User login
Outcome measures need context

Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
10 Triggers of inflammation to be avoided, to reduce the risk of depression
Neuroinflammation is well-established as an underlying mechanism in depression, as well as in other neuropsychiatric disorders, including schizophrenia, multiple sclerosis, stroke, Parkinson’s disease, and sleep disorders.1 There is a dearth of prevention strategies for neuropsychiatric disorders but, given emerging scientific knowledge about immune dysregulation and the associated rise in inflammatory markers during the course of depression,2,3 it is logical to postulate that avoiding triggers of neuroinflammation might be a useful tactic to prevent depression or, perhaps, to minimize its severity.
Challenge your patients to avoid triggers of depression
What is known about what instigates the rise of inflammatory markers in the body and the brain? Actually, quite a substantial body of knowledge exists on the subject.4 Consider the 10 risk factors for depression that I enumerate here (Table), and advise patients to avoid them.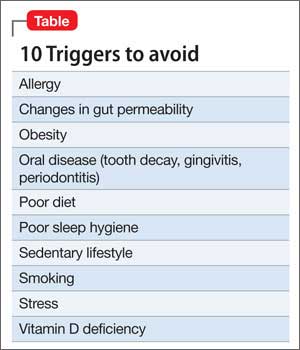
Sedentary lifestyle. Physical inactivity during childhood is associated with depression in adulthood. This is worrisome because video games seem ever more popular among children these days—more popular and prevalent than playing outdoors. Use this knowledge about the preventive benefit of exercise for long-range prevention in young patients.
Adults with a sedentary lifestyle usually have increased adiposity, which increases the risk of depression. Regular exercise has been shown to down-regulate systemic inflammation.
Smoking. Hundreds of toxic and inflammatory components in tobacco smoke (tars, metals, free radicals) can induce inflammation across the body and brain tissue, which explains not only depression but serious pulmonary and cerebrovascular diseases seen in smokers. People with depression are more likely to smoke than the general population, possibly because nicotine has a mild mood-elevating effect. Yet smoking might make depression worse by exacerbating inflammation, thus negating any mood-elevating effect of nicotine.
Poor diet. It is well known that the Western diet (processed meats, refined sugars, saturated fats) can increase the body’s level of inflammatory markers. The Mediterranean diet, on the other hand, which comprises fruits, vegetables, fish, legumes, and foods rich in omega-3 fatty acids (fish, nuts, leafy green vegetables), is anti-inflammatory. Furthermore, lycopene-containing foods (tomatoes, papaya, red cabbage, watermelon, carrots, asparagus) are rich in antioxidants and thus reduce inflammation.
The possible epigenetic effects of diet are an interesting phenomenon. Offspring of rats who were fed a diet rich in saturated fats have elevated levels of inflammatory markers, even when they had been fed a normal diet, suggesting a transgenerational effect. What parents eat before they conceive might doom their child’s health— regardless of what they feed them.
Tooth decay, gingivitis, periodontitis. Oral inflammation afflicts a large percentage of the population. These conditions can lead to systemic inflammation with elevated levels of C-reactive protein (CRP) and interleukins, which are conducive to depression.
Poor sleep hygiene. Sleep disorders, such as insomnia and insufficient sleep (which is epidemic in the United States), are risk factors for mood disorders. Sleep deprivation disrupts immune function and triggers the cascade of elevated cytokines, CRP, and tumor necrosis factor (TNF)-α. Just as depression is associated with impaired neurogenesis, so is chronic lack of sleep, suggesting a convergence of neurobiologic mechanisms.
Vitamin D deficiency. A link between vitamin D deficiency, now common in the United States, and depression and immune function has been recognized. Vitamin D has anti-inflammatory effects and can reduce oxidative stress, which culminates in inflammation. Vitamin D supplementation has been shown to alleviate neuro-immune disorders, such as multiple sclerosis.
Obesity. Obese people are >50% more likely to develop depression than non-obese people. Technically, obesity is a pro-inflammatory state, and inflammatory biomarkers, such as cytokines, are abundant in fat cells, especially abdominal (visceral or peri-omental) adiposity. When an obese person loses weight, levels of inflammatory markers (interleukin-6, TNF-α, leptin) decrease. We know that abdominal obesity is associated with neuroinflammation and early dementia.
Allergy involves inflammation triggered by the cascade of events consequent to the body’s fight against antigens, and the well-known hyper-sensitivity reaction, causing edema, coughing, sneezing, and itching. It is well-established that the incidence of atopy and allergy is high among people with depression.
Changes in gut permeability. Intestinal inflammatory diseases, such as ulcerative colitis, are recognized as pathways to depression. The mechanism is believed to be the immune response to lipopolysaccharides by commensal bacteria that live by the trillions in the gut. The result? Abnormal gut permeability, bacterial translocation, and depressed mood, possibly because serotonin is more abundant in the gut than in the CNS.
Stress. Arguably, the most common pathway to depression is stressful events of daily life. Stress-induced systemic inflammation hastens cardiovascular disease and leads to neuro-inflammation and neuropsychiatric disorders as well.
Especially malignant is the severe stress of childhood trauma (physical and sexual abuse, parental discord and death), which stimulates pro-inflammatory cytokines and detrimental neurobiological sensitization that lead to psychopathology, including depression and psychosis in adulthood. Childhood trauma has been reported to shorten life by 7 to 15 years.
Posttraumatic stress disorder is the best known clinical model of stress-induced depression and anxiety. The disorder is associated with a significant increase in pro-inflammatory cytokines and loss of brain tissue.
2-fold challenge: Reduce severity of disease, reduce risk before disease
We psychiatrists almost always see patients after they’ve developed depression and other psychiatric disorders in which neuroinflammation is already present. In addition to pharmacotherapy and psychotherapy (both reduce inflammation), educating patients about adopting a healthy lifestyle—not smoking, exercising, eating wisely, avoiding weight gain, getting enough sleep, maintaining good oral hygiene, and managing stress—might reduce psychiatric relapse and prolong their life.
We also should be challenged by the fact that the pathways to inflammation, including the 10 I’ve described here, are common among the population at large. Let’s increase our efforts to preemptively reduce the risk of brain disorders by encouraging parents and their children to adopt a healthy lifestyle and maintain wellness—and thus avoid falling victim to depression.
1. Baune BT. Inflammation and neurodegenerative disorders: is there still hope for therapeutic intervention? Curr Opin Psychiatry. 2015;28(2):148-154.
2. Leonard B, Maes M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neurosc Biobehav Rev. 2012;36(2):764-785.
3. Bakunina N, Pariante CM, Zunszain PA. Immune mechanisms linked to depression via oxidative stress and neuroprogression [published online January 10, 2015]. Immunology. 2015. doi: 10.1111/imm.12443.
4. Berk M, Williams LJ, Jacka FN, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013;11:200.
Neuroinflammation is well-established as an underlying mechanism in depression, as well as in other neuropsychiatric disorders, including schizophrenia, multiple sclerosis, stroke, Parkinson’s disease, and sleep disorders.1 There is a dearth of prevention strategies for neuropsychiatric disorders but, given emerging scientific knowledge about immune dysregulation and the associated rise in inflammatory markers during the course of depression,2,3 it is logical to postulate that avoiding triggers of neuroinflammation might be a useful tactic to prevent depression or, perhaps, to minimize its severity.
Challenge your patients to avoid triggers of depression
What is known about what instigates the rise of inflammatory markers in the body and the brain? Actually, quite a substantial body of knowledge exists on the subject.4 Consider the 10 risk factors for depression that I enumerate here (Table), and advise patients to avoid them.
Sedentary lifestyle. Physical inactivity during childhood is associated with depression in adulthood. This is worrisome because video games seem ever more popular among children these days—more popular and prevalent than playing outdoors. Use this knowledge about the preventive benefit of exercise for long-range prevention in young patients.
Adults with a sedentary lifestyle usually have increased adiposity, which increases the risk of depression. Regular exercise has been shown to down-regulate systemic inflammation.
Smoking. Hundreds of toxic and inflammatory components in tobacco smoke (tars, metals, free radicals) can induce inflammation across the body and brain tissue, which explains not only depression but serious pulmonary and cerebrovascular diseases seen in smokers. People with depression are more likely to smoke than the general population, possibly because nicotine has a mild mood-elevating effect. Yet smoking might make depression worse by exacerbating inflammation, thus negating any mood-elevating effect of nicotine.
Poor diet. It is well known that the Western diet (processed meats, refined sugars, saturated fats) can increase the body’s level of inflammatory markers. The Mediterranean diet, on the other hand, which comprises fruits, vegetables, fish, legumes, and foods rich in omega-3 fatty acids (fish, nuts, leafy green vegetables), is anti-inflammatory. Furthermore, lycopene-containing foods (tomatoes, papaya, red cabbage, watermelon, carrots, asparagus) are rich in antioxidants and thus reduce inflammation.
The possible epigenetic effects of diet are an interesting phenomenon. Offspring of rats who were fed a diet rich in saturated fats have elevated levels of inflammatory markers, even when they had been fed a normal diet, suggesting a transgenerational effect. What parents eat before they conceive might doom their child’s health— regardless of what they feed them.
Tooth decay, gingivitis, periodontitis. Oral inflammation afflicts a large percentage of the population. These conditions can lead to systemic inflammation with elevated levels of C-reactive protein (CRP) and interleukins, which are conducive to depression.
Poor sleep hygiene. Sleep disorders, such as insomnia and insufficient sleep (which is epidemic in the United States), are risk factors for mood disorders. Sleep deprivation disrupts immune function and triggers the cascade of elevated cytokines, CRP, and tumor necrosis factor (TNF)-α. Just as depression is associated with impaired neurogenesis, so is chronic lack of sleep, suggesting a convergence of neurobiologic mechanisms.
Vitamin D deficiency. A link between vitamin D deficiency, now common in the United States, and depression and immune function has been recognized. Vitamin D has anti-inflammatory effects and can reduce oxidative stress, which culminates in inflammation. Vitamin D supplementation has been shown to alleviate neuro-immune disorders, such as multiple sclerosis.
Obesity. Obese people are >50% more likely to develop depression than non-obese people. Technically, obesity is a pro-inflammatory state, and inflammatory biomarkers, such as cytokines, are abundant in fat cells, especially abdominal (visceral or peri-omental) adiposity. When an obese person loses weight, levels of inflammatory markers (interleukin-6, TNF-α, leptin) decrease. We know that abdominal obesity is associated with neuroinflammation and early dementia.
Allergy involves inflammation triggered by the cascade of events consequent to the body’s fight against antigens, and the well-known hyper-sensitivity reaction, causing edema, coughing, sneezing, and itching. It is well-established that the incidence of atopy and allergy is high among people with depression.
Changes in gut permeability. Intestinal inflammatory diseases, such as ulcerative colitis, are recognized as pathways to depression. The mechanism is believed to be the immune response to lipopolysaccharides by commensal bacteria that live by the trillions in the gut. The result? Abnormal gut permeability, bacterial translocation, and depressed mood, possibly because serotonin is more abundant in the gut than in the CNS.
Stress. Arguably, the most common pathway to depression is stressful events of daily life. Stress-induced systemic inflammation hastens cardiovascular disease and leads to neuro-inflammation and neuropsychiatric disorders as well.
Especially malignant is the severe stress of childhood trauma (physical and sexual abuse, parental discord and death), which stimulates pro-inflammatory cytokines and detrimental neurobiological sensitization that lead to psychopathology, including depression and psychosis in adulthood. Childhood trauma has been reported to shorten life by 7 to 15 years.
Posttraumatic stress disorder is the best known clinical model of stress-induced depression and anxiety. The disorder is associated with a significant increase in pro-inflammatory cytokines and loss of brain tissue.
2-fold challenge: Reduce severity of disease, reduce risk before disease
We psychiatrists almost always see patients after they’ve developed depression and other psychiatric disorders in which neuroinflammation is already present. In addition to pharmacotherapy and psychotherapy (both reduce inflammation), educating patients about adopting a healthy lifestyle—not smoking, exercising, eating wisely, avoiding weight gain, getting enough sleep, maintaining good oral hygiene, and managing stress—might reduce psychiatric relapse and prolong their life.
We also should be challenged by the fact that the pathways to inflammation, including the 10 I’ve described here, are common among the population at large. Let’s increase our efforts to preemptively reduce the risk of brain disorders by encouraging parents and their children to adopt a healthy lifestyle and maintain wellness—and thus avoid falling victim to depression.
Neuroinflammation is well-established as an underlying mechanism in depression, as well as in other neuropsychiatric disorders, including schizophrenia, multiple sclerosis, stroke, Parkinson’s disease, and sleep disorders.1 There is a dearth of prevention strategies for neuropsychiatric disorders but, given emerging scientific knowledge about immune dysregulation and the associated rise in inflammatory markers during the course of depression,2,3 it is logical to postulate that avoiding triggers of neuroinflammation might be a useful tactic to prevent depression or, perhaps, to minimize its severity.
Challenge your patients to avoid triggers of depression
What is known about what instigates the rise of inflammatory markers in the body and the brain? Actually, quite a substantial body of knowledge exists on the subject.4 Consider the 10 risk factors for depression that I enumerate here (Table), and advise patients to avoid them.
Sedentary lifestyle. Physical inactivity during childhood is associated with depression in adulthood. This is worrisome because video games seem ever more popular among children these days—more popular and prevalent than playing outdoors. Use this knowledge about the preventive benefit of exercise for long-range prevention in young patients.
Adults with a sedentary lifestyle usually have increased adiposity, which increases the risk of depression. Regular exercise has been shown to down-regulate systemic inflammation.
Smoking. Hundreds of toxic and inflammatory components in tobacco smoke (tars, metals, free radicals) can induce inflammation across the body and brain tissue, which explains not only depression but serious pulmonary and cerebrovascular diseases seen in smokers. People with depression are more likely to smoke than the general population, possibly because nicotine has a mild mood-elevating effect. Yet smoking might make depression worse by exacerbating inflammation, thus negating any mood-elevating effect of nicotine.
Poor diet. It is well known that the Western diet (processed meats, refined sugars, saturated fats) can increase the body’s level of inflammatory markers. The Mediterranean diet, on the other hand, which comprises fruits, vegetables, fish, legumes, and foods rich in omega-3 fatty acids (fish, nuts, leafy green vegetables), is anti-inflammatory. Furthermore, lycopene-containing foods (tomatoes, papaya, red cabbage, watermelon, carrots, asparagus) are rich in antioxidants and thus reduce inflammation.
The possible epigenetic effects of diet are an interesting phenomenon. Offspring of rats who were fed a diet rich in saturated fats have elevated levels of inflammatory markers, even when they had been fed a normal diet, suggesting a transgenerational effect. What parents eat before they conceive might doom their child’s health— regardless of what they feed them.
Tooth decay, gingivitis, periodontitis. Oral inflammation afflicts a large percentage of the population. These conditions can lead to systemic inflammation with elevated levels of C-reactive protein (CRP) and interleukins, which are conducive to depression.
Poor sleep hygiene. Sleep disorders, such as insomnia and insufficient sleep (which is epidemic in the United States), are risk factors for mood disorders. Sleep deprivation disrupts immune function and triggers the cascade of elevated cytokines, CRP, and tumor necrosis factor (TNF)-α. Just as depression is associated with impaired neurogenesis, so is chronic lack of sleep, suggesting a convergence of neurobiologic mechanisms.
Vitamin D deficiency. A link between vitamin D deficiency, now common in the United States, and depression and immune function has been recognized. Vitamin D has anti-inflammatory effects and can reduce oxidative stress, which culminates in inflammation. Vitamin D supplementation has been shown to alleviate neuro-immune disorders, such as multiple sclerosis.
Obesity. Obese people are >50% more likely to develop depression than non-obese people. Technically, obesity is a pro-inflammatory state, and inflammatory biomarkers, such as cytokines, are abundant in fat cells, especially abdominal (visceral or peri-omental) adiposity. When an obese person loses weight, levels of inflammatory markers (interleukin-6, TNF-α, leptin) decrease. We know that abdominal obesity is associated with neuroinflammation and early dementia.
Allergy involves inflammation triggered by the cascade of events consequent to the body’s fight against antigens, and the well-known hyper-sensitivity reaction, causing edema, coughing, sneezing, and itching. It is well-established that the incidence of atopy and allergy is high among people with depression.
Changes in gut permeability. Intestinal inflammatory diseases, such as ulcerative colitis, are recognized as pathways to depression. The mechanism is believed to be the immune response to lipopolysaccharides by commensal bacteria that live by the trillions in the gut. The result? Abnormal gut permeability, bacterial translocation, and depressed mood, possibly because serotonin is more abundant in the gut than in the CNS.
Stress. Arguably, the most common pathway to depression is stressful events of daily life. Stress-induced systemic inflammation hastens cardiovascular disease and leads to neuro-inflammation and neuropsychiatric disorders as well.
Especially malignant is the severe stress of childhood trauma (physical and sexual abuse, parental discord and death), which stimulates pro-inflammatory cytokines and detrimental neurobiological sensitization that lead to psychopathology, including depression and psychosis in adulthood. Childhood trauma has been reported to shorten life by 7 to 15 years.
Posttraumatic stress disorder is the best known clinical model of stress-induced depression and anxiety. The disorder is associated with a significant increase in pro-inflammatory cytokines and loss of brain tissue.
2-fold challenge: Reduce severity of disease, reduce risk before disease
We psychiatrists almost always see patients after they’ve developed depression and other psychiatric disorders in which neuroinflammation is already present. In addition to pharmacotherapy and psychotherapy (both reduce inflammation), educating patients about adopting a healthy lifestyle—not smoking, exercising, eating wisely, avoiding weight gain, getting enough sleep, maintaining good oral hygiene, and managing stress—might reduce psychiatric relapse and prolong their life.
We also should be challenged by the fact that the pathways to inflammation, including the 10 I’ve described here, are common among the population at large. Let’s increase our efforts to preemptively reduce the risk of brain disorders by encouraging parents and their children to adopt a healthy lifestyle and maintain wellness—and thus avoid falling victim to depression.
1. Baune BT. Inflammation and neurodegenerative disorders: is there still hope for therapeutic intervention? Curr Opin Psychiatry. 2015;28(2):148-154.
2. Leonard B, Maes M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neurosc Biobehav Rev. 2012;36(2):764-785.
3. Bakunina N, Pariante CM, Zunszain PA. Immune mechanisms linked to depression via oxidative stress and neuroprogression [published online January 10, 2015]. Immunology. 2015. doi: 10.1111/imm.12443.
4. Berk M, Williams LJ, Jacka FN, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013;11:200.
1. Baune BT. Inflammation and neurodegenerative disorders: is there still hope for therapeutic intervention? Curr Opin Psychiatry. 2015;28(2):148-154.
2. Leonard B, Maes M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neurosc Biobehav Rev. 2012;36(2):764-785.
3. Bakunina N, Pariante CM, Zunszain PA. Immune mechanisms linked to depression via oxidative stress and neuroprogression [published online January 10, 2015]. Immunology. 2015. doi: 10.1111/imm.12443.
4. Berk M, Williams LJ, Jacka FN, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013;11:200.
Recognition of latest CLL therapies highlights new options for other cancers
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Diagnostic certainty and the eosinophil
This issue of the Journal contains an article by Dr. David A. Katzka, titled “The ‘skinny’ on eosinophilic esophagitis.” Reading it, I was struck by two messages, one clinical and one biological.
