User login
Pooling knowledge to tailor an integrated delivery system
What an exciting and challenging year 2014 has been! As it draws to a close, we also celebrate the first year of the merger between The Journal of Supportive Oncology and Community Oncology to form our current title, The Journal of Community and Supportive Oncology. We hope that by combining the clinical and supportive/palliative components of our specialty, we are able to serve as a vital forum and resource by providing you with a “one-stop shop” to support you in your practice of oncology.
Click on the PDF icon at the top of this introduction to read the full article.
What an exciting and challenging year 2014 has been! As it draws to a close, we also celebrate the first year of the merger between The Journal of Supportive Oncology and Community Oncology to form our current title, The Journal of Community and Supportive Oncology. We hope that by combining the clinical and supportive/palliative components of our specialty, we are able to serve as a vital forum and resource by providing you with a “one-stop shop” to support you in your practice of oncology.
Click on the PDF icon at the top of this introduction to read the full article.
What an exciting and challenging year 2014 has been! As it draws to a close, we also celebrate the first year of the merger between The Journal of Supportive Oncology and Community Oncology to form our current title, The Journal of Community and Supportive Oncology. We hope that by combining the clinical and supportive/palliative components of our specialty, we are able to serve as a vital forum and resource by providing you with a “one-stop shop” to support you in your practice of oncology.
Click on the PDF icon at the top of this introduction to read the full article.
Nitrous oxide for labor pain
Neuraxial anesthesia, including epidural and combined spinal-epidural anesthetics, are the “gold standard” interventions for pain relief during labor because they provide a superb combination of reliable pain relief and safety for the mother and child.1 Many US birthing centers also offer additional options for managing labor pain, including continuous labor support,2 hydrotherapy,3 and parenteral opioids.4 In 2012, the US Food and Drug Administration (FDA) approved equipment to deliver a mixture of 50% nitrous oxide and 50% oxygen, which has offered a new option for laboring mothers.
Nitrous oxide is widely used for labor pain in the United Kingdom, Finland, Sweden, Canada, Australia, and New Zealand.5 In the United States, nitrous oxide has been a long-standing and common adjunct to general anesthetics, although it recently has fallen out of favor in place of better, more rapidly acting inhalation and intravenous general anesthetics. With these agents not suitable for labor analgesic use, however, nitrous oxide is undergoing a resurgence in popularity for obstetric analgesia in the United States, and we believe that it will evolve to have a prominent place among our interventions for labor pain.6 In this editorial, we detail the mechanism of action and the equipment’s use, as well as benefits for patients and cautions for clinicians.
How does nitrous oxide work?
Pharmacology. Nitrous oxide (N2O) was first synthesized by Joseph Priestley in 1772 and was used as an anesthetic for dental surgery in the mid-1800s. In the late 19th Century, nitrous oxide was tested as an agent for labor analgesia.7 It was introduced into clinical practice in the United Kingdom in the 1930s.8
The mechanism of action of nitrous oxide is not fully characterized. It is thought that the gas may produce analgesia by activating the endogenous opioid and noradrenergic systems, which in turn, modulate spinal cord transmission of pain signals.5

Administration to the laboring mother. For labor analgesia, nitrous oxide is typically administered as a mix of 50% N2O and 50% O2 using a portable unit with a gas mixer that is fed by small tanks of N2O and O2 or with a valve fed by a single tank containing a mixture of both N2O and O2. The portable units approved by the FDA contain an oxygen fail-safe system that ensures delivery of an appropriate oxygen concentration. The portable unit also contains a gas scavenging system that is attached to wall suction. The breathing circuit has a mask or a mouthpiece (according to patient preference) and demand valve. The patient places the mask over her nose and mouth, or uses just her mouth for the mouthpiece. With inhalation, the demand valve opens, releasing the gas mixture. On exhalation, the valve shunts the exhaled gases to the scavenging system.
Proper and safe use requires adherence to the principles of a true “patient-controlled” protocol. Only the patient is permitted to place the mask or mouthpiece over her nose and/or mouth. If the patient becomes drowsy, such that she cannot hold the mask to her face, then the internal demand valve will not deliver nitrous oxide and she will return to breathing room air. No one should hold the mask over the patient’s nose or mouth, and the mask should not be fixed in place with elastic bands because these actions may result in the inhalation of too much nitrous oxide.
Nitrous oxide has a rapid onset of action after inhalation and its action quickly dissipates after discontinuing inhalation. There is likely a dose-response relationship, with greater use of the nitrous oxide producing more drowsiness. With the intermittent inhalation method, the laboring patient using nitrous oxide is advised to initiate inhalation of nitrous oxide about 30 seconds before the onset of a contraction and discontinue inhalation at the peak of the contraction.
There is no time limit to the use of nitrous oxide. It can be used for hours during labor or only briefly for a particularly painful part of labor, such as during rapid cervical dilation or during the later portions of the second stage.
Patients report that nitrous oxide does not completely relieve pain but creates a diminished perception of the pain.9 As many as one-third of women are nonresponders and report no significant pain improvement with nitrous oxide use.10
The main side effects of inhalation of the gas are nausea, vomiting, dizziness, and drowsiness. Nausea has been reported in 5% to 40% of women, and vomiting has been reported in up to 15% of women using nitrous oxide.11
Cautions
Contraindications to nitrous oxide include a baseline arterial oxygenation saturation less than 95% on room air, acute asthma, emphysema, or pneumothorax, or any other air-filled compartment within the body, such as bowel obstruction or pneumocephalus. (Nitrous oxide can displace nitrogen from closed body spaces, which may lead to an increase in the volume of the closed space.12)
Nitrous oxide inactivates vitamin B12 by oxidation; therefore, vitamin B12 deficiency or related disorders may be considered a relative contraindication. However, compared with more extensive continuous use, such as during prolonged general anesthesia, intermittent use for a limited time during labor is associated with minimal to no hematologic effects.
If a laboring woman is using N2O, parenteral opioids should be administered only with great caution by an experienced clinician.
What do the data indicate?
The Agency for Healthcare Research and Quality (AHRQ) recently invited the Vanderbilt Evidence-based Practice Center to review the world literature on nitrous oxide for labor pain and to provide a summary of the research. Fifty-eight publications were identified, with 46 rated as poor quality.11,13 Given this overall poor quality of available research, many of the recommendations concerning the use of nitrous oxide for labor pain are based on clinical experience and expert opinion.
The experts concluded that, for the relief of labor pain, neuraxial anesthesia was more effective than nitrous oxide inhalation. In one randomized trial included in their systematic review, nulliparous laboring women were randomly assigned to neuraxial anesthesia or nitrous oxide plus meperidine.14 About 94% of nulliparous laboring women reported satisfaction with neuraxial anesthesia, compared with 54% treated with nitrous oxide and meperidine.14
Nitrous oxide is believed to be generally safe for mother and fetus. Its use does not impact the newborn Apgar score15 or alter uterine
contractility.16
Considering a nitrous oxide program for your birthing unit? Helpful hints to get started.
Catherine McGovern, RN, MSN, CNM
- Do your research to determine which type of equipment is right for the size and volume of your organization.
You need to consider ease of access and use for staff to bring this option to the bedside in a prompt and safe manner. Initial research includes visiting or speaking with practitioners on units currently using nitrous oxide. Use of nitrous oxide is growing, and networking is helpful in terms of planning your program. Making sure you have the correct gas line connectors for oxygen as well as for suction when using a scavenger system is a preliminary necessity. - Determine storage ability.
Your environmental safety officer is a good resource to determine location and regulations regarding safe storage as well as tank capacity. He or she also can help you determine where else in your organization nitrous oxide is used so you may be able to develop your unit-specific protocol from hospital-wide policy that is already in place. - Collaborate on a protocol.
After determining which type of equipment is best for you, propose the idea to committees that can contribute to the development of pain and sedation management protocols. The anesthesia department, pain committee, and postoperative pain management teams are knowledgeable resources and can help you write a safe protocol. Keep as the main focus the safe application and use of nitrous oxide for various patient populations. Potential medication interactions and contraindications for use should be discussed and included in a protocol.
One more department you want to include in your planning is infection control. For our unit, reviewing various types of equipment to determine the best infection control revealed some interesting design benefits to reduce infection risk. Because the nitrous oxide equipment would be mobile, the types of filter options, disposal options, and cleaning ability are important components for final equipment choice. - Include all parties in training and final roll out.
Once you develop your policy with input from all stakeholders, make sure you share it early and often before you go live. Include midwives, physicians, nurses, technicians, and administrative staff in training, which will help to dispel myths and increase awareness of availability within your unit. Provide background information to all trainees to ensure safe use and appropriate patient selection.
The most important determinant of success is the formation of an interprofessional team that works well together to develop a safe clinician- and patient-friendly program for the use of nitrous oxide.
Nitrous oxide, a bridge to an epidural or a natural childbirth
Many women start labor unsure about whether they want to use an epidural. For these women, nitrous oxide may be an option for reducing labor pain, thereby giving the woman more time to make a decision about whether to have an epidural anesthetic. In our practice, a significant percentage of women who use nitrous oxide early in labor subsequently request a neuraxial anesthetic. However, many women planning natural childbirth use nitrous oxide to reduce labor pain and successfully achieve their goal.
