User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Study Links Maternal Hidradenitis Suppurativa to Risk for Childhood Morbidity
SAN DIEGO — , and other conditions.
Those are key findings from a longitudinal cohort study that was presented during a poster session at the annual meeting of the American Academy of Dermatology.
“HS is associated with morbidity in women of reproductive age and adverse pregnancy outcomes, [but] its effect on offspring outcomes remains unclear,” corresponding author Kaiyang Li, a third-year medical student at McGill University, Quebec, Canada, and coauthors wrote in their abstract.
To investigate the association between maternal HS and offspring outcomes at birth and with up to 16 years of follow-up, the researchers drew from a longitudinal cohort of 1,275,593 children born in Quebec between April 1, 2006 and March 31, 2022. They matched children with their mothers and used identification numbers to follow the children to note morbidities that led to hospital admissions before age 16 years. The exposure of interest was HS, and the main outcome measure was childhood hospitalizations for respiratory, cardiovascular, metabolic, and other morbidities prior to age 16 years.
Next, they estimated hazard ratios (HR) and 95% CIs for the association of maternal HS with childhood morbidity in adjusted Cox proportional hazards regression models. “As prenatal exposure to hyperandrogenism may influence boys and girls differently, we carried out subgroup analyses stratified by child sex,” they wrote.
The study population included 1283 children whose mothers had HS and 1,274,310 unexposed children. As for infant outcomes, compared with no exposure, maternal HS was associated with an increased risk for preterm birth (relative risk [RR], 1.29; 95% CI, 1,08-1.55), neonatal death (RR, 2.07; 95% CI, 1.03-14.13), birth defects (RR, 1.29; 95% CI, 1.07-1.56), congenital heart defects (RR, 1.57; 95% CI, 1.02-2.44), and orofacial defects (RR 4.29; 95% CI, 1.85-9.97).
As for long-term outcomes in the children, compared with those whose mothers did not have HS, maternal HS was associated with an increased risk for any childhood hospitalization (HR, 1.31; 95% CI, 1.19-1.44), respiratory hospitalization (HR, 1.21; 95% CI, 1.05-1.40), metabolic hospitalization (HR, 2.64; 95% CI, 1.67-4.20), gastrointestinal hospitalization (HR, 1.34; 95% CI, 1.03-1.74), and developmental hospitalization (HR, 1.92; 95% CI, 1.43-2.58).
Commenting on the results after the meeting, Ms. Li said that the findings support the need for timely management of HS in expectant mothers and people planning to conceive, and for “interdisciplinary care and follow up for both the mother and the baby, involving the dermatologist, the obstetrician, and the neonatologist or pediatrician if needed.”
“HS is a multidisciplinary disease, plain and simple,” Adam Friedman, MD, professor and chair of dermatology, George Washington University, Washington, who was asked to comment on the study, said in an interview. “This study highlights the importance of collaboration between dermatology and obstetrician-gynecologist given the potential negative pregnancy outcomes, but to me raising alarm bells given the known gaps and delays in diagnosis matched to disease onset,” said Dr. Friedman, who was not involved with the study. “We need to do better to ensure the safety of both patient and patient-to-be.”
The researchers reported having no financial disclosures. The abstract was selected as the second-place winner in the AAD’s poster competition. Dr. Friedman has no relevant disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — , and other conditions.
Those are key findings from a longitudinal cohort study that was presented during a poster session at the annual meeting of the American Academy of Dermatology.
“HS is associated with morbidity in women of reproductive age and adverse pregnancy outcomes, [but] its effect on offspring outcomes remains unclear,” corresponding author Kaiyang Li, a third-year medical student at McGill University, Quebec, Canada, and coauthors wrote in their abstract.
To investigate the association between maternal HS and offspring outcomes at birth and with up to 16 years of follow-up, the researchers drew from a longitudinal cohort of 1,275,593 children born in Quebec between April 1, 2006 and March 31, 2022. They matched children with their mothers and used identification numbers to follow the children to note morbidities that led to hospital admissions before age 16 years. The exposure of interest was HS, and the main outcome measure was childhood hospitalizations for respiratory, cardiovascular, metabolic, and other morbidities prior to age 16 years.
Next, they estimated hazard ratios (HR) and 95% CIs for the association of maternal HS with childhood morbidity in adjusted Cox proportional hazards regression models. “As prenatal exposure to hyperandrogenism may influence boys and girls differently, we carried out subgroup analyses stratified by child sex,” they wrote.
The study population included 1283 children whose mothers had HS and 1,274,310 unexposed children. As for infant outcomes, compared with no exposure, maternal HS was associated with an increased risk for preterm birth (relative risk [RR], 1.29; 95% CI, 1,08-1.55), neonatal death (RR, 2.07; 95% CI, 1.03-14.13), birth defects (RR, 1.29; 95% CI, 1.07-1.56), congenital heart defects (RR, 1.57; 95% CI, 1.02-2.44), and orofacial defects (RR 4.29; 95% CI, 1.85-9.97).
As for long-term outcomes in the children, compared with those whose mothers did not have HS, maternal HS was associated with an increased risk for any childhood hospitalization (HR, 1.31; 95% CI, 1.19-1.44), respiratory hospitalization (HR, 1.21; 95% CI, 1.05-1.40), metabolic hospitalization (HR, 2.64; 95% CI, 1.67-4.20), gastrointestinal hospitalization (HR, 1.34; 95% CI, 1.03-1.74), and developmental hospitalization (HR, 1.92; 95% CI, 1.43-2.58).
Commenting on the results after the meeting, Ms. Li said that the findings support the need for timely management of HS in expectant mothers and people planning to conceive, and for “interdisciplinary care and follow up for both the mother and the baby, involving the dermatologist, the obstetrician, and the neonatologist or pediatrician if needed.”
“HS is a multidisciplinary disease, plain and simple,” Adam Friedman, MD, professor and chair of dermatology, George Washington University, Washington, who was asked to comment on the study, said in an interview. “This study highlights the importance of collaboration between dermatology and obstetrician-gynecologist given the potential negative pregnancy outcomes, but to me raising alarm bells given the known gaps and delays in diagnosis matched to disease onset,” said Dr. Friedman, who was not involved with the study. “We need to do better to ensure the safety of both patient and patient-to-be.”
The researchers reported having no financial disclosures. The abstract was selected as the second-place winner in the AAD’s poster competition. Dr. Friedman has no relevant disclosures.
A version of this article appeared on Medscape.com.
SAN DIEGO — , and other conditions.
Those are key findings from a longitudinal cohort study that was presented during a poster session at the annual meeting of the American Academy of Dermatology.
“HS is associated with morbidity in women of reproductive age and adverse pregnancy outcomes, [but] its effect on offspring outcomes remains unclear,” corresponding author Kaiyang Li, a third-year medical student at McGill University, Quebec, Canada, and coauthors wrote in their abstract.
To investigate the association between maternal HS and offspring outcomes at birth and with up to 16 years of follow-up, the researchers drew from a longitudinal cohort of 1,275,593 children born in Quebec between April 1, 2006 and March 31, 2022. They matched children with their mothers and used identification numbers to follow the children to note morbidities that led to hospital admissions before age 16 years. The exposure of interest was HS, and the main outcome measure was childhood hospitalizations for respiratory, cardiovascular, metabolic, and other morbidities prior to age 16 years.
Next, they estimated hazard ratios (HR) and 95% CIs for the association of maternal HS with childhood morbidity in adjusted Cox proportional hazards regression models. “As prenatal exposure to hyperandrogenism may influence boys and girls differently, we carried out subgroup analyses stratified by child sex,” they wrote.
The study population included 1283 children whose mothers had HS and 1,274,310 unexposed children. As for infant outcomes, compared with no exposure, maternal HS was associated with an increased risk for preterm birth (relative risk [RR], 1.29; 95% CI, 1,08-1.55), neonatal death (RR, 2.07; 95% CI, 1.03-14.13), birth defects (RR, 1.29; 95% CI, 1.07-1.56), congenital heart defects (RR, 1.57; 95% CI, 1.02-2.44), and orofacial defects (RR 4.29; 95% CI, 1.85-9.97).
As for long-term outcomes in the children, compared with those whose mothers did not have HS, maternal HS was associated with an increased risk for any childhood hospitalization (HR, 1.31; 95% CI, 1.19-1.44), respiratory hospitalization (HR, 1.21; 95% CI, 1.05-1.40), metabolic hospitalization (HR, 2.64; 95% CI, 1.67-4.20), gastrointestinal hospitalization (HR, 1.34; 95% CI, 1.03-1.74), and developmental hospitalization (HR, 1.92; 95% CI, 1.43-2.58).
Commenting on the results after the meeting, Ms. Li said that the findings support the need for timely management of HS in expectant mothers and people planning to conceive, and for “interdisciplinary care and follow up for both the mother and the baby, involving the dermatologist, the obstetrician, and the neonatologist or pediatrician if needed.”
“HS is a multidisciplinary disease, plain and simple,” Adam Friedman, MD, professor and chair of dermatology, George Washington University, Washington, who was asked to comment on the study, said in an interview. “This study highlights the importance of collaboration between dermatology and obstetrician-gynecologist given the potential negative pregnancy outcomes, but to me raising alarm bells given the known gaps and delays in diagnosis matched to disease onset,” said Dr. Friedman, who was not involved with the study. “We need to do better to ensure the safety of both patient and patient-to-be.”
The researchers reported having no financial disclosures. The abstract was selected as the second-place winner in the AAD’s poster competition. Dr. Friedman has no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Acne in Transmasculine Patients: Management Recommendations
SAN DIEGO — , a dermatologist told colleagues in a session at the American Academy of Dermatology annual meeting.
In these patients, treatment of acne is crucial, said Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “These are patients who are suffering and reporting that they’re having mental health impacts” related to acne.

In transmasculine patients — those who were biologically female at birth but identify as masculine — testosterone therapy greatly boosts the risk for acne, even in adults who are long past adolescence, Dr. Yeung said. Data suggest that acne appears within the first 6 months after testosterone therapy begins, he said, “and the maximal and complete effect occurs within 1-2 years.”
A 2021 study tracked 988 transgender patients receiving testosterone at Fenway Health in Boston and found that 31% had a diagnosis of acne, up from 6.3% prior to taking hormones. And 2 years following the start of therapy, 25.1% had acne, with cases especially common among those aged 18-20.75 years (29.6%). Even among those aged 28.25-66.5 years, 17.1% had acne.
Transmasculine patients may develop acne in areas across the body “in places that you normally won’t see by just looking at the patient,” Dr. Yeung said. Excoriation in addition to comedones, papules, pustules, and nodules can be common, he added.
Dr. Yeung highlighted a 2019 study of transgender men that linked higher levels of acne to higher levels of serum testosterone, higher body mass index, and current smoking. And in a 2014 study, 6% of 50 transmasculine patients had moderate to severe acne after an average of 10 years on testosterone therapy.
A 2020 study of 696 transgender adults surveyed in California and Georgia found that 14% of transmasculine patients had moderate to severe acne — two thirds attributed it to hormone therapy — vs 1% of transfeminine patients, said Dr. Yeung, the lead author of the study. However, transmasculine patients were less likely to have seen a dermatologist.
Dr. Yeung also highlighted a 2021 study he coauthored that linked current moderate to severe acne in transmasculine patients taking testosterone to higher levels of depression and anxiety vs counterparts who had never had those forms of acne.
Another factor affecting acne in transmasculine patients is the use of chest binders to reduce breast size. “Wearing a chest binder is really helpful for a lot of our patients and is associated with improved self-esteem, mood, mental health, and safety in public,” Dr. Yeung said. However, the binders can contribute to skin problems.