The clinical message relates to the psychology of diagnosis, or as Dr. Jerome Groopman discussed in his book How Doctors Think, misdiagnosis. In many patients, eosinophilic esophagitis, especially early in its course, can mimic gastroesophageal reflux disease (GERD), causing dysphagia and discomfort with eating that may be relieved at least in part with a proton pump inhibitor. When evaluating a patient who relates a history compatible with a common condition, we instinctively tend to embrace the diagnosis of that common syndrome, in this case GERD, rather than initially explore in depth the possibility of less-common mimics. Once the disease has progressed, with the patient experiencing frequent postprandial emesis or needing to dramatically limit the size of meals despite taking a full dose of a proton pump inhibitor, we will hopefully revisit and reassess our initial diagnosis, often with endoscopy and biopsy. But that may not always occur promptly, because we may have committed (per Groopman) an “anchoring error,” seizing on an initial symptom or finding, allowing it to cloud our clinical judgment, reaching “premature closure,” and not keeping our minds open to alternative diagnoses such as eosinophilic esophagitis. I wonder how many of the younger patients I have diagnosed with GERD who had histories of “food intolerances” actually had eosinophilic esophagitis.
The biological message is that the eosinophil is a fascinating and generally misunderstood cell, not just a marker and mediator of allergy. As an apparent defender against the macro-invaders—worms and other parasites—it carries an arsenal of defensive weapons. But eosinophil-dominant inflammatory reactions started by various molecular triggers and perpetuated by interleukin 5 and other promoters of eosinophil proliferation and chemotaxis have a common histopathologic footprint—fibrosis.
Long-standing significant asthma is characterized as much by airway remodeling and fibrosis as it is by bronchospasm. A myocardial hallmark of hypereosinophilic syndrome is fibrosis. Eosinophilic pneumonia can be followed by local scarring. Eosinophils have been implicated in the pathogenesis of primary biliary cirrhosis and the granulomatous cirrhosis of schistosomiasis. And as Dr. Katzka reminds us, the confluence of food hypersensitivity, gastric acid, and the products of eosinophil activation (likely including transforming growth factor beta) in the esophageal wall can result in a marked fibrotic reaction with dysmotility. It is unclear whether this is a dysregulated attempt at healing with resultant maladaptive “scar” formation, or perhaps a misdirected inflammatory response, with the goal of walling off a perceived invader (an allergen is not a worm).
There are probably many other mimic diseases that we are not recognizing often enough. And tissue eosinophils may portend detrimental fibrotic remodeling.
This issue of the Journal contains an article by Dr. David A. Katzka, titled “The ‘skinny’ on eosinophilic esophagitis.” Reading it, I was struck by two messages, one clinical and one biological.
The clinical message relates to the psychology of diagnosis, or as Dr. Jerome Groopman discussed in his book How Doctors Think, misdiagnosis. In many patients, eosinophilic esophagitis, especially early in its course, can mimic gastroesophageal reflux disease (GERD), causing dysphagia and discomfort with eating that may be relieved at least in part with a proton pump inhibitor. When evaluating a patient who relates a history compatible with a common condition, we instinctively tend to embrace the diagnosis of that common syndrome, in this case GERD, rather than initially explore in depth the possibility of less-common mimics. Once the disease has progressed, with the patient experiencing frequent postprandial emesis or needing to dramatically limit the size of meals despite taking a full dose of a proton pump inhibitor, we will hopefully revisit and reassess our initial diagnosis, often with endoscopy and biopsy. But that may not always occur promptly, because we may have committed (per Groopman) an “anchoring error,” seizing on an initial symptom or finding, allowing it to cloud our clinical judgment, reaching “premature closure,” and not keeping our minds open to alternative diagnoses such as eosinophilic esophagitis. I wonder how many of the younger patients I have diagnosed with GERD who had histories of “food intolerances” actually had eosinophilic esophagitis.
The biological message is that the eosinophil is a fascinating and generally misunderstood cell, not just a marker and mediator of allergy. As an apparent defender against the macro-invaders—worms and other parasites—it carries an arsenal of defensive weapons. But eosinophil-dominant inflammatory reactions started by various molecular triggers and perpetuated by interleukin 5 and other promoters of eosinophil proliferation and chemotaxis have a common histopathologic footprint—fibrosis.
Long-standing significant asthma is characterized as much by airway remodeling and fibrosis as it is by bronchospasm. A myocardial hallmark of hypereosinophilic syndrome is fibrosis. Eosinophilic pneumonia can be followed by local scarring. Eosinophils have been implicated in the pathogenesis of primary biliary cirrhosis and the granulomatous cirrhosis of schistosomiasis. And as Dr. Katzka reminds us, the confluence of food hypersensitivity, gastric acid, and the products of eosinophil activation (likely including transforming growth factor beta) in the esophageal wall can result in a marked fibrotic reaction with dysmotility. It is unclear whether this is a dysregulated attempt at healing with resultant maladaptive “scar” formation, or perhaps a misdirected inflammatory response, with the goal of walling off a perceived invader (an allergen is not a worm).
There are probably many other mimic diseases that we are not recognizing often enough. And tissue eosinophils may portend detrimental fibrotic remodeling.
This issue of the Journal contains an article by Dr. David A. Katzka, titled “The ‘skinny’ on eosinophilic esophagitis.” Reading it, I was struck by two messages, one clinical and one biological.
The clinical message relates to the psychology of diagnosis, or as Dr. Jerome Groopman discussed in his book How Doctors Think, misdiagnosis. In many patients, eosinophilic esophagitis, especially early in its course, can mimic gastroesophageal reflux disease (GERD), causing dysphagia and discomfort with eating that may be relieved at least in part with a proton pump inhibitor. When evaluating a patient who relates a history compatible with a common condition, we instinctively tend to embrace the diagnosis of that common syndrome, in this case GERD, rather than initially explore in depth the possibility of less-common mimics. Once the disease has progressed, with the patient experiencing frequent postprandial emesis or needing to dramatically limit the size of meals despite taking a full dose of a proton pump inhibitor, we will hopefully revisit and reassess our initial diagnosis, often with endoscopy and biopsy. But that may not always occur promptly, because we may have committed (per Groopman) an “anchoring error,” seizing on an initial symptom or finding, allowing it to cloud our clinical judgment, reaching “premature closure,” and not keeping our minds open to alternative diagnoses such as eosinophilic esophagitis. I wonder how many of the younger patients I have diagnosed with GERD who had histories of “food intolerances” actually had eosinophilic esophagitis.
The biological message is that the eosinophil is a fascinating and generally misunderstood cell, not just a marker and mediator of allergy. As an apparent defender against the macro-invaders—worms and other parasites—it carries an arsenal of defensive weapons. But eosinophil-dominant inflammatory reactions started by various molecular triggers and perpetuated by interleukin 5 and other promoters of eosinophil proliferation and chemotaxis have a common histopathologic footprint—fibrosis.
Long-standing significant asthma is characterized as much by airway remodeling and fibrosis as it is by bronchospasm. A myocardial hallmark of hypereosinophilic syndrome is fibrosis. Eosinophilic pneumonia can be followed by local scarring. Eosinophils have been implicated in the pathogenesis of primary biliary cirrhosis and the granulomatous cirrhosis of schistosomiasis. And as Dr. Katzka reminds us, the confluence of food hypersensitivity, gastric acid, and the products of eosinophil activation (likely including transforming growth factor beta) in the esophageal wall can result in a marked fibrotic reaction with dysmotility. It is unclear whether this is a dysregulated attempt at healing with resultant maladaptive “scar” formation, or perhaps a misdirected inflammatory response, with the goal of walling off a perceived invader (an allergen is not a worm).
There are probably many other mimic diseases that we are not recognizing often enough. And tissue eosinophils may portend detrimental fibrotic remodeling.
Optimal pharmacologic treatment of nausea and vomiting of pregnancy
CASE: Pregnant patient seeks medication for her NVP
A 23-year-old G1P0 woman at 9 weeks’ gestation presents to your office with nausea and vomiting that is interfering with work. She has tried many changes in her daily habits. She has tried eating small, frequent meals; snacking on nuts and crackers; using lemon-scented products; and avoiding coffee and strong odors. Following an evaluation you diagnose nausea and vomiting of pregnancy (NVP). She asks, “Is there a medication for my nausea that is safe for my baby?”
Nausea with or without vomiting is a common problem for pregnant women between 6 and 14 weeks of gestation. In one study, nausea with or without vomiting was reported by 69% of patients and resulted in pharmacologic treatment in 15%.1 In a Cochrane review of NVP, investigators analyzed 37 trials involving treatments such as acupressure, acustimulation, acupuncture, ginger, chamomile, lemon oil, vitamin B6, and antiemetic medications. The authors concluded, “There is a lack of high-quality evidence to support any particular intervention.”2 Clinicians are challenged to effectively treat the symptoms of NVP and simultaneously to minimize the risk that the fetus will be exposed to a teratogen during the first trimester, a vulnerable period in organ development.
In this editorial, I briefly review nonpharmacologic options for NVP, but focus on current pharmacologic treatments. Of those available to ObGyns, what is the best first-choice treatment given recent and accumulated data regarding associated congenital anomalies?
Nonpharmacologic treatment
Although the authors of the Cochrane review did not identify high-quality evidence to support nonpharmacologic interventions, results of multiple randomized trials have demonstrated that ginger is effective in reducing pregnancy-associated nausea and vomiting.3 Ginger treatment is recommended at doses of 250 mg in capsules or syrup four times daily.
First-line pharmacologic treatment: Doxylamine plus pyridoxine
The US Food and Drug Administration (FDA) has approved the combination of doxylamine plus pyridoxine (vitamin B6) in a delayed-release formulation for treatment of NVP (Diclegis). Doxylamine is an antihistamine that blocks H1-receptor sites in the chemoreceptor trigger zone. It also diminishes vestibular stimulation and depresses labyrinthine activity through central anticholinergic activity. Its elimination half-life is 10 to 12 hours (Lexicomp). Each tablet contains doxylamine 10 mg and pyridoxine 10 mg. The starting dose is 2 tablets at bedtime.
If the woman has persistent symptoms, a third tablet is added, to be taken in the morning. If symptoms continue, a fourth tablet is recommended to be taken in the afternoon. In a large, randomized clinical trial, doxylamine-pyridoxine treatment reduced nausea, vomiting, and retching and improved perceived quality of life compared with placebo.4 The FDA assigned doxylamine-pyridoxine pregnancy category A because of the extensive evidence that it does not cause an increase in fetal malformations.5,6
If the delayed-release doxylamine-pyridoxine formulation (Diclegis) is not available to the patient, alternative formulations of doxylamine and pyridoxine can be prescribed. Pyridoxine is widely available over the counter as 25-mg tablets, and one tablet can be prescribed two or three times daily. Doxylamine is available as a chewable prescription medicine in 5-mg tablets (Aldex AN) and two tablets can be prescribed two or three times daily. Doxylamine is also available as a 25-mg over-the-counter tablet in Unisom SleepTabs. One-half tablet can be prescribed two or three times daily. The patient should be alerted that Unisom SleepGels contain diphenhydramine, not doxylamine.
Second-line pharmacologic treatment
Metoclopramide Metoclopramide is a dopamine antagonist. It enhances upper gastrointestinal motility, accelerates gastric emptying, and increases lower esophageal sphincter tone. At higher doses it blocks serotonin receptors in the chemoreceptor trigger zone. Its elimination half-life is 5 to 6 hours (Lexicomp). There are no large, randomized, placebo-controlled trials of oral metoclopramide for the treatment of nausea and vomiting of early pregnancy.
I am recommending metoclopramide as a second-line treatment for NVP because it appears to be effective and is not known to be associated with an increased risk of congenital malformations. Metoclopramide is widely used to prevent and treat intraoperative and postoperative nausea associated with cesarean delivery.7 In addition, intravenous (IV) metoclopramide is commonly used to treat women hospitalized with hyperemesis gravidarum. Results of randomized clinical trials demonstrate that when used to treat hyperemesis gravidarum, IV metoclopramide (10 mg every 8 hours) has similar efficacy to IV ondansetron (4 mg every 8 hours)8 and IV promethazine (25 mg every 8 hours).9 When using metoclopramide as an oral treatment for NVP, 10 mg every 8 hours is a commonly recommended regimen.
The FDA has assigned metoclopramide to pregnancy category B, which indicates that there is no evidence of fetal risk. Studies from Israel and Denmark show that metoclopramide is not associated with an increased risk of congenital malformations. In the study from Israel, among 3,458 infants born to women who had filled a prescription for metoclopramide during the first trimester of pregnancy, there was no increase in major congenital malformations, low birth weight, preterm delivery, or perinatal death.10 In the study from Denmark, among 28,486 infants born to mothers who had filled a prescription for metoclopramide in the first trimester there was no increase in congenital malformations or any of 20 individual categories of malformations, including neural tube defects, transposition of the great vessels, ventricular septal defect, atrial septal defect, tetralogy of Fallot, coarctation of the aorta, cleft lip or palate, anorectal atresia/stenosis, or limb reduction.11 The results of these two large studies are reassuring that metoclopramide is not associated with an increased risk of congenital malformations.
Metoclopramide can cause tardive dyskinesia, a serious movement disorder that may be irreversible with discontinuation of the drug. This risk increases with dose and length of treatment. The FDA recommends that clinicians avoid the use of metoclopramide for more than 12 weeks.
Third-line pharmacologic treatment: Ondansetron
In the United States ondansetron is commonly used to treat NVP.12 The drug is a selective 5-HT3 antagonist that blocks serotonin action in the central nervous system chemoreceptor trigger zone. The elimination half-life of ondansetron is 3 to 6 hours (Lexicomp).
The frequent use of ondansetron may be due, in part, to the perception that it is a very effective antiemetic. For example, in one small clinical trial, ondansetron 4 mg every 8 hours was reported to be superior to a combination of pyridoxine 25 mg every 8 hours plus doxylamine 12.5 mg every 8 hours.13 (Note that the pyridoxine and doxylamine tablets used in this trial were not in a combination delayed-release formulation.) I am recommending ondansetron as a third-line treatment for NVP because, although it is effective, it may be associated with an increased risk of fetal cardiac anomalies.
Is ondansetron associated with cardiac malformations?
The FDA has assigned ondansetron to pregnancy category B; however, there is concern that it may be associated with congenital heart defects. In a recent study of 1,349 infants born to Swedish women who had filled a prescription for ondansetron in early pregnancy, a significantly increased risk of cardiovascular defect (odds ratio [OR], 1.62; 95% confidence interval [CI], 1.04−2.14) and cardiac septum defect (OR, 2.05; 95% CI, 1.19−3.28) was reported.14 The cardiac anomalies were mostly atrial septal or ventricular septal defects.
In a second study, reported as an abstract, authors analyzed congenital malformations in 1,248 infants born to Danish women who filled a prescription for ondansetron in early pregnancy. These authors also found an increased risk of a congenital heart malformation (OR, 2.0; 95% CI, 1.3−3.1).15
A US case-control study showed an association between ondansetron use and cleft palate.1 The Swedish14 and Danish15 studies reported above did not find an association between ondansetron use and cleft palate.
The FDA issued a warning in June 2012 that at a dose of 32 mg, administered intravenously, ondansetron may prolong the QT interval and result in a potentially fatal heart arrhythmia, torsades de pointes.16 In the announcement the FDA did not alter the recommendations for oral dosing because there is no strong evidence that oral dosing is associated with clinically significant arrhythmias. Authors of a recent systematic review concluded that IV administration of large doses of ondansetron may cause cardiac arrhythmias, especially in patients with cardiac disease and those taking other drugs that prolong the QT interval, but that a single oral dose of ondansetron does not have a significant risk of causing an arrhythmia.17
Health Canada18 has advised that many commonly prescribed medications increase serotonin activity. When multiple drugs that each increase serotonin activity are prescribed in combination, the risk of serotonin syndrome is increased. Serotonin syndrome results in hyperthermia, agitation, tachycardia, and muscle twitching and can be fatal. Ondansetron was specifically mentioned in the Health Canada warning, but a search of the literature revealed very few reported cases of ondansetron being implicated in the serotonin syndrome.19
My bottom-line recommendations
NVP is a common obstetric problem. When oral pharmacologic therapy is indicated, first-line treatment should be with the FDA-approved combination of doxylamine-pyridoxine because it is both effective and associated with no known increased risk of congenital malformations. An effective second-line agent is metoclopramide. Based on very limited data, metoclopramide appears effective and is not associated with an increased risk of congenital malformations. However, it is not FDA approved for treatment of NVP. Ondansetron appears to be effective but its use in early pregnancy may be associated with congenital anomalies. Consequently, ondansetron should not be used to treat NVP unless first- and second-line treatments have been ineffective to treat the patient’s symptoms.
INSTANT POLL
Which of the following pharmacologic treatments of nausea with or without vomiting during pregnancy is your first-line medication choice?
• Ondansetron
• Metoclopramide
• Doxylamine-pyridoxine
• Meclizine Promethazine
• Trimethobenzamide
Visit the Quick Poll on the homepage, give your answer, and then see how other ObGyns have answered.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Anderka M, Mitchell AA, Louik C, Werler MMA, Hernandez-Diaz S, Rasmussen SA; National Birth Defects Prevention Study. Medications used to treat nausea and vomiting of pregnancy and the risk of selected birth defects. Birth Defects Res A Clin Mol Teratol. 2012;94(1):22–30.
2. Matthews A, Haas Dm, O’Mathuna DP, Dowswell T, Doyle M. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2014;(3):CD007575.
3. Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA. Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstet Gynecol. 2005;105(4):849–856.
4. Koren G, Clark S, Hankins GD, et al. Effectiveness of delayed-release doxylamine and pyridoxine for nausea and vomiting of pregnancy: a randomized placebo controlled trial. Am J Obstet Gynecol. 2010;203(6):571.e1–7.
5. Einarson TR, Leeder JS, Koren G. A method for meta-analysis of epidemiologic studies. Drug Intell Clin Pharm. 1988;22(10):813–824.
6. McKeigue PM, Lamm SH, Linn S, Kutcher JS. Bendectin and birth defects. I. A meta-analysis of the epidemiologic studies. Teratology. 1994;50(1):27–37.
7. Mishriky BM, Habib AS. Metoclopramide for nausea and vomiting prophylaxis during and after cesarean delivery: a systematic review and meta-analysis. Br J Anaesth. 2012;108(3):374–383.
8. Abas MN, Tan PC, Azmi N, Omar SZ. Ondansetron compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2014;123(6):1272–1279.
9. Tan PC, Khine PP, Vallikkannu N, Omar SZ. Promethazine compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2010;115(5):975–981.
10. Matok I, Gorodischer R, Koren G, Sheiner E, Wiznitzer A, Levy A. The safety of metoclopramide use in the first trimester of pregnancy. N Engl J Med. 2009;360(24):2528–2535.
11. Pasternak B, Svanstrom H, Molgaard-Nielsen D, Melbye M, Hviid A. Metoclopramide in pregnancy and risk of major congenital malformations and fetal death. JAMA. 2013;310(15):1601–1611.
12. Koren G. Treating morning sickness in the United States—changes in prescribing are needed. Am J Obstet Gynecol. 2014;211(6):602–606.
13. Oliveira LG, Capp SM, You WB, Riffenburgh RH, Carstairs SH. Ondansetron compared with doxylamine and pyridoxine for treatment of nausea in pregnancy : a randomized controlled trial. Obstet Gynecol. 2014;124(4):735–742.
14. Danielsson B, Wikner BN, Kallen B. Use of ondansetron during pregnancy and congenital malformations in the infant. Reprod Toxicol. 2014;50:134–137.
15. Andersen JT, Jimenez-Solem E, Andersen NL, Poulsen HE. Ondansetron use in early pregnancy and the risk of congenital malformations—a registry based nationwide cohort study. Abstract presented at: 29th International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 25–28, 2013; Montreal, Canada. Abstract 25, Pregnancy Session 1. Pharmacoepidemiol Drug Saf. 2013;22(suppl 1):13–14.
16. US Food and Drug Administration. Ondansetron (Zofran) IV: drug safety communication - QT prolongation. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm310219.htm. Published June 29, 2012. Accessed December 26, 2014.
