User login
Transfer to the hospital for women planning a home birth: A high-risk obstetrics problem
CASE: Febrile laboring mother transferred to hospital
You are in the hospital managing the induction of labor for one of your nulliparous patients who is postterm. You are hoping for a quiet and uneventful shift.
At midnight the nursing administrator pages you and asks if you would please provide care to a pregnant woman attempting a home birth who is in labor and is being transferred to your hospital.
The woman is a 41-year-old G2P1 with one prior cesarean delivery who has attempted a trial of labor at home. According to the nursing administrator the patient has a temperature of 100.4°F and the most recent cervical examination shows her to be fully dilated at +3/5 station in an occiput posterior position. She has been fully dilated for 5 hours. The fetal heart rate, assessed by Doppler monitor, is reported to be reassuring.
What is your clinical plan?
The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics recommend that pregnant women should deliver at certified birth centers or hospital-based obstetric units to optimize clinical outcomes for newborns and mothers.1,2 Both organizations also recognize a woman’s right to exercise her autonomy and choose a planned home birth.
In 2012, approximately 0.8% of pregnant women in the United States planned a home birth (31,500 home births and 3,999,386 total births).3 In 2009, three states had home birth rates above 1.9%, including Montana (2.6%), Oregon (1.96%), and Vermont (1.91%). Five states had home birth rates above 1.5%, including Idaho, Pennsylvania, Utah, Washington, and Wisconsin.4 Because planned home births may require transport to the hospital to complete the birth, all obstetric units should develop written plans for dealing with these high-risk patients.
Hospital transfer is common for women attempting a home birth
Many home birth experts regard the Netherlands as the country with the best organized and most successful home birth system that is fully integrated with hospital-based obstetric care. Approximately 23% of births in Holland occur at home supervised by a midwife. A key feature of the highly regulated Dutch system is that all pregnant women with a high-risk condition are required to give birth in a hospital and cannot have a home delivery. Consequently, only women with a low-risk pregnancy are permitted to attempt a home birth.
By contrast, in the United States, with a less well-regulated home birth system, women with high-risk conditions, such as one or more prior cesarean deliveries, may try to birth at home. In a Dutch study of 168,618 low-risk women attempting a home birth, 32% (N=53,809) were transferred to the hospital. Most of the transfers occurred during labor.5
In England about 2.8% of births occur at home. In a study of 16,840 planned home births in England, 21% (N=3,530) of the women were transferred to the hospital.6 Of the 3,530 transfers to the hospital, 70% were transferred before delivery and 30% after birth. In this study among 4,568 nulliparous women attempting home birth, 45% were transferred to the hospital. Among 12,272 multiparous women attempting home birth, 12% were transferred to the hospital.
Among the nulliparous women, but not among the multiparous women, there was a significantly increased risk of adverse newborn outcomes. Adverse newborn outcome was a composite measure that included perinatal death, stillbirth after the onset of labor, neonatal encephalopathy, meconium aspiration syndrome, brachial plexus injury, or fractured humerus or clavicle. The risk of an adverse newborn outcome among nulliparous women was 0.9% for those delivering at home and 0.5% for those delivering at the hospital.6
Your patient asks you, “Are home births safe for the baby?”
No large-scale randomized trials have compared home birth versus hospital birth.1 Consequently, the best evidence evaluating the risks and benefits of home birth is based on observational studies of large cohorts. Recent studies from the United States have reported that neonatal complications, including the risk of a low Apgar score and neonatal seizures, is significantly increased with planned home birth compared with birth at a hospital.2,3 In one study, the risk of a 5-minute Apgar score of zero was 1 in 615 home births and 1 in 6,493 hospital births.3 Studies from the Netherlands also have reported that planned home birth is associated with increased perinatal mortality and morbidity.4,5
Because planned home birth is associated with an increased risk of neonatal morbidity and mortality, some experts conclude that obstetricians have an ethical obligation to recommend against home birth and to respond to refusal of that recommendation with respectful persuasion.6
References
1. Olsen O, Clausen JA. Planned hospital birth versus planned home birth. Cochrane Database Syst Rev. 2012; (9):CD000352.
2. Grunebaum A, McCullough LB, Sapra KJ, et al. Apgar score of 0 at 5 minutes and neonatal seizures or serious neurologic dysfunction in relation to birth setting. Am J Obstet Gynecol. 2013;209(4):323.e1–e6.
3. Cheng YW, Snowden JM, King TL, Caughey AB. Selected perinatal outcomes associated with planned home births in the United States. Am J Obstet Gynecol. 2013;209(4).325.e1–e8.
4. Evers AC, Brouwers HA, Hukkelhoven CW, et al. Perinatal mortality and severe morbidity in low and high risk term pregnancies in the Netherlands: Prospective cohort study. BMJ. 2010;341:c5639.
5. Arabin B, Visser GHA. Comparison of obstetric care in Germany and in the Netherlands. J Health Med Informat. 2013;S11:014.
6. Chervenak FA, McCullough LB, Arabin B. Obstetric ethics: An essential dimension of planned home birth. Obstet Gynecol. 2011;117(5):1183–1187.
Interprofessional team care
For the woman planning a home birth, transfer from home to the hospital is a jarring experience. The woman may feel that she has not achieved a highly desired and important life goal. In a survey of women birthing in the Netherlands, transfer from home to the hospital was associated with a high rate of patient dissatisfaction with their birthing experience. Compared with women who were satisfied with their birth experience, women who were dissatisfied more often reported that the care providers at the hospital were rushed, insensitive, rude, inconsiderate, condescending, and unhelpful.7
Creating a positive birthing experience
Given that transfer to the hospital is associated with an increased rate of being dissatisfied with the birth experience, and that dissatisfied women may perceive their care providers negatively, it is important for the interprofessional hospital team to devote adequate time to listen the patient’s concerns, demonstrate a high degree of sensitivity, and be especially polite and helpful. It is probably best to avoid referring to the transfer as a “failed home birth.” Trust may be enhanced by asking open-ended questions about the patient’s expectations and expressing empathy for her situation. The hospital professional team might prioritize acknowledging the right of the woman to make informed choices and provide an overview of the standard procedures used at the hospital. The clinicians should explicitly state that the health of the mother and newborn are their top priority. The hospital team should also express confidence in the benefit of the standard practices they use to ensure a safe birth experience.
Successful negotiation: An art best achieved as a small group
When a laboring woman is transferred from home to the hospital, a negotiation begins with the hospital professionals about the best clinical path to a successful birth. The patient often arrives with a support team that includes her partner, a support person, and a midwife or trained birth attendant. These individuals often demonstrate strong group cohesion and may be skeptical of the benefits of hospital birthing practices including intravenous access, oxytocin administration, epidural anesthesia, and operative delivery. The goal for the patient and her support team and the hospital professionals is to achieve a safe birth for the baby and mother. Because the goal is aligned among all parties, the negotiation is focused on the clinical path that will best achieve the goal with minimal risks.
To enhance the likelihood of a successful negotiation, it is best if the team of hospital professionals, including an obstetrician, a senior nurse, and an obstetric anesthesiologist, jointly discuss hospital birthing practices with the patient and her support team. An obstetrician, negotiating independently, is in the difficult position of one professional trying to redirect the choices of a cohesive team of four individuals. Most experienced negotiators would not voluntarily enter a situation in which acting alone they needed to simultaneously negotiate with four people. A joint discussion between the interprofessional team and the patient reduces the opportunity for the patient and her team to generate disagreements among the hospital professionals.
An important issue is that the home midwife or trained birth attendant is not permitted to participate in the practice of medicine at the hospital. Only credentialed and licensed nurses, obstetricians, anesthesiologists, and pediatricians are permitted to participate in the practice of medicine at the hospital. It may be prudent to provide the home midwife a written statement from the hospital indicating that home midwives are not permitted to practice medicine at the institution.
Related article: Lay midwives and the ObGyn: Is collaboration risky? Lucia DiVenere, MA (Practice Management; May 2012)
Occasionally, negotiations between the hospital professional team and the patient and her support team are unsuccessful and the patient refuses the best advice of the hospital team. In these situations there should be a written plan of how the patient–clinician conflict will be communicated to other members of the hospital staff and hospital leadership. For example, another senior clinician may be asked to join in the planning process.
A high-risk patient population
In some cases of planned home birth, the patient and midwife have made management decisions that are inconsistent with standard obstetric protocols. Commonly encountered situations include 1) conservative home management of spontaneous rupture of the membranes at term, 2) prolonged conservative management of the arrest of the active phase of the first stage of labor, 3) prolonged second stage of labor, up to 24 hours in length, and 4) attempted home birth after multiple previous cesarean deliveries. I am also aware of multiple reports of attempted home birth of a fetus in the breech presentation.
On arrival to the hospital these patients and their newborns are at exceptionally high risk for adverse birth outcomes. If an adverse outcome were to occur, it would be unjust to assign sole or primary responsibility to the obstetrician for the adverse outcome. Hence, the hospital should have a written plan for helping to minimize the risk that the obstetrician, playing the role of Good Samaritan, will bear primary responsibility for an adverse outcome.
Related article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. Robert L. Barbieri, MD (Editorial; August 2013)
CASE: Resolved
In the case presented above, the obstetrician, nurse, and obstetric anesthesiologist successfully negotiated with the patient. Intravenous access and an epidural anesthetic were established. Antibiotics were administered. Using ultrasound, the obstetrician confirmed that the fetus was in the occiput posterior position. The mother was exhausted from many hours of pushing and agreed to an operative delivery. Forceps were used to deliver a healthy baby and a perineal laceration was repaired.
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion No. 476: Planned home birth. Obstet Gynecol. 2011;117(2 Pt 1):425–428.
2. American Academy of Pediatrics. Policy statement: Planned home birth Pediatrics. 2013;131(5):1016–1002.
3. Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Wilson EC, Matthews TH. Births: Final data for 2010. Natl Vital Stat Rep. 2012;61(1):1–72.
4. MacDorman MF, Mathews TJ, Declercq E. Home births in the United States, 1990-2009. NCHS Data Brief. 2012;(84):1–8.
5. Amelink-Verburg MP, Verloove-Vanhorick SP, Hakkenberg RM, Veldhuijzen IM, Bennebroek Gravenhorst J, Buitendijk SE. Evaluation of 280,000 cases in Dutch midwifery practices: A descriptive study. BJOG. 2008;115(5):570–578.
6. Birthplace in England Collaborative Group. Perinatal and maternal outcomes by planned place of birth for health women with low risk pregnancies: The Birthplace in England national prospective cohort study. BMJ. 2011;343:d7400.
7. Rijnders M, Baston H, Schonbeck Y, et al. Perinatal factors related to negative or positive recall of birth experience in women 3 years postpartum in the Netherlands. Birth. 2008;35:107–116.

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: Febrile laboring mother transferred to hospital
You are in the hospital managing the induction of labor for one of your nulliparous patients who is postterm. You are hoping for a quiet and uneventful shift.
At midnight the nursing administrator pages you and asks if you would please provide care to a pregnant woman attempting a home birth who is in labor and is being transferred to your hospital.
The woman is a 41-year-old G2P1 with one prior cesarean delivery who has attempted a trial of labor at home. According to the nursing administrator the patient has a temperature of 100.4°F and the most recent cervical examination shows her to be fully dilated at +3/5 station in an occiput posterior position. She has been fully dilated for 5 hours. The fetal heart rate, assessed by Doppler monitor, is reported to be reassuring.
What is your clinical plan?
The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics recommend that pregnant women should deliver at certified birth centers or hospital-based obstetric units to optimize clinical outcomes for newborns and mothers.1,2 Both organizations also recognize a woman’s right to exercise her autonomy and choose a planned home birth.
In 2012, approximately 0.8% of pregnant women in the United States planned a home birth (31,500 home births and 3,999,386 total births).3 In 2009, three states had home birth rates above 1.9%, including Montana (2.6%), Oregon (1.96%), and Vermont (1.91%). Five states had home birth rates above 1.5%, including Idaho, Pennsylvania, Utah, Washington, and Wisconsin.4 Because planned home births may require transport to the hospital to complete the birth, all obstetric units should develop written plans for dealing with these high-risk patients.
