User login
The generalist’s dilemma: training and staying current in the face of increasing specialization
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Pericarditis as a window into the mind of the internist

In this issue of the Journal, Alraies et al comment on how extensively we should look for the cause of an initial episode of pericarditis.
The pericardium, like the pleura, peritoneum, and synovium, can be affected in a number of inflammatory and infectious disorders. The mechanisms by which these tissues are affected are not fully understood, nor is the process by which different diseases seem to selectively target the joint or pericardium. Why are the joints only minimally inflamed in systemic lupus erythematosus (SLE), while lupus pericarditis, in the uncommon occurrence of significant effusion, is often quite inflammatory, with a neutrophil predominance in the fluid? Why is pericardial involvement so often demonstrable by imaging in patients with SLE and rheumatoid arthritis, yet an acute pericarditis presentation with audible pericardial rubs is so seldom recognized?
Although nuances like these are not well understood, in medical school we all learned the association between connective tissue disease and pericarditis. The importance of recalling these associations is repeatedly reinforced during residency and in disease-focused review articles. During my training, woe to the resident who presented a patient at rounds who was admitted with unexplained pericarditis and was not evaluated for SLE with at least an antinuclear antibody (ANA) test, even if there were no other features to suggest the disease. Ordering the test reflected that we knew that, occasionally, pericardial disease is the sole presenting manifestation of lupus.
Such is the plight of the internist. Pericarditis can be the initial manifestation of an autoimmune or inflammatory disease, but this is more often relevant on certification examinations and in medical education than in everyday practice. We are now charged with ordering tests in a more cost-effective manner than in the past. This means that we should not order tests simply because of an epidemiologic association, but only when the result is likely to influence decisions about testing or treatment. But that creates the intellectual dissonance of knowing of a potential relationship (which someone, someday, may challenge us about) but not looking for it. There is an inherent conflict between satisfying intellectual curiosity and the need to be thorough while at the same time containing costs and avoiding the potential harm inherent in overtesting.
A partial solution is to try to define the immediate risk of not recognizing a life- or organ-threatening disease process that can be suggested by a positive nonspecific test (eg, ANA), and to refine the pretest likelihood of specific diagnoses by obtaining an accurate and complete history and performing a focused physical examination. For example, if we suspect that SLE may be the cause of an initial episode of symptomatic pericarditis, our initial evaluation should focus on the patient’s clinical picture. Is there bitemporal hair-thinning? New-onset Raynaud symptoms? Mild generalized adenopathy or lymphopenia? A borderline-low platelet count, or any proteinuria or microhematuria (which should warrant a prompt examination of a fresh urine sediment sample by a physician at the point of care to look for cellular casts indicative of glomerulonephritis)?
As internists, we should try to fulfill our need to be thorough and compulsive by using our honed skills as careful observers and historians—taking a careful history from the patient and family, performing a focused physical examination, and appropriately using disease-defining or staging tests before ordering less specific serologic or other tests. Practicing medicine in a conscientious and compulsive manner does not mean that every diagnostic possibility must be tested for at initial presentation.
Reading how experienced clinicians approach the problem of pericarditis in a specialized clinic provides a useful prompt to self-assess how we approach analogous clinical scenarios.
In this issue of the Journal, Alraies et al comment on how extensively we should look for the cause of an initial episode of pericarditis.
The pericardium, like the pleura, peritoneum, and synovium, can be affected in a number of inflammatory and infectious disorders. The mechanisms by which these tissues are affected are not fully understood, nor is the process by which different diseases seem to selectively target the joint or pericardium. Why are the joints only minimally inflamed in systemic lupus erythematosus (SLE), while lupus pericarditis, in the uncommon occurrence of significant effusion, is often quite inflammatory, with a neutrophil predominance in the fluid? Why is pericardial involvement so often demonstrable by imaging in patients with SLE and rheumatoid arthritis, yet an acute pericarditis presentation with audible pericardial rubs is so seldom recognized?
Although nuances like these are not well understood, in medical school we all learned the association between connective tissue disease and pericarditis. The importance of recalling these associations is repeatedly reinforced during residency and in disease-focused review articles. During my training, woe to the resident who presented a patient at rounds who was admitted with unexplained pericarditis and was not evaluated for SLE with at least an antinuclear antibody (ANA) test, even if there were no other features to suggest the disease. Ordering the test reflected that we knew that, occasionally, pericardial disease is the sole presenting manifestation of lupus.
Such is the plight of the internist. Pericarditis can be the initial manifestation of an autoimmune or inflammatory disease, but this is more often relevant on certification examinations and in medical education than in everyday practice. We are now charged with ordering tests in a more cost-effective manner than in the past. This means that we should not order tests simply because of an epidemiologic association, but only when the result is likely to influence decisions about testing or treatment. But that creates the intellectual dissonance of knowing of a potential relationship (which someone, someday, may challenge us about) but not looking for it. There is an inherent conflict between satisfying intellectual curiosity and the need to be thorough while at the same time containing costs and avoiding the potential harm inherent in overtesting.
A partial solution is to try to define the immediate risk of not recognizing a life- or organ-threatening disease process that can be suggested by a positive nonspecific test (eg, ANA), and to refine the pretest likelihood of specific diagnoses by obtaining an accurate and complete history and performing a focused physical examination. For example, if we suspect that SLE may be the cause of an initial episode of symptomatic pericarditis, our initial evaluation should focus on the patient’s clinical picture. Is there bitemporal hair-thinning? New-onset Raynaud symptoms? Mild generalized adenopathy or lymphopenia? A borderline-low platelet count, or any proteinuria or microhematuria (which should warrant a prompt examination of a fresh urine sediment sample by a physician at the point of care to look for cellular casts indicative of glomerulonephritis)?
As internists, we should try to fulfill our need to be thorough and compulsive by using our honed skills as careful observers and historians—taking a careful history from the patient and family, performing a focused physical examination, and appropriately using disease-defining or staging tests before ordering less specific serologic or other tests. Practicing medicine in a conscientious and compulsive manner does not mean that every diagnostic possibility must be tested for at initial presentation.
Reading how experienced clinicians approach the problem of pericarditis in a specialized clinic provides a useful prompt to self-assess how we approach analogous clinical scenarios.
In this issue of the Journal, Alraies et al comment on how extensively we should look for the cause of an initial episode of pericarditis.
The pericardium, like the pleura, peritoneum, and synovium, can be affected in a number of inflammatory and infectious disorders. The mechanisms by which these tissues are affected are not fully understood, nor is the process by which different diseases seem to selectively target the joint or pericardium. Why are the joints only minimally inflamed in systemic lupus erythematosus (SLE), while lupus pericarditis, in the uncommon occurrence of significant effusion, is often quite inflammatory, with a neutrophil predominance in the fluid? Why is pericardial involvement so often demonstrable by imaging in patients with SLE and rheumatoid arthritis, yet an acute pericarditis presentation with audible pericardial rubs is so seldom recognized?
Although nuances like these are not well understood, in medical school we all learned the association between connective tissue disease and pericarditis. The importance of recalling these associations is repeatedly reinforced during residency and in disease-focused review articles. During my training, woe to the resident who presented a patient at rounds who was admitted with unexplained pericarditis and was not evaluated for SLE with at least an antinuclear antibody (ANA) test, even if there were no other features to suggest the disease. Ordering the test reflected that we knew that, occasionally, pericardial disease is the sole presenting manifestation of lupus.
Such is the plight of the internist. Pericarditis can be the initial manifestation of an autoimmune or inflammatory disease, but this is more often relevant on certification examinations and in medical education than in everyday practice. We are now charged with ordering tests in a more cost-effective manner than in the past. This means that we should not order tests simply because of an epidemiologic association, but only when the result is likely to influence decisions about testing or treatment. But that creates the intellectual dissonance of knowing of a potential relationship (which someone, someday, may challenge us about) but not looking for it. There is an inherent conflict between satisfying intellectual curiosity and the need to be thorough while at the same time containing costs and avoiding the potential harm inherent in overtesting.
A partial solution is to try to define the immediate risk of not recognizing a life- or organ-threatening disease process that can be suggested by a positive nonspecific test (eg, ANA), and to refine the pretest likelihood of specific diagnoses by obtaining an accurate and complete history and performing a focused physical examination. For example, if we suspect that SLE may be the cause of an initial episode of symptomatic pericarditis, our initial evaluation should focus on the patient’s clinical picture. Is there bitemporal hair-thinning? New-onset Raynaud symptoms? Mild generalized adenopathy or lymphopenia? A borderline-low platelet count, or any proteinuria or microhematuria (which should warrant a prompt examination of a fresh urine sediment sample by a physician at the point of care to look for cellular casts indicative of glomerulonephritis)?
As internists, we should try to fulfill our need to be thorough and compulsive by using our honed skills as careful observers and historians—taking a careful history from the patient and family, performing a focused physical examination, and appropriately using disease-defining or staging tests before ordering less specific serologic or other tests. Practicing medicine in a conscientious and compulsive manner does not mean that every diagnostic possibility must be tested for at initial presentation.
Reading how experienced clinicians approach the problem of pericarditis in a specialized clinic provides a useful prompt to self-assess how we approach analogous clinical scenarios.
Why is obstetrics and gynecology a popular career choice for medical students?
Every year graduating medical students participate in the exciting, challenging, and anxiety-provoking process of applying to residency programs. After thousands of miles of travel, dozens of hotel overnight stays, and many interviews, the students are matched to their residency training site and begin specialty training. The first residency “Match” (conducted by the National Resident Matching Program) occurred in 1952 with 6,000 applicants and 10,400 available PGY-1 positions. In the 2014 Match, 34,270 applicants vied for 26,678 PGY-1 positions.1
Of great interest to medical students and educators are the relative balance of applicants and residency positions in each specialty, and the magnitude of risk that a US medical student will not match to his or her chosen specialty. For students who have devoted years preparing for residency training in a chosen specialty the day they learn that they have not matched is heartbreaking, painful, and a test of their resilience. The Match does sponsor a supplemental offer and acceptance program that helps unmatched applicants to identify unfilled positions. This process helps unmatched applicants to continue their professional development without a delay.
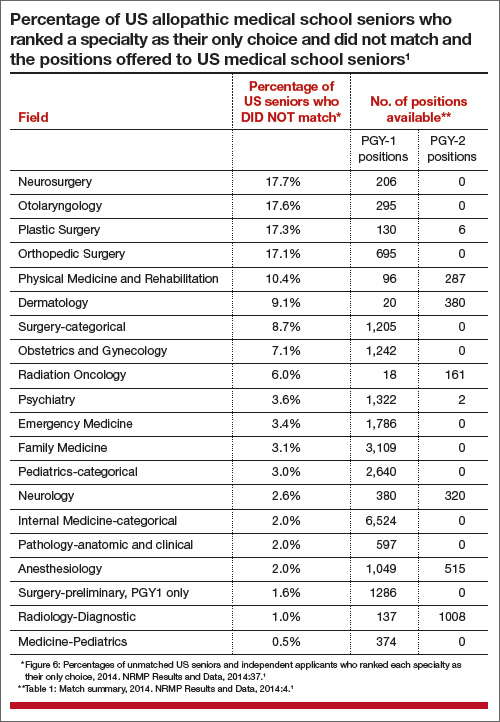
When researching for this editorial, I consulted the National Resident Matching Program’s Results and Data 2014 Main Residency Match.1 The TABLE shows the percentage of US medical school seniors who ranked a specialty as their only choice and did not match. The fields of neurosurgery, otolaryngology, plastic surgery, and orthopedic surgery had the greatest number of US medical school seniors (more than 17%) who ranked a specialty as their only choice and did not match in 2014. The fields of physical medicine and rehabilitation, dermatology, general surgery-categorical, obstetrics and gynecology, and radiation oncology had 6% to 11% of US seniors who ranked a specialty as their only choice not match in 2014. By contrast, almost all US applicants successfully matched in the fields of medicine-pediatrics, diagnostic radiology, anesthesiology, pathology, internal medicine-categorical, neurology, pediatrics-categorical, family medicine, emergency medicine, and psychiatry.
Clearly, obstetrics and gynecology is a popular career choice among medical students. Why might that be so?
Deeply meaningful relationships, continuity of care, plus surgical challenges
Students select a career in obstetrics and gynecology for many reasons. During their clinical experience in obstetrics and gynecology students often experience deeply meaningful relationships with patients at poignant life milestones, including conception, birth, and major surgery. In addition, students recognize that the field offers the opportunity to develop continuity relationships with patients and perform surgical procedures. Primary care specialists often develop deeply rewarding relationships with patients and their families that extend over decades, but they do not perform many surgical procedures. Procedure specialists, including general and orthopedic surgeons, perform hundreds of operations each year, but seldom have the opportunity to develop relationships with patients that last decades. Obstetrics and gynecology offers the combination of long-term continuity relationships with patients and training in surgical procedures.
Many other aspects of the field are attractive to students. Students report that their passion for the field was catalyzed by many factors and experiences, including:
- experiences with obstetricians and gynecologists who were superb role models
- the opportunity to support women and advocate for their needs over an entire lifetime
- the challenge of integrating unique cultural and religious perspectives with the medicine of family planning, sexuality, fertility, and birth
- the scientific and technical complexity of rapidly evolving diagnostic, medical, and surgical treatments, including comprehensive genetic testing and minimally invasive surgery techniques
- the opportunity to care for underserved women both domestically and globally
- delivering babies!
Renew your enthusiasm for our field—mentor!
For practicing obstetricians and gynecologists the combined challenges of complex cases with unfortunate clinical outcomes, ever growing administrative burdens, and the difficulty of balancing work and personal-life may cause them to doubt the wisdom of choosing to train in the field. One of the best ways to erase these doubts is to mentor one of the about
1,250 newly minted physicians who will start their training in obstetrics and gynecology in the summer of 2015 or one of the approximately 1,300 US medical students who will apply to enter the field in 2016.
Medical students have a world of opportunity in front of them, with dozens of exciting career options. The fact that so many students select a career in our field is heartening. These students will become excellent obstetrician-gynecologistsand dedicate themselves to advancingthe health of the 150 million women in the United States.
Would you select a career in obstetrics and gynecology again? Answer the Quick Poll on the home page and see how others have voted.
Why did you select a career in obstetrics and gynecology? Tell us at rbarbieri@frontlinemedcom.com Please include your name and city and state.
Reference
1. National Resident Matching Program. Results and Data: 2014 Main Residency Match. National Resident Matching Program; Washington DC. April 2014.

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Every year graduating medical students participate in the exciting, challenging, and anxiety-provoking process of applying to residency programs. After thousands of miles of travel, dozens of hotel overnight stays, and many interviews, the students are matched to their residency training site and begin specialty training. The first residency “Match” (conducted by the National Resident Matching Program) occurred in 1952 with 6,000 applicants and 10,400 available PGY-1 positions. In the 2014 Match, 34,270 applicants vied for 26,678 PGY-1 positions.1
Of great interest to medical students and educators are the relative balance of applicants and residency positions in each specialty, and the magnitude of risk that a US medical student will not match to his or her chosen specialty. For students who have devoted years preparing for residency training in a chosen specialty the day they learn that they have not matched is heartbreaking, painful, and a test of their resilience. The Match does sponsor a supplemental offer and acceptance program that helps unmatched applicants to identify unfilled positions. This process helps unmatched applicants to continue their professional development without a delay.
