User login
Taking the data and findings into the real-world setting
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Does your obstetric unit have a protocol for treating amniotic fluid embolism?
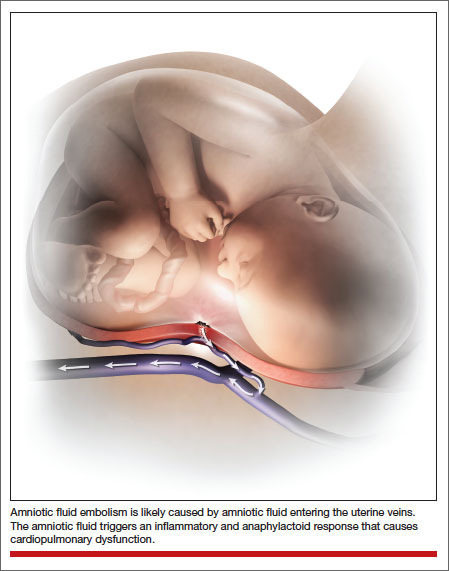
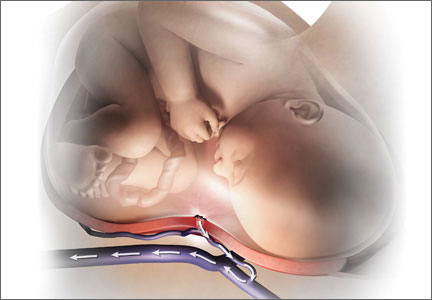
Amniotic fluid embolism (AFE) occurs in about 1 in 20,000 to 1 in 40,000 deliveries.1,2 Although the condition is rare, the case fatality rate is high, and AFE is a common cause of maternal death in developed countries. AFE cannot be predicted or prevented. Moreover, the condition is difficult to precisely define and is often a diagnosis of exclusion.
AFE should be considered in the differential diagnosis of a pregnant woman with sudden onset of shortness of breath, hypotension, or cardiac arrhythmia or arrest, followed by coagulopathy and hemorrhage. Premonitory symptoms, including restlessness, confusion, disorientation, agitation, chills, nausea, numbness, and tingling, are commonly reported just before the cardiorespiratory collapse. AFE is less likely if the initial obstetric event is hemorrhage in the absence of cardiorespiratory compromise or a preceding coagulopathy.3
Typically, the onset is just before birth, during birth, or within the first few hours after delivery. In the United Kingdom, which has a robust centralized registry for reporting AFE, about 56% of cases occur before birth and 44% after birth.4
Related article: Is the incidence of amniotic fluid embolism rising? John T. Repke, MD (Examining the Evidence, August 2010)
The resources available to obstetric units vary greatly. Each unit needs to assess its resources and develop an AFE treatment protocol that builds on the unique strengths of the unit. Treatment of AFE requires the coordinated actions of anesthesiologists, obstetricians, nurses, the blood bank, pharmacy, and cardiovascular specialists. Coordinated activity among the members of such a large multidisciplinary team requires a written protocol that is practiced on a regular basis.
Six important components of a multidisciplinary response to AFE treatment protocol are:
- high-quality cardiopulmonary resuscitation (CPR)
- a protocol for massive transfusion
- treatment of diffuse bleeding and coagulopathy
- treatment of uterine and pelvic bleeding
- extracorporeal lung and heart support
- post-AFE intensive care.
1. Initiate high-quality CPR
Hypotension and hypoxemia due to cardiac and pulmonary dysfunction are prominent features of AFE. Dysrythmias such as pulseless electrical activity, bradycardia, ventricular fibrillation, and asystole are common. Rapid institution of high-quality CPR is critical to the survival of women with AFE.
Interventions often used in CPR of patients with AFE include initiation of high-quality chest compressions, early defibrillation if indicated, immediate administration of 100% oxygen by mask ventilation followed by early intubation, and rapid establishment of peripheral, arterial, and central venous access. Volume assessment, fluid replacement, and administration of vasopressors and inotropes are also important.
CPR of pregnant women requires special interventions, including maximal left lateral displacement of the uterus to reduce compression of the descending aorta and vena cava. Lateral displacement of the uterus can be accomplished by left lateral tilt or by manual uterine displacement. To optimize the effectiveness of chest compressions, many experts recommend placing the woman in a supine position and using manual uterine displacement rather than a left lateral tilt.5 For chest compressions, the hands should be placed just above the center of the sternum to adjust for the elevation of the diaphragm caused by the gravid uterus.
The gravid uterus can compromise the effectiveness of CPR. Fetal viability and neurologic outcome are best if delivery occurs within 5 minutes of the onset of cardiopulmonary arrest. If the gestational age of the fetus is consistent with extrauterine viability and initial CPR has not restored cardiac function, it is best to initiate fetal delivery within 4 minutes of the onset of cardiopulmonary arrest with the intent to deliver the fetus within 5 minutes.6,7 If the fetus is beyond 20 weeks’ gestational age, delivery early in the course of CPR improves the effectiveness of maternal resuscitation and may increase the probability of maternal survival.
In one study of the response of anesthesiologists, obstetricians, and nurses to a simulated cardiac arrest caused by an AFE, the participants did not routinely use defibrillation when indicated, did not place a firm support under the back for chest compressions, and did not switch the provider of chest compressions every 2 minutes.8 This study indicates that additional training and routinely scheduled multidisciplinary simulation of the response to cardiopulmonary arrest could improve the quality of our CPR.
2. Use a massive transfusion protocol
Severe coagulopathy and diffuse bleeding are commonly encountered in AFE. Target goals for the replacement of blood products include:
- hemoglobin concentration ≥8 g/dL
- fibrinogen ≥150 to 200 mg/dL
- platelets ≥50,000/μL
- prothrombin time international normalized ratio (INR) ≤1.5.
Most massive transfusion protocols provide for the rapid delivery of 4 to 8 units of red blood cells and a similar number of units of fresh frozen plasma to the patient’s bedside. In the management of AFE, 20 to 30 units of red blood cells and a similar quantity of fresh frozen plasma may need to be transfused. Cryoprecipitate takes 20 to 30 minutes to thaw, so preparations to transfuse cryoprecipitate should be initiated as soon as the massive transfusion protocol is triggered. A case of AFE can completely empty the blood bank of all available blood products and necessitate the use of alternative agents.
Lyophilized fibrinogen concentrate (RiaSTAP) is approved by the US Food and Drug Administration for the treatment of congenital hypofibrinogenemia and also may be useful to replace fibrinogen in cases of AFE. In many hospitals, large quantities of fresh frozen plasma are not immediately available; lyophilized fibrinogen concentrate may be especially useful in these settings. Another advantage of fibrinogen concentrate is that large amounts of fibrinogen can be administered in a small volume of intravenous fluid. Fibrinogen concentrate typically is used at a dose of 70 mg/kg of body weight.9,10
Intraoperative red cell salvage occasionally is used in cases of obstetric hemorrhage. In one case report of the use of red cell salvage with leukocyte depletion filtration during treatment of an AFE, acute hypotension developed in the patient after the transfusion of salvaged red cells.11 This case report raises safety concerns about the use of salvaged cells in women with severe AFE.
Related article: 10 practical, evidence-based recommendations for the management of severe postpartum hemorrhage Baha M. Sibai, MD (June 2011)
3. Treat diffuse bleeding and coagulopathy
In addition to the initiation of the massive transfusion protocol, additional treatments that may be helpful in managing the coagulopathy of AFE include tranexamic acid, recombinant factor VIIa (rFVIIa), and exchange transfusion.
AFE is often associated with hyperfibrinolysis, which can cause excessive bleeding.12 Tranexamic acid blocks the lysine binding sites on plasminogen and thereby reduces the lysis of fibrin clots. Clinical trials in patients who have undergone trauma have demonstrated that the administration of tranexamic acid reduces blood loss.13 The dose of tranexamic acid is approximately 10 to 20 mg/kg of body weight, or approximately 1 g.
Controversy exists about the use of rFVIIa to treat the coagulopathy and bleeding caused by AFE. Some authorities believe that rFVIIa is associated with an increased AFE case fatality rate.14 Other authorities believe rFVIIa may be useful in the treatment of AFE coagulopathy, especially when bleeding persists despite aggressive blood and component replacement.”15 The dose of rFVIIa is approximately 90 µg/kg of body weight. rFVIIa is extremely expensive.
Exchange transfusion has been used successfully to treat AFE.16 In women with AFE, exchange transfusion removes circulating cells, cell fragments, and substances that trigger systemic anaphylaxis and coagulopathy, thereby enhancing rapid recovery.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial; March 2012)
4. Treat uterine and pelvic bleeding
Obstetrician-gynecologists are experts in the control of uterine and pelvic bleeding. Interventions that commonly are used to control uterine and pelvic bleeding in cases of postpartum hemorrhage, uterine rupture, or placenta accreta also can be applied in cases of AFE with uncontrolled uterine and pelvic bleeding. These techniques include:
- use of uterine compression sutures
- the Bakri balloon
- a uterine tourniquet
- vascular clamps on the ovarian vessels.17,18
In many cases of AFE, total or supracervical hysterectomy is necessary to control uterine bleeding. Uterine artery embolization, if available, has been reported to be helpful in select cases. However, many women with AFE are too unstable to survive transfer to an interventional radiology suite. Additional interventions to control bleeding include hypogastric artery ligation, infrarenal aortic compression, and pelvic packing.
Cross-clamping the aorta below the renal vessels can reduce blood flow to the pelvis and provide time for cardiopulmonary and volume resuscitation. Alternatively, placing pressure on the infrarenal aorta with a sponge or directly by hand can help reduce blood flow to the pelvis.19
In many cases of AFE, pelvic hemorrhage is difficult to control. Even if surgical pedicles are ligated securely, the coagulopathy of AFE may cause persistent oozing from areas of minor tissue trauma. Uncontrolled blood loss can be a proximate cause of death in women with AFE. All written protocols for responding to an AFE should include a plan to use pelvic packing for patients in whom standard operative procedures do not produce adequate control of bleeding. A “mushroom,” “parachute,” or “umbrella” pack has been reported to help stabilize the severely ill patient with pelvic bleeding and permit effective resuscitation and blood product replacement.20
Related articles:
A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures Robert L. Barbieri, MD (Editorial, December 2012)
Have you made the best use of the Bakri balloon in PPH? Robert L. Barbieri, MD (Editorial, July 2011)
5. Consider extracorporeal lung and heart support
In many cases of AFE, both lung and cardiac function are severely compromised. Both veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and full cardiopulmonary bypass provide support for the failing lung and heart. Based on a small number of case reports, extracorporeal lung and heart support appear to be useful in the treatment of AFE.21–26 Using the Seldinger technique,27 it is technically feasible to rapidly access a major vein and artery to provide the input and output ports for VA-ECMO. Unlike the cardiopulmonary bypass pump, the VA-ECMO pump does not have a reservoir that needs to be primed with blood and is smaller and more portable. To provide a patient with VA-ECMO or cardiopulmonary bypass, a cardiac interventionist and a perfusionist must be available. Extracorporeal lung and heart support require heparinization of the patient’s blood, which may result in increased bleeding. Both VA-ECMO and cardiopulmonary bypass, along with the diseases for which they are used, may cause renal dysfunction, neurologic injury, and infection.28
Alternative approaches that provide support of the heart—but not lung—are the Impella pump, TandemHeart, and the intra-aortic balloon pump. An alternative that provides lung support—but not cardiac support—is veno-venous ECMO.
In developing a written protocol for responding to an AFE, obstetricians should explore the potential availability of VA-ECMO, cardiopulmonary bypass, or other cardiopulmonary support devices as options for patients who have not responded to standard treatment of AFE and are at high risk of death.
6. Post-AFE intensive care
After stabilization, most women with AFE will require intensive care for 48 to 96 hours. Some experts have proposed that all survivors of cardiopulmonary arrest who are successfully resuscitated and stabilized be transferred to hospitals that specialize in post−cardiac arrest care to improve outcomes.
