User login
Sciatic Neuropathy From a Giant Hibernoma of the Thigh: A Case Report
Endovascular Management of Pseudoaneurysms Following Lower Limb Orthopedic Surgery
Asymmetric Bilateral Shoulder Dislocation Involving a Luxatio Erecta Dislocation
Solifenacin‐Induced Small Bowel Pseudo‐Obstruction
Solfenacin succinate, an antimuscarinic agent, is approved for the treatment of overactive bladder and described as well tolerated in the elderly.1 We present the case of solifenacin‐induced small bowel pseudo‐obstruction in an 89‐year‐old woman.
FINDINGS
An 89‐year‐old woman with untreated stage 0 chronic lymphocytic leukemia and a history of stage III colorectal cancer treated with hemicolectomy and adjuvant capecitabine in 2003 was admitted to Johns Hopkins Hospital in 2006. She reported feeling dehydrated, nauseated, and constipated, with decreased output from her colostomy. She also noted no urine output for 4 days and felt that she had to urinate, but I can't. This coincided with a decrease in fluid intake. She denied fevers, chills, abdominal pain, or loss of appetite. While waiting to be seen in the emergency department, the patient was finally able to urinate.
She had no evidence of colon cancer recurrence, with a normal postoperative positron‐emission tomography (PET) scan in 2003, colonoscopy in 2005, and screening computerized tomography (CT) scan in 2005. She also had a history of well‐controlled hypertension and hypothyroidism, hyperlipidemia, chemotherapy‐induced neuropathy, and anxiety.
Her home medication regimen included solifenacin 5 mg once daily (started 10 days prior to her admission) for bladder overactivity, buspirone 5 mg 3 times a day, metoprolol 25 mg twice a day, pantoprazole 40 mg once daily, levothyroxine 100 g once daily, lisinopril/hydrochlorathiazide 20 mg/25 mg twice daily, gabapentin 300 mg twice a day, and fenofibrate 145 mg nightly.
The patient appeared nontoxic. Her exam was remarkable only for hypoactive bowel sounds and mild diffuse abdominal tenderness without distension or peritoneal signs. A Foley catheter was placed, and her postvoid residual was only 50 cc of urine. Her admission serum blood urea nitrogen and creatinine were 90 and 3.4 mg/dL, respectively, as compared with 18 and 0.8 mg/dL 2 months prior to presentation. A CT scan of the abdomen (Figure 1) revealed multiple dilated loops of small bowel with a transition point at the left lower quadrant ostomy site, consistent with a small bowel obstruction. A PET scan revealed no evidence of malignancy. A renal ultrasound showed no evidence of obstruction.

With cessation of solifenacin and lisinopril/hydrochlorothiazide and hydration with normal saline, her constipation resolved, as did her acute renal failure and perception of urinary retention. She began to tolerate a regular diet after 4 days of hospitalization, and her colostomy output normalized. At follow‐up 8 months after admission, her creatinine was 0.8 mg/dL, and a screening abdominal CT showed complete resolution of the small bowel obstruction.
DISCUSSION
We believe that this patient developed small bowel pseudo‐obstruction as well the feeling of urinary retention because of treatment with solifenacin, an antimuscarinic agent approved for the treatment of bladder overactivity. Her acute renal failure was a result of prerenal azotemia. This particular patient was at increased risk for developing antimuscarinic‐induced bowel obstruction because of her previous surgery and exposure to chemotherapy.
In the 4 randomized trials cited in the prescribing information for solifenacin,2 only 189 patients of the 1811 who received the active drug were greater than 75 years old. Healthy elderly patients ranging from 64 to 78 years of age (mean 68.0 years) who received 2 weeks of treatment with solifenacin 5 and 10 mg had a mean AUC024 that was approximately 20% higher than that of younger subjects.3 In the 4 12‐week double‐blind clinical trials in which 1158 patients were treated with solifenacin 10 mg, there were 3 serious intestinal adverse events: 1 patient had a fecal impaction, 1 patient had a colonic obstruction, and 1 patient had an intestinal obstruction.2 Patients receiving solifenacin 5 and 10 mg were more likely to experience constipation than those receiving placebo (5.4%, 13.4%, and 2.9%, respectively).2 Given the dearth of clinical data on patients greater than 75 years old, the effects of age on the pharmacokinetics, the higher likelihood of bowel pathology in the elderly, the increased risk of solifenacin‐induced side effects in the elderly as reported in the pooled analysis of patients at least 65 years old,4 and the small clinical benefit of solifenacin,46 physicians should seriously consider whether the benefits of solifenacin outweigh both the known and the possible risks. 0
| Patients in safety analysis (n) | Constipation, n (%) | Micturition/24 hours | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 5 mg | 10 mg | Placebo | 5 mg | 10 mg | Baseline | Mean decrease from baseline | |||
| Placebo | 5 mg | 10 mg | ||||||||
| ||||||||||
| Chapple et al.6* | 267 | 279 | 268 | 5 (1.9) | 20 (7.2) | 21 (7.8) | 12.0812.32 | 1.2 | 2.19 | 2.61 |
| Cardozo et al.4* | 301 | 299 | 307 | 6 (2.0) | 11 (3.7) | 28 (9.1) | 12.0512.31 | 1.59 | 2.37 | 2.81 |
| Wagg3 | 422 | 192 | 431 | 18 (4.3) | 18 (9.4) | 78 (18.1) | 11.611.7 | 1.1 | 2.0 | 2.5 |
- .Solifenacin provides effective antimuscarinic therapy for the complete management of overactive bladder.Expert Opin Pharmacother.2006;7:2421–2434.
- Yamanouchi Pharma America, Inc.United States prescribing information for solifenacin succinate (Vesicare®), November2004.
- ,,,,.Effect of age on the pharmacokinetics of solifenacin in men and women.Int J Clin Pharmacol Ther.2005;43:227–238.
- ,,.Efficacy and tolerability of solifenacin in elderly subjects with overactive bladder syndrome: a pooled analysis.Am J Geriatr Pharmacother.2006;4(1):14–24.
- ,,, et al.Randomized, double‐blind placebo controlled trial of the once daily antimuscarinic agent solifenacin succinate in patients with overactive bladder.J Urol.2004;172(5 Pt 1):1919–1924.
- ,,, et al.Randomized, double‐blind placebo‐ and tolterodine‐controlled trial of the once‐daily antimuscarinic agent solifenacin in patients with symptomatic overactive bladder.BJU Int.2004;93:303–310.
Solfenacin succinate, an antimuscarinic agent, is approved for the treatment of overactive bladder and described as well tolerated in the elderly.1 We present the case of solifenacin‐induced small bowel pseudo‐obstruction in an 89‐year‐old woman.
FINDINGS
An 89‐year‐old woman with untreated stage 0 chronic lymphocytic leukemia and a history of stage III colorectal cancer treated with hemicolectomy and adjuvant capecitabine in 2003 was admitted to Johns Hopkins Hospital in 2006. She reported feeling dehydrated, nauseated, and constipated, with decreased output from her colostomy. She also noted no urine output for 4 days and felt that she had to urinate, but I can't. This coincided with a decrease in fluid intake. She denied fevers, chills, abdominal pain, or loss of appetite. While waiting to be seen in the emergency department, the patient was finally able to urinate.
She had no evidence of colon cancer recurrence, with a normal postoperative positron‐emission tomography (PET) scan in 2003, colonoscopy in 2005, and screening computerized tomography (CT) scan in 2005. She also had a history of well‐controlled hypertension and hypothyroidism, hyperlipidemia, chemotherapy‐induced neuropathy, and anxiety.
Her home medication regimen included solifenacin 5 mg once daily (started 10 days prior to her admission) for bladder overactivity, buspirone 5 mg 3 times a day, metoprolol 25 mg twice a day, pantoprazole 40 mg once daily, levothyroxine 100 g once daily, lisinopril/hydrochlorathiazide 20 mg/25 mg twice daily, gabapentin 300 mg twice a day, and fenofibrate 145 mg nightly.
