User login
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
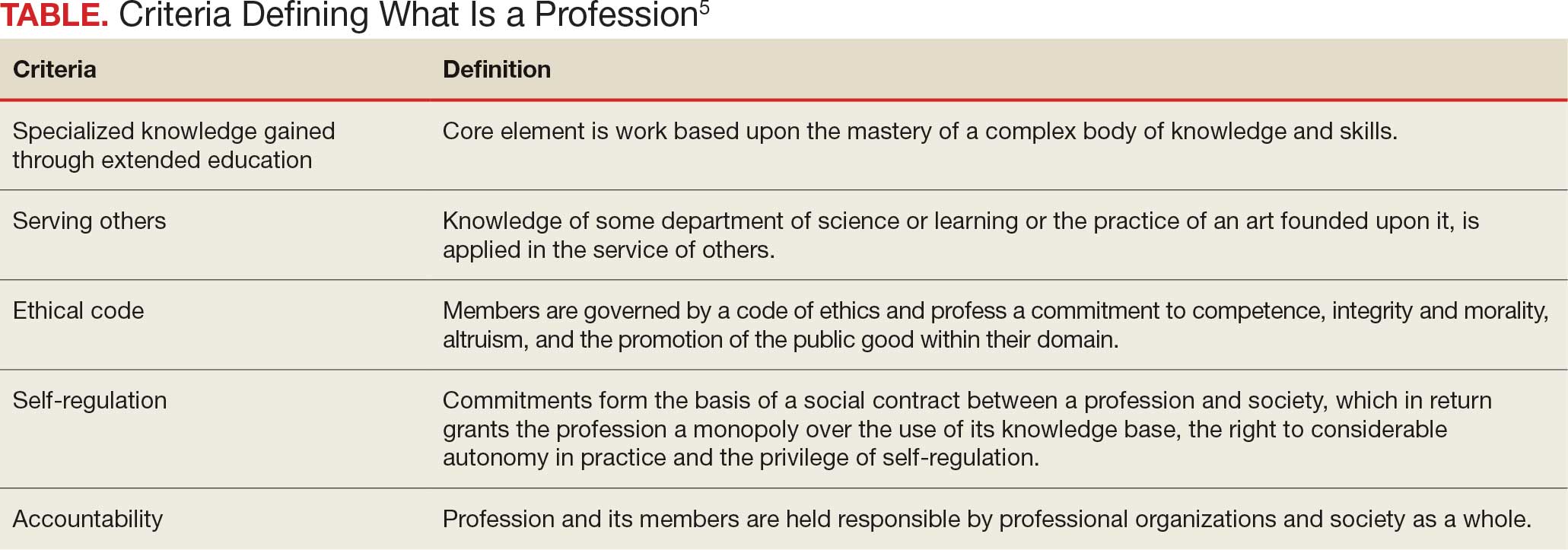
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?

Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
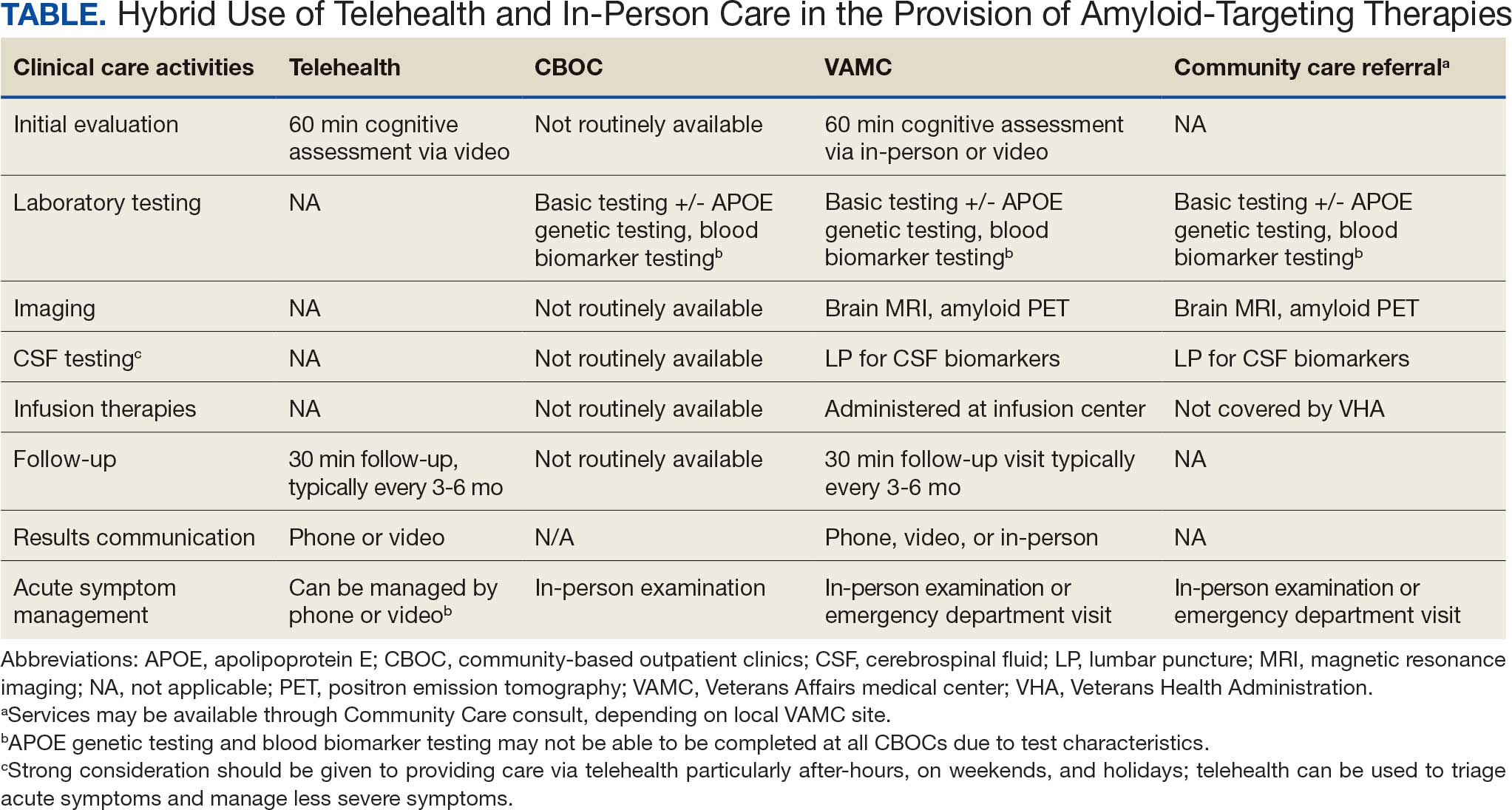
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
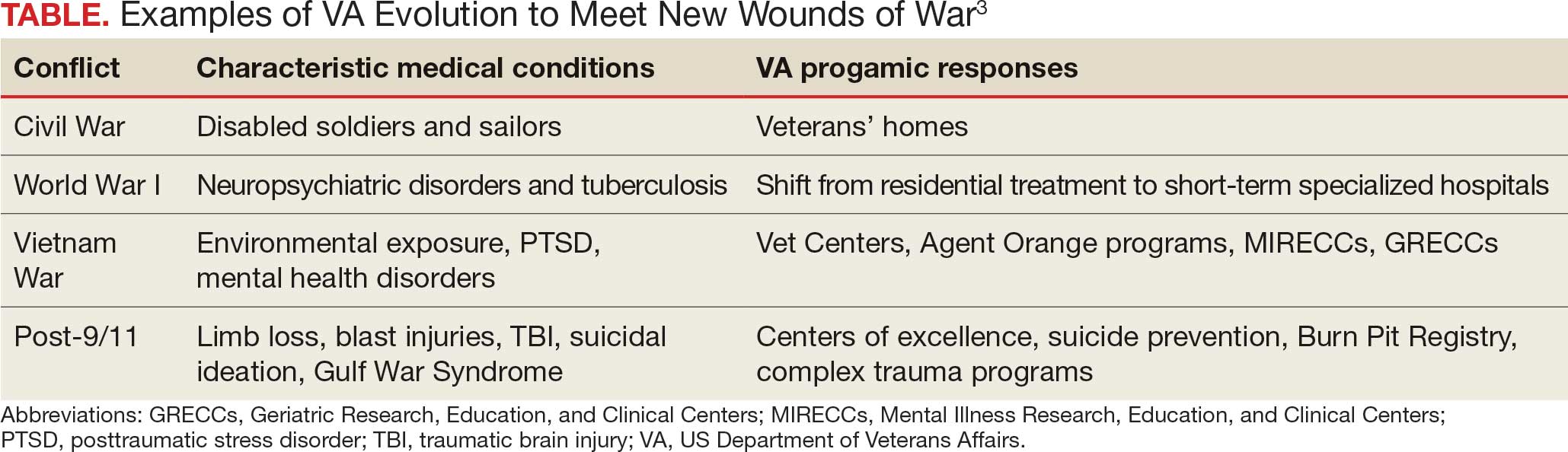
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration

Special Report II: Tackling Burnout
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Rosacea: We Still Haven’t Found What We’re Looking For
Rosacea: We Still Haven’t Found What We’re Looking For
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
Rosacea: We Still Haven’t Found What We’re Looking For
Rosacea: We Still Haven’t Found What We’re Looking For

Optimizing Clinical Teams in Dermatology: A Strategic Framework for Recruitment, Onboarding, and Retention
Optimizing Clinical Teams in Dermatology: A Strategic Framework for Recruitment, Onboarding, and Retention
Effective staffing is central to delivering high-quality, efficient dermatologic care. In the current landscape of American medicine, dermatologists manage complex medical conditions, perform surgical procedures, and in some cases expand into elective aesthetic services. The ability to offer advanced clinical services is dependent on the performance of those who operate equipment and sustain daily operations.
