User login
Four Factors Physicians Should Consider Before Job Termination

Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at sharris@mcdonaldhopkins.com.
Nutritional Intervention Can Improve Hospital Patients' Outcome, Reduce Costs

Health-care reform is on everyone’s mind these days, and SHM, along with numerous other groups, believes some reform goals can be achieved through the stomach.
Data show an effective program of nutritional intervention during a patient’s hospital stay can go a long way toward improving patient outcomes and reducing costs.1 Hospitalists, however, often have little formal nutrition training. A multidisciplinary approach to patient nutrition that brings together multiple stakeholders—hospitalists, nurses, and dietitians—might effectively address this need with a team tactic, according to Melissa Parkhurst, MD, medical director of the hospital medicine section at the University of Kansas Medical Center in Kansas City.1
Between 20% and 50% of inpatients suffer from malnutrition.2 Many patients, especially the elderly, are malnourished on admission. Many more become malnourished within a few days of their hospital stay due to NPO orders and the effects of disease on metabolism.2 Malnutrition has been associated with worsened discharge status, longer length of stay, higher costs, and greater mortality, as well as increased risk of:2
- Nosocomial infections;
- Falls;
- Pressure ulcers; and
- 30-day readmissions.

To address malnutrition prevalence and its detrimental effects, SHM and the Academy of Medical-Surgical Nurses (AMSN), the Academy of Nutrition and Dietetics (AND), the American Society of Parenteral and Enteral Nutrition (ASPEN), and Abbott Nutrition have formed the Alliance for Patient Nutrition. Kelly Tappenden, MD, PhD, professor of food science and human nutrition at the University of Illinois at Urbana, says the alliance aims to raise awareness of the impact nutrition can have on patient outcomes (see “Three Steps to Better Nutrition,” below).
The campaign is being initiated with the publication of a consensus paper in several peer-reviewed journals. A baseline survey will be conducted among professionals represented in the alliance to assess their familiarity with the prevalence of malnutrition in a hospital setting. The next step is to foster this change in patient care by providing resources on the alliance’s website (www.malnutrition.com), including malnutrition screening tools, a toolkit to facilitate multidisciplinary collaboration, and continuing medical education (CME) information.

As a founding member of the alliance, SHM is communicating this message to its members, encouraging hospitalists to lead the way in transforming hospital culture to recognize the critical role nutrition plays in patient care.
“Nutrition matters,” Dr. Parkhurst says. “You can be winning the battle and losing the war if you are not paying attention to patient nutrition.”
Team Approach

