User login
Suicide in the early months of the pandemic: Unexpected trends
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.

There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
What I want people to know about the Chauvin verdict
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.

There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Head to Toe: Recommendations for Physician Head and Shoe Coverings to Limit COVID-19 Transmission
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
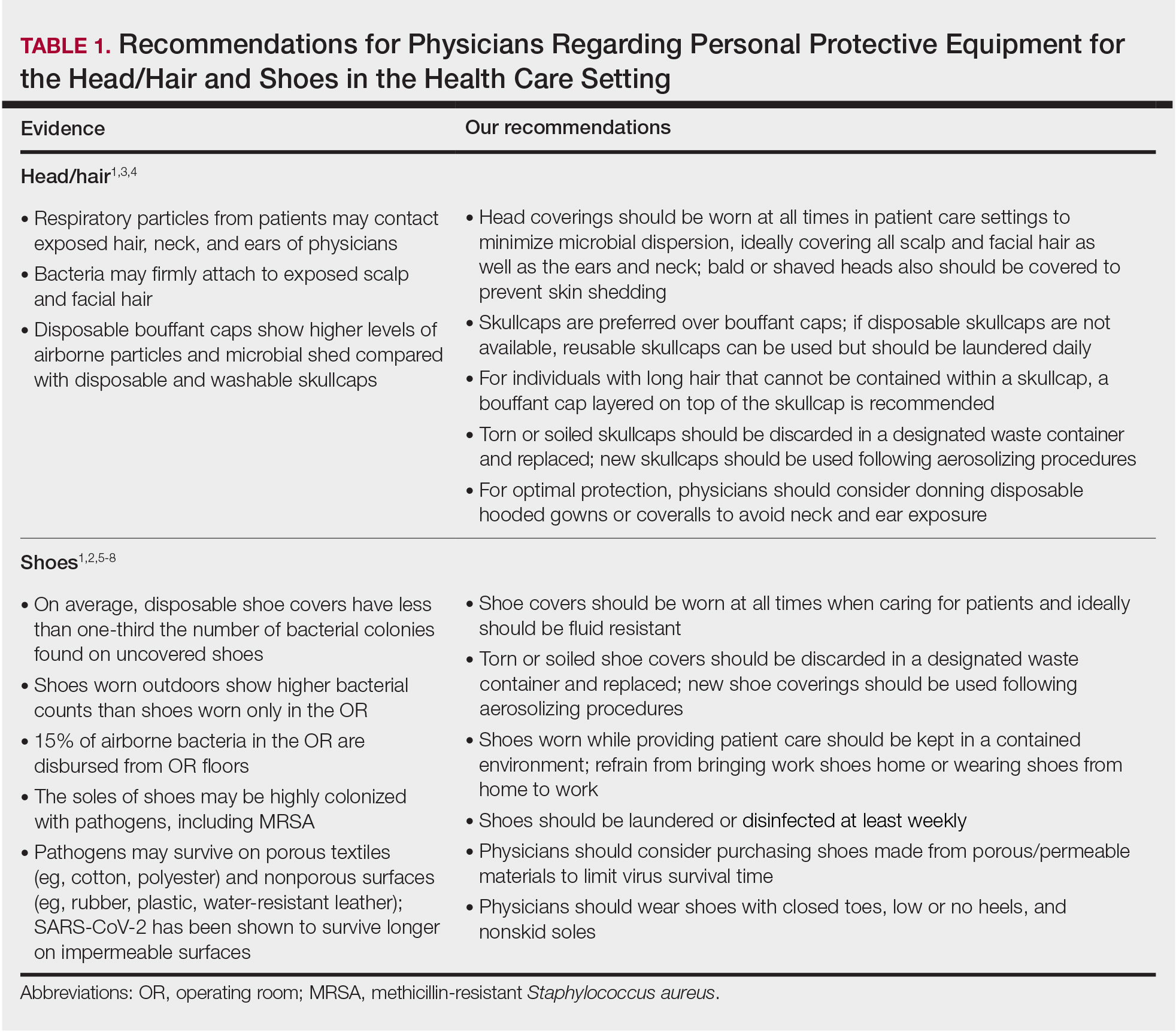
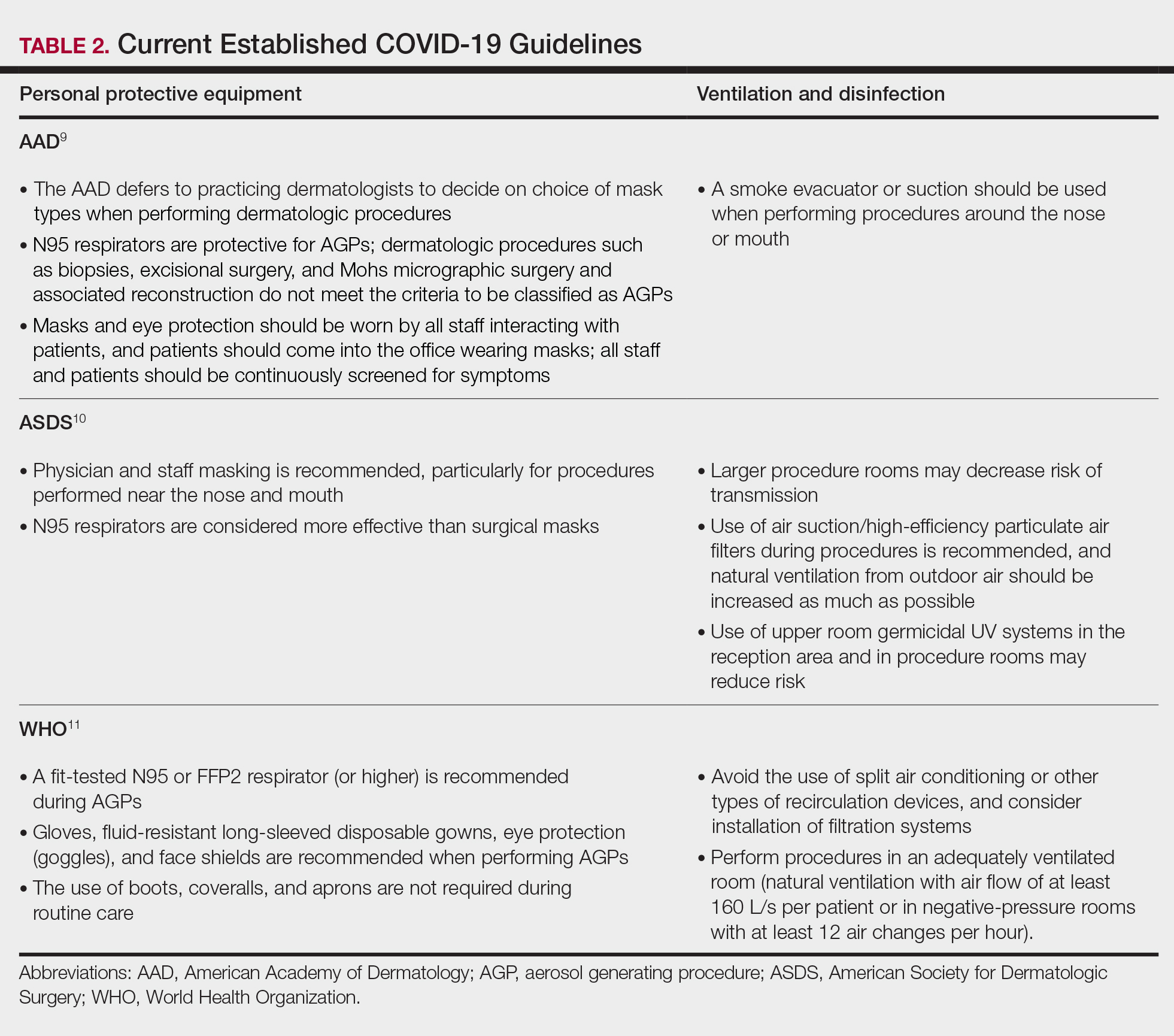
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Practice Points
- Consistent use of personal protective equipment, including masks, face shields, goggles, and gloves, may limit transmission of SARS-CoV-2.
- Hair and shoes also may transmit SARS-CoV-2, but recommendations for hair and shoe coverings to prevent SARS-CoV-2 are lacking.
A Practical Guide to Treatment of Hair Loss Beyond Standard Therapy
When I was a medical student rotating in dermatology, a patient with extensive alopecia looked at my long thick hair and said tearfully, “I just wish I could have hair like yours.”
I smiled, removed my wig, and replied, “You can have hair like mine.”
Determination and Perseverance
I was 2 years old when I was given a diagnosis of alopecia areata. Bald spots on my scalp would come and go for years but were not overly burdensome until I turned 12. At that point, my hair loss escalated despite frequent intralesional injections of triamcinolone; every 2 steps forward were followed by 3 steps backward.
As a freshman in high school, I finally took control of my condition and emotions, shaved my head, and purchased a wig—actions that confronted my hair loss and awoke a determination and perseverance that I did not think I would ever gain while living with this condition. As McGettigan1 wrote in the Journal of the American Academy of Dermatology in 2004, “Being diagnosed with [alopecia areata] does not mean one cannot have a full and meaningful life. By choosing to confront the condition and turn its negative aspects into positive actions, one can succeed in life.”1
As a Provider, Another Perspective
Now, as a dermatology resident, I have the distinct perspective of being patient and provider. Patients often want to know, “Why is this happening?”, “Is my hair going to grow back?”, and “What treatments are available?”
They want to feel supported, understood, and heard.
As health care providers, we must understand that hair loss can result in overwhelming fear, hopelessness, and loss of self-esteem. Although we can give good news and offer helpful treatment options to some patients, there are those for whom medical treatment fails, and we can offer no more than a supportive hand and warm smile.
But can we do even more than that? The answer is: “Yes.”
Management Options
I recommend that all patients with hair loss should receive a copy of the aforementioned McGettigan1 article, “Ahead With No Hair,” which is geared toward patients with alopecia areata but offers inspiring words to any patient struggling to cope with hair loss. Dermatologists also can offer management options for patients with hair loss, including camouflage, wigs, and cosmetic replacement of eyelashes and eyebrows. Of note, several companies offer wigs and brow replacement options for men and children.
Camouflage
We can offer creative and readily available camouflage options for patients with hair loss. For small bald spots and thinning hair on the scalp, keratin hair-building fibers can be extremely useful. This over-the-counter product comes in a variety of natural hair colors, conceals the underlying skin, and adds fullness to hair. The keratin fibers have an innate static charge that allows them to adhere to the hair shaft. Daily application typically is necessary; duration can be maximized if hair spray or other brand-specific bonding spray is used following application of the fibers. A simple online search using the term keratin hair building fibers will reveal many online and in-store options with 4- or 5-star reviews. Most negative reviews pertain to sweating or moisture that causes clumping, but overall this is an easy and affordable option for mild hair loss.