The “perfect” hire is therefore not a luxury but a necessity for practice survival: with shrinking reimbursements and rising administrative burden, staff capability influences clinic efficiency, medicolegal risk, and patient experience and outcomes. A dysfunctional team can contribute to physician burnout, whereas a high‑functioning one enables dermatologists to practice at the top of their license by focusing on diagnosis and complex interventions while the office functions efficiently. In this article, we examine the anatomy of modern dermatology hiring and highlight the benefits of shifting from reactive staffing to proactive talent acquisition.
PHASE 1: THE PHILOSOPHY OF THE DERMATOLOGY-SPECIFIC PROFILE
Before drafting a job description, it is important to have an idea of what the ideal candidate embodies. A medical assistant in a high-volume Mohs surgery suite requires a vastly different temperament and skill set than an aesthetic coordinator in a boutique cosmetic practice. Here are some factors to consider when approaching your ideal hire.
The Hybridity of the Specialty
Dermatology is unique in that the same patient can be treated for a life-threatening melanoma and a bothersome wrinkle within the same afternoon. This requires staff who can pivot emotionally and technically. When looking for a new employee, prioritize the 4 pillars of the ideal dermatology assistant: clinical competency, a hospitality mindset, digital agility, and a “get it done” mindset.
Clinical Competency—A basic understanding of skin anatomy and common pathologies is vital, even for nonclinical roles. A front-desk employee who understands the urgency of a changing mole in a patient with melanoma vs a new acne cyst is a vital triage asset.
Hospitality Mindset—When operating a dermatology clinic with offerings in the elective space (ie, aesthetics), be aware that patients increasingly are viewing themselves as consumers in these spaces. Dermatologists should look for candidates who have experience in high-end service industries such as retail, hospitality, or concierge services. These individuals understand that the patient experience begins in the parking lot and ends with the follow-up call.
Digital Agility—We are in the midst of a technological revolution. Between AI-driven diagnostic assistance, teledermatology platforms, and integrated electronic medical record/billing systems, the modern employee has to be more than just computer literate—they must be digitally native (eg, able to troubleshoot a tablet-based consent form or explain a patient portal with ease).
“Get It Done” Mindset—In a fast-paced dermatology clinic, it is important to find someone who looks for work instead of waiting for orders; otherwise, you might find yourself spending more time directing your employees than getting your actual work done.
The Culture Fit vs Culture Add
Traditionally, practices have prioritized hiring for “culture fit”—that is, looking for individuals who think and behave like existing staff. Contemporary management theory, however, favors hiring for “culture add,” recruiting candidates who contribute perspectives and skills absent from the current team. For practices expanding into aesthetics or focusing on a specific aspect of dermatology, the practice needs employees who bring perspectives it lacks. Perhaps the candidate has a background in hospitality, or they are involved in community health initiatives. These “adds” broaden the practice’s reach and depth.
PHASE 2: THE STRATEGIC RECRUITMENT PROCESS
The days of putting up “Help Wanted” signs are over. To find elite talent, dermatologists must treat recruitment like a diagnostic workup: thorough, methodical, and evidence based. Follow these steps for a thoughtful progression in finding the right candidate for your practice.
Step 1: Crafting a Magnetic Job Description
Most job postings read like a dry list of tasks: Take vitals, room patients, call in prescriptions. These descriptions attract clock-punchers. To attract careerists, the vision must be sold. An effective job description should include 2 main components: the vision statement and the growth path.
The Vision Statement—Start by stating your practice’s mission. If you’re focused on building a practice that values concierge-style care with long visit times, say so: “Join a team dedicated to patient care, slowing down, and personalized services.”
The Growth Path—High-quality candidates want to focus on their career trajectory. During the interview, mention opportunities for laser certification, scribe training, or management tracks. For those on a path toward higher education, describe the breadth of clinical training and experience.
Step 2: The Tiered Interview Protocol
We recommend a 3-tiered approach to the interview process to ensure multiple data points are collected before an offer is made: a behavior screen, a “shadow day,” and a “no doctor” zone.
Tier 1: The Behavioral Screen (Remote)—Conduct a 20-minute video call focused purely on soft skills using questions from the STAR method (Situation, Task, Action, Result). For example, ask something like, “Tell me about a time you may have faced an unsatisfied client. How did you de-escalate the situation?” Pay attention to whether the candidate takes responsibility or places blame.
Tier 2: The Shadow Day (Working Interview)—This can be an important part of the hiring process. We recommend inviting top candidates for a paid half- or full-day trial to assess how they perform in a real-world clinical setting. For medical assistant candidates, evaluate their ability to remain task focused and efficient and observe how they handle situations such as the sight of blood or interactions with needle-phobic patients. For front-desk candidates, pay attention to how they prioritize competing responsibilities and their openness to learning and feedback. For all positions, observing interactions with both patients and team members can provide valuable insight into professionalism, communication skills, and overall fit within the practice.
Tier 3: The “No-Doctor” Zone (Optional)—Leave the candidate alone with the current staff, if only for a few minutes. This allows the employer to gauge not only the candidate’s behavior with a senior member of staff but also with other members of the team, allowing for demonstration of character. Ask the team to assess if this is someone they would want to spend a workday with. If the staff says no, that may affect your choice of hire as well.
PHASE 3: THE OFFER AND THE LEGAL GUARDRAILS
After finding the unicorn candidate, the closing process must be professional and legally sound. Here are the steps we have found most helpful to take once a decision for a hire is made.
The Offer Letter as a Blueprint
An offer letter is more than a salary statement; it is a document of expectations. It should include the following components:
- Clear Compensation Structure: Base pay plus any performance-based incentives (eg, bonuses for retail skin care sales or conversion rates on cosmetic consultations).
- Specific Benefit Clauses: Paid time off, benefits such as health insurance and 401(k) matching if you are offering, and professional perks such as discounted treatments or skin care stipends.
- At-Will Statement: Ensure your legal counsel has reviewed your at-will employment clauses to protect the practice. This allows the employer to terminate an employee without legal liability and conversely gives the employee flexibility to leave the position if it does not fit their needs.
- Employee Manual: Once formally hired, make sure you have an employee handbook with your expectations and regulations—ranging from dress code and safety regulations to paid time off—clearly written. Be more specific than you think is necessary, which will prevent potential discrepancies down the road.
Onboarding: The First 90 Days
The first 90 days of employment are the most volatile. Statistics show that the majority of staff turnover happens in this window.1 To mitigate this, use the following 90-day success map:
- The Immersion Period (Days 1-30): The new hire should not be expected to produce. They are there to learn the culture of the clinic: the protocols for rooming, the vernacular for explaining procedures, and the standards for documentation.
