User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Could AI tool identify type 1 diabetes earlier in childhood?
An artificial intelligence (AI)–based predictive tool may be able to identify type 1 diabetes in children earlier, before they are diagnosed as a result of potentially fatal diabetic ketoacidosis (DKA), suggests a new U.K. study.
The tool was developed by Julia Townson, PhD, senior trial manager in children and young people at Cardiff University, U.K., and colleagues.
Her team had previously shown that children who develop type 1 diabetes have a different pattern of contact with primary care in the 6 months leading up to their diagnosis.
Symptoms of type 1 diabetes include going to the toilet more and being thirsty, tired, and thin, but GPs can still miss these signs.
So they tested different combinations of factors from GP records – such as urinary tract infections or bedwetting, being prescribed antibiotics or family history of type 1 diabetes – in approximately 1 million children in Wales, more than 2,000 of whom had been diagnosed with type 1 diabetes, to train the predictive tool.
In a separate study of around 1.5 million children in England, they found that the algorithm could identify type 1 diabetes in 75% of affected children 11 days earlier than without the tool, if it was set up as an alert at every one in 10 general practice consultations.
Dr. Townson presented her research at the recent Diabetes UK Professional Conference 2022.
One-quarter of kids diagnosed with type 1 diabetes are in DKA
During her presentation, Dr. Townson explained that, in the U.K., approximately 25% of children with type 1 diabetes are diagnosed while they are in DKA, a figure that has remained unchanged for 25 years.
“We know that delayed- and misdiagnosis are the most common reasons for a child presenting in DKA at diagnosis,” she said. “And of course, the reason why it’s so important to prevent presentation in DKA is because of the considerable morbidity and potentially mortality associated with it.”
Indeed, with a simple internet search, Dr. Townson was able to identify four children who lost their lives to DKA in the past 8 years in the U.K.
“It’s encouraging to see that this research could save many families a potentially traumatic trip to the hospital by helping family doctors diagnose type 1 diabetes more rapidly,” Conor McKeever, research communications manager at the type 1 diabetes charity JDRF, told this news organization.
“This approach could go hand-in-hand with population screening, which has the potential to identify people at high risk of developing type 1 diabetes before they experience any symptoms,” he added. The hope is that “far fewer families experience DKA at the start of their type 1 diabetes journey.”
“Finding a way to catch the condition and treat it early could help to avoid emergency hospital treatment and save lives,” agreed Lucy Chambers, PhD, head of research communications at Diabetes UK, which funded the research.
How to integrate tool into GP systems
“We are now looking to see how this tool might work with primary care computer systems,” Dr. Townson said. She said in an interview that they are exploring “how it could be ‘bolted’ on to the GP’s software system.”
“It works on many different levels, but one level is frequency of consultations in relation to the frequency of previous consultations, so it needs to be able to ‘look’ through the electronic health records, at the time of the consultation, to come up with a predictive score.”
Dr. Townson said it is not clear how “easy it will be to integrate it into current systems, and I do not know of any other machine learning applications which have been used like this in primary care.”
“But we are hopeful, and we have started to contact companies who are involved in providing these systems.”
The research was funded by Diabetes UK, and the Clinical Trials Unit was funded by Health and Care Research Wales. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
An artificial intelligence (AI)–based predictive tool may be able to identify type 1 diabetes in children earlier, before they are diagnosed as a result of potentially fatal diabetic ketoacidosis (DKA), suggests a new U.K. study.
The tool was developed by Julia Townson, PhD, senior trial manager in children and young people at Cardiff University, U.K., and colleagues.
Her team had previously shown that children who develop type 1 diabetes have a different pattern of contact with primary care in the 6 months leading up to their diagnosis.
Symptoms of type 1 diabetes include going to the toilet more and being thirsty, tired, and thin, but GPs can still miss these signs.
So they tested different combinations of factors from GP records – such as urinary tract infections or bedwetting, being prescribed antibiotics or family history of type 1 diabetes – in approximately 1 million children in Wales, more than 2,000 of whom had been diagnosed with type 1 diabetes, to train the predictive tool.
In a separate study of around 1.5 million children in England, they found that the algorithm could identify type 1 diabetes in 75% of affected children 11 days earlier than without the tool, if it was set up as an alert at every one in 10 general practice consultations.
Dr. Townson presented her research at the recent Diabetes UK Professional Conference 2022.
One-quarter of kids diagnosed with type 1 diabetes are in DKA
During her presentation, Dr. Townson explained that, in the U.K., approximately 25% of children with type 1 diabetes are diagnosed while they are in DKA, a figure that has remained unchanged for 25 years.
“We know that delayed- and misdiagnosis are the most common reasons for a child presenting in DKA at diagnosis,” she said. “And of course, the reason why it’s so important to prevent presentation in DKA is because of the considerable morbidity and potentially mortality associated with it.”
Indeed, with a simple internet search, Dr. Townson was able to identify four children who lost their lives to DKA in the past 8 years in the U.K.
“It’s encouraging to see that this research could save many families a potentially traumatic trip to the hospital by helping family doctors diagnose type 1 diabetes more rapidly,” Conor McKeever, research communications manager at the type 1 diabetes charity JDRF, told this news organization.
“This approach could go hand-in-hand with population screening, which has the potential to identify people at high risk of developing type 1 diabetes before they experience any symptoms,” he added. The hope is that “far fewer families experience DKA at the start of their type 1 diabetes journey.”
“Finding a way to catch the condition and treat it early could help to avoid emergency hospital treatment and save lives,” agreed Lucy Chambers, PhD, head of research communications at Diabetes UK, which funded the research.
How to integrate tool into GP systems
“We are now looking to see how this tool might work with primary care computer systems,” Dr. Townson said. She said in an interview that they are exploring “how it could be ‘bolted’ on to the GP’s software system.”
“It works on many different levels, but one level is frequency of consultations in relation to the frequency of previous consultations, so it needs to be able to ‘look’ through the electronic health records, at the time of the consultation, to come up with a predictive score.”
Dr. Townson said it is not clear how “easy it will be to integrate it into current systems, and I do not know of any other machine learning applications which have been used like this in primary care.”
“But we are hopeful, and we have started to contact companies who are involved in providing these systems.”
The research was funded by Diabetes UK, and the Clinical Trials Unit was funded by Health and Care Research Wales. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
An artificial intelligence (AI)–based predictive tool may be able to identify type 1 diabetes in children earlier, before they are diagnosed as a result of potentially fatal diabetic ketoacidosis (DKA), suggests a new U.K. study.
The tool was developed by Julia Townson, PhD, senior trial manager in children and young people at Cardiff University, U.K., and colleagues.
Her team had previously shown that children who develop type 1 diabetes have a different pattern of contact with primary care in the 6 months leading up to their diagnosis.
Symptoms of type 1 diabetes include going to the toilet more and being thirsty, tired, and thin, but GPs can still miss these signs.
So they tested different combinations of factors from GP records – such as urinary tract infections or bedwetting, being prescribed antibiotics or family history of type 1 diabetes – in approximately 1 million children in Wales, more than 2,000 of whom had been diagnosed with type 1 diabetes, to train the predictive tool.
In a separate study of around 1.5 million children in England, they found that the algorithm could identify type 1 diabetes in 75% of affected children 11 days earlier than without the tool, if it was set up as an alert at every one in 10 general practice consultations.