When researching for this editorial, I consulted the National Resident Matching Program’s Results and Data 2014 Main Residency Match.1 The TABLE shows the percentage of US medical school seniors who ranked a specialty as their only choice and did not match. The fields of neurosurgery, otolaryngology, plastic surgery, and orthopedic surgery had the greatest number of US medical school seniors (more than 17%) who ranked a specialty as their only choice and did not match in 2014. The fields of physical medicine and rehabilitation, dermatology, general surgery-categorical, obstetrics and gynecology, and radiation oncology had 6% to 11% of US seniors who ranked a specialty as their only choice not match in 2014. By contrast, almost all US applicants successfully matched in the fields of medicine-pediatrics, diagnostic radiology, anesthesiology, pathology, internal medicine-categorical, neurology, pediatrics-categorical, family medicine, emergency medicine, and psychiatry.
Clearly, obstetrics and gynecology is a popular career choice among medical students. Why might that be so?
Deeply meaningful relationships, continuity of care, plus surgical challenges
Students select a career in obstetrics and gynecology for many reasons. During their clinical experience in obstetrics and gynecology students often experience deeply meaningful relationships with patients at poignant life milestones, including conception, birth, and major surgery. In addition, students recognize that the field offers the opportunity to develop continuity relationships with patients and perform surgical procedures. Primary care specialists often develop deeply rewarding relationships with patients and their families that extend over decades, but they do not perform many surgical procedures. Procedure specialists, including general and orthopedic surgeons, perform hundreds of operations each year, but seldom have the opportunity to develop relationships with patients that last decades. Obstetrics and gynecology offers the combination of long-term continuity relationships with patients and training in surgical procedures.
Many other aspects of the field are attractive to students. Students report that their passion for the field was catalyzed by many factors and experiences, including:
- experiences with obstetricians and gynecologists who were superb role models
- the opportunity to support women and advocate for their needs over an entire lifetime
- the challenge of integrating unique cultural and religious perspectives with the medicine of family planning, sexuality, fertility, and birth
- the scientific and technical complexity of rapidly evolving diagnostic, medical, and surgical treatments, including comprehensive genetic testing and minimally invasive surgery techniques
- the opportunity to care for underserved women both domestically and globally
- delivering babies!
Renew your enthusiasm for our field—mentor!
For practicing obstetricians and gynecologists the combined challenges of complex cases with unfortunate clinical outcomes, ever growing administrative burdens, and the difficulty of balancing work and personal-life may cause them to doubt the wisdom of choosing to train in the field. One of the best ways to erase these doubts is to mentor one of the about
1,250 newly minted physicians who will start their training in obstetrics and gynecology in the summer of 2015 or one of the approximately 1,300 US medical students who will apply to enter the field in 2016.
Medical students have a world of opportunity in front of them, with dozens of exciting career options. The fact that so many students select a career in our field is heartening. These students will become excellent obstetrician-gynecologistsand dedicate themselves to advancingthe health of the 150 million women in the United States.
Would you select a career in obstetrics and gynecology again? Answer the Quick Poll on the home page and see how others have voted.
Why did you select a career in obstetrics and gynecology? Tell us at rbarbieri@frontlinemedcom.com Please include your name and city and state.
Every year graduating medical students participate in the exciting, challenging, and anxiety-provoking process of applying to residency programs. After thousands of miles of travel, dozens of hotel overnight stays, and many interviews, the students are matched to their residency training site and begin specialty training. The first residency “Match” (conducted by the National Resident Matching Program) occurred in 1952 with 6,000 applicants and 10,400 available PGY-1 positions. In the 2014 Match, 34,270 applicants vied for 26,678 PGY-1 positions.1
Of great interest to medical students and educators are the relative balance of applicants and residency positions in each specialty, and the magnitude of risk that a US medical student will not match to his or her chosen specialty. For students who have devoted years preparing for residency training in a chosen specialty the day they learn that they have not matched is heartbreaking, painful, and a test of their resilience. The Match does sponsor a supplemental offer and acceptance program that helps unmatched applicants to identify unfilled positions. This process helps unmatched applicants to continue their professional development without a delay.
When researching for this editorial, I consulted the National Resident Matching Program’s Results and Data 2014 Main Residency Match.1 The TABLE shows the percentage of US medical school seniors who ranked a specialty as their only choice and did not match. The fields of neurosurgery, otolaryngology, plastic surgery, and orthopedic surgery had the greatest number of US medical school seniors (more than 17%) who ranked a specialty as their only choice and did not match in 2014. The fields of physical medicine and rehabilitation, dermatology, general surgery-categorical, obstetrics and gynecology, and radiation oncology had 6% to 11% of US seniors who ranked a specialty as their only choice not match in 2014. By contrast, almost all US applicants successfully matched in the fields of medicine-pediatrics, diagnostic radiology, anesthesiology, pathology, internal medicine-categorical, neurology, pediatrics-categorical, family medicine, emergency medicine, and psychiatry.
Clearly, obstetrics and gynecology is a popular career choice among medical students. Why might that be so?
Deeply meaningful relationships, continuity of care, plus surgical challenges
Students select a career in obstetrics and gynecology for many reasons. During their clinical experience in obstetrics and gynecology students often experience deeply meaningful relationships with patients at poignant life milestones, including conception, birth, and major surgery. In addition, students recognize that the field offers the opportunity to develop continuity relationships with patients and perform surgical procedures. Primary care specialists often develop deeply rewarding relationships with patients and their families that extend over decades, but they do not perform many surgical procedures. Procedure specialists, including general and orthopedic surgeons, perform hundreds of operations each year, but seldom have the opportunity to develop relationships with patients that last decades. Obstetrics and gynecology offers the combination of long-term continuity relationships with patients and training in surgical procedures.
Many other aspects of the field are attractive to students. Students report that their passion for the field was catalyzed by many factors and experiences, including:
- experiences with obstetricians and gynecologists who were superb role models
- the opportunity to support women and advocate for their needs over an entire lifetime
- the challenge of integrating unique cultural and religious perspectives with the medicine of family planning, sexuality, fertility, and birth
- the scientific and technical complexity of rapidly evolving diagnostic, medical, and surgical treatments, including comprehensive genetic testing and minimally invasive surgery techniques
- the opportunity to care for underserved women both domestically and globally
- delivering babies!
Renew your enthusiasm for our field—mentor!
For practicing obstetricians and gynecologists the combined challenges of complex cases with unfortunate clinical outcomes, ever growing administrative burdens, and the difficulty of balancing work and personal-life may cause them to doubt the wisdom of choosing to train in the field. One of the best ways to erase these doubts is to mentor one of the about
1,250 newly minted physicians who will start their training in obstetrics and gynecology in the summer of 2015 or one of the approximately 1,300 US medical students who will apply to enter the field in 2016.
Medical students have a world of opportunity in front of them, with dozens of exciting career options. The fact that so many students select a career in our field is heartening. These students will become excellent obstetrician-gynecologistsand dedicate themselves to advancingthe health of the 150 million women in the United States.
Would you select a career in obstetrics and gynecology again? Answer the Quick Poll on the home page and see how others have voted.
Why did you select a career in obstetrics and gynecology? Tell us at rbarbieri@frontlinemedcom.com Please include your name and city and state.
Reference
1. National Resident Matching Program. Results and Data: 2014 Main Residency Match. National Resident Matching Program; Washington DC. April 2014.
Reference
1. National Resident Matching Program. Results and Data: 2014 Main Residency Match. National Resident Matching Program; Washington DC. April 2014.

Psychoneurogastroenterology: The abdominal brain, the microbiome, and psychiatry
This nervous system is located inside the wall of the GI tract, extending from the esophagus to the rectum. Technically, it is known as the enteric nervous system, or ENS, but it has been given other labels, too: “second brain,”2 “abdominal brain,” “other brain,” and “back-up brain.” Its neurologic disorders include abdominal epilepsy, abdominal migraine, and autism with intestinal symptoms, such as chronic enterocolitis.3
Impressive brain-like features
The ENS includes 100 million neurons (same as the spinal cord) with glia-like support cells. It contains >30 neurotransmitters, including several closely linked to psychopathology (serotonin, dopamine, γ-aminobutyric acid, and acetylcholine). The ENS is not part of the autonomic nervous system. It communicates with the brain via the vagus nerve.
A vast system of gut bacteria
The ENS maintains close links with, and is influenced by, the microbiome, an extensive universe of commensal (that is, symbiotic) bacteria in the gut that play a vital role in immune health, brain function, and signaling systems within the CNS. The role of the microbiome in neuropsychiatric disorders has become a sizzling area of research.
The numbers of the microbiome are astonishing, including approximately 1,000 species of bacteria; 100 trillion total bacterial organisms (outnumbering cells of the body by 100-fold); 4 million bacterial genes (compared with 26,000 genes in the host human genome); and a density as high as 1 trillion bacteria in a cubic milliliter—higher than any known microbial system.4
Significant GI−brain connections
It is of great relevance to psychiatry that 90% of the body’s serotonin and 50% of dopamine are found in the GI brain. Selective serotonin reuptake inhibitors often are associated with GI symptoms, such as nausea and diarrhea; antipsychotics, which are dopamine antagonists, are known for antiemetic effects. Clozapine’s potent anticholinergic effects can cause serious ileus.
Things get more interesting when one considers the association of GI disorders and psychiatric symptoms:
Irritable bowel syndrome is associated with panic disorder, generalized anxiety disorder, social phobia, dysthymia, and major depression.
Inflammatory bowel disease (IBD)— such as Crohn’s disease and ulcerative colitis (prevalence ranging from 6% in Canada to 14% in the United States to 46% in Mexico5)—is commonly associated with mood and anxiety disorders and personality changes. The psychiatric manifestations of IBD are so common that the authors of a recent article in World Journal of Gastroenterology urged gastroenterologists to collaborate with psychiatrists when managing IBD.6
Celiac disease has been repeatedly associated with several neuropsychiatric disorders, including ataxia, epilepsy, peripheral neuropathy, headache, anxiety, attention-deficit/hyperactivity disorder, autism spectrum disorder, and schizophrenia.
New, exciting challenges for medical science
There potentially are important implications for possible exploitation of the ENS and the microbiome in the diagnosis and treatment of neuropsychiatric disorders. For example, consider these speculative challenges:
• Can intestinal biopsy reveal neurotransmitter pathology in schizophrenia?
• Can early dopamine deficiency predict Parkinson’s disease, enabling early intervention?
• Can β-amyloid deposits, the degenerative neurologic stigmata of Alzheimer’s disease, be detected in abdominal neurons years before onset of symptoms to allow early intervention?
• Can the ENS become a therapeutic pathway by targeting the various neurotransmitters found there or by engaging the enormous human microbiome to manipulate its beneficial properties?
• Can foods or probiotic supplements be prescribed as microbiomal adjuncts to improve the mood and anxiety spectrum?
One recommendation I came across is that ingesting 10 to 100 million beneficial bacteria, such as Lactobacillus plantarum and Bifidobacterium infantis, might be helpful. Such prescriptions obviously are speculative but also are reasonably testable hypotheses of ways to exploit the “other brain” and the microbiome.
We must summon the guts to seize this opportunity
An independent second brain and a remarkable microbiome appear to be significant evolutionary adaptations and advantages for humans. For too long, neuropsychiatric researchers have ignored the ENS and the microbiome; now, they must focus on how to exploit these entities to yield innovative diagnostic and therapeutic advances. Integrating the ENS and the microbiome and enmeshing them into neuropsychiatric research and clinical applications hold great promise.
The field of psychoneurogastroenterology is in its infancy, but its growth and relevance will be momentous for neuropsychiatry. A major intellectual peristalsis is underway.
1. Robinson B. The abdominal and pelvic brain. Hammond, IN: Frank S. Betz; 1907.
2. Gershon M. The second brain: a groundbreaking new understanding of nervous disorders of the stomach and intestine. New York, NY: HarperCollins Publishers; 1998.
3. McMillin DL, Richards DG, Mein EA, et al. The abdominal brain and enteric nervous system. J Altern Complement Med. 1999;5(6):575-586.
4. Hill JM, Bhattacharjee S, Pogue AI, et al. The gastrointestinal tract microbiome and potential link to Alzheimer’s disease. Front Neurol. 2014;5:43.
5. Olden KW, Lydiard RB. Gastrointestinal disorders. In: Rundell JR, Wise MG. Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Association; 1994.
6. Filipovic BR, Filipovic BF. World J Gastroenterol. 2014;20(13):3552-3563.
This nervous system is located inside the wall of the GI tract, extending from the esophagus to the rectum. Technically, it is known as the enteric nervous system, or ENS, but it has been given other labels, too: “second brain,”2 “abdominal brain,” “other brain,” and “back-up brain.” Its neurologic disorders include abdominal epilepsy, abdominal migraine, and autism with intestinal symptoms, such as chronic enterocolitis.3
Impressive brain-like features
The ENS includes 100 million neurons (same as the spinal cord) with glia-like support cells. It contains >30 neurotransmitters, including several closely linked to psychopathology (serotonin, dopamine, γ-aminobutyric acid, and acetylcholine). The ENS is not part of the autonomic nervous system. It communicates with the brain via the vagus nerve.
A vast system of gut bacteria
The ENS maintains close links with, and is influenced by, the microbiome, an extensive universe of commensal (that is, symbiotic) bacteria in the gut that play a vital role in immune health, brain function, and signaling systems within the CNS. The role of the microbiome in neuropsychiatric disorders has become a sizzling area of research.
The numbers of the microbiome are astonishing, including approximately 1,000 species of bacteria; 100 trillion total bacterial organisms (outnumbering cells of the body by 100-fold); 4 million bacterial genes (compared with 26,000 genes in the host human genome); and a density as high as 1 trillion bacteria in a cubic milliliter—higher than any known microbial system.4
Significant GI−brain connections
It is of great relevance to psychiatry that 90% of the body’s serotonin and 50% of dopamine are found in the GI brain. Selective serotonin reuptake inhibitors often are associated with GI symptoms, such as nausea and diarrhea; antipsychotics, which are dopamine antagonists, are known for antiemetic effects. Clozapine’s potent anticholinergic effects can cause serious ileus.
Things get more interesting when one considers the association of GI disorders and psychiatric symptoms:
Irritable bowel syndrome is associated with panic disorder, generalized anxiety disorder, social phobia, dysthymia, and major depression.
Inflammatory bowel disease (IBD)— such as Crohn’s disease and ulcerative colitis (prevalence ranging from 6% in Canada to 14% in the United States to 46% in Mexico5)—is commonly associated with mood and anxiety disorders and personality changes. The psychiatric manifestations of IBD are so common that the authors of a recent article in World Journal of Gastroenterology urged gastroenterologists to collaborate with psychiatrists when managing IBD.6
Celiac disease has been repeatedly associated with several neuropsychiatric disorders, including ataxia, epilepsy, peripheral neuropathy, headache, anxiety, attention-deficit/hyperactivity disorder, autism spectrum disorder, and schizophrenia.
New, exciting challenges for medical science
There potentially are important implications for possible exploitation of the ENS and the microbiome in the diagnosis and treatment of neuropsychiatric disorders. For example, consider these speculative challenges:
• Can intestinal biopsy reveal neurotransmitter pathology in schizophrenia?
• Can early dopamine deficiency predict Parkinson’s disease, enabling early intervention?
• Can β-amyloid deposits, the degenerative neurologic stigmata of Alzheimer’s disease, be detected in abdominal neurons years before onset of symptoms to allow early intervention?
• Can the ENS become a therapeutic pathway by targeting the various neurotransmitters found there or by engaging the enormous human microbiome to manipulate its beneficial properties?
• Can foods or probiotic supplements be prescribed as microbiomal adjuncts to improve the mood and anxiety spectrum?
One recommendation I came across is that ingesting 10 to 100 million beneficial bacteria, such as Lactobacillus plantarum and Bifidobacterium infantis, might be helpful. Such prescriptions obviously are speculative but also are reasonably testable hypotheses of ways to exploit the “other brain” and the microbiome.