Postpartum pain reliever
Some women deliver without the use of any pain medicine. Sometimes birth is complicated by perineal lacerations requiring significant surgical repair. If a woman does not have adequate analgesia after injection of a local anesthetic, nitrous oxide may help reduce her pain during the perineal repair and facilitate quick completion of the procedure by allowing her to remain still. N2O also has been used to facilitate analgesia during manual removal of the placenta.
We predict an expanding role
There are many pharmacologic and nonpharmacologic options for managing labor pain, including a supportive birth environment, touch and massage, maternal positioning, relaxation and breathing techniques, continuous labor support, hydrotherapy, opioids, and neuraxial anesthesia. Midwives, labor nurses, and physicians have championed increasing the availability of nitrous oxide to laboring women in US birthing centers.17–20 With the FDA approval of inexpensive portable nitrous oxide units, it is likely that we will witness a resurgence of its use and gain important clinical experience in the role of nitrous oxide for managing labor pain.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Amin-Somuah M, Smyth R, Jones L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2011;(12):CD000331.
2. Hodnett ED, Gates S, Hofmeyr JG, Sakala C. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2013;(7):CD003766.
3. Cluett ER, Burns E. Immersion in water in labour and birth. Cochrane Database Syst Rev. 2009;(2):CD000111.
4. Ullman R, Smith LA, Burns E, Mori R, Dowswell T. Parenteral opioids for maternal pain management in labor. Cochrane Database Syst Rev. 2010;(9):CD007396.
5. Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl Nature):S110–S126.
6. Klomp T, van Poppel M, Jones L, Lazet J, Di Nisio M, Lagro-Janssen A. Inhaled analgesia for pain management in labor. Cochrane Database Syst Rev. 2012;(9):CD009351.
7. Richards W, Parbrook G, Wilson J. Stanislav Klikovitch (1853-1910). Pioneer of nitrous oxide and oxygen analgesia. Anaesthesia. 1976;31(7):933–940.
8. Minnitt R. Self-administered anesthesia in childbirth. Br Med J. 1934;1:501–503.
9. Camann W, Alexander K. Easy labor: Every Woman’s Guide to Choosing Less Pain and More Joy during Childbirth. New York: Ballantine Books; 2007.
10. Rosen M, Mushin WW, Jones PL, Jones EV. Field trial of methoxyflurane, nitrous oxide, and trichloroethylene as obstetric analgesics. Br Med J. 1969;3(5665):263–267.
11. Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153–167.
12. Eger EI 2nd, Saidman LJ. Hazards of nitrous oxide anesthesia in bowel obstruction and pneumothorax. Anesthesiology. 1965;26:61–66.
13. Agency for Healthcare Research and Quality. Nitrous oxide for the management of labor pain. Comparative Effectiveness Review Number 67. August 2012. http://www.effectivehealthcare.ahrq.gov/ehc/products/260/1175/CER67_NitrousOxideLaborPain_FinalReport_20120817.pdf. Accessed November 7, 2014.
14. Leong EW, Sivanesaratnam V, Oh LL, Chan YK. Epidural analgesia in primigravidae in spontaneous labor at term: a prospective study. J Obstet Gynaecol Res. 2000;26(4):271–275.
15. Clinical trials of different concentrations of oxygen and nitrous oxide for obstetric analgesia. Report to the Medical Research Council of the Committee on Nitrous Oxide and Oxygen Analgesia in Midwifery. Br Med J. 1970;1(5698):709–713.
16. Vasicka A, Kretchmer H. Effect of conduction and inhalation anesthesia on uterine contractions. Am J Obstet Gynecol. 1961;82:600–611.
17. Rooks JP. Labor pain management other than neuraxial: what do we know and where do we go next? Birth. 2012;39(4):318–322.
18. American College of Nurse-Midwives. From the American College of Nurse-Midwives. Nitrous oxide for labor analgesia. J Midwifery Womens Health. 2010;55(3):292–296.
19. Bishop JT. Administration of nitrous oxide in labor: expanding the options for women. J Midwifery Womens Health. 2007;52(3):308–309.
20. Rooks JP. Nitrous oxide for pain in labor—why not in the United States? Birth. 2007;34(1):3–5.
Robert L. Barbieri, MD; William Camann, MD; and Catherine McGovern, RN, MSN, CNM

Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.

Dr. Camann is Associate Professor, Anesthesia and Pain Management, Harvard Medical School; Director, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.

Ms. McGovern is Clinical Educator, Center for Labor and Birth, at Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Robert L. Barbieri, MD; William Camann, MD; and Catherine McGovern, RN, MSN, CNM
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Camann is Associate Professor, Anesthesia and Pain Management, Harvard Medical School; Director, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.
Ms. McGovern is Clinical Educator, Center for Labor and Birth, at Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Robert L. Barbieri, MD; William Camann, MD; and Catherine McGovern, RN, MSN, CNM
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Camann is Associate Professor, Anesthesia and Pain Management, Harvard Medical School; Director, Obstetric Anesthesiology, Brigham and Women’s Hospital, Boston, Massachusetts.
Ms. McGovern is Clinical Educator, Center for Labor and Birth, at Brigham and Women’s Hospital, Boston, Massachusetts.
The authors report no financial relationships relevant to this article.
Neuraxial anesthesia, including epidural and combined spinal-epidural anesthetics, are the “gold standard” interventions for pain relief during labor because they provide a superb combination of reliable pain relief and safety for the mother and child.1 Many US birthing centers also offer additional options for managing labor pain, including continuous labor support,2 hydrotherapy,3 and parenteral opioids.4 In 2012, the US Food and Drug Administration (FDA) approved equipment to deliver a mixture of 50% nitrous oxide and 50% oxygen, which has offered a new option for laboring mothers.
Nitrous oxide is widely used for labor pain in the United Kingdom, Finland, Sweden, Canada, Australia, and New Zealand.5 In the United States, nitrous oxide has been a long-standing and common adjunct to general anesthetics, although it recently has fallen out of favor in place of better, more rapidly acting inhalation and intravenous general anesthetics. With these agents not suitable for labor analgesic use, however, nitrous oxide is undergoing a resurgence in popularity for obstetric analgesia in the United States, and we believe that it will evolve to have a prominent place among our interventions for labor pain.6 In this editorial, we detail the mechanism of action and the equipment’s use, as well as benefits for patients and cautions for clinicians.
How does nitrous oxide work?
Pharmacology. Nitrous oxide (N2O) was first synthesized by Joseph Priestley in 1772 and was used as an anesthetic for dental surgery in the mid-1800s. In the late 19th Century, nitrous oxide was tested as an agent for labor analgesia.7 It was introduced into clinical practice in the United Kingdom in the 1930s.8
The mechanism of action of nitrous oxide is not fully characterized. It is thought that the gas may produce analgesia by activating the endogenous opioid and noradrenergic systems, which in turn, modulate spinal cord transmission of pain signals.5
Administration to the laboring mother. For labor analgesia, nitrous oxide is typically administered as a mix of 50% N2O and 50% O2 using a portable unit with a gas mixer that is fed by small tanks of N2O and O2 or with a valve fed by a single tank containing a mixture of both N2O and O2. The portable units approved by the FDA contain an oxygen fail-safe system that ensures delivery of an appropriate oxygen concentration. The portable unit also contains a gas scavenging system that is attached to wall suction. The breathing circuit has a mask or a mouthpiece (according to patient preference) and demand valve. The patient places the mask over her nose and mouth, or uses just her mouth for the mouthpiece. With inhalation, the demand valve opens, releasing the gas mixture. On exhalation, the valve shunts the exhaled gases to the scavenging system.
Proper and safe use requires adherence to the principles of a true “patient-controlled” protocol. Only the patient is permitted to place the mask or mouthpiece over her nose and/or mouth. If the patient becomes drowsy, such that she cannot hold the mask to her face, then the internal demand valve will not deliver nitrous oxide and she will return to breathing room air. No one should hold the mask over the patient’s nose or mouth, and the mask should not be fixed in place with elastic bands because these actions may result in the inhalation of too much nitrous oxide.
Nitrous oxide has a rapid onset of action after inhalation and its action quickly dissipates after discontinuing inhalation. There is likely a dose-response relationship, with greater use of the nitrous oxide producing more drowsiness. With the intermittent inhalation method, the laboring patient using nitrous oxide is advised to initiate inhalation of nitrous oxide about 30 seconds before the onset of a contraction and discontinue inhalation at the peak of the contraction.
There is no time limit to the use of nitrous oxide. It can be used for hours during labor or only briefly for a particularly painful part of labor, such as during rapid cervical dilation or during the later portions of the second stage.
Patients report that nitrous oxide does not completely relieve pain but creates a diminished perception of the pain.9 As many as one-third of women are nonresponders and report no significant pain improvement with nitrous oxide use.10
The main side effects of inhalation of the gas are nausea, vomiting, dizziness, and drowsiness. Nausea has been reported in 5% to 40% of women, and vomiting has been reported in up to 15% of women using nitrous oxide.11
Cautions
Contraindications to nitrous oxide include a baseline arterial oxygenation saturation less than 95% on room air, acute asthma, emphysema, or pneumothorax, or any other air-filled compartment within the body, such as bowel obstruction or pneumocephalus. (Nitrous oxide can displace nitrogen from closed body spaces, which may lead to an increase in the volume of the closed space.12)
Nitrous oxide inactivates vitamin B12 by oxidation; therefore, vitamin B12 deficiency or related disorders may be considered a relative contraindication. However, compared with more extensive continuous use, such as during prolonged general anesthesia, intermittent use for a limited time during labor is associated with minimal to no hematologic effects.