Beth Quatrara, DNP, RN, director of the nursing research program at the University of Virginia Health System in Charlottesville and nursing spokesperson for the alliance, says several shortcomings can be identified in the nutritional care U.S. hospitals provide from admission through discharge and beyond. For example, the Joint Commission requires that all patients be screened for malnutrition risk within 48 hours of admission. But screening is often as cursory as looking at the patient and deciding that he or she “looks fine.” Diets often are set for patients with no thought to taste, texture, or cultural preferences, or even to such practical matters as ascertaining whether the patient has dentures, Quatrara says. Meal trays are left when patients are out of their rooms for procedures and retrieved by dietary staff before patients return. And except for calorie count orders, accurate records often are not kept of actual food consumption.
The alliance, which is made possible with support from Abbott's nutrition business, recommends that physicians implement a three-step plan to improve patient outcomes. The approach begins with an evaluation of a patient’s nutritional status on admission using a simple, validated screening tool, such as the Malnutrition Screening Tool. When an at-risk status is determined, a more in-depth screening is performed. “When patients at risk for malnutrition can be identified faster, appropriate interventions can be put into place sooner,” Quatrara says.
The second step is nutrition intervention with a personalized nutritional care plan that takes into account the individual’s health conditions, caloric needs, physical limitations, tastes, and preferences. An interdisciplinary team approach can transform hospital nutrition, bringing together hospitalists, nurses, nursing assistants, registered dietitians, and the dietary staff to collaboratively develop a nutrition care plan that will be central to patient’s overall treatment, Dr. Tappenden says.
“There is a science behind nutrition and metabolic care,” Dr. Tappenden says. “Just like any other aspect of patient care, we can’t just throw out a blanket solution.”
But nutritional care cannot stop with developing this plan at the outset. Patients must be rescreened throughout their time at the hospital to measure any changes in nutritional status due to disease progression or treatment success.
For optimal impact, all members of the nutritional care team—nurses, nursing assistants, dietary support staff, and family members—should take responsibility for an essential component of the patient’s care: tracking and reporting consumption to the physician to open a dialogue about balancing an individual’s needs with tastes and preferences.
The hospitalist’s final step is developing a discharge plan that includes nutrition care and education so that patients, families, and caregivers can implement better nutrition at home.
“Nutrition makes sense,” Dr. Tappenden says. “Everything we are working toward in healthcare reform can be achieved by taking more care to make nutrition part of the solution.”
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Kirkland LL, Kashiwagi DT, Brantley S, Scheurer D, Varkey P. Nutrition in the hospitalized patient. J Hosp Med. 2013;8:52-58.
- Alliance for Patient Nutrition. Malnutrition Backgrounder.
- Banks M, Bauer J, Graves N, Ash S. Malnutrition and pressure ulcer risk in adults in Australian health care facilities. Clin Nutr. 2010;26:896-901.
- Fry DE, Pine M, Jones BL, Meimban RJ. Patient characteristics and the occurrence of never events. Arch Surg. 2010;145:148-151.
- Gariballa S, Forster S, Walters S, Powers H. A randomized, double-blind, placebo-controlled trial of nutritional supplementation during acute illness. Am J Med. 2006;119:693-699.
- Neelemaat F, Lips P, Bosmans J, Thijs A, Seidell JC, van Bokhorst-de van der Schuerer MA. Short-term oral nutritional intervention with protein and vitamin D decreases falls in malnourished older adults. J Am Geriatr Soc. 2012;60:691-699.
- Brugler L, DiPrinzio MJ, Bernstein L. The five-year evolution of a malnutrition treatment program in a community hospital. J Qual Improv. 1999;25:191-206.
- Stratton PJ, et al. Enteral nutritional support in prevention and treatment of pressure ulcers: a systematic review and meta-analysis. Ageing Res Rev. 2005;4:422-450.
- Lawson RM, Doshi MK, Barton JR, Cobden I. The effect of unselected post-operative nutritional supplementation on nutritional status and clinical outcomes of elderly orthopaedic patients. Clin Nutr. 2003;22:39-46.
Health-care reform is on everyone’s mind these days, and SHM, along with numerous other groups, believes some reform goals can be achieved through the stomach.
Data show an effective program of nutritional intervention during a patient’s hospital stay can go a long way toward improving patient outcomes and reducing costs.1 Hospitalists, however, often have little formal nutrition training. A multidisciplinary approach to patient nutrition that brings together multiple stakeholders—hospitalists, nurses, and dietitians—might effectively address this need with a team tactic, according to Melissa Parkhurst, MD, medical director of the hospital medicine section at the University of Kansas Medical Center in Kansas City.1
Between 20% and 50% of inpatients suffer from malnutrition.2 Many patients, especially the elderly, are malnourished on admission. Many more become malnourished within a few days of their hospital stay due to NPO orders and the effects of disease on metabolism.2 Malnutrition has been associated with worsened discharge status, longer length of stay, higher costs, and greater mortality, as well as increased risk of:2
- Nosocomial infections;
- Falls;
- Pressure ulcers; and
- 30-day readmissions.
To address malnutrition prevalence and its detrimental effects, SHM and the Academy of Medical-Surgical Nurses (AMSN), the Academy of Nutrition and Dietetics (AND), the American Society of Parenteral and Enteral Nutrition (ASPEN), and Abbott Nutrition have formed the Alliance for Patient Nutrition. Kelly Tappenden, MD, PhD, professor of food science and human nutrition at the University of Illinois at Urbana, says the alliance aims to raise awareness of the impact nutrition can have on patient outcomes (see “Three Steps to Better Nutrition,” below).