Hospital transfer is common for women attempting a home birth
Many home birth experts regard the Netherlands as the country with the best organized and most successful home birth system that is fully integrated with hospital-based obstetric care. Approximately 23% of births in Holland occur at home supervised by a midwife. A key feature of the highly regulated Dutch system is that all pregnant women with a high-risk condition are required to give birth in a hospital and cannot have a home delivery. Consequently, only women with a low-risk pregnancy are permitted to attempt a home birth.
By contrast, in the United States, with a less well-regulated home birth system, women with high-risk conditions, such as one or more prior cesarean deliveries, may try to birth at home. In a Dutch study of 168,618 low-risk women attempting a home birth, 32% (N=53,809) were transferred to the hospital. Most of the transfers occurred during labor.5
In England about 2.8% of births occur at home. In a study of 16,840 planned home births in England, 21% (N=3,530) of the women were transferred to the hospital.6 Of the 3,530 transfers to the hospital, 70% were transferred before delivery and 30% after birth. In this study among 4,568 nulliparous women attempting home birth, 45% were transferred to the hospital. Among 12,272 multiparous women attempting home birth, 12% were transferred to the hospital.
Among the nulliparous women, but not among the multiparous women, there was a significantly increased risk of adverse newborn outcomes. Adverse newborn outcome was a composite measure that included perinatal death, stillbirth after the onset of labor, neonatal encephalopathy, meconium aspiration syndrome, brachial plexus injury, or fractured humerus or clavicle. The risk of an adverse newborn outcome among nulliparous women was 0.9% for those delivering at home and 0.5% for those delivering at the hospital.6
Your patient asks you, “Are home births safe for the baby?”
No large-scale randomized trials have compared home birth versus hospital birth.1 Consequently, the best evidence evaluating the risks and benefits of home birth is based on observational studies of large cohorts. Recent studies from the United States have reported that neonatal complications, including the risk of a low Apgar score and neonatal seizures, is significantly increased with planned home birth compared with birth at a hospital.2,3 In one study, the risk of a 5-minute Apgar score of zero was 1 in 615 home births and 1 in 6,493 hospital births.3 Studies from the Netherlands also have reported that planned home birth is associated with increased perinatal mortality and morbidity.4,5
Because planned home birth is associated with an increased risk of neonatal morbidity and mortality, some experts conclude that obstetricians have an ethical obligation to recommend against home birth and to respond to refusal of that recommendation with respectful persuasion.6
References
1. Olsen O, Clausen JA. Planned hospital birth versus planned home birth. Cochrane Database Syst Rev. 2012; (9):CD000352.
2. Grunebaum A, McCullough LB, Sapra KJ, et al. Apgar score of 0 at 5 minutes and neonatal seizures or serious neurologic dysfunction in relation to birth setting. Am J Obstet Gynecol. 2013;209(4):323.e1–e6.
3. Cheng YW, Snowden JM, King TL, Caughey AB. Selected perinatal outcomes associated with planned home births in the United States. Am J Obstet Gynecol. 2013;209(4).325.e1–e8.
4. Evers AC, Brouwers HA, Hukkelhoven CW, et al. Perinatal mortality and severe morbidity in low and high risk term pregnancies in the Netherlands: Prospective cohort study. BMJ. 2010;341:c5639.
5. Arabin B, Visser GHA. Comparison of obstetric care in Germany and in the Netherlands. J Health Med Informat. 2013;S11:014.
6. Chervenak FA, McCullough LB, Arabin B. Obstetric ethics: An essential dimension of planned home birth. Obstet Gynecol. 2011;117(5):1183–1187.
Interprofessional team care
For the woman planning a home birth, transfer from home to the hospital is a jarring experience. The woman may feel that she has not achieved a highly desired and important life goal. In a survey of women birthing in the Netherlands, transfer from home to the hospital was associated with a high rate of patient dissatisfaction with their birthing experience. Compared with women who were satisfied with their birth experience, women who were dissatisfied more often reported that the care providers at the hospital were rushed, insensitive, rude, inconsiderate, condescending, and unhelpful.7
Creating a positive birthing experience
Given that transfer to the hospital is associated with an increased rate of being dissatisfied with the birth experience, and that dissatisfied women may perceive their care providers negatively, it is important for the interprofessional hospital team to devote adequate time to listen the patient’s concerns, demonstrate a high degree of sensitivity, and be especially polite and helpful. It is probably best to avoid referring to the transfer as a “failed home birth.” Trust may be enhanced by asking open-ended questions about the patient’s expectations and expressing empathy for her situation. The hospital professional team might prioritize acknowledging the right of the woman to make informed choices and provide an overview of the standard procedures used at the hospital. The clinicians should explicitly state that the health of the mother and newborn are their top priority. The hospital team should also express confidence in the benefit of the standard practices they use to ensure a safe birth experience.
Successful negotiation: An art best achieved as a small group
When a laboring woman is transferred from home to the hospital, a negotiation begins with the hospital professionals about the best clinical path to a successful birth. The patient often arrives with a support team that includes her partner, a support person, and a midwife or trained birth attendant. These individuals often demonstrate strong group cohesion and may be skeptical of the benefits of hospital birthing practices including intravenous access, oxytocin administration, epidural anesthesia, and operative delivery. The goal for the patient and her support team and the hospital professionals is to achieve a safe birth for the baby and mother. Because the goal is aligned among all parties, the negotiation is focused on the clinical path that will best achieve the goal with minimal risks.
To enhance the likelihood of a successful negotiation, it is best if the team of hospital professionals, including an obstetrician, a senior nurse, and an obstetric anesthesiologist, jointly discuss hospital birthing practices with the patient and her support team. An obstetrician, negotiating independently, is in the difficult position of one professional trying to redirect the choices of a cohesive team of four individuals. Most experienced negotiators would not voluntarily enter a situation in which acting alone they needed to simultaneously negotiate with four people. A joint discussion between the interprofessional team and the patient reduces the opportunity for the patient and her team to generate disagreements among the hospital professionals.
An important issue is that the home midwife or trained birth attendant is not permitted to participate in the practice of medicine at the hospital. Only credentialed and licensed nurses, obstetricians, anesthesiologists, and pediatricians are permitted to participate in the practice of medicine at the hospital. It may be prudent to provide the home midwife a written statement from the hospital indicating that home midwives are not permitted to practice medicine at the institution.
Related article: Lay midwives and the ObGyn: Is collaboration risky? Lucia DiVenere, MA (Practice Management; May 2012)
Occasionally, negotiations between the hospital professional team and the patient and her support team are unsuccessful and the patient refuses the best advice of the hospital team. In these situations there should be a written plan of how the patient–clinician conflict will be communicated to other members of the hospital staff and hospital leadership. For example, another senior clinician may be asked to join in the planning process.
A high-risk patient population
In some cases of planned home birth, the patient and midwife have made management decisions that are inconsistent with standard obstetric protocols. Commonly encountered situations include 1) conservative home management of spontaneous rupture of the membranes at term, 2) prolonged conservative management of the arrest of the active phase of the first stage of labor, 3) prolonged second stage of labor, up to 24 hours in length, and 4) attempted home birth after multiple previous cesarean deliveries. I am also aware of multiple reports of attempted home birth of a fetus in the breech presentation.
On arrival to the hospital these patients and their newborns are at exceptionally high risk for adverse birth outcomes. If an adverse outcome were to occur, it would be unjust to assign sole or primary responsibility to the obstetrician for the adverse outcome. Hence, the hospital should have a written plan for helping to minimize the risk that the obstetrician, playing the role of Good Samaritan, will bear primary responsibility for an adverse outcome.
Related article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. Robert L. Barbieri, MD (Editorial; August 2013)
CASE: Resolved
In the case presented above, the obstetrician, nurse, and obstetric anesthesiologist successfully negotiated with the patient. Intravenous access and an epidural anesthetic were established. Antibiotics were administered. Using ultrasound, the obstetrician confirmed that the fetus was in the occiput posterior position. The mother was exhausted from many hours of pushing and agreed to an operative delivery. Forceps were used to deliver a healthy baby and a perineal laceration was repaired.
CASE: Febrile laboring mother transferred to hospital
You are in the hospital managing the induction of labor for one of your nulliparous patients who is postterm. You are hoping for a quiet and uneventful shift.
At midnight the nursing administrator pages you and asks if you would please provide care to a pregnant woman attempting a home birth who is in labor and is being transferred to your hospital.
The woman is a 41-year-old G2P1 with one prior cesarean delivery who has attempted a trial of labor at home. According to the nursing administrator the patient has a temperature of 100.4°F and the most recent cervical examination shows her to be fully dilated at +3/5 station in an occiput posterior position. She has been fully dilated for 5 hours. The fetal heart rate, assessed by Doppler monitor, is reported to be reassuring.
What is your clinical plan?
The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics recommend that pregnant women should deliver at certified birth centers or hospital-based obstetric units to optimize clinical outcomes for newborns and mothers.1,2 Both organizations also recognize a woman’s right to exercise her autonomy and choose a planned home birth.
In 2012, approximately 0.8% of pregnant women in the United States planned a home birth (31,500 home births and 3,999,386 total births).3 In 2009, three states had home birth rates above 1.9%, including Montana (2.6%), Oregon (1.96%), and Vermont (1.91%). Five states had home birth rates above 1.5%, including Idaho, Pennsylvania, Utah, Washington, and Wisconsin.4 Because planned home births may require transport to the hospital to complete the birth, all obstetric units should develop written plans for dealing with these high-risk patients.
Hospital transfer is common for women attempting a home birth
Many home birth experts regard the Netherlands as the country with the best organized and most successful home birth system that is fully integrated with hospital-based obstetric care. Approximately 23% of births in Holland occur at home supervised by a midwife. A key feature of the highly regulated Dutch system is that all pregnant women with a high-risk condition are required to give birth in a hospital and cannot have a home delivery. Consequently, only women with a low-risk pregnancy are permitted to attempt a home birth.
By contrast, in the United States, with a less well-regulated home birth system, women with high-risk conditions, such as one or more prior cesarean deliveries, may try to birth at home. In a Dutch study of 168,618 low-risk women attempting a home birth, 32% (N=53,809) were transferred to the hospital. Most of the transfers occurred during labor.5
In England about 2.8% of births occur at home. In a study of 16,840 planned home births in England, 21% (N=3,530) of the women were transferred to the hospital.6 Of the 3,530 transfers to the hospital, 70% were transferred before delivery and 30% after birth. In this study among 4,568 nulliparous women attempting home birth, 45% were transferred to the hospital. Among 12,272 multiparous women attempting home birth, 12% were transferred to the hospital.
Among the nulliparous women, but not among the multiparous women, there was a significantly increased risk of adverse newborn outcomes. Adverse newborn outcome was a composite measure that included perinatal death, stillbirth after the onset of labor, neonatal encephalopathy, meconium aspiration syndrome, brachial plexus injury, or fractured humerus or clavicle. The risk of an adverse newborn outcome among nulliparous women was 0.9% for those delivering at home and 0.5% for those delivering at the hospital.6
Your patient asks you, “Are home births safe for the baby?”
No large-scale randomized trials have compared home birth versus hospital birth.1 Consequently, the best evidence evaluating the risks and benefits of home birth is based on observational studies of large cohorts. Recent studies from the United States have reported that neonatal complications, including the risk of a low Apgar score and neonatal seizures, is significantly increased with planned home birth compared with birth at a hospital.2,3 In one study, the risk of a 5-minute Apgar score of zero was 1 in 615 home births and 1 in 6,493 hospital births.3 Studies from the Netherlands also have reported that planned home birth is associated with increased perinatal mortality and morbidity.4,5
Because planned home birth is associated with an increased risk of neonatal morbidity and mortality, some experts conclude that obstetricians have an ethical obligation to recommend against home birth and to respond to refusal of that recommendation with respectful persuasion.6
References
1. Olsen O, Clausen JA. Planned hospital birth versus planned home birth. Cochrane Database Syst Rev. 2012; (9):CD000352.