Dr. Townson presented her research at the recent Diabetes UK Professional Conference 2022.
One-quarter of kids diagnosed with type 1 diabetes are in DKA
During her presentation, Dr. Townson explained that, in the U.K., approximately 25% of children with type 1 diabetes are diagnosed while they are in DKA, a figure that has remained unchanged for 25 years.
“We know that delayed- and misdiagnosis are the most common reasons for a child presenting in DKA at diagnosis,” she said. “And of course, the reason why it’s so important to prevent presentation in DKA is because of the considerable morbidity and potentially mortality associated with it.”
Indeed, with a simple internet search, Dr. Townson was able to identify four children who lost their lives to DKA in the past 8 years in the U.K.
“It’s encouraging to see that this research could save many families a potentially traumatic trip to the hospital by helping family doctors diagnose type 1 diabetes more rapidly,” Conor McKeever, research communications manager at the type 1 diabetes charity JDRF, told this news organization.
“This approach could go hand-in-hand with population screening, which has the potential to identify people at high risk of developing type 1 diabetes before they experience any symptoms,” he added. The hope is that “far fewer families experience DKA at the start of their type 1 diabetes journey.”
“Finding a way to catch the condition and treat it early could help to avoid emergency hospital treatment and save lives,” agreed Lucy Chambers, PhD, head of research communications at Diabetes UK, which funded the research.
How to integrate tool into GP systems
“We are now looking to see how this tool might work with primary care computer systems,” Dr. Townson said. She said in an interview that they are exploring “how it could be ‘bolted’ on to the GP’s software system.”
“It works on many different levels, but one level is frequency of consultations in relation to the frequency of previous consultations, so it needs to be able to ‘look’ through the electronic health records, at the time of the consultation, to come up with a predictive score.”
Dr. Townson said it is not clear how “easy it will be to integrate it into current systems, and I do not know of any other machine learning applications which have been used like this in primary care.”
“But we are hopeful, and we have started to contact companies who are involved in providing these systems.”
The research was funded by Diabetes UK, and the Clinical Trials Unit was funded by Health and Care Research Wales. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
Nanoparticle shows promise for ALS
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.

Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.
Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
SEATTLE – , which was the change in the summated motor unit index (MUNIX) from baseline to week 36.
The drug, CNM-Au8, is being developed by Clene, and would represent a novel mechanism of action. “This is a brand-new approach. We used it complementary with riluzole and it was well tolerated, so I see this as an add-on therapy. I think if we can show some more positivity and longer-term results, it’s going to be a game changer for ALS,” Matthew Kiernan, MBBS, PhD, said in an interview. Dr. Kiernan presented the results at the 2022 annual meeting of the American Academy of Neurology.
Riluzole (Rilutek), which received Food and Drug Administration approval in 1995, inhibits glutamate release to counter excitotoxicity, which is believed to play a role in ALS, Huntington’s disease, ischemia, and other acute and chronic neurodegenerative diseases. The other FDA-approved agent for ALS is the neuroprotective agent and free-radical scavenger edaravone (Radicava), approved in 2017.
CNM-Au8 is made up of catalytically active gold nanocrystals that cross the blood-brain barrier, but lacks the toxicity associated with other synthetic gold compounds, according to the company. The formulation is also being investigated for the treatment of Parkinson’s disease and multiple sclerosis. Basic research has shown that it stabilizes mitochondria and reduces accumulation of the TDP-43 protein, which is linked to spread of ALS through the brain, Dr. Kiernan said during his presentation.
The treatment is well tolerated. “Normally in an ALS trial, we see about a 25% dropout rate. There were no dropouts on the active compound in the clinical trial. There are less deaths, so improved survival,” said Dr. Kiernan, the Bushell chair of neurology at the University of Sydney and codirector of the Brain and Mind Center in Sydney.
Good safety signal
The fact that the trial missed its primary endpoint isn’t too concerning, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “ALS clinical trials are incredibly difficult to conduct, especially a phase 2 learning-phase clinical trial. At this phase, I’m much more buoyed by the fact that they have a good safety signal, and that they’re willing to move forward to that phase 3 clinical trial,” Dr. Johnson said in an interview. He is vice chair of research at Virginia Commonwealth University, Richmond.
A phase 3 clinical trial is in development in the United States and Europe. The drug also is included as part of the HEALEY ALS Platform Trial, which is testing multiple ALS therapies simultaneously. “The results from that should be available by the second half of this year and it will also inform us as to what the approach should be,” said Dr. Kiernan.
Dr. Johnson also was enthusiastic. “I’m excited to see the results in terms of the primary endpoints for that next phase 3 clinical trial,” he said.
Ongoing research
In September 2021, Clene announced a second expanded access program for people with ALS.
The study included a 36-week double-blind treatment period followed by long-term, open-label follow-up. Twenty-three patients received 30 mg CNM-Au8, and 22 received placebo. In the first 36 weeks, the treatment group was more likely to have no disease progression, defined as death, tracheostomy, noninvasive ventilation, or a gastronomy tube (P = .0125). The researchers compared the probability of experiencing a less than 6-point decline in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale. At 12 weeks, it was about 85% in both groups. At 24 weeks, it was about 60% to 50% in favor of the CNM-Au8 group, and at 36 weeks it was about 50% to 20% (P = .0350).
At 36 weeks, quality of life as measured by the ALS Specific Quality of Life–Short Form was better in the treatment group at 36 weeks (mean change, 0.9; P = .0177).
Survival was better in the treatment group at 96 weeks than the mortality derived from a European Network for the Cure of ALS prediction model (hazard ratio [HR], 0.2974; P = .0068). This benefit also was experienced by patients who received drug throughout the study (HR, 0.36; 95% confidence interval [CI], 0.12-1.1) and those who started out on placebo and converted to active drug during the open-label period (HR, 0.24; 95% CI, 0.064-0.88).
The study was funded by Clene and FightMND. Dr. Kiernan and Dr. Johnson have no relevant financial disclosures.
AT AAN 2022
Extraction of infected implanted cardiac devices rare, despite guidelines
The rates of infection involving cardiac implanted electronic devices (CIEDs), like pacemakers and cardioverter defibrillators (ICDs), are substantial, but only a minority of patients in the United States receive the guideline-directed recommendation of device removal, according to data from a Medicare population.
The study was conducted on the hypothesis that adherence to guidelines were low, “but we were surprised by how low the extraction rates turned out to be,” Sean D. Pokorney, MD, an electrophysiologist at the Duke Clinical Research Institute, Durham, N.C., reported at the annual scientific sessions of the American College of Cardiology.
The major U.S. and European guidelines are uniform in recommending complete extraction for a CIED infection. The American Heart Association and the Heart Rhythm Society and two out of the three other guidelines cited by Dr. Pokorney not only recommend extraction but specify prompt extraction.
Neither complete extraction nor prompt extraction are typical.
Of the 11,619 CIED infection cases identified in the Medicare database, 18.2% underwent extraction within 30 days of diagnosis. Only 13% were extracted within 6 days.
Lack of extraction may cause avoidable mortality
The result is likely to be avoidable mortality. Among those with extraction within 30 days, 80% were still alive 1 year later. Survival at 1 year fell to 67.6% in those without an extraction within this time frame.