We must summon the guts to seize this opportunity
An independent second brain and a remarkable microbiome appear to be significant evolutionary adaptations and advantages for humans. For too long, neuropsychiatric researchers have ignored the ENS and the microbiome; now, they must focus on how to exploit these entities to yield innovative diagnostic and therapeutic advances. Integrating the ENS and the microbiome and enmeshing them into neuropsychiatric research and clinical applications hold great promise.
The field of psychoneurogastroenterology is in its infancy, but its growth and relevance will be momentous for neuropsychiatry. A major intellectual peristalsis is underway.
This nervous system is located inside the wall of the GI tract, extending from the esophagus to the rectum. Technically, it is known as the enteric nervous system, or ENS, but it has been given other labels, too: “second brain,”2 “abdominal brain,” “other brain,” and “back-up brain.” Its neurologic disorders include abdominal epilepsy, abdominal migraine, and autism with intestinal symptoms, such as chronic enterocolitis.3
Impressive brain-like features
The ENS includes 100 million neurons (same as the spinal cord) with glia-like support cells. It contains >30 neurotransmitters, including several closely linked to psychopathology (serotonin, dopamine, γ-aminobutyric acid, and acetylcholine). The ENS is not part of the autonomic nervous system. It communicates with the brain via the vagus nerve.
A vast system of gut bacteria
The ENS maintains close links with, and is influenced by, the microbiome, an extensive universe of commensal (that is, symbiotic) bacteria in the gut that play a vital role in immune health, brain function, and signaling systems within the CNS. The role of the microbiome in neuropsychiatric disorders has become a sizzling area of research.
The numbers of the microbiome are astonishing, including approximately 1,000 species of bacteria; 100 trillion total bacterial organisms (outnumbering cells of the body by 100-fold); 4 million bacterial genes (compared with 26,000 genes in the host human genome); and a density as high as 1 trillion bacteria in a cubic milliliter—higher than any known microbial system.4
Significant GI−brain connections
It is of great relevance to psychiatry that 90% of the body’s serotonin and 50% of dopamine are found in the GI brain. Selective serotonin reuptake inhibitors often are associated with GI symptoms, such as nausea and diarrhea; antipsychotics, which are dopamine antagonists, are known for antiemetic effects. Clozapine’s potent anticholinergic effects can cause serious ileus.
Things get more interesting when one considers the association of GI disorders and psychiatric symptoms:
Irritable bowel syndrome is associated with panic disorder, generalized anxiety disorder, social phobia, dysthymia, and major depression.
Inflammatory bowel disease (IBD)— such as Crohn’s disease and ulcerative colitis (prevalence ranging from 6% in Canada to 14% in the United States to 46% in Mexico5)—is commonly associated with mood and anxiety disorders and personality changes. The psychiatric manifestations of IBD are so common that the authors of a recent article in World Journal of Gastroenterology urged gastroenterologists to collaborate with psychiatrists when managing IBD.6
Celiac disease has been repeatedly associated with several neuropsychiatric disorders, including ataxia, epilepsy, peripheral neuropathy, headache, anxiety, attention-deficit/hyperactivity disorder, autism spectrum disorder, and schizophrenia.
New, exciting challenges for medical science
There potentially are important implications for possible exploitation of the ENS and the microbiome in the diagnosis and treatment of neuropsychiatric disorders. For example, consider these speculative challenges:
• Can intestinal biopsy reveal neurotransmitter pathology in schizophrenia?
• Can early dopamine deficiency predict Parkinson’s disease, enabling early intervention?
• Can β-amyloid deposits, the degenerative neurologic stigmata of Alzheimer’s disease, be detected in abdominal neurons years before onset of symptoms to allow early intervention?
• Can the ENS become a therapeutic pathway by targeting the various neurotransmitters found there or by engaging the enormous human microbiome to manipulate its beneficial properties?
• Can foods or probiotic supplements be prescribed as microbiomal adjuncts to improve the mood and anxiety spectrum?
One recommendation I came across is that ingesting 10 to 100 million beneficial bacteria, such as Lactobacillus plantarum and Bifidobacterium infantis, might be helpful. Such prescriptions obviously are speculative but also are reasonably testable hypotheses of ways to exploit the “other brain” and the microbiome.
We must summon the guts to seize this opportunity
An independent second brain and a remarkable microbiome appear to be significant evolutionary adaptations and advantages for humans. For too long, neuropsychiatric researchers have ignored the ENS and the microbiome; now, they must focus on how to exploit these entities to yield innovative diagnostic and therapeutic advances. Integrating the ENS and the microbiome and enmeshing them into neuropsychiatric research and clinical applications hold great promise.
The field of psychoneurogastroenterology is in its infancy, but its growth and relevance will be momentous for neuropsychiatry. A major intellectual peristalsis is underway.
1. Robinson B. The abdominal and pelvic brain. Hammond, IN: Frank S. Betz; 1907.
2. Gershon M. The second brain: a groundbreaking new understanding of nervous disorders of the stomach and intestine. New York, NY: HarperCollins Publishers; 1998.
3. McMillin DL, Richards DG, Mein EA, et al. The abdominal brain and enteric nervous system. J Altern Complement Med. 1999;5(6):575-586.
4. Hill JM, Bhattacharjee S, Pogue AI, et al. The gastrointestinal tract microbiome and potential link to Alzheimer’s disease. Front Neurol. 2014;5:43.
5. Olden KW, Lydiard RB. Gastrointestinal disorders. In: Rundell JR, Wise MG. Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Association; 1994.
6. Filipovic BR, Filipovic BF. World J Gastroenterol. 2014;20(13):3552-3563.
1. Robinson B. The abdominal and pelvic brain. Hammond, IN: Frank S. Betz; 1907.
2. Gershon M. The second brain: a groundbreaking new understanding of nervous disorders of the stomach and intestine. New York, NY: HarperCollins Publishers; 1998.
3. McMillin DL, Richards DG, Mein EA, et al. The abdominal brain and enteric nervous system. J Altern Complement Med. 1999;5(6):575-586.
4. Hill JM, Bhattacharjee S, Pogue AI, et al. The gastrointestinal tract microbiome and potential link to Alzheimer’s disease. Front Neurol. 2014;5:43.
5. Olden KW, Lydiard RB. Gastrointestinal disorders. In: Rundell JR, Wise MG. Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Association; 1994.
6. Filipovic BR, Filipovic BF. World J Gastroenterol. 2014;20(13):3552-3563.
Managing change in oncology
The art and science of clinical medicine and editorial policy
The article by Dr. Alison Colantino et al in this issue on when to resume anticoagulation after a hemorrhagic event is relevant to the discussion of clinical decision-making that I started here last month. My thoughts then were prompted by a commentary by Dr. Vinay Prasad on incorporating appropriate study outcomes in clinical decision-making (Cleve Clin J Med 2015; 82:146–150).
In the clinic or hospital, we make many decisions without being able to cite specific applicable clinical studies. I base some decisions on my overall impression from the literature (including formal trials), some on general recall of a specific study (which I hopefully either find time to review afterwards, or ask one of our trainees to read and discuss with our team the next day), and others on my knowledge of clinical guidelines or clearly accepted practice. Most clinical decisions are made without any directly applicable data from available clinical studies. This is the “art” of medicine.
Should this art make its way into our clinical journals, and if so, how extensively, and how should it be framed? It is relatively easy when we are talking about the science of clinical practice. Journals receive the (hopefully complete) data, get peer reviews to improve the paper, and publish it with the authors’ opinions presented in the discussion section. Then, dialogue ensues in the published literature, in educational lectures, and in blogs posted on the Internet. But where does the art go? Does it belong in our traditionally conservative textbooks or newer go-to online resources, which emphasize the need for authors to provide updated specific references for their treatment recommendations? We believe that after our best efforts at peer review it is appropriate to publish it in the CCJM because hopefully it can provide additional perspective on how we deliver care to our patients.
In the arena of new therapies, regulatory approval requires hard data documenting efficacy and safety. And that often leaves me without approved or sometimes even “proven effective” therapies to use when treating patients with relatively uncommon conditions, such as refractory uveitis with threatened visual loss or idiopathic aortitis. Yet I still need to treat the patient.
Another aspect of the art of medicine relates to how best to use therapies that have been approved. We have had antibiotics for many decades, but data are still being generated on how long to treat specific infections, and relatively few scenarios have been studied. Huge media coverage and (mostly) appropriate hype were generated over the need to treat patients with postmenopausal osteoporosis as diagnosed by dual-energy x-ray absorptiometry. But even after evidence emerged regarding atypical femoral fractures in patients receiving long-term bisphosphonate therapy, the question of how long treatment should continue remains more art than science.
The field of anticoagulation has seen many recent advances. We have new heparins, new target-specific oral anticoagulants, and a lot of new science on the natural history of some thrombotic disorders and the efficacy and safety of these new agents. But how long to treat specific thrombotic conditions, which agent to use, how intense the anticoagulation needs to be, when to use bridging therapy, and, as discussed by Dr. Colantino et al, when to resume anticoagulation after a hemorrhagic event mostly remain part of the art of medicine.
I highlight the Colantino paper in the context of both clinical and editorial decision-making because it is an example of experienced clinical authors discussing their solutions to thorny clinical scenarios we often face with inadequate data. While some journals avoid this approach, we embrace the opportunity to provide thoughtful expert opinions to our readers. We push authors from the start of the editorial process and through aggressive peer review to provide evidence to support their practice recommendations when appropriate. But we also encourage them to make recommendations and describe their own decision-making process in situations that may not be fully described in the literature.
Most of our readers do not have ready access to consultants who have had years of experience within multidisciplinary teams at referral institutions regularly managing patients with permutations of these complex clinical problems. Though generic consultation advice must be evaluated within the context of the specific patient, we hope that by framing the clinical issues with relevant clinical science the opinions of experienced authors will be of use in guiding your (and my) approach to similar clinical scenarios.
If you think we are not striking the right balance between the science and the art of medical practice, please let me know.
The article by Dr. Alison Colantino et al in this issue on when to resume anticoagulation after a hemorrhagic event is relevant to the discussion of clinical decision-making that I started here last month. My thoughts then were prompted by a commentary by Dr. Vinay Prasad on incorporating appropriate study outcomes in clinical decision-making (Cleve Clin J Med 2015; 82:146–150).
In the clinic or hospital, we make many decisions without being able to cite specific applicable clinical studies. I base some decisions on my overall impression from the literature (including formal trials), some on general recall of a specific study (which I hopefully either find time to review afterwards, or ask one of our trainees to read and discuss with our team the next day), and others on my knowledge of clinical guidelines or clearly accepted practice. Most clinical decisions are made without any directly applicable data from available clinical studies. This is the “art” of medicine.
Should this art make its way into our clinical journals, and if so, how extensively, and how should it be framed? It is relatively easy when we are talking about the science of clinical practice. Journals receive the (hopefully complete) data, get peer reviews to improve the paper, and publish it with the authors’ opinions presented in the discussion section. Then, dialogue ensues in the published literature, in educational lectures, and in blogs posted on the Internet. But where does the art go? Does it belong in our traditionally conservative textbooks or newer go-to online resources, which emphasize the need for authors to provide updated specific references for their treatment recommendations? We believe that after our best efforts at peer review it is appropriate to publish it in the CCJM because hopefully it can provide additional perspective on how we deliver care to our patients.
In the arena of new therapies, regulatory approval requires hard data documenting efficacy and safety. And that often leaves me without approved or sometimes even “proven effective” therapies to use when treating patients with relatively uncommon conditions, such as refractory uveitis with threatened visual loss or idiopathic aortitis. Yet I still need to treat the patient.
Another aspect of the art of medicine relates to how best to use therapies that have been approved. We have had antibiotics for many decades, but data are still being generated on how long to treat specific infections, and relatively few scenarios have been studied. Huge media coverage and (mostly) appropriate hype were generated over the need to treat patients with postmenopausal osteoporosis as diagnosed by dual-energy x-ray absorptiometry. But even after evidence emerged regarding atypical femoral fractures in patients receiving long-term bisphosphonate therapy, the question of how long treatment should continue remains more art than science.
The field of anticoagulation has seen many recent advances. We have new heparins, new target-specific oral anticoagulants, and a lot of new science on the natural history of some thrombotic disorders and the efficacy and safety of these new agents. But how long to treat specific thrombotic conditions, which agent to use, how intense the anticoagulation needs to be, when to use bridging therapy, and, as discussed by Dr. Colantino et al, when to resume anticoagulation after a hemorrhagic event mostly remain part of the art of medicine.
I highlight the Colantino paper in the context of both clinical and editorial decision-making because it is an example of experienced clinical authors discussing their solutions to thorny clinical scenarios we often face with inadequate data. While some journals avoid this approach, we embrace the opportunity to provide thoughtful expert opinions to our readers. We push authors from the start of the editorial process and through aggressive peer review to provide evidence to support their practice recommendations when appropriate. But we also encourage them to make recommendations and describe their own decision-making process in situations that may not be fully described in the literature.
Most of our readers do not have ready access to consultants who have had years of experience within multidisciplinary teams at referral institutions regularly managing patients with permutations of these complex clinical problems. Though generic consultation advice must be evaluated within the context of the specific patient, we hope that by framing the clinical issues with relevant clinical science the opinions of experienced authors will be of use in guiding your (and my) approach to similar clinical scenarios.
If you think we are not striking the right balance between the science and the art of medical practice, please let me know.
The article by Dr. Alison Colantino et al in this issue on when to resume anticoagulation after a hemorrhagic event is relevant to the discussion of clinical decision-making that I started here last month. My thoughts then were prompted by a commentary by Dr. Vinay Prasad on incorporating appropriate study outcomes in clinical decision-making (Cleve Clin J Med 2015; 82:146–150).
In the clinic or hospital, we make many decisions without being able to cite specific applicable clinical studies. I base some decisions on my overall impression from the literature (including formal trials), some on general recall of a specific study (which I hopefully either find time to review afterwards, or ask one of our trainees to read and discuss with our team the next day), and others on my knowledge of clinical guidelines or clearly accepted practice. Most clinical decisions are made without any directly applicable data from available clinical studies. This is the “art” of medicine.
Should this art make its way into our clinical journals, and if so, how extensively, and how should it be framed? It is relatively easy when we are talking about the science of clinical practice. Journals receive the (hopefully complete) data, get peer reviews to improve the paper, and publish it with the authors’ opinions presented in the discussion section. Then, dialogue ensues in the published literature, in educational lectures, and in blogs posted on the Internet. But where does the art go? Does it belong in our traditionally conservative textbooks or newer go-to online resources, which emphasize the need for authors to provide updated specific references for their treatment recommendations? We believe that after our best efforts at peer review it is appropriate to publish it in the CCJM because hopefully it can provide additional perspective on how we deliver care to our patients.
In the arena of new therapies, regulatory approval requires hard data documenting efficacy and safety. And that often leaves me without approved or sometimes even “proven effective” therapies to use when treating patients with relatively uncommon conditions, such as refractory uveitis with threatened visual loss or idiopathic aortitis. Yet I still need to treat the patient.
Another aspect of the art of medicine relates to how best to use therapies that have been approved. We have had antibiotics for many decades, but data are still being generated on how long to treat specific infections, and relatively few scenarios have been studied. Huge media coverage and (mostly) appropriate hype were generated over the need to treat patients with postmenopausal osteoporosis as diagnosed by dual-energy x-ray absorptiometry. But even after evidence emerged regarding atypical femoral fractures in patients receiving long-term bisphosphonate therapy, the question of how long treatment should continue remains more art than science.
The field of anticoagulation has seen many recent advances. We have new heparins, new target-specific oral anticoagulants, and a lot of new science on the natural history of some thrombotic disorders and the efficacy and safety of these new agents. But how long to treat specific thrombotic conditions, which agent to use, how intense the anticoagulation needs to be, when to use bridging therapy, and, as discussed by Dr. Colantino et al, when to resume anticoagulation after a hemorrhagic event mostly remain part of the art of medicine.
