User login
Medicare drug changes ought to benefit rheumatology patients
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.

But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.
But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
Changes in Medicare law will help some patients who need costly rheumatology treatments, including several medicines for which competition has been kept in check for many years.
In fact, this field of medicine includes prime examples of the kinds of products that drove Congress to give the giant federal health program leverage to try to restrain rising pharmaceutical costs through negotiations. The Inflation Reduction Act, signed into law by President Joe Biden on Aug. 16, also provides some fairly quick aid for people enrolled in Medicare who struggle with pharmacy bills.
As described in an official summary from the Congressional Research Service, the law establishes:
- A cap on annual Medicare Part D out-of-pocket spending that starts in 2025 at $2,000, with planned annual adjustments thereafter.
- A limit on cost-sharing under Medicare Part D for a month’s supply of covered insulin products at $35 for 2023 through 2025, with plans for continued limits on this cost in the years after pegged to negotiated prices.
- A program under which drug manufacturers provide discounts to beneficiaries who have incurred costs above the annual deductible beginning in 2025.
- A requirement that drugmakers issue rebates to Medicare for certain brand-name drugs covered without generic equivalents for which prices increase faster than inflation.
- An obligation for Medicare Part D plans to pay for adult vaccines that are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices without requiring cost sharing.
The law’s marquee health provision sets the stage for Medicare, the nation’s largest purchaser of drugs, for the first time to leverage its clout directly in negotiating for lower costs for medicines. Democrats sought to build what amount to guardrails into this program, seeking to spare from competition new and innovative drugs and ones developed by smaller companies. Drugs likely to soon face competition from copycat versions also would fall outside of the pool for negotiations.
In effect, the design of the program would allow Medicare to negotiate in the future in cases such as those seen in recent years with blockbuster medicines often in rheumatology. That’s due in a large part to legal challenges that have helped thwart the introduction of copycat versions of these kinds of products known as biosimilars.
Etanercept (Enbrel) has been sold in the United States since 1998 and adalimumab (Humira) since 2003. Both products face competition from copycat versions called biosimilars in other nations, but the introductions of these products have been delayed in the United States until 2029 for etanercept and 2023 for adalimumab, the Office of Inspector General for the Department of Health & Human Services said in a March 2022 report. The OIG said in the report that the combined 2019 Medicare Part D tab for the two biologics was more than $5 billion.
Rheumatology drugs rival cancer medicines for dominance among the most expensive drugs for people enrolled in Medicare. The average 2020 spending for the most widely used forms of adalimumab by people in Medicare’s Part D pharmacy program topped $51,000, according to federal data. The price per dosage-unit for the drug rose about 7% from 2019 to 2020.
The pharmaceutical industry defends the high introductory costs of medicines and subsequent rising prices as necessary payback for research on products sold and the ones still in development. Since the initial Food and Drug Administration approval of adalimumab on Dec. 31, 2002, Abbott Laboratories and its AbbVie spin-off have made changes to the drug’s administration and paid for studies to expand its approved indications.
Still, the investment in adalimumab appears to have been paid well.
Abbott Labs acquired adalimumab as part of its purchase of BASF’s pharmaceutical operations in 2001, a purchase that also included the thyroid drug Synthroid. Abbott paid $7.2 billion, or roughly $12 billion in current dollars. In 2021 alone, Humira sales were $20.7 billion, with the United States accounting for $17.3 billion of the product’s revenue.
Losing access to treatment when moving to Medicare
Sue Lee of Crestwood, Ky., is among the patients waiting to see if the changes in Medicare law might allow her to again afford adalimumab. For now, Ms. Lee said she is hoping her plaque psoriasis stays manageable with the topical ointments and moisturizers she has been using since losing access to adalimumab. Ms. Lee, 80, took the medicine during her working years for her plaque psoriasis.
“I told people: ‘I’m on the wonder drug. Look at me. I can show my skin now. I don’t have all of these sores,’ ” she said in an interview.
But after she retired at 75, she was shocked at the tab she faced after switching from private insurance to Medicare. She said it could have cost her close to $10,000 a year to take Humira. Ms. Lee’s Social Security earnings make her ineligible for certain assistance with drug costs.
“I cried a lot,” she said about the loss of affordable access to the drug.
What’s the path ahead?
The American College of Rheumatology and the Coalition of State Rheumatology Organizations are among the physician groups that pressed Congress for years for action to lower drug costs. Their members have been on the frontline of the crisis in the United States among patients unable to afford medicines.
“The financial burden of skyrocketing drug prices has forced many of our patients to spread their treatment out longer than prescribed, delay care, abandon prescriptions, or forgo treatment entirely – all of which risks flare-ups, disease regression, permanent disability, and even premature death,” said Blair Solow, MD, chair of the ACR’s Government Affairs Committee, in a statement on the new Medicare provisions.
In an interview, Dr. Solow, an assistant professor of medicine in the division of rheumatic diseases at University of Texas Southwestern Medical Center, Dallas, noted that there are concerns about how changes in Medicare drug pricing might affect future development of medicines. This has been a chief criticism of the pharmaceutical industry of efforts to allow Medicare to negotiate for lower prices.
“Of note, drug companies research, create, and produce medications that will perform well in the market, not necessarily those that may be most needed,” Dr. Solow wrote. “We can hope the new medications put forth by manufacturers are those that improve the lives of patients.”
In July, the Congressional Budget Office released a report on an earlier version of the Democrats’ plans for Medicare drug negotiations that suggested the potential loss to drugmakers’ productivity may be relatively small. The CBO expects that about 1,300 drugs will be approved over the next 30 years. The legislation as proposed in July might reduce the tally by 15 drugs. The CBO said these estimates fell in the middle of the distribution of possible outcomes and are subject to uncertainty, and it is still working on an estimate of the expects effects of the final version of the law.
“CBO did not predict what kind of drugs would be affected or analyze the effects of forgone innovation on public health,” the agency said.
Dr. Solow also said there may be some challenges for physicians in explaining to patients the timeline for the new law’s Medicare provisions. People need to be aware of how long it will take to implement the plan and the potential for changes or delays.
“I think this is important, because the interpretation of the law can be done in a way that was not necessarily what Congress intended, and depending on the control of Congress and the Administration, this could impact downstream effects in how this law plays out,” she said in an interview.
CMS has substantial work ahead of it in choosing the drugs for which there will be subject to negotiations. The new law limits the number of drugs that can be negotiated to 10 annually in 2026, increasing to 20 drugs annually by 2029. Drugs would be eligible for negotiated prices from 9 years after drug approval or 13 years for biologics, until entry of a generic or biosimilar competitor.
The new law calls for taxes and other penalties for companies that refuse to negotiate or offer the agreed price, Thomas J. Hwang, MD; Aaron S. Kesselheim, MD, JD, MPH; and Benjamin N. Rome, MD, MPH, all of Harvard Medical School, Boston, wrote in an Aug. 19 viewpoint article in JAMA. U.S. lawmakers took a different approach to negotiations about drug prices than those used in other countries, they wrote.
“Notably, the Inflation Reduction Act shields new drugs from negotiated prices for the first 9-13 years on the market,” they wrote. “In contrast, most other peer countries typically negotiate drug prices at the time of market entry, and no peer country limits the number of drugs negotiated.”
Missed opportunities
Madelaine Feldman, MD, president of the CSRO and a rheumatologist in private practice with The Rheumatology Group in New Orleans, said in an interview that she welcomes many of the provisions of the new law, as they will help her rheumatology patients afford their medicine.
But she considers one of the provisions of the law to be a disappointment. The law further delays the start date for a federal rule intended to allow people on Medicare Part D to directly benefit from discounts negotiated on drugs. This is a point often overlooked in news reports on the law.
Insurers use what are called pharmacy benefit manager (PBM) services to obtain rebates on medicines, but they don’t fully or directly share these price reductions with people enrolled in Part D plans. Instead, people in the Part D plans have their cost sharing pegged closer to listed prices, the ones set before the rebates obtained by PBMs. The PBM industry argues that the rebates, often based on the list price of the drug, serve to keep monthly insurance premiums low. But there’s been concern about perverse incentives in this approach, where more expensive drugs are preferred by PBMs, leading to higher rebates.
Congress had already delayed its implementation of the PBM rule, which would apply savings more directly to patients, until 2027 and did so again in the Inflation Reduction Act.
Implementing this rule on Medicare Part D prescription drug rebates would be a help for patients struggling to pay for costly drugs, such as those used in rheumatology, Dr. Feldman said.
“It just doesn’t make any sense to hold off on these changes if you really want to cut Medicare’s beneficiaries’ cost sharing and attempt to stop the perverse incentive that puts higher priced drugs on Part D formularies,” she said.
Children and COVID: New cases increase; hospital admissions could follow
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.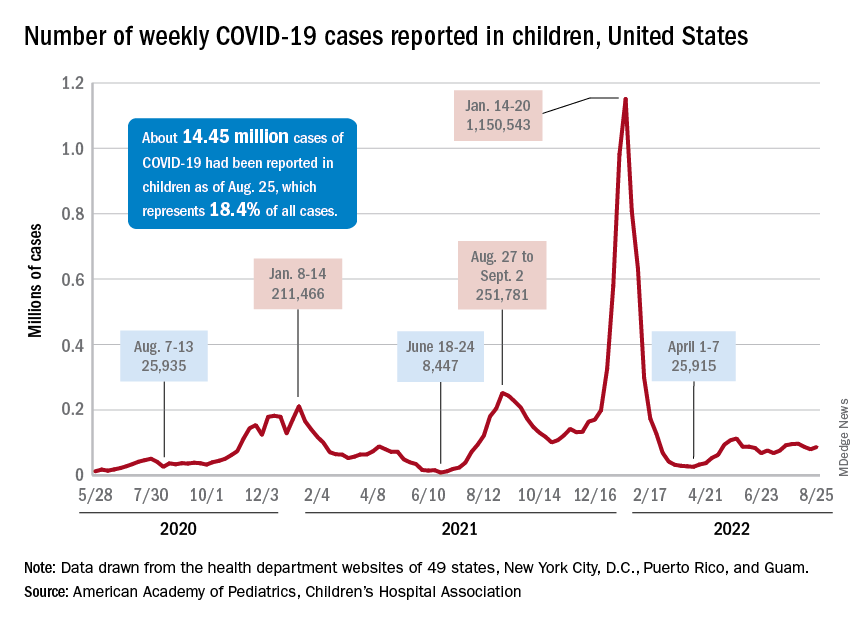
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.

Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.
Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.
Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
At-home test for oral/throat cancer launched in U.S.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
OMERACT continues to set standards on research outcomes, enhancing the patient voice
Clinical research in rheumatology was suffering from an identity crisis of sorts 40 years ago. A lack of consensus across continents resulted in differing views about clinical outcome measures and judgments about treatments.
Patients were not allowed to be the generating source of a clinical outcome, according to Peter Tugwell, MSc, MD. “The only outcomes that were acceptable were clinician assessments, blood tests, and imaging,” said Dr. Tugwell, professor of medicine, epidemiology, and public health at the University of Ottawa (Ont.) and a practicing rheumatologist at Ottawa Hospital.
Clinicians were coming to different conclusions about patient responses to treatment when managing rheumatoid arthritis in clinical practice.
OMERACT sought to address this lack of uniformity. This international group, formed in 1992, leverages stakeholder groups to improve outcome measurement in rheumatology endpoints through a consensus-building, data-driven format.
It was originally known as “Outcome Measures in Rheumatoid Arthritis Clinical Trials,” but its leaders have since broadened its scope to “Outcome Measures in Rheumatology.” Over the years, it has evolved into an international network that assesses measurement across a wide variety of intervention studies. Now 30 years old, the network spans 40 active working groups and has influenced work in patient outcomes across 500 peer-reviewed publications.