This translated to a 22% lower rate of death at 1 year (hazard ratio, 0.78; P = .008) in those who underwent extraction within 30 days.
For those in whom the device was extracted within 7 days, the associated HR for death at 1 year was more than 40% lower (HR, 0.59; P < .001), reported Dr. Pokorney, who characterized these reductions as occurring in “a dose-response fashion.”
The very high risk of relapse despite antibiotics is the reason that “there is a class 1 indication for complete hardware removal,” Dr. Pokorney. He cited five studies that addressed this question. With partial device removal or medical therapy alone, relapse was consistently 50% or greater. In one study, it was 67%. In another it was 100%.
With complete removal, the rate of infection relapse was 1% or lower in four. In the fifth, the rate was 4.2%.
Infections can occur early or late after implantation, but cases accumulate over time. In the Medicare data sample, infection rates climbed from 0.3% at 1 year to 0.6% at 2 years and then to 1.1% at 3 years, Dr. Pokorney reported.
Other studies have also shown a steady increase in the proportion of implanted devices associated with infection over time. In a cohort study conducted in Olmstead County, Minnesota, the cumulative probability of a CIED infection reached 6.2% after 15 years and 11.7% after 25 years. While about half of these were infections localized to the device pocket, the others were potentially life-threatening systemic infections, according to Dr. Pokorney, who cited this study.
In his analysis of the Medicare data, all fee-for-service patients receiving a first CIED implant over a period of 14 years were included. The 14-year period ended just before the COVID-19 epidemic.
The more than 11,000 CIED infections were identified in 1,065,549 total CIED patients. Most (72%) had received a pacemaker. Of the others , more than half received an ICD and the others received a cardiac resynchronization device. The median age was 78 years.
Female and Black patients even less likely to undergo extraction
About half (49.1%) of the overall study population was female, but females represented only about 40% of those who developed an infection. Blacks represented just under 8% of the population but nearly 16% of the CIED infections. Both females and Blacks were significantly less likely than the overall study population to undergo extraction for their infection (P < .001 for both).
Perhaps predictably, patients with comorbidities were more likely to develop CIED infections. For example, 87% of those with infection, versus only 64.9% of the overall population, were in heart failure at the time of implantation. Diabetes (68.3% vs. 49.3%), ischemic heart disease (91.9% vs. 79.4%), renal disease (70.5% vs. 37.9%), and chronic obstructive pulmonary disease (70.6% vs. 55.0%) were also more common at baseline in those who went on to a CIED infection than in the overall population.
Based on the evidence that there is a large unmet need to improve adherence to the guidelines, Dr. Pokorney called for care pathways and other quality initiatives to address the problem.
The reasons that so many patients are not undergoing prompt device extraction at the time of infection is unclear, but Dr. Pokorney offered some hypotheses.
“There appears to be a false belief in the efficacy of antibiotics for treating CIED infections,” Dr. Pokorney said.
Comorbidities shouldn’t delay extraction
It is also possible that clinicians are concerned about performing extractions in patients with multiple comorbidities. If clinicians are delaying extractions for this reason, Dr. Pokorney suggested this behavior is misdirected given the fact that delays appear to increase mortality risk.
Several experts, including Rachel Lambert, MD, an electrophysiologist and professor of medicine at Yale University, New Haven, Conn., agreed that these data deserve a response.
“I was not surprised by the mortality data, but I was surprised at this low extraction rate,” said Dr. Lambert, who concurs with the guidelines. She indicated this study provides teeth to prompt action.
“It is great to have these data about the increased mortality risk to back up the guidelines,” she said.
More information is needed to understand exactly why CIED infection is not now leading to guideline-directed care. Dr. Pokorney said: “Where do we go from here is a key question.”
While several different types of initiatives might be needed, Dr. Pokorney called for regionalization of care to address the fact that not every center that places CIEDs has the capability to perform extractions.
“Extraction is not available at every center, and it probably should not be available at every center, so mechanisms are need to get patients with infection to the specialized centers that provide care,” he said.
Dr. Pokorney has financial relationships with Boston Scientific, Bristol-Myers Squibb, Gilead, Janssen, Medtronic, Pfizer, and Philips. Dr. Lambert reported financial relationships with Abbott, Amgen, and Medtronic.
The rates of infection involving cardiac implanted electronic devices (CIEDs), like pacemakers and cardioverter defibrillators (ICDs), are substantial, but only a minority of patients in the United States receive the guideline-directed recommendation of device removal, according to data from a Medicare population.
The study was conducted on the hypothesis that adherence to guidelines were low, “but we were surprised by how low the extraction rates turned out to be,” Sean D. Pokorney, MD, an electrophysiologist at the Duke Clinical Research Institute, Durham, N.C., reported at the annual scientific sessions of the American College of Cardiology.
The major U.S. and European guidelines are uniform in recommending complete extraction for a CIED infection. The American Heart Association and the Heart Rhythm Society and two out of the three other guidelines cited by Dr. Pokorney not only recommend extraction but specify prompt extraction.
Neither complete extraction nor prompt extraction are typical.
Of the 11,619 CIED infection cases identified in the Medicare database, 18.2% underwent extraction within 30 days of diagnosis. Only 13% were extracted within 6 days.
Lack of extraction may cause avoidable mortality
The result is likely to be avoidable mortality. Among those with extraction within 30 days, 80% were still alive 1 year later. Survival at 1 year fell to 67.6% in those without an extraction within this time frame.
This translated to a 22% lower rate of death at 1 year (hazard ratio, 0.78; P = .008) in those who underwent extraction within 30 days.
For those in whom the device was extracted within 7 days, the associated HR for death at 1 year was more than 40% lower (HR, 0.59; P < .001), reported Dr. Pokorney, who characterized these reductions as occurring in “a dose-response fashion.”
The very high risk of relapse despite antibiotics is the reason that “there is a class 1 indication for complete hardware removal,” Dr. Pokorney. He cited five studies that addressed this question. With partial device removal or medical therapy alone, relapse was consistently 50% or greater. In one study, it was 67%. In another it was 100%.
With complete removal, the rate of infection relapse was 1% or lower in four. In the fifth, the rate was 4.2%.
Infections can occur early or late after implantation, but cases accumulate over time. In the Medicare data sample, infection rates climbed from 0.3% at 1 year to 0.6% at 2 years and then to 1.1% at 3 years, Dr. Pokorney reported.
Other studies have also shown a steady increase in the proportion of implanted devices associated with infection over time. In a cohort study conducted in Olmstead County, Minnesota, the cumulative probability of a CIED infection reached 6.2% after 15 years and 11.7% after 25 years. While about half of these were infections localized to the device pocket, the others were potentially life-threatening systemic infections, according to Dr. Pokorney, who cited this study.
In his analysis of the Medicare data, all fee-for-service patients receiving a first CIED implant over a period of 14 years were included. The 14-year period ended just before the COVID-19 epidemic.
The more than 11,000 CIED infections were identified in 1,065,549 total CIED patients. Most (72%) had received a pacemaker. Of the others , more than half received an ICD and the others received a cardiac resynchronization device. The median age was 78 years.
Female and Black patients even less likely to undergo extraction
About half (49.1%) of the overall study population was female, but females represented only about 40% of those who developed an infection. Blacks represented just under 8% of the population but nearly 16% of the CIED infections. Both females and Blacks were significantly less likely than the overall study population to undergo extraction for their infection (P < .001 for both).
