User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Double the pleasure: Stim patch delays early ejaculation: Study
A wearable patch that delivers electrical stimulation to the perineum may postpone premature ejaculation, according to research presented at the annual meeting of the American Urological Association. The disposable device appears to work by helping men contract the muscles in the pelvic floor, allowing them to postpone climax.
Among 34 men with a lifelong history of premature ejaculation, average intravaginal ejaculatory latency time – the time from vaginal penetration to ejaculation – increased from about 67 seconds at baseline to 123 seconds when they used the device.
Another 17 participants received a sham treatment – stimulation they could feel but that did not activate muscles. In this group, time to ejaculation increased from 63 seconds to 81 seconds.
The longer duration with active treatment was statistically significant (P < .0001), whereas the increase in the control group was not (P = .1653), said Ege Can Serefoglu, MD, a researcher at Biruni University, Istanbul, and editor-in-chief of the International Journal of Impotence Research.
Dr. Serefoglu is a member of the scientific advisory board for Virility Medical, a company in Hod Hasharon, Israel, that is developing the stimulator. Marketed as vPatch, the device is expected to be available in 2023, Dr. Serefoglu said. It was cleared by the Food and Drug Administration in November and has CE-mark approval in Europe, according to the company.
Common problem, limited options
Research shows that 20%-30% of men are not happy with their time to ejaculation, Dr. Serefoglu said.
The International Society for Sexual Medicine defines premature ejaculation as ejaculation which always or almost always occurs within about 1 minute of penetration, the patient is unable to delay this occurrence, and the condition causes personal distress.
“Unfortunately, in spite of its high prevalence we do not really have any satisfying treatment options,” Dr. Serefoglu said.
Topical anesthetics may be used to decrease the sensitivity of the glans penis, and selective serotonin reuptake inhibitors may help delay ejaculation. But these options have limited efficacy and low adherence, he said.
Preclinical studies have shown that injection of botulinum toxin into the bulbospongiosus muscles is associated with a dose-dependent increase in ejaculation latency in rats.
Data on ClinicalTrials.gov show that this approach also may increase ejaculation latency in men, Dr. Serefoglu said. Although investigators found no safety concerns, drugmaker Allergan made a strategic business decision to stop developing this treatment approach, according to the registration entry for the study.
The idea for vPatch came from researchers wondering if instead of paralyzing the muscles with botulinum toxin, they used electrical stimulation to cause contraction of those muscles, Dr. Serefoglu said. A smaller proof-of-concept study demonstrated the feasibility and safety of this technique.
To further assess the safety and efficacy of a transcutaneous perineal electrical stimulator for the treatment of premature ejaculation, investigators conducted the randomized, double-blind, sham-controlled trial at Rambam Medical Centre, Haifa, Israel, and Villa Donatello Clinic, Florence, Italy.
The trial included males with premature ejaculation aged 18-60 years. Their female partners measured IELT using a stopwatch during four sexual intercourse sessions before treatment, and four times on treatment, at home.
In addition to the increased time to ejaculation, perceived control over ejaculation, satisfaction with sexual intercourse, personal distress related to ejaculation, and interpersonal difficulty related to ejaculation all significantly improved with vPatch, the researchers found.
Of participants who received active treatment, 73.5% reported a subjective sense of improvement versus 41.2% of the control group.
Potential reactions
No serious adverse events were observed, Dr. Serefoglu reported. Potential adverse reactions include redness, discomfort, and localized pain, according to the company’s website.
Men should not use vPatch if they have been diagnosed with pelvic cancer, or if they have an implanted electronic device, diabetes with peripheral neuropathy, or perineal dermatologic diseases, irritations, or lesions. Other precautions include avoiding use of the vPatch in water or humid environments. The device has not been tested on use with a pregnant partner.
The disposable patches are meant for one-time use. “The miniaturized perineal stimulation device may become an on-demand, drug-free therapeutic option,” Dr. Serefoglu said.
Combining electrical stimulation with other treatment approaches may provide additional benefit, said Bradley Schwartz, DO, professor and chairman of urology at Southern Illinois University, Springfield, who moderated the session at the AUA meeting at which the results of the study were presented.
“You go from 1 to 2 minutes just with this device,” Dr. Schwartz said. “If you went from 2 to 3 minutes, you would essentially be tripling their pleasure or their time, which might make a significant difference.”
Serefoglu agreed that combining the stimulator with other treatment approaches such as topical anesthetics could increase patient satisfaction.
Comoderator Kelly Healy, MD, assistant professor of urology at Columbia University Medical Center, New York, highlighted a direction for future research: examining outcomes according to different types of relationships, as well as partner satisfaction.
“That is a perfect question that should also be considered in the future trials,” Dr. Serefoglu said. “This was mainly focused on the man’s satisfaction. But men are trying to delay their ejaculation to satisfy their partner.”
Dr. Serefoglu is on the scientific advisory board for Virility Medical, which sponsored the study. Dr. Healy had no disclosures. Dr. Schwartz disclosed ties to Cook Medical.
A version of this article first appeared on Medscape.com.
A wearable patch that delivers electrical stimulation to the perineum may postpone premature ejaculation, according to research presented at the annual meeting of the American Urological Association. The disposable device appears to work by helping men contract the muscles in the pelvic floor, allowing them to postpone climax.
Among 34 men with a lifelong history of premature ejaculation, average intravaginal ejaculatory latency time – the time from vaginal penetration to ejaculation – increased from about 67 seconds at baseline to 123 seconds when they used the device.
Another 17 participants received a sham treatment – stimulation they could feel but that did not activate muscles. In this group, time to ejaculation increased from 63 seconds to 81 seconds.
The longer duration with active treatment was statistically significant (P < .0001), whereas the increase in the control group was not (P = .1653), said Ege Can Serefoglu, MD, a researcher at Biruni University, Istanbul, and editor-in-chief of the International Journal of Impotence Research.
Dr. Serefoglu is a member of the scientific advisory board for Virility Medical, a company in Hod Hasharon, Israel, that is developing the stimulator. Marketed as vPatch, the device is expected to be available in 2023, Dr. Serefoglu said. It was cleared by the Food and Drug Administration in November and has CE-mark approval in Europe, according to the company.
Common problem, limited options
Research shows that 20%-30% of men are not happy with their time to ejaculation, Dr. Serefoglu said.
The International Society for Sexual Medicine defines premature ejaculation as ejaculation which always or almost always occurs within about 1 minute of penetration, the patient is unable to delay this occurrence, and the condition causes personal distress.
“Unfortunately, in spite of its high prevalence we do not really have any satisfying treatment options,” Dr. Serefoglu said.
Topical anesthetics may be used to decrease the sensitivity of the glans penis, and selective serotonin reuptake inhibitors may help delay ejaculation. But these options have limited efficacy and low adherence, he said.
Preclinical studies have shown that injection of botulinum toxin into the bulbospongiosus muscles is associated with a dose-dependent increase in ejaculation latency in rats.
Data on ClinicalTrials.gov show that this approach also may increase ejaculation latency in men, Dr. Serefoglu said. Although investigators found no safety concerns, drugmaker Allergan made a strategic business decision to stop developing this treatment approach, according to the registration entry for the study.
The idea for vPatch came from researchers wondering if instead of paralyzing the muscles with botulinum toxin, they used electrical stimulation to cause contraction of those muscles, Dr. Serefoglu said. A smaller proof-of-concept study demonstrated the feasibility and safety of this technique.
To further assess the safety and efficacy of a transcutaneous perineal electrical stimulator for the treatment of premature ejaculation, investigators conducted the randomized, double-blind, sham-controlled trial at Rambam Medical Centre, Haifa, Israel, and Villa Donatello Clinic, Florence, Italy.
The trial included males with premature ejaculation aged 18-60 years. Their female partners measured IELT using a stopwatch during four sexual intercourse sessions before treatment, and four times on treatment, at home.
In addition to the increased time to ejaculation, perceived control over ejaculation, satisfaction with sexual intercourse, personal distress related to ejaculation, and interpersonal difficulty related to ejaculation all significantly improved with vPatch, the researchers found.
Of participants who received active treatment, 73.5% reported a subjective sense of improvement versus 41.2% of the control group.
Potential reactions
No serious adverse events were observed, Dr. Serefoglu reported. Potential adverse reactions include redness, discomfort, and localized pain, according to the company’s website.
Men should not use vPatch if they have been diagnosed with pelvic cancer, or if they have an implanted electronic device, diabetes with peripheral neuropathy, or perineal dermatologic diseases, irritations, or lesions. Other precautions include avoiding use of the vPatch in water or humid environments. The device has not been tested on use with a pregnant partner.
The disposable patches are meant for one-time use. “The miniaturized perineal stimulation device may become an on-demand, drug-free therapeutic option,” Dr. Serefoglu said.
Combining electrical stimulation with other treatment approaches may provide additional benefit, said Bradley Schwartz, DO, professor and chairman of urology at Southern Illinois University, Springfield, who moderated the session at the AUA meeting at which the results of the study were presented.
“You go from 1 to 2 minutes just with this device,” Dr. Schwartz said. “If you went from 2 to 3 minutes, you would essentially be tripling their pleasure or their time, which might make a significant difference.”
Serefoglu agreed that combining the stimulator with other treatment approaches such as topical anesthetics could increase patient satisfaction.
Comoderator Kelly Healy, MD, assistant professor of urology at Columbia University Medical Center, New York, highlighted a direction for future research: examining outcomes according to different types of relationships, as well as partner satisfaction.
“That is a perfect question that should also be considered in the future trials,” Dr. Serefoglu said. “This was mainly focused on the man’s satisfaction. But men are trying to delay their ejaculation to satisfy their partner.”
Dr. Serefoglu is on the scientific advisory board for Virility Medical, which sponsored the study. Dr. Healy had no disclosures. Dr. Schwartz disclosed ties to Cook Medical.
A version of this article first appeared on Medscape.com.
A wearable patch that delivers electrical stimulation to the perineum may postpone premature ejaculation, according to research presented at the annual meeting of the American Urological Association. The disposable device appears to work by helping men contract the muscles in the pelvic floor, allowing them to postpone climax.
Among 34 men with a lifelong history of premature ejaculation, average intravaginal ejaculatory latency time – the time from vaginal penetration to ejaculation – increased from about 67 seconds at baseline to 123 seconds when they used the device.
Another 17 participants received a sham treatment – stimulation they could feel but that did not activate muscles. In this group, time to ejaculation increased from 63 seconds to 81 seconds.
The longer duration with active treatment was statistically significant (P < .0001), whereas the increase in the control group was not (P = .1653), said Ege Can Serefoglu, MD, a researcher at Biruni University, Istanbul, and editor-in-chief of the International Journal of Impotence Research.
Dr. Serefoglu is a member of the scientific advisory board for Virility Medical, a company in Hod Hasharon, Israel, that is developing the stimulator. Marketed as vPatch, the device is expected to be available in 2023, Dr. Serefoglu said. It was cleared by the Food and Drug Administration in November and has CE-mark approval in Europe, according to the company.
Common problem, limited options
Research shows that 20%-30% of men are not happy with their time to ejaculation, Dr. Serefoglu said.
The International Society for Sexual Medicine defines premature ejaculation as ejaculation which always or almost always occurs within about 1 minute of penetration, the patient is unable to delay this occurrence, and the condition causes personal distress.
“Unfortunately, in spite of its high prevalence we do not really have any satisfying treatment options,” Dr. Serefoglu said.
Topical anesthetics may be used to decrease the sensitivity of the glans penis, and selective serotonin reuptake inhibitors may help delay ejaculation. But these options have limited efficacy and low adherence, he said.
Preclinical studies have shown that injection of botulinum toxin into the bulbospongiosus muscles is associated with a dose-dependent increase in ejaculation latency in rats.
Data on ClinicalTrials.gov show that this approach also may increase ejaculation latency in men, Dr. Serefoglu said. Although investigators found no safety concerns, drugmaker Allergan made a strategic business decision to stop developing this treatment approach, according to the registration entry for the study.
The idea for vPatch came from researchers wondering if instead of paralyzing the muscles with botulinum toxin, they used electrical stimulation to cause contraction of those muscles, Dr. Serefoglu said. A smaller proof-of-concept study demonstrated the feasibility and safety of this technique.
To further assess the safety and efficacy of a transcutaneous perineal electrical stimulator for the treatment of premature ejaculation, investigators conducted the randomized, double-blind, sham-controlled trial at Rambam Medical Centre, Haifa, Israel, and Villa Donatello Clinic, Florence, Italy.
The trial included males with premature ejaculation aged 18-60 years. Their female partners measured IELT using a stopwatch during four sexual intercourse sessions before treatment, and four times on treatment, at home.
In addition to the increased time to ejaculation, perceived control over ejaculation, satisfaction with sexual intercourse, personal distress related to ejaculation, and interpersonal difficulty related to ejaculation all significantly improved with vPatch, the researchers found.
Of participants who received active treatment, 73.5% reported a subjective sense of improvement versus 41.2% of the control group.
Potential reactions
No serious adverse events were observed, Dr. Serefoglu reported. Potential adverse reactions include redness, discomfort, and localized pain, according to the company’s website.
Men should not use vPatch if they have been diagnosed with pelvic cancer, or if they have an implanted electronic device, diabetes with peripheral neuropathy, or perineal dermatologic diseases, irritations, or lesions. Other precautions include avoiding use of the vPatch in water or humid environments. The device has not been tested on use with a pregnant partner.
The disposable patches are meant for one-time use. “The miniaturized perineal stimulation device may become an on-demand, drug-free therapeutic option,” Dr. Serefoglu said.
Combining electrical stimulation with other treatment approaches may provide additional benefit, said Bradley Schwartz, DO, professor and chairman of urology at Southern Illinois University, Springfield, who moderated the session at the AUA meeting at which the results of the study were presented.
“You go from 1 to 2 minutes just with this device,” Dr. Schwartz said. “If you went from 2 to 3 minutes, you would essentially be tripling their pleasure or their time, which might make a significant difference.”
Serefoglu agreed that combining the stimulator with other treatment approaches such as topical anesthetics could increase patient satisfaction.
Comoderator Kelly Healy, MD, assistant professor of urology at Columbia University Medical Center, New York, highlighted a direction for future research: examining outcomes according to different types of relationships, as well as partner satisfaction.
“That is a perfect question that should also be considered in the future trials,” Dr. Serefoglu said. “This was mainly focused on the man’s satisfaction. But men are trying to delay their ejaculation to satisfy their partner.”
Dr. Serefoglu is on the scientific advisory board for Virility Medical, which sponsored the study. Dr. Healy had no disclosures. Dr. Schwartz disclosed ties to Cook Medical.
A version of this article first appeared on Medscape.com.