Dr. Yeung said he and his colleagues emphasize the importance of breathable material in binders and suggest to patients that they not wear them when they’re in “safe spaces.”
Isotretinoin, Contraception Considerations
As for treatment of acne in transgender patients, Dr. Yeung cautioned colleagues to not automatically reject isotretinoin as an option for transgender patients who have a history of depression. Dermatologists may be tempted to avoid the drug in these patients because of its link to suicide, he said. (This apparent association has long been debated.) But, Dr. Yeung said, it’s important to consider that many of these patients suffered from anxiety and depression because of the lack of access to proper gender-reassignment treatment.
When using isotretinoin, he emphasized, it’s crucial to consider whether transmasculine patients could become pregnant while on this therapy. Consider whether the patient has the organs needed to become pregnant and ask questions about the potential that they could be impregnated.
“Remember that sexual behavior is different from gender identity,” Dr. Yeung said. A transmasculine person with a uterus and vagina, for example, may still have vaginal intercourse with males and potentially become pregnant. “So, we need to assess what kind of sexual behavior our patients are taking part in.”
Contraceptives such as intrauterine devices, implants, and injectable options may be helpful for transmasculine patients because they can reduce menstrual symptoms like spotting that can be distressing to them, he said. By helping a patient take a contraceptive, “you may actually be helping with their gender dysphoria and helping them get on isotretinoin.”
Dr. Yeung disclosed fees from JAMA and American Academy of Dermatology; grants/research funding from the American Acne & Rosacea Society, Dermatology Foundation, Department of Veterans Affairs, National Eczema Association, and National Institutes of Health; and speaker/faculty education honoraria from Dermatology Digest.
A version of this article appeared on Medscape.com.
SAN DIEGO — , a dermatologist told colleagues in a session at the American Academy of Dermatology annual meeting.
In these patients, treatment of acne is crucial, said Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “These are patients who are suffering and reporting that they’re having mental health impacts” related to acne.
In transmasculine patients — those who were biologically female at birth but identify as masculine — testosterone therapy greatly boosts the risk for acne, even in adults who are long past adolescence, Dr. Yeung said. Data suggest that acne appears within the first 6 months after testosterone therapy begins, he said, “and the maximal and complete effect occurs within 1-2 years.”
A 2021 study tracked 988 transgender patients receiving testosterone at Fenway Health in Boston and found that 31% had a diagnosis of acne, up from 6.3% prior to taking hormones. And 2 years following the start of therapy, 25.1% had acne, with cases especially common among those aged 18-20.75 years (29.6%). Even among those aged 28.25-66.5 years, 17.1% had acne.
Transmasculine patients may develop acne in areas across the body “in places that you normally won’t see by just looking at the patient,” Dr. Yeung said. Excoriation in addition to comedones, papules, pustules, and nodules can be common, he added.
Dr. Yeung highlighted a 2019 study of transgender men that linked higher levels of acne to higher levels of serum testosterone, higher body mass index, and current smoking. And in a 2014 study, 6% of 50 transmasculine patients had moderate to severe acne after an average of 10 years on testosterone therapy.
A 2020 study of 696 transgender adults surveyed in California and Georgia found that 14% of transmasculine patients had moderate to severe acne — two thirds attributed it to hormone therapy — vs 1% of transfeminine patients, said Dr. Yeung, the lead author of the study. However, transmasculine patients were less likely to have seen a dermatologist.
Dr. Yeung also highlighted a 2021 study he coauthored that linked current moderate to severe acne in transmasculine patients taking testosterone to higher levels of depression and anxiety vs counterparts who had never had those forms of acne.
Another factor affecting acne in transmasculine patients is the use of chest binders to reduce breast size. “Wearing a chest binder is really helpful for a lot of our patients and is associated with improved self-esteem, mood, mental health, and safety in public,” Dr. Yeung said. However, the binders can contribute to skin problems.
Dr. Yeung said he and his colleagues emphasize the importance of breathable material in binders and suggest to patients that they not wear them when they’re in “safe spaces.”
Isotretinoin, Contraception Considerations
As for treatment of acne in transgender patients, Dr. Yeung cautioned colleagues to not automatically reject isotretinoin as an option for transgender patients who have a history of depression. Dermatologists may be tempted to avoid the drug in these patients because of its link to suicide, he said. (This apparent association has long been debated.) But, Dr. Yeung said, it’s important to consider that many of these patients suffered from anxiety and depression because of the lack of access to proper gender-reassignment treatment.
When using isotretinoin, he emphasized, it’s crucial to consider whether transmasculine patients could become pregnant while on this therapy. Consider whether the patient has the organs needed to become pregnant and ask questions about the potential that they could be impregnated.
“Remember that sexual behavior is different from gender identity,” Dr. Yeung said. A transmasculine person with a uterus and vagina, for example, may still have vaginal intercourse with males and potentially become pregnant. “So, we need to assess what kind of sexual behavior our patients are taking part in.”
Contraceptives such as intrauterine devices, implants, and injectable options may be helpful for transmasculine patients because they can reduce menstrual symptoms like spotting that can be distressing to them, he said. By helping a patient take a contraceptive, “you may actually be helping with their gender dysphoria and helping them get on isotretinoin.”
Dr. Yeung disclosed fees from JAMA and American Academy of Dermatology; grants/research funding from the American Acne & Rosacea Society, Dermatology Foundation, Department of Veterans Affairs, National Eczema Association, and National Institutes of Health; and speaker/faculty education honoraria from Dermatology Digest.
A version of this article appeared on Medscape.com.
SAN DIEGO — , a dermatologist told colleagues in a session at the American Academy of Dermatology annual meeting.
In these patients, treatment of acne is crucial, said Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “These are patients who are suffering and reporting that they’re having mental health impacts” related to acne.
In transmasculine patients — those who were biologically female at birth but identify as masculine — testosterone therapy greatly boosts the risk for acne, even in adults who are long past adolescence, Dr. Yeung said. Data suggest that acne appears within the first 6 months after testosterone therapy begins, he said, “and the maximal and complete effect occurs within 1-2 years.”
A 2021 study tracked 988 transgender patients receiving testosterone at Fenway Health in Boston and found that 31% had a diagnosis of acne, up from 6.3% prior to taking hormones. And 2 years following the start of therapy, 25.1% had acne, with cases especially common among those aged 18-20.75 years (29.6%). Even among those aged 28.25-66.5 years, 17.1% had acne.
Transmasculine patients may develop acne in areas across the body “in places that you normally won’t see by just looking at the patient,” Dr. Yeung said. Excoriation in addition to comedones, papules, pustules, and nodules can be common, he added.
Dr. Yeung highlighted a 2019 study of transgender men that linked higher levels of acne to higher levels of serum testosterone, higher body mass index, and current smoking. And in a 2014 study, 6% of 50 transmasculine patients had moderate to severe acne after an average of 10 years on testosterone therapy.
A 2020 study of 696 transgender adults surveyed in California and Georgia found that 14% of transmasculine patients had moderate to severe acne — two thirds attributed it to hormone therapy — vs 1% of transfeminine patients, said Dr. Yeung, the lead author of the study. However, transmasculine patients were less likely to have seen a dermatologist.
Dr. Yeung also highlighted a 2021 study he coauthored that linked current moderate to severe acne in transmasculine patients taking testosterone to higher levels of depression and anxiety vs counterparts who had never had those forms of acne.
Another factor affecting acne in transmasculine patients is the use of chest binders to reduce breast size. “Wearing a chest binder is really helpful for a lot of our patients and is associated with improved self-esteem, mood, mental health, and safety in public,” Dr. Yeung said. However, the binders can contribute to skin problems.
Dr. Yeung said he and his colleagues emphasize the importance of breathable material in binders and suggest to patients that they not wear them when they’re in “safe spaces.”
Isotretinoin, Contraception Considerations
As for treatment of acne in transgender patients, Dr. Yeung cautioned colleagues to not automatically reject isotretinoin as an option for transgender patients who have a history of depression. Dermatologists may be tempted to avoid the drug in these patients because of its link to suicide, he said. (This apparent association has long been debated.) But, Dr. Yeung said, it’s important to consider that many of these patients suffered from anxiety and depression because of the lack of access to proper gender-reassignment treatment.
When using isotretinoin, he emphasized, it’s crucial to consider whether transmasculine patients could become pregnant while on this therapy. Consider whether the patient has the organs needed to become pregnant and ask questions about the potential that they could be impregnated.
“Remember that sexual behavior is different from gender identity,” Dr. Yeung said. A transmasculine person with a uterus and vagina, for example, may still have vaginal intercourse with males and potentially become pregnant. “So, we need to assess what kind of sexual behavior our patients are taking part in.”
Contraceptives such as intrauterine devices, implants, and injectable options may be helpful for transmasculine patients because they can reduce menstrual symptoms like spotting that can be distressing to them, he said. By helping a patient take a contraceptive, “you may actually be helping with their gender dysphoria and helping them get on isotretinoin.”
Dr. Yeung disclosed fees from JAMA and American Academy of Dermatology; grants/research funding from the American Acne & Rosacea Society, Dermatology Foundation, Department of Veterans Affairs, National Eczema Association, and National Institutes of Health; and speaker/faculty education honoraria from Dermatology Digest.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Novel Agent Shows Promise for Hidradenitis Suppurativa
SAN DIEGO — After 24 weeks of treatment with subcutaneously administered relative to baseline, results from a randomized clinical trial showed.
Sonelokimab is a novel humanized nanobody that selectively binds to interleukin (IL)-17A and IL-17F, presenting author Brian Kirby, MD, a dermatologist at St. Vincent’s Private Hospital, Dublin, Ireland, said during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology. Sonelokimab is smaller than traditional monoclonal antibodies, he said, “which means it may be able to penetrate tissues better and stay there longer.” It is being developed by MoonLake Immunotherapeutics, based in Zug, Switzerland

According to a press release from the company, nanobodies represent a new generation of targeted therapies derived from antibodies. They consist of one or more domains based on the small antigen-binding variable regions of heavy-chain-only antibodies.
In a phase 2 study known as the MIRA trial, researchers recruited 234 patients with moderate to severe HS to evaluate two different doses of sonelokimab (120 mg and 240 mg every 2 weeks) with a placebo control arm and adalimumab as an active reference arm. The primary endpoint of was the percentage of participants who achieved a HiSCR75. The study population included adults with Hurley Stage II or III HS who had HS lesions in 2 or more anatomical areas and a total abscess and inflammatory nodule (AN) count of 5 or more lesions; and had been treated with 2 or fewer biologics.
Dr. Kirby reported results from 67 patients in the sonelokimab 120 mg arm, 66 in the sonelokimab 240 mg arm, and 39 in the placebo arm. “It’s worth noting that the baseline AN count ranged between 12 and nearly 15, the mean draining tunnel count ranged between 2.9 and 3.7, and between 7% and 13% of patients were on concomitant antibiotics,” he said.
At 24 weeks, 43.3% of patients in the sonelokimab 120 mg arm achieved a HiSCR 75, compared with 34.8% of those in the sonelokimab 240 mg arm and 14.7% of those in the placebo arm, he reported. Meanwhile, 65.7% of patients in the sonelokimab 120 mg arm achieved an HiSCR 75, compared with 53% of those in the sonelokimab 240 mg arm and 27.9% of those in the placebo arm. Discontinuation rates were low and similar between treatment arms, with fewer than 10% of patients failing to complete week 24 of treatment.