2. Grunebaum A, McCullough LB, Sapra KJ, et al. Apgar score of 0 at 5 minutes and neonatal seizures or serious neurologic dysfunction in relation to birth setting. Am J Obstet Gynecol. 2013;209(4):323.e1–e6.
3. Cheng YW, Snowden JM, King TL, Caughey AB. Selected perinatal outcomes associated with planned home births in the United States. Am J Obstet Gynecol. 2013;209(4).325.e1–e8.
4. Evers AC, Brouwers HA, Hukkelhoven CW, et al. Perinatal mortality and severe morbidity in low and high risk term pregnancies in the Netherlands: Prospective cohort study. BMJ. 2010;341:c5639.
5. Arabin B, Visser GHA. Comparison of obstetric care in Germany and in the Netherlands. J Health Med Informat. 2013;S11:014.
6. Chervenak FA, McCullough LB, Arabin B. Obstetric ethics: An essential dimension of planned home birth. Obstet Gynecol. 2011;117(5):1183–1187.
Interprofessional team care
For the woman planning a home birth, transfer from home to the hospital is a jarring experience. The woman may feel that she has not achieved a highly desired and important life goal. In a survey of women birthing in the Netherlands, transfer from home to the hospital was associated with a high rate of patient dissatisfaction with their birthing experience. Compared with women who were satisfied with their birth experience, women who were dissatisfied more often reported that the care providers at the hospital were rushed, insensitive, rude, inconsiderate, condescending, and unhelpful.7
Creating a positive birthing experience
Given that transfer to the hospital is associated with an increased rate of being dissatisfied with the birth experience, and that dissatisfied women may perceive their care providers negatively, it is important for the interprofessional hospital team to devote adequate time to listen the patient’s concerns, demonstrate a high degree of sensitivity, and be especially polite and helpful. It is probably best to avoid referring to the transfer as a “failed home birth.” Trust may be enhanced by asking open-ended questions about the patient’s expectations and expressing empathy for her situation. The hospital professional team might prioritize acknowledging the right of the woman to make informed choices and provide an overview of the standard procedures used at the hospital. The clinicians should explicitly state that the health of the mother and newborn are their top priority. The hospital team should also express confidence in the benefit of the standard practices they use to ensure a safe birth experience.
Successful negotiation: An art best achieved as a small group
When a laboring woman is transferred from home to the hospital, a negotiation begins with the hospital professionals about the best clinical path to a successful birth. The patient often arrives with a support team that includes her partner, a support person, and a midwife or trained birth attendant. These individuals often demonstrate strong group cohesion and may be skeptical of the benefits of hospital birthing practices including intravenous access, oxytocin administration, epidural anesthesia, and operative delivery. The goal for the patient and her support team and the hospital professionals is to achieve a safe birth for the baby and mother. Because the goal is aligned among all parties, the negotiation is focused on the clinical path that will best achieve the goal with minimal risks.
To enhance the likelihood of a successful negotiation, it is best if the team of hospital professionals, including an obstetrician, a senior nurse, and an obstetric anesthesiologist, jointly discuss hospital birthing practices with the patient and her support team. An obstetrician, negotiating independently, is in the difficult position of one professional trying to redirect the choices of a cohesive team of four individuals. Most experienced negotiators would not voluntarily enter a situation in which acting alone they needed to simultaneously negotiate with four people. A joint discussion between the interprofessional team and the patient reduces the opportunity for the patient and her team to generate disagreements among the hospital professionals.
An important issue is that the home midwife or trained birth attendant is not permitted to participate in the practice of medicine at the hospital. Only credentialed and licensed nurses, obstetricians, anesthesiologists, and pediatricians are permitted to participate in the practice of medicine at the hospital. It may be prudent to provide the home midwife a written statement from the hospital indicating that home midwives are not permitted to practice medicine at the institution.
Related article: Lay midwives and the ObGyn: Is collaboration risky? Lucia DiVenere, MA (Practice Management; May 2012)
Occasionally, negotiations between the hospital professional team and the patient and her support team are unsuccessful and the patient refuses the best advice of the hospital team. In these situations there should be a written plan of how the patient–clinician conflict will be communicated to other members of the hospital staff and hospital leadership. For example, another senior clinician may be asked to join in the planning process.
A high-risk patient population
In some cases of planned home birth, the patient and midwife have made management decisions that are inconsistent with standard obstetric protocols. Commonly encountered situations include 1) conservative home management of spontaneous rupture of the membranes at term, 2) prolonged conservative management of the arrest of the active phase of the first stage of labor, 3) prolonged second stage of labor, up to 24 hours in length, and 4) attempted home birth after multiple previous cesarean deliveries. I am also aware of multiple reports of attempted home birth of a fetus in the breech presentation.
On arrival to the hospital these patients and their newborns are at exceptionally high risk for adverse birth outcomes. If an adverse outcome were to occur, it would be unjust to assign sole or primary responsibility to the obstetrician for the adverse outcome. Hence, the hospital should have a written plan for helping to minimize the risk that the obstetrician, playing the role of Good Samaritan, will bear primary responsibility for an adverse outcome.
Related article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. Robert L. Barbieri, MD (Editorial; August 2013)
CASE: Resolved
In the case presented above, the obstetrician, nurse, and obstetric anesthesiologist successfully negotiated with the patient. Intravenous access and an epidural anesthetic were established. Antibiotics were administered. Using ultrasound, the obstetrician confirmed that the fetus was in the occiput posterior position. The mother was exhausted from many hours of pushing and agreed to an operative delivery. Forceps were used to deliver a healthy baby and a perineal laceration was repaired.
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion No. 476: Planned home birth. Obstet Gynecol. 2011;117(2 Pt 1):425–428.
2. American Academy of Pediatrics. Policy statement: Planned home birth Pediatrics. 2013;131(5):1016–1002.
3. Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Wilson EC, Matthews TH. Births: Final data for 2010. Natl Vital Stat Rep. 2012;61(1):1–72.
4. MacDorman MF, Mathews TJ, Declercq E. Home births in the United States, 1990-2009. NCHS Data Brief. 2012;(84):1–8.
5. Amelink-Verburg MP, Verloove-Vanhorick SP, Hakkenberg RM, Veldhuijzen IM, Bennebroek Gravenhorst J, Buitendijk SE. Evaluation of 280,000 cases in Dutch midwifery practices: A descriptive study. BJOG. 2008;115(5):570–578.
6. Birthplace in England Collaborative Group. Perinatal and maternal outcomes by planned place of birth for health women with low risk pregnancies: The Birthplace in England national prospective cohort study. BMJ. 2011;343:d7400.
7. Rijnders M, Baston H, Schonbeck Y, et al. Perinatal factors related to negative or positive recall of birth experience in women 3 years postpartum in the Netherlands. Birth. 2008;35:107–116.
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion No. 476: Planned home birth. Obstet Gynecol. 2011;117(2 Pt 1):425–428.
2. American Academy of Pediatrics. Policy statement: Planned home birth Pediatrics. 2013;131(5):1016–1002.
3. Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Wilson EC, Matthews TH. Births: Final data for 2010. Natl Vital Stat Rep. 2012;61(1):1–72.
4. MacDorman MF, Mathews TJ, Declercq E. Home births in the United States, 1990-2009. NCHS Data Brief. 2012;(84):1–8.
5. Amelink-Verburg MP, Verloove-Vanhorick SP, Hakkenberg RM, Veldhuijzen IM, Bennebroek Gravenhorst J, Buitendijk SE. Evaluation of 280,000 cases in Dutch midwifery practices: A descriptive study. BJOG. 2008;115(5):570–578.
6. Birthplace in England Collaborative Group. Perinatal and maternal outcomes by planned place of birth for health women with low risk pregnancies: The Birthplace in England national prospective cohort study. BMJ. 2011;343:d7400.
7. Rijnders M, Baston H, Schonbeck Y, et al. Perinatal factors related to negative or positive recall of birth experience in women 3 years postpartum in the Netherlands. Birth. 2008;35:107–116.

On being up to date and linked in
We are mindful of our role in providing our readers with quality research- and literature-based articles about emerging therapies and diagnostic and palliative approaches that will have a positive impact on how they practice. So far this year, we have brought you articles on current therapies for metastatic melanoma and hairy cell leukemia as well as updates on managing chronic myelogenous leukemia, the late effects of cancer therapies, and most recently, small renal tumors...
Click on the PDF icon at the top of this introduction to read the full article.
We are mindful of our role in providing our readers with quality research- and literature-based articles about emerging therapies and diagnostic and palliative approaches that will have a positive impact on how they practice. So far this year, we have brought you articles on current therapies for metastatic melanoma and hairy cell leukemia as well as updates on managing chronic myelogenous leukemia, the late effects of cancer therapies, and most recently, small renal tumors...
Click on the PDF icon at the top of this introduction to read the full article.
We are mindful of our role in providing our readers with quality research- and literature-based articles about emerging therapies and diagnostic and palliative approaches that will have a positive impact on how they practice. So far this year, we have brought you articles on current therapies for metastatic melanoma and hairy cell leukemia as well as updates on managing chronic myelogenous leukemia, the late effects of cancer therapies, and most recently, small renal tumors...
Click on the PDF icon at the top of this introduction to read the full article.
For couples seeking to conceive, offer advice on reducing the risk of schizophrenia in their child
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
Hormone therapy for menopausal vasomotor symptoms
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1). 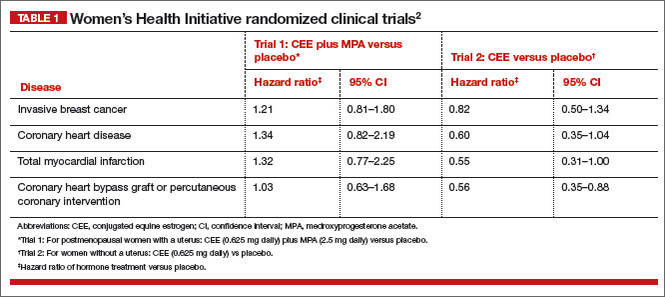
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women. 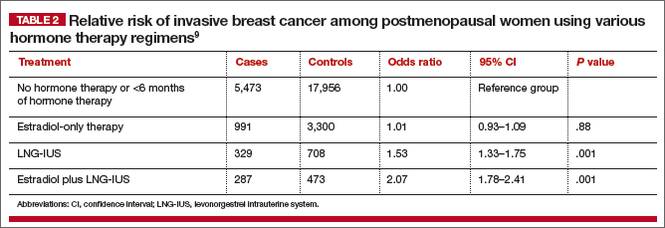
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.

Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1).
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women.
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
Estrogen therapy is highly effective in the treatment of hot flashes among postmenopausal women. For postmenopausal women with a uterus, estrogen treatment for hot flashes is almost always combined with a progestin to reduce the risk of endometrial polyps, hyperplasia, and cancer. For instance, in the Postmenopausal Estrogen/Progestin Interventions Trial, 62% of the women with a uterus treated with conjugated equine estrogen (CEE) 0.625 mg daily without a progestin developed endometrial hyperplasia.1
In the United States, the most commonly prescribed progestin for hormone therapy has been medroxyprogesterone acetate (MPA; Provera). However, data from the Women’s Health Initiative (WHI) trials indicate that MPA, when combined with CEE, may have adverse health effects among postmenopausal women.
Let’s examine the WHI data
Among women 50 to 59 years of age with a uterus, the combination of CEE plus MPA was associated with a trend toward an increased risk of breast cancer, coronary heart disease, and myocardial infarction.2 In contrast, among women 50 to 59 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of invasive breast cancer, coronary heart disease, and myocardial infarction (TABLE 1).