- The Guided Execution Period (Days 31-60): They begin performing tasks under the direct supervision of a senior lead.
- The Independent Integration Period (Days 61-90): They take on a full load, with weekly check-ins to address friction points.
PHASE 4: RETENTION THROUGH PROFESSIONAL DEVELOPMENT
In dermatology practices, staff members frequently are approached by competitors, medical spas, and industry representatives to work for them. Retention is not just about the paycheck; it’s about the “professional home.” Staff members want to feel valued and have a responsible role in the workplace.
As dermatologists, we often are seen as the captain of the ship; however, the most successful practices operate as high-reliability organizations. In this type of practice, everyone from the janitorial staff to the senior associate is encouraged to speak up if there is a safety issue or an efficiency gap. Here are some techniques to foster this culture.
The Weekly Huddle—For practices that are just starting to expand, this is a great way to make sure that friction points and difficulties are addressed before becoming a larger issue. Gathering the staff for just 15 minutes in the morning before clinic begins can be a great way to address housekeeping issues, encourage staff to speak up about problems they may have identified, and provide a chance for everyone to feel heard.
The Educational Bend—Encourage staff to grow their wealth of knowledge, whether from industry-sponsored educational product events to formal certifications. A front desk assistant who then moves on to get their advanced degree may return to the practice as a nurse and become a valuable partner and asset.
PHASE 5: LOOKING TOWARD THE FUTURE
As we look toward 2027 and beyond, the employee of the future may not be entirely human. We already are seeing the integration of AI scribes and automated billing auditors. Practices should look for candidates who aren’t afraid of AI but are excited by it. A medical assistant who can oversee an AI scribe while still maintaining eye contact and holding a patient’s hand during a painful injection is the gold standard.
Final Thoughts
Our medical school training prepares us for the “what” of dermatology, but it rarely prepares us for the “who.” As practice managers, we are thrust into the role of CEO, human resources director, and culture architect without a formal syllabus. By applying the same clinical rigor to the hiring process that we do to a complex diagnostic case, we can build teams that don’t just work for us but build with us. The goal is a practice where the physician can focus on the art and science of the skin, confident that every other aspect of the patient journey is being handled by a team that is as dedicated, ethical, and clinical as they are. Hiring is one of the most difficult procedures you will likely perform in your practice; it also is the one with the highest long-term success rate if performed with thoughtfulness, precision, and above all, kindness.
- 2026 NSI National Health Care Retention & RN Staffing Report. NSI Nursing Solutions. Published March, 2026. Accessed June 17, 2026. https://www.google.com/url?q=https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf
Effective staffing is central to delivering high-quality, efficient dermatologic care. In the current landscape of American medicine, dermatologists manage complex medical conditions, perform surgical procedures, and in some cases expand into elective aesthetic services. The ability to offer advanced clinical services is dependent on the performance of those who operate equipment and sustain daily operations.
The “perfect” hire is therefore not a luxury but a necessity for practice survival: with shrinking reimbursements and rising administrative burden, staff capability influences clinic efficiency, medicolegal risk, and patient experience and outcomes. A dysfunctional team can contribute to physician burnout, whereas a high‑functioning one enables dermatologists to practice at the top of their license by focusing on diagnosis and complex interventions while the office functions efficiently. In this article, we examine the anatomy of modern dermatology hiring and highlight the benefits of shifting from reactive staffing to proactive talent acquisition.
PHASE 1: THE PHILOSOPHY OF THE DERMATOLOGY-SPECIFIC PROFILE
Before drafting a job description, it is important to have an idea of what the ideal candidate embodies. A medical assistant in a high-volume Mohs surgery suite requires a vastly different temperament and skill set than an aesthetic coordinator in a boutique cosmetic practice. Here are some factors to consider when approaching your ideal hire.
The Hybridity of the Specialty
Dermatology is unique in that the same patient can be treated for a life-threatening melanoma and a bothersome wrinkle within the same afternoon. This requires staff who can pivot emotionally and technically. When looking for a new employee, prioritize the 4 pillars of the ideal dermatology assistant: clinical competency, a hospitality mindset, digital agility, and a “get it done” mindset.
Clinical Competency—A basic understanding of skin anatomy and common pathologies is vital, even for nonclinical roles. A front-desk employee who understands the urgency of a changing mole in a patient with melanoma vs a new acne cyst is a vital triage asset.
Hospitality Mindset—When operating a dermatology clinic with offerings in the elective space (ie, aesthetics), be aware that patients increasingly are viewing themselves as consumers in these spaces. Dermatologists should look for candidates who have experience in high-end service industries such as retail, hospitality, or concierge services. These individuals understand that the patient experience begins in the parking lot and ends with the follow-up call.
Digital Agility—We are in the midst of a technological revolution. Between AI-driven diagnostic assistance, teledermatology platforms, and integrated electronic medical record/billing systems, the modern employee has to be more than just computer literate—they must be digitally native (eg, able to troubleshoot a tablet-based consent form or explain a patient portal with ease).
“Get It Done” Mindset—In a fast-paced dermatology clinic, it is important to find someone who looks for work instead of waiting for orders; otherwise, you might find yourself spending more time directing your employees than getting your actual work done.
The Culture Fit vs Culture Add
Traditionally, practices have prioritized hiring for “culture fit”—that is, looking for individuals who think and behave like existing staff. Contemporary management theory, however, favors hiring for “culture add,” recruiting candidates who contribute perspectives and skills absent from the current team. For practices expanding into aesthetics or focusing on a specific aspect of dermatology, the practice needs employees who bring perspectives it lacks. Perhaps the candidate has a background in hospitality, or they are involved in community health initiatives. These “adds” broaden the practice’s reach and depth.
PHASE 2: THE STRATEGIC RECRUITMENT PROCESS
The days of putting up “Help Wanted” signs are over. To find elite talent, dermatologists must treat recruitment like a diagnostic workup: thorough, methodical, and evidence based. Follow these steps for a thoughtful progression in finding the right candidate for your practice.
Step 1: Crafting a Magnetic Job Description
Most job postings read like a dry list of tasks: Take vitals, room patients, call in prescriptions. These descriptions attract clock-punchers. To attract careerists, the vision must be sold. An effective job description should include 2 main components: the vision statement and the growth path.
The Vision Statement—Start by stating your practice’s mission. If you’re focused on building a practice that values concierge-style care with long visit times, say so: “Join a team dedicated to patient care, slowing down, and personalized services.”
The Growth Path—High-quality candidates want to focus on their career trajectory. During the interview, mention opportunities for laser certification, scribe training, or management tracks. For those on a path toward higher education, describe the breadth of clinical training and experience.
Step 2: The Tiered Interview Protocol
We recommend a 3-tiered approach to the interview process to ensure multiple data points are collected before an offer is made: a behavior screen, a “shadow day,” and a “no doctor” zone.
Tier 1: The Behavioral Screen (Remote)—Conduct a 20-minute video call focused purely on soft skills using questions from the STAR method (Situation, Task, Action, Result). For example, ask something like, “Tell me about a time you may have faced an unsatisfied client. How did you de-escalate the situation?” Pay attention to whether the candidate takes responsibility or places blame.
Tier 2: The Shadow Day (Working Interview)—This can be an important part of the hiring process. We recommend inviting top candidates for a paid half- or full-day trial to assess how they perform in a real-world clinical setting. For medical assistant candidates, evaluate their ability to remain task focused and efficient and observe how they handle situations such as the sight of blood or interactions with needle-phobic patients. For front-desk candidates, pay attention to how they prioritize competing responsibilities and their openness to learning and feedback. For all positions, observing interactions with both patients and team members can provide valuable insight into professionalism, communication skills, and overall fit within the practice.
Tier 3: The “No-Doctor” Zone (Optional)—Leave the candidate alone with the current staff, if only for a few minutes. This allows the employer to gauge not only the candidate’s behavior with a senior member of staff but also with other members of the team, allowing for demonstration of character. Ask the team to assess if this is someone they would want to spend a workday with. If the staff says no, that may affect your choice of hire as well.
