that a third dose of its COVID-19 vaccine boosted immune protection in children aged 5-11 years in a phase 2/3 trial. Protection against the Omicron strain was 36 times higher than the two previous doses, the companies said, adding that they plan to submit a request for emergency use authorization of a booster dose in the near future.
The ongoing vaccination effort, however, produced mixed results in the last week. Initial vaccinations among children aged 5-11 years fell 14.5% to another new low while initial doses were up 9.3% for those aged 12-17, the AAP said. Overall, just 28.2% of the country’s 5- to 11-year-olds are fully vaccinated, compared with 58.7% of those aged 12-17, the CDC reported.
It was a good run while it lasted.
according to the American Academy of Pediatrics and the Children’s Hospital Association.
The number of reported pediatric cases for the week was 33,146, and the actual increase from the previous week was just 7,231 cases, the AAP and CHA said, but some reports suggest that the new COVID variants and subvariants are starting to have an effect on incidence in some areas while mask mandates continue to fall.
Data from the Centers for Disease Control and Prevention show that, over the last week or two, the 7-day average for percentage of emergency department visits with diagnosed COVID has risen from 0.5% to 0.6% in children aged 0-11 years, from 0.3% to 0.5% among 12- to 15-year-olds, and from 0.3% to 0.4% in 16- and 17-year-olds. Small increases, to be sure, but increases nonetheless.
A somewhat similar scenario is playing out for new admissions of children aged 0-17, which have leveled out after dropping from a high of 1.25 per 100,000 population in mid-January to 0.13 per 100,000 in early April. Over the last 2 weeks, the rate has been alternating between 0.13 and 0.14 per 100,000, the CDC said on its COVID Data Tracker.
The latest news on the vaccination front came from Pfizer and BIoNTech, which announced that a third dose of its COVID-19 vaccine boosted immune protection in children aged 5-11 years in a phase 2/3 trial. Protection against the Omicron strain was 36 times higher than the two previous doses, the companies said, adding that they plan to submit a request for emergency use authorization of a booster dose in the near future.
The ongoing vaccination effort, however, produced mixed results in the last week. Initial vaccinations among children aged 5-11 years fell 14.5% to another new low while initial doses were up 9.3% for those aged 12-17, the AAP said. Overall, just 28.2% of the country’s 5- to 11-year-olds are fully vaccinated, compared with 58.7% of those aged 12-17, the CDC reported.