The network meets every 2 years to address what is always a challenging agenda, said Dr. Tugwell, one of its founding members and chair. “There’s lots of strong opinions.” Participating in the discussions are individuals from all stages of seniority in rheumatology and clinical epidemiology, patient research partners, industry, approval agencies, and many countries who are committed to the spirit of OMERACT.
“The secret to our success has been getting world leaders to come together and have those discussions, work them through, and identify common ground in such a way that the approval agencies accept these outcome measures in clinical trials,” he added.
“My impression was the founders perceived a problem in the early 1990s and devised a consensus method in an attempt to quantify clinical parameters to define disease activity in rheumatoid arthritis – an important first step to do clinical trials and allow comparisons between them,” said Patricia Woo, CBE, FMedSci, FRCP, emeritus professor of pediatric rheumatology and previous head of the Centre for Paediatric and Adolescent Rheumatology at UCL, London. At that time, even disease definitions varied between the United States and Europe and other parts of the world, said Dr. Woo, who is not a part of OMERACT. “This was especially true for pediatric rheumatology.”
Fusing the continental divide
OMERACT arose from a need to streamline clinical outcome measures in rheumatology. Research papers during the 1980s demonstrated a lack of coherence in managing patients with rheumatoid arthritis in routine practice. In addition, the measures used to define clinical endpoints in clinical trials operated in silos – they were either too specific to a certain trial, overlapped with other concepts, or didn’t reflect changes in treatment.
Approval agencies in Europe and North America were approving only outcomes measures developed by their respective researchers. This was also true of patients they tested on. “This seemed crazy,” Dr. Tugwell said.
Dr. Tugwell was involved in the Cochrane collaboration, which conducts systematic reviews of best evidence across the world that assesses the magnitude of benefits versus harms.
To achieve this goal, “you need to pull studies from around the world,” he said. Maarten Boers, MD, PhD, a rheumatologist (and later professor of clinical epidemiology at Amsterdam University Medical Center) from the Netherlands, spent a year in Ontario, Canada, to train as a clinical epidemiologist. Together, Dr. Tugwell and Dr. Boers began discussing options to develop more streamlined outcome measures.

They initiated the first OMERACT conference in Maastricht, the Netherlands, in 1992. The Food and Drug Administration and European Medicines Agency participated, along with leaders of outcomes measurement in Europe and in North America.
Discussions centered on methods to develop outcomes in a meaningful fashion. During the first meeting, North American and European approval agencies agreed to accept each other’s studies and endpoints and patient reported outcomes.
Agreement was achieved on a preliminary set of outcome domains and measures that later became known as the WHO-ILAR (World Health Organization–International League of Associations for Rheumatology) core set. The set included seven outcome domains: tender joints, swollen joints, pain, physician global assessment, patient global assessment, physical disability, and acute phase reactants, and one additional outcome domain for studies lasting 1 year or more: radiographs of the joints.
“A proactive program was planned to test not only the validity of these endpoints, but also the methods for their measurement. This was the start of a continuing process,” OMERACT members said in a joint statement for this article. Meetings have since taken place every 2 years.

OMERACT accomplishments
OMERACT now requires buy-in from four continents: Asia, Australia, Europe, and North America.
Its leaders have developed an explicit process for gaining endorsement of core outcome domains and instrument measurement sets. To fully capture the possibilities of “what to measure,” i.e., “measurable aspects of health conditions,” OMERACT has developed a framework of concepts, core areas, and outcome domains. The key concepts are pathophysiology (with a core area termed “manifestations/abnormalities”) and impact (with core areas of “death/lifespan,” and “life impact,” and the optional area of “societal/resource use”). An outcome domain defines an element of a core area to measure the effects of a treatment, such as blood markers, pain intensity, physical function, or emotional well-being.
A core outcome domain set is developed by agreeing to at least one outcome domain within one of the three core areas. Subsequently, a core outcome measurement set is developed by agreeing to at least one applicable measurement instrument for each core outcome domain. This requires documentation of validity, summarized under three metrics: truth, discrimination, and feasibility.
OMERACT’s handbook provides tutelage on establishing and implementing core outcomes, and several workbooks offer guidance on developing core outcome domain sets, selecting instruments for core outcome measurement sets, and OMERACT methodology.
All this work has led to widespread adoption.
Approval agencies have accepted OMERACT’s filter and methods advances, which have been adopted by many research groups in rheumatology and among nonrheumatology research groups. Organizations such as the U.S. National Institutes of Health’s National Institute of Neurological Disorders and Stroke have sought its advice.
Its core outcomes have been adopted and used for approval in the great majority of studies on rheumatoid arthritis, Dr. Tugwell said.
Several BMJ articles underscore the influence and uptake of OMERACT’s core outcome set. One 2017 paper, which analyzed 273 randomized trials of rheumatoid arthritis drug treatments on ClinicalTrials.gov, found that the WHO-ILAR arthritis core outcome set was reported in 81% of the studies. “The adoption of a core outcome set has the potential to increase consistency in outcomes measured across trials and ensure that trials are more likely to measure appropriate outcomes,” the authors concluded.
Since the initial 1992 meeting, OMERACT has broadened its focus from rheumatoid arthritis to 25 other musculoskeletal conditions.
For example, other OMERACT conferences have led to consensus on core sets of measures for osteoarthritis and osteoporosis, psoriasis/psoriatic arthritis, psychosocial measures, and a core set of data for cost-effectiveness evaluations.
‘Speed is a limitation’
OMERACT is a bottom-up volunteer organization. It doesn’t represent any official organization of any clinical society. “We’ve not asked to be adopted by the American College of Rheumatology, EULAR [European Alliance of Associations for Rheumatology], or other international organizations,” Dr. Tugwell said. It offers a chance for patients, users, and doers of research to work together to agree on rigorous criteria accepted by the approval agencies and take the necessary time to work things through.
This is not a fast process, usually taking 4-6 years to initiate and establish an outcome domain set, he emphasized. “It would be beneficial to do it faster if we had the resources to meet every year. The fact is we’re a volunteer organization that meets every 2 years.”
Speed is a limitation, he acknowledged, but it’s an acceptable trade-off for doing things correctly.
The group has faced other challenges during the COVID-19 pandemic, pivoting to a virtual format that had benefits and limitations.
In one respect, moving to a virtual meeting increased uptake in participation and voting, Dr. Tugwell said. Patient participants with severe rheumatoid arthritis no longer faced the challenges of travel. “On the other hand, we didn’t have the same opportunity to achieve common ground virtually,” he said. “Where there are strong disagreements, I’m a great believer that people need to know one another. There needs to be relationship building.”
OMERACT’s emerging leader program has been a cornerstone of its in-person meetings, engaging young rheumatologists to interact with some of the leaders of outcome measurement. The virtual format dampened this process somewhat, eliminating those important “café chats” between the stakeholders.
The hope is to bring people face-to-face once more at the next meeting in May 2023. The agenda will focus on relationship building, identifying controversial areas, and bringing younger people to develop relationships, Dr. Tugwell said. OMERACT will retain a virtual option for the worldwide voting, “which will allow for more buy-in from so many more people,” he added.
A consensus on pain
The onus of developing outcome measures that move with the times is sometimes too great for one group to manage. In 2018, OMERACT became a part of the Red Hat Group (RHG), an organization conceived at the COMET (Core Outcome Measures in Effectiveness Trials) VII meeting in Amsterdam.
RHG aims to improve the choice of outcomes in health research. It includes eight groups: COMET; OMERACT; the Cochrane Skin Core Outcome Set Initiative; Grading of Recommendations, Assessment, Development and Evaluations; Center for Medical Technology Policy; COnsensus-based Standards for the selection of health Measurement Instruments; Clinical Data Interchange Standards Consortium; and Standardized Outcomes in Nephrology.
The collaboration between groups offers a “very interesting interface between consensus building as well as hard evidence,” Dr. Tugwell said. The focus goes beyond rheumatology to other clinical areas of common interest, exploring how one classifies outcome domains in terms of symptoms, life impact, or death.
Pain is an important common denominator that the RHG has evaluated.
“We believe it’s too general. We’re trying to define pain across all Red Hat Groups because it’s clear that the research community has all these different scales for defining pain severity,” Dr. Tugwell said. “We have to find a way to make ruthless decisions and rules for doing it. And of course, it has to be transparent.”
Looking ahead
As part of its ongoing work, OMERACT is evaluating the robustness of instruments that rheumatologists use as outcome measures in clinical trials, which can be a laborious process. The OMERACT Filter 2.0, part of the latest iteration of the handbook, offers strong guidance for researchers but needs a long-term strategy and key methodological support. “To that end, we set up a technical advisory group to help people in the instrument selection work and that remains an ongoing process,” OMERACT leaders said in their joint statement.
OMERACT is looking at opportunities to create benchmark processes for developing core sets outside of rheumatology and a methodology around outcome measures such as contextual factors, composites, and surrogates.
It will also be taking a step back to solicit opinions from the approval agencies represented by the OMERACT membership on the OMERACT handbook.
The goal is to make sure the handbook aligns with everyone else’s approval and labeling requirements.
OMERACT’s patient participants bring important perspectives
OMERACT over the years has sought to become a more patient-centered group. Patients have been involved in OMERACT activities since its sixth meeting, forming an independent, yet integrated, group within the network. They have their own steering committee and produced and helped to update a glossary for OMERACT patients and professionals.
Catherine (McGowan) Hofstetter, who was diagnosed with rheumatoid arthritis 30 years ago, chairs OMERACT’s Patient Research Partners Support Team. In a Q&A, she discussed the importance of patient voices and OMERACT’s plans to further educate and include patients in the dialogue on outcomes.
Question: Have patients always been a part of OMERACT meetings?
Answer: Patients have been involved with OMERACT since 2002. The patient voice adds relevance to all the work that OMERACT does. You can’t begin to talk about outcomes unless there is a patient at the table with lived experience.
Q: Can you cite a few examples of how the patient voice enriches the conversation on outcomes research?
A: Outcomes and priorities that are important to patients are often completely different than those of the clinician. For instance, a work outcome is important to someone who doesn’t have any medical insurance or disability insurance, so that you can ensure that there is food on the table and a roof over your head. Or it may be important to someone because the employment provides medical and disability insurance to provide security for them and their family. These are two different perspectives on work and therefore work priorities and outcomes.
Q: What have been some of the challenges of getting patients to participate?
A: Training patients is one challenge. OMERACT’s work has a very steep learning curve, and while the basics are the same between the groups in terms of looking at what we measure and how we measure it, the nuances of different working groups require a lot of time and energy to be comfortable enough with the work, and then be confident enough to bring your perspective and lived experience to the table. It’s also a very accomplished group, which can be quite intimidating. Self-disclosure is a very personal and intimate undertaking that requires patience, compassion, and respect.
Q: Are there any plans to enhance patient engagement?
A: When we had OMERACT 2020 it was a virtual conference that took place over about 6 months. We had far more patient research partners [PRPs] participate than we have ever had at any OMERACT face-to-face meeting. There is a desire and passion on the part of patients to lend their voices to the work. The working groups meet virtually throughout the year to advance their agendas, and PRPs are a part of each of the working groups.
Hopefully, we can start working toward including more voices at the conferences by enabling a hybrid model. The PRP Support Team will begin engaging patients this fall with education, mentoring, and team-building exercises so by the time we meet in person in May 2023, they will have enough background knowledge and information to give them the confidence that will enhance their experience at the face-to-face meeting.