Assessment of organ injury is important after an AFE. In addition, encephalopathy is a common complication of AFE, and sequential neurologic examination is a priority. Therapeutic hypothermia (TH) may help to preserve neurologic function after AFE.29 However, TH may cause a mild coagulopathy by inhibiting platelet activation and enzyme activity of clotting factors. Because coagulopathy is a prominent feature of AFE, TH may be contraindicated if the patient has a clinically significant baseline coagulopathy.30
DEVELOP AN AFE PROTOCOL AND PRACTICE THE COMPONENTS
Practicing the components of obstetric protocols can improve unit performance and patient outcomes.31 The components of an AFE protocol, as described in this article, include high-quality CPR, a protocol for massive transfusion, treatment of diffuse bleeding and coagulopathy, treatment of uterine and pelvic bleeding, extracorporeal lung and heart support, and post-AFE intensive care. Practicing these components of an AFE protocol will enhance performance across many common obstetric complications including postpartum hemorrhage, uterine rupture, placenta accreta, and pulmonary embolism.
When Chesley “Sully” Sullenberger and his copilot landed Flight 1549 in the Hudson River in New York, he had never practiced that specific response to twin engine failure, but he had practiced many emergency responses involving related scenarios. The combination of exceptional flight experience and years of practicing the response to emergency scenarios in simulation exercises permitted him and his copilot to execute a uniquely clever plan to solve a life-threatening
emergency. In a related way, practicing the components of AFE treatment will help obstetricians, obstetric anesthesiologists, and their multidisciplinary team to improve the responses to all major obstetric emergencies.
INSTANT POLL
Does your obstetric unit have a written protocol for treating an amniotic fluid embolism (AFE)? Has your obstetric unit practiced any of the components of the AFE treatment protocol: 1) high-quality cardiopulmonary resuscitation, 2) a protocol for massive transfusion protocol, 3) treatment of diffuse bleeding and coagulopathy, 4) treatment of uterine and pelvic bleeding, 5) extracorporeal lung and heart support, and 6) post-AFE intensive care?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Kramer MS, Rouleau J, Baskett TF, Joseph KS; Maternal Health Study Group of the Canadian Perinatal Surveillance System. Amniotic-fluid embolism and medical induction of labour: A retrospective, population-based cohort study. Lancet. 2006;368(9545):1444–1448.
- Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid embolism: A population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–49.e8.
- Tuffnell D, Knight M, Plaat F. Amniotic fluid embolism—An update. Anaesthesia. 2011;66(1):3–6.
- Knight M, Tuffnell D, Brocklehurst P, Spark P, Kurinczuk JJ; UK Obstetric Surveillance System. Incidence and risk factors for amniotic-fluid embolism. Obstet Gynecol. 2010;115(5):910–917.
- Kundra P, Khanna S, Habeebullahg S, Ravishankar M. Manual displacement of the uterus during Caesarean section. Anaesthesia. 2007;62(5):460–465.
- Katz VL, Dotters DJ, Droegemueller W. Perimortem cesarean delivery. Obstet Gynecol. 1986;68(4):571–576.
- Katz V, Balderston K, DeFreest M. Perimortem cesarean delivery: Were our assumptions correct? Am J Obstet Gynecol. 2005;192(6):1916–1920.
- Lipman SS, Daniels KI, Carvalho B, et al. Deficits in the provision of cardiopulmonary resuscitation during simulated obstetric crises. Am J Obstet Gynecol. 2010;203(2):179.e1–179.e5.
- Bell SF, Rayment R, Collins PW, Collis RE. The use of fibrinogen concentrate to correct hypofibrinogenaemia rapidly during obstetric haemorrhage. Int J Obstet Anesth. 2010;19(2):218–223.
- Sorensen B, Tang M, Larsen OH, Laursen PN, Fenger-Eriksen C, Rea CJ. The role of fibrinogen: A new paradigm in the treatment of coagulopathic bleeding. Thromb Res. 2011;128(Suppl 1):S13–S16.
- Rogers WK, Wernimont SA, Kumar GC, Bennett E, Chestnut DH. Acute hypotension associated with intraoperative cell salvage using a leukocyte depletion filter during management of obstetric hemorrhage due to amniotic fluid embolism. Anesth Analg. 2013;117(2):449–452.
- Collins NF, Bloor M, McDonnell NJ. Hyperfibrinolysis diagnosed by rotational thromboelastometry in a case of suspected amniotic fluid embolism. Int J Obstet Anesth. 2013;22(1):71–76.
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: Systematic review and cumulative meta-analysis. BMJ. 2012;344:e3054.
- Leighton BL, Wall MH, Lockhart EM, Phillips LE, Zatta AJ. Use of recombinant factor VIIa in patients with amniotic fluid embolism: A systematic review of case reports. Anesthesiology. 2011;115(6):1201–1208.
- Huber AW, Raio L, Alberio L, Ghezzi F, Surbek DV. Recombinant human factor VIIa prevents hysterectomy in severe postpartum hemorrhage: single center study. J Perinat Med. 2011;40(1):43–49.
- Dodgson J, Martin J, Boswell J, Goodall HB, Smith R. Probable amniotic fluid embolism precipitated by amniocentesis and treated by exchange transfusion. Brit Med J (Clin Res Ed). 1987;294(6583):1322–1323.
- Barbieri RL. A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures. OBG Manage. 2012;24(12):6, 8, 10, 11.
- Barbieri RL. Have you made the best use of the Bakri balloon in PPH? OBG Manage. 2011;23(7):6, 8, 9.
- Belfort MA, Zimmerman J, Schemmer G, Oldroyd R, Smilanich R, Pearce M. Aortic compression and cross clamping in a case of placenta percreta and amniotic fluid embolism: A case report. AJP Rep. 2011;1(1):33–36.
- Dildy GA, Scott JR, Saffer CS, Belfort MA. An
effective pressure pack for severe pelvic hemorrhage. Obstet Gynecol. 2006;108(5):1222–1226. - Stanten RD, Iverson LI, Daugharty TM, Lovett SM, Terry C, Blumenstock E. Amniotic fluid embolism causing catastrophic pulmonary vasoconstriction: Diagnosis by transesophageal echocardiogram and treatment by cardiopulmonary bypass. Obstet Gynecol. 2003;102(3):496–498.
- Ho CH, Chen KB, Liu SK, Liu YF, Cheng HC, Wu RS. Early application of extracorporeal membrane oxygenation in a patient with amniotic fluid embolism. Acta Anaesthesiol Taiwan. 2009;47(2):99–102.
- Shen HP, Chang WC, Yeh LS, Ho M. Amniotic fluid embolism treated with emergency extracorporeal membrane oxygenation: A case report.
J Reprod Med. 2009;54(11–12):706–708. - Lee PH, Shulman MS, Vellayappan U, Symes JF, Olenchock SA Jr. Surgical treatment of amniotic fluid embolism with cardiopulmonary collapse. Ann Thorac Surg. 2010;90(5):1694–1696.
- Firstenberg MS, Abel E, Blais D, et al. Temporary extracorporeal circulatory support and pulmonary embolectomy for catastrophic amniotic fluid embolism. Heart Surg Forum. 2011;14(3):E157–E159.
- Ecker JL, Solt K, Fitzsimons MG, MacGillivray TE. Case records of the Massachusetts General Hospital. Case 40-2012: A 43-year-old woman with cardiorespiratory arrest after a cesarean section. N Engl J Med. 2012;367(26):2528–2536.
- Seldinger SI. Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta Radiol. 1953;39(5):368–376.
- Cheng R, Hachamovitch R, Kittelson M, et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann Thorac Surg. 2013; epub Nov 8.
- Rittenberger JC, Kelly E, Jang D, Greer K, Heffner A. Successful outcome utilizing hypothermia after cardiac arrest in pregnancy: A case report. Crit Care Med. 2008;36(4):1354–1356.
- Michelson AD, MacGregor H, Barnard MR, Krestin AS, Rohrer MJ, Valeri CR. Reversible inhibition of human platelet activation by hypothermia in vivo and in vitro. Thromb Haemost. 1994;71(5):633–640.
- Rivzi F, Mackey R, Barrett T, McKenna P, Geary M. Successful reduction of massive postpartum haemorrhage by use of guidelines and staff education. BJOG. 2004;111(5):495–498.

Robert L. Barbieri, MD, is Editor in Chief, OBG Management , and Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital, as well as Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.

Michaela K. Farber, MD, is an Instructor in Anesthesia, Harvard Medical School, and Fellowship Director, Obstetric Anesthesia, Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Robert L. Barbieri, MD, is Editor in Chief, OBG Management , and Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital, as well as Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Michaela K. Farber, MD, is an Instructor in Anesthesia, Harvard Medical School, and Fellowship Director, Obstetric Anesthesia, Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Robert L. Barbieri, MD, is Editor in Chief, OBG Management , and Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital, as well as Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Michaela K. Farber, MD, is an Instructor in Anesthesia, Harvard Medical School, and Fellowship Director, Obstetric Anesthesia, Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Amniotic fluid embolism (AFE) occurs in about 1 in 20,000 to 1 in 40,000 deliveries.1,2 Although the condition is rare, the case fatality rate is high, and AFE is a common cause of maternal death in developed countries. AFE cannot be predicted or prevented. Moreover, the condition is difficult to precisely define and is often a diagnosis of exclusion.
AFE should be considered in the differential diagnosis of a pregnant woman with sudden onset of shortness of breath, hypotension, or cardiac arrhythmia or arrest, followed by coagulopathy and hemorrhage. Premonitory symptoms, including restlessness, confusion, disorientation, agitation, chills, nausea, numbness, and tingling, are commonly reported just before the cardiorespiratory collapse. AFE is less likely if the initial obstetric event is hemorrhage in the absence of cardiorespiratory compromise or a preceding coagulopathy.3
Typically, the onset is just before birth, during birth, or within the first few hours after delivery. In the United Kingdom, which has a robust centralized registry for reporting AFE, about 56% of cases occur before birth and 44% after birth.4
Related article: Is the incidence of amniotic fluid embolism rising? John T. Repke, MD (Examining the Evidence, August 2010)
The resources available to obstetric units vary greatly. Each unit needs to assess its resources and develop an AFE treatment protocol that builds on the unique strengths of the unit. Treatment of AFE requires the coordinated actions of anesthesiologists, obstetricians, nurses, the blood bank, pharmacy, and cardiovascular specialists. Coordinated activity among the members of such a large multidisciplinary team requires a written protocol that is practiced on a regular basis.
Six important components of a multidisciplinary response to AFE treatment protocol are:
- high-quality cardiopulmonary resuscitation (CPR)
- a protocol for massive transfusion
- treatment of diffuse bleeding and coagulopathy
- treatment of uterine and pelvic bleeding
- extracorporeal lung and heart support
- post-AFE intensive care.
1. Initiate high-quality CPR
Hypotension and hypoxemia due to cardiac and pulmonary dysfunction are prominent features of AFE. Dysrythmias such as pulseless electrical activity, bradycardia, ventricular fibrillation, and asystole are common. Rapid institution of high-quality CPR is critical to the survival of women with AFE.
Interventions often used in CPR of patients with AFE include initiation of high-quality chest compressions, early defibrillation if indicated, immediate administration of 100% oxygen by mask ventilation followed by early intubation, and rapid establishment of peripheral, arterial, and central venous access. Volume assessment, fluid replacement, and administration of vasopressors and inotropes are also important.
CPR of pregnant women requires special interventions, including maximal left lateral displacement of the uterus to reduce compression of the descending aorta and vena cava. Lateral displacement of the uterus can be accomplished by left lateral tilt or by manual uterine displacement. To optimize the effectiveness of chest compressions, many experts recommend placing the woman in a supine position and using manual uterine displacement rather than a left lateral tilt.5 For chest compressions, the hands should be placed just above the center of the sternum to adjust for the elevation of the diaphragm caused by the gravid uterus.
The gravid uterus can compromise the effectiveness of CPR. Fetal viability and neurologic outcome are best if delivery occurs within 5 minutes of the onset of cardiopulmonary arrest. If the gestational age of the fetus is consistent with extrauterine viability and initial CPR has not restored cardiac function, it is best to initiate fetal delivery within 4 minutes of the onset of cardiopulmonary arrest with the intent to deliver the fetus within 5 minutes.6,7 If the fetus is beyond 20 weeks’ gestational age, delivery early in the course of CPR improves the effectiveness of maternal resuscitation and may increase the probability of maternal survival.