Among women 50 to 79 years of age with a uterus, the combination of CEE plus MPA was associated with a significantly increased risk of breast cancer (hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.01–1.53; P = .04).2 In contrast, among women 50 to 79 years of age without a uterus, CEE monotherapy was associated with a trend toward a decreased risk of breast cancer (HR, 0.79; 95% CI, 0.61–1.02, P = .07).2
Related article: In the latest report from the WHI, the data contradict the conclusions. Holly Thacker, MD (Commentary; March 2014)
When the analysis was limited to women consistently adherent to their CEE monotherapy, the estrogen treatment significantly decreased the risk of invasive breast cancer (HR, 0.67; 95% CI, 0.47–0.97; P = .03).3
The addition of MPA to CEE appears to reverse some of the health benefits of CEE monotherapy, although the biological mechanisms are unclear. This observation should prompt us to explore alternative and novel treatments of vasomotor symptoms that do not utilize MPA. Some options for MPA-free hormone therapy include:
- transdermal estradiol plus micronized progesterone
- CEE plus a levonorgestrel-releasing intrauterine system
- bazedoxifene plus CEE.
In addition, nonhormonal treatment of hot flashes is an option, with selective serotonin reuptake inhibitors (SSRIs).
Related article: Is one oral estrogen formulation safer than another for menopausal women? Andrew M. Kaunitz, MD (Examining the Evidence; January 2014)
MPA-free hormone therapy for hot flashes
Estrogen plus micronized progesterone
When using an estrogen plus progestin regimen to treat hot flashes, many experts favor a combination of low-dose transdermal estradiol and oral micronized progesterone (Prometrium). This combination is believed by some experts to result in a lower risk of venous thromboembolism, stroke, cardiovascular disease, and breast cancer than an estrogen-MPA combination.4–7
When prescribing transdermal estradiol plus oral micronized progesterone for a woman within 1 to 2 years of her last menses, a cyclic regimen can help reduce episodes of irregular, unscheduled uterine bleeding. I often use this cyclic regimen: transdermal estradiol 0.0375 mg plus cyclic oral micronized progesterone 200 mg prior to bedtime for calendar days 1 to 12.
When using transdermal estradiol plus oral micronized progesterone in a woman more than 2 years from her last menses, a continuous regimen is often prescribed. I often use this continuous regimen: transdermal estradiol 0.0375 mg plus continuous oral micronized progesterone 100 mg daily prior to bedtime.
Related article: When should a menopausal woman discontinue hormone therapy? Andrew M. Kaunitz, MD (Cases in Menopause; February 2014)
Estrogen plus a levonorgestrel-releasing intrauterine systemThe levonorgestrel intrauterine system (LNG-IUS; 20 µg daily; Mirena) is frequently used in Europe to protect the endometrium against the adverse effects of estrogen therapy in postmenopausal women. In a meta-analysis of five clinical trials involving postmenopausal women, the LNG-IUS provided excellent protection against endometrial hyperplasia, compared with MPA.8
One caution about using the LNG-IUS system with estrogen in postmenopausal women is that an observational study of all women with breast cancer in Finland from 1995 through 2007 reported a significantly increased risk of breast cancer among postmenopausal women using an LNG-IUS compared with women who did not use hormones or used only estrogen because they had a hysterectomy (TABLE 2).9 This study was not a randomized clinical trial and patients at higher baseline risk for breast cancer, including women with a high body mass index, may have been preferentially treated with an LNG-IUS. More information is needed to better understand the relationship between the LNG-IUS and breast cancer in postmenopausal women.
Related article: What we’ve learned from 2 decades’ experience with the LNG-IUS. Q&A with Oskari Heikinheimo, MD, PhD (February 2011)
Progestin-free hormone treatment, bazedoxifene plus CEE
The main reason for adding a progestin to estrogen therapy for vasomotor symptoms in postmenopausal women with a uterus is to prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer. A major innovation in hormone therapy is the discovery that third-generation selective estrogen receptor modulators (SERMs), such as bazedoxifene (BZA), can prevent estrogen-induced development of endometrial polyps, hyperplasia, and cancer but do not interfere with the efficacy of estrogen in the treatment of vasomotor symptoms.
BZA is an estrogen agonist in bone and an estrogen antagonist in the endometrium.10–12 The combination of BZA (20 mg daily) plus CEE (0.45 mg daily) (Duavee) is approved for the treatment of moderate to severe vasomotor symptoms and prevention of osteoporosis.13–15 Over 24 months of therapy, various doses of BZA plus CEE reduced reported daily hot flashes by 52% to 86%.16 In the same study, placebo treatment was associated with a 17% reduction in hot flashes.16
The main adverse effect of BZA/CEE is an increased risk of deep venous thrombosis. Therefore, BZA/CEE is contraindicated in women with a known thrombophilia or a personal history of hormone-induced deep venous thrombosis. The effect of BZA/CEE on the risk of developing invasive breast cancer is not known; over 52 weeks of therapy it did not increase breast density on mammogram.17,18
BZA/CEE is a remarkable advance in hormone therapy. It is progestin-free, uses estrogen to treat vasomotor symptoms, and uses BZA to protect the endometrium against estrogen-induced hyperplasia.
Related article: New option for treating menopausal vasomotor symptoms receives FDA approval. (News for your Practice; October 2013)
Nonhormone treatment of vasomotor symptoms Paroxetine mesylateFor postmenopausal women with vasomotor symptoms who cannot take estrogen, SSRIs are modestly effective in reducing moderate to severe hot flashes. The US Food and Drug Administration recently approved paroxetine mesylate (Brisdelle) for the treatment of postmenopausal vasomotor symptoms. The approved dose is 7.5 mg daily taken at bedtime.
Data supporting the efficacy of paroxetine mesylate are available from two studies involving 1,184 menopausal women with vasomotor symptoms randomly assigned to receive paroxetine 7.5 mg daily or placebo for 12 weeks of treatment.19-22 In one of the two clinical trials, women treated with paroxetine mesylate 7.5 mg daily had 5.6 fewer moderate to severe hot flashes daily after 12 weeks of treatment compared with 3.9 fewer hot flashes with placebo (median treatment difference, 1.7; P<.001).21
Paroxetine can block the metabolism of tamoxifen to its highly potent metabolite, endoxifen. Consequently, paroxetine may reduce the effectiveness of tamoxifen treatment for breast cancer and should be used with caution in postmenopausal women with breast cancer being treated with tamoxifen.
Related article: Paroxetine mesylate 7.5 mg found to be a safe alternative to hormone therapy for menopausal women with hot flashes. (News for your Practice; June 2014)
Escitalopram
Gynecologists are familiar with the use of venlafaxine, desvenlafaxine, clonidine, citalopram, sertraline, and fluoxetine for the treatment of postmenopausal hot flashes. Recently, escitalopram (Lexapro) at doses of 10 to 20 mg daily has been shown to be more effective than placebo in the treatment of hot flashes and sleep disturbances in postmenopausal women.23,24 In one trial of escitalopram 10 to 20 mg daily versus placebo in 205 postmenopausal women averaging 9.8 hot flashes daily at baseline, escitalopram and placebo reduced mean daily hot flashes by 4.6 and 3.2, respectively (P<.001), after 8 weeks of treatment.
In a meta-analysis of SSRIs for the treatment of hot flashes, data from a mixed-treatment comparison analysis indicated that the rank order from most to least effective therapy for hot flashes was: escitalopram > paroxetine > sertraline > citalopram > fluoxetine.25 Venlafaxine and desvenlafaxine, two serotonin and norepinephrine reuptake inhibitors that are effective in the treatment of hot flashes, were not included in the mixed-treatment comparison.
Use of alternatives to MPA could mean fewer health risks for women on a wide scale
Substantial data indicate that MPA is not an optimal progestin to combine with estrogen for hormone therapy. Currently, many health insurance plans and Medicare use pharmacy management formularies that prioritize dispensing MPA for postmenopausal hormone therapy. Dispensing an alternative to MPA, such as micronized progesterone, often requires the patient to make a significant copayment.
Hopefully, health insurance companies, Medicare, and their affiliated pharmacy management administrators will soon stop their current policy of using financial incentives to favor dispensing MPA when hormone therapy is prescribed because alternatives to MPA appear to be associated with fewer health risks for postmenopausal women.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: rbarbieri@frontlinemedcom.com
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.
1. The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375.
2. Manson JE, Chlebowski RT, Stefnick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
3. Stefanick ML, Anderson GL, Margolis KL, et al; WHI Investigators. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. JAMA. 2006;295(14):1647–1657.
4. Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? [published online head of print January 6, 2014]. Menopause. PMID: 24398406.
5. Manson JE. Current recommendations: What is the clinician to do? Fertil Steril. 2014;101(4):916–921.
6. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: Results from the E3N cohort study [published correction appears in Breast Cancer Res Treat. 2008;107(2):307–308]. Breast Cancer Res Treat. 2008;107(1):103–111.
7. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: A nested case-control study. BMJ. 2010;340:c2519.
8. Somboonpom W, Panna S, Temtanakitpaisan T, Kaewrudee S, Soontrapa S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause. 2011;18(10):1060–1066.
9. Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A case-control study on hormone therapy as a risk factor for breast cancer in Finland: Intrauterine system carries a risk as well. Int J Cancer. 2010;126(2):483–489.
10. Komm BS, Mirkin S. An overview of current and emerging SERMs. J Steroid Biochem Mol Biol. 2014;143C:207–222.
11. Ethun KF, Wood CE, Cline JM, Register TC, Appt SE, Clarkson TB. Endometrial profile of bazedoxifene acetate alone and in combination with conjugated equine estrogens in a primate model. Menopause. 2013;20(7):777–784.
12. Pinkerton JV, Harvey JA, Lindsay R, et al; SMART-5 Investigators. Effects of bazedoxifene/conjugated estrogens on the endometrium and bone: A randomized trial. J Clin Endocrinol Metab. 2014;99(2):E189–E198.
13. Pinkerton JV, Pickar JH, Racketa J, Mirkin S. Bazedoxifene/conjugated estrogens for menopausal symptom treatment and osteoporosis prevention. Climacteric. 2012;15(5):411–418.
14. Pinkerton JV, Abraham L, Bushmakin AG, et al. Evaluation of the efficacy and safety of bazedoxifene/conjugated estrogens for secondary outcomes including vasomotor symptoms in postmenopausal women by years since menopause in the Selective estrogens, Menopause and Response to Therapy (SMART) trials. J Womens Health (Larchmt). 2014;23(1):18–28.
15. Pinkerton JV, Harvey JA, Pan K, et al. Breast effects of bazedoxifene-conjugated estrogens: A randomized controlled trial. Obstet Gynecol. 2013;121(5):959–968.
16. Lobo RA, Pinkerton JV, Gass ML, et al. Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic parameters and overall safety profile. Fertil Steril. 2009;92(3):1025–1038.
17. Harvey JA, Holm MK, Ranganath R, Guse PA, Trott EA, Helzner E. The effects of bazedoxifene on mammographic breast density in postmenopausal women with osteoporosis. Menopause. 2009;16(6):1193–1196.
18. Harvey JA, Pinkerton JV, Baracat EC, Shi H, Chines AA, Mirkin S. Breast density changes in a randomized controlled trial evaluating bazedoxifene/conjugated estrogens. Menopause. 2013;20(2):138–145.
19. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause. 2013;20(10):1027–1035.
20. Simon JA, Portman DJ, Kazempour K, Mekonnen H, Bhaskar S, Lippman J. Safety profile of paroxetine 7.5 mg in women with moderate-to-severe vasomotor symptoms. Obstet Gynecol. 2014;123(suppl 1):132S–133S.
21. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flashes. N Engl J Med. 2014;370(19):1777–1779.
22. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
23. Freeman EW, Guthrie KA, Caan B, et al. Efficacy of escitalopram for hot flashes in health menopausal women. A randomized controlled trial. JAMA. 2011;305(3):267–274.
24. Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: A randomized controlled trial. Menopause. 2012;19(8):848–855.
25. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: A systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213.

Smart testing: An old idea, a new series

It’s simple. It’s obvious. None of us would like to be known as someone who orders diagnostic tests in a careless or stupid manner. And none of us order that way—just ask us! Yet, when critically evaluated, someone is ordering slews of unnecessary or inappropriate tests. In my own hospital we saved about $100,000 last year by putting “hard stops” on duplicated blood tests that were ordered too frequently to be of clinical value. This is an obvious and easily enacted intervention, but it is just the tip of the testing iceberg.