We also need to ensure that those patients who want to stay engaged can. This means that the education and training should continue long after the face-to-face meeting is over. We need to build capacity in the PRP group and look to succession planning and be a resource to working groups struggling to find PRPs to work with them on a longer-term basis.
Clinical research in rheumatology was suffering from an identity crisis of sorts 40 years ago. A lack of consensus across continents resulted in differing views about clinical outcome measures and judgments about treatments.
Patients were not allowed to be the generating source of a clinical outcome, according to Peter Tugwell, MSc, MD. “The only outcomes that were acceptable were clinician assessments, blood tests, and imaging,” said Dr. Tugwell, professor of medicine, epidemiology, and public health at the University of Ottawa (Ont.) and a practicing rheumatologist at Ottawa Hospital.
Clinicians were coming to different conclusions about patient responses to treatment when managing rheumatoid arthritis in clinical practice.
OMERACT sought to address this lack of uniformity. This international group, formed in 1992, leverages stakeholder groups to improve outcome measurement in rheumatology endpoints through a consensus-building, data-driven format.
It was originally known as “Outcome Measures in Rheumatoid Arthritis Clinical Trials,” but its leaders have since broadened its scope to “Outcome Measures in Rheumatology.” Over the years, it has evolved into an international network that assesses measurement across a wide variety of intervention studies. Now 30 years old, the network spans 40 active working groups and has influenced work in patient outcomes across 500 peer-reviewed publications.
The network meets every 2 years to address what is always a challenging agenda, said Dr. Tugwell, one of its founding members and chair. “There’s lots of strong opinions.” Participating in the discussions are individuals from all stages of seniority in rheumatology and clinical epidemiology, patient research partners, industry, approval agencies, and many countries who are committed to the spirit of OMERACT.
“The secret to our success has been getting world leaders to come together and have those discussions, work them through, and identify common ground in such a way that the approval agencies accept these outcome measures in clinical trials,” he added.
“My impression was the founders perceived a problem in the early 1990s and devised a consensus method in an attempt to quantify clinical parameters to define disease activity in rheumatoid arthritis – an important first step to do clinical trials and allow comparisons between them,” said Patricia Woo, CBE, FMedSci, FRCP, emeritus professor of pediatric rheumatology and previous head of the Centre for Paediatric and Adolescent Rheumatology at UCL, London. At that time, even disease definitions varied between the United States and Europe and other parts of the world, said Dr. Woo, who is not a part of OMERACT. “This was especially true for pediatric rheumatology.”
Fusing the continental divide
OMERACT arose from a need to streamline clinical outcome measures in rheumatology. Research papers during the 1980s demonstrated a lack of coherence in managing patients with rheumatoid arthritis in routine practice. In addition, the measures used to define clinical endpoints in clinical trials operated in silos – they were either too specific to a certain trial, overlapped with other concepts, or didn’t reflect changes in treatment.
Approval agencies in Europe and North America were approving only outcomes measures developed by their respective researchers. This was also true of patients they tested on. “This seemed crazy,” Dr. Tugwell said.
Dr. Tugwell was involved in the Cochrane collaboration, which conducts systematic reviews of best evidence across the world that assesses the magnitude of benefits versus harms.
To achieve this goal, “you need to pull studies from around the world,” he said. Maarten Boers, MD, PhD, a rheumatologist (and later professor of clinical epidemiology at Amsterdam University Medical Center) from the Netherlands, spent a year in Ontario, Canada, to train as a clinical epidemiologist. Together, Dr. Tugwell and Dr. Boers began discussing options to develop more streamlined outcome measures.
They initiated the first OMERACT conference in Maastricht, the Netherlands, in 1992. The Food and Drug Administration and European Medicines Agency participated, along with leaders of outcomes measurement in Europe and in North America.
Discussions centered on methods to develop outcomes in a meaningful fashion. During the first meeting, North American and European approval agencies agreed to accept each other’s studies and endpoints and patient reported outcomes.
Agreement was achieved on a preliminary set of outcome domains and measures that later became known as the WHO-ILAR (World Health Organization–International League of Associations for Rheumatology) core set. The set included seven outcome domains: tender joints, swollen joints, pain, physician global assessment, patient global assessment, physical disability, and acute phase reactants, and one additional outcome domain for studies lasting 1 year or more: radiographs of the joints.
“A proactive program was planned to test not only the validity of these endpoints, but also the methods for their measurement. This was the start of a continuing process,” OMERACT members said in a joint statement for this article. Meetings have since taken place every 2 years.
OMERACT accomplishments
OMERACT now requires buy-in from four continents: Asia, Australia, Europe, and North America.
Its leaders have developed an explicit process for gaining endorsement of core outcome domains and instrument measurement sets. To fully capture the possibilities of “what to measure,” i.e., “measurable aspects of health conditions,” OMERACT has developed a framework of concepts, core areas, and outcome domains. The key concepts are pathophysiology (with a core area termed “manifestations/abnormalities”) and impact (with core areas of “death/lifespan,” and “life impact,” and the optional area of “societal/resource use”). An outcome domain defines an element of a core area to measure the effects of a treatment, such as blood markers, pain intensity, physical function, or emotional well-being.
A core outcome domain set is developed by agreeing to at least one outcome domain within one of the three core areas. Subsequently, a core outcome measurement set is developed by agreeing to at least one applicable measurement instrument for each core outcome domain. This requires documentation of validity, summarized under three metrics: truth, discrimination, and feasibility.
OMERACT’s handbook provides tutelage on establishing and implementing core outcomes, and several workbooks offer guidance on developing core outcome domain sets, selecting instruments for core outcome measurement sets, and OMERACT methodology.
All this work has led to widespread adoption.
Approval agencies have accepted OMERACT’s filter and methods advances, which have been adopted by many research groups in rheumatology and among nonrheumatology research groups. Organizations such as the U.S. National Institutes of Health’s National Institute of Neurological Disorders and Stroke have sought its advice.
Its core outcomes have been adopted and used for approval in the great majority of studies on rheumatoid arthritis, Dr. Tugwell said.
Several BMJ articles underscore the influence and uptake of OMERACT’s core outcome set. One 2017 paper, which analyzed 273 randomized trials of rheumatoid arthritis drug treatments on ClinicalTrials.gov, found that the WHO-ILAR arthritis core outcome set was reported in 81% of the studies. “The adoption of a core outcome set has the potential to increase consistency in outcomes measured across trials and ensure that trials are more likely to measure appropriate outcomes,” the authors concluded.
Since the initial 1992 meeting, OMERACT has broadened its focus from rheumatoid arthritis to 25 other musculoskeletal conditions.
For example, other OMERACT conferences have led to consensus on core sets of measures for osteoarthritis and osteoporosis, psoriasis/psoriatic arthritis, psychosocial measures, and a core set of data for cost-effectiveness evaluations.
‘Speed is a limitation’
OMERACT is a bottom-up volunteer organization. It doesn’t represent any official organization of any clinical society. “We’ve not asked to be adopted by the American College of Rheumatology, EULAR [European Alliance of Associations for Rheumatology], or other international organizations,” Dr. Tugwell said. It offers a chance for patients, users, and doers of research to work together to agree on rigorous criteria accepted by the approval agencies and take the necessary time to work things through.
This is not a fast process, usually taking 4-6 years to initiate and establish an outcome domain set, he emphasized. “It would be beneficial to do it faster if we had the resources to meet every year. The fact is we’re a volunteer organization that meets every 2 years.”
Speed is a limitation, he acknowledged, but it’s an acceptable trade-off for doing things correctly.
The group has faced other challenges during the COVID-19 pandemic, pivoting to a virtual format that had benefits and limitations.
In one respect, moving to a virtual meeting increased uptake in participation and voting, Dr. Tugwell said. Patient participants with severe rheumatoid arthritis no longer faced the challenges of travel. “On the other hand, we didn’t have the same opportunity to achieve common ground virtually,” he said. “Where there are strong disagreements, I’m a great believer that people need to know one another. There needs to be relationship building.”
OMERACT’s emerging leader program has been a cornerstone of its in-person meetings, engaging young rheumatologists to interact with some of the leaders of outcome measurement. The virtual format dampened this process somewhat, eliminating those important “café chats” between the stakeholders.
The hope is to bring people face-to-face once more at the next meeting in May 2023. The agenda will focus on relationship building, identifying controversial areas, and bringing younger people to develop relationships, Dr. Tugwell said. OMERACT will retain a virtual option for the worldwide voting, “which will allow for more buy-in from so many more people,” he added.
A consensus on pain
The onus of developing outcome measures that move with the times is sometimes too great for one group to manage. In 2018, OMERACT became a part of the Red Hat Group (RHG), an organization conceived at the COMET (Core Outcome Measures in Effectiveness Trials) VII meeting in Amsterdam.
RHG aims to improve the choice of outcomes in health research. It includes eight groups: COMET; OMERACT; the Cochrane Skin Core Outcome Set Initiative; Grading of Recommendations, Assessment, Development and Evaluations; Center for Medical Technology Policy; COnsensus-based Standards for the selection of health Measurement Instruments; Clinical Data Interchange Standards Consortium; and Standardized Outcomes in Nephrology.
The collaboration between groups offers a “very interesting interface between consensus building as well as hard evidence,” Dr. Tugwell said. The focus goes beyond rheumatology to other clinical areas of common interest, exploring how one classifies outcome domains in terms of symptoms, life impact, or death.
Pain is an important common denominator that the RHG has evaluated.
“We believe it’s too general. We’re trying to define pain across all Red Hat Groups because it’s clear that the research community has all these different scales for defining pain severity,” Dr. Tugwell said. “We have to find a way to make ruthless decisions and rules for doing it. And of course, it has to be transparent.”
Looking ahead
As part of its ongoing work, OMERACT is evaluating the robustness of instruments that rheumatologists use as outcome measures in clinical trials, which can be a laborious process. The OMERACT Filter 2.0, part of the latest iteration of the handbook, offers strong guidance for researchers but needs a long-term strategy and key methodological support. “To that end, we set up a technical advisory group to help people in the instrument selection work and that remains an ongoing process,” OMERACT leaders said in their joint statement.
OMERACT is looking at opportunities to create benchmark processes for developing core sets outside of rheumatology and a methodology around outcome measures such as contextual factors, composites, and surrogates.
It will also be taking a step back to solicit opinions from the approval agencies represented by the OMERACT membership on the OMERACT handbook.
The goal is to make sure the handbook aligns with everyone else’s approval and labeling requirements.
OMERACT’s patient participants bring important perspectives
OMERACT over the years has sought to become a more patient-centered group. Patients have been involved in OMERACT activities since its sixth meeting, forming an independent, yet integrated, group within the network. They have their own steering committee and produced and helped to update a glossary for OMERACT patients and professionals.
Catherine (McGowan) Hofstetter, who was diagnosed with rheumatoid arthritis 30 years ago, chairs OMERACT’s Patient Research Partners Support Team. In a Q&A, she discussed the importance of patient voices and OMERACT’s plans to further educate and include patients in the dialogue on outcomes.
Question: Have patients always been a part of OMERACT meetings?
Answer: Patients have been involved with OMERACT since 2002. The patient voice adds relevance to all the work that OMERACT does. You can’t begin to talk about outcomes unless there is a patient at the table with lived experience.
Q: Can you cite a few examples of how the patient voice enriches the conversation on outcomes research?
A: Outcomes and priorities that are important to patients are often completely different than those of the clinician. For instance, a work outcome is important to someone who doesn’t have any medical insurance or disability insurance, so that you can ensure that there is food on the table and a roof over your head. Or it may be important to someone because the employment provides medical and disability insurance to provide security for them and their family. These are two different perspectives on work and therefore work priorities and outcomes.