In one study of the response of anesthesiologists, obstetricians, and nurses to a simulated cardiac arrest caused by an AFE, the participants did not routinely use defibrillation when indicated, did not place a firm support under the back for chest compressions, and did not switch the provider of chest compressions every 2 minutes.8 This study indicates that additional training and routinely scheduled multidisciplinary simulation of the response to cardiopulmonary arrest could improve the quality of our CPR.
2. Use a massive transfusion protocol
Severe coagulopathy and diffuse bleeding are commonly encountered in AFE. Target goals for the replacement of blood products include:
- hemoglobin concentration ≥8 g/dL
- fibrinogen ≥150 to 200 mg/dL
- platelets ≥50,000/μL
- prothrombin time international normalized ratio (INR) ≤1.5.
Most massive transfusion protocols provide for the rapid delivery of 4 to 8 units of red blood cells and a similar number of units of fresh frozen plasma to the patient’s bedside. In the management of AFE, 20 to 30 units of red blood cells and a similar quantity of fresh frozen plasma may need to be transfused. Cryoprecipitate takes 20 to 30 minutes to thaw, so preparations to transfuse cryoprecipitate should be initiated as soon as the massive transfusion protocol is triggered. A case of AFE can completely empty the blood bank of all available blood products and necessitate the use of alternative agents.
Lyophilized fibrinogen concentrate (RiaSTAP) is approved by the US Food and Drug Administration for the treatment of congenital hypofibrinogenemia and also may be useful to replace fibrinogen in cases of AFE. In many hospitals, large quantities of fresh frozen plasma are not immediately available; lyophilized fibrinogen concentrate may be especially useful in these settings. Another advantage of fibrinogen concentrate is that large amounts of fibrinogen can be administered in a small volume of intravenous fluid. Fibrinogen concentrate typically is used at a dose of 70 mg/kg of body weight.9,10
Intraoperative red cell salvage occasionally is used in cases of obstetric hemorrhage. In one case report of the use of red cell salvage with leukocyte depletion filtration during treatment of an AFE, acute hypotension developed in the patient after the transfusion of salvaged red cells.11 This case report raises safety concerns about the use of salvaged cells in women with severe AFE.
Related article: 10 practical, evidence-based recommendations for the management of severe postpartum hemorrhage Baha M. Sibai, MD (June 2011)
3. Treat diffuse bleeding and coagulopathy
In addition to the initiation of the massive transfusion protocol, additional treatments that may be helpful in managing the coagulopathy of AFE include tranexamic acid, recombinant factor VIIa (rFVIIa), and exchange transfusion.
AFE is often associated with hyperfibrinolysis, which can cause excessive bleeding.12 Tranexamic acid blocks the lysine binding sites on plasminogen and thereby reduces the lysis of fibrin clots. Clinical trials in patients who have undergone trauma have demonstrated that the administration of tranexamic acid reduces blood loss.13 The dose of tranexamic acid is approximately 10 to 20 mg/kg of body weight, or approximately 1 g.
Controversy exists about the use of rFVIIa to treat the coagulopathy and bleeding caused by AFE. Some authorities believe that rFVIIa is associated with an increased AFE case fatality rate.14 Other authorities believe rFVIIa may be useful in the treatment of AFE coagulopathy, especially when bleeding persists despite aggressive blood and component replacement.”15 The dose of rFVIIa is approximately 90 µg/kg of body weight. rFVIIa is extremely expensive.
Exchange transfusion has been used successfully to treat AFE.16 In women with AFE, exchange transfusion removes circulating cells, cell fragments, and substances that trigger systemic anaphylaxis and coagulopathy, thereby enhancing rapid recovery.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial; March 2012)
4. Treat uterine and pelvic bleeding
Obstetrician-gynecologists are experts in the control of uterine and pelvic bleeding. Interventions that commonly are used to control uterine and pelvic bleeding in cases of postpartum hemorrhage, uterine rupture, or placenta accreta also can be applied in cases of AFE with uncontrolled uterine and pelvic bleeding. These techniques include:
- use of uterine compression sutures
- the Bakri balloon
- a uterine tourniquet
- vascular clamps on the ovarian vessels.17,18
In many cases of AFE, total or supracervical hysterectomy is necessary to control uterine bleeding. Uterine artery embolization, if available, has been reported to be helpful in select cases. However, many women with AFE are too unstable to survive transfer to an interventional radiology suite. Additional interventions to control bleeding include hypogastric artery ligation, infrarenal aortic compression, and pelvic packing.
Cross-clamping the aorta below the renal vessels can reduce blood flow to the pelvis and provide time for cardiopulmonary and volume resuscitation. Alternatively, placing pressure on the infrarenal aorta with a sponge or directly by hand can help reduce blood flow to the pelvis.19
In many cases of AFE, pelvic hemorrhage is difficult to control. Even if surgical pedicles are ligated securely, the coagulopathy of AFE may cause persistent oozing from areas of minor tissue trauma. Uncontrolled blood loss can be a proximate cause of death in women with AFE. All written protocols for responding to an AFE should include a plan to use pelvic packing for patients in whom standard operative procedures do not produce adequate control of bleeding. A “mushroom,” “parachute,” or “umbrella” pack has been reported to help stabilize the severely ill patient with pelvic bleeding and permit effective resuscitation and blood product replacement.20
Related articles:
A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures Robert L. Barbieri, MD (Editorial, December 2012)
Have you made the best use of the Bakri balloon in PPH? Robert L. Barbieri, MD (Editorial, July 2011)
5. Consider extracorporeal lung and heart support
In many cases of AFE, both lung and cardiac function are severely compromised. Both veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and full cardiopulmonary bypass provide support for the failing lung and heart. Based on a small number of case reports, extracorporeal lung and heart support appear to be useful in the treatment of AFE.21–26 Using the Seldinger technique,27 it is technically feasible to rapidly access a major vein and artery to provide the input and output ports for VA-ECMO. Unlike the cardiopulmonary bypass pump, the VA-ECMO pump does not have a reservoir that needs to be primed with blood and is smaller and more portable. To provide a patient with VA-ECMO or cardiopulmonary bypass, a cardiac interventionist and a perfusionist must be available. Extracorporeal lung and heart support require heparinization of the patient’s blood, which may result in increased bleeding. Both VA-ECMO and cardiopulmonary bypass, along with the diseases for which they are used, may cause renal dysfunction, neurologic injury, and infection.28
Alternative approaches that provide support of the heart—but not lung—are the Impella pump, TandemHeart, and the intra-aortic balloon pump. An alternative that provides lung support—but not cardiac support—is veno-venous ECMO.
In developing a written protocol for responding to an AFE, obstetricians should explore the potential availability of VA-ECMO, cardiopulmonary bypass, or other cardiopulmonary support devices as options for patients who have not responded to standard treatment of AFE and are at high risk of death.
6. Post-AFE intensive care
After stabilization, most women with AFE will require intensive care for 48 to 96 hours. Some experts have proposed that all survivors of cardiopulmonary arrest who are successfully resuscitated and stabilized be transferred to hospitals that specialize in post−cardiac arrest care to improve outcomes.
Assessment of organ injury is important after an AFE. In addition, encephalopathy is a common complication of AFE, and sequential neurologic examination is a priority. Therapeutic hypothermia (TH) may help to preserve neurologic function after AFE.29 However, TH may cause a mild coagulopathy by inhibiting platelet activation and enzyme activity of clotting factors. Because coagulopathy is a prominent feature of AFE, TH may be contraindicated if the patient has a clinically significant baseline coagulopathy.30
DEVELOP AN AFE PROTOCOL AND PRACTICE THE COMPONENTS
Practicing the components of obstetric protocols can improve unit performance and patient outcomes.31 The components of an AFE protocol, as described in this article, include high-quality CPR, a protocol for massive transfusion, treatment of diffuse bleeding and coagulopathy, treatment of uterine and pelvic bleeding, extracorporeal lung and heart support, and post-AFE intensive care. Practicing these components of an AFE protocol will enhance performance across many common obstetric complications including postpartum hemorrhage, uterine rupture, placenta accreta, and pulmonary embolism.
When Chesley “Sully” Sullenberger and his copilot landed Flight 1549 in the Hudson River in New York, he had never practiced that specific response to twin engine failure, but he had practiced many emergency responses involving related scenarios. The combination of exceptional flight experience and years of practicing the response to emergency scenarios in simulation exercises permitted him and his copilot to execute a uniquely clever plan to solve a life-threatening
emergency. In a related way, practicing the components of AFE treatment will help obstetricians, obstetric anesthesiologists, and their multidisciplinary team to improve the responses to all major obstetric emergencies.
INSTANT POLL
Does your obstetric unit have a written protocol for treating an amniotic fluid embolism (AFE)? Has your obstetric unit practiced any of the components of the AFE treatment protocol: 1) high-quality cardiopulmonary resuscitation, 2) a protocol for massive transfusion protocol, 3) treatment of diffuse bleeding and coagulopathy, 4) treatment of uterine and pelvic bleeding, 5) extracorporeal lung and heart support, and 6) post-AFE intensive care?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Amniotic fluid embolism (AFE) occurs in about 1 in 20,000 to 1 in 40,000 deliveries.1,2 Although the condition is rare, the case fatality rate is high, and AFE is a common cause of maternal death in developed countries. AFE cannot be predicted or prevented. Moreover, the condition is difficult to precisely define and is often a diagnosis of exclusion.
AFE should be considered in the differential diagnosis of a pregnant woman with sudden onset of shortness of breath, hypotension, or cardiac arrhythmia or arrest, followed by coagulopathy and hemorrhage. Premonitory symptoms, including restlessness, confusion, disorientation, agitation, chills, nausea, numbness, and tingling, are commonly reported just before the cardiorespiratory collapse. AFE is less likely if the initial obstetric event is hemorrhage in the absence of cardiorespiratory compromise or a preceding coagulopathy.3
Typically, the onset is just before birth, during birth, or within the first few hours after delivery. In the United Kingdom, which has a robust centralized registry for reporting AFE, about 56% of cases occur before birth and 44% after birth.4
Related article: Is the incidence of amniotic fluid embolism rising? John T. Repke, MD (Examining the Evidence, August 2010)
The resources available to obstetric units vary greatly. Each unit needs to assess its resources and develop an AFE treatment protocol that builds on the unique strengths of the unit. Treatment of AFE requires the coordinated actions of anesthesiologists, obstetricians, nurses, the blood bank, pharmacy, and cardiovascular specialists. Coordinated activity among the members of such a large multidisciplinary team requires a written protocol that is practiced on a regular basis.
Six important components of a multidisciplinary response to AFE treatment protocol are:
- high-quality cardiopulmonary resuscitation (CPR)
- a protocol for massive transfusion
- treatment of diffuse bleeding and coagulopathy
- treatment of uterine and pelvic bleeding
- extracorporeal lung and heart support
- post-AFE intensive care.
1. Initiate high-quality CPR
Hypotension and hypoxemia due to cardiac and pulmonary dysfunction are prominent features of AFE. Dysrythmias such as pulseless electrical activity, bradycardia, ventricular fibrillation, and asystole are common. Rapid institution of high-quality CPR is critical to the survival of women with AFE.
Interventions often used in CPR of patients with AFE include initiation of high-quality chest compressions, early defibrillation if indicated, immediate administration of 100% oxygen by mask ventilation followed by early intubation, and rapid establishment of peripheral, arterial, and central venous access. Volume assessment, fluid replacement, and administration of vasopressors and inotropes are also important.
CPR of pregnant women requires special interventions, including maximal left lateral displacement of the uterus to reduce compression of the descending aorta and vena cava. Lateral displacement of the uterus can be accomplished by left lateral tilt or by manual uterine displacement. To optimize the effectiveness of chest compressions, many experts recommend placing the woman in a supine position and using manual uterine displacement rather than a left lateral tilt.5 For chest compressions, the hands should be placed just above the center of the sternum to adjust for the elevation of the diaphragm caused by the gravid uterus.
The gravid uterus can compromise the effectiveness of CPR. Fetal viability and neurologic outcome are best if delivery occurs within 5 minutes of the onset of cardiopulmonary arrest. If the gestational age of the fetus is consistent with extrauterine viability and initial CPR has not restored cardiac function, it is best to initiate fetal delivery within 4 minutes of the onset of cardiopulmonary arrest with the intent to deliver the fetus within 5 minutes.6,7 If the fetus is beyond 20 weeks’ gestational age, delivery early in the course of CPR improves the effectiveness of maternal resuscitation and may increase the probability of maternal survival.