In other findings, 69% of patients in the 120 mg arm achieved a HiSCR 50 at week 24 compared with 60.3% in the 240 mg arm; 56.9% in the 120 mg arm achieved a HiSCR 75 compared with 37.9% in the 240 mg arm; and 37.9% in the 120 mg arm achieved a HiSCR 75 compared with 27.6% in the 240 mg arm.
In addition, complete inflammatory remission as defined by the International HS Severity Score System (IHS4-100) continued to increase to week 24, with 24.1% of patients in the 120 mg arm achieving complete remission, compared with 15.5% of those in the 240 mg arm. Meaningful improvements in quality of life, skin pain, and HS symptoms reported by patients treated with sonelokimab were maintained or increased to week 24. Specifically, more than 60% of patients had a meaningful clinical improvement in their Dermatology Life Quality Index, over 45% had a minimum of a 30% increase in the Numerical Rating Scale **30, and more than 41% of patients reported absent or minimal symptoms on the Patient’s Global Impression of their Disease Severity, “which is a high bar to achieve in HS,” Dr. Kirby said.
No Serious Safety Signals Noted
There were no unexpected safety signals to week 24. The incidence of treatment-related adverse events was low, and there were no cases of inflammatory bowel disease. There were no serious infections, no major adverse cardiovascular event (MACE) reports, and no significant abnormalities on liver function tests. “There were also no safety signals on suicidal behavior, attempted suicides, or completed suicides,” he said.
“As you would expect with in IL-17 inhibitor, there was a signal for candidiasis, but all cases were judged to be mild or moderate, and no cases led to discontinuation of treatment from the trial because of candidal infection.”
Based on these data, Dr. Kirby said that larger and longer-term phase 3 trials are planned to further examine the safety and efficacy of sonelokimab at the 120 mg dose for the treatment of moderate-to-severe HS.
One of the session moderators, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, asked Dr. Kirby why he thought the lower dose resulted in generally better outcomes compared with the higher dose.
“There were no statistically significant differences between the two groups,” Dr. Kirby responded. “The 120 mg dose we know is highly effective in psoriasis, so there may be a ceiling effect. This may also be due to population variability, but the bottom line is that the 120 mg dose performs extremely well.”
Dr. Kirby disclosed that he has received research support from/has been a principal investigator for several pharmaceutical companies, including MoonLake Immunotherapeutics. Dr. Gelfand reported that he has been a consultant to and/or a member of the data safety monitoring board member for several pharmaceutical companies, including MoonLake.
SAN DIEGO — After 24 weeks of treatment with subcutaneously administered relative to baseline, results from a randomized clinical trial showed.
Sonelokimab is a novel humanized nanobody that selectively binds to interleukin (IL)-17A and IL-17F, presenting author Brian Kirby, MD, a dermatologist at St. Vincent’s Private Hospital, Dublin, Ireland, said during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology. Sonelokimab is smaller than traditional monoclonal antibodies, he said, “which means it may be able to penetrate tissues better and stay there longer.” It is being developed by MoonLake Immunotherapeutics, based in Zug, Switzerland
According to a press release from the company, nanobodies represent a new generation of targeted therapies derived from antibodies. They consist of one or more domains based on the small antigen-binding variable regions of heavy-chain-only antibodies.
In a phase 2 study known as the MIRA trial, researchers recruited 234 patients with moderate to severe HS to evaluate two different doses of sonelokimab (120 mg and 240 mg every 2 weeks) with a placebo control arm and adalimumab as an active reference arm. The primary endpoint of was the percentage of participants who achieved a HiSCR75. The study population included adults with Hurley Stage II or III HS who had HS lesions in 2 or more anatomical areas and a total abscess and inflammatory nodule (AN) count of 5 or more lesions; and had been treated with 2 or fewer biologics.
Dr. Kirby reported results from 67 patients in the sonelokimab 120 mg arm, 66 in the sonelokimab 240 mg arm, and 39 in the placebo arm. “It’s worth noting that the baseline AN count ranged between 12 and nearly 15, the mean draining tunnel count ranged between 2.9 and 3.7, and between 7% and 13% of patients were on concomitant antibiotics,” he said.
At 24 weeks, 43.3% of patients in the sonelokimab 120 mg arm achieved a HiSCR 75, compared with 34.8% of those in the sonelokimab 240 mg arm and 14.7% of those in the placebo arm, he reported. Meanwhile, 65.7% of patients in the sonelokimab 120 mg arm achieved an HiSCR 75, compared with 53% of those in the sonelokimab 240 mg arm and 27.9% of those in the placebo arm. Discontinuation rates were low and similar between treatment arms, with fewer than 10% of patients failing to complete week 24 of treatment.
In other findings, 69% of patients in the 120 mg arm achieved a HiSCR 50 at week 24 compared with 60.3% in the 240 mg arm; 56.9% in the 120 mg arm achieved a HiSCR 75 compared with 37.9% in the 240 mg arm; and 37.9% in the 120 mg arm achieved a HiSCR 75 compared with 27.6% in the 240 mg arm.
In addition, complete inflammatory remission as defined by the International HS Severity Score System (IHS4-100) continued to increase to week 24, with 24.1% of patients in the 120 mg arm achieving complete remission, compared with 15.5% of those in the 240 mg arm. Meaningful improvements in quality of life, skin pain, and HS symptoms reported by patients treated with sonelokimab were maintained or increased to week 24. Specifically, more than 60% of patients had a meaningful clinical improvement in their Dermatology Life Quality Index, over 45% had a minimum of a 30% increase in the Numerical Rating Scale **30, and more than 41% of patients reported absent or minimal symptoms on the Patient’s Global Impression of their Disease Severity, “which is a high bar to achieve in HS,” Dr. Kirby said.
No Serious Safety Signals Noted
There were no unexpected safety signals to week 24. The incidence of treatment-related adverse events was low, and there were no cases of inflammatory bowel disease. There were no serious infections, no major adverse cardiovascular event (MACE) reports, and no significant abnormalities on liver function tests. “There were also no safety signals on suicidal behavior, attempted suicides, or completed suicides,” he said.
“As you would expect with in IL-17 inhibitor, there was a signal for candidiasis, but all cases were judged to be mild or moderate, and no cases led to discontinuation of treatment from the trial because of candidal infection.”
Based on these data, Dr. Kirby said that larger and longer-term phase 3 trials are planned to further examine the safety and efficacy of sonelokimab at the 120 mg dose for the treatment of moderate-to-severe HS.
One of the session moderators, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, asked Dr. Kirby why he thought the lower dose resulted in generally better outcomes compared with the higher dose.
“There were no statistically significant differences between the two groups,” Dr. Kirby responded. “The 120 mg dose we know is highly effective in psoriasis, so there may be a ceiling effect. This may also be due to population variability, but the bottom line is that the 120 mg dose performs extremely well.”
Dr. Kirby disclosed that he has received research support from/has been a principal investigator for several pharmaceutical companies, including MoonLake Immunotherapeutics. Dr. Gelfand reported that he has been a consultant to and/or a member of the data safety monitoring board member for several pharmaceutical companies, including MoonLake.
SAN DIEGO — After 24 weeks of treatment with subcutaneously administered relative to baseline, results from a randomized clinical trial showed.
Sonelokimab is a novel humanized nanobody that selectively binds to interleukin (IL)-17A and IL-17F, presenting author Brian Kirby, MD, a dermatologist at St. Vincent’s Private Hospital, Dublin, Ireland, said during a late-breaking abstract session at the annual meeting of the American Academy of Dermatology. Sonelokimab is smaller than traditional monoclonal antibodies, he said, “which means it may be able to penetrate tissues better and stay there longer.” It is being developed by MoonLake Immunotherapeutics, based in Zug, Switzerland
According to a press release from the company, nanobodies represent a new generation of targeted therapies derived from antibodies. They consist of one or more domains based on the small antigen-binding variable regions of heavy-chain-only antibodies.
In a phase 2 study known as the MIRA trial, researchers recruited 234 patients with moderate to severe HS to evaluate two different doses of sonelokimab (120 mg and 240 mg every 2 weeks) with a placebo control arm and adalimumab as an active reference arm. The primary endpoint of was the percentage of participants who achieved a HiSCR75. The study population included adults with Hurley Stage II or III HS who had HS lesions in 2 or more anatomical areas and a total abscess and inflammatory nodule (AN) count of 5 or more lesions; and had been treated with 2 or fewer biologics.
Dr. Kirby reported results from 67 patients in the sonelokimab 120 mg arm, 66 in the sonelokimab 240 mg arm, and 39 in the placebo arm. “It’s worth noting that the baseline AN count ranged between 12 and nearly 15, the mean draining tunnel count ranged between 2.9 and 3.7, and between 7% and 13% of patients were on concomitant antibiotics,” he said.
At 24 weeks, 43.3% of patients in the sonelokimab 120 mg arm achieved a HiSCR 75, compared with 34.8% of those in the sonelokimab 240 mg arm and 14.7% of those in the placebo arm, he reported. Meanwhile, 65.7% of patients in the sonelokimab 120 mg arm achieved an HiSCR 75, compared with 53% of those in the sonelokimab 240 mg arm and 27.9% of those in the placebo arm. Discontinuation rates were low and similar between treatment arms, with fewer than 10% of patients failing to complete week 24 of treatment.
In other findings, 69% of patients in the 120 mg arm achieved a HiSCR 50 at week 24 compared with 60.3% in the 240 mg arm; 56.9% in the 120 mg arm achieved a HiSCR 75 compared with 37.9% in the 240 mg arm; and 37.9% in the 120 mg arm achieved a HiSCR 75 compared with 27.6% in the 240 mg arm.
In addition, complete inflammatory remission as defined by the International HS Severity Score System (IHS4-100) continued to increase to week 24, with 24.1% of patients in the 120 mg arm achieving complete remission, compared with 15.5% of those in the 240 mg arm. Meaningful improvements in quality of life, skin pain, and HS symptoms reported by patients treated with sonelokimab were maintained or increased to week 24. Specifically, more than 60% of patients had a meaningful clinical improvement in their Dermatology Life Quality Index, over 45% had a minimum of a 30% increase in the Numerical Rating Scale **30, and more than 41% of patients reported absent or minimal symptoms on the Patient’s Global Impression of their Disease Severity, “which is a high bar to achieve in HS,” Dr. Kirby said.
No Serious Safety Signals Noted
There were no unexpected safety signals to week 24. The incidence of treatment-related adverse events was low, and there were no cases of inflammatory bowel disease. There were no serious infections, no major adverse cardiovascular event (MACE) reports, and no significant abnormalities on liver function tests. “There were also no safety signals on suicidal behavior, attempted suicides, or completed suicides,” he said.
“As you would expect with in IL-17 inhibitor, there was a signal for candidiasis, but all cases were judged to be mild or moderate, and no cases led to discontinuation of treatment from the trial because of candidal infection.”
Based on these data, Dr. Kirby said that larger and longer-term phase 3 trials are planned to further examine the safety and efficacy of sonelokimab at the 120 mg dose for the treatment of moderate-to-severe HS.
One of the session moderators, Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, asked Dr. Kirby why he thought the lower dose resulted in generally better outcomes compared with the higher dose.
“There were no statistically significant differences between the two groups,” Dr. Kirby responded. “The 120 mg dose we know is highly effective in psoriasis, so there may be a ceiling effect. This may also be due to population variability, but the bottom line is that the 120 mg dose performs extremely well.”
Dr. Kirby disclosed that he has received research support from/has been a principal investigator for several pharmaceutical companies, including MoonLake Immunotherapeutics. Dr. Gelfand reported that he has been a consultant to and/or a member of the data safety monitoring board member for several pharmaceutical companies, including MoonLake.