PHASE 3: THE OFFER AND THE LEGAL GUARDRAILS
After finding the unicorn candidate, the closing process must be professional and legally sound. Here are the steps we have found most helpful to take once a decision for a hire is made.
The Offer Letter as a Blueprint
An offer letter is more than a salary statement; it is a document of expectations. It should include the following components:
- Clear Compensation Structure: Base pay plus any performance-based incentives (eg, bonuses for retail skin care sales or conversion rates on cosmetic consultations).
- Specific Benefit Clauses: Paid time off, benefits such as health insurance and 401(k) matching if you are offering, and professional perks such as discounted treatments or skin care stipends.
- At-Will Statement: Ensure your legal counsel has reviewed your at-will employment clauses to protect the practice. This allows the employer to terminate an employee without legal liability and conversely gives the employee flexibility to leave the position if it does not fit their needs.
- Employee Manual: Once formally hired, make sure you have an employee handbook with your expectations and regulations—ranging from dress code and safety regulations to paid time off—clearly written. Be more specific than you think is necessary, which will prevent potential discrepancies down the road.
Onboarding: The First 90 Days
The first 90 days of employment are the most volatile. Statistics show that the majority of staff turnover happens in this window.1 To mitigate this, use the following 90-day success map:
- The Immersion Period (Days 1-30): The new hire should not be expected to produce. They are there to learn the culture of the clinic: the protocols for rooming, the vernacular for explaining procedures, and the standards for documentation.
- The Guided Execution Period (Days 31-60): They begin performing tasks under the direct supervision of a senior lead.
- The Independent Integration Period (Days 61-90): They take on a full load, with weekly check-ins to address friction points.
PHASE 4: RETENTION THROUGH PROFESSIONAL DEVELOPMENT
In dermatology practices, staff members frequently are approached by competitors, medical spas, and industry representatives to work for them. Retention is not just about the paycheck; it’s about the “professional home.” Staff members want to feel valued and have a responsible role in the workplace.
As dermatologists, we often are seen as the captain of the ship; however, the most successful practices operate as high-reliability organizations. In this type of practice, everyone from the janitorial staff to the senior associate is encouraged to speak up if there is a safety issue or an efficiency gap. Here are some techniques to foster this culture.
The Weekly Huddle—For practices that are just starting to expand, this is a great way to make sure that friction points and difficulties are addressed before becoming a larger issue. Gathering the staff for just 15 minutes in the morning before clinic begins can be a great way to address housekeeping issues, encourage staff to speak up about problems they may have identified, and provide a chance for everyone to feel heard.
The Educational Bend—Encourage staff to grow their wealth of knowledge, whether from industry-sponsored educational product events to formal certifications. A front desk assistant who then moves on to get their advanced degree may return to the practice as a nurse and become a valuable partner and asset.
PHASE 5: LOOKING TOWARD THE FUTURE
As we look toward 2027 and beyond, the employee of the future may not be entirely human. We already are seeing the integration of AI scribes and automated billing auditors. Practices should look for candidates who aren’t afraid of AI but are excited by it. A medical assistant who can oversee an AI scribe while still maintaining eye contact and holding a patient’s hand during a painful injection is the gold standard.
Final Thoughts
Our medical school training prepares us for the “what” of dermatology, but it rarely prepares us for the “who.” As practice managers, we are thrust into the role of CEO, human resources director, and culture architect without a formal syllabus. By applying the same clinical rigor to the hiring process that we do to a complex diagnostic case, we can build teams that don’t just work for us but build with us. The goal is a practice where the physician can focus on the art and science of the skin, confident that every other aspect of the patient journey is being handled by a team that is as dedicated, ethical, and clinical as they are. Hiring is one of the most difficult procedures you will likely perform in your practice; it also is the one with the highest long-term success rate if performed with thoughtfulness, precision, and above all, kindness.
Effective staffing is central to delivering high-quality, efficient dermatologic care. In the current landscape of American medicine, dermatologists manage complex medical conditions, perform surgical procedures, and in some cases expand into elective aesthetic services. The ability to offer advanced clinical services is dependent on the performance of those who operate equipment and sustain daily operations.
The “perfect” hire is therefore not a luxury but a necessity for practice survival: with shrinking reimbursements and rising administrative burden, staff capability influences clinic efficiency, medicolegal risk, and patient experience and outcomes. A dysfunctional team can contribute to physician burnout, whereas a high‑functioning one enables dermatologists to practice at the top of their license by focusing on diagnosis and complex interventions while the office functions efficiently. In this article, we examine the anatomy of modern dermatology hiring and highlight the benefits of shifting from reactive staffing to proactive talent acquisition.
PHASE 1: THE PHILOSOPHY OF THE DERMATOLOGY-SPECIFIC PROFILE
Before drafting a job description, it is important to have an idea of what the ideal candidate embodies. A medical assistant in a high-volume Mohs surgery suite requires a vastly different temperament and skill set than an aesthetic coordinator in a boutique cosmetic practice. Here are some factors to consider when approaching your ideal hire.
The Hybridity of the Specialty
Dermatology is unique in that the same patient can be treated for a life-threatening melanoma and a bothersome wrinkle within the same afternoon. This requires staff who can pivot emotionally and technically. When looking for a new employee, prioritize the 4 pillars of the ideal dermatology assistant: clinical competency, a hospitality mindset, digital agility, and a “get it done” mindset.
Clinical Competency—A basic understanding of skin anatomy and common pathologies is vital, even for nonclinical roles. A front-desk employee who understands the urgency of a changing mole in a patient with melanoma vs a new acne cyst is a vital triage asset.
Hospitality Mindset—When operating a dermatology clinic with offerings in the elective space (ie, aesthetics), be aware that patients increasingly are viewing themselves as consumers in these spaces. Dermatologists should look for candidates who have experience in high-end service industries such as retail, hospitality, or concierge services. These individuals understand that the patient experience begins in the parking lot and ends with the follow-up call.
Digital Agility—We are in the midst of a technological revolution. Between AI-driven diagnostic assistance, teledermatology platforms, and integrated electronic medical record/billing systems, the modern employee has to be more than just computer literate—they must be digitally native (eg, able to troubleshoot a tablet-based consent form or explain a patient portal with ease).
“Get It Done” Mindset—In a fast-paced dermatology clinic, it is important to find someone who looks for work instead of waiting for orders; otherwise, you might find yourself spending more time directing your employees than getting your actual work done.
The Culture Fit vs Culture Add
Traditionally, practices have prioritized hiring for “culture fit”—that is, looking for individuals who think and behave like existing staff. Contemporary management theory, however, favors hiring for “culture add,” recruiting candidates who contribute perspectives and skills absent from the current team. For practices expanding into aesthetics or focusing on a specific aspect of dermatology, the practice needs employees who bring perspectives it lacks. Perhaps the candidate has a background in hospitality, or they are involved in community health initiatives. These “adds” broaden the practice’s reach and depth.
PHASE 2: THE STRATEGIC RECRUITMENT PROCESS
The days of putting up “Help Wanted” signs are over. To find elite talent, dermatologists must treat recruitment like a diagnostic workup: thorough, methodical, and evidence based. Follow these steps for a thoughtful progression in finding the right candidate for your practice.
Step 1: Crafting a Magnetic Job Description
Most job postings read like a dry list of tasks: Take vitals, room patients, call in prescriptions. These descriptions attract clock-punchers. To attract careerists, the vision must be sold. An effective job description should include 2 main components: the vision statement and the growth path.
The Vision Statement—Start by stating your practice’s mission. If you’re focused on building a practice that values concierge-style care with long visit times, say so: “Join a team dedicated to patient care, slowing down, and personalized services.”
The Growth Path—High-quality candidates want to focus on their career trajectory. During the interview, mention opportunities for laser certification, scribe training, or management tracks. For those on a path toward higher education, describe the breadth of clinical training and experience.
Step 2: The Tiered Interview Protocol
We recommend a 3-tiered approach to the interview process to ensure multiple data points are collected before an offer is made: a behavior screen, a “shadow day,” and a “no doctor” zone.