In one study of the response of anesthesiologists, obstetricians, and nurses to a simulated cardiac arrest caused by an AFE, the participants did not routinely use defibrillation when indicated, did not place a firm support under the back for chest compressions, and did not switch the provider of chest compressions every 2 minutes.8 This study indicates that additional training and routinely scheduled multidisciplinary simulation of the response to cardiopulmonary arrest could improve the quality of our CPR.
2. Use a massive transfusion protocol
Severe coagulopathy and diffuse bleeding are commonly encountered in AFE. Target goals for the replacement of blood products include:
- hemoglobin concentration ≥8 g/dL
- fibrinogen ≥150 to 200 mg/dL
- platelets ≥50,000/μL
- prothrombin time international normalized ratio (INR) ≤1.5.
Most massive transfusion protocols provide for the rapid delivery of 4 to 8 units of red blood cells and a similar number of units of fresh frozen plasma to the patient’s bedside. In the management of AFE, 20 to 30 units of red blood cells and a similar quantity of fresh frozen plasma may need to be transfused. Cryoprecipitate takes 20 to 30 minutes to thaw, so preparations to transfuse cryoprecipitate should be initiated as soon as the massive transfusion protocol is triggered. A case of AFE can completely empty the blood bank of all available blood products and necessitate the use of alternative agents.
Lyophilized fibrinogen concentrate (RiaSTAP) is approved by the US Food and Drug Administration for the treatment of congenital hypofibrinogenemia and also may be useful to replace fibrinogen in cases of AFE. In many hospitals, large quantities of fresh frozen plasma are not immediately available; lyophilized fibrinogen concentrate may be especially useful in these settings. Another advantage of fibrinogen concentrate is that large amounts of fibrinogen can be administered in a small volume of intravenous fluid. Fibrinogen concentrate typically is used at a dose of 70 mg/kg of body weight.9,10
Intraoperative red cell salvage occasionally is used in cases of obstetric hemorrhage. In one case report of the use of red cell salvage with leukocyte depletion filtration during treatment of an AFE, acute hypotension developed in the patient after the transfusion of salvaged red cells.11 This case report raises safety concerns about the use of salvaged cells in women with severe AFE.
Related article: 10 practical, evidence-based recommendations for the management of severe postpartum hemorrhage Baha M. Sibai, MD (June 2011)
3. Treat diffuse bleeding and coagulopathy
In addition to the initiation of the massive transfusion protocol, additional treatments that may be helpful in managing the coagulopathy of AFE include tranexamic acid, recombinant factor VIIa (rFVIIa), and exchange transfusion.
AFE is often associated with hyperfibrinolysis, which can cause excessive bleeding.12 Tranexamic acid blocks the lysine binding sites on plasminogen and thereby reduces the lysis of fibrin clots. Clinical trials in patients who have undergone trauma have demonstrated that the administration of tranexamic acid reduces blood loss.13 The dose of tranexamic acid is approximately 10 to 20 mg/kg of body weight, or approximately 1 g.
Controversy exists about the use of rFVIIa to treat the coagulopathy and bleeding caused by AFE. Some authorities believe that rFVIIa is associated with an increased AFE case fatality rate.14 Other authorities believe rFVIIa may be useful in the treatment of AFE coagulopathy, especially when bleeding persists despite aggressive blood and component replacement.”15 The dose of rFVIIa is approximately 90 µg/kg of body weight. rFVIIa is extremely expensive.
Exchange transfusion has been used successfully to treat AFE.16 In women with AFE, exchange transfusion removes circulating cells, cell fragments, and substances that trigger systemic anaphylaxis and coagulopathy, thereby enhancing rapid recovery.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial; March 2012)
4. Treat uterine and pelvic bleeding
Obstetrician-gynecologists are experts in the control of uterine and pelvic bleeding. Interventions that commonly are used to control uterine and pelvic bleeding in cases of postpartum hemorrhage, uterine rupture, or placenta accreta also can be applied in cases of AFE with uncontrolled uterine and pelvic bleeding. These techniques include:
- use of uterine compression sutures
- the Bakri balloon
- a uterine tourniquet
- vascular clamps on the ovarian vessels.17,18
In many cases of AFE, total or supracervical hysterectomy is necessary to control uterine bleeding. Uterine artery embolization, if available, has been reported to be helpful in select cases. However, many women with AFE are too unstable to survive transfer to an interventional radiology suite. Additional interventions to control bleeding include hypogastric artery ligation, infrarenal aortic compression, and pelvic packing.
Cross-clamping the aorta below the renal vessels can reduce blood flow to the pelvis and provide time for cardiopulmonary and volume resuscitation. Alternatively, placing pressure on the infrarenal aorta with a sponge or directly by hand can help reduce blood flow to the pelvis.19
In many cases of AFE, pelvic hemorrhage is difficult to control. Even if surgical pedicles are ligated securely, the coagulopathy of AFE may cause persistent oozing from areas of minor tissue trauma. Uncontrolled blood loss can be a proximate cause of death in women with AFE. All written protocols for responding to an AFE should include a plan to use pelvic packing for patients in whom standard operative procedures do not produce adequate control of bleeding. A “mushroom,” “parachute,” or “umbrella” pack has been reported to help stabilize the severely ill patient with pelvic bleeding and permit effective resuscitation and blood product replacement.20
Related articles:
A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures Robert L. Barbieri, MD (Editorial, December 2012)
Have you made the best use of the Bakri balloon in PPH? Robert L. Barbieri, MD (Editorial, July 2011)
5. Consider extracorporeal lung and heart support
In many cases of AFE, both lung and cardiac function are severely compromised. Both veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and full cardiopulmonary bypass provide support for the failing lung and heart. Based on a small number of case reports, extracorporeal lung and heart support appear to be useful in the treatment of AFE.21–26 Using the Seldinger technique,27 it is technically feasible to rapidly access a major vein and artery to provide the input and output ports for VA-ECMO. Unlike the cardiopulmonary bypass pump, the VA-ECMO pump does not have a reservoir that needs to be primed with blood and is smaller and more portable. To provide a patient with VA-ECMO or cardiopulmonary bypass, a cardiac interventionist and a perfusionist must be available. Extracorporeal lung and heart support require heparinization of the patient’s blood, which may result in increased bleeding. Both VA-ECMO and cardiopulmonary bypass, along with the diseases for which they are used, may cause renal dysfunction, neurologic injury, and infection.28
Alternative approaches that provide support of the heart—but not lung—are the Impella pump, TandemHeart, and the intra-aortic balloon pump. An alternative that provides lung support—but not cardiac support—is veno-venous ECMO.
In developing a written protocol for responding to an AFE, obstetricians should explore the potential availability of VA-ECMO, cardiopulmonary bypass, or other cardiopulmonary support devices as options for patients who have not responded to standard treatment of AFE and are at high risk of death.
6. Post-AFE intensive care
After stabilization, most women with AFE will require intensive care for 48 to 96 hours. Some experts have proposed that all survivors of cardiopulmonary arrest who are successfully resuscitated and stabilized be transferred to hospitals that specialize in post−cardiac arrest care to improve outcomes.
Assessment of organ injury is important after an AFE. In addition, encephalopathy is a common complication of AFE, and sequential neurologic examination is a priority. Therapeutic hypothermia (TH) may help to preserve neurologic function after AFE.29 However, TH may cause a mild coagulopathy by inhibiting platelet activation and enzyme activity of clotting factors. Because coagulopathy is a prominent feature of AFE, TH may be contraindicated if the patient has a clinically significant baseline coagulopathy.30
DEVELOP AN AFE PROTOCOL AND PRACTICE THE COMPONENTS
Practicing the components of obstetric protocols can improve unit performance and patient outcomes.31 The components of an AFE protocol, as described in this article, include high-quality CPR, a protocol for massive transfusion, treatment of diffuse bleeding and coagulopathy, treatment of uterine and pelvic bleeding, extracorporeal lung and heart support, and post-AFE intensive care. Practicing these components of an AFE protocol will enhance performance across many common obstetric complications including postpartum hemorrhage, uterine rupture, placenta accreta, and pulmonary embolism.
When Chesley “Sully” Sullenberger and his copilot landed Flight 1549 in the Hudson River in New York, he had never practiced that specific response to twin engine failure, but he had practiced many emergency responses involving related scenarios. The combination of exceptional flight experience and years of practicing the response to emergency scenarios in simulation exercises permitted him and his copilot to execute a uniquely clever plan to solve a life-threatening
emergency. In a related way, practicing the components of AFE treatment will help obstetricians, obstetric anesthesiologists, and their multidisciplinary team to improve the responses to all major obstetric emergencies.
INSTANT POLL
Does your obstetric unit have a written protocol for treating an amniotic fluid embolism (AFE)? Has your obstetric unit practiced any of the components of the AFE treatment protocol: 1) high-quality cardiopulmonary resuscitation, 2) a protocol for massive transfusion protocol, 3) treatment of diffuse bleeding and coagulopathy, 4) treatment of uterine and pelvic bleeding, 5) extracorporeal lung and heart support, and 6) post-AFE intensive care?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Kramer MS, Rouleau J, Baskett TF, Joseph KS; Maternal Health Study Group of the Canadian Perinatal Surveillance System. Amniotic-fluid embolism and medical induction of labour: A retrospective, population-based cohort study. Lancet. 2006;368(9545):1444–1448.
- Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid embolism: A population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–49.e8.
- Tuffnell D, Knight M, Plaat F. Amniotic fluid embolism—An update. Anaesthesia. 2011;66(1):3–6.
- Knight M, Tuffnell D, Brocklehurst P, Spark P, Kurinczuk JJ; UK Obstetric Surveillance System. Incidence and risk factors for amniotic-fluid embolism. Obstet Gynecol. 2010;115(5):910–917.
- Kundra P, Khanna S, Habeebullahg S, Ravishankar M. Manual displacement of the uterus during Caesarean section. Anaesthesia. 2007;62(5):460–465.
- Katz VL, Dotters DJ, Droegemueller W. Perimortem cesarean delivery. Obstet Gynecol. 1986;68(4):571–576.
- Katz V, Balderston K, DeFreest M. Perimortem cesarean delivery: Were our assumptions correct? Am J Obstet Gynecol. 2005;192(6):1916–1920.
- Lipman SS, Daniels KI, Carvalho B, et al. Deficits in the provision of cardiopulmonary resuscitation during simulated obstetric crises. Am J Obstet Gynecol. 2010;203(2):179.e1–179.e5.
- Bell SF, Rayment R, Collins PW, Collis RE. The use of fibrinogen concentrate to correct hypofibrinogenaemia rapidly during obstetric haemorrhage. Int J Obstet Anesth. 2010;19(2):218–223.
- Sorensen B, Tang M, Larsen OH, Laursen PN, Fenger-Eriksen C, Rea CJ. The role of fibrinogen: A new paradigm in the treatment of coagulopathic bleeding. Thromb Res. 2011;128(Suppl 1):S13–S16.
- Rogers WK, Wernimont SA, Kumar GC, Bennett E, Chestnut DH. Acute hypotension associated with intraoperative cell salvage using a leukocyte depletion filter during management of obstetric hemorrhage due to amniotic fluid embolism. Anesth Analg. 2013;117(2):449–452.
- Collins NF, Bloor M, McDonnell NJ. Hyperfibrinolysis diagnosed by rotational thromboelastometry in a case of suspected amniotic fluid embolism. Int J Obstet Anesth. 2013;22(1):71–76.
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: Systematic review and cumulative meta-analysis. BMJ. 2012;344:e3054.
- Leighton BL, Wall MH, Lockhart EM, Phillips LE, Zatta AJ. Use of recombinant factor VIIa in patients with amniotic fluid embolism: A systematic review of case reports. Anesthesiology. 2011;115(6):1201–1208.
- Huber AW, Raio L, Alberio L, Ghezzi F, Surbek DV. Recombinant human factor VIIa prevents hysterectomy in severe postpartum hemorrhage: single center study. J Perinat Med. 2011;40(1):43–49.
- Dodgson J, Martin J, Boswell J, Goodall HB, Smith R. Probable amniotic fluid embolism precipitated by amniocentesis and treated by exchange transfusion. Brit Med J (Clin Res Ed). 1987;294(6583):1322–1323.
