User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Lung cancer in 2030: Expand genotyping
In recent years, –both of which have led to improved survival rates. But what will lung cancer look like in 2030?
Pasi A. Janne, MD, PhD, of the Dana-Farber Cancer Institute, Boston, hopes to see improved access to tumor and blood-based genotyping.
Dr. Janne, who serves as director of the Lowe Center for Thoracic Oncology at Dana-Farber, gave a keynote presentation at the 2022 European Lung Cancer Congress, where he highlighted the need to broaden the scope of targeted therapies, make “great drugs work even better,” improve the ability to treat patients based on risk level, and expand the use of targeted therapies in the adjuvant and neoadjuvant setting to make significant progress in the treatment lung cancer treatment in coming years.
Genotyping is underutilized, he said. A 2019 multicenter study reported at the annual meeting of the American Society of Clinical Oncology showed that only 54% of 1,203 patients underwent testing for EGFR mutations, 22% were tested for EGFR, ALK, ROS1, and BRAF mutations, and only 7% were tested for all biomarkers recommended by National Comprehensive Cancer Network guidelines at the time.
That study also showed that only 45% of patients received biomarker-driven treatment, even when driver mutations were detected.
“Immunotherapy was often prescribed instead of targeted therapy, even when molecular results were available,” Dr. Janne said.
Another study, reported at the 2021 ASCO annual meeting, showed some improvement in testing rates, but still, only 37% of patients were tested for all biomarkers as recommended.
Racial disparities in testing have also been observed. Bruno and colleagues found that any next-generation sequencing was performed in 50.1% of White patients, compared with 39.8% of black patients, and NGS prior to first-line therapy was performed in 35.5% and 25.8%, respectively.
The study, also reported at ASCO in 2021, showed that trial participation was observed among 3.9% of White patients and 1.9% of Black patients.
“The studies really highlight the need for increased testing rates and appropriate utilization of testing results to deliver optimal care to our patients with advanced lung cancer. We have a long way to go. To live the promise and appreciate the promise of precision therapy ... we need to be able to offer this testing to all of our patients with lung cancer,” he said.
Dr. Janne reported relationships with numerous pharmaceutical companies, including consulting, research support and stock ownership. He also receives postmarketing royalties from Dana-Farber Cancer Institute–owned intellectual property on EGFR mutations.
In recent years, –both of which have led to improved survival rates. But what will lung cancer look like in 2030?
Pasi A. Janne, MD, PhD, of the Dana-Farber Cancer Institute, Boston, hopes to see improved access to tumor and blood-based genotyping.
Dr. Janne, who serves as director of the Lowe Center for Thoracic Oncology at Dana-Farber, gave a keynote presentation at the 2022 European Lung Cancer Congress, where he highlighted the need to broaden the scope of targeted therapies, make “great drugs work even better,” improve the ability to treat patients based on risk level, and expand the use of targeted therapies in the adjuvant and neoadjuvant setting to make significant progress in the treatment lung cancer treatment in coming years.
Genotyping is underutilized, he said. A 2019 multicenter study reported at the annual meeting of the American Society of Clinical Oncology showed that only 54% of 1,203 patients underwent testing for EGFR mutations, 22% were tested for EGFR, ALK, ROS1, and BRAF mutations, and only 7% were tested for all biomarkers recommended by National Comprehensive Cancer Network guidelines at the time.
That study also showed that only 45% of patients received biomarker-driven treatment, even when driver mutations were detected.
“Immunotherapy was often prescribed instead of targeted therapy, even when molecular results were available,” Dr. Janne said.
Another study, reported at the 2021 ASCO annual meeting, showed some improvement in testing rates, but still, only 37% of patients were tested for all biomarkers as recommended.
Racial disparities in testing have also been observed. Bruno and colleagues found that any next-generation sequencing was performed in 50.1% of White patients, compared with 39.8% of black patients, and NGS prior to first-line therapy was performed in 35.5% and 25.8%, respectively.
The study, also reported at ASCO in 2021, showed that trial participation was observed among 3.9% of White patients and 1.9% of Black patients.
“The studies really highlight the need for increased testing rates and appropriate utilization of testing results to deliver optimal care to our patients with advanced lung cancer. We have a long way to go. To live the promise and appreciate the promise of precision therapy ... we need to be able to offer this testing to all of our patients with lung cancer,” he said.
Dr. Janne reported relationships with numerous pharmaceutical companies, including consulting, research support and stock ownership. He also receives postmarketing royalties from Dana-Farber Cancer Institute–owned intellectual property on EGFR mutations.
In recent years, –both of which have led to improved survival rates. But what will lung cancer look like in 2030?
Pasi A. Janne, MD, PhD, of the Dana-Farber Cancer Institute, Boston, hopes to see improved access to tumor and blood-based genotyping.
Dr. Janne, who serves as director of the Lowe Center for Thoracic Oncology at Dana-Farber, gave a keynote presentation at the 2022 European Lung Cancer Congress, where he highlighted the need to broaden the scope of targeted therapies, make “great drugs work even better,” improve the ability to treat patients based on risk level, and expand the use of targeted therapies in the adjuvant and neoadjuvant setting to make significant progress in the treatment lung cancer treatment in coming years.
Genotyping is underutilized, he said. A 2019 multicenter study reported at the annual meeting of the American Society of Clinical Oncology showed that only 54% of 1,203 patients underwent testing for EGFR mutations, 22% were tested for EGFR, ALK, ROS1, and BRAF mutations, and only 7% were tested for all biomarkers recommended by National Comprehensive Cancer Network guidelines at the time.
That study also showed that only 45% of patients received biomarker-driven treatment, even when driver mutations were detected.
“Immunotherapy was often prescribed instead of targeted therapy, even when molecular results were available,” Dr. Janne said.
Another study, reported at the 2021 ASCO annual meeting, showed some improvement in testing rates, but still, only 37% of patients were tested for all biomarkers as recommended.
Racial disparities in testing have also been observed. Bruno and colleagues found that any next-generation sequencing was performed in 50.1% of White patients, compared with 39.8% of black patients, and NGS prior to first-line therapy was performed in 35.5% and 25.8%, respectively.
The study, also reported at ASCO in 2021, showed that trial participation was observed among 3.9% of White patients and 1.9% of Black patients.
“The studies really highlight the need for increased testing rates and appropriate utilization of testing results to deliver optimal care to our patients with advanced lung cancer. We have a long way to go. To live the promise and appreciate the promise of precision therapy ... we need to be able to offer this testing to all of our patients with lung cancer,” he said.
Dr. Janne reported relationships with numerous pharmaceutical companies, including consulting, research support and stock ownership. He also receives postmarketing royalties from Dana-Farber Cancer Institute–owned intellectual property on EGFR mutations.
FROM ELCC 2022
Weighing the complexity of pathological response in lung cancer
studies, but much work remains to be done, said William D. Travis, MD, director of thoracic pathology at Memorial Sloan Kettering Cancer Center, New York.
In a keynote address at the 2022 European Lung Cancer Conference, Dr. Travis highlighted advances in the use of pathological response in this setting and outlined areas that need refinement. “Pathologic response after preoperative therapy is important because the extent of pathologic response strongly correlates with improved overall survival, and it is reflective of neoadjuvant therapy. The degree of response is associated with the degree of benefit in survival, and it’s being used as a surrogate for survival in phase 2 and 3 neoadjuvant clinical trials.”
In fact, multiple studies have demonstrated that non–small cell lung cancer patients with 10% or less viable residual tumor after treatment have improved overall survival and disease-free survival, compared with patients who have more residual tumor, he explained.
Recent studies have demonstrated the value of pathological response as an endpoint in the neoadjuvant therapy and molecular targeted therapy setting, he said, citing a study published in the Journal of Clinical Oncology that showed major pathological response rates of 14%-45% and pathological complete response rates up to 29% in patients treated with single-agent checkpoint inhibition.
In the CheckMate 816 trial, both major pathologic response and pathological complete response were significantly higher in patients treated with combination nivolumab and chemotherapy, compared with those treated with chemotherapy alone (37% vs. 8.9% and 24% vs. 2%, respectively).
“This high rate of responses with combined immunotherapy and chemotherapy is quite exciting,” he said.
Dr. Travis also stressed the importance of consulting the current International Association for the Study of Lung Cancer Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy.
He highlighted several key points regarding pathological response in lung cancer:
- Major pathological response (MPR) is calculated as the estimated size of viable tumor divided by the size of the tumor bed.
- Optimal cutoffs for determining MPR is currently 10%, but recent data suggest that in the conventional chemotherapy setting this may vary by tumor histology, with much higher cutoffs of about 65% for adenocarcinoma.
- Estimating the amount of viable tumor is “quite complicated and requires quite a number of steps,” and one the most important steps is “for the surgeon to the pathologist know that given specimen is from a patient who received neoadjuvant therapy.”
- Determining the border of the tumor bed can be challenging, therefore “resection specimens after neoadjuvant therapy should be sampled to optimize comprehensive gross and histologic assessment of the lung tumor bed for pathologic response ... as outlined in the guidelines.”
- The IASLC panel determined that having a single approach for estimating treatment effect would be best, despite the different therapy types and combinations used, but “it is recognized that there may be certain types of features that need to be addressed,” such as immune cell infiltrates in pats who received immunotherapy.
- The recommendations provide specific guidance for measuring tumor size for staging, including for special circumstances.
As for future direction, Dr. Travis said, “one question is how to assess treatment effect in lymph node samples.
“This is done for lymph nodes in breast cancer but not in lung cancer. We need system[s] for lung cancer.”
Good “infrastructure for pathology departments” is needed to support clinical trials, he said, noting that the team at Memorial Sloan Kettering Cancer Center includes physician assistants, tissue procurement staff, frozen section techs, research fellows, and research assistants.
Future work should also aim to standardize pathology assessment for clinical trials, improve the current recommendations, make use of new technology like artificial intelligence, optimize banking protocols and special techniques, and identify radiologic-pathological correlations, he said.
He added that “IASLC is promoting the design and implementation of an international database to collect uniformly clinical and pathologic information with the ultimate goal of fostering collaboration and to facilitate the identification of surrogate endpoints of long-term survival.”
Dr. Travis is a nonpaid pathology consultant for the LCMC3 and LCMC4 trials.
studies, but much work remains to be done, said William D. Travis, MD, director of thoracic pathology at Memorial Sloan Kettering Cancer Center, New York.
In a keynote address at the 2022 European Lung Cancer Conference, Dr. Travis highlighted advances in the use of pathological response in this setting and outlined areas that need refinement. “Pathologic response after preoperative therapy is important because the extent of pathologic response strongly correlates with improved overall survival, and it is reflective of neoadjuvant therapy. The degree of response is associated with the degree of benefit in survival, and it’s being used as a surrogate for survival in phase 2 and 3 neoadjuvant clinical trials.”
In fact, multiple studies have demonstrated that non–small cell lung cancer patients with 10% or less viable residual tumor after treatment have improved overall survival and disease-free survival, compared with patients who have more residual tumor, he explained.
Recent studies have demonstrated the value of pathological response as an endpoint in the neoadjuvant therapy and molecular targeted therapy setting, he said, citing a study published in the Journal of Clinical Oncology that showed major pathological response rates of 14%-45% and pathological complete response rates up to 29% in patients treated with single-agent checkpoint inhibition.
In the CheckMate 816 trial, both major pathologic response and pathological complete response were significantly higher in patients treated with combination nivolumab and chemotherapy, compared with those treated with chemotherapy alone (37% vs. 8.9% and 24% vs. 2%, respectively).
“This high rate of responses with combined immunotherapy and chemotherapy is quite exciting,” he said.
Dr. Travis also stressed the importance of consulting the current International Association for the Study of Lung Cancer Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy.
He highlighted several key points regarding pathological response in lung cancer:
- Major pathological response (MPR) is calculated as the estimated size of viable tumor divided by the size of the tumor bed.
- Optimal cutoffs for determining MPR is currently 10%, but recent data suggest that in the conventional chemotherapy setting this may vary by tumor histology, with much higher cutoffs of about 65% for adenocarcinoma.
- Estimating the amount of viable tumor is “quite complicated and requires quite a number of steps,” and one the most important steps is “for the surgeon to the pathologist know that given specimen is from a patient who received neoadjuvant therapy.”
- Determining the border of the tumor bed can be challenging, therefore “resection specimens after neoadjuvant therapy should be sampled to optimize comprehensive gross and histologic assessment of the lung tumor bed for pathologic response ... as outlined in the guidelines.”
- The IASLC panel determined that having a single approach for estimating treatment effect would be best, despite the different therapy types and combinations used, but “it is recognized that there may be certain types of features that need to be addressed,” such as immune cell infiltrates in pats who received immunotherapy.
- The recommendations provide specific guidance for measuring tumor size for staging, including for special circumstances.
As for future direction, Dr. Travis said, “one question is how to assess treatment effect in lymph node samples.
“This is done for lymph nodes in breast cancer but not in lung cancer. We need system[s] for lung cancer.”
Good “infrastructure for pathology departments” is needed to support clinical trials, he said, noting that the team at Memorial Sloan Kettering Cancer Center includes physician assistants, tissue procurement staff, frozen section techs, research fellows, and research assistants.