Q: What have been some of the challenges of getting patients to participate?
A: Training patients is one challenge. OMERACT’s work has a very steep learning curve, and while the basics are the same between the groups in terms of looking at what we measure and how we measure it, the nuances of different working groups require a lot of time and energy to be comfortable enough with the work, and then be confident enough to bring your perspective and lived experience to the table. It’s also a very accomplished group, which can be quite intimidating. Self-disclosure is a very personal and intimate undertaking that requires patience, compassion, and respect.
Q: Are there any plans to enhance patient engagement?
A: When we had OMERACT 2020 it was a virtual conference that took place over about 6 months. We had far more patient research partners [PRPs] participate than we have ever had at any OMERACT face-to-face meeting. There is a desire and passion on the part of patients to lend their voices to the work. The working groups meet virtually throughout the year to advance their agendas, and PRPs are a part of each of the working groups.
Hopefully, we can start working toward including more voices at the conferences by enabling a hybrid model. The PRP Support Team will begin engaging patients this fall with education, mentoring, and team-building exercises so by the time we meet in person in May 2023, they will have enough background knowledge and information to give them the confidence that will enhance their experience at the face-to-face meeting.
We also need to ensure that those patients who want to stay engaged can. This means that the education and training should continue long after the face-to-face meeting is over. We need to build capacity in the PRP group and look to succession planning and be a resource to working groups struggling to find PRPs to work with them on a longer-term basis.
Clinical research in rheumatology was suffering from an identity crisis of sorts 40 years ago. A lack of consensus across continents resulted in differing views about clinical outcome measures and judgments about treatments.
Patients were not allowed to be the generating source of a clinical outcome, according to Peter Tugwell, MSc, MD. “The only outcomes that were acceptable were clinician assessments, blood tests, and imaging,” said Dr. Tugwell, professor of medicine, epidemiology, and public health at the University of Ottawa (Ont.) and a practicing rheumatologist at Ottawa Hospital.
Clinicians were coming to different conclusions about patient responses to treatment when managing rheumatoid arthritis in clinical practice.
OMERACT sought to address this lack of uniformity. This international group, formed in 1992, leverages stakeholder groups to improve outcome measurement in rheumatology endpoints through a consensus-building, data-driven format.
It was originally known as “Outcome Measures in Rheumatoid Arthritis Clinical Trials,” but its leaders have since broadened its scope to “Outcome Measures in Rheumatology.” Over the years, it has evolved into an international network that assesses measurement across a wide variety of intervention studies. Now 30 years old, the network spans 40 active working groups and has influenced work in patient outcomes across 500 peer-reviewed publications.
The network meets every 2 years to address what is always a challenging agenda, said Dr. Tugwell, one of its founding members and chair. “There’s lots of strong opinions.” Participating in the discussions are individuals from all stages of seniority in rheumatology and clinical epidemiology, patient research partners, industry, approval agencies, and many countries who are committed to the spirit of OMERACT.
“The secret to our success has been getting world leaders to come together and have those discussions, work them through, and identify common ground in such a way that the approval agencies accept these outcome measures in clinical trials,” he added.
“My impression was the founders perceived a problem in the early 1990s and devised a consensus method in an attempt to quantify clinical parameters to define disease activity in rheumatoid arthritis – an important first step to do clinical trials and allow comparisons between them,” said Patricia Woo, CBE, FMedSci, FRCP, emeritus professor of pediatric rheumatology and previous head of the Centre for Paediatric and Adolescent Rheumatology at UCL, London. At that time, even disease definitions varied between the United States and Europe and other parts of the world, said Dr. Woo, who is not a part of OMERACT. “This was especially true for pediatric rheumatology.”
Fusing the continental divide
OMERACT arose from a need to streamline clinical outcome measures in rheumatology. Research papers during the 1980s demonstrated a lack of coherence in managing patients with rheumatoid arthritis in routine practice. In addition, the measures used to define clinical endpoints in clinical trials operated in silos – they were either too specific to a certain trial, overlapped with other concepts, or didn’t reflect changes in treatment.
Approval agencies in Europe and North America were approving only outcomes measures developed by their respective researchers. This was also true of patients they tested on. “This seemed crazy,” Dr. Tugwell said.
Dr. Tugwell was involved in the Cochrane collaboration, which conducts systematic reviews of best evidence across the world that assesses the magnitude of benefits versus harms.
To achieve this goal, “you need to pull studies from around the world,” he said. Maarten Boers, MD, PhD, a rheumatologist (and later professor of clinical epidemiology at Amsterdam University Medical Center) from the Netherlands, spent a year in Ontario, Canada, to train as a clinical epidemiologist. Together, Dr. Tugwell and Dr. Boers began discussing options to develop more streamlined outcome measures.
They initiated the first OMERACT conference in Maastricht, the Netherlands, in 1992. The Food and Drug Administration and European Medicines Agency participated, along with leaders of outcomes measurement in Europe and in North America.
Discussions centered on methods to develop outcomes in a meaningful fashion. During the first meeting, North American and European approval agencies agreed to accept each other’s studies and endpoints and patient reported outcomes.
Agreement was achieved on a preliminary set of outcome domains and measures that later became known as the WHO-ILAR (World Health Organization–International League of Associations for Rheumatology) core set. The set included seven outcome domains: tender joints, swollen joints, pain, physician global assessment, patient global assessment, physical disability, and acute phase reactants, and one additional outcome domain for studies lasting 1 year or more: radiographs of the joints.
“A proactive program was planned to test not only the validity of these endpoints, but also the methods for their measurement. This was the start of a continuing process,” OMERACT members said in a joint statement for this article. Meetings have since taken place every 2 years.
OMERACT accomplishments
OMERACT now requires buy-in from four continents: Asia, Australia, Europe, and North America.
Its leaders have developed an explicit process for gaining endorsement of core outcome domains and instrument measurement sets. To fully capture the possibilities of “what to measure,” i.e., “measurable aspects of health conditions,” OMERACT has developed a framework of concepts, core areas, and outcome domains. The key concepts are pathophysiology (with a core area termed “manifestations/abnormalities”) and impact (with core areas of “death/lifespan,” and “life impact,” and the optional area of “societal/resource use”). An outcome domain defines an element of a core area to measure the effects of a treatment, such as blood markers, pain intensity, physical function, or emotional well-being.
A core outcome domain set is developed by agreeing to at least one outcome domain within one of the three core areas. Subsequently, a core outcome measurement set is developed by agreeing to at least one applicable measurement instrument for each core outcome domain. This requires documentation of validity, summarized under three metrics: truth, discrimination, and feasibility.
OMERACT’s handbook provides tutelage on establishing and implementing core outcomes, and several workbooks offer guidance on developing core outcome domain sets, selecting instruments for core outcome measurement sets, and OMERACT methodology.
All this work has led to widespread adoption.
Approval agencies have accepted OMERACT’s filter and methods advances, which have been adopted by many research groups in rheumatology and among nonrheumatology research groups. Organizations such as the U.S. National Institutes of Health’s National Institute of Neurological Disorders and Stroke have sought its advice.
Its core outcomes have been adopted and used for approval in the great majority of studies on rheumatoid arthritis, Dr. Tugwell said.
Several BMJ articles underscore the influence and uptake of OMERACT’s core outcome set. One 2017 paper, which analyzed 273 randomized trials of rheumatoid arthritis drug treatments on ClinicalTrials.gov, found that the WHO-ILAR arthritis core outcome set was reported in 81% of the studies. “The adoption of a core outcome set has the potential to increase consistency in outcomes measured across trials and ensure that trials are more likely to measure appropriate outcomes,” the authors concluded.
Since the initial 1992 meeting, OMERACT has broadened its focus from rheumatoid arthritis to 25 other musculoskeletal conditions.
For example, other OMERACT conferences have led to consensus on core sets of measures for osteoarthritis and osteoporosis, psoriasis/psoriatic arthritis, psychosocial measures, and a core set of data for cost-effectiveness evaluations.
‘Speed is a limitation’
OMERACT is a bottom-up volunteer organization. It doesn’t represent any official organization of any clinical society. “We’ve not asked to be adopted by the American College of Rheumatology, EULAR [European Alliance of Associations for Rheumatology], or other international organizations,” Dr. Tugwell said. It offers a chance for patients, users, and doers of research to work together to agree on rigorous criteria accepted by the approval agencies and take the necessary time to work things through.
This is not a fast process, usually taking 4-6 years to initiate and establish an outcome domain set, he emphasized. “It would be beneficial to do it faster if we had the resources to meet every year. The fact is we’re a volunteer organization that meets every 2 years.”
Speed is a limitation, he acknowledged, but it’s an acceptable trade-off for doing things correctly.
The group has faced other challenges during the COVID-19 pandemic, pivoting to a virtual format that had benefits and limitations.
In one respect, moving to a virtual meeting increased uptake in participation and voting, Dr. Tugwell said. Patient participants with severe rheumatoid arthritis no longer faced the challenges of travel. “On the other hand, we didn’t have the same opportunity to achieve common ground virtually,” he said. “Where there are strong disagreements, I’m a great believer that people need to know one another. There needs to be relationship building.”
OMERACT’s emerging leader program has been a cornerstone of its in-person meetings, engaging young rheumatologists to interact with some of the leaders of outcome measurement. The virtual format dampened this process somewhat, eliminating those important “café chats” between the stakeholders.
The hope is to bring people face-to-face once more at the next meeting in May 2023. The agenda will focus on relationship building, identifying controversial areas, and bringing younger people to develop relationships, Dr. Tugwell said. OMERACT will retain a virtual option for the worldwide voting, “which will allow for more buy-in from so many more people,” he added.
A consensus on pain
The onus of developing outcome measures that move with the times is sometimes too great for one group to manage. In 2018, OMERACT became a part of the Red Hat Group (RHG), an organization conceived at the COMET (Core Outcome Measures in Effectiveness Trials) VII meeting in Amsterdam.
RHG aims to improve the choice of outcomes in health research. It includes eight groups: COMET; OMERACT; the Cochrane Skin Core Outcome Set Initiative; Grading of Recommendations, Assessment, Development and Evaluations; Center for Medical Technology Policy; COnsensus-based Standards for the selection of health Measurement Instruments; Clinical Data Interchange Standards Consortium; and Standardized Outcomes in Nephrology.
The collaboration between groups offers a “very interesting interface between consensus building as well as hard evidence,” Dr. Tugwell said. The focus goes beyond rheumatology to other clinical areas of common interest, exploring how one classifies outcome domains in terms of symptoms, life impact, or death.
Pain is an important common denominator that the RHG has evaluated.
“We believe it’s too general. We’re trying to define pain across all Red Hat Groups because it’s clear that the research community has all these different scales for defining pain severity,” Dr. Tugwell said. “We have to find a way to make ruthless decisions and rules for doing it. And of course, it has to be transparent.”
Looking ahead
As part of its ongoing work, OMERACT is evaluating the robustness of instruments that rheumatologists use as outcome measures in clinical trials, which can be a laborious process. The OMERACT Filter 2.0, part of the latest iteration of the handbook, offers strong guidance for researchers but needs a long-term strategy and key methodological support. “To that end, we set up a technical advisory group to help people in the instrument selection work and that remains an ongoing process,” OMERACT leaders said in their joint statement.
OMERACT is looking at opportunities to create benchmark processes for developing core sets outside of rheumatology and a methodology around outcome measures such as contextual factors, composites, and surrogates.
It will also be taking a step back to solicit opinions from the approval agencies represented by the OMERACT membership on the OMERACT handbook.