- Barbieri RL. A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures. OBG Manage. 2012;24(12):6, 8, 10, 11.
- Barbieri RL. Have you made the best use of the Bakri balloon in PPH? OBG Manage. 2011;23(7):6, 8, 9.
- Belfort MA, Zimmerman J, Schemmer G, Oldroyd R, Smilanich R, Pearce M. Aortic compression and cross clamping in a case of placenta percreta and amniotic fluid embolism: A case report. AJP Rep. 2011;1(1):33–36.
- Dildy GA, Scott JR, Saffer CS, Belfort MA. An
effective pressure pack for severe pelvic hemorrhage. Obstet Gynecol. 2006;108(5):1222–1226. - Stanten RD, Iverson LI, Daugharty TM, Lovett SM, Terry C, Blumenstock E. Amniotic fluid embolism causing catastrophic pulmonary vasoconstriction: Diagnosis by transesophageal echocardiogram and treatment by cardiopulmonary bypass. Obstet Gynecol. 2003;102(3):496–498.
- Ho CH, Chen KB, Liu SK, Liu YF, Cheng HC, Wu RS. Early application of extracorporeal membrane oxygenation in a patient with amniotic fluid embolism. Acta Anaesthesiol Taiwan. 2009;47(2):99–102.
- Shen HP, Chang WC, Yeh LS, Ho M. Amniotic fluid embolism treated with emergency extracorporeal membrane oxygenation: A case report.
J Reprod Med. 2009;54(11–12):706–708. - Lee PH, Shulman MS, Vellayappan U, Symes JF, Olenchock SA Jr. Surgical treatment of amniotic fluid embolism with cardiopulmonary collapse. Ann Thorac Surg. 2010;90(5):1694–1696.
- Firstenberg MS, Abel E, Blais D, et al. Temporary extracorporeal circulatory support and pulmonary embolectomy for catastrophic amniotic fluid embolism. Heart Surg Forum. 2011;14(3):E157–E159.
- Ecker JL, Solt K, Fitzsimons MG, MacGillivray TE. Case records of the Massachusetts General Hospital. Case 40-2012: A 43-year-old woman with cardiorespiratory arrest after a cesarean section. N Engl J Med. 2012;367(26):2528–2536.
- Seldinger SI. Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta Radiol. 1953;39(5):368–376.
- Cheng R, Hachamovitch R, Kittelson M, et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann Thorac Surg. 2013; epub Nov 8.
- Rittenberger JC, Kelly E, Jang D, Greer K, Heffner A. Successful outcome utilizing hypothermia after cardiac arrest in pregnancy: A case report. Crit Care Med. 2008;36(4):1354–1356.
- Michelson AD, MacGregor H, Barnard MR, Krestin AS, Rohrer MJ, Valeri CR. Reversible inhibition of human platelet activation by hypothermia in vivo and in vitro. Thromb Haemost. 1994;71(5):633–640.
- Rivzi F, Mackey R, Barrett T, McKenna P, Geary M. Successful reduction of massive postpartum haemorrhage by use of guidelines and staff education. BJOG. 2004;111(5):495–498.
- Kramer MS, Rouleau J, Baskett TF, Joseph KS; Maternal Health Study Group of the Canadian Perinatal Surveillance System. Amniotic-fluid embolism and medical induction of labour: A retrospective, population-based cohort study. Lancet. 2006;368(9545):1444–1448.
- Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid embolism: A population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–49.e8.
- Tuffnell D, Knight M, Plaat F. Amniotic fluid embolism—An update. Anaesthesia. 2011;66(1):3–6.
- Knight M, Tuffnell D, Brocklehurst P, Spark P, Kurinczuk JJ; UK Obstetric Surveillance System. Incidence and risk factors for amniotic-fluid embolism. Obstet Gynecol. 2010;115(5):910–917.
- Kundra P, Khanna S, Habeebullahg S, Ravishankar M. Manual displacement of the uterus during Caesarean section. Anaesthesia. 2007;62(5):460–465.
- Katz VL, Dotters DJ, Droegemueller W. Perimortem cesarean delivery. Obstet Gynecol. 1986;68(4):571–576.
- Katz V, Balderston K, DeFreest M. Perimortem cesarean delivery: Were our assumptions correct? Am J Obstet Gynecol. 2005;192(6):1916–1920.
- Lipman SS, Daniels KI, Carvalho B, et al. Deficits in the provision of cardiopulmonary resuscitation during simulated obstetric crises. Am J Obstet Gynecol. 2010;203(2):179.e1–179.e5.
- Bell SF, Rayment R, Collins PW, Collis RE. The use of fibrinogen concentrate to correct hypofibrinogenaemia rapidly during obstetric haemorrhage. Int J Obstet Anesth. 2010;19(2):218–223.
- Sorensen B, Tang M, Larsen OH, Laursen PN, Fenger-Eriksen C, Rea CJ. The role of fibrinogen: A new paradigm in the treatment of coagulopathic bleeding. Thromb Res. 2011;128(Suppl 1):S13–S16.
- Rogers WK, Wernimont SA, Kumar GC, Bennett E, Chestnut DH. Acute hypotension associated with intraoperative cell salvage using a leukocyte depletion filter during management of obstetric hemorrhage due to amniotic fluid embolism. Anesth Analg. 2013;117(2):449–452.
- Collins NF, Bloor M, McDonnell NJ. Hyperfibrinolysis diagnosed by rotational thromboelastometry in a case of suspected amniotic fluid embolism. Int J Obstet Anesth. 2013;22(1):71–76.
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: Systematic review and cumulative meta-analysis. BMJ. 2012;344:e3054.
- Leighton BL, Wall MH, Lockhart EM, Phillips LE, Zatta AJ. Use of recombinant factor VIIa in patients with amniotic fluid embolism: A systematic review of case reports. Anesthesiology. 2011;115(6):1201–1208.
- Huber AW, Raio L, Alberio L, Ghezzi F, Surbek DV. Recombinant human factor VIIa prevents hysterectomy in severe postpartum hemorrhage: single center study. J Perinat Med. 2011;40(1):43–49.
- Dodgson J, Martin J, Boswell J, Goodall HB, Smith R. Probable amniotic fluid embolism precipitated by amniocentesis and treated by exchange transfusion. Brit Med J (Clin Res Ed). 1987;294(6583):1322–1323.
- Barbieri RL. A stitch in time: The B-Lynch, Hayman and Pereira uterine compression sutures. OBG Manage. 2012;24(12):6, 8, 10, 11.
- Barbieri RL. Have you made the best use of the Bakri balloon in PPH? OBG Manage. 2011;23(7):6, 8, 9.
- Belfort MA, Zimmerman J, Schemmer G, Oldroyd R, Smilanich R, Pearce M. Aortic compression and cross clamping in a case of placenta percreta and amniotic fluid embolism: A case report. AJP Rep. 2011;1(1):33–36.
- Dildy GA, Scott JR, Saffer CS, Belfort MA. An
effective pressure pack for severe pelvic hemorrhage. Obstet Gynecol. 2006;108(5):1222–1226. - Stanten RD, Iverson LI, Daugharty TM, Lovett SM, Terry C, Blumenstock E. Amniotic fluid embolism causing catastrophic pulmonary vasoconstriction: Diagnosis by transesophageal echocardiogram and treatment by cardiopulmonary bypass. Obstet Gynecol. 2003;102(3):496–498.
- Ho CH, Chen KB, Liu SK, Liu YF, Cheng HC, Wu RS. Early application of extracorporeal membrane oxygenation in a patient with amniotic fluid embolism. Acta Anaesthesiol Taiwan. 2009;47(2):99–102.
- Shen HP, Chang WC, Yeh LS, Ho M. Amniotic fluid embolism treated with emergency extracorporeal membrane oxygenation: A case report.
J Reprod Med. 2009;54(11–12):706–708. - Lee PH, Shulman MS, Vellayappan U, Symes JF, Olenchock SA Jr. Surgical treatment of amniotic fluid embolism with cardiopulmonary collapse. Ann Thorac Surg. 2010;90(5):1694–1696.
- Firstenberg MS, Abel E, Blais D, et al. Temporary extracorporeal circulatory support and pulmonary embolectomy for catastrophic amniotic fluid embolism. Heart Surg Forum. 2011;14(3):E157–E159.
- Ecker JL, Solt K, Fitzsimons MG, MacGillivray TE. Case records of the Massachusetts General Hospital. Case 40-2012: A 43-year-old woman with cardiorespiratory arrest after a cesarean section. N Engl J Med. 2012;367(26):2528–2536.
- Seldinger SI. Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta Radiol. 1953;39(5):368–376.
- Cheng R, Hachamovitch R, Kittelson M, et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann Thorac Surg. 2013; epub Nov 8.
- Rittenberger JC, Kelly E, Jang D, Greer K, Heffner A. Successful outcome utilizing hypothermia after cardiac arrest in pregnancy: A case report. Crit Care Med. 2008;36(4):1354–1356.
- Michelson AD, MacGregor H, Barnard MR, Krestin AS, Rohrer MJ, Valeri CR. Reversible inhibition of human platelet activation by hypothermia in vivo and in vitro. Thromb Haemost. 1994;71(5):633–640.
- Rivzi F, Mackey R, Barrett T, McKenna P, Geary M. Successful reduction of massive postpartum haemorrhage by use of guidelines and staff education. BJOG. 2004;111(5):495–498.
The generalist, the specialist, and the patient with chronic kidney disease

A key part of medical practice is managing professional relationships. This includes effective communication with each other: primary care provider, specialist, and patient in all permutations. I have previously written about how technologic advances both facilitate and hamper interphysician communication. But as payment models morph, as health systems become more complex and insulated, and as the medicine subspecialty workforce changes, the relationship between generalist and nonprocedural specialist will continue to evolve. I can offer personal testimony to the enormous value of sharing our electronic medical record with my nephrology colleagues within the institution; online (nondisruptive) management “conversation” is common in real time while I am with a patient in the office.
Gone is the time when referral was a necessary mechanism to build a practice, when a primary care physician would send everyone with an elevated alkaline phosphatase to the neighboring gastroenterologist, who in turn would send everyone without a primary care doctor to him or her. But there has always been the potential for professional, ego-based tension between primary care and nonprocedural specialist physicians, although this tension is rarely discussed. When does referral to a specialist by a general internist imply a lack of appropriate knowledge or an unwillingness to do an appropriate literature review? When should a specialist be concerned about “interfering” in primary care—by initiating more aggressive blood pressure control, or by giving the patient a needed vaccination? And what should be done if the patient decides to change the captain of the medical team? Maybe in the new medical care arena we will indeed function and be judged as a team, physician communication and transitions will be seamless, and all that matters will be the patient. Time will tell.
For now, the comanagement of patients with a chronic disease is often a challenge. The discussion by Sakhuja et al of patients with chronic kidney disease (CKD) highlights important clinical issues faced by primary care providers and nephrologists. With the increased diagnosis of early CKD, there may not be enough consulting nephrologists to see all these patients. And when CKD is diagnosed at an early stage, not all patients may warrant a specialist consultation. Yet the gaps in clinical care are clear. Too many patients with “a little” proteinuria or microhematuria do not get an adequate microscopic urinalysis to look for a treatable inflammatory renal disorder. Too many patients with a “slightly” elevated creatinine and blood pressure do not have their pressure aggressively treated, despite evidence that a systolic blood pressure in the high 130s is associated with more rapid progression of CKD. Should we establish expectations for ourselves, or should we just take a step back and refer all these patients to a nephrologist and await guidance? This is where I believe that a few clearly written and widely disseminated guidelines would help. Knowledge of appropriate and basic guidelines for diagnosing and managing common disorders (not just CKD) should be the focus of continuing medical education and should be required for maintaining certification for all internists, including specialists. But, as always, guidelines often need to be tailored for the patient in our examining room.
There are nuances in the care of patients with CKD that, as a nonspecialist, I will not automatically know need to be implemented. As an internist, I should know the value of starting inhibition of the angiotensin pathway in patients with proteinuria, but as CKD progresses in a specific patient, should this be decreased? Should I initiate urate-lowering therapy,1 hoping to slow the rate of my patient’s renal demise?
When do we know enough to know that we do not need to ask for a specialist’s input? How well do we self-assess our clinical knowledge and skills? How can we achieve the right balance between referral and self-management? We try to save our patient the cost of the time and the copayment to see a specialist, and with bundled care we try to minimize consultant fees and time. But in the meantime, are we ordering unnecessary tests or delaying appropriate therapy?
