User login
Hospitalists Can Address Causes of Skyrocketing Health Care Costs


Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”

—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.

—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Hospitalists Applaud Stress-Free CME Sessions, MOC Training at HM13




Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Behavioral Economics Can Accelerate Adoption of Choosing Wisely Campaign

SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
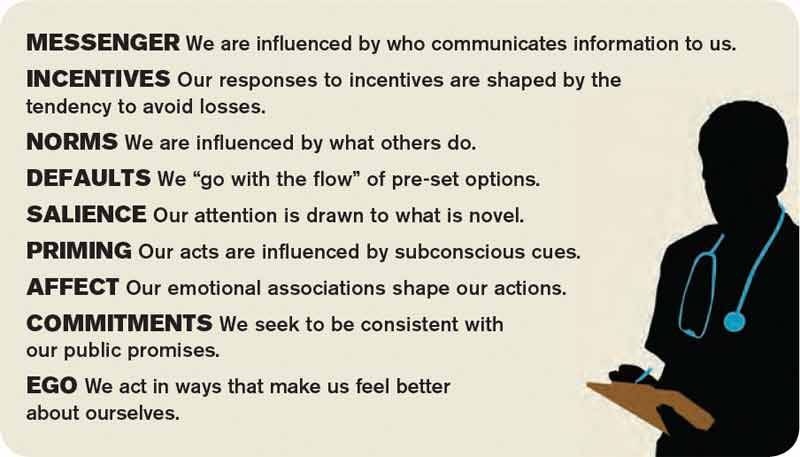
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
What Is the Best Management of Hereditary Angioedema?

Case
A 36-year-old man with a known history of hereditary angioedema (HAE) presents with severe orofacial swelling and laryngeal angioedema, requiring expectant management, including endotracheal intubation. His previous angioedema (AE) episodes involved his hands, feet, and genitalia; episodes generally occurred after physical trauma. Ten years prior to admission, he had an episode of secondary small bowel obstruction. The patient had been prescribed prophylactic danazol (Danacrine) 100 mg BID but he had gradually been reducing the dosage due to mood changes; at the time of presentation, he had already tapered to 100 mg danazol three times per week (Monday, Wednesday, and Friday).
Overview
HAE is an autosomal dominant condition characterized by localized, episodic swelling of the deeper dermal layers and/or mucosal tissue. Its acute presentation can vary in severity; presentations can be lethal.
HAE is generally unresponsive to conventional treatments used for other causes of AE (e.g. food or drug reactions) including glucocorticoids, antihistamines, and epinephrine. The pharmacologic treatment of acute attacks, as well as for short- and long-term prophylaxis of HAE, has evolved significantly in recent years and now includes several forms of C1 inhibitor (C1INH) protein replacement, as well as a bradykinin antagonist, and a kallikrein inhibitor.
Review of the Data
Epidemiology. HAE is an autosomal dominant disease with prevalence in the U.S. of 1 in 10,000 to 1 in 50,000 patients. All ethnic groups are equally affected, with no gender predilection. In most cases, a positive family history is present; however, in 25% of cases, spontaneous mutations occur such that an unremarkable family history does not rule out the diagnosis.1
Pathophysiology. In the past decade, there has been substantial advancement in our understanding of HAE pathophysiology. HAE occurs as a result of functional or quantitative C1 esterase inhibitor (C1INH) deficiency.
C1INH belongs to a group of proteins known as serpins (serine protease inhibitors). The C1INH gene is located on chromosome 11, and has several polymorphic sites, which predispose to spontaneous mutations.1
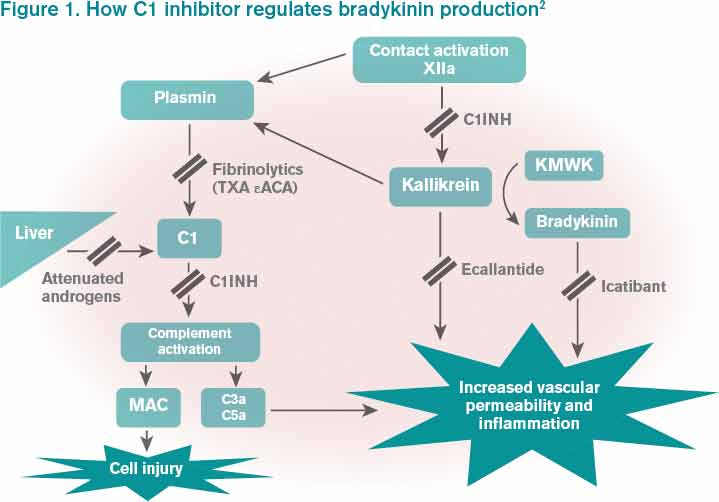
Bradykinin is the core bioactive mediator, which causes vasodilation, smooth muscle contraction, and subsequent edema.1 C1INH regulates bradykinin production by blocking kallikrein’s conversion of factor XII into XIIa, prekallikrein to kallikrein, and cleavage of high-molecular-weight kininogen by activated kallikrein to form bradykinin (see Figure 1).1,2
Clinical Manifestations
HAE is characterized by recurrent episodes of swelling, the frequency and severity of which are quite variable. Virtually all HAE patients have abdominal- and extremity-swelling episodes, and 50% will have episodes of laryngeal swelling; other involved areas might include the face, oropharynx, and genitalia.4 These episodes are usually unilateral; edema is nonpruritic, nonpitting, and often painless. Episodes involving the oropharynx, larynx, and abdomen can be associated with potentially serious morbidity and mortality.1, 3
HAE episodes usually commence during late childhood and early puberty (on average at age 11). Approximately half of HAE patients will have oropharyngeal involvement that might occur many years, even decades, after the initial onset of the disease. The annual rate of severe, life-threatening laryngeal edema was 0.9% in a recent retrospective study.4
Severity of the disease is variable. Attacks are episodic, and occur on average every 10 to 20 days in untreated patients. These attacks typically peak over 24 hours, then usually resolve after 48 to 72 hours. However, the complete resolution of signs and symptoms can last for up to one week after the attacks.5
There is no concomitant pruritus or urticaria that accompanies the AE. However, erythema marginatum, an evanescent nonpruritic rash with serpiginous borders involving the trunk and inner surface of extremities but sparing the face, might herald the onset of an episode. This rash usually has central pallor that blanches with pressure and worsens with heat.
HAE can be triggered by stressful events, including trauma, surgery, menstruation, and viral infections. However, in many instances, HAE attacks occur without an identifiable cause.5
Differential Diagnosis from Other Causes of Angioedema
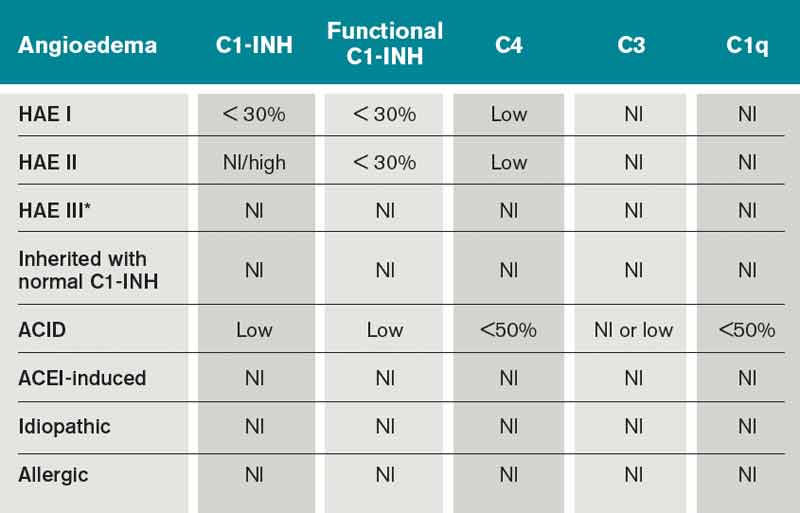
Type I HAE is characterized by a quantitative C1INH deficiency (which is functionally abnormal as well), and occurs in 85% of patients. Type II HAE occurs in 15% of patients, and results from a functionally abnormal C1INH.
In patients with Type I and II HAE, as well as acquired C1 inhibitor deficiency (ACID), C4 levels are low during and between attacks. C2 levels are also low during acute attacks. In ACID, levels of C1q are also reduced; these patients require further workup to rule out an undiagnosed malignancy or an autoimmune process. In contrast, patients with ACE-induced, idiopathic, and allergic AE have normal complement profiles.3,6
Type III is a more recently described type of HAE that is rare, not well understood, and generally affects women.3,6 Clinically, it resembles Type I and Type II HAE but complement levels, including C1 inhibitor, are normal (see Table 1).
Treatment
HAE types I, II, III, and ACID are generally unresponsive to glucocorticoids, antihistamines, and epinephrine. These forms of AE may be exacerbated by exogenous estrogen.1,8 For this reason, HAE patients should avoid oral hormonal contraception and estrogen replacement therapy. In addition, ACE inhibitors should also be avoided based on their effect on bradykinin degradation.
Until the introduction of newer therapeutic choices, as noted in our case, the treatment of acute attacks of AE was essentially supportive. Patients with impending laryngeal obstruction were managed with intubation prior to progression of the AE to limit airway patency. Prior to the modern era, a substantial proportion of HAE patients died of asphyxiation.
Fresh frozen plasma (FFP) has been used to treat acute HAE attacks, but given its content of contact system proteins (in addition to C1INH), FFP might also pose a risk for worsening of HAE; for this reason, it must be given cautiously to patients who are symptomatic.9
In the past decade, there has been significant progress in the available treatments for HAE. Currently in the U.S., there are several agents recently approved by, or have pending approvals from, the FDA, including several forms of C1INH replacement, a bradykinin antagonist, and a kallikrein inhibitor.
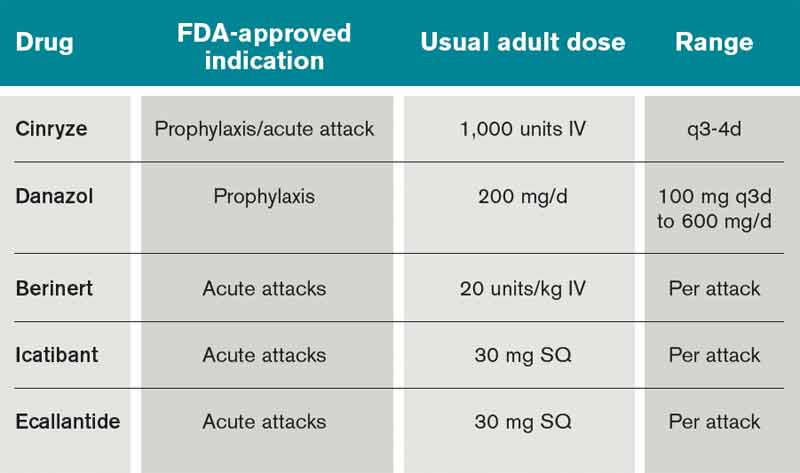
The C1 esterase inhibitor (human) drugs are administered intravenously; both have been shown to be efficacious and safe. Nanofiltered C1 inhibitor provided relief in a median time of two hours when used acutely; when used as prophylaxis, it decreased the number of attacks in a three-month period by 50% (six vs. 12 with placebo, P<0.001).11
The other C1INH is rhucin, still not approved in U.S. This drug is characterized by a short half-life (approximately two to four hours) compared with the plasma-derived C1INH agents (24 to 48 hours). It is contraindicated in patients with rabbit hypersensitivity, as it is purified from rabbit breast milk.10
Ecallantide is a kallikrein inhibitor for acute therapy that is administered via three subcutaneous injections. This agent has been linked to allergic/anaphylactic reactions in a minority of patients (approximately 4%); therefore, it should be administered cautiously, by a health-care provider, and in a setting where anaphylaxis can be successfully managed.12 Icatibant is a bradykinin antagonist recently approved in the U.S. and administered SC via a single injection.10
In light of the development of these new agents, there is a need for updated guidelines for the long- and short-term prophylaxis and acute management of HAE. A recent guideline focused on the management of HAE in gynecologic and obstetric patients recommended the use of plasma-derived C1INH C1 esterase inhibitor (human) (Cinryze) for short- and long-term prophylaxis and acute treatment of HAE.13 The effect of pregnancy on HAE is variable: Some women worsen and other women have less swelling during their pregnancy. Swelling at the time of parturition is rare; however, the risk rises during the post-partum period.
Type III HAE. An additional form of HAE has been recognized with a pattern of AE episodes that mimics Type I or Type II HAE but with unremarkable laboratory studies of the complement cascade, including C1 inhibitor level and function. At this time, there is no laboratory test with which a diagnosis of Type III HAE can be confirmed. The diagnosis should be suspected in patients with a strong family history of AE reflecting autosomal dominant inheritance. In some, but not all, cases, the condition is manifest in association with high estrogen levels (e.g. pregnancy or administration of oral contraceptives). Type III HAE patients have a salutary response to the same agents that are efficacious for Type I and II HAE.