If a laboring woman is using N2O, parenteral opioids should be administered only with great caution by an experienced clinician.
What do the data indicate?
The Agency for Healthcare Research and Quality (AHRQ) recently invited the Vanderbilt Evidence-based Practice Center to review the world literature on nitrous oxide for labor pain and to provide a summary of the research. Fifty-eight publications were identified, with 46 rated as poor quality.11,13 Given this overall poor quality of available research, many of the recommendations concerning the use of nitrous oxide for labor pain are based on clinical experience and expert opinion.
The experts concluded that, for the relief of labor pain, neuraxial anesthesia was more effective than nitrous oxide inhalation. In one randomized trial included in their systematic review, nulliparous laboring women were randomly assigned to neuraxial anesthesia or nitrous oxide plus meperidine.14 About 94% of nulliparous laboring women reported satisfaction with neuraxial anesthesia, compared with 54% treated with nitrous oxide and meperidine.14
Nitrous oxide is believed to be generally safe for mother and fetus. Its use does not impact the newborn Apgar score15 or alter uterine
contractility.16
Considering a nitrous oxide program for your birthing unit? Helpful hints to get started.
Catherine McGovern, RN, MSN, CNM
- Do your research to determine which type of equipment is right for the size and volume of your organization.
You need to consider ease of access and use for staff to bring this option to the bedside in a prompt and safe manner. Initial research includes visiting or speaking with practitioners on units currently using nitrous oxide. Use of nitrous oxide is growing, and networking is helpful in terms of planning your program. Making sure you have the correct gas line connectors for oxygen as well as for suction when using a scavenger system is a preliminary necessity. - Determine storage ability.
Your environmental safety officer is a good resource to determine location and regulations regarding safe storage as well as tank capacity. He or she also can help you determine where else in your organization nitrous oxide is used so you may be able to develop your unit-specific protocol from hospital-wide policy that is already in place. - Collaborate on a protocol.
After determining which type of equipment is best for you, propose the idea to committees that can contribute to the development of pain and sedation management protocols. The anesthesia department, pain committee, and postoperative pain management teams are knowledgeable resources and can help you write a safe protocol. Keep as the main focus the safe application and use of nitrous oxide for various patient populations. Potential medication interactions and contraindications for use should be discussed and included in a protocol.
One more department you want to include in your planning is infection control. For our unit, reviewing various types of equipment to determine the best infection control revealed some interesting design benefits to reduce infection risk. Because the nitrous oxide equipment would be mobile, the types of filter options, disposal options, and cleaning ability are important components for final equipment choice. - Include all parties in training and final roll out.
Once you develop your policy with input from all stakeholders, make sure you share it early and often before you go live. Include midwives, physicians, nurses, technicians, and administrative staff in training, which will help to dispel myths and increase awareness of availability within your unit. Provide background information to all trainees to ensure safe use and appropriate patient selection.
The most important determinant of success is the formation of an interprofessional team that works well together to develop a safe clinician- and patient-friendly program for the use of nitrous oxide.
Nitrous oxide, a bridge to an epidural or a natural childbirth
Many women start labor unsure about whether they want to use an epidural. For these women, nitrous oxide may be an option for reducing labor pain, thereby giving the woman more time to make a decision about whether to have an epidural anesthetic. In our practice, a significant percentage of women who use nitrous oxide early in labor subsequently request a neuraxial anesthetic. However, many women planning natural childbirth use nitrous oxide to reduce labor pain and successfully achieve their goal.
Postpartum pain reliever
Some women deliver without the use of any pain medicine. Sometimes birth is complicated by perineal lacerations requiring significant surgical repair. If a woman does not have adequate analgesia after injection of a local anesthetic, nitrous oxide may help reduce her pain during the perineal repair and facilitate quick completion of the procedure by allowing her to remain still. N2O also has been used to facilitate analgesia during manual removal of the placenta.
We predict an expanding role
There are many pharmacologic and nonpharmacologic options for managing labor pain, including a supportive birth environment, touch and massage, maternal positioning, relaxation and breathing techniques, continuous labor support, hydrotherapy, opioids, and neuraxial anesthesia. Midwives, labor nurses, and physicians have championed increasing the availability of nitrous oxide to laboring women in US birthing centers.17–20 With the FDA approval of inexpensive portable nitrous oxide units, it is likely that we will witness a resurgence of its use and gain important clinical experience in the role of nitrous oxide for managing labor pain.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Neuraxial anesthesia, including epidural and combined spinal-epidural anesthetics, are the “gold standard” interventions for pain relief during labor because they provide a superb combination of reliable pain relief and safety for the mother and child.1 Many US birthing centers also offer additional options for managing labor pain, including continuous labor support,2 hydrotherapy,3 and parenteral opioids.4 In 2012, the US Food and Drug Administration (FDA) approved equipment to deliver a mixture of 50% nitrous oxide and 50% oxygen, which has offered a new option for laboring mothers.
Nitrous oxide is widely used for labor pain in the United Kingdom, Finland, Sweden, Canada, Australia, and New Zealand.5 In the United States, nitrous oxide has been a long-standing and common adjunct to general anesthetics, although it recently has fallen out of favor in place of better, more rapidly acting inhalation and intravenous general anesthetics. With these agents not suitable for labor analgesic use, however, nitrous oxide is undergoing a resurgence in popularity for obstetric analgesia in the United States, and we believe that it will evolve to have a prominent place among our interventions for labor pain.6 In this editorial, we detail the mechanism of action and the equipment’s use, as well as benefits for patients and cautions for clinicians.
How does nitrous oxide work?
Pharmacology. Nitrous oxide (N2O) was first synthesized by Joseph Priestley in 1772 and was used as an anesthetic for dental surgery in the mid-1800s. In the late 19th Century, nitrous oxide was tested as an agent for labor analgesia.7 It was introduced into clinical practice in the United Kingdom in the 1930s.8
The mechanism of action of nitrous oxide is not fully characterized. It is thought that the gas may produce analgesia by activating the endogenous opioid and noradrenergic systems, which in turn, modulate spinal cord transmission of pain signals.5
Administration to the laboring mother. For labor analgesia, nitrous oxide is typically administered as a mix of 50% N2O and 50% O2 using a portable unit with a gas mixer that is fed by small tanks of N2O and O2 or with a valve fed by a single tank containing a mixture of both N2O and O2. The portable units approved by the FDA contain an oxygen fail-safe system that ensures delivery of an appropriate oxygen concentration. The portable unit also contains a gas scavenging system that is attached to wall suction. The breathing circuit has a mask or a mouthpiece (according to patient preference) and demand valve. The patient places the mask over her nose and mouth, or uses just her mouth for the mouthpiece. With inhalation, the demand valve opens, releasing the gas mixture. On exhalation, the valve shunts the exhaled gases to the scavenging system.
Proper and safe use requires adherence to the principles of a true “patient-controlled” protocol. Only the patient is permitted to place the mask or mouthpiece over her nose and/or mouth. If the patient becomes drowsy, such that she cannot hold the mask to her face, then the internal demand valve will not deliver nitrous oxide and she will return to breathing room air. No one should hold the mask over the patient’s nose or mouth, and the mask should not be fixed in place with elastic bands because these actions may result in the inhalation of too much nitrous oxide.
Nitrous oxide has a rapid onset of action after inhalation and its action quickly dissipates after discontinuing inhalation. There is likely a dose-response relationship, with greater use of the nitrous oxide producing more drowsiness. With the intermittent inhalation method, the laboring patient using nitrous oxide is advised to initiate inhalation of nitrous oxide about 30 seconds before the onset of a contraction and discontinue inhalation at the peak of the contraction.
There is no time limit to the use of nitrous oxide. It can be used for hours during labor or only briefly for a particularly painful part of labor, such as during rapid cervical dilation or during the later portions of the second stage.
Patients report that nitrous oxide does not completely relieve pain but creates a diminished perception of the pain.9 As many as one-third of women are nonresponders and report no significant pain improvement with nitrous oxide use.10
The main side effects of inhalation of the gas are nausea, vomiting, dizziness, and drowsiness. Nausea has been reported in 5% to 40% of women, and vomiting has been reported in up to 15% of women using nitrous oxide.11
Cautions
Contraindications to nitrous oxide include a baseline arterial oxygenation saturation less than 95% on room air, acute asthma, emphysema, or pneumothorax, or any other air-filled compartment within the body, such as bowel obstruction or pneumocephalus. (Nitrous oxide can displace nitrogen from closed body spaces, which may lead to an increase in the volume of the closed space.12)
Nitrous oxide inactivates vitamin B12 by oxidation; therefore, vitamin B12 deficiency or related disorders may be considered a relative contraindication. However, compared with more extensive continuous use, such as during prolonged general anesthesia, intermittent use for a limited time during labor is associated with minimal to no hematologic effects.
If a laboring woman is using N2O, parenteral opioids should be administered only with great caution by an experienced clinician.
What do the data indicate?
The Agency for Healthcare Research and Quality (AHRQ) recently invited the Vanderbilt Evidence-based Practice Center to review the world literature on nitrous oxide for labor pain and to provide a summary of the research. Fifty-eight publications were identified, with 46 rated as poor quality.11,13 Given this overall poor quality of available research, many of the recommendations concerning the use of nitrous oxide for labor pain are based on clinical experience and expert opinion.