The goal is to make sure the handbook aligns with everyone else’s approval and labeling requirements.
OMERACT’s patient participants bring important perspectives
OMERACT over the years has sought to become a more patient-centered group. Patients have been involved in OMERACT activities since its sixth meeting, forming an independent, yet integrated, group within the network. They have their own steering committee and produced and helped to update a glossary for OMERACT patients and professionals.
Catherine (McGowan) Hofstetter, who was diagnosed with rheumatoid arthritis 30 years ago, chairs OMERACT’s Patient Research Partners Support Team. In a Q&A, she discussed the importance of patient voices and OMERACT’s plans to further educate and include patients in the dialogue on outcomes.
Question: Have patients always been a part of OMERACT meetings?
Answer: Patients have been involved with OMERACT since 2002. The patient voice adds relevance to all the work that OMERACT does. You can’t begin to talk about outcomes unless there is a patient at the table with lived experience.
Q: Can you cite a few examples of how the patient voice enriches the conversation on outcomes research?
A: Outcomes and priorities that are important to patients are often completely different than those of the clinician. For instance, a work outcome is important to someone who doesn’t have any medical insurance or disability insurance, so that you can ensure that there is food on the table and a roof over your head. Or it may be important to someone because the employment provides medical and disability insurance to provide security for them and their family. These are two different perspectives on work and therefore work priorities and outcomes.
Q: What have been some of the challenges of getting patients to participate?
A: Training patients is one challenge. OMERACT’s work has a very steep learning curve, and while the basics are the same between the groups in terms of looking at what we measure and how we measure it, the nuances of different working groups require a lot of time and energy to be comfortable enough with the work, and then be confident enough to bring your perspective and lived experience to the table. It’s also a very accomplished group, which can be quite intimidating. Self-disclosure is a very personal and intimate undertaking that requires patience, compassion, and respect.
Q: Are there any plans to enhance patient engagement?
A: When we had OMERACT 2020 it was a virtual conference that took place over about 6 months. We had far more patient research partners [PRPs] participate than we have ever had at any OMERACT face-to-face meeting. There is a desire and passion on the part of patients to lend their voices to the work. The working groups meet virtually throughout the year to advance their agendas, and PRPs are a part of each of the working groups.
Hopefully, we can start working toward including more voices at the conferences by enabling a hybrid model. The PRP Support Team will begin engaging patients this fall with education, mentoring, and team-building exercises so by the time we meet in person in May 2023, they will have enough background knowledge and information to give them the confidence that will enhance their experience at the face-to-face meeting.
We also need to ensure that those patients who want to stay engaged can. This means that the education and training should continue long after the face-to-face meeting is over. We need to build capacity in the PRP group and look to succession planning and be a resource to working groups struggling to find PRPs to work with them on a longer-term basis.
How do you live with COVID? One doctor’s personal experience
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”

“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
In America, cancer patients endure debt on top of disease
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Levels of West Nile virus higher than normal in northern Italy
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
How docs in firearm-friendly states talk gun safety
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
High-dose loop diuretic can raise post–cardiac surgery mortality
The study covered in this summary was published on ResearchSquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
- High-dose furosemide after cardiac surgery is associated with increased mortality and other adverse outcomes.
Why this matters
- The influence of furosemide on prognosis after cardiac surgery is not fully understood.
- The current findings suggest that high-dose furosemide after cardiac surgery is associated with increased risk for death and other adverse events and therefore should be used cautiously in that setting.
Study design
- The retrospective cohort of 6,752 cardiac surgery patients was divided into two groups according to average daily furosemide dosage after cardiac surgery: less than 20 mg (low-dose group, n = 6,033) and at least 20 mg (high-dose group, n = 719).
- The group were compared for total furosemide dose, total furosemide dose of at least 200 mg, total dose of furosemide by patient weight, and average daily furosemide dose of at least 20 mg.
- The primary outcomes were in-hospital mortality and mortality at 1 year after cardiac surgery. Secondary outcomes were length of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours.
- The study excluded patients aged younger than 18 whose weight data was missing or who had more than 5% of their data missing.
Key results
- Patients in the high-dose furosemide group tended to be older and have a higher body mass index (BMI) and higher rates of diabetes, chronic pulmonary diseases, heart failure, renal failure, blood transfusion, vasopressor use, and valvular surgery.
- They also tended have higher white cell counts and higher levels of blood urea nitrogen, creatinine, glucose, and lactate.
- Those in the high-dose group also were on vasopressors and ventilatory support longer.
- In adjusted multivariate analysis, increased in-hospital mortality was associated with average daily furosemide dose, average daily dose of at least 20 mg/d, and total dose of at least 200 mg.
- Increased mortality at 1 year was associated with total furosemide dose and average daily furosemide dose.
- Significant multivariate predictors of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours after cardiac surgery included total furosemide dose, total dose by weight, average daily furosemide dose of at least 20 mg/d, and total dose of at least 200 mg.
- In subgroup analyses, average daily furosemide dose of at least 20 mg/d significantly increased risk for in-hospital mortality among patients younger than 60 years or with BMI of at least 28 who received vasopressors or blood transfusions, those with renal failure, and those with heart failure not involving congestion.
Limitations
- No limitations were discussed.
Disclosures
- The study was supported by grants from the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Jiangsu Postdoctoral Science Foundation.
- The authors declared that they have no competing interests.
This is a summary of a preprint research study, “Association between furosemide administration and outcomes in patients undergoing cardiac surgery,” from Jinghang Li, First Affiliated Hospital of Nanjing (China) Medical University, and colleagues on published on ResearchSquare.com. This study has not yet been peer reviewed. The full text of the study can be found on ResearchSquare.com. A version of this article first appeared on Medscape.com.
The study covered in this summary was published on ResearchSquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
- High-dose furosemide after cardiac surgery is associated with increased mortality and other adverse outcomes.
Why this matters
- The influence of furosemide on prognosis after cardiac surgery is not fully understood.
- The current findings suggest that high-dose furosemide after cardiac surgery is associated with increased risk for death and other adverse events and therefore should be used cautiously in that setting.
Study design
- The retrospective cohort of 6,752 cardiac surgery patients was divided into two groups according to average daily furosemide dosage after cardiac surgery: less than 20 mg (low-dose group, n = 6,033) and at least 20 mg (high-dose group, n = 719).
- The group were compared for total furosemide dose, total furosemide dose of at least 200 mg, total dose of furosemide by patient weight, and average daily furosemide dose of at least 20 mg.
- The primary outcomes were in-hospital mortality and mortality at 1 year after cardiac surgery. Secondary outcomes were length of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours.
- The study excluded patients aged younger than 18 whose weight data was missing or who had more than 5% of their data missing.
Key results
- Patients in the high-dose furosemide group tended to be older and have a higher body mass index (BMI) and higher rates of diabetes, chronic pulmonary diseases, heart failure, renal failure, blood transfusion, vasopressor use, and valvular surgery.
- They also tended have higher white cell counts and higher levels of blood urea nitrogen, creatinine, glucose, and lactate.
- Those in the high-dose group also were on vasopressors and ventilatory support longer.
- In adjusted multivariate analysis, increased in-hospital mortality was associated with average daily furosemide dose, average daily dose of at least 20 mg/d, and total dose of at least 200 mg.
- Increased mortality at 1 year was associated with total furosemide dose and average daily furosemide dose.
- Significant multivariate predictors of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours after cardiac surgery included total furosemide dose, total dose by weight, average daily furosemide dose of at least 20 mg/d, and total dose of at least 200 mg.
- In subgroup analyses, average daily furosemide dose of at least 20 mg/d significantly increased risk for in-hospital mortality among patients younger than 60 years or with BMI of at least 28 who received vasopressors or blood transfusions, those with renal failure, and those with heart failure not involving congestion.
Limitations
- No limitations were discussed.
Disclosures
- The study was supported by grants from the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Jiangsu Postdoctoral Science Foundation.
- The authors declared that they have no competing interests.
This is a summary of a preprint research study, “Association between furosemide administration and outcomes in patients undergoing cardiac surgery,” from Jinghang Li, First Affiliated Hospital of Nanjing (China) Medical University, and colleagues on published on ResearchSquare.com. This study has not yet been peer reviewed. The full text of the study can be found on ResearchSquare.com. A version of this article first appeared on Medscape.com.
The study covered in this summary was published on ResearchSquare.com as a preprint and has not yet been peer reviewed.
Key takeaway
- High-dose furosemide after cardiac surgery is associated with increased mortality and other adverse outcomes.
Why this matters
- The influence of furosemide on prognosis after cardiac surgery is not fully understood.
- The current findings suggest that high-dose furosemide after cardiac surgery is associated with increased risk for death and other adverse events and therefore should be used cautiously in that setting.
Study design
- The retrospective cohort of 6,752 cardiac surgery patients was divided into two groups according to average daily furosemide dosage after cardiac surgery: less than 20 mg (low-dose group, n = 6,033) and at least 20 mg (high-dose group, n = 719).
- The group were compared for total furosemide dose, total furosemide dose of at least 200 mg, total dose of furosemide by patient weight, and average daily furosemide dose of at least 20 mg.
- The primary outcomes were in-hospital mortality and mortality at 1 year after cardiac surgery. Secondary outcomes were length of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours.
- The study excluded patients aged younger than 18 whose weight data was missing or who had more than 5% of their data missing.
Key results
- Patients in the high-dose furosemide group tended to be older and have a higher body mass index (BMI) and higher rates of diabetes, chronic pulmonary diseases, heart failure, renal failure, blood transfusion, vasopressor use, and valvular surgery.
- They also tended have higher white cell counts and higher levels of blood urea nitrogen, creatinine, glucose, and lactate.
- Those in the high-dose group also were on vasopressors and ventilatory support longer.
- In adjusted multivariate analysis, increased in-hospital mortality was associated with average daily furosemide dose, average daily dose of at least 20 mg/d, and total dose of at least 200 mg.
- Increased mortality at 1 year was associated with total furosemide dose and average daily furosemide dose.
- Significant multivariate predictors of hospital stay of at least 14 days, length of ICU stay of at least 3 days, and mechanical ventilation for at least 48 hours after cardiac surgery included total furosemide dose, total dose by weight, average daily furosemide dose of at least 20 mg/d, and total dose of at least 200 mg.
- In subgroup analyses, average daily furosemide dose of at least 20 mg/d significantly increased risk for in-hospital mortality among patients younger than 60 years or with BMI of at least 28 who received vasopressors or blood transfusions, those with renal failure, and those with heart failure not involving congestion.
Limitations
- No limitations were discussed.
Disclosures
- The study was supported by grants from the National Natural Science Foundation of China, China Postdoctoral Science Foundation, and Jiangsu Postdoctoral Science Foundation.
- The authors declared that they have no competing interests.
This is a summary of a preprint research study, “Association between furosemide administration and outcomes in patients undergoing cardiac surgery,” from Jinghang Li, First Affiliated Hospital of Nanjing (China) Medical University, and colleagues on published on ResearchSquare.com. This study has not yet been peer reviewed. The full text of the study can be found on ResearchSquare.com. A version of this article first appeared on Medscape.com.
State of the science in PCOS: Emerging neuroendocrine involvement driving research
Polycystic ovary syndrome (PCOS) affects an estimated 8%-13% of women, and yet “it has been quite a black box for many years,” as Margo Hudson, MD, an assistant professor of endocrinology, diabetes, and hypertension at Harvard Medical School, Boston, puts it. That black box encompasses not only uncertainty about the etiology and pathophysiology of the condition but even what constitutes a diagnosis.