The campaign is being initiated with the publication of a consensus paper in several peer-reviewed journals. A baseline survey will be conducted among professionals represented in the alliance to assess their familiarity with the prevalence of malnutrition in a hospital setting. The next step is to foster this change in patient care by providing resources on the alliance’s website (www.malnutrition.com), including malnutrition screening tools, a toolkit to facilitate multidisciplinary collaboration, and continuing medical education (CME) information.
As a founding member of the alliance, SHM is communicating this message to its members, encouraging hospitalists to lead the way in transforming hospital culture to recognize the critical role nutrition plays in patient care.
“Nutrition matters,” Dr. Parkhurst says. “You can be winning the battle and losing the war if you are not paying attention to patient nutrition.”
Team Approach
Beth Quatrara, DNP, RN, director of the nursing research program at the University of Virginia Health System in Charlottesville and nursing spokesperson for the alliance, says several shortcomings can be identified in the nutritional care U.S. hospitals provide from admission through discharge and beyond. For example, the Joint Commission requires that all patients be screened for malnutrition risk within 48 hours of admission. But screening is often as cursory as looking at the patient and deciding that he or she “looks fine.” Diets often are set for patients with no thought to taste, texture, or cultural preferences, or even to such practical matters as ascertaining whether the patient has dentures, Quatrara says. Meal trays are left when patients are out of their rooms for procedures and retrieved by dietary staff before patients return. And except for calorie count orders, accurate records often are not kept of actual food consumption.
The alliance, which is made possible with support from Abbott's nutrition business, recommends that physicians implement a three-step plan to improve patient outcomes. The approach begins with an evaluation of a patient’s nutritional status on admission using a simple, validated screening tool, such as the Malnutrition Screening Tool. When an at-risk status is determined, a more in-depth screening is performed. “When patients at risk for malnutrition can be identified faster, appropriate interventions can be put into place sooner,” Quatrara says.
The second step is nutrition intervention with a personalized nutritional care plan that takes into account the individual’s health conditions, caloric needs, physical limitations, tastes, and preferences. An interdisciplinary team approach can transform hospital nutrition, bringing together hospitalists, nurses, nursing assistants, registered dietitians, and the dietary staff to collaboratively develop a nutrition care plan that will be central to patient’s overall treatment, Dr. Tappenden says.
“There is a science behind nutrition and metabolic care,” Dr. Tappenden says. “Just like any other aspect of patient care, we can’t just throw out a blanket solution.”
But nutritional care cannot stop with developing this plan at the outset. Patients must be rescreened throughout their time at the hospital to measure any changes in nutritional status due to disease progression or treatment success.
For optimal impact, all members of the nutritional care team—nurses, nursing assistants, dietary support staff, and family members—should take responsibility for an essential component of the patient’s care: tracking and reporting consumption to the physician to open a dialogue about balancing an individual’s needs with tastes and preferences.
The hospitalist’s final step is developing a discharge plan that includes nutrition care and education so that patients, families, and caregivers can implement better nutrition at home.
“Nutrition makes sense,” Dr. Tappenden says. “Everything we are working toward in healthcare reform can be achieved by taking more care to make nutrition part of the solution.”
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Kirkland LL, Kashiwagi DT, Brantley S, Scheurer D, Varkey P. Nutrition in the hospitalized patient. J Hosp Med. 2013;8:52-58.
- Alliance for Patient Nutrition. Malnutrition Backgrounder.
- Banks M, Bauer J, Graves N, Ash S. Malnutrition and pressure ulcer risk in adults in Australian health care facilities. Clin Nutr. 2010;26:896-901.
- Fry DE, Pine M, Jones BL, Meimban RJ. Patient characteristics and the occurrence of never events. Arch Surg. 2010;145:148-151.
- Gariballa S, Forster S, Walters S, Powers H. A randomized, double-blind, placebo-controlled trial of nutritional supplementation during acute illness. Am J Med. 2006;119:693-699.
- Neelemaat F, Lips P, Bosmans J, Thijs A, Seidell JC, van Bokhorst-de van der Schuerer MA. Short-term oral nutritional intervention with protein and vitamin D decreases falls in malnourished older adults. J Am Geriatr Soc. 2012;60:691-699.
- Brugler L, DiPrinzio MJ, Bernstein L. The five-year evolution of a malnutrition treatment program in a community hospital. J Qual Improv. 1999;25:191-206.
- Stratton PJ, et al. Enteral nutritional support in prevention and treatment of pressure ulcers: a systematic review and meta-analysis. Ageing Res Rev. 2005;4:422-450.
- Lawson RM, Doshi MK, Barton JR, Cobden I. The effect of unselected post-operative nutritional supplementation on nutritional status and clinical outcomes of elderly orthopaedic patients. Clin Nutr. 2003;22:39-46.
Health-care reform is on everyone’s mind these days, and SHM, along with numerous other groups, believes some reform goals can be achieved through the stomach.
Data show an effective program of nutritional intervention during a patient’s hospital stay can go a long way toward improving patient outcomes and reducing costs.1 Hospitalists, however, often have little formal nutrition training. A multidisciplinary approach to patient nutrition that brings together multiple stakeholders—hospitalists, nurses, and dietitians—might effectively address this need with a team tactic, according to Melissa Parkhurst, MD, medical director of the hospital medicine section at the University of Kansas Medical Center in Kansas City.1
Between 20% and 50% of inpatients suffer from malnutrition.2 Many patients, especially the elderly, are malnourished on admission. Many more become malnourished within a few days of their hospital stay due to NPO orders and the effects of disease on metabolism.2 Malnutrition has been associated with worsened discharge status, longer length of stay, higher costs, and greater mortality, as well as increased risk of:2