The patient appeared nontoxic. Her exam was remarkable only for hypoactive bowel sounds and mild diffuse abdominal tenderness without distension or peritoneal signs. A Foley catheter was placed, and her postvoid residual was only 50 cc of urine. Her admission serum blood urea nitrogen and creatinine were 90 and 3.4 mg/dL, respectively, as compared with 18 and 0.8 mg/dL 2 months prior to presentation. A CT scan of the abdomen (Figure 1) revealed multiple dilated loops of small bowel with a transition point at the left lower quadrant ostomy site, consistent with a small bowel obstruction. A PET scan revealed no evidence of malignancy. A renal ultrasound showed no evidence of obstruction.
With cessation of solifenacin and lisinopril/hydrochlorothiazide and hydration with normal saline, her constipation resolved, as did her acute renal failure and perception of urinary retention. She began to tolerate a regular diet after 4 days of hospitalization, and her colostomy output normalized. At follow‐up 8 months after admission, her creatinine was 0.8 mg/dL, and a screening abdominal CT showed complete resolution of the small bowel obstruction.
DISCUSSION
We believe that this patient developed small bowel pseudo‐obstruction as well the feeling of urinary retention because of treatment with solifenacin, an antimuscarinic agent approved for the treatment of bladder overactivity. Her acute renal failure was a result of prerenal azotemia. This particular patient was at increased risk for developing antimuscarinic‐induced bowel obstruction because of her previous surgery and exposure to chemotherapy.
In the 4 randomized trials cited in the prescribing information for solifenacin,2 only 189 patients of the 1811 who received the active drug were greater than 75 years old. Healthy elderly patients ranging from 64 to 78 years of age (mean 68.0 years) who received 2 weeks of treatment with solifenacin 5 and 10 mg had a mean AUC024 that was approximately 20% higher than that of younger subjects.3 In the 4 12‐week double‐blind clinical trials in which 1158 patients were treated with solifenacin 10 mg, there were 3 serious intestinal adverse events: 1 patient had a fecal impaction, 1 patient had a colonic obstruction, and 1 patient had an intestinal obstruction.2 Patients receiving solifenacin 5 and 10 mg were more likely to experience constipation than those receiving placebo (5.4%, 13.4%, and 2.9%, respectively).2 Given the dearth of clinical data on patients greater than 75 years old, the effects of age on the pharmacokinetics, the higher likelihood of bowel pathology in the elderly, the increased risk of solifenacin‐induced side effects in the elderly as reported in the pooled analysis of patients at least 65 years old,4 and the small clinical benefit of solifenacin,46 physicians should seriously consider whether the benefits of solifenacin outweigh both the known and the possible risks. 0
| Patients in safety analysis (n) | Constipation, n (%) | Micturition/24 hours | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 5 mg | 10 mg | Placebo | 5 mg | 10 mg | Baseline | Mean decrease from baseline | |||
| Placebo | 5 mg | 10 mg | ||||||||
| ||||||||||
| Chapple et al.6* | 267 | 279 | 268 | 5 (1.9) | 20 (7.2) | 21 (7.8) | 12.0812.32 | 1.2 | 2.19 | 2.61 |
| Cardozo et al.4* | 301 | 299 | 307 | 6 (2.0) | 11 (3.7) | 28 (9.1) | 12.0512.31 | 1.59 | 2.37 | 2.81 |
| Wagg3 | 422 | 192 | 431 | 18 (4.3) | 18 (9.4) | 78 (18.1) | 11.611.7 | 1.1 | 2.0 | 2.5 |
Solfenacin succinate, an antimuscarinic agent, is approved for the treatment of overactive bladder and described as well tolerated in the elderly.1 We present the case of solifenacin‐induced small bowel pseudo‐obstruction in an 89‐year‐old woman.
FINDINGS
An 89‐year‐old woman with untreated stage 0 chronic lymphocytic leukemia and a history of stage III colorectal cancer treated with hemicolectomy and adjuvant capecitabine in 2003 was admitted to Johns Hopkins Hospital in 2006. She reported feeling dehydrated, nauseated, and constipated, with decreased output from her colostomy. She also noted no urine output for 4 days and felt that she had to urinate, but I can't. This coincided with a decrease in fluid intake. She denied fevers, chills, abdominal pain, or loss of appetite. While waiting to be seen in the emergency department, the patient was finally able to urinate.
She had no evidence of colon cancer recurrence, with a normal postoperative positron‐emission tomography (PET) scan in 2003, colonoscopy in 2005, and screening computerized tomography (CT) scan in 2005. She also had a history of well‐controlled hypertension and hypothyroidism, hyperlipidemia, chemotherapy‐induced neuropathy, and anxiety.
Her home medication regimen included solifenacin 5 mg once daily (started 10 days prior to her admission) for bladder overactivity, buspirone 5 mg 3 times a day, metoprolol 25 mg twice a day, pantoprazole 40 mg once daily, levothyroxine 100 g once daily, lisinopril/hydrochlorathiazide 20 mg/25 mg twice daily, gabapentin 300 mg twice a day, and fenofibrate 145 mg nightly.
The patient appeared nontoxic. Her exam was remarkable only for hypoactive bowel sounds and mild diffuse abdominal tenderness without distension or peritoneal signs. A Foley catheter was placed, and her postvoid residual was only 50 cc of urine. Her admission serum blood urea nitrogen and creatinine were 90 and 3.4 mg/dL, respectively, as compared with 18 and 0.8 mg/dL 2 months prior to presentation. A CT scan of the abdomen (Figure 1) revealed multiple dilated loops of small bowel with a transition point at the left lower quadrant ostomy site, consistent with a small bowel obstruction. A PET scan revealed no evidence of malignancy. A renal ultrasound showed no evidence of obstruction.
With cessation of solifenacin and lisinopril/hydrochlorothiazide and hydration with normal saline, her constipation resolved, as did her acute renal failure and perception of urinary retention. She began to tolerate a regular diet after 4 days of hospitalization, and her colostomy output normalized. At follow‐up 8 months after admission, her creatinine was 0.8 mg/dL, and a screening abdominal CT showed complete resolution of the small bowel obstruction.
DISCUSSION
We believe that this patient developed small bowel pseudo‐obstruction as well the feeling of urinary retention because of treatment with solifenacin, an antimuscarinic agent approved for the treatment of bladder overactivity. Her acute renal failure was a result of prerenal azotemia. This particular patient was at increased risk for developing antimuscarinic‐induced bowel obstruction because of her previous surgery and exposure to chemotherapy.
In the 4 randomized trials cited in the prescribing information for solifenacin,2 only 189 patients of the 1811 who received the active drug were greater than 75 years old. Healthy elderly patients ranging from 64 to 78 years of age (mean 68.0 years) who received 2 weeks of treatment with solifenacin 5 and 10 mg had a mean AUC024 that was approximately 20% higher than that of younger subjects.3 In the 4 12‐week double‐blind clinical trials in which 1158 patients were treated with solifenacin 10 mg, there were 3 serious intestinal adverse events: 1 patient had a fecal impaction, 1 patient had a colonic obstruction, and 1 patient had an intestinal obstruction.2 Patients receiving solifenacin 5 and 10 mg were more likely to experience constipation than those receiving placebo (5.4%, 13.4%, and 2.9%, respectively).2 Given the dearth of clinical data on patients greater than 75 years old, the effects of age on the pharmacokinetics, the higher likelihood of bowel pathology in the elderly, the increased risk of solifenacin‐induced side effects in the elderly as reported in the pooled analysis of patients at least 65 years old,4 and the small clinical benefit of solifenacin,46 physicians should seriously consider whether the benefits of solifenacin outweigh both the known and the possible risks. 0
| Patients in safety analysis (n) | Constipation, n (%) | Micturition/24 hours | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 5 mg | 10 mg | Placebo | 5 mg | 10 mg | Baseline | Mean decrease from baseline | |||
| Placebo | 5 mg | 10 mg | ||||||||
| ||||||||||
| Chapple et al.6* | 267 | 279 | 268 | 5 (1.9) | 20 (7.2) | 21 (7.8) | 12.0812.32 | 1.2 | 2.19 | 2.61 |
| Cardozo et al.4* | 301 | 299 | 307 | 6 (2.0) | 11 (3.7) | 28 (9.1) | 12.0512.31 | 1.59 | 2.37 | 2.81 |
| Wagg3 | 422 | 192 | 431 | 18 (4.3) | 18 (9.4) | 78 (18.1) | 11.611.7 | 1.1 | 2.0 | 2.5 |
- .Solifenacin provides effective antimuscarinic therapy for the complete management of overactive bladder.Expert Opin Pharmacother.2006;7:2421–2434.