I highlight the Colantino paper in the context of both clinical and editorial decision-making because it is an example of experienced clinical authors discussing their solutions to thorny clinical scenarios we often face with inadequate data. While some journals avoid this approach, we embrace the opportunity to provide thoughtful expert opinions to our readers. We push authors from the start of the editorial process and through aggressive peer review to provide evidence to support their practice recommendations when appropriate. But we also encourage them to make recommendations and describe their own decision-making process in situations that may not be fully described in the literature.
Most of our readers do not have ready access to consultants who have had years of experience within multidisciplinary teams at referral institutions regularly managing patients with permutations of these complex clinical problems. Though generic consultation advice must be evaluated within the context of the specific patient, we hope that by framing the clinical issues with relevant clinical science the opinions of experienced authors will be of use in guiding your (and my) approach to similar clinical scenarios.
If you think we are not striking the right balance between the science and the art of medical practice, please let me know.
Uterus transplantation: Medical breakthrough or surgical folly?
Case: Patient asks for transplantation referral
During an annual ObGyn visit, a 28-year-old G0 with congenital absence of the uterus excitedly tells you about the news report of the first birth following uterus transplantation. She always has dreamed of becoming pregnant, and this medical breakthrough has spurred her imagination of what might be. You ask if she would consider adoption or a gestational carrier. Responding that she prefers to carry her own pregnancy, she asks you to refer her to a uterus transplantation program. You promise to look into this option for her. As she opens the door to leave your office, she mentions that her mother has volunteered to be the uterus donor.
Later, you have misgivings about making a referral for uterus transplantation. You wonder: Is this procedure an appropriate use of health care resources? Do its risks outweigh the benefits?
In September 2014, a 36-year-old Swedish woman gave birth following uterus transplantation. A 61-year-old family friend donated the uterus for the procedure.1 Prior to this breakthrough, women without a uterus had 3 reproductive alternatives: remain childless, adopt a child, or use a gestational carrier to give birth to their child. In many countries and some religions there are prohibitions against the use of a gestational carrier, leaving adoption as the only option to parenthood.
The first successful uterus transplantation did not occur by serendipity; a decade of careful work led to this breakthrough.2–4 Remarkably, it is now proven that this type of transplantation can result in the successful birth of a baby—but at what cost?
The Brännström Uterus Transplantation Program: A medical breakthrough
Dr. Mats Brännström at the University of Gothenburg, Sweden, is the leader of the courageous and innovative team that developed the world’s first successful uterus transplantation program. The team required a broad range of expertise and skills and included physicians, scientists, and support staff from Sahlgrenska University Hospital and Stockholm IVF in Sweden; University of Valencia, Spain; Griffith University, Australia; and the Cleveland Clinic, Florida. Two recent publications report on the outcomes of the first 9 uterus transplants.5,6
The successful protocol. The first step in the program is an exhaustive medical and psychosocial evaluation of the prospective uterus donor and recipient. Among the first 9 uterus recipients, 8 women had congenital absence of the uterus and 1 woman had a hysterectomy for cervical cancer. The uterus donors were mothers (in 5 cases), a mother-in-law, a sister, an aunt, and a friend.
After the recipient is approved for uterus transplantation, she undergoes in vitro fertilization (IVF) with cryopreservation of all embryos. IVF is recommended because it may not be possible to include the fallopian tubes in the uterus transplant or the tubes may not function properly following transplantation. The donor organ is harvested, using a modified radical hysterectomy with extended vascular pedicles, and transplanted into the pelvis of the recipient.
Following transplantation, immunosuppressive medications are prescribed daily to reduce the risk of organ rejection. The recipient is followed on a regular basis with physical examination and cervical biopsy to identify histologic markers of organ rejection. Episodes of rejection are treated with glucocorticoids and adjustment in the dose of immunosuppression medications. Fertility treatment with the recipient’s previously cryopreserved embryo begins 1 year following transplantation.
A unique feature of uterus transplantation is that the organ can be removed after childbearing is complete, thereby limiting lifetime exposure to immunosuppressive medications.
Uterus transplantation: Surgical folly?
Transplantation of a uterus involves major surgery. The inescapable reality is that the procedure will cause complications in some donors and recipients.
Specific complications faced. In the Brännström series, 1 uterus donor developed a postoperative ureterovaginal fistula, likely caused by extensive dissection of her ureters. This donor needed an additional operation to repair the fistula. Two of the 9 uterus transplants failed. One uterus was removed from the recipient 3 days after transplantation due to vascular occlusion and 1 uterus was removed 105 days after transplantation due to chronic infection resistant to antibiotic treatment. Seven of the transplants were successful and functioning in situ 12 months after transplantation as evidenced by regular menstrual bleeding. Five of the 7 recipients had rejection episodes, as demonstrated by the histology of cervix biopsies. Two of the recipients had 3 episodes of rejection. The rejection episodes were treated successfully with glucocorticoids and adjustment of immunosuppression medications.
Pregnancy in women with uterus transplantation is high risk because of the complications caused by immunosuppressive drugs and the high blood flow through the vascular grafts.7–9 In the Brännström series, the agents utilized for immunosuppression included mycophenolate mofetil, azathioprine, tacrolimus, and glucocorticoids. Mycophenolate mofetil is a potent teratogen and routinely is discontinued prior to initiating attempts at pregnancy. Azathioprine is associated with an increased rate of congenital anomalies, but the benefits of this immunosuppressive are believed to outweigh the risks for most pregnant women with an organ transplant. Tacrolimus increases the risk of developing hypertension, preeclampsia, and intrauterine growth restriction during pregnancy.
In the Brännström case report, the woman who became pregnant following uterus transplantation took tacrolimus and azathioprine to prevent organ rejection both before and during her pregnancy. Not unexpectedly, she developed preeclampsia with severe features at 31 weeks and 5 days. After admission to the hospital, a worrisome fetal heart rate pattern developed and a cesarean delivery was performed. The newborn male weighed 1,775 g, and no congenital anomalies were observed. During pregnancy, blood flow to the uterus is in the range of 500 mL/min, the equivalent of 1 unit of whole blood per minute.10 This torrential pulsating flow may increase the risk of a vascular catastrophe such as the rupture of a major artery at one of the graft anastomoses, potentially causing the death of the fetus or mother. Much more experience will be needed to fully characterize the pattern of pregnancy complications that occurs following uterus transplantation.
The cost issue. Uterus transplantation is an extremely expensive medical procedure. In the United States each transplantation is likely to cost hundreds of thousands of dollars. Health care resources used to support uterus transplantation are not available for other pressing medical needs. Given that it is an experimental procedure, it is unlikely that health insurance will reimburse the costs of the medical care. Transplantation programs will need to seek major donors to support the costs, as was done in the Brännström program, or identify patients capable of paying for the transplant. If programs plan to have most patients pay for the procedure, bioethical concerns of equitable access and fair selection of recipients will need to be addressed.
Ethics. Uterus transplantation raises many bioethical concerns and programs need to engage biomedical ethicists to guide their activities.11–13 Careful attention to thorough informed consent, risk-benefit analysis, equitable access, and fair selection of participants will be critical to running an ethical program. To reduce the risks of the procedure, programs likely will explore the use of uteri obtained from women who are brain dead or cadavers to spare altruistic living donors from undergoing hysterectomy surgery.
“Group of fools” or Nobel Prize in wait?
On December 23, 1954, the first successful kidney transplant was performed by Dr. Joseph E. Murray and his team at the Peter Bent Brigham Hospital, a predecessor to the Brigham and Women’s Hospital.14 His small group of physicians worked for years to perfect the kidney transplantation technique in the laboratory prior to attempting the case. A key to their success was the decision to perform the transplant with identical twins as the donor and recipient.
In the 1950s there was great controversy about whether kidney transplantation was a medical breakthrough or surgical folly. The lead surgical team was referred to as the “group of fools” by some colleagues. But Dr. Murray and his team succeeded in their efforts and opened the field of solid organ transplant. Recognizing the importance of his accomplishment, the Nobel Prize Committee awarded Dr. Murray the 1990 Nobel Prize in Physiology or Medicine. Dr. E. Donnell Thomas, a co-recipient of the award, was simultaneously recognized for developing bone marrow transplantation as a treatment for leukemia.
A medical breakthrough…
Organ transplantation medicine initially focused on the treatment of life-threatening diseases, including kidney, heart, lung, and liver failure. With recent innovations in composite tissue transplants, including face and limb, transplantation medicine is evolving to expand its focus to the repair of functional deficits that are not life threatening but do significantly impact quality of life. Uterus transplantation is an example of the new era of using transplants to repair functional deficits. The clinicians and patients involved in these innovative programs are courageous pioneers opening new vistas and helping to realize previously impossible dreams. In our time, many stakeholders are likely to conclude that uterus transplantation is a surgical folly. However, I predict that our children will conclude that uterus transplantation represents a medical breakthrough.
Share your thoughts on this article! Send your Letter to the Editor to Please include your name and the city and state in which you practice.
Weigh in at the Quick Poll on the homepage. Send your answers to these cases and any comments to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Brännström M, Johannesson L, Bokstrom H, et al. Livebirth after uterus transplantation. Lancet. 2015;385(9968):607–616.
2. Johannesson L, Enskog A, Mölne J, et al. Preclinical report on allogeneic uterus transplantation in nonhuman primates. Hum Reprod. 2013;28(1):189–198.
3. Brännström M, Diaz-Garcia C, Hanafy A, Olausson M, Tzakis A. Uterus transplantation: animal research and human possibilities. Fertil Steril. 2012;97(6):1269–1276.
4. Brännström M, Wranning CA, Altchek A. Experimental uterus transplantation. Hum Reprod Update. 2010;16(3):329–345.
5. Brännström M, Johannesson L, Dahm-Kähler P, et al. First clinical uterus transplant trial: a six-month report. Fertil Steril. 2014;101(5):1228–1236.
6. Johannesson L, Kvarnstrom N, Mölne J, et al. Uterus transplantation trial: 1-year outcome. Fertil Steril. 2015;103(1):199–204.
7. Concepcion BP, Schaefer HM. Caring for the pregnant kidney transplant recipient. Clin Transplant. 2011;25(6):821–829.
8. Rupley DM, Janda AM, Kapeles SR, Wilson TM, Berman D, Mathur AK. Preconception counseling, fertility and pregnancy complications after abdominal organ transplantation: a survey and cohort study of 532 recipients. Clin Transplant. 2014;28(9):937–945.
9. McKay DB, Josephson MA. Pregnancy in recipients of solid organs—effects on mother and child. N Engl J Med. 2006;354(12):1281–1293.
10. Metcalfe J, Romney SL, Ramsey LH, Reid DH, Burwell CS. Estimation of uterine blood flow in normal human pregnancy at term. J Clin Invest. 1955;34(11):1632–1638.
11. Olausson M, Johannesson L, Brattgård D, et al. Ethics of uterus transplantation with live donors. Fertil Steril. 2014;102(1):40–43.
12. Del Priore G, Saso S, Meslin EM, et al. Uterine transplantation—a real possibility? The Indianapolis consensus. Hum Reprod. 2013;28(2):288–291.
13. Brosens I, Ghaem-Maghami S, Pijnenborg R. Uterus transplantation in the human: a complex surgical, medical and ethical challenge. Human Reprod. 2013;28(2):292–293.
14. Desai SP, Desai MS, Wood DN, Maddi R, Leeson S, Tilney NL. A semi-centennial report on the participants depicted in Joel Babb’s portrait, “The First Successful Kidney Transplantation”. Am J Transplant. 2007;7(7):1683–1688.

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Case: Patient asks for transplantation referral
During an annual ObGyn visit, a 28-year-old G0 with congenital absence of the uterus excitedly tells you about the news report of the first birth following uterus transplantation. She always has dreamed of becoming pregnant, and this medical breakthrough has spurred her imagination of what might be. You ask if she would consider adoption or a gestational carrier. Responding that she prefers to carry her own pregnancy, she asks you to refer her to a uterus transplantation program. You promise to look into this option for her. As she opens the door to leave your office, she mentions that her mother has volunteered to be the uterus donor.
Later, you have misgivings about making a referral for uterus transplantation. You wonder: Is this procedure an appropriate use of health care resources? Do its risks outweigh the benefits?
In September 2014, a 36-year-old Swedish woman gave birth following uterus transplantation. A 61-year-old family friend donated the uterus for the procedure.1 Prior to this breakthrough, women without a uterus had 3 reproductive alternatives: remain childless, adopt a child, or use a gestational carrier to give birth to their child. In many countries and some religions there are prohibitions against the use of a gestational carrier, leaving adoption as the only option to parenthood.
The first successful uterus transplantation did not occur by serendipity; a decade of careful work led to this breakthrough.2–4 Remarkably, it is now proven that this type of transplantation can result in the successful birth of a baby—but at what cost?
The Brännström Uterus Transplantation Program: A medical breakthrough
Dr. Mats Brännström at the University of Gothenburg, Sweden, is the leader of the courageous and innovative team that developed the world’s first successful uterus transplantation program. The team required a broad range of expertise and skills and included physicians, scientists, and support staff from Sahlgrenska University Hospital and Stockholm IVF in Sweden; University of Valencia, Spain; Griffith University, Australia; and the Cleveland Clinic, Florida. Two recent publications report on the outcomes of the first 9 uterus transplants.5,6
The successful protocol. The first step in the program is an exhaustive medical and psychosocial evaluation of the prospective uterus donor and recipient. Among the first 9 uterus recipients, 8 women had congenital absence of the uterus and 1 woman had a hysterectomy for cervical cancer. The uterus donors were mothers (in 5 cases), a mother-in-law, a sister, an aunt, and a friend.
After the recipient is approved for uterus transplantation, she undergoes in vitro fertilization (IVF) with cryopreservation of all embryos. IVF is recommended because it may not be possible to include the fallopian tubes in the uterus transplant or the tubes may not function properly following transplantation. The donor organ is harvested, using a modified radical hysterectomy with extended vascular pedicles, and transplanted into the pelvis of the recipient.
Following transplantation, immunosuppressive medications are prescribed daily to reduce the risk of organ rejection. The recipient is followed on a regular basis with physical examination and cervical biopsy to identify histologic markers of organ rejection. Episodes of rejection are treated with glucocorticoids and adjustment in the dose of immunosuppression medications. Fertility treatment with the recipient’s previously cryopreserved embryo begins 1 year following transplantation.
A unique feature of uterus transplantation is that the organ can be removed after childbearing is complete, thereby limiting lifetime exposure to immunosuppressive medications.
Uterus transplantation: Surgical folly?
Transplantation of a uterus involves major surgery. The inescapable reality is that the procedure will cause complications in some donors and recipients.
Specific complications faced. In the Brännström series, 1 uterus donor developed a postoperative ureterovaginal fistula, likely caused by extensive dissection of her ureters. This donor needed an additional operation to repair the fistula. Two of the 9 uterus transplants failed. One uterus was removed from the recipient 3 days after transplantation due to vascular occlusion and 1 uterus was removed 105 days after transplantation due to chronic infection resistant to antibiotic treatment. Seven of the transplants were successful and functioning in situ 12 months after transplantation as evidenced by regular menstrual bleeding. Five of the 7 recipients had rejection episodes, as demonstrated by the histology of cervix biopsies. Two of the recipients had 3 episodes of rejection. The rejection episodes were treated successfully with glucocorticoids and adjustment of immunosuppression medications.