Tier 1: The Behavioral Screen (Remote)—Conduct a 20-minute video call focused purely on soft skills using questions from the STAR method (Situation, Task, Action, Result). For example, ask something like, “Tell me about a time you may have faced an unsatisfied client. How did you de-escalate the situation?” Pay attention to whether the candidate takes responsibility or places blame.
Tier 2: The Shadow Day (Working Interview)—This can be an important part of the hiring process. We recommend inviting top candidates for a paid half- or full-day trial to assess how they perform in a real-world clinical setting. For medical assistant candidates, evaluate their ability to remain task focused and efficient and observe how they handle situations such as the sight of blood or interactions with needle-phobic patients. For front-desk candidates, pay attention to how they prioritize competing responsibilities and their openness to learning and feedback. For all positions, observing interactions with both patients and team members can provide valuable insight into professionalism, communication skills, and overall fit within the practice.
Tier 3: The “No-Doctor” Zone (Optional)—Leave the candidate alone with the current staff, if only for a few minutes. This allows the employer to gauge not only the candidate’s behavior with a senior member of staff but also with other members of the team, allowing for demonstration of character. Ask the team to assess if this is someone they would want to spend a workday with. If the staff says no, that may affect your choice of hire as well.
PHASE 3: THE OFFER AND THE LEGAL GUARDRAILS
After finding the unicorn candidate, the closing process must be professional and legally sound. Here are the steps we have found most helpful to take once a decision for a hire is made.
The Offer Letter as a Blueprint
An offer letter is more than a salary statement; it is a document of expectations. It should include the following components:
- Clear Compensation Structure: Base pay plus any performance-based incentives (eg, bonuses for retail skin care sales or conversion rates on cosmetic consultations).
- Specific Benefit Clauses: Paid time off, benefits such as health insurance and 401(k) matching if you are offering, and professional perks such as discounted treatments or skin care stipends.
- At-Will Statement: Ensure your legal counsel has reviewed your at-will employment clauses to protect the practice. This allows the employer to terminate an employee without legal liability and conversely gives the employee flexibility to leave the position if it does not fit their needs.
- Employee Manual: Once formally hired, make sure you have an employee handbook with your expectations and regulations—ranging from dress code and safety regulations to paid time off—clearly written. Be more specific than you think is necessary, which will prevent potential discrepancies down the road.
Onboarding: The First 90 Days
The first 90 days of employment are the most volatile. Statistics show that the majority of staff turnover happens in this window.1 To mitigate this, use the following 90-day success map:
- The Immersion Period (Days 1-30): The new hire should not be expected to produce. They are there to learn the culture of the clinic: the protocols for rooming, the vernacular for explaining procedures, and the standards for documentation.
- The Guided Execution Period (Days 31-60): They begin performing tasks under the direct supervision of a senior lead.
- The Independent Integration Period (Days 61-90): They take on a full load, with weekly check-ins to address friction points.
PHASE 4: RETENTION THROUGH PROFESSIONAL DEVELOPMENT
In dermatology practices, staff members frequently are approached by competitors, medical spas, and industry representatives to work for them. Retention is not just about the paycheck; it’s about the “professional home.” Staff members want to feel valued and have a responsible role in the workplace.
As dermatologists, we often are seen as the captain of the ship; however, the most successful practices operate as high-reliability organizations. In this type of practice, everyone from the janitorial staff to the senior associate is encouraged to speak up if there is a safety issue or an efficiency gap. Here are some techniques to foster this culture.
The Weekly Huddle—For practices that are just starting to expand, this is a great way to make sure that friction points and difficulties are addressed before becoming a larger issue. Gathering the staff for just 15 minutes in the morning before clinic begins can be a great way to address housekeeping issues, encourage staff to speak up about problems they may have identified, and provide a chance for everyone to feel heard.
The Educational Bend—Encourage staff to grow their wealth of knowledge, whether from industry-sponsored educational product events to formal certifications. A front desk assistant who then moves on to get their advanced degree may return to the practice as a nurse and become a valuable partner and asset.
PHASE 5: LOOKING TOWARD THE FUTURE
As we look toward 2027 and beyond, the employee of the future may not be entirely human. We already are seeing the integration of AI scribes and automated billing auditors. Practices should look for candidates who aren’t afraid of AI but are excited by it. A medical assistant who can oversee an AI scribe while still maintaining eye contact and holding a patient’s hand during a painful injection is the gold standard.
Final Thoughts
Our medical school training prepares us for the “what” of dermatology, but it rarely prepares us for the “who.” As practice managers, we are thrust into the role of CEO, human resources director, and culture architect without a formal syllabus. By applying the same clinical rigor to the hiring process that we do to a complex diagnostic case, we can build teams that don’t just work for us but build with us. The goal is a practice where the physician can focus on the art and science of the skin, confident that every other aspect of the patient journey is being handled by a team that is as dedicated, ethical, and clinical as they are. Hiring is one of the most difficult procedures you will likely perform in your practice; it also is the one with the highest long-term success rate if performed with thoughtfulness, precision, and above all, kindness.
- 2026 NSI National Health Care Retention & RN Staffing Report. NSI Nursing Solutions. Published March, 2026. Accessed June 17, 2026. https://www.google.com/url?q=https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf
- 2026 NSI National Health Care Retention & RN Staffing Report. NSI Nursing Solutions. Published March, 2026. Accessed June 17, 2026. https://www.google.com/url?q=https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf
Optimizing Clinical Teams in Dermatology: A Strategic Framework for Recruitment, Onboarding, and Retention
Optimizing Clinical Teams in Dermatology: A Strategic Framework for Recruitment, Onboarding, and Retention
Practice Points
- Dermatology requires a unique workforce that can balance clinical knowledge, customer service, technology use, and adaptability across medical and cosmetic settings.
- Effective hiring is a strategic process that relies on clearly defined candidate profiles, structured recruitment, and thoughtful onboarding.
- Practice success depends on retention and growth, with strong workplace culture, professional development, and readiness for AI-driven changes playing key roles.

Managing Acne Relapse After Isotretinoin: Tips from John Barbieri, MD, MBA
Managing Acne Relapse After Isotretinoin: Tips from John Barbieri, MD, MBA
Recent data suggest that approximately 20% to 40% of patients treated with isotretinoin have recurrence of acne. How should dermatologists interpret these findings?
DR. BARBIERI: While isotretinoin is highly effective and capable of delivering long-term remission, we should be careful to avoid describing it as a “cure” when counseling patients. Importantly, when acne does recur, it is often milder, and about half of those who have acne recurrence can be managed with topicals alone. For those who do require a subsequent course of isotretinoin, we should view this as an outcome that can be expected to happen in about 1 in 10 treated with isotretinoin rather than a treatment failure.
How important is cumulative dose in preventing relapse, and should we be rethinking traditional dosing targets?
DR. BARBIERI: Cumulative dose is one of the most important factors in preventing recurrence. Multiple studies support that higher cumulative dose is a strong predictor of long-term clearance. In contrast, daily dose does not seem to be as important a factor. However, higher cumulative dose also means longer courses and more potential for adverse effects, including long-term skin and eye dryness. For this reason, I prefer to treat to clinical endpoints of clear skin for 2 to 3 months and at least 120 to 150 mg/kg cumulative dose to balance achieving high cumulative doses with potential adverse effects and risks. For those with fewer adverse effects or who prioritize long-term clearance, we might go a little longer and for those with more adverse effects, we might use a shorter course and accept a higher risk for recurrence. By taking this approach, we can individualize our dosing approach to each patient.
What factors most strongly predict relapse after a completed isotretinoin course?
DR. BARBIERI: Some demographic factors that have been associated with higher rates of recurrence include greater baseline severity and younger age at treatment. Women with a strong hormonal component to their acne, such as those with polyendocrine metabolic ovarian syndrome (formerly polycystic ovary syndrome), also may be more likely to have recurrence. With respect to clinical factors, increasing cumulative dose has been associated with reduced risk for recurrence in multiple studies, and treating until a clinical endpoint of clear skin for 2 to 3 months also may be predictive of long-term clearance.
When a patient relapses, how do you decide between topical therapy, hormonal treatment, or a second isotretinoin course?