Pilonidal disease, other conditions may benefit from laser treatment
SAN DIEGO – Pilonidal disease – a chronic inflammatory condition that can trigger the formation of cysts and sinuses in the superior portion of the intragluteal cleft or the sacrococcygeal area – remains challenging to manage, but mounting evidence supports the use of lasers to enhance treatment success.
“Draining sinuses or acute abscesses are usually associated with an underlying cyst and associated granulation tissue, fibrosis, and tufts of hair,” Catherine M. DiGiorgio, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “This is why laser hair removal can help with the treatment of these patients.”

The suspected etiology is a foreign body reaction to the entrapped hairs, which are found in the sinuses in about 75% of cases. “The treatment for that is surgery,” said Dr. DiGiorgio, a laser and cosmetic dermatologist in Boston. Laser hair reduction decreases the recurrence of cyst formation and drainage, and is usually covered by insurance, she noted.
Supportive evidence
In a comparative study, French researchers retrospectively reviewed the efficacy of laser hair removal after surgery in reducing recurrence rate of pilonidal cysts, versus surgery alone. Of the 41 study participants, 12 had laser hair removal plus surgery and 29 had surgery alone. The rate of cyst recurrence was significantly lower in the laser hair removal plus surgery group, compared with the surgery only group (8.3% vs. 51.7%, respectively; P < .001).
In another study, researchers from the United Kingdom and The Johns Hopkins Hospital, Baltimore, evaluated the use of the long-pulsed Alexandrite laser in 19 patients with recurrent pilonidal disease who had undergone multiple surgeries.They were treated with the laser for hair removal in the sinus area, requiring 4-12 sessions. The researchers found that 84.2% of patients had a reduction of hair density to less than 5 hairs/cm2, while 15.8% had a reduction of hair density to 5-10 hairs/cm2. They also noted a statistically significant increase in disease-free time in the laser-treated group compared with those treated with surgical management only (P < .01).
Lasers for pseudofolliculitis barbae, HS
Lasers also play a significant role in the treatment of pseudofolliculitis barbae, a chronic, inflammatory disease that primarily affects the bearded area of men with thick hairs, usually those with a darker Fitzpatrick skin type. This can also occur in women, particularly those with polycystic ovary syndrome, Dr. DiGiorgio said.
In people with pseudofolliculitis barbae, the hair follicle is positioned at an acute angle to the skin surface and the sharp end of shaved hair reenters the skin, which results in the formation of pustules, papules, secondary infection, and keloids. Treatment involves a variety of medical therapies including retinoids, benzoyl peroxide, antibiotics, and keratolytics, “but laser hair removal is the best way to get rid of this issue, and results in permanent reduction,” she said. “When treating male patients with laser hair removal in the bearded area, you have to tell them that they won’t be able to grow a beard going forward. Most of them are okay with that.”
A 2002 study, led by E. Victor Ross, MD, of the Naval Medical Center, San Diego, evaluated treatment of pseudofolliculitis barbae in patients with skin types IV, V, and VI with a long-pulsed Nd:YAG laser. For the first phase of the study, the investigators tested epidermal tolerance on the thighs of 37 patients and determined that the laser was safe and effective. For the second phase 2 weeks later, they treated a 15x15-mm submental area with the highest fluence tolerated in phase 1 of the trial and used an adjacent site as the control.
After 90 days, the mean papule count was 6.95 for the control site compared with 1 for the laser-treated site. The researchers observed that miniaturization and elimination of hair shafts resulted in decreased inflamed papules. “We know that this works,” Dr. DiGiorgio said.
In another study from investigators at the Naval Medical Center, San Diego, 22 patients with skin types IV, V, and VI who had pseudofolliculitis barbae underwent 5 weekly treatments with a 1,064 nm Nd:YAG laser. Topical anesthesia was not used, and 10 evaluators used a Global Assessment Scale (GAS) to assess treatment success from photos taken at baseline and at 4 weeks. At 4 weeks, 11 patients demonstrated 83% improvement on the GAS (P < .01), the investigators reported.
Laser and energy-based treatments can also be used to treat hidradenitis suppurativa (HS), a chronic condition that affects apocrine gland–bearing skin. “The hypothesized pathogenesis is that it’s an inflammatory disorder of the hair follicle, where the follicle rupture introduces its contents into the surrounding dermis,” Dr. DiGiorgio said. “The skin reacts with a chemotactic response and abscess formation. This results in inflammatory nodules and sterile abscesses, which can lead to sinus tracts and hypertrophic scars and chronic drainage, which can be foul-smelling. This frequently leads to depression and psychological distress for the patients.”
Possible laser and energy-based treatments for HS include follicular destruction with the Nd:YAG laser, the diode laser, the Alexandrite laser, microwave technology, or intense pulsed light, she said. Microwave technology or radiofrequency can be used for sweat gland destruction, while CO2 lasers can be used to debulk tissue, and the ablative fractional CO2 laser can be used to reduce scarring and improve range of motion.
In a prospective, randomized, intraindividual comparative trial conducted at eight centers in France, researchers evaluated the use of a long-pulsed Nd:YAG laser to treat 36 patients with mild to moderate HS; 27 had inguinal disease and 9 had axillary disease. They received four laser treatments at 6-week intervals; laser settings varied depending on the patient skin type.
At 1 month, there was a significant reduction in the number of inflammatory lesions on the areas treated with lasers, compared to the untreated areas, but the difference was not significant at 3 months. There was no significant difference in the number of flares between the treated and untreated sites at 1 or 3 months.
In a separate study, researchers found that the Nd:YAG laser in combination with topical benzoyl peroxide and clindamycin was significantly more effective than topical benzoyl peroxide and clindamycin alone for the treatment of HS in 22 patients with Hurley stage II disease. The patients received monthly treatments for 4 months and were followed up 2 months after the last treatment; the Hidradenitis Suppurativa Area and Severity Index was used to measure treatment response.
Statistically significant improvements were observed in the inguinal and axillary areas but not in the inframammary areas. Most patients (90%) reported less frequent breakouts while 10% reported no change. “In addition, 92% of subjects felt that the use of laser was more effective than other treatments they had tried but 8% stated it was equal to the other treatments they had tried,” said Dr. DiGiorgio, who was not affiliated with the study. “The researchers noted continued improvement with subsequent laser sessions,” she added.
According to 2019 guidelines from the United States and Canadian HS Foundations on the management of HS – in the section on light, laser, and energy sources – an Nd:YAG laser is recommended in patients with Hurley stage II or III disease on the basis of randomized, controlled trials and case series data, and in patients with Hurley stage I disease based on expert consensus. “Other wavelengths that are used for follicular destruction are recommended on the basis of lower-quality evidence,” the recommendations state.
The guidelines also state that CO2 laser excision “is recommended in patients with Hurley stage II or III disease with fibrotic sinus tracts” while “external beam radiation and PDT have a limited role in the management of patients with HS.”
Dr. DiGiorgio reported having no relevant disclosures.
SAN DIEGO – Pilonidal disease – a chronic inflammatory condition that can trigger the formation of cysts and sinuses in the superior portion of the intragluteal cleft or the sacrococcygeal area – remains challenging to manage, but mounting evidence supports the use of lasers to enhance treatment success.
“Draining sinuses or acute abscesses are usually associated with an underlying cyst and associated granulation tissue, fibrosis, and tufts of hair,” Catherine M. DiGiorgio, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “This is why laser hair removal can help with the treatment of these patients.”
The suspected etiology is a foreign body reaction to the entrapped hairs, which are found in the sinuses in about 75% of cases. “The treatment for that is surgery,” said Dr. DiGiorgio, a laser and cosmetic dermatologist in Boston. Laser hair reduction decreases the recurrence of cyst formation and drainage, and is usually covered by insurance, she noted.
Supportive evidence
In a comparative study, French researchers retrospectively reviewed the efficacy of laser hair removal after surgery in reducing recurrence rate of pilonidal cysts, versus surgery alone. Of the 41 study participants, 12 had laser hair removal plus surgery and 29 had surgery alone. The rate of cyst recurrence was significantly lower in the laser hair removal plus surgery group, compared with the surgery only group (8.3% vs. 51.7%, respectively; P < .001).
In another study, researchers from the United Kingdom and The Johns Hopkins Hospital, Baltimore, evaluated the use of the long-pulsed Alexandrite laser in 19 patients with recurrent pilonidal disease who had undergone multiple surgeries.They were treated with the laser for hair removal in the sinus area, requiring 4-12 sessions. The researchers found that 84.2% of patients had a reduction of hair density to less than 5 hairs/cm2, while 15.8% had a reduction of hair density to 5-10 hairs/cm2. They also noted a statistically significant increase in disease-free time in the laser-treated group compared with those treated with surgical management only (P < .01).
Lasers for pseudofolliculitis barbae, HS
Lasers also play a significant role in the treatment of pseudofolliculitis barbae, a chronic, inflammatory disease that primarily affects the bearded area of men with thick hairs, usually those with a darker Fitzpatrick skin type. This can also occur in women, particularly those with polycystic ovary syndrome, Dr. DiGiorgio said.
In people with pseudofolliculitis barbae, the hair follicle is positioned at an acute angle to the skin surface and the sharp end of shaved hair reenters the skin, which results in the formation of pustules, papules, secondary infection, and keloids. Treatment involves a variety of medical therapies including retinoids, benzoyl peroxide, antibiotics, and keratolytics, “but laser hair removal is the best way to get rid of this issue, and results in permanent reduction,” she said. “When treating male patients with laser hair removal in the bearded area, you have to tell them that they won’t be able to grow a beard going forward. Most of them are okay with that.”
A 2002 study, led by E. Victor Ross, MD, of the Naval Medical Center, San Diego, evaluated treatment of pseudofolliculitis barbae in patients with skin types IV, V, and VI with a long-pulsed Nd:YAG laser. For the first phase of the study, the investigators tested epidermal tolerance on the thighs of 37 patients and determined that the laser was safe and effective. For the second phase 2 weeks later, they treated a 15x15-mm submental area with the highest fluence tolerated in phase 1 of the trial and used an adjacent site as the control.
After 90 days, the mean papule count was 6.95 for the control site compared with 1 for the laser-treated site. The researchers observed that miniaturization and elimination of hair shafts resulted in decreased inflamed papules. “We know that this works,” Dr. DiGiorgio said.
In another study from investigators at the Naval Medical Center, San Diego, 22 patients with skin types IV, V, and VI who had pseudofolliculitis barbae underwent 5 weekly treatments with a 1,064 nm Nd:YAG laser. Topical anesthesia was not used, and 10 evaluators used a Global Assessment Scale (GAS) to assess treatment success from photos taken at baseline and at 4 weeks. At 4 weeks, 11 patients demonstrated 83% improvement on the GAS (P < .01), the investigators reported.
Laser and energy-based treatments can also be used to treat hidradenitis suppurativa (HS), a chronic condition that affects apocrine gland–bearing skin. “The hypothesized pathogenesis is that it’s an inflammatory disorder of the hair follicle, where the follicle rupture introduces its contents into the surrounding dermis,” Dr. DiGiorgio said. “The skin reacts with a chemotactic response and abscess formation. This results in inflammatory nodules and sterile abscesses, which can lead to sinus tracts and hypertrophic scars and chronic drainage, which can be foul-smelling. This frequently leads to depression and psychological distress for the patients.”
Possible laser and energy-based treatments for HS include follicular destruction with the Nd:YAG laser, the diode laser, the Alexandrite laser, microwave technology, or intense pulsed light, she said. Microwave technology or radiofrequency can be used for sweat gland destruction, while CO2 lasers can be used to debulk tissue, and the ablative fractional CO2 laser can be used to reduce scarring and improve range of motion.
In a prospective, randomized, intraindividual comparative trial conducted at eight centers in France, researchers evaluated the use of a long-pulsed Nd:YAG laser to treat 36 patients with mild to moderate HS; 27 had inguinal disease and 9 had axillary disease. They received four laser treatments at 6-week intervals; laser settings varied depending on the patient skin type.
At 1 month, there was a significant reduction in the number of inflammatory lesions on the areas treated with lasers, compared to the untreated areas, but the difference was not significant at 3 months. There was no significant difference in the number of flares between the treated and untreated sites at 1 or 3 months.
In a separate study, researchers found that the Nd:YAG laser in combination with topical benzoyl peroxide and clindamycin was significantly more effective than topical benzoyl peroxide and clindamycin alone for the treatment of HS in 22 patients with Hurley stage II disease. The patients received monthly treatments for 4 months and were followed up 2 months after the last treatment; the Hidradenitis Suppurativa Area and Severity Index was used to measure treatment response.
Statistically significant improvements were observed in the inguinal and axillary areas but not in the inframammary areas. Most patients (90%) reported less frequent breakouts while 10% reported no change. “In addition, 92% of subjects felt that the use of laser was more effective than other treatments they had tried but 8% stated it was equal to the other treatments they had tried,” said Dr. DiGiorgio, who was not affiliated with the study. “The researchers noted continued improvement with subsequent laser sessions,” she added.
According to 2019 guidelines from the United States and Canadian HS Foundations on the management of HS – in the section on light, laser, and energy sources – an Nd:YAG laser is recommended in patients with Hurley stage II or III disease on the basis of randomized, controlled trials and case series data, and in patients with Hurley stage I disease based on expert consensus. “Other wavelengths that are used for follicular destruction are recommended on the basis of lower-quality evidence,” the recommendations state.
The guidelines also state that CO2 laser excision “is recommended in patients with Hurley stage II or III disease with fibrotic sinus tracts” while “external beam radiation and PDT have a limited role in the management of patients with HS.”
Dr. DiGiorgio reported having no relevant disclosures.
SAN DIEGO – Pilonidal disease – a chronic inflammatory condition that can trigger the formation of cysts and sinuses in the superior portion of the intragluteal cleft or the sacrococcygeal area – remains challenging to manage, but mounting evidence supports the use of lasers to enhance treatment success.
“Draining sinuses or acute abscesses are usually associated with an underlying cyst and associated granulation tissue, fibrosis, and tufts of hair,” Catherine M. DiGiorgio, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “This is why laser hair removal can help with the treatment of these patients.”
The suspected etiology is a foreign body reaction to the entrapped hairs, which are found in the sinuses in about 75% of cases. “The treatment for that is surgery,” said Dr. DiGiorgio, a laser and cosmetic dermatologist in Boston. Laser hair reduction decreases the recurrence of cyst formation and drainage, and is usually covered by insurance, she noted.
Supportive evidence
In a comparative study, French researchers retrospectively reviewed the efficacy of laser hair removal after surgery in reducing recurrence rate of pilonidal cysts, versus surgery alone. Of the 41 study participants, 12 had laser hair removal plus surgery and 29 had surgery alone. The rate of cyst recurrence was significantly lower in the laser hair removal plus surgery group, compared with the surgery only group (8.3% vs. 51.7%, respectively; P < .001).