As we think about the comanagement of patients with CKD, we need to recognize and utilize the nuanced improvements in care that our nephrology colleagues can provide. As non-nephrologists, we should be able to start a thoughtful diagnostic evaluation. For example, an antinuclear antibody test in the absence of evidence of glomerulonephritis is not likely to be informative in determining the cause of an isolated elevated creatinine; a urinalysis is. We should be able to recognize potential renal injury (proteinuria, decreased glomerular filtration rate, microhematuria, hypertension), and initiate aggressive mitigation of factors that are known to enhance progression of the CKD (proteinuria, hypertension) and contribute to the significant morbidity and mortality of CKD-associated cardiovascular disease.
We should already be managing hypertension, diabetes, and hyperlipidemia, but CKD should be a red flag, driving us to more aggressively control these comorbidities, and driving us to do better than control only the estimated 46.4% of hypertensive patients in 2009 and 2010 whose hypertension was adequately controlled.2 There is no reason for us to step back and wait for direction in addressing these most common issues. And our specialist colleagues will be there to efficiently assist in refining the nuances of care.
- Levy GD, Rashid N, Niu F, Cheetham TC. Effect of urate-lowering therapies on renal disease progression in patients with hyperuricemia. J Rheumatol 2014; Apr 1, doi: 10.3899/jrheum.131159. Epub ahead of print.
- Guo F, He D, Zhang W, Walton RG. Trends in prevalence, awareness, management, and control of hypertension among United States adults, 1999 to 2010. J Am Coll Cardiol 2012; 60:599–606.
A key part of medical practice is managing professional relationships. This includes effective communication with each other: primary care provider, specialist, and patient in all permutations. I have previously written about how technologic advances both facilitate and hamper interphysician communication. But as payment models morph, as health systems become more complex and insulated, and as the medicine subspecialty workforce changes, the relationship between generalist and nonprocedural specialist will continue to evolve. I can offer personal testimony to the enormous value of sharing our electronic medical record with my nephrology colleagues within the institution; online (nondisruptive) management “conversation” is common in real time while I am with a patient in the office.
Gone is the time when referral was a necessary mechanism to build a practice, when a primary care physician would send everyone with an elevated alkaline phosphatase to the neighboring gastroenterologist, who in turn would send everyone without a primary care doctor to him or her. But there has always been the potential for professional, ego-based tension between primary care and nonprocedural specialist physicians, although this tension is rarely discussed. When does referral to a specialist by a general internist imply a lack of appropriate knowledge or an unwillingness to do an appropriate literature review? When should a specialist be concerned about “interfering” in primary care—by initiating more aggressive blood pressure control, or by giving the patient a needed vaccination? And what should be done if the patient decides to change the captain of the medical team? Maybe in the new medical care arena we will indeed function and be judged as a team, physician communication and transitions will be seamless, and all that matters will be the patient. Time will tell.
For now, the comanagement of patients with a chronic disease is often a challenge. The discussion by Sakhuja et al of patients with chronic kidney disease (CKD) highlights important clinical issues faced by primary care providers and nephrologists. With the increased diagnosis of early CKD, there may not be enough consulting nephrologists to see all these patients. And when CKD is diagnosed at an early stage, not all patients may warrant a specialist consultation. Yet the gaps in clinical care are clear. Too many patients with “a little” proteinuria or microhematuria do not get an adequate microscopic urinalysis to look for a treatable inflammatory renal disorder. Too many patients with a “slightly” elevated creatinine and blood pressure do not have their pressure aggressively treated, despite evidence that a systolic blood pressure in the high 130s is associated with more rapid progression of CKD. Should we establish expectations for ourselves, or should we just take a step back and refer all these patients to a nephrologist and await guidance? This is where I believe that a few clearly written and widely disseminated guidelines would help. Knowledge of appropriate and basic guidelines for diagnosing and managing common disorders (not just CKD) should be the focus of continuing medical education and should be required for maintaining certification for all internists, including specialists. But, as always, guidelines often need to be tailored for the patient in our examining room.
There are nuances in the care of patients with CKD that, as a nonspecialist, I will not automatically know need to be implemented. As an internist, I should know the value of starting inhibition of the angiotensin pathway in patients with proteinuria, but as CKD progresses in a specific patient, should this be decreased? Should I initiate urate-lowering therapy,1 hoping to slow the rate of my patient’s renal demise?
When do we know enough to know that we do not need to ask for a specialist’s input? How well do we self-assess our clinical knowledge and skills? How can we achieve the right balance between referral and self-management? We try to save our patient the cost of the time and the copayment to see a specialist, and with bundled care we try to minimize consultant fees and time. But in the meantime, are we ordering unnecessary tests or delaying appropriate therapy?
As we think about the comanagement of patients with CKD, we need to recognize and utilize the nuanced improvements in care that our nephrology colleagues can provide. As non-nephrologists, we should be able to start a thoughtful diagnostic evaluation. For example, an antinuclear antibody test in the absence of evidence of glomerulonephritis is not likely to be informative in determining the cause of an isolated elevated creatinine; a urinalysis is. We should be able to recognize potential renal injury (proteinuria, decreased glomerular filtration rate, microhematuria, hypertension), and initiate aggressive mitigation of factors that are known to enhance progression of the CKD (proteinuria, hypertension) and contribute to the significant morbidity and mortality of CKD-associated cardiovascular disease.
We should already be managing hypertension, diabetes, and hyperlipidemia, but CKD should be a red flag, driving us to more aggressively control these comorbidities, and driving us to do better than control only the estimated 46.4% of hypertensive patients in 2009 and 2010 whose hypertension was adequately controlled.2 There is no reason for us to step back and wait for direction in addressing these most common issues. And our specialist colleagues will be there to efficiently assist in refining the nuances of care.
A key part of medical practice is managing professional relationships. This includes effective communication with each other: primary care provider, specialist, and patient in all permutations. I have previously written about how technologic advances both facilitate and hamper interphysician communication. But as payment models morph, as health systems become more complex and insulated, and as the medicine subspecialty workforce changes, the relationship between generalist and nonprocedural specialist will continue to evolve. I can offer personal testimony to the enormous value of sharing our electronic medical record with my nephrology colleagues within the institution; online (nondisruptive) management “conversation” is common in real time while I am with a patient in the office.
Gone is the time when referral was a necessary mechanism to build a practice, when a primary care physician would send everyone with an elevated alkaline phosphatase to the neighboring gastroenterologist, who in turn would send everyone without a primary care doctor to him or her. But there has always been the potential for professional, ego-based tension between primary care and nonprocedural specialist physicians, although this tension is rarely discussed. When does referral to a specialist by a general internist imply a lack of appropriate knowledge or an unwillingness to do an appropriate literature review? When should a specialist be concerned about “interfering” in primary care—by initiating more aggressive blood pressure control, or by giving the patient a needed vaccination? And what should be done if the patient decides to change the captain of the medical team? Maybe in the new medical care arena we will indeed function and be judged as a team, physician communication and transitions will be seamless, and all that matters will be the patient. Time will tell.
For now, the comanagement of patients with a chronic disease is often a challenge. The discussion by Sakhuja et al of patients with chronic kidney disease (CKD) highlights important clinical issues faced by primary care providers and nephrologists. With the increased diagnosis of early CKD, there may not be enough consulting nephrologists to see all these patients. And when CKD is diagnosed at an early stage, not all patients may warrant a specialist consultation. Yet the gaps in clinical care are clear. Too many patients with “a little” proteinuria or microhematuria do not get an adequate microscopic urinalysis to look for a treatable inflammatory renal disorder. Too many patients with a “slightly” elevated creatinine and blood pressure do not have their pressure aggressively treated, despite evidence that a systolic blood pressure in the high 130s is associated with more rapid progression of CKD. Should we establish expectations for ourselves, or should we just take a step back and refer all these patients to a nephrologist and await guidance? This is where I believe that a few clearly written and widely disseminated guidelines would help. Knowledge of appropriate and basic guidelines for diagnosing and managing common disorders (not just CKD) should be the focus of continuing medical education and should be required for maintaining certification for all internists, including specialists. But, as always, guidelines often need to be tailored for the patient in our examining room.
There are nuances in the care of patients with CKD that, as a nonspecialist, I will not automatically know need to be implemented. As an internist, I should know the value of starting inhibition of the angiotensin pathway in patients with proteinuria, but as CKD progresses in a specific patient, should this be decreased? Should I initiate urate-lowering therapy,1 hoping to slow the rate of my patient’s renal demise?
When do we know enough to know that we do not need to ask for a specialist’s input? How well do we self-assess our clinical knowledge and skills? How can we achieve the right balance between referral and self-management? We try to save our patient the cost of the time and the copayment to see a specialist, and with bundled care we try to minimize consultant fees and time. But in the meantime, are we ordering unnecessary tests or delaying appropriate therapy?
As we think about the comanagement of patients with CKD, we need to recognize and utilize the nuanced improvements in care that our nephrology colleagues can provide. As non-nephrologists, we should be able to start a thoughtful diagnostic evaluation. For example, an antinuclear antibody test in the absence of evidence of glomerulonephritis is not likely to be informative in determining the cause of an isolated elevated creatinine; a urinalysis is. We should be able to recognize potential renal injury (proteinuria, decreased glomerular filtration rate, microhematuria, hypertension), and initiate aggressive mitigation of factors that are known to enhance progression of the CKD (proteinuria, hypertension) and contribute to the significant morbidity and mortality of CKD-associated cardiovascular disease.
We should already be managing hypertension, diabetes, and hyperlipidemia, but CKD should be a red flag, driving us to more aggressively control these comorbidities, and driving us to do better than control only the estimated 46.4% of hypertensive patients in 2009 and 2010 whose hypertension was adequately controlled.2 There is no reason for us to step back and wait for direction in addressing these most common issues. And our specialist colleagues will be there to efficiently assist in refining the nuances of care.
- Levy GD, Rashid N, Niu F, Cheetham TC. Effect of urate-lowering therapies on renal disease progression in patients with hyperuricemia. J Rheumatol 2014; Apr 1, doi: 10.3899/jrheum.131159. Epub ahead of print.
- Guo F, He D, Zhang W, Walton RG. Trends in prevalence, awareness, management, and control of hypertension among United States adults, 1999 to 2010. J Am Coll Cardiol 2012; 60:599–606.
- Levy GD, Rashid N, Niu F, Cheetham TC. Effect of urate-lowering therapies on renal disease progression in patients with hyperuricemia. J Rheumatol 2014; Apr 1, doi: 10.3899/jrheum.131159. Epub ahead of print.
- Guo F, He D, Zhang W, Walton RG. Trends in prevalence, awareness, management, and control of hypertension among United States adults, 1999 to 2010. J Am Coll Cardiol 2012; 60:599–606.
100 years of solicitude: Do global traumatic events have a transgenerational effect?
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
Taking on racial and ethnic disparities in cancer care
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Continuity of Patient Care: A Value Worth Preserving
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.

Appreciating the appetite for reflective practice
The article by Dickstein et al on eating disorders in this issue of the Journal made me think about my experience long ago as an internist comanaging patients who had severe eating disorders.
As a rheumatologist, I noticed that these young women had a very high prevalence of fibromyalgia and associated visceral pain syndromes such as irritable bowel syndrome and interstitial cystitis. Because they had been experiencing fatigue and generalized pain, many of them had been tested for lupus. Since about 20% of young women may have a low-positive antinuclear antibody titer, some of these patients had been diagnosed with lupus, and some had been offered therapy.
Other factors reinforced their physicians’ appropriate concerns about possible connective tissue disease. For example, modest leukopenia is not infrequent in malnourished patients, and Raynaud phenomenon is common in young women. Bulimia is associated with gastroesophageal dysmotility, and some of these women had slightly elevated creatine kinase levels. These abnormalities were generally the result of over-vigorous exercise, ipecac use, emesis, and hypokalemia. However, myositis or scleroderma overlap syndromes had occasionally been diagnosed in some patients, especially when the severity of the primary eating disorder was unappreciated.