DR. BARBIERI: It depends on relapse severity and patient goals. Mild recurrence often responds well to topical therapies such as retinoids, benzoyl peroxide, antibiotics, and clascoterone. About half of those with recurrence will be able to manage it with topical therapies alone. For those with more severe acne requiring systemic therapy, about half will decide on a repeat course of isotretinoin, which I often find works faster and better than the first course. For second courses, I will typically try to use micronized isotretinoin due to the more consistent pharmacokinetics. For women—especially those with signs of hyperandrogenism such as hirsutism, irregular periods, or flaring with menstrual cycle—hormonal therapy such as combined oral contraceptives or spironolactone can be a great option. Oral antibiotics also can be a consideration for those with recurrence, though we need to be thoughtful about antimicrobial stewardship and risks of long-term antibiotic use.
Are low-dose or shorter-course regimens contributing to higher relapse rates?
DR. BARBIERI: While there is some evidence that higher daily doses may be associated with lower risk for recurrence, when you control for cumulative dose, it doesn’t seem like daily dose has much influence. In contrast, cumulative dose has a large effect on frequency of long-term clearance. While I don’t think low-dose regimens are inherently problematic, if they result in shorter cumulative dose courses, that could increase the risk for recurrence.
How does hormonal acne influence long-term outcomes after isotretinoin?
DR. BARBIERI: While all acne is “hormonal,” those with a stronger hormonal pathogenesis, such as women with polyendocrine metabolic ovarian syndrome or other signs of hyperandrogenism, may have a higher likelihood of recurrence after treatment. In these patients, I often find hormonal therapy such as combined oral contraceptives or spironolactone to be highly effective, even if they haven't worked before.
Should maintenance therapy be routine after isotretinoin, and if so, what strategies are most effective?
DR. BARBIERI: Since many patients have a goal of long-term clearance after isotretinoin, I do not routinely recommend maintenance therapy, as this seems antithetical to this goal. However, for those who are very concerned about recurrence or who would like to be on a topical retinoid for other reasons, I will sometimes start a topical retinoid after treatment with isotretinoin.
How should dermatologists counsel patients about expectations with respect to relapse before starting isotretinoin?
DR. BARBIERI: We should be careful to set appropriate expectations with isotretinoin. I counsel patients that isotretinoin is an incredibly effective therapy for severe acne, with a high likelihood of long-term remission, but not a guaranteed permanent cure. Setting this expectation upfront reduces disappointment if acne does recur and improves shared decision-making.
Recent data suggest that approximately 20% to 40% of patients treated with isotretinoin have recurrence of acne. How should dermatologists interpret these findings?
DR. BARBIERI: While isotretinoin is highly effective and capable of delivering long-term remission, we should be careful to avoid describing it as a “cure” when counseling patients. Importantly, when acne does recur, it is often milder, and about half of those who have acne recurrence can be managed with topicals alone. For those who do require a subsequent course of isotretinoin, we should view this as an outcome that can be expected to happen in about 1 in 10 treated with isotretinoin rather than a treatment failure.
How important is cumulative dose in preventing relapse, and should we be rethinking traditional dosing targets?
DR. BARBIERI: Cumulative dose is one of the most important factors in preventing recurrence. Multiple studies support that higher cumulative dose is a strong predictor of long-term clearance. In contrast, daily dose does not seem to be as important a factor. However, higher cumulative dose also means longer courses and more potential for adverse effects, including long-term skin and eye dryness. For this reason, I prefer to treat to clinical endpoints of clear skin for 2 to 3 months and at least 120 to 150 mg/kg cumulative dose to balance achieving high cumulative doses with potential adverse effects and risks. For those with fewer adverse effects or who prioritize long-term clearance, we might go a little longer and for those with more adverse effects, we might use a shorter course and accept a higher risk for recurrence. By taking this approach, we can individualize our dosing approach to each patient.
What factors most strongly predict relapse after a completed isotretinoin course?
DR. BARBIERI: Some demographic factors that have been associated with higher rates of recurrence include greater baseline severity and younger age at treatment. Women with a strong hormonal component to their acne, such as those with polyendocrine metabolic ovarian syndrome (formerly polycystic ovary syndrome), also may be more likely to have recurrence. With respect to clinical factors, increasing cumulative dose has been associated with reduced risk for recurrence in multiple studies, and treating until a clinical endpoint of clear skin for 2 to 3 months also may be predictive of long-term clearance.
When a patient relapses, how do you decide between topical therapy, hormonal treatment, or a second isotretinoin course?
DR. BARBIERI: It depends on relapse severity and patient goals. Mild recurrence often responds well to topical therapies such as retinoids, benzoyl peroxide, antibiotics, and clascoterone. About half of those with recurrence will be able to manage it with topical therapies alone. For those with more severe acne requiring systemic therapy, about half will decide on a repeat course of isotretinoin, which I often find works faster and better than the first course. For second courses, I will typically try to use micronized isotretinoin due to the more consistent pharmacokinetics. For women—especially those with signs of hyperandrogenism such as hirsutism, irregular periods, or flaring with menstrual cycle—hormonal therapy such as combined oral contraceptives or spironolactone can be a great option. Oral antibiotics also can be a consideration for those with recurrence, though we need to be thoughtful about antimicrobial stewardship and risks of long-term antibiotic use.
Are low-dose or shorter-course regimens contributing to higher relapse rates?
DR. BARBIERI: While there is some evidence that higher daily doses may be associated with lower risk for recurrence, when you control for cumulative dose, it doesn’t seem like daily dose has much influence. In contrast, cumulative dose has a large effect on frequency of long-term clearance. While I don’t think low-dose regimens are inherently problematic, if they result in shorter cumulative dose courses, that could increase the risk for recurrence.
How does hormonal acne influence long-term outcomes after isotretinoin?
DR. BARBIERI: While all acne is “hormonal,” those with a stronger hormonal pathogenesis, such as women with polyendocrine metabolic ovarian syndrome or other signs of hyperandrogenism, may have a higher likelihood of recurrence after treatment. In these patients, I often find hormonal therapy such as combined oral contraceptives or spironolactone to be highly effective, even if they haven't worked before.
Should maintenance therapy be routine after isotretinoin, and if so, what strategies are most effective?
DR. BARBIERI: Since many patients have a goal of long-term clearance after isotretinoin, I do not routinely recommend maintenance therapy, as this seems antithetical to this goal. However, for those who are very concerned about recurrence or who would like to be on a topical retinoid for other reasons, I will sometimes start a topical retinoid after treatment with isotretinoin.
How should dermatologists counsel patients about expectations with respect to relapse before starting isotretinoin?
DR. BARBIERI: We should be careful to set appropriate expectations with isotretinoin. I counsel patients that isotretinoin is an incredibly effective therapy for severe acne, with a high likelihood of long-term remission, but not a guaranteed permanent cure. Setting this expectation upfront reduces disappointment if acne does recur and improves shared decision-making.
Recent data suggest that approximately 20% to 40% of patients treated with isotretinoin have recurrence of acne. How should dermatologists interpret these findings?
DR. BARBIERI: While isotretinoin is highly effective and capable of delivering long-term remission, we should be careful to avoid describing it as a “cure” when counseling patients. Importantly, when acne does recur, it is often milder, and about half of those who have acne recurrence can be managed with topicals alone. For those who do require a subsequent course of isotretinoin, we should view this as an outcome that can be expected to happen in about 1 in 10 treated with isotretinoin rather than a treatment failure.
How important is cumulative dose in preventing relapse, and should we be rethinking traditional dosing targets?
DR. BARBIERI: Cumulative dose is one of the most important factors in preventing recurrence. Multiple studies support that higher cumulative dose is a strong predictor of long-term clearance. In contrast, daily dose does not seem to be as important a factor. However, higher cumulative dose also means longer courses and more potential for adverse effects, including long-term skin and eye dryness. For this reason, I prefer to treat to clinical endpoints of clear skin for 2 to 3 months and at least 120 to 150 mg/kg cumulative dose to balance achieving high cumulative doses with potential adverse effects and risks. For those with fewer adverse effects or who prioritize long-term clearance, we might go a little longer and for those with more adverse effects, we might use a shorter course and accept a higher risk for recurrence. By taking this approach, we can individualize our dosing approach to each patient.
What factors most strongly predict relapse after a completed isotretinoin course?