Wigs
For patients hoping to mask moderate or severe hair loss, I recommend wigs, which can be made from synthetic fibers or human hair. In order to effectively guide patients, it is helpful for providers to have some knowledge about the 2 types of wigs. Synthetic wigs are of variable quality, ranging from costume-grade to top-quality products that look and feel like human hair. They are more affordable and often are easier to maintain than human-hair wigs, and hairstyles hold up better after washing. Many synthetic wigs cannot withstand heat from a hot iron and have a slightly shorter lifespan (6–12 months) than human-hair wigs (1–2 years).
Human hair wigs are made of real human hair, so they look and feel natural. These wigs can be made from European, African, Indian, Malaysian, Chinese, or other ethnic hair. Patients can choose the texture of the hair, including silky (smooth), kinky (mimicking natural blow-dried Black hair), and yaki (mimicking relaxed Black hair), as well as the curl pattern (straight, wavy, or curly), length, color, density, and cap construction.
The cap of a wig is what the hair is tied to. The construction of wig caps varies to allow for realistic hair lines as well as security for active use or up-dos. Among the many cap-construction options, the most realistic-appearing are hand-tied monofilament, lace-front, and full-lace wigs, all of which may require tape or glue to keep them in place. Some wig companies offer nonslip so-called “alopecia caps” for patients with no scalp hair. Patients who find their wig irritating to the scalp should consider wearing a nylon wig cap or liner.
Wigs can be purchased in store or online and can be pre-made or custom-built to be tailored to the patient’s specific desires and expectations. The cost depends on the type and quality of hair, cap construction, and length; prices can range from less than $100 to more than $5000.
When choosing a wig, which option—synthetic or human hair—is better for a given patient? Synthetic wigs are rather inexpensive and easy to care for, making them great for new users and those who want to try different styles and colors. Human-hair wigs can be custom-made to match the patient’s natural hair; however, they require extra care to maintain their longevity. Both types of wigs have pros and cons depending on the patient’s budget, time required for maintenance and styling, and needs (Table 1). I encourage patients to have fun with all wig options: Now is the time, I tell them, to try out the cute or daring hair style they have always wanted. The great thing is that if the patient does not like their wig, they can readily change it.
Good-quality wigs are expensive but sometimes are necessary to regain self-confidence and improve one’s quality of life. Advise patients to call their health insurance company to find out if a cranial or scalp prosthesis is covered by their policy. Coverage might require a written prescription for a cranial prosthesis, listing the diagnosis, diagnosis code, and letter of medical necessity. Patients can then purchase the wig online or through a certified distributor depending on their insurance requirements and obtain reimbursement (partial or full coverage). If a wig is not covered by insurance, a cranial prosthesis might be a flexible spending account–eligible expense. For guidance on the reimbursability of wigs, visit the National Alopecia Areata Foundation (NAAF) website (www.naaf.org/AccessHealthcare).
Eyelashes and Eyebrows
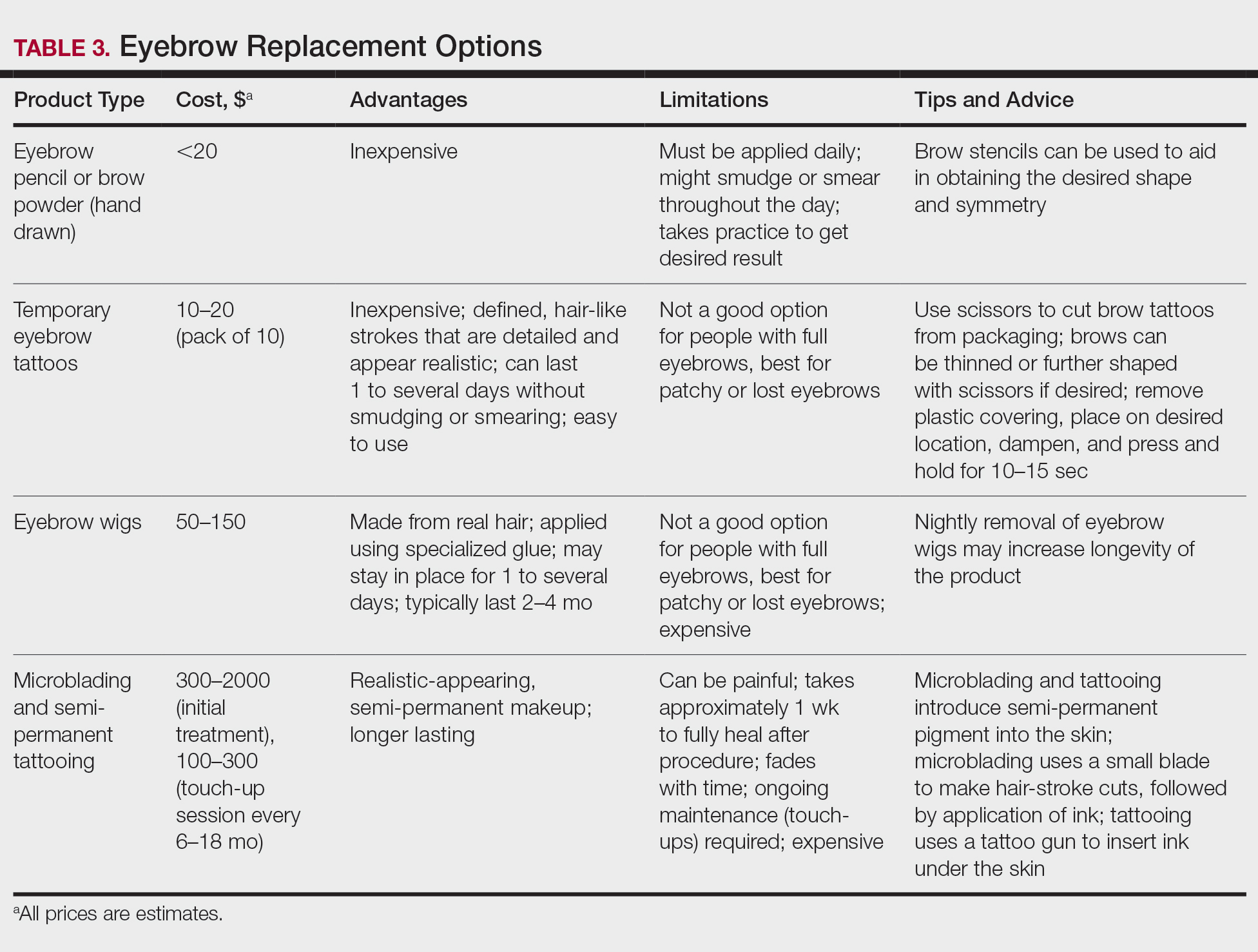
Cosmetic replacement of eyelashes (Table 2) and eyebrows (Table 3) is another treatment option that physicians can offer to hair-loss patients. For patients who desire false eyelashes, strip lashes that are glued to the eyelid margin are easiest to apply (but with caution—do not get glue in the eyes!). There are magnetic lashes, but these require natural lashes on which to adhere them. Eyebrows can be hand-drawn using brow pencils or powders with or without a stencil to maintain symmetry. There are even brow wigs and temporary brow tattoos that can last 1 to several days. Semi-permanent tattooing, including microblading, is an option that has amazing results but can be painful and expensive, often requiring touch-ups every 6 to 18 months.
Resources Abound
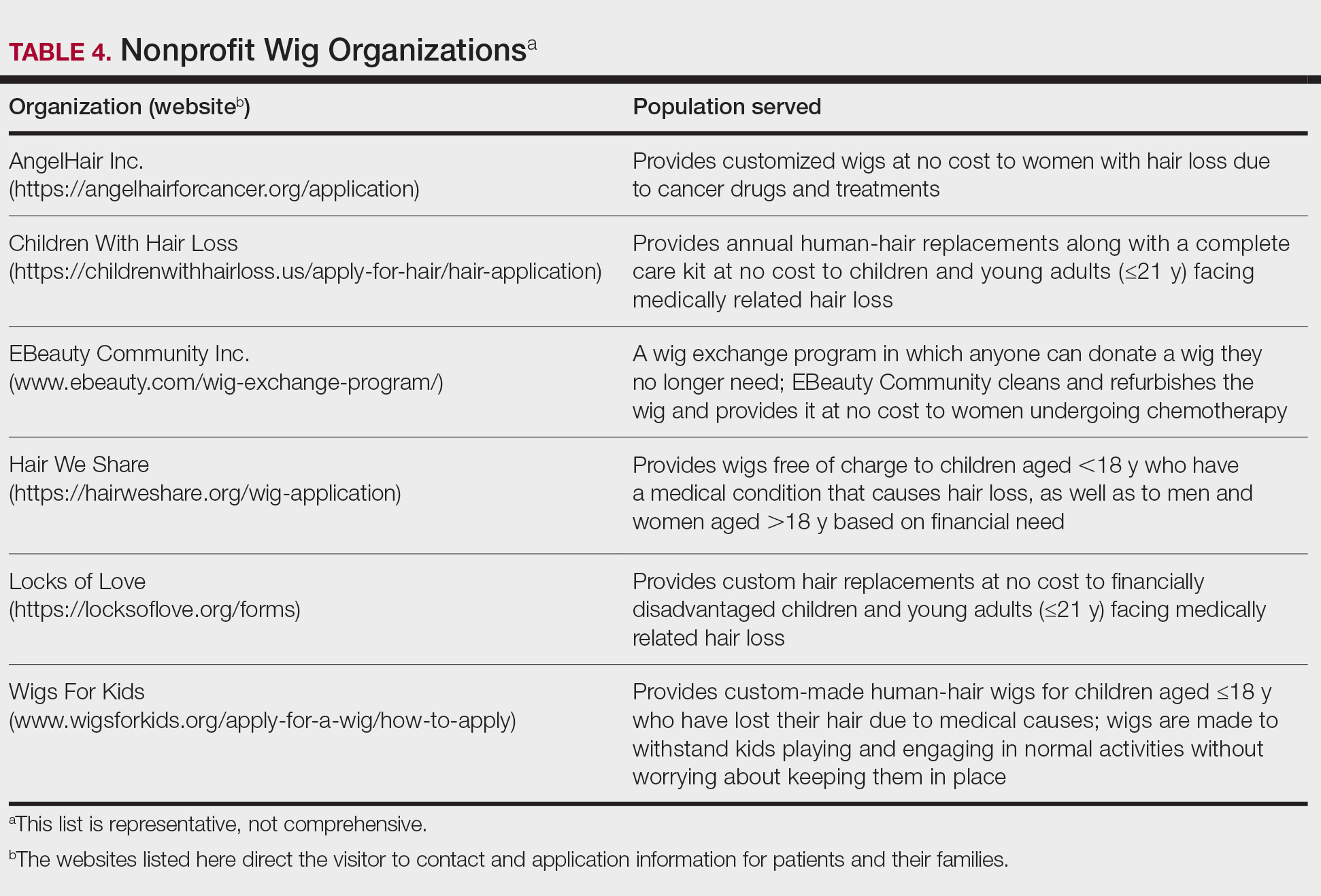
Experiencing and treating hair loss can be overwhelming, but there are countless resources available for patients. The NAAF has utility beyond the concerns of alopecia areata patients; there also is useful information on YouTube and social media, and support groups exist for hair-loss patients. I recommend starting with the NAAF website, which offers many helpful resources and support groups for patients and their families, including tips on applying for insurance reimbursement and drafting an appeal letter. Lastly, several nonprofit organizations serve the hair-replacement needs of children and adults with hair loss (Table 4).