FROM AAD 2024
Non-Radical Surgery a Win-Win for Early Cervical Cancer
according to results of the GOG-278 trial.
In fact, patients’ quality of life was improved after surgery in both groups, and their concerns about cancer recurrence decreased, especially for those undergoing simple hysterectomy, said Allan Covens, MD, in his late-breaking abstract presentation at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
“Cone biopsy patients reported less concerns about reproductive fertility after surgery and over time compared to preop assessments,” he added.
Due to screening in developed countries, a large proportion of cervical cancers are discovered at an early stage. Treatment of these cancers with radical surgery is associated with high cure rates but significant adverse effects on quality of life, said Dr. Covens, who is with the University of Toronto, Toronto, Ontario, Canada.
He and his colleagues wanted to see if non-radical surgery could be safely used instead. “Multiple case series have indicated that non-radical surgery is associated with less morbidity and improved quality of life,” he explained. “If this can be proven in a prospective evaluation, it will change future practice.”
GOG-278 was a prospective cohort study of women with stage IA1 (lymph-vascular space invasion+) and IA2-IB1 (≤ 2 cm) carcinoma of the cervix who underwent non-radical surgery (simple hysterectomy or fertility-preserving cone biopsy) and pelvic lymphadenectomy. Criteria included ≤ 10 mm stromal invasion and negative margins on the final cone biopsy.
The primary objectives were to assess changes in functional outcomes of quality of life (bladder/bowel function, sexual function, cancer worry, and reproductive concerns), using validated instruments. Findings were based on 55 patients who underwent cone biopsy and 113 who underwent simple hysterectomy.
Both simple hysterectomy and cone biopsy were associated with “small” declines in sexual function and bladder/bowel function at 4-6 weeks after surgery, but function “quickly” recovered to baseline by 6 months, Dr. Covens reported.
Twelve patients reported a diagnosis of lymphedema, with a Gynecologic Cancer Lymphedema Questionnaire score change of 4 or higher on at least two consecutive evaluations from baseline. This occurred in six cone biopsy and six simple hysterectomy patients.
In a separate presentation, Dr. Covens reported secondary oncologic outcomes from GOG-278, which suggest that non-radical surgery for early-stage cervical cancer is safe, with low perioperative morbidity, although longer follow-up is needed.
He also reported 16 pregnancies in 15 patients who had undergone cone biopsies; 12 of these were successful, and there were four early pregnancy losses.
‘Impressive’ Data
Study discussant Kristin Bixel, MD, with The Ohio State University, Columbus, Ohio, said the data are “impressive” and clearly show that non-radical surgery has “minimal impact on bladder/bowel function, with no long-term differences from baseline.”
She added that the incidence of lymphedema was “honestly significantly lower than what I typically counsel patients about” and wondered if the percentage of patients with lymphedema would increase over time.
Dr. Bixel particularly noted the decrease in cancer worry scores after surgery, as sometimes patients who have less radical procedures fear that this comes with an increased risk for recurrence.
The “growing body of data suggests that less radical surgery is safe and effective for early-stage low-risk cervical cancer and highlights the potential reproductive success,” she concluded.
Funding for the study was provided by grants from NRG Oncology. Dr. Covens had no disclosures. Dr. Bixel has received research funding from the Intuitive Foundation.
A version of this article appeared on Medscape.com.
according to results of the GOG-278 trial.
In fact, patients’ quality of life was improved after surgery in both groups, and their concerns about cancer recurrence decreased, especially for those undergoing simple hysterectomy, said Allan Covens, MD, in his late-breaking abstract presentation at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
“Cone biopsy patients reported less concerns about reproductive fertility after surgery and over time compared to preop assessments,” he added.
Due to screening in developed countries, a large proportion of cervical cancers are discovered at an early stage. Treatment of these cancers with radical surgery is associated with high cure rates but significant adverse effects on quality of life, said Dr. Covens, who is with the University of Toronto, Toronto, Ontario, Canada.
He and his colleagues wanted to see if non-radical surgery could be safely used instead. “Multiple case series have indicated that non-radical surgery is associated with less morbidity and improved quality of life,” he explained. “If this can be proven in a prospective evaluation, it will change future practice.”
GOG-278 was a prospective cohort study of women with stage IA1 (lymph-vascular space invasion+) and IA2-IB1 (≤ 2 cm) carcinoma of the cervix who underwent non-radical surgery (simple hysterectomy or fertility-preserving cone biopsy) and pelvic lymphadenectomy. Criteria included ≤ 10 mm stromal invasion and negative margins on the final cone biopsy.
The primary objectives were to assess changes in functional outcomes of quality of life (bladder/bowel function, sexual function, cancer worry, and reproductive concerns), using validated instruments. Findings were based on 55 patients who underwent cone biopsy and 113 who underwent simple hysterectomy.
Both simple hysterectomy and cone biopsy were associated with “small” declines in sexual function and bladder/bowel function at 4-6 weeks after surgery, but function “quickly” recovered to baseline by 6 months, Dr. Covens reported.
Twelve patients reported a diagnosis of lymphedema, with a Gynecologic Cancer Lymphedema Questionnaire score change of 4 or higher on at least two consecutive evaluations from baseline. This occurred in six cone biopsy and six simple hysterectomy patients.
In a separate presentation, Dr. Covens reported secondary oncologic outcomes from GOG-278, which suggest that non-radical surgery for early-stage cervical cancer is safe, with low perioperative morbidity, although longer follow-up is needed.
He also reported 16 pregnancies in 15 patients who had undergone cone biopsies; 12 of these were successful, and there were four early pregnancy losses.
‘Impressive’ Data
Study discussant Kristin Bixel, MD, with The Ohio State University, Columbus, Ohio, said the data are “impressive” and clearly show that non-radical surgery has “minimal impact on bladder/bowel function, with no long-term differences from baseline.”
She added that the incidence of lymphedema was “honestly significantly lower than what I typically counsel patients about” and wondered if the percentage of patients with lymphedema would increase over time.
Dr. Bixel particularly noted the decrease in cancer worry scores after surgery, as sometimes patients who have less radical procedures fear that this comes with an increased risk for recurrence.
The “growing body of data suggests that less radical surgery is safe and effective for early-stage low-risk cervical cancer and highlights the potential reproductive success,” she concluded.
Funding for the study was provided by grants from NRG Oncology. Dr. Covens had no disclosures. Dr. Bixel has received research funding from the Intuitive Foundation.
A version of this article appeared on Medscape.com.
according to results of the GOG-278 trial.
In fact, patients’ quality of life was improved after surgery in both groups, and their concerns about cancer recurrence decreased, especially for those undergoing simple hysterectomy, said Allan Covens, MD, in his late-breaking abstract presentation at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
“Cone biopsy patients reported less concerns about reproductive fertility after surgery and over time compared to preop assessments,” he added.
Due to screening in developed countries, a large proportion of cervical cancers are discovered at an early stage. Treatment of these cancers with radical surgery is associated with high cure rates but significant adverse effects on quality of life, said Dr. Covens, who is with the University of Toronto, Toronto, Ontario, Canada.
He and his colleagues wanted to see if non-radical surgery could be safely used instead. “Multiple case series have indicated that non-radical surgery is associated with less morbidity and improved quality of life,” he explained. “If this can be proven in a prospective evaluation, it will change future practice.”
GOG-278 was a prospective cohort study of women with stage IA1 (lymph-vascular space invasion+) and IA2-IB1 (≤ 2 cm) carcinoma of the cervix who underwent non-radical surgery (simple hysterectomy or fertility-preserving cone biopsy) and pelvic lymphadenectomy. Criteria included ≤ 10 mm stromal invasion and negative margins on the final cone biopsy.
The primary objectives were to assess changes in functional outcomes of quality of life (bladder/bowel function, sexual function, cancer worry, and reproductive concerns), using validated instruments. Findings were based on 55 patients who underwent cone biopsy and 113 who underwent simple hysterectomy.
Both simple hysterectomy and cone biopsy were associated with “small” declines in sexual function and bladder/bowel function at 4-6 weeks after surgery, but function “quickly” recovered to baseline by 6 months, Dr. Covens reported.
Twelve patients reported a diagnosis of lymphedema, with a Gynecologic Cancer Lymphedema Questionnaire score change of 4 or higher on at least two consecutive evaluations from baseline. This occurred in six cone biopsy and six simple hysterectomy patients.
In a separate presentation, Dr. Covens reported secondary oncologic outcomes from GOG-278, which suggest that non-radical surgery for early-stage cervical cancer is safe, with low perioperative morbidity, although longer follow-up is needed.
He also reported 16 pregnancies in 15 patients who had undergone cone biopsies; 12 of these were successful, and there were four early pregnancy losses.
‘Impressive’ Data
Study discussant Kristin Bixel, MD, with The Ohio State University, Columbus, Ohio, said the data are “impressive” and clearly show that non-radical surgery has “minimal impact on bladder/bowel function, with no long-term differences from baseline.”
She added that the incidence of lymphedema was “honestly significantly lower than what I typically counsel patients about” and wondered if the percentage of patients with lymphedema would increase over time.
Dr. Bixel particularly noted the decrease in cancer worry scores after surgery, as sometimes patients who have less radical procedures fear that this comes with an increased risk for recurrence.
The “growing body of data suggests that less radical surgery is safe and effective for early-stage low-risk cervical cancer and highlights the potential reproductive success,” she concluded.
Funding for the study was provided by grants from NRG Oncology. Dr. Covens had no disclosures. Dr. Bixel has received research funding from the Intuitive Foundation.
A version of this article appeared on Medscape.com.
FROM SGO 2024
Very Low-Energy Diet Safe, Acceptable for Adolescents
More research is needed to understand which patients are best suited for the diet; “however, given the associated rapid weight loss, the use of [very low-energy diets] should be emphasized in clinical practice guidelines for the treatment of severe obesity and obesity-related complications in adolescents, especially before pharmacological or surgical intervention,” first author Megan Gow, PhD, of Children’s Hospital Westmead Clinical School, The University of Sydney, Westmead, Australia, said in a press statement.
The study will be presented in May at the upcoming European Congress on Obesity, in Venice, Italy.
While very low-calorie diets have been shown to promote rapid weight loss in adolescents, research is lacking on general side effects and acceptability of the regimens. Data is also lacking on important issues including the diet’s effect on growth, heart health, and psychological wellbeing.
To investigate, Dr. Gow and colleagues conducted a subanalysis of the 52-week Fast Track to Health study evaluating the acceptability of different dietary plans for adolescents with obesity.
The analysis included 141 adolescents between the ages of 13 and 17 years with moderate to severe obesity (average body mass index, 35 kg/m2) and at least one obesity-related complication, such as high blood pressure or insulin resistance.
The participants were placed on a nutritionally balanced very low-energy diet consisting of 800 calories per day.
The diet involved one of two regimens — either four Optifast-formulated meal replacement products per day, including shakes, soups, bars, and/or dessert, along with low carbohydrate vegetables, such as broccoli, celery, capsicum, mushrooms, and tomatoes, with one teaspoon of vegetable oil, or a regimen of three Optifast-formulated meal replacements and one meal consisting of 100-150 g lean cooked meat, low-carbohydrate vegetables, and one teaspoon of vegetable oil.
Participants, about half of whom were women, also received dietitian support at least weekly.
After 4 weeks, most of the adolescents, ie, 134 of the 141, with an average age of 14.9 years, completed the diet, with an average weight loss of 5.5 kg or 12 pounds (P < .001).