Future work should also aim to standardize pathology assessment for clinical trials, improve the current recommendations, make use of new technology like artificial intelligence, optimize banking protocols and special techniques, and identify radiologic-pathological correlations, he said.
He added that “IASLC is promoting the design and implementation of an international database to collect uniformly clinical and pathologic information with the ultimate goal of fostering collaboration and to facilitate the identification of surrogate endpoints of long-term survival.”
Dr. Travis is a nonpaid pathology consultant for the LCMC3 and LCMC4 trials.
studies, but much work remains to be done, said William D. Travis, MD, director of thoracic pathology at Memorial Sloan Kettering Cancer Center, New York.
In a keynote address at the 2022 European Lung Cancer Conference, Dr. Travis highlighted advances in the use of pathological response in this setting and outlined areas that need refinement. “Pathologic response after preoperative therapy is important because the extent of pathologic response strongly correlates with improved overall survival, and it is reflective of neoadjuvant therapy. The degree of response is associated with the degree of benefit in survival, and it’s being used as a surrogate for survival in phase 2 and 3 neoadjuvant clinical trials.”
In fact, multiple studies have demonstrated that non–small cell lung cancer patients with 10% or less viable residual tumor after treatment have improved overall survival and disease-free survival, compared with patients who have more residual tumor, he explained.
Recent studies have demonstrated the value of pathological response as an endpoint in the neoadjuvant therapy and molecular targeted therapy setting, he said, citing a study published in the Journal of Clinical Oncology that showed major pathological response rates of 14%-45% and pathological complete response rates up to 29% in patients treated with single-agent checkpoint inhibition.
In the CheckMate 816 trial, both major pathologic response and pathological complete response were significantly higher in patients treated with combination nivolumab and chemotherapy, compared with those treated with chemotherapy alone (37% vs. 8.9% and 24% vs. 2%, respectively).
“This high rate of responses with combined immunotherapy and chemotherapy is quite exciting,” he said.
Dr. Travis also stressed the importance of consulting the current International Association for the Study of Lung Cancer Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy.
He highlighted several key points regarding pathological response in lung cancer:
- Major pathological response (MPR) is calculated as the estimated size of viable tumor divided by the size of the tumor bed.
- Optimal cutoffs for determining MPR is currently 10%, but recent data suggest that in the conventional chemotherapy setting this may vary by tumor histology, with much higher cutoffs of about 65% for adenocarcinoma.
- Estimating the amount of viable tumor is “quite complicated and requires quite a number of steps,” and one the most important steps is “for the surgeon to the pathologist know that given specimen is from a patient who received neoadjuvant therapy.”
- Determining the border of the tumor bed can be challenging, therefore “resection specimens after neoadjuvant therapy should be sampled to optimize comprehensive gross and histologic assessment of the lung tumor bed for pathologic response ... as outlined in the guidelines.”
- The IASLC panel determined that having a single approach for estimating treatment effect would be best, despite the different therapy types and combinations used, but “it is recognized that there may be certain types of features that need to be addressed,” such as immune cell infiltrates in pats who received immunotherapy.
- The recommendations provide specific guidance for measuring tumor size for staging, including for special circumstances.
As for future direction, Dr. Travis said, “one question is how to assess treatment effect in lymph node samples.
“This is done for lymph nodes in breast cancer but not in lung cancer. We need system[s] for lung cancer.”
Good “infrastructure for pathology departments” is needed to support clinical trials, he said, noting that the team at Memorial Sloan Kettering Cancer Center includes physician assistants, tissue procurement staff, frozen section techs, research fellows, and research assistants.
Future work should also aim to standardize pathology assessment for clinical trials, improve the current recommendations, make use of new technology like artificial intelligence, optimize banking protocols and special techniques, and identify radiologic-pathological correlations, he said.
He added that “IASLC is promoting the design and implementation of an international database to collect uniformly clinical and pathologic information with the ultimate goal of fostering collaboration and to facilitate the identification of surrogate endpoints of long-term survival.”
Dr. Travis is a nonpaid pathology consultant for the LCMC3 and LCMC4 trials.
FROM ELCC 2022
Hospitalists and PCPs crave greater communication
Hospitalists and PCPs want more dialogue while patients are in the hospital in order to coordinate and personalize care, according to data collected at Beth Israel Deaconess Medical Center, Boston. The results were presented at the annual meeting of the Society of General Internal Medicine.
“I think a major takeaway is that both hospitalists and primary care doctors agree that it’s important for primary care doctors to be involved in a patient’s hospitalization. They both identified a value that PCPs can bring to the table,” coresearcher Kristen Flint, MD, a primary care resident, told this news organization.
A majority in both camps reported that communication with the other party occurred in less than 25% of cases, whereas ideally it would happen half of the time. Dr. Flint noted that communication tools differ among hospitals, limiting the applicability of the findings.
The research team surveyed 39 hospitalists and 28 PCPs employed by the medical center during the first half of 2021. They also interviewed six hospitalists as they admitted and discharged patients.
The hospitalist movement, which took hold in response to cost and efficiency demands of managed care, led to the start of inpatient specialists, thereby reducing the need for PCPs to commute between their offices and the hospital to care for patients in both settings.
Primary care involvement is important during hospitalization
In the Beth Israel Deaconess survey, four out of five hospitalists and three-quarters of PCPs agreed that primary care involvement is still important during hospitalization, most critically during discharge and admission. Hospitalists reported that PCPs provide valuable data about a patient’s medical status, social supports, mental health, and goals for care. They also said having such data helps to boost patient trust and improve the quality of inpatient care.
“Most projects around communication between inpatient and outpatient doctors have really focused on the time of discharge,” when clinicians identify what care a patient will need after they leave the hospital, Dr. Flint said. “But we found that both sides felt increased communication at time of admission would also be beneficial.”
The biggest barrier for PCPs, cited by 82% of respondents, was lack of time. Hospitalists’ top impediment was being unable to find contact information for the other party, which was cited by 79% of these survey participants.
Hospitalists operate ‘in a very stressful environment’
The Beth Israel Deaconess research “documents what has largely been suspected,” said primary care general internist Allan Goroll, MD.
Dr. Goroll, a professor of medicine at Harvard Medical School, Boston, said in an interview that hospitalists operate “in a very stressful environment.”
“They [hospitalists] appreciate accurate information about a patient’s recent medical history, test results, and responses to treatment as well as a briefing on patient values and preferences, family dynamics, and priorities for the admission. It makes for a safer, more personalized, and more efficient hospital admission,” said Dr. Goroll, who was not involved in the research.
In a 2015 article in the New England Journal of Medicine, Dr. Goroll and Daniel Hunt, MD, director of hospital medicine at Emory University, Atlanta, proposed a collaborative model in which PCPs visit hospitalized patients and serve as consultants to inpatient staff. Dr. Goroll said Massachusetts General Hospital in Boston, where he practices, initiated a study of that approach, but it was interrupted by the pandemic.
“As limited time is the most often cited barrier to communication, future interventions such as asynchronous forms of communication between the two groups should be considered,” the researchers wrote in the NEJM perspective.
To narrow the gap, Beth Israel Deaconess will study converting an admission notification letter sent to PCPs into a two-way communication tool in which PCPs can insert patient information, Dr. Flint said.
Dr. Flint and Dr. Goroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hospitalists and PCPs want more dialogue while patients are in the hospital in order to coordinate and personalize care, according to data collected at Beth Israel Deaconess Medical Center, Boston. The results were presented at the annual meeting of the Society of General Internal Medicine.
“I think a major takeaway is that both hospitalists and primary care doctors agree that it’s important for primary care doctors to be involved in a patient’s hospitalization. They both identified a value that PCPs can bring to the table,” coresearcher Kristen Flint, MD, a primary care resident, told this news organization.
A majority in both camps reported that communication with the other party occurred in less than 25% of cases, whereas ideally it would happen half of the time. Dr. Flint noted that communication tools differ among hospitals, limiting the applicability of the findings.
The research team surveyed 39 hospitalists and 28 PCPs employed by the medical center during the first half of 2021. They also interviewed six hospitalists as they admitted and discharged patients.
The hospitalist movement, which took hold in response to cost and efficiency demands of managed care, led to the start of inpatient specialists, thereby reducing the need for PCPs to commute between their offices and the hospital to care for patients in both settings.
Primary care involvement is important during hospitalization
In the Beth Israel Deaconess survey, four out of five hospitalists and three-quarters of PCPs agreed that primary care involvement is still important during hospitalization, most critically during discharge and admission. Hospitalists reported that PCPs provide valuable data about a patient’s medical status, social supports, mental health, and goals for care. They also said having such data helps to boost patient trust and improve the quality of inpatient care.
“Most projects around communication between inpatient and outpatient doctors have really focused on the time of discharge,” when clinicians identify what care a patient will need after they leave the hospital, Dr. Flint said. “But we found that both sides felt increased communication at time of admission would also be beneficial.”
The biggest barrier for PCPs, cited by 82% of respondents, was lack of time. Hospitalists’ top impediment was being unable to find contact information for the other party, which was cited by 79% of these survey participants.
Hospitalists operate ‘in a very stressful environment’
The Beth Israel Deaconess research “documents what has largely been suspected,” said primary care general internist Allan Goroll, MD.
Dr. Goroll, a professor of medicine at Harvard Medical School, Boston, said in an interview that hospitalists operate “in a very stressful environment.”
“They [hospitalists] appreciate accurate information about a patient’s recent medical history, test results, and responses to treatment as well as a briefing on patient values and preferences, family dynamics, and priorities for the admission. It makes for a safer, more personalized, and more efficient hospital admission,” said Dr. Goroll, who was not involved in the research.
In a 2015 article in the New England Journal of Medicine, Dr. Goroll and Daniel Hunt, MD, director of hospital medicine at Emory University, Atlanta, proposed a collaborative model in which PCPs visit hospitalized patients and serve as consultants to inpatient staff. Dr. Goroll said Massachusetts General Hospital in Boston, where he practices, initiated a study of that approach, but it was interrupted by the pandemic.
“As limited time is the most often cited barrier to communication, future interventions such as asynchronous forms of communication between the two groups should be considered,” the researchers wrote in the NEJM perspective.
To narrow the gap, Beth Israel Deaconess will study converting an admission notification letter sent to PCPs into a two-way communication tool in which PCPs can insert patient information, Dr. Flint said.
Dr. Flint and Dr. Goroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hospitalists and PCPs want more dialogue while patients are in the hospital in order to coordinate and personalize care, according to data collected at Beth Israel Deaconess Medical Center, Boston. The results were presented at the annual meeting of the Society of General Internal Medicine.
“I think a major takeaway is that both hospitalists and primary care doctors agree that it’s important for primary care doctors to be involved in a patient’s hospitalization. They both identified a value that PCPs can bring to the table,” coresearcher Kristen Flint, MD, a primary care resident, told this news organization.
A majority in both camps reported that communication with the other party occurred in less than 25% of cases, whereas ideally it would happen half of the time. Dr. Flint noted that communication tools differ among hospitals, limiting the applicability of the findings.
The research team surveyed 39 hospitalists and 28 PCPs employed by the medical center during the first half of 2021. They also interviewed six hospitalists as they admitted and discharged patients.
The hospitalist movement, which took hold in response to cost and efficiency demands of managed care, led to the start of inpatient specialists, thereby reducing the need for PCPs to commute between their offices and the hospital to care for patients in both settings.
Primary care involvement is important during hospitalization
In the Beth Israel Deaconess survey, four out of five hospitalists and three-quarters of PCPs agreed that primary care involvement is still important during hospitalization, most critically during discharge and admission. Hospitalists reported that PCPs provide valuable data about a patient’s medical status, social supports, mental health, and goals for care. They also said having such data helps to boost patient trust and improve the quality of inpatient care.
“Most projects around communication between inpatient and outpatient doctors have really focused on the time of discharge,” when clinicians identify what care a patient will need after they leave the hospital, Dr. Flint said. “But we found that both sides felt increased communication at time of admission would also be beneficial.”
The biggest barrier for PCPs, cited by 82% of respondents, was lack of time. Hospitalists’ top impediment was being unable to find contact information for the other party, which was cited by 79% of these survey participants.
Hospitalists operate ‘in a very stressful environment’
The Beth Israel Deaconess research “documents what has largely been suspected,” said primary care general internist Allan Goroll, MD.
Dr. Goroll, a professor of medicine at Harvard Medical School, Boston, said in an interview that hospitalists operate “in a very stressful environment.”
“They [hospitalists] appreciate accurate information about a patient’s recent medical history, test results, and responses to treatment as well as a briefing on patient values and preferences, family dynamics, and priorities for the admission. It makes for a safer, more personalized, and more efficient hospital admission,” said Dr. Goroll, who was not involved in the research.
In a 2015 article in the New England Journal of Medicine, Dr. Goroll and Daniel Hunt, MD, director of hospital medicine at Emory University, Atlanta, proposed a collaborative model in which PCPs visit hospitalized patients and serve as consultants to inpatient staff. Dr. Goroll said Massachusetts General Hospital in Boston, where he practices, initiated a study of that approach, but it was interrupted by the pandemic.
“As limited time is the most often cited barrier to communication, future interventions such as asynchronous forms of communication between the two groups should be considered,” the researchers wrote in the NEJM perspective.