Final Thoughts
My experience as a patient with alopecia has been long and initially was challenging; however, I found the silver lining after choosing to confront my literal and figurative “losses” and move forward—to grow, so to speak. With the use of custom-made human-hair wigs, false strip eyelashes, and a mix of eyebrow replacement options, I have been able to regain my confidence and self-esteem. Now, my goal as a physician—a goal that I hope you will share—is to be knowledgeable about hair-replacement options and provide information and resources to patients to help them feel empowered, brave, and beautiful.
- McGettigan ML. Ahead with no hair. J Am Acad Dermatol. 2004;51(1 suppl):18-19.
When I was a medical student rotating in dermatology, a patient with extensive alopecia looked at my long thick hair and said tearfully, “I just wish I could have hair like yours.”
I smiled, removed my wig, and replied, “You can have hair like mine.”
Determination and Perseverance
I was 2 years old when I was given a diagnosis of alopecia areata. Bald spots on my scalp would come and go for years but were not overly burdensome until I turned 12. At that point, my hair loss escalated despite frequent intralesional injections of triamcinolone; every 2 steps forward were followed by 3 steps backward.
As a freshman in high school, I finally took control of my condition and emotions, shaved my head, and purchased a wig—actions that confronted my hair loss and awoke a determination and perseverance that I did not think I would ever gain while living with this condition. As McGettigan1 wrote in the Journal of the American Academy of Dermatology in 2004, “Being diagnosed with [alopecia areata] does not mean one cannot have a full and meaningful life. By choosing to confront the condition and turn its negative aspects into positive actions, one can succeed in life.”1
As a Provider, Another Perspective
Now, as a dermatology resident, I have the distinct perspective of being patient and provider. Patients often want to know, “Why is this happening?”, “Is my hair going to grow back?”, and “What treatments are available?”
They want to feel supported, understood, and heard.
As health care providers, we must understand that hair loss can result in overwhelming fear, hopelessness, and loss of self-esteem. Although we can give good news and offer helpful treatment options to some patients, there are those for whom medical treatment fails, and we can offer no more than a supportive hand and warm smile.
But can we do even more than that? The answer is: “Yes.”
Management Options
I recommend that all patients with hair loss should receive a copy of the aforementioned McGettigan1 article, “Ahead With No Hair,” which is geared toward patients with alopecia areata but offers inspiring words to any patient struggling to cope with hair loss. Dermatologists also can offer management options for patients with hair loss, including camouflage, wigs, and cosmetic replacement of eyelashes and eyebrows. Of note, several companies offer wigs and brow replacement options for men and children.
Camouflage
We can offer creative and readily available camouflage options for patients with hair loss. For small bald spots and thinning hair on the scalp, keratin hair-building fibers can be extremely useful. This over-the-counter product comes in a variety of natural hair colors, conceals the underlying skin, and adds fullness to hair. The keratin fibers have an innate static charge that allows them to adhere to the hair shaft. Daily application typically is necessary; duration can be maximized if hair spray or other brand-specific bonding spray is used following application of the fibers. A simple online search using the term keratin hair building fibers will reveal many online and in-store options with 4- or 5-star reviews. Most negative reviews pertain to sweating or moisture that causes clumping, but overall this is an easy and affordable option for mild hair loss.
Wigs
For patients hoping to mask moderate or severe hair loss, I recommend wigs, which can be made from synthetic fibers or human hair. In order to effectively guide patients, it is helpful for providers to have some knowledge about the 2 types of wigs. Synthetic wigs are of variable quality, ranging from costume-grade to top-quality products that look and feel like human hair. They are more affordable and often are easier to maintain than human-hair wigs, and hairstyles hold up better after washing. Many synthetic wigs cannot withstand heat from a hot iron and have a slightly shorter lifespan (6–12 months) than human-hair wigs (1–2 years).
Human hair wigs are made of real human hair, so they look and feel natural. These wigs can be made from European, African, Indian, Malaysian, Chinese, or other ethnic hair. Patients can choose the texture of the hair, including silky (smooth), kinky (mimicking natural blow-dried Black hair), and yaki (mimicking relaxed Black hair), as well as the curl pattern (straight, wavy, or curly), length, color, density, and cap construction.
The cap of a wig is what the hair is tied to. The construction of wig caps varies to allow for realistic hair lines as well as security for active use or up-dos. Among the many cap-construction options, the most realistic-appearing are hand-tied monofilament, lace-front, and full-lace wigs, all of which may require tape or glue to keep them in place. Some wig companies offer nonslip so-called “alopecia caps” for patients with no scalp hair. Patients who find their wig irritating to the scalp should consider wearing a nylon wig cap or liner.
Wigs can be purchased in store or online and can be pre-made or custom-built to be tailored to the patient’s specific desires and expectations. The cost depends on the type and quality of hair, cap construction, and length; prices can range from less than $100 to more than $5000.
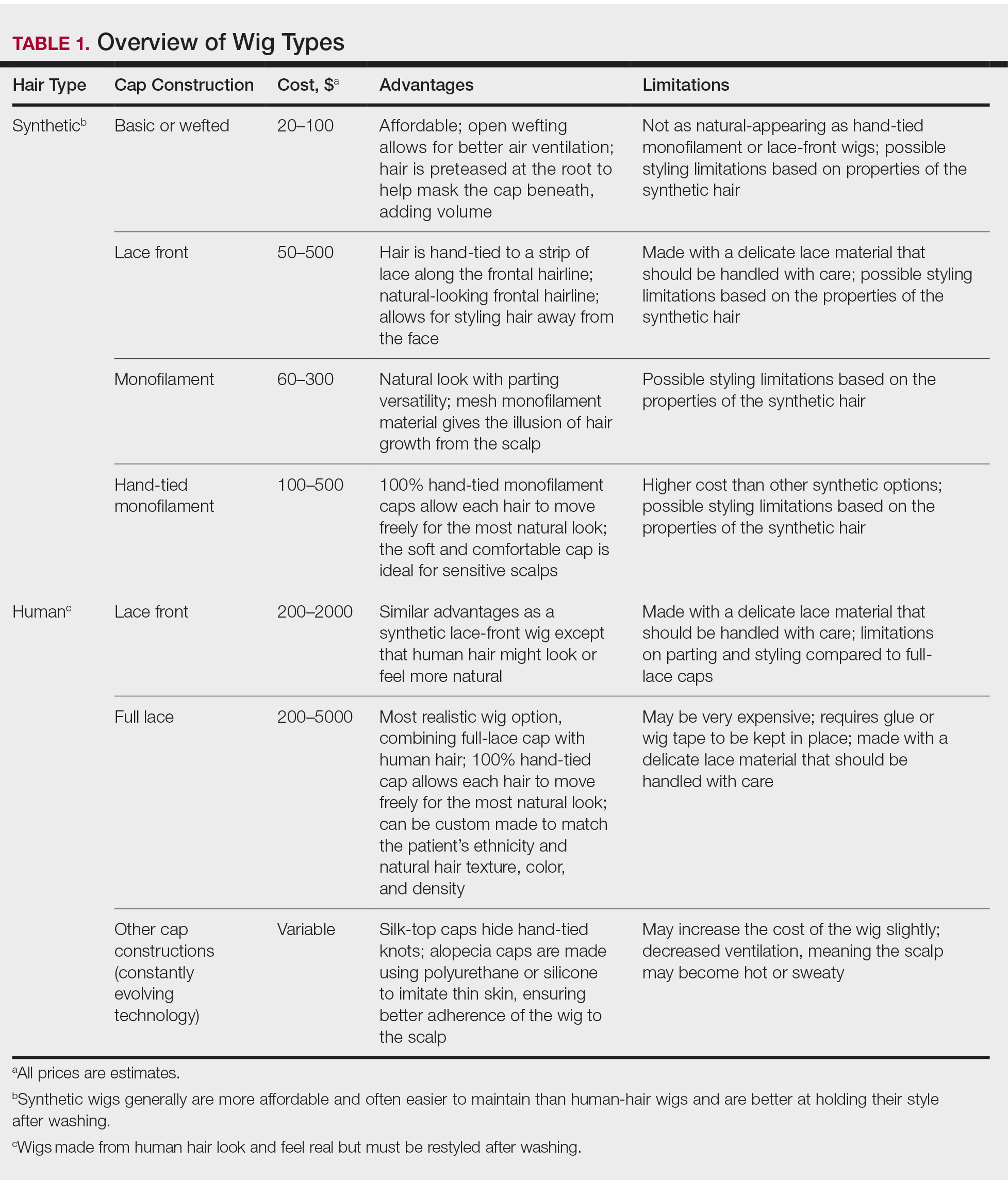
When choosing a wig, which option—synthetic or human hair—is better for a given patient? Synthetic wigs are rather inexpensive and easy to care for, making them great for new users and those who want to try different styles and colors. Human-hair wigs can be custom-made to match the patient’s natural hair; however, they require extra care to maintain their longevity. Both types of wigs have pros and cons depending on the patient’s budget, time required for maintenance and styling, and needs (Table 1). I encourage patients to have fun with all wig options: Now is the time, I tell them, to try out the cute or daring hair style they have always wanted. The great thing is that if the patient does not like their wig, they can readily change it.
Good-quality wigs are expensive but sometimes are necessary to regain self-confidence and improve one’s quality of life. Advise patients to call their health insurance company to find out if a cranial or scalp prosthesis is covered by their policy. Coverage might require a written prescription for a cranial prosthesis, listing the diagnosis, diagnosis code, and letter of medical necessity. Patients can then purchase the wig online or through a certified distributor depending on their insurance requirements and obtain reimbursement (partial or full coverage). If a wig is not covered by insurance, a cranial prosthesis might be a flexible spending account–eligible expense. For guidance on the reimbursability of wigs, visit the National Alopecia Areata Foundation (NAAF) website (www.naaf.org/AccessHealthcare).