Most patients (95%) experienced at least one side effect, and 70% reported at least 3 of the side effects, with the most common side effects including hunger, fatigue, headache, irritability, loose stools, constipation, nausea, and a lack of concentration.
Viral infections occurred in seven participants.
While most side effects occurred at the end of week 1, the development of side effects earlier, at day 3-4, was associated with higher levels of weight loss at the 4-week cut-off, which the authors noted could suggest a greater adherence to the diet at that stage.
One adverse event occurred, consisting of a single fainting episode determined to be potentially related to the dietary intervention.
In surveys, the adolescents gave the intervention an acceptability rating of 61 on a scale of 100, the score was 53 of 100 in terms of being “enjoyable to follow.”
The most-liked aspects of the intervention were losing weight (described by 34% of participants) and the prescriptive structure (listed by 28% of participants).
The least-liked aspects included the diet’s restrictive nature, described by 45% of participants, and the taste of meal replacement products, listed by 20% of participants.
Alternative to Weight Loss Drugs?
While weight loss drugs are transforming the obesity treatment and semaglutide is now approved for adolescents as young as age 12 years, “access to these medications is limited, and not all families want to commence on medication for their child›s obesity,” Dr. Gow said.
As an alternative, a very low-energy diet, with the interaction of a dietitian, can enable adolescents “to develop a healthier relationship with food, including encouraging the consumption of more fruits and vegetables in their diet, not only to assist in weight loss but for good health,” she said.
Very Low-Calorie Diet Concerns for Adolescents Addressed
Early studies suggested concerns of health effects from very low-calorie diets in adolescents, including potential cardiac effects; however, subsequent studies, including a systematic review published by Dr. Gow and her team, have shown that such results were likely the result of nutritional deficiencies in the diets, which can be overcome with careful food selection and dietary counseling.
Another key concern has been a potential effect on growth, but Dr. Gow noted that “in our short-term study we saw small increase in height (0.1 cm), and other more recent studies suggest that a short-term very low-energy diet does not impact growth.”
And in an earlier pilot study, the authors also found an association between the very low-calorie diet and an improvement in the quality of life for youth with type 2 diabetes.
A key caveat with the findings is that participants in the study all received supervision and monitoring from a trained dietitian, and Gow noted that that element is essential.
“We therefore do not recommend adolescents in the community undertake this type of diet without appropriate support,” she said.
“Close monitoring of adolescents by a health professional following a very low-energy diet is essential to ensure that the very low-energy diet is leading to holistic health benefits for the individual.”
Following the 4-week regimen, participants were randomized to transition to interventions of either continuous energy restriction or intermittent energy restriction over the 52 weeks, and further findings from the study will be presented at the obesity meeting in May.
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.
More research is needed to understand which patients are best suited for the diet; “however, given the associated rapid weight loss, the use of [very low-energy diets] should be emphasized in clinical practice guidelines for the treatment of severe obesity and obesity-related complications in adolescents, especially before pharmacological or surgical intervention,” first author Megan Gow, PhD, of Children’s Hospital Westmead Clinical School, The University of Sydney, Westmead, Australia, said in a press statement.
The study will be presented in May at the upcoming European Congress on Obesity, in Venice, Italy.
While very low-calorie diets have been shown to promote rapid weight loss in adolescents, research is lacking on general side effects and acceptability of the regimens. Data is also lacking on important issues including the diet’s effect on growth, heart health, and psychological wellbeing.
To investigate, Dr. Gow and colleagues conducted a subanalysis of the 52-week Fast Track to Health study evaluating the acceptability of different dietary plans for adolescents with obesity.
The analysis included 141 adolescents between the ages of 13 and 17 years with moderate to severe obesity (average body mass index, 35 kg/m2) and at least one obesity-related complication, such as high blood pressure or insulin resistance.
The participants were placed on a nutritionally balanced very low-energy diet consisting of 800 calories per day.
The diet involved one of two regimens — either four Optifast-formulated meal replacement products per day, including shakes, soups, bars, and/or dessert, along with low carbohydrate vegetables, such as broccoli, celery, capsicum, mushrooms, and tomatoes, with one teaspoon of vegetable oil, or a regimen of three Optifast-formulated meal replacements and one meal consisting of 100-150 g lean cooked meat, low-carbohydrate vegetables, and one teaspoon of vegetable oil.
Participants, about half of whom were women, also received dietitian support at least weekly.
After 4 weeks, most of the adolescents, ie, 134 of the 141, with an average age of 14.9 years, completed the diet, with an average weight loss of 5.5 kg or 12 pounds (P < .001).
Most patients (95%) experienced at least one side effect, and 70% reported at least 3 of the side effects, with the most common side effects including hunger, fatigue, headache, irritability, loose stools, constipation, nausea, and a lack of concentration.
Viral infections occurred in seven participants.
While most side effects occurred at the end of week 1, the development of side effects earlier, at day 3-4, was associated with higher levels of weight loss at the 4-week cut-off, which the authors noted could suggest a greater adherence to the diet at that stage.
One adverse event occurred, consisting of a single fainting episode determined to be potentially related to the dietary intervention.
In surveys, the adolescents gave the intervention an acceptability rating of 61 on a scale of 100, the score was 53 of 100 in terms of being “enjoyable to follow.”
The most-liked aspects of the intervention were losing weight (described by 34% of participants) and the prescriptive structure (listed by 28% of participants).
The least-liked aspects included the diet’s restrictive nature, described by 45% of participants, and the taste of meal replacement products, listed by 20% of participants.
Alternative to Weight Loss Drugs?
While weight loss drugs are transforming the obesity treatment and semaglutide is now approved for adolescents as young as age 12 years, “access to these medications is limited, and not all families want to commence on medication for their child›s obesity,” Dr. Gow said.
As an alternative, a very low-energy diet, with the interaction of a dietitian, can enable adolescents “to develop a healthier relationship with food, including encouraging the consumption of more fruits and vegetables in their diet, not only to assist in weight loss but for good health,” she said.
Very Low-Calorie Diet Concerns for Adolescents Addressed
Early studies suggested concerns of health effects from very low-calorie diets in adolescents, including potential cardiac effects; however, subsequent studies, including a systematic review published by Dr. Gow and her team, have shown that such results were likely the result of nutritional deficiencies in the diets, which can be overcome with careful food selection and dietary counseling.
Another key concern has been a potential effect on growth, but Dr. Gow noted that “in our short-term study we saw small increase in height (0.1 cm), and other more recent studies suggest that a short-term very low-energy diet does not impact growth.”
And in an earlier pilot study, the authors also found an association between the very low-calorie diet and an improvement in the quality of life for youth with type 2 diabetes.
A key caveat with the findings is that participants in the study all received supervision and monitoring from a trained dietitian, and Gow noted that that element is essential.
“We therefore do not recommend adolescents in the community undertake this type of diet without appropriate support,” she said.
“Close monitoring of adolescents by a health professional following a very low-energy diet is essential to ensure that the very low-energy diet is leading to holistic health benefits for the individual.”
Following the 4-week regimen, participants were randomized to transition to interventions of either continuous energy restriction or intermittent energy restriction over the 52 weeks, and further findings from the study will be presented at the obesity meeting in May.
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.
More research is needed to understand which patients are best suited for the diet; “however, given the associated rapid weight loss, the use of [very low-energy diets] should be emphasized in clinical practice guidelines for the treatment of severe obesity and obesity-related complications in adolescents, especially before pharmacological or surgical intervention,” first author Megan Gow, PhD, of Children’s Hospital Westmead Clinical School, The University of Sydney, Westmead, Australia, said in a press statement.
The study will be presented in May at the upcoming European Congress on Obesity, in Venice, Italy.
While very low-calorie diets have been shown to promote rapid weight loss in adolescents, research is lacking on general side effects and acceptability of the regimens. Data is also lacking on important issues including the diet’s effect on growth, heart health, and psychological wellbeing.
To investigate, Dr. Gow and colleagues conducted a subanalysis of the 52-week Fast Track to Health study evaluating the acceptability of different dietary plans for adolescents with obesity.
The analysis included 141 adolescents between the ages of 13 and 17 years with moderate to severe obesity (average body mass index, 35 kg/m2) and at least one obesity-related complication, such as high blood pressure or insulin resistance.
The participants were placed on a nutritionally balanced very low-energy diet consisting of 800 calories per day.
The diet involved one of two regimens — either four Optifast-formulated meal replacement products per day, including shakes, soups, bars, and/or dessert, along with low carbohydrate vegetables, such as broccoli, celery, capsicum, mushrooms, and tomatoes, with one teaspoon of vegetable oil, or a regimen of three Optifast-formulated meal replacements and one meal consisting of 100-150 g lean cooked meat, low-carbohydrate vegetables, and one teaspoon of vegetable oil.
Participants, about half of whom were women, also received dietitian support at least weekly.
After 4 weeks, most of the adolescents, ie, 134 of the 141, with an average age of 14.9 years, completed the diet, with an average weight loss of 5.5 kg or 12 pounds (P < .001).
Most patients (95%) experienced at least one side effect, and 70% reported at least 3 of the side effects, with the most common side effects including hunger, fatigue, headache, irritability, loose stools, constipation, nausea, and a lack of concentration.
Viral infections occurred in seven participants.
While most side effects occurred at the end of week 1, the development of side effects earlier, at day 3-4, was associated with higher levels of weight loss at the 4-week cut-off, which the authors noted could suggest a greater adherence to the diet at that stage.
One adverse event occurred, consisting of a single fainting episode determined to be potentially related to the dietary intervention.
In surveys, the adolescents gave the intervention an acceptability rating of 61 on a scale of 100, the score was 53 of 100 in terms of being “enjoyable to follow.”
The most-liked aspects of the intervention were losing weight (described by 34% of participants) and the prescriptive structure (listed by 28% of participants).
The least-liked aspects included the diet’s restrictive nature, described by 45% of participants, and the taste of meal replacement products, listed by 20% of participants.
Alternative to Weight Loss Drugs?
While weight loss drugs are transforming the obesity treatment and semaglutide is now approved for adolescents as young as age 12 years, “access to these medications is limited, and not all families want to commence on medication for their child›s obesity,” Dr. Gow said.
As an alternative, a very low-energy diet, with the interaction of a dietitian, can enable adolescents “to develop a healthier relationship with food, including encouraging the consumption of more fruits and vegetables in their diet, not only to assist in weight loss but for good health,” she said.
Very Low-Calorie Diet Concerns for Adolescents Addressed
Early studies suggested concerns of health effects from very low-calorie diets in adolescents, including potential cardiac effects; however, subsequent studies, including a systematic review published by Dr. Gow and her team, have shown that such results were likely the result of nutritional deficiencies in the diets, which can be overcome with careful food selection and dietary counseling.
Another key concern has been a potential effect on growth, but Dr. Gow noted that “in our short-term study we saw small increase in height (0.1 cm), and other more recent studies suggest that a short-term very low-energy diet does not impact growth.”
And in an earlier pilot study, the authors also found an association between the very low-calorie diet and an improvement in the quality of life for youth with type 2 diabetes.
A key caveat with the findings is that participants in the study all received supervision and monitoring from a trained dietitian, and Gow noted that that element is essential.
“We therefore do not recommend adolescents in the community undertake this type of diet without appropriate support,” she said.
“Close monitoring of adolescents by a health professional following a very low-energy diet is essential to ensure that the very low-energy diet is leading to holistic health benefits for the individual.”
Following the 4-week regimen, participants were randomized to transition to interventions of either continuous energy restriction or intermittent energy restriction over the 52 weeks, and further findings from the study will be presented at the obesity meeting in May.