Acquired C1 inhibitor deficiency (ACID). ACID generally occurs in adults and is clinically indistinguishable from HAE. ACID is not associated with a remarkable family history of AE. In contrast to HAE, this is a consumptive deficiency of C1 inhibitor and results from enhanced catabolism that exceeds the capacity for regenerating C1 inhibitor protein. It is often associated with neoplastic (usually lymphoproliferative) or autoimmune disorders; treatment of the underlying condition frequently leads to improvement in ACID. Although its management is similar to HAE, it tends to be more responsive to anti-fibrinolytics. A salutary response to C1INH replacement therapy might not occur in patients with autoantibodies to C1 inhibitor, but efficacy of ecallantide and icatibant for the treatment of acquired AE has been reported.14, 15
ACEI angioedema. Treatment with angiotensin-converting enzyme inhibitors (ACE-I) has been associated with recurrent AE without urticaria in 0.1 to 0.7% of patients exposed to these drugs.16 Angioedema from ACE-I more frequently occurs within the first few months of therapy, but it might occur even after years of continuous therapy. ACEI-induced AE is secondary to impaired degradation of bradykinin. The main treatment is to discontinue the offending agent and avoid all other ACE-I, as this is a class-specific reaction.17
Angiotensin receptor blockers (ARBs) have been associated less commonly with AE. The mechanism for ARB-associated AE has not been elucidated. A meta-analysis showed that in 2% to 17% of patients who were switched to ARBs, recurrence of AE was observed.18 From the pooling of these data with two randomized controlled trials, it is estimated that approximately 10% or less of patients with ACEI-associated AE who switched to ARBs will develop AE.19 In the majority of cases, patients can be switched to ARBs with no recurrence of AE; however, the decision to prescribe an ARB to a patient who has had AE while receiving ACEI should be made carefully on an individualized risk/benefit basis.19
Preventive Treatment
The 17 α-alkylated androgens that can be used for treatment of HAE are danazol (Danacrine), stanozolol (Winstrol), oxandralone (Oxandrine) and methyltestosterone (Android). In patients with HAE, attenuated androgens can significantly reduce the frequency and severity of attacks; however, their use is limited by risk for untoward effects (virilization, abnormal liver function tests, change in libido, anxiety, etc.).21 There is also a risk for hepatotoxicity, including development of hepatic adenomas and hepatic carcinoma.
Antifibrinolytics also may have efficacy for HAE, but these agents have been associated with a variety of adverse effects, including nausea and diarrhea, postural hypotension, fatigue, enhanced thrombosis, retinal changes, and teratogenicity.8, 22, 23
In 2009, long-term prophylaxis with C1-INH concentrate was recommended for patients with HAE with frequent or disabling attacks, a history of laryngeal attacks, and poor quality of life. The 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of HAE recommended long-term prophylaxis in patients with more than one monthly severe HAE attack, more than five days of disability per month, or any history of airway compromise.24, 25
The decision to prescribe long-term prophylaxis, and the dose/frequency of medication required, should be individualized based on clinical parameters, such as frequency and severity of attacks, and not on C1 INH or C4 levels.
Perioperative Considerations
It is well established that any trauma, including dental procedures or surgery, can precipitate HAE attacks. For this reason, short-term prophylactic treatment in HAE patients undergoing procedures is recommended. Ideally, avoiding endotracheal intubation is the best approach; however, if intubation cannot be avoided, then adequate prophylaxis should be administered.2
Attenuated androgens can be given up to seven days before a procedure, or C1 INH can be administered 24 hours in advance. If C1 INH is unavailable, FFP can be given six to 12 hours in advance in patients who are not symptomatic; in case of endotracheal intubation, either FFP or C1 INH should be administered immediately before.2
Several case reports in multiple specialty surgical patients (abdominal surgery, cardiopulmonary bypass, orthopedic surgery, etc.) have confirmed the successful use of C1 INH in the prevention of acute attacks with favorable outcomes.2
There is no need to follow C1 INH levels, as it has no clinical relevance.
Back to the Case
The patient was admitted to the ICU and received a total of eight units of FFP. He was transferred to our institution and was able to be extubated three days after initial presentation. Laboratory studies revealed C4 10mg/dL and C1 esterase inhibitor 10mg/dL (both low).
Danazol was resumed. However, within several months after discharge, Cinryze became available in the U.S. market and was eventually prescribed. The patient has not had further significant attacks requiring inpatient management.
Dr. Auron is an assistant professor of medicine and pediatrics at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University. Dr. Lang is co-director of the Asthma Center and director of the Allergy/Immunology Fellowship Training Program at the Cleveland Clinic.
References
- Bernstein, JA. Update on angioedema: evaluation, diagnosis, and treatment. Allergy Asthma Proc. 2011;32(6):408-412.
- Levy JH, Freiberger DJ, Roback J. Hereditary angioedema: current and emerging treatment options. Anesth Analg. 2010;110(5):1271-1280.
- Busse PJ. Angioedema: Differential diagnosis and treatment. Allergy Asthma Proc. 2011;32:Suppl 1:S3-S11.
- Khan DA. Hereditary angioedema: historical aspects, classification, pathophysiology, clinical presentation, and laboratory diagnosis. Allergy Asthma Proc. 2011;32(1):1-10.
- Bork K, Meng G, Staubach P, Hardt, J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119(3):267-274.
- Zuraw BL, Christiansen SC. Pathogenesis and laboratory diagnosis of hereditary angioedema. Allergy Asthma Proc. 2009;30:487-492.
- Frazer-Abel A, Giclas PC. Update on laboratory tests for the diagnosis and differentiation of hereditary angioedema and acquired angioedema. Allergy Asthma Proc. 2011;32:Suppl 1:S17-S21.
- Banerjee A. Current treatment of hereditary angioedema: an update on clinical studies. Allergy Asthma Proc. 2010;31:398-406.
- Donaldson VH. Therapy of "the neurotic edema." N Engl J Med. 1972;286(15):835-836.
- Riedl MA. Update on the acute treatment of hereditary angioedema. Allergy Asthma Proc. 2011;32:11-16.
- Zuraw BL, Busse PJ, White M, et al. Nanofiltered C1 inhibitor concentrate for treatment of hereditary angioedema. N Engl J Med. 2010;363:513-522.
- Cicardi M, Levy RJ, McNeil DL. Ecallantide for the treatment of acute attacks in hereditary angioedema. N Engl J Med. 2010;363:523-531.
- Caballero T, Farkas H, Bouillet L, et al. International consensus and practical guidelines on the gynecologic and obstetric management of female patients with hereditary angioedema caused by C1 inhibitor deficiency. J Allergy Clin Immunol. 2012;129(2):308-320.
- Cicardi M, Zanichelli A. Acquired angioedema. J Allergy Clin Immunol. 2010;6(1):14.
- Zanichelli A, Badini M, Nataloni I, Montano N, Cicardi M. Treatment of acquired angioedema with icatibant: a case report. Intern Emerg Med. 2011;6(3):279-280.
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Haymore BR, Yoon J, Mikita CP, Klote MM, DeZee KJ. Risk of angioedema with angiotensin receptor blockers in patients with prior angioedema associated with angiotensin-converting enzyme inhibitors: a meta-analysis. Ann Allergy Asthma Immunol. 2008;101(5):495-499.
- Beavers CJ, Dunn SP, Macaulay TE. The role of angiotensin receptor blockers in patients with angiotensin-converting enzyme inhibitor-induced angioedema. Ann Pharmacother. 2011;45(4):520-524.
- Nzeako UC. Diagnosis and management of angioedema with abdominal involvement: a gastroenterology perspective. World J Gastroenterol. 2010; 16(39):4913-4921.
- Banerji A, Sloane DE, Sheffer AL. Hereditary angioedema: a current state-of-the-art review, V: attenuated androgens for the treatment of hereditary angioedema. Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S19-22.
- Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008; 359(10):1027-1036.
- Zuraw BL. Hereditary angioedema: a current state-of-the-art review, IV: short- and long-term treatment of hereditary angioedema: out with the old and in with the new? Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S13-S18.
- Bowen T, Cicardi M, Bork K, et al. Hereditary angioedema: a current state-of-the-art review, VII: Canadian Hungarian 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of Hereditary Angioedema. Ann Allergy Asthma Immunol. 2008;100(1)(Suppl 2):S30-40.
- Craig T, Riedl M, Dykewicz M, et al. When is prophylaxis for hereditary angioedema necessary? Ann Allergy Asthma Immunol. 2009.102(5):366-372.
- Frank MM. Update on preventive therapy (prophylaxis) of hereditary angioedema. Allergy Asthma Proc. 2011;32(1):17-21.
Case
A 36-year-old man with a known history of hereditary angioedema (HAE) presents with severe orofacial swelling and laryngeal angioedema, requiring expectant management, including endotracheal intubation. His previous angioedema (AE) episodes involved his hands, feet, and genitalia; episodes generally occurred after physical trauma. Ten years prior to admission, he had an episode of secondary small bowel obstruction. The patient had been prescribed prophylactic danazol (Danacrine) 100 mg BID but he had gradually been reducing the dosage due to mood changes; at the time of presentation, he had already tapered to 100 mg danazol three times per week (Monday, Wednesday, and Friday).
Overview
HAE is an autosomal dominant condition characterized by localized, episodic swelling of the deeper dermal layers and/or mucosal tissue. Its acute presentation can vary in severity; presentations can be lethal.
HAE is generally unresponsive to conventional treatments used for other causes of AE (e.g. food or drug reactions) including glucocorticoids, antihistamines, and epinephrine. The pharmacologic treatment of acute attacks, as well as for short- and long-term prophylaxis of HAE, has evolved significantly in recent years and now includes several forms of C1 inhibitor (C1INH) protein replacement, as well as a bradykinin antagonist, and a kallikrein inhibitor.
Review of the Data
Epidemiology. HAE is an autosomal dominant disease with prevalence in the U.S. of 1 in 10,000 to 1 in 50,000 patients. All ethnic groups are equally affected, with no gender predilection. In most cases, a positive family history is present; however, in 25% of cases, spontaneous mutations occur such that an unremarkable family history does not rule out the diagnosis.1
Pathophysiology. In the past decade, there has been substantial advancement in our understanding of HAE pathophysiology. HAE occurs as a result of functional or quantitative C1 esterase inhibitor (C1INH) deficiency.
C1INH belongs to a group of proteins known as serpins (serine protease inhibitors). The C1INH gene is located on chromosome 11, and has several polymorphic sites, which predispose to spontaneous mutations.1
Bradykinin is the core bioactive mediator, which causes vasodilation, smooth muscle contraction, and subsequent edema.1 C1INH regulates bradykinin production by blocking kallikrein’s conversion of factor XII into XIIa, prekallikrein to kallikrein, and cleavage of high-molecular-weight kininogen by activated kallikrein to form bradykinin (see Figure 1).1,2
Clinical Manifestations
HAE is characterized by recurrent episodes of swelling, the frequency and severity of which are quite variable. Virtually all HAE patients have abdominal- and extremity-swelling episodes, and 50% will have episodes of laryngeal swelling; other involved areas might include the face, oropharynx, and genitalia.4 These episodes are usually unilateral; edema is nonpruritic, nonpitting, and often painless. Episodes involving the oropharynx, larynx, and abdomen can be associated with potentially serious morbidity and mortality.1, 3
HAE episodes usually commence during late childhood and early puberty (on average at age 11). Approximately half of HAE patients will have oropharyngeal involvement that might occur many years, even decades, after the initial onset of the disease. The annual rate of severe, life-threatening laryngeal edema was 0.9% in a recent retrospective study.4
Severity of the disease is variable. Attacks are episodic, and occur on average every 10 to 20 days in untreated patients. These attacks typically peak over 24 hours, then usually resolve after 48 to 72 hours. However, the complete resolution of signs and symptoms can last for up to one week after the attacks.5
There is no concomitant pruritus or urticaria that accompanies the AE. However, erythema marginatum, an evanescent nonpruritic rash with serpiginous borders involving the trunk and inner surface of extremities but sparing the face, might herald the onset of an episode. This rash usually has central pallor that blanches with pressure and worsens with heat.
HAE can be triggered by stressful events, including trauma, surgery, menstruation, and viral infections. However, in many instances, HAE attacks occur without an identifiable cause.5
Differential Diagnosis from Other Causes of Angioedema
Type I HAE is characterized by a quantitative C1INH deficiency (which is functionally abnormal as well), and occurs in 85% of patients. Type II HAE occurs in 15% of patients, and results from a functionally abnormal C1INH.
In patients with Type I and II HAE, as well as acquired C1 inhibitor deficiency (ACID), C4 levels are low during and between attacks. C2 levels are also low during acute attacks. In ACID, levels of C1q are also reduced; these patients require further workup to rule out an undiagnosed malignancy or an autoimmune process. In contrast, patients with ACE-induced, idiopathic, and allergic AE have normal complement profiles.3,6
Type III is a more recently described type of HAE that is rare, not well understood, and generally affects women.3,6 Clinically, it resembles Type I and Type II HAE but complement levels, including C1 inhibitor, are normal (see Table 1).
Treatment
HAE types I, II, III, and ACID are generally unresponsive to glucocorticoids, antihistamines, and epinephrine. These forms of AE may be exacerbated by exogenous estrogen.1,8 For this reason, HAE patients should avoid oral hormonal contraception and estrogen replacement therapy. In addition, ACE inhibitors should also be avoided based on their effect on bradykinin degradation.