As technology advances, our testing practices must change. For example, the ventilation-perfusion nuclear scan is now seldom the test of choice when evaluating a patient with possible pulmonary embolism. However, it still has a role for experienced clinicians evaluating selected patients who have unexplained dyspnea or pulmonary hypertension. There is value in knowing the old as well as new testing modalities.
We like to think we practice evidence-based diagnostic testing. We talk about the gold-standard value of randomized controlled trials and using published data on pretest and posttest diagnostic likelihoods to assist us in choosing the appropriate test. However, the individual patient in front of us may have comorbidities that would have excluded her from the randomized trials. Who knows if my diagnostic acumen in determining the pretest likelihood of disease is better or worse than that of the clinicians who published the paper on the utility of that test? Sometimes choosing a test is not so simple.
Much of my clinical decision-making occurs in a gray zone of uncertainty. Rarely will a single test provide an indisputable diagnosis. So, I may bristle when someone, often for cost reasons, questions the necessity of a diagnostic test that I have ordered to help me understand a clinical problem in a specific patient.
Nevertheless, as Dr. Patrick Alguire points out in an editorial, the frequent use of sophisticated and expensive testing in the United States has not resulted in better clinical outcomes. And as Drs. Alraies and Buitrago et al discuss in letters to the editor, even relatively simple and minimally invasive tests can result in dire, unexpected outcomes. The choice of test matters to individual patients and to the health care system as a whole.
I do not minimize the financial impact of inappropriate testing, but in the clinic I am a doctor, not a businessman. I am far more swayed by clinical arguments than financial ones when making decisions for the patient on the examining table in front of me. Despite the general examples I provided above as to why regulated, cookbook approaches to test-ordering may lead to suboptimal care and physician and patient dissatisfaction (albeit while decreasing costs), sometimes ordering certain tests in certain circumstances just doesn’t make sense. Yet, there are many questionable test and scenario pairings that are ingrained in common practice. Some we learned during our training but have become less useful in light of new knowledge, some we may have adopted because of anecdotal experiences, and some are “demanded” by our patients. It is these that we hope to help expunge from routine clinical care.
In this issue of the Journal we are initiating a new series within our 1-Minute Consults, called Smart Testing. We are joining the efforts of the American College of Physicians (ACP) in educating physicians about reasons to avoid ordering frequently misused tests—tests that may add more harm, cost, or both than clinical utility to the care of our patients. The ACP also has an educational initiative called “High Value Care” that can be accessed (at no cost) at http://hvc.acponline.org/index.html. We at the Journal are very pleased to be working with physicians at the ACP to offer you this peer-reviewed series of patient vignettes that will focus, in an evidence-based and common-sense way, on the clinical value of selected tests in specific scenarios. Next month we will also be presenting a commentary on the impact that “defensive medicine” plays in test ordering and malpractice case decisions.
The tests and scenarios to be presented are chosen in clinician group discussions. Some of the tests have also been identified by specialty societies as providing limited value to patients. In selecting the topics, we pick common scenarios, realizing that there can often (always?) be some situational nuance that negates the accompanying discussion. We are not expecting to throw light on those nuanced zones of uncertainty, but we do hope to change test-ordering behaviors in situations in which there is a smart—and a not-so-smart—way to pursue a diagnosis.
It’s simple. It’s obvious. None of us would like to be known as someone who orders diagnostic tests in a careless or stupid manner. And none of us order that way—just ask us! Yet, when critically evaluated, someone is ordering slews of unnecessary or inappropriate tests. In my own hospital we saved about $100,000 last year by putting “hard stops” on duplicated blood tests that were ordered too frequently to be of clinical value. This is an obvious and easily enacted intervention, but it is just the tip of the testing iceberg.
As technology advances, our testing practices must change. For example, the ventilation-perfusion nuclear scan is now seldom the test of choice when evaluating a patient with possible pulmonary embolism. However, it still has a role for experienced clinicians evaluating selected patients who have unexplained dyspnea or pulmonary hypertension. There is value in knowing the old as well as new testing modalities.
We like to think we practice evidence-based diagnostic testing. We talk about the gold-standard value of randomized controlled trials and using published data on pretest and posttest diagnostic likelihoods to assist us in choosing the appropriate test. However, the individual patient in front of us may have comorbidities that would have excluded her from the randomized trials. Who knows if my diagnostic acumen in determining the pretest likelihood of disease is better or worse than that of the clinicians who published the paper on the utility of that test? Sometimes choosing a test is not so simple.
Much of my clinical decision-making occurs in a gray zone of uncertainty. Rarely will a single test provide an indisputable diagnosis. So, I may bristle when someone, often for cost reasons, questions the necessity of a diagnostic test that I have ordered to help me understand a clinical problem in a specific patient.
Nevertheless, as Dr. Patrick Alguire points out in an editorial, the frequent use of sophisticated and expensive testing in the United States has not resulted in better clinical outcomes. And as Drs. Alraies and Buitrago et al discuss in letters to the editor, even relatively simple and minimally invasive tests can result in dire, unexpected outcomes. The choice of test matters to individual patients and to the health care system as a whole.
I do not minimize the financial impact of inappropriate testing, but in the clinic I am a doctor, not a businessman. I am far more swayed by clinical arguments than financial ones when making decisions for the patient on the examining table in front of me. Despite the general examples I provided above as to why regulated, cookbook approaches to test-ordering may lead to suboptimal care and physician and patient dissatisfaction (albeit while decreasing costs), sometimes ordering certain tests in certain circumstances just doesn’t make sense. Yet, there are many questionable test and scenario pairings that are ingrained in common practice. Some we learned during our training but have become less useful in light of new knowledge, some we may have adopted because of anecdotal experiences, and some are “demanded” by our patients. It is these that we hope to help expunge from routine clinical care.
In this issue of the Journal we are initiating a new series within our 1-Minute Consults, called Smart Testing. We are joining the efforts of the American College of Physicians (ACP) in educating physicians about reasons to avoid ordering frequently misused tests—tests that may add more harm, cost, or both than clinical utility to the care of our patients. The ACP also has an educational initiative called “High Value Care” that can be accessed (at no cost) at http://hvc.acponline.org/index.html. We at the Journal are very pleased to be working with physicians at the ACP to offer you this peer-reviewed series of patient vignettes that will focus, in an evidence-based and common-sense way, on the clinical value of selected tests in specific scenarios. Next month we will also be presenting a commentary on the impact that “defensive medicine” plays in test ordering and malpractice case decisions.
The tests and scenarios to be presented are chosen in clinician group discussions. Some of the tests have also been identified by specialty societies as providing limited value to patients. In selecting the topics, we pick common scenarios, realizing that there can often (always?) be some situational nuance that negates the accompanying discussion. We are not expecting to throw light on those nuanced zones of uncertainty, but we do hope to change test-ordering behaviors in situations in which there is a smart—and a not-so-smart—way to pursue a diagnosis.
It’s simple. It’s obvious. None of us would like to be known as someone who orders diagnostic tests in a careless or stupid manner. And none of us order that way—just ask us! Yet, when critically evaluated, someone is ordering slews of unnecessary or inappropriate tests. In my own hospital we saved about $100,000 last year by putting “hard stops” on duplicated blood tests that were ordered too frequently to be of clinical value. This is an obvious and easily enacted intervention, but it is just the tip of the testing iceberg.
As technology advances, our testing practices must change. For example, the ventilation-perfusion nuclear scan is now seldom the test of choice when evaluating a patient with possible pulmonary embolism. However, it still has a role for experienced clinicians evaluating selected patients who have unexplained dyspnea or pulmonary hypertension. There is value in knowing the old as well as new testing modalities.
We like to think we practice evidence-based diagnostic testing. We talk about the gold-standard value of randomized controlled trials and using published data on pretest and posttest diagnostic likelihoods to assist us in choosing the appropriate test. However, the individual patient in front of us may have comorbidities that would have excluded her from the randomized trials. Who knows if my diagnostic acumen in determining the pretest likelihood of disease is better or worse than that of the clinicians who published the paper on the utility of that test? Sometimes choosing a test is not so simple.
Much of my clinical decision-making occurs in a gray zone of uncertainty. Rarely will a single test provide an indisputable diagnosis. So, I may bristle when someone, often for cost reasons, questions the necessity of a diagnostic test that I have ordered to help me understand a clinical problem in a specific patient.
Nevertheless, as Dr. Patrick Alguire points out in an editorial, the frequent use of sophisticated and expensive testing in the United States has not resulted in better clinical outcomes. And as Drs. Alraies and Buitrago et al discuss in letters to the editor, even relatively simple and minimally invasive tests can result in dire, unexpected outcomes. The choice of test matters to individual patients and to the health care system as a whole.
I do not minimize the financial impact of inappropriate testing, but in the clinic I am a doctor, not a businessman. I am far more swayed by clinical arguments than financial ones when making decisions for the patient on the examining table in front of me. Despite the general examples I provided above as to why regulated, cookbook approaches to test-ordering may lead to suboptimal care and physician and patient dissatisfaction (albeit while decreasing costs), sometimes ordering certain tests in certain circumstances just doesn’t make sense. Yet, there are many questionable test and scenario pairings that are ingrained in common practice. Some we learned during our training but have become less useful in light of new knowledge, some we may have adopted because of anecdotal experiences, and some are “demanded” by our patients. It is these that we hope to help expunge from routine clinical care.
In this issue of the Journal we are initiating a new series within our 1-Minute Consults, called Smart Testing. We are joining the efforts of the American College of Physicians (ACP) in educating physicians about reasons to avoid ordering frequently misused tests—tests that may add more harm, cost, or both than clinical utility to the care of our patients. The ACP also has an educational initiative called “High Value Care” that can be accessed (at no cost) at http://hvc.acponline.org/index.html. We at the Journal are very pleased to be working with physicians at the ACP to offer you this peer-reviewed series of patient vignettes that will focus, in an evidence-based and common-sense way, on the clinical value of selected tests in specific scenarios. Next month we will also be presenting a commentary on the impact that “defensive medicine” plays in test ordering and malpractice case decisions.
The tests and scenarios to be presented are chosen in clinician group discussions. Some of the tests have also been identified by specialty societies as providing limited value to patients. In selecting the topics, we pick common scenarios, realizing that there can often (always?) be some situational nuance that negates the accompanying discussion. We are not expecting to throw light on those nuanced zones of uncertainty, but we do hope to change test-ordering behaviors in situations in which there is a smart—and a not-so-smart—way to pursue a diagnosis.
Targeted sessions for targeted therapies at ASCO
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
It’s likely that you have just returned from ASCO 2014 in Chicago with 33,000 of your closest oncology friends, or that you have at least heard all about the meeting and some of the exciting presentations. Either way, you must be wondering how best to sift through the mountain of data and information that came out of the meeting so that you can organize it, absorb it, and here’s the real challenge, apply it in the real-clinic setting going forward.
Click on the PDF icon at the top of this introduction to read the full article.
Post-World War II psychiatry: 70 years of momentous change
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
A large percentage of psychiatrists practicing today are Boomers, and have experienced the tumultuous change in their profession since the end of World War II. At a recent Grand Rounds presentation in the Department of Neurology & Psychiatry at Saint Louis University, participants examined major changes and paradigm shifts that have reshaped psychiatry since 1946. The audience, which included me, contributed historical observations to the list of those changes and shifts, which I’ve classified here for your benefit, whether or not you are a Boomer.
Medical advances
Consider these discoveries and developments:
• Penicillin in 1947, which led to a reduction in cases of psychosis caused by tertiary syphilis, a disease that accounted for 10% to 15% of state hospital admissions.
• Lithium in 1948, the first pharmaceutical treatment for mania.
• Chlorpromazine, the first antipsychotic drug, in 1952, launching the psychopharmacology era and ending lifetime institutional sequestration as the only “treatment” for serious mental disorders.
• Monoamine oxidase inhibitors in 1959, from observations that iproniazid, a drug used in tuberculosis sanitariums, improved the mood of tuberculosis patients. This was the first pharmacotherapy for depression, which had been treated with electroconvulsive therapy (ECT), developed in the 1930s.