Perhaps predictably, patients with comorbidities were more likely to develop CIED infections. For example, 87% of those with infection, versus only 64.9% of the overall population, were in heart failure at the time of implantation. Diabetes (68.3% vs. 49.3%), ischemic heart disease (91.9% vs. 79.4%), renal disease (70.5% vs. 37.9%), and chronic obstructive pulmonary disease (70.6% vs. 55.0%) were also more common at baseline in those who went on to a CIED infection than in the overall population.
Based on the evidence that there is a large unmet need to improve adherence to the guidelines, Dr. Pokorney called for care pathways and other quality initiatives to address the problem.
The reasons that so many patients are not undergoing prompt device extraction at the time of infection is unclear, but Dr. Pokorney offered some hypotheses.
“There appears to be a false belief in the efficacy of antibiotics for treating CIED infections,” Dr. Pokorney said.
Comorbidities shouldn’t delay extraction
It is also possible that clinicians are concerned about performing extractions in patients with multiple comorbidities. If clinicians are delaying extractions for this reason, Dr. Pokorney suggested this behavior is misdirected given the fact that delays appear to increase mortality risk.
Several experts, including Rachel Lambert, MD, an electrophysiologist and professor of medicine at Yale University, New Haven, Conn., agreed that these data deserve a response.
“I was not surprised by the mortality data, but I was surprised at this low extraction rate,” said Dr. Lambert, who concurs with the guidelines. She indicated this study provides teeth to prompt action.
“It is great to have these data about the increased mortality risk to back up the guidelines,” she said.
More information is needed to understand exactly why CIED infection is not now leading to guideline-directed care. Dr. Pokorney said: “Where do we go from here is a key question.”
While several different types of initiatives might be needed, Dr. Pokorney called for regionalization of care to address the fact that not every center that places CIEDs has the capability to perform extractions.
“Extraction is not available at every center, and it probably should not be available at every center, so mechanisms are need to get patients with infection to the specialized centers that provide care,” he said.
Dr. Pokorney has financial relationships with Boston Scientific, Bristol-Myers Squibb, Gilead, Janssen, Medtronic, Pfizer, and Philips. Dr. Lambert reported financial relationships with Abbott, Amgen, and Medtronic.
The rates of infection involving cardiac implanted electronic devices (CIEDs), like pacemakers and cardioverter defibrillators (ICDs), are substantial, but only a minority of patients in the United States receive the guideline-directed recommendation of device removal, according to data from a Medicare population.
The study was conducted on the hypothesis that adherence to guidelines were low, “but we were surprised by how low the extraction rates turned out to be,” Sean D. Pokorney, MD, an electrophysiologist at the Duke Clinical Research Institute, Durham, N.C., reported at the annual scientific sessions of the American College of Cardiology.
The major U.S. and European guidelines are uniform in recommending complete extraction for a CIED infection. The American Heart Association and the Heart Rhythm Society and two out of the three other guidelines cited by Dr. Pokorney not only recommend extraction but specify prompt extraction.
Neither complete extraction nor prompt extraction are typical.
Of the 11,619 CIED infection cases identified in the Medicare database, 18.2% underwent extraction within 30 days of diagnosis. Only 13% were extracted within 6 days.
Lack of extraction may cause avoidable mortality
The result is likely to be avoidable mortality. Among those with extraction within 30 days, 80% were still alive 1 year later. Survival at 1 year fell to 67.6% in those without an extraction within this time frame.
This translated to a 22% lower rate of death at 1 year (hazard ratio, 0.78; P = .008) in those who underwent extraction within 30 days.
For those in whom the device was extracted within 7 days, the associated HR for death at 1 year was more than 40% lower (HR, 0.59; P < .001), reported Dr. Pokorney, who characterized these reductions as occurring in “a dose-response fashion.”
The very high risk of relapse despite antibiotics is the reason that “there is a class 1 indication for complete hardware removal,” Dr. Pokorney. He cited five studies that addressed this question. With partial device removal or medical therapy alone, relapse was consistently 50% or greater. In one study, it was 67%. In another it was 100%.
With complete removal, the rate of infection relapse was 1% or lower in four. In the fifth, the rate was 4.2%.
Infections can occur early or late after implantation, but cases accumulate over time. In the Medicare data sample, infection rates climbed from 0.3% at 1 year to 0.6% at 2 years and then to 1.1% at 3 years, Dr. Pokorney reported.
Other studies have also shown a steady increase in the proportion of implanted devices associated with infection over time. In a cohort study conducted in Olmstead County, Minnesota, the cumulative probability of a CIED infection reached 6.2% after 15 years and 11.7% after 25 years. While about half of these were infections localized to the device pocket, the others were potentially life-threatening systemic infections, according to Dr. Pokorney, who cited this study.
In his analysis of the Medicare data, all fee-for-service patients receiving a first CIED implant over a period of 14 years were included. The 14-year period ended just before the COVID-19 epidemic.
The more than 11,000 CIED infections were identified in 1,065,549 total CIED patients. Most (72%) had received a pacemaker. Of the others , more than half received an ICD and the others received a cardiac resynchronization device. The median age was 78 years.
Female and Black patients even less likely to undergo extraction
About half (49.1%) of the overall study population was female, but females represented only about 40% of those who developed an infection. Blacks represented just under 8% of the population but nearly 16% of the CIED infections. Both females and Blacks were significantly less likely than the overall study population to undergo extraction for their infection (P < .001 for both).
Perhaps predictably, patients with comorbidities were more likely to develop CIED infections. For example, 87% of those with infection, versus only 64.9% of the overall population, were in heart failure at the time of implantation. Diabetes (68.3% vs. 49.3%), ischemic heart disease (91.9% vs. 79.4%), renal disease (70.5% vs. 37.9%), and chronic obstructive pulmonary disease (70.6% vs. 55.0%) were also more common at baseline in those who went on to a CIED infection than in the overall population.
Based on the evidence that there is a large unmet need to improve adherence to the guidelines, Dr. Pokorney called for care pathways and other quality initiatives to address the problem.
The reasons that so many patients are not undergoing prompt device extraction at the time of infection is unclear, but Dr. Pokorney offered some hypotheses.
“There appears to be a false belief in the efficacy of antibiotics for treating CIED infections,” Dr. Pokorney said.
Comorbidities shouldn’t delay extraction
It is also possible that clinicians are concerned about performing extractions in patients with multiple comorbidities. If clinicians are delaying extractions for this reason, Dr. Pokorney suggested this behavior is misdirected given the fact that delays appear to increase mortality risk.
Several experts, including Rachel Lambert, MD, an electrophysiologist and professor of medicine at Yale University, New Haven, Conn., agreed that these data deserve a response.
“I was not surprised by the mortality data, but I was surprised at this low extraction rate,” said Dr. Lambert, who concurs with the guidelines. She indicated this study provides teeth to prompt action.
“It is great to have these data about the increased mortality risk to back up the guidelines,” she said.
More information is needed to understand exactly why CIED infection is not now leading to guideline-directed care. Dr. Pokorney said: “Where do we go from here is a key question.”
While several different types of initiatives might be needed, Dr. Pokorney called for regionalization of care to address the fact that not every center that places CIEDs has the capability to perform extractions.