Pregnancy in women with uterus transplantation is high risk because of the complications caused by immunosuppressive drugs and the high blood flow through the vascular grafts.7–9 In the Brännström series, the agents utilized for immunosuppression included mycophenolate mofetil, azathioprine, tacrolimus, and glucocorticoids. Mycophenolate mofetil is a potent teratogen and routinely is discontinued prior to initiating attempts at pregnancy. Azathioprine is associated with an increased rate of congenital anomalies, but the benefits of this immunosuppressive are believed to outweigh the risks for most pregnant women with an organ transplant. Tacrolimus increases the risk of developing hypertension, preeclampsia, and intrauterine growth restriction during pregnancy.
In the Brännström case report, the woman who became pregnant following uterus transplantation took tacrolimus and azathioprine to prevent organ rejection both before and during her pregnancy. Not unexpectedly, she developed preeclampsia with severe features at 31 weeks and 5 days. After admission to the hospital, a worrisome fetal heart rate pattern developed and a cesarean delivery was performed. The newborn male weighed 1,775 g, and no congenital anomalies were observed. During pregnancy, blood flow to the uterus is in the range of 500 mL/min, the equivalent of 1 unit of whole blood per minute.10 This torrential pulsating flow may increase the risk of a vascular catastrophe such as the rupture of a major artery at one of the graft anastomoses, potentially causing the death of the fetus or mother. Much more experience will be needed to fully characterize the pattern of pregnancy complications that occurs following uterus transplantation.
The cost issue. Uterus transplantation is an extremely expensive medical procedure. In the United States each transplantation is likely to cost hundreds of thousands of dollars. Health care resources used to support uterus transplantation are not available for other pressing medical needs. Given that it is an experimental procedure, it is unlikely that health insurance will reimburse the costs of the medical care. Transplantation programs will need to seek major donors to support the costs, as was done in the Brännström program, or identify patients capable of paying for the transplant. If programs plan to have most patients pay for the procedure, bioethical concerns of equitable access and fair selection of recipients will need to be addressed.
Ethics. Uterus transplantation raises many bioethical concerns and programs need to engage biomedical ethicists to guide their activities.11–13 Careful attention to thorough informed consent, risk-benefit analysis, equitable access, and fair selection of participants will be critical to running an ethical program. To reduce the risks of the procedure, programs likely will explore the use of uteri obtained from women who are brain dead or cadavers to spare altruistic living donors from undergoing hysterectomy surgery.
“Group of fools” or Nobel Prize in wait?
On December 23, 1954, the first successful kidney transplant was performed by Dr. Joseph E. Murray and his team at the Peter Bent Brigham Hospital, a predecessor to the Brigham and Women’s Hospital.14 His small group of physicians worked for years to perfect the kidney transplantation technique in the laboratory prior to attempting the case. A key to their success was the decision to perform the transplant with identical twins as the donor and recipient.
In the 1950s there was great controversy about whether kidney transplantation was a medical breakthrough or surgical folly. The lead surgical team was referred to as the “group of fools” by some colleagues. But Dr. Murray and his team succeeded in their efforts and opened the field of solid organ transplant. Recognizing the importance of his accomplishment, the Nobel Prize Committee awarded Dr. Murray the 1990 Nobel Prize in Physiology or Medicine. Dr. E. Donnell Thomas, a co-recipient of the award, was simultaneously recognized for developing bone marrow transplantation as a treatment for leukemia.
A medical breakthrough…
Organ transplantation medicine initially focused on the treatment of life-threatening diseases, including kidney, heart, lung, and liver failure. With recent innovations in composite tissue transplants, including face and limb, transplantation medicine is evolving to expand its focus to the repair of functional deficits that are not life threatening but do significantly impact quality of life. Uterus transplantation is an example of the new era of using transplants to repair functional deficits. The clinicians and patients involved in these innovative programs are courageous pioneers opening new vistas and helping to realize previously impossible dreams. In our time, many stakeholders are likely to conclude that uterus transplantation is a surgical folly. However, I predict that our children will conclude that uterus transplantation represents a medical breakthrough.
Share your thoughts on this article! Send your Letter to the Editor to Please include your name and the city and state in which you practice.
Weigh in at the Quick Poll on the homepage. Send your answers to these cases and any comments to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Case: Patient asks for transplantation referral
During an annual ObGyn visit, a 28-year-old G0 with congenital absence of the uterus excitedly tells you about the news report of the first birth following uterus transplantation. She always has dreamed of becoming pregnant, and this medical breakthrough has spurred her imagination of what might be. You ask if she would consider adoption or a gestational carrier. Responding that she prefers to carry her own pregnancy, she asks you to refer her to a uterus transplantation program. You promise to look into this option for her. As she opens the door to leave your office, she mentions that her mother has volunteered to be the uterus donor.
Later, you have misgivings about making a referral for uterus transplantation. You wonder: Is this procedure an appropriate use of health care resources? Do its risks outweigh the benefits?
In September 2014, a 36-year-old Swedish woman gave birth following uterus transplantation. A 61-year-old family friend donated the uterus for the procedure.1 Prior to this breakthrough, women without a uterus had 3 reproductive alternatives: remain childless, adopt a child, or use a gestational carrier to give birth to their child. In many countries and some religions there are prohibitions against the use of a gestational carrier, leaving adoption as the only option to parenthood.
The first successful uterus transplantation did not occur by serendipity; a decade of careful work led to this breakthrough.2–4 Remarkably, it is now proven that this type of transplantation can result in the successful birth of a baby—but at what cost?
The Brännström Uterus Transplantation Program: A medical breakthrough
Dr. Mats Brännström at the University of Gothenburg, Sweden, is the leader of the courageous and innovative team that developed the world’s first successful uterus transplantation program. The team required a broad range of expertise and skills and included physicians, scientists, and support staff from Sahlgrenska University Hospital and Stockholm IVF in Sweden; University of Valencia, Spain; Griffith University, Australia; and the Cleveland Clinic, Florida. Two recent publications report on the outcomes of the first 9 uterus transplants.5,6
The successful protocol. The first step in the program is an exhaustive medical and psychosocial evaluation of the prospective uterus donor and recipient. Among the first 9 uterus recipients, 8 women had congenital absence of the uterus and 1 woman had a hysterectomy for cervical cancer. The uterus donors were mothers (in 5 cases), a mother-in-law, a sister, an aunt, and a friend.
After the recipient is approved for uterus transplantation, she undergoes in vitro fertilization (IVF) with cryopreservation of all embryos. IVF is recommended because it may not be possible to include the fallopian tubes in the uterus transplant or the tubes may not function properly following transplantation. The donor organ is harvested, using a modified radical hysterectomy with extended vascular pedicles, and transplanted into the pelvis of the recipient.
Following transplantation, immunosuppressive medications are prescribed daily to reduce the risk of organ rejection. The recipient is followed on a regular basis with physical examination and cervical biopsy to identify histologic markers of organ rejection. Episodes of rejection are treated with glucocorticoids and adjustment in the dose of immunosuppression medications. Fertility treatment with the recipient’s previously cryopreserved embryo begins 1 year following transplantation.
A unique feature of uterus transplantation is that the organ can be removed after childbearing is complete, thereby limiting lifetime exposure to immunosuppressive medications.
Uterus transplantation: Surgical folly?
Transplantation of a uterus involves major surgery. The inescapable reality is that the procedure will cause complications in some donors and recipients.
Specific complications faced. In the Brännström series, 1 uterus donor developed a postoperative ureterovaginal fistula, likely caused by extensive dissection of her ureters. This donor needed an additional operation to repair the fistula. Two of the 9 uterus transplants failed. One uterus was removed from the recipient 3 days after transplantation due to vascular occlusion and 1 uterus was removed 105 days after transplantation due to chronic infection resistant to antibiotic treatment. Seven of the transplants were successful and functioning in situ 12 months after transplantation as evidenced by regular menstrual bleeding. Five of the 7 recipients had rejection episodes, as demonstrated by the histology of cervix biopsies. Two of the recipients had 3 episodes of rejection. The rejection episodes were treated successfully with glucocorticoids and adjustment of immunosuppression medications.
Pregnancy in women with uterus transplantation is high risk because of the complications caused by immunosuppressive drugs and the high blood flow through the vascular grafts.7–9 In the Brännström series, the agents utilized for immunosuppression included mycophenolate mofetil, azathioprine, tacrolimus, and glucocorticoids. Mycophenolate mofetil is a potent teratogen and routinely is discontinued prior to initiating attempts at pregnancy. Azathioprine is associated with an increased rate of congenital anomalies, but the benefits of this immunosuppressive are believed to outweigh the risks for most pregnant women with an organ transplant. Tacrolimus increases the risk of developing hypertension, preeclampsia, and intrauterine growth restriction during pregnancy.
In the Brännström case report, the woman who became pregnant following uterus transplantation took tacrolimus and azathioprine to prevent organ rejection both before and during her pregnancy. Not unexpectedly, she developed preeclampsia with severe features at 31 weeks and 5 days. After admission to the hospital, a worrisome fetal heart rate pattern developed and a cesarean delivery was performed. The newborn male weighed 1,775 g, and no congenital anomalies were observed. During pregnancy, blood flow to the uterus is in the range of 500 mL/min, the equivalent of 1 unit of whole blood per minute.10 This torrential pulsating flow may increase the risk of a vascular catastrophe such as the rupture of a major artery at one of the graft anastomoses, potentially causing the death of the fetus or mother. Much more experience will be needed to fully characterize the pattern of pregnancy complications that occurs following uterus transplantation.
The cost issue. Uterus transplantation is an extremely expensive medical procedure. In the United States each transplantation is likely to cost hundreds of thousands of dollars. Health care resources used to support uterus transplantation are not available for other pressing medical needs. Given that it is an experimental procedure, it is unlikely that health insurance will reimburse the costs of the medical care. Transplantation programs will need to seek major donors to support the costs, as was done in the Brännström program, or identify patients capable of paying for the transplant. If programs plan to have most patients pay for the procedure, bioethical concerns of equitable access and fair selection of recipients will need to be addressed.
Ethics. Uterus transplantation raises many bioethical concerns and programs need to engage biomedical ethicists to guide their activities.11–13 Careful attention to thorough informed consent, risk-benefit analysis, equitable access, and fair selection of participants will be critical to running an ethical program. To reduce the risks of the procedure, programs likely will explore the use of uteri obtained from women who are brain dead or cadavers to spare altruistic living donors from undergoing hysterectomy surgery.
“Group of fools” or Nobel Prize in wait?
On December 23, 1954, the first successful kidney transplant was performed by Dr. Joseph E. Murray and his team at the Peter Bent Brigham Hospital, a predecessor to the Brigham and Women’s Hospital.14 His small group of physicians worked for years to perfect the kidney transplantation technique in the laboratory prior to attempting the case. A key to their success was the decision to perform the transplant with identical twins as the donor and recipient.
In the 1950s there was great controversy about whether kidney transplantation was a medical breakthrough or surgical folly. The lead surgical team was referred to as the “group of fools” by some colleagues. But Dr. Murray and his team succeeded in their efforts and opened the field of solid organ transplant. Recognizing the importance of his accomplishment, the Nobel Prize Committee awarded Dr. Murray the 1990 Nobel Prize in Physiology or Medicine. Dr. E. Donnell Thomas, a co-recipient of the award, was simultaneously recognized for developing bone marrow transplantation as a treatment for leukemia.
A medical breakthrough…
Organ transplantation medicine initially focused on the treatment of life-threatening diseases, including kidney, heart, lung, and liver failure. With recent innovations in composite tissue transplants, including face and limb, transplantation medicine is evolving to expand its focus to the repair of functional deficits that are not life threatening but do significantly impact quality of life. Uterus transplantation is an example of the new era of using transplants to repair functional deficits. The clinicians and patients involved in these innovative programs are courageous pioneers opening new vistas and helping to realize previously impossible dreams. In our time, many stakeholders are likely to conclude that uterus transplantation is a surgical folly. However, I predict that our children will conclude that uterus transplantation represents a medical breakthrough.
Share your thoughts on this article! Send your Letter to the Editor to Please include your name and the city and state in which you practice.
Weigh in at the Quick Poll on the homepage. Send your answers to these cases and any comments to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Brännström M, Johannesson L, Bokstrom H, et al. Livebirth after uterus transplantation. Lancet. 2015;385(9968):607–616.
2. Johannesson L, Enskog A, Mölne J, et al. Preclinical report on allogeneic uterus transplantation in nonhuman primates. Hum Reprod. 2013;28(1):189–198.
3. Brännström M, Diaz-Garcia C, Hanafy A, Olausson M, Tzakis A. Uterus transplantation: animal research and human possibilities. Fertil Steril. 2012;97(6):1269–1276.
4. Brännström M, Wranning CA, Altchek A. Experimental uterus transplantation. Hum Reprod Update. 2010;16(3):329–345.
5. Brännström M, Johannesson L, Dahm-Kähler P, et al. First clinical uterus transplant trial: a six-month report. Fertil Steril. 2014;101(5):1228–1236.
6. Johannesson L, Kvarnstrom N, Mölne J, et al. Uterus transplantation trial: 1-year outcome. Fertil Steril. 2015;103(1):199–204.
7. Concepcion BP, Schaefer HM. Caring for the pregnant kidney transplant recipient. Clin Transplant. 2011;25(6):821–829.
8. Rupley DM, Janda AM, Kapeles SR, Wilson TM, Berman D, Mathur AK. Preconception counseling, fertility and pregnancy complications after abdominal organ transplantation: a survey and cohort study of 532 recipients. Clin Transplant. 2014;28(9):937–945.
9. McKay DB, Josephson MA. Pregnancy in recipients of solid organs—effects on mother and child. N Engl J Med. 2006;354(12):1281–1293.
10. Metcalfe J, Romney SL, Ramsey LH, Reid DH, Burwell CS. Estimation of uterine blood flow in normal human pregnancy at term. J Clin Invest. 1955;34(11):1632–1638.
11. Olausson M, Johannesson L, Brattgård D, et al. Ethics of uterus transplantation with live donors. Fertil Steril. 2014;102(1):40–43.
12. Del Priore G, Saso S, Meslin EM, et al. Uterine transplantation—a real possibility? The Indianapolis consensus. Hum Reprod. 2013;28(2):288–291.
13. Brosens I, Ghaem-Maghami S, Pijnenborg R. Uterus transplantation in the human: a complex surgical, medical and ethical challenge. Human Reprod. 2013;28(2):292–293.
14. Desai SP, Desai MS, Wood DN, Maddi R, Leeson S, Tilney NL. A semi-centennial report on the participants depicted in Joel Babb’s portrait, “The First Successful Kidney Transplantation”. Am J Transplant. 2007;7(7):1683–1688.
1. Brännström M, Johannesson L, Bokstrom H, et al. Livebirth after uterus transplantation. Lancet. 2015;385(9968):607–616.
2. Johannesson L, Enskog A, Mölne J, et al. Preclinical report on allogeneic uterus transplantation in nonhuman primates. Hum Reprod. 2013;28(1):189–198.
3. Brännström M, Diaz-Garcia C, Hanafy A, Olausson M, Tzakis A. Uterus transplantation: animal research and human possibilities. Fertil Steril. 2012;97(6):1269–1276.
4. Brännström M, Wranning CA, Altchek A. Experimental uterus transplantation. Hum Reprod Update. 2010;16(3):329–345.
5. Brännström M, Johannesson L, Dahm-Kähler P, et al. First clinical uterus transplant trial: a six-month report. Fertil Steril. 2014;101(5):1228–1236.
6. Johannesson L, Kvarnstrom N, Mölne J, et al. Uterus transplantation trial: 1-year outcome. Fertil Steril. 2015;103(1):199–204.
7. Concepcion BP, Schaefer HM. Caring for the pregnant kidney transplant recipient. Clin Transplant. 2011;25(6):821–829.
8. Rupley DM, Janda AM, Kapeles SR, Wilson TM, Berman D, Mathur AK. Preconception counseling, fertility and pregnancy complications after abdominal organ transplantation: a survey and cohort study of 532 recipients. Clin Transplant. 2014;28(9):937–945.