17. Freedman SB, Uleryk E, Rumantir M, Finkelstein Y. Ondansetron and the risk of cardiac arrhythmias: a systematic review and postmarketing analysis. Ann Emerg Med. 2014;64(1):19–25.
18. Health Canada. Canadian Adverse Reaction Newsletter. 2003;13(3). http://www.hc-sc.gc.ca/dhp-mps/medeff/bulletin/carn-bcei_v13n3-eng.php. Published June 24, 2003. Accessed December 26, 2014.
19. Turkel SB, Nadala JG, Wincor MZ. Possible serotonin syndrome in association with 5-HT3 antagonist agents. Psychosomatics. 2001;42(3):258–260.

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: Pregnant patient seeks medication for her NVP
A 23-year-old G1P0 woman at 9 weeks’ gestation presents to your office with nausea and vomiting that is interfering with work. She has tried many changes in her daily habits. She has tried eating small, frequent meals; snacking on nuts and crackers; using lemon-scented products; and avoiding coffee and strong odors. Following an evaluation you diagnose nausea and vomiting of pregnancy (NVP). She asks, “Is there a medication for my nausea that is safe for my baby?”
Nausea with or without vomiting is a common problem for pregnant women between 6 and 14 weeks of gestation. In one study, nausea with or without vomiting was reported by 69% of patients and resulted in pharmacologic treatment in 15%.1 In a Cochrane review of NVP, investigators analyzed 37 trials involving treatments such as acupressure, acustimulation, acupuncture, ginger, chamomile, lemon oil, vitamin B6, and antiemetic medications. The authors concluded, “There is a lack of high-quality evidence to support any particular intervention.”2 Clinicians are challenged to effectively treat the symptoms of NVP and simultaneously to minimize the risk that the fetus will be exposed to a teratogen during the first trimester, a vulnerable period in organ development.
In this editorial, I briefly review nonpharmacologic options for NVP, but focus on current pharmacologic treatments. Of those available to ObGyns, what is the best first-choice treatment given recent and accumulated data regarding associated congenital anomalies?
Nonpharmacologic treatment
Although the authors of the Cochrane review did not identify high-quality evidence to support nonpharmacologic interventions, results of multiple randomized trials have demonstrated that ginger is effective in reducing pregnancy-associated nausea and vomiting.3 Ginger treatment is recommended at doses of 250 mg in capsules or syrup four times daily.
First-line pharmacologic treatment: Doxylamine plus pyridoxine
The US Food and Drug Administration (FDA) has approved the combination of doxylamine plus pyridoxine (vitamin B6) in a delayed-release formulation for treatment of NVP (Diclegis). Doxylamine is an antihistamine that blocks H1-receptor sites in the chemoreceptor trigger zone. It also diminishes vestibular stimulation and depresses labyrinthine activity through central anticholinergic activity. Its elimination half-life is 10 to 12 hours (Lexicomp). Each tablet contains doxylamine 10 mg and pyridoxine 10 mg. The starting dose is 2 tablets at bedtime.
If the woman has persistent symptoms, a third tablet is added, to be taken in the morning. If symptoms continue, a fourth tablet is recommended to be taken in the afternoon. In a large, randomized clinical trial, doxylamine-pyridoxine treatment reduced nausea, vomiting, and retching and improved perceived quality of life compared with placebo.4 The FDA assigned doxylamine-pyridoxine pregnancy category A because of the extensive evidence that it does not cause an increase in fetal malformations.5,6
If the delayed-release doxylamine-pyridoxine formulation (Diclegis) is not available to the patient, alternative formulations of doxylamine and pyridoxine can be prescribed. Pyridoxine is widely available over the counter as 25-mg tablets, and one tablet can be prescribed two or three times daily. Doxylamine is available as a chewable prescription medicine in 5-mg tablets (Aldex AN) and two tablets can be prescribed two or three times daily. Doxylamine is also available as a 25-mg over-the-counter tablet in Unisom SleepTabs. One-half tablet can be prescribed two or three times daily. The patient should be alerted that Unisom SleepGels contain diphenhydramine, not doxylamine.
Second-line pharmacologic treatment
Metoclopramide Metoclopramide is a dopamine antagonist. It enhances upper gastrointestinal motility, accelerates gastric emptying, and increases lower esophageal sphincter tone. At higher doses it blocks serotonin receptors in the chemoreceptor trigger zone. Its elimination half-life is 5 to 6 hours (Lexicomp). There are no large, randomized, placebo-controlled trials of oral metoclopramide for the treatment of nausea and vomiting of early pregnancy.
I am recommending metoclopramide as a second-line treatment for NVP because it appears to be effective and is not known to be associated with an increased risk of congenital malformations. Metoclopramide is widely used to prevent and treat intraoperative and postoperative nausea associated with cesarean delivery.7 In addition, intravenous (IV) metoclopramide is commonly used to treat women hospitalized with hyperemesis gravidarum. Results of randomized clinical trials demonstrate that when used to treat hyperemesis gravidarum, IV metoclopramide (10 mg every 8 hours) has similar efficacy to IV ondansetron (4 mg every 8 hours)8 and IV promethazine (25 mg every 8 hours).9 When using metoclopramide as an oral treatment for NVP, 10 mg every 8 hours is a commonly recommended regimen.
The FDA has assigned metoclopramide to pregnancy category B, which indicates that there is no evidence of fetal risk. Studies from Israel and Denmark show that metoclopramide is not associated with an increased risk of congenital malformations. In the study from Israel, among 3,458 infants born to women who had filled a prescription for metoclopramide during the first trimester of pregnancy, there was no increase in major congenital malformations, low birth weight, preterm delivery, or perinatal death.10 In the study from Denmark, among 28,486 infants born to mothers who had filled a prescription for metoclopramide in the first trimester there was no increase in congenital malformations or any of 20 individual categories of malformations, including neural tube defects, transposition of the great vessels, ventricular septal defect, atrial septal defect, tetralogy of Fallot, coarctation of the aorta, cleft lip or palate, anorectal atresia/stenosis, or limb reduction.11 The results of these two large studies are reassuring that metoclopramide is not associated with an increased risk of congenital malformations.
Metoclopramide can cause tardive dyskinesia, a serious movement disorder that may be irreversible with discontinuation of the drug. This risk increases with dose and length of treatment. The FDA recommends that clinicians avoid the use of metoclopramide for more than 12 weeks.
Third-line pharmacologic treatment: Ondansetron
In the United States ondansetron is commonly used to treat NVP.12 The drug is a selective 5-HT3 antagonist that blocks serotonin action in the central nervous system chemoreceptor trigger zone. The elimination half-life of ondansetron is 3 to 6 hours (Lexicomp).
The frequent use of ondansetron may be due, in part, to the perception that it is a very effective antiemetic. For example, in one small clinical trial, ondansetron 4 mg every 8 hours was reported to be superior to a combination of pyridoxine 25 mg every 8 hours plus doxylamine 12.5 mg every 8 hours.13 (Note that the pyridoxine and doxylamine tablets used in this trial were not in a combination delayed-release formulation.) I am recommending ondansetron as a third-line treatment for NVP because, although it is effective, it may be associated with an increased risk of fetal cardiac anomalies.
Is ondansetron associated with cardiac malformations?
The FDA has assigned ondansetron to pregnancy category B; however, there is concern that it may be associated with congenital heart defects. In a recent study of 1,349 infants born to Swedish women who had filled a prescription for ondansetron in early pregnancy, a significantly increased risk of cardiovascular defect (odds ratio [OR], 1.62; 95% confidence interval [CI], 1.04−2.14) and cardiac septum defect (OR, 2.05; 95% CI, 1.19−3.28) was reported.14 The cardiac anomalies were mostly atrial septal or ventricular septal defects.
In a second study, reported as an abstract, authors analyzed congenital malformations in 1,248 infants born to Danish women who filled a prescription for ondansetron in early pregnancy. These authors also found an increased risk of a congenital heart malformation (OR, 2.0; 95% CI, 1.3−3.1).15
A US case-control study showed an association between ondansetron use and cleft palate.1 The Swedish14 and Danish15 studies reported above did not find an association between ondansetron use and cleft palate.
The FDA issued a warning in June 2012 that at a dose of 32 mg, administered intravenously, ondansetron may prolong the QT interval and result in a potentially fatal heart arrhythmia, torsades de pointes.16 In the announcement the FDA did not alter the recommendations for oral dosing because there is no strong evidence that oral dosing is associated with clinically significant arrhythmias. Authors of a recent systematic review concluded that IV administration of large doses of ondansetron may cause cardiac arrhythmias, especially in patients with cardiac disease and those taking other drugs that prolong the QT interval, but that a single oral dose of ondansetron does not have a significant risk of causing an arrhythmia.17
Health Canada18 has advised that many commonly prescribed medications increase serotonin activity. When multiple drugs that each increase serotonin activity are prescribed in combination, the risk of serotonin syndrome is increased. Serotonin syndrome results in hyperthermia, agitation, tachycardia, and muscle twitching and can be fatal. Ondansetron was specifically mentioned in the Health Canada warning, but a search of the literature revealed very few reported cases of ondansetron being implicated in the serotonin syndrome.19
My bottom-line recommendations
NVP is a common obstetric problem. When oral pharmacologic therapy is indicated, first-line treatment should be with the FDA-approved combination of doxylamine-pyridoxine because it is both effective and associated with no known increased risk of congenital malformations. An effective second-line agent is metoclopramide. Based on very limited data, metoclopramide appears effective and is not associated with an increased risk of congenital malformations. However, it is not FDA approved for treatment of NVP. Ondansetron appears to be effective but its use in early pregnancy may be associated with congenital anomalies. Consequently, ondansetron should not be used to treat NVP unless first- and second-line treatments have been ineffective to treat the patient’s symptoms.
INSTANT POLL
Which of the following pharmacologic treatments of nausea with or without vomiting during pregnancy is your first-line medication choice?
• Ondansetron
• Metoclopramide
• Doxylamine-pyridoxine
• Meclizine Promethazine
• Trimethobenzamide
Visit the Quick Poll on the homepage, give your answer, and then see how other ObGyns have answered.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
CASE: Pregnant patient seeks medication for her NVP
A 23-year-old G1P0 woman at 9 weeks’ gestation presents to your office with nausea and vomiting that is interfering with work. She has tried many changes in her daily habits. She has tried eating small, frequent meals; snacking on nuts and crackers; using lemon-scented products; and avoiding coffee and strong odors. Following an evaluation you diagnose nausea and vomiting of pregnancy (NVP). She asks, “Is there a medication for my nausea that is safe for my baby?”
Nausea with or without vomiting is a common problem for pregnant women between 6 and 14 weeks of gestation. In one study, nausea with or without vomiting was reported by 69% of patients and resulted in pharmacologic treatment in 15%.1 In a Cochrane review of NVP, investigators analyzed 37 trials involving treatments such as acupressure, acustimulation, acupuncture, ginger, chamomile, lemon oil, vitamin B6, and antiemetic medications. The authors concluded, “There is a lack of high-quality evidence to support any particular intervention.”2 Clinicians are challenged to effectively treat the symptoms of NVP and simultaneously to minimize the risk that the fetus will be exposed to a teratogen during the first trimester, a vulnerable period in organ development.
In this editorial, I briefly review nonpharmacologic options for NVP, but focus on current pharmacologic treatments. Of those available to ObGyns, what is the best first-choice treatment given recent and accumulated data regarding associated congenital anomalies?
Nonpharmacologic treatment
Although the authors of the Cochrane review did not identify high-quality evidence to support nonpharmacologic interventions, results of multiple randomized trials have demonstrated that ginger is effective in reducing pregnancy-associated nausea and vomiting.3 Ginger treatment is recommended at doses of 250 mg in capsules or syrup four times daily.
First-line pharmacologic treatment: Doxylamine plus pyridoxine
The US Food and Drug Administration (FDA) has approved the combination of doxylamine plus pyridoxine (vitamin B6) in a delayed-release formulation for treatment of NVP (Diclegis). Doxylamine is an antihistamine that blocks H1-receptor sites in the chemoreceptor trigger zone. It also diminishes vestibular stimulation and depresses labyrinthine activity through central anticholinergic activity. Its elimination half-life is 10 to 12 hours (Lexicomp). Each tablet contains doxylamine 10 mg and pyridoxine 10 mg. The starting dose is 2 tablets at bedtime.
If the woman has persistent symptoms, a third tablet is added, to be taken in the morning. If symptoms continue, a fourth tablet is recommended to be taken in the afternoon. In a large, randomized clinical trial, doxylamine-pyridoxine treatment reduced nausea, vomiting, and retching and improved perceived quality of life compared with placebo.4 The FDA assigned doxylamine-pyridoxine pregnancy category A because of the extensive evidence that it does not cause an increase in fetal malformations.5,6
If the delayed-release doxylamine-pyridoxine formulation (Diclegis) is not available to the patient, alternative formulations of doxylamine and pyridoxine can be prescribed. Pyridoxine is widely available over the counter as 25-mg tablets, and one tablet can be prescribed two or three times daily. Doxylamine is available as a chewable prescription medicine in 5-mg tablets (Aldex AN) and two tablets can be prescribed two or three times daily. Doxylamine is also available as a 25-mg over-the-counter tablet in Unisom SleepTabs. One-half tablet can be prescribed two or three times daily. The patient should be alerted that Unisom SleepGels contain diphenhydramine, not doxylamine.
Second-line pharmacologic treatment
Metoclopramide Metoclopramide is a dopamine antagonist. It enhances upper gastrointestinal motility, accelerates gastric emptying, and increases lower esophageal sphincter tone. At higher doses it blocks serotonin receptors in the chemoreceptor trigger zone. Its elimination half-life is 5 to 6 hours (Lexicomp). There are no large, randomized, placebo-controlled trials of oral metoclopramide for the treatment of nausea and vomiting of early pregnancy.
I am recommending metoclopramide as a second-line treatment for NVP because it appears to be effective and is not known to be associated with an increased risk of congenital malformations. Metoclopramide is widely used to prevent and treat intraoperative and postoperative nausea associated with cesarean delivery.7 In addition, intravenous (IV) metoclopramide is commonly used to treat women hospitalized with hyperemesis gravidarum. Results of randomized clinical trials demonstrate that when used to treat hyperemesis gravidarum, IV metoclopramide (10 mg every 8 hours) has similar efficacy to IV ondansetron (4 mg every 8 hours)8 and IV promethazine (25 mg every 8 hours).9 When using metoclopramide as an oral treatment for NVP, 10 mg every 8 hours is a commonly recommended regimen.
The FDA has assigned metoclopramide to pregnancy category B, which indicates that there is no evidence of fetal risk. Studies from Israel and Denmark show that metoclopramide is not associated with an increased risk of congenital malformations. In the study from Israel, among 3,458 infants born to women who had filled a prescription for metoclopramide during the first trimester of pregnancy, there was no increase in major congenital malformations, low birth weight, preterm delivery, or perinatal death.10 In the study from Denmark, among 28,486 infants born to mothers who had filled a prescription for metoclopramide in the first trimester there was no increase in congenital malformations or any of 20 individual categories of malformations, including neural tube defects, transposition of the great vessels, ventricular septal defect, atrial septal defect, tetralogy of Fallot, coarctation of the aorta, cleft lip or palate, anorectal atresia/stenosis, or limb reduction.11 The results of these two large studies are reassuring that metoclopramide is not associated with an increased risk of congenital malformations.
Metoclopramide can cause tardive dyskinesia, a serious movement disorder that may be irreversible with discontinuation of the drug. This risk increases with dose and length of treatment. The FDA recommends that clinicians avoid the use of metoclopramide for more than 12 weeks.
Third-line pharmacologic treatment: Ondansetron
In the United States ondansetron is commonly used to treat NVP.12 The drug is a selective 5-HT3 antagonist that blocks serotonin action in the central nervous system chemoreceptor trigger zone. The elimination half-life of ondansetron is 3 to 6 hours (Lexicomp).
The frequent use of ondansetron may be due, in part, to the perception that it is a very effective antiemetic. For example, in one small clinical trial, ondansetron 4 mg every 8 hours was reported to be superior to a combination of pyridoxine 25 mg every 8 hours plus doxylamine 12.5 mg every 8 hours.13 (Note that the pyridoxine and doxylamine tablets used in this trial were not in a combination delayed-release formulation.) I am recommending ondansetron as a third-line treatment for NVP because, although it is effective, it may be associated with an increased risk of fetal cardiac anomalies.
Is ondansetron associated with cardiac malformations?
The FDA has assigned ondansetron to pregnancy category B; however, there is concern that it may be associated with congenital heart defects. In a recent study of 1,349 infants born to Swedish women who had filled a prescription for ondansetron in early pregnancy, a significantly increased risk of cardiovascular defect (odds ratio [OR], 1.62; 95% confidence interval [CI], 1.04−2.14) and cardiac septum defect (OR, 2.05; 95% CI, 1.19−3.28) was reported.14 The cardiac anomalies were mostly atrial septal or ventricular septal defects.
In a second study, reported as an abstract, authors analyzed congenital malformations in 1,248 infants born to Danish women who filled a prescription for ondansetron in early pregnancy. These authors also found an increased risk of a congenital heart malformation (OR, 2.0; 95% CI, 1.3−3.1).15
A US case-control study showed an association between ondansetron use and cleft palate.1 The Swedish14 and Danish15 studies reported above did not find an association between ondansetron use and cleft palate.
The FDA issued a warning in June 2012 that at a dose of 32 mg, administered intravenously, ondansetron may prolong the QT interval and result in a potentially fatal heart arrhythmia, torsades de pointes.16 In the announcement the FDA did not alter the recommendations for oral dosing because there is no strong evidence that oral dosing is associated with clinically significant arrhythmias. Authors of a recent systematic review concluded that IV administration of large doses of ondansetron may cause cardiac arrhythmias, especially in patients with cardiac disease and those taking other drugs that prolong the QT interval, but that a single oral dose of ondansetron does not have a significant risk of causing an arrhythmia.17
Health Canada18 has advised that many commonly prescribed medications increase serotonin activity. When multiple drugs that each increase serotonin activity are prescribed in combination, the risk of serotonin syndrome is increased. Serotonin syndrome results in hyperthermia, agitation, tachycardia, and muscle twitching and can be fatal. Ondansetron was specifically mentioned in the Health Canada warning, but a search of the literature revealed very few reported cases of ondansetron being implicated in the serotonin syndrome.19
My bottom-line recommendations
NVP is a common obstetric problem. When oral pharmacologic therapy is indicated, first-line treatment should be with the FDA-approved combination of doxylamine-pyridoxine because it is both effective and associated with no known increased risk of congenital malformations. An effective second-line agent is metoclopramide. Based on very limited data, metoclopramide appears effective and is not associated with an increased risk of congenital malformations. However, it is not FDA approved for treatment of NVP. Ondansetron appears to be effective but its use in early pregnancy may be associated with congenital anomalies. Consequently, ondansetron should not be used to treat NVP unless first- and second-line treatments have been ineffective to treat the patient’s symptoms.
INSTANT POLL
Which of the following pharmacologic treatments of nausea with or without vomiting during pregnancy is your first-line medication choice?
• Ondansetron
• Metoclopramide
• Doxylamine-pyridoxine
• Meclizine Promethazine
• Trimethobenzamide
Visit the Quick Poll on the homepage, give your answer, and then see how other ObGyns have answered.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Anderka M, Mitchell AA, Louik C, Werler MMA, Hernandez-Diaz S, Rasmussen SA; National Birth Defects Prevention Study. Medications used to treat nausea and vomiting of pregnancy and the risk of selected birth defects. Birth Defects Res A Clin Mol Teratol. 2012;94(1):22–30.
2. Matthews A, Haas Dm, O’Mathuna DP, Dowswell T, Doyle M. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2014;(3):CD007575.
3. Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA. Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstet Gynecol. 2005;105(4):849–856.
4. Koren G, Clark S, Hankins GD, et al. Effectiveness of delayed-release doxylamine and pyridoxine for nausea and vomiting of pregnancy: a randomized placebo controlled trial. Am J Obstet Gynecol. 2010;203(6):571.e1–7.
5. Einarson TR, Leeder JS, Koren G. A method for meta-analysis of epidemiologic studies. Drug Intell Clin Pharm. 1988;22(10):813–824.
6. McKeigue PM, Lamm SH, Linn S, Kutcher JS. Bendectin and birth defects. I. A meta-analysis of the epidemiologic studies. Teratology. 1994;50(1):27–37.
7. Mishriky BM, Habib AS. Metoclopramide for nausea and vomiting prophylaxis during and after cesarean delivery: a systematic review and meta-analysis. Br J Anaesth. 2012;108(3):374–383.
8. Abas MN, Tan PC, Azmi N, Omar SZ. Ondansetron compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2014;123(6):1272–1279.
9. Tan PC, Khine PP, Vallikkannu N, Omar SZ. Promethazine compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2010;115(5):975–981.
10. Matok I, Gorodischer R, Koren G, Sheiner E, Wiznitzer A, Levy A. The safety of metoclopramide use in the first trimester of pregnancy. N Engl J Med. 2009;360(24):2528–2535.
11. Pasternak B, Svanstrom H, Molgaard-Nielsen D, Melbye M, Hviid A. Metoclopramide in pregnancy and risk of major congenital malformations and fetal death. JAMA. 2013;310(15):1601–1611.
12. Koren G. Treating morning sickness in the United States—changes in prescribing are needed. Am J Obstet Gynecol. 2014;211(6):602–606.
13. Oliveira LG, Capp SM, You WB, Riffenburgh RH, Carstairs SH. Ondansetron compared with doxylamine and pyridoxine for treatment of nausea in pregnancy : a randomized controlled trial. Obstet Gynecol. 2014;124(4):735–742.
14. Danielsson B, Wikner BN, Kallen B. Use of ondansetron during pregnancy and congenital malformations in the infant. Reprod Toxicol. 2014;50:134–137.
15. Andersen JT, Jimenez-Solem E, Andersen NL, Poulsen HE. Ondansetron use in early pregnancy and the risk of congenital malformations—a registry based nationwide cohort study. Abstract presented at: 29th International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 25–28, 2013; Montreal, Canada. Abstract 25, Pregnancy Session 1. Pharmacoepidemiol Drug Saf. 2013;22(suppl 1):13–14.
16. US Food and Drug Administration. Ondansetron (Zofran) IV: drug safety communication - QT prolongation. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm310219.htm. Published June 29, 2012. Accessed December 26, 2014.
17. Freedman SB, Uleryk E, Rumantir M, Finkelstein Y. Ondansetron and the risk of cardiac arrhythmias: a systematic review and postmarketing analysis. Ann Emerg Med. 2014;64(1):19–25.
18. Health Canada. Canadian Adverse Reaction Newsletter. 2003;13(3). http://www.hc-sc.gc.ca/dhp-mps/medeff/bulletin/carn-bcei_v13n3-eng.php. Published June 24, 2003. Accessed December 26, 2014.
19. Turkel SB, Nadala JG, Wincor MZ. Possible serotonin syndrome in association with 5-HT3 antagonist agents. Psychosomatics. 2001;42(3):258–260.
1. Anderka M, Mitchell AA, Louik C, Werler MMA, Hernandez-Diaz S, Rasmussen SA; National Birth Defects Prevention Study. Medications used to treat nausea and vomiting of pregnancy and the risk of selected birth defects. Birth Defects Res A Clin Mol Teratol. 2012;94(1):22–30.
2. Matthews A, Haas Dm, O’Mathuna DP, Dowswell T, Doyle M. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2014;(3):CD007575.
3. Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA. Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstet Gynecol. 2005;105(4):849–856.
4. Koren G, Clark S, Hankins GD, et al. Effectiveness of delayed-release doxylamine and pyridoxine for nausea and vomiting of pregnancy: a randomized placebo controlled trial. Am J Obstet Gynecol. 2010;203(6):571.e1–7.
5. Einarson TR, Leeder JS, Koren G. A method for meta-analysis of epidemiologic studies. Drug Intell Clin Pharm. 1988;22(10):813–824.
6. McKeigue PM, Lamm SH, Linn S, Kutcher JS. Bendectin and birth defects. I. A meta-analysis of the epidemiologic studies. Teratology. 1994;50(1):27–37.
7. Mishriky BM, Habib AS. Metoclopramide for nausea and vomiting prophylaxis during and after cesarean delivery: a systematic review and meta-analysis. Br J Anaesth. 2012;108(3):374–383.
8. Abas MN, Tan PC, Azmi N, Omar SZ. Ondansetron compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2014;123(6):1272–1279.
9. Tan PC, Khine PP, Vallikkannu N, Omar SZ. Promethazine compared with metoclopramide for hyperemesis gravidarum: a randomized controlled trial. Obstet Gynecol. 2010;115(5):975–981.
10. Matok I, Gorodischer R, Koren G, Sheiner E, Wiznitzer A, Levy A. The safety of metoclopramide use in the first trimester of pregnancy. N Engl J Med. 2009;360(24):2528–2535.
11. Pasternak B, Svanstrom H, Molgaard-Nielsen D, Melbye M, Hviid A. Metoclopramide in pregnancy and risk of major congenital malformations and fetal death. JAMA. 2013;310(15):1601–1611.
12. Koren G. Treating morning sickness in the United States—changes in prescribing are needed. Am J Obstet Gynecol. 2014;211(6):602–606.
13. Oliveira LG, Capp SM, You WB, Riffenburgh RH, Carstairs SH. Ondansetron compared with doxylamine and pyridoxine for treatment of nausea in pregnancy : a randomized controlled trial. Obstet Gynecol. 2014;124(4):735–742.
14. Danielsson B, Wikner BN, Kallen B. Use of ondansetron during pregnancy and congenital malformations in the infant. Reprod Toxicol. 2014;50:134–137.
15. Andersen JT, Jimenez-Solem E, Andersen NL, Poulsen HE. Ondansetron use in early pregnancy and the risk of congenital malformations—a registry based nationwide cohort study. Abstract presented at: 29th International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 25–28, 2013; Montreal, Canada. Abstract 25, Pregnancy Session 1. Pharmacoepidemiol Drug Saf. 2013;22(suppl 1):13–14.
16. US Food and Drug Administration. Ondansetron (Zofran) IV: drug safety communication - QT prolongation. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm310219.htm. Published June 29, 2012. Accessed December 26, 2014.
17. Freedman SB, Uleryk E, Rumantir M, Finkelstein Y. Ondansetron and the risk of cardiac arrhythmias: a systematic review and postmarketing analysis. Ann Emerg Med. 2014;64(1):19–25.
18. Health Canada. Canadian Adverse Reaction Newsletter. 2003;13(3). http://www.hc-sc.gc.ca/dhp-mps/medeff/bulletin/carn-bcei_v13n3-eng.php. Published June 24, 2003. Accessed December 26, 2014.
19. Turkel SB, Nadala JG, Wincor MZ. Possible serotonin syndrome in association with 5-HT3 antagonist agents. Psychosomatics. 2001;42(3):258–260.

10 Recent paradigm shifts in the neurobiology and treatment of depression
Nowhere is that change in landscape more apparent than in major depression, the No. 1 disabling condition in all of medicine, according to the World Health Organization. The past decade has generated at least 10 paradigm shifts in the neurobiology and pharmacotherapeutics of depression.
Clinging to simplistic tradition
Most contemporary clinicians continue to practice the traditional model of depression, which is based on the assumption that depression is caused by a deficiency of monoamines: serotonin (5-HT) and norepinephrine (NE). The entire antidepressant armamentarium approved for use by the FDA was designed according to the amine deficiency hypothesis. Depressed patients uniformly receive reuptake inhibitors of 5-HT and NE, but few achieve full remission, as the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study showed.1
As scientific paradigm shifts infiltrate clinical practice, however, the tired notion of “chemical imbalance” will yield to more complex and evidence-based models.
Usually, it would be remarkable to witness a single paradigm shift in the understanding of a brain disorder. Imagine the disruptive impact of multiple scientific shifts within the past decade! Consider the following departures from the old dogma about the simplistic old explanation of depression.
1. From neurotransmitters to neuroplasticity
For half a century, our field tenaciously held to the monoamine theory, which posits that depression is caused by a deficiency of 5-HT or NE, or both. All antidepressants in use today were developed to increase brain monoamines by inhibiting their reuptake at the synaptic cleft. Now, research points to other causes:
• impaired neuroplasticity
• a decrement of neurogenesis
• synaptic deficits
• decreased neurotrophins (such as brain-derived neurotrophic factor)
• dendritic pathology.2,3
2. From ‘chemical imbalance’ to neuroinflammation
The simplistic notion that depression is a chemical imbalance, so to speak, in the brain is giving way to rapidly emerging evidence that depression is associated with neuroinflammation.4
Pro-inflammatory cytokines are elevated in the plasma of depressed patients, and subside when the acute episode is treated. Current antidepressants actually have anti-inflammatory effects that have gone unrecognized.5 A meta-analysis of the use of anti-inflammatory agents (such as nonsteroidal anti-inflammatory drugs and aspirin) in depression shows promising efficacy.6 Some inflammatory markers, such as C-reactive protein, already have been reported to predict response to some antidepressants, but not to others.7
3. From 5-HT and NE pathways to glutamate NMDA receptors
Recent landmark studies8 have, taken together, demonstrated that a single IV dose of the N-methyl-d-aspartate (NMDA) receptor antagonist ketamine (a psychotogenic drug of abuse FDA-approved only as an anesthetic) can produce clinical improvement of severe depression and even full remission for several days. Such studies demonstrate that the old dogma of 5-HT and NE deficiency might not be a valid overarching hypothesis of the depression syndrome.
Long-term maintenance studies of ketamine to document its safety and continued efficacy need to be conducted. The mechanism of action of ketamine is believed to be a rapid trigger for enhancing neuroplasticity.
4. From oral to parenteral administration
Several studies have been published showing the efficacy of IV or intranasal administration of new agents for depression. Ketamine studies, for example, were conducted using an IV infusion of a 150-mg dose over 1 hour. Other IV studies used the anticholinergic scopolamine.9
Intranasal ketamine also has been shown to be clinically efficacious.10 Inhalable nitrous oxide (laughing gas, an NMDA antagonist) recently was reported to improve depression as well.11
It is possible that parenteral administration of antidepressant agents may exert a different neurobiological effect and provide a more rapid response than oral medication.
5. From delayed efficacy (weeks) to immediate onset (1 or 2 hours)
The widely entrenched notion that depression takes several weeks to improve with an antidepressant has collapsed with emerging evidence that symptoms of the disorder (even suicidal ideation) can be reversed within 1 or 2 hours.12 IV ketamine isn’t the only example; IV scopolamine,9 inhalable nitrous oxide,11 and overnight sleep deprivation13 also exert a rapid therapeutic effect. This is a major rethinking of how quickly the curtain of severe depression can be lifted, and is great news for patients and their family.
6. From psychological symptoms to cortical or subcortical changes
Depression traditionally has been recognized as a clinical syndrome of sadness, self-deprecation, cognitive dulling, and vegetative symptoms. In recent studies, however, researchers report that low hippocampus volume14 in healthy young girls predicts future depression. Patients with unremitting depression have been reported to have an abnormally shaped hippocampus.15
In addition, gray-matter volume in the subgenual anterior cingulate (Brodmann area 24) is hypoplastic in depressed persons,16 making that area a target for deep-brain stimulation (DBS). Brain morphological changes such as a hypoplastic hippocampus might become useful biomarkers for identifying persons at risk of severe depression, and might become a useful adjunctive biomarker for making a clinical diagnosis.
7. From healing the mind to repairing the brain
It is well-established that depression is associated with loss of dendritic spines and arborizations, loss of synapses, and diminishment of glial cells, especially in the hippocampus17 and anterior cingulate.18 Treating depression, whether pharmaceutical or somatic, involves reversing these changes by increasing neurotrophic factors, enhancing neurogenesis and gliogenesis, and restoring synaptic and dendritic health and cell survival in the hippocampus and frontal cortex.19,20 Treating depression involves brain repair, which is reflected, ultimately, in healing the mind.
8. From pharmacotherapy to neuromodulation
Although drugs remain the predominant treatment modality for depression, there is palpable escalation in the use of neuromodulation methods.
The oldest of these neuromodulatory techniques is electroconvulsive therapy, an excellent treatment for severe depression (and one that enhances hippocampal neurogenesis). In addition, several novel neuromodulation methods have been approved (transcranial magnetic stimulation and vagus nerve stimulation) or are in development (transcranial direct-current stimulation, cranial electrotherapy stimulation, and DBS).21 These somatic approaches to treating the brain directly to alleviate depression target regions involved in depression and reduce the needless risks associated with exposing other organ systems to a drug.
9. From monotherapy to combination therapy
The use of combination therapy for depression has escalated with FDA approval of adjunctive use of atypical antipsychotics in unipolar and bipolar depression. In addition, the landmark STAR*D study1 demonstrated the value of augmentation therapy with a second antidepressant when 1 agent fails. Other controlled studies have shown that combining 2 antidepressants is superior to administering 1.22
Just as other serious medical disorders—such as cancer and hypertension—are treated with 2 or 3 medications, severe depression might require a similar strategy. The field gradually is adopting that approach.
10. From cortical folds to wrinkles on the face
Last, a new (and unexpected) paradigm shift recently emerged, which is genuinely intriguing—even baffling. Using placebo-controlled designs, several researchers have reported significant, persistent improvement of depressive symptoms after injection of onabotulinumtoxinA in the corrugator muscles of the glabellar region of the face, where the omega sign often appears in a depressed person.23,24
The longest of the studies25 was 6 months; investigators reported that improvement continued even after the effect of the botulinum toxin on the omega sign wore off. The proposed mechanism of action is the facial feedback hypothesis, which suggests that, biologically, facial expression has an impact on one’s emotional state.
Big payoffs coming from research in neuroscience
These 10 paradigm shifts in a single psychiatric syndrome are emblematic of exciting clinical and research advances in our field. Like all syndromes, depression is associated with multiple genetic and environmental causes; it isn’t surprising that myriad treatment approaches are emerging.
The days of clinging to monolithic, serendipity-generated models surely are over. Evidence-based psychiatric brain research is shattering aging dogmas that have, for decades, stifled innovation in psychiatric therapeutics that is now moving in novel directions.
Take note, however, that the only paradigm shift that matters to depressed patients is the one that transcends mere control of their symptoms and restores their wellness, functional capacity, and quality of life. With the explosive momentum of neuroscience discovery, psychiatry is, at last, poised to deliver—in splendid, even seismic, fashion.
1. Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Eng J Med. 2006;354(12):1243-1252.
2. Serafini G, Hayley S, Pompili M, et al. Hippocampal neurogenesis, neurotrophic factors and depression: possible therapeutic targets [published online November 30, 2014]? CNS Neurol Disord Drug Targets. doi: 10.2174/1871527313666141130223723.
3. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: potential therapeutic targets. Science. 2012;338(6103):68-72.
4. Iwata M, Ota KT, Duman RS. The inflammasome: pathways linking psychological stress, depression, and systemic illnesses. Brain Behav Immun. 2013;31:105-114.
5. Sacre S, Medghalichi M, Gregory B, et al. Fluoxetine and citalopram exhibit potent anti-inflammatory activity in human and murine models of rheumatoid arthritis and inhibit toll-like receptors. Arthritis Rheum. 2010;62(3):683-693.
6. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
7. Uher R, Tansey KE, Dew T, et al. An inflammatory biomarker as a differential predictor of outcome of depression treatment with escitalopram and nortiptyline. Am J Psychiatry. 2014;171(14):1278-1286.
8. Abdallah CG, Sanacora G, Duman RS, et al. Ketamine and rapid-acting antidepressants: a window into a new neurobiology for mood disorder therapeutics [published online October 17, 2014]. Annual Rev Med. doi: 10.1146/annurev-med-053013-062946.
9. Furey ML, Khanna A, Hoffman EM, et al. Scopolamine produces larger antidepressant and antianxiety effects in women than in men. Neuropsychopharmacology. 2010;35(12):2479-2488.
10. Lapidus KA, Levitch CF, Perez AM, et al. A randomized controlled trial of intranasal ketamine in major depressive disorder. Biol Psychiatry. 2014; 76(12):970-976.
11. Nagele P, Duma A, Kopec M, et al. Nitrous oxide for treatment-resistant major depression: a proof-of-concept trial [published December 14, 2014]. Biol Psychiatry. doi: http://dx.doi.org/10.1016/j.biopsych.2014.11.016.
12. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
13. Bunney BG, Bunney WE. Mechanisms of rapid antidepressant effects of sleep deprivation therapy: clock genes and circadian rhythms. Biol Psychiatry. 2013;73(12):1164-1171.
14. Chen MC, Hamilton JP, Gotlib IH. Decreased hippocampal volume in healthy girls at risk for depression. Arch Gen Psychiatry. 2010;67(3):270-276.
15. Tae WS, Kim SS, Lee KU, et al. Hippocampal shape deformation in female patients with unremitting major depressive disorder. AJNR Am J Neuroradiol. 2011;32(4):671-676.
16. Hamani C, Mayberg H, Synder B, et al. Deep brain stimulation of the subcallosal cingulate gyrus for depression: anatomical location of active contacts in clinical responders and a suggested guideline for targeting. J Neurosurg. 2009;111(6):1209-1215.
17. Sheline YI, Gado MH, Kraemer HC. Untreated depression and hippocampal volume loss. Am J Psychiatry. 2003;160(8):1516-1518.
18. Redlich R, Almeoda JJ, Grotegerd D, et al. Brain morphometric biomarkers distinguishing unipolar and bipolar depression. A voxel-based morphometry-pattern classification approach. JAMA Psychiatry. 2014;71(11):1222-1230.
19. Mendez-David I, Hen R, Gardier AM, et al. Adult hippocampal neurogenesis: an actor in the antidepressant-like action. Ann Pharm Fr. 2013;71(3):143-149.
20. Serafini G. Neuroplasticity and major depression, the role of modern antidepressant drugs. World J Psychiatry. 2012;2(3):49-57.
21. Rosa MA, Lisanby SH. Somatic treatments for mood disorders. Neuropsychopharmacology. 2012;37(1):102-116.
22. Blier P, Ward HE, Tremblay P, et al. Combination of antidepressant medications from treatment initiation for major depressive disorder: a double-blind randomized study. Am J Psychiatry. 2010;167(3):281-288.
23. Wollmer MA, de Boer C, Kalak N, et al. Facing depression with botulinum toxin: a randomized controlled trial. J Psychiatr Res. 2012;46(5):574-581.
24. Finzi E, Rosenthal NE. Treatment of depression with onabotulinumtoxinA: a randomized, double-blind, placebo controlled trial. J Psychiatr Res. 2014;52:1-6.
25. Magid M, Reichenberg JS, Poth PE, et al. Treatment of major depressive disorder using botulinum toxin A: a 24-week randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2014;75(8):837-844.
Nowhere is that change in landscape more apparent than in major depression, the No. 1 disabling condition in all of medicine, according to the World Health Organization. The past decade has generated at least 10 paradigm shifts in the neurobiology and pharmacotherapeutics of depression.
Clinging to simplistic tradition
Most contemporary clinicians continue to practice the traditional model of depression, which is based on the assumption that depression is caused by a deficiency of monoamines: serotonin (5-HT) and norepinephrine (NE). The entire antidepressant armamentarium approved for use by the FDA was designed according to the amine deficiency hypothesis. Depressed patients uniformly receive reuptake inhibitors of 5-HT and NE, but few achieve full remission, as the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study showed.1
As scientific paradigm shifts infiltrate clinical practice, however, the tired notion of “chemical imbalance” will yield to more complex and evidence-based models.