Until the introduction of newer therapeutic choices, as noted in our case, the treatment of acute attacks of AE was essentially supportive. Patients with impending laryngeal obstruction were managed with intubation prior to progression of the AE to limit airway patency. Prior to the modern era, a substantial proportion of HAE patients died of asphyxiation.
Fresh frozen plasma (FFP) has been used to treat acute HAE attacks, but given its content of contact system proteins (in addition to C1INH), FFP might also pose a risk for worsening of HAE; for this reason, it must be given cautiously to patients who are symptomatic.9
In the past decade, there has been significant progress in the available treatments for HAE. Currently in the U.S., there are several agents recently approved by, or have pending approvals from, the FDA, including several forms of C1INH replacement, a bradykinin antagonist, and a kallikrein inhibitor.
The C1 esterase inhibitor (human) drugs are administered intravenously; both have been shown to be efficacious and safe. Nanofiltered C1 inhibitor provided relief in a median time of two hours when used acutely; when used as prophylaxis, it decreased the number of attacks in a three-month period by 50% (six vs. 12 with placebo, P<0.001).11
The other C1INH is rhucin, still not approved in U.S. This drug is characterized by a short half-life (approximately two to four hours) compared with the plasma-derived C1INH agents (24 to 48 hours). It is contraindicated in patients with rabbit hypersensitivity, as it is purified from rabbit breast milk.10
Ecallantide is a kallikrein inhibitor for acute therapy that is administered via three subcutaneous injections. This agent has been linked to allergic/anaphylactic reactions in a minority of patients (approximately 4%); therefore, it should be administered cautiously, by a health-care provider, and in a setting where anaphylaxis can be successfully managed.12 Icatibant is a bradykinin antagonist recently approved in the U.S. and administered SC via a single injection.10
In light of the development of these new agents, there is a need for updated guidelines for the long- and short-term prophylaxis and acute management of HAE. A recent guideline focused on the management of HAE in gynecologic and obstetric patients recommended the use of plasma-derived C1INH C1 esterase inhibitor (human) (Cinryze) for short- and long-term prophylaxis and acute treatment of HAE.13 The effect of pregnancy on HAE is variable: Some women worsen and other women have less swelling during their pregnancy. Swelling at the time of parturition is rare; however, the risk rises during the post-partum period.
Type III HAE. An additional form of HAE has been recognized with a pattern of AE episodes that mimics Type I or Type II HAE but with unremarkable laboratory studies of the complement cascade, including C1 inhibitor level and function. At this time, there is no laboratory test with which a diagnosis of Type III HAE can be confirmed. The diagnosis should be suspected in patients with a strong family history of AE reflecting autosomal dominant inheritance. In some, but not all, cases, the condition is manifest in association with high estrogen levels (e.g. pregnancy or administration of oral contraceptives). Type III HAE patients have a salutary response to the same agents that are efficacious for Type I and II HAE.
Acquired C1 inhibitor deficiency (ACID). ACID generally occurs in adults and is clinically indistinguishable from HAE. ACID is not associated with a remarkable family history of AE. In contrast to HAE, this is a consumptive deficiency of C1 inhibitor and results from enhanced catabolism that exceeds the capacity for regenerating C1 inhibitor protein. It is often associated with neoplastic (usually lymphoproliferative) or autoimmune disorders; treatment of the underlying condition frequently leads to improvement in ACID. Although its management is similar to HAE, it tends to be more responsive to anti-fibrinolytics. A salutary response to C1INH replacement therapy might not occur in patients with autoantibodies to C1 inhibitor, but efficacy of ecallantide and icatibant for the treatment of acquired AE has been reported.14, 15
ACEI angioedema. Treatment with angiotensin-converting enzyme inhibitors (ACE-I) has been associated with recurrent AE without urticaria in 0.1 to 0.7% of patients exposed to these drugs.16 Angioedema from ACE-I more frequently occurs within the first few months of therapy, but it might occur even after years of continuous therapy. ACEI-induced AE is secondary to impaired degradation of bradykinin. The main treatment is to discontinue the offending agent and avoid all other ACE-I, as this is a class-specific reaction.17
Angiotensin receptor blockers (ARBs) have been associated less commonly with AE. The mechanism for ARB-associated AE has not been elucidated. A meta-analysis showed that in 2% to 17% of patients who were switched to ARBs, recurrence of AE was observed.18 From the pooling of these data with two randomized controlled trials, it is estimated that approximately 10% or less of patients with ACEI-associated AE who switched to ARBs will develop AE.19 In the majority of cases, patients can be switched to ARBs with no recurrence of AE; however, the decision to prescribe an ARB to a patient who has had AE while receiving ACEI should be made carefully on an individualized risk/benefit basis.19
Preventive Treatment
The 17 α-alkylated androgens that can be used for treatment of HAE are danazol (Danacrine), stanozolol (Winstrol), oxandralone (Oxandrine) and methyltestosterone (Android). In patients with HAE, attenuated androgens can significantly reduce the frequency and severity of attacks; however, their use is limited by risk for untoward effects (virilization, abnormal liver function tests, change in libido, anxiety, etc.).21 There is also a risk for hepatotoxicity, including development of hepatic adenomas and hepatic carcinoma.
Antifibrinolytics also may have efficacy for HAE, but these agents have been associated with a variety of adverse effects, including nausea and diarrhea, postural hypotension, fatigue, enhanced thrombosis, retinal changes, and teratogenicity.8, 22, 23
In 2009, long-term prophylaxis with C1-INH concentrate was recommended for patients with HAE with frequent or disabling attacks, a history of laryngeal attacks, and poor quality of life. The 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of HAE recommended long-term prophylaxis in patients with more than one monthly severe HAE attack, more than five days of disability per month, or any history of airway compromise.24, 25
The decision to prescribe long-term prophylaxis, and the dose/frequency of medication required, should be individualized based on clinical parameters, such as frequency and severity of attacks, and not on C1 INH or C4 levels.
Perioperative Considerations
It is well established that any trauma, including dental procedures or surgery, can precipitate HAE attacks. For this reason, short-term prophylactic treatment in HAE patients undergoing procedures is recommended. Ideally, avoiding endotracheal intubation is the best approach; however, if intubation cannot be avoided, then adequate prophylaxis should be administered.2
Attenuated androgens can be given up to seven days before a procedure, or C1 INH can be administered 24 hours in advance. If C1 INH is unavailable, FFP can be given six to 12 hours in advance in patients who are not symptomatic; in case of endotracheal intubation, either FFP or C1 INH should be administered immediately before.2
Several case reports in multiple specialty surgical patients (abdominal surgery, cardiopulmonary bypass, orthopedic surgery, etc.) have confirmed the successful use of C1 INH in the prevention of acute attacks with favorable outcomes.2
There is no need to follow C1 INH levels, as it has no clinical relevance.
Back to the Case
The patient was admitted to the ICU and received a total of eight units of FFP. He was transferred to our institution and was able to be extubated three days after initial presentation. Laboratory studies revealed C4 10mg/dL and C1 esterase inhibitor 10mg/dL (both low).
Danazol was resumed. However, within several months after discharge, Cinryze became available in the U.S. market and was eventually prescribed. The patient has not had further significant attacks requiring inpatient management.
Dr. Auron is an assistant professor of medicine and pediatrics at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University. Dr. Lang is co-director of the Asthma Center and director of the Allergy/Immunology Fellowship Training Program at the Cleveland Clinic.
References
- Bernstein, JA. Update on angioedema: evaluation, diagnosis, and treatment. Allergy Asthma Proc. 2011;32(6):408-412.
- Levy JH, Freiberger DJ, Roback J. Hereditary angioedema: current and emerging treatment options. Anesth Analg. 2010;110(5):1271-1280.
- Busse PJ. Angioedema: Differential diagnosis and treatment. Allergy Asthma Proc. 2011;32:Suppl 1:S3-S11.
- Khan DA. Hereditary angioedema: historical aspects, classification, pathophysiology, clinical presentation, and laboratory diagnosis. Allergy Asthma Proc. 2011;32(1):1-10.
- Bork K, Meng G, Staubach P, Hardt, J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119(3):267-274.
- Zuraw BL, Christiansen SC. Pathogenesis and laboratory diagnosis of hereditary angioedema. Allergy Asthma Proc. 2009;30:487-492.
- Frazer-Abel A, Giclas PC. Update on laboratory tests for the diagnosis and differentiation of hereditary angioedema and acquired angioedema. Allergy Asthma Proc. 2011;32:Suppl 1:S17-S21.
- Banerjee A. Current treatment of hereditary angioedema: an update on clinical studies. Allergy Asthma Proc. 2010;31:398-406.
- Donaldson VH. Therapy of "the neurotic edema." N Engl J Med. 1972;286(15):835-836.
- Riedl MA. Update on the acute treatment of hereditary angioedema. Allergy Asthma Proc. 2011;32:11-16.
- Zuraw BL, Busse PJ, White M, et al. Nanofiltered C1 inhibitor concentrate for treatment of hereditary angioedema. N Engl J Med. 2010;363:513-522.
- Cicardi M, Levy RJ, McNeil DL. Ecallantide for the treatment of acute attacks in hereditary angioedema. N Engl J Med. 2010;363:523-531.
- Caballero T, Farkas H, Bouillet L, et al. International consensus and practical guidelines on the gynecologic and obstetric management of female patients with hereditary angioedema caused by C1 inhibitor deficiency. J Allergy Clin Immunol. 2012;129(2):308-320.
- Cicardi M, Zanichelli A. Acquired angioedema. J Allergy Clin Immunol. 2010;6(1):14.
- Zanichelli A, Badini M, Nataloni I, Montano N, Cicardi M. Treatment of acquired angioedema with icatibant: a case report. Intern Emerg Med. 2011;6(3):279-280.
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Haymore BR, Yoon J, Mikita CP, Klote MM, DeZee KJ. Risk of angioedema with angiotensin receptor blockers in patients with prior angioedema associated with angiotensin-converting enzyme inhibitors: a meta-analysis. Ann Allergy Asthma Immunol. 2008;101(5):495-499.
- Beavers CJ, Dunn SP, Macaulay TE. The role of angiotensin receptor blockers in patients with angiotensin-converting enzyme inhibitor-induced angioedema. Ann Pharmacother. 2011;45(4):520-524.
- Nzeako UC. Diagnosis and management of angioedema with abdominal involvement: a gastroenterology perspective. World J Gastroenterol. 2010; 16(39):4913-4921.
- Banerji A, Sloane DE, Sheffer AL. Hereditary angioedema: a current state-of-the-art review, V: attenuated androgens for the treatment of hereditary angioedema. Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S19-22.
- Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008; 359(10):1027-1036.
- Zuraw BL. Hereditary angioedema: a current state-of-the-art review, IV: short- and long-term treatment of hereditary angioedema: out with the old and in with the new? Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S13-S18.
- Bowen T, Cicardi M, Bork K, et al. Hereditary angioedema: a current state-of-the-art review, VII: Canadian Hungarian 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of Hereditary Angioedema. Ann Allergy Asthma Immunol. 2008;100(1)(Suppl 2):S30-40.
- Craig T, Riedl M, Dykewicz M, et al. When is prophylaxis for hereditary angioedema necessary? Ann Allergy Asthma Immunol. 2009.102(5):366-372.
- Frank MM. Update on preventive therapy (prophylaxis) of hereditary angioedema. Allergy Asthma Proc. 2011;32(1):17-21.
Case
A 36-year-old man with a known history of hereditary angioedema (HAE) presents with severe orofacial swelling and laryngeal angioedema, requiring expectant management, including endotracheal intubation. His previous angioedema (AE) episodes involved his hands, feet, and genitalia; episodes generally occurred after physical trauma. Ten years prior to admission, he had an episode of secondary small bowel obstruction. The patient had been prescribed prophylactic danazol (Danacrine) 100 mg BID but he had gradually been reducing the dosage due to mood changes; at the time of presentation, he had already tapered to 100 mg danazol three times per week (Monday, Wednesday, and Friday).
Overview
HAE is an autosomal dominant condition characterized by localized, episodic swelling of the deeper dermal layers and/or mucosal tissue. Its acute presentation can vary in severity; presentations can be lethal.
HAE is generally unresponsive to conventional treatments used for other causes of AE (e.g. food or drug reactions) including glucocorticoids, antihistamines, and epinephrine. The pharmacologic treatment of acute attacks, as well as for short- and long-term prophylaxis of HAE, has evolved significantly in recent years and now includes several forms of C1 inhibitor (C1INH) protein replacement, as well as a bradykinin antagonist, and a kallikrein inhibitor.
Review of the Data
Epidemiology. HAE is an autosomal dominant disease with prevalence in the U.S. of 1 in 10,000 to 1 in 50,000 patients. All ethnic groups are equally affected, with no gender predilection. In most cases, a positive family history is present; however, in 25% of cases, spontaneous mutations occur such that an unremarkable family history does not rule out the diagnosis.1
Pathophysiology. In the past decade, there has been substantial advancement in our understanding of HAE pathophysiology. HAE occurs as a result of functional or quantitative C1 esterase inhibitor (C1INH) deficiency.