“Extraction is not available at every center, and it probably should not be available at every center, so mechanisms are need to get patients with infection to the specialized centers that provide care,” he said.
Dr. Pokorney has financial relationships with Boston Scientific, Bristol-Myers Squibb, Gilead, Janssen, Medtronic, Pfizer, and Philips. Dr. Lambert reported financial relationships with Abbott, Amgen, and Medtronic.
FROM ACC 2022
Physical fitness tied to lower risk of Alzheimer’s disease
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
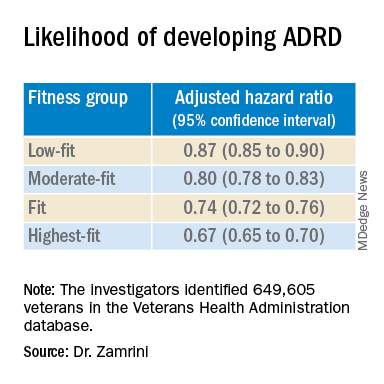
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
More years of ice hockey play tied to higher CTE risk
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Novel medication tied to better quality of life in major depression
DENVER –
In a phase 3 trial that included more than 500 adult patients with MDD, those who received zuranolone for 14 days showed greater improvement at day 15 across numerous QoL outcomes, compared with their counterparts in the placebo group.

In addition, combined analysis of four zuranolone clinical trials showed “mental well-being and functioning improved to near general population norm levels” for the active-treatment group, reported the researchers, led by Anita H. Clayton, MD, chair and professor of psychiatry, University of Virginia, Charlottesville.
“Based on these integrated analyses, the benefit of treatment with zuranolone may extend beyond reduction in depressive symptoms to include potential improvement in quality of life and overall health, as perceived by patients,” they add.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
First oral formulation
Zuranolone represents the second entry in the new class of neuroactive steroid drugs, which modulate GABA-A receptor activity – but it would be the first to have an oral formulation. Brexanolone, which was approved by the Food and Drug Administration in 2019 for postpartum depression, is administered through continuous IV infusion over 60 hours.
As previously reported by this news organization, zuranolone improved depressive symptoms as early as day 3, achieving the primary endpoint of significantly greater reduction in scores on the 17-item Hamilton Rating Scale for Depression from baseline to day 15 versus placebo (P = .014).
In the new analysis, patient-reported measures of functional health and well-being were assessed in the WATERFALL trial. It included 266 patients with MDD who were treated with zuranolone 50 mg daily for 2 weeks and 268 patients with MDD who were treated with placebo.
The study used the Short Form–36 (SF-36v2), which covers a wide range of patient-reported measures, including physical function, bodily pain, general health, vitality, social function, and “role-emotional” symptoms.
Results showed that although the treatment and placebo groups had similar baseline SF-36v2 scores, those receiving zuranolone reported significantly greater improvements at day 15 in almost all of the assessment’s domains, including physical function (treatment difference, 0.8), general health (1.0), vitality (3.1), social functioning (1.1), and role-emotional symptoms (1.5; for all comparisons, P < .05). The only exceptions were in role-physical symptoms and bodily pain.
In measures that included physical function, bodily pain, and general health, the patients achieved improvements at day 15 that were consistent with normal levels, with the improvement in vitality considered clinically meaningful versus placebo.
Integrated data
In further analysis of integrated data from four zuranolone clinical trials in the NEST and LANDSCAPE programs for patients with MDD and postpartum depression, results showed similar improvements at day 15 for zuranolone in QoL and overall health across all of the SF-36v2 functioning and well-being domains (P <.05), with the exceptions of physical measure and bodily pain.
By day 42, all of the domains showed significantly greater improvement with zuranolone versus placebo (all, P <.05).
Among the strongest score improvements in the integrated trials were measures in social functioning, which improved from baseline scores of 29.66 to 42.82 on day 15 and to 43.59 on day 42.
Emotional domain scores improved from 24.43 at baseline to 39.13 on day 15 and to 39.82 on day 42. For mental health, the integrated scores for the zuranolone group improved from 27.13 at baseline to 42.40 on day 15 and 42.62 on day 42.
Of note, the baseline scores for mental health represented just 54.3% of those in the normal population; with the increase at day 15, the level was 84.8% of the normal population.
“Across four completed placebo-controlled NEST and LANDSCAPE clinical trials, patient reports of functional health and well-being as assessed by the SF-36v2 indicated substantial impairment at baseline compared to the population norm,” the researchers reported.
The improvements are especially important in light of the fact that in some patients with MDD, functional improvement is a top priority.
“Patients have often prioritized returning to their usual level of functioning over reduction in depressive symptoms, and functional recovery has been associated with better prognosis of depression,” the investigators wrote.
Zuranolone trials have shown that treatment-emergent adverse events (AEs) occur among about 60% of patients, versus about 44% with placebo. The most common AEs are somnolence, dizziness, headache, sedation, and diarrhea, with no increases in suicidal ideation or withdrawal.
The rates of severe AEs are low, and they are observed in about 3% of patients, versus 1.1% with placebo, the researchers noted.
Further, as opposed to serotonergic antidepressants such as SNRIs and SSRIs, zuranolone does not appear to have the undesirable side effects of decreased libido and sexual dysfunction, they added.
Clinically meaningful?
Andrew J. Cutler, MD, clinical associate professor of psychiatry at State University of New York, Syracuse, said the data are “very significant” for a number of reasons.
“We need more options to treat depression, especially ones with novel mechanisms of action and faster onset of efficacy, such as zuranolone,” said Dr. Cutler, who was not involved in the current study. He has coauthored other studies on zuranolone.
Regarding the study’s QoL outcomes, “while improvement in depressive symptoms is very important, what really matters to patients is improvement in function and quality of life,” Dr. Cutler noted.
Also commenting on the study, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences and professor of psychiatry, neuroscience, and pediatrics at Albert Einstein College of Medicine, New York, said the investigational drug could represent an important addition to the armamentarium for treating depression.
“Zuranolone has good oral bioavailability and would represent the first neuroactive steroid antidepressant available in oral form and, indeed, the first non–monoamine-based antidepressant available in oral form,” he said in an interview.

Dr. Alpert was not involved in the research and has no relationship with the drug’s development.
He noted that although there are modest differences between the patients who received zuranolone and those who received placebo in the trials, “this may have been related to high placebo response rates, which often complicate antidepressant trials.
“Further research is needed to determine whether differences between zuranolone and placebo are clinically meaningful, though the separation between drug and placebo on the primary endpoint, as well as some other measures, such as quality of life measures, is promising,” Dr. Alpert said.
However, he added that comparisons with other active antidepressants in terms of efficacy and tolerability remain to be seen.
“Given the large number of individuals with major depressive disorder who have incomplete response to or do not tolerate monoaminergic antidepressants, the development of agents that leverage novel nonmonoaminergic mechanisms is important,” Dr. Alpert concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Cutler has been involved in research of zuranolone for Sage Therapeutics. Dr. Alpert has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER –
In a phase 3 trial that included more than 500 adult patients with MDD, those who received zuranolone for 14 days showed greater improvement at day 15 across numerous QoL outcomes, compared with their counterparts in the placebo group.
In addition, combined analysis of four zuranolone clinical trials showed “mental well-being and functioning improved to near general population norm levels” for the active-treatment group, reported the researchers, led by Anita H. Clayton, MD, chair and professor of psychiatry, University of Virginia, Charlottesville.