The authors had no disclosures to report.
A version of this article appeared on Medscape.com.
FROM THE EUROPEAN CONGRESS ON OBESITY
Flexibility Recommended for Patients With Personality Disorders
SAN DIEGO — .
“You want to recognize the personality disorder, understand that there are underlying conflicts and needs, and adjust accordingly,” Dr. Nakamura, clinical assistant professor of dermatology at the University of Michigan, Ann Arbor, said at the annual meeting of the American Academy of Dermatology.

Personality disorders, which she defined as enduring patterns of maladaptive thinking and behavior that deviate from the cultural norm, affect up to 15% of the general population and can be difficult “if not impossible to treat, which can be frustrating.” She shared her approach to providing dermatologic care for individuals with these three conditions:
Borderline personality disorder (BPD). This condition is marked by instability in interpersonal relationships, self-image, and emotions. Affected individuals are usually impulsive and often demonstrate self-injurious conduct such as risky sexual behaviors, cutting, or suicide attempts. “They often express feelings of emptiness, a fear of abandonment, and they are labile and sensitive to environmental circumstances,” Dr. Nakamura said. “They can be needy and display inappropriate, intense anger.”
In her clinical experience, a patient’s presenting dermatologic complaint is often a “screen” to hide a real, inner psychological problem, “a need to fill the emptiness,” she explained. “They’re kind of lonely, and there is a fear of abandonment. Rejection is frequently perceived as abandonment, creating intense anger and other negative emotions such as splitting.”
She advises against providing tests, treatments, or procedures for individuals with BPD that are not clinically indicated. “If the test is negative, such patients may ask for further testing,” she said. “Especially for cosmetic procedures, the patient may be more dissatisfied with the outcome of a procedure compared to before. Don’t let the patient’s emotions cloud your judgment. Trying to reason with the patient is often ineffective.”
To avoid saying “no” to such patients, Dr. Nakamura recommended discussing other treatment options so that they don’t feel abandoned. “Show that you care,” she said. “Meet the patient’s emotional needs, which may be the real agenda, and schedule regular follow-ups.”
Obsessive-compulsive personality disorder (OCPD). This condition is characterized by a preoccupation with orderliness, perfectionism, and control. “OCPD individuals are excessively concerned with details, rules, and organization to the extent that the major point of the activity is often lost,” Dr. Nakamura said. “They can be over-conscientious with excessive regard for morality and ethics.”
Such patients often fear losing control, she continued, which can lead to anxiety, depression, and sometimes anger. During office visits with patients with OCPD, she recommends that dermatologists “focus on facts and knowledge to replace or subdue emotions. Knowledge and information give a sense of control over illness.” Her approach involves professional, structured encounters that include detailed explanations and plans. “Provide step-by-step written instructions and give specific reasons for the prescribed treatment,” Dr. Nakamura advised. “Schedule regular follow-up appointments.”
Narcissistic personality disorder (NPD). This condition is characterized by a grandiose sense of self-importance, in which the person believes that they are special, unique, and superior to others. These individuals have a sense of entitlement, fantasize about unlimited success or power, display a lack of empathy toward others, and show a constant need for admiration. “The patient’s personality traits are often a ‘screen’ to hide a real, inner psychological problem such as unrecognized low self-esteem or insecurity,” Dr. Nakamura said. “These patients need praise and a sense of power.”
To provide patients with NPD with “a sense of uniqueness,” she recommended engaging with them at a medical level as one might with a work colleague. “Such patients often respond better to respect and concern rather than warmth and caring,” she said. Asking them to make decisions about their care can also give them a sense of power: asking them, for example, about which type of topical steroid they might prefer from those in the same class, whether they prefer creams or ointments, and that they can choose to follow up in 4 weeks or 6 weeks.
“Do not let the patient dictate the encounter [or] get under your skin,” Dr. Nakamura emphasized. “Be careful about rejecting the patient from your practice. Even though that is perfectly within your rights, it could lead to ‘narcissistic injury’ where the patient becomes very angry and wants to get back at you.”
Dr. Nakamura disclosed that she is an investigator for Amgen, argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Regeneron. She is also a member of the advisory board for argenx, Boehringer Ingelheim, and Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
SAN DIEGO — .
“You want to recognize the personality disorder, understand that there are underlying conflicts and needs, and adjust accordingly,” Dr. Nakamura, clinical assistant professor of dermatology at the University of Michigan, Ann Arbor, said at the annual meeting of the American Academy of Dermatology.
Personality disorders, which she defined as enduring patterns of maladaptive thinking and behavior that deviate from the cultural norm, affect up to 15% of the general population and can be difficult “if not impossible to treat, which can be frustrating.” She shared her approach to providing dermatologic care for individuals with these three conditions:
Borderline personality disorder (BPD). This condition is marked by instability in interpersonal relationships, self-image, and emotions. Affected individuals are usually impulsive and often demonstrate self-injurious conduct such as risky sexual behaviors, cutting, or suicide attempts. “They often express feelings of emptiness, a fear of abandonment, and they are labile and sensitive to environmental circumstances,” Dr. Nakamura said. “They can be needy and display inappropriate, intense anger.”
In her clinical experience, a patient’s presenting dermatologic complaint is often a “screen” to hide a real, inner psychological problem, “a need to fill the emptiness,” she explained. “They’re kind of lonely, and there is a fear of abandonment. Rejection is frequently perceived as abandonment, creating intense anger and other negative emotions such as splitting.”
She advises against providing tests, treatments, or procedures for individuals with BPD that are not clinically indicated. “If the test is negative, such patients may ask for further testing,” she said. “Especially for cosmetic procedures, the patient may be more dissatisfied with the outcome of a procedure compared to before. Don’t let the patient’s emotions cloud your judgment. Trying to reason with the patient is often ineffective.”
To avoid saying “no” to such patients, Dr. Nakamura recommended discussing other treatment options so that they don’t feel abandoned. “Show that you care,” she said. “Meet the patient’s emotional needs, which may be the real agenda, and schedule regular follow-ups.”
Obsessive-compulsive personality disorder (OCPD). This condition is characterized by a preoccupation with orderliness, perfectionism, and control. “OCPD individuals are excessively concerned with details, rules, and organization to the extent that the major point of the activity is often lost,” Dr. Nakamura said. “They can be over-conscientious with excessive regard for morality and ethics.”
Such patients often fear losing control, she continued, which can lead to anxiety, depression, and sometimes anger. During office visits with patients with OCPD, she recommends that dermatologists “focus on facts and knowledge to replace or subdue emotions. Knowledge and information give a sense of control over illness.” Her approach involves professional, structured encounters that include detailed explanations and plans. “Provide step-by-step written instructions and give specific reasons for the prescribed treatment,” Dr. Nakamura advised. “Schedule regular follow-up appointments.”
Narcissistic personality disorder (NPD). This condition is characterized by a grandiose sense of self-importance, in which the person believes that they are special, unique, and superior to others. These individuals have a sense of entitlement, fantasize about unlimited success or power, display a lack of empathy toward others, and show a constant need for admiration. “The patient’s personality traits are often a ‘screen’ to hide a real, inner psychological problem such as unrecognized low self-esteem or insecurity,” Dr. Nakamura said. “These patients need praise and a sense of power.”
To provide patients with NPD with “a sense of uniqueness,” she recommended engaging with them at a medical level as one might with a work colleague. “Such patients often respond better to respect and concern rather than warmth and caring,” she said. Asking them to make decisions about their care can also give them a sense of power: asking them, for example, about which type of topical steroid they might prefer from those in the same class, whether they prefer creams or ointments, and that they can choose to follow up in 4 weeks or 6 weeks.
“Do not let the patient dictate the encounter [or] get under your skin,” Dr. Nakamura emphasized. “Be careful about rejecting the patient from your practice. Even though that is perfectly within your rights, it could lead to ‘narcissistic injury’ where the patient becomes very angry and wants to get back at you.”
Dr. Nakamura disclosed that she is an investigator for Amgen, argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Regeneron. She is also a member of the advisory board for argenx, Boehringer Ingelheim, and Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
SAN DIEGO — .
“You want to recognize the personality disorder, understand that there are underlying conflicts and needs, and adjust accordingly,” Dr. Nakamura, clinical assistant professor of dermatology at the University of Michigan, Ann Arbor, said at the annual meeting of the American Academy of Dermatology.
Personality disorders, which she defined as enduring patterns of maladaptive thinking and behavior that deviate from the cultural norm, affect up to 15% of the general population and can be difficult “if not impossible to treat, which can be frustrating.” She shared her approach to providing dermatologic care for individuals with these three conditions:
Borderline personality disorder (BPD). This condition is marked by instability in interpersonal relationships, self-image, and emotions. Affected individuals are usually impulsive and often demonstrate self-injurious conduct such as risky sexual behaviors, cutting, or suicide attempts. “They often express feelings of emptiness, a fear of abandonment, and they are labile and sensitive to environmental circumstances,” Dr. Nakamura said. “They can be needy and display inappropriate, intense anger.”
In her clinical experience, a patient’s presenting dermatologic complaint is often a “screen” to hide a real, inner psychological problem, “a need to fill the emptiness,” she explained. “They’re kind of lonely, and there is a fear of abandonment. Rejection is frequently perceived as abandonment, creating intense anger and other negative emotions such as splitting.”
She advises against providing tests, treatments, or procedures for individuals with BPD that are not clinically indicated. “If the test is negative, such patients may ask for further testing,” she said. “Especially for cosmetic procedures, the patient may be more dissatisfied with the outcome of a procedure compared to before. Don’t let the patient’s emotions cloud your judgment. Trying to reason with the patient is often ineffective.”
To avoid saying “no” to such patients, Dr. Nakamura recommended discussing other treatment options so that they don’t feel abandoned. “Show that you care,” she said. “Meet the patient’s emotional needs, which may be the real agenda, and schedule regular follow-ups.”
Obsessive-compulsive personality disorder (OCPD). This condition is characterized by a preoccupation with orderliness, perfectionism, and control. “OCPD individuals are excessively concerned with details, rules, and organization to the extent that the major point of the activity is often lost,” Dr. Nakamura said. “They can be over-conscientious with excessive regard for morality and ethics.”
Such patients often fear losing control, she continued, which can lead to anxiety, depression, and sometimes anger. During office visits with patients with OCPD, she recommends that dermatologists “focus on facts and knowledge to replace or subdue emotions. Knowledge and information give a sense of control over illness.” Her approach involves professional, structured encounters that include detailed explanations and plans. “Provide step-by-step written instructions and give specific reasons for the prescribed treatment,” Dr. Nakamura advised. “Schedule regular follow-up appointments.”
Narcissistic personality disorder (NPD). This condition is characterized by a grandiose sense of self-importance, in which the person believes that they are special, unique, and superior to others. These individuals have a sense of entitlement, fantasize about unlimited success or power, display a lack of empathy toward others, and show a constant need for admiration. “The patient’s personality traits are often a ‘screen’ to hide a real, inner psychological problem such as unrecognized low self-esteem or insecurity,” Dr. Nakamura said. “These patients need praise and a sense of power.”
To provide patients with NPD with “a sense of uniqueness,” she recommended engaging with them at a medical level as one might with a work colleague. “Such patients often respond better to respect and concern rather than warmth and caring,” she said. Asking them to make decisions about their care can also give them a sense of power: asking them, for example, about which type of topical steroid they might prefer from those in the same class, whether they prefer creams or ointments, and that they can choose to follow up in 4 weeks or 6 weeks.