- Nosocomial infections;
- Falls;
- Pressure ulcers; and
- 30-day readmissions.
To address malnutrition prevalence and its detrimental effects, SHM and the Academy of Medical-Surgical Nurses (AMSN), the Academy of Nutrition and Dietetics (AND), the American Society of Parenteral and Enteral Nutrition (ASPEN), and Abbott Nutrition have formed the Alliance for Patient Nutrition. Kelly Tappenden, MD, PhD, professor of food science and human nutrition at the University of Illinois at Urbana, says the alliance aims to raise awareness of the impact nutrition can have on patient outcomes (see “Three Steps to Better Nutrition,” below).
The campaign is being initiated with the publication of a consensus paper in several peer-reviewed journals. A baseline survey will be conducted among professionals represented in the alliance to assess their familiarity with the prevalence of malnutrition in a hospital setting. The next step is to foster this change in patient care by providing resources on the alliance’s website (www.malnutrition.com), including malnutrition screening tools, a toolkit to facilitate multidisciplinary collaboration, and continuing medical education (CME) information.
As a founding member of the alliance, SHM is communicating this message to its members, encouraging hospitalists to lead the way in transforming hospital culture to recognize the critical role nutrition plays in patient care.
“Nutrition matters,” Dr. Parkhurst says. “You can be winning the battle and losing the war if you are not paying attention to patient nutrition.”
Team Approach
Beth Quatrara, DNP, RN, director of the nursing research program at the University of Virginia Health System in Charlottesville and nursing spokesperson for the alliance, says several shortcomings can be identified in the nutritional care U.S. hospitals provide from admission through discharge and beyond. For example, the Joint Commission requires that all patients be screened for malnutrition risk within 48 hours of admission. But screening is often as cursory as looking at the patient and deciding that he or she “looks fine.” Diets often are set for patients with no thought to taste, texture, or cultural preferences, or even to such practical matters as ascertaining whether the patient has dentures, Quatrara says. Meal trays are left when patients are out of their rooms for procedures and retrieved by dietary staff before patients return. And except for calorie count orders, accurate records often are not kept of actual food consumption.
The alliance, which is made possible with support from Abbott's nutrition business, recommends that physicians implement a three-step plan to improve patient outcomes. The approach begins with an evaluation of a patient’s nutritional status on admission using a simple, validated screening tool, such as the Malnutrition Screening Tool. When an at-risk status is determined, a more in-depth screening is performed. “When patients at risk for malnutrition can be identified faster, appropriate interventions can be put into place sooner,” Quatrara says.
The second step is nutrition intervention with a personalized nutritional care plan that takes into account the individual’s health conditions, caloric needs, physical limitations, tastes, and preferences. An interdisciplinary team approach can transform hospital nutrition, bringing together hospitalists, nurses, nursing assistants, registered dietitians, and the dietary staff to collaboratively develop a nutrition care plan that will be central to patient’s overall treatment, Dr. Tappenden says.
“There is a science behind nutrition and metabolic care,” Dr. Tappenden says. “Just like any other aspect of patient care, we can’t just throw out a blanket solution.”
But nutritional care cannot stop with developing this plan at the outset. Patients must be rescreened throughout their time at the hospital to measure any changes in nutritional status due to disease progression or treatment success.
For optimal impact, all members of the nutritional care team—nurses, nursing assistants, dietary support staff, and family members—should take responsibility for an essential component of the patient’s care: tracking and reporting consumption to the physician to open a dialogue about balancing an individual’s needs with tastes and preferences.
The hospitalist’s final step is developing a discharge plan that includes nutrition care and education so that patients, families, and caregivers can implement better nutrition at home.
“Nutrition makes sense,” Dr. Tappenden says. “Everything we are working toward in healthcare reform can be achieved by taking more care to make nutrition part of the solution.”
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Kirkland LL, Kashiwagi DT, Brantley S, Scheurer D, Varkey P. Nutrition in the hospitalized patient. J Hosp Med. 2013;8:52-58.
- Alliance for Patient Nutrition. Malnutrition Backgrounder.
- Banks M, Bauer J, Graves N, Ash S. Malnutrition and pressure ulcer risk in adults in Australian health care facilities. Clin Nutr. 2010;26:896-901.
- Fry DE, Pine M, Jones BL, Meimban RJ. Patient characteristics and the occurrence of never events. Arch Surg. 2010;145:148-151.
- Gariballa S, Forster S, Walters S, Powers H. A randomized, double-blind, placebo-controlled trial of nutritional supplementation during acute illness. Am J Med. 2006;119:693-699.
- Neelemaat F, Lips P, Bosmans J, Thijs A, Seidell JC, van Bokhorst-de van der Schuerer MA. Short-term oral nutritional intervention with protein and vitamin D decreases falls in malnourished older adults. J Am Geriatr Soc. 2012;60:691-699.
- Brugler L, DiPrinzio MJ, Bernstein L. The five-year evolution of a malnutrition treatment program in a community hospital. J Qual Improv. 1999;25:191-206.
- Stratton PJ, et al. Enteral nutritional support in prevention and treatment of pressure ulcers: a systematic review and meta-analysis. Ageing Res Rev. 2005;4:422-450.
- Lawson RM, Doshi MK, Barton JR, Cobden I. The effect of unselected post-operative nutritional supplementation on nutritional status and clinical outcomes of elderly orthopaedic patients. Clin Nutr. 2003;22:39-46.
Empathy Can Help Hospitalists Improve Patient Experience, Outcomes