C1INH belongs to a group of proteins known as serpins (serine protease inhibitors). The C1INH gene is located on chromosome 11, and has several polymorphic sites, which predispose to spontaneous mutations.1
Bradykinin is the core bioactive mediator, which causes vasodilation, smooth muscle contraction, and subsequent edema.1 C1INH regulates bradykinin production by blocking kallikrein’s conversion of factor XII into XIIa, prekallikrein to kallikrein, and cleavage of high-molecular-weight kininogen by activated kallikrein to form bradykinin (see Figure 1).1,2
Clinical Manifestations
HAE is characterized by recurrent episodes of swelling, the frequency and severity of which are quite variable. Virtually all HAE patients have abdominal- and extremity-swelling episodes, and 50% will have episodes of laryngeal swelling; other involved areas might include the face, oropharynx, and genitalia.4 These episodes are usually unilateral; edema is nonpruritic, nonpitting, and often painless. Episodes involving the oropharynx, larynx, and abdomen can be associated with potentially serious morbidity and mortality.1, 3
HAE episodes usually commence during late childhood and early puberty (on average at age 11). Approximately half of HAE patients will have oropharyngeal involvement that might occur many years, even decades, after the initial onset of the disease. The annual rate of severe, life-threatening laryngeal edema was 0.9% in a recent retrospective study.4
Severity of the disease is variable. Attacks are episodic, and occur on average every 10 to 20 days in untreated patients. These attacks typically peak over 24 hours, then usually resolve after 48 to 72 hours. However, the complete resolution of signs and symptoms can last for up to one week after the attacks.5
There is no concomitant pruritus or urticaria that accompanies the AE. However, erythema marginatum, an evanescent nonpruritic rash with serpiginous borders involving the trunk and inner surface of extremities but sparing the face, might herald the onset of an episode. This rash usually has central pallor that blanches with pressure and worsens with heat.
HAE can be triggered by stressful events, including trauma, surgery, menstruation, and viral infections. However, in many instances, HAE attacks occur without an identifiable cause.5
Differential Diagnosis from Other Causes of Angioedema
Type I HAE is characterized by a quantitative C1INH deficiency (which is functionally abnormal as well), and occurs in 85% of patients. Type II HAE occurs in 15% of patients, and results from a functionally abnormal C1INH.
In patients with Type I and II HAE, as well as acquired C1 inhibitor deficiency (ACID), C4 levels are low during and between attacks. C2 levels are also low during acute attacks. In ACID, levels of C1q are also reduced; these patients require further workup to rule out an undiagnosed malignancy or an autoimmune process. In contrast, patients with ACE-induced, idiopathic, and allergic AE have normal complement profiles.3,6
Type III is a more recently described type of HAE that is rare, not well understood, and generally affects women.3,6 Clinically, it resembles Type I and Type II HAE but complement levels, including C1 inhibitor, are normal (see Table 1).
Treatment
HAE types I, II, III, and ACID are generally unresponsive to glucocorticoids, antihistamines, and epinephrine. These forms of AE may be exacerbated by exogenous estrogen.1,8 For this reason, HAE patients should avoid oral hormonal contraception and estrogen replacement therapy. In addition, ACE inhibitors should also be avoided based on their effect on bradykinin degradation.
Until the introduction of newer therapeutic choices, as noted in our case, the treatment of acute attacks of AE was essentially supportive. Patients with impending laryngeal obstruction were managed with intubation prior to progression of the AE to limit airway patency. Prior to the modern era, a substantial proportion of HAE patients died of asphyxiation.
Fresh frozen plasma (FFP) has been used to treat acute HAE attacks, but given its content of contact system proteins (in addition to C1INH), FFP might also pose a risk for worsening of HAE; for this reason, it must be given cautiously to patients who are symptomatic.9
In the past decade, there has been significant progress in the available treatments for HAE. Currently in the U.S., there are several agents recently approved by, or have pending approvals from, the FDA, including several forms of C1INH replacement, a bradykinin antagonist, and a kallikrein inhibitor.
The C1 esterase inhibitor (human) drugs are administered intravenously; both have been shown to be efficacious and safe. Nanofiltered C1 inhibitor provided relief in a median time of two hours when used acutely; when used as prophylaxis, it decreased the number of attacks in a three-month period by 50% (six vs. 12 with placebo, P<0.001).11
The other C1INH is rhucin, still not approved in U.S. This drug is characterized by a short half-life (approximately two to four hours) compared with the plasma-derived C1INH agents (24 to 48 hours). It is contraindicated in patients with rabbit hypersensitivity, as it is purified from rabbit breast milk.10
Ecallantide is a kallikrein inhibitor for acute therapy that is administered via three subcutaneous injections. This agent has been linked to allergic/anaphylactic reactions in a minority of patients (approximately 4%); therefore, it should be administered cautiously, by a health-care provider, and in a setting where anaphylaxis can be successfully managed.12 Icatibant is a bradykinin antagonist recently approved in the U.S. and administered SC via a single injection.10
In light of the development of these new agents, there is a need for updated guidelines for the long- and short-term prophylaxis and acute management of HAE. A recent guideline focused on the management of HAE in gynecologic and obstetric patients recommended the use of plasma-derived C1INH C1 esterase inhibitor (human) (Cinryze) for short- and long-term prophylaxis and acute treatment of HAE.13 The effect of pregnancy on HAE is variable: Some women worsen and other women have less swelling during their pregnancy. Swelling at the time of parturition is rare; however, the risk rises during the post-partum period.
Type III HAE. An additional form of HAE has been recognized with a pattern of AE episodes that mimics Type I or Type II HAE but with unremarkable laboratory studies of the complement cascade, including C1 inhibitor level and function. At this time, there is no laboratory test with which a diagnosis of Type III HAE can be confirmed. The diagnosis should be suspected in patients with a strong family history of AE reflecting autosomal dominant inheritance. In some, but not all, cases, the condition is manifest in association with high estrogen levels (e.g. pregnancy or administration of oral contraceptives). Type III HAE patients have a salutary response to the same agents that are efficacious for Type I and II HAE.
Acquired C1 inhibitor deficiency (ACID). ACID generally occurs in adults and is clinically indistinguishable from HAE. ACID is not associated with a remarkable family history of AE. In contrast to HAE, this is a consumptive deficiency of C1 inhibitor and results from enhanced catabolism that exceeds the capacity for regenerating C1 inhibitor protein. It is often associated with neoplastic (usually lymphoproliferative) or autoimmune disorders; treatment of the underlying condition frequently leads to improvement in ACID. Although its management is similar to HAE, it tends to be more responsive to anti-fibrinolytics. A salutary response to C1INH replacement therapy might not occur in patients with autoantibodies to C1 inhibitor, but efficacy of ecallantide and icatibant for the treatment of acquired AE has been reported.14, 15
ACEI angioedema. Treatment with angiotensin-converting enzyme inhibitors (ACE-I) has been associated with recurrent AE without urticaria in 0.1 to 0.7% of patients exposed to these drugs.16 Angioedema from ACE-I more frequently occurs within the first few months of therapy, but it might occur even after years of continuous therapy. ACEI-induced AE is secondary to impaired degradation of bradykinin. The main treatment is to discontinue the offending agent and avoid all other ACE-I, as this is a class-specific reaction.17
Angiotensin receptor blockers (ARBs) have been associated less commonly with AE. The mechanism for ARB-associated AE has not been elucidated. A meta-analysis showed that in 2% to 17% of patients who were switched to ARBs, recurrence of AE was observed.18 From the pooling of these data with two randomized controlled trials, it is estimated that approximately 10% or less of patients with ACEI-associated AE who switched to ARBs will develop AE.19 In the majority of cases, patients can be switched to ARBs with no recurrence of AE; however, the decision to prescribe an ARB to a patient who has had AE while receiving ACEI should be made carefully on an individualized risk/benefit basis.19
Preventive Treatment
The 17 α-alkylated androgens that can be used for treatment of HAE are danazol (Danacrine), stanozolol (Winstrol), oxandralone (Oxandrine) and methyltestosterone (Android). In patients with HAE, attenuated androgens can significantly reduce the frequency and severity of attacks; however, their use is limited by risk for untoward effects (virilization, abnormal liver function tests, change in libido, anxiety, etc.).21 There is also a risk for hepatotoxicity, including development of hepatic adenomas and hepatic carcinoma.
Antifibrinolytics also may have efficacy for HAE, but these agents have been associated with a variety of adverse effects, including nausea and diarrhea, postural hypotension, fatigue, enhanced thrombosis, retinal changes, and teratogenicity.8, 22, 23
In 2009, long-term prophylaxis with C1-INH concentrate was recommended for patients with HAE with frequent or disabling attacks, a history of laryngeal attacks, and poor quality of life. The 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of HAE recommended long-term prophylaxis in patients with more than one monthly severe HAE attack, more than five days of disability per month, or any history of airway compromise.24, 25
The decision to prescribe long-term prophylaxis, and the dose/frequency of medication required, should be individualized based on clinical parameters, such as frequency and severity of attacks, and not on C1 INH or C4 levels.
Perioperative Considerations
It is well established that any trauma, including dental procedures or surgery, can precipitate HAE attacks. For this reason, short-term prophylactic treatment in HAE patients undergoing procedures is recommended. Ideally, avoiding endotracheal intubation is the best approach; however, if intubation cannot be avoided, then adequate prophylaxis should be administered.2
Attenuated androgens can be given up to seven days before a procedure, or C1 INH can be administered 24 hours in advance. If C1 INH is unavailable, FFP can be given six to 12 hours in advance in patients who are not symptomatic; in case of endotracheal intubation, either FFP or C1 INH should be administered immediately before.2
Several case reports in multiple specialty surgical patients (abdominal surgery, cardiopulmonary bypass, orthopedic surgery, etc.) have confirmed the successful use of C1 INH in the prevention of acute attacks with favorable outcomes.2
There is no need to follow C1 INH levels, as it has no clinical relevance.
Back to the Case
The patient was admitted to the ICU and received a total of eight units of FFP. He was transferred to our institution and was able to be extubated three days after initial presentation. Laboratory studies revealed C4 10mg/dL and C1 esterase inhibitor 10mg/dL (both low).
Danazol was resumed. However, within several months after discharge, Cinryze became available in the U.S. market and was eventually prescribed. The patient has not had further significant attacks requiring inpatient management.
Dr. Auron is an assistant professor of medicine and pediatrics at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University. Dr. Lang is co-director of the Asthma Center and director of the Allergy/Immunology Fellowship Training Program at the Cleveland Clinic.
References
- Bernstein, JA. Update on angioedema: evaluation, diagnosis, and treatment. Allergy Asthma Proc. 2011;32(6):408-412.
- Levy JH, Freiberger DJ, Roback J. Hereditary angioedema: current and emerging treatment options. Anesth Analg. 2010;110(5):1271-1280.
- Busse PJ. Angioedema: Differential diagnosis and treatment. Allergy Asthma Proc. 2011;32:Suppl 1:S3-S11.
- Khan DA. Hereditary angioedema: historical aspects, classification, pathophysiology, clinical presentation, and laboratory diagnosis. Allergy Asthma Proc. 2011;32(1):1-10.
- Bork K, Meng G, Staubach P, Hardt, J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119(3):267-274.
- Zuraw BL, Christiansen SC. Pathogenesis and laboratory diagnosis of hereditary angioedema. Allergy Asthma Proc. 2009;30:487-492.
- Frazer-Abel A, Giclas PC. Update on laboratory tests for the diagnosis and differentiation of hereditary angioedema and acquired angioedema. Allergy Asthma Proc. 2011;32:Suppl 1:S17-S21.
- Banerjee A. Current treatment of hereditary angioedema: an update on clinical studies. Allergy Asthma Proc. 2010;31:398-406.
- Donaldson VH. Therapy of "the neurotic edema." N Engl J Med. 1972;286(15):835-836.
- Riedl MA. Update on the acute treatment of hereditary angioedema. Allergy Asthma Proc. 2011;32:11-16.
- Zuraw BL, Busse PJ, White M, et al. Nanofiltered C1 inhibitor concentrate for treatment of hereditary angioedema. N Engl J Med. 2010;363:513-522.
- Cicardi M, Levy RJ, McNeil DL. Ecallantide for the treatment of acute attacks in hereditary angioedema. N Engl J Med. 2010;363:523-531.
- Caballero T, Farkas H, Bouillet L, et al. International consensus and practical guidelines on the gynecologic and obstetric management of female patients with hereditary angioedema caused by C1 inhibitor deficiency. J Allergy Clin Immunol. 2012;129(2):308-320.
- Cicardi M, Zanichelli A. Acquired angioedema. J Allergy Clin Immunol. 2010;6(1):14.
- Zanichelli A, Badini M, Nataloni I, Montano N, Cicardi M. Treatment of acquired angioedema with icatibant: a case report. Intern Emerg Med. 2011;6(3):279-280.
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737.
- Haymore BR, Yoon J, Mikita CP, Klote MM, DeZee KJ. Risk of angioedema with angiotensin receptor blockers in patients with prior angioedema associated with angiotensin-converting enzyme inhibitors: a meta-analysis. Ann Allergy Asthma Immunol. 2008;101(5):495-499.
- Beavers CJ, Dunn SP, Macaulay TE. The role of angiotensin receptor blockers in patients with angiotensin-converting enzyme inhibitor-induced angioedema. Ann Pharmacother. 2011;45(4):520-524.
- Nzeako UC. Diagnosis and management of angioedema with abdominal involvement: a gastroenterology perspective. World J Gastroenterol. 2010; 16(39):4913-4921.