In another study, researchers from the United Kingdom and The Johns Hopkins Hospital, Baltimore, evaluated the use of the long-pulsed Alexandrite laser in 19 patients with recurrent pilonidal disease who had undergone multiple surgeries.They were treated with the laser for hair removal in the sinus area, requiring 4-12 sessions. The researchers found that 84.2% of patients had a reduction of hair density to less than 5 hairs/cm2, while 15.8% had a reduction of hair density to 5-10 hairs/cm2. They also noted a statistically significant increase in disease-free time in the laser-treated group compared with those treated with surgical management only (P < .01).
Lasers for pseudofolliculitis barbae, HS
Lasers also play a significant role in the treatment of pseudofolliculitis barbae, a chronic, inflammatory disease that primarily affects the bearded area of men with thick hairs, usually those with a darker Fitzpatrick skin type. This can also occur in women, particularly those with polycystic ovary syndrome, Dr. DiGiorgio said.
In people with pseudofolliculitis barbae, the hair follicle is positioned at an acute angle to the skin surface and the sharp end of shaved hair reenters the skin, which results in the formation of pustules, papules, secondary infection, and keloids. Treatment involves a variety of medical therapies including retinoids, benzoyl peroxide, antibiotics, and keratolytics, “but laser hair removal is the best way to get rid of this issue, and results in permanent reduction,” she said. “When treating male patients with laser hair removal in the bearded area, you have to tell them that they won’t be able to grow a beard going forward. Most of them are okay with that.”
A 2002 study, led by E. Victor Ross, MD, of the Naval Medical Center, San Diego, evaluated treatment of pseudofolliculitis barbae in patients with skin types IV, V, and VI with a long-pulsed Nd:YAG laser. For the first phase of the study, the investigators tested epidermal tolerance on the thighs of 37 patients and determined that the laser was safe and effective. For the second phase 2 weeks later, they treated a 15x15-mm submental area with the highest fluence tolerated in phase 1 of the trial and used an adjacent site as the control.
After 90 days, the mean papule count was 6.95 for the control site compared with 1 for the laser-treated site. The researchers observed that miniaturization and elimination of hair shafts resulted in decreased inflamed papules. “We know that this works,” Dr. DiGiorgio said.
In another study from investigators at the Naval Medical Center, San Diego, 22 patients with skin types IV, V, and VI who had pseudofolliculitis barbae underwent 5 weekly treatments with a 1,064 nm Nd:YAG laser. Topical anesthesia was not used, and 10 evaluators used a Global Assessment Scale (GAS) to assess treatment success from photos taken at baseline and at 4 weeks. At 4 weeks, 11 patients demonstrated 83% improvement on the GAS (P < .01), the investigators reported.
Laser and energy-based treatments can also be used to treat hidradenitis suppurativa (HS), a chronic condition that affects apocrine gland–bearing skin. “The hypothesized pathogenesis is that it’s an inflammatory disorder of the hair follicle, where the follicle rupture introduces its contents into the surrounding dermis,” Dr. DiGiorgio said. “The skin reacts with a chemotactic response and abscess formation. This results in inflammatory nodules and sterile abscesses, which can lead to sinus tracts and hypertrophic scars and chronic drainage, which can be foul-smelling. This frequently leads to depression and psychological distress for the patients.”
Possible laser and energy-based treatments for HS include follicular destruction with the Nd:YAG laser, the diode laser, the Alexandrite laser, microwave technology, or intense pulsed light, she said. Microwave technology or radiofrequency can be used for sweat gland destruction, while CO2 lasers can be used to debulk tissue, and the ablative fractional CO2 laser can be used to reduce scarring and improve range of motion.
In a prospective, randomized, intraindividual comparative trial conducted at eight centers in France, researchers evaluated the use of a long-pulsed Nd:YAG laser to treat 36 patients with mild to moderate HS; 27 had inguinal disease and 9 had axillary disease. They received four laser treatments at 6-week intervals; laser settings varied depending on the patient skin type.
At 1 month, there was a significant reduction in the number of inflammatory lesions on the areas treated with lasers, compared to the untreated areas, but the difference was not significant at 3 months. There was no significant difference in the number of flares between the treated and untreated sites at 1 or 3 months.
In a separate study, researchers found that the Nd:YAG laser in combination with topical benzoyl peroxide and clindamycin was significantly more effective than topical benzoyl peroxide and clindamycin alone for the treatment of HS in 22 patients with Hurley stage II disease. The patients received monthly treatments for 4 months and were followed up 2 months after the last treatment; the Hidradenitis Suppurativa Area and Severity Index was used to measure treatment response.
Statistically significant improvements were observed in the inguinal and axillary areas but not in the inframammary areas. Most patients (90%) reported less frequent breakouts while 10% reported no change. “In addition, 92% of subjects felt that the use of laser was more effective than other treatments they had tried but 8% stated it was equal to the other treatments they had tried,” said Dr. DiGiorgio, who was not affiliated with the study. “The researchers noted continued improvement with subsequent laser sessions,” she added.
According to 2019 guidelines from the United States and Canadian HS Foundations on the management of HS – in the section on light, laser, and energy sources – an Nd:YAG laser is recommended in patients with Hurley stage II or III disease on the basis of randomized, controlled trials and case series data, and in patients with Hurley stage I disease based on expert consensus. “Other wavelengths that are used for follicular destruction are recommended on the basis of lower-quality evidence,” the recommendations state.
The guidelines also state that CO2 laser excision “is recommended in patients with Hurley stage II or III disease with fibrotic sinus tracts” while “external beam radiation and PDT have a limited role in the management of patients with HS.”
Dr. DiGiorgio reported having no relevant disclosures.
AT ASLMS 2022
Fractional lasers appear to treat more than a fraction of skin, expert says
SAN DIEGO – Using the according to Molly Wanner, MD, MBA.
As a case in point, Dr. Wanner discussed the results of a trial of 48 people over aged 60 years with actinic damage, who received ablative fractional laser treatment on one arm and no treatment on the other arm, which served as the control. At 24 months, only two nonmelanoma skin cancers (NMSCs) developed on the treated arms, compared with 26 on the treated arms.
“What I find interesting is that the treated arm did not develop basal cell carcinoma, only squamous cell carcinoma,” she said at the annual meeting of the American Society for Laser Medicine and Surgery. “It appears that this is working through more than just treatment of the AK precursor lesions, for which fractional lasers are cleared for use. It appears to impact both types of NMSCs.”
The ablative fractional laser and other wounding therapies can modulate a response to UV light – a process that naturally diminishes with age, according to Dr. Wanner, a dermatologist at Massachusetts General Hospital’s Dermatology Laser and Cosmetic Center in Boston. “This ability to repair DNA is actually modulated by insulin-like growth factor 1,” she said. “IGF-1 is produced by papillary dermal fibroblasts and communicates with keratinocytes. If keratinocytes are exposed to UV light and there is no IGF-1 around, you get a mutated cell, and that keeps spreading, and you could potentially get a skin cancer.”
On the other hand, she continued, if IGF-1 is injected around the keratinocytes, they are able to respond. “Keratinocytes, which are the most superficial layer of the skin, are really active,” noted Dr. Wanner, who is also an assistant professor of dermatology at Harvard Medical School, Boston. “They’re dividing and replicating, whereas fibroblasts are more non-proliferative and more long-lived. They stick around for a long time. I think of them as the adults in the room, giving these new keratinocytes direction.”
In a review of wounding therapies for the prevention of photocarcinogenesis, she and her coauthors noted that IGF-1 increases nucleotide excision repair of damaged DNA, promotes checkpoint signaling and suppression of DNA synthesis, favors specialized polymerases that are better able to repair DNA damage, and enhances p53-dependent transcriptional responses to DNA damage.
“Older fibroblasts produce less IGF-1 and lead to a situation where keratinocytes can grow unchecked,” she said. “We can use fractional laser to help with this. Fractional laser increases fibroblast production and decreases senescent fibroblasts.”
In a 2017 review on the impact of age and IGF-1 on DNA damage responses in UV-irradiated skin, the authors noted the high levels of IGF-1 in the skin of younger individuals and lower levels in the skin of their older counterparts.
“But once older skin has been treated with either dermabrasion or fractional laser, the levels of IGF-1 are restored to that of a young adult,” Dr. Wanner said. “The restoration of IGF-1 then restores that level of appropriate response to UV light. So, what’s interesting is that fractional lasers treat more than a fraction [of skin]. Fractional lasers were developed to have an easier way to improve wound healing by leaving the skin intact around these columns [of treated skin]. It turns out that treatment of these columns of skin does not just impact the cells in that area. There is a true global effect that’s allowing us to almost normalize skin.”
Dr. Wanner now thinks of fractional lasers as stimulating a laser-cell biology interaction, not just a laser-tissue interaction. “It’s incredible that we can use these photons to not only impact the tissue itself but how the cells actually respond,” she said. “What’s going to be interesting for us in the next few years is to look at how lasers impact our cellular biology. How can we harness it to help our patients?”
She and her colleagues are conducting a trial of different wounding modalities to assess their impact on IGF-1. “Does depth matter? Does density matter? Does the wavelength matter?” she asked. “The bottom line is, it turns out that when the skin looks healthier, it is healthier. Cosmetic treatments can impact medical outcomes.”
Dr. Wanner disclosed that she is a consultant and advisor to Nu Skin. She has also received research funding and equipment from Solta.
SAN DIEGO – Using the according to Molly Wanner, MD, MBA.
As a case in point, Dr. Wanner discussed the results of a trial of 48 people over aged 60 years with actinic damage, who received ablative fractional laser treatment on one arm and no treatment on the other arm, which served as the control. At 24 months, only two nonmelanoma skin cancers (NMSCs) developed on the treated arms, compared with 26 on the treated arms.
“What I find interesting is that the treated arm did not develop basal cell carcinoma, only squamous cell carcinoma,” she said at the annual meeting of the American Society for Laser Medicine and Surgery. “It appears that this is working through more than just treatment of the AK precursor lesions, for which fractional lasers are cleared for use. It appears to impact both types of NMSCs.”
The ablative fractional laser and other wounding therapies can modulate a response to UV light – a process that naturally diminishes with age, according to Dr. Wanner, a dermatologist at Massachusetts General Hospital’s Dermatology Laser and Cosmetic Center in Boston. “This ability to repair DNA is actually modulated by insulin-like growth factor 1,” she said. “IGF-1 is produced by papillary dermal fibroblasts and communicates with keratinocytes. If keratinocytes are exposed to UV light and there is no IGF-1 around, you get a mutated cell, and that keeps spreading, and you could potentially get a skin cancer.”
On the other hand, she continued, if IGF-1 is injected around the keratinocytes, they are able to respond. “Keratinocytes, which are the most superficial layer of the skin, are really active,” noted Dr. Wanner, who is also an assistant professor of dermatology at Harvard Medical School, Boston. “They’re dividing and replicating, whereas fibroblasts are more non-proliferative and more long-lived. They stick around for a long time. I think of them as the adults in the room, giving these new keratinocytes direction.”
In a review of wounding therapies for the prevention of photocarcinogenesis, she and her coauthors noted that IGF-1 increases nucleotide excision repair of damaged DNA, promotes checkpoint signaling and suppression of DNA synthesis, favors specialized polymerases that are better able to repair DNA damage, and enhances p53-dependent transcriptional responses to DNA damage.
“Older fibroblasts produce less IGF-1 and lead to a situation where keratinocytes can grow unchecked,” she said. “We can use fractional laser to help with this. Fractional laser increases fibroblast production and decreases senescent fibroblasts.”
In a 2017 review on the impact of age and IGF-1 on DNA damage responses in UV-irradiated skin, the authors noted the high levels of IGF-1 in the skin of younger individuals and lower levels in the skin of their older counterparts.
“But once older skin has been treated with either dermabrasion or fractional laser, the levels of IGF-1 are restored to that of a young adult,” Dr. Wanner said. “The restoration of IGF-1 then restores that level of appropriate response to UV light. So, what’s interesting is that fractional lasers treat more than a fraction [of skin]. Fractional lasers were developed to have an easier way to improve wound healing by leaving the skin intact around these columns [of treated skin]. It turns out that treatment of these columns of skin does not just impact the cells in that area. There is a true global effect that’s allowing us to almost normalize skin.”
Dr. Wanner now thinks of fractional lasers as stimulating a laser-cell biology interaction, not just a laser-tissue interaction. “It’s incredible that we can use these photons to not only impact the tissue itself but how the cells actually respond,” she said. “What’s going to be interesting for us in the next few years is to look at how lasers impact our cellular biology. How can we harness it to help our patients?”
She and her colleagues are conducting a trial of different wounding modalities to assess their impact on IGF-1. “Does depth matter? Does density matter? Does the wavelength matter?” she asked. “The bottom line is, it turns out that when the skin looks healthier, it is healthier. Cosmetic treatments can impact medical outcomes.”
Dr. Wanner disclosed that she is a consultant and advisor to Nu Skin. She has also received research funding and equipment from Solta.
SAN DIEGO – Using the according to Molly Wanner, MD, MBA.
As a case in point, Dr. Wanner discussed the results of a trial of 48 people over aged 60 years with actinic damage, who received ablative fractional laser treatment on one arm and no treatment on the other arm, which served as the control. At 24 months, only two nonmelanoma skin cancers (NMSCs) developed on the treated arms, compared with 26 on the treated arms.
“What I find interesting is that the treated arm did not develop basal cell carcinoma, only squamous cell carcinoma,” she said at the annual meeting of the American Society for Laser Medicine and Surgery. “It appears that this is working through more than just treatment of the AK precursor lesions, for which fractional lasers are cleared for use. It appears to impact both types of NMSCs.”
The ablative fractional laser and other wounding therapies can modulate a response to UV light – a process that naturally diminishes with age, according to Dr. Wanner, a dermatologist at Massachusetts General Hospital’s Dermatology Laser and Cosmetic Center in Boston. “This ability to repair DNA is actually modulated by insulin-like growth factor 1,” she said. “IGF-1 is produced by papillary dermal fibroblasts and communicates with keratinocytes. If keratinocytes are exposed to UV light and there is no IGF-1 around, you get a mutated cell, and that keeps spreading, and you could potentially get a skin cancer.”
On the other hand, she continued, if IGF-1 is injected around the keratinocytes, they are able to respond. “Keratinocytes, which are the most superficial layer of the skin, are really active,” noted Dr. Wanner, who is also an assistant professor of dermatology at Harvard Medical School, Boston. “They’re dividing and replicating, whereas fibroblasts are more non-proliferative and more long-lived. They stick around for a long time. I think of them as the adults in the room, giving these new keratinocytes direction.”
In a review of wounding therapies for the prevention of photocarcinogenesis, she and her coauthors noted that IGF-1 increases nucleotide excision repair of damaged DNA, promotes checkpoint signaling and suppression of DNA synthesis, favors specialized polymerases that are better able to repair DNA damage, and enhances p53-dependent transcriptional responses to DNA damage.