Even the international guidelines on PCOS management endorsed by the American Society for Reproductive Medicine – a document developed over 15 months with the input of 37 medical organizations covering 71 countries – notes that PCOS diagnosis is “controversial and assessment and management are inconsistent.” The result, the guidelines note, is that “the needs of women with PCOS are not being adequately met.”
One of the earliest diagnostic criteria, defined in 1990 by the National Institutes of Health, required only hyperandrogenism and irregular menstruation. Then the 2003 Rotterdam Criteria added presence of polycystic ovaries on ultrasound as a third criterion. Then the Androgen Excess Society determined that PCOS required presence of hyperandrogenism with either polycystic ovaries or oligo/amenorrhea anovulation. Yet the Endocrine Society notes that excess androgen levels are seen in 60%-80% of those with PCOS, suggesting it’s not an essential requirement for diagnosis, leaving most to diagnose it in people who have two of the three key criteria. The only real agreement on diagnosis is the need to eliminate other potential diagnoses first, making PCOS always a diagnosis of exclusion.
Further, though PCOS is known as the leading cause of infertility in women, it is more than a reproductive condition, with metabolic and psychological features as well. Then there is the range of comorbidities, none of which occur in all patients with PCOS but all of which occur in a majority and which are themselves interrelated. Insulin resistance is a common feature, occurring in 50%-70% of people with PCOS. Accordingly, metabolic syndrome occurs in at least a third of people with PCOS and type 2 diabetes prevalence is higher in those with PCOS as well.
Obesity occurs in an estimated 80% of women with PCOS in the United States, though it affects only about 50% of women with PCOS outside the United States, and those with PCOS have an increased risk of hypertension. Mood disorders, particularly anxiety and depression but also, to a lesser extent, bipolar disorder and obsessive-compulsive disorder, are more likely in people with PCOS. And given that these comorbidities are all cardiovascular risk factors, it’s unsurprising that recent studies are finding those with PCOS to be at greater risk for cardiometabolic disease and major cardiovascular events.
“The reality is that PCOS is a heterogenous entity. It’s not one thing – it’s a syndrome,” Lubna Pal, MBBS, a professor of ob.gyn. and director of the PCOS Program at Yale University, New Haven, Conn., said in an interview. A whole host of factors are likely playing a role in the causes of PCOS, and those factors interact differently within different people. “We’re looking at things like lipid metabolism, fetal origins, the gut microbiome, genetics, epigenetics, and then dietary and environmental factors,” Nichole Tyson, MD, division chief of pediatric and adolescent gynecology and a clinical associate professor at Stanford (Calif.) Medicine Children’s Health, said in an interview. And most studies have identified associations that may or may not be causal. Take, for example, endocrine disruptors. BPA levels have been shown to be higher in women with PCOS than women without, but that correlation may or may not be related to the etiology of the condition.
The hypothalamic-pituitary-gonadal axis
In trying to understand the pathophysiology of the condition, much of the latest research has zeroed in on potential mechanisms in the hypothalamic-pituitary-gonadal axis. “A consistent feature of PCOS is disordered gonadotropin secretion with elevated mean LH [luteinizing hormone], low or low normal FSH [follicle-stimulating hormone], and a persistently rapid frequency of GnRH [gonadotropin-releasing hormone] pulse secretion,” wrote authors of a scientific statement on aspects of PCOS.
“I think the balance is heading more to central neurologic control of the reproductive system and that disturbances there impact the GnRH cells in the hypothalamus, which then go on to give us the findings that we can measure peripherally with the LH-FSH ratio,” Dr. Hudson said in an interview.
The increased LH levels are thought to be a major driver of increased androgen levels. Current thinking suggests that the primary driver of increased LH is GnRH pulsatility, supported not only by human studies but by animal models as well. This leads to the question of what drives GnRH dysregulation. One hypothesis posits that GABA neurons play a role here, given findings that GABA levels in cerebrospinal fluid were higher in women with PCOS than those with normal ovulation.
But the culprit garnering the most attention is kisspeptin, a protein encoded by the KISS1 gene that stimulates GnRH neurons and has been linked to regulation of LH and FSH secretion. Kisspeptin, along with neurokinin B and dynorphin, is part of the triumvirate that comprises KNDy neurons, also recently implicated in menopausal vasomotor symptoms. Multiple systematic reviewsand meta-analyses have found a correlation between higher kisspeptin levels in the blood and higher circulating LH levels, regardless of body mass index. While kisspeptin is expressed in several tissues, including liver, pancreas, gonad, and adipose, it’s neural kisspeptin signaling that appears most likely to play a role in activating GnRH hormones and disrupting normal function of the hypothalamic-pituitary-gonadal axis.
But as noted, in at least one systematic review of kisspeptin and PCOS, “findings from animal studies suggest that kisspeptin levels are not increased in all subtypes of PCOS.” And another review found “altered” levels of kisspeptin levels in non-PCOS patients who had obesity, potentially raising questions about any associations between kisspeptin and obesity or insulin resistance.
Remaining chicken-and-egg questions
A hallmark of PCOS has long been, and continues to be, the string of chicken-or-egg questions that plague understanding of it. One of these is how depression and anxiety fit into the etiology of PCOS. Exploring the role of specific neurons that may overstimulate GnRH pulsatility may hold clues to a common underlying mechanism for the involvement of depression and anxiety in patients with PCOS, Dr. Hudson speculated. While previous assumptions often attributed depression and anxiety in PCOS to the symptoms – such as thin scalp hair and increased facial hair, excess weight, acne, and irregular periods – Dr. Hudson pointed out that women can address many of these symptoms with laser hair removal, weight loss, acne treatment, and similar interventions, yet they still have a lot of underlying mental health issues.
It’s also unclear whether metabolic factors so common with PCOS, particularly insulin resistance and obesity, are a result of the condition or are contributors to it. Is insulin resistance contributing to dysregulation in the neurons that interferes with normal functioning of the hypothalamic-pituitary-adrenal axis? Is abnormal functioning along this axis contributing to insulin resistance? Or neither? Or both? Or does it depend? The authors of one paper wrote that “insulin may play both direct and indirect roles in the pathogenesis of androgen excess in PCOS,” since insulin can “stimulate ovarian androgen production” and “enhance ovarian growth and follicular cyst formation in rats.”
Dr. Pal noted that “obesity itself can evolve into a PCOS-like picture,” raising questions about whether obesity or insulin resistance might be part of the causal pathway to PCOS, or whether either can trigger its development in those genetically predisposed.
“Obesity does appear to exacerbate many aspects of the PCOS phenotype, particularly those risk factors related to metabolic syndrome,” wrote the authors of a scientific statement on aspects of PCOS, but they add that “it is currently debated whether obesity per se can cause PCOS.” While massive weight loss in those with PCOS and obesity has improved multiple reproductive and metabolic issues, it hasn’t resolved all of them, they write.
Dr. Hudson said she expects there’s “some degree of appetite dysregulation and metabolic dysregulation” that contributes, but then there are other women who don’t have much of an appetite or overeat and still struggle with their weight. Evidence has also found insulin resistance in women of normal weight with PCOS. “There may be some kind of metabolic dysregulation that they have at some level, and others are clearly bothered by overeating,” Dr. Hudson said.
Similarly, it’s not clear whether the recent discovery of increased cardiovascular risks in people with PCOS is a result of the comorbidities so common with PCOS, such as obesity, or whether an underlying mechanism links the cardiovascular risk and the dysregulation of hormones. Dr. Pal would argue that, again, it’s probably both, depending on the patient.
Then there is the key feature of hyperandrogenemia. “An outstanding debate is whether the elevated androgens in PCOS women are merely a downstream endocrine response to hyperactive GnRH and LH secretion driving the ovary, or do the elevated androgens themselves act in the brain (or pituitary) during development and/or adulthood to sculpt and maintain the hypersecretion of GnRH and LH?” wrote Eulalia A. Coutinho, PhD, and Alexander S. Kauffman, PhD, in a 2019 review of the brain’s role in PCOS.
These problems may be bidirectional or part of various feedback loops. Sleep apnea is more common in people with PCOS, Dr. Tyson noted, but sleep apnea is also linked to cardiovascular, metabolic, and depression risks, and depression can play a role in obesity, which increases the risk of obstructive sleep apnea. “So you’re in this vicious cycle,” Dr. Tyson said. That’s why she also believes it’s important to change the dialogue and perspective on PCOS, to reduce the stigma attached to it, and work with patients to empower them in treating its symptoms and reducing their risk of comorbidities.
Recent and upcoming changes in treatment
Current treatment of PCOS already changes according to the symptoms posing the greatest problems at each stage of a person’s life, Dr. Hudson said. Younger women tend to be more bothered about the cosmetic effects of PCOS, including hair growth patterns and acne, but as they grow out of adolescence and into their 20s and 30s, infertility becomes a bigger concern for many. Then, as they start approaching menopause, metabolic and cardiovascular issues take the lead, with more of a focus on lipids, diabetes risk, and heart health.
In some ways, management of PCOS hasn’t changed much in the past several decades, except in an increased awareness of the metabolic and cardiovascular risks, which has led to more frequent screening to catch potential conditions earlier in life. What has changed, however, is improvements in the treatments used for symptoms, such as expanded bariatric surgery options and GLP-1 agonists for treating obesity. Other examples include better options for menstrual management, such as new progesterone IUDs, and optimized fertility treatments, Dr. Tyson said.
“I think with more of these large-scale studies about the pathophysiology of PCOS and how it may look in different people and the different outcomes, we may be able to tailor our treatments even further,” Dr. Tyson said. She emphasized the importance of identifying the condition early, particularly in adolescents, even if it’s identifying young people at risk for the condition rather than actually having it yet.
Early identification “gives us this chance to do a lot of preventative care and motivate older teens to have a great lifestyle, work on their diet and exercise, and manage cardiovascular” risk factors, Dr. Tyson said.
“What we do know and recognize is that there’s so many spokes to this PCOS wheel that there really should be a multidisciplinary approach to care,” Dr. Tyson said. “When I think about who would be the real doctors for patients with PCOS, these would be gynecologists, endocrinologists, dermatologists, nutritionists, psychologists, sleep specialists, and primary care at a minimum.”
Dr. Pal worries that the label of PCOS leaves it in the laps of ob.gyns. whereas, “if it was called something else, everybody would be involved in being vigilant and managing those patients.” She frequently reiterated that the label of PCOS is less important than ensuring clinicians treat the symptoms that most bother the patient.
And even if kisspeptin does play a causal role in PCOS for some patients, it’s only a subset of individuals with PCOS who would benefit from therapies developed to target it. Given the complexity of the syndrome and its many manifestations, a “galaxy of pathways” are involved in different potential subtypes of the condition. “You can’t treat PCOS as one entity,” Dr. Pal said.
Still, Dr. Hudson is optimistic that the research into potential neuroendocrine contributions to PCOS will yield therapies that go beyond just managing symptoms.
“There aren’t a lot of treatments available yet, but there may be some on the horizon,” Dr. Hudson said. “We’re still in this very primitive stage in terms of therapeutics, where we’re only addressing specific symptoms, and we haven’t been able to really address the underlying cause because we haven’t understood it as well and because we don’t have therapies that can target it,” Dr. Hudson said. “But once there are therapies developed that will target some of these central mechanisms, I think it will change completely the approach to treating PCOS for patients.”
This story was updated on Sept. 6, 2022.
Polycystic ovary syndrome (PCOS) affects an estimated 8%-13% of women, and yet “it has been quite a black box for many years,” as Margo Hudson, MD, an assistant professor of endocrinology, diabetes, and hypertension at Harvard Medical School, Boston, puts it. That black box encompasses not only uncertainty about the etiology and pathophysiology of the condition but even what constitutes a diagnosis.