Eyelashes and Eyebrows
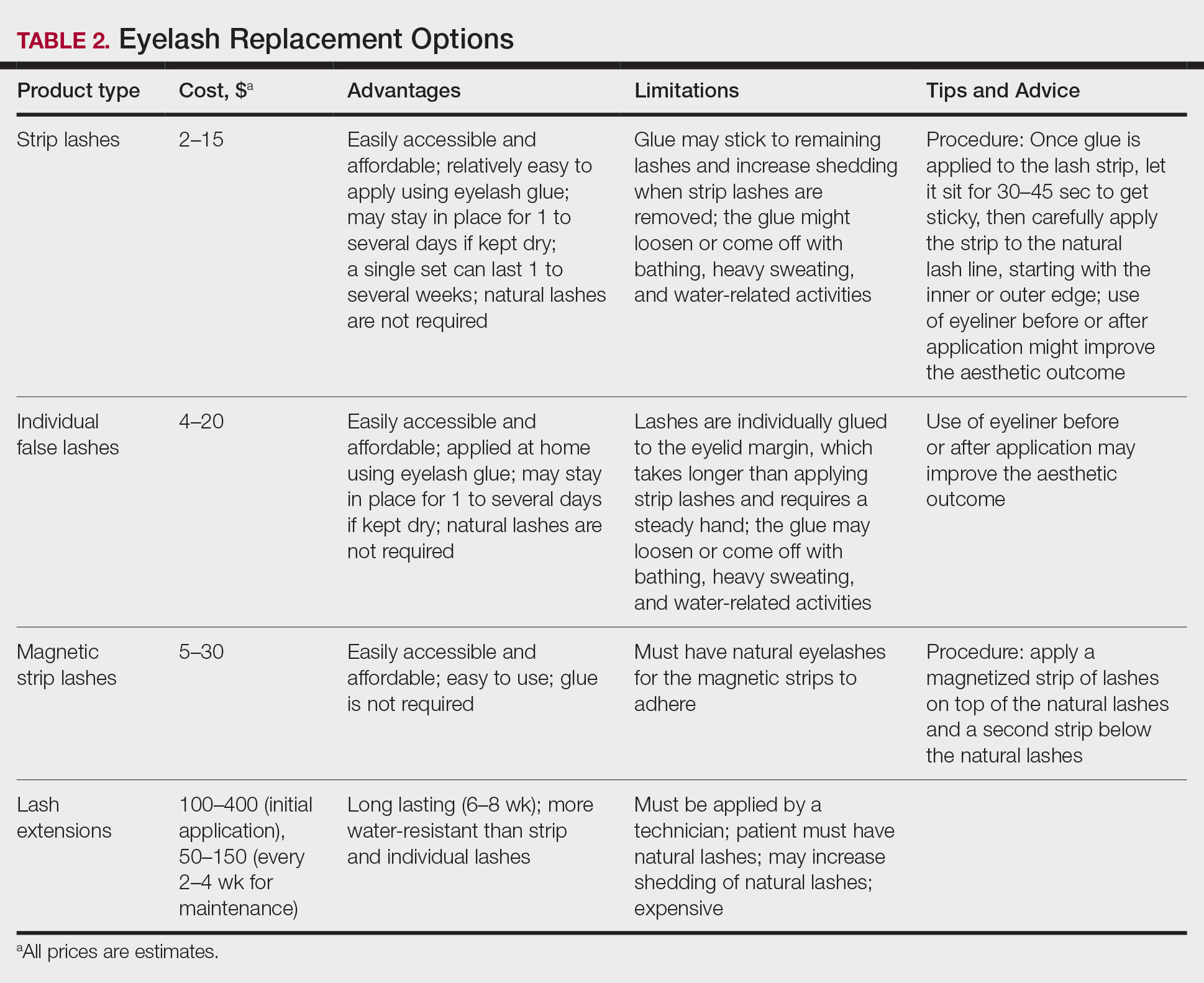
Cosmetic replacement of eyelashes (Table 2) and eyebrows (Table 3) is another treatment option that physicians can offer to hair-loss patients. For patients who desire false eyelashes, strip lashes that are glued to the eyelid margin are easiest to apply (but with caution—do not get glue in the eyes!). There are magnetic lashes, but these require natural lashes on which to adhere them. Eyebrows can be hand-drawn using brow pencils or powders with or without a stencil to maintain symmetry. There are even brow wigs and temporary brow tattoos that can last 1 to several days. Semi-permanent tattooing, including microblading, is an option that has amazing results but can be painful and expensive, often requiring touch-ups every 6 to 18 months.
Resources Abound
Experiencing and treating hair loss can be overwhelming, but there are countless resources available for patients. The NAAF has utility beyond the concerns of alopecia areata patients; there also is useful information on YouTube and social media, and support groups exist for hair-loss patients. I recommend starting with the NAAF website, which offers many helpful resources and support groups for patients and their families, including tips on applying for insurance reimbursement and drafting an appeal letter. Lastly, several nonprofit organizations serve the hair-replacement needs of children and adults with hair loss (Table 4).
Final Thoughts
My experience as a patient with alopecia has been long and initially was challenging; however, I found the silver lining after choosing to confront my literal and figurative “losses” and move forward—to grow, so to speak. With the use of custom-made human-hair wigs, false strip eyelashes, and a mix of eyebrow replacement options, I have been able to regain my confidence and self-esteem. Now, my goal as a physician—a goal that I hope you will share—is to be knowledgeable about hair-replacement options and provide information and resources to patients to help them feel empowered, brave, and beautiful.
When I was a medical student rotating in dermatology, a patient with extensive alopecia looked at my long thick hair and said tearfully, “I just wish I could have hair like yours.”
I smiled, removed my wig, and replied, “You can have hair like mine.”
Determination and Perseverance
I was 2 years old when I was given a diagnosis of alopecia areata. Bald spots on my scalp would come and go for years but were not overly burdensome until I turned 12. At that point, my hair loss escalated despite frequent intralesional injections of triamcinolone; every 2 steps forward were followed by 3 steps backward.
As a freshman in high school, I finally took control of my condition and emotions, shaved my head, and purchased a wig—actions that confronted my hair loss and awoke a determination and perseverance that I did not think I would ever gain while living with this condition. As McGettigan1 wrote in the Journal of the American Academy of Dermatology in 2004, “Being diagnosed with [alopecia areata] does not mean one cannot have a full and meaningful life. By choosing to confront the condition and turn its negative aspects into positive actions, one can succeed in life.”1
As a Provider, Another Perspective
Now, as a dermatology resident, I have the distinct perspective of being patient and provider. Patients often want to know, “Why is this happening?”, “Is my hair going to grow back?”, and “What treatments are available?”
They want to feel supported, understood, and heard.
As health care providers, we must understand that hair loss can result in overwhelming fear, hopelessness, and loss of self-esteem. Although we can give good news and offer helpful treatment options to some patients, there are those for whom medical treatment fails, and we can offer no more than a supportive hand and warm smile.
But can we do even more than that? The answer is: “Yes.”
Management Options
I recommend that all patients with hair loss should receive a copy of the aforementioned McGettigan1 article, “Ahead With No Hair,” which is geared toward patients with alopecia areata but offers inspiring words to any patient struggling to cope with hair loss. Dermatologists also can offer management options for patients with hair loss, including camouflage, wigs, and cosmetic replacement of eyelashes and eyebrows. Of note, several companies offer wigs and brow replacement options for men and children.
Camouflage
We can offer creative and readily available camouflage options for patients with hair loss. For small bald spots and thinning hair on the scalp, keratin hair-building fibers can be extremely useful. This over-the-counter product comes in a variety of natural hair colors, conceals the underlying skin, and adds fullness to hair. The keratin fibers have an innate static charge that allows them to adhere to the hair shaft. Daily application typically is necessary; duration can be maximized if hair spray or other brand-specific bonding spray is used following application of the fibers. A simple online search using the term keratin hair building fibers will reveal many online and in-store options with 4- or 5-star reviews. Most negative reviews pertain to sweating or moisture that causes clumping, but overall this is an easy and affordable option for mild hair loss.
Wigs
For patients hoping to mask moderate or severe hair loss, I recommend wigs, which can be made from synthetic fibers or human hair. In order to effectively guide patients, it is helpful for providers to have some knowledge about the 2 types of wigs. Synthetic wigs are of variable quality, ranging from costume-grade to top-quality products that look and feel like human hair. They are more affordable and often are easier to maintain than human-hair wigs, and hairstyles hold up better after washing. Many synthetic wigs cannot withstand heat from a hot iron and have a slightly shorter lifespan (6–12 months) than human-hair wigs (1–2 years).
Human hair wigs are made of real human hair, so they look and feel natural. These wigs can be made from European, African, Indian, Malaysian, Chinese, or other ethnic hair. Patients can choose the texture of the hair, including silky (smooth), kinky (mimicking natural blow-dried Black hair), and yaki (mimicking relaxed Black hair), as well as the curl pattern (straight, wavy, or curly), length, color, density, and cap construction.
The cap of a wig is what the hair is tied to. The construction of wig caps varies to allow for realistic hair lines as well as security for active use or up-dos. Among the many cap-construction options, the most realistic-appearing are hand-tied monofilament, lace-front, and full-lace wigs, all of which may require tape or glue to keep them in place. Some wig companies offer nonslip so-called “alopecia caps” for patients with no scalp hair. Patients who find their wig irritating to the scalp should consider wearing a nylon wig cap or liner.
Wigs can be purchased in store or online and can be pre-made or custom-built to be tailored to the patient’s specific desires and expectations. The cost depends on the type and quality of hair, cap construction, and length; prices can range from less than $100 to more than $5000.
When choosing a wig, which option—synthetic or human hair—is better for a given patient? Synthetic wigs are rather inexpensive and easy to care for, making them great for new users and those who want to try different styles and colors. Human-hair wigs can be custom-made to match the patient’s natural hair; however, they require extra care to maintain their longevity. Both types of wigs have pros and cons depending on the patient’s budget, time required for maintenance and styling, and needs (Table 1). I encourage patients to have fun with all wig options: Now is the time, I tell them, to try out the cute or daring hair style they have always wanted. The great thing is that if the patient does not like their wig, they can readily change it.