“Based on these integrated analyses, the benefit of treatment with zuranolone may extend beyond reduction in depressive symptoms to include potential improvement in quality of life and overall health, as perceived by patients,” they add.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
First oral formulation
Zuranolone represents the second entry in the new class of neuroactive steroid drugs, which modulate GABA-A receptor activity – but it would be the first to have an oral formulation. Brexanolone, which was approved by the Food and Drug Administration in 2019 for postpartum depression, is administered through continuous IV infusion over 60 hours.
As previously reported by this news organization, zuranolone improved depressive symptoms as early as day 3, achieving the primary endpoint of significantly greater reduction in scores on the 17-item Hamilton Rating Scale for Depression from baseline to day 15 versus placebo (P = .014).
In the new analysis, patient-reported measures of functional health and well-being were assessed in the WATERFALL trial. It included 266 patients with MDD who were treated with zuranolone 50 mg daily for 2 weeks and 268 patients with MDD who were treated with placebo.
The study used the Short Form–36 (SF-36v2), which covers a wide range of patient-reported measures, including physical function, bodily pain, general health, vitality, social function, and “role-emotional” symptoms.
Results showed that although the treatment and placebo groups had similar baseline SF-36v2 scores, those receiving zuranolone reported significantly greater improvements at day 15 in almost all of the assessment’s domains, including physical function (treatment difference, 0.8), general health (1.0), vitality (3.1), social functioning (1.1), and role-emotional symptoms (1.5; for all comparisons, P < .05). The only exceptions were in role-physical symptoms and bodily pain.
In measures that included physical function, bodily pain, and general health, the patients achieved improvements at day 15 that were consistent with normal levels, with the improvement in vitality considered clinically meaningful versus placebo.
Integrated data
In further analysis of integrated data from four zuranolone clinical trials in the NEST and LANDSCAPE programs for patients with MDD and postpartum depression, results showed similar improvements at day 15 for zuranolone in QoL and overall health across all of the SF-36v2 functioning and well-being domains (P <.05), with the exceptions of physical measure and bodily pain.
By day 42, all of the domains showed significantly greater improvement with zuranolone versus placebo (all, P <.05).
Among the strongest score improvements in the integrated trials were measures in social functioning, which improved from baseline scores of 29.66 to 42.82 on day 15 and to 43.59 on day 42.
Emotional domain scores improved from 24.43 at baseline to 39.13 on day 15 and to 39.82 on day 42. For mental health, the integrated scores for the zuranolone group improved from 27.13 at baseline to 42.40 on day 15 and 42.62 on day 42.
Of note, the baseline scores for mental health represented just 54.3% of those in the normal population; with the increase at day 15, the level was 84.8% of the normal population.
“Across four completed placebo-controlled NEST and LANDSCAPE clinical trials, patient reports of functional health and well-being as assessed by the SF-36v2 indicated substantial impairment at baseline compared to the population norm,” the researchers reported.
The improvements are especially important in light of the fact that in some patients with MDD, functional improvement is a top priority.
“Patients have often prioritized returning to their usual level of functioning over reduction in depressive symptoms, and functional recovery has been associated with better prognosis of depression,” the investigators wrote.
Zuranolone trials have shown that treatment-emergent adverse events (AEs) occur among about 60% of patients, versus about 44% with placebo. The most common AEs are somnolence, dizziness, headache, sedation, and diarrhea, with no increases in suicidal ideation or withdrawal.
The rates of severe AEs are low, and they are observed in about 3% of patients, versus 1.1% with placebo, the researchers noted.
Further, as opposed to serotonergic antidepressants such as SNRIs and SSRIs, zuranolone does not appear to have the undesirable side effects of decreased libido and sexual dysfunction, they added.
Clinically meaningful?
Andrew J. Cutler, MD, clinical associate professor of psychiatry at State University of New York, Syracuse, said the data are “very significant” for a number of reasons.
“We need more options to treat depression, especially ones with novel mechanisms of action and faster onset of efficacy, such as zuranolone,” said Dr. Cutler, who was not involved in the current study. He has coauthored other studies on zuranolone.
Regarding the study’s QoL outcomes, “while improvement in depressive symptoms is very important, what really matters to patients is improvement in function and quality of life,” Dr. Cutler noted.
Also commenting on the study, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences and professor of psychiatry, neuroscience, and pediatrics at Albert Einstein College of Medicine, New York, said the investigational drug could represent an important addition to the armamentarium for treating depression.
“Zuranolone has good oral bioavailability and would represent the first neuroactive steroid antidepressant available in oral form and, indeed, the first non–monoamine-based antidepressant available in oral form,” he said in an interview.
Dr. Alpert was not involved in the research and has no relationship with the drug’s development.
He noted that although there are modest differences between the patients who received zuranolone and those who received placebo in the trials, “this may have been related to high placebo response rates, which often complicate antidepressant trials.
“Further research is needed to determine whether differences between zuranolone and placebo are clinically meaningful, though the separation between drug and placebo on the primary endpoint, as well as some other measures, such as quality of life measures, is promising,” Dr. Alpert said.
However, he added that comparisons with other active antidepressants in terms of efficacy and tolerability remain to be seen.
“Given the large number of individuals with major depressive disorder who have incomplete response to or do not tolerate monoaminergic antidepressants, the development of agents that leverage novel nonmonoaminergic mechanisms is important,” Dr. Alpert concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Cutler has been involved in research of zuranolone for Sage Therapeutics. Dr. Alpert has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER –
In a phase 3 trial that included more than 500 adult patients with MDD, those who received zuranolone for 14 days showed greater improvement at day 15 across numerous QoL outcomes, compared with their counterparts in the placebo group.
In addition, combined analysis of four zuranolone clinical trials showed “mental well-being and functioning improved to near general population norm levels” for the active-treatment group, reported the researchers, led by Anita H. Clayton, MD, chair and professor of psychiatry, University of Virginia, Charlottesville.
“Based on these integrated analyses, the benefit of treatment with zuranolone may extend beyond reduction in depressive symptoms to include potential improvement in quality of life and overall health, as perceived by patients,” they add.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
First oral formulation
Zuranolone represents the second entry in the new class of neuroactive steroid drugs, which modulate GABA-A receptor activity – but it would be the first to have an oral formulation. Brexanolone, which was approved by the Food and Drug Administration in 2019 for postpartum depression, is administered through continuous IV infusion over 60 hours.
As previously reported by this news organization, zuranolone improved depressive symptoms as early as day 3, achieving the primary endpoint of significantly greater reduction in scores on the 17-item Hamilton Rating Scale for Depression from baseline to day 15 versus placebo (P = .014).
In the new analysis, patient-reported measures of functional health and well-being were assessed in the WATERFALL trial. It included 266 patients with MDD who were treated with zuranolone 50 mg daily for 2 weeks and 268 patients with MDD who were treated with placebo.
The study used the Short Form–36 (SF-36v2), which covers a wide range of patient-reported measures, including physical function, bodily pain, general health, vitality, social function, and “role-emotional” symptoms.
Results showed that although the treatment and placebo groups had similar baseline SF-36v2 scores, those receiving zuranolone reported significantly greater improvements at day 15 in almost all of the assessment’s domains, including physical function (treatment difference, 0.8), general health (1.0), vitality (3.1), social functioning (1.1), and role-emotional symptoms (1.5; for all comparisons, P < .05). The only exceptions were in role-physical symptoms and bodily pain.