To narrow the gap, Beth Israel Deaconess will study converting an admission notification letter sent to PCPs into a two-way communication tool in which PCPs can insert patient information, Dr. Flint said.
Dr. Flint and Dr. Goroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SGIM 2022
DIAMOND: Adding patiromer helps optimize HF meds, foils hyperkalemia
Several of the core medications for patients with heart failure with reduced ejection fraction (HFrEF) come with a well-known risk of causing hyperkalemia, to which many clinicians respond by pulling back on dosing or withdrawing the culprit drug.
But accompanying renin-angiotensin system–inhibiting agents with the potassium-sequestrant patiromer (Veltassa, Vifor Pharma) appears to shield patients against hyperkalemia enough that they can take more RASI medications at higher doses, suggests a randomized, a controlled study.

The DIAMOND trial’s HFrEF patients, who had current or a history of RASI-related hyperkalemia, added either patiromer or placebo to their guideline-directed medical therapy (GDMT), which includes, even emphasizes, the culprit medication. They include ACE inhibitors, angiotensin-receptor blockers (ARBs), angiotensin-receptor/neprilysin inhibitors (ARNIs), and mineralocorticoid receptor antagonists (MRAs).
Those taking patiromer tolerated more intense RASI therapy – including MRAs, which are especially prone to causing hyperkalemia – than the patients assigned to placebo. They also maintained lower potassium concentrations and experienced fewer clinically important hyperkalemia episodes, reported Javed Butler, MD, MPH, MBA, Baylor Scott and White Research Institute, Dallas, at the annual scientific sessions of the American College of Cardiology.
The apparent benefit from patiromer came in part from an advantage for a composite hyperkalemia-event endpoint that included mortality, Dr. Butler noted. That advantage seemed to hold regardless of age, sex, body mass index, HFrEF symptom severity, or initial natriuretic peptide levels.
Patients who took patiromer, compared with those who took placebo, showed a 37% reduction in risk for hyperkalemia (P = .006), defined as potassium levels exceeding 5.5 mEq/L, over a median follow-up of 27 weeks. They were 38% less likely to have their MRA dosage reduced to below target level (P = .006).
More patients in the patiromer group than in the control group attained at least 50% of target dosage for MRAs and ACE inhibitors, ARBs, or ARNIs (92% vs. 87%; P = .015).
Patients with HFrEF are unlikely to achieve best possible outcomes without GDMT optimization, but failure to optimize is often attributed to hyperkalemia concerns. DIAMOND, Dr. Butler said, suggests that, by adding the potassium sequestrant to GDMT, “you can simultaneously control potassium and optimize RASI therapy.” Many clinicians seem to believe they can achieve only one or the other.
DIAMOND was too underpowered to show whether preventing hyperkalemia with patiromer could improve clinical outcomes. But failure to optimize RASI medication in HFrEF can worsen risk for heart failure events and death. So “it stands to reason that optimization of RASI therapy without a concomitant risk of hyperkalemia may, in the long run, lead to better outcomes for these patients,” Dr. Butler said in an interview.
Given the drug’s ability to keep potassium levels in check during RASI therapy, Dr. Butler said, “hypokalemia should not be a reason for suboptimal therapy.”
Patiromer and other potassium sequestrants have been available in the United States and Europe for 4-6 years, but their value as adjuncts to RASI medication in HFrEF or other heart failure has been unclear.

“There’s a good opportunity to expand the use of the drug. The question is, in whom and when?” James L. Januzzi, MD, Massachusetts General Hospital, Boston, said in an interview.
Some HFrEF patients on GDMT “should be treated with patiromer. The bigger question is, should we give someone who has a history of hyperkalemia another chance at GDMT before we treat them with patiromer? Because they may not necessarily develop hyperkalemia a second time,” said Dr. Januzzi, who was on the DIAMOND endpoint-adjudication committee.
Among the most notable findings of the trial, he said, is that the number of people who developed hyperkalemia on RASI medication, although significantly elevated, “wasn’t as high as they expected it would be,” he said. “The data from DIAMOND argue that if a really significant majority does not become hyperkalemic on rechallenge, jumping straight to a potassium-binding drug may be premature.”
Physicians across specialties can differ in how they interpret potassium-level elevation and can use various cut points to flag when to stop RASI medication or at least hold back on up-titration, Dr. Butler observed. “Cardiologists have a different threshold of potassium that they tolerate than say, for instance, a nephrologist.”
Useful, then, might be a way to tell which patients are most likely to develop hyperkalemia with RASI up-titration and so might benefit from a potassium-binding agent right away. But DIAMOND, Dr. Butler said, “does not necessarily define any patient phenotype or any potassium level where we would say that you should use a potassium binder.”
The trial entered 1,642 patients with HFrEF and current or past RASI-related hyperkalemia to a 12-week run-in phase for optimization of GDMT with patiromer. The trial was conducted at nearly 400 centers in 21 countries.
RASI medication could be optimized in 85% of the cohort, from which 878 patients were randomly assigned either to continue optimized GDMT with patiromer or to have the potassium-sequestrant replaced with a placebo.
The patients on patiromer showed a 0.03-mEq/L mean rise in serum potassium levels from randomization to the end of the study, the primary endpoint, compared with a 0.13 mEq/L mean increase for those in the control group (P < .001), Dr. Butler reported.
The win ratio for a RASI-use score hierarchically featuring cardiovascular death and CV hospitalization for hyperkalemia at several levels of severity was 1.25 (95% confidence interval, 1.003-1.564; P = .048), favoring the patiromer group. The win ratio solely for hyperkalemia-related events also favored patients on patiromer, at 1.53 (95% CI, 1.23-1.91; P < .001).
Patiromer also seemed well tolerated, Dr. Butler said.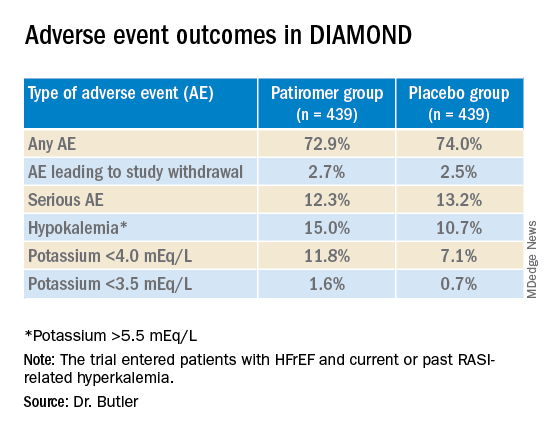
Hyperkalemia is “one of the most common excuses” from clinicians for failing to up-titrate RASI medicine in patients with heart failure, Dr. Januzzi said. DIAMOND was less about patiromer itself than about ways “to facilitate better GDMT, where we’re really falling short of the mark. During the run-in phase they were able to get the vast majority of individuals to target, which to me is a critically important point, and emblematic of the need for things that facilitate this kind of excellent care.”
DIAMOND was funded by Vifor Pharma. Dr. Butler disclosed receiving consulting fees from Abbott, Adrenomed, Amgen, Applied Therapeutics, Array, AstraZeneca, Bayer, Boehringer Ingelheim, CVRx, G3 Pharma, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, Novo Nordisk, Relypsa, Sequana Medical, and Vifor Pharma. Dr. Januzzi disclosed receiving consultant fees or honoraria from Abbott Laboratories, Imbria, Jana Care, Novartis, Prevencio, and Roche Diagnostics; serving on a data safety monitoring board for AbbVie, Amgen, Bayer Healthcare Pharmaceuticals, Beyer, CVRx, and Takeda Pharmaceuticals North America; and receiving research grants from Abbott Laboratories, Janssen, and Vifor Pharma.
A version of this article first appeared on Medscape.com.
Several of the core medications for patients with heart failure with reduced ejection fraction (HFrEF) come with a well-known risk of causing hyperkalemia, to which many clinicians respond by pulling back on dosing or withdrawing the culprit drug.
But accompanying renin-angiotensin system–inhibiting agents with the potassium-sequestrant patiromer (Veltassa, Vifor Pharma) appears to shield patients against hyperkalemia enough that they can take more RASI medications at higher doses, suggests a randomized, a controlled study.
The DIAMOND trial’s HFrEF patients, who had current or a history of RASI-related hyperkalemia, added either patiromer or placebo to their guideline-directed medical therapy (GDMT), which includes, even emphasizes, the culprit medication. They include ACE inhibitors, angiotensin-receptor blockers (ARBs), angiotensin-receptor/neprilysin inhibitors (ARNIs), and mineralocorticoid receptor antagonists (MRAs).
Those taking patiromer tolerated more intense RASI therapy – including MRAs, which are especially prone to causing hyperkalemia – than the patients assigned to placebo. They also maintained lower potassium concentrations and experienced fewer clinically important hyperkalemia episodes, reported Javed Butler, MD, MPH, MBA, Baylor Scott and White Research Institute, Dallas, at the annual scientific sessions of the American College of Cardiology.
The apparent benefit from patiromer came in part from an advantage for a composite hyperkalemia-event endpoint that included mortality, Dr. Butler noted. That advantage seemed to hold regardless of age, sex, body mass index, HFrEF symptom severity, or initial natriuretic peptide levels.
Patients who took patiromer, compared with those who took placebo, showed a 37% reduction in risk for hyperkalemia (P = .006), defined as potassium levels exceeding 5.5 mEq/L, over a median follow-up of 27 weeks. They were 38% less likely to have their MRA dosage reduced to below target level (P = .006).
More patients in the patiromer group than in the control group attained at least 50% of target dosage for MRAs and ACE inhibitors, ARBs, or ARNIs (92% vs. 87%; P = .015).
Patients with HFrEF are unlikely to achieve best possible outcomes without GDMT optimization, but failure to optimize is often attributed to hyperkalemia concerns. DIAMOND, Dr. Butler said, suggests that, by adding the potassium sequestrant to GDMT, “you can simultaneously control potassium and optimize RASI therapy.” Many clinicians seem to believe they can achieve only one or the other.
DIAMOND was too underpowered to show whether preventing hyperkalemia with patiromer could improve clinical outcomes. But failure to optimize RASI medication in HFrEF can worsen risk for heart failure events and death. So “it stands to reason that optimization of RASI therapy without a concomitant risk of hyperkalemia may, in the long run, lead to better outcomes for these patients,” Dr. Butler said in an interview.
Given the drug’s ability to keep potassium levels in check during RASI therapy, Dr. Butler said, “hypokalemia should not be a reason for suboptimal therapy.”
Patiromer and other potassium sequestrants have been available in the United States and Europe for 4-6 years, but their value as adjuncts to RASI medication in HFrEF or other heart failure has been unclear.
“There’s a good opportunity to expand the use of the drug. The question is, in whom and when?” James L. Januzzi, MD, Massachusetts General Hospital, Boston, said in an interview.
Some HFrEF patients on GDMT “should be treated with patiromer. The bigger question is, should we give someone who has a history of hyperkalemia another chance at GDMT before we treat them with patiromer? Because they may not necessarily develop hyperkalemia a second time,” said Dr. Januzzi, who was on the DIAMOND endpoint-adjudication committee.
Among the most notable findings of the trial, he said, is that the number of people who developed hyperkalemia on RASI medication, although significantly elevated, “wasn’t as high as they expected it would be,” he said. “The data from DIAMOND argue that if a really significant majority does not become hyperkalemic on rechallenge, jumping straight to a potassium-binding drug may be premature.”
Physicians across specialties can differ in how they interpret potassium-level elevation and can use various cut points to flag when to stop RASI medication or at least hold back on up-titration, Dr. Butler observed. “Cardiologists have a different threshold of potassium that they tolerate than say, for instance, a nephrologist.”
Useful, then, might be a way to tell which patients are most likely to develop hyperkalemia with RASI up-titration and so might benefit from a potassium-binding agent right away. But DIAMOND, Dr. Butler said, “does not necessarily define any patient phenotype or any potassium level where we would say that you should use a potassium binder.”
The trial entered 1,642 patients with HFrEF and current or past RASI-related hyperkalemia to a 12-week run-in phase for optimization of GDMT with patiromer. The trial was conducted at nearly 400 centers in 21 countries.
RASI medication could be optimized in 85% of the cohort, from which 878 patients were randomly assigned either to continue optimized GDMT with patiromer or to have the potassium-sequestrant replaced with a placebo.
The patients on patiromer showed a 0.03-mEq/L mean rise in serum potassium levels from randomization to the end of the study, the primary endpoint, compared with a 0.13 mEq/L mean increase for those in the control group (P < .001), Dr. Butler reported.
The win ratio for a RASI-use score hierarchically featuring cardiovascular death and CV hospitalization for hyperkalemia at several levels of severity was 1.25 (95% confidence interval, 1.003-1.564; P = .048), favoring the patiromer group. The win ratio solely for hyperkalemia-related events also favored patients on patiromer, at 1.53 (95% CI, 1.23-1.91; P < .001).
Patiromer also seemed well tolerated, Dr. Butler said.