- Yamanouchi Pharma America, Inc.United States prescribing information for solifenacin succinate (Vesicare®), November2004.
- ,,,,.Effect of age on the pharmacokinetics of solifenacin in men and women.Int J Clin Pharmacol Ther.2005;43:227–238.
- ,,.Efficacy and tolerability of solifenacin in elderly subjects with overactive bladder syndrome: a pooled analysis.Am J Geriatr Pharmacother.2006;4(1):14–24.
- ,,, et al.Randomized, double‐blind placebo controlled trial of the once daily antimuscarinic agent solifenacin succinate in patients with overactive bladder.J Urol.2004;172(5 Pt 1):1919–1924.
- ,,, et al.Randomized, double‐blind placebo‐ and tolterodine‐controlled trial of the once‐daily antimuscarinic agent solifenacin in patients with symptomatic overactive bladder.BJU Int.2004;93:303–310.
- .Solifenacin provides effective antimuscarinic therapy for the complete management of overactive bladder.Expert Opin Pharmacother.2006;7:2421–2434.
- Yamanouchi Pharma America, Inc.United States prescribing information for solifenacin succinate (Vesicare®), November2004.
- ,,,,.Effect of age on the pharmacokinetics of solifenacin in men and women.Int J Clin Pharmacol Ther.2005;43:227–238.
- ,,.Efficacy and tolerability of solifenacin in elderly subjects with overactive bladder syndrome: a pooled analysis.Am J Geriatr Pharmacother.2006;4(1):14–24.
- ,,, et al.Randomized, double‐blind placebo controlled trial of the once daily antimuscarinic agent solifenacin succinate in patients with overactive bladder.J Urol.2004;172(5 Pt 1):1919–1924.
- ,,, et al.Randomized, double‐blind placebo‐ and tolterodine‐controlled trial of the once‐daily antimuscarinic agent solifenacin in patients with symptomatic overactive bladder.BJU Int.2004;93:303–310.

Hepatitis C–Associated Penile Necrosis
Leukocytoclastic vasculitis (LCCV) and deep venous thrombosis (DVT) are uncommon manifestations of hepatitis C and when seen, are usually associated with cryoglobulinemia. The presence of hepatitis Cassociated antiphospholipid antibodies (APLAs) such as anticardiolipin antibodies may increase the risk of deep venous thrombosis. Hepatitis Cassociated APLAs and LCCV leading to penile necrosis has not previously been reported, to our knowledge.
CASE
A previously healthy 57‐year‐old white man with hepatitis C presented with a 2‐ to 3‐day history of testicular pain and spreading, tender erythema on his left inner thigh. He reported 2 days of testicular and penile swelling and blackening of his penis 1 day prior to admission. He denied feeling ill, fevers, chills, nausea, vomiting, dysuria, hematuria, abdominal, back or penile pain or trauma, unusual sexual practices, or new medications.
His medical history was significant for IV drug use, hepatitis C infection, and hypertension in the remote past. He was in a 2‐year monogamous relationship with his female partner and denied any history of sexually transmitted diseases; however, he did report erectile dysfunction over the last few months. He worked as a bartender and reportedly drank 1 glass of wine per night. He denied tobacco or current IV drug use and did occasionally smoke marijuana. His medications included atenolol, hydrochlorothiazide, fish oil, cottonseed oil, and a multivitamin. He denied use of any herbal supplements or erectile dysfunction medications.
On physical exam he did not appear toxic. Vital signs were temperature of 37.3C, blood pressure of 155/80, pulse of 100, and O2 saturation of 97% on room air. His HEENT, cardiovascular, lung, and abdominal exams were unremarkable. He had a 5‐cm indurated, dark, erythematous lesion on his left thigh, surrounded by diffuse tracking erythema, and an erythematous and indurated suprapubic region. His uncircumcised penis was swollen and black, with a sharp demarcation near the base of the shaft (Fig. 1). A CT scan with oral and IV contrast demonstrated thickening and edema of the scrotum, suprapubic soft tissue, and penis, with asymmetric enlargement of the left corpora. Mild cirrhosis with associated small gastric varices was also noted. No thrombosis, atherosclerosis, or gas or fluid collection was noted. The bladder, prostate, and seminal vesicles were normal.

A punch biopsy of the leg lesion revealed LCCV with dense fibrin deposition throughout the vessels. Abnormal laboratory data included a mildly elevated WBC count, decreased hemoglobin, thrombocytopenia, mild hyponatremia, low albumin, mildly increased glucose, mild transaminitis, and increased bilirubin. He also had an increased aPTT, elevated ESR, positive hepatitis C PCR and antibodies, positive rheumatoid factor, and high titers of anticardiolipin IgM and anti‐B2GPI IgM.
On hospital day 2, a urological surgery was performed to remove the necrotic penile tissue, including the foreskin, down to the spared tunica albuginea. Pathology studies of the tissue specimens revealed highly vascular subcutaneous tissue with hemorrhage and focal denudation, consistent with necrosis. Following surgery, the patient's platelet count and INR returned to normal levels. No steroids or cytotoxic agents were given. On hospital day 6, the patient developed bilateral leg pain and swelling. Lower extremity doppler ultrasound examination revealed occlusive DVT of the right gastrocnemius, popliteal, and greater saphenous veins, as well thromboses in the left gastrocnemius, soleal, posterior tibial, and greater saphenous veins; thus, enoxaparin therapy was initiated. On hospital day 8, the patient returned to the operating room for a penile tunneling procedure, in which the penis was surgically inserted into the scrotum as an alternative to skin grafting. He recovered well from the surgeries and was discharged on hospital day 11 on oral anticoagulation with warfarin. At follow‐up 1 month after discharge, the patient was doing well and planned for surgery to free his penis from the scrotal sac in 2 months' time.
DISCUSSION
This case illustrates uncommon extrahepatic manifestations of hepatitis C, including leukocytoclastic vasculitis and deep venous thromboses. Our patient, with abnormal LFTs and positive hepatitis C titers, presented with tissue necrosis of the penis and an unidentifiable erythematous lesion on the leg and subsequently developed multiple deep venous thromboses during his hospital course. Initial diagnostic considerations of the penile and skin lesions included fixed drug reaction, trauma, ischemia, infection, arachnid bite, and vasculitis. The patient denied exposure to NSAIDS, antibiotics, anticonvulsants, or anticoagulants, which are commonly reported causes of fixed drug reactions. He denied trauma or spider or bug bites, was nontoxic appearing, afebrile, and had a near‐normal white blood cell count. While awaiting laboratory and biopsy results, we did not initiate pharmacological therapy because of the unknown etiology of the patient's pathology. The patient's workup revealed that his symptoms were most likely secondary to cryoglobulin‐negative hepatitis C infection with leukocytoclastic vasculitis and antiphospholipid antibodies, leading to necrosis of the penile prepucean entity that, to our knowledge, has not been reported.