“Older fibroblasts produce less IGF-1 and lead to a situation where keratinocytes can grow unchecked,” she said. “We can use fractional laser to help with this. Fractional laser increases fibroblast production and decreases senescent fibroblasts.”
In a 2017 review on the impact of age and IGF-1 on DNA damage responses in UV-irradiated skin, the authors noted the high levels of IGF-1 in the skin of younger individuals and lower levels in the skin of their older counterparts.
“But once older skin has been treated with either dermabrasion or fractional laser, the levels of IGF-1 are restored to that of a young adult,” Dr. Wanner said. “The restoration of IGF-1 then restores that level of appropriate response to UV light. So, what’s interesting is that fractional lasers treat more than a fraction [of skin]. Fractional lasers were developed to have an easier way to improve wound healing by leaving the skin intact around these columns [of treated skin]. It turns out that treatment of these columns of skin does not just impact the cells in that area. There is a true global effect that’s allowing us to almost normalize skin.”
Dr. Wanner now thinks of fractional lasers as stimulating a laser-cell biology interaction, not just a laser-tissue interaction. “It’s incredible that we can use these photons to not only impact the tissue itself but how the cells actually respond,” she said. “What’s going to be interesting for us in the next few years is to look at how lasers impact our cellular biology. How can we harness it to help our patients?”
She and her colleagues are conducting a trial of different wounding modalities to assess their impact on IGF-1. “Does depth matter? Does density matter? Does the wavelength matter?” she asked. “The bottom line is, it turns out that when the skin looks healthier, it is healthier. Cosmetic treatments can impact medical outcomes.”
Dr. Wanner disclosed that she is a consultant and advisor to Nu Skin. She has also received research funding and equipment from Solta.
AT ASLMS 2022
Psychological intervention looks promising in Crohn’s disease
SAN DIEGO – A combination of cognitive-behavioral therapy and mindfulness meditation could reduce pain and fatigue from Crohn’s disease, researchers say.
Patients who followed the program not only felt better but were also more often able to show up for work and leisure activities, compared with a control group assigned to a wait list, said Shmuel Odes, MD, a professor of internal medicine at Ben-Gurion University of the Negev in Beersheba, Israel. He presented the finding at Digestive Diseases Week® (DDW) 2022.
Psychological and social factors affect the gut and vice versa, Dr. Odes said. Yet many inflammatory bowel disease clinics overlook psychological interventions.
To address these issues, Dr. Odes and colleagues developed cognitive-behavioral– and mindfulness-based stress reduction (COBMINDEX) training, which can be taught by clinical social workers over the Internet. “The patient learns to relax,” Dr. Odes told MDedge News. “He learns not to fight his condition.”
In a previous paper, published in the journal Inflammatory Bowel Diseases, Dr. Odes and colleagues reported that patients who learned the technique showed improvement on a variety of psychological and quality-of-life measures, accompanied by changes in inflammatory cytokines and cortisol.
In a follow-up analysis presented here, the researchers looked at measures of pain and fatigue and then examined whether these were associated with productivity at work and other daily activities.
The study investigators randomly assigned 72 patients to an intervention group who got COBMINDEX training right away, and another 70 to a control group assigned to a wait list of 12 weeks before they could get the training. At baseline, the two groups were not significantly different in any demographic or clinical variable the researchers could find.
Social workers provided COBMINDEX training for the patients in seven 60-minute session over 12 weeks. Five of the sessions were devoted to cognitive-behavioral therapy and two to mindfulness-based stress reduction. The social workers asked the patients to do exercises at least once a day and report outcomes through an app.
Twelve patients dropped out of the COBMINDEX group and four dropped from the wait-list group because of lack of interest, time constraints, pregnancy, or illness.
The researchers created a composite score with a 0-15 scale (with higher scores indicating greater pain) from three pain items from the Harvey-Bradshaw Index for Crohn’s Disease, the Short Inflammatory Bowel Disease Questionnaire, and the 12-Item Short Form Survey.
To measure fatigue, they used the Functional Assessment of Chronic Illness Therapy-Fatigue, which has a 0-52 scale, with lower scores indicating greater fatigue.
To measure impairment while working and other daily activities, they used the Work Productivity and Activity Impairment Questionnaire: Crohn’s Disease. Scores on this measure are expressed as a percentage, with higher values indicating greater impairment.
Both the COBMINDEX and the wait-list groups improved on all these scales, but the improvements were significantly greater for the COBMINDEX group.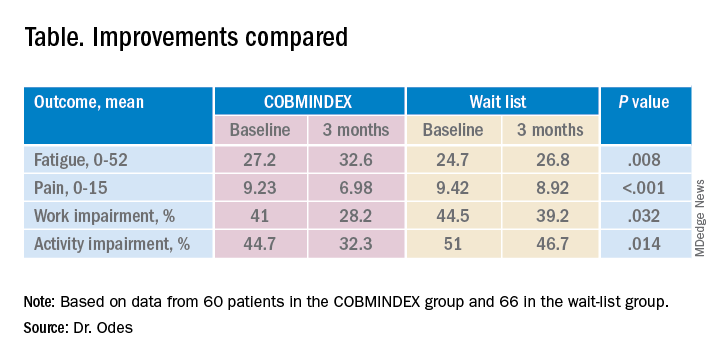
Through statistical analysis, the researchers found that the improvements in pain and fatigue indirectly caused the improvements in work and activity impairment, and that pain and fatigue improvements made independent contributions of similar magnitudes. COBMINDEX did not directly improve work or activity.
Psychological interventions are too often overlooked in Crohn’s disease, said the session comoderator Paul Moayyedi, MD, a professor of gastroenterology at McMaster University in Hamilton, Ont. “We need to realize how important this is to patients and urgently make this available,” he told MDedge.
A variety of interventions are being researched, and this study makes an important contribution, he said. However, he questioned whether people on a wait list can serve as an adequate control. “If you have to wait for something, you tend to have more pain, and you could have less productivity just because of waiting,” he said. “Ideally they should do a randomized trial with a sham intervention, not a wait list.”
Dr. Odes responded that it is very difficult to recruit people to a trial if they only have a 50% chance of getting a real treatment. And he noted that the people on the wait list in this trial did not show any signs of increased symptoms.
Physicians wanting to provide psychological help to their Crohn’s disease patients can refer them to social workers or psychotherapists, Dr. Odes said, but these professionals may lack training for applying cognitive-behavioral therapy and mindfulness-based stress reduction to patients with Crohn’s disease. His team hopes to make an app publicly available soon.
Neither Dr. Odes nor Dr. Moayyedi reported any relevant financial interests. The study was supported by a grant from the Leona M. and Harry B. Helmsley Charitable Trust.
SAN DIEGO – A combination of cognitive-behavioral therapy and mindfulness meditation could reduce pain and fatigue from Crohn’s disease, researchers say.
Patients who followed the program not only felt better but were also more often able to show up for work and leisure activities, compared with a control group assigned to a wait list, said Shmuel Odes, MD, a professor of internal medicine at Ben-Gurion University of the Negev in Beersheba, Israel. He presented the finding at Digestive Diseases Week® (DDW) 2022.
Psychological and social factors affect the gut and vice versa, Dr. Odes said. Yet many inflammatory bowel disease clinics overlook psychological interventions.
To address these issues, Dr. Odes and colleagues developed cognitive-behavioral– and mindfulness-based stress reduction (COBMINDEX) training, which can be taught by clinical social workers over the Internet. “The patient learns to relax,” Dr. Odes told MDedge News. “He learns not to fight his condition.”
In a previous paper, published in the journal Inflammatory Bowel Diseases, Dr. Odes and colleagues reported that patients who learned the technique showed improvement on a variety of psychological and quality-of-life measures, accompanied by changes in inflammatory cytokines and cortisol.
In a follow-up analysis presented here, the researchers looked at measures of pain and fatigue and then examined whether these were associated with productivity at work and other daily activities.
The study investigators randomly assigned 72 patients to an intervention group who got COBMINDEX training right away, and another 70 to a control group assigned to a wait list of 12 weeks before they could get the training. At baseline, the two groups were not significantly different in any demographic or clinical variable the researchers could find.
Social workers provided COBMINDEX training for the patients in seven 60-minute session over 12 weeks. Five of the sessions were devoted to cognitive-behavioral therapy and two to mindfulness-based stress reduction. The social workers asked the patients to do exercises at least once a day and report outcomes through an app.
Twelve patients dropped out of the COBMINDEX group and four dropped from the wait-list group because of lack of interest, time constraints, pregnancy, or illness.
The researchers created a composite score with a 0-15 scale (with higher scores indicating greater pain) from three pain items from the Harvey-Bradshaw Index for Crohn’s Disease, the Short Inflammatory Bowel Disease Questionnaire, and the 12-Item Short Form Survey.
To measure fatigue, they used the Functional Assessment of Chronic Illness Therapy-Fatigue, which has a 0-52 scale, with lower scores indicating greater fatigue.
To measure impairment while working and other daily activities, they used the Work Productivity and Activity Impairment Questionnaire: Crohn’s Disease. Scores on this measure are expressed as a percentage, with higher values indicating greater impairment.
Both the COBMINDEX and the wait-list groups improved on all these scales, but the improvements were significantly greater for the COBMINDEX group.
Through statistical analysis, the researchers found that the improvements in pain and fatigue indirectly caused the improvements in work and activity impairment, and that pain and fatigue improvements made independent contributions of similar magnitudes. COBMINDEX did not directly improve work or activity.
Psychological interventions are too often overlooked in Crohn’s disease, said the session comoderator Paul Moayyedi, MD, a professor of gastroenterology at McMaster University in Hamilton, Ont. “We need to realize how important this is to patients and urgently make this available,” he told MDedge.
A variety of interventions are being researched, and this study makes an important contribution, he said. However, he questioned whether people on a wait list can serve as an adequate control. “If you have to wait for something, you tend to have more pain, and you could have less productivity just because of waiting,” he said. “Ideally they should do a randomized trial with a sham intervention, not a wait list.”
Dr. Odes responded that it is very difficult to recruit people to a trial if they only have a 50% chance of getting a real treatment. And he noted that the people on the wait list in this trial did not show any signs of increased symptoms.
Physicians wanting to provide psychological help to their Crohn’s disease patients can refer them to social workers or psychotherapists, Dr. Odes said, but these professionals may lack training for applying cognitive-behavioral therapy and mindfulness-based stress reduction to patients with Crohn’s disease. His team hopes to make an app publicly available soon.
Neither Dr. Odes nor Dr. Moayyedi reported any relevant financial interests. The study was supported by a grant from the Leona M. and Harry B. Helmsley Charitable Trust.
SAN DIEGO – A combination of cognitive-behavioral therapy and mindfulness meditation could reduce pain and fatigue from Crohn’s disease, researchers say.
Patients who followed the program not only felt better but were also more often able to show up for work and leisure activities, compared with a control group assigned to a wait list, said Shmuel Odes, MD, a professor of internal medicine at Ben-Gurion University of the Negev in Beersheba, Israel. He presented the finding at Digestive Diseases Week® (DDW) 2022.
Psychological and social factors affect the gut and vice versa, Dr. Odes said. Yet many inflammatory bowel disease clinics overlook psychological interventions.
To address these issues, Dr. Odes and colleagues developed cognitive-behavioral– and mindfulness-based stress reduction (COBMINDEX) training, which can be taught by clinical social workers over the Internet. “The patient learns to relax,” Dr. Odes told MDedge News. “He learns not to fight his condition.”
In a previous paper, published in the journal Inflammatory Bowel Diseases, Dr. Odes and colleagues reported that patients who learned the technique showed improvement on a variety of psychological and quality-of-life measures, accompanied by changes in inflammatory cytokines and cortisol.
In a follow-up analysis presented here, the researchers looked at measures of pain and fatigue and then examined whether these were associated with productivity at work and other daily activities.
The study investigators randomly assigned 72 patients to an intervention group who got COBMINDEX training right away, and another 70 to a control group assigned to a wait list of 12 weeks before they could get the training. At baseline, the two groups were not significantly different in any demographic or clinical variable the researchers could find.
Social workers provided COBMINDEX training for the patients in seven 60-minute session over 12 weeks. Five of the sessions were devoted to cognitive-behavioral therapy and two to mindfulness-based stress reduction. The social workers asked the patients to do exercises at least once a day and report outcomes through an app.
Twelve patients dropped out of the COBMINDEX group and four dropped from the wait-list group because of lack of interest, time constraints, pregnancy, or illness.
The researchers created a composite score with a 0-15 scale (with higher scores indicating greater pain) from three pain items from the Harvey-Bradshaw Index for Crohn’s Disease, the Short Inflammatory Bowel Disease Questionnaire, and the 12-Item Short Form Survey.
To measure fatigue, they used the Functional Assessment of Chronic Illness Therapy-Fatigue, which has a 0-52 scale, with lower scores indicating greater fatigue.
To measure impairment while working and other daily activities, they used the Work Productivity and Activity Impairment Questionnaire: Crohn’s Disease. Scores on this measure are expressed as a percentage, with higher values indicating greater impairment.
Both the COBMINDEX and the wait-list groups improved on all these scales, but the improvements were significantly greater for the COBMINDEX group.
Through statistical analysis, the researchers found that the improvements in pain and fatigue indirectly caused the improvements in work and activity impairment, and that pain and fatigue improvements made independent contributions of similar magnitudes. COBMINDEX did not directly improve work or activity.
Psychological interventions are too often overlooked in Crohn’s disease, said the session comoderator Paul Moayyedi, MD, a professor of gastroenterology at McMaster University in Hamilton, Ont. “We need to realize how important this is to patients and urgently make this available,” he told MDedge.
A variety of interventions are being researched, and this study makes an important contribution, he said. However, he questioned whether people on a wait list can serve as an adequate control. “If you have to wait for something, you tend to have more pain, and you could have less productivity just because of waiting,” he said. “Ideally they should do a randomized trial with a sham intervention, not a wait list.”
Dr. Odes responded that it is very difficult to recruit people to a trial if they only have a 50% chance of getting a real treatment. And he noted that the people on the wait list in this trial did not show any signs of increased symptoms.
Physicians wanting to provide psychological help to their Crohn’s disease patients can refer them to social workers or psychotherapists, Dr. Odes said, but these professionals may lack training for applying cognitive-behavioral therapy and mindfulness-based stress reduction to patients with Crohn’s disease. His team hopes to make an app publicly available soon.
Neither Dr. Odes nor Dr. Moayyedi reported any relevant financial interests. The study was supported by a grant from the Leona M. and Harry B. Helmsley Charitable Trust.
AT DDW 2022
Medical trauma an under-recognized trigger for PTSD
NEW ORLEANS – Recent studies have confirmed that posttraumatic stress disorder can be triggered by health-related stress such as stints in the ICU and life-threatening medical emergencies, but most psychiatrists may not be aware of the latest research, according to an expert in mental trauma.