- Banerji A, Sloane DE, Sheffer AL. Hereditary angioedema: a current state-of-the-art review, V: attenuated androgens for the treatment of hereditary angioedema. Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S19-22.
- Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008; 359(10):1027-1036.
- Zuraw BL. Hereditary angioedema: a current state-of-the-art review, IV: short- and long-term treatment of hereditary angioedema: out with the old and in with the new? Ann Allergy Asthma Immunol. 2008;100(1) (Suppl 2):S13-S18.
- Bowen T, Cicardi M, Bork K, et al. Hereditary angioedema: a current state-of-the-art review, VII: Canadian Hungarian 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of Hereditary Angioedema. Ann Allergy Asthma Immunol. 2008;100(1)(Suppl 2):S30-40.
- Craig T, Riedl M, Dykewicz M, et al. When is prophylaxis for hereditary angioedema necessary? Ann Allergy Asthma Immunol. 2009.102(5):366-372.
- Frank MM. Update on preventive therapy (prophylaxis) of hereditary angioedema. Allergy Asthma Proc. 2011;32(1):17-21.
Nonurgent Pediatric Admissions on Weekends Bump Up Hospital Costs

Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Physician Reviews of Hospital Medicine-Related Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Prices for common hospital procedures not readily available
- Antibiotics associated with decreased mortality in acute COPD exacerbation
- Endovascular therapy has no benefit to systemic t-PA in acute stroke
- Net harm observed with rivaroxaban for thromboprophylaxis
- Noninvasive ventilation more effective, safer for AECOPD patients
- Synthetic cannabinoid use and acute kidney injury
- Dabigatran vs. warfarin in the extended treatment of VTE
- Spironolactone improves diastolic function
- Real-time EMR-based prediction tool for clinical deterioration
- Hypothermia protocol and cardiac arrest
Prices for Common Hospital Procedures Not Readily Available
Clinical question: Are patients able to select health-care providers based on price of service?
Background: With health-care costs rising, patients are encouraged to take a more active role in cost containment. Many initiatives call for greater pricing transparency in the health-care system. This study evaluated price availability for a common surgical procedure.
Study design: Telephone inquiries with standardized interview script.
Setting: Twenty top-ranked orthopedic hospitals and 102 non-top-ranked U.S. hospitals.
Synopsis: Hospitals were contacted by phone with a standardized, scripted request for their price of an elective total hip arthroplasty. The script described the patient as a 62-year-old grandmother without insurance who is able to pay out of pocket and wishes to compare hospital prices. On the first or second attempt, 40% of top-ranked and 32% of non-top-ranked hospitals were able to provide their price; after five attempts, authors were unable to obtain full pricing information (both hospital and physician fee) from 40% of top-ranked and 37% of non-top-ranked hospitals. Neither fee was made available by 15% of top-ranked and 16% of non-top-ranked hospitals. Wide variation of pricing was found across hospitals. The authors commented on the difficulties they encountered, such as the transfer of calls between departments and the uncertainty of representatives on how to assist.
Bottom line: For individual patients, applying basic economic principles as a consumer might be tiresome and often impossible, with no major differences between top-ranked and non-top-ranked hospitals.
Citation: Rosenthal JA, Lu X, Cram P. Availability of consumer prices from US hospitals for a common surgical procedure. JAMA Intern Med. 2013;173(6):427-432.
Antibiotics Associated with Decreased Mortality in Acute COPD Exacerbation
Clinical question: Do antibiotics when added to systemic steroids provide clinical benefit for patients with acute COPD exacerbation?
Background: Despite widespread use of antibiotics in the treatment of acute COPD, their benefit is not clear.
Study design: Retrospective cohort study.Setting: Four hundred ten U.S. hospitals participating in Perspective, an inpatient administrative database.
Synopsis: More than 50,000 patients treated with systemic steroids for acute COPD exacerbation were included in this study; 85% of them received empiric antibiotics within the first two hospital days. They were compared with those treated with systemic steroids alone. In-hospital mortality was 1.02% for patients on steroids plus antibiotics versus 1.78% on steroids alone. Use of antibiotics was associated with a 40% reduction in the odds of in-hospital mortality (OR, 0.60; 95% CI, 0.50-0.74) and reduced readmissions. In an analysis of matched cohorts, hospital mortality was 1% for patients on antibiotics and 1.8% for patients without antibiotics (OR, 0.53; 95% CI, 0.40-0.71). The risk for readmission for Clostridium difficile colitis was not different between the groups, but other potential adverse effects of antibiotic use, such as development of resistant micro-organisms, were not studied. In a subset analysis, three groups of antibiotics were compared: macrolides, quinolones, and cephalosporins. None was better than another, but those treated with macrolides had a lower readmission rate for C. diff.
Bottom line: Treatment with antibiotics when added to systemic steroids is associated with improved outcomes in acute COPD exacerbations, but there is no clear advantage of one antibiotic class over another.
Citation: Stefan MS, Rothberg MB, Shieh M, Pekow PS, Lindenauer PK. Association between antibiotic treatment and outcomes in patients hospitalized with acute exacerbation of COPD treated with systemic steroids. Chest. 2013;143(1):82-90.
Endovascular Therapy Added to Systemic t-PA Has No Benefit in Acute Stroke
Clinical question: Does adding endovascular therapy to intravenous tissue plasminogen activator (t-PA) reduce disability in acute stroke?
Background: Early systemic t-PA is the only proven reperfusion therapy in acute stroke, but it is unknown if adding localized endovascular therapy is beneficial.
Study design: Randomized, open-label, blinded-outcome trial.
Setting: Fifty-eight centers in North America, Europe, and Australia.
Synopsis: Patients aged 18 to 82 with acute ischemic stroke were eligible if they received t-PA within three hours of enrollment and had moderate to severe neurologic deficit (National Institutes of Health Stroke Scale [NIHSS] >10, or NIHSS 8 or 9 with CT angiographic evidence of specific major artery occlusion). All patients received standard-dose t-PA; those randomized to endovascular treatment underwent angiography, and, if indicated, underwent one of the endovascular treatments chosen by the neurointerventionalist. The primary outcome measure was a modified Rankin score of 2 or lower (indicating functional independence) at 90 days (assessed by a neurologist).
After enrollment of 656 patients, the trial was terminated early for futility. There was no significant difference in the primary outcome, with 40.8% of patients in the endovascular intervention group and 38.7% in the t-PA-only group having a modified Rankin score of 2 or lower. There was also no difference in mortality or other secondary outcomes, even when the analysis was limited to patients presenting with more severe neurologic deficits.
Bottom line: The addition of endovascular therapy to systemic t-PA in acute ischemic stroke does not improve functional outcomes or mortality.
Citation: Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368:893-903.
Rivaroxaban Compared with Enoxaparin for Thromboprophylaxis
Clinical question: Is extended-duration rivaroxaban more effective than standard-duration enoxaparin in preventing deep venous thrombosis in acutely ill medical patients?
Background: Trials have shown benefits of thromboprophylaxis in acutely ill medical patients at increased risk of venous thrombosis, but the optimal duration and type of anticoagulation is unknown.
Study design: Prospective, randomized, double-blinded, active-comparator controlled trial.
Setting: Five hundred fifty-two centers in 52 countries.
Synopsis: The trial enrolled 8,428 patients hospitalized with an acute medical condition and reduced mobility. Patients were randomized to receive either enoxaparin for 10 (+/-4) days or rivaroxaban for 35 (+/-4) days. The co-primary composite outcomes were the incidence of asymptomatic proximal deep venous thrombosis, symptomatic deep venous thrombosis, pulmonary embolism, or death related to venous thromboembolism over 10 days and over 35 days.
Both groups had a 2.7% incidence of the primary endpoint over 10 days; over 35 days, the extended-duration rivaroxaban group had a reduced incidence of the primary endpoint of 4.4% compared with 5.7% for enoxaparin. However, there was an increase of clinically relevant bleeding in the rivaroxaban group, occurring in 2.8% and 4.1% of patients over 10 and 35 days, respectively, compared with 1.2% and 1.7% for enoxaparin.
Overall, there was net harm with rivaroxaban over both time periods: 6.6% and 9.4% of patients in the rivaroxaban group had a negative outcome at 10 and 35 days, compared with 4.4% and 7.8% with enoxaparin.
Bottom line: There was net harm with extended-duration rivaroxaban versus standard-duration enoxaparin for thromboprophylaxis in hospitalized medical patients.
Citation: Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368:513-523.
Noninvasive Ventilation More Effective, Safer for Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD)
Clinical question: What are the patterns in use of noninvasive ventilation (NIV) and invasive mechanical ventilation (IMV) in patients with AECOPD, and which method produces better outcomes?
Background: Multiple randomized controlled trials and meta-analyses have suggested a mortality benefit with NIV compared to standard medical care in AECOPD. However, little evidence exists on head-to-head comparisons of NIV and IMV.
Study design: Retrospective cohort study.
Setting: Non-federal, short-term, general, and other specialty hospitals nationwide.
Synopsis: A sample of 67,651 ED visits for AECOPD with acute respiratory failure was analyzed from the National Emergency Department Sample (NEDS) database between 2006 and 2008. The study found that NIV use increased to 16% in 2008 from 14% in 2006. Use varied widely between hospitals and was more utilized in higher-case-volume, nonmetropolitan, and Northeastern hospitals. Compared with IMV, NIV was associated with 46% lower inpatient mortality (risk ratio 0.54, 95% confidence interval [CI] 0.50-0.59), shortened hospital length of stay (-3.2 days, 95% CI -3.4 to -2.9), lower hospital charges (-$35,012, 95% CI -$36,848 to -$33,176), and lower risk of iatrogenic pneumothorax (0.05% vs. 0.5%, P<0.001). Causality could not be established given the observational study design.
Bottom line: NIV is associated with better outcomes than IMV in the management of AECOPD, and might be underutilized.
Citation: Tsai CL, Lee WY, Delclos GL, Hanania NA, Camargo CA Jr. Comparative effectiveness of noninvasive ventilation vs. invasive mechanical ventilation in chronic obstructive pulmonary disease patients with acute respiratory failure. J Hosp Med. 2013;8(4):165-172.
Synthetic Cannabinoid Use May Cause Acute Kidney Injury
Clinical question: Are synthetic cannabinoids associated with acute kidney injury (AKI)?
Background: Synthetic cannabinoids are designer drugs of abuse with a growing popularity in the U.S.
Study design: Retrospective case series.
Setting: Hospitals in Wyoming, Oklahoma, Rhode Island, New York, Kansas, and Oregon.
Synopsis: The Centers for Disease Control and Prevention (CDC) issued an alert when 16 cases of unexplained AKI after exposure to synthetic cannabinoids were reported between March and December 2012. Synthetic cannabinoid use is associated with neurologic, sympathomimetic, and cardiovascular toxicity; however, this is the first case series reporting renal toxicity. The 16 patients included 15 males and one female, aged 15-33 years, with no pre-existing renal disease or nephrotoxic medication consumption. All used synthetic cannabinoids within hours to days before developing nausea, vomiting, abdominal, and flank and/or back pain.
Creatinine peaked one to six days after symptom onset. Five patients required hemodialysis, and all 16 recovered. There was no finding specific for all cases on ultrasound and/or biopsy. Toxicologic analysis of specimens was possible in seven cases and revealed a previously unreported fluorinated synthetic cannabinoid compound XLR-11 in all clinical specimens of patients who used the drug within two days of being tested.
Overall, the analysis did not reveal any single compound or brand that could explain all cases.
Bottom line: Clinicians should be aware of the potential for renal or other toxicities in users of synthetic cannabinoid products and should ask about their use in cases of unexplained AKI.
Citation: Murphy TD, Weidenbach KN, Van Houten C, et al. Centers for Disease Control and Prevention. Acute kidney injury associated with synthetic cannabinoid use—multiple states, 2012. MMWR Morb Mortal Wkly Rep. 2013;62(6):93-98.
Dabigatran versus Warfarin in Extended VTE Treatment
Clinical question: Is dabigatran suitable for extended treatment VTE?
Background: In contrast to warfarin (Coumadin), dabigatran (Pradaxa) is given in a fixed dose and does not require frequent laboratory monitoring. Dabigatran has been shown to be noninferior to warfarin in the initial six-month treatment of VTE.
Study design: Two double-blinded, randomized trials: an active-control study and a placebo-control study.
Setting: Two hundred sixty-five sites in 33 countries for the active-control study, and 147 sites in 21 countries for the placebo-control study.
Synopsis: This study enrolled 4,299 adult patients with objectively confirmed, symptomatic, proximal deep vein thrombosis or pulmonary embolism. In the active-control study comparing warfarin and dabigatran, recurrent objectively confirmed symptomatic or fatal VTE was observed in 1.8% of patients in the dabigatran group compared with 1.3% of patients in the warfarin group (P=0.01 for noninferiority). While major or clinically relevant bleeding was less frequent with dabigatran compared to warfarin (hazard ratio, 0.54), more acute coronary syndromes were observed with dabigatran (0.9% vs. 0.2%, P=0.02). In the placebo-control study, symptomatic or fatal VTE was observed in 0.4% of patients in the dabigatran group compared with 5.6% in the placebo group. Clinically relevant bleeding was more common with dabigatran (5.3% vs. 1.8%; hazard ratio 2.92).