Leukocytoclastic vasculitis is a complication of many diseases including Henoch‐Schnlein purpura, Wegener's granulomatosis, sepsis, ANCA‐associated vasculitis, SLE, and hepatitis C.14 Leukocytoclastic vasculitis often presents with palpable purpura but may also present with frank necrosis.4 Penile leukocytoclastic vasculitis has been reported in the literature previously5; however, most of these cases involve Wegener's granulomatosis and Henoch‐Schnlein purpura. One case series demonstrated that approximately 1% of patients with hepatitis C develop vasculitis during the course of their illness.19 There has been 1 reported case of penile leukocytoclastic vasculitis, which occurred in a patient with hepatitis C who was found to also have cryoglobulinemia.6 Our patient tested negative for cryoglobulins twice during his hospital stay and also had normal complement levels, which strongly weighs against cryoglobulinemia. One study reported that up to 75% of patients with hepatitis C who develop leukocytoclastic vasculitis will test positive for cryoglobulins6; thus, our patient's presentation with cryoglobulin‐negative leukocytoclastic vasculitis is rare.
Our patient also had a positive titer of anticardiolipin antibodies, which are a subset of APLAs. Antiphospholipid antibodies can be found in autoimmune disease, acute and chronic viral infections, and malignancy.7, 8 Furthermore, APLAs can manifest with arterial and venous thrombosis, and up to 33% of patients with hepatitis C test positive for APLAs.7 The etiology and thrombogenicity of these autoantibodies in the setting of chronic viral hepatitis is still largely unknown, but it has been hypothesized that APLAs may be an autoimmune manifestation of hepatitis C.
Our patient also tested positive for anti‐beta2‐glycoprotien‐1 antibodies, the presence of which may be associated with the occurrence of thrombotic events.9 The presence of these antibodies strengthens the likelihood that this patient's APLAs were pathogenic and likely associated with his skin necrosis as well as his numerous venous thromboses. Previously documented thromboses in patients with hepatitis C and APLAs include avascular bone necrosis, venous thromboembolism, MI, stroke, and cutaneous necrosis.10 There was 1 reported case of a patient with HIV and anticardiolipin antibodies with cutaneous necrosis and testicular thrombosis,10 however, to our knowledge there have been no reported cases of penile necrosis in association with APLAs in a patient with hepatitis C. In this case, treatment with steroids or cytotoxic agents was not warranted because of insufficient evidence to support this practice. However, lifelong anticoagulation with moderate‐intensity warfarin to prevent future thrombosis is indicated.11 These antibodies and their treatment are poorly understood, and further studies are needed to gain insight into both their development and their role in the pathogenesis of disease in patients with viral hepatitis.
In summary, this patient experienced devastating complications of chronic hepatitis C infection, leading to necrosis of the penile prepuce and multiple venous thromboses. This case demonstrates that extrahepatic symptoms of hepatitis C infection, including skin manifestations secondary to leukocytoclastic vasculitis with or without cryglobulinemia, may occur. Furthermore, this case illustrates the increased risk of thrombosis and cutaneous necrosis in patients with chronic hepatitis C infection and associated antiphospholipid antibodies.
Acknowledgements
The authors acknowledge Alan Hunter, MD, Thomas DeLoughery, MD, Brittany Wilson, MD, and Kevin White, MD.
- ,.Dermatologic manifestations of hepatitis C infection.Int J Dermatol.1997;36:251–254.
- ,.Extrahepatic manifestations in patients with chronic hepatitis C virus infection.Curr Opin Rheumatol.2005;17:447–455.
- ,.The prevalence of dermatologic manifestations related to chronic hepatitis C virus infection in a study from a single center in Turkey.Acta Dermatovenerol Alp Panonica Adriat.2005;14:93–98.
- ,,,.Management of leukocytoclastic vasculitis.J Dermatolog Treat.2005;16:193–206.
- ,,, et al.Hepatitis C, cryoglbulinemia, and cutaneous vasculitis associated with unusual and serious manifestations.Am J Gastroenterol.2001;96:2489–2493.
- ,,, et al.Extrahepatic manifestations of chronic hepatitis C.Arthritis Rheumatism.1999;42:2204–2212.
- ,,.Prevalence of antiphospholipid antibodies in patients with chronic lever disease related to alcohol or hepatitis C virus: correlation with liver injury.J Lab Clin Med.1998;31:243–250.
- ,.Antiphospholipid antibodies and antiphospholipid syndrome.Curr Opin Rheumatol.1995;7:389–94.
- ,.Anticardiolipin antibodies in chronic viral hepatitis. Do they have clinical consequences?Eur J Gastroenterol Hepatol.2003;15:717–719.
- ,,, et al.Clinical features related to antiphospholipid syndrome in patients with chronic viral infections (hepatits C virus/HIV infection): description of 82 cases.CID.2004;38:1009–1016.
- ,,.Management of antiphospholipid antibody syndrome: A systematic review.JAMA.2006;295:1050–1057.
Leukocytoclastic vasculitis (LCCV) and deep venous thrombosis (DVT) are uncommon manifestations of hepatitis C and when seen, are usually associated with cryoglobulinemia. The presence of hepatitis Cassociated antiphospholipid antibodies (APLAs) such as anticardiolipin antibodies may increase the risk of deep venous thrombosis. Hepatitis Cassociated APLAs and LCCV leading to penile necrosis has not previously been reported, to our knowledge.
CASE
A previously healthy 57‐year‐old white man with hepatitis C presented with a 2‐ to 3‐day history of testicular pain and spreading, tender erythema on his left inner thigh. He reported 2 days of testicular and penile swelling and blackening of his penis 1 day prior to admission. He denied feeling ill, fevers, chills, nausea, vomiting, dysuria, hematuria, abdominal, back or penile pain or trauma, unusual sexual practices, or new medications.
His medical history was significant for IV drug use, hepatitis C infection, and hypertension in the remote past. He was in a 2‐year monogamous relationship with his female partner and denied any history of sexually transmitted diseases; however, he did report erectile dysfunction over the last few months. He worked as a bartender and reportedly drank 1 glass of wine per night. He denied tobacco or current IV drug use and did occasionally smoke marijuana. His medications included atenolol, hydrochlorothiazide, fish oil, cottonseed oil, and a multivitamin. He denied use of any herbal supplements or erectile dysfunction medications.
On physical exam he did not appear toxic. Vital signs were temperature of 37.3C, blood pressure of 155/80, pulse of 100, and O2 saturation of 97% on room air. His HEENT, cardiovascular, lung, and abdominal exams were unremarkable. He had a 5‐cm indurated, dark, erythematous lesion on his left thigh, surrounded by diffuse tracking erythema, and an erythematous and indurated suprapubic region. His uncircumcised penis was swollen and black, with a sharp demarcation near the base of the shaft (Fig. 1). A CT scan with oral and IV contrast demonstrated thickening and edema of the scrotum, suprapubic soft tissue, and penis, with asymmetric enlargement of the left corpora. Mild cirrhosis with associated small gastric varices was also noted. No thrombosis, atherosclerosis, or gas or fluid collection was noted. The bladder, prostate, and seminal vesicles were normal.
A punch biopsy of the leg lesion revealed LCCV with dense fibrin deposition throughout the vessels. Abnormal laboratory data included a mildly elevated WBC count, decreased hemoglobin, thrombocytopenia, mild hyponatremia, low albumin, mildly increased glucose, mild transaminitis, and increased bilirubin. He also had an increased aPTT, elevated ESR, positive hepatitis C PCR and antibodies, positive rheumatoid factor, and high titers of anticardiolipin IgM and anti‐B2GPI IgM.
On hospital day 2, a urological surgery was performed to remove the necrotic penile tissue, including the foreskin, down to the spared tunica albuginea. Pathology studies of the tissue specimens revealed highly vascular subcutaneous tissue with hemorrhage and focal denudation, consistent with necrosis. Following surgery, the patient's platelet count and INR returned to normal levels. No steroids or cytotoxic agents were given. On hospital day 6, the patient developed bilateral leg pain and swelling. Lower extremity doppler ultrasound examination revealed occlusive DVT of the right gastrocnemius, popliteal, and greater saphenous veins, as well thromboses in the left gastrocnemius, soleal, posterior tibial, and greater saphenous veins; thus, enoxaparin therapy was initiated. On hospital day 8, the patient returned to the operating room for a penile tunneling procedure, in which the penis was surgically inserted into the scrotum as an alternative to skin grafting. He recovered well from the surgeries and was discharged on hospital day 11 on oral anticoagulation with warfarin. At follow‐up 1 month after discharge, the patient was doing well and planned for surgery to free his penis from the scrotal sac in 2 months' time.