Even the international guidelines on PCOS management endorsed by the American Society for Reproductive Medicine – a document developed over 15 months with the input of 37 medical organizations covering 71 countries – notes that PCOS diagnosis is “controversial and assessment and management are inconsistent.” The result, the guidelines note, is that “the needs of women with PCOS are not being adequately met.”
One of the earliest diagnostic criteria, defined in 1990 by the National Institutes of Health, required only hyperandrogenism and irregular menstruation. Then the 2003 Rotterdam Criteria added presence of polycystic ovaries on ultrasound as a third criterion. Then the Androgen Excess Society determined that PCOS required presence of hyperandrogenism with either polycystic ovaries or oligo/amenorrhea anovulation. Yet the Endocrine Society notes that excess androgen levels are seen in 60%-80% of those with PCOS, suggesting it’s not an essential requirement for diagnosis, leaving most to diagnose it in people who have two of the three key criteria. The only real agreement on diagnosis is the need to eliminate other potential diagnoses first, making PCOS always a diagnosis of exclusion.
Further, though PCOS is known as the leading cause of infertility in women, it is more than a reproductive condition, with metabolic and psychological features as well. Then there is the range of comorbidities, none of which occur in all patients with PCOS but all of which occur in a majority and which are themselves interrelated. Insulin resistance is a common feature, occurring in 50%-70% of people with PCOS. Accordingly, metabolic syndrome occurs in at least a third of people with PCOS and type 2 diabetes prevalence is higher in those with PCOS as well.
Obesity occurs in an estimated 80% of women with PCOS in the United States, though it affects only about 50% of women with PCOS outside the United States, and those with PCOS have an increased risk of hypertension. Mood disorders, particularly anxiety and depression but also, to a lesser extent, bipolar disorder and obsessive-compulsive disorder, are more likely in people with PCOS. And given that these comorbidities are all cardiovascular risk factors, it’s unsurprising that recent studies are finding those with PCOS to be at greater risk for cardiometabolic disease and major cardiovascular events.
“The reality is that PCOS is a heterogenous entity. It’s not one thing – it’s a syndrome,” Lubna Pal, MBBS, a professor of ob.gyn. and director of the PCOS Program at Yale University, New Haven, Conn., said in an interview. A whole host of factors are likely playing a role in the causes of PCOS, and those factors interact differently within different people. “We’re looking at things like lipid metabolism, fetal origins, the gut microbiome, genetics, epigenetics, and then dietary and environmental factors,” Nichole Tyson, MD, division chief of pediatric and adolescent gynecology and a clinical associate professor at Stanford (Calif.) Medicine Children’s Health, said in an interview. And most studies have identified associations that may or may not be causal. Take, for example, endocrine disruptors. BPA levels have been shown to be higher in women with PCOS than women without, but that correlation may or may not be related to the etiology of the condition.
The hypothalamic-pituitary-gonadal axis
In trying to understand the pathophysiology of the condition, much of the latest research has zeroed in on potential mechanisms in the hypothalamic-pituitary-gonadal axis. “A consistent feature of PCOS is disordered gonadotropin secretion with elevated mean LH [luteinizing hormone], low or low normal FSH [follicle-stimulating hormone], and a persistently rapid frequency of GnRH [gonadotropin-releasing hormone] pulse secretion,” wrote authors of a scientific statement on aspects of PCOS.
“I think the balance is heading more to central neurologic control of the reproductive system and that disturbances there impact the GnRH cells in the hypothalamus, which then go on to give us the findings that we can measure peripherally with the LH-FSH ratio,” Dr. Hudson said in an interview.
The increased LH levels are thought to be a major driver of increased androgen levels. Current thinking suggests that the primary driver of increased LH is GnRH pulsatility, supported not only by human studies but by animal models as well. This leads to the question of what drives GnRH dysregulation. One hypothesis posits that GABA neurons play a role here, given findings that GABA levels in cerebrospinal fluid were higher in women with PCOS than those with normal ovulation.
But the culprit garnering the most attention is kisspeptin, a protein encoded by the KISS1 gene that stimulates GnRH neurons and has been linked to regulation of LH and FSH secretion. Kisspeptin, along with neurokinin B and dynorphin, is part of the triumvirate that comprises KNDy neurons, also recently implicated in menopausal vasomotor symptoms. Multiple systematic reviewsand meta-analyses have found a correlation between higher kisspeptin levels in the blood and higher circulating LH levels, regardless of body mass index. While kisspeptin is expressed in several tissues, including liver, pancreas, gonad, and adipose, it’s neural kisspeptin signaling that appears most likely to play a role in activating GnRH hormones and disrupting normal function of the hypothalamic-pituitary-gonadal axis.
But as noted, in at least one systematic review of kisspeptin and PCOS, “findings from animal studies suggest that kisspeptin levels are not increased in all subtypes of PCOS.” And another review found “altered” levels of kisspeptin levels in non-PCOS patients who had obesity, potentially raising questions about any associations between kisspeptin and obesity or insulin resistance.
Remaining chicken-and-egg questions
A hallmark of PCOS has long been, and continues to be, the string of chicken-or-egg questions that plague understanding of it. One of these is how depression and anxiety fit into the etiology of PCOS. Exploring the role of specific neurons that may overstimulate GnRH pulsatility may hold clues to a common underlying mechanism for the involvement of depression and anxiety in patients with PCOS, Dr. Hudson speculated. While previous assumptions often attributed depression and anxiety in PCOS to the symptoms – such as thin scalp hair and increased facial hair, excess weight, acne, and irregular periods – Dr. Hudson pointed out that women can address many of these symptoms with laser hair removal, weight loss, acne treatment, and similar interventions, yet they still have a lot of underlying mental health issues.
It’s also unclear whether metabolic factors so common with PCOS, particularly insulin resistance and obesity, are a result of the condition or are contributors to it. Is insulin resistance contributing to dysregulation in the neurons that interferes with normal functioning of the hypothalamic-pituitary-adrenal axis? Is abnormal functioning along this axis contributing to insulin resistance? Or neither? Or both? Or does it depend? The authors of one paper wrote that “insulin may play both direct and indirect roles in the pathogenesis of androgen excess in PCOS,” since insulin can “stimulate ovarian androgen production” and “enhance ovarian growth and follicular cyst formation in rats.”
Dr. Pal noted that “obesity itself can evolve into a PCOS-like picture,” raising questions about whether obesity or insulin resistance might be part of the causal pathway to PCOS, or whether either can trigger its development in those genetically predisposed.
“Obesity does appear to exacerbate many aspects of the PCOS phenotype, particularly those risk factors related to metabolic syndrome,” wrote the authors of a scientific statement on aspects of PCOS, but they add that “it is currently debated whether obesity per se can cause PCOS.” While massive weight loss in those with PCOS and obesity has improved multiple reproductive and metabolic issues, it hasn’t resolved all of them, they write.
Dr. Hudson said she expects there’s “some degree of appetite dysregulation and metabolic dysregulation” that contributes, but then there are other women who don’t have much of an appetite or overeat and still struggle with their weight. Evidence has also found insulin resistance in women of normal weight with PCOS. “There may be some kind of metabolic dysregulation that they have at some level, and others are clearly bothered by overeating,” Dr. Hudson said.
Similarly, it’s not clear whether the recent discovery of increased cardiovascular risks in people with PCOS is a result of the comorbidities so common with PCOS, such as obesity, or whether an underlying mechanism links the cardiovascular risk and the dysregulation of hormones. Dr. Pal would argue that, again, it’s probably both, depending on the patient.
Then there is the key feature of hyperandrogenemia. “An outstanding debate is whether the elevated androgens in PCOS women are merely a downstream endocrine response to hyperactive GnRH and LH secretion driving the ovary, or do the elevated androgens themselves act in the brain (or pituitary) during development and/or adulthood to sculpt and maintain the hypersecretion of GnRH and LH?” wrote Eulalia A. Coutinho, PhD, and Alexander S. Kauffman, PhD, in a 2019 review of the brain’s role in PCOS.
These problems may be bidirectional or part of various feedback loops. Sleep apnea is more common in people with PCOS, Dr. Tyson noted, but sleep apnea is also linked to cardiovascular, metabolic, and depression risks, and depression can play a role in obesity, which increases the risk of obstructive sleep apnea. “So you’re in this vicious cycle,” Dr. Tyson said. That’s why she also believes it’s important to change the dialogue and perspective on PCOS, to reduce the stigma attached to it, and work with patients to empower them in treating its symptoms and reducing their risk of comorbidities.
Recent and upcoming changes in treatment
Current treatment of PCOS already changes according to the symptoms posing the greatest problems at each stage of a person’s life, Dr. Hudson said. Younger women tend to be more bothered about the cosmetic effects of PCOS, including hair growth patterns and acne, but as they grow out of adolescence and into their 20s and 30s, infertility becomes a bigger concern for many. Then, as they start approaching menopause, metabolic and cardiovascular issues take the lead, with more of a focus on lipids, diabetes risk, and heart health.
In some ways, management of PCOS hasn’t changed much in the past several decades, except in an increased awareness of the metabolic and cardiovascular risks, which has led to more frequent screening to catch potential conditions earlier in life. What has changed, however, is improvements in the treatments used for symptoms, such as expanded bariatric surgery options and GLP-1 agonists for treating obesity. Other examples include better options for menstrual management, such as new progesterone IUDs, and optimized fertility treatments, Dr. Tyson said.
“I think with more of these large-scale studies about the pathophysiology of PCOS and how it may look in different people and the different outcomes, we may be able to tailor our treatments even further,” Dr. Tyson said. She emphasized the importance of identifying the condition early, particularly in adolescents, even if it’s identifying young people at risk for the condition rather than actually having it yet.
Early identification “gives us this chance to do a lot of preventative care and motivate older teens to have a great lifestyle, work on their diet and exercise, and manage cardiovascular” risk factors, Dr. Tyson said.
“What we do know and recognize is that there’s so many spokes to this PCOS wheel that there really should be a multidisciplinary approach to care,” Dr. Tyson said. “When I think about who would be the real doctors for patients with PCOS, these would be gynecologists, endocrinologists, dermatologists, nutritionists, psychologists, sleep specialists, and primary care at a minimum.”
Dr. Pal worries that the label of PCOS leaves it in the laps of ob.gyns. whereas, “if it was called something else, everybody would be involved in being vigilant and managing those patients.” She frequently reiterated that the label of PCOS is less important than ensuring clinicians treat the symptoms that most bother the patient.
And even if kisspeptin does play a causal role in PCOS for some patients, it’s only a subset of individuals with PCOS who would benefit from therapies developed to target it. Given the complexity of the syndrome and its many manifestations, a “galaxy of pathways” are involved in different potential subtypes of the condition. “You can’t treat PCOS as one entity,” Dr. Pal said.
Still, Dr. Hudson is optimistic that the research into potential neuroendocrine contributions to PCOS will yield therapies that go beyond just managing symptoms.
“There aren’t a lot of treatments available yet, but there may be some on the horizon,” Dr. Hudson said. “We’re still in this very primitive stage in terms of therapeutics, where we’re only addressing specific symptoms, and we haven’t been able to really address the underlying cause because we haven’t understood it as well and because we don’t have therapies that can target it,” Dr. Hudson said. “But once there are therapies developed that will target some of these central mechanisms, I think it will change completely the approach to treating PCOS for patients.”
This story was updated on Sept. 6, 2022.