Bottom line: Treatment with dabigatran met the pre-specified noninferiority margin in this study. However, it is worth noting that patients with VTE given extended treatment with dabigatran had significantly higher rates of recurrent symptomatic or fatal VTE than patients treated with warfarin.
Citation: Schulman S, Kearson C, Kakkar AK, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med. 2013;368(8):709-718.
Spironolactone Improves Diastolic Function
Clinical question: What is the efficacy of aldosterone receptor blockers on diastolic function and exercise capacity?
Background: Mineralocorticoid receptor activation by aldosterone contributes to the pathophysiology of heart failure (HF) in patients with and without reduced ejection fraction (EF). Aldosterone receptor blockers (spironolactone) reduce overall and cardiovascular mortality in HF patients with reduced EF; however, its effect on HF patients with preserved EF is unknown.
Study design: Prospective, randomized, double-blinded, placebo-controlled trial.
Setting: Ten ambulatory sites in Germany and Austria.
Synopsis: This study enrolled 422 men and women, aged 50 or older, with New York Heart Association (NYHA) Class II or III HF and preserved EF, and randomized them to receive spironolactone 25 mg daily or placebo for one year.
The endpoints included echocardiographic measures of diastolic function and remodeling; N-terminal pro b-type natriuretic peptide (NT pro-BNP) levels; exercise capacity; quality of life; and HF symptoms.
In the spironolactone group, there was significant improvement in echocardiographic measures of diastolic function and remodeling as well as NT pro-BNP levels. However, there was no difference in exercise capacity, quality of life, or HF symptoms when compared to placebo.
The spironolactone group had significantly lower blood pressure than the control group, which may account for some of the remodeling effects. The study may have been underpowered, and the study population might not have had severe enough disease to detect a difference in clinical measures. It remains unknown if structural changes on echocardiography will translate into clinical benefits.
Bottom line: Compared to placebo, spironolactone did improve diastolic function by echo but did not improve exercise capacity.
Citation: Edelmann F, Wachter R, Schmidt A, et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA. 2013;309(8):781-791.
Real-Time, EMR-Based Prediction Tool Accurately Predicts ICU Transfer Risks
Clinical question: Can clinical deterioration be accurately predicted using real-time data from an electronic medical record (EMR), and can it lead to better outcomes using a floor-based intervention?
Background: Research has shown that EMR-based prediction tools can help identify real-time clinical deterioration in ward patients, but an intervention based on these computer-based alerts has not been shown to be effective.
Study design: Randomized controlled crossover study.
Setting: Eight adult medicine wards in an academic medical center in the Midwest.
Synopsis: There were 20,031 patients assigned to intervention versus control based on their floor location. Computerized alerts were generated using a prediction algorithm. For patients admitted to intervention wards, the alerts were sent to the charge nurse via pager. Patients meeting the alert threshold based on the computerized prediction tool had five times higher risk of ICU transfer, and nine times higher risk of death than patients not meeting the alert threshold. Intervention of charge nurse notification via pager did not result in any significant change in length of stay (LOS), ICU transfer, or mortality. Charge nurses in the intervention group were supposed to alert a physician after receiving the computer alert, but the authors did not measure how often this occurred.
Bottom line: A real-time EMR-based prediction tool accurately predicts higher risk of ICU transfer and death, as well as LOS, but a floor-based intervention to alert the charge nurse in real time did not lead to better outcomes.
Citation: Bailey TC, Chen Y, Mao Y, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medicine wards. J Hosp Med. 2013 Feb 25. doi: 10.1002/jhm.2009 [Epub ahead of print].
Hypothermia Protocol and Cardiac Arrest
Clinical question: Is mild therapeutic hypothermia (MTH) following cardiac arrest beneficial and safe?
Background: Those with sudden cardiac arrest often have poor neurologic outcome. There are some studies that show benefit with hypothermia, but information on safety is limited.
Study design: Meta-analysis.
Setting: Europe, the United Kingdom, the U.S., Canada, Japan, and South Korea.
Synopsis: This study pooled data from 63 studies that looked at MTH protocols in the setting of comatose patients as a result of cardiac arrest. The end points included mortality and any complication potentially attributed to the MTH.
When restricting the analysis to include only randomized controlled trials, MTH was associated with decreased risk of in-hospital mortality (RR=0.75, 95% CI: 0.62-0.92), 30-day mortality (RR=0.61, 95% CI 0.45-0.81), and six-month mortality (RR=0.73, 95% CI 0.61-0.88). MTH was associated with increased risk of arrhythmia (RR=1.25, 95% CI: 1.00-1.55) and hypokalemia (RR=2.35, 95% CI: 1.35-4.11); all other complications were similar between groups.
There were inconsistent results regarding benefit in pediatric patients, as well as comatose patients with non-ventricular fibrillation (non-v-fib) arrest (i.e. asystole or pulseless electrical activity).
Bottom line: Mild therapeutic hypothermia can improve survival of comatose patients after v-fib cardiac arrest and is generally safe.
Citation: Xiao G, Guo Q, Xie X, et al. Safety profile and outcome of mild therapeutic hypothermia in patients following cardiac arrest: systematic review and meta-analysis. Emerg Med J. 2013;30:90-100.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Prices for common hospital procedures not readily available
- Antibiotics associated with decreased mortality in acute COPD exacerbation
- Endovascular therapy has no benefit to systemic t-PA in acute stroke
- Net harm observed with rivaroxaban for thromboprophylaxis
- Noninvasive ventilation more effective, safer for AECOPD patients
- Synthetic cannabinoid use and acute kidney injury
- Dabigatran vs. warfarin in the extended treatment of VTE
- Spironolactone improves diastolic function
- Real-time EMR-based prediction tool for clinical deterioration
- Hypothermia protocol and cardiac arrest
Prices for Common Hospital Procedures Not Readily Available
Clinical question: Are patients able to select health-care providers based on price of service?
Background: With health-care costs rising, patients are encouraged to take a more active role in cost containment. Many initiatives call for greater pricing transparency in the health-care system. This study evaluated price availability for a common surgical procedure.
Study design: Telephone inquiries with standardized interview script.
Setting: Twenty top-ranked orthopedic hospitals and 102 non-top-ranked U.S. hospitals.
Synopsis: Hospitals were contacted by phone with a standardized, scripted request for their price of an elective total hip arthroplasty. The script described the patient as a 62-year-old grandmother without insurance who is able to pay out of pocket and wishes to compare hospital prices. On the first or second attempt, 40% of top-ranked and 32% of non-top-ranked hospitals were able to provide their price; after five attempts, authors were unable to obtain full pricing information (both hospital and physician fee) from 40% of top-ranked and 37% of non-top-ranked hospitals. Neither fee was made available by 15% of top-ranked and 16% of non-top-ranked hospitals. Wide variation of pricing was found across hospitals. The authors commented on the difficulties they encountered, such as the transfer of calls between departments and the uncertainty of representatives on how to assist.
Bottom line: For individual patients, applying basic economic principles as a consumer might be tiresome and often impossible, with no major differences between top-ranked and non-top-ranked hospitals.
Citation: Rosenthal JA, Lu X, Cram P. Availability of consumer prices from US hospitals for a common surgical procedure. JAMA Intern Med. 2013;173(6):427-432.
Antibiotics Associated with Decreased Mortality in Acute COPD Exacerbation
Clinical question: Do antibiotics when added to systemic steroids provide clinical benefit for patients with acute COPD exacerbation?
Background: Despite widespread use of antibiotics in the treatment of acute COPD, their benefit is not clear.
Study design: Retrospective cohort study.Setting: Four hundred ten U.S. hospitals participating in Perspective, an inpatient administrative database.
Synopsis: More than 50,000 patients treated with systemic steroids for acute COPD exacerbation were included in this study; 85% of them received empiric antibiotics within the first two hospital days. They were compared with those treated with systemic steroids alone. In-hospital mortality was 1.02% for patients on steroids plus antibiotics versus 1.78% on steroids alone. Use of antibiotics was associated with a 40% reduction in the odds of in-hospital mortality (OR, 0.60; 95% CI, 0.50-0.74) and reduced readmissions. In an analysis of matched cohorts, hospital mortality was 1% for patients on antibiotics and 1.8% for patients without antibiotics (OR, 0.53; 95% CI, 0.40-0.71). The risk for readmission for Clostridium difficile colitis was not different between the groups, but other potential adverse effects of antibiotic use, such as development of resistant micro-organisms, were not studied. In a subset analysis, three groups of antibiotics were compared: macrolides, quinolones, and cephalosporins. None was better than another, but those treated with macrolides had a lower readmission rate for C. diff.
Bottom line: Treatment with antibiotics when added to systemic steroids is associated with improved outcomes in acute COPD exacerbations, but there is no clear advantage of one antibiotic class over another.
Citation: Stefan MS, Rothberg MB, Shieh M, Pekow PS, Lindenauer PK. Association between antibiotic treatment and outcomes in patients hospitalized with acute exacerbation of COPD treated with systemic steroids. Chest. 2013;143(1):82-90.
Endovascular Therapy Added to Systemic t-PA Has No Benefit in Acute Stroke
Clinical question: Does adding endovascular therapy to intravenous tissue plasminogen activator (t-PA) reduce disability in acute stroke?
Background: Early systemic t-PA is the only proven reperfusion therapy in acute stroke, but it is unknown if adding localized endovascular therapy is beneficial.
Study design: Randomized, open-label, blinded-outcome trial.
Setting: Fifty-eight centers in North America, Europe, and Australia.
Synopsis: Patients aged 18 to 82 with acute ischemic stroke were eligible if they received t-PA within three hours of enrollment and had moderate to severe neurologic deficit (National Institutes of Health Stroke Scale [NIHSS] >10, or NIHSS 8 or 9 with CT angiographic evidence of specific major artery occlusion). All patients received standard-dose t-PA; those randomized to endovascular treatment underwent angiography, and, if indicated, underwent one of the endovascular treatments chosen by the neurointerventionalist. The primary outcome measure was a modified Rankin score of 2 or lower (indicating functional independence) at 90 days (assessed by a neurologist).
After enrollment of 656 patients, the trial was terminated early for futility. There was no significant difference in the primary outcome, with 40.8% of patients in the endovascular intervention group and 38.7% in the t-PA-only group having a modified Rankin score of 2 or lower. There was also no difference in mortality or other secondary outcomes, even when the analysis was limited to patients presenting with more severe neurologic deficits.
Bottom line: The addition of endovascular therapy to systemic t-PA in acute ischemic stroke does not improve functional outcomes or mortality.
Citation: Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368:893-903.
Rivaroxaban Compared with Enoxaparin for Thromboprophylaxis
Clinical question: Is extended-duration rivaroxaban more effective than standard-duration enoxaparin in preventing deep venous thrombosis in acutely ill medical patients?
Background: Trials have shown benefits of thromboprophylaxis in acutely ill medical patients at increased risk of venous thrombosis, but the optimal duration and type of anticoagulation is unknown.
Study design: Prospective, randomized, double-blinded, active-comparator controlled trial.
Setting: Five hundred fifty-two centers in 52 countries.
Synopsis: The trial enrolled 8,428 patients hospitalized with an acute medical condition and reduced mobility. Patients were randomized to receive either enoxaparin for 10 (+/-4) days or rivaroxaban for 35 (+/-4) days. The co-primary composite outcomes were the incidence of asymptomatic proximal deep venous thrombosis, symptomatic deep venous thrombosis, pulmonary embolism, or death related to venous thromboembolism over 10 days and over 35 days.
Both groups had a 2.7% incidence of the primary endpoint over 10 days; over 35 days, the extended-duration rivaroxaban group had a reduced incidence of the primary endpoint of 4.4% compared with 5.7% for enoxaparin. However, there was an increase of clinically relevant bleeding in the rivaroxaban group, occurring in 2.8% and 4.1% of patients over 10 and 35 days, respectively, compared with 1.2% and 1.7% for enoxaparin.
Overall, there was net harm with rivaroxaban over both time periods: 6.6% and 9.4% of patients in the rivaroxaban group had a negative outcome at 10 and 35 days, compared with 4.4% and 7.8% with enoxaparin.
Bottom line: There was net harm with extended-duration rivaroxaban versus standard-duration enoxaparin for thromboprophylaxis in hospitalized medical patients.
Citation: Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368:513-523.
Noninvasive Ventilation More Effective, Safer for Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD)
Clinical question: What are the patterns in use of noninvasive ventilation (NIV) and invasive mechanical ventilation (IMV) in patients with AECOPD, and which method produces better outcomes?
Background: Multiple randomized controlled trials and meta-analyses have suggested a mortality benefit with NIV compared to standard medical care in AECOPD. However, little evidence exists on head-to-head comparisons of NIV and IMV.
Study design: Retrospective cohort study.
Setting: Non-federal, short-term, general, and other specialty hospitals nationwide.
Synopsis: A sample of 67,651 ED visits for AECOPD with acute respiratory failure was analyzed from the National Emergency Department Sample (NEDS) database between 2006 and 2008. The study found that NIV use increased to 16% in 2008 from 14% in 2006. Use varied widely between hospitals and was more utilized in higher-case-volume, nonmetropolitan, and Northeastern hospitals. Compared with IMV, NIV was associated with 46% lower inpatient mortality (risk ratio 0.54, 95% confidence interval [CI] 0.50-0.59), shortened hospital length of stay (-3.2 days, 95% CI -3.4 to -2.9), lower hospital charges (-$35,012, 95% CI -$36,848 to -$33,176), and lower risk of iatrogenic pneumothorax (0.05% vs. 0.5%, P<0.001). Causality could not be established given the observational study design.