Hyperkalemia is “one of the most common excuses” from clinicians for failing to up-titrate RASI medicine in patients with heart failure, Dr. Januzzi said. DIAMOND was less about patiromer itself than about ways “to facilitate better GDMT, where we’re really falling short of the mark. During the run-in phase they were able to get the vast majority of individuals to target, which to me is a critically important point, and emblematic of the need for things that facilitate this kind of excellent care.”
DIAMOND was funded by Vifor Pharma. Dr. Butler disclosed receiving consulting fees from Abbott, Adrenomed, Amgen, Applied Therapeutics, Array, AstraZeneca, Bayer, Boehringer Ingelheim, CVRx, G3 Pharma, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, Novo Nordisk, Relypsa, Sequana Medical, and Vifor Pharma. Dr. Januzzi disclosed receiving consultant fees or honoraria from Abbott Laboratories, Imbria, Jana Care, Novartis, Prevencio, and Roche Diagnostics; serving on a data safety monitoring board for AbbVie, Amgen, Bayer Healthcare Pharmaceuticals, Beyer, CVRx, and Takeda Pharmaceuticals North America; and receiving research grants from Abbott Laboratories, Janssen, and Vifor Pharma.
A version of this article first appeared on Medscape.com.
Several of the core medications for patients with heart failure with reduced ejection fraction (HFrEF) come with a well-known risk of causing hyperkalemia, to which many clinicians respond by pulling back on dosing or withdrawing the culprit drug.
But accompanying renin-angiotensin system–inhibiting agents with the potassium-sequestrant patiromer (Veltassa, Vifor Pharma) appears to shield patients against hyperkalemia enough that they can take more RASI medications at higher doses, suggests a randomized, a controlled study.
The DIAMOND trial’s HFrEF patients, who had current or a history of RASI-related hyperkalemia, added either patiromer or placebo to their guideline-directed medical therapy (GDMT), which includes, even emphasizes, the culprit medication. They include ACE inhibitors, angiotensin-receptor blockers (ARBs), angiotensin-receptor/neprilysin inhibitors (ARNIs), and mineralocorticoid receptor antagonists (MRAs).
Those taking patiromer tolerated more intense RASI therapy – including MRAs, which are especially prone to causing hyperkalemia – than the patients assigned to placebo. They also maintained lower potassium concentrations and experienced fewer clinically important hyperkalemia episodes, reported Javed Butler, MD, MPH, MBA, Baylor Scott and White Research Institute, Dallas, at the annual scientific sessions of the American College of Cardiology.
The apparent benefit from patiromer came in part from an advantage for a composite hyperkalemia-event endpoint that included mortality, Dr. Butler noted. That advantage seemed to hold regardless of age, sex, body mass index, HFrEF symptom severity, or initial natriuretic peptide levels.
Patients who took patiromer, compared with those who took placebo, showed a 37% reduction in risk for hyperkalemia (P = .006), defined as potassium levels exceeding 5.5 mEq/L, over a median follow-up of 27 weeks. They were 38% less likely to have their MRA dosage reduced to below target level (P = .006).
More patients in the patiromer group than in the control group attained at least 50% of target dosage for MRAs and ACE inhibitors, ARBs, or ARNIs (92% vs. 87%; P = .015).
Patients with HFrEF are unlikely to achieve best possible outcomes without GDMT optimization, but failure to optimize is often attributed to hyperkalemia concerns. DIAMOND, Dr. Butler said, suggests that, by adding the potassium sequestrant to GDMT, “you can simultaneously control potassium and optimize RASI therapy.” Many clinicians seem to believe they can achieve only one or the other.
DIAMOND was too underpowered to show whether preventing hyperkalemia with patiromer could improve clinical outcomes. But failure to optimize RASI medication in HFrEF can worsen risk for heart failure events and death. So “it stands to reason that optimization of RASI therapy without a concomitant risk of hyperkalemia may, in the long run, lead to better outcomes for these patients,” Dr. Butler said in an interview.
Given the drug’s ability to keep potassium levels in check during RASI therapy, Dr. Butler said, “hypokalemia should not be a reason for suboptimal therapy.”
Patiromer and other potassium sequestrants have been available in the United States and Europe for 4-6 years, but their value as adjuncts to RASI medication in HFrEF or other heart failure has been unclear.
“There’s a good opportunity to expand the use of the drug. The question is, in whom and when?” James L. Januzzi, MD, Massachusetts General Hospital, Boston, said in an interview.
Some HFrEF patients on GDMT “should be treated with patiromer. The bigger question is, should we give someone who has a history of hyperkalemia another chance at GDMT before we treat them with patiromer? Because they may not necessarily develop hyperkalemia a second time,” said Dr. Januzzi, who was on the DIAMOND endpoint-adjudication committee.
Among the most notable findings of the trial, he said, is that the number of people who developed hyperkalemia on RASI medication, although significantly elevated, “wasn’t as high as they expected it would be,” he said. “The data from DIAMOND argue that if a really significant majority does not become hyperkalemic on rechallenge, jumping straight to a potassium-binding drug may be premature.”
Physicians across specialties can differ in how they interpret potassium-level elevation and can use various cut points to flag when to stop RASI medication or at least hold back on up-titration, Dr. Butler observed. “Cardiologists have a different threshold of potassium that they tolerate than say, for instance, a nephrologist.”
Useful, then, might be a way to tell which patients are most likely to develop hyperkalemia with RASI up-titration and so might benefit from a potassium-binding agent right away. But DIAMOND, Dr. Butler said, “does not necessarily define any patient phenotype or any potassium level where we would say that you should use a potassium binder.”
The trial entered 1,642 patients with HFrEF and current or past RASI-related hyperkalemia to a 12-week run-in phase for optimization of GDMT with patiromer. The trial was conducted at nearly 400 centers in 21 countries.
RASI medication could be optimized in 85% of the cohort, from which 878 patients were randomly assigned either to continue optimized GDMT with patiromer or to have the potassium-sequestrant replaced with a placebo.
The patients on patiromer showed a 0.03-mEq/L mean rise in serum potassium levels from randomization to the end of the study, the primary endpoint, compared with a 0.13 mEq/L mean increase for those in the control group (P < .001), Dr. Butler reported.
The win ratio for a RASI-use score hierarchically featuring cardiovascular death and CV hospitalization for hyperkalemia at several levels of severity was 1.25 (95% confidence interval, 1.003-1.564; P = .048), favoring the patiromer group. The win ratio solely for hyperkalemia-related events also favored patients on patiromer, at 1.53 (95% CI, 1.23-1.91; P < .001).
Patiromer also seemed well tolerated, Dr. Butler said.
Hyperkalemia is “one of the most common excuses” from clinicians for failing to up-titrate RASI medicine in patients with heart failure, Dr. Januzzi said. DIAMOND was less about patiromer itself than about ways “to facilitate better GDMT, where we’re really falling short of the mark. During the run-in phase they were able to get the vast majority of individuals to target, which to me is a critically important point, and emblematic of the need for things that facilitate this kind of excellent care.”
DIAMOND was funded by Vifor Pharma. Dr. Butler disclosed receiving consulting fees from Abbott, Adrenomed, Amgen, Applied Therapeutics, Array, AstraZeneca, Bayer, Boehringer Ingelheim, CVRx, G3 Pharma, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, Novo Nordisk, Relypsa, Sequana Medical, and Vifor Pharma. Dr. Januzzi disclosed receiving consultant fees or honoraria from Abbott Laboratories, Imbria, Jana Care, Novartis, Prevencio, and Roche Diagnostics; serving on a data safety monitoring board for AbbVie, Amgen, Bayer Healthcare Pharmaceuticals, Beyer, CVRx, and Takeda Pharmaceuticals North America; and receiving research grants from Abbott Laboratories, Janssen, and Vifor Pharma.
A version of this article first appeared on Medscape.com.
FROM ACC 2022
Apremilast has neutral effect on vascular inflammation in psoriasis study
BOSTON – Treatment with , and glucose metabolism, in a study presented at the 2022 American Academy of Dermatology annual meeting.
In the phase 4, open-label, single arm trial, participants also lost subcutaneous and visceral fat after 16 weeks on the oral medication, a phosphodiesterase 4 (PDE4) inhibitor, and maintained that loss at 52 weeks.
People with psoriasis have an increased risk of obesity, type 2 diabetes, and cardiovascular events. Patients with more significant psoriasis “tend to die about 5 years younger than they should, based on their risk factors for mortality,” Joel Gelfand, MD, MSCE, professor of dermatology and epidemiology and vice chair of clinical research in dermatology at the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
He led the research and presented the findings at the AAD meeting March 26. “As a result, there has been a keen interest in understanding how psoriasis therapies impact cardiovascular risk, the idea being that by controlling inflammation, you may lower the risk of these patients developing cardiovascular disease over time,” he said.
Previous trials looking at the effect of psoriasis therapies on vascular inflammation “have been, for the most part, inconclusive,” Michael Garshick, MD, a cardiologist at NYU Langone Health, told this news organization. Dr. Garshick was not involved with the research. A 2021 systematic review of psoriasis clinicals trials reported that the tumor necrosis factor (TNF) blocker adalimumab (Humira) and phototherapy had the greatest effect on cardiometabolic markers, while ustekinumab (Stelara), an interleukin (IL)-12 and IL-23 antagonist, was the only treatment that improved vascular inflammation. These variable findings make this area “ripe for study,” noted Dr. Garshick.
To observe how apremilast, which is approved by the FDA for treating psoriasis and psoriatic arthritis, affected vascular inflammation, adiposity, and blood-based cardiometabolic markers, Dr. Gelfand organized an open-label study in adults with moderate-to-severe psoriasis. All participants were 18 years or older, had psoriasis for at least 6 months, and were candidates for systemic therapy. All patients underwent FDG PET/CT scans to assess aortic vascular inflammation and had blood work at baseline. Of the 70 patients originally enrolled in the study, 60 remained in the study at week 16, including 57 who underwent imaging for the second time. Thirty-nine participants remained in the study until week 52, and all except one had another scan.
The average age of participants was 47 years, and their mean BMI was 30. More than 80% of participants were White (83%) and 77% were male. The study population had lived with psoriasis for an average of 16 years and 8 patients also had psoriatic arthritis. At baseline, on average, participants had a Psoriasis Area and Severity Index (PASI) score of 18.62, a dermatology life quality index (DLQI) score of 11.60, and 22% of participants’ BSA (body surface area) were affected. The mean TBRmax, the marker for vascular inflammation, was 1.61.
Treatment responses were as expected for apremilast, with 35% of patients achieving PASI 75 and 65% of participants reporting DLQI scores of 5 or less by 16 weeks. At 52 weeks, 31% of the cohort had achieved PASI 75, and 67% reported DLQI score of 5 or higher. All psoriasis endpoints had improved since baseline (P = .001).
Throughout the study period, there was no significant change in TBRmax. However, in a sensitivity analysis, the 16 patients with a baseline TBRmax of 1.6 or higher had an absolute reduction of 0.21 in TBR by week 52. “That suggests that maybe a subset of people who have higher levels of aortic inflammation at baseline may experience some reduction that portend, potentially, some health benefits over time,” Dr. Gelfand said. “Ultimately, I wouldn’t hang my hat on the finding,” he said, noting that additional research comparing the treatment to placebo is necessary.
Both visceral and subcutaneous adipose tissue (VAT and SAT) decreased by week 16, and this reduction was maintained through week 52. In the first 16 weeks of the study, VAT decreased by 5.32% (P = .0009), and SAT decreased by 5.53% (P = .0005). From baseline to 52 weeks, VAT decreased by 5.52% (P = .0148), and SAT decreased by 5.50% (P = .0096). There were no significant differences between week 16 and week 52 in VAT or SAT.
Of the 68 blood biomarkers analyzed, there were significant decreases in the inflammatory markers ferritin (P = .015) and IL-beta (P = .006), the lipid metabolism biomarker HDL-cholesterol efflux (P = .008), and ketone bodies (P = .006). There were also increases in the inflammatory marker IL-8 (P = .003), the lipid metabolism marker ApoA (P = .05), and insulin (P = .05). Ferritin was the only biomarker that was reduced on both week 16 and week 52.
“If you want to be a purist, this was a negative trial,” said Dr. Garshick, because apremilast was not found to decrease vascular inflammation; however, he noted that the biomarker changes “were hopeful secondary endpoints.” It could be, he said, that another outcome measure may be better able to show changes in vascular inflammation compared with FDG. “It’s always hard to figure out what a good surrogate endpoint is in cardiovascular trials,” he noted, “so it may be that FDG/PET is too noisy or not reliable enough to see the outcome that we want to see.”
Dr. Gelfand reports consulting fees/grants from Amgen, AbbVie, BMS, Boehringer Ingelheim, Janssen Biologics, Novartis Corp, Pfizer, and UCB (DSMB). He serves as the Deputy Editor for the Journal of Investigative Dermatology and the Chief Medical Editor at Healio Psoriatic Disease and receives honoraria for both roles. Dr. Garshick has received consulting fees from AbbVie.
A version of this article first appeared on Medscape.com.
BOSTON – Treatment with , and glucose metabolism, in a study presented at the 2022 American Academy of Dermatology annual meeting.
In the phase 4, open-label, single arm trial, participants also lost subcutaneous and visceral fat after 16 weeks on the oral medication, a phosphodiesterase 4 (PDE4) inhibitor, and maintained that loss at 52 weeks.