DISCUSSION
This case illustrates uncommon extrahepatic manifestations of hepatitis C, including leukocytoclastic vasculitis and deep venous thromboses. Our patient, with abnormal LFTs and positive hepatitis C titers, presented with tissue necrosis of the penis and an unidentifiable erythematous lesion on the leg and subsequently developed multiple deep venous thromboses during his hospital course. Initial diagnostic considerations of the penile and skin lesions included fixed drug reaction, trauma, ischemia, infection, arachnid bite, and vasculitis. The patient denied exposure to NSAIDS, antibiotics, anticonvulsants, or anticoagulants, which are commonly reported causes of fixed drug reactions. He denied trauma or spider or bug bites, was nontoxic appearing, afebrile, and had a near‐normal white blood cell count. While awaiting laboratory and biopsy results, we did not initiate pharmacological therapy because of the unknown etiology of the patient's pathology. The patient's workup revealed that his symptoms were most likely secondary to cryoglobulin‐negative hepatitis C infection with leukocytoclastic vasculitis and antiphospholipid antibodies, leading to necrosis of the penile prepucean entity that, to our knowledge, has not been reported.
Leukocytoclastic vasculitis is a complication of many diseases including Henoch‐Schnlein purpura, Wegener's granulomatosis, sepsis, ANCA‐associated vasculitis, SLE, and hepatitis C.14 Leukocytoclastic vasculitis often presents with palpable purpura but may also present with frank necrosis.4 Penile leukocytoclastic vasculitis has been reported in the literature previously5; however, most of these cases involve Wegener's granulomatosis and Henoch‐Schnlein purpura. One case series demonstrated that approximately 1% of patients with hepatitis C develop vasculitis during the course of their illness.19 There has been 1 reported case of penile leukocytoclastic vasculitis, which occurred in a patient with hepatitis C who was found to also have cryoglobulinemia.6 Our patient tested negative for cryoglobulins twice during his hospital stay and also had normal complement levels, which strongly weighs against cryoglobulinemia. One study reported that up to 75% of patients with hepatitis C who develop leukocytoclastic vasculitis will test positive for cryoglobulins6; thus, our patient's presentation with cryoglobulin‐negative leukocytoclastic vasculitis is rare.
Our patient also had a positive titer of anticardiolipin antibodies, which are a subset of APLAs. Antiphospholipid antibodies can be found in autoimmune disease, acute and chronic viral infections, and malignancy.7, 8 Furthermore, APLAs can manifest with arterial and venous thrombosis, and up to 33% of patients with hepatitis C test positive for APLAs.7 The etiology and thrombogenicity of these autoantibodies in the setting of chronic viral hepatitis is still largely unknown, but it has been hypothesized that APLAs may be an autoimmune manifestation of hepatitis C.
Our patient also tested positive for anti‐beta2‐glycoprotien‐1 antibodies, the presence of which may be associated with the occurrence of thrombotic events.9 The presence of these antibodies strengthens the likelihood that this patient's APLAs were pathogenic and likely associated with his skin necrosis as well as his numerous venous thromboses. Previously documented thromboses in patients with hepatitis C and APLAs include avascular bone necrosis, venous thromboembolism, MI, stroke, and cutaneous necrosis.10 There was 1 reported case of a patient with HIV and anticardiolipin antibodies with cutaneous necrosis and testicular thrombosis,10 however, to our knowledge there have been no reported cases of penile necrosis in association with APLAs in a patient with hepatitis C. In this case, treatment with steroids or cytotoxic agents was not warranted because of insufficient evidence to support this practice. However, lifelong anticoagulation with moderate‐intensity warfarin to prevent future thrombosis is indicated.11 These antibodies and their treatment are poorly understood, and further studies are needed to gain insight into both their development and their role in the pathogenesis of disease in patients with viral hepatitis.
In summary, this patient experienced devastating complications of chronic hepatitis C infection, leading to necrosis of the penile prepuce and multiple venous thromboses. This case demonstrates that extrahepatic symptoms of hepatitis C infection, including skin manifestations secondary to leukocytoclastic vasculitis with or without cryglobulinemia, may occur. Furthermore, this case illustrates the increased risk of thrombosis and cutaneous necrosis in patients with chronic hepatitis C infection and associated antiphospholipid antibodies.
Acknowledgements
The authors acknowledge Alan Hunter, MD, Thomas DeLoughery, MD, Brittany Wilson, MD, and Kevin White, MD.
Leukocytoclastic vasculitis (LCCV) and deep venous thrombosis (DVT) are uncommon manifestations of hepatitis C and when seen, are usually associated with cryoglobulinemia. The presence of hepatitis Cassociated antiphospholipid antibodies (APLAs) such as anticardiolipin antibodies may increase the risk of deep venous thrombosis. Hepatitis Cassociated APLAs and LCCV leading to penile necrosis has not previously been reported, to our knowledge.
CASE
A previously healthy 57‐year‐old white man with hepatitis C presented with a 2‐ to 3‐day history of testicular pain and spreading, tender erythema on his left inner thigh. He reported 2 days of testicular and penile swelling and blackening of his penis 1 day prior to admission. He denied feeling ill, fevers, chills, nausea, vomiting, dysuria, hematuria, abdominal, back or penile pain or trauma, unusual sexual practices, or new medications.
His medical history was significant for IV drug use, hepatitis C infection, and hypertension in the remote past. He was in a 2‐year monogamous relationship with his female partner and denied any history of sexually transmitted diseases; however, he did report erectile dysfunction over the last few months. He worked as a bartender and reportedly drank 1 glass of wine per night. He denied tobacco or current IV drug use and did occasionally smoke marijuana. His medications included atenolol, hydrochlorothiazide, fish oil, cottonseed oil, and a multivitamin. He denied use of any herbal supplements or erectile dysfunction medications.
On physical exam he did not appear toxic. Vital signs were temperature of 37.3C, blood pressure of 155/80, pulse of 100, and O2 saturation of 97% on room air. His HEENT, cardiovascular, lung, and abdominal exams were unremarkable. He had a 5‐cm indurated, dark, erythematous lesion on his left thigh, surrounded by diffuse tracking erythema, and an erythematous and indurated suprapubic region. His uncircumcised penis was swollen and black, with a sharp demarcation near the base of the shaft (Fig. 1). A CT scan with oral and IV contrast demonstrated thickening and edema of the scrotum, suprapubic soft tissue, and penis, with asymmetric enlargement of the left corpora. Mild cirrhosis with associated small gastric varices was also noted. No thrombosis, atherosclerosis, or gas or fluid collection was noted. The bladder, prostate, and seminal vesicles were normal.
A punch biopsy of the leg lesion revealed LCCV with dense fibrin deposition throughout the vessels. Abnormal laboratory data included a mildly elevated WBC count, decreased hemoglobin, thrombocytopenia, mild hyponatremia, low albumin, mildly increased glucose, mild transaminitis, and increased bilirubin. He also had an increased aPTT, elevated ESR, positive hepatitis C PCR and antibodies, positive rheumatoid factor, and high titers of anticardiolipin IgM and anti‐B2GPI IgM.
On hospital day 2, a urological surgery was performed to remove the necrotic penile tissue, including the foreskin, down to the spared tunica albuginea. Pathology studies of the tissue specimens revealed highly vascular subcutaneous tissue with hemorrhage and focal denudation, consistent with necrosis. Following surgery, the patient's platelet count and INR returned to normal levels. No steroids or cytotoxic agents were given. On hospital day 6, the patient developed bilateral leg pain and swelling. Lower extremity doppler ultrasound examination revealed occlusive DVT of the right gastrocnemius, popliteal, and greater saphenous veins, as well thromboses in the left gastrocnemius, soleal, posterior tibial, and greater saphenous veins; thus, enoxaparin therapy was initiated. On hospital day 8, the patient returned to the operating room for a penile tunneling procedure, in which the penis was surgically inserted into the scrotum as an alternative to skin grafting. He recovered well from the surgeries and was discharged on hospital day 11 on oral anticoagulation with warfarin. At follow‐up 1 month after discharge, the patient was doing well and planned for surgery to free his penis from the scrotal sac in 2 months' time.