“This is true among children as well as adults, but it is not generally appreciated by psychiatrists and not at all by non-physicians,” said Charles B. Nemeroff, MD, PhD, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin’s Dell Medical School, in a presentation at the annual meeting of the American Psychiatric Association. “It’s something that we all need to educate our colleagues about.”

As Dr. Nemeroff noted in a wide-ranging discussion about the latest trends in PTSD diagnosis and treatment, the DSM-5 doesn’t yet mention medical trauma in its definition of PTSD but refers more vaguely to triggering events that involve “actual or threatened death, serious injury, or sexual violence.”
However, multiple recent studies have linked medical trauma to PTSD. A 2019 study in Intensive Care Medicine found that 25% of 99 patients who were treated for emergency respiratory or cardiovascular crises showed PTSD symptoms at 6 months, and the percentage of childhood cancer survivors with PTSD was estimated at as high as 22%, according to research published in Frontiers in Psychology.In 2013, a meta-analysis suggested that 23% of stroke survivors have PTSD symptoms within 1 year, and 11% after 1 year.
PTSD is unique
Dr. Nemeroff noted that PTSD is the only diagnosis in the DSM-5 that’s directly linked to an environmental event. Specifically, he said, PTSD is caused by “very unexpected traumatic events that occur outside the normal repertoire of human behavior.”
In response, “most people that have an acute stress disorder response will fundamentally extinguish it and end up returning to the baseline level of functioning,” he said. But those with PTSD do not recover.
Dr. Nemeroff recommends the use of the 20-question self-report tool known as PCL-5. “It’s your friend,” he said. “It takes a few minutes for the patients to fill out while in the front office, and it doesn’t cost anything. Most patients who have PTSD will have a score of 50-55, maybe 60. You’re going to try to get them down to below 30, and you’re going to give this to them every time they come to your office to follow their progress. It works like a charm.”
As for treatment, psychotherapy and medications remain standard, he said, although “PTSD is a tough disorder to treat.”
According to him, brief cognitive behavioral therapy (CBT) – 4-5 sessions – has shown the greatest benefit and highest level of evidence in support when initiated within 4-30 days of trauma. Group therapy may be helpful, while it’s not clear if spiritual support and “psychological first aid” are useful during this time period.
There’s no evidence that medications such as SSRIs and atypical antipsychotics will prevent PTSD from developing; typical antipsychotics are not recommended. Individual or group “debriefing” is highly not recommended, Dr. Nemeroff said, because the experience can re-traumatize patients, as researchers learned after 9/11 when encouraging people to relive their experiences triggered PTSD and heartbreak.
Also not recommended: Benzodiazepines and formal psychotherapy in people without symptoms.
Exposure-based CBT has been proven to be successful, Dr. Nemeroff said, but it must be provided by a trained professional. “Going for a weekend course isn’t sufficient,” he said, and research suggests that group CBT is not as helpfulas individual CBT.
As for medication over the longer term, research supports SNRIs and SSRIs such as sertaline (Zoloft) and paroxetine (Paxil). Dr. Nemeroff is a fan of venlafaxine (Effexor): “It has a wide dose range. I can go from 75 to 150 milligrams at the low end and 450 and even 600 milligrams at the high end. I’ve had some amazing successes.”
In addition, atypical antipsychotics can be helpful in non-responders or psychotic PTSD patients, he said.
Dr. Nemeroff said he’s skeptical of ketamine as a treatment for PTSD, but he’s most hopeful about MDMA-assisted therapy due to “impressive data” regarding PTSD that was released last year. A bid for FDA approval is in the works, he said.
He added that data is promising from trials examining transcranial magnetic stimulationand (in work by his own team) electroconvulsive therapy. Both therapies are worth considering, he said.
Dr. Nemeroff reported multiple disclosures including research/grant support, stock holdings, scientific advisory board service, consulting relationships, board of director service, and patents.
NEW ORLEANS – Recent studies have confirmed that posttraumatic stress disorder can be triggered by health-related stress such as stints in the ICU and life-threatening medical emergencies, but most psychiatrists may not be aware of the latest research, according to an expert in mental trauma.
“This is true among children as well as adults, but it is not generally appreciated by psychiatrists and not at all by non-physicians,” said Charles B. Nemeroff, MD, PhD, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin’s Dell Medical School, in a presentation at the annual meeting of the American Psychiatric Association. “It’s something that we all need to educate our colleagues about.”
As Dr. Nemeroff noted in a wide-ranging discussion about the latest trends in PTSD diagnosis and treatment, the DSM-5 doesn’t yet mention medical trauma in its definition of PTSD but refers more vaguely to triggering events that involve “actual or threatened death, serious injury, or sexual violence.”
However, multiple recent studies have linked medical trauma to PTSD. A 2019 study in Intensive Care Medicine found that 25% of 99 patients who were treated for emergency respiratory or cardiovascular crises showed PTSD symptoms at 6 months, and the percentage of childhood cancer survivors with PTSD was estimated at as high as 22%, according to research published in Frontiers in Psychology.In 2013, a meta-analysis suggested that 23% of stroke survivors have PTSD symptoms within 1 year, and 11% after 1 year.
PTSD is unique
Dr. Nemeroff noted that PTSD is the only diagnosis in the DSM-5 that’s directly linked to an environmental event. Specifically, he said, PTSD is caused by “very unexpected traumatic events that occur outside the normal repertoire of human behavior.”
In response, “most people that have an acute stress disorder response will fundamentally extinguish it and end up returning to the baseline level of functioning,” he said. But those with PTSD do not recover.
Dr. Nemeroff recommends the use of the 20-question self-report tool known as PCL-5. “It’s your friend,” he said. “It takes a few minutes for the patients to fill out while in the front office, and it doesn’t cost anything. Most patients who have PTSD will have a score of 50-55, maybe 60. You’re going to try to get them down to below 30, and you’re going to give this to them every time they come to your office to follow their progress. It works like a charm.”
As for treatment, psychotherapy and medications remain standard, he said, although “PTSD is a tough disorder to treat.”
According to him, brief cognitive behavioral therapy (CBT) – 4-5 sessions – has shown the greatest benefit and highest level of evidence in support when initiated within 4-30 days of trauma. Group therapy may be helpful, while it’s not clear if spiritual support and “psychological first aid” are useful during this time period.
There’s no evidence that medications such as SSRIs and atypical antipsychotics will prevent PTSD from developing; typical antipsychotics are not recommended. Individual or group “debriefing” is highly not recommended, Dr. Nemeroff said, because the experience can re-traumatize patients, as researchers learned after 9/11 when encouraging people to relive their experiences triggered PTSD and heartbreak.
Also not recommended: Benzodiazepines and formal psychotherapy in people without symptoms.
Exposure-based CBT has been proven to be successful, Dr. Nemeroff said, but it must be provided by a trained professional. “Going for a weekend course isn’t sufficient,” he said, and research suggests that group CBT is not as helpfulas individual CBT.
As for medication over the longer term, research supports SNRIs and SSRIs such as sertaline (Zoloft) and paroxetine (Paxil). Dr. Nemeroff is a fan of venlafaxine (Effexor): “It has a wide dose range. I can go from 75 to 150 milligrams at the low end and 450 and even 600 milligrams at the high end. I’ve had some amazing successes.”
In addition, atypical antipsychotics can be helpful in non-responders or psychotic PTSD patients, he said.
Dr. Nemeroff said he’s skeptical of ketamine as a treatment for PTSD, but he’s most hopeful about MDMA-assisted therapy due to “impressive data” regarding PTSD that was released last year. A bid for FDA approval is in the works, he said.
He added that data is promising from trials examining transcranial magnetic stimulationand (in work by his own team) electroconvulsive therapy. Both therapies are worth considering, he said.
Dr. Nemeroff reported multiple disclosures including research/grant support, stock holdings, scientific advisory board service, consulting relationships, board of director service, and patents.
NEW ORLEANS – Recent studies have confirmed that posttraumatic stress disorder can be triggered by health-related stress such as stints in the ICU and life-threatening medical emergencies, but most psychiatrists may not be aware of the latest research, according to an expert in mental trauma.
“This is true among children as well as adults, but it is not generally appreciated by psychiatrists and not at all by non-physicians,” said Charles B. Nemeroff, MD, PhD, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin’s Dell Medical School, in a presentation at the annual meeting of the American Psychiatric Association. “It’s something that we all need to educate our colleagues about.”
As Dr. Nemeroff noted in a wide-ranging discussion about the latest trends in PTSD diagnosis and treatment, the DSM-5 doesn’t yet mention medical trauma in its definition of PTSD but refers more vaguely to triggering events that involve “actual or threatened death, serious injury, or sexual violence.”
However, multiple recent studies have linked medical trauma to PTSD. A 2019 study in Intensive Care Medicine found that 25% of 99 patients who were treated for emergency respiratory or cardiovascular crises showed PTSD symptoms at 6 months, and the percentage of childhood cancer survivors with PTSD was estimated at as high as 22%, according to research published in Frontiers in Psychology.In 2013, a meta-analysis suggested that 23% of stroke survivors have PTSD symptoms within 1 year, and 11% after 1 year.
PTSD is unique
Dr. Nemeroff noted that PTSD is the only diagnosis in the DSM-5 that’s directly linked to an environmental event. Specifically, he said, PTSD is caused by “very unexpected traumatic events that occur outside the normal repertoire of human behavior.”
In response, “most people that have an acute stress disorder response will fundamentally extinguish it and end up returning to the baseline level of functioning,” he said. But those with PTSD do not recover.
Dr. Nemeroff recommends the use of the 20-question self-report tool known as PCL-5. “It’s your friend,” he said. “It takes a few minutes for the patients to fill out while in the front office, and it doesn’t cost anything. Most patients who have PTSD will have a score of 50-55, maybe 60. You’re going to try to get them down to below 30, and you’re going to give this to them every time they come to your office to follow their progress. It works like a charm.”
As for treatment, psychotherapy and medications remain standard, he said, although “PTSD is a tough disorder to treat.”
According to him, brief cognitive behavioral therapy (CBT) – 4-5 sessions – has shown the greatest benefit and highest level of evidence in support when initiated within 4-30 days of trauma. Group therapy may be helpful, while it’s not clear if spiritual support and “psychological first aid” are useful during this time period.
There’s no evidence that medications such as SSRIs and atypical antipsychotics will prevent PTSD from developing; typical antipsychotics are not recommended. Individual or group “debriefing” is highly not recommended, Dr. Nemeroff said, because the experience can re-traumatize patients, as researchers learned after 9/11 when encouraging people to relive their experiences triggered PTSD and heartbreak.
Also not recommended: Benzodiazepines and formal psychotherapy in people without symptoms.
Exposure-based CBT has been proven to be successful, Dr. Nemeroff said, but it must be provided by a trained professional. “Going for a weekend course isn’t sufficient,” he said, and research suggests that group CBT is not as helpfulas individual CBT.
As for medication over the longer term, research supports SNRIs and SSRIs such as sertaline (Zoloft) and paroxetine (Paxil). Dr. Nemeroff is a fan of venlafaxine (Effexor): “It has a wide dose range. I can go from 75 to 150 milligrams at the low end and 450 and even 600 milligrams at the high end. I’ve had some amazing successes.”
In addition, atypical antipsychotics can be helpful in non-responders or psychotic PTSD patients, he said.
Dr. Nemeroff said he’s skeptical of ketamine as a treatment for PTSD, but he’s most hopeful about MDMA-assisted therapy due to “impressive data” regarding PTSD that was released last year. A bid for FDA approval is in the works, he said.
He added that data is promising from trials examining transcranial magnetic stimulationand (in work by his own team) electroconvulsive therapy. Both therapies are worth considering, he said.
Dr. Nemeroff reported multiple disclosures including research/grant support, stock holdings, scientific advisory board service, consulting relationships, board of director service, and patents.
at APA 2022
Telepsychiatry helped maintain standard of schizophrenia care during COVID
, new survey data show.
“Mental health centers rose to the challenge and did what they needed to do for their patients,” study investigator Dawn Velligan, PhD, University of Texas Health Science Center at San Antonio, told this news organization.
“Some decided to put patients on longer-acting injectable formulations. Some centers gave injections outside to make people feel safer,” Dr. Velligan said.
She added that other patients who might not have had transportation, or were too afraid to come in, were switched to oral medications. However, “switching to orals isn’t something that should be done lightly. I would only want patients to switch to orals as a last resort, but you do what you have to do,” Dr. Velligan said.
The findings were presented at the annual meeting of the American Psychiatric Association.
No going back?
When COVID hit, many mental health clinics closed for in-person visits. “This was unprecedented and we wanted to understand how clinics adapted their services and clinical management of patients with schizophrenia” on LAIs, Dr. Velligan said.
She and her colleagues surveyed 35 mental health clinics, with one respondent at each clinic, between October and November 2020.
All 35 clinics reported using telepsychiatry; 15 had been using telepsychiatry before the pandemic, while 20 (57%) began using it after COVID hit.
Across outpatient visit types, telepsychiatry use for noninjection visits rose from 12%-15% before the pandemic to 45%-69% after the pandemic.
In addition, patients were more apt to keep their telehealth visit. The frequency of appointment “no shows” and/or cancellations for telepsychiatry visits decreased by roughly one-third after the pandemic, compared with before the pandemic.
For patients with schizophrenia treated with LAIs, the frequency of telepsychiatry visits increased in 46% of the clinics during the pandemic.
For these patients, management options included switching patients from LAIs to oral antipsychotics in 34% of clinics and switching patients to LAIs with longer injection intervals in 31% of clinics.
Chief barriers to telepsychiatry visits were low reimbursement rate and lack of access to technology/reliable Internet.
Nearly all respondents reported being satisfied with the use of telepsychiatry to support patients with schizophrenia, whether treated with LAIs (94%) or with oral antipsychotics (97%).
Sixty percent of respondents reported no change in medication adherence for patients treated with LAIs since the start of the pandemic, while less than half (43%) reported no change in adherence to oral antipsychotics.
Most respondents (69%) felt that telepsychiatry visits would very likely continue to be used in combination with in-person office visits after the pandemic.
“Telemedicine is here to stay,” Dr. Velligan said.
Moving to a ‘hybrid universe’
Hector Colon-Rivera, MD, University of Pittsburgh Medical Center and president of the APA’s Hispanic Caucus, agrees.

Commenting on the findings, he noted that, because of shifts in care brought on by COVID, psychiatrists had to adopt telemedicine practices. As a result, many “now feel more comfortable” with telehealth visits for medication management and psychotherapy, said Dr. Colon-Rivera, who was not involved with the research.
He added this study is important because it shows that even patients with severe mental illness can be successfully managed with telepsychiatry, and with good adherence.
“Especially for patients with schizophrenia who have access issues, telepsychiatry is really helpful,” Dr. Colon-Rivera said.