People with psoriasis have an increased risk of obesity, type 2 diabetes, and cardiovascular events. Patients with more significant psoriasis “tend to die about 5 years younger than they should, based on their risk factors for mortality,” Joel Gelfand, MD, MSCE, professor of dermatology and epidemiology and vice chair of clinical research in dermatology at the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
He led the research and presented the findings at the AAD meeting March 26. “As a result, there has been a keen interest in understanding how psoriasis therapies impact cardiovascular risk, the idea being that by controlling inflammation, you may lower the risk of these patients developing cardiovascular disease over time,” he said.
Previous trials looking at the effect of psoriasis therapies on vascular inflammation “have been, for the most part, inconclusive,” Michael Garshick, MD, a cardiologist at NYU Langone Health, told this news organization. Dr. Garshick was not involved with the research. A 2021 systematic review of psoriasis clinicals trials reported that the tumor necrosis factor (TNF) blocker adalimumab (Humira) and phototherapy had the greatest effect on cardiometabolic markers, while ustekinumab (Stelara), an interleukin (IL)-12 and IL-23 antagonist, was the only treatment that improved vascular inflammation. These variable findings make this area “ripe for study,” noted Dr. Garshick.
To observe how apremilast, which is approved by the FDA for treating psoriasis and psoriatic arthritis, affected vascular inflammation, adiposity, and blood-based cardiometabolic markers, Dr. Gelfand organized an open-label study in adults with moderate-to-severe psoriasis. All participants were 18 years or older, had psoriasis for at least 6 months, and were candidates for systemic therapy. All patients underwent FDG PET/CT scans to assess aortic vascular inflammation and had blood work at baseline. Of the 70 patients originally enrolled in the study, 60 remained in the study at week 16, including 57 who underwent imaging for the second time. Thirty-nine participants remained in the study until week 52, and all except one had another scan.
The average age of participants was 47 years, and their mean BMI was 30. More than 80% of participants were White (83%) and 77% were male. The study population had lived with psoriasis for an average of 16 years and 8 patients also had psoriatic arthritis. At baseline, on average, participants had a Psoriasis Area and Severity Index (PASI) score of 18.62, a dermatology life quality index (DLQI) score of 11.60, and 22% of participants’ BSA (body surface area) were affected. The mean TBRmax, the marker for vascular inflammation, was 1.61.
Treatment responses were as expected for apremilast, with 35% of patients achieving PASI 75 and 65% of participants reporting DLQI scores of 5 or less by 16 weeks. At 52 weeks, 31% of the cohort had achieved PASI 75, and 67% reported DLQI score of 5 or higher. All psoriasis endpoints had improved since baseline (P = .001).
Throughout the study period, there was no significant change in TBRmax. However, in a sensitivity analysis, the 16 patients with a baseline TBRmax of 1.6 or higher had an absolute reduction of 0.21 in TBR by week 52. “That suggests that maybe a subset of people who have higher levels of aortic inflammation at baseline may experience some reduction that portend, potentially, some health benefits over time,” Dr. Gelfand said. “Ultimately, I wouldn’t hang my hat on the finding,” he said, noting that additional research comparing the treatment to placebo is necessary.
Both visceral and subcutaneous adipose tissue (VAT and SAT) decreased by week 16, and this reduction was maintained through week 52. In the first 16 weeks of the study, VAT decreased by 5.32% (P = .0009), and SAT decreased by 5.53% (P = .0005). From baseline to 52 weeks, VAT decreased by 5.52% (P = .0148), and SAT decreased by 5.50% (P = .0096). There were no significant differences between week 16 and week 52 in VAT or SAT.
Of the 68 blood biomarkers analyzed, there were significant decreases in the inflammatory markers ferritin (P = .015) and IL-beta (P = .006), the lipid metabolism biomarker HDL-cholesterol efflux (P = .008), and ketone bodies (P = .006). There were also increases in the inflammatory marker IL-8 (P = .003), the lipid metabolism marker ApoA (P = .05), and insulin (P = .05). Ferritin was the only biomarker that was reduced on both week 16 and week 52.
“If you want to be a purist, this was a negative trial,” said Dr. Garshick, because apremilast was not found to decrease vascular inflammation; however, he noted that the biomarker changes “were hopeful secondary endpoints.” It could be, he said, that another outcome measure may be better able to show changes in vascular inflammation compared with FDG. “It’s always hard to figure out what a good surrogate endpoint is in cardiovascular trials,” he noted, “so it may be that FDG/PET is too noisy or not reliable enough to see the outcome that we want to see.”
Dr. Gelfand reports consulting fees/grants from Amgen, AbbVie, BMS, Boehringer Ingelheim, Janssen Biologics, Novartis Corp, Pfizer, and UCB (DSMB). He serves as the Deputy Editor for the Journal of Investigative Dermatology and the Chief Medical Editor at Healio Psoriatic Disease and receives honoraria for both roles. Dr. Garshick has received consulting fees from AbbVie.
A version of this article first appeared on Medscape.com.
BOSTON – Treatment with , and glucose metabolism, in a study presented at the 2022 American Academy of Dermatology annual meeting.
In the phase 4, open-label, single arm trial, participants also lost subcutaneous and visceral fat after 16 weeks on the oral medication, a phosphodiesterase 4 (PDE4) inhibitor, and maintained that loss at 52 weeks.
People with psoriasis have an increased risk of obesity, type 2 diabetes, and cardiovascular events. Patients with more significant psoriasis “tend to die about 5 years younger than they should, based on their risk factors for mortality,” Joel Gelfand, MD, MSCE, professor of dermatology and epidemiology and vice chair of clinical research in dermatology at the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
He led the research and presented the findings at the AAD meeting March 26. “As a result, there has been a keen interest in understanding how psoriasis therapies impact cardiovascular risk, the idea being that by controlling inflammation, you may lower the risk of these patients developing cardiovascular disease over time,” he said.
Previous trials looking at the effect of psoriasis therapies on vascular inflammation “have been, for the most part, inconclusive,” Michael Garshick, MD, a cardiologist at NYU Langone Health, told this news organization. Dr. Garshick was not involved with the research. A 2021 systematic review of psoriasis clinicals trials reported that the tumor necrosis factor (TNF) blocker adalimumab (Humira) and phototherapy had the greatest effect on cardiometabolic markers, while ustekinumab (Stelara), an interleukin (IL)-12 and IL-23 antagonist, was the only treatment that improved vascular inflammation. These variable findings make this area “ripe for study,” noted Dr. Garshick.
To observe how apremilast, which is approved by the FDA for treating psoriasis and psoriatic arthritis, affected vascular inflammation, adiposity, and blood-based cardiometabolic markers, Dr. Gelfand organized an open-label study in adults with moderate-to-severe psoriasis. All participants were 18 years or older, had psoriasis for at least 6 months, and were candidates for systemic therapy. All patients underwent FDG PET/CT scans to assess aortic vascular inflammation and had blood work at baseline. Of the 70 patients originally enrolled in the study, 60 remained in the study at week 16, including 57 who underwent imaging for the second time. Thirty-nine participants remained in the study until week 52, and all except one had another scan.
The average age of participants was 47 years, and their mean BMI was 30. More than 80% of participants were White (83%) and 77% were male. The study population had lived with psoriasis for an average of 16 years and 8 patients also had psoriatic arthritis. At baseline, on average, participants had a Psoriasis Area and Severity Index (PASI) score of 18.62, a dermatology life quality index (DLQI) score of 11.60, and 22% of participants’ BSA (body surface area) were affected. The mean TBRmax, the marker for vascular inflammation, was 1.61.
Treatment responses were as expected for apremilast, with 35% of patients achieving PASI 75 and 65% of participants reporting DLQI scores of 5 or less by 16 weeks. At 52 weeks, 31% of the cohort had achieved PASI 75, and 67% reported DLQI score of 5 or higher. All psoriasis endpoints had improved since baseline (P = .001).
Throughout the study period, there was no significant change in TBRmax. However, in a sensitivity analysis, the 16 patients with a baseline TBRmax of 1.6 or higher had an absolute reduction of 0.21 in TBR by week 52. “That suggests that maybe a subset of people who have higher levels of aortic inflammation at baseline may experience some reduction that portend, potentially, some health benefits over time,” Dr. Gelfand said. “Ultimately, I wouldn’t hang my hat on the finding,” he said, noting that additional research comparing the treatment to placebo is necessary.
Both visceral and subcutaneous adipose tissue (VAT and SAT) decreased by week 16, and this reduction was maintained through week 52. In the first 16 weeks of the study, VAT decreased by 5.32% (P = .0009), and SAT decreased by 5.53% (P = .0005). From baseline to 52 weeks, VAT decreased by 5.52% (P = .0148), and SAT decreased by 5.50% (P = .0096). There were no significant differences between week 16 and week 52 in VAT or SAT.
Of the 68 blood biomarkers analyzed, there were significant decreases in the inflammatory markers ferritin (P = .015) and IL-beta (P = .006), the lipid metabolism biomarker HDL-cholesterol efflux (P = .008), and ketone bodies (P = .006). There were also increases in the inflammatory marker IL-8 (P = .003), the lipid metabolism marker ApoA (P = .05), and insulin (P = .05). Ferritin was the only biomarker that was reduced on both week 16 and week 52.
“If you want to be a purist, this was a negative trial,” said Dr. Garshick, because apremilast was not found to decrease vascular inflammation; however, he noted that the biomarker changes “were hopeful secondary endpoints.” It could be, he said, that another outcome measure may be better able to show changes in vascular inflammation compared with FDG. “It’s always hard to figure out what a good surrogate endpoint is in cardiovascular trials,” he noted, “so it may be that FDG/PET is too noisy or not reliable enough to see the outcome that we want to see.”
Dr. Gelfand reports consulting fees/grants from Amgen, AbbVie, BMS, Boehringer Ingelheim, Janssen Biologics, Novartis Corp, Pfizer, and UCB (DSMB). He serves as the Deputy Editor for the Journal of Investigative Dermatology and the Chief Medical Editor at Healio Psoriatic Disease and receives honoraria for both roles. Dr. Garshick has received consulting fees from AbbVie.
A version of this article first appeared on Medscape.com.
AT AAD 2022
Study suggests keto diet increases tumor growth in ovarian cancer
A ketogenic diet fed to mice with epithelial ovarian cancer led to significantly increased tumor growth and gut microbiome alterations, according to study recently presented at the annual meeting of the Society of Gynecologic Oncology.
“The keto diet is very popular, especially among patients who believe it may treat cancer by starving tumors of the fuel they need to grow, altering the immune system, and other anticancer effects,” said study leader Mariam AlHilli, MD, of the Cleveland Clinic.
The findings are surprising because in other studies the high-fat, zero-carb ketogenic diet has demonstrated tumor-suppressing effects. It has been under study as a possible adjuvant therapy for other cancers, such as glioblastoma, colon cancer, prostate cancer, and pancreatic cancer.
“While we don’t know yet whether these findings extend to patients, the results in animals indicate that instead of being protective, the keto diet appears to promote ovarian cancer growth and progression,” Dr. AlHilli said. In the present study, tumor bearing mice were fed a keto diet consisting of 10% protein, 0% carbohydrates, and 90% fat, while the high-fat diet was 10% protein, 15% carbohydrates, and 75% fat. The control diet consisted of 10% protein, 77% carbohydrates, and 13% fat. Epithelial ovarian cancer tumor growth was monitored weekly.
Over the 6- to 10-week course of study, a 9.1-fold increase from baseline in tumor growth was observed in the keto diet-fed mice (n = 20). Among mice fed a high-fat diet (n = 20) that included some carbohydrates, tumor growth increased 2.0-fold from baseline, and among control group mice (n = 20) fed a low-fat, high carbohydrate diet, tumor growth increased 3.1-fold.
The investigators observed several hallmarks of tumor progression: tumor associated macrophages were enriched significantly, activated lymphoid cells (natural killer cells) were significantly reduced (P < .001), and M2:M1 polarization trended higher. Also, in keto diet–fed mice, gene set enrichment analysis revealed that epithelial ovarian cancer tumors had increased angiogenesis and inflammatory responses, enhanced epithelial-to-mesenchymal transition phenotype, and altered lipid metabolism. Compared with high-fat diet–fed mice, the keto-fed mice had increases in lipid catalytic activity and catabolism, as well as decreases in lipid synthesis.
“The tumor increase could be mediated by the gut microbiome or by gene alterations or by metabolite levels that influence tumor growth. It’s possible that each cancer type is different. The composition of the diet may be a factor, as well as how tumors metabolize fat and ketones,” Dr. AlHilli said.
The results need to be confirmed in preclinical animal studies and in additional models, she added.
The study was funded by a K12 Grant and internal funding from Cleveland Clinic. Dr. AlHilli declared no relevant disclosures.
A ketogenic diet fed to mice with epithelial ovarian cancer led to significantly increased tumor growth and gut microbiome alterations, according to study recently presented at the annual meeting of the Society of Gynecologic Oncology.
“The keto diet is very popular, especially among patients who believe it may treat cancer by starving tumors of the fuel they need to grow, altering the immune system, and other anticancer effects,” said study leader Mariam AlHilli, MD, of the Cleveland Clinic.