Good-quality wigs are expensive but sometimes are necessary to regain self-confidence and improve one’s quality of life. Advise patients to call their health insurance company to find out if a cranial or scalp prosthesis is covered by their policy. Coverage might require a written prescription for a cranial prosthesis, listing the diagnosis, diagnosis code, and letter of medical necessity. Patients can then purchase the wig online or through a certified distributor depending on their insurance requirements and obtain reimbursement (partial or full coverage). If a wig is not covered by insurance, a cranial prosthesis might be a flexible spending account–eligible expense. For guidance on the reimbursability of wigs, visit the National Alopecia Areata Foundation (NAAF) website (www.naaf.org/AccessHealthcare).
Eyelashes and Eyebrows
Cosmetic replacement of eyelashes (Table 2) and eyebrows (Table 3) is another treatment option that physicians can offer to hair-loss patients. For patients who desire false eyelashes, strip lashes that are glued to the eyelid margin are easiest to apply (but with caution—do not get glue in the eyes!). There are magnetic lashes, but these require natural lashes on which to adhere them. Eyebrows can be hand-drawn using brow pencils or powders with or without a stencil to maintain symmetry. There are even brow wigs and temporary brow tattoos that can last 1 to several days. Semi-permanent tattooing, including microblading, is an option that has amazing results but can be painful and expensive, often requiring touch-ups every 6 to 18 months.
Resources Abound
Experiencing and treating hair loss can be overwhelming, but there are countless resources available for patients. The NAAF has utility beyond the concerns of alopecia areata patients; there also is useful information on YouTube and social media, and support groups exist for hair-loss patients. I recommend starting with the NAAF website, which offers many helpful resources and support groups for patients and their families, including tips on applying for insurance reimbursement and drafting an appeal letter. Lastly, several nonprofit organizations serve the hair-replacement needs of children and adults with hair loss (Table 4).
Final Thoughts
My experience as a patient with alopecia has been long and initially was challenging; however, I found the silver lining after choosing to confront my literal and figurative “losses” and move forward—to grow, so to speak. With the use of custom-made human-hair wigs, false strip eyelashes, and a mix of eyebrow replacement options, I have been able to regain my confidence and self-esteem. Now, my goal as a physician—a goal that I hope you will share—is to be knowledgeable about hair-replacement options and provide information and resources to patients to help them feel empowered, brave, and beautiful.
- McGettigan ML. Ahead with no hair. J Am Acad Dermatol. 2004;51(1 suppl):18-19.
- McGettigan ML. Ahead with no hair. J Am Acad Dermatol. 2004;51(1 suppl):18-19.
Practice Points
- Keratin hair-building fibers can help thinning hair appear thick and full.
- Wigs are useful in masking moderate to severe hair loss.
- False eyelashes, eyebrow wigs, temporary eyebrow tattoos, microblading, and other semipermanent makeup can disguise the loss of eyelashes and eyebrows.
Commentary: Functional assessment developed for older adults with sickle cell disease
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.

Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.
Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.
Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
IMvigor130: A treasure trove of data for urothelial carcinoma

A second interim overall survival (OS) analysis suggested that atezolizumab monotherapy provides a clinical benefit as first-line treatment for mUC patients with PD-L1–expressing immune cells representing at least 5% of the tumor area (IC2/3), including patients who are cisplatin ineligible.
The analysis also suggested that atezolizumab plus chemotherapy produces similar OS results as chemotherapy plus placebo, but patients receiving atezolizumab may do better with cisplatin-based chemotherapy than with carboplatin-based chemotherapy.
These results were reported in two presentations at the American Association for Cancer Research Annual Meeting 2021: Week 1.
Current guidelines from the National Comprehensive Cancer Network and the European Society for Medical Oncology recommend atezolizumab monotherapy for cisplatin-ineligible patients with mUC and PD-L1 IC2/3.
The ongoing phase 3 IMvigor130 trial was designed to compare atezolizumab plus gemcitabine/platinum chemotherapy, atezolizumab monotherapy, and placebo plus chemotherapy. Platinum-based chemotherapy included either cisplatin or carboplatin, per investigator choice.
Coprimary endpoints for IMvigor130 were progression-free survival (PFS) and OS for atezolizumab plus chemotherapy versus placebo plus chemotherapy. The hierarchical study design dictated that OS would only be assessed for the comparison of atezolizumab monotherapy versus placebo-chemotherapy in the overall and PD-L1 IC2/3 populations if there was statistical improvement in OS for the atezolizumab-chemotherapy arm over the placebo-chemotherapy arm.
Secondary endpoints were overall response rate (ORR; per RECIST 1.1), duration of response (DOR) for all patients, and PFS for the comparison between atezolizumab monotherapy and placebo-chemotherapy. Exploratory analyses were performed on cisplatin-ineligible patients by PD-L1 status.
At the time of the primary analysis, an OS benefit for atezolizumab-chemotherapy over placebo-chemotherapy was not observed. Therefore, the OS benefit of atezolizumab monotherapy versus placebo-chemotherapy was not assessed. However, a trend toward improved OS was noted with atezolizumab for PD-L1 IC2/3 patients, including cisplatin-ineligible patients.
Atezolizumab vs. placebo-chemo
Ian D. Davis, MBBS, PhD, of Monash University in Melbourne, presented the second interim analysis of OS with atezolizumab monotherapy versus placebo plus chemotherapy (Abstract CT040).
The median follow-up was 14.9 months for atezolizumab monotherapy (n = 360) and 11.8 months for placebo-chemotherapy (n = 359). The median OS was 15.2 months and 13.1 months, respectively (hazard ratio, 0.99; 95% confidence interval, 0.83-1.19). There was no apparent OS benefit of atezolizumab for any clinically selected subgroup.
The ORR was 23.4% for atezolizumab monotherapy and 44.1% for placebo-chemotherapy. The median DOR was more than 3.5 times longer for atezolizumab monotherapy than for placebo-chemotherapy – 29.6 months and 8.1 months, respectively.
Although there was no formal statistical comparison, exploratory subgroup analyses demonstrated that the median OS for the PD-L1 IC2/3 patients appeared higher in the atezolizumab monotherapy arm than in the placebo-chemotherapy arm – 27.5 months and 16.7 months, respectively.
Similarly, the median OS for cisplatin-ineligible PD-L1 IC2/3 patients appeared higher for atezolizumab monotherapy than for placebo-chemotherapy – 18.6 months and 10.0 months, respectively.
In terms of safety, atezolizumab monotherapy compared favorably with placebo plus chemotherapy. There were similar numbers of grade 3/4 adverse events and comparable adverse events leading to discontinuation of treatment in both arms.
The atezolizumab monotherapy arm had fewer adverse events leading to withdrawal from any treatment, when compared with the placebo-chemotherapy arm – 7% and 34%, respectively. Two patients in the atezolizumab arm and one in the placebo-chemotherapy died of treatment-related causes.
Atezolizumab-chemo vs. placebo-chemo
Matthew D. Galsky, MD, of Mount Sinai Health System and Icahn School of Medicine at Mount Sinai in New York, presented the second interim OS comparison of atezolizumab plus chemotherapy with placebo plus chemotherapy (Abstract CT042).
The primary analysis had shown a statistically significant improvement in PFS for patients on atezolizumab-chemotherapy, in comparison with placebo-chemotherapy, with encouraging OS improvement, but the boundary for declaring significance for the OS endpoint was not crossed (Lancet. 2020 May 16;395[10236]:1547-1557).
Because IMvigor130 included both patients who received cisplatin and patients who investigators deemed cisplatin ineligible, the second interim analysis included an exploratory analysis of whether there was a difference in outcome between patients who received or did not receive cisplatin.
At a median follow-up of 13.3 months, the median OS was not significantly different in the atezolizumab-chemotherapy arm (n = 451) and the placebo-chemotherapy arm (n = 400) – 16.1 months and 13.4 months, respectively (HR, 0.84; 95% CI, 0.71-1.00; P = .026).
There were no clinically or pathologically defined subgroups that experienced an OS benefit from atezolizumab-chemotherapy over placebo-chemotherapy.
As for subsequent nonprotocol therapy, 24% of the placebo-chemotherapy arm received an immune checkpoint inhibitor at progression, as did 7% of the atezolizumab-chemotherapy arm. There was no difference in receipt of an immune checkpoint inhibitor post progression among patients treated with cisplatin versus carboplatin.
The benefit of combining atezolizumab with chemotherapy appeared more substantial with cisplatin-based chemotherapy than with carboplatin-based treatment. With cisplatin, the median OS was 21.6 months for the atezolizumab-chemotherapy arm and 14.6 months for the placebo-chemotherapy arm. With carboplatin, the median OS was 14.3 months and 13.0 months, respectively.
PD-L1 status was prognostic for patients who received cisplatin, with lower OS being observed for patients with PD-L1 IC0/1 status and higher OS observed for patients with PD-L1 IC2/3 status. Atezolizumab plus cisplatin-based chemotherapy appeared superior to cisplatin-based chemotherapy alone in both PD-L1–low and –high groups.
Atezolizumab did not seem to benefit patients who were treated with carboplatin, and PD-L1 status did not seem to influence OS among the carboplatin-treated patients.
Although similar ORR results were seen with cisplatin and carboplatin, there appeared to be a longer median DOR among cisplatin-treated patients who received atezolizumab than among those who did not – 13.2 months and 8.3 months, respectively.
No such benefit from atezolizumab was seen in carboplatin-treated patients. The median DOR was 8.1 months among patients who received atezolizumab and 7.1 months among those who did not.
The overall safety profile for atezolizumab plus chemotherapy was consistent with prior reports of the combination. Treatment-related grade 3-5 adverse events were similar on the atezolizumab-chemotherapy arm and the placebo-chemotherapy arm.
The present and future
The investigators who presented the second interim analysis for OS of the IMvigor130 trial were appropriately modest in their conclusions. After all, the prespecified boundary for significant improvement in OS for the addition of atezolizumab to chemotherapy was not crossed. No change in guideline-based clinical practice would be appropriate at the present time.
The various exploratory analyses are hypothesis generating and invite potential mechanistic explanations. However, given the nonrandom allocation of patients to cisplatin- or carboplatin-based chemotherapy, unrecognized variables may have influenced any appearance of a difference in OS between the regimens.
In IMvigor130, treatment was given until unacceptable toxicity or disease progression. It is uncertain whether the current National Comprehensive Cancer Network category 1 recommendation of chemotherapy induction followed by immune checkpoint inhibitor maintenance therapy will prove superior to the IMvigor130 strategy.
Clearly – and concordant with current treatment guidelines – atezolizumab monotherapy can benefit some patients, though the response rate for atezolizumab monotherapy was lower than for chemotherapy (23.4% vs. 44.1%).