Bottom line: NIV is associated with better outcomes than IMV in the management of AECOPD, and might be underutilized.
Citation: Tsai CL, Lee WY, Delclos GL, Hanania NA, Camargo CA Jr. Comparative effectiveness of noninvasive ventilation vs. invasive mechanical ventilation in chronic obstructive pulmonary disease patients with acute respiratory failure. J Hosp Med. 2013;8(4):165-172.
Synthetic Cannabinoid Use May Cause Acute Kidney Injury
Clinical question: Are synthetic cannabinoids associated with acute kidney injury (AKI)?
Background: Synthetic cannabinoids are designer drugs of abuse with a growing popularity in the U.S.
Study design: Retrospective case series.
Setting: Hospitals in Wyoming, Oklahoma, Rhode Island, New York, Kansas, and Oregon.
Synopsis: The Centers for Disease Control and Prevention (CDC) issued an alert when 16 cases of unexplained AKI after exposure to synthetic cannabinoids were reported between March and December 2012. Synthetic cannabinoid use is associated with neurologic, sympathomimetic, and cardiovascular toxicity; however, this is the first case series reporting renal toxicity. The 16 patients included 15 males and one female, aged 15-33 years, with no pre-existing renal disease or nephrotoxic medication consumption. All used synthetic cannabinoids within hours to days before developing nausea, vomiting, abdominal, and flank and/or back pain.
Creatinine peaked one to six days after symptom onset. Five patients required hemodialysis, and all 16 recovered. There was no finding specific for all cases on ultrasound and/or biopsy. Toxicologic analysis of specimens was possible in seven cases and revealed a previously unreported fluorinated synthetic cannabinoid compound XLR-11 in all clinical specimens of patients who used the drug within two days of being tested.
Overall, the analysis did not reveal any single compound or brand that could explain all cases.
Bottom line: Clinicians should be aware of the potential for renal or other toxicities in users of synthetic cannabinoid products and should ask about their use in cases of unexplained AKI.
Citation: Murphy TD, Weidenbach KN, Van Houten C, et al. Centers for Disease Control and Prevention. Acute kidney injury associated with synthetic cannabinoid use—multiple states, 2012. MMWR Morb Mortal Wkly Rep. 2013;62(6):93-98.
Dabigatran versus Warfarin in Extended VTE Treatment
Clinical question: Is dabigatran suitable for extended treatment VTE?
Background: In contrast to warfarin (Coumadin), dabigatran (Pradaxa) is given in a fixed dose and does not require frequent laboratory monitoring. Dabigatran has been shown to be noninferior to warfarin in the initial six-month treatment of VTE.
Study design: Two double-blinded, randomized trials: an active-control study and a placebo-control study.
Setting: Two hundred sixty-five sites in 33 countries for the active-control study, and 147 sites in 21 countries for the placebo-control study.
Synopsis: This study enrolled 4,299 adult patients with objectively confirmed, symptomatic, proximal deep vein thrombosis or pulmonary embolism. In the active-control study comparing warfarin and dabigatran, recurrent objectively confirmed symptomatic or fatal VTE was observed in 1.8% of patients in the dabigatran group compared with 1.3% of patients in the warfarin group (P=0.01 for noninferiority). While major or clinically relevant bleeding was less frequent with dabigatran compared to warfarin (hazard ratio, 0.54), more acute coronary syndromes were observed with dabigatran (0.9% vs. 0.2%, P=0.02). In the placebo-control study, symptomatic or fatal VTE was observed in 0.4% of patients in the dabigatran group compared with 5.6% in the placebo group. Clinically relevant bleeding was more common with dabigatran (5.3% vs. 1.8%; hazard ratio 2.92).
Bottom line: Treatment with dabigatran met the pre-specified noninferiority margin in this study. However, it is worth noting that patients with VTE given extended treatment with dabigatran had significantly higher rates of recurrent symptomatic or fatal VTE than patients treated with warfarin.
Citation: Schulman S, Kearson C, Kakkar AK, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med. 2013;368(8):709-718.
Spironolactone Improves Diastolic Function
Clinical question: What is the efficacy of aldosterone receptor blockers on diastolic function and exercise capacity?
Background: Mineralocorticoid receptor activation by aldosterone contributes to the pathophysiology of heart failure (HF) in patients with and without reduced ejection fraction (EF). Aldosterone receptor blockers (spironolactone) reduce overall and cardiovascular mortality in HF patients with reduced EF; however, its effect on HF patients with preserved EF is unknown.
Study design: Prospective, randomized, double-blinded, placebo-controlled trial.
Setting: Ten ambulatory sites in Germany and Austria.
Synopsis: This study enrolled 422 men and women, aged 50 or older, with New York Heart Association (NYHA) Class II or III HF and preserved EF, and randomized them to receive spironolactone 25 mg daily or placebo for one year.
The endpoints included echocardiographic measures of diastolic function and remodeling; N-terminal pro b-type natriuretic peptide (NT pro-BNP) levels; exercise capacity; quality of life; and HF symptoms.
In the spironolactone group, there was significant improvement in echocardiographic measures of diastolic function and remodeling as well as NT pro-BNP levels. However, there was no difference in exercise capacity, quality of life, or HF symptoms when compared to placebo.
The spironolactone group had significantly lower blood pressure than the control group, which may account for some of the remodeling effects. The study may have been underpowered, and the study population might not have had severe enough disease to detect a difference in clinical measures. It remains unknown if structural changes on echocardiography will translate into clinical benefits.
Bottom line: Compared to placebo, spironolactone did improve diastolic function by echo but did not improve exercise capacity.
Citation: Edelmann F, Wachter R, Schmidt A, et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA. 2013;309(8):781-791.
Real-Time, EMR-Based Prediction Tool Accurately Predicts ICU Transfer Risks
Clinical question: Can clinical deterioration be accurately predicted using real-time data from an electronic medical record (EMR), and can it lead to better outcomes using a floor-based intervention?
Background: Research has shown that EMR-based prediction tools can help identify real-time clinical deterioration in ward patients, but an intervention based on these computer-based alerts has not been shown to be effective.
Study design: Randomized controlled crossover study.
Setting: Eight adult medicine wards in an academic medical center in the Midwest.
Synopsis: There were 20,031 patients assigned to intervention versus control based on their floor location. Computerized alerts were generated using a prediction algorithm. For patients admitted to intervention wards, the alerts were sent to the charge nurse via pager. Patients meeting the alert threshold based on the computerized prediction tool had five times higher risk of ICU transfer, and nine times higher risk of death than patients not meeting the alert threshold. Intervention of charge nurse notification via pager did not result in any significant change in length of stay (LOS), ICU transfer, or mortality. Charge nurses in the intervention group were supposed to alert a physician after receiving the computer alert, but the authors did not measure how often this occurred.
Bottom line: A real-time EMR-based prediction tool accurately predicts higher risk of ICU transfer and death, as well as LOS, but a floor-based intervention to alert the charge nurse in real time did not lead to better outcomes.
Citation: Bailey TC, Chen Y, Mao Y, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medicine wards. J Hosp Med. 2013 Feb 25. doi: 10.1002/jhm.2009 [Epub ahead of print].
Hypothermia Protocol and Cardiac Arrest
Clinical question: Is mild therapeutic hypothermia (MTH) following cardiac arrest beneficial and safe?
Background: Those with sudden cardiac arrest often have poor neurologic outcome. There are some studies that show benefit with hypothermia, but information on safety is limited.
Study design: Meta-analysis.
Setting: Europe, the United Kingdom, the U.S., Canada, Japan, and South Korea.
Synopsis: This study pooled data from 63 studies that looked at MTH protocols in the setting of comatose patients as a result of cardiac arrest. The end points included mortality and any complication potentially attributed to the MTH.
When restricting the analysis to include only randomized controlled trials, MTH was associated with decreased risk of in-hospital mortality (RR=0.75, 95% CI: 0.62-0.92), 30-day mortality (RR=0.61, 95% CI 0.45-0.81), and six-month mortality (RR=0.73, 95% CI 0.61-0.88). MTH was associated with increased risk of arrhythmia (RR=1.25, 95% CI: 1.00-1.55) and hypokalemia (RR=2.35, 95% CI: 1.35-4.11); all other complications were similar between groups.
There were inconsistent results regarding benefit in pediatric patients, as well as comatose patients with non-ventricular fibrillation (non-v-fib) arrest (i.e. asystole or pulseless electrical activity).
Bottom line: Mild therapeutic hypothermia can improve survival of comatose patients after v-fib cardiac arrest and is generally safe.
Citation: Xiao G, Guo Q, Xie X, et al. Safety profile and outcome of mild therapeutic hypothermia in patients following cardiac arrest: systematic review and meta-analysis. Emerg Med J. 2013;30:90-100.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Prices for common hospital procedures not readily available
- Antibiotics associated with decreased mortality in acute COPD exacerbation
- Endovascular therapy has no benefit to systemic t-PA in acute stroke
- Net harm observed with rivaroxaban for thromboprophylaxis
- Noninvasive ventilation more effective, safer for AECOPD patients
- Synthetic cannabinoid use and acute kidney injury
- Dabigatran vs. warfarin in the extended treatment of VTE
- Spironolactone improves diastolic function
- Real-time EMR-based prediction tool for clinical deterioration
- Hypothermia protocol and cardiac arrest
Prices for Common Hospital Procedures Not Readily Available
Clinical question: Are patients able to select health-care providers based on price of service?
Background: With health-care costs rising, patients are encouraged to take a more active role in cost containment. Many initiatives call for greater pricing transparency in the health-care system. This study evaluated price availability for a common surgical procedure.
Study design: Telephone inquiries with standardized interview script.
Setting: Twenty top-ranked orthopedic hospitals and 102 non-top-ranked U.S. hospitals.
Synopsis: Hospitals were contacted by phone with a standardized, scripted request for their price of an elective total hip arthroplasty. The script described the patient as a 62-year-old grandmother without insurance who is able to pay out of pocket and wishes to compare hospital prices. On the first or second attempt, 40% of top-ranked and 32% of non-top-ranked hospitals were able to provide their price; after five attempts, authors were unable to obtain full pricing information (both hospital and physician fee) from 40% of top-ranked and 37% of non-top-ranked hospitals. Neither fee was made available by 15% of top-ranked and 16% of non-top-ranked hospitals. Wide variation of pricing was found across hospitals. The authors commented on the difficulties they encountered, such as the transfer of calls between departments and the uncertainty of representatives on how to assist.
Bottom line: For individual patients, applying basic economic principles as a consumer might be tiresome and often impossible, with no major differences between top-ranked and non-top-ranked hospitals.
Citation: Rosenthal JA, Lu X, Cram P. Availability of consumer prices from US hospitals for a common surgical procedure. JAMA Intern Med. 2013;173(6):427-432.
Antibiotics Associated with Decreased Mortality in Acute COPD Exacerbation
Clinical question: Do antibiotics when added to systemic steroids provide clinical benefit for patients with acute COPD exacerbation?
Background: Despite widespread use of antibiotics in the treatment of acute COPD, their benefit is not clear.
Study design: Retrospective cohort study.Setting: Four hundred ten U.S. hospitals participating in Perspective, an inpatient administrative database.
Synopsis: More than 50,000 patients treated with systemic steroids for acute COPD exacerbation were included in this study; 85% of them received empiric antibiotics within the first two hospital days. They were compared with those treated with systemic steroids alone. In-hospital mortality was 1.02% for patients on steroids plus antibiotics versus 1.78% on steroids alone. Use of antibiotics was associated with a 40% reduction in the odds of in-hospital mortality (OR, 0.60; 95% CI, 0.50-0.74) and reduced readmissions. In an analysis of matched cohorts, hospital mortality was 1% for patients on antibiotics and 1.8% for patients without antibiotics (OR, 0.53; 95% CI, 0.40-0.71). The risk for readmission for Clostridium difficile colitis was not different between the groups, but other potential adverse effects of antibiotic use, such as development of resistant micro-organisms, were not studied. In a subset analysis, three groups of antibiotics were compared: macrolides, quinolones, and cephalosporins. None was better than another, but those treated with macrolides had a lower readmission rate for C. diff.
Bottom line: Treatment with antibiotics when added to systemic steroids is associated with improved outcomes in acute COPD exacerbations, but there is no clear advantage of one antibiotic class over another.
Citation: Stefan MS, Rothberg MB, Shieh M, Pekow PS, Lindenauer PK. Association between antibiotic treatment and outcomes in patients hospitalized with acute exacerbation of COPD treated with systemic steroids. Chest. 2013;143(1):82-90.
Endovascular Therapy Added to Systemic t-PA Has No Benefit in Acute Stroke
Clinical question: Does adding endovascular therapy to intravenous tissue plasminogen activator (t-PA) reduce disability in acute stroke?
Background: Early systemic t-PA is the only proven reperfusion therapy in acute stroke, but it is unknown if adding localized endovascular therapy is beneficial.