The findings are surprising because in other studies the high-fat, zero-carb ketogenic diet has demonstrated tumor-suppressing effects. It has been under study as a possible adjuvant therapy for other cancers, such as glioblastoma, colon cancer, prostate cancer, and pancreatic cancer.
“While we don’t know yet whether these findings extend to patients, the results in animals indicate that instead of being protective, the keto diet appears to promote ovarian cancer growth and progression,” Dr. AlHilli said. In the present study, tumor bearing mice were fed a keto diet consisting of 10% protein, 0% carbohydrates, and 90% fat, while the high-fat diet was 10% protein, 15% carbohydrates, and 75% fat. The control diet consisted of 10% protein, 77% carbohydrates, and 13% fat. Epithelial ovarian cancer tumor growth was monitored weekly.
Over the 6- to 10-week course of study, a 9.1-fold increase from baseline in tumor growth was observed in the keto diet-fed mice (n = 20). Among mice fed a high-fat diet (n = 20) that included some carbohydrates, tumor growth increased 2.0-fold from baseline, and among control group mice (n = 20) fed a low-fat, high carbohydrate diet, tumor growth increased 3.1-fold.
The investigators observed several hallmarks of tumor progression: tumor associated macrophages were enriched significantly, activated lymphoid cells (natural killer cells) were significantly reduced (P < .001), and M2:M1 polarization trended higher. Also, in keto diet–fed mice, gene set enrichment analysis revealed that epithelial ovarian cancer tumors had increased angiogenesis and inflammatory responses, enhanced epithelial-to-mesenchymal transition phenotype, and altered lipid metabolism. Compared with high-fat diet–fed mice, the keto-fed mice had increases in lipid catalytic activity and catabolism, as well as decreases in lipid synthesis.
“The tumor increase could be mediated by the gut microbiome or by gene alterations or by metabolite levels that influence tumor growth. It’s possible that each cancer type is different. The composition of the diet may be a factor, as well as how tumors metabolize fat and ketones,” Dr. AlHilli said.
The results need to be confirmed in preclinical animal studies and in additional models, she added.
The study was funded by a K12 Grant and internal funding from Cleveland Clinic. Dr. AlHilli declared no relevant disclosures.
A ketogenic diet fed to mice with epithelial ovarian cancer led to significantly increased tumor growth and gut microbiome alterations, according to study recently presented at the annual meeting of the Society of Gynecologic Oncology.
“The keto diet is very popular, especially among patients who believe it may treat cancer by starving tumors of the fuel they need to grow, altering the immune system, and other anticancer effects,” said study leader Mariam AlHilli, MD, of the Cleveland Clinic.
The findings are surprising because in other studies the high-fat, zero-carb ketogenic diet has demonstrated tumor-suppressing effects. It has been under study as a possible adjuvant therapy for other cancers, such as glioblastoma, colon cancer, prostate cancer, and pancreatic cancer.
“While we don’t know yet whether these findings extend to patients, the results in animals indicate that instead of being protective, the keto diet appears to promote ovarian cancer growth and progression,” Dr. AlHilli said. In the present study, tumor bearing mice were fed a keto diet consisting of 10% protein, 0% carbohydrates, and 90% fat, while the high-fat diet was 10% protein, 15% carbohydrates, and 75% fat. The control diet consisted of 10% protein, 77% carbohydrates, and 13% fat. Epithelial ovarian cancer tumor growth was monitored weekly.
Over the 6- to 10-week course of study, a 9.1-fold increase from baseline in tumor growth was observed in the keto diet-fed mice (n = 20). Among mice fed a high-fat diet (n = 20) that included some carbohydrates, tumor growth increased 2.0-fold from baseline, and among control group mice (n = 20) fed a low-fat, high carbohydrate diet, tumor growth increased 3.1-fold.
The investigators observed several hallmarks of tumor progression: tumor associated macrophages were enriched significantly, activated lymphoid cells (natural killer cells) were significantly reduced (P < .001), and M2:M1 polarization trended higher. Also, in keto diet–fed mice, gene set enrichment analysis revealed that epithelial ovarian cancer tumors had increased angiogenesis and inflammatory responses, enhanced epithelial-to-mesenchymal transition phenotype, and altered lipid metabolism. Compared with high-fat diet–fed mice, the keto-fed mice had increases in lipid catalytic activity and catabolism, as well as decreases in lipid synthesis.
“The tumor increase could be mediated by the gut microbiome or by gene alterations or by metabolite levels that influence tumor growth. It’s possible that each cancer type is different. The composition of the diet may be a factor, as well as how tumors metabolize fat and ketones,” Dr. AlHilli said.
The results need to be confirmed in preclinical animal studies and in additional models, she added.
The study was funded by a K12 Grant and internal funding from Cleveland Clinic. Dr. AlHilli declared no relevant disclosures.
FROM SGO 2022
AI model predicts ovarian cancer responses
The model, using still-frame images from pretreatment laparoscopic surgical videos, had an overall accuracy rate of 93%, according to the pilot study’s first author, Deanna Glassman, MD, an oncologic fellow at the University of Texas MD Anderson Cancer Center, Houston.
Dr. Glassman described her research in a presentation given at the annual meeting of the Society of Gynecologic Oncology.
While the AI model successfully identified all excellent-response patients, it did classify about a third of patients with poor responses as excellent responses. The smaller number of images in the poor-response category, Dr. Glassman speculated, may explain the misclassification.
Researchers took 435 representative still-frame images from pretreatment laparoscopic surgical videos of 113 patients with pathologically proven high-grade serous ovarian cancer. Using 70% of the images to train the model, they used 10% for validation and 20% for the actual testing. They developed the AI model with images from four anatomical locations (diaphragm, omentum, peritoneum, and pelvis), training it using deep learning and neural networks to extract morphological disease patterns for correlation with either of two outcomes: excellent response or poor response. An excellent response was defined as progression-free survival of 12 months or more, and poor response as PFS of 6 months or less. In the retrospective study of images, after excluding 32 gray-zone patients, 75 patients (66%) had durable responses to therapy and 6 (5%) had poor responses.
The PFS was 19 months in the excellent-response group and 3 months in the poor-response group.
Clinicians have often observed differences in gross morphology within the single histologic diagnosis of high-grade serous ovarian cancer. The research intent was to determine if AI could detect these distinct morphological patterns in the still frame images taken at the time of laparoscopy, and correlate them with the eventual clinical outcomes. Dr. Glassman and colleagues are currently validating the model with a much larger cohort, and will look into clinical testing.
“The big-picture goal,” Dr. Glassman said in an interview, “would be to utilize the model to predict which patients would do well with traditional standard of care treatments and those who wouldn’t do well so that we can personalize the treatment plan for those patients with alternative agents and therapies.”
Once validated, the model could also be employed to identify patterns of disease in other gynecologic cancers or distinguish between viable and necrosed malignant tissue.
The study’s predominant limitation was the small sample size which is being addressed in a larger ongoing study.
Funding was provided by a T32 grant, MD Anderson Cancer Center Support Grant, MD Anderson Ovarian Cancer Moon Shot, SPORE in Ovarian Cancer, the American Cancer Society, and the Ovarian Cancer Research Alliance. Dr. Glassman declared no relevant financial relationships.
The model, using still-frame images from pretreatment laparoscopic surgical videos, had an overall accuracy rate of 93%, according to the pilot study’s first author, Deanna Glassman, MD, an oncologic fellow at the University of Texas MD Anderson Cancer Center, Houston.
Dr. Glassman described her research in a presentation given at the annual meeting of the Society of Gynecologic Oncology.
While the AI model successfully identified all excellent-response patients, it did classify about a third of patients with poor responses as excellent responses. The smaller number of images in the poor-response category, Dr. Glassman speculated, may explain the misclassification.
Researchers took 435 representative still-frame images from pretreatment laparoscopic surgical videos of 113 patients with pathologically proven high-grade serous ovarian cancer. Using 70% of the images to train the model, they used 10% for validation and 20% for the actual testing. They developed the AI model with images from four anatomical locations (diaphragm, omentum, peritoneum, and pelvis), training it using deep learning and neural networks to extract morphological disease patterns for correlation with either of two outcomes: excellent response or poor response. An excellent response was defined as progression-free survival of 12 months or more, and poor response as PFS of 6 months or less. In the retrospective study of images, after excluding 32 gray-zone patients, 75 patients (66%) had durable responses to therapy and 6 (5%) had poor responses.
The PFS was 19 months in the excellent-response group and 3 months in the poor-response group.
Clinicians have often observed differences in gross morphology within the single histologic diagnosis of high-grade serous ovarian cancer. The research intent was to determine if AI could detect these distinct morphological patterns in the still frame images taken at the time of laparoscopy, and correlate them with the eventual clinical outcomes. Dr. Glassman and colleagues are currently validating the model with a much larger cohort, and will look into clinical testing.
“The big-picture goal,” Dr. Glassman said in an interview, “would be to utilize the model to predict which patients would do well with traditional standard of care treatments and those who wouldn’t do well so that we can personalize the treatment plan for those patients with alternative agents and therapies.”
Once validated, the model could also be employed to identify patterns of disease in other gynecologic cancers or distinguish between viable and necrosed malignant tissue.
The study’s predominant limitation was the small sample size which is being addressed in a larger ongoing study.
Funding was provided by a T32 grant, MD Anderson Cancer Center Support Grant, MD Anderson Ovarian Cancer Moon Shot, SPORE in Ovarian Cancer, the American Cancer Society, and the Ovarian Cancer Research Alliance. Dr. Glassman declared no relevant financial relationships.
The model, using still-frame images from pretreatment laparoscopic surgical videos, had an overall accuracy rate of 93%, according to the pilot study’s first author, Deanna Glassman, MD, an oncologic fellow at the University of Texas MD Anderson Cancer Center, Houston.
Dr. Glassman described her research in a presentation given at the annual meeting of the Society of Gynecologic Oncology.
While the AI model successfully identified all excellent-response patients, it did classify about a third of patients with poor responses as excellent responses. The smaller number of images in the poor-response category, Dr. Glassman speculated, may explain the misclassification.
Researchers took 435 representative still-frame images from pretreatment laparoscopic surgical videos of 113 patients with pathologically proven high-grade serous ovarian cancer. Using 70% of the images to train the model, they used 10% for validation and 20% for the actual testing. They developed the AI model with images from four anatomical locations (diaphragm, omentum, peritoneum, and pelvis), training it using deep learning and neural networks to extract morphological disease patterns for correlation with either of two outcomes: excellent response or poor response. An excellent response was defined as progression-free survival of 12 months or more, and poor response as PFS of 6 months or less. In the retrospective study of images, after excluding 32 gray-zone patients, 75 patients (66%) had durable responses to therapy and 6 (5%) had poor responses.
The PFS was 19 months in the excellent-response group and 3 months in the poor-response group.
Clinicians have often observed differences in gross morphology within the single histologic diagnosis of high-grade serous ovarian cancer. The research intent was to determine if AI could detect these distinct morphological patterns in the still frame images taken at the time of laparoscopy, and correlate them with the eventual clinical outcomes. Dr. Glassman and colleagues are currently validating the model with a much larger cohort, and will look into clinical testing.
“The big-picture goal,” Dr. Glassman said in an interview, “would be to utilize the model to predict which patients would do well with traditional standard of care treatments and those who wouldn’t do well so that we can personalize the treatment plan for those patients with alternative agents and therapies.”
Once validated, the model could also be employed to identify patterns of disease in other gynecologic cancers or distinguish between viable and necrosed malignant tissue.
The study’s predominant limitation was the small sample size which is being addressed in a larger ongoing study.
Funding was provided by a T32 grant, MD Anderson Cancer Center Support Grant, MD Anderson Ovarian Cancer Moon Shot, SPORE in Ovarian Cancer, the American Cancer Society, and the Ovarian Cancer Research Alliance. Dr. Glassman declared no relevant financial relationships.
FROM SGO 2022
Steroids counter ataxia telangiectasia
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
SEATTLE –
The disease is an autosomal recessive disorder caused by mutations in the ATM gene, which is critical to the response to cellular insults such as DNA breaks, oxidative damage, and other forms of stress. The result is clinical manifestations that range from a suppressed immune system to organ damage and neurological symptoms that typically lead patients to be wheelchair bound by their teenage years.
“It’s really multisystem and a very, very difficult disease for people to live with,” Howard M. Lederman, MD, PhD, said in an interview. Dr. Lederman is a coauthor of the study, which was presented by Stefan Zielen, PhD, professor at the University of Goethe, at the 2022 annual meeting of the American Academy of Neurology.
Various therapies have been developed to improve immunodeficiency, lung disease, and some of the other clinical aspects of the condition, but there is no treatment for its neurological effects. “There’s not really been a good animal model, which has been a big problem in trying to test drugs and design treatment trials,” said Dr. Lederman, professor of pediatrics and medicine at Johns Hopkins University, Baltimore.
The new results may change that. “In the children under the age of 9, there was really a very clear slowdown in the neurodegeneration, and specifically the time that it took for them to lose the ability to ambulate. It’s very exciting, because it’s the first time that anybody has really shown in a double-blind, placebo-controlled, large phase 3 study that any drug has been able to do this. And there were really no steroid side effects, which is the other really remarkable thing about this study,” said Dr. Lederman.