In measures that included physical function, bodily pain, and general health, the patients achieved improvements at day 15 that were consistent with normal levels, with the improvement in vitality considered clinically meaningful versus placebo.
Integrated data
In further analysis of integrated data from four zuranolone clinical trials in the NEST and LANDSCAPE programs for patients with MDD and postpartum depression, results showed similar improvements at day 15 for zuranolone in QoL and overall health across all of the SF-36v2 functioning and well-being domains (P <.05), with the exceptions of physical measure and bodily pain.
By day 42, all of the domains showed significantly greater improvement with zuranolone versus placebo (all, P <.05).
Among the strongest score improvements in the integrated trials were measures in social functioning, which improved from baseline scores of 29.66 to 42.82 on day 15 and to 43.59 on day 42.
Emotional domain scores improved from 24.43 at baseline to 39.13 on day 15 and to 39.82 on day 42. For mental health, the integrated scores for the zuranolone group improved from 27.13 at baseline to 42.40 on day 15 and 42.62 on day 42.
Of note, the baseline scores for mental health represented just 54.3% of those in the normal population; with the increase at day 15, the level was 84.8% of the normal population.
“Across four completed placebo-controlled NEST and LANDSCAPE clinical trials, patient reports of functional health and well-being as assessed by the SF-36v2 indicated substantial impairment at baseline compared to the population norm,” the researchers reported.
The improvements are especially important in light of the fact that in some patients with MDD, functional improvement is a top priority.
“Patients have often prioritized returning to their usual level of functioning over reduction in depressive symptoms, and functional recovery has been associated with better prognosis of depression,” the investigators wrote.
Zuranolone trials have shown that treatment-emergent adverse events (AEs) occur among about 60% of patients, versus about 44% with placebo. The most common AEs are somnolence, dizziness, headache, sedation, and diarrhea, with no increases in suicidal ideation or withdrawal.
The rates of severe AEs are low, and they are observed in about 3% of patients, versus 1.1% with placebo, the researchers noted.
Further, as opposed to serotonergic antidepressants such as SNRIs and SSRIs, zuranolone does not appear to have the undesirable side effects of decreased libido and sexual dysfunction, they added.
Clinically meaningful?
Andrew J. Cutler, MD, clinical associate professor of psychiatry at State University of New York, Syracuse, said the data are “very significant” for a number of reasons.
“We need more options to treat depression, especially ones with novel mechanisms of action and faster onset of efficacy, such as zuranolone,” said Dr. Cutler, who was not involved in the current study. He has coauthored other studies on zuranolone.
Regarding the study’s QoL outcomes, “while improvement in depressive symptoms is very important, what really matters to patients is improvement in function and quality of life,” Dr. Cutler noted.
Also commenting on the study, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences and professor of psychiatry, neuroscience, and pediatrics at Albert Einstein College of Medicine, New York, said the investigational drug could represent an important addition to the armamentarium for treating depression.
“Zuranolone has good oral bioavailability and would represent the first neuroactive steroid antidepressant available in oral form and, indeed, the first non–monoamine-based antidepressant available in oral form,” he said in an interview.
Dr. Alpert was not involved in the research and has no relationship with the drug’s development.
He noted that although there are modest differences between the patients who received zuranolone and those who received placebo in the trials, “this may have been related to high placebo response rates, which often complicate antidepressant trials.
“Further research is needed to determine whether differences between zuranolone and placebo are clinically meaningful, though the separation between drug and placebo on the primary endpoint, as well as some other measures, such as quality of life measures, is promising,” Dr. Alpert said.
However, he added that comparisons with other active antidepressants in terms of efficacy and tolerability remain to be seen.
“Given the large number of individuals with major depressive disorder who have incomplete response to or do not tolerate monoaminergic antidepressants, the development of agents that leverage novel nonmonoaminergic mechanisms is important,” Dr. Alpert concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Cutler has been involved in research of zuranolone for Sage Therapeutics. Dr. Alpert has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ADAA 2022
Brain implant is a potential life-changer for paralyzed patients
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
, results of a small, first-in-human study show.
A potential life changer for patients with amyotrophic lateral sclerosis (ALS), the minimally invasive device enables patients to carry out important activities of daily living.
“Our participants are able to use the device to perform tasks like sending email, texting loved ones and caregivers, browsing the web, and doing personal finances such as online banking,” study investigator Douglas J. Weber, PhD, professor of mechanical engineering and neuroscience, Carnegie Mellon University, Pittsburgh, told a press briefing.
The technology allowed one patient to write a book (due out later this year) and another patient to maintain communication despite losing his ability to speak, said the study’s lead investigator, Bruce Campbell, MBBS, PhD, professor of neurology, Royal Melbourne Hospital, University of Melbourne.
“In addition to providing patients with communicative capabilities not possible as a result of their disease, it is our goal to enable patients to be more independently involved in their care going forward, by enabling effective and faster communication directly with their caregiver and physician,” said Dr. Campbell.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Minimally invasive
ALS, also known as Lou Gehrig’s disease, is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. Patients with ALS eventually lose the ability to control muscle movement, often leading to total paralysis.
“Extending the period in which patients are able to communicate with loved ones and caregivers could provide a very meaningful benefit to patients with ALS,” said Dr. Weber.
Brain-computer interfaces measure and translate brain signals, with some functioning as motor neuro-prostheses. These devices provide direct communication between the brain and an external device by recording and decoding signals from the precentral gyrus as the result of movement intention.
“The technology has potential to empower the more than five million people in the U.S. who are severely paralyzed to once again perform important activities of daily living independently,” said Dr. Weber.
Until now, motor neuro-prostheses required surgery to remove a portion of the skull and place electrodes on to the brain. However, the new minimally invasive motor neuro-prostheses reach the brain by vascular access, dispensing with the need for a craniotomy.
“The brain-computer interface device used in our study is unique in that it does not require invasive open surgery to implant,” said Dr. Weber. “Instead this is an endovascular brain-computer interface.”
Using a catheter, surgeons feed the BCI through one of two jugular veins in the neck. They position an array of 16 sensors or electrodes on a stent-like scaffold that deploys against the walls of the superior sagittal sinus.
No adverse events
Describing the device, Dr. Weber said the electrodes or sensing elements are tiny and the body of the stent, which serves as a scaffold to support the electrodes, resembles a standard endovascular stent.
“It’s very small at the time of delivery because it’s held within the body of a catheter, but then when deployed it expands to contact the wall of the vein.”
The device transmits brain signals from the motor cortex to an electronics unit, located in a subcutaneous pocket that decodes movement signals. The machine-learning decoder is programmed as follows: When a trainer asked participants to attempt certain movements, like tapping their foot or extending their knee, the decoder analyzes nerve cell signals from those movement attempts. The decoder is able to translate movement signals into computer navigation.
The study included four patients with ALS who were paralyzed because of the disease and were trained to use the device.
A key safety endpoint was device-related serious adverse events resulting in death or increased disability during the post-implant evaluation period. Results showed all four participants successfully completed the 12-month follow-up with no serious adverse events.
Researchers also assessed target vessel patency and incidence of device migration at 3 and 12 months. Postoperative imaging showed that in all participants, the blood vessel that held the implanted device remained open and stayed in place.