Study design: Randomized, open-label, blinded-outcome trial.
Setting: Fifty-eight centers in North America, Europe, and Australia.
Synopsis: Patients aged 18 to 82 with acute ischemic stroke were eligible if they received t-PA within three hours of enrollment and had moderate to severe neurologic deficit (National Institutes of Health Stroke Scale [NIHSS] >10, or NIHSS 8 or 9 with CT angiographic evidence of specific major artery occlusion). All patients received standard-dose t-PA; those randomized to endovascular treatment underwent angiography, and, if indicated, underwent one of the endovascular treatments chosen by the neurointerventionalist. The primary outcome measure was a modified Rankin score of 2 or lower (indicating functional independence) at 90 days (assessed by a neurologist).
After enrollment of 656 patients, the trial was terminated early for futility. There was no significant difference in the primary outcome, with 40.8% of patients in the endovascular intervention group and 38.7% in the t-PA-only group having a modified Rankin score of 2 or lower. There was also no difference in mortality or other secondary outcomes, even when the analysis was limited to patients presenting with more severe neurologic deficits.
Bottom line: The addition of endovascular therapy to systemic t-PA in acute ischemic stroke does not improve functional outcomes or mortality.
Citation: Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368:893-903.
Rivaroxaban Compared with Enoxaparin for Thromboprophylaxis
Clinical question: Is extended-duration rivaroxaban more effective than standard-duration enoxaparin in preventing deep venous thrombosis in acutely ill medical patients?
Background: Trials have shown benefits of thromboprophylaxis in acutely ill medical patients at increased risk of venous thrombosis, but the optimal duration and type of anticoagulation is unknown.
Study design: Prospective, randomized, double-blinded, active-comparator controlled trial.
Setting: Five hundred fifty-two centers in 52 countries.
Synopsis: The trial enrolled 8,428 patients hospitalized with an acute medical condition and reduced mobility. Patients were randomized to receive either enoxaparin for 10 (+/-4) days or rivaroxaban for 35 (+/-4) days. The co-primary composite outcomes were the incidence of asymptomatic proximal deep venous thrombosis, symptomatic deep venous thrombosis, pulmonary embolism, or death related to venous thromboembolism over 10 days and over 35 days.
Both groups had a 2.7% incidence of the primary endpoint over 10 days; over 35 days, the extended-duration rivaroxaban group had a reduced incidence of the primary endpoint of 4.4% compared with 5.7% for enoxaparin. However, there was an increase of clinically relevant bleeding in the rivaroxaban group, occurring in 2.8% and 4.1% of patients over 10 and 35 days, respectively, compared with 1.2% and 1.7% for enoxaparin.
Overall, there was net harm with rivaroxaban over both time periods: 6.6% and 9.4% of patients in the rivaroxaban group had a negative outcome at 10 and 35 days, compared with 4.4% and 7.8% with enoxaparin.
Bottom line: There was net harm with extended-duration rivaroxaban versus standard-duration enoxaparin for thromboprophylaxis in hospitalized medical patients.
Citation: Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368:513-523.
Noninvasive Ventilation More Effective, Safer for Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD)
Clinical question: What are the patterns in use of noninvasive ventilation (NIV) and invasive mechanical ventilation (IMV) in patients with AECOPD, and which method produces better outcomes?
Background: Multiple randomized controlled trials and meta-analyses have suggested a mortality benefit with NIV compared to standard medical care in AECOPD. However, little evidence exists on head-to-head comparisons of NIV and IMV.
Study design: Retrospective cohort study.
Setting: Non-federal, short-term, general, and other specialty hospitals nationwide.
Synopsis: A sample of 67,651 ED visits for AECOPD with acute respiratory failure was analyzed from the National Emergency Department Sample (NEDS) database between 2006 and 2008. The study found that NIV use increased to 16% in 2008 from 14% in 2006. Use varied widely between hospitals and was more utilized in higher-case-volume, nonmetropolitan, and Northeastern hospitals. Compared with IMV, NIV was associated with 46% lower inpatient mortality (risk ratio 0.54, 95% confidence interval [CI] 0.50-0.59), shortened hospital length of stay (-3.2 days, 95% CI -3.4 to -2.9), lower hospital charges (-$35,012, 95% CI -$36,848 to -$33,176), and lower risk of iatrogenic pneumothorax (0.05% vs. 0.5%, P<0.001). Causality could not be established given the observational study design.
Bottom line: NIV is associated with better outcomes than IMV in the management of AECOPD, and might be underutilized.
Citation: Tsai CL, Lee WY, Delclos GL, Hanania NA, Camargo CA Jr. Comparative effectiveness of noninvasive ventilation vs. invasive mechanical ventilation in chronic obstructive pulmonary disease patients with acute respiratory failure. J Hosp Med. 2013;8(4):165-172.
Synthetic Cannabinoid Use May Cause Acute Kidney Injury
Clinical question: Are synthetic cannabinoids associated with acute kidney injury (AKI)?
Background: Synthetic cannabinoids are designer drugs of abuse with a growing popularity in the U.S.
Study design: Retrospective case series.
Setting: Hospitals in Wyoming, Oklahoma, Rhode Island, New York, Kansas, and Oregon.
Synopsis: The Centers for Disease Control and Prevention (CDC) issued an alert when 16 cases of unexplained AKI after exposure to synthetic cannabinoids were reported between March and December 2012. Synthetic cannabinoid use is associated with neurologic, sympathomimetic, and cardiovascular toxicity; however, this is the first case series reporting renal toxicity. The 16 patients included 15 males and one female, aged 15-33 years, with no pre-existing renal disease or nephrotoxic medication consumption. All used synthetic cannabinoids within hours to days before developing nausea, vomiting, abdominal, and flank and/or back pain.
Creatinine peaked one to six days after symptom onset. Five patients required hemodialysis, and all 16 recovered. There was no finding specific for all cases on ultrasound and/or biopsy. Toxicologic analysis of specimens was possible in seven cases and revealed a previously unreported fluorinated synthetic cannabinoid compound XLR-11 in all clinical specimens of patients who used the drug within two days of being tested.
Overall, the analysis did not reveal any single compound or brand that could explain all cases.
Bottom line: Clinicians should be aware of the potential for renal or other toxicities in users of synthetic cannabinoid products and should ask about their use in cases of unexplained AKI.
Citation: Murphy TD, Weidenbach KN, Van Houten C, et al. Centers for Disease Control and Prevention. Acute kidney injury associated with synthetic cannabinoid use—multiple states, 2012. MMWR Morb Mortal Wkly Rep. 2013;62(6):93-98.
Dabigatran versus Warfarin in Extended VTE Treatment
Clinical question: Is dabigatran suitable for extended treatment VTE?
Background: In contrast to warfarin (Coumadin), dabigatran (Pradaxa) is given in a fixed dose and does not require frequent laboratory monitoring. Dabigatran has been shown to be noninferior to warfarin in the initial six-month treatment of VTE.
Study design: Two double-blinded, randomized trials: an active-control study and a placebo-control study.
Setting: Two hundred sixty-five sites in 33 countries for the active-control study, and 147 sites in 21 countries for the placebo-control study.
Synopsis: This study enrolled 4,299 adult patients with objectively confirmed, symptomatic, proximal deep vein thrombosis or pulmonary embolism. In the active-control study comparing warfarin and dabigatran, recurrent objectively confirmed symptomatic or fatal VTE was observed in 1.8% of patients in the dabigatran group compared with 1.3% of patients in the warfarin group (P=0.01 for noninferiority). While major or clinically relevant bleeding was less frequent with dabigatran compared to warfarin (hazard ratio, 0.54), more acute coronary syndromes were observed with dabigatran (0.9% vs. 0.2%, P=0.02). In the placebo-control study, symptomatic or fatal VTE was observed in 0.4% of patients in the dabigatran group compared with 5.6% in the placebo group. Clinically relevant bleeding was more common with dabigatran (5.3% vs. 1.8%; hazard ratio 2.92).
Bottom line: Treatment with dabigatran met the pre-specified noninferiority margin in this study. However, it is worth noting that patients with VTE given extended treatment with dabigatran had significantly higher rates of recurrent symptomatic or fatal VTE than patients treated with warfarin.
Citation: Schulman S, Kearson C, Kakkar AK, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med. 2013;368(8):709-718.
Spironolactone Improves Diastolic Function
Clinical question: What is the efficacy of aldosterone receptor blockers on diastolic function and exercise capacity?
Background: Mineralocorticoid receptor activation by aldosterone contributes to the pathophysiology of heart failure (HF) in patients with and without reduced ejection fraction (EF). Aldosterone receptor blockers (spironolactone) reduce overall and cardiovascular mortality in HF patients with reduced EF; however, its effect on HF patients with preserved EF is unknown.
Study design: Prospective, randomized, double-blinded, placebo-controlled trial.
Setting: Ten ambulatory sites in Germany and Austria.
Synopsis: This study enrolled 422 men and women, aged 50 or older, with New York Heart Association (NYHA) Class II or III HF and preserved EF, and randomized them to receive spironolactone 25 mg daily or placebo for one year.
The endpoints included echocardiographic measures of diastolic function and remodeling; N-terminal pro b-type natriuretic peptide (NT pro-BNP) levels; exercise capacity; quality of life; and HF symptoms.
In the spironolactone group, there was significant improvement in echocardiographic measures of diastolic function and remodeling as well as NT pro-BNP levels. However, there was no difference in exercise capacity, quality of life, or HF symptoms when compared to placebo.
The spironolactone group had significantly lower blood pressure than the control group, which may account for some of the remodeling effects. The study may have been underpowered, and the study population might not have had severe enough disease to detect a difference in clinical measures. It remains unknown if structural changes on echocardiography will translate into clinical benefits.
Bottom line: Compared to placebo, spironolactone did improve diastolic function by echo but did not improve exercise capacity.
Citation: Edelmann F, Wachter R, Schmidt A, et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA. 2013;309(8):781-791.
Real-Time, EMR-Based Prediction Tool Accurately Predicts ICU Transfer Risks
Clinical question: Can clinical deterioration be accurately predicted using real-time data from an electronic medical record (EMR), and can it lead to better outcomes using a floor-based intervention?
Background: Research has shown that EMR-based prediction tools can help identify real-time clinical deterioration in ward patients, but an intervention based on these computer-based alerts has not been shown to be effective.
Study design: Randomized controlled crossover study.
Setting: Eight adult medicine wards in an academic medical center in the Midwest.
Synopsis: There were 20,031 patients assigned to intervention versus control based on their floor location. Computerized alerts were generated using a prediction algorithm. For patients admitted to intervention wards, the alerts were sent to the charge nurse via pager. Patients meeting the alert threshold based on the computerized prediction tool had five times higher risk of ICU transfer, and nine times higher risk of death than patients not meeting the alert threshold. Intervention of charge nurse notification via pager did not result in any significant change in length of stay (LOS), ICU transfer, or mortality. Charge nurses in the intervention group were supposed to alert a physician after receiving the computer alert, but the authors did not measure how often this occurred.
Bottom line: A real-time EMR-based prediction tool accurately predicts higher risk of ICU transfer and death, as well as LOS, but a floor-based intervention to alert the charge nurse in real time did not lead to better outcomes.
Citation: Bailey TC, Chen Y, Mao Y, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medicine wards. J Hosp Med. 2013 Feb 25. doi: 10.1002/jhm.2009 [Epub ahead of print].
Hypothermia Protocol and Cardiac Arrest
Clinical question: Is mild therapeutic hypothermia (MTH) following cardiac arrest beneficial and safe?
Background: Those with sudden cardiac arrest often have poor neurologic outcome. There are some studies that show benefit with hypothermia, but information on safety is limited.
Study design: Meta-analysis.
Setting: Europe, the United Kingdom, the U.S., Canada, Japan, and South Korea.
Synopsis: This study pooled data from 63 studies that looked at MTH protocols in the setting of comatose patients as a result of cardiac arrest. The end points included mortality and any complication potentially attributed to the MTH.
When restricting the analysis to include only randomized controlled trials, MTH was associated with decreased risk of in-hospital mortality (RR=0.75, 95% CI: 0.62-0.92), 30-day mortality (RR=0.61, 95% CI 0.45-0.81), and six-month mortality (RR=0.73, 95% CI 0.61-0.88). MTH was associated with increased risk of arrhythmia (RR=1.25, 95% CI: 1.00-1.55) and hypokalemia (RR=2.35, 95% CI: 1.35-4.11); all other complications were similar between groups.
There were inconsistent results regarding benefit in pediatric patients, as well as comatose patients with non-ventricular fibrillation (non-v-fib) arrest (i.e. asystole or pulseless electrical activity).
Bottom line: Mild therapeutic hypothermia can improve survival of comatose patients after v-fib cardiac arrest and is generally safe.
Citation: Xiao G, Guo Q, Xie X, et al. Safety profile and outcome of mild therapeutic hypothermia in patients following cardiac arrest: systematic review and meta-analysis. Emerg Med J. 2013;30:90-100.
SHM Supports Clarification to Observational Status Loophole for Medicare Patients
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
SHM Welcomes Nonphysician Fellows to Hospital Medicine
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
A Tracheostomy Collar Facilitates Quicker Transition


Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Hospitalists Can’t Ignore Rise in CRE Infections
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.