9. McKay DB, Josephson MA. Pregnancy in recipients of solid organs—effects on mother and child. N Engl J Med. 2006;354(12):1281–1293.
10. Metcalfe J, Romney SL, Ramsey LH, Reid DH, Burwell CS. Estimation of uterine blood flow in normal human pregnancy at term. J Clin Invest. 1955;34(11):1632–1638.
11. Olausson M, Johannesson L, Brattgård D, et al. Ethics of uterus transplantation with live donors. Fertil Steril. 2014;102(1):40–43.
12. Del Priore G, Saso S, Meslin EM, et al. Uterine transplantation—a real possibility? The Indianapolis consensus. Hum Reprod. 2013;28(2):288–291.
13. Brosens I, Ghaem-Maghami S, Pijnenborg R. Uterus transplantation in the human: a complex surgical, medical and ethical challenge. Human Reprod. 2013;28(2):292–293.
14. Desai SP, Desai MS, Wood DN, Maddi R, Leeson S, Tilney NL. A semi-centennial report on the participants depicted in Joel Babb’s portrait, “The First Successful Kidney Transplantation”. Am J Transplant. 2007;7(7):1683–1688.
Unmet needs and hassles of psychiatric practice
Recently, my umbrage at these practices soared to a new height when a colleague told me that he had to fight for, and then wait to receive, permission from an insurance employee to increase, by a notch, the maintenance dosage of a long-acting antipsychotic for his patient.
Can anyone justify why an absentee person who has never met the patient should, sight-unseen, second-guess our clinical judgment that a patient’s symptoms are still not well-controlled and require upward adjustment of the dosage? Why are insurance companies allowed to micromanage clinical decision-making? Such outrageous intrusiveness is a signal that insurance companies have “jumped the shark” in their effort to push business interests ahead of the needs of their subscribers.
Whose interests are being put first?
I recall instances when I refused to buckle to pressure from a patient’s third-party payer to switch from 1 antidepressant to another, a move that would save the insurer money but put my patient at risk of relapse. I informed the insurance company representative that my attorney was going to file a lawsuit on behalf of my depressed patient if he were to relapse or attempt suicide because he had been switched from an antidepressant that was working to another that might not.
Fighting back paid off: In each case, I was told the payer would “make an exception” for that patient.
Frustrations of this kind have become commonplace in psychiatric practice. They tend to detract from the stimulating and gratifying aspects of the care we provide, and reinforce the perception that insurance companies’ primary goal is to fatten profits, not facilitate patients’ return to health.
Here are other reasons for chronic frustration in psychiatric practice. They reflect serious, unmet needs that we hope will be resolved soon.
Improved diagnostic schema. We need a valid—and more than simply reliable—evidence-based diagnostic system that is rooted in scientifically established pathophysiology. The basic clinical elements of DSM-5 should be gradually amalgamated with rapidly emerging genetics and biological endophenotypes. The continuum of and boundary between “normal” and “pathologic” human behavior should be further clarified.
Biomarkers. Our field eagerly awaits development of biomarkers (laboratory tests) to bolster psychiatric practice in several ways, including:
• confirming the clinical diagnosis
• identifying biological subtypes
• monitoring response
• guiding selection of drugs
• predicting side effects
• measuring severity of disease.
Elusive parity. We’ve been patient, but we’re tired and angry at empty promises of full parity for psychiatric care. We’ve also had it with the stigmatizing and discriminatory “carve-out” status that allows insurance companies to treat reimbursement for psychiatric services more restrictively than for other medical and surgical specialties. Policy makers must end the egregious discrimination that gives half a loaf to some brain disorders (psychiatric) and a full loaf to other brain disorders (neurologic).
Better medications. We need a stronger commitment from the pharmaceutical industry, on which we rely entirely for development of psychoactive drugs, to wage a relentless war on serious mental illness. The private sector should accelerate translation of groundbreaking neuroscientific discoveries—thanks to research funded by the public sector, such as the National Institutes of Health—into innovative new mechanisms of action. Patients who suffer from psychiatric brain disorders for which there are no approved treatments await that commitment and bold action.
Collaborative care. Psychiatry needs a more consistent, more productive bidirectional relationship with primary care. A stronger bond will improve the care of patients on both sides and would, I believe, increase the satisfaction of clinical practice for both specialists. Because structure can facilitate function, co-locating providers can help achieve this vision.
Legal entanglement. Psychiatry must be unshackled from an oppressive set of laws that tie our hands when we treat patients with brain pathology who are incapable of understanding their illness and their need to be treated. Those laws were imposed long before scientific advances showed that prolonged and untreated episodes of psychosis, mania, depression, and anxiety are associated with neurotoxic processes (neuroinflammation, oxidative and nitrosative stress). Medical urgency and patient protection must trump legalisms, just as unconscious stroke and myocardial infarction patients are treated immediately without filing multiple forms or waiting for a court order.
Another legal beef: We psychiatrists are exasperated with the expanding criminalization of our patients— hapless victims of brain diseases that impair their reality testing and behavior. Should a person who suffers a first epileptic seizure or a stroke while driving and kills the driver of an oncoming car be incarcerated with hardened murderers and rapists and treated for epilepsy in a prison instead of a neurology ward? Our patients belong in a secure hospital, a medical asylum, where they are given compassionate medical care, not the degrading treatment afforded to a felon.
More resources. There is a dire need for psychiatric hospital beds in many parts of the country, because many wards were closed and renovated into more profitable, procedure-oriented specialties. There also is a severe shortage of psychiatrists in our country, as I discussed in my editorial, “Signs, symptoms, and treatment of psychiatrynemia,” (December 2014). The 25% of the population who suffer a mental disorder are clearly underserved at this time.
Furthermore, because today’s research is tomorrow’s new treatment, funding for psychiatric research must increase substantially to find cures and to thus reduce huge direct and indirect costs of mental illness and addictions.
Public enlightenment. A well-informed populace would be a major boon to our sophisticated medical specialty, which remains shrouded by primitive beliefs and archaic attitudes. For many people who desperately need mental health care, negative perceptions of psychiatric disorders and their treatment are a major impediment to seeking help. Psychiatrists can catalyze the process of enlightenment by dedicating time to elevating public understanding of the biology and the medical basis of mental illness.
All this notwithstanding, our work is gratifying
Despite the hassles and unmet needs I’ve enumerated, psychiatry continues to be one of the most exciting fields in medicine. We provide more therapeutic face-time and verbal interactions with our patients than any other medical specialty. Imagine, then, how much more enjoyable psychiatric practice would be if these pesky obstacles were eliminated and the unmet needs of patients and practitioners were addressed.
Recently, my umbrage at these practices soared to a new height when a colleague told me that he had to fight for, and then wait to receive, permission from an insurance employee to increase, by a notch, the maintenance dosage of a long-acting antipsychotic for his patient.
Can anyone justify why an absentee person who has never met the patient should, sight-unseen, second-guess our clinical judgment that a patient’s symptoms are still not well-controlled and require upward adjustment of the dosage? Why are insurance companies allowed to micromanage clinical decision-making? Such outrageous intrusiveness is a signal that insurance companies have “jumped the shark” in their effort to push business interests ahead of the needs of their subscribers.
Whose interests are being put first?
I recall instances when I refused to buckle to pressure from a patient’s third-party payer to switch from 1 antidepressant to another, a move that would save the insurer money but put my patient at risk of relapse. I informed the insurance company representative that my attorney was going to file a lawsuit on behalf of my depressed patient if he were to relapse or attempt suicide because he had been switched from an antidepressant that was working to another that might not.
Fighting back paid off: In each case, I was told the payer would “make an exception” for that patient.
Frustrations of this kind have become commonplace in psychiatric practice. They tend to detract from the stimulating and gratifying aspects of the care we provide, and reinforce the perception that insurance companies’ primary goal is to fatten profits, not facilitate patients’ return to health.
Here are other reasons for chronic frustration in psychiatric practice. They reflect serious, unmet needs that we hope will be resolved soon.
Improved diagnostic schema. We need a valid—and more than simply reliable—evidence-based diagnostic system that is rooted in scientifically established pathophysiology. The basic clinical elements of DSM-5 should be gradually amalgamated with rapidly emerging genetics and biological endophenotypes. The continuum of and boundary between “normal” and “pathologic” human behavior should be further clarified.
Biomarkers. Our field eagerly awaits development of biomarkers (laboratory tests) to bolster psychiatric practice in several ways, including:
• confirming the clinical diagnosis
• identifying biological subtypes
• monitoring response
• guiding selection of drugs
• predicting side effects
• measuring severity of disease.
Elusive parity. We’ve been patient, but we’re tired and angry at empty promises of full parity for psychiatric care. We’ve also had it with the stigmatizing and discriminatory “carve-out” status that allows insurance companies to treat reimbursement for psychiatric services more restrictively than for other medical and surgical specialties. Policy makers must end the egregious discrimination that gives half a loaf to some brain disorders (psychiatric) and a full loaf to other brain disorders (neurologic).
Better medications. We need a stronger commitment from the pharmaceutical industry, on which we rely entirely for development of psychoactive drugs, to wage a relentless war on serious mental illness. The private sector should accelerate translation of groundbreaking neuroscientific discoveries—thanks to research funded by the public sector, such as the National Institutes of Health—into innovative new mechanisms of action. Patients who suffer from psychiatric brain disorders for which there are no approved treatments await that commitment and bold action.
Collaborative care. Psychiatry needs a more consistent, more productive bidirectional relationship with primary care. A stronger bond will improve the care of patients on both sides and would, I believe, increase the satisfaction of clinical practice for both specialists. Because structure can facilitate function, co-locating providers can help achieve this vision.
Legal entanglement. Psychiatry must be unshackled from an oppressive set of laws that tie our hands when we treat patients with brain pathology who are incapable of understanding their illness and their need to be treated. Those laws were imposed long before scientific advances showed that prolonged and untreated episodes of psychosis, mania, depression, and anxiety are associated with neurotoxic processes (neuroinflammation, oxidative and nitrosative stress). Medical urgency and patient protection must trump legalisms, just as unconscious stroke and myocardial infarction patients are treated immediately without filing multiple forms or waiting for a court order.
Another legal beef: We psychiatrists are exasperated with the expanding criminalization of our patients— hapless victims of brain diseases that impair their reality testing and behavior. Should a person who suffers a first epileptic seizure or a stroke while driving and kills the driver of an oncoming car be incarcerated with hardened murderers and rapists and treated for epilepsy in a prison instead of a neurology ward? Our patients belong in a secure hospital, a medical asylum, where they are given compassionate medical care, not the degrading treatment afforded to a felon.
More resources. There is a dire need for psychiatric hospital beds in many parts of the country, because many wards were closed and renovated into more profitable, procedure-oriented specialties. There also is a severe shortage of psychiatrists in our country, as I discussed in my editorial, “Signs, symptoms, and treatment of psychiatrynemia,” (December 2014). The 25% of the population who suffer a mental disorder are clearly underserved at this time.
Furthermore, because today’s research is tomorrow’s new treatment, funding for psychiatric research must increase substantially to find cures and to thus reduce huge direct and indirect costs of mental illness and addictions.
Public enlightenment. A well-informed populace would be a major boon to our sophisticated medical specialty, which remains shrouded by primitive beliefs and archaic attitudes. For many people who desperately need mental health care, negative perceptions of psychiatric disorders and their treatment are a major impediment to seeking help. Psychiatrists can catalyze the process of enlightenment by dedicating time to elevating public understanding of the biology and the medical basis of mental illness.
All this notwithstanding, our work is gratifying
Despite the hassles and unmet needs I’ve enumerated, psychiatry continues to be one of the most exciting fields in medicine. We provide more therapeutic face-time and verbal interactions with our patients than any other medical specialty. Imagine, then, how much more enjoyable psychiatric practice would be if these pesky obstacles were eliminated and the unmet needs of patients and practitioners were addressed.
Recently, my umbrage at these practices soared to a new height when a colleague told me that he had to fight for, and then wait to receive, permission from an insurance employee to increase, by a notch, the maintenance dosage of a long-acting antipsychotic for his patient.
Can anyone justify why an absentee person who has never met the patient should, sight-unseen, second-guess our clinical judgment that a patient’s symptoms are still not well-controlled and require upward adjustment of the dosage? Why are insurance companies allowed to micromanage clinical decision-making? Such outrageous intrusiveness is a signal that insurance companies have “jumped the shark” in their effort to push business interests ahead of the needs of their subscribers.
Whose interests are being put first?
I recall instances when I refused to buckle to pressure from a patient’s third-party payer to switch from 1 antidepressant to another, a move that would save the insurer money but put my patient at risk of relapse. I informed the insurance company representative that my attorney was going to file a lawsuit on behalf of my depressed patient if he were to relapse or attempt suicide because he had been switched from an antidepressant that was working to another that might not.
Fighting back paid off: In each case, I was told the payer would “make an exception” for that patient.
Frustrations of this kind have become commonplace in psychiatric practice. They tend to detract from the stimulating and gratifying aspects of the care we provide, and reinforce the perception that insurance companies’ primary goal is to fatten profits, not facilitate patients’ return to health.
Here are other reasons for chronic frustration in psychiatric practice. They reflect serious, unmet needs that we hope will be resolved soon.
Improved diagnostic schema. We need a valid—and more than simply reliable—evidence-based diagnostic system that is rooted in scientifically established pathophysiology. The basic clinical elements of DSM-5 should be gradually amalgamated with rapidly emerging genetics and biological endophenotypes. The continuum of and boundary between “normal” and “pathologic” human behavior should be further clarified.
Biomarkers. Our field eagerly awaits development of biomarkers (laboratory tests) to bolster psychiatric practice in several ways, including:
• confirming the clinical diagnosis
• identifying biological subtypes
• monitoring response
• guiding selection of drugs
• predicting side effects
• measuring severity of disease.
Elusive parity. We’ve been patient, but we’re tired and angry at empty promises of full parity for psychiatric care. We’ve also had it with the stigmatizing and discriminatory “carve-out” status that allows insurance companies to treat reimbursement for psychiatric services more restrictively than for other medical and surgical specialties. Policy makers must end the egregious discrimination that gives half a loaf to some brain disorders (psychiatric) and a full loaf to other brain disorders (neurologic).
Better medications. We need a stronger commitment from the pharmaceutical industry, on which we rely entirely for development of psychoactive drugs, to wage a relentless war on serious mental illness. The private sector should accelerate translation of groundbreaking neuroscientific discoveries—thanks to research funded by the public sector, such as the National Institutes of Health—into innovative new mechanisms of action. Patients who suffer from psychiatric brain disorders for which there are no approved treatments await that commitment and bold action.
Collaborative care. Psychiatry needs a more consistent, more productive bidirectional relationship with primary care. A stronger bond will improve the care of patients on both sides and would, I believe, increase the satisfaction of clinical practice for both specialists. Because structure can facilitate function, co-locating providers can help achieve this vision.
Legal entanglement. Psychiatry must be unshackled from an oppressive set of laws that tie our hands when we treat patients with brain pathology who are incapable of understanding their illness and their need to be treated. Those laws were imposed long before scientific advances showed that prolonged and untreated episodes of psychosis, mania, depression, and anxiety are associated with neurotoxic processes (neuroinflammation, oxidative and nitrosative stress). Medical urgency and patient protection must trump legalisms, just as unconscious stroke and myocardial infarction patients are treated immediately without filing multiple forms or waiting for a court order.