The experts concluded that, for the relief of labor pain, neuraxial anesthesia was more effective than nitrous oxide inhalation. In one randomized trial included in their systematic review, nulliparous laboring women were randomly assigned to neuraxial anesthesia or nitrous oxide plus meperidine.14 About 94% of nulliparous laboring women reported satisfaction with neuraxial anesthesia, compared with 54% treated with nitrous oxide and meperidine.14
Nitrous oxide is believed to be generally safe for mother and fetus. Its use does not impact the newborn Apgar score15 or alter uterine
contractility.16
Considering a nitrous oxide program for your birthing unit? Helpful hints to get started.
Catherine McGovern, RN, MSN, CNM
- Do your research to determine which type of equipment is right for the size and volume of your organization.
You need to consider ease of access and use for staff to bring this option to the bedside in a prompt and safe manner. Initial research includes visiting or speaking with practitioners on units currently using nitrous oxide. Use of nitrous oxide is growing, and networking is helpful in terms of planning your program. Making sure you have the correct gas line connectors for oxygen as well as for suction when using a scavenger system is a preliminary necessity. - Determine storage ability.
Your environmental safety officer is a good resource to determine location and regulations regarding safe storage as well as tank capacity. He or she also can help you determine where else in your organization nitrous oxide is used so you may be able to develop your unit-specific protocol from hospital-wide policy that is already in place. - Collaborate on a protocol.
After determining which type of equipment is best for you, propose the idea to committees that can contribute to the development of pain and sedation management protocols. The anesthesia department, pain committee, and postoperative pain management teams are knowledgeable resources and can help you write a safe protocol. Keep as the main focus the safe application and use of nitrous oxide for various patient populations. Potential medication interactions and contraindications for use should be discussed and included in a protocol.
One more department you want to include in your planning is infection control. For our unit, reviewing various types of equipment to determine the best infection control revealed some interesting design benefits to reduce infection risk. Because the nitrous oxide equipment would be mobile, the types of filter options, disposal options, and cleaning ability are important components for final equipment choice. - Include all parties in training and final roll out.
Once you develop your policy with input from all stakeholders, make sure you share it early and often before you go live. Include midwives, physicians, nurses, technicians, and administrative staff in training, which will help to dispel myths and increase awareness of availability within your unit. Provide background information to all trainees to ensure safe use and appropriate patient selection.
The most important determinant of success is the formation of an interprofessional team that works well together to develop a safe clinician- and patient-friendly program for the use of nitrous oxide.
Nitrous oxide, a bridge to an epidural or a natural childbirth
Many women start labor unsure about whether they want to use an epidural. For these women, nitrous oxide may be an option for reducing labor pain, thereby giving the woman more time to make a decision about whether to have an epidural anesthetic. In our practice, a significant percentage of women who use nitrous oxide early in labor subsequently request a neuraxial anesthetic. However, many women planning natural childbirth use nitrous oxide to reduce labor pain and successfully achieve their goal.
Postpartum pain reliever
Some women deliver without the use of any pain medicine. Sometimes birth is complicated by perineal lacerations requiring significant surgical repair. If a woman does not have adequate analgesia after injection of a local anesthetic, nitrous oxide may help reduce her pain during the perineal repair and facilitate quick completion of the procedure by allowing her to remain still. N2O also has been used to facilitate analgesia during manual removal of the placenta.
We predict an expanding role
There are many pharmacologic and nonpharmacologic options for managing labor pain, including a supportive birth environment, touch and massage, maternal positioning, relaxation and breathing techniques, continuous labor support, hydrotherapy, opioids, and neuraxial anesthesia. Midwives, labor nurses, and physicians have championed increasing the availability of nitrous oxide to laboring women in US birthing centers.17–20 With the FDA approval of inexpensive portable nitrous oxide units, it is likely that we will witness a resurgence of its use and gain important clinical experience in the role of nitrous oxide for managing labor pain.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Amin-Somuah M, Smyth R, Jones L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2011;(12):CD000331.
2. Hodnett ED, Gates S, Hofmeyr JG, Sakala C. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2013;(7):CD003766.
3. Cluett ER, Burns E. Immersion in water in labour and birth. Cochrane Database Syst Rev. 2009;(2):CD000111.
4. Ullman R, Smith LA, Burns E, Mori R, Dowswell T. Parenteral opioids for maternal pain management in labor. Cochrane Database Syst Rev. 2010;(9):CD007396.
5. Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl Nature):S110–S126.
6. Klomp T, van Poppel M, Jones L, Lazet J, Di Nisio M, Lagro-Janssen A. Inhaled analgesia for pain management in labor. Cochrane Database Syst Rev. 2012;(9):CD009351.
7. Richards W, Parbrook G, Wilson J. Stanislav Klikovitch (1853-1910). Pioneer of nitrous oxide and oxygen analgesia. Anaesthesia. 1976;31(7):933–940.
8. Minnitt R. Self-administered anesthesia in childbirth. Br Med J. 1934;1:501–503.
9. Camann W, Alexander K. Easy labor: Every Woman’s Guide to Choosing Less Pain and More Joy during Childbirth. New York: Ballantine Books; 2007.
10. Rosen M, Mushin WW, Jones PL, Jones EV. Field trial of methoxyflurane, nitrous oxide, and trichloroethylene as obstetric analgesics. Br Med J. 1969;3(5665):263–267.
11. Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153–167.
12. Eger EI 2nd, Saidman LJ. Hazards of nitrous oxide anesthesia in bowel obstruction and pneumothorax. Anesthesiology. 1965;26:61–66.
13. Agency for Healthcare Research and Quality. Nitrous oxide for the management of labor pain. Comparative Effectiveness Review Number 67. August 2012. http://www.effectivehealthcare.ahrq.gov/ehc/products/260/1175/CER67_NitrousOxideLaborPain_FinalReport_20120817.pdf. Accessed November 7, 2014.
14. Leong EW, Sivanesaratnam V, Oh LL, Chan YK. Epidural analgesia in primigravidae in spontaneous labor at term: a prospective study. J Obstet Gynaecol Res. 2000;26(4):271–275.
15. Clinical trials of different concentrations of oxygen and nitrous oxide for obstetric analgesia. Report to the Medical Research Council of the Committee on Nitrous Oxide and Oxygen Analgesia in Midwifery. Br Med J. 1970;1(5698):709–713.
16. Vasicka A, Kretchmer H. Effect of conduction and inhalation anesthesia on uterine contractions. Am J Obstet Gynecol. 1961;82:600–611.
17. Rooks JP. Labor pain management other than neuraxial: what do we know and where do we go next? Birth. 2012;39(4):318–322.
18. American College of Nurse-Midwives. From the American College of Nurse-Midwives. Nitrous oxide for labor analgesia. J Midwifery Womens Health. 2010;55(3):292–296.
19. Bishop JT. Administration of nitrous oxide in labor: expanding the options for women. J Midwifery Womens Health. 2007;52(3):308–309.
20. Rooks JP. Nitrous oxide for pain in labor—why not in the United States? Birth. 2007;34(1):3–5.
1. Amin-Somuah M, Smyth R, Jones L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2011;(12):CD000331.
2. Hodnett ED, Gates S, Hofmeyr JG, Sakala C. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2013;(7):CD003766.
3. Cluett ER, Burns E. Immersion in water in labour and birth. Cochrane Database Syst Rev. 2009;(2):CD000111.
4. Ullman R, Smith LA, Burns E, Mori R, Dowswell T. Parenteral opioids for maternal pain management in labor. Cochrane Database Syst Rev. 2010;(9):CD007396.
5. Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5 suppl Nature):S110–S126.
6. Klomp T, van Poppel M, Jones L, Lazet J, Di Nisio M, Lagro-Janssen A. Inhaled analgesia for pain management in labor. Cochrane Database Syst Rev. 2012;(9):CD009351.
7. Richards W, Parbrook G, Wilson J. Stanislav Klikovitch (1853-1910). Pioneer of nitrous oxide and oxygen analgesia. Anaesthesia. 1976;31(7):933–940.
8. Minnitt R. Self-administered anesthesia in childbirth. Br Med J. 1934;1:501–503.
9. Camann W, Alexander K. Easy labor: Every Woman’s Guide to Choosing Less Pain and More Joy during Childbirth. New York: Ballantine Books; 2007.
10. Rosen M, Mushin WW, Jones PL, Jones EV. Field trial of methoxyflurane, nitrous oxide, and trichloroethylene as obstetric analgesics. Br Med J. 1969;3(5665):263–267.
11. Likis FE, Andrews JC, Collins MR, et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153–167.
12. Eger EI 2nd, Saidman LJ. Hazards of nitrous oxide anesthesia in bowel obstruction and pneumothorax. Anesthesiology. 1965;26:61–66.
13. Agency for Healthcare Research and Quality. Nitrous oxide for the management of labor pain. Comparative Effectiveness Review Number 67. August 2012. http://www.effectivehealthcare.ahrq.gov/ehc/products/260/1175/CER67_NitrousOxideLaborPain_FinalReport_20120817.pdf. Accessed November 7, 2014.
14. Leong EW, Sivanesaratnam V, Oh LL, Chan YK. Epidural analgesia in primigravidae in spontaneous labor at term: a prospective study. J Obstet Gynaecol Res. 2000;26(4):271–275.
15. Clinical trials of different concentrations of oxygen and nitrous oxide for obstetric analgesia. Report to the Medical Research Council of the Committee on Nitrous Oxide and Oxygen Analgesia in Midwifery. Br Med J. 1970;1(5698):709–713.