“Telepsychiatry is becoming standard. Most clinics are moving to the hybrid universe now by having a telemedicine component and also seeing patients in person. Even places like emergency rooms and psychiatrists who do consults on medical floors are using telepsychiatry as an option,” he added.
Study funding was provided by Alkermes. Dr. Velligan has reported financial relationships with Alkermes, Otsuka, Janssen, and Lyndra. Dr. Colon-Rivera has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new survey data show.
“Mental health centers rose to the challenge and did what they needed to do for their patients,” study investigator Dawn Velligan, PhD, University of Texas Health Science Center at San Antonio, told this news organization.
“Some decided to put patients on longer-acting injectable formulations. Some centers gave injections outside to make people feel safer,” Dr. Velligan said.
She added that other patients who might not have had transportation, or were too afraid to come in, were switched to oral medications. However, “switching to orals isn’t something that should be done lightly. I would only want patients to switch to orals as a last resort, but you do what you have to do,” Dr. Velligan said.
The findings were presented at the annual meeting of the American Psychiatric Association.
No going back?
When COVID hit, many mental health clinics closed for in-person visits. “This was unprecedented and we wanted to understand how clinics adapted their services and clinical management of patients with schizophrenia” on LAIs, Dr. Velligan said.
She and her colleagues surveyed 35 mental health clinics, with one respondent at each clinic, between October and November 2020.
All 35 clinics reported using telepsychiatry; 15 had been using telepsychiatry before the pandemic, while 20 (57%) began using it after COVID hit.
Across outpatient visit types, telepsychiatry use for noninjection visits rose from 12%-15% before the pandemic to 45%-69% after the pandemic.
In addition, patients were more apt to keep their telehealth visit. The frequency of appointment “no shows” and/or cancellations for telepsychiatry visits decreased by roughly one-third after the pandemic, compared with before the pandemic.
For patients with schizophrenia treated with LAIs, the frequency of telepsychiatry visits increased in 46% of the clinics during the pandemic.
For these patients, management options included switching patients from LAIs to oral antipsychotics in 34% of clinics and switching patients to LAIs with longer injection intervals in 31% of clinics.
Chief barriers to telepsychiatry visits were low reimbursement rate and lack of access to technology/reliable Internet.
Nearly all respondents reported being satisfied with the use of telepsychiatry to support patients with schizophrenia, whether treated with LAIs (94%) or with oral antipsychotics (97%).
Sixty percent of respondents reported no change in medication adherence for patients treated with LAIs since the start of the pandemic, while less than half (43%) reported no change in adherence to oral antipsychotics.
Most respondents (69%) felt that telepsychiatry visits would very likely continue to be used in combination with in-person office visits after the pandemic.
“Telemedicine is here to stay,” Dr. Velligan said.
Moving to a ‘hybrid universe’
Hector Colon-Rivera, MD, University of Pittsburgh Medical Center and president of the APA’s Hispanic Caucus, agrees.
Commenting on the findings, he noted that, because of shifts in care brought on by COVID, psychiatrists had to adopt telemedicine practices. As a result, many “now feel more comfortable” with telehealth visits for medication management and psychotherapy, said Dr. Colon-Rivera, who was not involved with the research.
He added this study is important because it shows that even patients with severe mental illness can be successfully managed with telepsychiatry, and with good adherence.
“Especially for patients with schizophrenia who have access issues, telepsychiatry is really helpful,” Dr. Colon-Rivera said.
“Telepsychiatry is becoming standard. Most clinics are moving to the hybrid universe now by having a telemedicine component and also seeing patients in person. Even places like emergency rooms and psychiatrists who do consults on medical floors are using telepsychiatry as an option,” he added.
Study funding was provided by Alkermes. Dr. Velligan has reported financial relationships with Alkermes, Otsuka, Janssen, and Lyndra. Dr. Colon-Rivera has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new survey data show.
“Mental health centers rose to the challenge and did what they needed to do for their patients,” study investigator Dawn Velligan, PhD, University of Texas Health Science Center at San Antonio, told this news organization.
“Some decided to put patients on longer-acting injectable formulations. Some centers gave injections outside to make people feel safer,” Dr. Velligan said.
She added that other patients who might not have had transportation, or were too afraid to come in, were switched to oral medications. However, “switching to orals isn’t something that should be done lightly. I would only want patients to switch to orals as a last resort, but you do what you have to do,” Dr. Velligan said.
The findings were presented at the annual meeting of the American Psychiatric Association.
No going back?
When COVID hit, many mental health clinics closed for in-person visits. “This was unprecedented and we wanted to understand how clinics adapted their services and clinical management of patients with schizophrenia” on LAIs, Dr. Velligan said.
She and her colleagues surveyed 35 mental health clinics, with one respondent at each clinic, between October and November 2020.
All 35 clinics reported using telepsychiatry; 15 had been using telepsychiatry before the pandemic, while 20 (57%) began using it after COVID hit.
Across outpatient visit types, telepsychiatry use for noninjection visits rose from 12%-15% before the pandemic to 45%-69% after the pandemic.
In addition, patients were more apt to keep their telehealth visit. The frequency of appointment “no shows” and/or cancellations for telepsychiatry visits decreased by roughly one-third after the pandemic, compared with before the pandemic.
For patients with schizophrenia treated with LAIs, the frequency of telepsychiatry visits increased in 46% of the clinics during the pandemic.
For these patients, management options included switching patients from LAIs to oral antipsychotics in 34% of clinics and switching patients to LAIs with longer injection intervals in 31% of clinics.
Chief barriers to telepsychiatry visits were low reimbursement rate and lack of access to technology/reliable Internet.
Nearly all respondents reported being satisfied with the use of telepsychiatry to support patients with schizophrenia, whether treated with LAIs (94%) or with oral antipsychotics (97%).
Sixty percent of respondents reported no change in medication adherence for patients treated with LAIs since the start of the pandemic, while less than half (43%) reported no change in adherence to oral antipsychotics.
Most respondents (69%) felt that telepsychiatry visits would very likely continue to be used in combination with in-person office visits after the pandemic.
“Telemedicine is here to stay,” Dr. Velligan said.
Moving to a ‘hybrid universe’
Hector Colon-Rivera, MD, University of Pittsburgh Medical Center and president of the APA’s Hispanic Caucus, agrees.
Commenting on the findings, he noted that, because of shifts in care brought on by COVID, psychiatrists had to adopt telemedicine practices. As a result, many “now feel more comfortable” with telehealth visits for medication management and psychotherapy, said Dr. Colon-Rivera, who was not involved with the research.
He added this study is important because it shows that even patients with severe mental illness can be successfully managed with telepsychiatry, and with good adherence.
“Especially for patients with schizophrenia who have access issues, telepsychiatry is really helpful,” Dr. Colon-Rivera said.
“Telepsychiatry is becoming standard. Most clinics are moving to the hybrid universe now by having a telemedicine component and also seeing patients in person. Even places like emergency rooms and psychiatrists who do consults on medical floors are using telepsychiatry as an option,” he added.
Study funding was provided by Alkermes. Dr. Velligan has reported financial relationships with Alkermes, Otsuka, Janssen, and Lyndra. Dr. Colon-Rivera has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM APA 2022
Race-, ethnicity-based clinical guidelines miss the mark: Study
SAN DIEGO – Race-based recommendations and clinical algorithms may be doing more harm than good, according to a systematic review of databases and guidelines.
The study found examples of screening recommendations based on race or ethnicity that were likely misleading since these are social constructs that don’t reflect a patient’s individual risk, said Shazia Siddique, MD, who presented the study at the annual Digestive Disease Week® (DDW). “Historically, we’ve made so many clinical decisions based on somebody’s race and ethnicity. We walk into a room, we don’t even ask people which racial or ethnic category they identify with. We just look at them and we say, ‘Their skin color looks black, and therefore we’re going to apply a different equation to them.’ ”

However, a patient’s risks and unique health circumstances are much more complicated than that. They may be related to genetics, or environmental exposures, or level of access to quality health care. Race can often be inappropriately used as a stand-in for these and other factors, she explained.
“These [racial] categories are truly a social construct. It’s becoming very problematic that people are literally making decisions based on somebody’s skin color. That’s just not what the science supports. If there are specific genes or environmental factors, or differences in access to health care that then impact outcomes for certain racial or ethnic groups, we need to figure out what those are,” said Dr. Siddique, who is an assistant professor of medicine at the University of Pennsylvania, Philadelphia.
Those messages are still entrenched in medical education. “I graduated medical school in 2012, and it was taught to me to use race and ethnicity in clinical decision-making. We need to start in medical education to shift the way that we’re thinking. On the research side, we really need to think about how we can replace or remove race and ethnicity and understand the consequences of that, so that over time we can make a shift,” said Dr. Siddique.
For example, Dr. Siddique discussed recommendations that suggest Asian heritage as a risk factor for hepatitis B screening, but that’s not a good factor to consider: “People were saying that Asians should be screened at an earlier age, but it’s really people that were born and raised in Asian countries where it’s endemic or they may have gotten it from their mothers at birth. It’s a marker for how long you have had the disease and how much virus is in your bloodstream. It’s not because you’re Asian. If you’re born and raised in the United States, and you don’t have any of those risk factors, you shouldn’t be treated differently based on your identified racial and ethnic group,” said Dr. Siddique.
These questions have become even more important in recent years because of patients with multiracial identifies and other considerations. “Now the proxy for which race was being used is even messier,” said Dr. Siddique.
So, how should physicians think about assessing a patient’s personalized risks? The key, said Dr. Siddique, is to look at each patient’s individual factors, such as health care access, environmental exposures from jobs or living conditions, or the country they emigrated from if they weren’t born in the United States. “Disease prevalences are different in different areas, and that changes your index of suspicion,” she said.
And when considering current guidelines that incorporate race or ethnicity, she recommends viewing them skeptically: “If there is a current algorithm in your health system or in a guideline that you’re reading that says you should be making a change based on race and ethnicity, you should look at that with a close eye and say, “What do I think it’s being used as a proxy for, and how can I elicit that from my patient?’ ”
The issues raised by Dr. Siddique’s study are important, but there also could be concerns in taking them too far, according to Gary Falk, MD, a professor of medicine at the University of Pennsylvania who comoderated the session where Dr. Siddique presented. He was not involved in the study, but was listed on Dr. Siddique’s acknowledgement slide.
Dr. Falk coauthored Barrett’s esophagus guidelines in 2016 that incorporated White race as a risk factor.
“There are certain clear ethnic factors or country of origin factors that impact one’s risk for cancer, and there are certain diseases that are more common in certain ethnic groups. I think that if we homogenize everybody, we may potentially hurt some people in the effort to be inclusive. That’s my only concern. I think it’s totally correct that we have to get out of our comfort zone, but I hate to see us reach too far on the other end, and homogenize things to the point that people who have increased risk are not being recognized for that reason,” said Dr. Falk.
He acknowledged that White race as a risk for Barrett’s is not easy to define given the uncertainty of the genetic risk, for example, in patients with mixed heritage. “This is all very provocative. We have to think about it carefully,” said Dr. Falk.
Dr. Siddique and Dr. Falk have no relevant financial disclosures.
SAN DIEGO – Race-based recommendations and clinical algorithms may be doing more harm than good, according to a systematic review of databases and guidelines.
The study found examples of screening recommendations based on race or ethnicity that were likely misleading since these are social constructs that don’t reflect a patient’s individual risk, said Shazia Siddique, MD, who presented the study at the annual Digestive Disease Week® (DDW). “Historically, we’ve made so many clinical decisions based on somebody’s race and ethnicity. We walk into a room, we don’t even ask people which racial or ethnic category they identify with. We just look at them and we say, ‘Their skin color looks black, and therefore we’re going to apply a different equation to them.’ ”
However, a patient’s risks and unique health circumstances are much more complicated than that. They may be related to genetics, or environmental exposures, or level of access to quality health care. Race can often be inappropriately used as a stand-in for these and other factors, she explained.
“These [racial] categories are truly a social construct. It’s becoming very problematic that people are literally making decisions based on somebody’s skin color. That’s just not what the science supports. If there are specific genes or environmental factors, or differences in access to health care that then impact outcomes for certain racial or ethnic groups, we need to figure out what those are,” said Dr. Siddique, who is an assistant professor of medicine at the University of Pennsylvania, Philadelphia.
Those messages are still entrenched in medical education. “I graduated medical school in 2012, and it was taught to me to use race and ethnicity in clinical decision-making. We need to start in medical education to shift the way that we’re thinking. On the research side, we really need to think about how we can replace or remove race and ethnicity and understand the consequences of that, so that over time we can make a shift,” said Dr. Siddique.
For example, Dr. Siddique discussed recommendations that suggest Asian heritage as a risk factor for hepatitis B screening, but that’s not a good factor to consider: “People were saying that Asians should be screened at an earlier age, but it’s really people that were born and raised in Asian countries where it’s endemic or they may have gotten it from their mothers at birth. It’s a marker for how long you have had the disease and how much virus is in your bloodstream. It’s not because you’re Asian. If you’re born and raised in the United States, and you don’t have any of those risk factors, you shouldn’t be treated differently based on your identified racial and ethnic group,” said Dr. Siddique.
These questions have become even more important in recent years because of patients with multiracial identifies and other considerations. “Now the proxy for which race was being used is even messier,” said Dr. Siddique.
So, how should physicians think about assessing a patient’s personalized risks? The key, said Dr. Siddique, is to look at each patient’s individual factors, such as health care access, environmental exposures from jobs or living conditions, or the country they emigrated from if they weren’t born in the United States. “Disease prevalences are different in different areas, and that changes your index of suspicion,” she said.
And when considering current guidelines that incorporate race or ethnicity, she recommends viewing them skeptically: “If there is a current algorithm in your health system or in a guideline that you’re reading that says you should be making a change based on race and ethnicity, you should look at that with a close eye and say, “What do I think it’s being used as a proxy for, and how can I elicit that from my patient?’ ”
The issues raised by Dr. Siddique’s study are important, but there also could be concerns in taking them too far, according to Gary Falk, MD, a professor of medicine at the University of Pennsylvania who comoderated the session where Dr. Siddique presented. He was not involved in the study, but was listed on Dr. Siddique’s acknowledgement slide.
Dr. Falk coauthored Barrett’s esophagus guidelines in 2016 that incorporated White race as a risk factor.
“There are certain clear ethnic factors or country of origin factors that impact one’s risk for cancer, and there are certain diseases that are more common in certain ethnic groups. I think that if we homogenize everybody, we may potentially hurt some people in the effort to be inclusive. That’s my only concern. I think it’s totally correct that we have to get out of our comfort zone, but I hate to see us reach too far on the other end, and homogenize things to the point that people who have increased risk are not being recognized for that reason,” said Dr. Falk.