As noted by the session chair, Marina Chiara Garassino, MD, of the University of Chicago, the OS curves were initially superior for chemotherapy over atezolizumab. However, the apparent early OS benefit for chemotherapy dissipated over time and, among responders to atezolizumab, response duration was considerably longer than for chemotherapy.
IMvigor130 will ultimately have a final OS analysis to clarify the relative benefits of the various treatment strategies. Fortunately, this large phase 3 study will yield a treasure trove of data to inform future research and build on the advances of recent years for patients with advanced urothelial cancer.
IMvigor130 is sponsored by Hoffmann-La Roche. Dr. Davis, Dr. Galsky, and Dr. Garassino disclosed relationships with Hoffmann-La Roche and many other companies.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
A second interim overall survival (OS) analysis suggested that atezolizumab monotherapy provides a clinical benefit as first-line treatment for mUC patients with PD-L1–expressing immune cells representing at least 5% of the tumor area (IC2/3), including patients who are cisplatin ineligible.
The analysis also suggested that atezolizumab plus chemotherapy produces similar OS results as chemotherapy plus placebo, but patients receiving atezolizumab may do better with cisplatin-based chemotherapy than with carboplatin-based chemotherapy.
These results were reported in two presentations at the American Association for Cancer Research Annual Meeting 2021: Week 1.
Current guidelines from the National Comprehensive Cancer Network and the European Society for Medical Oncology recommend atezolizumab monotherapy for cisplatin-ineligible patients with mUC and PD-L1 IC2/3.
The ongoing phase 3 IMvigor130 trial was designed to compare atezolizumab plus gemcitabine/platinum chemotherapy, atezolizumab monotherapy, and placebo plus chemotherapy. Platinum-based chemotherapy included either cisplatin or carboplatin, per investigator choice.
Coprimary endpoints for IMvigor130 were progression-free survival (PFS) and OS for atezolizumab plus chemotherapy versus placebo plus chemotherapy. The hierarchical study design dictated that OS would only be assessed for the comparison of atezolizumab monotherapy versus placebo-chemotherapy in the overall and PD-L1 IC2/3 populations if there was statistical improvement in OS for the atezolizumab-chemotherapy arm over the placebo-chemotherapy arm.
Secondary endpoints were overall response rate (ORR; per RECIST 1.1), duration of response (DOR) for all patients, and PFS for the comparison between atezolizumab monotherapy and placebo-chemotherapy. Exploratory analyses were performed on cisplatin-ineligible patients by PD-L1 status.
At the time of the primary analysis, an OS benefit for atezolizumab-chemotherapy over placebo-chemotherapy was not observed. Therefore, the OS benefit of atezolizumab monotherapy versus placebo-chemotherapy was not assessed. However, a trend toward improved OS was noted with atezolizumab for PD-L1 IC2/3 patients, including cisplatin-ineligible patients.
Atezolizumab vs. placebo-chemo
Ian D. Davis, MBBS, PhD, of Monash University in Melbourne, presented the second interim analysis of OS with atezolizumab monotherapy versus placebo plus chemotherapy (Abstract CT040).
The median follow-up was 14.9 months for atezolizumab monotherapy (n = 360) and 11.8 months for placebo-chemotherapy (n = 359). The median OS was 15.2 months and 13.1 months, respectively (hazard ratio, 0.99; 95% confidence interval, 0.83-1.19). There was no apparent OS benefit of atezolizumab for any clinically selected subgroup.
The ORR was 23.4% for atezolizumab monotherapy and 44.1% for placebo-chemotherapy. The median DOR was more than 3.5 times longer for atezolizumab monotherapy than for placebo-chemotherapy – 29.6 months and 8.1 months, respectively.
Although there was no formal statistical comparison, exploratory subgroup analyses demonstrated that the median OS for the PD-L1 IC2/3 patients appeared higher in the atezolizumab monotherapy arm than in the placebo-chemotherapy arm – 27.5 months and 16.7 months, respectively.
Similarly, the median OS for cisplatin-ineligible PD-L1 IC2/3 patients appeared higher for atezolizumab monotherapy than for placebo-chemotherapy – 18.6 months and 10.0 months, respectively.
In terms of safety, atezolizumab monotherapy compared favorably with placebo plus chemotherapy. There were similar numbers of grade 3/4 adverse events and comparable adverse events leading to discontinuation of treatment in both arms.
The atezolizumab monotherapy arm had fewer adverse events leading to withdrawal from any treatment, when compared with the placebo-chemotherapy arm – 7% and 34%, respectively. Two patients in the atezolizumab arm and one in the placebo-chemotherapy died of treatment-related causes.
Atezolizumab-chemo vs. placebo-chemo
Matthew D. Galsky, MD, of Mount Sinai Health System and Icahn School of Medicine at Mount Sinai in New York, presented the second interim OS comparison of atezolizumab plus chemotherapy with placebo plus chemotherapy (Abstract CT042).
The primary analysis had shown a statistically significant improvement in PFS for patients on atezolizumab-chemotherapy, in comparison with placebo-chemotherapy, with encouraging OS improvement, but the boundary for declaring significance for the OS endpoint was not crossed (Lancet. 2020 May 16;395[10236]:1547-1557).
Because IMvigor130 included both patients who received cisplatin and patients who investigators deemed cisplatin ineligible, the second interim analysis included an exploratory analysis of whether there was a difference in outcome between patients who received or did not receive cisplatin.
At a median follow-up of 13.3 months, the median OS was not significantly different in the atezolizumab-chemotherapy arm (n = 451) and the placebo-chemotherapy arm (n = 400) – 16.1 months and 13.4 months, respectively (HR, 0.84; 95% CI, 0.71-1.00; P = .026).
There were no clinically or pathologically defined subgroups that experienced an OS benefit from atezolizumab-chemotherapy over placebo-chemotherapy.
As for subsequent nonprotocol therapy, 24% of the placebo-chemotherapy arm received an immune checkpoint inhibitor at progression, as did 7% of the atezolizumab-chemotherapy arm. There was no difference in receipt of an immune checkpoint inhibitor post progression among patients treated with cisplatin versus carboplatin.
The benefit of combining atezolizumab with chemotherapy appeared more substantial with cisplatin-based chemotherapy than with carboplatin-based treatment. With cisplatin, the median OS was 21.6 months for the atezolizumab-chemotherapy arm and 14.6 months for the placebo-chemotherapy arm. With carboplatin, the median OS was 14.3 months and 13.0 months, respectively.
PD-L1 status was prognostic for patients who received cisplatin, with lower OS being observed for patients with PD-L1 IC0/1 status and higher OS observed for patients with PD-L1 IC2/3 status. Atezolizumab plus cisplatin-based chemotherapy appeared superior to cisplatin-based chemotherapy alone in both PD-L1–low and –high groups.
Atezolizumab did not seem to benefit patients who were treated with carboplatin, and PD-L1 status did not seem to influence OS among the carboplatin-treated patients.
Although similar ORR results were seen with cisplatin and carboplatin, there appeared to be a longer median DOR among cisplatin-treated patients who received atezolizumab than among those who did not – 13.2 months and 8.3 months, respectively.
No such benefit from atezolizumab was seen in carboplatin-treated patients. The median DOR was 8.1 months among patients who received atezolizumab and 7.1 months among those who did not.
The overall safety profile for atezolizumab plus chemotherapy was consistent with prior reports of the combination. Treatment-related grade 3-5 adverse events were similar on the atezolizumab-chemotherapy arm and the placebo-chemotherapy arm.
The present and future
The investigators who presented the second interim analysis for OS of the IMvigor130 trial were appropriately modest in their conclusions. After all, the prespecified boundary for significant improvement in OS for the addition of atezolizumab to chemotherapy was not crossed. No change in guideline-based clinical practice would be appropriate at the present time.
The various exploratory analyses are hypothesis generating and invite potential mechanistic explanations. However, given the nonrandom allocation of patients to cisplatin- or carboplatin-based chemotherapy, unrecognized variables may have influenced any appearance of a difference in OS between the regimens.
In IMvigor130, treatment was given until unacceptable toxicity or disease progression. It is uncertain whether the current National Comprehensive Cancer Network category 1 recommendation of chemotherapy induction followed by immune checkpoint inhibitor maintenance therapy will prove superior to the IMvigor130 strategy.
Clearly – and concordant with current treatment guidelines – atezolizumab monotherapy can benefit some patients, though the response rate for atezolizumab monotherapy was lower than for chemotherapy (23.4% vs. 44.1%).
As noted by the session chair, Marina Chiara Garassino, MD, of the University of Chicago, the OS curves were initially superior for chemotherapy over atezolizumab. However, the apparent early OS benefit for chemotherapy dissipated over time and, among responders to atezolizumab, response duration was considerably longer than for chemotherapy.
IMvigor130 will ultimately have a final OS analysis to clarify the relative benefits of the various treatment strategies. Fortunately, this large phase 3 study will yield a treasure trove of data to inform future research and build on the advances of recent years for patients with advanced urothelial cancer.
IMvigor130 is sponsored by Hoffmann-La Roche. Dr. Davis, Dr. Galsky, and Dr. Garassino disclosed relationships with Hoffmann-La Roche and many other companies.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
A second interim overall survival (OS) analysis suggested that atezolizumab monotherapy provides a clinical benefit as first-line treatment for mUC patients with PD-L1–expressing immune cells representing at least 5% of the tumor area (IC2/3), including patients who are cisplatin ineligible.
The analysis also suggested that atezolizumab plus chemotherapy produces similar OS results as chemotherapy plus placebo, but patients receiving atezolizumab may do better with cisplatin-based chemotherapy than with carboplatin-based chemotherapy.
These results were reported in two presentations at the American Association for Cancer Research Annual Meeting 2021: Week 1.
Current guidelines from the National Comprehensive Cancer Network and the European Society for Medical Oncology recommend atezolizumab monotherapy for cisplatin-ineligible patients with mUC and PD-L1 IC2/3.
The ongoing phase 3 IMvigor130 trial was designed to compare atezolizumab plus gemcitabine/platinum chemotherapy, atezolizumab monotherapy, and placebo plus chemotherapy. Platinum-based chemotherapy included either cisplatin or carboplatin, per investigator choice.
Coprimary endpoints for IMvigor130 were progression-free survival (PFS) and OS for atezolizumab plus chemotherapy versus placebo plus chemotherapy. The hierarchical study design dictated that OS would only be assessed for the comparison of atezolizumab monotherapy versus placebo-chemotherapy in the overall and PD-L1 IC2/3 populations if there was statistical improvement in OS for the atezolizumab-chemotherapy arm over the placebo-chemotherapy arm.
Secondary endpoints were overall response rate (ORR; per RECIST 1.1), duration of response (DOR) for all patients, and PFS for the comparison between atezolizumab monotherapy and placebo-chemotherapy. Exploratory analyses were performed on cisplatin-ineligible patients by PD-L1 status.