16. Vasicka A, Kretchmer H. Effect of conduction and inhalation anesthesia on uterine contractions. Am J Obstet Gynecol. 1961;82:600–611.
17. Rooks JP. Labor pain management other than neuraxial: what do we know and where do we go next? Birth. 2012;39(4):318–322.
18. American College of Nurse-Midwives. From the American College of Nurse-Midwives. Nitrous oxide for labor analgesia. J Midwifery Womens Health. 2010;55(3):292–296.
19. Bishop JT. Administration of nitrous oxide in labor: expanding the options for women. J Midwifery Womens Health. 2007;52(3):308–309.
20. Rooks JP. Nitrous oxide for pain in labor—why not in the United States? Birth. 2007;34(1):3–5.

Human experimentation: The good, the bad, and the ugly
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.

Ebola—lessons still to be learned

In this issue of the Journal, Dr. Kyle Brizendine reviews the basics of the Ebola virus and its natural history, diagnosis, and management.
Like many of you, I have followed the Ebola story with disquietude. So far, the disease has barely touched our country, with fewer than 10 confirmed cases on US soil, but it has had a big impact on our health care system and our national psyche.
The creation of specialized containment and management units may deplete some hospitals and their communities of intensive care beds. Specially trained caregivers will need to be diverted to staff these units, and the public’s fear may dissuade patients from undergoing elective procedures at hospitals caring for patients with Ebola. All of these pose a financial challenge to the hospitals most capable of dealing with these patients.
We have yet to hear about management guidelines dealing with renal replacement therapy and ventilator support, which may extend life but also pose extra risks to caregivers. Do we understand the disease well enough to know when advanced supportive therapies might be futile? Many lessons were learned from the Liberian patient who died of Ebola in Dallas, but many more clinical questions remain. I had hoped that in our sophisticated ICUs patients treated relatively early with aggressive supportive care would likely survive. We do not yet know if that is true. One death does not make it false, but it does give one pause.
About a half dozen other Ebola patients have survived with treatment here, but they were not African. Does genetic background play a role in disease severity and survival? Were the survivors treated sooner or differently in ways that matter? How much of the end-organ damage from the virus is from direct organ infection that cannot be reversed or prevented by even the best supportive treatment? Does the ability of the virus to suppress the immune system doom patients to opportunistic infections during prolonged supportive therapy? Is the viral-associated immunosuppression enough to prevent some patients from mounting an effective innate (interferon-based) or acquired (viral-specific T-cell or humoral) antiviral response? And is transfusing blood from survivors, presumably conferring passive immunity, actually efficacious?
I was relieved there were no new Ebola cases among the staff caring for Mr. Duncan at his second emergency room visit in Dallas, since at that time he was clearly quite ill, viremic, and contagious. Universal safety precautions must have helped. But how did the other nurses become infected, even though they presumably wore better protection? Hopefully, we will gain further understanding of transmissibility and resistance. We need this knowledge to inform safe and manageable protocols of care, particularly if successful vaccine development is delayed.
In this issue of the Journal, Dr. Kyle Brizendine reviews the basics of the Ebola virus and its natural history, diagnosis, and management.
Like many of you, I have followed the Ebola story with disquietude. So far, the disease has barely touched our country, with fewer than 10 confirmed cases on US soil, but it has had a big impact on our health care system and our national psyche.
The creation of specialized containment and management units may deplete some hospitals and their communities of intensive care beds. Specially trained caregivers will need to be diverted to staff these units, and the public’s fear may dissuade patients from undergoing elective procedures at hospitals caring for patients with Ebola. All of these pose a financial challenge to the hospitals most capable of dealing with these patients.
We have yet to hear about management guidelines dealing with renal replacement therapy and ventilator support, which may extend life but also pose extra risks to caregivers. Do we understand the disease well enough to know when advanced supportive therapies might be futile? Many lessons were learned from the Liberian patient who died of Ebola in Dallas, but many more clinical questions remain. I had hoped that in our sophisticated ICUs patients treated relatively early with aggressive supportive care would likely survive. We do not yet know if that is true. One death does not make it false, but it does give one pause.
About a half dozen other Ebola patients have survived with treatment here, but they were not African. Does genetic background play a role in disease severity and survival? Were the survivors treated sooner or differently in ways that matter? How much of the end-organ damage from the virus is from direct organ infection that cannot be reversed or prevented by even the best supportive treatment? Does the ability of the virus to suppress the immune system doom patients to opportunistic infections during prolonged supportive therapy? Is the viral-associated immunosuppression enough to prevent some patients from mounting an effective innate (interferon-based) or acquired (viral-specific T-cell or humoral) antiviral response? And is transfusing blood from survivors, presumably conferring passive immunity, actually efficacious?
I was relieved there were no new Ebola cases among the staff caring for Mr. Duncan at his second emergency room visit in Dallas, since at that time he was clearly quite ill, viremic, and contagious. Universal safety precautions must have helped. But how did the other nurses become infected, even though they presumably wore better protection? Hopefully, we will gain further understanding of transmissibility and resistance. We need this knowledge to inform safe and manageable protocols of care, particularly if successful vaccine development is delayed.
In this issue of the Journal, Dr. Kyle Brizendine reviews the basics of the Ebola virus and its natural history, diagnosis, and management.
Like many of you, I have followed the Ebola story with disquietude. So far, the disease has barely touched our country, with fewer than 10 confirmed cases on US soil, but it has had a big impact on our health care system and our national psyche.
The creation of specialized containment and management units may deplete some hospitals and their communities of intensive care beds. Specially trained caregivers will need to be diverted to staff these units, and the public’s fear may dissuade patients from undergoing elective procedures at hospitals caring for patients with Ebola. All of these pose a financial challenge to the hospitals most capable of dealing with these patients.
We have yet to hear about management guidelines dealing with renal replacement therapy and ventilator support, which may extend life but also pose extra risks to caregivers. Do we understand the disease well enough to know when advanced supportive therapies might be futile? Many lessons were learned from the Liberian patient who died of Ebola in Dallas, but many more clinical questions remain. I had hoped that in our sophisticated ICUs patients treated relatively early with aggressive supportive care would likely survive. We do not yet know if that is true. One death does not make it false, but it does give one pause.
About a half dozen other Ebola patients have survived with treatment here, but they were not African. Does genetic background play a role in disease severity and survival? Were the survivors treated sooner or differently in ways that matter? How much of the end-organ damage from the virus is from direct organ infection that cannot be reversed or prevented by even the best supportive treatment? Does the ability of the virus to suppress the immune system doom patients to opportunistic infections during prolonged supportive therapy? Is the viral-associated immunosuppression enough to prevent some patients from mounting an effective innate (interferon-based) or acquired (viral-specific T-cell or humoral) antiviral response? And is transfusing blood from survivors, presumably conferring passive immunity, actually efficacious?
I was relieved there were no new Ebola cases among the staff caring for Mr. Duncan at his second emergency room visit in Dallas, since at that time he was clearly quite ill, viremic, and contagious. Universal safety precautions must have helped. But how did the other nurses become infected, even though they presumably wore better protection? Hopefully, we will gain further understanding of transmissibility and resistance. We need this knowledge to inform safe and manageable protocols of care, particularly if successful vaccine development is delayed.
Signs, symptoms, and treatment of psychiatrynemia
Millions of people suffer because they lack access to psychiatric care that they desperately need. The shortage of psychiatrists grows worse every day.
As a result of this anemic supply of psychiatrists, the mental health of the country’s populace is in jeopardy.
The facts paint the picture
The landmark National Institutes of Health-funded Epidemiologic Catchment Area (ECA) study, published a quarter of a century ago, found that 25% of the population suffered from a psychiatric disorder at some point in their life.1 In 1990, that translated to 62 million people; today, the number would be 82 million.
Regrettably, the findings of the ECA were not followed by necessary action—simply, ensuring sufficient psychiatrists to meet the significant mental health needs of the nation.
Signs and symptoms
Manifestations of psychiatrynemia continue unabated:
• frustration by primary care providers when they try to refer a patient to a psychiatrist—with appointments often unavailable for 4 to 6 months
• lack of access to a psychiatrist within 100 miles in many rural areas
• a large number of unfilled positions for psychiatrists in many health care settings nationwide, which has created a thriving locum tenens industry
• emergency rooms packed with psychiatric patients
• a huge patient load in community mental health centers
• a large increase in the percentage of seriously mentally ill people in jails and prisons because of a lack of psychiatrists and psychiatric beds; according to Torrey et al,2 the percentage of mentally ill patients incarcerated in the United States today is the same as it was in 1840, the pre-asylum era—shameful for a civilized country
• an escalation of cash-only practices and concierge psychiatry
• a suicide rate that continues to rise (one wonders how many of the 40,600 deaths by suicide and 650,000 suicide attempts in 20123 could have been prevented by prompt access to psychiatric care)
• a severe shortage of psychiatric subspecialists (child, geriatric, addiction, psychosomatic); their numbers need to rise by 200% to 300% to meet the needs of those populations
• an alarming overreliance on absurdly brief 15-minute med-checks as a way to cope with a large patient load.
What can be done?
To boost the number of psychiatric clinicians and provide better access to care, I offer several prescriptions in the Box.4 (Yes, polytherapy is needed.)
Curing psychiatrynemia requires bold action on multiple fronts by different stakeholders. Considering the failure to act over the past 25 years, however, prospects for a quick remission are low.
We’re past needing an ounce of prevention; we need many pounds.