The therapy grew out of a study by researchers in Italy who treated pediatric ataxia telangiectasia patients with corticosteroids and found some transitory improvements in gross motor function, but concerns about long-term exposure to steroids limited its application. EryDel, which specializes in encapsulating therapeutics in red blood cells, became interested and developed a formulation using the patient’s own red blood cells infused with DSP. Reinfused to the patients, the red blood cells slowly release the steroid.
It isn’t clear how dexamethasone works. There are data suggesting that it might lead to transcription of small pieces of the ATM protein, “but that has really not been nailed down in any way at this point. Corticosteroids act on all kinds of cells in all kinds of ways, and so there might be a little bit of this so-called mini-ATM that’s produced, but that may or may not be related to the way in which corticosteroids have a beneficial effect on the rate of neurodegeneration,” said Dr. Lederman.
The treatment process is not easy. Children must have 50-60 cc of blood removed. Red blood cells treated to become porous are exposed to DSP, and then resealed. Then the cells are reinfused. “The whole process takes from beginning to end probably about 3 hours, with a really experienced team of people doing it. And it’s limiting because it’s not easy to put in an IV and take 50 or 60 cc of blood out of children much younger than 5 or 6. The process is now being modified to see whether we could do it with 20 to 30 cc instead,” said Dr. Lederman.
A ‘promising and impressive’ study
The study is promising, according to Nicholas Johnson, MD, who comoderated the session where the study was presented. “They were able to show a slower rate of neurological degeneration or duration on both the lower and higher dose compared with the placebo. This is promising and impressive, in the sense that it’s a really large (trial) for a rare condition,” Dr. Johnson, vice chair of research at Virginia Commonwealth University, Richmond, said in an interview.
The study included 164 patients Europe, Australia, Israel, Tunisia, India, and the United States, who received 5-10 mg dexamethasone, 14-22 mg DSP, or placebo. Mean ages in each group ranged from 9.6 to 10.4 years.
In an intention-to-treat analysis, modified International Cooperative Ataxia Rating Scale (mICARS) scores trended toward improvement in the low-dose (–1.37; P = .0847) and high-dose groups (–1.40; P = .0765) when determined by central raters during the COVID-19 pandemic. There was also a trend toward improvement when determined by local raters in the low dose group (–1.73; P = .0720) and a statistically significant change in the high dose group (–2.11; P = .0277). The researchers noted some inconsistency between local and central raters, due to inconsistency of videography and language challenges for central raters.
An intention-to-treat analysis of a subgroup of 89 patients age 6-9, who were compared with natural history data from 245 patients, found a deterioration of mICARS of 3.7 per year, compared with 0.92 in the high-dose group, for a reduction of 75% (P = .020). In the high-dose group, 51.7% had a minimal or significant improvement compared with baseline according to the Clinical Global Impression of Change, as did 29.0% on low dose, and 27.6% in the placebo group.
AT AAN 2022
Type 2 diabetes remission possible for those with lower BMI
A weight-loss program can lead to type 2 diabetes remission, even in individuals with a normal body mass index (BMI), via loss of body fat, particularly in the liver and pancreas, shows a U.K. study.
The ReTUNE trial, funded by Diabetes UK, involved 20 people with type 2 diabetes of less than 6 year’s duration and a BMI of 27 kg/m2 or lower.

After 1 year, participants had lost 9% of their body weight.
Their body fat decreased significantly, to the same level as controls without type 2 diabetes, and they experienced decreases in liver fat, total triglycerides, and pancreatic fat.
The research, presented at the 2022 Diabetes UK Professional Conference, also showed this was accompanied by increases in insulin secretion and reductions in hemoglobin A1c and fasting plasma glucose levels.
Lead author Roy Taylor, MD, PhD, professor of medicine and metabolism, Newcastle University, Newcastle upon Tyne, England, said the findings indicate that the “etiology and pathophysiology of type 2 diabetes is the same whether BMI is normal or raised.”
This information should make a profound difference in what doctors advise their patients, Dr. Taylor added.
“One of the dramatic things about dealing with people in this group,” he said, “is they feel very resentful that healthcare professionals tell them not to lose weight.”
Based on the current results, Dr. Taylor believes this is “inappropriate advice, and it’s that personal advice that I think that this study points a way towards.”
Weight loss ‘first line of treatment’
These findings support the theory of a personal fat threshold, above which “type 2 diabetes occurs,” said Dr. Taylor. “Weight loss is the first-line treatment for all with type 2 diabetes, irrespective of BMI.”
Dr. Taylor already showed in the DiRECT trial that a calorie-restricted liquid diet followed by gradual food reintroduction and a weight-loss maintenance program can achieve and sustain type 2 diabetes remission at 2 years in people who are overweight or obese.
As reported this news organization, 36% of 300 patients enrolled in the trial attained diabetes remission and maintained it out to 24 months, compared with negligible changes in the control group.
Inspired by the results of DiRECT and the DROPLET study, the National Health Service has been rolling out a low calorie–diet treatment program for people who are overweight and living with diabetes.
Asked during the postpresentation discussion whether the current results could have implications for the NHS program, Dr. Taylor said it remains, in effect, a study and will not change things for now.
Chris Askew, chief executive of Diabetes UK, said in a release: “This game-changing study ... advances our understanding of why type 2 diabetes develops and what can be done to treat it.
“Our ambition is for as many people as possible to have the chance to put their type 2 diabetes into remission and live well for longer.”
Mr. Askew continued: “The findings of ReTUNE potentially take us a significant step closer to achieving this goal by showing that remission isn’t only possible for people of certain body weights.”
Weight and body fat decrease led to remission
For ReTUNE, the team recruited 20 individuals with type 2 diabetes of less than 6 year’s duration who had a BMI of 21-27 and compared them with 20 matched controls, with a follow-up of 52 weeks.
Patients were an average age of 59.0 years, 13 were women, mean BMI was 24.8, and average duration of diabetes was 2.8 years. Mean A1c was 54 mmol/mol.
Fourteen of the patients were taking metformin at enrollment and two were being treated with gliclazide. These medications were stopped when the individuals with type 2 diabetes entered a weight-loss program incremented in 5% steps, followed by 6 weeks of weight stability.
Overall, weight decreased by an average of 9%, while body fat decreased from 32% at baseline to 28% at 1 year (P < .001), the same percentage as that seen in the controls.
Liver fats also decreased significantly from baseline (P < .001) down to approximately the same level as controls at 1 year, a pattern also seen with very low-density lipoprotein cholesterol and triglyceride levels.
Pancreatic fat decreased steadily and significantly over the course of the 52-week follow-up (P < .05), although remained above the level seen in controls.
Insulin secretion increased significantly over the course of the study (P = .005) to finish just over the threshold for the lower range of normal at 52 weeks.
This, Dr. Taylor showed, was enough for the 14 patients who achieved type 2 diabetes remission to see their A1c levels fall significantly during follow-up (P < .001), alongside fasting plasma glucose levels (P < .001).
ReTUNE is funded by Diabetes UK. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A weight-loss program can lead to type 2 diabetes remission, even in individuals with a normal body mass index (BMI), via loss of body fat, particularly in the liver and pancreas, shows a U.K. study.
The ReTUNE trial, funded by Diabetes UK, involved 20 people with type 2 diabetes of less than 6 year’s duration and a BMI of 27 kg/m2 or lower.
After 1 year, participants had lost 9% of their body weight.
Their body fat decreased significantly, to the same level as controls without type 2 diabetes, and they experienced decreases in liver fat, total triglycerides, and pancreatic fat.
The research, presented at the 2022 Diabetes UK Professional Conference, also showed this was accompanied by increases in insulin secretion and reductions in hemoglobin A1c and fasting plasma glucose levels.
Lead author Roy Taylor, MD, PhD, professor of medicine and metabolism, Newcastle University, Newcastle upon Tyne, England, said the findings indicate that the “etiology and pathophysiology of type 2 diabetes is the same whether BMI is normal or raised.”
This information should make a profound difference in what doctors advise their patients, Dr. Taylor added.
“One of the dramatic things about dealing with people in this group,” he said, “is they feel very resentful that healthcare professionals tell them not to lose weight.”
Based on the current results, Dr. Taylor believes this is “inappropriate advice, and it’s that personal advice that I think that this study points a way towards.”
Weight loss ‘first line of treatment’
These findings support the theory of a personal fat threshold, above which “type 2 diabetes occurs,” said Dr. Taylor. “Weight loss is the first-line treatment for all with type 2 diabetes, irrespective of BMI.”
Dr. Taylor already showed in the DiRECT trial that a calorie-restricted liquid diet followed by gradual food reintroduction and a weight-loss maintenance program can achieve and sustain type 2 diabetes remission at 2 years in people who are overweight or obese.
As reported this news organization, 36% of 300 patients enrolled in the trial attained diabetes remission and maintained it out to 24 months, compared with negligible changes in the control group.
Inspired by the results of DiRECT and the DROPLET study, the National Health Service has been rolling out a low calorie–diet treatment program for people who are overweight and living with diabetes.
Asked during the postpresentation discussion whether the current results could have implications for the NHS program, Dr. Taylor said it remains, in effect, a study and will not change things for now.
Chris Askew, chief executive of Diabetes UK, said in a release: “This game-changing study ... advances our understanding of why type 2 diabetes develops and what can be done to treat it.
“Our ambition is for as many people as possible to have the chance to put their type 2 diabetes into remission and live well for longer.”
Mr. Askew continued: “The findings of ReTUNE potentially take us a significant step closer to achieving this goal by showing that remission isn’t only possible for people of certain body weights.”
Weight and body fat decrease led to remission
For ReTUNE, the team recruited 20 individuals with type 2 diabetes of less than 6 year’s duration who had a BMI of 21-27 and compared them with 20 matched controls, with a follow-up of 52 weeks.
Patients were an average age of 59.0 years, 13 were women, mean BMI was 24.8, and average duration of diabetes was 2.8 years. Mean A1c was 54 mmol/mol.
Fourteen of the patients were taking metformin at enrollment and two were being treated with gliclazide. These medications were stopped when the individuals with type 2 diabetes entered a weight-loss program incremented in 5% steps, followed by 6 weeks of weight stability.
Overall, weight decreased by an average of 9%, while body fat decreased from 32% at baseline to 28% at 1 year (P < .001), the same percentage as that seen in the controls.
Liver fats also decreased significantly from baseline (P < .001) down to approximately the same level as controls at 1 year, a pattern also seen with very low-density lipoprotein cholesterol and triglyceride levels.
Pancreatic fat decreased steadily and significantly over the course of the 52-week follow-up (P < .05), although remained above the level seen in controls.
Insulin secretion increased significantly over the course of the study (P = .005) to finish just over the threshold for the lower range of normal at 52 weeks.
This, Dr. Taylor showed, was enough for the 14 patients who achieved type 2 diabetes remission to see their A1c levels fall significantly during follow-up (P < .001), alongside fasting plasma glucose levels (P < .001).
ReTUNE is funded by Diabetes UK. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A weight-loss program can lead to type 2 diabetes remission, even in individuals with a normal body mass index (BMI), via loss of body fat, particularly in the liver and pancreas, shows a U.K. study.
The ReTUNE trial, funded by Diabetes UK, involved 20 people with type 2 diabetes of less than 6 year’s duration and a BMI of 27 kg/m2 or lower.
After 1 year, participants had lost 9% of their body weight.
Their body fat decreased significantly, to the same level as controls without type 2 diabetes, and they experienced decreases in liver fat, total triglycerides, and pancreatic fat.
The research, presented at the 2022 Diabetes UK Professional Conference, also showed this was accompanied by increases in insulin secretion and reductions in hemoglobin A1c and fasting plasma glucose levels.
Lead author Roy Taylor, MD, PhD, professor of medicine and metabolism, Newcastle University, Newcastle upon Tyne, England, said the findings indicate that the “etiology and pathophysiology of type 2 diabetes is the same whether BMI is normal or raised.”
This information should make a profound difference in what doctors advise their patients, Dr. Taylor added.
“One of the dramatic things about dealing with people in this group,” he said, “is they feel very resentful that healthcare professionals tell them not to lose weight.”
Based on the current results, Dr. Taylor believes this is “inappropriate advice, and it’s that personal advice that I think that this study points a way towards.”
Weight loss ‘first line of treatment’
These findings support the theory of a personal fat threshold, above which “type 2 diabetes occurs,” said Dr. Taylor. “Weight loss is the first-line treatment for all with type 2 diabetes, irrespective of BMI.”
Dr. Taylor already showed in the DiRECT trial that a calorie-restricted liquid diet followed by gradual food reintroduction and a weight-loss maintenance program can achieve and sustain type 2 diabetes remission at 2 years in people who are overweight or obese.
As reported this news organization, 36% of 300 patients enrolled in the trial attained diabetes remission and maintained it out to 24 months, compared with negligible changes in the control group.
Inspired by the results of DiRECT and the DROPLET study, the National Health Service has been rolling out a low calorie–diet treatment program for people who are overweight and living with diabetes.
Asked during the postpresentation discussion whether the current results could have implications for the NHS program, Dr. Taylor said it remains, in effect, a study and will not change things for now.