• Tricyclic antidepressants, starting with imipramine in the late 1950s, during attempts to synthesize additional phenothiazine antipsychotics.
• Diazepam, introduced in 1963 for its anti-anxiety effects, became the most widely used drug in the world over the next 2 decades.
• Pre-frontal lobotomy to treat severe psychiatric disorders. The neurosurgeon-inventor of this so-called medical advance won the 1949 Nobel Prize for Medicine or Physiology. The procedure was rapidly discredited after the development of antipsychotic drugs.
• Fluoxetine, the first selective serotonin reuptake inhibitor, in 1987, revolutionized the treatment of depression, especially in primary care settings.
• Clozapine, as an effective treatment for refractory and suicidal schizophrenia, and the spawning of second-generation antipsychotics. These newer agents shifted focus from neurologic adverse effects (extrapyramidal symptoms, tardive dyskinesia) to cardio-metabolic side effects (obesity, diabetes, dyslipidemia, and hypertension).
Changes to the landscape of health care
Three noteworthy developments made the list:
• The Community Mental Health Act of 1963, signed into law by President John F. Kennedy, revolutionized psychiatric care by shifting delivery of care from inpatient, hospital-based facilities to outpatient, clinic-based centers. There are now close to 800 community mental health centers in the United States, where care is dominated by non-physician mental health providers—in contrast to the era of state hospitals, during which physicians and nurses provided care for mentally ill patients.
• Deinstitutionalization. This move-ment gathered momentum in the 1970s and 1980s, leading to closing of the majority of state hospitals, with tragic consequences for the seriously mentally ill—including early demise, homelessness, substance abuse, and incarceration. In fact, the large percentage of mentally ill people in U.S. jails and prisons, instead of in a hospital, represents what has been labeled trans-institutionalization (see my March 2008 editorial, “Bring back the asylums?,” available at CurrentPsychiatry.com).
• Managed care, emerging in the late 1980s and early 1990s, caused a seismic disturbance in the delivery of, and reimbursement for, psychiatric care. The result was a significant decline in access to, and quality of, care—especially the so-called carve-out model that reduced payment for psychiatric care even more drastically than for general medical care. Under managed care, the priority became saving money, rather than saving lives. Average hospital stay for patients who had a psychiatric disorder, which was years in the pre-pharmacotherapy era, and weeks or months after that, shrunk to a few days under managed care.
Changes in professional direction
Two major shifts in the complexion of the specialty were identified:
• The decline of psychoanalysis, which had dominated psychiatry for decades (the 1940s through the 1970s), was a major shift in the conceptualization, training, and delivery of care in psychiatry. The rise of biological psychiatry and the medical model of psychiatric brain disorders, as well as the emergence of evidence-based (and briefer) psychotherapies (eg, cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy), gradually replaced the Freudian model of mental illness.
As a result, it became no longer necessary to be a certified psychoanalyst to be named chair of a department of psychiatry. The impact of this change on psychiatric training has been profound, because medical management by psychiatrists superseded psychotherapy— given the brief hospitalization that is required and the diminishing coverage for psychotherapy by insurers.
• Delegation of psychosocial treatments to non-psychiatrists. The unintended consequences of psychiatrists’ change of focus to 1) consultation on medical/surgical patients and 2) the medical evaluation, diagnosis, and pharmacotherapy of mental disorders led to the so-called “dual treatment model” for the most seriously mentally ill patients: The physician provides medical management and non-physician mental health professionals provide counseling, psychosocial therapy, and rehabilitation.
Disruptive breakthroughs
Several are notable:
• National Institute of Mental Health (NIMH). Establishment of NIMH in April 1949 was a major step toward funding research into psychiatric disorders. Billions of dollars have been invested to generate knowledge about the causes, treatment, course, and prevention of mental illness. No other country has spent as much on psychiatric research. It would have been nearly impossible to discover what we know today without the work of NIMH.
• Neuroscience. The meteoric rise of neuroscience from the 1960s to the present has had a dramatic effect, transforming old psychiatry and the study and therapy of the mind to a focus on the brain-mind continuum and the prospects of brain repair and neuroplasticity. Psychiatry is now regarded as a clinical neuroscience specialty of brain disorders that manifest as changes in thought, affect, mood, cognition, and behavior.
• Brain imaging. Techniques developed since the 1970s—the veritable alphabet soup of CT, PET, SPECT, MRI, MRS, fMRI, and DTI— has revolutionized understanding of brain structure and function in all psychiatric disorders but especially in psychotic and mood disorders.
• Molecular genetics. Advances over the past 2 decades have shed unprecedented light on the complex genetics of psychiatric disorders. It is becoming apparent that most psychiatric disorders are caused via gene-by-environment interaction; etiology is therefore a consequence of genetic and non-genetic variables. Risk genes, copy number variants, and de novo mutations are being discovered almost weekly, and progress in epigenetics holds promise for preventing medical disorders, including psychiatric illness.
• Neuromodulation. Advances represent an important paradigm shift, from pharmacotherapy to brain stimulation. Several techniques have been approved by the FDA, including transcranial magnetic stimulation, vagus nerve stimulation, and deep brain stimulation, to supplement, and perhaps eventually supplant, ECT.
Legal intrusiveness
No other medical specialty has been subject to laws governing clinical practice as psychiatry has been. Progressive intrusion of laws (ostensibly, enacted to protect the civil rights of “the disabled”) ends up hurting patients who refuse admission and then often harm themselves or others or decline urgent treatment, which can be associated with loss of brain tissue in acute psychotic, manic, and depressed states. No legal shackles apply to treating unconscious stroke patients, delirious geriatric patients, or semiconscious myocardial infarction patients when they are admitted to a hospital.
Distortions of the anti-psychiatry movement
The antipsychiatry movement preceded the Baby Boomer era by a century but has continued unabated. The movement gained momentum and became more defamatory after release of the movie One Flew Over the Cuckoo’s Nest in 1975, which portrayed psychiatry in a purely negative light. Despite progress in public understanding of psychiatry, and tangible improvements in practice, the stigma of mental illness persists. Media portrayals, including motion pictures, continue to distort the good that psychiatrists do for their patients.
Gender and sexuality
• Gender distribution of psychiatrists. A major shift occurred over the past 7 decades, reflecting the same pattern that has been documented in other medical specialties. At least one-half of psychiatry residents are now women—a welcome change from the pre-1946 era, when nearly all psychiatrists were men. This demographic transformation has had an impact on the dynamics of psychiatric practice.
• Acceptance and depathologization of homosexuality. Until 1974, homosexuality was considered a psychiatric disorder, and many homosexual persons sought treatment. That year, membership of the American Psychiatric Association voted to remove homosexuality from DSM-II and to no longer regard it as a behavioral abnormality. This was a huge step toward de-pathologizing same-sex orientation and love, and might have been the major impetus for the progressive social acceptance of gay, lesbian, and transgendered people over the past 4 decades.
The DSM paradigm shift in psychiatric diagnosis
• DSM-III. Perhaps the most radical change in the diagnostic criteria of psychiatric disorders occurred in 1980, with introduction of DSM-III to replace DSM-I and DSM-II, which were absurdly vague, unreliable, and with poor validity.
The move toward more operational and reliable diagnostic requirements began with the Research Diagnostic Criteria, developed by the Department of Psychiatry at Washington University in St. Louis. DSM-III represented a complete paradigm shift in psychiatric diagnosis. Subsequent editions maintained the same methodology, with relatively modest changes. The field expects continued evolution in DSM diagnostic criteria, including the future inclusion of biomarkers, based on sound, controlled studies.
• Recognizing PTSD. Develop-ment of posttraumatic stress disorder (PTSD) as a diagnostic entity, and its inclusion in DSM-III, were major changes in psychiatric nosology. At last, the old terms—shell shock, battle fatigue, neurasthenia—were legitimized as a recognizable syndrome secondary to major life trauma, including war and rape. That legitimacy has instigated substantial clinical and research interest in identifying how serious psychopathology can be triggered by life events.
Pharmaceutical industry debacle
Few industries have fallen so far from grace in the eyes of psychiatric professionals and the public as the manufacturers of psychotropic drugs.
At the dawn of the psychopharmacology era (the 1950s, 1960s, and 1970s) pharmaceutical companies were respected and regarded by physicians and patients as a vital partner in health care for their discovery and development of medications to treat psychiatric disorders. That image was tarnished in the 1990s, however, with the approval and release of several atypical antipsychotics. Cutthroat competition, questionable publication methods, concealment of negative findings, and excessive spending on marketing, including FDA-approved educational programs for clinicians on efficacy, safety, and dosing, all contributed to escalating cynicism about the industry. Academic faculty who received research grants to conduct FDA-required clinical trials of new agents were painted with the same brush.
Disclosure of potential conflict of interest became a mandatory procedure at universities and for NIMH grant applicants and journal publishers. Class-action lawsuits against companies that manufacture second-generation antipsychotics—filed for lack of transparency about metabolic side effects—exacerbated the intensity of criticism and condemnation.
Although new drug development has become measurably more rigorous and ethical because of self-regulation, combined with vigorous government scrutiny and regulation, demonization of the pharmaceutical industry remains unabated. That might be the reason why several major pharmaceutical companies have abandoned research and development of psychotropic drugs. That is likely to impede progress in psychopharmacotherapeutics; after all, no other private or government entity develops drugs for patients who have a psychiatric illness. The need for such agents is great: There is no FDA-indicated drug for the majority of DSM-5 diagnoses.
We entrust the future to next generations
Momentous events have transformed psychiatry during the lifespan of Baby Boomers like me and many of you. Because the cohort of 80 million Baby Boomers has comprised a significant percentage of the nation’s scientists, media representatives, members of the American Psychiatric Association, academicians, and community leaders over the past few decades, it is conceivable that the Baby Boomer generation helped trigger most of the transformative changes in psychiatry we have seen over the past 70 years.
I can only wonder: What direction will psychiatry take in the age of Generation X, Generation Y, and the Millennials? Only this is certain: Psychiatry will continue to evolve— long after Baby Boomers are gone.
Doing it right
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News

COPD: More options mean potentially better control
Some common diseases outside of my specialty areas of interest have, over time, blended into the background of daily practice. When patients have clearly inadequately controlled disease I refer them back to their internist or relevant subspecialist. Otherwise I find myself accepting the clinical status quo, providing stopgap care when necessary, utilizing my present knowledge of the disease process. But if I am not aware of any paradigm shifts in management, I tend to just peruse the published studies of new drug therapies as they appear in major journals, and not necessarily incorporate new therapies into my practice.
Chronic obstructive pulmonary disease (COPD) is one of those diseases, and the update by Hatipoğlu and Aboussouan in this issue of the Journal provided the opportunity to review some important things I have missed and to take note of the therapeutic principles that haven’t changed that much.
The incidence of COPD seems to be increasing. Cigarette smoking remains the major reversible cause, but one-fourth of current COPD patients have never smoked.
Patients who have early COPD may not be asked about or may not volunteer complaints specific to COPD. Lung examinations are insensitive, and chest radiography, if done, rarely identifies patients with early disease, so it is no surprise that COPD is underdiagnosed. While for many patients it is unclear whether the natural progression of lung damage can be dramatically altered by early diagnosis, other than by stopping smoking, that may not be the case for subsets of patients such as those with alpha-1 antitrypsin deficiency. But COPD generally has to be suspected in order to prompt appropriate screening for it.
COPD is still diagnosed by spirometry, with findings demonstrating incompletely reversible airway obstruction. The forced expiratory volume in 1 second (FEV1), a spirometric measure required to make the diagnosis, has been a useful surrogate marker of drug efficacy, but it is far from the ideal measure of disease progression and risk of death. Patients who have frequent exacerbations requiring hospitalization tend to have a tumultuous clinical course. The best predictor of future exacerbations is the patient’s history of exacerbations. Reducing the exacerbation rate improves the quality of life but may not translate to a benefit in terms of the mortality risk.