1. Robins LN, Regier DA. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: The File Press; 1991.
2. Torrey EF, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than in hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/ storage/documents/final_jails_v_hospitals_ study.pdf. Published May 2010. Accessed November 12, 2014.
3. Xu JQ, Kochanek KD, Murphy SL, et al. Mortality in the United States, 2012. NCHS data brief, no 168. Hyattsville, MD: National Center for Health Statistics; 2014.
4. Malowney M, Keltz S, Fischer D, et al. Availability of outpatient care from psychiatrists: a simulated-patient study in three U.S. cities [published online October 15, 2014]. Psychiatr Serv. doi: 10.1176/appi. ps.201400051.
Millions of people suffer because they lack access to psychiatric care that they desperately need. The shortage of psychiatrists grows worse every day.
As a result of this anemic supply of psychiatrists, the mental health of the country’s populace is in jeopardy.
The facts paint the picture
The landmark National Institutes of Health-funded Epidemiologic Catchment Area (ECA) study, published a quarter of a century ago, found that 25% of the population suffered from a psychiatric disorder at some point in their life.1 In 1990, that translated to 62 million people; today, the number would be 82 million.
Regrettably, the findings of the ECA were not followed by necessary action—simply, ensuring sufficient psychiatrists to meet the significant mental health needs of the nation.
Signs and symptoms
Manifestations of psychiatrynemia continue unabated:
• frustration by primary care providers when they try to refer a patient to a psychiatrist—with appointments often unavailable for 4 to 6 months
• lack of access to a psychiatrist within 100 miles in many rural areas
• a large number of unfilled positions for psychiatrists in many health care settings nationwide, which has created a thriving locum tenens industry
• emergency rooms packed with psychiatric patients
• a huge patient load in community mental health centers
• a large increase in the percentage of seriously mentally ill people in jails and prisons because of a lack of psychiatrists and psychiatric beds; according to Torrey et al,2 the percentage of mentally ill patients incarcerated in the United States today is the same as it was in 1840, the pre-asylum era—shameful for a civilized country
• an escalation of cash-only practices and concierge psychiatry
• a suicide rate that continues to rise (one wonders how many of the 40,600 deaths by suicide and 650,000 suicide attempts in 20123 could have been prevented by prompt access to psychiatric care)
• a severe shortage of psychiatric subspecialists (child, geriatric, addiction, psychosomatic); their numbers need to rise by 200% to 300% to meet the needs of those populations
• an alarming overreliance on absurdly brief 15-minute med-checks as a way to cope with a large patient load.
What can be done?
To boost the number of psychiatric clinicians and provide better access to care, I offer several prescriptions in the Box.4 (Yes, polytherapy is needed.)
Curing psychiatrynemia requires bold action on multiple fronts by different stakeholders. Considering the failure to act over the past 25 years, however, prospects for a quick remission are low.
We’re past needing an ounce of prevention; we need many pounds.
Millions of people suffer because they lack access to psychiatric care that they desperately need. The shortage of psychiatrists grows worse every day.
As a result of this anemic supply of psychiatrists, the mental health of the country’s populace is in jeopardy.
The facts paint the picture
The landmark National Institutes of Health-funded Epidemiologic Catchment Area (ECA) study, published a quarter of a century ago, found that 25% of the population suffered from a psychiatric disorder at some point in their life.1 In 1990, that translated to 62 million people; today, the number would be 82 million.
Regrettably, the findings of the ECA were not followed by necessary action—simply, ensuring sufficient psychiatrists to meet the significant mental health needs of the nation.
Signs and symptoms
Manifestations of psychiatrynemia continue unabated:
• frustration by primary care providers when they try to refer a patient to a psychiatrist—with appointments often unavailable for 4 to 6 months
• lack of access to a psychiatrist within 100 miles in many rural areas
• a large number of unfilled positions for psychiatrists in many health care settings nationwide, which has created a thriving locum tenens industry
• emergency rooms packed with psychiatric patients
• a huge patient load in community mental health centers
• a large increase in the percentage of seriously mentally ill people in jails and prisons because of a lack of psychiatrists and psychiatric beds; according to Torrey et al,2 the percentage of mentally ill patients incarcerated in the United States today is the same as it was in 1840, the pre-asylum era—shameful for a civilized country
• an escalation of cash-only practices and concierge psychiatry
• a suicide rate that continues to rise (one wonders how many of the 40,600 deaths by suicide and 650,000 suicide attempts in 20123 could have been prevented by prompt access to psychiatric care)
• a severe shortage of psychiatric subspecialists (child, geriatric, addiction, psychosomatic); their numbers need to rise by 200% to 300% to meet the needs of those populations
• an alarming overreliance on absurdly brief 15-minute med-checks as a way to cope with a large patient load.
What can be done?
To boost the number of psychiatric clinicians and provide better access to care, I offer several prescriptions in the Box.4 (Yes, polytherapy is needed.)
Curing psychiatrynemia requires bold action on multiple fronts by different stakeholders. Considering the failure to act over the past 25 years, however, prospects for a quick remission are low.
We’re past needing an ounce of prevention; we need many pounds.
1. Robins LN, Regier DA. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: The File Press; 1991.
2. Torrey EF, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than in hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/ storage/documents/final_jails_v_hospitals_ study.pdf. Published May 2010. Accessed November 12, 2014.
3. Xu JQ, Kochanek KD, Murphy SL, et al. Mortality in the United States, 2012. NCHS data brief, no 168. Hyattsville, MD: National Center for Health Statistics; 2014.
4. Malowney M, Keltz S, Fischer D, et al. Availability of outpatient care from psychiatrists: a simulated-patient study in three U.S. cities [published online October 15, 2014]. Psychiatr Serv. doi: 10.1176/appi. ps.201400051.
1. Robins LN, Regier DA. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: The File Press; 1991.
2. Torrey EF, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than in hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/ storage/documents/final_jails_v_hospitals_ study.pdf. Published May 2010. Accessed November 12, 2014.
3. Xu JQ, Kochanek KD, Murphy SL, et al. Mortality in the United States, 2012. NCHS data brief, no 168. Hyattsville, MD: National Center for Health Statistics; 2014.
4. Malowney M, Keltz S, Fischer D, et al. Availability of outpatient care from psychiatrists: a simulated-patient study in three U.S. cities [published online October 15, 2014]. Psychiatr Serv. doi: 10.1176/appi. ps.201400051.
Letrozole versus clomiphene for ovulation induction
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
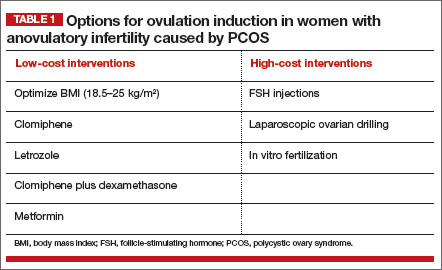
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
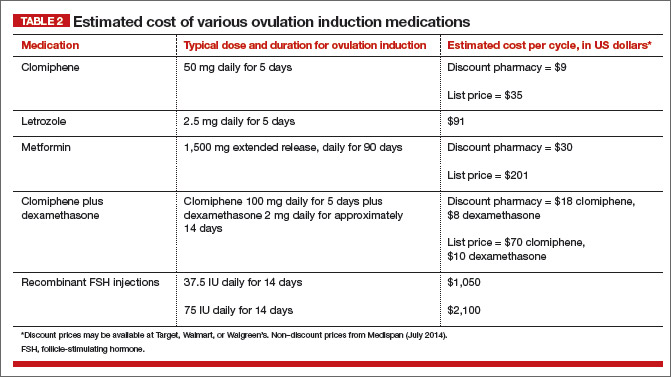
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018
Screening guidelines: A matter of perspective
Medical screening consists of trying to detect an occult disease at a point in its course—earlier than if diagnosed by clinical manifestations—when treatment offers a meaningful benefit to the patient. If the cost is acceptable, one would think that most care providers and patients would embrace the concept. So why are there such heated controversies surrounding screening for breast, prostate, and lung cancer?
The answer to that question is interpretive and philosophical and depends in part on the frame of reference. Are we looking at screening from the perspective of the health care system or from the perspective of the individual patient who is contemplating being screened?
The US Preventive Services Task Force (USPSTF), whose guidelines on screening are reviewed by Dr. Craig Nielsen in this issue of the Journal, went to great lengths to generate evidence-based guidelines based on rigorously conducted trials. They did not consider observational information or the emotional contextual biases of individual patients. Since their guidelines carry great weight, they have a big impact, sometimes including effects on insurance reimbursement for certain screening tests.
As with all “evidence-based” decisions, when applying guidelines or trial data in the clinic, we weigh the effect of our recommendations on individual patients, not on populations. Is a test worthwhile if it offers a 1 in 250 (or fill in your own number) chance of prolonging a specific patient’s life but is expensive and uncomfortable and poses the possible stress of a false-positive result that will warrant more testing? Which is actually more stressful: undergoing additional testing (with expense and discomfort) or not knowing whether you have a potentially lethal tumor? What is a reasonable cost to the patient and to a financially failing health system in attempting to delay the end of life to some time in the future when the patient may well be frail and perhaps even incapacitated?
People may differ in how they answer these questions, some of which may not even be answerable. The USPSTF guidelines, I believe, offer solid scaffolding for informed discussion. But we and our patients should use the offered evidence-based guidelines, and perhaps assume some costs, within a personalized context. Guidelines are only guidelines.