Chris Askew, chief executive of Diabetes UK, said in a release: “This game-changing study ... advances our understanding of why type 2 diabetes develops and what can be done to treat it.
“Our ambition is for as many people as possible to have the chance to put their type 2 diabetes into remission and live well for longer.”
Mr. Askew continued: “The findings of ReTUNE potentially take us a significant step closer to achieving this goal by showing that remission isn’t only possible for people of certain body weights.”
Weight and body fat decrease led to remission
For ReTUNE, the team recruited 20 individuals with type 2 diabetes of less than 6 year’s duration who had a BMI of 21-27 and compared them with 20 matched controls, with a follow-up of 52 weeks.
Patients were an average age of 59.0 years, 13 were women, mean BMI was 24.8, and average duration of diabetes was 2.8 years. Mean A1c was 54 mmol/mol.
Fourteen of the patients were taking metformin at enrollment and two were being treated with gliclazide. These medications were stopped when the individuals with type 2 diabetes entered a weight-loss program incremented in 5% steps, followed by 6 weeks of weight stability.
Overall, weight decreased by an average of 9%, while body fat decreased from 32% at baseline to 28% at 1 year (P < .001), the same percentage as that seen in the controls.
Liver fats also decreased significantly from baseline (P < .001) down to approximately the same level as controls at 1 year, a pattern also seen with very low-density lipoprotein cholesterol and triglyceride levels.
Pancreatic fat decreased steadily and significantly over the course of the 52-week follow-up (P < .05), although remained above the level seen in controls.
Insulin secretion increased significantly over the course of the study (P = .005) to finish just over the threshold for the lower range of normal at 52 weeks.
This, Dr. Taylor showed, was enough for the 14 patients who achieved type 2 diabetes remission to see their A1c levels fall significantly during follow-up (P < .001), alongside fasting plasma glucose levels (P < .001).
ReTUNE is funded by Diabetes UK. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hospital factors drive many discharges against medical advice
The analysis found that in about 1 in 5 cases, shortcomings in the quality of care and other factors beyond patients’ control explain why they leave the hospital before completing recommended treatment.
Clinicians may be quick to blame patients for so-called discharges against medical advice (AMA), which comprise up to 2% of hospital admissions and are associated with an increased risk of mortality and readmission. But “we as providers are very much involved in the reasons why these patients left,” Kushinga Bvute, MD, MPH, a second-year internal medicine resident at Florida Atlantic University, Boca Raton, who led the new study, told this news organization. Dr. Bvute and her colleagues presented their findings April 6 at the Society of General Internal Medicine (SGIM) 2022 Annual Meeting, Orlando, Florida.
Dr. Bvute and her colleagues reviewed the records of 548 AMA discharges – out of a total of 354,767 discharges – from Boca Raton Regional Hospital from January 2020 to January 2021. In 44% of cases, patients cited their own reasons for leaving. But in nearly 20% of AMA discharges, the researchers identified factors linked to treatment.
Hospital-related reasons patients cited for leaving AMA were general wait times (3.5%), provider wait times (2.6%), provider care (2.9%), the hospital environment (2.7%), wanting a private room (2%), and seeking medical care elsewhere (6.2%).
Patient-related factors were refusing treatment (27%), feeling better (3.5%), addiction problems (2.9%), financial complications (2.9%), and dependent care (2.4%). Ten (1.8%) eloped, according to the researchers.
Nearly 60% of patients who were discharged AMA were men, with a mean age of 56 years (standard deviation, 19.13). The average stay was 1.64 days.
In roughly one-third of cases, there was no documented reason for the departure – underscoring the need for better reporting, according to the researchers.
To address AMA discharges, hospitals “need to focus on factors they influence, such as high-quality patient care, the hospital environment, and provider-patient relationships,” the researchers report.
New procedures needed
The hospital is working on procedures to ensure that reasons for AMA discharges are documented. The administration also is implementing preventive steps, such as communicating with patients about the risks of leaving and providing discharge plans to reduce the likelihood that a patient will return, Dr. Bvute told this news organization.
Dr. Bvute said the findings should encourage individual clinicians to “remove any stereotypes that sometimes come attached to having those three letters on your charts.”
Data were collected during the COVID-19 pandemic, but Dr. Bvute does not believe that fear of coronavirus exposure drove many patients to leave the hospital prematurely.
The study is notable for approaching AMA discharges from a quality improvement perspective, David Alfandre, MD, MPH, a health care ethicist at the VA National Center for Ethics in Health Care, Washington, D.C., said in an interview.
Dr. Alfandre, who was not involved in the study, said it reflects growing recognition that hospitals can take steps to reduce adverse outcomes associated with AMA discharges. “It’s starting to shift the conversation to saying, this isn’t just the patient’s problem, but this is the health care provider’s problem,” he said.
Dr. Alfandre co-authored a 2021 analysis showing that hospital characteristics account for 7.3% of variation in the probability of a patient being discharged AMA. However, research is needed to identify effective interventions besides the established use of buprenorphine and naloxone for patients with opioid use disorder. “I think everybody recognizes the quality of communication is poor, but that doesn’t really help us operationalize that to know what to do,” he said.
Emily Holmes, MD, MPH, medical director of the Changing Health Outcomes Through Integrated Care Excellence Program at IU Health, Indianapolis, cautioned that data may be biased because defining AMA discharge can be subjective.
Reasons are not consistently documented and can be difficult to capture because they are often multifactorial, Dr. Holmes said. “For example, long wait times are more problematic when a patient is worried about finances and care for a child,” she said.
But Dr. Holmes, who was not involved in the study, said it does encourage clinicians “to think about what we can do systematically to reduce AMA discharges.”
Dr. Bvute, Dr. Alfandre, and Dr. Holmes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The analysis found that in about 1 in 5 cases, shortcomings in the quality of care and other factors beyond patients’ control explain why they leave the hospital before completing recommended treatment.
Clinicians may be quick to blame patients for so-called discharges against medical advice (AMA), which comprise up to 2% of hospital admissions and are associated with an increased risk of mortality and readmission. But “we as providers are very much involved in the reasons why these patients left,” Kushinga Bvute, MD, MPH, a second-year internal medicine resident at Florida Atlantic University, Boca Raton, who led the new study, told this news organization. Dr. Bvute and her colleagues presented their findings April 6 at the Society of General Internal Medicine (SGIM) 2022 Annual Meeting, Orlando, Florida.
Dr. Bvute and her colleagues reviewed the records of 548 AMA discharges – out of a total of 354,767 discharges – from Boca Raton Regional Hospital from January 2020 to January 2021. In 44% of cases, patients cited their own reasons for leaving. But in nearly 20% of AMA discharges, the researchers identified factors linked to treatment.
Hospital-related reasons patients cited for leaving AMA were general wait times (3.5%), provider wait times (2.6%), provider care (2.9%), the hospital environment (2.7%), wanting a private room (2%), and seeking medical care elsewhere (6.2%).
Patient-related factors were refusing treatment (27%), feeling better (3.5%), addiction problems (2.9%), financial complications (2.9%), and dependent care (2.4%). Ten (1.8%) eloped, according to the researchers.
Nearly 60% of patients who were discharged AMA were men, with a mean age of 56 years (standard deviation, 19.13). The average stay was 1.64 days.
In roughly one-third of cases, there was no documented reason for the departure – underscoring the need for better reporting, according to the researchers.
To address AMA discharges, hospitals “need to focus on factors they influence, such as high-quality patient care, the hospital environment, and provider-patient relationships,” the researchers report.
New procedures needed
The hospital is working on procedures to ensure that reasons for AMA discharges are documented. The administration also is implementing preventive steps, such as communicating with patients about the risks of leaving and providing discharge plans to reduce the likelihood that a patient will return, Dr. Bvute told this news organization.
Dr. Bvute said the findings should encourage individual clinicians to “remove any stereotypes that sometimes come attached to having those three letters on your charts.”
Data were collected during the COVID-19 pandemic, but Dr. Bvute does not believe that fear of coronavirus exposure drove many patients to leave the hospital prematurely.
The study is notable for approaching AMA discharges from a quality improvement perspective, David Alfandre, MD, MPH, a health care ethicist at the VA National Center for Ethics in Health Care, Washington, D.C., said in an interview.
Dr. Alfandre, who was not involved in the study, said it reflects growing recognition that hospitals can take steps to reduce adverse outcomes associated with AMA discharges. “It’s starting to shift the conversation to saying, this isn’t just the patient’s problem, but this is the health care provider’s problem,” he said.
Dr. Alfandre co-authored a 2021 analysis showing that hospital characteristics account for 7.3% of variation in the probability of a patient being discharged AMA. However, research is needed to identify effective interventions besides the established use of buprenorphine and naloxone for patients with opioid use disorder. “I think everybody recognizes the quality of communication is poor, but that doesn’t really help us operationalize that to know what to do,” he said.
Emily Holmes, MD, MPH, medical director of the Changing Health Outcomes Through Integrated Care Excellence Program at IU Health, Indianapolis, cautioned that data may be biased because defining AMA discharge can be subjective.
Reasons are not consistently documented and can be difficult to capture because they are often multifactorial, Dr. Holmes said. “For example, long wait times are more problematic when a patient is worried about finances and care for a child,” she said.
But Dr. Holmes, who was not involved in the study, said it does encourage clinicians “to think about what we can do systematically to reduce AMA discharges.”
Dr. Bvute, Dr. Alfandre, and Dr. Holmes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The analysis found that in about 1 in 5 cases, shortcomings in the quality of care and other factors beyond patients’ control explain why they leave the hospital before completing recommended treatment.
Clinicians may be quick to blame patients for so-called discharges against medical advice (AMA), which comprise up to 2% of hospital admissions and are associated with an increased risk of mortality and readmission. But “we as providers are very much involved in the reasons why these patients left,” Kushinga Bvute, MD, MPH, a second-year internal medicine resident at Florida Atlantic University, Boca Raton, who led the new study, told this news organization. Dr. Bvute and her colleagues presented their findings April 6 at the Society of General Internal Medicine (SGIM) 2022 Annual Meeting, Orlando, Florida.
Dr. Bvute and her colleagues reviewed the records of 548 AMA discharges – out of a total of 354,767 discharges – from Boca Raton Regional Hospital from January 2020 to January 2021. In 44% of cases, patients cited their own reasons for leaving. But in nearly 20% of AMA discharges, the researchers identified factors linked to treatment.
Hospital-related reasons patients cited for leaving AMA were general wait times (3.5%), provider wait times (2.6%), provider care (2.9%), the hospital environment (2.7%), wanting a private room (2%), and seeking medical care elsewhere (6.2%).
Patient-related factors were refusing treatment (27%), feeling better (3.5%), addiction problems (2.9%), financial complications (2.9%), and dependent care (2.4%). Ten (1.8%) eloped, according to the researchers.
Nearly 60% of patients who were discharged AMA were men, with a mean age of 56 years (standard deviation, 19.13). The average stay was 1.64 days.
In roughly one-third of cases, there was no documented reason for the departure – underscoring the need for better reporting, according to the researchers.
To address AMA discharges, hospitals “need to focus on factors they influence, such as high-quality patient care, the hospital environment, and provider-patient relationships,” the researchers report.
New procedures needed
The hospital is working on procedures to ensure that reasons for AMA discharges are documented. The administration also is implementing preventive steps, such as communicating with patients about the risks of leaving and providing discharge plans to reduce the likelihood that a patient will return, Dr. Bvute told this news organization.
Dr. Bvute said the findings should encourage individual clinicians to “remove any stereotypes that sometimes come attached to having those three letters on your charts.”
Data were collected during the COVID-19 pandemic, but Dr. Bvute does not believe that fear of coronavirus exposure drove many patients to leave the hospital prematurely.
The study is notable for approaching AMA discharges from a quality improvement perspective, David Alfandre, MD, MPH, a health care ethicist at the VA National Center for Ethics in Health Care, Washington, D.C., said in an interview.
Dr. Alfandre, who was not involved in the study, said it reflects growing recognition that hospitals can take steps to reduce adverse outcomes associated with AMA discharges. “It’s starting to shift the conversation to saying, this isn’t just the patient’s problem, but this is the health care provider’s problem,” he said.
Dr. Alfandre co-authored a 2021 analysis showing that hospital characteristics account for 7.3% of variation in the probability of a patient being discharged AMA. However, research is needed to identify effective interventions besides the established use of buprenorphine and naloxone for patients with opioid use disorder. “I think everybody recognizes the quality of communication is poor, but that doesn’t really help us operationalize that to know what to do,” he said.
Emily Holmes, MD, MPH, medical director of the Changing Health Outcomes Through Integrated Care Excellence Program at IU Health, Indianapolis, cautioned that data may be biased because defining AMA discharge can be subjective.
Reasons are not consistently documented and can be difficult to capture because they are often multifactorial, Dr. Holmes said. “For example, long wait times are more problematic when a patient is worried about finances and care for a child,” she said.
But Dr. Holmes, who was not involved in the study, said it does encourage clinicians “to think about what we can do systematically to reduce AMA discharges.”
Dr. Bvute, Dr. Alfandre, and Dr. Holmes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SGIM 2022