Addressing the potential for blood clots, Dr. Weber said that so far there has been no sign of clotting or vascular occlusion.
“The device itself integrates well into the walls of the blood vessel over time,” he said. “Within the acute period after implantation, there’s time where the device is exposed to the blood stream, but once it becomes encapsulated and fully integrated into the blood vessel wall, the risks of thrombosis diminish.”
Greater independence
Researchers also recorded signal fidelity and stability over 12 months and use of the brain-computer interface to perform routine tasks. All participants learned to use the motor neuro-prostheses with eye tracking for computer use. Eye tracking technology helps a computer determine what a person is looking at.
Using the system, patients were able to complete tasks without help. These included text messaging and managing finances. “Since the device is fully implanted and easy for patients to use, they can use the technology independently and in their own home,” said Dr. Weber.
Although the study started with patients with ALS, those paralyzed from other causes, such as an upper spinal cord injury or brain-stem stroke could also benefit from this technology, Dr. Weber said. In addition, the technology could be expanded to broaden brain communication capabilities potentially to include robotic limbs, he said.
There’s even the potential to use this minimally invasive brain interface technology to deliver therapies like deep brain stimulation, which Dr. Weber noted is a growing field. “It’s [the] early days, but it’s a very exciting new direction for brain interface technology,” he said.
Researchers are now recruiting patients for the first U.S.-based feasibility trial of the device that will be funded by the NIH, said Dr. Weber. A limitation of the research was the study’s small size.
Advancing the field
Reached for a comment, Kevin C. Davis, an MD and PhD student in the department of biomedical engineering, University of Miami Miller School of Medicine, said this new work moves the field forward in an important way.
Dr. Davis and colleagues have shown the effectiveness of another technology used to overcome paralysis – a small portable system that facilitates hand grasp of a patient with a spinal cord injury. He reported on this DBS-based BCI system at the American Association of Neurological Surgeons (AANS) 2021 Annual Meeting.
Developing effective brain-computer interfaces, and motor neural prosthetics that avoid surgery, as the team did in this new study, is “worth exploring,” said Dr. Davis.
However, although the device used in this new study avoids cranial surgery, “sole vascular access may limit the device’s ability to reach other areas of the brain more suitable for upper-limb motor prosthetics,” he said.
“Determining how much function such a device could provide to individuals with locked-in syndrome or paralysis will be important in determining its viability as an eventual clinical tool for patients.”
The study was supported by Synchron, the maker of the device, the U.S. Defense Advanced Research Projects Agency, the Office of Naval Research, the National Health and Medical Research Council of Australia, the Australian Federal Government Foundation, and the Motor Neuron Disease Research Institute of Australia.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Antiseizure medication appears safe in pregnancy
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.

Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.
Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
SEATTLE – , according to new results from the Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study.
The study follows results from the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study, which found no evidence of cognitive harm in children who were exposed in utero to antiepileptic drugs. “[In the NEAD study] we followed our cohort to age 6 and found them to have actually an improvement in cognition by about 4 IQ points by the time they got to age 6,” Kimford J. Meador, MD, said during a presentation of the results of the MONEAD study at the 2022 annual meeting of the American Academy of Neurology.
Breastfeeding has health benefits for both mothers and children, including reduced risk of respiratory tract infections, atopic dermatitis, asthma, and diabetes in children, and reduced risk of diabetes, breast cancer, ovarian cancer, and postpartum depression in mothers. Despite those benefits, concerns about harms from exposure to antiepileptic drugs may prompt some women to avoid breastfeeding.
The results of NEAD and MONEAD should reassure patients, according to Dr. Meador, professor of neurology at Stanford (Calif.) University. “Given the known multiple benefits of breastfeeding … women with epilepsy should be encouraged to breastfeed,” he said.
A responsibility to ‘engage and educate’ patients
Jennifer Hopp, MD, who served as a discussant for the presentation, underscored the need for neurologists to address pregnancy with female patients of childbearing agents. “The issues may include fertility, peripartum management, and outcomes that really go through the lifespan to also include issues of menopause,” Dr. Hopp, associate professor of neurology at the University of Maryland, Baltimore, said during her presentation.
Dr. Hopp noted one study showing lower rates of breastfeeding among mothers with epilepsy. “Breastfeeding rates in women with epilepsy are strikingly lower than in women who do not have epilepsy,” said Dr. Hopp. Another study showed that women with epilepsy were less likely to sustain breastfeeding after 6 weeks.
Dr. Hopp implored neurologists to address this. “It’s our responsibility to engage and educate our patients. These data provide us messaging to our patients that the newer drugs do not adversely affect outcome independently of their other exposure, and really support well-informed choices in breastfeeding,” said Dr. Hopp.
Outdated attitudes still persist
Dr. Meador referred to the stigma that surrounds epilepsy, including some state laws that called for sterilization of women with epilepsy that lasted until the 1960s. One might think that such attitudes are gone, “but it’s still there,” said Dr. Meador, who recounted a story a colleague told him about a woman on antiseizure medication. In the hospital, the nurse told her not to breastfeed. The neurological consult told her not to breastfeed. She breastfed anyway. “Then they reported her for child neglect, and that was just a few years ago. So I think the message needs to be loud and clear that we encourage [women with epilepsy] to breastfeed because we have the known benefits, and now several studies showing clearly no adverse effects of breastfeeding while taking antiseizure medications,” said Dr. Meador.
MONEAD findings
The MONEAD study included women from 20 different sites, with 145 participating investigators. The researchers compared outcomes in 284 women with epilepsy and 87 healthy women. The maternal mean IQ was 98 among women with epilepsy (95% confidence interval [CI], 96-99), and 105 (95% CI, 102-107) among healthy women. Seventy-six percent of women with epilepsy breastfed, versus 89% of controls.
Among the study cohort, 79% of women with epilepsy were on monotherapy, and 21% were on polytherapy. Thirty-five percent received lamotrigine, 28% levetiracetam, 16% were on another monotherapy, 10% received a combination of lamotrigine and levetiracetam, and 11% received a different combination.
At age 3, there was no association between the verbal index score of the child and whether the mother had epilepsy or not (difference, 0.4; P = .770). The researchers did find associations with the mother’s IQ (0.3; P < .001), male versus female child sex (–4.9; P < .001), Hispanic or Latino ethnicity (vs. Non-Hispanic, –5.5; P < .001), mother without college degree (–7.0; P < .001), average Beck Anxiety Inventory score after birth (–0.4; P < .001), and weeks of gestational age at enrollment.
The researchers found no association between third trimester antiseizure medication blood levels and verbal index score after adjustment (–2.9; P = .149), with the exception of levetiracetam (–9.0; P = .033). “This is interesting (but) not to be overblown, because overall the children on levetiracetam did well. But it must be remembered that teratogens act in an exposure dependent manner, so we’re constantly in this balancing act of trying to make sure you get enough medication on board to stop the seizures and protect the mother and the child, and at the same time, not too much on board where we increase the risk of teratogenicity in the child,” said Dr. Meador.
The study was funded by the National Institutes of Health. Dr. Meador and Dr. Hopp have no relevant financial disclosures.
AT AAN 2022
Migraine linked to preeclampsia and other pregnancy complications
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Keto diet in MS tied to less disability, better quality of life
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022