Medical screening consists of trying to detect an occult disease at a point in its course—earlier than if diagnosed by clinical manifestations—when treatment offers a meaningful benefit to the patient. If the cost is acceptable, one would think that most care providers and patients would embrace the concept. So why are there such heated controversies surrounding screening for breast, prostate, and lung cancer?
The answer to that question is interpretive and philosophical and depends in part on the frame of reference. Are we looking at screening from the perspective of the health care system or from the perspective of the individual patient who is contemplating being screened?
The US Preventive Services Task Force (USPSTF), whose guidelines on screening are reviewed by Dr. Craig Nielsen in this issue of the Journal, went to great lengths to generate evidence-based guidelines based on rigorously conducted trials. They did not consider observational information or the emotional contextual biases of individual patients. Since their guidelines carry great weight, they have a big impact, sometimes including effects on insurance reimbursement for certain screening tests.
As with all “evidence-based” decisions, when applying guidelines or trial data in the clinic, we weigh the effect of our recommendations on individual patients, not on populations. Is a test worthwhile if it offers a 1 in 250 (or fill in your own number) chance of prolonging a specific patient’s life but is expensive and uncomfortable and poses the possible stress of a false-positive result that will warrant more testing? Which is actually more stressful: undergoing additional testing (with expense and discomfort) or not knowing whether you have a potentially lethal tumor? What is a reasonable cost to the patient and to a financially failing health system in attempting to delay the end of life to some time in the future when the patient may well be frail and perhaps even incapacitated?
People may differ in how they answer these questions, some of which may not even be answerable. The USPSTF guidelines, I believe, offer solid scaffolding for informed discussion. But we and our patients should use the offered evidence-based guidelines, and perhaps assume some costs, within a personalized context. Guidelines are only guidelines.
Medical screening consists of trying to detect an occult disease at a point in its course—earlier than if diagnosed by clinical manifestations—when treatment offers a meaningful benefit to the patient. If the cost is acceptable, one would think that most care providers and patients would embrace the concept. So why are there such heated controversies surrounding screening for breast, prostate, and lung cancer?
The answer to that question is interpretive and philosophical and depends in part on the frame of reference. Are we looking at screening from the perspective of the health care system or from the perspective of the individual patient who is contemplating being screened?
The US Preventive Services Task Force (USPSTF), whose guidelines on screening are reviewed by Dr. Craig Nielsen in this issue of the Journal, went to great lengths to generate evidence-based guidelines based on rigorously conducted trials. They did not consider observational information or the emotional contextual biases of individual patients. Since their guidelines carry great weight, they have a big impact, sometimes including effects on insurance reimbursement for certain screening tests.
As with all “evidence-based” decisions, when applying guidelines or trial data in the clinic, we weigh the effect of our recommendations on individual patients, not on populations. Is a test worthwhile if it offers a 1 in 250 (or fill in your own number) chance of prolonging a specific patient’s life but is expensive and uncomfortable and poses the possible stress of a false-positive result that will warrant more testing? Which is actually more stressful: undergoing additional testing (with expense and discomfort) or not knowing whether you have a potentially lethal tumor? What is a reasonable cost to the patient and to a financially failing health system in attempting to delay the end of life to some time in the future when the patient may well be frail and perhaps even incapacitated?
People may differ in how they answer these questions, some of which may not even be answerable. The USPSTF guidelines, I believe, offer solid scaffolding for informed discussion. But we and our patients should use the offered evidence-based guidelines, and perhaps assume some costs, within a personalized context. Guidelines are only guidelines.
Turning back the clock: the increase in bilateral mastectomies
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
The sins and peccadillos of psychiatric practice
But as professionals, and by virtue of our rigorous training, we continually reflect on our thoughts and feelings when we care for our patients, and we examine the effect of our behavior and communication patterns on them. Such self-reflection is especially important when it comes to countertransference while treating a person who has been made vulnerable by emotional turmoil and who develops strong transference feelings toward the treating psychiatrist.
Personal integrity is paramount in psychiatric practice; it’s an indispensable ingredient when dealing with the intimate thoughts, feelings, and impulses of people who are seeking psychiatric help. In addition, the wisdom to recognize one’s limitations as a provider of care is an important attributes of seasoned practitioners. Patients might perceive us as demigods, but we know better than to be carried away with hubris and pretend that we are.
Exercising sound judgment isn’t easy
This is especially true when dealing with the varying degrees of ambiguity that shroud complex psychiatric conditions. The overriding principle for good clinical judgment in any medical practice is the patient’s welfare, and that must dominate the moral, ethical, medical, and scientific decision-making of all psychiatrists. Those of us in charge of training medical students and residents emphasize this principle every day at the bedside and in the clinic. Upholding those principles, side by side with the knowledge and skills of psychiatric practice, are the hallmarks of good medical training.
But missteps occur. Peccadillos, infractions, and even transgressions happen—accidentally by competent, ethical psychiatrists; deliberately, sometimes, by a few unethical scoundrels. The sins of psychiatric practice come in a range of gravity and consequences. Here are some I’ve observed among colleagues over the years:
Becoming sexually intimate with one’s patient. Violating the sacred boundary of the doctor-patient relationship is unforgivable; it’s a sin that scars the patient and can destroy the psychiatrist’s reputation and career. We must respect and uphold that boundary—not only during active treatment but even after care is terminated.
Divulging clinical details to other without the patient’s consent. Breach of trust is not only an ethical misstep; it is a violation of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), with substantial penalties attached.
Treating the mind while ignoring the body and brain. We are physicians first, psychiatrists second. We must fully assess patients who present with psychiatric signs and symptoms to rule out a general medical condition that could be generating behavioral symptoms. Such co-occurring medical conditions might involve various organ systems, such as endocrinopathies, or might emanate from brain lesions, whether traumatic, degenerative, demyelinating, infectious, or neoplastic. Without careful medical evaluation, the wrong diagnosis might be made and inappropriate, even harmful, treatment provided while necessary care is delayed.
Treatment plans can sometimes overlook potential harmful effects of some medications on physical health— whether metabolic, cardiovascular, neurologic, gastrointestinal, hormonal, hematologic, or dermatologic. An optimal treatment plan embarks on healing the mind without ignoring or harming the body.
Failing to obtain additional information from sources who know the patient or who can provide old records. Such information is vital in psychiatry, because the patient’s account often is incomplete, even distorted, because of cognitive deficits or psychopathologic factors. Additional information can be corroborative or contradictory, and is sometimes critical—significantly influencing the diagnosis or the treatment plan, or both.
Allowing personal beliefs to influence care. This transgression includes inserting one’s views about religion, politics, sexual orientation, ethnic origin, and socioeconomic class into medical care. The same unimpeachable, high caliber of care must be provided to every patient, and must not differ in any way from the care that we would recommend to our own family members.
Reducing psychiatry to prescribing a pill. However unacceptable and deficient this reductionist degradation of psychiatric management is, it is sometimes imposed by organizations in which the caseload is huge and the number of providers insufficient. We must resist the temptation to compromise, and must strive to address not only the biological aspects of illness but psychological and social dimensions as well. Patients will not have an optimal if we don’t.
Practicing with an outdated knowledge base—one acquired during residency years, often years or even decades, earlier. There is no medical or ethical justification for using 1985, or even 2005, standards of psychiatric care in 2015.
Psychiatry is rapidly evolving, with many ongoing changes and advances. Updating one’s practice pattern through lifelong learning is an absolute must for psychiatrists (and for all health care professionals). Utilizing the latest, evidence-based data to guide diagnosis and treatment is an indispensable component of good psychiatric care.
Neglecting to consider treatment options. Consider just a few scenarios: The recurrently relapsing patient with psychosis who is not switched to a long-acting injectable formulation; the persistently psychotic patient who does not receive a trial of clozapine; the treatment-resistant depression patient who is not referred for electroconvulsive therapy or transcranial magnetic stimulation; and the patient receiving an atypical antipsychotic who is monitored inconsistently for metabolic dysregulation.
Treating patients but not vigorously advocating for them—thus allowing a broken, convoluted mental health system to delay or prevent access to care; incarcerate relapsed patients instead of hospitalizing them; permit insurance companies to discriminate against coverage of mental illness; and tie the hands of psychiatrists who want to select medication they judge best for their patients.
None of us is 'without sin'
We all aspire to help our patients in the best way we can, and to avoid errors. However, even a seasoned psychiatrist can stumble unwittingly, and that is understandable and forgivable. It is willful, recurring neglect of the patient’s welfare that can be deleterious and that, in my opinion, qualifies as a cardinal sin. Fortunately, such neglect is a low-frequency event in psychiatric practice, but even a single occurrence is one too many.
But as professionals, and by virtue of our rigorous training, we continually reflect on our thoughts and feelings when we care for our patients, and we examine the effect of our behavior and communication patterns on them. Such self-reflection is especially important when it comes to countertransference while treating a person who has been made vulnerable by emotional turmoil and who develops strong transference feelings toward the treating psychiatrist.
Personal integrity is paramount in psychiatric practice; it’s an indispensable ingredient when dealing with the intimate thoughts, feelings, and impulses of people who are seeking psychiatric help. In addition, the wisdom to recognize one’s limitations as a provider of care is an important attributes of seasoned practitioners. Patients might perceive us as demigods, but we know better than to be carried away with hubris and pretend that we are.