At the time of the primary analysis, an OS benefit for atezolizumab-chemotherapy over placebo-chemotherapy was not observed. Therefore, the OS benefit of atezolizumab monotherapy versus placebo-chemotherapy was not assessed. However, a trend toward improved OS was noted with atezolizumab for PD-L1 IC2/3 patients, including cisplatin-ineligible patients.
Atezolizumab vs. placebo-chemo
Ian D. Davis, MBBS, PhD, of Monash University in Melbourne, presented the second interim analysis of OS with atezolizumab monotherapy versus placebo plus chemotherapy (Abstract CT040).
The median follow-up was 14.9 months for atezolizumab monotherapy (n = 360) and 11.8 months for placebo-chemotherapy (n = 359). The median OS was 15.2 months and 13.1 months, respectively (hazard ratio, 0.99; 95% confidence interval, 0.83-1.19). There was no apparent OS benefit of atezolizumab for any clinically selected subgroup.
The ORR was 23.4% for atezolizumab monotherapy and 44.1% for placebo-chemotherapy. The median DOR was more than 3.5 times longer for atezolizumab monotherapy than for placebo-chemotherapy – 29.6 months and 8.1 months, respectively.
Although there was no formal statistical comparison, exploratory subgroup analyses demonstrated that the median OS for the PD-L1 IC2/3 patients appeared higher in the atezolizumab monotherapy arm than in the placebo-chemotherapy arm – 27.5 months and 16.7 months, respectively.
Similarly, the median OS for cisplatin-ineligible PD-L1 IC2/3 patients appeared higher for atezolizumab monotherapy than for placebo-chemotherapy – 18.6 months and 10.0 months, respectively.
In terms of safety, atezolizumab monotherapy compared favorably with placebo plus chemotherapy. There were similar numbers of grade 3/4 adverse events and comparable adverse events leading to discontinuation of treatment in both arms.
The atezolizumab monotherapy arm had fewer adverse events leading to withdrawal from any treatment, when compared with the placebo-chemotherapy arm – 7% and 34%, respectively. Two patients in the atezolizumab arm and one in the placebo-chemotherapy died of treatment-related causes.
Atezolizumab-chemo vs. placebo-chemo
Matthew D. Galsky, MD, of Mount Sinai Health System and Icahn School of Medicine at Mount Sinai in New York, presented the second interim OS comparison of atezolizumab plus chemotherapy with placebo plus chemotherapy (Abstract CT042).
The primary analysis had shown a statistically significant improvement in PFS for patients on atezolizumab-chemotherapy, in comparison with placebo-chemotherapy, with encouraging OS improvement, but the boundary for declaring significance for the OS endpoint was not crossed (Lancet. 2020 May 16;395[10236]:1547-1557).
Because IMvigor130 included both patients who received cisplatin and patients who investigators deemed cisplatin ineligible, the second interim analysis included an exploratory analysis of whether there was a difference in outcome between patients who received or did not receive cisplatin.
At a median follow-up of 13.3 months, the median OS was not significantly different in the atezolizumab-chemotherapy arm (n = 451) and the placebo-chemotherapy arm (n = 400) – 16.1 months and 13.4 months, respectively (HR, 0.84; 95% CI, 0.71-1.00; P = .026).
There were no clinically or pathologically defined subgroups that experienced an OS benefit from atezolizumab-chemotherapy over placebo-chemotherapy.
As for subsequent nonprotocol therapy, 24% of the placebo-chemotherapy arm received an immune checkpoint inhibitor at progression, as did 7% of the atezolizumab-chemotherapy arm. There was no difference in receipt of an immune checkpoint inhibitor post progression among patients treated with cisplatin versus carboplatin.
The benefit of combining atezolizumab with chemotherapy appeared more substantial with cisplatin-based chemotherapy than with carboplatin-based treatment. With cisplatin, the median OS was 21.6 months for the atezolizumab-chemotherapy arm and 14.6 months for the placebo-chemotherapy arm. With carboplatin, the median OS was 14.3 months and 13.0 months, respectively.
PD-L1 status was prognostic for patients who received cisplatin, with lower OS being observed for patients with PD-L1 IC0/1 status and higher OS observed for patients with PD-L1 IC2/3 status. Atezolizumab plus cisplatin-based chemotherapy appeared superior to cisplatin-based chemotherapy alone in both PD-L1–low and –high groups.
Atezolizumab did not seem to benefit patients who were treated with carboplatin, and PD-L1 status did not seem to influence OS among the carboplatin-treated patients.
Although similar ORR results were seen with cisplatin and carboplatin, there appeared to be a longer median DOR among cisplatin-treated patients who received atezolizumab than among those who did not – 13.2 months and 8.3 months, respectively.
No such benefit from atezolizumab was seen in carboplatin-treated patients. The median DOR was 8.1 months among patients who received atezolizumab and 7.1 months among those who did not.
The overall safety profile for atezolizumab plus chemotherapy was consistent with prior reports of the combination. Treatment-related grade 3-5 adverse events were similar on the atezolizumab-chemotherapy arm and the placebo-chemotherapy arm.
The present and future
The investigators who presented the second interim analysis for OS of the IMvigor130 trial were appropriately modest in their conclusions. After all, the prespecified boundary for significant improvement in OS for the addition of atezolizumab to chemotherapy was not crossed. No change in guideline-based clinical practice would be appropriate at the present time.
The various exploratory analyses are hypothesis generating and invite potential mechanistic explanations. However, given the nonrandom allocation of patients to cisplatin- or carboplatin-based chemotherapy, unrecognized variables may have influenced any appearance of a difference in OS between the regimens.
In IMvigor130, treatment was given until unacceptable toxicity or disease progression. It is uncertain whether the current National Comprehensive Cancer Network category 1 recommendation of chemotherapy induction followed by immune checkpoint inhibitor maintenance therapy will prove superior to the IMvigor130 strategy.
Clearly – and concordant with current treatment guidelines – atezolizumab monotherapy can benefit some patients, though the response rate for atezolizumab monotherapy was lower than for chemotherapy (23.4% vs. 44.1%).
As noted by the session chair, Marina Chiara Garassino, MD, of the University of Chicago, the OS curves were initially superior for chemotherapy over atezolizumab. However, the apparent early OS benefit for chemotherapy dissipated over time and, among responders to atezolizumab, response duration was considerably longer than for chemotherapy.
IMvigor130 will ultimately have a final OS analysis to clarify the relative benefits of the various treatment strategies. Fortunately, this large phase 3 study will yield a treasure trove of data to inform future research and build on the advances of recent years for patients with advanced urothelial cancer.
IMvigor130 is sponsored by Hoffmann-La Roche. Dr. Davis, Dr. Galsky, and Dr. Garassino disclosed relationships with Hoffmann-La Roche and many other companies.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
AACR 2021
How about contraceptives for men?
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.

The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.
The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.
The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
Surgery for early-stage cervical cancer: Are we still too radical?
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.

Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at obnews@mdedge.com.
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.
Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at obnews@mdedge.com.
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.
Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at obnews@mdedge.com.
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
Pros and cons of proposed recommendation for prediabetes and T2D screening
. If accepted as written, the new recommendation will be to “screen all asymptomatic adults ages 35 to 70 years who are overweight or obese.” Upon diagnosis of prediabetes, the recommendation is to offer or refer patients to preventive interventions.

This new recommendation would replace the one from 2015, which recommended screening adults aged 40-70 who are overweight or obese, lowering the age at which screening begins by 5 years. It would also replace the recommendation of referral to intensive behavioral counseling to promote a healthy diet and exercise.1
The American Diabetes Association (ADA) identifies A1c, fasting plasma glucose, or oral glucose tolerance tests as appropriate tests for the diagnosis of prediabetes and type 2 DM, and the new draft recommendation does not provide a preference for method of screening.2
The USPSTF’s draft recommendation could expand screening with the hope of identifying patients with prediabetes, or those with diabetes who are asymptomatic, with the intent of beginning treatment before there are serious complications.
Unknown diabetes or prediabetes diagnosis common
It has been estimated by the Centers for Disease Control and Prevention that 12% of U.S. adults had DM as of 2015, though nearly 24% were not aware that they had it. Also, according to the CDC, the prevalence of DM increases with age and is higher in those with less than a high school education. The same report indicates that more than 30% of U.S. adults have prediabetes, and with less than 12% of those individuals are aware of it.3 A possible explanation for a patient’s being unaware of a diagnosis could be that it has been documented in a chart but the patient does not know such information is in his or her health record. According to the evidence provided for the updated recommendation, earlier diagnosis may have an important benefit in preventing serious complications.
A modeling study compared simulated screening strategies and found that the most optimal screening strategy from a cost-effectiveness perspective begins between the ages of 30 and 45, with rescreening every 3-5 years. Further models have led researchers to conclude that early diagnosis can lead to decreased cardiovascular events as well as an opportunity for multifactorial treatment.1 For this reason, it makes sense to expand the ages of screening for obese and overweight individuals.
Treatment recommendations are more flexible
The change in treatment recommendations for a new diagnosis of prediabetes is potentially more useful. It may not be feasible or reasonable for physicians to always provide or refer their patients for intensive behavior interventions. The updated recommendation would allow for the inclusion of not only behavioral counseling and health education, but also potential medication options that are currently available but not approved, or that may be available in the future. The evidence review seemed to be mixed in outcome in this area, so the increased flexibility will likely allow for future opportunities.
Screening criteria may be too narrow
This recommendation, does not, however, provide any guidance on screening of individuals who have other risk factors besides a body mass index consistent with overweight or obesity. It seems that this may be a missed opportunity.
The draft statement clearly indicates that there are other factors associated with increased risk of developing DM, but does not consider these factors in determining which patients should be screened. Both the ADA and the American Association of Clinical Endocrinology (AACE) have recommendations for universal screening for all adults 45 and older, acknowledging that incidence of DM increases with age. The ADA also recommends screening individuals who are overweight or obese and have an additional risk factor regardless of age. The AACE recommends screening all individuals for risk factors regardless of age.
The current and draft recommendations by the USPSTF do not address other risk factors and indicate only that further research is needed to understand the risk associated with DM and the natural history of pre-DM and who may progress to DM or revert to normoglycemia. Without comment on other risk factors or universal screening with age, the USPSTF recommendation potentially would not be sensitive enough to capture all those who may meet criteria for prediabetes or DM.2,4
In addition to not addressing other risk factors and screening for those of normal and underweight BMI, the USPSTF recommendation does not address frequency of screening. The recommendations from both the ADA and the AACE indicate screening at 3-year intervals for those who are eligible – for any reason. The supporting evidence review did not seem to address this aspect, and so it is understandable that there was no comment. However, I feel this will lead physicians to turn to the other guidelines for guidance where there is disagreement in other aspects.