Empathy: ability to understand and share the feelings of another.
In today’s increasingly hyper-measured healthcare world, we are looking more and more at measures of patient outcomes. The Institute for Healthcare Improvement (IHI) touts the Triple Aim principle as the lens through which we should be approaching our work. The Triple Aim is the three-part goal and simultaneous focus of improving the health of the community and our patients, improving affordability of care, and finally and perhaps most elusively, improving the patient experience. Who wouldn’t want to hit on these admirable goals? How do we do it?
In approaching the health aspect of the Triple Aim, we, as hospitalists, have tried-and-true frameworks of process improvement. Clinical research and peer-reviewed publication advance the knowledge of what medicines and procedures can improve care. Although powerful and generally truthful, this system results in a slow diffusion of practice improvement, not to mention idiosyncratic and nonstandardized care. This has led to a new toolkit of improvement techniques: continuous quality improvement, Lean, and Six Sigma. We learn and adopt these and watch our scores go up at a steady pace.
Improving affordability has its challenges, some huge, like our basic cultural ethos that “more is better.” Yet affordability is still something we can grasp. It is rooted in systems we are all familiar with, from basic personal finance to resource allocation to generally accepted accounting principles. We all can grasp that the current system of pay for widgets is teetering at the edge, just waiting for a shove from CMS to send it to its doom. Once this happens, affordability likely will become something we can start to make serious headway against.
Improving the experience of patients and families is perhaps the toughest of the three and where I would like to focus.
Patients First
First, a question: Are experience scores reflective of the true experience of a patient?
Two weeks after discharge, when patients receive their HCAHPS questionnaire in the mail, do they remember the details of their stay? And who was their doctor anyway? The cardiologist who placed a stent? The on-call doctor? The hospitalist who visited them every morning? If all we focus on is the scores, and we lack faith that the scores represent the true experience of patients, then how can we ever truly create a more satisfying experience for our patients?
I believe that the answer lies with empathy. What’s unique about this part of the Triple Aim is that many of the answers are within us. Gaining empathy with our patients requires us to ask questions of them and also to ask questions of ourselves. It requires us to invoke ancient methods of learning and thinking, like walking in another’s shoes for a day or using the Golden Rule. Experience doesn’t lend itself to being taught by PowerPoint. It must be lived and channeled back and out through our emotional selves as empathy.
Using the wisdom of patients themselves is one way to understand their needs and develop the empathy to motivate us to change how we do things in health care. Many organizations around the country have used some form of patient focus group to help learn from patients. Park Nicollet, a large health system in Minnesota, has incorporated family councils in nearly every clinic and care area. They usually are patients or caregivers from the area, bound together by a common disease or location. They dedicate their time, often meeting monthly, to share their stories, give opinions on care processes, and even to shape the design of a care area. Currently, there are more than 100 patient councils in the system, and the number continues to grow.
Film, when done skillfully, is a powerful tool in helping us gain empathy. The Cleveland Clinic has produced an amazing short film called “Empathy: The Human Connection to Patient Care.” It follows patients, families, and staff through the care system. As the camera focuses on each person, floating text appears near them, explaining their situation, inner thoughts, or fears, all overlaid by an emotional piano score. Tears will flow. Understanding follows.
Jim Merlino, MD, Cleveland Clinic’s chief experience officer, explains, “We need to understand that being on the other side of health care is frightening, and our job, our responsibility as people responsible for other people, is to help ease that fear.” Cleveland Clinic has done a remarkable job in reminding us why we went in to health care.
Morgan Spurlock of “Super Size Me” fame produced a reality series called “30 Days.” In each episode, a participant spent 30 days in the shoes of another. In the “Life in a Wheelchair” episode, Super Bowl-winning football player Ray Crockett lives in a wheelchair for 30 days and explores what it is like going through recovery and the healthcare system. He meets several rehabbing paraplegics and quadriplegics and accompanies them through their daily lives at home and the hospital. Viewers gain empathy directly in seeing these patients struggle to get better and work with the healthcare system. We also gain empathy watching Crockett gain empathy. The combination is powerful.
In Patients’ Shoes
In addition to listening and observation, we can begin to literally walk in the shoes of our patients.
I recently attended IHI’s International Forum in London. The National Health Service (NHS) in England is using a new tool to help providers understand what it is like for geriatric patients who must navigate the healthcare system with diminished senses and capabilities. Providers put on an age-simulation suit (www.age-simulation-suit.com) that mimics the impairments of aging. Special goggles fog the vision and narrow the visual field. Head mobility is reduced so that it becomes difficult to see beyond the field cuts. Earmuffs reduce high-frequency hearing and the ability to understand speech clearly. The overall suit impedes motion and reduces strength. Thick gloves make it difficult to coordinate fine motions. Wearing this suit and trying to go through a hospital or clinic setting instantly makes the wearer gain empathy for our patients’ needs.
Most important, be a patient. SHM immediate past president Shaun Frost, MD, SFHM, whose personal mission during his tenure was to help the society understand patient experience, explained it best to me. “In one episode in the hospital with a family member, I learned more about patient experience than all the reading and self-educating I have been doing for the last year.”
I think any of us who have been a patient in the hospital, or accompanied a loved one, comes out frustrated that the healthcare system is so convoluted and lacking in clarity for patients. Then there is often a sense of renewal, hopefully,followed by evangelism to spread their newfound empathy to others in the system.
In our busy work lives as hospitalists, it isn’t easy turning our daily focus away from efficiency and productivity. Yet we must always remain mindful of that core idea every one of us wrote down as the heart of our personal statements on our applications to medical school. Do you remember writing something like this? “I want to help people and relieve suffering in their time of need.”
Empathy is the start of our work.
Dr. Kealey is medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn. He is an SHM board member and SHM president-elect.
Empathy: ability to understand and share the feelings of another.