Usually, it would be remarkable to witness a single paradigm shift in the understanding of a brain disorder. Imagine the disruptive impact of multiple scientific shifts within the past decade! Consider the following departures from the old dogma about the simplistic old explanation of depression.
1. From neurotransmitters to neuroplasticity
For half a century, our field tenaciously held to the monoamine theory, which posits that depression is caused by a deficiency of 5-HT or NE, or both. All antidepressants in use today were developed to increase brain monoamines by inhibiting their reuptake at the synaptic cleft. Now, research points to other causes:
• impaired neuroplasticity
• a decrement of neurogenesis
• synaptic deficits
• decreased neurotrophins (such as brain-derived neurotrophic factor)
• dendritic pathology.2,3
2. From ‘chemical imbalance’ to neuroinflammation
The simplistic notion that depression is a chemical imbalance, so to speak, in the brain is giving way to rapidly emerging evidence that depression is associated with neuroinflammation.4
Pro-inflammatory cytokines are elevated in the plasma of depressed patients, and subside when the acute episode is treated. Current antidepressants actually have anti-inflammatory effects that have gone unrecognized.5 A meta-analysis of the use of anti-inflammatory agents (such as nonsteroidal anti-inflammatory drugs and aspirin) in depression shows promising efficacy.6 Some inflammatory markers, such as C-reactive protein, already have been reported to predict response to some antidepressants, but not to others.7
3. From 5-HT and NE pathways to glutamate NMDA receptors
Recent landmark studies8 have, taken together, demonstrated that a single IV dose of the N-methyl-d-aspartate (NMDA) receptor antagonist ketamine (a psychotogenic drug of abuse FDA-approved only as an anesthetic) can produce clinical improvement of severe depression and even full remission for several days. Such studies demonstrate that the old dogma of 5-HT and NE deficiency might not be a valid overarching hypothesis of the depression syndrome.
Long-term maintenance studies of ketamine to document its safety and continued efficacy need to be conducted. The mechanism of action of ketamine is believed to be a rapid trigger for enhancing neuroplasticity.
4. From oral to parenteral administration
Several studies have been published showing the efficacy of IV or intranasal administration of new agents for depression. Ketamine studies, for example, were conducted using an IV infusion of a 150-mg dose over 1 hour. Other IV studies used the anticholinergic scopolamine.9
Intranasal ketamine also has been shown to be clinically efficacious.10 Inhalable nitrous oxide (laughing gas, an NMDA antagonist) recently was reported to improve depression as well.11
It is possible that parenteral administration of antidepressant agents may exert a different neurobiological effect and provide a more rapid response than oral medication.
5. From delayed efficacy (weeks) to immediate onset (1 or 2 hours)
The widely entrenched notion that depression takes several weeks to improve with an antidepressant has collapsed with emerging evidence that symptoms of the disorder (even suicidal ideation) can be reversed within 1 or 2 hours.12 IV ketamine isn’t the only example; IV scopolamine,9 inhalable nitrous oxide,11 and overnight sleep deprivation13 also exert a rapid therapeutic effect. This is a major rethinking of how quickly the curtain of severe depression can be lifted, and is great news for patients and their family.
6. From psychological symptoms to cortical or subcortical changes
Depression traditionally has been recognized as a clinical syndrome of sadness, self-deprecation, cognitive dulling, and vegetative symptoms. In recent studies, however, researchers report that low hippocampus volume14 in healthy young girls predicts future depression. Patients with unremitting depression have been reported to have an abnormally shaped hippocampus.15
In addition, gray-matter volume in the subgenual anterior cingulate (Brodmann area 24) is hypoplastic in depressed persons,16 making that area a target for deep-brain stimulation (DBS). Brain morphological changes such as a hypoplastic hippocampus might become useful biomarkers for identifying persons at risk of severe depression, and might become a useful adjunctive biomarker for making a clinical diagnosis.
7. From healing the mind to repairing the brain
It is well-established that depression is associated with loss of dendritic spines and arborizations, loss of synapses, and diminishment of glial cells, especially in the hippocampus17 and anterior cingulate.18 Treating depression, whether pharmaceutical or somatic, involves reversing these changes by increasing neurotrophic factors, enhancing neurogenesis and gliogenesis, and restoring synaptic and dendritic health and cell survival in the hippocampus and frontal cortex.19,20 Treating depression involves brain repair, which is reflected, ultimately, in healing the mind.
8. From pharmacotherapy to neuromodulation
Although drugs remain the predominant treatment modality for depression, there is palpable escalation in the use of neuromodulation methods.
The oldest of these neuromodulatory techniques is electroconvulsive therapy, an excellent treatment for severe depression (and one that enhances hippocampal neurogenesis). In addition, several novel neuromodulation methods have been approved (transcranial magnetic stimulation and vagus nerve stimulation) or are in development (transcranial direct-current stimulation, cranial electrotherapy stimulation, and DBS).21 These somatic approaches to treating the brain directly to alleviate depression target regions involved in depression and reduce the needless risks associated with exposing other organ systems to a drug.
9. From monotherapy to combination therapy
The use of combination therapy for depression has escalated with FDA approval of adjunctive use of atypical antipsychotics in unipolar and bipolar depression. In addition, the landmark STAR*D study1 demonstrated the value of augmentation therapy with a second antidepressant when 1 agent fails. Other controlled studies have shown that combining 2 antidepressants is superior to administering 1.22
Just as other serious medical disorders—such as cancer and hypertension—are treated with 2 or 3 medications, severe depression might require a similar strategy. The field gradually is adopting that approach.
10. From cortical folds to wrinkles on the face
Last, a new (and unexpected) paradigm shift recently emerged, which is genuinely intriguing—even baffling. Using placebo-controlled designs, several researchers have reported significant, persistent improvement of depressive symptoms after injection of onabotulinumtoxinA in the corrugator muscles of the glabellar region of the face, where the omega sign often appears in a depressed person.23,24
The longest of the studies25 was 6 months; investigators reported that improvement continued even after the effect of the botulinum toxin on the omega sign wore off. The proposed mechanism of action is the facial feedback hypothesis, which suggests that, biologically, facial expression has an impact on one’s emotional state.
Big payoffs coming from research in neuroscience
These 10 paradigm shifts in a single psychiatric syndrome are emblematic of exciting clinical and research advances in our field. Like all syndromes, depression is associated with multiple genetic and environmental causes; it isn’t surprising that myriad treatment approaches are emerging.
The days of clinging to monolithic, serendipity-generated models surely are over. Evidence-based psychiatric brain research is shattering aging dogmas that have, for decades, stifled innovation in psychiatric therapeutics that is now moving in novel directions.
Take note, however, that the only paradigm shift that matters to depressed patients is the one that transcends mere control of their symptoms and restores their wellness, functional capacity, and quality of life. With the explosive momentum of neuroscience discovery, psychiatry is, at last, poised to deliver—in splendid, even seismic, fashion.
Nowhere is that change in landscape more apparent than in major depression, the No. 1 disabling condition in all of medicine, according to the World Health Organization. The past decade has generated at least 10 paradigm shifts in the neurobiology and pharmacotherapeutics of depression.
Clinging to simplistic tradition
Most contemporary clinicians continue to practice the traditional model of depression, which is based on the assumption that depression is caused by a deficiency of monoamines: serotonin (5-HT) and norepinephrine (NE). The entire antidepressant armamentarium approved for use by the FDA was designed according to the amine deficiency hypothesis. Depressed patients uniformly receive reuptake inhibitors of 5-HT and NE, but few achieve full remission, as the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study showed.1
As scientific paradigm shifts infiltrate clinical practice, however, the tired notion of “chemical imbalance” will yield to more complex and evidence-based models.
Usually, it would be remarkable to witness a single paradigm shift in the understanding of a brain disorder. Imagine the disruptive impact of multiple scientific shifts within the past decade! Consider the following departures from the old dogma about the simplistic old explanation of depression.
1. From neurotransmitters to neuroplasticity
For half a century, our field tenaciously held to the monoamine theory, which posits that depression is caused by a deficiency of 5-HT or NE, or both. All antidepressants in use today were developed to increase brain monoamines by inhibiting their reuptake at the synaptic cleft. Now, research points to other causes:
• impaired neuroplasticity
• a decrement of neurogenesis
• synaptic deficits
• decreased neurotrophins (such as brain-derived neurotrophic factor)
• dendritic pathology.2,3
2. From ‘chemical imbalance’ to neuroinflammation
The simplistic notion that depression is a chemical imbalance, so to speak, in the brain is giving way to rapidly emerging evidence that depression is associated with neuroinflammation.4
Pro-inflammatory cytokines are elevated in the plasma of depressed patients, and subside when the acute episode is treated. Current antidepressants actually have anti-inflammatory effects that have gone unrecognized.5 A meta-analysis of the use of anti-inflammatory agents (such as nonsteroidal anti-inflammatory drugs and aspirin) in depression shows promising efficacy.6 Some inflammatory markers, such as C-reactive protein, already have been reported to predict response to some antidepressants, but not to others.7
3. From 5-HT and NE pathways to glutamate NMDA receptors
Recent landmark studies8 have, taken together, demonstrated that a single IV dose of the N-methyl-d-aspartate (NMDA) receptor antagonist ketamine (a psychotogenic drug of abuse FDA-approved only as an anesthetic) can produce clinical improvement of severe depression and even full remission for several days. Such studies demonstrate that the old dogma of 5-HT and NE deficiency might not be a valid overarching hypothesis of the depression syndrome.
Long-term maintenance studies of ketamine to document its safety and continued efficacy need to be conducted. The mechanism of action of ketamine is believed to be a rapid trigger for enhancing neuroplasticity.
4. From oral to parenteral administration
Several studies have been published showing the efficacy of IV or intranasal administration of new agents for depression. Ketamine studies, for example, were conducted using an IV infusion of a 150-mg dose over 1 hour. Other IV studies used the anticholinergic scopolamine.9
Intranasal ketamine also has been shown to be clinically efficacious.10 Inhalable nitrous oxide (laughing gas, an NMDA antagonist) recently was reported to improve depression as well.11
It is possible that parenteral administration of antidepressant agents may exert a different neurobiological effect and provide a more rapid response than oral medication.
5. From delayed efficacy (weeks) to immediate onset (1 or 2 hours)
The widely entrenched notion that depression takes several weeks to improve with an antidepressant has collapsed with emerging evidence that symptoms of the disorder (even suicidal ideation) can be reversed within 1 or 2 hours.12 IV ketamine isn’t the only example; IV scopolamine,9 inhalable nitrous oxide,11 and overnight sleep deprivation13 also exert a rapid therapeutic effect. This is a major rethinking of how quickly the curtain of severe depression can be lifted, and is great news for patients and their family.
6. From psychological symptoms to cortical or subcortical changes
Depression traditionally has been recognized as a clinical syndrome of sadness, self-deprecation, cognitive dulling, and vegetative symptoms. In recent studies, however, researchers report that low hippocampus volume14 in healthy young girls predicts future depression. Patients with unremitting depression have been reported to have an abnormally shaped hippocampus.15
In addition, gray-matter volume in the subgenual anterior cingulate (Brodmann area 24) is hypoplastic in depressed persons,16 making that area a target for deep-brain stimulation (DBS). Brain morphological changes such as a hypoplastic hippocampus might become useful biomarkers for identifying persons at risk of severe depression, and might become a useful adjunctive biomarker for making a clinical diagnosis.
7. From healing the mind to repairing the brain
It is well-established that depression is associated with loss of dendritic spines and arborizations, loss of synapses, and diminishment of glial cells, especially in the hippocampus17 and anterior cingulate.18 Treating depression, whether pharmaceutical or somatic, involves reversing these changes by increasing neurotrophic factors, enhancing neurogenesis and gliogenesis, and restoring synaptic and dendritic health and cell survival in the hippocampus and frontal cortex.19,20 Treating depression involves brain repair, which is reflected, ultimately, in healing the mind.
8. From pharmacotherapy to neuromodulation
Although drugs remain the predominant treatment modality for depression, there is palpable escalation in the use of neuromodulation methods.
The oldest of these neuromodulatory techniques is electroconvulsive therapy, an excellent treatment for severe depression (and one that enhances hippocampal neurogenesis). In addition, several novel neuromodulation methods have been approved (transcranial magnetic stimulation and vagus nerve stimulation) or are in development (transcranial direct-current stimulation, cranial electrotherapy stimulation, and DBS).21 These somatic approaches to treating the brain directly to alleviate depression target regions involved in depression and reduce the needless risks associated with exposing other organ systems to a drug.
9. From monotherapy to combination therapy
The use of combination therapy for depression has escalated with FDA approval of adjunctive use of atypical antipsychotics in unipolar and bipolar depression. In addition, the landmark STAR*D study1 demonstrated the value of augmentation therapy with a second antidepressant when 1 agent fails. Other controlled studies have shown that combining 2 antidepressants is superior to administering 1.22
Just as other serious medical disorders—such as cancer and hypertension—are treated with 2 or 3 medications, severe depression might require a similar strategy. The field gradually is adopting that approach.
10. From cortical folds to wrinkles on the face
Last, a new (and unexpected) paradigm shift recently emerged, which is genuinely intriguing—even baffling. Using placebo-controlled designs, several researchers have reported significant, persistent improvement of depressive symptoms after injection of onabotulinumtoxinA in the corrugator muscles of the glabellar region of the face, where the omega sign often appears in a depressed person.23,24
The longest of the studies25 was 6 months; investigators reported that improvement continued even after the effect of the botulinum toxin on the omega sign wore off. The proposed mechanism of action is the facial feedback hypothesis, which suggests that, biologically, facial expression has an impact on one’s emotional state.
Big payoffs coming from research in neuroscience
These 10 paradigm shifts in a single psychiatric syndrome are emblematic of exciting clinical and research advances in our field. Like all syndromes, depression is associated with multiple genetic and environmental causes; it isn’t surprising that myriad treatment approaches are emerging.
The days of clinging to monolithic, serendipity-generated models surely are over. Evidence-based psychiatric brain research is shattering aging dogmas that have, for decades, stifled innovation in psychiatric therapeutics that is now moving in novel directions.
Take note, however, that the only paradigm shift that matters to depressed patients is the one that transcends mere control of their symptoms and restores their wellness, functional capacity, and quality of life. With the explosive momentum of neuroscience discovery, psychiatry is, at last, poised to deliver—in splendid, even seismic, fashion.
1. Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Eng J Med. 2006;354(12):1243-1252.
2. Serafini G, Hayley S, Pompili M, et al. Hippocampal neurogenesis, neurotrophic factors and depression: possible therapeutic targets [published online November 30, 2014]? CNS Neurol Disord Drug Targets. doi: 10.2174/1871527313666141130223723.
3. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: potential therapeutic targets. Science. 2012;338(6103):68-72.
4. Iwata M, Ota KT, Duman RS. The inflammasome: pathways linking psychological stress, depression, and systemic illnesses. Brain Behav Immun. 2013;31:105-114.
5. Sacre S, Medghalichi M, Gregory B, et al. Fluoxetine and citalopram exhibit potent anti-inflammatory activity in human and murine models of rheumatoid arthritis and inhibit toll-like receptors. Arthritis Rheum. 2010;62(3):683-693.
6. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
7. Uher R, Tansey KE, Dew T, et al. An inflammatory biomarker as a differential predictor of outcome of depression treatment with escitalopram and nortiptyline. Am J Psychiatry. 2014;171(14):1278-1286.
8. Abdallah CG, Sanacora G, Duman RS, et al. Ketamine and rapid-acting antidepressants: a window into a new neurobiology for mood disorder therapeutics [published online October 17, 2014]. Annual Rev Med. doi: 10.1146/annurev-med-053013-062946.
9. Furey ML, Khanna A, Hoffman EM, et al. Scopolamine produces larger antidepressant and antianxiety effects in women than in men. Neuropsychopharmacology. 2010;35(12):2479-2488.
10. Lapidus KA, Levitch CF, Perez AM, et al. A randomized controlled trial of intranasal ketamine in major depressive disorder. Biol Psychiatry. 2014; 76(12):970-976.
11. Nagele P, Duma A, Kopec M, et al. Nitrous oxide for treatment-resistant major depression: a proof-of-concept trial [published December 14, 2014]. Biol Psychiatry. doi: http://dx.doi.org/10.1016/j.biopsych.2014.11.016.
12. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
13. Bunney BG, Bunney WE. Mechanisms of rapid antidepressant effects of sleep deprivation therapy: clock genes and circadian rhythms. Biol Psychiatry. 2013;73(12):1164-1171.
14. Chen MC, Hamilton JP, Gotlib IH. Decreased hippocampal volume in healthy girls at risk for depression. Arch Gen Psychiatry. 2010;67(3):270-276.
15. Tae WS, Kim SS, Lee KU, et al. Hippocampal shape deformation in female patients with unremitting major depressive disorder. AJNR Am J Neuroradiol. 2011;32(4):671-676.
16. Hamani C, Mayberg H, Synder B, et al. Deep brain stimulation of the subcallosal cingulate gyrus for depression: anatomical location of active contacts in clinical responders and a suggested guideline for targeting. J Neurosurg. 2009;111(6):1209-1215.
17. Sheline YI, Gado MH, Kraemer HC. Untreated depression and hippocampal volume loss. Am J Psychiatry. 2003;160(8):1516-1518.
18. Redlich R, Almeoda JJ, Grotegerd D, et al. Brain morphometric biomarkers distinguishing unipolar and bipolar depression. A voxel-based morphometry-pattern classification approach. JAMA Psychiatry. 2014;71(11):1222-1230.
19. Mendez-David I, Hen R, Gardier AM, et al. Adult hippocampal neurogenesis: an actor in the antidepressant-like action. Ann Pharm Fr. 2013;71(3):143-149.
20. Serafini G. Neuroplasticity and major depression, the role of modern antidepressant drugs. World J Psychiatry. 2012;2(3):49-57.
21. Rosa MA, Lisanby SH. Somatic treatments for mood disorders. Neuropsychopharmacology. 2012;37(1):102-116.
22. Blier P, Ward HE, Tremblay P, et al. Combination of antidepressant medications from treatment initiation for major depressive disorder: a double-blind randomized study. Am J Psychiatry. 2010;167(3):281-288.
23. Wollmer MA, de Boer C, Kalak N, et al. Facing depression with botulinum toxin: a randomized controlled trial. J Psychiatr Res. 2012;46(5):574-581.
24. Finzi E, Rosenthal NE. Treatment of depression with onabotulinumtoxinA: a randomized, double-blind, placebo controlled trial. J Psychiatr Res. 2014;52:1-6.
25. Magid M, Reichenberg JS, Poth PE, et al. Treatment of major depressive disorder using botulinum toxin A: a 24-week randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2014;75(8):837-844.
1. Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Eng J Med. 2006;354(12):1243-1252.
2. Serafini G, Hayley S, Pompili M, et al. Hippocampal neurogenesis, neurotrophic factors and depression: possible therapeutic targets [published online November 30, 2014]? CNS Neurol Disord Drug Targets. doi: 10.2174/1871527313666141130223723.
3. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: potential therapeutic targets. Science. 2012;338(6103):68-72.
4. Iwata M, Ota KT, Duman RS. The inflammasome: pathways linking psychological stress, depression, and systemic illnesses. Brain Behav Immun. 2013;31:105-114.
5. Sacre S, Medghalichi M, Gregory B, et al. Fluoxetine and citalopram exhibit potent anti-inflammatory activity in human and murine models of rheumatoid arthritis and inhibit toll-like receptors. Arthritis Rheum. 2010;62(3):683-693.
6. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
7. Uher R, Tansey KE, Dew T, et al. An inflammatory biomarker as a differential predictor of outcome of depression treatment with escitalopram and nortiptyline. Am J Psychiatry. 2014;171(14):1278-1286.
8. Abdallah CG, Sanacora G, Duman RS, et al. Ketamine and rapid-acting antidepressants: a window into a new neurobiology for mood disorder therapeutics [published online October 17, 2014]. Annual Rev Med. doi: 10.1146/annurev-med-053013-062946.
9. Furey ML, Khanna A, Hoffman EM, et al. Scopolamine produces larger antidepressant and antianxiety effects in women than in men. Neuropsychopharmacology. 2010;35(12):2479-2488.
10. Lapidus KA, Levitch CF, Perez AM, et al. A randomized controlled trial of intranasal ketamine in major depressive disorder. Biol Psychiatry. 2014; 76(12):970-976.
11. Nagele P, Duma A, Kopec M, et al. Nitrous oxide for treatment-resistant major depression: a proof-of-concept trial [published December 14, 2014]. Biol Psychiatry. doi: http://dx.doi.org/10.1016/j.biopsych.2014.11.016.
12. Köhler O, Benros ME, Nordentoft M, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2014;71(12): 1381-1391.
13. Bunney BG, Bunney WE. Mechanisms of rapid antidepressant effects of sleep deprivation therapy: clock genes and circadian rhythms. Biol Psychiatry. 2013;73(12):1164-1171.
14. Chen MC, Hamilton JP, Gotlib IH. Decreased hippocampal volume in healthy girls at risk for depression. Arch Gen Psychiatry. 2010;67(3):270-276.
15. Tae WS, Kim SS, Lee KU, et al. Hippocampal shape deformation in female patients with unremitting major depressive disorder. AJNR Am J Neuroradiol. 2011;32(4):671-676.
16. Hamani C, Mayberg H, Synder B, et al. Deep brain stimulation of the subcallosal cingulate gyrus for depression: anatomical location of active contacts in clinical responders and a suggested guideline for targeting. J Neurosurg. 2009;111(6):1209-1215.
17. Sheline YI, Gado MH, Kraemer HC. Untreated depression and hippocampal volume loss. Am J Psychiatry. 2003;160(8):1516-1518.
18. Redlich R, Almeoda JJ, Grotegerd D, et al. Brain morphometric biomarkers distinguishing unipolar and bipolar depression. A voxel-based morphometry-pattern classification approach. JAMA Psychiatry. 2014;71(11):1222-1230.
19. Mendez-David I, Hen R, Gardier AM, et al. Adult hippocampal neurogenesis: an actor in the antidepressant-like action. Ann Pharm Fr. 2013;71(3):143-149.
20. Serafini G. Neuroplasticity and major depression, the role of modern antidepressant drugs. World J Psychiatry. 2012;2(3):49-57.
21. Rosa MA, Lisanby SH. Somatic treatments for mood disorders. Neuropsychopharmacology. 2012;37(1):102-116.
22. Blier P, Ward HE, Tremblay P, et al. Combination of antidepressant medications from treatment initiation for major depressive disorder: a double-blind randomized study. Am J Psychiatry. 2010;167(3):281-288.
23. Wollmer MA, de Boer C, Kalak N, et al. Facing depression with botulinum toxin: a randomized controlled trial. J Psychiatr Res. 2012;46(5):574-581.
24. Finzi E, Rosenthal NE. Treatment of depression with onabotulinumtoxinA: a randomized, double-blind, placebo controlled trial. J Psychiatr Res. 2014;52:1-6.
25. Magid M, Reichenberg JS, Poth PE, et al. Treatment of major depressive disorder using botulinum toxin A: a 24-week randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2014;75(8):837-844.
Dying in America: implications for oncology of the recent IOM report
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Stop using the hCG discriminatory zone of 1,500 to 2,000 mIU/mL to guide intervention during early pregnancy
Approximately 15% of early pregnancies are complicated by pelvic or abdominal pain and uterine bleeding or spotting. In these situations, you must determine whether your patient has a viable intrauterine pregnancy, a pregnancy that will end in a miscarriage (spontaneous abortion), or an ectopic pregnancy.
To guide you to the correct diagnosis, a medical history and physical examination can be helpful. For example, a woman with a prior ectopic pregnancy who now has an early pregnancy complicated by pelvic pain and uterine bleeding is at high risk for an ectopic pregnancy. Physical examination also is important; if the pelvic examination reveals a dilated cervix with pregnancy tissue in the cervical os it is likely that a miscarriage is in progress. For most cases of early pregnancy complicated by pelvic pain and/or uterine bleeding, however, a pelvic sonogram and serial quantitative measurement of human chorionic gonadotropin (hCG) are needed to achieve the correct diagnosis.
Here I outline the clinical markers for transvaginal ultrasonography that indicate a viable or failed intrauterine pregnancy as well as an ectopic pregnancy. I also present data on single vs serial hCG measurement and discuss serial hCG levels that indicate viable or nonviable intrauterine or ectopic pregnancy.
Is an early gestation viable? Clinical evaluationTransvaginal pelvic ultrasoundTransvaginal and transabdominal ultrasonography play a critical role in evaluating early pregnancy problems. In a normal pregnancy, key developmental milestones that can be observed reliably on ultrasound are1,2:
- intrauterine gestational sac at 5 weeks
- yolk sac at 5.5 weeks
- embryonic pole and fetal heart beat at 6 to 6.5 weeks’ gestation.
A pelvic ultrasound also may provide evidence that an intrauterine pregnancy will fail and result in a miscarriage. Findings diagnostic of a failed intrauterine pregnancy include3:
- crown-rump length ≥7 mm and no fetal heartbeat
- mean sac diameter ≥25 mm and no embryo
- absence of an embryo with a heartbeat more than 2 weeks after an ultrasound scan that showed a gestational sac without a yolk sac
- absence of an embryo with a heartbeat more than 11 days after a scan that showed a gestational sac with a yolk sac.
Findings suspicious for a failing intrauterine pregnancy include3:
- crown-rump length <7 mm and no fetal heartbeat
- mean sac diameter of 16 to 24 mm and no embryo
- no heartbeat 7 to 13 days after an ultrasound scan that showed a gestational sac without a yolk sac
- no heartbeat 7 to 10 days after an ultrasound scan that showed a gestational sac with a yolk sac.
When it’s an ectopic pregnancy. Definitive ultrasonographic evidence of an ectopic pregnancy is identification of a fetal heartbeat outside the uterus or a gestational sac and yolk sac outside of the uterus. An adnexal mass can be identified on ultrasonography in most cases of ectopic pregnancy. In one study of 291 ectopic pregnancies, an adnexal mass was identified in 94% of cases, and a moderate to large amount of free pelvic fluid was found in 36% of cases.4 The adnexal masses included nonspecific (54% of all ectopic cases), a tubal ring without a yolk sac or embryo (25%), a yolk sac but no embryonic heartbeat (8%), and an embryo with cardiac activity (7%).
In clinical units with high-quality gynecologic ultrasonography available, most ectopic pregnancies will be detected on initial scan and only 10% to 15% of ectopic pregnancies will have an ultrasound finding of no intrauterine pregnancy and no evidence for an extrauterine pregnancy.5

Almost all (in the range of 99%) viable intrauterine pregnancies demonstrate an increase in hCG level of 53% or more over 48 hours, whereas only 21% of ectopic pregnancies demonstrate a rise of 53% or more.7
Most pregnancies that will end in a miscarriage demonstrate a decrease in hCG level over 48 hours. If the initial hCG value is 2,000 mIU/mL, 90% of pregnancies that will end in miscarriage will have an approximate 30% decrease in hCG over 48 hours. If the initial hCG is 1,000 mIU/mL, 95% of spontaneous abortions will have a 28% decline in 48 hours.7 About 10% of ectopic pregnancies also will demonstrate a 30% decrease in hCG over 48 hours.
A minor disadvantage of serial hCG measurements is that patients may become anxious and fearful as they await the result of life-altering test results.
When a gestation is found to be nonviable A viable intrauterine pregnancy is highly unlikely in a woman with no ultrasound evidence of an intrauterine pregnancy or an adnexal mass and an hCG level that rises very little, plateaus, or decreases over 48 hours. In this situation, a Karman cannula aspiration of uterine contents with rush pathology analysis can help clarify the likely diagnosis and guide therapy.
Women with documented villi on pathology likely are experiencing a miscarriage and can have their hCG level followed to resolution. Women with no documented villi and no decrease in hCG after the Karman
cannula aspiration can be presumed to have an ectopic pregnancy. If stable, these women may be candidates for treatment with methotrexate.8,9
Many experts have counseled against the use of a single hCG measurement in the discriminatory zone of 1,500 to 2,000 mIU/mL to trigger methotrexate treatment. Here is a sampling of their advice:
“An hCG level of 2,000 mIU/mL, without ultrasound findings of intrauterine pregnancy, while suggestive of abnormal pregnancy, is not diagnostic. Per the results of recent studies, it is reasonable to closely follow up rather than treat many of these early, stable cases of ectopic pregnancy.”
—Mehta et al.1
“Our data demonstrate that using a single value of serum hCG in a pregnancy of unknown location (PUL) population is of limited value.... A significant proportion of failing PULs and early intrauterine pregnancies in a PUL population have high serum hCG levels at presentation.”
—Condus et al.2
“The hCG discriminatory level should not be used to determine the management of a hemodynamically stable patient with suspected ectopic pregnancy, if sonography demonstrates no findings of intrauterine or ectopic pregnancy.”
—Doubilet et al.3
“There is almost no reason to give methotrexate on first encounter with a patient. If a patient is symptomatic with severe pain or signs of rupture, a surgical approach is indicated and methotrexate is contraindicated.”
—Barnhart et al.4
[When using the discriminatory zone]... “there is a chance of harming a viable intrauterine pregnancy, especially if the hCG level is 2000 to 3000 mIU/mL.... There is limited risk in taking a few extra days to make a definitive diagnosis in a woman with a pregnancy of unknown location who has no signs or symptoms of rupture and no ultrasonographic evidence of ectopic pregnancy.”
—Doubliet et al.3
“Viable intrauterine pregnancy is possible in patients with pregnancy of unknown location and hCG levels above the generally accept discriminatory zone, strict adherence to which can potentially disrupt a normal pregnancy. We support the need for judicious use of the hCG discriminatory level in hemodynamically stable patients with pregnancy of unknown location, and the decision to intervene should not be based solely on a single hCG level.”
—Ko and Cheung.5
References
- Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.
- Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
- Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
- Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
Stop using the discriminatory zone and a single hCG measurement to trigger clinical intervention As noted above, a single hCG measurement is of very little value in determining whether an early pregnancy is a viable or nonviable intrauterine pregnancy or is ectopic. Many experts have reported that if a single hCG measurement shows a value of more than 1,500 mIU/mL and a pelvic ultrasound shows no intrauterine pregnancy, an ectopic or nonviable intrauterine pregnancy is likely. Some experts have used the presence of an hCG value of more than 1,500 mIU/mL plus an ultrasound scan without evidence of an intrauterine pregnancy to clinically diagnose the absence of a viable intrauterine pregnancy and administer methotrexate to treat a presumptive ectopic pregnancy. Many experts believe, however, that this approach will necessarily result in the treatment of viable intrauterine pregnancies with methotrexate.5,10
Based on one analysis, for 100 women with an initial hCG value between 2,000 and 3,000 mIU/mL and no intrauterine pregnancy or adnexal mass seen on ultrasound, follow-up will reveal that 65.5% had a failed intrauterine pregnancy, 33% had an ectopic pregnancy, and 1.5% had a viable intrauterine pregnancy.3,10,11 If all of these 100 women had been treated with methotrexate for a presumed ectopic pregnancy, approximately two women with a viable intrauterine pregnancy would have been exposed to methotrexate. This exposure would likely result in either a pregnancy loss or, if the pregnancy continues, an increased risk of fetal anomalies.
If the patient is obese, has fibroids, or has adenomyosis, she has an increased risk of an ultrasound failing to detect an early intrauterine pregnancy when the hCG value ranges from 1,500 to 3,000 mIU/mL.12 If the discriminatory zone is raised to 4,000 mIU/mL, the likelihood of mistakenly diagnosing a viable intrauterine pregnancy as a failed or ectopic pregnancy is much less (but not zero).
There is almost no clinical situation in which methotrexate should be given to a patient suspected of having an ectopic pregnancy on the first visit, unless ultrasound demonstrates an adnexal mass indicative of ectopic pregnancy.13,14 If the patient has severe pain or bleeding, or has signs consistent with a ruptured ectopic pregnancy, surgical intervention likely is warranted. If the patient is clinically stable, a safe option is to repeat the hCG measurement in 48 hours, with an ultrasound if indicated.
The discriminatory zone is an interesting and elegant idea. But in practice it is fraught with serious dangers, the greatest of which is methotrexate administration to a patient with a viable intrauterine gestation. My advice is that gynecologists should stop relying on a discriminatory zone of 1,500 to 2,000 mIU/mL to trigger clinical intervention.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Bree RL, Edwards M, Böhm-Vélez M, et al. Transvaginal sonography in the evaluation of normal early pregnancy: correlation with hCG level. AJR Am J Roentgenol. 1989;153(1):75–79.
2. Goldstein I, Zimmer EA, Tamir A, Peretz BA, Paldi E. Evaluation of normal gestational sac growth: appearance of embryonic heartbeat and embryo body movements using the transvaginal technique. Obstet Gynecol. 1991;77(6):885–888.
3. Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
4. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
5. Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
6. Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361(4):379–387.
7. Silva C, Sammel MD, Zhou L, et al. Human chorionic gonadotropin profile for women with ectopic pregnancy. Obstet Gynecol. 2006;107(3):605–610.
8. Shaunik A, Kulp J, Appleby DH, Sammel MD, Barnhart KT. Utility of dilation and curettage in the diagnosis of pregnancy of unknown location. Am J Obstet Gynecol. 2011;204(2):130.e1–6.
9. Brady P, Imudia AN, Awonuga AO, Wright DL, Syter AK, Toth TL. Pregnancies of unknown location after in vitro fertilization: minimally invasive management with Karman cannula aspiration. Fertil Steril. 2014;101(2):420–426.
10. Doubilet PM, Benson CB. Further evidence against the reliability of the human chorionic discriminatory level. J Ultrasound Med. 2011;30(12):1637–1642.
11. Benson CB, Doubilet PM, Peters HE, Frates MC. Intrauterine fluid with ectopic pregnancy: a reappraisal. J Ultrasound Med. 2013;32(3):389–393.
12. Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
13. Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
14. Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.

Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Approximately 15% of early pregnancies are complicated by pelvic or abdominal pain and uterine bleeding or spotting. In these situations, you must determine whether your patient has a viable intrauterine pregnancy, a pregnancy that will end in a miscarriage (spontaneous abortion), or an ectopic pregnancy.
To guide you to the correct diagnosis, a medical history and physical examination can be helpful. For example, a woman with a prior ectopic pregnancy who now has an early pregnancy complicated by pelvic pain and uterine bleeding is at high risk for an ectopic pregnancy. Physical examination also is important; if the pelvic examination reveals a dilated cervix with pregnancy tissue in the cervical os it is likely that a miscarriage is in progress. For most cases of early pregnancy complicated by pelvic pain and/or uterine bleeding, however, a pelvic sonogram and serial quantitative measurement of human chorionic gonadotropin (hCG) are needed to achieve the correct diagnosis.
Here I outline the clinical markers for transvaginal ultrasonography that indicate a viable or failed intrauterine pregnancy as well as an ectopic pregnancy. I also present data on single vs serial hCG measurement and discuss serial hCG levels that indicate viable or nonviable intrauterine or ectopic pregnancy.
Is an early gestation viable? Clinical evaluationTransvaginal pelvic ultrasoundTransvaginal and transabdominal ultrasonography play a critical role in evaluating early pregnancy problems. In a normal pregnancy, key developmental milestones that can be observed reliably on ultrasound are1,2:
- intrauterine gestational sac at 5 weeks
- yolk sac at 5.5 weeks
- embryonic pole and fetal heart beat at 6 to 6.5 weeks’ gestation.
A pelvic ultrasound also may provide evidence that an intrauterine pregnancy will fail and result in a miscarriage. Findings diagnostic of a failed intrauterine pregnancy include3:
- crown-rump length ≥7 mm and no fetal heartbeat
- mean sac diameter ≥25 mm and no embryo
- absence of an embryo with a heartbeat more than 2 weeks after an ultrasound scan that showed a gestational sac without a yolk sac
- absence of an embryo with a heartbeat more than 11 days after a scan that showed a gestational sac with a yolk sac.
Findings suspicious for a failing intrauterine pregnancy include3:
- crown-rump length <7 mm and no fetal heartbeat
- mean sac diameter of 16 to 24 mm and no embryo
- no heartbeat 7 to 13 days after an ultrasound scan that showed a gestational sac without a yolk sac
- no heartbeat 7 to 10 days after an ultrasound scan that showed a gestational sac with a yolk sac.
When it’s an ectopic pregnancy. Definitive ultrasonographic evidence of an ectopic pregnancy is identification of a fetal heartbeat outside the uterus or a gestational sac and yolk sac outside of the uterus. An adnexal mass can be identified on ultrasonography in most cases of ectopic pregnancy. In one study of 291 ectopic pregnancies, an adnexal mass was identified in 94% of cases, and a moderate to large amount of free pelvic fluid was found in 36% of cases.4 The adnexal masses included nonspecific (54% of all ectopic cases), a tubal ring without a yolk sac or embryo (25%), a yolk sac but no embryonic heartbeat (8%), and an embryo with cardiac activity (7%).
In clinical units with high-quality gynecologic ultrasonography available, most ectopic pregnancies will be detected on initial scan and only 10% to 15% of ectopic pregnancies will have an ultrasound finding of no intrauterine pregnancy and no evidence for an extrauterine pregnancy.5
Almost all (in the range of 99%) viable intrauterine pregnancies demonstrate an increase in hCG level of 53% or more over 48 hours, whereas only 21% of ectopic pregnancies demonstrate a rise of 53% or more.7
Most pregnancies that will end in a miscarriage demonstrate a decrease in hCG level over 48 hours. If the initial hCG value is 2,000 mIU/mL, 90% of pregnancies that will end in miscarriage will have an approximate 30% decrease in hCG over 48 hours. If the initial hCG is 1,000 mIU/mL, 95% of spontaneous abortions will have a 28% decline in 48 hours.7 About 10% of ectopic pregnancies also will demonstrate a 30% decrease in hCG over 48 hours.
A minor disadvantage of serial hCG measurements is that patients may become anxious and fearful as they await the result of life-altering test results.
When a gestation is found to be nonviable A viable intrauterine pregnancy is highly unlikely in a woman with no ultrasound evidence of an intrauterine pregnancy or an adnexal mass and an hCG level that rises very little, plateaus, or decreases over 48 hours. In this situation, a Karman cannula aspiration of uterine contents with rush pathology analysis can help clarify the likely diagnosis and guide therapy.
Women with documented villi on pathology likely are experiencing a miscarriage and can have their hCG level followed to resolution. Women with no documented villi and no decrease in hCG after the Karman
cannula aspiration can be presumed to have an ectopic pregnancy. If stable, these women may be candidates for treatment with methotrexate.8,9
Many experts have counseled against the use of a single hCG measurement in the discriminatory zone of 1,500 to 2,000 mIU/mL to trigger methotrexate treatment. Here is a sampling of their advice:
“An hCG level of 2,000 mIU/mL, without ultrasound findings of intrauterine pregnancy, while suggestive of abnormal pregnancy, is not diagnostic. Per the results of recent studies, it is reasonable to closely follow up rather than treat many of these early, stable cases of ectopic pregnancy.”