Another legal beef: We psychiatrists are exasperated with the expanding criminalization of our patients— hapless victims of brain diseases that impair their reality testing and behavior. Should a person who suffers a first epileptic seizure or a stroke while driving and kills the driver of an oncoming car be incarcerated with hardened murderers and rapists and treated for epilepsy in a prison instead of a neurology ward? Our patients belong in a secure hospital, a medical asylum, where they are given compassionate medical care, not the degrading treatment afforded to a felon.
More resources. There is a dire need for psychiatric hospital beds in many parts of the country, because many wards were closed and renovated into more profitable, procedure-oriented specialties. There also is a severe shortage of psychiatrists in our country, as I discussed in my editorial, “Signs, symptoms, and treatment of psychiatrynemia,” (December 2014). The 25% of the population who suffer a mental disorder are clearly underserved at this time.
Furthermore, because today’s research is tomorrow’s new treatment, funding for psychiatric research must increase substantially to find cures and to thus reduce huge direct and indirect costs of mental illness and addictions.
Public enlightenment. A well-informed populace would be a major boon to our sophisticated medical specialty, which remains shrouded by primitive beliefs and archaic attitudes. For many people who desperately need mental health care, negative perceptions of psychiatric disorders and their treatment are a major impediment to seeking help. Psychiatrists can catalyze the process of enlightenment by dedicating time to elevating public understanding of the biology and the medical basis of mental illness.
All this notwithstanding, our work is gratifying
Despite the hassles and unmet needs I’ve enumerated, psychiatry continues to be one of the most exciting fields in medicine. We provide more therapeutic face-time and verbal interactions with our patients than any other medical specialty. Imagine, then, how much more enjoyable psychiatric practice would be if these pesky obstacles were eliminated and the unmet needs of patients and practitioners were addressed.
Precision medicine in the making
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Hysterotomy incision and repair: Many options, many personal preferences
CASE: Your colleague’s hysterotomy practices vary from yours
You are in the hospital on a weekend inducing labor in your patient with hypertension. A colleague asks you to assist at a primary cesarean delivery for failure to progress in the second stage. You are glad to help. During the cesarean delivery, your colleague does not create a bladder flap, makes a superficial incision in the uterus and enters the uterine cavity bluntly with her index finger, uses blunt cephalad-caudad expansion of the uterine incision, and closes the uterine incision in a single-layer of continuous suture.
In your practice your general preference is to routinely dissect a bladder flap, enter the uterus using Allis clamps and sharp dissection; use blunt transverse expansion of the uterine incision; and close the uterine incision in two layers, locking the first layer. You wonder, is there any evidence that there is one best approach to managing the hysterotomy incision?
For many obstetrician-gynecologists, cesarean delivery is the major operation we perform most frequently. In planning and performing a cesarean delivery there are many technical surgical decision points, each with many options. A recent Cochrane review concluded that for most surgical options for uterine incision and closure, short-term maternal outcomes were similar among the options and that surgeons should use the techniques that they prefer and are comfortable performing.1 However, other authorities believe that the available evidence indicates that certain surgical techniques are associated with better maternal outcomes.2,3
In this editorial I focus on the varying surgical options available when performing a low transverse hysterotomy during cesarean delivery and the impact of these choices on maternal outcomes.
The bladder flap—surgeon’s choice
Theoretically, dissecting a bladder flap moves the dome of the bladder away from the anterior surface of the lower uterine segment, thereby protecting it from injury during the hysterotomy incision and repair. Three randomized trials have evaluated maternal outcomes following a hysterotomy with or without a bladder flap. All three trials reported that maternal outcomes were similar whether or not a bladder flap was created.4–6 In one trial, the creation of a bladder flap during a primary cesarean delivery was associated with increased adhesions between the parietal and visceral peritoneum and between the bladder and uterus at a repeat cesarean delivery.5
Some authorities have concluded that in most cesarean deliveries it is not necessary to create a bladder flap because the evidence does not indicate that it improves surgical outcomes.3 However, there may be clinical situations where a bladder flap is warranted. For example, during a repeat cesarean delivery, if the bladder is observed to be advanced high on the anterior uterine wall because of previous uterine surgery, a bladder flap may be helpful to ensure that the hysterotomy incision is performed in the lower uterine segment and not in the thickest, most muscular part of the uterine wall.
A second example is a case of arrested labor in the second stage with a deep transverse arrest of a macrosomic fetus. Lower segment lacerations may occur in this scenario, and some clinicians elect to dissect a bladder flap in anticipation of the risk of multiple extensions and a difficult hysterotomy repair. Since bladder injury occurs in less than 1% of cesarean deliveries, it would be difficult to perform a study with sufficient statistical power to determine whether creating a bladder flap influences the rate of bladder injury.7
Entering the uterine cavity—Try blunt entry
There are few clinical trial data to guide the technique for entering the uterine cavity. A major goal is to minimize the risk of a fetal laceration. One technique to reduce this risk is to superficially incise the uterus with a scalpel and then enter the uterus bluntly with a finger. Both the Misgav Ladach and modified Joel-Cohen techniques for cesarean delivery advocate the use of a superficial incision of the lower uterine segment with blunt entry into the uterine cavity.8,9 Other surgical options for entering the uterine cavity with minimal risk to the fetus include:
- Superficially incise the uterus with a scalpel and then apply Allis clamps to the upper and lower incision. Pull the tissue away from the underlying fetus before incising the final layer of uterine tissue and entering the cavity.10
- Apply the tip of the suction tubing with suction on and gently elevate the tissue trapped in the suction tip, incising the tissue to enter the uterus.
- Use a surgical device designed to reduce fetal lacerations (such as C-SAFE, CooperSurgical) to enter the uterus and extend the hysterotomy incision.11
Expanding the uterine incision—Use blunt expansion
Authors of a recent Cochrane meta-analysis analyzed five randomized controlled trials, involving
2,141 women, that evaluated blunt versus sharp expansion of a low transverse uterine incision.1 There was no difference in maternal febrile morbidity or major morbidity between the two techniques. However, blunt expansion of the uterine incision was associated with slightly less maternal blood loss and a lower risk of maternal blood transfusion than sharp incision (0.7% vs 3.1%).1 In another meta-analysis blunt expansion of the uterine incision with the surgeon’s fingers resulted in a smaller decrease in hematocrit and hemoglobin levels and fewer unintended extensions, but no difference in the rate of blood transfusion.12 Based on these findings some authorities recommend using blunt expansion of the uterine incision when a lower uterine segment incision is performed.3
One study, involving 811 women, compared cephalad-caudad blunt expansion versus transverse blunt expansion of the uterine incision.13 Cephalad-caudad blunt expansion compared with transverse blunt expansion resulted in a trend to less blood loss (398 mL versus 440 mL; P = .09), a significantly lower rate of unintended extension of the uterine incision (3.7% vs 7.4%, P = .03) and fewer cases with blood loss greater than 1,500 mL (0.2% vs 2.0%, P = .04). However, there was no difference in the rate of transfusion (0.7% vs 0.7%, P = 1.0) between cephalad-caudad versus transverse blunt expansion. Based on the results from this one trial, some authorities recommend that cephalad-caudad blunt extension be utilized rather than transverse blunt extension.3
Closing the uterine incision—One or two layers?
In the recent Cochrane meta-analysis, researchers compared outcomes of single-layer and two-layer closure of the uterine incision in 14 studies involving 13,890 women.1 There was no difference in rates of febrile morbidity (5.0% vs 5.1%), wound infection (9.4% vs 9.5%), or blood transfusion (2.1% vs 2.4%) between the two techniques. Authors of another systematic review of 20 trials of single- versus double-layer closure of the uterine incision concluded that, based on the available evidence from randomized trials, single- and double-layer closure appeared to produce similar outcomes.14 These authors cautioned, however, that based on nonrandomized studies, single layer closure might be associated with an increased risk of uterine rupture in a subsequent pregnancy.15,16
A uterine incision that was closed with a locked single-layer closure may be at an especially high risk of rupture during a subsequent trial of labor. In one analysis of relevant reports with heterogeneous study designs, the risk of uterine rupture during a trial of labor after a prior cesarean was 1.8% with a double-layer closure, 3.5% with an unlocked single-layer closure, and 6.2% with a locked single-layer closure.17 My perspective is that a double-layer closure generally is preferred because in a future pregnancy with a planned vaginal delivery, the double-layer closure may be associated with a lower rate of uterine rupture.
Some authorities recommend single-layer uterine closure if the patient is sure that she has no future plans to conceive. For example, a woman who is undergoing a tubal ligation at the time of cesarean delivery may be an optimal candidate for single-layer closure.3
Individualization and innovation in surgical care
Surgeons advance their skills by continually using the best evidence and advice from colleagues to guide changes in their practice. Many clinical situations present unique combinations of medical and anatomic problems, and surgeons need to use both creativity and expert judgment to solve these unique problems. Surgical choices that are guided by both the best evidence and hard-won clinical experience will result in optimal patient outcomes.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Dodd JM, Anderson ER, Gates S, Grivell RM. Surgical techniques for uterine incision and uterine closure at the time of cesarean section. Cochrane Database Sys Rev. 2014;7(3):CD004732.
2. Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery. Am J Obstet Gynecol. 2005;193(5):1607–1617.
3. Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
4. Hohlagschwandtner M, Ruecklinger E, Husslein P, Joura EA. Is the formation of a bladder flap at cesarean necessary? A randomized trial. Obstet Gynecol. 2001;98(6):1089–1092.
5. Malvasi A, Tinelli A, Guido M, et al. Effect of avoiding bladder flap formation in caesarean section on repeat caesarean delivery Eur J Obstet Gynecol. 2011;159(2):300–304.
6. Tuuli MG, Obido AO, Fogertey P, Roehl K, Stamilio D, Macones GA. Utility of the bladder flap at cesarean delivery. A randomized controlled trial. Obstet Gynecol. 2012;119(4):815–821.
7. Cahill AG, Stout MJ, Stamillo DM, Odibo AO, Peipert JF, Macones GA. Risk factors for bladder injury in patients with a prior hysterotomy. Obstet Gynecol. 2008;112(1):116–120.
8. Holmgren G, Sjoholm L, Stark M. The Misgav-Ladach method for cesarean section: method description. Acta Obstet Gynecol Scand. 1999;78(7):615–621.
9. Wallin G, Fall O. Modified Joel-Cohen technique for cesarean delivery. Br J Obstet Gynaecol. 1999;106(3):221–226.
10. Gilstrap LC, Cunningham FG, Van Dorsten JP, eds. Operative Obstetrics, 2nd ed. New York, NY: McGraw Hill; 2002.
11. C SAFE. http://www.csafe.us/. Trumbull, CT: CooperSurgical, Inc.
12. Saad AF, Rahman M, Costantine MM, Saade GR. Blunt versus sharp uterine incision expansion during low transverse cesarean delivery: a metaanalysis. Am J Obstet Gynecol. 2014;211(6):684.e1–e11.
13. Cromi A, Ghezzi F, Di Naro E, Siesto G, Loverro G, Bolis P. Blunt expansion of the low transverse uterine incision at cesarean delivery: a randomized comparison of 2 techniques. Am J Obstet Gynecol. 2008;199(3):292.e1–e6.
14. Roberge S, Demers S, Berghella V, Chaillet N, Moore L, Bujold E. Impact of single- and double-layer closure on adverse outcomes and uterine scar defect: a systematic review and metaanalysis. Am J Obstet Gynecol. 2014; 211(5):453–460.
15. Yasmin S, Sadaf J, Fatima N. Impact of methods for uterine incision closure on repeat cesarean section scar of lower uterine segment. J Coll Physicians Surg Pak. 2011;21(9): 522–526.
16. Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187(5): 1199–1202.
17. Roberge S, Chaillet N, Boutin A, et al. Single- versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet. 2011;115(1): 5–10.

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: Your colleague’s hysterotomy practices vary from yours
You are in the hospital on a weekend inducing labor in your patient with hypertension. A colleague asks you to assist at a primary cesarean delivery for failure to progress in the second stage. You are glad to help. During the cesarean delivery, your colleague does not create a bladder flap, makes a superficial incision in the uterus and enters the uterine cavity bluntly with her index finger, uses blunt cephalad-caudad expansion of the uterine incision, and closes the uterine incision in a single-layer of continuous suture.
In your practice your general preference is to routinely dissect a bladder flap, enter the uterus using Allis clamps and sharp dissection; use blunt transverse expansion of the uterine incision; and close the uterine incision in two layers, locking the first layer. You wonder, is there any evidence that there is one best approach to managing the hysterotomy incision?
For many obstetrician-gynecologists, cesarean delivery is the major operation we perform most frequently. In planning and performing a cesarean delivery there are many technical surgical decision points, each with many options. A recent Cochrane review concluded that for most surgical options for uterine incision and closure, short-term maternal outcomes were similar among the options and that surgeons should use the techniques that they prefer and are comfortable performing.1 However, other authorities believe that the available evidence indicates that certain surgical techniques are associated with better maternal outcomes.2,3
In this editorial I focus on the varying surgical options available when performing a low transverse hysterotomy during cesarean delivery and the impact of these choices on maternal outcomes.
The bladder flap—surgeon’s choice
Theoretically, dissecting a bladder flap moves the dome of the bladder away from the anterior surface of the lower uterine segment, thereby protecting it from injury during the hysterotomy incision and repair. Three randomized trials have evaluated maternal outcomes following a hysterotomy with or without a bladder flap. All three trials reported that maternal outcomes were similar whether or not a bladder flap was created.4–6 In one trial, the creation of a bladder flap during a primary cesarean delivery was associated with increased adhesions between the parietal and visceral peritoneum and between the bladder and uterus at a repeat cesarean delivery.5
Some authorities have concluded that in most cesarean deliveries it is not necessary to create a bladder flap because the evidence does not indicate that it improves surgical outcomes.3 However, there may be clinical situations where a bladder flap is warranted. For example, during a repeat cesarean delivery, if the bladder is observed to be advanced high on the anterior uterine wall because of previous uterine surgery, a bladder flap may be helpful to ensure that the hysterotomy incision is performed in the lower uterine segment and not in the thickest, most muscular part of the uterine wall.
A second example is a case of arrested labor in the second stage with a deep transverse arrest of a macrosomic fetus. Lower segment lacerations may occur in this scenario, and some clinicians elect to dissect a bladder flap in anticipation of the risk of multiple extensions and a difficult hysterotomy repair. Since bladder injury occurs in less than 1% of cesarean deliveries, it would be difficult to perform a study with sufficient statistical power to determine whether creating a bladder flap influences the rate of bladder injury.7
Entering the uterine cavity—Try blunt entry
There are few clinical trial data to guide the technique for entering the uterine cavity. A major goal is to minimize the risk of a fetal laceration. One technique to reduce this risk is to superficially incise the uterus with a scalpel and then enter the uterus bluntly with a finger. Both the Misgav Ladach and modified Joel-Cohen techniques for cesarean delivery advocate the use of a superficial incision of the lower uterine segment with blunt entry into the uterine cavity.8,9 Other surgical options for entering the uterine cavity with minimal risk to the fetus include:
- Superficially incise the uterus with a scalpel and then apply Allis clamps to the upper and lower incision. Pull the tissue away from the underlying fetus before incising the final layer of uterine tissue and entering the cavity.10
- Apply the tip of the suction tubing with suction on and gently elevate the tissue trapped in the suction tip, incising the tissue to enter the uterus.