A lower risk of death is most consistently attained by helping patients stop smoking and, if they have sustained hypoxemia, giving them supplemental oxygen. The former intervention is the population game-changer—yet the US Centers for Disease Control and Prevention reports that 18% of American adults still smoke cigarettes, a number that dropped only slightly between 2005 and 2012. Americans with less education and less income more frequently smoke cigarettes, and it is estimated that one in 13 Americans currently 17 years or younger will die prematurely from the effects of cigarette smoking.
As for newer therapies, many that are applicable to most patients with COPD represent a fine-tuning of drug therapies we have been using for decades. Thus, it is not surprising that no dramatic increase in survival rates has been achieved. The advantage of several of the newer therapies in terms of FEV1 or exacerbation rate is statistically significant but relatively modest in terms of clinical impact. Their clinical promise (including specific antibiotics in low doses), revealed in recent studies, may be dependent upon using them in the most appropriate patients. Reducing the exacerbation rate is a significant advantage, but I would also like to know which drugs or drug combinations are most likely to permit major reductions in patients’ corticosteroid requirements. Hopefully, these data will come from real-world comparative efficacy studies.
Reading the article by Hatipoğlu and Aboussouan, I was reminded that utilizing our pulmonary colleagues’ expertise is of particular value in individualizing therapy for our patients with COPD—using newer drugs and combinations when most appropriate, not just because they are readily available. As physicians who are not pulmonary specialists, we need to be vigilant in recognizing the treatable comorbidities that contribute to dyspnea and poor outcome in patients with COPD, such as obstructive sleep apnea, congestive heart failure, obesity, and thromboembolism.
But to make the largest impact on the mortality rate, we need to continue to engage in and expand the ongoing war against cigarette use.
Some common diseases outside of my specialty areas of interest have, over time, blended into the background of daily practice. When patients have clearly inadequately controlled disease I refer them back to their internist or relevant subspecialist. Otherwise I find myself accepting the clinical status quo, providing stopgap care when necessary, utilizing my present knowledge of the disease process. But if I am not aware of any paradigm shifts in management, I tend to just peruse the published studies of new drug therapies as they appear in major journals, and not necessarily incorporate new therapies into my practice.
Chronic obstructive pulmonary disease (COPD) is one of those diseases, and the update by Hatipoğlu and Aboussouan in this issue of the Journal provided the opportunity to review some important things I have missed and to take note of the therapeutic principles that haven’t changed that much.
The incidence of COPD seems to be increasing. Cigarette smoking remains the major reversible cause, but one-fourth of current COPD patients have never smoked.
Patients who have early COPD may not be asked about or may not volunteer complaints specific to COPD. Lung examinations are insensitive, and chest radiography, if done, rarely identifies patients with early disease, so it is no surprise that COPD is underdiagnosed. While for many patients it is unclear whether the natural progression of lung damage can be dramatically altered by early diagnosis, other than by stopping smoking, that may not be the case for subsets of patients such as those with alpha-1 antitrypsin deficiency. But COPD generally has to be suspected in order to prompt appropriate screening for it.
COPD is still diagnosed by spirometry, with findings demonstrating incompletely reversible airway obstruction. The forced expiratory volume in 1 second (FEV1), a spirometric measure required to make the diagnosis, has been a useful surrogate marker of drug efficacy, but it is far from the ideal measure of disease progression and risk of death. Patients who have frequent exacerbations requiring hospitalization tend to have a tumultuous clinical course. The best predictor of future exacerbations is the patient’s history of exacerbations. Reducing the exacerbation rate improves the quality of life but may not translate to a benefit in terms of the mortality risk.
A lower risk of death is most consistently attained by helping patients stop smoking and, if they have sustained hypoxemia, giving them supplemental oxygen. The former intervention is the population game-changer—yet the US Centers for Disease Control and Prevention reports that 18% of American adults still smoke cigarettes, a number that dropped only slightly between 2005 and 2012. Americans with less education and less income more frequently smoke cigarettes, and it is estimated that one in 13 Americans currently 17 years or younger will die prematurely from the effects of cigarette smoking.
As for newer therapies, many that are applicable to most patients with COPD represent a fine-tuning of drug therapies we have been using for decades. Thus, it is not surprising that no dramatic increase in survival rates has been achieved. The advantage of several of the newer therapies in terms of FEV1 or exacerbation rate is statistically significant but relatively modest in terms of clinical impact. Their clinical promise (including specific antibiotics in low doses), revealed in recent studies, may be dependent upon using them in the most appropriate patients. Reducing the exacerbation rate is a significant advantage, but I would also like to know which drugs or drug combinations are most likely to permit major reductions in patients’ corticosteroid requirements. Hopefully, these data will come from real-world comparative efficacy studies.
Reading the article by Hatipoğlu and Aboussouan, I was reminded that utilizing our pulmonary colleagues’ expertise is of particular value in individualizing therapy for our patients with COPD—using newer drugs and combinations when most appropriate, not just because they are readily available. As physicians who are not pulmonary specialists, we need to be vigilant in recognizing the treatable comorbidities that contribute to dyspnea and poor outcome in patients with COPD, such as obstructive sleep apnea, congestive heart failure, obesity, and thromboembolism.
But to make the largest impact on the mortality rate, we need to continue to engage in and expand the ongoing war against cigarette use.
Some common diseases outside of my specialty areas of interest have, over time, blended into the background of daily practice. When patients have clearly inadequately controlled disease I refer them back to their internist or relevant subspecialist. Otherwise I find myself accepting the clinical status quo, providing stopgap care when necessary, utilizing my present knowledge of the disease process. But if I am not aware of any paradigm shifts in management, I tend to just peruse the published studies of new drug therapies as they appear in major journals, and not necessarily incorporate new therapies into my practice.
Chronic obstructive pulmonary disease (COPD) is one of those diseases, and the update by Hatipoğlu and Aboussouan in this issue of the Journal provided the opportunity to review some important things I have missed and to take note of the therapeutic principles that haven’t changed that much.
The incidence of COPD seems to be increasing. Cigarette smoking remains the major reversible cause, but one-fourth of current COPD patients have never smoked.
Patients who have early COPD may not be asked about or may not volunteer complaints specific to COPD. Lung examinations are insensitive, and chest radiography, if done, rarely identifies patients with early disease, so it is no surprise that COPD is underdiagnosed. While for many patients it is unclear whether the natural progression of lung damage can be dramatically altered by early diagnosis, other than by stopping smoking, that may not be the case for subsets of patients such as those with alpha-1 antitrypsin deficiency. But COPD generally has to be suspected in order to prompt appropriate screening for it.
COPD is still diagnosed by spirometry, with findings demonstrating incompletely reversible airway obstruction. The forced expiratory volume in 1 second (FEV1), a spirometric measure required to make the diagnosis, has been a useful surrogate marker of drug efficacy, but it is far from the ideal measure of disease progression and risk of death. Patients who have frequent exacerbations requiring hospitalization tend to have a tumultuous clinical course. The best predictor of future exacerbations is the patient’s history of exacerbations. Reducing the exacerbation rate improves the quality of life but may not translate to a benefit in terms of the mortality risk.
A lower risk of death is most consistently attained by helping patients stop smoking and, if they have sustained hypoxemia, giving them supplemental oxygen. The former intervention is the population game-changer—yet the US Centers for Disease Control and Prevention reports that 18% of American adults still smoke cigarettes, a number that dropped only slightly between 2005 and 2012. Americans with less education and less income more frequently smoke cigarettes, and it is estimated that one in 13 Americans currently 17 years or younger will die prematurely from the effects of cigarette smoking.
As for newer therapies, many that are applicable to most patients with COPD represent a fine-tuning of drug therapies we have been using for decades. Thus, it is not surprising that no dramatic increase in survival rates has been achieved. The advantage of several of the newer therapies in terms of FEV1 or exacerbation rate is statistically significant but relatively modest in terms of clinical impact. Their clinical promise (including specific antibiotics in low doses), revealed in recent studies, may be dependent upon using them in the most appropriate patients. Reducing the exacerbation rate is a significant advantage, but I would also like to know which drugs or drug combinations are most likely to permit major reductions in patients’ corticosteroid requirements. Hopefully, these data will come from real-world comparative efficacy studies.
Reading the article by Hatipoğlu and Aboussouan, I was reminded that utilizing our pulmonary colleagues’ expertise is of particular value in individualizing therapy for our patients with COPD—using newer drugs and combinations when most appropriate, not just because they are readily available. As physicians who are not pulmonary specialists, we need to be vigilant in recognizing the treatable comorbidities that contribute to dyspnea and poor outcome in patients with COPD, such as obstructive sleep apnea, congestive heart failure, obesity, and thromboembolism.
But to make the largest impact on the mortality rate, we need to continue to engage in and expand the ongoing war against cigarette use.
The transient truths of medical ‘progress’
I might have a jaundiced view of progress but, across most medical specialties, diseases are still managed, not cured. Chronicity is almost ubiquitous among medical ailments, and no specialty can boast that it restores function completely and fully restores patients’ quality of life.
Psychiatry has had its share of missteps
Prefrontal lobotomy is perhaps the most infamous of many discredited treatments that were introduced as a great solution to severe brain disorders such as schizophrenia.1 Prefrontal lobotomy (leucotomy) was initially heralded as a major medical advance in 1935; its originator, neurosurgeon António Egas Moniz, shared the Nobel Prize in Medicine or Physiology in 1949 for what is now regarded as mayhem. Prefrontal lobotomy was widely used for many conditions—not just for psychosis—but it fell from favor rapidly after the discovery of anti-psychotic drugs.
A similar fate befell other treatments that were introduced to psychiatry:
• malaria therapy (1917) for general paresis of the insane (the condition was later recognized as tertiary syphilis)
• deep sleep therapy (1920) for schizophrenia
• insulin shock therapy (1933), also for schizophrenia.
Those discredited therapies were lauded as significant advances, only to be shunned later as harmful, even barbaric.
Treating addiction is another saga of false steps. Fifty-nine different treatments for addiction have been introduced over the past few decades, many later discredited as “psychoquackery.”2 In the breathless rush to cure desperate conditions, there often is the risk that pseudoscience will masquerade as science. Many patients suffer needlessly before the medical community examines the accumulated evidence and discredits useless or harmful treatments.
Psychiatry isn’t alone in lacking cures
A fitting slogan of many non-psychiatric medical specialties is “to treat, perchance to cure.” Consider some examples:
• In cardiology, congestive heart failure, a chronic illness, is managed but rarely cured, and leads to early mortality.
• Nephrologists struggle to maintain a semblance of kidney function in renal failure patients, before placing them on the long waiting list for a kidney transplant.
• Gastroenterologists can only hope to maintain liver function in severe hepatitis, or to alleviate the misery of ulcerative colitis.
• Rheumatologists do what they can to relieve the debilitating symptoms of rheumatoid arthritis, systemic lupus erythematosus, and Sjögren’s syndrome.
• Pulmonologists know they can never restore normal lung function for their patients with chronic obstructive pulmonary disease; they can only help them hang on with partial function.
• Oncologists valiantly fight aggressive cancers with the hope of prolonging life for a few months or years.
• Neurologists valiantly try to manage multiple sclerosis, Parkinson’s disease, Alzheimer’s disease, epilepsy, stroke, myasthenia gravis, and amyotrophic lateral sclerosis—often with limited, if any, success at achieving remission.
Internal medicine has had its share of discredited therapies, too—ones that were withdrawn because they caused harm or were of dubious or inconclusive efficacy.3 Thanks to careful analysis of the efficacy and safety of medical procedures introduced during the past decade, we know that 40% of 146 procedures examined were eventually discredited and withdrawn. (That kind of analysis should be undertaken in psychotherapy, where evidence-based therapies can be counted on one hand but dozens more are promoted as legitimate.4 Psychotherapy can be harmful.5)
As with patients in psychiatry, patients of all these specialties are at risk of suffering disruptive iatrogenic side effects that, at times, approach torture—just to have progression of disease halted but not necessarily to deliver full remission. The quality of life for patients who have a chronic disease ranges from barely tolerable to poor, but is rarely good or optimal—and that is the case across all of medicine, including psychiatry.