Ultimately, the draft updated recommendation will provide physicians with the opportunity to identify more patients with prediabetes and DM. This will be wonderful in terms of being able to offer treatments and lifestyle interventions to decrease the morbidity patients would face were these conditions not diagnosed. I hope that future recommendations will also address risk factors in addition to BMI as well as frequency of screening for those who remain at increased risk but initially screen negative.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. Screening for prediabetes and type 2 diabetes mellitus. U.S. Preventive Services Task Force. 2021 Mar 16.
2. Classification and diagnosis of diabetes: Standards of medical care in diabetes – 2020. American Diabetes Association. Diabetes Care. 2020 Jan. doi: 10.2337/dc20-S002.
3. National Diabetes Statistics Report, 2020. Centers for Disease Control and Prevention.
4. American Association of Clinical Endocrinologists and American College of Endocrinology – clinical practice guidelines for developing a diabetes mellitus comprehensive care plan. Hadelsman Y et al. Endocr Pract. 2015 Apr. 1-87. doi: 10.4158/EP15672.GL.
. If accepted as written, the new recommendation will be to “screen all asymptomatic adults ages 35 to 70 years who are overweight or obese.” Upon diagnosis of prediabetes, the recommendation is to offer or refer patients to preventive interventions.
This new recommendation would replace the one from 2015, which recommended screening adults aged 40-70 who are overweight or obese, lowering the age at which screening begins by 5 years. It would also replace the recommendation of referral to intensive behavioral counseling to promote a healthy diet and exercise.1
The American Diabetes Association (ADA) identifies A1c, fasting plasma glucose, or oral glucose tolerance tests as appropriate tests for the diagnosis of prediabetes and type 2 DM, and the new draft recommendation does not provide a preference for method of screening.2
The USPSTF’s draft recommendation could expand screening with the hope of identifying patients with prediabetes, or those with diabetes who are asymptomatic, with the intent of beginning treatment before there are serious complications.
Unknown diabetes or prediabetes diagnosis common
It has been estimated by the Centers for Disease Control and Prevention that 12% of U.S. adults had DM as of 2015, though nearly 24% were not aware that they had it. Also, according to the CDC, the prevalence of DM increases with age and is higher in those with less than a high school education. The same report indicates that more than 30% of U.S. adults have prediabetes, and with less than 12% of those individuals are aware of it.3 A possible explanation for a patient’s being unaware of a diagnosis could be that it has been documented in a chart but the patient does not know such information is in his or her health record. According to the evidence provided for the updated recommendation, earlier diagnosis may have an important benefit in preventing serious complications.
A modeling study compared simulated screening strategies and found that the most optimal screening strategy from a cost-effectiveness perspective begins between the ages of 30 and 45, with rescreening every 3-5 years. Further models have led researchers to conclude that early diagnosis can lead to decreased cardiovascular events as well as an opportunity for multifactorial treatment.1 For this reason, it makes sense to expand the ages of screening for obese and overweight individuals.
Treatment recommendations are more flexible
The change in treatment recommendations for a new diagnosis of prediabetes is potentially more useful. It may not be feasible or reasonable for physicians to always provide or refer their patients for intensive behavior interventions. The updated recommendation would allow for the inclusion of not only behavioral counseling and health education, but also potential medication options that are currently available but not approved, or that may be available in the future. The evidence review seemed to be mixed in outcome in this area, so the increased flexibility will likely allow for future opportunities.
Screening criteria may be too narrow
This recommendation, does not, however, provide any guidance on screening of individuals who have other risk factors besides a body mass index consistent with overweight or obesity. It seems that this may be a missed opportunity.
The draft statement clearly indicates that there are other factors associated with increased risk of developing DM, but does not consider these factors in determining which patients should be screened. Both the ADA and the American Association of Clinical Endocrinology (AACE) have recommendations for universal screening for all adults 45 and older, acknowledging that incidence of DM increases with age. The ADA also recommends screening individuals who are overweight or obese and have an additional risk factor regardless of age. The AACE recommends screening all individuals for risk factors regardless of age.
The current and draft recommendations by the USPSTF do not address other risk factors and indicate only that further research is needed to understand the risk associated with DM and the natural history of pre-DM and who may progress to DM or revert to normoglycemia. Without comment on other risk factors or universal screening with age, the USPSTF recommendation potentially would not be sensitive enough to capture all those who may meet criteria for prediabetes or DM.2,4
In addition to not addressing other risk factors and screening for those of normal and underweight BMI, the USPSTF recommendation does not address frequency of screening. The recommendations from both the ADA and the AACE indicate screening at 3-year intervals for those who are eligible – for any reason. The supporting evidence review did not seem to address this aspect, and so it is understandable that there was no comment. However, I feel this will lead physicians to turn to the other guidelines for guidance where there is disagreement in other aspects.
Ultimately, the draft updated recommendation will provide physicians with the opportunity to identify more patients with prediabetes and DM. This will be wonderful in terms of being able to offer treatments and lifestyle interventions to decrease the morbidity patients would face were these conditions not diagnosed. I hope that future recommendations will also address risk factors in addition to BMI as well as frequency of screening for those who remain at increased risk but initially screen negative.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. Screening for prediabetes and type 2 diabetes mellitus. U.S. Preventive Services Task Force. 2021 Mar 16.
2. Classification and diagnosis of diabetes: Standards of medical care in diabetes – 2020. American Diabetes Association. Diabetes Care. 2020 Jan. doi: 10.2337/dc20-S002.
3. National Diabetes Statistics Report, 2020. Centers for Disease Control and Prevention.
4. American Association of Clinical Endocrinologists and American College of Endocrinology – clinical practice guidelines for developing a diabetes mellitus comprehensive care plan. Hadelsman Y et al. Endocr Pract. 2015 Apr. 1-87. doi: 10.4158/EP15672.GL.
. If accepted as written, the new recommendation will be to “screen all asymptomatic adults ages 35 to 70 years who are overweight or obese.” Upon diagnosis of prediabetes, the recommendation is to offer or refer patients to preventive interventions.
This new recommendation would replace the one from 2015, which recommended screening adults aged 40-70 who are overweight or obese, lowering the age at which screening begins by 5 years. It would also replace the recommendation of referral to intensive behavioral counseling to promote a healthy diet and exercise.1
The American Diabetes Association (ADA) identifies A1c, fasting plasma glucose, or oral glucose tolerance tests as appropriate tests for the diagnosis of prediabetes and type 2 DM, and the new draft recommendation does not provide a preference for method of screening.2
The USPSTF’s draft recommendation could expand screening with the hope of identifying patients with prediabetes, or those with diabetes who are asymptomatic, with the intent of beginning treatment before there are serious complications.
Unknown diabetes or prediabetes diagnosis common
It has been estimated by the Centers for Disease Control and Prevention that 12% of U.S. adults had DM as of 2015, though nearly 24% were not aware that they had it. Also, according to the CDC, the prevalence of DM increases with age and is higher in those with less than a high school education. The same report indicates that more than 30% of U.S. adults have prediabetes, and with less than 12% of those individuals are aware of it.3 A possible explanation for a patient’s being unaware of a diagnosis could be that it has been documented in a chart but the patient does not know such information is in his or her health record. According to the evidence provided for the updated recommendation, earlier diagnosis may have an important benefit in preventing serious complications.
A modeling study compared simulated screening strategies and found that the most optimal screening strategy from a cost-effectiveness perspective begins between the ages of 30 and 45, with rescreening every 3-5 years. Further models have led researchers to conclude that early diagnosis can lead to decreased cardiovascular events as well as an opportunity for multifactorial treatment.1 For this reason, it makes sense to expand the ages of screening for obese and overweight individuals.
Treatment recommendations are more flexible
The change in treatment recommendations for a new diagnosis of prediabetes is potentially more useful. It may not be feasible or reasonable for physicians to always provide or refer their patients for intensive behavior interventions. The updated recommendation would allow for the inclusion of not only behavioral counseling and health education, but also potential medication options that are currently available but not approved, or that may be available in the future. The evidence review seemed to be mixed in outcome in this area, so the increased flexibility will likely allow for future opportunities.
Screening criteria may be too narrow
This recommendation, does not, however, provide any guidance on screening of individuals who have other risk factors besides a body mass index consistent with overweight or obesity. It seems that this may be a missed opportunity.
The draft statement clearly indicates that there are other factors associated with increased risk of developing DM, but does not consider these factors in determining which patients should be screened. Both the ADA and the American Association of Clinical Endocrinology (AACE) have recommendations for universal screening for all adults 45 and older, acknowledging that incidence of DM increases with age. The ADA also recommends screening individuals who are overweight or obese and have an additional risk factor regardless of age. The AACE recommends screening all individuals for risk factors regardless of age.
The current and draft recommendations by the USPSTF do not address other risk factors and indicate only that further research is needed to understand the risk associated with DM and the natural history of pre-DM and who may progress to DM or revert to normoglycemia. Without comment on other risk factors or universal screening with age, the USPSTF recommendation potentially would not be sensitive enough to capture all those who may meet criteria for prediabetes or DM.2,4
In addition to not addressing other risk factors and screening for those of normal and underweight BMI, the USPSTF recommendation does not address frequency of screening. The recommendations from both the ADA and the AACE indicate screening at 3-year intervals for those who are eligible – for any reason. The supporting evidence review did not seem to address this aspect, and so it is understandable that there was no comment. However, I feel this will lead physicians to turn to the other guidelines for guidance where there is disagreement in other aspects.
Ultimately, the draft updated recommendation will provide physicians with the opportunity to identify more patients with prediabetes and DM. This will be wonderful in terms of being able to offer treatments and lifestyle interventions to decrease the morbidity patients would face were these conditions not diagnosed. I hope that future recommendations will also address risk factors in addition to BMI as well as frequency of screening for those who remain at increased risk but initially screen negative.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. Screening for prediabetes and type 2 diabetes mellitus. U.S. Preventive Services Task Force. 2021 Mar 16.
2. Classification and diagnosis of diabetes: Standards of medical care in diabetes – 2020. American Diabetes Association. Diabetes Care. 2020 Jan. doi: 10.2337/dc20-S002.
3. National Diabetes Statistics Report, 2020. Centers for Disease Control and Prevention.
4. American Association of Clinical Endocrinologists and American College of Endocrinology – clinical practice guidelines for developing a diabetes mellitus comprehensive care plan. Hadelsman Y et al. Endocr Pract. 2015 Apr. 1-87. doi: 10.4158/EP15672.GL.