DR. BARBIERI: Some demographic factors that have been associated with higher rates of recurrence include greater baseline severity and younger age at treatment. Women with a strong hormonal component to their acne, such as those with polyendocrine metabolic ovarian syndrome (formerly polycystic ovary syndrome), also may be more likely to have recurrence. With respect to clinical factors, increasing cumulative dose has been associated with reduced risk for recurrence in multiple studies, and treating until a clinical endpoint of clear skin for 2 to 3 months also may be predictive of long-term clearance.
When a patient relapses, how do you decide between topical therapy, hormonal treatment, or a second isotretinoin course?
DR. BARBIERI: It depends on relapse severity and patient goals. Mild recurrence often responds well to topical therapies such as retinoids, benzoyl peroxide, antibiotics, and clascoterone. About half of those with recurrence will be able to manage it with topical therapies alone. For those with more severe acne requiring systemic therapy, about half will decide on a repeat course of isotretinoin, which I often find works faster and better than the first course. For second courses, I will typically try to use micronized isotretinoin due to the more consistent pharmacokinetics. For women—especially those with signs of hyperandrogenism such as hirsutism, irregular periods, or flaring with menstrual cycle—hormonal therapy such as combined oral contraceptives or spironolactone can be a great option. Oral antibiotics also can be a consideration for those with recurrence, though we need to be thoughtful about antimicrobial stewardship and risks of long-term antibiotic use.
Are low-dose or shorter-course regimens contributing to higher relapse rates?
DR. BARBIERI: While there is some evidence that higher daily doses may be associated with lower risk for recurrence, when you control for cumulative dose, it doesn’t seem like daily dose has much influence. In contrast, cumulative dose has a large effect on frequency of long-term clearance. While I don’t think low-dose regimens are inherently problematic, if they result in shorter cumulative dose courses, that could increase the risk for recurrence.
How does hormonal acne influence long-term outcomes after isotretinoin?
DR. BARBIERI: While all acne is “hormonal,” those with a stronger hormonal pathogenesis, such as women with polyendocrine metabolic ovarian syndrome or other signs of hyperandrogenism, may have a higher likelihood of recurrence after treatment. In these patients, I often find hormonal therapy such as combined oral contraceptives or spironolactone to be highly effective, even if they haven't worked before.
Should maintenance therapy be routine after isotretinoin, and if so, what strategies are most effective?
DR. BARBIERI: Since many patients have a goal of long-term clearance after isotretinoin, I do not routinely recommend maintenance therapy, as this seems antithetical to this goal. However, for those who are very concerned about recurrence or who would like to be on a topical retinoid for other reasons, I will sometimes start a topical retinoid after treatment with isotretinoin.
How should dermatologists counsel patients about expectations with respect to relapse before starting isotretinoin?
DR. BARBIERI: We should be careful to set appropriate expectations with isotretinoin. I counsel patients that isotretinoin is an incredibly effective therapy for severe acne, with a high likelihood of long-term remission, but not a guaranteed permanent cure. Setting this expectation upfront reduces disappointment if acne does recur and improves shared decision-making.
Managing Acne Relapse After Isotretinoin: Tips from John Barbieri, MD, MBA
Managing Acne Relapse After Isotretinoin: Tips from John Barbieri, MD, MBA
What They Want and What They Need: The End-of-Life Conflict
What They Want and What They Need: The End-of-Life Conflict
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
When contemplating the state of ethical dialogue in our modern world, the philosopher Alasdair MacIntyre had this to say: “I can only answer the question, ‘What am I to do?’ If I can answer the prior question ‘Of what story or stories do I find myself a part?’”1 That is, our ethics must proceed from our understanding of ourselves, others, and the world. David Hume might scoff, but we do need an “is” to appreciate and grasp our “ought.” This is just as true for medical ethics as it is for the rest of life. Questions about what we should do in medicine should draw us to deeper questions about identity and purpose.
In this issue, Ruskin et al present a tragic case of a man who spent his later years walking the line between life and a self-chosen death.2 After enduring the chronic decline of Parkinson disease, he faced a final diagnosis of glioblastoma. The patient enrolled in hospice while considering how he might move elsewhere to avail himself of assisted suicide. Before he had a chance to do that, he was admitted to an inpatient hospice unit where he weakened further. In the throes of what may have been delirium or a last effort to enact his wish of a hastened death, he attempted suicide on the hospice unit. He survived only to die days later from the cancer.
The authors reflect on the complexities of this case, including the distress of a clinician who may want to satisfy a veteran’s wish but cannot due to legal constraints, and the challenges of identifying pathologic suicidal ideation from an earnest and rational desire for a hastened death. How should they handle these conversations? They conclude by suggesting ways clinicians may assess and respond to requests for a hastened death, recognizing that assisted suicide remains illegal within the Veterans Health Administration (VHA).
Clinicians can return to the foundation of our profession to better consider these questions. The case report authors acknowledge this but avoid learning from what the conflict might teach us: “The inability to help veterans achieve their care preferences [to receive a hastened death] conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.” Before feeling like they have failed the veteran, a clinician must ask if it is really within their scope of practice to end someone’s life. While it is true that “the mission of VHA’s [Palliative and Hospice Care] program is to honor veterans’ preferences for care,” this mission exists within a greater context of appreciating that not all preferences can or should be honored.3 An obvious example is when a veteran requests an intervention that is not clinically indicated (eg, antibiotics for a viral infection). Clinicians are not bound to honor this preference; not because there is a law directing the clinicians’ decision making (there is not) but because there is a standard of care that accounts for but can supersede the veteran’s preference.
Is assisted suicide ever clinically indicated? While the answer shifts depending on the jurisdiction, the case report authors acknowledge why the preference for assisted suicide cannot be honored in a VHA facility: it is against the law.4 However, as they explain, this is insufficient to assuage the moral distress that might arise for some clinicians who want to fulfill a veteran’s request. They recommend several different strategies for clinicians to consider when receiving a request for assisted suicide. Distress in the form of cognitive dissonance may also arise from the tension that exists between stopping some forms of suicide while assisting in others.
While it is important to assess whether the request for a hastened death is driven by an untreated symptom or mental illness, this will only get a clinician so far when the request is made in earnest with no remediable drivers. While I cannot argue the point here, I accept that there are forms of suicide which are rational. However, that alone is insufficient to justify the act or assist someone with it; we must assess the good that the rational choice seeks to realize.5 If suicide can be rational, clinicians should ask whether it is within the goals of medicine to assist in suicide. The authors seem to take it for granted that the distressed clinician in the case hopes to hasten this veteran’s death or at least refer him to someone who could. Perhaps his suicide attempt on the hospice unit was, in part, a consequence of being incapable of offering such assistance. These presuppositions should be considered explicitly to better align one’s practice both with the mission of VHA and with the goals of medicine.
One way to do this is to consider whether we can cast assisted suicide as a medical therapy. Sulmasy proposes the provisional “canons of therapy” which might guide clinicians in assessing medical therapies.6 This article distinguishes 3 types of clinically and ethically distinct practices. I have split his first canon (proportionality) into 2 for the sake of clarity.
Priority: Do the benefits outweigh the burdens of the intervention?
The challenge of assessing priority when considering assisted suicide is that we cannot explain any benefits or burdens that might accrue after death; it is beyond our knowledge and informed consent is impossible. While there is always some uncertainty in discerning the benefits and burdens of an intervention, death presents an insurmountable procedural problem for informed consent to assisted suicide.
Fit: Are the means appropriate for the outcome of interest?
The outcomes of interest when considering assisted suicide are many—many—they range from symptom relief or avoidance to reclaiming dignity. In the case described by Ruskin et al, the interdisciplinary team offered the veteran a number of interventions to assuage his symptoms. Dignity therapy may have been employed as a meaningful, useful way of bringing closure to a life.7,8 Ultimately, however, some distress, particularly existential distress, may be intractable and clinicians must commit, as they did in this case, to doing what they can to remedy other symptoms and not abandon the veteran. Suicide is a tempting option because it may eliminate some of these concerns, but one must first grapple with the ethical question of whether suicide is ever an appropriate way to pursue any of these outcomes. Addressing that question is beyond the scope of this commentary, but both clinicians and patients should consider whether and why suicide should be considered appropriate and whether it is appropriate for the medical profession to assist with it.