He acknowledged that White race as a risk for Barrett’s is not easy to define given the uncertainty of the genetic risk, for example, in patients with mixed heritage. “This is all very provocative. We have to think about it carefully,” said Dr. Falk.
Dr. Siddique and Dr. Falk have no relevant financial disclosures.
SAN DIEGO – Race-based recommendations and clinical algorithms may be doing more harm than good, according to a systematic review of databases and guidelines.
The study found examples of screening recommendations based on race or ethnicity that were likely misleading since these are social constructs that don’t reflect a patient’s individual risk, said Shazia Siddique, MD, who presented the study at the annual Digestive Disease Week® (DDW). “Historically, we’ve made so many clinical decisions based on somebody’s race and ethnicity. We walk into a room, we don’t even ask people which racial or ethnic category they identify with. We just look at them and we say, ‘Their skin color looks black, and therefore we’re going to apply a different equation to them.’ ”
However, a patient’s risks and unique health circumstances are much more complicated than that. They may be related to genetics, or environmental exposures, or level of access to quality health care. Race can often be inappropriately used as a stand-in for these and other factors, she explained.
“These [racial] categories are truly a social construct. It’s becoming very problematic that people are literally making decisions based on somebody’s skin color. That’s just not what the science supports. If there are specific genes or environmental factors, or differences in access to health care that then impact outcomes for certain racial or ethnic groups, we need to figure out what those are,” said Dr. Siddique, who is an assistant professor of medicine at the University of Pennsylvania, Philadelphia.
Those messages are still entrenched in medical education. “I graduated medical school in 2012, and it was taught to me to use race and ethnicity in clinical decision-making. We need to start in medical education to shift the way that we’re thinking. On the research side, we really need to think about how we can replace or remove race and ethnicity and understand the consequences of that, so that over time we can make a shift,” said Dr. Siddique.
For example, Dr. Siddique discussed recommendations that suggest Asian heritage as a risk factor for hepatitis B screening, but that’s not a good factor to consider: “People were saying that Asians should be screened at an earlier age, but it’s really people that were born and raised in Asian countries where it’s endemic or they may have gotten it from their mothers at birth. It’s a marker for how long you have had the disease and how much virus is in your bloodstream. It’s not because you’re Asian. If you’re born and raised in the United States, and you don’t have any of those risk factors, you shouldn’t be treated differently based on your identified racial and ethnic group,” said Dr. Siddique.
These questions have become even more important in recent years because of patients with multiracial identifies and other considerations. “Now the proxy for which race was being used is even messier,” said Dr. Siddique.
So, how should physicians think about assessing a patient’s personalized risks? The key, said Dr. Siddique, is to look at each patient’s individual factors, such as health care access, environmental exposures from jobs or living conditions, or the country they emigrated from if they weren’t born in the United States. “Disease prevalences are different in different areas, and that changes your index of suspicion,” she said.
And when considering current guidelines that incorporate race or ethnicity, she recommends viewing them skeptically: “If there is a current algorithm in your health system or in a guideline that you’re reading that says you should be making a change based on race and ethnicity, you should look at that with a close eye and say, “What do I think it’s being used as a proxy for, and how can I elicit that from my patient?’ ”
The issues raised by Dr. Siddique’s study are important, but there also could be concerns in taking them too far, according to Gary Falk, MD, a professor of medicine at the University of Pennsylvania who comoderated the session where Dr. Siddique presented. He was not involved in the study, but was listed on Dr. Siddique’s acknowledgement slide.
Dr. Falk coauthored Barrett’s esophagus guidelines in 2016 that incorporated White race as a risk factor.
“There are certain clear ethnic factors or country of origin factors that impact one’s risk for cancer, and there are certain diseases that are more common in certain ethnic groups. I think that if we homogenize everybody, we may potentially hurt some people in the effort to be inclusive. That’s my only concern. I think it’s totally correct that we have to get out of our comfort zone, but I hate to see us reach too far on the other end, and homogenize things to the point that people who have increased risk are not being recognized for that reason,” said Dr. Falk.
He acknowledged that White race as a risk for Barrett’s is not easy to define given the uncertainty of the genetic risk, for example, in patients with mixed heritage. “This is all very provocative. We have to think about it carefully,” said Dr. Falk.
Dr. Siddique and Dr. Falk have no relevant financial disclosures.
AT DDW 2022
Index cholecystectomy reduces readmissions after acute cholangitis
SAN DIEGO – Patients with acute cholangitis are twice as likely to be readmitted within 30 days if they don’t get a cholecystectomy in the same hospital admission for which they get biliary decompression, researchers say.
The readmissions result mostly from sepsis and recurrence of the acute cholangitis, said Ahmad Khan, MD, MS, a gastroenterology fellow at Case Western Reserve University in Cleveland, at Digestive Diseases Week® (DDW) 2022. “These added readmissions can cause a significant burden in terms of costs and extra days of hospitalization in these patients.”
Acute cholangitis in patients without bile duct stents is most often caused by biliary calculi, benign biliary stricture, or malignancy. A gastrointestinal emergency, it requires treatment with biliary decompression followed by cholecystectomy, but the cholecystectomy is considered an elective procedure.
Surgeons may delay it if the patient is very sick, or simply for scheduling reasons, Dr. Khan said. “There are some areas where the surgeons may be too busy,” he said. Or if the patient first presents at the end of the week, some surgeons will send the patient home so they don’t have to operate on the weekend, he said.
To understand the consequences of these decisions, Dr. Khan and his colleagues analyzed data from 2016 to 2018 from the National Readmission Database of the U.S. Agency for Healthcare Research and Quality.
They found that 11% of patients who went home before returning for a cholecystectomy had to be readmitted versus only 5.5% of those who got a cholecystectomy during the same (index) admission as their biliary decompression.
Patients who got cholecystectomies during their index admissions were slightly younger and healthier: Their mean age was 67.29 years and 20.59% had three or more comorbidities at index admission versus 70.77 years of age and 39.80% with three or more comorbidities at index admission for those who got their cholecystectomies later.
The researchers did not find any significant differences in the hospitals’ characteristics, such as being urban or academic, between the two groups.
Mortality was higher for those who received their cholecystectomy after returning home, but they spent less time in the hospital at lower total cost. The differences in outcomes between the index admission and readmission were all statistically significant (P < .01).
This observational study could not determine cause and effect, but it justifies a prospective trial that could more definitely determine which approach results in better outcomes, Dr. Khan said.
That patients are less likely to need readmission if they return home without a gall bladder after treatment for acute cholangitis “makes sense,” said session comoderator Richard Sterling, MD, MSc, chief of hepatology at Virginia Commonwealth University in Richmond.
“Should you do it immediately or can you wait a day or 2? They didn’t really address when during that admission, so we still don’t know the optimal sequence of events.”
If a patient has so many comorbidities that the surgeon and anesthesiologist don’t think the patient could survive a cholecystectomy, then the surgeon might do a cholecystostomy instead, he said.
Dr. Khan said he hopes to delve deeper into the data to determine what factors might have influenced the surgeons’ decisions to delay the cholecystectomy. “I want to see, of the patients who did not get same-admission cholecystectomies, how many had diabetes, how many had coronary artery disease, how many were on blood thinners, and things like that.”
Neither Dr. Khan nor Dr. Sterling reported any relevant financial interests.
SAN DIEGO – Patients with acute cholangitis are twice as likely to be readmitted within 30 days if they don’t get a cholecystectomy in the same hospital admission for which they get biliary decompression, researchers say.
The readmissions result mostly from sepsis and recurrence of the acute cholangitis, said Ahmad Khan, MD, MS, a gastroenterology fellow at Case Western Reserve University in Cleveland, at Digestive Diseases Week® (DDW) 2022. “These added readmissions can cause a significant burden in terms of costs and extra days of hospitalization in these patients.”
Acute cholangitis in patients without bile duct stents is most often caused by biliary calculi, benign biliary stricture, or malignancy. A gastrointestinal emergency, it requires treatment with biliary decompression followed by cholecystectomy, but the cholecystectomy is considered an elective procedure.
Surgeons may delay it if the patient is very sick, or simply for scheduling reasons, Dr. Khan said. “There are some areas where the surgeons may be too busy,” he said. Or if the patient first presents at the end of the week, some surgeons will send the patient home so they don’t have to operate on the weekend, he said.
To understand the consequences of these decisions, Dr. Khan and his colleagues analyzed data from 2016 to 2018 from the National Readmission Database of the U.S. Agency for Healthcare Research and Quality.
They found that 11% of patients who went home before returning for a cholecystectomy had to be readmitted versus only 5.5% of those who got a cholecystectomy during the same (index) admission as their biliary decompression.
Patients who got cholecystectomies during their index admissions were slightly younger and healthier: Their mean age was 67.29 years and 20.59% had three or more comorbidities at index admission versus 70.77 years of age and 39.80% with three or more comorbidities at index admission for those who got their cholecystectomies later.
The researchers did not find any significant differences in the hospitals’ characteristics, such as being urban or academic, between the two groups.
Mortality was higher for those who received their cholecystectomy after returning home, but they spent less time in the hospital at lower total cost. The differences in outcomes between the index admission and readmission were all statistically significant (P < .01).
This observational study could not determine cause and effect, but it justifies a prospective trial that could more definitely determine which approach results in better outcomes, Dr. Khan said.
That patients are less likely to need readmission if they return home without a gall bladder after treatment for acute cholangitis “makes sense,” said session comoderator Richard Sterling, MD, MSc, chief of hepatology at Virginia Commonwealth University in Richmond.
“Should you do it immediately or can you wait a day or 2? They didn’t really address when during that admission, so we still don’t know the optimal sequence of events.”
If a patient has so many comorbidities that the surgeon and anesthesiologist don’t think the patient could survive a cholecystectomy, then the surgeon might do a cholecystostomy instead, he said.
Dr. Khan said he hopes to delve deeper into the data to determine what factors might have influenced the surgeons’ decisions to delay the cholecystectomy. “I want to see, of the patients who did not get same-admission cholecystectomies, how many had diabetes, how many had coronary artery disease, how many were on blood thinners, and things like that.”
Neither Dr. Khan nor Dr. Sterling reported any relevant financial interests.
SAN DIEGO – Patients with acute cholangitis are twice as likely to be readmitted within 30 days if they don’t get a cholecystectomy in the same hospital admission for which they get biliary decompression, researchers say.
The readmissions result mostly from sepsis and recurrence of the acute cholangitis, said Ahmad Khan, MD, MS, a gastroenterology fellow at Case Western Reserve University in Cleveland, at Digestive Diseases Week® (DDW) 2022. “These added readmissions can cause a significant burden in terms of costs and extra days of hospitalization in these patients.”
Acute cholangitis in patients without bile duct stents is most often caused by biliary calculi, benign biliary stricture, or malignancy. A gastrointestinal emergency, it requires treatment with biliary decompression followed by cholecystectomy, but the cholecystectomy is considered an elective procedure.
Surgeons may delay it if the patient is very sick, or simply for scheduling reasons, Dr. Khan said. “There are some areas where the surgeons may be too busy,” he said. Or if the patient first presents at the end of the week, some surgeons will send the patient home so they don’t have to operate on the weekend, he said.
To understand the consequences of these decisions, Dr. Khan and his colleagues analyzed data from 2016 to 2018 from the National Readmission Database of the U.S. Agency for Healthcare Research and Quality.
They found that 11% of patients who went home before returning for a cholecystectomy had to be readmitted versus only 5.5% of those who got a cholecystectomy during the same (index) admission as their biliary decompression.
Patients who got cholecystectomies during their index admissions were slightly younger and healthier: Their mean age was 67.29 years and 20.59% had three or more comorbidities at index admission versus 70.77 years of age and 39.80% with three or more comorbidities at index admission for those who got their cholecystectomies later.
The researchers did not find any significant differences in the hospitals’ characteristics, such as being urban or academic, between the two groups.
Mortality was higher for those who received their cholecystectomy after returning home, but they spent less time in the hospital at lower total cost. The differences in outcomes between the index admission and readmission were all statistically significant (P < .01).
This observational study could not determine cause and effect, but it justifies a prospective trial that could more definitely determine which approach results in better outcomes, Dr. Khan said.
That patients are less likely to need readmission if they return home without a gall bladder after treatment for acute cholangitis “makes sense,” said session comoderator Richard Sterling, MD, MSc, chief of hepatology at Virginia Commonwealth University in Richmond.
“Should you do it immediately or can you wait a day or 2? They didn’t really address when during that admission, so we still don’t know the optimal sequence of events.”
If a patient has so many comorbidities that the surgeon and anesthesiologist don’t think the patient could survive a cholecystectomy, then the surgeon might do a cholecystostomy instead, he said.
Dr. Khan said he hopes to delve deeper into the data to determine what factors might have influenced the surgeons’ decisions to delay the cholecystectomy. “I want to see, of the patients who did not get same-admission cholecystectomies, how many had diabetes, how many had coronary artery disease, how many were on blood thinners, and things like that.”
Neither Dr. Khan nor Dr. Sterling reported any relevant financial interests.
AT DDW 2022
‘Double-edged’ impact of sparring on the brains of MMA fighters
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.

“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.

“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.
“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.
“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.
“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.
“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
FROM APA 2022
Antipsychotic safe, effective for resistant depression in phase 3 trial
, new results from a phase 3 study show.
Already approved by the U.S. Food and Drug Administration to treat adults with schizophrenia and manic, mixed, or depressive episodes of bipolar I disorder, cariprazine is under investigation as an add-on therapy for MDD.
“Even patients who appear to be nonresponsive to standard antidepressant drugs have a very good chance of responding” to cariprazine, lead study author Gary Sachs, MD, associate clinical professor of psychiatry at Massachusetts General Hospital, Boston, told this news organization.

He noted that cariprazine, which is a partial agonist at D2 and D3, as well as 5-HT1A, “is an entirely different class” of drugs.
“It’s worth understanding how to use drugs like cariprazine and expanding our nomenclature; instead of referring to these drugs as atypical antipsychotics, perhaps referring to them as atypical antidepressants makes more sense,” Dr. Sachs said.
The findings were presented at the annual meeting of the American Psychiatric Association.
More options critical
MDD is among the most common psychiatric disorders in the United States. In 2020, an estimated 21 million adults had at least one major depressive episode.
Previous research has shown almost half of patients with MDD do not experience satisfactory results from their current treatment regimen. Therefore, research on more options for patients is critical, Dr. Sachs said.
Results from a previously published placebo-controlled study showed adjunctive treatment with cariprazine at 2-mg to 4.5-mg per day doses was more effective than placebo in improving depressive symptoms in adults with MDD.
The new analysis included patients with MDD and an inadequate response to antidepressant therapy, including selective serotonin reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors (SNRIs), or tricyclic antidepressants. They were recruited from 116 centers in the United States and Europe.
Dr. Sachs noted that a nonresponse to an adequate dose of an antidepressant typically means having less than a 50% improvement over 6 weeks or more.