Desperation often drives dubious innovation
There are numerous “desperate” diseases across all medical specialties, including psychiatry. Radical and harmful measures are sometimes proposed and marketed to treat many of those conditions; more often, useless, ineffective, futile “treatments” are introduced, and it might take years before they are discredited and withdrawn.6,7 Useless treatments can be harmful, too, because they delay the use of potentially effective procedures.
Move forward with caution!
What does this brief look at the missteps of medicine tell us? First, medical progress is like the mambo: We take steps forward but then step backward again; and, as Karl Popper noted, science learns more from its failures than from its successes.8 Second, all physicians must be judicious and guided by evidence when they select treatments.
For your patients’ sake, choose wisely!9
1. Valenstein ES. Great and desperate cures: The rise and decline of psychosurgery and other radical treatments for mental illness. New York, NY: Basic Books; 1986.
2. Norcross JC, Koocher GP, Fala NC, et al. What does not work? Expert consensus on discredited treatments in the addictions. J Addic Med. 2010;4(3):174-180.
3. Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc. 2013;88(8):790-798.
4. Corsini RJ. Handbook of innovative therapy. Philadelphia, PA: John Wiley & Sons, Inc; 2001.
5. Berk M, Parker G. The elephant on the couch: side-effects of psychotherapy. Austr N Z J Psychiatry. 2009;43(9):787-794.
6. Iaonnidis JP. Contradicted and initially stronger effects in highly cited clinical research. JAMA. 2005;294(2): 218-228.
7. Elshang AG, Watt AM, Mundy L, et al. Over 150 potentially low-value health care practices: an Australian study. Med J Aust. 2012;197(10):556-560.
8. Popper K. The logic of scientific discovery. London, United Kingdom: Hutchinson & Co.; 1959.
9. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decision about their care. JAMA. 2012;307(17):1801-1802.
I might have a jaundiced view of progress but, across most medical specialties, diseases are still managed, not cured. Chronicity is almost ubiquitous among medical ailments, and no specialty can boast that it restores function completely and fully restores patients’ quality of life.
Psychiatry has had its share of missteps
Prefrontal lobotomy is perhaps the most infamous of many discredited treatments that were introduced as a great solution to severe brain disorders such as schizophrenia.1 Prefrontal lobotomy (leucotomy) was initially heralded as a major medical advance in 1935; its originator, neurosurgeon António Egas Moniz, shared the Nobel Prize in Medicine or Physiology in 1949 for what is now regarded as mayhem. Prefrontal lobotomy was widely used for many conditions—not just for psychosis—but it fell from favor rapidly after the discovery of anti-psychotic drugs.
A similar fate befell other treatments that were introduced to psychiatry:
• malaria therapy (1917) for general paresis of the insane (the condition was later recognized as tertiary syphilis)
• deep sleep therapy (1920) for schizophrenia
• insulin shock therapy (1933), also for schizophrenia.
Those discredited therapies were lauded as significant advances, only to be shunned later as harmful, even barbaric.
Treating addiction is another saga of false steps. Fifty-nine different treatments for addiction have been introduced over the past few decades, many later discredited as “psychoquackery.”2 In the breathless rush to cure desperate conditions, there often is the risk that pseudoscience will masquerade as science. Many patients suffer needlessly before the medical community examines the accumulated evidence and discredits useless or harmful treatments.
Psychiatry isn’t alone in lacking cures
A fitting slogan of many non-psychiatric medical specialties is “to treat, perchance to cure.” Consider some examples:
• In cardiology, congestive heart failure, a chronic illness, is managed but rarely cured, and leads to early mortality.
• Nephrologists struggle to maintain a semblance of kidney function in renal failure patients, before placing them on the long waiting list for a kidney transplant.
• Gastroenterologists can only hope to maintain liver function in severe hepatitis, or to alleviate the misery of ulcerative colitis.
• Rheumatologists do what they can to relieve the debilitating symptoms of rheumatoid arthritis, systemic lupus erythematosus, and Sjögren’s syndrome.
• Pulmonologists know they can never restore normal lung function for their patients with chronic obstructive pulmonary disease; they can only help them hang on with partial function.
• Oncologists valiantly fight aggressive cancers with the hope of prolonging life for a few months or years.
• Neurologists valiantly try to manage multiple sclerosis, Parkinson’s disease, Alzheimer’s disease, epilepsy, stroke, myasthenia gravis, and amyotrophic lateral sclerosis—often with limited, if any, success at achieving remission.
Internal medicine has had its share of discredited therapies, too—ones that were withdrawn because they caused harm or were of dubious or inconclusive efficacy.3 Thanks to careful analysis of the efficacy and safety of medical procedures introduced during the past decade, we know that 40% of 146 procedures examined were eventually discredited and withdrawn. (That kind of analysis should be undertaken in psychotherapy, where evidence-based therapies can be counted on one hand but dozens more are promoted as legitimate.4 Psychotherapy can be harmful.5)
As with patients in psychiatry, patients of all these specialties are at risk of suffering disruptive iatrogenic side effects that, at times, approach torture—just to have progression of disease halted but not necessarily to deliver full remission. The quality of life for patients who have a chronic disease ranges from barely tolerable to poor, but is rarely good or optimal—and that is the case across all of medicine, including psychiatry.
Desperation often drives dubious innovation
There are numerous “desperate” diseases across all medical specialties, including psychiatry. Radical and harmful measures are sometimes proposed and marketed to treat many of those conditions; more often, useless, ineffective, futile “treatments” are introduced, and it might take years before they are discredited and withdrawn.6,7 Useless treatments can be harmful, too, because they delay the use of potentially effective procedures.
Move forward with caution!
What does this brief look at the missteps of medicine tell us? First, medical progress is like the mambo: We take steps forward but then step backward again; and, as Karl Popper noted, science learns more from its failures than from its successes.8 Second, all physicians must be judicious and guided by evidence when they select treatments.
For your patients’ sake, choose wisely!9
I might have a jaundiced view of progress but, across most medical specialties, diseases are still managed, not cured. Chronicity is almost ubiquitous among medical ailments, and no specialty can boast that it restores function completely and fully restores patients’ quality of life.
Psychiatry has had its share of missteps
Prefrontal lobotomy is perhaps the most infamous of many discredited treatments that were introduced as a great solution to severe brain disorders such as schizophrenia.1 Prefrontal lobotomy (leucotomy) was initially heralded as a major medical advance in 1935; its originator, neurosurgeon António Egas Moniz, shared the Nobel Prize in Medicine or Physiology in 1949 for what is now regarded as mayhem. Prefrontal lobotomy was widely used for many conditions—not just for psychosis—but it fell from favor rapidly after the discovery of anti-psychotic drugs.
A similar fate befell other treatments that were introduced to psychiatry:
• malaria therapy (1917) for general paresis of the insane (the condition was later recognized as tertiary syphilis)
• deep sleep therapy (1920) for schizophrenia
• insulin shock therapy (1933), also for schizophrenia.
Those discredited therapies were lauded as significant advances, only to be shunned later as harmful, even barbaric.
Treating addiction is another saga of false steps. Fifty-nine different treatments for addiction have been introduced over the past few decades, many later discredited as “psychoquackery.”2 In the breathless rush to cure desperate conditions, there often is the risk that pseudoscience will masquerade as science. Many patients suffer needlessly before the medical community examines the accumulated evidence and discredits useless or harmful treatments.
Psychiatry isn’t alone in lacking cures
A fitting slogan of many non-psychiatric medical specialties is “to treat, perchance to cure.” Consider some examples:
• In cardiology, congestive heart failure, a chronic illness, is managed but rarely cured, and leads to early mortality.
• Nephrologists struggle to maintain a semblance of kidney function in renal failure patients, before placing them on the long waiting list for a kidney transplant.
• Gastroenterologists can only hope to maintain liver function in severe hepatitis, or to alleviate the misery of ulcerative colitis.
• Rheumatologists do what they can to relieve the debilitating symptoms of rheumatoid arthritis, systemic lupus erythematosus, and Sjögren’s syndrome.
• Pulmonologists know they can never restore normal lung function for their patients with chronic obstructive pulmonary disease; they can only help them hang on with partial function.
• Oncologists valiantly fight aggressive cancers with the hope of prolonging life for a few months or years.
• Neurologists valiantly try to manage multiple sclerosis, Parkinson’s disease, Alzheimer’s disease, epilepsy, stroke, myasthenia gravis, and amyotrophic lateral sclerosis—often with limited, if any, success at achieving remission.
Internal medicine has had its share of discredited therapies, too—ones that were withdrawn because they caused harm or were of dubious or inconclusive efficacy.3 Thanks to careful analysis of the efficacy and safety of medical procedures introduced during the past decade, we know that 40% of 146 procedures examined were eventually discredited and withdrawn. (That kind of analysis should be undertaken in psychotherapy, where evidence-based therapies can be counted on one hand but dozens more are promoted as legitimate.4 Psychotherapy can be harmful.5)
As with patients in psychiatry, patients of all these specialties are at risk of suffering disruptive iatrogenic side effects that, at times, approach torture—just to have progression of disease halted but not necessarily to deliver full remission. The quality of life for patients who have a chronic disease ranges from barely tolerable to poor, but is rarely good or optimal—and that is the case across all of medicine, including psychiatry.
Desperation often drives dubious innovation
There are numerous “desperate” diseases across all medical specialties, including psychiatry. Radical and harmful measures are sometimes proposed and marketed to treat many of those conditions; more often, useless, ineffective, futile “treatments” are introduced, and it might take years before they are discredited and withdrawn.6,7 Useless treatments can be harmful, too, because they delay the use of potentially effective procedures.
Move forward with caution!
What does this brief look at the missteps of medicine tell us? First, medical progress is like the mambo: We take steps forward but then step backward again; and, as Karl Popper noted, science learns more from its failures than from its successes.8 Second, all physicians must be judicious and guided by evidence when they select treatments.
For your patients’ sake, choose wisely!9
1. Valenstein ES. Great and desperate cures: The rise and decline of psychosurgery and other radical treatments for mental illness. New York, NY: Basic Books; 1986.
2. Norcross JC, Koocher GP, Fala NC, et al. What does not work? Expert consensus on discredited treatments in the addictions. J Addic Med. 2010;4(3):174-180.
3. Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc. 2013;88(8):790-798.
4. Corsini RJ. Handbook of innovative therapy. Philadelphia, PA: John Wiley & Sons, Inc; 2001.
5. Berk M, Parker G. The elephant on the couch: side-effects of psychotherapy. Austr N Z J Psychiatry. 2009;43(9):787-794.
6. Iaonnidis JP. Contradicted and initially stronger effects in highly cited clinical research. JAMA. 2005;294(2): 218-228.
7. Elshang AG, Watt AM, Mundy L, et al. Over 150 potentially low-value health care practices: an Australian study. Med J Aust. 2012;197(10):556-560.
8. Popper K. The logic of scientific discovery. London, United Kingdom: Hutchinson & Co.; 1959.
9. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decision about their care. JAMA. 2012;307(17):1801-1802.
1. Valenstein ES. Great and desperate cures: The rise and decline of psychosurgery and other radical treatments for mental illness. New York, NY: Basic Books; 1986.
2. Norcross JC, Koocher GP, Fala NC, et al. What does not work? Expert consensus on discredited treatments in the addictions. J Addic Med. 2010;4(3):174-180.
3. Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc. 2013;88(8):790-798.
4. Corsini RJ. Handbook of innovative therapy. Philadelphia, PA: John Wiley & Sons, Inc; 2001.
5. Berk M, Parker G. The elephant on the couch: side-effects of psychotherapy. Austr N Z J Psychiatry. 2009;43(9):787-794.
6. Iaonnidis JP. Contradicted and initially stronger effects in highly cited clinical research. JAMA. 2005;294(2): 218-228.
7. Elshang AG, Watt AM, Mundy L, et al. Over 150 potentially low-value health care practices: an Australian study. Med J Aust. 2012;197(10):556-560.
8. Popper K. The logic of scientific discovery. London, United Kingdom: Hutchinson & Co.; 1959.
9. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decision about their care. JAMA. 2012;307(17):1801-1802.