Parsimony: Is this the least invasive, least burdensome intervention available?
In US jurisdictions where it is legal, assisted suicide is considered an intervention of last resort. Assisted suicide seems to be neither invasive (it involves taking medications) nor burdensome: the medications usually work quickly and without adverse effects, although there are risks (eg, vomiting). Broadening our view beyond the individual reveals something different.
In a cultural sense, assisted suicide is invasive. It changes how clinicians and patients consider health and medical care. We no longer have the profession of medicine with another intervention in the toolbox; we have a totally different profession which now intends death instead of health for its patients. It changes medicine and society at large profoundly. This makes it culturally invasive.
Furthermore, although the veteran in the case recurrently grappled with the choice of suicide, most people do not. They live by default. Offering assisted suicide, even in broad, general terms, may still leave them deciding to live, but the offer has also taken from them the possibility of living by default. They must justify their choice if only to themselves, considering the reasons they continue to pursue life-prolonging treatment and incur financial, emotional, and physical costs for their family. This is a dangerous cultural burden ironically imposed by the offer of more choices.9 Clinicians, by offering assisted suicide even if a patient declines it, also affirm the reasonableness of ending one’s life given the circumstances. That affirmation may be burdensome (eg, “They see my life as not worth living”) rather than validating.10
Restoration: Will this intervention help to restore the patient overall (even if not immediately)?
It would seem restoration is impossible for someone who is dying. Dying is terrible and so one possibility would be to hasten the process with assisted suicide. If health is in view, though, clinicians could recognize that restoration is always possible as long as someone is alive.
For someone dying, restoration may look like symptom relief (restoring bodily distress) which in turn may restore one’s capacity to sleep or to converse with loved ones. Assisted suicide does not fit in this paradigm. Is it intended to help patients sustain and restore their health, whatever amount they have (this is what the hospice and psychiatric services attempted to do in the case). Or is it intended to help patients pursue whatever goals seem good to the patient even those goals which conflict with health? Happily, most patients want their health sustained or restored so there is usually no conflict. As medical technology advances, though, conflicts arise: Should a clinician prescribe stimulants to enhance a healthy student’s wakefulness during final exams? Should a clinician engineer embryos to provide parents with a particular kind of child? Should a clinician end a patient’s life? Assisted suicide is obviously not aimed at restoration. It is a concession to the intractability of one’s disease and disability and one’s impending death. Without clarity and agreement on the goal of medicine, the default provision of care centers instead on satisfying patient preferences whatever they are.
Holism: Does the intervention prioritize the whole patient (vs prioritizing a part for the sake of the whole)?
Clinicians offering assisted suicide suggest that providing a death on a patient’s own terms restores autonomy and brings coherence to a life narrative that, at its end, is fraught with tragedy. This is what it looks like to honor “the whole patient.” A clinician must scrutinize that judgment to determine whether the patient meets statutory criteria for assisted suicide. The impulse underlying the moral distress described by Ruskin et al and many other clinicians is that a patient’s judgment, once determined to be sound, should trump a clinician’s judgment about what is best for the patient’s health and whether there are limits on what the clinician can do to satisfy a patient’s preferences. Ironically, assisted suicide prioritizes a patient’s judgment about how their life should end above other considerations, namely, that medicine has traditionally sought the patient’s good by sustaining and restoring their health, not by intending and causing their death. Notably, there was no lack of holism in the care provided the veteran in the case both before and after his suicide attempt.
Discretion: What are the limits of the intervention itself? What is the scope of medicine in general? What is the limit of one’s own individual knowledge and skill?
Assisted suicide has a substantial limit: it does not offer relief from suffering because there will be no one left alive to experience relief. Assisted suicide cannot achieve anything for the patient because they are dead by the time they fully receive what has been given. This profound limit makes assisted suicide unlike anything else offered in medicine and should give clinicians pause before adopting it, prompting them to grapple with whether causing a patient’s death is within the scope of medicine. If so, how did this come to be after thousands of years to the contrary across cultures and traditions, and what justifies this change? Finally, clinicians must contend with the limits of informed consent.
This brief reflection on how clinicians should consider medical therapies brings us back to MacIntyre’s exhortation: We cannot decide what to do until we have discerned the story to which we belong. One way of telling the story of medicine is to tell it with the techniques front and center: we prescribe, we operate, we irradiate, make the numbers go in the right direction, cure infections, and shrink masses. We can also tell that story by rejoicing that technology is giving us increasing control over our bodies and we can put that power to whatever use we desire. Often that will align with health, but it may not and that is for many patients increasingly acceptable. There is another, better story to tell: the profession of medicine exists to help people sustain and restore health, whatever bit of it they have and even as they lay dying. All those things just listed may help clinicians in that pursuit or they may not, given the specific context.
Ruskin et al tell a story of clinicians living in the tension of wanting to satisfy the desires their patients bring to them but must settle for the best that medicine can provide. Medical intervention as preference satisfaction is a story we have been living and practicing for 50 years since Beauchamp and Childress described the 4-principle framework for biomedical ethics: respect for autonomy, justice, nonmaleficence, beneficence.
Medicine-as-preference-satisfaction conflicts with the VHA mission to “honor America’s veterans by providing exceptional health care that improves their health and well-being.” VHA does not owe veterans whatever they request. VHA owes them exceptional health care. When a patient comes to a clinician, a clinician owes them a bounded set of things in service to their health. The dissonance a clinician might experience in trying to discern whether a patient’s death can serve that patient’s own health should signal a need to step back and reflect on how they understand the foundations of medical practice.
I do not disagree with the authors in their general approach to how clinicians might discuss this with patients who request a hastened death. I also seek to assuage symptoms, validate emotions, and remain steadfast through someone’s dying. I also affirm my commitment as a physician to care for a person’s health which, while someone is dying, usually entails managing symptoms. It never entails ending someone’s life. The clinicians in the case did an excellent job caring for this veteran and could not have done better by helping him end his life.
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
- MacIntyre A. After Virtue: A Study in Moral Theory. 3rd ed. 2007.
- Ruskin A, Bauer M, Alrojolah L. Managing requests for medical aid in dying within the US Department of Veterans Affairs Health Care System. Fed Pract. 2026;43:238-242. doi:10.12788/fp.0739
- VHA Directive 1139: Palliative care consult teams and Veterans Integrated Service Network Leads. September 9, 2022. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9930
- Assisted Suicide Funding Restriction Act of 1997. 42 USC § 14401.
- Safranek JP. Autonomy and assisted suicide the execution of freedom. Hastings Cent Rep. 1998;28:32-36. doi:10.2307/3528611
- Sulmasy DP. The last low whispers of our dead: when is it ethically justifiable to render a patient unconscious until death? Theor Med Bioeth. 2018;39:233-263. doi:10.1007/s11017-018-9459-7
- Chochinov HM. Dying, Dignity, and new horizons in palliative end-of-life care. CA Cancer J Clin. 2006;56:84-103. doi:10.3322/canjclin.56.2.84
- Chochinov HM. Intensive caring: reminding families they matter. J Palliat Med. 2024;27:152-155.
- Velleman JD. Against the right to die. J Med Philos. 1992;17:665-681.
- Peace WJ. Comfort Care as Denial of Personhood. Hastings Cent Rep. 2012;42:14-17. doi:10.1002/hast.38
What They Want and What They Need: The End-of-Life Conflict
What They Want and What They Need: The End-of-Life Conflict
A Cost-Effectiveness and Psychological Evaluation of Early Skin Biopsies vs Later-Onset Surgeries in Melanoma Management
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Practice Points
- Early melanoma detection via skin biopsy is generally more cost-effective than managing advanced-stage disease, largely due to the high costs associated with systemic therapies (eg, immunotherapy) used in later-stage melanoma.
- Earlier diagnosis is associated with improved patient outcomes, including better quality of life and reduced psychological distress, compared with later-stage melanoma diagnoses requiring more extensive intervention.
- Integrated prevention and early detection strategies—such as dermoscopy, teledermoscopy, and public health initiatives—may optimize melanoma outcomes while reducing overall health care expenditures.