Exercising sound judgment isn’t easy
This is especially true when dealing with the varying degrees of ambiguity that shroud complex psychiatric conditions. The overriding principle for good clinical judgment in any medical practice is the patient’s welfare, and that must dominate the moral, ethical, medical, and scientific decision-making of all psychiatrists. Those of us in charge of training medical students and residents emphasize this principle every day at the bedside and in the clinic. Upholding those principles, side by side with the knowledge and skills of psychiatric practice, are the hallmarks of good medical training.
But missteps occur. Peccadillos, infractions, and even transgressions happen—accidentally by competent, ethical psychiatrists; deliberately, sometimes, by a few unethical scoundrels. The sins of psychiatric practice come in a range of gravity and consequences. Here are some I’ve observed among colleagues over the years:
Becoming sexually intimate with one’s patient. Violating the sacred boundary of the doctor-patient relationship is unforgivable; it’s a sin that scars the patient and can destroy the psychiatrist’s reputation and career. We must respect and uphold that boundary—not only during active treatment but even after care is terminated.
Divulging clinical details to other without the patient’s consent. Breach of trust is not only an ethical misstep; it is a violation of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), with substantial penalties attached.
Treating the mind while ignoring the body and brain. We are physicians first, psychiatrists second. We must fully assess patients who present with psychiatric signs and symptoms to rule out a general medical condition that could be generating behavioral symptoms. Such co-occurring medical conditions might involve various organ systems, such as endocrinopathies, or might emanate from brain lesions, whether traumatic, degenerative, demyelinating, infectious, or neoplastic. Without careful medical evaluation, the wrong diagnosis might be made and inappropriate, even harmful, treatment provided while necessary care is delayed.
Treatment plans can sometimes overlook potential harmful effects of some medications on physical health— whether metabolic, cardiovascular, neurologic, gastrointestinal, hormonal, hematologic, or dermatologic. An optimal treatment plan embarks on healing the mind without ignoring or harming the body.
Failing to obtain additional information from sources who know the patient or who can provide old records. Such information is vital in psychiatry, because the patient’s account often is incomplete, even distorted, because of cognitive deficits or psychopathologic factors. Additional information can be corroborative or contradictory, and is sometimes critical—significantly influencing the diagnosis or the treatment plan, or both.
Allowing personal beliefs to influence care. This transgression includes inserting one’s views about religion, politics, sexual orientation, ethnic origin, and socioeconomic class into medical care. The same unimpeachable, high caliber of care must be provided to every patient, and must not differ in any way from the care that we would recommend to our own family members.
Reducing psychiatry to prescribing a pill. However unacceptable and deficient this reductionist degradation of psychiatric management is, it is sometimes imposed by organizations in which the caseload is huge and the number of providers insufficient. We must resist the temptation to compromise, and must strive to address not only the biological aspects of illness but psychological and social dimensions as well. Patients will not have an optimal if we don’t.
Practicing with an outdated knowledge base—one acquired during residency years, often years or even decades, earlier. There is no medical or ethical justification for using 1985, or even 2005, standards of psychiatric care in 2015.
Psychiatry is rapidly evolving, with many ongoing changes and advances. Updating one’s practice pattern through lifelong learning is an absolute must for psychiatrists (and for all health care professionals). Utilizing the latest, evidence-based data to guide diagnosis and treatment is an indispensable component of good psychiatric care.
Neglecting to consider treatment options. Consider just a few scenarios: The recurrently relapsing patient with psychosis who is not switched to a long-acting injectable formulation; the persistently psychotic patient who does not receive a trial of clozapine; the treatment-resistant depression patient who is not referred for electroconvulsive therapy or transcranial magnetic stimulation; and the patient receiving an atypical antipsychotic who is monitored inconsistently for metabolic dysregulation.
Treating patients but not vigorously advocating for them—thus allowing a broken, convoluted mental health system to delay or prevent access to care; incarcerate relapsed patients instead of hospitalizing them; permit insurance companies to discriminate against coverage of mental illness; and tie the hands of psychiatrists who want to select medication they judge best for their patients.
None of us is 'without sin'
We all aspire to help our patients in the best way we can, and to avoid errors. However, even a seasoned psychiatrist can stumble unwittingly, and that is understandable and forgivable. It is willful, recurring neglect of the patient’s welfare that can be deleterious and that, in my opinion, qualifies as a cardinal sin. Fortunately, such neglect is a low-frequency event in psychiatric practice, but even a single occurrence is one too many.
But as professionals, and by virtue of our rigorous training, we continually reflect on our thoughts and feelings when we care for our patients, and we examine the effect of our behavior and communication patterns on them. Such self-reflection is especially important when it comes to countertransference while treating a person who has been made vulnerable by emotional turmoil and who develops strong transference feelings toward the treating psychiatrist.
Personal integrity is paramount in psychiatric practice; it’s an indispensable ingredient when dealing with the intimate thoughts, feelings, and impulses of people who are seeking psychiatric help. In addition, the wisdom to recognize one’s limitations as a provider of care is an important attributes of seasoned practitioners. Patients might perceive us as demigods, but we know better than to be carried away with hubris and pretend that we are.
Exercising sound judgment isn’t easy
This is especially true when dealing with the varying degrees of ambiguity that shroud complex psychiatric conditions. The overriding principle for good clinical judgment in any medical practice is the patient’s welfare, and that must dominate the moral, ethical, medical, and scientific decision-making of all psychiatrists. Those of us in charge of training medical students and residents emphasize this principle every day at the bedside and in the clinic. Upholding those principles, side by side with the knowledge and skills of psychiatric practice, are the hallmarks of good medical training.
But missteps occur. Peccadillos, infractions, and even transgressions happen—accidentally by competent, ethical psychiatrists; deliberately, sometimes, by a few unethical scoundrels. The sins of psychiatric practice come in a range of gravity and consequences. Here are some I’ve observed among colleagues over the years:
Becoming sexually intimate with one’s patient. Violating the sacred boundary of the doctor-patient relationship is unforgivable; it’s a sin that scars the patient and can destroy the psychiatrist’s reputation and career. We must respect and uphold that boundary—not only during active treatment but even after care is terminated.
Divulging clinical details to other without the patient’s consent. Breach of trust is not only an ethical misstep; it is a violation of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), with substantial penalties attached.
Treating the mind while ignoring the body and brain. We are physicians first, psychiatrists second. We must fully assess patients who present with psychiatric signs and symptoms to rule out a general medical condition that could be generating behavioral symptoms. Such co-occurring medical conditions might involve various organ systems, such as endocrinopathies, or might emanate from brain lesions, whether traumatic, degenerative, demyelinating, infectious, or neoplastic. Without careful medical evaluation, the wrong diagnosis might be made and inappropriate, even harmful, treatment provided while necessary care is delayed.
Treatment plans can sometimes overlook potential harmful effects of some medications on physical health— whether metabolic, cardiovascular, neurologic, gastrointestinal, hormonal, hematologic, or dermatologic. An optimal treatment plan embarks on healing the mind without ignoring or harming the body.
Failing to obtain additional information from sources who know the patient or who can provide old records. Such information is vital in psychiatry, because the patient’s account often is incomplete, even distorted, because of cognitive deficits or psychopathologic factors. Additional information can be corroborative or contradictory, and is sometimes critical—significantly influencing the diagnosis or the treatment plan, or both.
Allowing personal beliefs to influence care. This transgression includes inserting one’s views about religion, politics, sexual orientation, ethnic origin, and socioeconomic class into medical care. The same unimpeachable, high caliber of care must be provided to every patient, and must not differ in any way from the care that we would recommend to our own family members.
Reducing psychiatry to prescribing a pill. However unacceptable and deficient this reductionist degradation of psychiatric management is, it is sometimes imposed by organizations in which the caseload is huge and the number of providers insufficient. We must resist the temptation to compromise, and must strive to address not only the biological aspects of illness but psychological and social dimensions as well. Patients will not have an optimal if we don’t.
Practicing with an outdated knowledge base—one acquired during residency years, often years or even decades, earlier. There is no medical or ethical justification for using 1985, or even 2005, standards of psychiatric care in 2015.
Psychiatry is rapidly evolving, with many ongoing changes and advances. Updating one’s practice pattern through lifelong learning is an absolute must for psychiatrists (and for all health care professionals). Utilizing the latest, evidence-based data to guide diagnosis and treatment is an indispensable component of good psychiatric care.
Neglecting to consider treatment options. Consider just a few scenarios: The recurrently relapsing patient with psychosis who is not switched to a long-acting injectable formulation; the persistently psychotic patient who does not receive a trial of clozapine; the treatment-resistant depression patient who is not referred for electroconvulsive therapy or transcranial magnetic stimulation; and the patient receiving an atypical antipsychotic who is monitored inconsistently for metabolic dysregulation.
Treating patients but not vigorously advocating for them—thus allowing a broken, convoluted mental health system to delay or prevent access to care; incarcerate relapsed patients instead of hospitalizing them; permit insurance companies to discriminate against coverage of mental illness; and tie the hands of psychiatrists who want to select medication they judge best for their patients.
None of us is 'without sin'
We all aspire to help our patients in the best way we can, and to avoid errors. However, even a seasoned psychiatrist can stumble unwittingly, and that is understandable and forgivable. It is willful, recurring neglect of the patient’s welfare that can be deleterious and that, in my opinion, qualifies as a cardinal sin. Fortunately, such neglect is a low-frequency event in psychiatric practice, but even a single occurrence is one too many.
The Joys of a Life in Surgery
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.