Researchers randomly assigned the patients to oral cariprazine 1.5 mg/day, cariprazine 3 mg/day, or placebo. All continued to take their antidepressant monotherapy.
The analysis included 757 mostly White participants (mean age, 44.8 years; 73.4% women). All had experienced depression for a “huge” part of their life (average, about 14 years), “not to mention their adult life,” said Dr. Sachs.
In addition, at the start of the study, the participants had been depressed for almost 8 months on average.
The primary endpoint was change at week 6 in Montgomery-Åsberg Depression Rating Scale (MADRS) total score. The mean baseline MADRS total score was 32.5.
Less is sometimes more
Results showed a significantly greater mean reduction in MADRS total score for cariprazine 1.5 mg/day vs. placebo at week 6 (P = .005). Significant differences from placebo were observed as early as week 2 and were maintained at week 4, as well as week 6.
“I can say with great confidence that the 1.5-mg dose met all the standards for efficacy,” Dr. Sachs said.
However, this was not the case for the 3-mg/day dose. Although there was a numerically greater reduction in MADRS total score for this dosage of the drug vs. placebo at week 6, the difference was not statistically significant (P = .07).
At week 6, more patients taking the active drug at 1.5 mg/day than placebo responded to treatment, defined as 50% or greater reduction in MADRS total score (44% vs. 34.9%, respectively; P < .05).
Researchers also assessed scores on the Clinical Global Impressions, finding significantly greater score improvement for both the 1.5-mg/day (P = .0026) and 3-mg/day (P =.0076) groups vs. the placebo group.
Improvement at week 6 in mean total score on the Hamilton Depression Rating Scale (HAM-17) reached nominal significance for cariprazine 1.5 mg/day vs. placebo – but not for 3 mg/day.
The results of this “high-quality” double-blind, randomized, controlled, parallel group study provide “what I regard as proven efficacy,” Dr. Sachs said.
He added that the investigational drug was also relatively safe. “The vast majority of patients tolerated it quite well,” he stressed. In addition, the drop-out rate because of adverse events was “quite low overall.”
The only adverse events (AEs) that occurred with the active treatment at a frequency of 5% or more and double that of placebo were akathisia and nausea. Changes in weight were relatively small, at less than 1 kg, in all treatment groups.
There was one serious AE in each active drug group, one of which was a kidney infection. There were two serious AEs reported in the placebo group, including one patient with multiple sclerosis. There were no deaths.
Dr. Sachs noted an advantage of cariprazine is its long half-life, which makes it more user-friendly because “it forgives you if you miss a dose or two.”
Drug manufacturer AbbVie’s supplemental New Drug Application for cariprazine is currently under review by the FDA for expanded use as adjunctive treatment of MDD. A decision by the agency is expected by the end of this year.
Another potential treatment option
Commenting on the findings, James Murrough, MD, PhD, associate professor of psychiatry and of neuroscience and director of the Depression and Anxiety Center for Discovery and Treatment at the Icahn School of Medicine at Mount Sinai, New York, said he welcomes research into additional treatments for MDD.

“Each medicine in a particular class has a unique pharmacology, so a larger number of medication options may help the clinician find a good match for a particular patient,” said Dr. Murrough, who was not involved with the research.
He noted cariprazine is “somewhat unique” among the dopamine modulators in “preferring interactions with the D3 receptor, one of many types of dopamine receptors.”
Although the study results showed cariprazine was effective in MDD, it “does not entirely break new ground” because previous research has already established the drug’s efficacy as adjunctive therapy for patients with depression not responding to a standard antidepressant, said Dr. Murrough.
He also noted that the lower dose, but not the higher dose, of the drug was found to be significantly beneficial for patients, compared with placebo.
“This is a good reminder that higher doses of a medication are not always better,” Dr. Murrough said.
The study was funded by AbbVie. Dr. Sachs is a full-time employee of Signant Health, which conducted the training and quality control for this study. Dr. Murrough has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new results from a phase 3 study show.
Already approved by the U.S. Food and Drug Administration to treat adults with schizophrenia and manic, mixed, or depressive episodes of bipolar I disorder, cariprazine is under investigation as an add-on therapy for MDD.
“Even patients who appear to be nonresponsive to standard antidepressant drugs have a very good chance of responding” to cariprazine, lead study author Gary Sachs, MD, associate clinical professor of psychiatry at Massachusetts General Hospital, Boston, told this news organization.
He noted that cariprazine, which is a partial agonist at D2 and D3, as well as 5-HT1A, “is an entirely different class” of drugs.
“It’s worth understanding how to use drugs like cariprazine and expanding our nomenclature; instead of referring to these drugs as atypical antipsychotics, perhaps referring to them as atypical antidepressants makes more sense,” Dr. Sachs said.
The findings were presented at the annual meeting of the American Psychiatric Association.
More options critical
MDD is among the most common psychiatric disorders in the United States. In 2020, an estimated 21 million adults had at least one major depressive episode.
Previous research has shown almost half of patients with MDD do not experience satisfactory results from their current treatment regimen. Therefore, research on more options for patients is critical, Dr. Sachs said.
Results from a previously published placebo-controlled study showed adjunctive treatment with cariprazine at 2-mg to 4.5-mg per day doses was more effective than placebo in improving depressive symptoms in adults with MDD.
The new analysis included patients with MDD and an inadequate response to antidepressant therapy, including selective serotonin reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors (SNRIs), or tricyclic antidepressants. They were recruited from 116 centers in the United States and Europe.
Dr. Sachs noted that a nonresponse to an adequate dose of an antidepressant typically means having less than a 50% improvement over 6 weeks or more.
Researchers randomly assigned the patients to oral cariprazine 1.5 mg/day, cariprazine 3 mg/day, or placebo. All continued to take their antidepressant monotherapy.
The analysis included 757 mostly White participants (mean age, 44.8 years; 73.4% women). All had experienced depression for a “huge” part of their life (average, about 14 years), “not to mention their adult life,” said Dr. Sachs.
In addition, at the start of the study, the participants had been depressed for almost 8 months on average.
The primary endpoint was change at week 6 in Montgomery-Åsberg Depression Rating Scale (MADRS) total score. The mean baseline MADRS total score was 32.5.
Less is sometimes more
Results showed a significantly greater mean reduction in MADRS total score for cariprazine 1.5 mg/day vs. placebo at week 6 (P = .005). Significant differences from placebo were observed as early as week 2 and were maintained at week 4, as well as week 6.
“I can say with great confidence that the 1.5-mg dose met all the standards for efficacy,” Dr. Sachs said.
However, this was not the case for the 3-mg/day dose. Although there was a numerically greater reduction in MADRS total score for this dosage of the drug vs. placebo at week 6, the difference was not statistically significant (P = .07).
At week 6, more patients taking the active drug at 1.5 mg/day than placebo responded to treatment, defined as 50% or greater reduction in MADRS total score (44% vs. 34.9%, respectively; P < .05).
Researchers also assessed scores on the Clinical Global Impressions, finding significantly greater score improvement for both the 1.5-mg/day (P = .0026) and 3-mg/day (P =.0076) groups vs. the placebo group.
Improvement at week 6 in mean total score on the Hamilton Depression Rating Scale (HAM-17) reached nominal significance for cariprazine 1.5 mg/day vs. placebo – but not for 3 mg/day.
The results of this “high-quality” double-blind, randomized, controlled, parallel group study provide “what I regard as proven efficacy,” Dr. Sachs said.
He added that the investigational drug was also relatively safe. “The vast majority of patients tolerated it quite well,” he stressed. In addition, the drop-out rate because of adverse events was “quite low overall.”
The only adverse events (AEs) that occurred with the active treatment at a frequency of 5% or more and double that of placebo were akathisia and nausea. Changes in weight were relatively small, at less than 1 kg, in all treatment groups.
There was one serious AE in each active drug group, one of which was a kidney infection. There were two serious AEs reported in the placebo group, including one patient with multiple sclerosis. There were no deaths.
Dr. Sachs noted an advantage of cariprazine is its long half-life, which makes it more user-friendly because “it forgives you if you miss a dose or two.”
Drug manufacturer AbbVie’s supplemental New Drug Application for cariprazine is currently under review by the FDA for expanded use as adjunctive treatment of MDD. A decision by the agency is expected by the end of this year.
Another potential treatment option
Commenting on the findings, James Murrough, MD, PhD, associate professor of psychiatry and of neuroscience and director of the Depression and Anxiety Center for Discovery and Treatment at the Icahn School of Medicine at Mount Sinai, New York, said he welcomes research into additional treatments for MDD.
“Each medicine in a particular class has a unique pharmacology, so a larger number of medication options may help the clinician find a good match for a particular patient,” said Dr. Murrough, who was not involved with the research.
He noted cariprazine is “somewhat unique” among the dopamine modulators in “preferring interactions with the D3 receptor, one of many types of dopamine receptors.”
Although the study results showed cariprazine was effective in MDD, it “does not entirely break new ground” because previous research has already established the drug’s efficacy as adjunctive therapy for patients with depression not responding to a standard antidepressant, said Dr. Murrough.
He also noted that the lower dose, but not the higher dose, of the drug was found to be significantly beneficial for patients, compared with placebo.
“This is a good reminder that higher doses of a medication are not always better,” Dr. Murrough said.
The study was funded by AbbVie. Dr. Sachs is a full-time employee of Signant Health, which conducted the training and quality control for this study. Dr. Murrough has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new results from a phase 3 study show.
Already approved by the U.S. Food and Drug Administration to treat adults with schizophrenia and manic, mixed, or depressive episodes of bipolar I disorder, cariprazine is under investigation as an add-on therapy for MDD.
“Even patients who appear to be nonresponsive to standard antidepressant drugs have a very good chance of responding” to cariprazine, lead study author Gary Sachs, MD, associate clinical professor of psychiatry at Massachusetts General Hospital, Boston, told this news organization.
He noted that cariprazine, which is a partial agonist at D2 and D3, as well as 5-HT1A, “is an entirely different class” of drugs.
“It’s worth understanding how to use drugs like cariprazine and expanding our nomenclature; instead of referring to these drugs as atypical antipsychotics, perhaps referring to them as atypical antidepressants makes more sense,” Dr. Sachs said.
The findings were presented at the annual meeting of the American Psychiatric Association.
More options critical
MDD is among the most common psychiatric disorders in the United States. In 2020, an estimated 21 million adults had at least one major depressive episode.
Previous research has shown almost half of patients with MDD do not experience satisfactory results from their current treatment regimen. Therefore, research on more options for patients is critical, Dr. Sachs said.
Results from a previously published placebo-controlled study showed adjunctive treatment with cariprazine at 2-mg to 4.5-mg per day doses was more effective than placebo in improving depressive symptoms in adults with MDD.
The new analysis included patients with MDD and an inadequate response to antidepressant therapy, including selective serotonin reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors (SNRIs), or tricyclic antidepressants. They were recruited from 116 centers in the United States and Europe.
Dr. Sachs noted that a nonresponse to an adequate dose of an antidepressant typically means having less than a 50% improvement over 6 weeks or more.
Researchers randomly assigned the patients to oral cariprazine 1.5 mg/day, cariprazine 3 mg/day, or placebo. All continued to take their antidepressant monotherapy.
The analysis included 757 mostly White participants (mean age, 44.8 years; 73.4% women). All had experienced depression for a “huge” part of their life (average, about 14 years), “not to mention their adult life,” said Dr. Sachs.
In addition, at the start of the study, the participants had been depressed for almost 8 months on average.
The primary endpoint was change at week 6 in Montgomery-Åsberg Depression Rating Scale (MADRS) total score. The mean baseline MADRS total score was 32.5.
Less is sometimes more
Results showed a significantly greater mean reduction in MADRS total score for cariprazine 1.5 mg/day vs. placebo at week 6 (P = .005). Significant differences from placebo were observed as early as week 2 and were maintained at week 4, as well as week 6.
“I can say with great confidence that the 1.5-mg dose met all the standards for efficacy,” Dr. Sachs said.
However, this was not the case for the 3-mg/day dose. Although there was a numerically greater reduction in MADRS total score for this dosage of the drug vs. placebo at week 6, the difference was not statistically significant (P = .07).
At week 6, more patients taking the active drug at 1.5 mg/day than placebo responded to treatment, defined as 50% or greater reduction in MADRS total score (44% vs. 34.9%, respectively; P < .05).
Researchers also assessed scores on the Clinical Global Impressions, finding significantly greater score improvement for both the 1.5-mg/day (P = .0026) and 3-mg/day (P =.0076) groups vs. the placebo group.
Improvement at week 6 in mean total score on the Hamilton Depression Rating Scale (HAM-17) reached nominal significance for cariprazine 1.5 mg/day vs. placebo – but not for 3 mg/day.
The results of this “high-quality” double-blind, randomized, controlled, parallel group study provide “what I regard as proven efficacy,” Dr. Sachs said.
He added that the investigational drug was also relatively safe. “The vast majority of patients tolerated it quite well,” he stressed. In addition, the drop-out rate because of adverse events was “quite low overall.”
The only adverse events (AEs) that occurred with the active treatment at a frequency of 5% or more and double that of placebo were akathisia and nausea. Changes in weight were relatively small, at less than 1 kg, in all treatment groups.
There was one serious AE in each active drug group, one of which was a kidney infection. There were two serious AEs reported in the placebo group, including one patient with multiple sclerosis. There were no deaths.
Dr. Sachs noted an advantage of cariprazine is its long half-life, which makes it more user-friendly because “it forgives you if you miss a dose or two.”
Drug manufacturer AbbVie’s supplemental New Drug Application for cariprazine is currently under review by the FDA for expanded use as adjunctive treatment of MDD. A decision by the agency is expected by the end of this year.
Another potential treatment option
Commenting on the findings, James Murrough, MD, PhD, associate professor of psychiatry and of neuroscience and director of the Depression and Anxiety Center for Discovery and Treatment at the Icahn School of Medicine at Mount Sinai, New York, said he welcomes research into additional treatments for MDD.
“Each medicine in a particular class has a unique pharmacology, so a larger number of medication options may help the clinician find a good match for a particular patient,” said Dr. Murrough, who was not involved with the research.
He noted cariprazine is “somewhat unique” among the dopamine modulators in “preferring interactions with the D3 receptor, one of many types of dopamine receptors.”
Although the study results showed cariprazine was effective in MDD, it “does not entirely break new ground” because previous research has already established the drug’s efficacy as adjunctive therapy for patients with depression not responding to a standard antidepressant, said Dr. Murrough.
He also noted that the lower dose, but not the higher dose, of the drug was found to be significantly beneficial for patients, compared with placebo.
“This is a good reminder that higher doses of a medication are not always better,” Dr. Murrough said.
The study was funded by AbbVie. Dr. Sachs is a full-time employee of Signant Health, which conducted the training and quality control for this study. Dr. Murrough has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM APA 2022