—Mehta et al.1
“Our data demonstrate that using a single value of serum hCG in a pregnancy of unknown location (PUL) population is of limited value.... A significant proportion of failing PULs and early intrauterine pregnancies in a PUL population have high serum hCG levels at presentation.”
—Condus et al.2
“The hCG discriminatory level should not be used to determine the management of a hemodynamically stable patient with suspected ectopic pregnancy, if sonography demonstrates no findings of intrauterine or ectopic pregnancy.”
—Doubilet et al.3
“There is almost no reason to give methotrexate on first encounter with a patient. If a patient is symptomatic with severe pain or signs of rupture, a surgical approach is indicated and methotrexate is contraindicated.”
—Barnhart et al.4
[When using the discriminatory zone]... “there is a chance of harming a viable intrauterine pregnancy, especially if the hCG level is 2000 to 3000 mIU/mL.... There is limited risk in taking a few extra days to make a definitive diagnosis in a woman with a pregnancy of unknown location who has no signs or symptoms of rupture and no ultrasonographic evidence of ectopic pregnancy.”
—Doubliet et al.3
“Viable intrauterine pregnancy is possible in patients with pregnancy of unknown location and hCG levels above the generally accept discriminatory zone, strict adherence to which can potentially disrupt a normal pregnancy. We support the need for judicious use of the hCG discriminatory level in hemodynamically stable patients with pregnancy of unknown location, and the decision to intervene should not be based solely on a single hCG level.”
—Ko and Cheung.5
References
- Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.
- Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
- Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
- Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
Stop using the discriminatory zone and a single hCG measurement to trigger clinical intervention As noted above, a single hCG measurement is of very little value in determining whether an early pregnancy is a viable or nonviable intrauterine pregnancy or is ectopic. Many experts have reported that if a single hCG measurement shows a value of more than 1,500 mIU/mL and a pelvic ultrasound shows no intrauterine pregnancy, an ectopic or nonviable intrauterine pregnancy is likely. Some experts have used the presence of an hCG value of more than 1,500 mIU/mL plus an ultrasound scan without evidence of an intrauterine pregnancy to clinically diagnose the absence of a viable intrauterine pregnancy and administer methotrexate to treat a presumptive ectopic pregnancy. Many experts believe, however, that this approach will necessarily result in the treatment of viable intrauterine pregnancies with methotrexate.5,10
Based on one analysis, for 100 women with an initial hCG value between 2,000 and 3,000 mIU/mL and no intrauterine pregnancy or adnexal mass seen on ultrasound, follow-up will reveal that 65.5% had a failed intrauterine pregnancy, 33% had an ectopic pregnancy, and 1.5% had a viable intrauterine pregnancy.3,10,11 If all of these 100 women had been treated with methotrexate for a presumed ectopic pregnancy, approximately two women with a viable intrauterine pregnancy would have been exposed to methotrexate. This exposure would likely result in either a pregnancy loss or, if the pregnancy continues, an increased risk of fetal anomalies.
If the patient is obese, has fibroids, or has adenomyosis, she has an increased risk of an ultrasound failing to detect an early intrauterine pregnancy when the hCG value ranges from 1,500 to 3,000 mIU/mL.12 If the discriminatory zone is raised to 4,000 mIU/mL, the likelihood of mistakenly diagnosing a viable intrauterine pregnancy as a failed or ectopic pregnancy is much less (but not zero).
There is almost no clinical situation in which methotrexate should be given to a patient suspected of having an ectopic pregnancy on the first visit, unless ultrasound demonstrates an adnexal mass indicative of ectopic pregnancy.13,14 If the patient has severe pain or bleeding, or has signs consistent with a ruptured ectopic pregnancy, surgical intervention likely is warranted. If the patient is clinically stable, a safe option is to repeat the hCG measurement in 48 hours, with an ultrasound if indicated.
The discriminatory zone is an interesting and elegant idea. But in practice it is fraught with serious dangers, the greatest of which is methotrexate administration to a patient with a viable intrauterine gestation. My advice is that gynecologists should stop relying on a discriminatory zone of 1,500 to 2,000 mIU/mL to trigger clinical intervention.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Approximately 15% of early pregnancies are complicated by pelvic or abdominal pain and uterine bleeding or spotting. In these situations, you must determine whether your patient has a viable intrauterine pregnancy, a pregnancy that will end in a miscarriage (spontaneous abortion), or an ectopic pregnancy.
To guide you to the correct diagnosis, a medical history and physical examination can be helpful. For example, a woman with a prior ectopic pregnancy who now has an early pregnancy complicated by pelvic pain and uterine bleeding is at high risk for an ectopic pregnancy. Physical examination also is important; if the pelvic examination reveals a dilated cervix with pregnancy tissue in the cervical os it is likely that a miscarriage is in progress. For most cases of early pregnancy complicated by pelvic pain and/or uterine bleeding, however, a pelvic sonogram and serial quantitative measurement of human chorionic gonadotropin (hCG) are needed to achieve the correct diagnosis.
Here I outline the clinical markers for transvaginal ultrasonography that indicate a viable or failed intrauterine pregnancy as well as an ectopic pregnancy. I also present data on single vs serial hCG measurement and discuss serial hCG levels that indicate viable or nonviable intrauterine or ectopic pregnancy.
Is an early gestation viable? Clinical evaluationTransvaginal pelvic ultrasoundTransvaginal and transabdominal ultrasonography play a critical role in evaluating early pregnancy problems. In a normal pregnancy, key developmental milestones that can be observed reliably on ultrasound are1,2:
- intrauterine gestational sac at 5 weeks
- yolk sac at 5.5 weeks
- embryonic pole and fetal heart beat at 6 to 6.5 weeks’ gestation.
A pelvic ultrasound also may provide evidence that an intrauterine pregnancy will fail and result in a miscarriage. Findings diagnostic of a failed intrauterine pregnancy include3:
- crown-rump length ≥7 mm and no fetal heartbeat
- mean sac diameter ≥25 mm and no embryo
- absence of an embryo with a heartbeat more than 2 weeks after an ultrasound scan that showed a gestational sac without a yolk sac
- absence of an embryo with a heartbeat more than 11 days after a scan that showed a gestational sac with a yolk sac.
Findings suspicious for a failing intrauterine pregnancy include3:
- crown-rump length <7 mm and no fetal heartbeat
- mean sac diameter of 16 to 24 mm and no embryo
- no heartbeat 7 to 13 days after an ultrasound scan that showed a gestational sac without a yolk sac
- no heartbeat 7 to 10 days after an ultrasound scan that showed a gestational sac with a yolk sac.
When it’s an ectopic pregnancy. Definitive ultrasonographic evidence of an ectopic pregnancy is identification of a fetal heartbeat outside the uterus or a gestational sac and yolk sac outside of the uterus. An adnexal mass can be identified on ultrasonography in most cases of ectopic pregnancy. In one study of 291 ectopic pregnancies, an adnexal mass was identified in 94% of cases, and a moderate to large amount of free pelvic fluid was found in 36% of cases.4 The adnexal masses included nonspecific (54% of all ectopic cases), a tubal ring without a yolk sac or embryo (25%), a yolk sac but no embryonic heartbeat (8%), and an embryo with cardiac activity (7%).
In clinical units with high-quality gynecologic ultrasonography available, most ectopic pregnancies will be detected on initial scan and only 10% to 15% of ectopic pregnancies will have an ultrasound finding of no intrauterine pregnancy and no evidence for an extrauterine pregnancy.5
Almost all (in the range of 99%) viable intrauterine pregnancies demonstrate an increase in hCG level of 53% or more over 48 hours, whereas only 21% of ectopic pregnancies demonstrate a rise of 53% or more.7
Most pregnancies that will end in a miscarriage demonstrate a decrease in hCG level over 48 hours. If the initial hCG value is 2,000 mIU/mL, 90% of pregnancies that will end in miscarriage will have an approximate 30% decrease in hCG over 48 hours. If the initial hCG is 1,000 mIU/mL, 95% of spontaneous abortions will have a 28% decline in 48 hours.7 About 10% of ectopic pregnancies also will demonstrate a 30% decrease in hCG over 48 hours.
A minor disadvantage of serial hCG measurements is that patients may become anxious and fearful as they await the result of life-altering test results.
When a gestation is found to be nonviable A viable intrauterine pregnancy is highly unlikely in a woman with no ultrasound evidence of an intrauterine pregnancy or an adnexal mass and an hCG level that rises very little, plateaus, or decreases over 48 hours. In this situation, a Karman cannula aspiration of uterine contents with rush pathology analysis can help clarify the likely diagnosis and guide therapy.
Women with documented villi on pathology likely are experiencing a miscarriage and can have their hCG level followed to resolution. Women with no documented villi and no decrease in hCG after the Karman
cannula aspiration can be presumed to have an ectopic pregnancy. If stable, these women may be candidates for treatment with methotrexate.8,9
Many experts have counseled against the use of a single hCG measurement in the discriminatory zone of 1,500 to 2,000 mIU/mL to trigger methotrexate treatment. Here is a sampling of their advice:
“An hCG level of 2,000 mIU/mL, without ultrasound findings of intrauterine pregnancy, while suggestive of abnormal pregnancy, is not diagnostic. Per the results of recent studies, it is reasonable to closely follow up rather than treat many of these early, stable cases of ectopic pregnancy.”
—Mehta et al.1
“Our data demonstrate that using a single value of serum hCG in a pregnancy of unknown location (PUL) population is of limited value.... A significant proportion of failing PULs and early intrauterine pregnancies in a PUL population have high serum hCG levels at presentation.”
—Condus et al.2
“The hCG discriminatory level should not be used to determine the management of a hemodynamically stable patient with suspected ectopic pregnancy, if sonography demonstrates no findings of intrauterine or ectopic pregnancy.”
—Doubilet et al.3
“There is almost no reason to give methotrexate on first encounter with a patient. If a patient is symptomatic with severe pain or signs of rupture, a surgical approach is indicated and methotrexate is contraindicated.”
—Barnhart et al.4
[When using the discriminatory zone]... “there is a chance of harming a viable intrauterine pregnancy, especially if the hCG level is 2000 to 3000 mIU/mL.... There is limited risk in taking a few extra days to make a definitive diagnosis in a woman with a pregnancy of unknown location who has no signs or symptoms of rupture and no ultrasonographic evidence of ectopic pregnancy.”
—Doubliet et al.3
“Viable intrauterine pregnancy is possible in patients with pregnancy of unknown location and hCG levels above the generally accept discriminatory zone, strict adherence to which can potentially disrupt a normal pregnancy. We support the need for judicious use of the hCG discriminatory level in hemodynamically stable patients with pregnancy of unknown location, and the decision to intervene should not be based solely on a single hCG level.”
—Ko and Cheung.5
References
- Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.
- Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
- Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
- Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
Stop using the discriminatory zone and a single hCG measurement to trigger clinical intervention As noted above, a single hCG measurement is of very little value in determining whether an early pregnancy is a viable or nonviable intrauterine pregnancy or is ectopic. Many experts have reported that if a single hCG measurement shows a value of more than 1,500 mIU/mL and a pelvic ultrasound shows no intrauterine pregnancy, an ectopic or nonviable intrauterine pregnancy is likely. Some experts have used the presence of an hCG value of more than 1,500 mIU/mL plus an ultrasound scan without evidence of an intrauterine pregnancy to clinically diagnose the absence of a viable intrauterine pregnancy and administer methotrexate to treat a presumptive ectopic pregnancy. Many experts believe, however, that this approach will necessarily result in the treatment of viable intrauterine pregnancies with methotrexate.5,10
Based on one analysis, for 100 women with an initial hCG value between 2,000 and 3,000 mIU/mL and no intrauterine pregnancy or adnexal mass seen on ultrasound, follow-up will reveal that 65.5% had a failed intrauterine pregnancy, 33% had an ectopic pregnancy, and 1.5% had a viable intrauterine pregnancy.3,10,11 If all of these 100 women had been treated with methotrexate for a presumed ectopic pregnancy, approximately two women with a viable intrauterine pregnancy would have been exposed to methotrexate. This exposure would likely result in either a pregnancy loss or, if the pregnancy continues, an increased risk of fetal anomalies.
If the patient is obese, has fibroids, or has adenomyosis, she has an increased risk of an ultrasound failing to detect an early intrauterine pregnancy when the hCG value ranges from 1,500 to 3,000 mIU/mL.12 If the discriminatory zone is raised to 4,000 mIU/mL, the likelihood of mistakenly diagnosing a viable intrauterine pregnancy as a failed or ectopic pregnancy is much less (but not zero).
There is almost no clinical situation in which methotrexate should be given to a patient suspected of having an ectopic pregnancy on the first visit, unless ultrasound demonstrates an adnexal mass indicative of ectopic pregnancy.13,14 If the patient has severe pain or bleeding, or has signs consistent with a ruptured ectopic pregnancy, surgical intervention likely is warranted. If the patient is clinically stable, a safe option is to repeat the hCG measurement in 48 hours, with an ultrasound if indicated.
The discriminatory zone is an interesting and elegant idea. But in practice it is fraught with serious dangers, the greatest of which is methotrexate administration to a patient with a viable intrauterine gestation. My advice is that gynecologists should stop relying on a discriminatory zone of 1,500 to 2,000 mIU/mL to trigger clinical intervention.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Bree RL, Edwards M, Böhm-Vélez M, et al. Transvaginal sonography in the evaluation of normal early pregnancy: correlation with hCG level. AJR Am J Roentgenol. 1989;153(1):75–79.
2. Goldstein I, Zimmer EA, Tamir A, Peretz BA, Paldi E. Evaluation of normal gestational sac growth: appearance of embryonic heartbeat and embryo body movements using the transvaginal technique. Obstet Gynecol. 1991;77(6):885–888.
3. Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
4. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
5. Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
6. Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361(4):379–387.
7. Silva C, Sammel MD, Zhou L, et al. Human chorionic gonadotropin profile for women with ectopic pregnancy. Obstet Gynecol. 2006;107(3):605–610.
8. Shaunik A, Kulp J, Appleby DH, Sammel MD, Barnhart KT. Utility of dilation and curettage in the diagnosis of pregnancy of unknown location. Am J Obstet Gynecol. 2011;204(2):130.e1–6.
9. Brady P, Imudia AN, Awonuga AO, Wright DL, Syter AK, Toth TL. Pregnancies of unknown location after in vitro fertilization: minimally invasive management with Karman cannula aspiration. Fertil Steril. 2014;101(2):420–426.
10. Doubilet PM, Benson CB. Further evidence against the reliability of the human chorionic discriminatory level. J Ultrasound Med. 2011;30(12):1637–1642.
11. Benson CB, Doubilet PM, Peters HE, Frates MC. Intrauterine fluid with ectopic pregnancy: a reappraisal. J Ultrasound Med. 2013;32(3):389–393.
12. Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
13. Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
14. Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.
1. Bree RL, Edwards M, Böhm-Vélez M, et al. Transvaginal sonography in the evaluation of normal early pregnancy: correlation with hCG level. AJR Am J Roentgenol. 1989;153(1):75–79.
2. Goldstein I, Zimmer EA, Tamir A, Peretz BA, Paldi E. Evaluation of normal gestational sac growth: appearance of embryonic heartbeat and embryo body movements using the transvaginal technique. Obstet Gynecol. 1991;77(6):885–888.
3. Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
4. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
5. Condous G, Kirk E, Lu C, et al. Diagnostic accuracy of varying discriminatory zones for the prediction of ectopic pregnancy in women with pregnancy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–775.
6. Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361(4):379–387.
7. Silva C, Sammel MD, Zhou L, et al. Human chorionic gonadotropin profile for women with ectopic pregnancy. Obstet Gynecol. 2006;107(3):605–610.
8. Shaunik A, Kulp J, Appleby DH, Sammel MD, Barnhart KT. Utility of dilation and curettage in the diagnosis of pregnancy of unknown location. Am J Obstet Gynecol. 2011;204(2):130.e1–6.
9. Brady P, Imudia AN, Awonuga AO, Wright DL, Syter AK, Toth TL. Pregnancies of unknown location after in vitro fertilization: minimally invasive management with Karman cannula aspiration. Fertil Steril. 2014;101(2):420–426.
10. Doubilet PM, Benson CB. Further evidence against the reliability of the human chorionic discriminatory level. J Ultrasound Med. 2011;30(12):1637–1642.
11. Benson CB, Doubilet PM, Peters HE, Frates MC. Intrauterine fluid with ectopic pregnancy: a reappraisal. J Ultrasound Med. 2013;32(3):389–393.
12. Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location. J Ultrasound Med. 2014;33(3):465–471.
13. Barnhart KT. Early pregnancy failure: beware of the pitfalls of modern management. Fertil Steril. 2012;98(5):1061–1065.
14. Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2):569–573.

A new year and a new face for www.ccjm.org
Bob Dylan’s song “The Times They Are a-Changin’” was released in January 1964. As with many things Dylan, the song’s true intent is a bit unclear, but it remains one of the most invoked lyrical symbols of change 51 years later. In 2015, the Journal, planning to “heed the call,” is changing its online visage. I hope that our intent will not be viewed as unclear.
Our mission is unchanged: to provide our readers with free access to credible, relevant, readable information, and the opportunity to earn free CME credit. So why change the website? Innovations in digital publishing, the ability to offer a broader landscape of medical information—and the chance to more effectively solicit advertising to pay for it all—prompted us to collaborate with another publisher, Frontline Medical Communications.
Frontline describes itself as health care’s largest medical communications company and as a leader in digital, print, and live events. You likely have encountered their products, which include Internal Medicine News, Cardiology News, and Clinical Endocrinology News, and CME courses such as Perspectives in Rheumatic Diseases, which I codirect. Our collaboration will allow us to offer you links to new and, we hope, interesting material. For example, our online readers will have access to MD-IQ, a popular interactive self-test, as well as brief reports and timely commentaries from specialty scientific meetings.
But even though www.ccjm.org has a new look, everything on it remains open to all and free of charge. You will still have easy access to other educational and clinical information offered by Cleveland Clinic, including information about Clinic authors. At your first visit to our revamped site you will be asked to register, but your subsequent visits will be unencumbered except for a request to sign in using your e-mail address if you log in from a different device. The e-mail address is used for identification purposes only, as site sponsors want to know the (depersonalized) demographics of our readership. You will receive occasional e-mails with links to clinical content that may interest you. If you do not wish to receive these e-mails, just follow the instructions to opt out of them. Our goal is to be unobtrusive.
Our free CME process is the same. Each CME article includes a link to the Cleveland Clinic Center for Continuing Education site with instructions on how to complete the activity. Plus, the CME pull-down menu at the top of our home page will provide easy access to all currently active journal CME offerings. We hope the transition glitches will be few and the benefits many. And the option remains for you to read, download, and print our articles in PDF format, just as you always have.
As we start the new year, we at the Journal wish you our readers a happy, healthy, peaceful, and educational 2015.
Bob Dylan’s song “The Times They Are a-Changin’” was released in January 1964. As with many things Dylan, the song’s true intent is a bit unclear, but it remains one of the most invoked lyrical symbols of change 51 years later. In 2015, the Journal, planning to “heed the call,” is changing its online visage. I hope that our intent will not be viewed as unclear.
Our mission is unchanged: to provide our readers with free access to credible, relevant, readable information, and the opportunity to earn free CME credit. So why change the website? Innovations in digital publishing, the ability to offer a broader landscape of medical information—and the chance to more effectively solicit advertising to pay for it all—prompted us to collaborate with another publisher, Frontline Medical Communications.
Frontline describes itself as health care’s largest medical communications company and as a leader in digital, print, and live events. You likely have encountered their products, which include Internal Medicine News, Cardiology News, and Clinical Endocrinology News, and CME courses such as Perspectives in Rheumatic Diseases, which I codirect. Our collaboration will allow us to offer you links to new and, we hope, interesting material. For example, our online readers will have access to MD-IQ, a popular interactive self-test, as well as brief reports and timely commentaries from specialty scientific meetings.