DISCUSSION
This case illustrates uncommon extrahepatic manifestations of hepatitis C, including leukocytoclastic vasculitis and deep venous thromboses. Our patient, with abnormal LFTs and positive hepatitis C titers, presented with tissue necrosis of the penis and an unidentifiable erythematous lesion on the leg and subsequently developed multiple deep venous thromboses during his hospital course. Initial diagnostic considerations of the penile and skin lesions included fixed drug reaction, trauma, ischemia, infection, arachnid bite, and vasculitis. The patient denied exposure to NSAIDS, antibiotics, anticonvulsants, or anticoagulants, which are commonly reported causes of fixed drug reactions. He denied trauma or spider or bug bites, was nontoxic appearing, afebrile, and had a near‐normal white blood cell count. While awaiting laboratory and biopsy results, we did not initiate pharmacological therapy because of the unknown etiology of the patient's pathology. The patient's workup revealed that his symptoms were most likely secondary to cryoglobulin‐negative hepatitis C infection with leukocytoclastic vasculitis and antiphospholipid antibodies, leading to necrosis of the penile prepucean entity that, to our knowledge, has not been reported.
Leukocytoclastic vasculitis is a complication of many diseases including Henoch‐Schnlein purpura, Wegener's granulomatosis, sepsis, ANCA‐associated vasculitis, SLE, and hepatitis C.14 Leukocytoclastic vasculitis often presents with palpable purpura but may also present with frank necrosis.4 Penile leukocytoclastic vasculitis has been reported in the literature previously5; however, most of these cases involve Wegener's granulomatosis and Henoch‐Schnlein purpura. One case series demonstrated that approximately 1% of patients with hepatitis C develop vasculitis during the course of their illness.19 There has been 1 reported case of penile leukocytoclastic vasculitis, which occurred in a patient with hepatitis C who was found to also have cryoglobulinemia.6 Our patient tested negative for cryoglobulins twice during his hospital stay and also had normal complement levels, which strongly weighs against cryoglobulinemia. One study reported that up to 75% of patients with hepatitis C who develop leukocytoclastic vasculitis will test positive for cryoglobulins6; thus, our patient's presentation with cryoglobulin‐negative leukocytoclastic vasculitis is rare.
Our patient also had a positive titer of anticardiolipin antibodies, which are a subset of APLAs. Antiphospholipid antibodies can be found in autoimmune disease, acute and chronic viral infections, and malignancy.7, 8 Furthermore, APLAs can manifest with arterial and venous thrombosis, and up to 33% of patients with hepatitis C test positive for APLAs.7 The etiology and thrombogenicity of these autoantibodies in the setting of chronic viral hepatitis is still largely unknown, but it has been hypothesized that APLAs may be an autoimmune manifestation of hepatitis C.
Our patient also tested positive for anti‐beta2‐glycoprotien‐1 antibodies, the presence of which may be associated with the occurrence of thrombotic events.9 The presence of these antibodies strengthens the likelihood that this patient's APLAs were pathogenic and likely associated with his skin necrosis as well as his numerous venous thromboses. Previously documented thromboses in patients with hepatitis C and APLAs include avascular bone necrosis, venous thromboembolism, MI, stroke, and cutaneous necrosis.10 There was 1 reported case of a patient with HIV and anticardiolipin antibodies with cutaneous necrosis and testicular thrombosis,10 however, to our knowledge there have been no reported cases of penile necrosis in association with APLAs in a patient with hepatitis C. In this case, treatment with steroids or cytotoxic agents was not warranted because of insufficient evidence to support this practice. However, lifelong anticoagulation with moderate‐intensity warfarin to prevent future thrombosis is indicated.11 These antibodies and their treatment are poorly understood, and further studies are needed to gain insight into both their development and their role in the pathogenesis of disease in patients with viral hepatitis.
In summary, this patient experienced devastating complications of chronic hepatitis C infection, leading to necrosis of the penile prepuce and multiple venous thromboses. This case demonstrates that extrahepatic symptoms of hepatitis C infection, including skin manifestations secondary to leukocytoclastic vasculitis with or without cryglobulinemia, may occur. Furthermore, this case illustrates the increased risk of thrombosis and cutaneous necrosis in patients with chronic hepatitis C infection and associated antiphospholipid antibodies.
Acknowledgements
The authors acknowledge Alan Hunter, MD, Thomas DeLoughery, MD, Brittany Wilson, MD, and Kevin White, MD.
- ,.Dermatologic manifestations of hepatitis C infection.Int J Dermatol.1997;36:251–254.
- ,.Extrahepatic manifestations in patients with chronic hepatitis C virus infection.Curr Opin Rheumatol.2005;17:447–455.
- ,.The prevalence of dermatologic manifestations related to chronic hepatitis C virus infection in a study from a single center in Turkey.Acta Dermatovenerol Alp Panonica Adriat.2005;14:93–98.
- ,,,.Management of leukocytoclastic vasculitis.J Dermatolog Treat.2005;16:193–206.
- ,,, et al.Hepatitis C, cryoglbulinemia, and cutaneous vasculitis associated with unusual and serious manifestations.Am J Gastroenterol.2001;96:2489–2493.
- ,,, et al.Extrahepatic manifestations of chronic hepatitis C.Arthritis Rheumatism.1999;42:2204–2212.
- ,,.Prevalence of antiphospholipid antibodies in patients with chronic lever disease related to alcohol or hepatitis C virus: correlation with liver injury.J Lab Clin Med.1998;31:243–250.
- ,.Antiphospholipid antibodies and antiphospholipid syndrome.Curr Opin Rheumatol.1995;7:389–94.
- ,.Anticardiolipin antibodies in chronic viral hepatitis. Do they have clinical consequences?Eur J Gastroenterol Hepatol.2003;15:717–719.
- ,,, et al.Clinical features related to antiphospholipid syndrome in patients with chronic viral infections (hepatits C virus/HIV infection): description of 82 cases.CID.2004;38:1009–1016.
- ,,.Management of antiphospholipid antibody syndrome: A systematic review.JAMA.2006;295:1050–1057.
- ,.Dermatologic manifestations of hepatitis C infection.Int J Dermatol.1997;36:251–254.
- ,.Extrahepatic manifestations in patients with chronic hepatitis C virus infection.Curr Opin Rheumatol.2005;17:447–455.
- ,.The prevalence of dermatologic manifestations related to chronic hepatitis C virus infection in a study from a single center in Turkey.Acta Dermatovenerol Alp Panonica Adriat.2005;14:93–98.
- ,,,.Management of leukocytoclastic vasculitis.J Dermatolog Treat.2005;16:193–206.
- ,,, et al.Hepatitis C, cryoglbulinemia, and cutaneous vasculitis associated with unusual and serious manifestations.Am J Gastroenterol.2001;96:2489–2493.
- ,,, et al.Extrahepatic manifestations of chronic hepatitis C.Arthritis Rheumatism.1999;42:2204–2212.
- ,,.Prevalence of antiphospholipid antibodies in patients with chronic lever disease related to alcohol or hepatitis C virus: correlation with liver injury.J Lab Clin Med.1998;31:243–250.
- ,.Antiphospholipid antibodies and antiphospholipid syndrome.Curr Opin Rheumatol.1995;7:389–94.
- ,.Anticardiolipin antibodies in chronic viral hepatitis. Do they have clinical consequences?Eur J Gastroenterol Hepatol.2003;15:717–719.
- ,,, et al.Clinical features related to antiphospholipid syndrome in patients with chronic viral infections (hepatits C virus/HIV infection): description of 82 cases.CID.2004;38:1009–1016.