“Do not let the patient dictate the encounter [or] get under your skin,” Dr. Nakamura emphasized. “Be careful about rejecting the patient from your practice. Even though that is perfectly within your rights, it could lead to ‘narcissistic injury’ where the patient becomes very angry and wants to get back at you.”
Dr. Nakamura disclosed that she is an investigator for Amgen, argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Regeneron. She is also a member of the advisory board for argenx, Boehringer Ingelheim, and Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Topical Roflumilast Effective in 4 Weeks for Atopic Dermatitis in Young Children
SAN DIEGO — Treatment with (AD), according to the results of a phase 3 study reported at the annual meeting of the American Academy of Dermatology.
Among patients treated with roflumilast cream, 0.05%, 25.4% reached the primary endpoint of “clear” or “almost clear” plus a two-grade improvement from baseline at week 4 vs 10.7% among those in the vehicle group (P < .0001) in a phase 3 randomized controlled trial of children. The findings were released in a late-breaker session at the meeting.
Roflumilast cream, 0.3% (Zoryve), is approved by the Food and Drug Administration (FDA) for treating psoriasis in patients 6 years and older, and lower doses are being evaluated for AD: 0.15% for adults and children ages 6 and older, and 0.05% for ages 2-5. Roflumilast is a phosphodiesterase-4 inhibitor. In 2023, the FDA accepted a supplemental drug application from the manufacturer, Arcutis, for roflumilast, 0.15%, for treating AD in patients ages 6 and older, based on the results from two recently published phase 3 trials, INTEGUMENT-1 and INTEGUMENT-2.
The study of younger children, INTEGUMENT-PED, recruited 652 patients aged 2-5 with mild to moderate AD, with a Validated Investigator Global Assessment scale for AD (vlGA-AD) score of 2 or 3, a mean body surface area of 22% overall (range, 3%-82%), and an Eczema Area and Severity Index (EASI) score of at least 5. Of the patients enrolled, 437 were assigned to 0.05% roflumilast cream, applied once a day for 4 weeks (mean age, 3.3 years; 51.6% male; 67.4% White; 15.6% Black; 8.5% Asian; 8.5% other or more than one race; 80.5% not Latino/Hispanic). The remaining 215 children were assigned to vehicle cream and had similar characteristics.
About 52% of the patients in both groups had an inadequate response, intolerance, or contraindications to topical corticosteroids (and about 17% for topical calcineurin inhibitors and about 9% for crisaborole).
The proportions of patients who reached “clear” (0) or “almost clear” (1) on the vlGA-AD scale were 35.4% and 14.6%, respectively, at week 4 (P < .0001) for roflumilast and vehicle, respectively, according to the lead author of the study, Lawrence M. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, who presented the results at the meeting. In addition, 39.4% and 20.6% achieved an EASI-75 (a secondary endpoint), respectively (P < .0001), and itch also improved within 24 hours of starting treatment.
With regard to safety, 29.7% of patients taking roflumilast had treatment-emergent adverse effects (including upper respiratory tract infections in 4.1%) vs 21.9% of those in the vehicle arm (including upper respiratory tract infections in 1.4%). Reports of pain at the administration site were low (1.6% for roflumilast vs 1.9% for vehicle). Only one patient, a 2-year-old girl, had a treatment-emergent serious adverse event. The child, who was in the roflumilast group, had cellulitis involving noneczematous skin and was treated with antibiotics in the hospital for 3 days. The event was not attributed to roflumilast, which was stopped for 5 days, according to Dr. Eichenfield.
In an interview, Fairfield, Connecticut–based dermatologist Brittany Craiglow, MD, who was not involved in the study, said topical roflumilast would be an “important” new treatment because there are still few nonsteroidal options for the treatment of AD in children under 12. “The excellent local tolerability combined with early improvements in itch and skin clearance will make this a particularly attractive option, if approved,” she said.
Dr. Eichenfield disclosed multiple relationships with various drugmakers. He and several other study authors are investigators and/or consultants for Arcutis and received grants/research funding and/or honoraria. Two authors are Arcutis employees. Other disclosure information for the authors was not immediately available. Dr. Craiglow had no disclosures.
A version of this article appeared on Medscape.com .
SAN DIEGO — Treatment with (AD), according to the results of a phase 3 study reported at the annual meeting of the American Academy of Dermatology.
Among patients treated with roflumilast cream, 0.05%, 25.4% reached the primary endpoint of “clear” or “almost clear” plus a two-grade improvement from baseline at week 4 vs 10.7% among those in the vehicle group (P < .0001) in a phase 3 randomized controlled trial of children. The findings were released in a late-breaker session at the meeting.
Roflumilast cream, 0.3% (Zoryve), is approved by the Food and Drug Administration (FDA) for treating psoriasis in patients 6 years and older, and lower doses are being evaluated for AD: 0.15% for adults and children ages 6 and older, and 0.05% for ages 2-5. Roflumilast is a phosphodiesterase-4 inhibitor. In 2023, the FDA accepted a supplemental drug application from the manufacturer, Arcutis, for roflumilast, 0.15%, for treating AD in patients ages 6 and older, based on the results from two recently published phase 3 trials, INTEGUMENT-1 and INTEGUMENT-2.
The study of younger children, INTEGUMENT-PED, recruited 652 patients aged 2-5 with mild to moderate AD, with a Validated Investigator Global Assessment scale for AD (vlGA-AD) score of 2 or 3, a mean body surface area of 22% overall (range, 3%-82%), and an Eczema Area and Severity Index (EASI) score of at least 5. Of the patients enrolled, 437 were assigned to 0.05% roflumilast cream, applied once a day for 4 weeks (mean age, 3.3 years; 51.6% male; 67.4% White; 15.6% Black; 8.5% Asian; 8.5% other or more than one race; 80.5% not Latino/Hispanic). The remaining 215 children were assigned to vehicle cream and had similar characteristics.
About 52% of the patients in both groups had an inadequate response, intolerance, or contraindications to topical corticosteroids (and about 17% for topical calcineurin inhibitors and about 9% for crisaborole).
The proportions of patients who reached “clear” (0) or “almost clear” (1) on the vlGA-AD scale were 35.4% and 14.6%, respectively, at week 4 (P < .0001) for roflumilast and vehicle, respectively, according to the lead author of the study, Lawrence M. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, who presented the results at the meeting. In addition, 39.4% and 20.6% achieved an EASI-75 (a secondary endpoint), respectively (P < .0001), and itch also improved within 24 hours of starting treatment.
With regard to safety, 29.7% of patients taking roflumilast had treatment-emergent adverse effects (including upper respiratory tract infections in 4.1%) vs 21.9% of those in the vehicle arm (including upper respiratory tract infections in 1.4%). Reports of pain at the administration site were low (1.6% for roflumilast vs 1.9% for vehicle). Only one patient, a 2-year-old girl, had a treatment-emergent serious adverse event. The child, who was in the roflumilast group, had cellulitis involving noneczematous skin and was treated with antibiotics in the hospital for 3 days. The event was not attributed to roflumilast, which was stopped for 5 days, according to Dr. Eichenfield.
In an interview, Fairfield, Connecticut–based dermatologist Brittany Craiglow, MD, who was not involved in the study, said topical roflumilast would be an “important” new treatment because there are still few nonsteroidal options for the treatment of AD in children under 12. “The excellent local tolerability combined with early improvements in itch and skin clearance will make this a particularly attractive option, if approved,” she said.
Dr. Eichenfield disclosed multiple relationships with various drugmakers. He and several other study authors are investigators and/or consultants for Arcutis and received grants/research funding and/or honoraria. Two authors are Arcutis employees. Other disclosure information for the authors was not immediately available. Dr. Craiglow had no disclosures.
A version of this article appeared on Medscape.com .
SAN DIEGO — Treatment with (AD), according to the results of a phase 3 study reported at the annual meeting of the American Academy of Dermatology.
Among patients treated with roflumilast cream, 0.05%, 25.4% reached the primary endpoint of “clear” or “almost clear” plus a two-grade improvement from baseline at week 4 vs 10.7% among those in the vehicle group (P < .0001) in a phase 3 randomized controlled trial of children. The findings were released in a late-breaker session at the meeting.
Roflumilast cream, 0.3% (Zoryve), is approved by the Food and Drug Administration (FDA) for treating psoriasis in patients 6 years and older, and lower doses are being evaluated for AD: 0.15% for adults and children ages 6 and older, and 0.05% for ages 2-5. Roflumilast is a phosphodiesterase-4 inhibitor. In 2023, the FDA accepted a supplemental drug application from the manufacturer, Arcutis, for roflumilast, 0.15%, for treating AD in patients ages 6 and older, based on the results from two recently published phase 3 trials, INTEGUMENT-1 and INTEGUMENT-2.
The study of younger children, INTEGUMENT-PED, recruited 652 patients aged 2-5 with mild to moderate AD, with a Validated Investigator Global Assessment scale for AD (vlGA-AD) score of 2 or 3, a mean body surface area of 22% overall (range, 3%-82%), and an Eczema Area and Severity Index (EASI) score of at least 5. Of the patients enrolled, 437 were assigned to 0.05% roflumilast cream, applied once a day for 4 weeks (mean age, 3.3 years; 51.6% male; 67.4% White; 15.6% Black; 8.5% Asian; 8.5% other or more than one race; 80.5% not Latino/Hispanic). The remaining 215 children were assigned to vehicle cream and had similar characteristics.
About 52% of the patients in both groups had an inadequate response, intolerance, or contraindications to topical corticosteroids (and about 17% for topical calcineurin inhibitors and about 9% for crisaborole).
The proportions of patients who reached “clear” (0) or “almost clear” (1) on the vlGA-AD scale were 35.4% and 14.6%, respectively, at week 4 (P < .0001) for roflumilast and vehicle, respectively, according to the lead author of the study, Lawrence M. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, who presented the results at the meeting. In addition, 39.4% and 20.6% achieved an EASI-75 (a secondary endpoint), respectively (P < .0001), and itch also improved within 24 hours of starting treatment.
With regard to safety, 29.7% of patients taking roflumilast had treatment-emergent adverse effects (including upper respiratory tract infections in 4.1%) vs 21.9% of those in the vehicle arm (including upper respiratory tract infections in 1.4%). Reports of pain at the administration site were low (1.6% for roflumilast vs 1.9% for vehicle). Only one patient, a 2-year-old girl, had a treatment-emergent serious adverse event. The child, who was in the roflumilast group, had cellulitis involving noneczematous skin and was treated with antibiotics in the hospital for 3 days. The event was not attributed to roflumilast, which was stopped for 5 days, according to Dr. Eichenfield.
In an interview, Fairfield, Connecticut–based dermatologist Brittany Craiglow, MD, who was not involved in the study, said topical roflumilast would be an “important” new treatment because there are still few nonsteroidal options for the treatment of AD in children under 12. “The excellent local tolerability combined with early improvements in itch and skin clearance will make this a particularly attractive option, if approved,” she said.
Dr. Eichenfield disclosed multiple relationships with various drugmakers. He and several other study authors are investigators and/or consultants for Arcutis and received grants/research funding and/or honoraria. Two authors are Arcutis employees. Other disclosure information for the authors was not immediately available. Dr. Craiglow had no disclosures.
A version of this article appeared on Medscape.com .