- Use a surgical device designed to reduce fetal lacerations (such as C-SAFE, CooperSurgical) to enter the uterus and extend the hysterotomy incision.11
Expanding the uterine incision—Use blunt expansion
Authors of a recent Cochrane meta-analysis analyzed five randomized controlled trials, involving
2,141 women, that evaluated blunt versus sharp expansion of a low transverse uterine incision.1 There was no difference in maternal febrile morbidity or major morbidity between the two techniques. However, blunt expansion of the uterine incision was associated with slightly less maternal blood loss and a lower risk of maternal blood transfusion than sharp incision (0.7% vs 3.1%).1 In another meta-analysis blunt expansion of the uterine incision with the surgeon’s fingers resulted in a smaller decrease in hematocrit and hemoglobin levels and fewer unintended extensions, but no difference in the rate of blood transfusion.12 Based on these findings some authorities recommend using blunt expansion of the uterine incision when a lower uterine segment incision is performed.3
One study, involving 811 women, compared cephalad-caudad blunt expansion versus transverse blunt expansion of the uterine incision.13 Cephalad-caudad blunt expansion compared with transverse blunt expansion resulted in a trend to less blood loss (398 mL versus 440 mL; P = .09), a significantly lower rate of unintended extension of the uterine incision (3.7% vs 7.4%, P = .03) and fewer cases with blood loss greater than 1,500 mL (0.2% vs 2.0%, P = .04). However, there was no difference in the rate of transfusion (0.7% vs 0.7%, P = 1.0) between cephalad-caudad versus transverse blunt expansion. Based on the results from this one trial, some authorities recommend that cephalad-caudad blunt extension be utilized rather than transverse blunt extension.3
Closing the uterine incision—One or two layers?
In the recent Cochrane meta-analysis, researchers compared outcomes of single-layer and two-layer closure of the uterine incision in 14 studies involving 13,890 women.1 There was no difference in rates of febrile morbidity (5.0% vs 5.1%), wound infection (9.4% vs 9.5%), or blood transfusion (2.1% vs 2.4%) between the two techniques. Authors of another systematic review of 20 trials of single- versus double-layer closure of the uterine incision concluded that, based on the available evidence from randomized trials, single- and double-layer closure appeared to produce similar outcomes.14 These authors cautioned, however, that based on nonrandomized studies, single layer closure might be associated with an increased risk of uterine rupture in a subsequent pregnancy.15,16
A uterine incision that was closed with a locked single-layer closure may be at an especially high risk of rupture during a subsequent trial of labor. In one analysis of relevant reports with heterogeneous study designs, the risk of uterine rupture during a trial of labor after a prior cesarean was 1.8% with a double-layer closure, 3.5% with an unlocked single-layer closure, and 6.2% with a locked single-layer closure.17 My perspective is that a double-layer closure generally is preferred because in a future pregnancy with a planned vaginal delivery, the double-layer closure may be associated with a lower rate of uterine rupture.
Some authorities recommend single-layer uterine closure if the patient is sure that she has no future plans to conceive. For example, a woman who is undergoing a tubal ligation at the time of cesarean delivery may be an optimal candidate for single-layer closure.3
Individualization and innovation in surgical care
Surgeons advance their skills by continually using the best evidence and advice from colleagues to guide changes in their practice. Many clinical situations present unique combinations of medical and anatomic problems, and surgeons need to use both creativity and expert judgment to solve these unique problems. Surgical choices that are guided by both the best evidence and hard-won clinical experience will result in optimal patient outcomes.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
CASE: Your colleague’s hysterotomy practices vary from yours
You are in the hospital on a weekend inducing labor in your patient with hypertension. A colleague asks you to assist at a primary cesarean delivery for failure to progress in the second stage. You are glad to help. During the cesarean delivery, your colleague does not create a bladder flap, makes a superficial incision in the uterus and enters the uterine cavity bluntly with her index finger, uses blunt cephalad-caudad expansion of the uterine incision, and closes the uterine incision in a single-layer of continuous suture.
In your practice your general preference is to routinely dissect a bladder flap, enter the uterus using Allis clamps and sharp dissection; use blunt transverse expansion of the uterine incision; and close the uterine incision in two layers, locking the first layer. You wonder, is there any evidence that there is one best approach to managing the hysterotomy incision?
For many obstetrician-gynecologists, cesarean delivery is the major operation we perform most frequently. In planning and performing a cesarean delivery there are many technical surgical decision points, each with many options. A recent Cochrane review concluded that for most surgical options for uterine incision and closure, short-term maternal outcomes were similar among the options and that surgeons should use the techniques that they prefer and are comfortable performing.1 However, other authorities believe that the available evidence indicates that certain surgical techniques are associated with better maternal outcomes.2,3
In this editorial I focus on the varying surgical options available when performing a low transverse hysterotomy during cesarean delivery and the impact of these choices on maternal outcomes.
The bladder flap—surgeon’s choice
Theoretically, dissecting a bladder flap moves the dome of the bladder away from the anterior surface of the lower uterine segment, thereby protecting it from injury during the hysterotomy incision and repair. Three randomized trials have evaluated maternal outcomes following a hysterotomy with or without a bladder flap. All three trials reported that maternal outcomes were similar whether or not a bladder flap was created.4–6 In one trial, the creation of a bladder flap during a primary cesarean delivery was associated with increased adhesions between the parietal and visceral peritoneum and between the bladder and uterus at a repeat cesarean delivery.5
Some authorities have concluded that in most cesarean deliveries it is not necessary to create a bladder flap because the evidence does not indicate that it improves surgical outcomes.3 However, there may be clinical situations where a bladder flap is warranted. For example, during a repeat cesarean delivery, if the bladder is observed to be advanced high on the anterior uterine wall because of previous uterine surgery, a bladder flap may be helpful to ensure that the hysterotomy incision is performed in the lower uterine segment and not in the thickest, most muscular part of the uterine wall.
A second example is a case of arrested labor in the second stage with a deep transverse arrest of a macrosomic fetus. Lower segment lacerations may occur in this scenario, and some clinicians elect to dissect a bladder flap in anticipation of the risk of multiple extensions and a difficult hysterotomy repair. Since bladder injury occurs in less than 1% of cesarean deliveries, it would be difficult to perform a study with sufficient statistical power to determine whether creating a bladder flap influences the rate of bladder injury.7
Entering the uterine cavity—Try blunt entry
There are few clinical trial data to guide the technique for entering the uterine cavity. A major goal is to minimize the risk of a fetal laceration. One technique to reduce this risk is to superficially incise the uterus with a scalpel and then enter the uterus bluntly with a finger. Both the Misgav Ladach and modified Joel-Cohen techniques for cesarean delivery advocate the use of a superficial incision of the lower uterine segment with blunt entry into the uterine cavity.8,9 Other surgical options for entering the uterine cavity with minimal risk to the fetus include:
- Superficially incise the uterus with a scalpel and then apply Allis clamps to the upper and lower incision. Pull the tissue away from the underlying fetus before incising the final layer of uterine tissue and entering the cavity.10
- Apply the tip of the suction tubing with suction on and gently elevate the tissue trapped in the suction tip, incising the tissue to enter the uterus.
- Use a surgical device designed to reduce fetal lacerations (such as C-SAFE, CooperSurgical) to enter the uterus and extend the hysterotomy incision.11
Expanding the uterine incision—Use blunt expansion
Authors of a recent Cochrane meta-analysis analyzed five randomized controlled trials, involving
2,141 women, that evaluated blunt versus sharp expansion of a low transverse uterine incision.1 There was no difference in maternal febrile morbidity or major morbidity between the two techniques. However, blunt expansion of the uterine incision was associated with slightly less maternal blood loss and a lower risk of maternal blood transfusion than sharp incision (0.7% vs 3.1%).1 In another meta-analysis blunt expansion of the uterine incision with the surgeon’s fingers resulted in a smaller decrease in hematocrit and hemoglobin levels and fewer unintended extensions, but no difference in the rate of blood transfusion.12 Based on these findings some authorities recommend using blunt expansion of the uterine incision when a lower uterine segment incision is performed.3
One study, involving 811 women, compared cephalad-caudad blunt expansion versus transverse blunt expansion of the uterine incision.13 Cephalad-caudad blunt expansion compared with transverse blunt expansion resulted in a trend to less blood loss (398 mL versus 440 mL; P = .09), a significantly lower rate of unintended extension of the uterine incision (3.7% vs 7.4%, P = .03) and fewer cases with blood loss greater than 1,500 mL (0.2% vs 2.0%, P = .04). However, there was no difference in the rate of transfusion (0.7% vs 0.7%, P = 1.0) between cephalad-caudad versus transverse blunt expansion. Based on the results from this one trial, some authorities recommend that cephalad-caudad blunt extension be utilized rather than transverse blunt extension.3
Closing the uterine incision—One or two layers?
In the recent Cochrane meta-analysis, researchers compared outcomes of single-layer and two-layer closure of the uterine incision in 14 studies involving 13,890 women.1 There was no difference in rates of febrile morbidity (5.0% vs 5.1%), wound infection (9.4% vs 9.5%), or blood transfusion (2.1% vs 2.4%) between the two techniques. Authors of another systematic review of 20 trials of single- versus double-layer closure of the uterine incision concluded that, based on the available evidence from randomized trials, single- and double-layer closure appeared to produce similar outcomes.14 These authors cautioned, however, that based on nonrandomized studies, single layer closure might be associated with an increased risk of uterine rupture in a subsequent pregnancy.15,16
A uterine incision that was closed with a locked single-layer closure may be at an especially high risk of rupture during a subsequent trial of labor. In one analysis of relevant reports with heterogeneous study designs, the risk of uterine rupture during a trial of labor after a prior cesarean was 1.8% with a double-layer closure, 3.5% with an unlocked single-layer closure, and 6.2% with a locked single-layer closure.17 My perspective is that a double-layer closure generally is preferred because in a future pregnancy with a planned vaginal delivery, the double-layer closure may be associated with a lower rate of uterine rupture.
Some authorities recommend single-layer uterine closure if the patient is sure that she has no future plans to conceive. For example, a woman who is undergoing a tubal ligation at the time of cesarean delivery may be an optimal candidate for single-layer closure.3
Individualization and innovation in surgical care
Surgeons advance their skills by continually using the best evidence and advice from colleagues to guide changes in their practice. Many clinical situations present unique combinations of medical and anatomic problems, and surgeons need to use both creativity and expert judgment to solve these unique problems. Surgical choices that are guided by both the best evidence and hard-won clinical experience will result in optimal patient outcomes.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
1. Dodd JM, Anderson ER, Gates S, Grivell RM. Surgical techniques for uterine incision and uterine closure at the time of cesarean section. Cochrane Database Sys Rev. 2014;7(3):CD004732.
2. Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery. Am J Obstet Gynecol. 2005;193(5):1607–1617.
3. Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
4. Hohlagschwandtner M, Ruecklinger E, Husslein P, Joura EA. Is the formation of a bladder flap at cesarean necessary? A randomized trial. Obstet Gynecol. 2001;98(6):1089–1092.
5. Malvasi A, Tinelli A, Guido M, et al. Effect of avoiding bladder flap formation in caesarean section on repeat caesarean delivery Eur J Obstet Gynecol. 2011;159(2):300–304.
6. Tuuli MG, Obido AO, Fogertey P, Roehl K, Stamilio D, Macones GA. Utility of the bladder flap at cesarean delivery. A randomized controlled trial. Obstet Gynecol. 2012;119(4):815–821.
7. Cahill AG, Stout MJ, Stamillo DM, Odibo AO, Peipert JF, Macones GA. Risk factors for bladder injury in patients with a prior hysterotomy. Obstet Gynecol. 2008;112(1):116–120.
8. Holmgren G, Sjoholm L, Stark M. The Misgav-Ladach method for cesarean section: method description. Acta Obstet Gynecol Scand. 1999;78(7):615–621.
9. Wallin G, Fall O. Modified Joel-Cohen technique for cesarean delivery. Br J Obstet Gynaecol. 1999;106(3):221–226.
10. Gilstrap LC, Cunningham FG, Van Dorsten JP, eds. Operative Obstetrics, 2nd ed. New York, NY: McGraw Hill; 2002.
11. C SAFE. http://www.csafe.us/. Trumbull, CT: CooperSurgical, Inc.
12. Saad AF, Rahman M, Costantine MM, Saade GR. Blunt versus sharp uterine incision expansion during low transverse cesarean delivery: a metaanalysis. Am J Obstet Gynecol. 2014;211(6):684.e1–e11.
13. Cromi A, Ghezzi F, Di Naro E, Siesto G, Loverro G, Bolis P. Blunt expansion of the low transverse uterine incision at cesarean delivery: a randomized comparison of 2 techniques. Am J Obstet Gynecol. 2008;199(3):292.e1–e6.
14. Roberge S, Demers S, Berghella V, Chaillet N, Moore L, Bujold E. Impact of single- and double-layer closure on adverse outcomes and uterine scar defect: a systematic review and metaanalysis. Am J Obstet Gynecol. 2014; 211(5):453–460.
15. Yasmin S, Sadaf J, Fatima N. Impact of methods for uterine incision closure on repeat cesarean section scar of lower uterine segment. J Coll Physicians Surg Pak. 2011;21(9): 522–526.
16. Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187(5): 1199–1202.
17. Roberge S, Chaillet N, Boutin A, et al. Single- versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet. 2011;115(1): 5–10.
1. Dodd JM, Anderson ER, Gates S, Grivell RM. Surgical techniques for uterine incision and uterine closure at the time of cesarean section. Cochrane Database Sys Rev. 2014;7(3):CD004732.
2. Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery. Am J Obstet Gynecol. 2005;193(5):1607–1617.
3. Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
4. Hohlagschwandtner M, Ruecklinger E, Husslein P, Joura EA. Is the formation of a bladder flap at cesarean necessary? A randomized trial. Obstet Gynecol. 2001;98(6):1089–1092.
5. Malvasi A, Tinelli A, Guido M, et al. Effect of avoiding bladder flap formation in caesarean section on repeat caesarean delivery Eur J Obstet Gynecol. 2011;159(2):300–304.
6. Tuuli MG, Obido AO, Fogertey P, Roehl K, Stamilio D, Macones GA. Utility of the bladder flap at cesarean delivery. A randomized controlled trial. Obstet Gynecol. 2012;119(4):815–821.
7. Cahill AG, Stout MJ, Stamillo DM, Odibo AO, Peipert JF, Macones GA. Risk factors for bladder injury in patients with a prior hysterotomy. Obstet Gynecol. 2008;112(1):116–120.
8. Holmgren G, Sjoholm L, Stark M. The Misgav-Ladach method for cesarean section: method description. Acta Obstet Gynecol Scand. 1999;78(7):615–621.
9. Wallin G, Fall O. Modified Joel-Cohen technique for cesarean delivery. Br J Obstet Gynaecol. 1999;106(3):221–226.
10. Gilstrap LC, Cunningham FG, Van Dorsten JP, eds. Operative Obstetrics, 2nd ed. New York, NY: McGraw Hill; 2002.
11. C SAFE. http://www.csafe.us/. Trumbull, CT: CooperSurgical, Inc.
12. Saad AF, Rahman M, Costantine MM, Saade GR. Blunt versus sharp uterine incision expansion during low transverse cesarean delivery: a metaanalysis. Am J Obstet Gynecol. 2014;211(6):684.e1–e11.
13. Cromi A, Ghezzi F, Di Naro E, Siesto G, Loverro G, Bolis P. Blunt expansion of the low transverse uterine incision at cesarean delivery: a randomized comparison of 2 techniques. Am J Obstet Gynecol. 2008;199(3):292.e1–e6.
14. Roberge S, Demers S, Berghella V, Chaillet N, Moore L, Bujold E. Impact of single- and double-layer closure on adverse outcomes and uterine scar defect: a systematic review and metaanalysis. Am J Obstet Gynecol. 2014; 211(5):453–460.
15. Yasmin S, Sadaf J, Fatima N. Impact of methods for uterine incision closure on repeat cesarean section scar of lower uterine segment. J Coll Physicians Surg Pak. 2011;21(9): 522–526.
16. Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187(5): 1199–1202.
17. Roberge S, Chaillet N, Boutin A, et al. Single- versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet. 2011;115(1): 5–10.