- ,,.Management of antiphospholipid antibody syndrome: A systematic review.JAMA.2006;295:1050–1057.

Unusual Cardiac Rhythm Device Infection
A 35‐year‐old woman with a history of hypertrophic cardiomyopathy survived a ventricular fibrillation cardiac arrest. She subsequently underwent placement of a single, transvenous right ventricular lead implantable cardioverter defibrillator (ICD) system. The lead was an active fixation model, and the generator was placed in a left infraclavicular subcutaneous pocket.
Six months later, she presented with a 5‐week illness consisting of productive cough, fever, anorexia, and myalgias. Physical exam was notable for a rapid heart rate with a variable S1. Labs were notable for a leukocytosis with predominance of neutrophils. An ECG demonstrated atrial fibrillation.
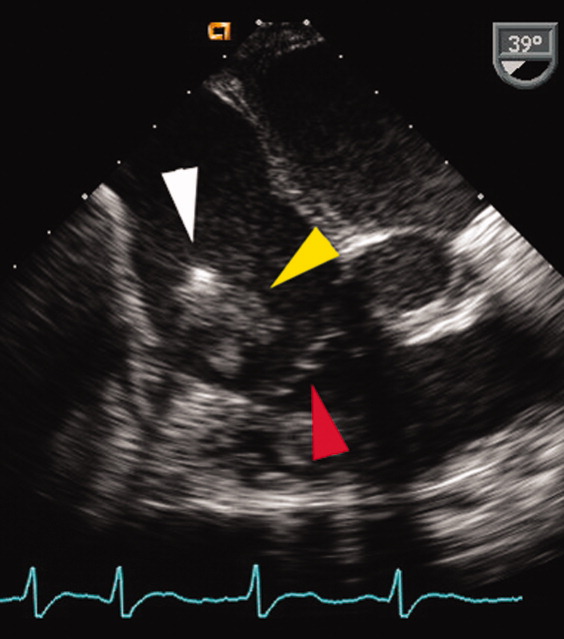
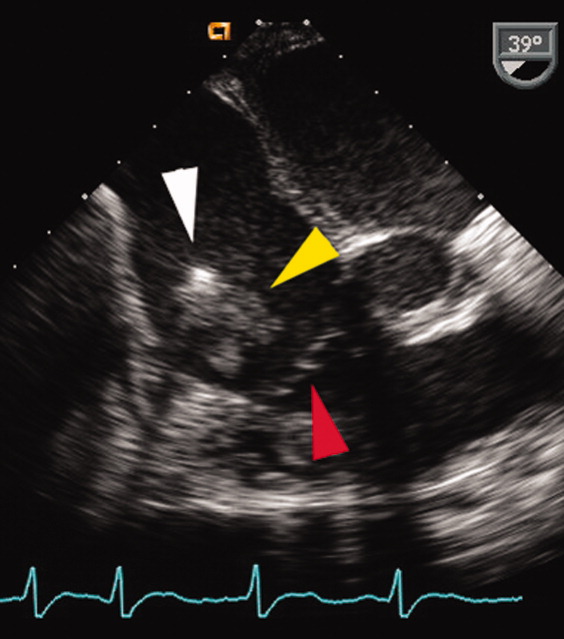
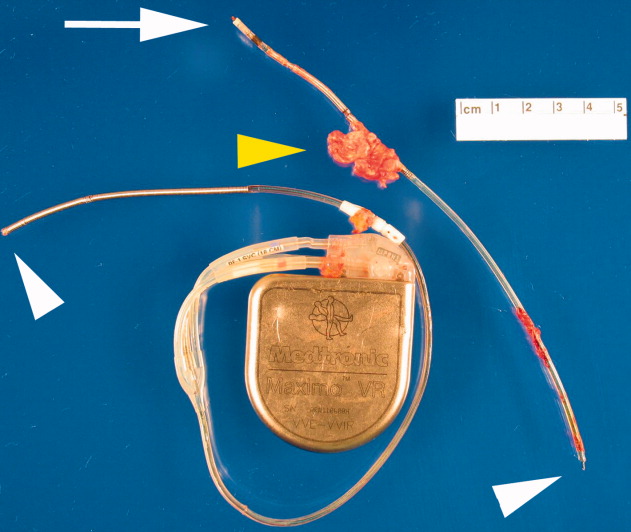
A transesophageal echocardiogram (TEE) was performed in anticipation of a cardioversion for atrial fibrillation. The TEE demonstrated a mass in the right atrium that was attached to the ICD lead, with possible involvement of the tricuspid valve leaflets (Fig. 1). The mass, characterized as multiple confluent bulky segments, was freely mobile and measured about 1.8 cm at its greatest dimension. Therefore, cardioversion was not performed. Within 72 hours, multiple aerobic BACTEC blood cultures identified Haemophilus parainfluenzae, beta lactamase negative. The patient underwent a median sternotomy to remove the ICD lead and generator (Fig. 2). The septal leaflet of the tricuspid valve was debrided. The patient was treated with a prolonged course of ceftriaxone without clinical or microbiologic signs of persistent infection.
DISCUSSION
Research has demonstrated that the rise in cardiac device infections is greater than the rise in the rate of implantation of these devices over the same time period.1 Most infections with cardiac rhythm devices are primary infections, which begin at the pocket and frequently present around generator placement or exchange.2, 3 Because the intravascular leads are continuous to the pocket, there remains a risk for lead and systemic infection.
This case illustrates 2 important concepts. Secondary device infections, which usually result from bacteria originating at a site other than the generator pocket, are less common and tend to involve the intravascular lead.2, 4 Seeding of the intravascular lead frequently occurs with either Staphylococcus aureus or coagulase‐negative Staphylococci.2, 4 Therefore, H. parainfluenzae, a gram‐negative bacillus that can be part of the normal flora of the upper respiratory tract, is not a commonly encountered pathogen for secondary lead infections. Given the respiratory tract symptoms, this was likely the source in this patient. When the lead, generator, or both are infected, this necessitates removal of the entire system.
Furthermore, H. parainfluenzae is categorized with the HACEK organisms (Haemophilus species including H. aphrophilus, H. parainfluenzae, and H. paraphrophilus; Actinobacillus actinomycetemcomitans; Cardiobacterium hominis; Eikenella corrodens; Kingella kingae), a group of fastidious gram‐negative bacilli historically thought to be a common cause of culture‐negative endocarditis. Recent retrospective studies suggest that a prolonged incubation for HACEK organisms is generally not necessary because of advances in culture media and automated blood culture systems.5, 6 As shown in this case, the organism was cultured in less than 72 hours. Therefore, HACEK organisms, when used with modern culture media in addition to automated blood culture systems, are unlikely to be causes of true culture‐negative device or valve infection, provided the patient has had no recent exposure to antibiotics and adequate blood cultures have been obtained. If a cardiac device infection is suspected, blood cultures obtained before commencement of antibiotics and adequate sampling of blood for culture are more likely to identify the pathogen than are blood cultures from prolonged incubation.
- ,,, et al.Increasing rates of cardiac device infections among Medicare beneficiaries: 1990–1999.Am Heart J.2004;147:582–586.
- ,.Infections of intracardiac devices. Cardiol Clin. 2003; 21: 253–271
- ,,,,,.Diagnosis and management of infections involving implantable electrophysiologic cardiac devices.Ann Intern Med.2000;133:604–608.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104:1029–1033.
- ,,, et al.Utility of extended blood culture incubation for isolation of Haemophilus, Actinobacillus, Cardiobacterium, Eikenella and Kingella organisms: a retrospective multicenter evaluation.J Clin Microbiol.2006;44(1):257–259.
- ,,.Prolonged incubation and extensive subculturing do not increase recovery of clinically significant microorganisms from standard automated blood cultures.Clin Infect Dis.2005;41:1677–1680.
A 35‐year‐old woman with a history of hypertrophic cardiomyopathy survived a ventricular fibrillation cardiac arrest. She subsequently underwent placement of a single, transvenous right ventricular lead implantable cardioverter defibrillator (ICD) system. The lead was an active fixation model, and the generator was placed in a left infraclavicular subcutaneous pocket.