FROM AAD 2024
New Research Dissects Transgenerational Obesity and Diabetes
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
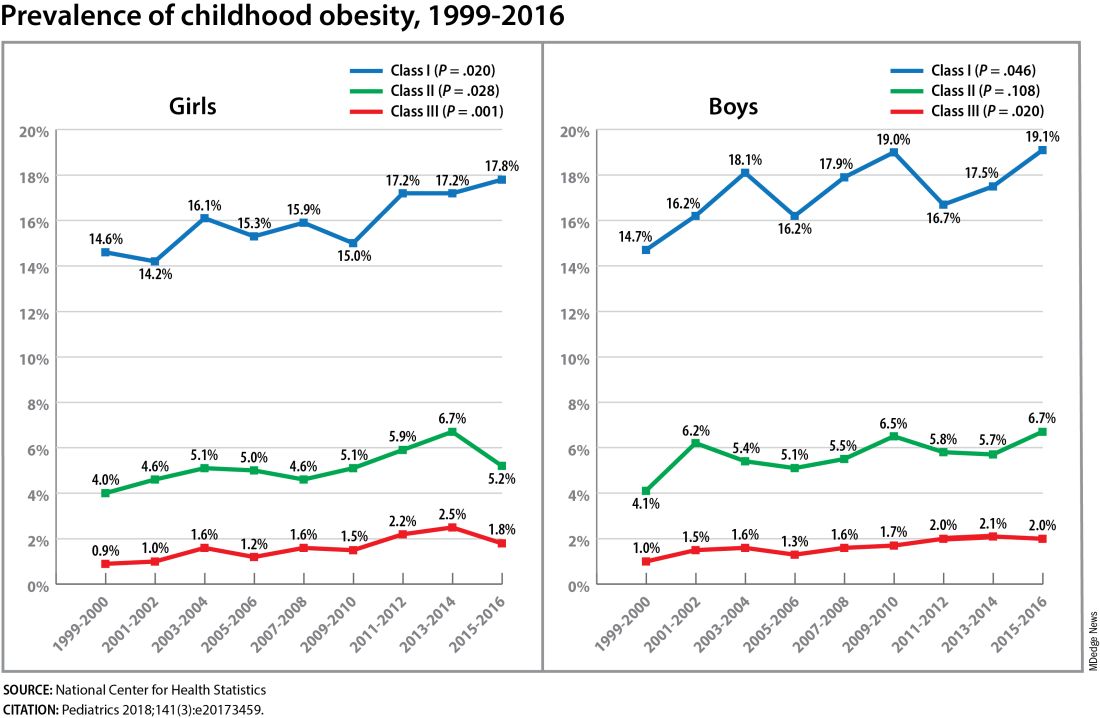
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FROM DPSG-NA 2023
QOL Not Harmed With Add-On Pembrolizumab in Cervical Cancer
according to patient-reported outcome analyses from the KEYNOTE-A18 trial.
Progression-free survival data from the trial, reported at the 2023 meeting of the European Society for Medical Oncology, showed a 30% reduction in the risk for progression (P =.002) with the addition of pembrolizumab vs placebo, as well as favorable overall survival trends, reported Leslie Randall, MD, with VCU Health in Richmond, Virginia. Now the new analyses bring the “voices of the patients from this large phase 3 study.”
“I think the data can put us at ease and give patients a measure of comfort because there was no detriment in the quality of life,” said Dr. Randall, who presented the data on March 17 at the Society of Gynecologic Oncology (SGO) 2024 conference.
The phase 3 KEYNOTE-A18 trial enrolled 1060 patients new to treatment who had either stage 1B2-2B disease with lymph node involvement or stage 3-4A disease. They were randomly allocated to receive pembrolizumab or placebo plus concurrent chemoradiotherapy.
Patient-reported outcome instruments used in the study were the European Organization for Research and Treatment of Cancer (EORTC) 30-item quality-of-life (QOL) core questionnaire (QLQ-C30), the EORTC cervical cancer–specific module (QLQ-CX24), and the EuroQol EQ-5D-5L visual analog scale (VAS).
Prespecified secondary study endpoints were changes from baseline to week 36 in QLQ-C30 global health status/QOL (GHS/QOL) and physical functioning, and the QLQ-CX24 symptom-experience scale.
At baseline, patient-reported outcome scores were similar between treatment groups. Patients in both treatment groups had an initial decrease in QLQ-C30 GHS/QOL and physical functioning subscale and EQ-5D-5L VAS scores at weeks 3 and 6, but these improved relative to baseline at week 12 and subsequent weeks.
A similar number of patients in the pembrolizumab and placebo groups had improved or stable scores for QLQ-C30 GHS/QOL (76% vs 75%), QLQ-C30 physical functioning (77% vs 77%), QLQ-CX24 symptom experience (85% vs 85%) and EQ-5D-5L VAS (73% vs 76%).
Across all QOL instruments evaluated, there were no meaningful differences in patient-reported outcomes among patients who received pembrolizumab compared with those who received placebo, said Dr. Randall.
The improvement in progression-free survival, coupled with the patient-reported outcomes showing no additional harms to quality of life, support pembrolizumab plus concurrent chemoradiotherapy as a “new standard of care” for patients with high-risk locally advanced cervical cancer, she told attendees.
“We have had stunning success in cervical cancer treatments over the past 10-15 years, and now we see that the addition of pembrolizumab to standard chemotherapy not only improves outcome but very importantly does not significantly impact the quality of life in our patients,” said study discussant R. Wendel Naumann, MD, Atrium Health Levine Cancer Institute, Charlotte, North Carolina.
Funding for KEYNOTE-A18 was provided by Merck. Dr. Randall has disclosed relationships with Seagen/Genmab, Merck, GSK, ImmunoGen, AstraZeneca, and On Target Laboratories. Dr. Naumann has no relevant disclosures.
A version of this article appeared on Medscape.com.
according to patient-reported outcome analyses from the KEYNOTE-A18 trial.
Progression-free survival data from the trial, reported at the 2023 meeting of the European Society for Medical Oncology, showed a 30% reduction in the risk for progression (P =.002) with the addition of pembrolizumab vs placebo, as well as favorable overall survival trends, reported Leslie Randall, MD, with VCU Health in Richmond, Virginia. Now the new analyses bring the “voices of the patients from this large phase 3 study.”
“I think the data can put us at ease and give patients a measure of comfort because there was no detriment in the quality of life,” said Dr. Randall, who presented the data on March 17 at the Society of Gynecologic Oncology (SGO) 2024 conference.
The phase 3 KEYNOTE-A18 trial enrolled 1060 patients new to treatment who had either stage 1B2-2B disease with lymph node involvement or stage 3-4A disease. They were randomly allocated to receive pembrolizumab or placebo plus concurrent chemoradiotherapy.
Patient-reported outcome instruments used in the study were the European Organization for Research and Treatment of Cancer (EORTC) 30-item quality-of-life (QOL) core questionnaire (QLQ-C30), the EORTC cervical cancer–specific module (QLQ-CX24), and the EuroQol EQ-5D-5L visual analog scale (VAS).
Prespecified secondary study endpoints were changes from baseline to week 36 in QLQ-C30 global health status/QOL (GHS/QOL) and physical functioning, and the QLQ-CX24 symptom-experience scale.
At baseline, patient-reported outcome scores were similar between treatment groups. Patients in both treatment groups had an initial decrease in QLQ-C30 GHS/QOL and physical functioning subscale and EQ-5D-5L VAS scores at weeks 3 and 6, but these improved relative to baseline at week 12 and subsequent weeks.
A similar number of patients in the pembrolizumab and placebo groups had improved or stable scores for QLQ-C30 GHS/QOL (76% vs 75%), QLQ-C30 physical functioning (77% vs 77%), QLQ-CX24 symptom experience (85% vs 85%) and EQ-5D-5L VAS (73% vs 76%).
Across all QOL instruments evaluated, there were no meaningful differences in patient-reported outcomes among patients who received pembrolizumab compared with those who received placebo, said Dr. Randall.
The improvement in progression-free survival, coupled with the patient-reported outcomes showing no additional harms to quality of life, support pembrolizumab plus concurrent chemoradiotherapy as a “new standard of care” for patients with high-risk locally advanced cervical cancer, she told attendees.
“We have had stunning success in cervical cancer treatments over the past 10-15 years, and now we see that the addition of pembrolizumab to standard chemotherapy not only improves outcome but very importantly does not significantly impact the quality of life in our patients,” said study discussant R. Wendel Naumann, MD, Atrium Health Levine Cancer Institute, Charlotte, North Carolina.
Funding for KEYNOTE-A18 was provided by Merck. Dr. Randall has disclosed relationships with Seagen/Genmab, Merck, GSK, ImmunoGen, AstraZeneca, and On Target Laboratories. Dr. Naumann has no relevant disclosures.
A version of this article appeared on Medscape.com.
according to patient-reported outcome analyses from the KEYNOTE-A18 trial.
Progression-free survival data from the trial, reported at the 2023 meeting of the European Society for Medical Oncology, showed a 30% reduction in the risk for progression (P =.002) with the addition of pembrolizumab vs placebo, as well as favorable overall survival trends, reported Leslie Randall, MD, with VCU Health in Richmond, Virginia. Now the new analyses bring the “voices of the patients from this large phase 3 study.”
“I think the data can put us at ease and give patients a measure of comfort because there was no detriment in the quality of life,” said Dr. Randall, who presented the data on March 17 at the Society of Gynecologic Oncology (SGO) 2024 conference.
The phase 3 KEYNOTE-A18 trial enrolled 1060 patients new to treatment who had either stage 1B2-2B disease with lymph node involvement or stage 3-4A disease. They were randomly allocated to receive pembrolizumab or placebo plus concurrent chemoradiotherapy.
Patient-reported outcome instruments used in the study were the European Organization for Research and Treatment of Cancer (EORTC) 30-item quality-of-life (QOL) core questionnaire (QLQ-C30), the EORTC cervical cancer–specific module (QLQ-CX24), and the EuroQol EQ-5D-5L visual analog scale (VAS).
Prespecified secondary study endpoints were changes from baseline to week 36 in QLQ-C30 global health status/QOL (GHS/QOL) and physical functioning, and the QLQ-CX24 symptom-experience scale.
At baseline, patient-reported outcome scores were similar between treatment groups. Patients in both treatment groups had an initial decrease in QLQ-C30 GHS/QOL and physical functioning subscale and EQ-5D-5L VAS scores at weeks 3 and 6, but these improved relative to baseline at week 12 and subsequent weeks.
A similar number of patients in the pembrolizumab and placebo groups had improved or stable scores for QLQ-C30 GHS/QOL (76% vs 75%), QLQ-C30 physical functioning (77% vs 77%), QLQ-CX24 symptom experience (85% vs 85%) and EQ-5D-5L VAS (73% vs 76%).
Across all QOL instruments evaluated, there were no meaningful differences in patient-reported outcomes among patients who received pembrolizumab compared with those who received placebo, said Dr. Randall.
The improvement in progression-free survival, coupled with the patient-reported outcomes showing no additional harms to quality of life, support pembrolizumab plus concurrent chemoradiotherapy as a “new standard of care” for patients with high-risk locally advanced cervical cancer, she told attendees.
“We have had stunning success in cervical cancer treatments over the past 10-15 years, and now we see that the addition of pembrolizumab to standard chemotherapy not only improves outcome but very importantly does not significantly impact the quality of life in our patients,” said study discussant R. Wendel Naumann, MD, Atrium Health Levine Cancer Institute, Charlotte, North Carolina.
Funding for KEYNOTE-A18 was provided by Merck. Dr. Randall has disclosed relationships with Seagen/Genmab, Merck, GSK, ImmunoGen, AstraZeneca, and On Target Laboratories. Dr. Naumann has no relevant disclosures.
A version of this article appeared on Medscape.com.
Hormones and Viruses Influence Each Other: Consider These Connections in Your Patients
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.