But even though www.ccjm.org has a new look, everything on it remains open to all and free of charge. You will still have easy access to other educational and clinical information offered by Cleveland Clinic, including information about Clinic authors. At your first visit to our revamped site you will be asked to register, but your subsequent visits will be unencumbered except for a request to sign in using your e-mail address if you log in from a different device. The e-mail address is used for identification purposes only, as site sponsors want to know the (depersonalized) demographics of our readership. You will receive occasional e-mails with links to clinical content that may interest you. If you do not wish to receive these e-mails, just follow the instructions to opt out of them. Our goal is to be unobtrusive.
Our free CME process is the same. Each CME article includes a link to the Cleveland Clinic Center for Continuing Education site with instructions on how to complete the activity. Plus, the CME pull-down menu at the top of our home page will provide easy access to all currently active journal CME offerings. We hope the transition glitches will be few and the benefits many. And the option remains for you to read, download, and print our articles in PDF format, just as you always have.
As we start the new year, we at the Journal wish you our readers a happy, healthy, peaceful, and educational 2015.
Bob Dylan’s song “The Times They Are a-Changin’” was released in January 1964. As with many things Dylan, the song’s true intent is a bit unclear, but it remains one of the most invoked lyrical symbols of change 51 years later. In 2015, the Journal, planning to “heed the call,” is changing its online visage. I hope that our intent will not be viewed as unclear.
Our mission is unchanged: to provide our readers with free access to credible, relevant, readable information, and the opportunity to earn free CME credit. So why change the website? Innovations in digital publishing, the ability to offer a broader landscape of medical information—and the chance to more effectively solicit advertising to pay for it all—prompted us to collaborate with another publisher, Frontline Medical Communications.
Frontline describes itself as health care’s largest medical communications company and as a leader in digital, print, and live events. You likely have encountered their products, which include Internal Medicine News, Cardiology News, and Clinical Endocrinology News, and CME courses such as Perspectives in Rheumatic Diseases, which I codirect. Our collaboration will allow us to offer you links to new and, we hope, interesting material. For example, our online readers will have access to MD-IQ, a popular interactive self-test, as well as brief reports and timely commentaries from specialty scientific meetings.
But even though www.ccjm.org has a new look, everything on it remains open to all and free of charge. You will still have easy access to other educational and clinical information offered by Cleveland Clinic, including information about Clinic authors. At your first visit to our revamped site you will be asked to register, but your subsequent visits will be unencumbered except for a request to sign in using your e-mail address if you log in from a different device. The e-mail address is used for identification purposes only, as site sponsors want to know the (depersonalized) demographics of our readership. You will receive occasional e-mails with links to clinical content that may interest you. If you do not wish to receive these e-mails, just follow the instructions to opt out of them. Our goal is to be unobtrusive.
Our free CME process is the same. Each CME article includes a link to the Cleveland Clinic Center for Continuing Education site with instructions on how to complete the activity. Plus, the CME pull-down menu at the top of our home page will provide easy access to all currently active journal CME offerings. We hope the transition glitches will be few and the benefits many. And the option remains for you to read, download, and print our articles in PDF format, just as you always have.
As we start the new year, we at the Journal wish you our readers a happy, healthy, peaceful, and educational 2015.
From bedlam to biomarkers: The transformation of psychiatry’s terminology reflects its 4 conceptual earthquakes
Consider here my journey in psychiatry since my adolescence. Growing up in the 1960s and 1970s, I did not watch much television; my father was convinced TV would be “too distracting” for us children. At first, I was angry about his rule, and would occasionally watch programs such as Bonanza at sleep-overs.
The lure of psychoanalysis
Gradually, I became grateful to my father because—in contrast to my classmates, who sat passively for hours watching TV after school—I voraciously read the piles of fiction and nonfiction books that I checked out from the school library every week, expanding my general knowledge and perspectives. One of my favorite genres became psychology and psychiatry, including many of Sigmund Freud’s works.
I was enchanted by psychoanalysis and its explanation of mental illness because, growing up, I had been told that madness is caused by demonic spirits and bad behavior and it is completely untreatable. By the time I was in high school, I had decided to become a psychiatrist, and was practicing what I read by “counseling” my classmates about family conflicts, raging drives, and frustrating relationships with girlfriends.
Rising tide of psychopharmacology
My love for psychiatry never wavered during my undergraduate years. I focused not only on required pre-med courses but enthusiastically took many psychology, sociology, and anthropology electives to expand my understanding of human behavior. In medical school, I enjoyed all rotations, but psychiatry was simply sublime. Often, I offered (to my classmates’ delight) to take their weekend call at the psychiatric hospital so I could see more patients.
After my internship, I married my wife (a behavioral psychologist) and embarked on psychiatry residency training with gusto. I was far better prepared, I realized, than my fellow residents; my faculty supervisors noticed that I answered questions more often than many others during rounds and lectures. (Thanks, Dad, for banning television!) I relished every psychotherapy session and spent hours listening to audiotapes of my patients’ sessions to improve my skills and to discover the psychodynamic nuances of their psychopathology. Being supervised by expert psychoanalysts was the highlight of my week as I honed my psychodynamic psychotherapy skills.
But something interesting happened during my residency: Psychopharmacology and electroconvulsive therapy were helping my severely ill psychotic, manic, and depressed patients much faster than psychotherapy could. Length of stay in the wards typically was 30 days (there was no managed care back then to limit stay to an absurd 5 days), and I saw substantial improvement in many of my patients before discharge.
I was so enthralled by the rising tide of psychopharmacology that I decided in PGY-2 to conduct psychopharmacology research—which, I came to realize, was easier than research on psychotherapy. I secured a mentor from the department of pharmacology. In PGY-3, I presented my data at the Annual Meeting of the American Psychiatric Association; in PGY-4, the paper was published in the American Journal of Psychiatry.
By the end of residency, I had applied to the National Institute of Mental Health (NIMH) to pursue a research fellowship in the neuropharmacology of schizophrenia to prepare me for an academic career. I participated in numerous studies on the NIMH research ward, brimming with patients who had refractory schizophrenia (before the advent of clozapine in 1989), and I published many articles with mentors and fellow researchers.
Investigating brain biology
Then another funny thing happened: During my fellowship, one of my mentors shared with me some early studies about postmortem structural changes in the brain of schizophrenia patients. That prompted me to spend hours in the basement of the pathology department examining the brains of dozens of patients with schizophrenia, noting atrophic changes and performing measurements and histopathologic studies.
Consequently, I embarked on neuroimaging research to study the morphological abnormalities of cortical and subcortical regions in living patients. I found myself going beyond neuropsychopharmacology and diving into neuroanatomy books and neuroscience journals. I realized that I was continuously learning and using a new scientific language in my daily work.
After I left NIMH to begin a career of teaching, research, and patient care in a medical school setting, I was engulfed by meteoric advances in neuroscience producing unprecedented insights about the molecular biology of schizophrenia and other severe neuropsychiatric disorders, leading me to pursue new opportunities in neurobiology while continuing my psychopharmacology research.
The rate of transformation is mind-boggling
Looking back at the span of time from childhood through the exciting journey of my psychiatry career, I realize how massive a transformation I have witnessed and experienced. The specialty has shifted its clinical and scientific paradigms through several conceptual models—from demonic possession to psychoanalysis to psychopharmacology and, last, to molecular neurobiology. Four times in my life, the lexicon of psychiatry has undergone a complete makeover. This is a light-speed pace of scientific progress over a few decades—truly breathtaking! It’s like rewriting a dictionary over and over, with no 2 successive editions resembling each other whatsoever.
The Table shows 4 sets of examples of psychiatric terminology, each representing 1 of the 4 paradigmatic models that my generation of psychiatrists has had to adopt and use in clinical care and research. I cannot think of any other medical specialty that has come close to evolving and transforming its language and conceptual models of etiology and treatment at such a rapid pace.
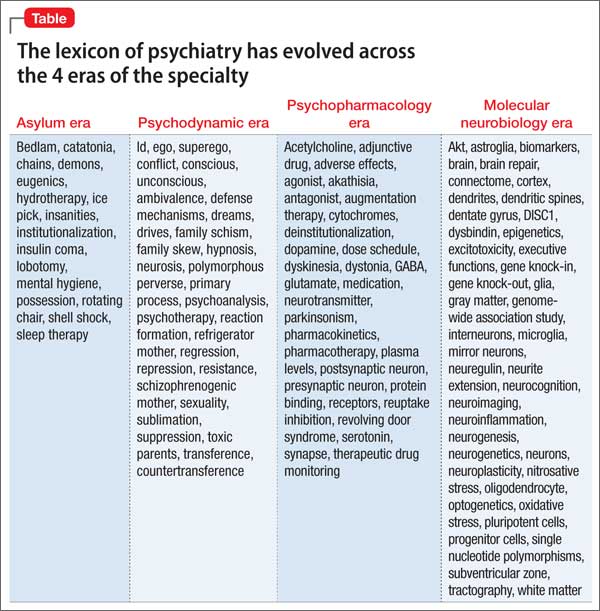
When I embraced psychiatry in adolescence as my future career, I never imagined, in my wildest dreams, that I would experience such successive scientific earthquakes in my beloved medical specialty. Perhaps that’s what kept me stimulated and eager to come to work every day; I use all the models and treatment tools I have learned in understanding and helping my patients with evolving psychotherapeutic and biopharmaceutical tools; I also teach my students and residents about the multifaceted wonders of the human mind and the magnificent complexities of the brain in health and disease.
Psychiatry has been, and will continue to be, a Pandora’s box of medicine, full of stunning scientific twists and surprises and a transformative lexicon to match.
Consider here my journey in psychiatry since my adolescence. Growing up in the 1960s and 1970s, I did not watch much television; my father was convinced TV would be “too distracting” for us children. At first, I was angry about his rule, and would occasionally watch programs such as Bonanza at sleep-overs.
The lure of psychoanalysis
Gradually, I became grateful to my father because—in contrast to my classmates, who sat passively for hours watching TV after school—I voraciously read the piles of fiction and nonfiction books that I checked out from the school library every week, expanding my general knowledge and perspectives. One of my favorite genres became psychology and psychiatry, including many of Sigmund Freud’s works.
I was enchanted by psychoanalysis and its explanation of mental illness because, growing up, I had been told that madness is caused by demonic spirits and bad behavior and it is completely untreatable. By the time I was in high school, I had decided to become a psychiatrist, and was practicing what I read by “counseling” my classmates about family conflicts, raging drives, and frustrating relationships with girlfriends.
Rising tide of psychopharmacology
My love for psychiatry never wavered during my undergraduate years. I focused not only on required pre-med courses but enthusiastically took many psychology, sociology, and anthropology electives to expand my understanding of human behavior. In medical school, I enjoyed all rotations, but psychiatry was simply sublime. Often, I offered (to my classmates’ delight) to take their weekend call at the psychiatric hospital so I could see more patients.
After my internship, I married my wife (a behavioral psychologist) and embarked on psychiatry residency training with gusto. I was far better prepared, I realized, than my fellow residents; my faculty supervisors noticed that I answered questions more often than many others during rounds and lectures. (Thanks, Dad, for banning television!) I relished every psychotherapy session and spent hours listening to audiotapes of my patients’ sessions to improve my skills and to discover the psychodynamic nuances of their psychopathology. Being supervised by expert psychoanalysts was the highlight of my week as I honed my psychodynamic psychotherapy skills.
But something interesting happened during my residency: Psychopharmacology and electroconvulsive therapy were helping my severely ill psychotic, manic, and depressed patients much faster than psychotherapy could. Length of stay in the wards typically was 30 days (there was no managed care back then to limit stay to an absurd 5 days), and I saw substantial improvement in many of my patients before discharge.
I was so enthralled by the rising tide of psychopharmacology that I decided in PGY-2 to conduct psychopharmacology research—which, I came to realize, was easier than research on psychotherapy. I secured a mentor from the department of pharmacology. In PGY-3, I presented my data at the Annual Meeting of the American Psychiatric Association; in PGY-4, the paper was published in the American Journal of Psychiatry.
By the end of residency, I had applied to the National Institute of Mental Health (NIMH) to pursue a research fellowship in the neuropharmacology of schizophrenia to prepare me for an academic career. I participated in numerous studies on the NIMH research ward, brimming with patients who had refractory schizophrenia (before the advent of clozapine in 1989), and I published many articles with mentors and fellow researchers.
Investigating brain biology
Then another funny thing happened: During my fellowship, one of my mentors shared with me some early studies about postmortem structural changes in the brain of schizophrenia patients. That prompted me to spend hours in the basement of the pathology department examining the brains of dozens of patients with schizophrenia, noting atrophic changes and performing measurements and histopathologic studies.
Consequently, I embarked on neuroimaging research to study the morphological abnormalities of cortical and subcortical regions in living patients. I found myself going beyond neuropsychopharmacology and diving into neuroanatomy books and neuroscience journals. I realized that I was continuously learning and using a new scientific language in my daily work.
After I left NIMH to begin a career of teaching, research, and patient care in a medical school setting, I was engulfed by meteoric advances in neuroscience producing unprecedented insights about the molecular biology of schizophrenia and other severe neuropsychiatric disorders, leading me to pursue new opportunities in neurobiology while continuing my psychopharmacology research.
The rate of transformation is mind-boggling
Looking back at the span of time from childhood through the exciting journey of my psychiatry career, I realize how massive a transformation I have witnessed and experienced. The specialty has shifted its clinical and scientific paradigms through several conceptual models—from demonic possession to psychoanalysis to psychopharmacology and, last, to molecular neurobiology. Four times in my life, the lexicon of psychiatry has undergone a complete makeover. This is a light-speed pace of scientific progress over a few decades—truly breathtaking! It’s like rewriting a dictionary over and over, with no 2 successive editions resembling each other whatsoever.
The Table shows 4 sets of examples of psychiatric terminology, each representing 1 of the 4 paradigmatic models that my generation of psychiatrists has had to adopt and use in clinical care and research. I cannot think of any other medical specialty that has come close to evolving and transforming its language and conceptual models of etiology and treatment at such a rapid pace.
When I embraced psychiatry in adolescence as my future career, I never imagined, in my wildest dreams, that I would experience such successive scientific earthquakes in my beloved medical specialty. Perhaps that’s what kept me stimulated and eager to come to work every day; I use all the models and treatment tools I have learned in understanding and helping my patients with evolving psychotherapeutic and biopharmaceutical tools; I also teach my students and residents about the multifaceted wonders of the human mind and the magnificent complexities of the brain in health and disease.
Psychiatry has been, and will continue to be, a Pandora’s box of medicine, full of stunning scientific twists and surprises and a transformative lexicon to match.
Consider here my journey in psychiatry since my adolescence. Growing up in the 1960s and 1970s, I did not watch much television; my father was convinced TV would be “too distracting” for us children. At first, I was angry about his rule, and would occasionally watch programs such as Bonanza at sleep-overs.
The lure of psychoanalysis
Gradually, I became grateful to my father because—in contrast to my classmates, who sat passively for hours watching TV after school—I voraciously read the piles of fiction and nonfiction books that I checked out from the school library every week, expanding my general knowledge and perspectives. One of my favorite genres became psychology and psychiatry, including many of Sigmund Freud’s works.
I was enchanted by psychoanalysis and its explanation of mental illness because, growing up, I had been told that madness is caused by demonic spirits and bad behavior and it is completely untreatable. By the time I was in high school, I had decided to become a psychiatrist, and was practicing what I read by “counseling” my classmates about family conflicts, raging drives, and frustrating relationships with girlfriends.
Rising tide of psychopharmacology
My love for psychiatry never wavered during my undergraduate years. I focused not only on required pre-med courses but enthusiastically took many psychology, sociology, and anthropology electives to expand my understanding of human behavior. In medical school, I enjoyed all rotations, but psychiatry was simply sublime. Often, I offered (to my classmates’ delight) to take their weekend call at the psychiatric hospital so I could see more patients.
After my internship, I married my wife (a behavioral psychologist) and embarked on psychiatry residency training with gusto. I was far better prepared, I realized, than my fellow residents; my faculty supervisors noticed that I answered questions more often than many others during rounds and lectures. (Thanks, Dad, for banning television!) I relished every psychotherapy session and spent hours listening to audiotapes of my patients’ sessions to improve my skills and to discover the psychodynamic nuances of their psychopathology. Being supervised by expert psychoanalysts was the highlight of my week as I honed my psychodynamic psychotherapy skills.
But something interesting happened during my residency: Psychopharmacology and electroconvulsive therapy were helping my severely ill psychotic, manic, and depressed patients much faster than psychotherapy could. Length of stay in the wards typically was 30 days (there was no managed care back then to limit stay to an absurd 5 days), and I saw substantial improvement in many of my patients before discharge.
I was so enthralled by the rising tide of psychopharmacology that I decided in PGY-2 to conduct psychopharmacology research—which, I came to realize, was easier than research on psychotherapy. I secured a mentor from the department of pharmacology. In PGY-3, I presented my data at the Annual Meeting of the American Psychiatric Association; in PGY-4, the paper was published in the American Journal of Psychiatry.
By the end of residency, I had applied to the National Institute of Mental Health (NIMH) to pursue a research fellowship in the neuropharmacology of schizophrenia to prepare me for an academic career. I participated in numerous studies on the NIMH research ward, brimming with patients who had refractory schizophrenia (before the advent of clozapine in 1989), and I published many articles with mentors and fellow researchers.
Investigating brain biology
Then another funny thing happened: During my fellowship, one of my mentors shared with me some early studies about postmortem structural changes in the brain of schizophrenia patients. That prompted me to spend hours in the basement of the pathology department examining the brains of dozens of patients with schizophrenia, noting atrophic changes and performing measurements and histopathologic studies.
Consequently, I embarked on neuroimaging research to study the morphological abnormalities of cortical and subcortical regions in living patients. I found myself going beyond neuropsychopharmacology and diving into neuroanatomy books and neuroscience journals. I realized that I was continuously learning and using a new scientific language in my daily work.
After I left NIMH to begin a career of teaching, research, and patient care in a medical school setting, I was engulfed by meteoric advances in neuroscience producing unprecedented insights about the molecular biology of schizophrenia and other severe neuropsychiatric disorders, leading me to pursue new opportunities in neurobiology while continuing my psychopharmacology research.
The rate of transformation is mind-boggling
Looking back at the span of time from childhood through the exciting journey of my psychiatry career, I realize how massive a transformation I have witnessed and experienced. The specialty has shifted its clinical and scientific paradigms through several conceptual models—from demonic possession to psychoanalysis to psychopharmacology and, last, to molecular neurobiology. Four times in my life, the lexicon of psychiatry has undergone a complete makeover. This is a light-speed pace of scientific progress over a few decades—truly breathtaking! It’s like rewriting a dictionary over and over, with no 2 successive editions resembling each other whatsoever.
The Table shows 4 sets of examples of psychiatric terminology, each representing 1 of the 4 paradigmatic models that my generation of psychiatrists has had to adopt and use in clinical care and research. I cannot think of any other medical specialty that has come close to evolving and transforming its language and conceptual models of etiology and treatment at such a rapid pace.
When I embraced psychiatry in adolescence as my future career, I never imagined, in my wildest dreams, that I would experience such successive scientific earthquakes in my beloved medical specialty. Perhaps that’s what kept me stimulated and eager to come to work every day; I use all the models and treatment tools I have learned in understanding and helping my patients with evolving psychotherapeutic and biopharmaceutical tools; I also teach my students and residents about the multifaceted wonders of the human mind and the magnificent complexities of the brain in health and disease.
Psychiatry has been, and will continue to be, a Pandora’s box of medicine, full of stunning scientific twists and surprises and a transformative lexicon to match.