Six months later, she presented with a 5‐week illness consisting of productive cough, fever, anorexia, and myalgias. Physical exam was notable for a rapid heart rate with a variable S1. Labs were notable for a leukocytosis with predominance of neutrophils. An ECG demonstrated atrial fibrillation.
A transesophageal echocardiogram (TEE) was performed in anticipation of a cardioversion for atrial fibrillation. The TEE demonstrated a mass in the right atrium that was attached to the ICD lead, with possible involvement of the tricuspid valve leaflets (Fig. 1). The mass, characterized as multiple confluent bulky segments, was freely mobile and measured about 1.8 cm at its greatest dimension. Therefore, cardioversion was not performed. Within 72 hours, multiple aerobic BACTEC blood cultures identified Haemophilus parainfluenzae, beta lactamase negative. The patient underwent a median sternotomy to remove the ICD lead and generator (Fig. 2). The septal leaflet of the tricuspid valve was debrided. The patient was treated with a prolonged course of ceftriaxone without clinical or microbiologic signs of persistent infection.
DISCUSSION
Research has demonstrated that the rise in cardiac device infections is greater than the rise in the rate of implantation of these devices over the same time period.1 Most infections with cardiac rhythm devices are primary infections, which begin at the pocket and frequently present around generator placement or exchange.2, 3 Because the intravascular leads are continuous to the pocket, there remains a risk for lead and systemic infection.
This case illustrates 2 important concepts. Secondary device infections, which usually result from bacteria originating at a site other than the generator pocket, are less common and tend to involve the intravascular lead.2, 4 Seeding of the intravascular lead frequently occurs with either Staphylococcus aureus or coagulase‐negative Staphylococci.2, 4 Therefore, H. parainfluenzae, a gram‐negative bacillus that can be part of the normal flora of the upper respiratory tract, is not a commonly encountered pathogen for secondary lead infections. Given the respiratory tract symptoms, this was likely the source in this patient. When the lead, generator, or both are infected, this necessitates removal of the entire system.
Furthermore, H. parainfluenzae is categorized with the HACEK organisms (Haemophilus species including H. aphrophilus, H. parainfluenzae, and H. paraphrophilus; Actinobacillus actinomycetemcomitans; Cardiobacterium hominis; Eikenella corrodens; Kingella kingae), a group of fastidious gram‐negative bacilli historically thought to be a common cause of culture‐negative endocarditis. Recent retrospective studies suggest that a prolonged incubation for HACEK organisms is generally not necessary because of advances in culture media and automated blood culture systems.5, 6 As shown in this case, the organism was cultured in less than 72 hours. Therefore, HACEK organisms, when used with modern culture media in addition to automated blood culture systems, are unlikely to be causes of true culture‐negative device or valve infection, provided the patient has had no recent exposure to antibiotics and adequate blood cultures have been obtained. If a cardiac device infection is suspected, blood cultures obtained before commencement of antibiotics and adequate sampling of blood for culture are more likely to identify the pathogen than are blood cultures from prolonged incubation.
A 35‐year‐old woman with a history of hypertrophic cardiomyopathy survived a ventricular fibrillation cardiac arrest. She subsequently underwent placement of a single, transvenous right ventricular lead implantable cardioverter defibrillator (ICD) system. The lead was an active fixation model, and the generator was placed in a left infraclavicular subcutaneous pocket.
Six months later, she presented with a 5‐week illness consisting of productive cough, fever, anorexia, and myalgias. Physical exam was notable for a rapid heart rate with a variable S1. Labs were notable for a leukocytosis with predominance of neutrophils. An ECG demonstrated atrial fibrillation.
A transesophageal echocardiogram (TEE) was performed in anticipation of a cardioversion for atrial fibrillation. The TEE demonstrated a mass in the right atrium that was attached to the ICD lead, with possible involvement of the tricuspid valve leaflets (Fig. 1). The mass, characterized as multiple confluent bulky segments, was freely mobile and measured about 1.8 cm at its greatest dimension. Therefore, cardioversion was not performed. Within 72 hours, multiple aerobic BACTEC blood cultures identified Haemophilus parainfluenzae, beta lactamase negative. The patient underwent a median sternotomy to remove the ICD lead and generator (Fig. 2). The septal leaflet of the tricuspid valve was debrided. The patient was treated with a prolonged course of ceftriaxone without clinical or microbiologic signs of persistent infection.
DISCUSSION
Research has demonstrated that the rise in cardiac device infections is greater than the rise in the rate of implantation of these devices over the same time period.1 Most infections with cardiac rhythm devices are primary infections, which begin at the pocket and frequently present around generator placement or exchange.2, 3 Because the intravascular leads are continuous to the pocket, there remains a risk for lead and systemic infection.
This case illustrates 2 important concepts. Secondary device infections, which usually result from bacteria originating at a site other than the generator pocket, are less common and tend to involve the intravascular lead.2, 4 Seeding of the intravascular lead frequently occurs with either Staphylococcus aureus or coagulase‐negative Staphylococci.2, 4 Therefore, H. parainfluenzae, a gram‐negative bacillus that can be part of the normal flora of the upper respiratory tract, is not a commonly encountered pathogen for secondary lead infections. Given the respiratory tract symptoms, this was likely the source in this patient. When the lead, generator, or both are infected, this necessitates removal of the entire system.
Furthermore, H. parainfluenzae is categorized with the HACEK organisms (Haemophilus species including H. aphrophilus, H. parainfluenzae, and H. paraphrophilus; Actinobacillus actinomycetemcomitans; Cardiobacterium hominis; Eikenella corrodens; Kingella kingae), a group of fastidious gram‐negative bacilli historically thought to be a common cause of culture‐negative endocarditis. Recent retrospective studies suggest that a prolonged incubation for HACEK organisms is generally not necessary because of advances in culture media and automated blood culture systems.5, 6 As shown in this case, the organism was cultured in less than 72 hours. Therefore, HACEK organisms, when used with modern culture media in addition to automated blood culture systems, are unlikely to be causes of true culture‐negative device or valve infection, provided the patient has had no recent exposure to antibiotics and adequate blood cultures have been obtained. If a cardiac device infection is suspected, blood cultures obtained before commencement of antibiotics and adequate sampling of blood for culture are more likely to identify the pathogen than are blood cultures from prolonged incubation.
- ,,, et al.Increasing rates of cardiac device infections among Medicare beneficiaries: 1990–1999.Am Heart J.2004;147:582–586.
- ,.Infections of intracardiac devices. Cardiol Clin. 2003; 21: 253–271
- ,,,,,.Diagnosis and management of infections involving implantable electrophysiologic cardiac devices.Ann Intern Med.2000;133:604–608.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104:1029–1033.
- ,,, et al.Utility of extended blood culture incubation for isolation of Haemophilus, Actinobacillus, Cardiobacterium, Eikenella and Kingella organisms: a retrospective multicenter evaluation.J Clin Microbiol.2006;44(1):257–259.
- ,,.Prolonged incubation and extensive subculturing do not increase recovery of clinically significant microorganisms from standard automated blood cultures.Clin Infect Dis.2005;41:1677–1680.
- ,,, et al.Increasing rates of cardiac device infections among Medicare beneficiaries: 1990–1999.Am Heart J.2004;147:582–586.
- ,.Infections of intracardiac devices. Cardiol Clin. 2003; 21: 253–271
- ,,,,,.Diagnosis and management of infections involving implantable electrophysiologic cardiac devices.Ann Intern Med.2000;133:604–608.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104:1029–1033.
- ,,, et al.Utility of extended blood culture incubation for isolation of Haemophilus, Actinobacillus, Cardiobacterium, Eikenella and Kingella organisms: a retrospective multicenter evaluation.J Clin Microbiol.2006;44(1):257–259.
- ,,.Prolonged incubation and extensive subculturing do not increase recovery of clinically significant microorganisms from standard automated blood cultures.Clin Infect Dis.2005;41:1677–1680.