In today’s increasingly hyper-measured healthcare world, we are looking more and more at measures of patient outcomes. The Institute for Healthcare Improvement (IHI) touts the Triple Aim principle as the lens through which we should be approaching our work. The Triple Aim is the three-part goal and simultaneous focus of improving the health of the community and our patients, improving affordability of care, and finally and perhaps most elusively, improving the patient experience. Who wouldn’t want to hit on these admirable goals? How do we do it?
In approaching the health aspect of the Triple Aim, we, as hospitalists, have tried-and-true frameworks of process improvement. Clinical research and peer-reviewed publication advance the knowledge of what medicines and procedures can improve care. Although powerful and generally truthful, this system results in a slow diffusion of practice improvement, not to mention idiosyncratic and nonstandardized care. This has led to a new toolkit of improvement techniques: continuous quality improvement, Lean, and Six Sigma. We learn and adopt these and watch our scores go up at a steady pace.
Improving affordability has its challenges, some huge, like our basic cultural ethos that “more is better.” Yet affordability is still something we can grasp. It is rooted in systems we are all familiar with, from basic personal finance to resource allocation to generally accepted accounting principles. We all can grasp that the current system of pay for widgets is teetering at the edge, just waiting for a shove from CMS to send it to its doom. Once this happens, affordability likely will become something we can start to make serious headway against.
Improving the experience of patients and families is perhaps the toughest of the three and where I would like to focus.
Patients First
First, a question: Are experience scores reflective of the true experience of a patient?
Two weeks after discharge, when patients receive their HCAHPS questionnaire in the mail, do they remember the details of their stay? And who was their doctor anyway? The cardiologist who placed a stent? The on-call doctor? The hospitalist who visited them every morning? If all we focus on is the scores, and we lack faith that the scores represent the true experience of patients, then how can we ever truly create a more satisfying experience for our patients?
I believe that the answer lies with empathy. What’s unique about this part of the Triple Aim is that many of the answers are within us. Gaining empathy with our patients requires us to ask questions of them and also to ask questions of ourselves. It requires us to invoke ancient methods of learning and thinking, like walking in another’s shoes for a day or using the Golden Rule. Experience doesn’t lend itself to being taught by PowerPoint. It must be lived and channeled back and out through our emotional selves as empathy.
Using the wisdom of patients themselves is one way to understand their needs and develop the empathy to motivate us to change how we do things in health care. Many organizations around the country have used some form of patient focus group to help learn from patients. Park Nicollet, a large health system in Minnesota, has incorporated family councils in nearly every clinic and care area. They usually are patients or caregivers from the area, bound together by a common disease or location. They dedicate their time, often meeting monthly, to share their stories, give opinions on care processes, and even to shape the design of a care area. Currently, there are more than 100 patient councils in the system, and the number continues to grow.
Film, when done skillfully, is a powerful tool in helping us gain empathy. The Cleveland Clinic has produced an amazing short film called “Empathy: The Human Connection to Patient Care.” It follows patients, families, and staff through the care system. As the camera focuses on each person, floating text appears near them, explaining their situation, inner thoughts, or fears, all overlaid by an emotional piano score. Tears will flow. Understanding follows.
Jim Merlino, MD, Cleveland Clinic’s chief experience officer, explains, “We need to understand that being on the other side of health care is frightening, and our job, our responsibility as people responsible for other people, is to help ease that fear.” Cleveland Clinic has done a remarkable job in reminding us why we went in to health care.
Morgan Spurlock of “Super Size Me” fame produced a reality series called “30 Days.” In each episode, a participant spent 30 days in the shoes of another. In the “Life in a Wheelchair” episode, Super Bowl-winning football player Ray Crockett lives in a wheelchair for 30 days and explores what it is like going through recovery and the healthcare system. He meets several rehabbing paraplegics and quadriplegics and accompanies them through their daily lives at home and the hospital. Viewers gain empathy directly in seeing these patients struggle to get better and work with the healthcare system. We also gain empathy watching Crockett gain empathy. The combination is powerful.
In Patients’ Shoes
In addition to listening and observation, we can begin to literally walk in the shoes of our patients.
I recently attended IHI’s International Forum in London. The National Health Service (NHS) in England is using a new tool to help providers understand what it is like for geriatric patients who must navigate the healthcare system with diminished senses and capabilities. Providers put on an age-simulation suit (www.age-simulation-suit.com) that mimics the impairments of aging. Special goggles fog the vision and narrow the visual field. Head mobility is reduced so that it becomes difficult to see beyond the field cuts. Earmuffs reduce high-frequency hearing and the ability to understand speech clearly. The overall suit impedes motion and reduces strength. Thick gloves make it difficult to coordinate fine motions. Wearing this suit and trying to go through a hospital or clinic setting instantly makes the wearer gain empathy for our patients’ needs.
Most important, be a patient. SHM immediate past president Shaun Frost, MD, SFHM, whose personal mission during his tenure was to help the society understand patient experience, explained it best to me. “In one episode in the hospital with a family member, I learned more about patient experience than all the reading and self-educating I have been doing for the last year.”
I think any of us who have been a patient in the hospital, or accompanied a loved one, comes out frustrated that the healthcare system is so convoluted and lacking in clarity for patients. Then there is often a sense of renewal, hopefully,followed by evangelism to spread their newfound empathy to others in the system.
In our busy work lives as hospitalists, it isn’t easy turning our daily focus away from efficiency and productivity. Yet we must always remain mindful of that core idea every one of us wrote down as the heart of our personal statements on our applications to medical school. Do you remember writing something like this? “I want to help people and relieve suffering in their time of need.”
Empathy is the start of our work.
Dr. Kealey is medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn. He is an SHM board member and SHM president-elect.
Empathy: ability to understand and share the feelings of another.