Many, including myself, have written about the strengths and limitations of evidence-based medicine. We routinely make both evidence- and experience-based clinical decisions, often with little time to reflect on the exact reason for each decision. As I think back on my stint in the eating disorders clinic, recalling individual patients and lessons learned, I am struck by how observation-based my management of those patients was and how those experiences have stuck with me.
Reflective clinical care (also known as anecdotal experience) can have a lasting impact on the way we practice. Twenty-five years later, I still think about eating disorders when I evaluate young women who have severe fibromyalgia.
The article by Dickstein et al on eating disorders in this issue of the Journal made me think about my experience long ago as an internist comanaging patients who had severe eating disorders.
As a rheumatologist, I noticed that these young women had a very high prevalence of fibromyalgia and associated visceral pain syndromes such as irritable bowel syndrome and interstitial cystitis. Because they had been experiencing fatigue and generalized pain, many of them had been tested for lupus. Since about 20% of young women may have a low-positive antinuclear antibody titer, some of these patients had been diagnosed with lupus, and some had been offered therapy.
Other factors reinforced their physicians’ appropriate concerns about possible connective tissue disease. For example, modest leukopenia is not infrequent in malnourished patients, and Raynaud phenomenon is common in young women. Bulimia is associated with gastroesophageal dysmotility, and some of these women had slightly elevated creatine kinase levels. These abnormalities were generally the result of over-vigorous exercise, ipecac use, emesis, and hypokalemia. However, myositis or scleroderma overlap syndromes had occasionally been diagnosed in some patients, especially when the severity of the primary eating disorder was unappreciated.
Many, including myself, have written about the strengths and limitations of evidence-based medicine. We routinely make both evidence- and experience-based clinical decisions, often with little time to reflect on the exact reason for each decision. As I think back on my stint in the eating disorders clinic, recalling individual patients and lessons learned, I am struck by how observation-based my management of those patients was and how those experiences have stuck with me.
Reflective clinical care (also known as anecdotal experience) can have a lasting impact on the way we practice. Twenty-five years later, I still think about eating disorders when I evaluate young women who have severe fibromyalgia.
The article by Dickstein et al on eating disorders in this issue of the Journal made me think about my experience long ago as an internist comanaging patients who had severe eating disorders.
As a rheumatologist, I noticed that these young women had a very high prevalence of fibromyalgia and associated visceral pain syndromes such as irritable bowel syndrome and interstitial cystitis. Because they had been experiencing fatigue and generalized pain, many of them had been tested for lupus. Since about 20% of young women may have a low-positive antinuclear antibody titer, some of these patients had been diagnosed with lupus, and some had been offered therapy.
Other factors reinforced their physicians’ appropriate concerns about possible connective tissue disease. For example, modest leukopenia is not infrequent in malnourished patients, and Raynaud phenomenon is common in young women. Bulimia is associated with gastroesophageal dysmotility, and some of these women had slightly elevated creatine kinase levels. These abnormalities were generally the result of over-vigorous exercise, ipecac use, emesis, and hypokalemia. However, myositis or scleroderma overlap syndromes had occasionally been diagnosed in some patients, especially when the severity of the primary eating disorder was unappreciated.
Many, including myself, have written about the strengths and limitations of evidence-based medicine. We routinely make both evidence- and experience-based clinical decisions, often with little time to reflect on the exact reason for each decision. As I think back on my stint in the eating disorders clinic, recalling individual patients and lessons learned, I am struck by how observation-based my management of those patients was and how those experiences have stuck with me.
Reflective clinical care (also known as anecdotal experience) can have a lasting impact on the way we practice. Twenty-five years later, I still think about eating disorders when I evaluate young women who have severe fibromyalgia.
Q: Following cesarean delivery, what is the optimal oxytocin infusion duration to prevent postpartum bleeding?
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.

Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at rbarbieri@frontlinemedcom.com Please include your name and city and state.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.

Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
rbarbieri@frontlinemedcom.com
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
rbarbieri@frontlinemedcom.com
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
rbarbieri@frontlinemedcom.com
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.
Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at rbarbieri@frontlinemedcom.com Please include your name and city and state.
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.
Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at rbarbieri@frontlinemedcom.com Please include your name and city and state.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.

From our pages to your practice
We have some interesting and insightful articles lined up for you this month, beginning with a Commentary by Samuel and Stone on treating HER2-positive breast cancer and asking whether the era of trastuzumab therapy is over. The Commentary and accompanying Community Translations report explore the use of pertuzumab and trastuzumab together, especially in the neoadjuvant setting. The Cleopatra trial has already shown that combining pertuzumab with trastuzumab plus docetaxel as a first-line treatment for HER2-positive metastatic breast cancer significantly prolonged progression-free survival with no increase in cardiac toxic effects, compared with placebo plus trastuzumab plus docetaxel, so perhaps using pertuzumab and trastuzumab upfront might be equally successful.
Click on the PDF icon at the top of this introduction to read the full article.
We have some interesting and insightful articles lined up for you this month, beginning with a Commentary by Samuel and Stone on treating HER2-positive breast cancer and asking whether the era of trastuzumab therapy is over. The Commentary and accompanying Community Translations report explore the use of pertuzumab and trastuzumab together, especially in the neoadjuvant setting. The Cleopatra trial has already shown that combining pertuzumab with trastuzumab plus docetaxel as a first-line treatment for HER2-positive metastatic breast cancer significantly prolonged progression-free survival with no increase in cardiac toxic effects, compared with placebo plus trastuzumab plus docetaxel, so perhaps using pertuzumab and trastuzumab upfront might be equally successful.
Click on the PDF icon at the top of this introduction to read the full article.
We have some interesting and insightful articles lined up for you this month, beginning with a Commentary by Samuel and Stone on treating HER2-positive breast cancer and asking whether the era of trastuzumab therapy is over. The Commentary and accompanying Community Translations report explore the use of pertuzumab and trastuzumab together, especially in the neoadjuvant setting. The Cleopatra trial has already shown that combining pertuzumab with trastuzumab plus docetaxel as a first-line treatment for HER2-positive metastatic breast cancer significantly prolonged progression-free survival with no increase in cardiac toxic effects, compared with placebo plus trastuzumab plus docetaxel, so perhaps using pertuzumab and trastuzumab upfront might be equally successful.
Click on the PDF icon at the top of this introduction to read the full article.
Borderline personality disorder is a heritable brain disease
The prevailing view among many psychiatrists and mental health professionals is that borderline personality disorder (BPD) is a “psychological” condition. BPD often is conceptualized as a behavioral consequence of childhood trauma; treatment approaches have emphasized intensive psychotherapeutic modalities, less so biologic interventions. You might not be aware that a large body of research over the past decade provides strong evidence that BPD is a neurobiological illness—a finding that would drastically alter how the disorder should be conceptualized and managed.
Neuropathology underpins the personality disorder
Foremost, BPD must be regarded as a serious, disabling brain disorder, not simply an aberration of personality. In DSM-5, symptoms of BPD are listed as: feelings of abandonment; unstable and intense interpersonal relationships; unstable sense of self; impulsivity; suicidal or self-mutilating behavior; affective instability (dysphoria, irritability, anxiety); chronic feelings of emptiness; intense anger episodes; and transient paranoid or dissociative symptoms. Clearly, these clusters of psychopathological and behavioral symptoms reflect a pervasive brain disorder associated with abnormal neurobiology and neural circuitry that might, at times, stubbornly defy therapeutic intervention.
No wonder that 42 published studies report that, compared with healthy controls, people who have BPD display extensive cortical and subcortical abnormalities in brain structure and function.1 These anomalous patterns have been detected across all 4 available neuroimaging techniques.
Magnetic resonance imaging. MRI studies have revealed the following abnormalities in BPD:
• hypoplasia of the hippocampus, caudate, and dorsolateral prefrontal cortex
• variations in the CA1 region of the hippocampus and subiculum
• smaller-than-normal orbitofrontal cortex (by 24%, compared with healthy controls) and the mid-temporal and left cingulate gyrii (by 26%)
• larger-than-normal volume of the right inferior parietal cortex and the right parahippocampal gyrus
• loss of gray matter in the frontal, temporal, and parietal cortices
• an enlarged third cerebral ventricle
• in women, reduced size of the medial temporal lobe and amygdala
• in men, a decreased concentration of gray matter in the anterior cingulate
• reversal of normal right-greater-than-left asymmetry of the orbitofrontal cortex gray matter, reflecting loss of gray matter on the right side
• a lower concentration of gray matter in the rostral/subgenual anterior cingulate cortex
• a smaller frontal lobe.
In an analysis of MRI studies,2 correlation was found between structural brain abnormalities and specific symptoms of BPD, such as impulsivity, suicidality, and aggression. These findings might someday guide personalized interventions—for example, using neurostimulation techniques such as repetitive transcranial magnetic stimulation and deep brain stimulation—to modulate the activity of a given region of the brain (depending on which symptom is most prominent or disabling).
Magnetic resonance spectroscopy. In BPD, MRS studies reveal:
• compared with controls, a higher glutamate level in the anterior cingulate cortex
• reduced levels of N-acetyl aspartate (NAA; found in neurons) and creatinine in the left amygdala
• a reduction (on average, 19%) in the NAA concentration in the dorsolateral prefrontal cortex.
Functional magnetic resonance imaging. From fMRI studies, there is evidence in BPD of:
• greater activation of the amygdala and prolonged return to baseline
• increased functional connectivity in the left frontopolar cortex and left insula
• decreased connectivity in the left cuneus and left inferior parietal and the right middle temporal lobes
• marked frontal hypometabolism
• hypermetabolism in the motor cortex, medial and anterior cingulate, and occipital and temporal poles
• lower connectivity between the amygdala during a neutral stimulus
• higher connectivity between the amygdala during fear stimulus
• higher connectivity between the amygdala during fear stimulus
• deactivation of the opioid system in the left nucleus accumbens, hypothalamus, and hippocampus
• hyperactivation of the left medial prefrontal cortex during social exclusion
• more mistakes made in differentiating an emotional and a neutral facial expression.
Diffusion tensor imaging. DTI white-matter integrity studies of BPD show:
• a bilateral decrease in fractional anisotropy (FA) in frontal, uncinated, and occipitalfrontal fasciculi
• a decrease in FA in the genu and rostrum of the corpus callosum
• a decrease in inter-hemispheric connectivity between right and left anterior cigulate cortices.
Genetic Studies
There is substantial scientific evidence that BPD is highly heritable—a finding that suggests that brain abnormalities of this disorder are a consequence of genes involved in brain development (similar to what is known about schizophrenia, bipolar disorder, and autism).
A systematic review of the heritability of BPD examined 59 published studies that were categorized into 12 family studies, 18 twin studies, 24 association studies, and 5 gene-environment interaction studies.3 The authors concluded that BPD has a strong genetic component, although there also is evidence of gene-environment (G.E) interactions (ie, how nature and nurture influence each other).
The G.E interaction model appears to be consistent with the theory that expression of plasticity genes is modified by childhood experiences and environment, such as physical or sexual abuse. Some studies have found evidence of hypermethylation in BPD, which can exert epigenetic effects. Childhood abuse might, therefore, disrupt certain neuroplasticity genes, culminating in morphological, neurochemical, metabolic, and white-matter aberrations—leading to pathological behavioral patterns identified as BPD.
The neuropsychiatric basis of BPD must guide treatment
There is no such thing as a purely psychological disorder: Invariably, it is an abnormality of brain circuits that disrupts normal development of emotions, thought, behavior, and social cognition. BPD is an exemplar of such neuropsychiatric illness, and treatment should support psychotherapeutic approaches to mend the mind at the same time it moves aggressively to repair the brain.
1. McKenzie CE, Nasrallah HA. Neuroimaging abnormalities in borderline personality disorder: MRI, MRS, fMRI and DTI findings. Poster presented at: 52nd Annual Meeting of the American College of Neuropsychopharmacology; December 8-12, 2013; Hollywood, FL.
2. McKenzie CE, Nasrallah HA. Clinical symptoms of borderline personality disorder are associated with cortical and subcortical abnormalities on brain magnetic resonance imaging (MRI). Poster presented at: 26th Annual Meeting of the U.S. Psychiatric and Mental Health Congress; September 31-October 3, 2013; Las Vegas, NV.
3. Amad A, Ramoz N, Thomas P, et al. Genetics of borderline personality disorder: systematic review and proposal of an integrative model. Neurosci Biobehav Rev. 2014;40C:6-19.
The prevailing view among many psychiatrists and mental health professionals is that borderline personality disorder (BPD) is a “psychological” condition. BPD often is conceptualized as a behavioral consequence of childhood trauma; treatment approaches have emphasized intensive psychotherapeutic modalities, less so biologic interventions. You might not be aware that a large body of research over the past decade provides strong evidence that BPD is a neurobiological illness—a finding that would drastically alter how the disorder should be conceptualized and managed.
Neuropathology underpins the personality disorder
Foremost, BPD must be regarded as a serious, disabling brain disorder, not simply an aberration of personality. In DSM-5, symptoms of BPD are listed as: feelings of abandonment; unstable and intense interpersonal relationships; unstable sense of self; impulsivity; suicidal or self-mutilating behavior; affective instability (dysphoria, irritability, anxiety); chronic feelings of emptiness; intense anger episodes; and transient paranoid or dissociative symptoms. Clearly, these clusters of psychopathological and behavioral symptoms reflect a pervasive brain disorder associated with abnormal neurobiology and neural circuitry that might, at times, stubbornly defy therapeutic intervention.
No wonder that 42 published studies report that, compared with healthy controls, people who have BPD display extensive cortical and subcortical abnormalities in brain structure and function.1 These anomalous patterns have been detected across all 4 available neuroimaging techniques.
Magnetic resonance imaging. MRI studies have revealed the following abnormalities in BPD:
• hypoplasia of the hippocampus, caudate, and dorsolateral prefrontal cortex
• variations in the CA1 region of the hippocampus and subiculum
• smaller-than-normal orbitofrontal cortex (by 24%, compared with healthy controls) and the mid-temporal and left cingulate gyrii (by 26%)
• larger-than-normal volume of the right inferior parietal cortex and the right parahippocampal gyrus
• loss of gray matter in the frontal, temporal, and parietal cortices
• an enlarged third cerebral ventricle
• in women, reduced size of the medial temporal lobe and amygdala
• in men, a decreased concentration of gray matter in the anterior cingulate
• reversal of normal right-greater-than-left asymmetry of the orbitofrontal cortex gray matter, reflecting loss of gray matter on the right side
• a lower concentration of gray matter in the rostral/subgenual anterior cingulate cortex
• a smaller frontal lobe.
In an analysis of MRI studies,2 correlation was found between structural brain abnormalities and specific symptoms of BPD, such as impulsivity, suicidality, and aggression. These findings might someday guide personalized interventions—for example, using neurostimulation techniques such as repetitive transcranial magnetic stimulation and deep brain stimulation—to modulate the activity of a given region of the brain (depending on which symptom is most prominent or disabling).
Magnetic resonance spectroscopy. In BPD, MRS studies reveal:
• compared with controls, a higher glutamate level in the anterior cingulate cortex
• reduced levels of N-acetyl aspartate (NAA; found in neurons) and creatinine in the left amygdala
• a reduction (on average, 19%) in the NAA concentration in the dorsolateral prefrontal cortex.
Functional magnetic resonance imaging. From fMRI studies, there is evidence in BPD of:
• greater activation of the amygdala and prolonged return to baseline
• increased functional connectivity in the left frontopolar cortex and left insula
• decreased connectivity in the left cuneus and left inferior parietal and the right middle temporal lobes
• marked frontal hypometabolism
• hypermetabolism in the motor cortex, medial and anterior cingulate, and occipital and temporal poles
• lower connectivity between the amygdala during a neutral stimulus
• higher connectivity between the amygdala during fear stimulus
• higher connectivity between the amygdala during fear stimulus
• deactivation of the opioid system in the left nucleus accumbens, hypothalamus, and hippocampus
• hyperactivation of the left medial prefrontal cortex during social exclusion
• more mistakes made in differentiating an emotional and a neutral facial expression.
Diffusion tensor imaging. DTI white-matter integrity studies of BPD show:
• a bilateral decrease in fractional anisotropy (FA) in frontal, uncinated, and occipitalfrontal fasciculi
• a decrease in FA in the genu and rostrum of the corpus callosum
• a decrease in inter-hemispheric connectivity between right and left anterior cigulate cortices.
Genetic Studies
There is substantial scientific evidence that BPD is highly heritable—a finding that suggests that brain abnormalities of this disorder are a consequence of genes involved in brain development (similar to what is known about schizophrenia, bipolar disorder, and autism).
A systematic review of the heritability of BPD examined 59 published studies that were categorized into 12 family studies, 18 twin studies, 24 association studies, and 5 gene-environment interaction studies.3 The authors concluded that BPD has a strong genetic component, although there also is evidence of gene-environment (G.E) interactions (ie, how nature and nurture influence each other).
The G.E interaction model appears to be consistent with the theory that expression of plasticity genes is modified by childhood experiences and environment, such as physical or sexual abuse. Some studies have found evidence of hypermethylation in BPD, which can exert epigenetic effects. Childhood abuse might, therefore, disrupt certain neuroplasticity genes, culminating in morphological, neurochemical, metabolic, and white-matter aberrations—leading to pathological behavioral patterns identified as BPD.
The neuropsychiatric basis of BPD must guide treatment
There is no such thing as a purely psychological disorder: Invariably, it is an abnormality of brain circuits that disrupts normal development of emotions, thought, behavior, and social cognition. BPD is an exemplar of such neuropsychiatric illness, and treatment should support psychotherapeutic approaches to mend the mind at the same time it moves aggressively to repair the brain.
The prevailing view among many psychiatrists and mental health professionals is that borderline personality disorder (BPD) is a “psychological” condition. BPD often is conceptualized as a behavioral consequence of childhood trauma; treatment approaches have emphasized intensive psychotherapeutic modalities, less so biologic interventions. You might not be aware that a large body of research over the past decade provides strong evidence that BPD is a neurobiological illness—a finding that would drastically alter how the disorder should be conceptualized and managed.
Neuropathology underpins the personality disorder
Foremost, BPD must be regarded as a serious, disabling brain disorder, not simply an aberration of personality. In DSM-5, symptoms of BPD are listed as: feelings of abandonment; unstable and intense interpersonal relationships; unstable sense of self; impulsivity; suicidal or self-mutilating behavior; affective instability (dysphoria, irritability, anxiety); chronic feelings of emptiness; intense anger episodes; and transient paranoid or dissociative symptoms. Clearly, these clusters of psychopathological and behavioral symptoms reflect a pervasive brain disorder associated with abnormal neurobiology and neural circuitry that might, at times, stubbornly defy therapeutic intervention.
No wonder that 42 published studies report that, compared with healthy controls, people who have BPD display extensive cortical and subcortical abnormalities in brain structure and function.1 These anomalous patterns have been detected across all 4 available neuroimaging techniques.
Magnetic resonance imaging. MRI studies have revealed the following abnormalities in BPD:
• hypoplasia of the hippocampus, caudate, and dorsolateral prefrontal cortex
• variations in the CA1 region of the hippocampus and subiculum
• smaller-than-normal orbitofrontal cortex (by 24%, compared with healthy controls) and the mid-temporal and left cingulate gyrii (by 26%)
• larger-than-normal volume of the right inferior parietal cortex and the right parahippocampal gyrus
• loss of gray matter in the frontal, temporal, and parietal cortices
• an enlarged third cerebral ventricle
• in women, reduced size of the medial temporal lobe and amygdala
• in men, a decreased concentration of gray matter in the anterior cingulate
• reversal of normal right-greater-than-left asymmetry of the orbitofrontal cortex gray matter, reflecting loss of gray matter on the right side
• a lower concentration of gray matter in the rostral/subgenual anterior cingulate cortex
• a smaller frontal lobe.
In an analysis of MRI studies,2 correlation was found between structural brain abnormalities and specific symptoms of BPD, such as impulsivity, suicidality, and aggression. These findings might someday guide personalized interventions—for example, using neurostimulation techniques such as repetitive transcranial magnetic stimulation and deep brain stimulation—to modulate the activity of a given region of the brain (depending on which symptom is most prominent or disabling).
Magnetic resonance spectroscopy. In BPD, MRS studies reveal:
• compared with controls, a higher glutamate level in the anterior cingulate cortex
• reduced levels of N-acetyl aspartate (NAA; found in neurons) and creatinine in the left amygdala
• a reduction (on average, 19%) in the NAA concentration in the dorsolateral prefrontal cortex.
Functional magnetic resonance imaging. From fMRI studies, there is evidence in BPD of:
• greater activation of the amygdala and prolonged return to baseline
• increased functional connectivity in the left frontopolar cortex and left insula
• decreased connectivity in the left cuneus and left inferior parietal and the right middle temporal lobes
• marked frontal hypometabolism
• hypermetabolism in the motor cortex, medial and anterior cingulate, and occipital and temporal poles
• lower connectivity between the amygdala during a neutral stimulus
• higher connectivity between the amygdala during fear stimulus
• higher connectivity between the amygdala during fear stimulus
• deactivation of the opioid system in the left nucleus accumbens, hypothalamus, and hippocampus
• hyperactivation of the left medial prefrontal cortex during social exclusion
• more mistakes made in differentiating an emotional and a neutral facial expression.
Diffusion tensor imaging. DTI white-matter integrity studies of BPD show:
• a bilateral decrease in fractional anisotropy (FA) in frontal, uncinated, and occipitalfrontal fasciculi
• a decrease in FA in the genu and rostrum of the corpus callosum
• a decrease in inter-hemispheric connectivity between right and left anterior cigulate cortices.
Genetic Studies
There is substantial scientific evidence that BPD is highly heritable—a finding that suggests that brain abnormalities of this disorder are a consequence of genes involved in brain development (similar to what is known about schizophrenia, bipolar disorder, and autism).
A systematic review of the heritability of BPD examined 59 published studies that were categorized into 12 family studies, 18 twin studies, 24 association studies, and 5 gene-environment interaction studies.3 The authors concluded that BPD has a strong genetic component, although there also is evidence of gene-environment (G.E) interactions (ie, how nature and nurture influence each other).
The G.E interaction model appears to be consistent with the theory that expression of plasticity genes is modified by childhood experiences and environment, such as physical or sexual abuse. Some studies have found evidence of hypermethylation in BPD, which can exert epigenetic effects. Childhood abuse might, therefore, disrupt certain neuroplasticity genes, culminating in morphological, neurochemical, metabolic, and white-matter aberrations—leading to pathological behavioral patterns identified as BPD.
The neuropsychiatric basis of BPD must guide treatment
There is no such thing as a purely psychological disorder: Invariably, it is an abnormality of brain circuits that disrupts normal development of emotions, thought, behavior, and social cognition. BPD is an exemplar of such neuropsychiatric illness, and treatment should support psychotherapeutic approaches to mend the mind at the same time it moves aggressively to repair the brain.
1. McKenzie CE, Nasrallah HA. Neuroimaging abnormalities in borderline personality disorder: MRI, MRS, fMRI and DTI findings. Poster presented at: 52nd Annual Meeting of the American College of Neuropsychopharmacology; December 8-12, 2013; Hollywood, FL.
2. McKenzie CE, Nasrallah HA. Clinical symptoms of borderline personality disorder are associated with cortical and subcortical abnormalities on brain magnetic resonance imaging (MRI). Poster presented at: 26th Annual Meeting of the U.S. Psychiatric and Mental Health Congress; September 31-October 3, 2013; Las Vegas, NV.
3. Amad A, Ramoz N, Thomas P, et al. Genetics of borderline personality disorder: systematic review and proposal of an integrative model. Neurosci Biobehav Rev. 2014;40C:6-19.
1. McKenzie CE, Nasrallah HA. Neuroimaging abnormalities in borderline personality disorder: MRI, MRS, fMRI and DTI findings. Poster presented at: 52nd Annual Meeting of the American College of Neuropsychopharmacology; December 8-12, 2013; Hollywood, FL.
2. McKenzie CE, Nasrallah HA. Clinical symptoms of borderline personality disorder are associated with cortical and subcortical abnormalities on brain magnetic resonance imaging (MRI). Poster presented at: 26th Annual Meeting of the U.S. Psychiatric and Mental Health Congress; September 31-October 3, 2013; Las Vegas, NV.
3. Amad A, Ramoz N, Thomas P, et al. Genetics of borderline personality disorder: systematic review and proposal of an integrative model. Neurosci Biobehav Rev. 2014;40C:6-19.