Polycystic ovary syndrome (PCOS) affects an estimated 8%-13% of women, and yet “it has been quite a black box for many years,” as Margo Hudson, MD, an assistant professor of endocrinology, diabetes, and hypertension at Harvard Medical School, Boston, puts it. That black box encompasses not only uncertainty about the etiology and pathophysiology of the condition but even what constitutes a diagnosis.
Even the international guidelines on PCOS management endorsed by the American Society for Reproductive Medicine – a document developed over 15 months with the input of 37 medical organizations covering 71 countries – notes that PCOS diagnosis is “controversial and assessment and management are inconsistent.” The result, the guidelines note, is that “the needs of women with PCOS are not being adequately met.”
One of the earliest diagnostic criteria, defined in 1990 by the National Institutes of Health, required only hyperandrogenism and irregular menstruation. Then the 2003 Rotterdam Criteria added presence of polycystic ovaries on ultrasound as a third criterion. Then the Androgen Excess Society determined that PCOS required presence of hyperandrogenism with either polycystic ovaries or oligo/amenorrhea anovulation. Yet the Endocrine Society notes that excess androgen levels are seen in 60%-80% of those with PCOS, suggesting it’s not an essential requirement for diagnosis, leaving most to diagnose it in people who have two of the three key criteria. The only real agreement on diagnosis is the need to eliminate other potential diagnoses first, making PCOS always a diagnosis of exclusion.
Further, though PCOS is known as the leading cause of infertility in women, it is more than a reproductive condition, with metabolic and psychological features as well. Then there is the range of comorbidities, none of which occur in all patients with PCOS but all of which occur in a majority and which are themselves interrelated. Insulin resistance is a common feature, occurring in 50%-70% of people with PCOS. Accordingly, metabolic syndrome occurs in at least a third of people with PCOS and type 2 diabetes prevalence is higher in those with PCOS as well.
Obesity occurs in an estimated 80% of women with PCOS in the United States, though it affects only about 50% of women with PCOS outside the United States, and those with PCOS have an increased risk of hypertension. Mood disorders, particularly anxiety and depression but also, to a lesser extent, bipolar disorder and obsessive-compulsive disorder, are more likely in people with PCOS. And given that these comorbidities are all cardiovascular risk factors, it’s unsurprising that recent studies are finding those with PCOS to be at greater risk for cardiometabolic disease and major cardiovascular events.
“The reality is that PCOS is a heterogenous entity. It’s not one thing – it’s a syndrome,” Lubna Pal, MBBS, a professor of ob.gyn. and director of the PCOS Program at Yale University, New Haven, Conn., said in an interview. A whole host of factors are likely playing a role in the causes of PCOS, and those factors interact differently within different people. “We’re looking at things like lipid metabolism, fetal origins, the gut microbiome, genetics, epigenetics, and then dietary and environmental factors,” Nichole Tyson, MD, division chief of pediatric and adolescent gynecology and a clinical associate professor at Stanford (Calif.) Medicine Children’s Health, said in an interview. And most studies have identified associations that may or may not be causal. Take, for example, endocrine disruptors. BPA levels have been shown to be higher in women with PCOS than women without, but that correlation may or may not be related to the etiology of the condition.
The hypothalamic-pituitary-gonadal axis
In trying to understand the pathophysiology of the condition, much of the latest research has zeroed in on potential mechanisms in the hypothalamic-pituitary-gonadal axis. “A consistent feature of PCOS is disordered gonadotropin secretion with elevated mean LH [luteinizing hormone], low or low normal FSH [follicle-stimulating hormone], and a persistently rapid frequency of GnRH [gonadotropin-releasing hormone] pulse secretion,” wrote authors of a scientific statement on aspects of PCOS.
“I think the balance is heading more to central neurologic control of the reproductive system and that disturbances there impact the GnRH cells in the hypothalamus, which then go on to give us the findings that we can measure peripherally with the LH-FSH ratio,” Dr. Hudson said in an interview.
The increased LH levels are thought to be a major driver of increased androgen levels. Current thinking suggests that the primary driver of increased LH is GnRH pulsatility, supported not only by human studies but by animal models as well. This leads to the question of what drives GnRH dysregulation. One hypothesis posits that GABA neurons play a role here, given findings that GABA levels in cerebrospinal fluid were higher in women with PCOS than those with normal ovulation.
But the culprit garnering the most attention is kisspeptin, a protein encoded by the KISS1 gene that stimulates GnRH neurons and has been linked to regulation of LH and FSH secretion. Kisspeptin, along with neurokinin B and dynorphin, is part of the triumvirate that comprises KNDy neurons, also recently implicated in menopausal vasomotor symptoms. Multiple systematic reviewsand meta-analyses have found a correlation between higher kisspeptin levels in the blood and higher circulating LH levels, regardless of body mass index. While kisspeptin is expressed in several tissues, including liver, pancreas, gonad, and adipose, it’s neural kisspeptin signaling that appears most likely to play a role in activating GnRH hormones and disrupting normal function of the hypothalamic-pituitary-gonadal axis.
But as noted, in at least one systematic review of kisspeptin and PCOS, “findings from animal studies suggest that kisspeptin levels are not increased in all subtypes of PCOS.” And another review found “altered” levels of kisspeptin levels in non-PCOS patients who had obesity, potentially raising questions about any associations between kisspeptin and obesity or insulin resistance.
Remaining chicken-and-egg questions
A hallmark of PCOS has long been, and continues to be, the string of chicken-or-egg questions that plague understanding of it. One of these is how depression and anxiety fit into the etiology of PCOS. Exploring the role of specific neurons that may overstimulate GnRH pulsatility may hold clues to a common underlying mechanism for the involvement of depression and anxiety in patients with PCOS, Dr. Hudson speculated. While previous assumptions often attributed depression and anxiety in PCOS to the symptoms – such as thin scalp hair and increased facial hair, excess weight, acne, and irregular periods – Dr. Hudson pointed out that women can address many of these symptoms with laser hair removal, weight loss, acne treatment, and similar interventions, yet they still have a lot of underlying mental health issues.
It’s also unclear whether metabolic factors so common with PCOS, particularly insulin resistance and obesity, are a result of the condition or are contributors to it. Is insulin resistance contributing to dysregulation in the neurons that interferes with normal functioning of the hypothalamic-pituitary-adrenal axis? Is abnormal functioning along this axis contributing to insulin resistance? Or neither? Or both? Or does it depend? The authors of one paper wrote that “insulin may play both direct and indirect roles in the pathogenesis of androgen excess in PCOS,” since insulin can “stimulate ovarian androgen production” and “enhance ovarian growth and follicular cyst formation in rats.”
Dr. Pal noted that “obesity itself can evolve into a PCOS-like picture,” raising questions about whether obesity or insulin resistance might be part of the causal pathway to PCOS, or whether either can trigger its development in those genetically predisposed.
“Obesity does appear to exacerbate many aspects of the PCOS phenotype, particularly those risk factors related to metabolic syndrome,” wrote the authors of a scientific statement on aspects of PCOS, but they add that “it is currently debated whether obesity per se can cause PCOS.” While massive weight loss in those with PCOS and obesity has improved multiple reproductive and metabolic issues, it hasn’t resolved all of them, they write.
Dr. Hudson said she expects there’s “some degree of appetite dysregulation and metabolic dysregulation” that contributes, but then there are other women who don’t have much of an appetite or overeat and still struggle with their weight. Evidence has also found insulin resistance in women of normal weight with PCOS. “There may be some kind of metabolic dysregulation that they have at some level, and others are clearly bothered by overeating,” Dr. Hudson said.
Similarly, it’s not clear whether the recent discovery of increased cardiovascular risks in people with PCOS is a result of the comorbidities so common with PCOS, such as obesity, or whether an underlying mechanism links the cardiovascular risk and the dysregulation of hormones. Dr. Pal would argue that, again, it’s probably both, depending on the patient.
Then there is the key feature of hyperandrogenemia. “An outstanding debate is whether the elevated androgens in PCOS women are merely a downstream endocrine response to hyperactive GnRH and LH secretion driving the ovary, or do the elevated androgens themselves act in the brain (or pituitary) during development and/or adulthood to sculpt and maintain the hypersecretion of GnRH and LH?” wrote Eulalia A. Coutinho, PhD, and Alexander S. Kauffman, PhD, in a 2019 review of the brain’s role in PCOS.
These problems may be bidirectional or part of various feedback loops. Sleep apnea is more common in people with PCOS, Dr. Tyson noted, but sleep apnea is also linked to cardiovascular, metabolic, and depression risks, and depression can play a role in obesity, which increases the risk of obstructive sleep apnea. “So you’re in this vicious cycle,” Dr. Tyson said. That’s why she also believes it’s important to change the dialogue and perspective on PCOS, to reduce the stigma attached to it, and work with patients to empower them in treating its symptoms and reducing their risk of comorbidities.
Recent and upcoming changes in treatment
Current treatment of PCOS already changes according to the symptoms posing the greatest problems at each stage of a person’s life, Dr. Hudson said. Younger women tend to be more bothered about the cosmetic effects of PCOS, including hair growth patterns and acne, but as they grow out of adolescence and into their 20s and 30s, infertility becomes a bigger concern for many. Then, as they start approaching menopause, metabolic and cardiovascular issues take the lead, with more of a focus on lipids, diabetes risk, and heart health.
In some ways, management of PCOS hasn’t changed much in the past several decades, except in an increased awareness of the metabolic and cardiovascular risks, which has led to more frequent screening to catch potential conditions earlier in life. What has changed, however, is improvements in the treatments used for symptoms, such as expanded bariatric surgery options and GLP-1 agonists for treating obesity. Other examples include better options for menstrual management, such as new progesterone IUDs, and optimized fertility treatments, Dr. Tyson said.
“I think with more of these large-scale studies about the pathophysiology of PCOS and how it may look in different people and the different outcomes, we may be able to tailor our treatments even further,” Dr. Tyson said. She emphasized the importance of identifying the condition early, particularly in adolescents, even if it’s identifying young people at risk for the condition rather than actually having it yet.
Early identification “gives us this chance to do a lot of preventative care and motivate older teens to have a great lifestyle, work on their diet and exercise, and manage cardiovascular” risk factors, Dr. Tyson said.
“What we do know and recognize is that there’s so many spokes to this PCOS wheel that there really should be a multidisciplinary approach to care,” Dr. Tyson said. “When I think about who would be the real doctors for patients with PCOS, these would be gynecologists, endocrinologists, dermatologists, nutritionists, psychologists, sleep specialists, and primary care at a minimum.”
Dr. Pal worries that the label of PCOS leaves it in the laps of ob.gyns. whereas, “if it was called something else, everybody would be involved in being vigilant and managing those patients.” She frequently reiterated that the label of PCOS is less important than ensuring clinicians treat the symptoms that most bother the patient.
And even if kisspeptin does play a causal role in PCOS for some patients, it’s only a subset of individuals with PCOS who would benefit from therapies developed to target it. Given the complexity of the syndrome and its many manifestations, a “galaxy of pathways” are involved in different potential subtypes of the condition. “You can’t treat PCOS as one entity,” Dr. Pal said.
Still, Dr. Hudson is optimistic that the research into potential neuroendocrine contributions to PCOS will yield therapies that go beyond just managing symptoms.
“There aren’t a lot of treatments available yet, but there may be some on the horizon,” Dr. Hudson said. “We’re still in this very primitive stage in terms of therapeutics, where we’re only addressing specific symptoms, and we haven’t been able to really address the underlying cause because we haven’t understood it as well and because we don’t have therapies that can target it,” Dr. Hudson said. “But once there are therapies developed that will target some of these central mechanisms, I think it will change completely the approach to treating PCOS for patients.”
This story was updated on Sept. 6, 2022.