In today’s increasingly hyper-measured healthcare world, we are looking more and more at measures of patient outcomes. The Institute for Healthcare Improvement (IHI) touts the Triple Aim principle as the lens through which we should be approaching our work. The Triple Aim is the three-part goal and simultaneous focus of improving the health of the community and our patients, improving affordability of care, and finally and perhaps most elusively, improving the patient experience. Who wouldn’t want to hit on these admirable goals? How do we do it?
In approaching the health aspect of the Triple Aim, we, as hospitalists, have tried-and-true frameworks of process improvement. Clinical research and peer-reviewed publication advance the knowledge of what medicines and procedures can improve care. Although powerful and generally truthful, this system results in a slow diffusion of practice improvement, not to mention idiosyncratic and nonstandardized care. This has led to a new toolkit of improvement techniques: continuous quality improvement, Lean, and Six Sigma. We learn and adopt these and watch our scores go up at a steady pace.
Improving affordability has its challenges, some huge, like our basic cultural ethos that “more is better.” Yet affordability is still something we can grasp. It is rooted in systems we are all familiar with, from basic personal finance to resource allocation to generally accepted accounting principles. We all can grasp that the current system of pay for widgets is teetering at the edge, just waiting for a shove from CMS to send it to its doom. Once this happens, affordability likely will become something we can start to make serious headway against.
Improving the experience of patients and families is perhaps the toughest of the three and where I would like to focus.
Patients First
First, a question: Are experience scores reflective of the true experience of a patient?
Two weeks after discharge, when patients receive their HCAHPS questionnaire in the mail, do they remember the details of their stay? And who was their doctor anyway? The cardiologist who placed a stent? The on-call doctor? The hospitalist who visited them every morning? If all we focus on is the scores, and we lack faith that the scores represent the true experience of patients, then how can we ever truly create a more satisfying experience for our patients?
I believe that the answer lies with empathy. What’s unique about this part of the Triple Aim is that many of the answers are within us. Gaining empathy with our patients requires us to ask questions of them and also to ask questions of ourselves. It requires us to invoke ancient methods of learning and thinking, like walking in another’s shoes for a day or using the Golden Rule. Experience doesn’t lend itself to being taught by PowerPoint. It must be lived and channeled back and out through our emotional selves as empathy.
Using the wisdom of patients themselves is one way to understand their needs and develop the empathy to motivate us to change how we do things in health care. Many organizations around the country have used some form of patient focus group to help learn from patients. Park Nicollet, a large health system in Minnesota, has incorporated family councils in nearly every clinic and care area. They usually are patients or caregivers from the area, bound together by a common disease or location. They dedicate their time, often meeting monthly, to share their stories, give opinions on care processes, and even to shape the design of a care area. Currently, there are more than 100 patient councils in the system, and the number continues to grow.
Film, when done skillfully, is a powerful tool in helping us gain empathy. The Cleveland Clinic has produced an amazing short film called “Empathy: The Human Connection to Patient Care.” It follows patients, families, and staff through the care system. As the camera focuses on each person, floating text appears near them, explaining their situation, inner thoughts, or fears, all overlaid by an emotional piano score. Tears will flow. Understanding follows.
Jim Merlino, MD, Cleveland Clinic’s chief experience officer, explains, “We need to understand that being on the other side of health care is frightening, and our job, our responsibility as people responsible for other people, is to help ease that fear.” Cleveland Clinic has done a remarkable job in reminding us why we went in to health care.
Morgan Spurlock of “Super Size Me” fame produced a reality series called “30 Days.” In each episode, a participant spent 30 days in the shoes of another. In the “Life in a Wheelchair” episode, Super Bowl-winning football player Ray Crockett lives in a wheelchair for 30 days and explores what it is like going through recovery and the healthcare system. He meets several rehabbing paraplegics and quadriplegics and accompanies them through their daily lives at home and the hospital. Viewers gain empathy directly in seeing these patients struggle to get better and work with the healthcare system. We also gain empathy watching Crockett gain empathy. The combination is powerful.
In Patients’ Shoes
In addition to listening and observation, we can begin to literally walk in the shoes of our patients.
I recently attended IHI’s International Forum in London. The National Health Service (NHS) in England is using a new tool to help providers understand what it is like for geriatric patients who must navigate the healthcare system with diminished senses and capabilities. Providers put on an age-simulation suit (www.age-simulation-suit.com) that mimics the impairments of aging. Special goggles fog the vision and narrow the visual field. Head mobility is reduced so that it becomes difficult to see beyond the field cuts. Earmuffs reduce high-frequency hearing and the ability to understand speech clearly. The overall suit impedes motion and reduces strength. Thick gloves make it difficult to coordinate fine motions. Wearing this suit and trying to go through a hospital or clinic setting instantly makes the wearer gain empathy for our patients’ needs.
Most important, be a patient. SHM immediate past president Shaun Frost, MD, SFHM, whose personal mission during his tenure was to help the society understand patient experience, explained it best to me. “In one episode in the hospital with a family member, I learned more about patient experience than all the reading and self-educating I have been doing for the last year.”
I think any of us who have been a patient in the hospital, or accompanied a loved one, comes out frustrated that the healthcare system is so convoluted and lacking in clarity for patients. Then there is often a sense of renewal, hopefully,followed by evangelism to spread their newfound empathy to others in the system.
In our busy work lives as hospitalists, it isn’t easy turning our daily focus away from efficiency and productivity. Yet we must always remain mindful of that core idea every one of us wrote down as the heart of our personal statements on our applications to medical school. Do you remember writing something like this? “I want to help people and relieve suffering in their time of need.”
Empathy is the start of our work.
Dr. Kealey is medical director of hospital specialties at HealthPartners Medical Group in St. Paul, Minn. He is an SHM board member and SHM president-elect.
Pediatric Hospital Medicine Conference Marks 10th Year
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
Advanced-Practice Providers Have More to Offer Hospital Medicine Groups

Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
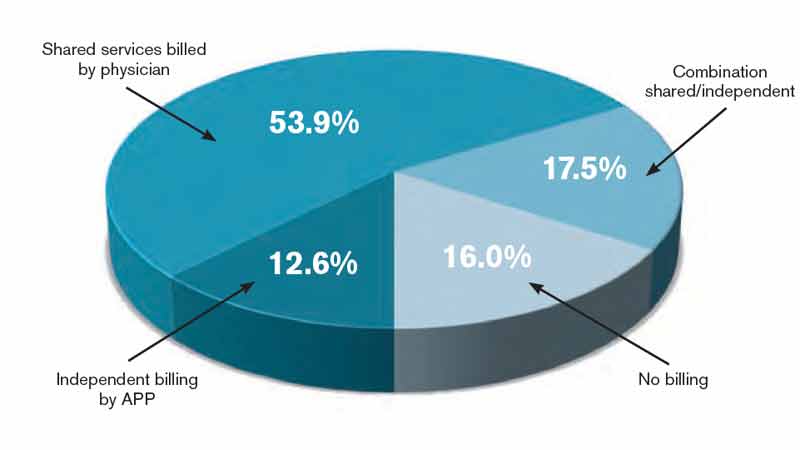
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Start Planning Now for HM14

Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO

Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Quality Improvement (QI) Remains a Central Theme at HM13


Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Pediatric Hospitalist Charts Decade-Long Journey in Health Care

Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Speakers at HM13 Stress Overarching Reform, Day-to-Day Implementation

To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.

“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”

Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.

What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalization Rates Higher Among Abused Elderly
A study published online in JAMA Internal Medicine finds a clear association between elder abuse and hospitalization rates.4
Unadjusted mean annual rate of hospitalization was 1.97% for those with reported elder abuse to social service agencies among 6,674 participants in the Chicago Health and Aging Project between 1993 and 2010.4 That rate was more than three times the rate for those without reported abuse.
The authors define elder abuse to include physical, sexual, or psychological abuse, caregiver neglect, and financial exploitation. Its identification as a risk factor for increased hospitalizations poses important policy implications for the need to identify elder abuse and caregiver neglect, says lead author XinQi Dong, MD, a researcher and geriatrician at Rush University in Chicago. Hospitalists, according to Dr. Dong, should consider screening patients who present with dehydration, malnutrition, delirium, and skin ulcers.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
A study published online in JAMA Internal Medicine finds a clear association between elder abuse and hospitalization rates.4
Unadjusted mean annual rate of hospitalization was 1.97% for those with reported elder abuse to social service agencies among 6,674 participants in the Chicago Health and Aging Project between 1993 and 2010.4 That rate was more than three times the rate for those without reported abuse.
The authors define elder abuse to include physical, sexual, or psychological abuse, caregiver neglect, and financial exploitation. Its identification as a risk factor for increased hospitalizations poses important policy implications for the need to identify elder abuse and caregiver neglect, says lead author XinQi Dong, MD, a researcher and geriatrician at Rush University in Chicago. Hospitalists, according to Dr. Dong, should consider screening patients who present with dehydration, malnutrition, delirium, and skin ulcers.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
A study published online in JAMA Internal Medicine finds a clear association between elder abuse and hospitalization rates.4
Unadjusted mean annual rate of hospitalization was 1.97% for those with reported elder abuse to social service agencies among 6,674 participants in the Chicago Health and Aging Project between 1993 and 2010.4 That rate was more than three times the rate for those without reported abuse.
The authors define elder abuse to include physical, sexual, or psychological abuse, caregiver neglect, and financial exploitation. Its identification as a risk factor for increased hospitalizations poses important policy implications for the need to identify elder abuse and caregiver neglect, says lead author XinQi Dong, MD, a researcher and geriatrician at Rush University in Chicago. Hospitalists, according to Dr. Dong, should consider screening patients who present with dehydration, malnutrition, delirium, and skin ulcers.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed