User login
Acute paraplegia in a patient with AIDS and a normal CSF examination
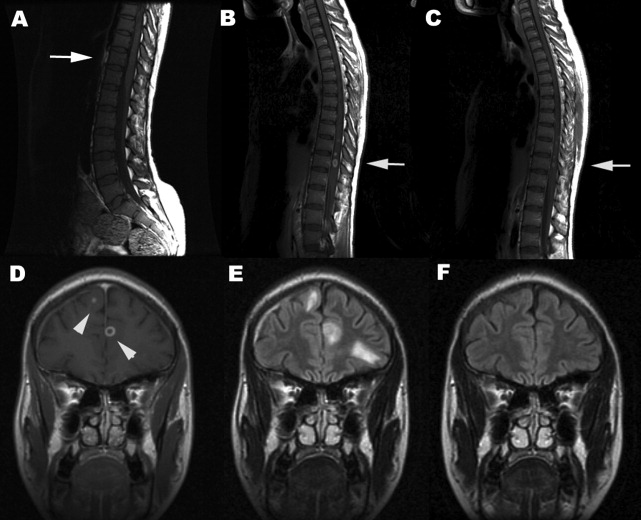
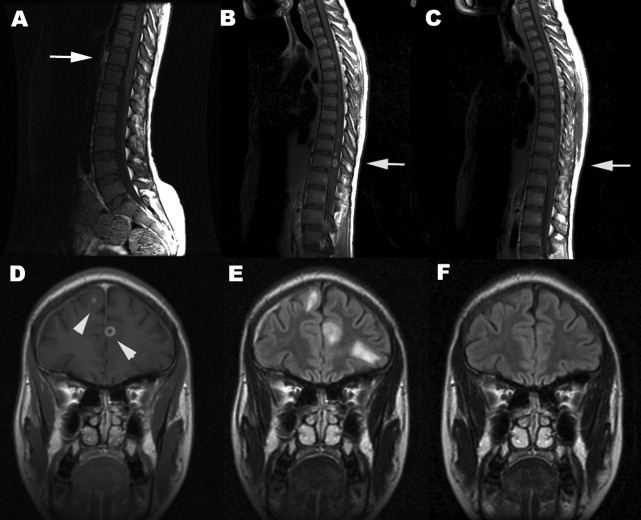
A 35‐year‐old Zimbabwean woman living in London, England, presented to the local accident and emergency department with a history of cough, shortness of breath, nausea, vomiting, diarrhea, and weight loss of 3 months' duration. Her chest X‐ray showed miliary shadowing. She was admitted to the hospital and commenced on antituberculous medications and offered an HIV test. Two weeks later, her sputum grew acid‐fast bacilli (AFB) and her HIV‐1 test came back positive. Her baseline T‐lymphocyte CD4 cell count was 6 cells/mm3 (reference range 4551320), and her HIV‐1 RNA viral load (VL) was 4,760,000 copies/mL. However, because of her multiple symptoms, her antiretroviral therapy was postponed. Four weeks later the patient's general condition improved, but she started to experience pain in her right thigh, followed by progressive right leg weakness without sensory loss. This new change affected her mobility, and she fell while walking. Within a week the patient developed progressive flaccid paraparesis with radicular sensory disturbance. This was followed by acute onset of flaccid paraplegia, extensor plantars, sensory loss to T10, and urinary incontinence. Her cerebrospinal fluid (CSF) examination revealed normal protein, glucose, and white cell count and no AFB or malignant cells, A second CSF after 3 weeks was abnormal, with protein of 0.79 g/L, normal glucose, 7 white cells (no malignant cells), and positive oligoclonal bands. The CSF screening for AFB‐PCR, treponemes, toxoplasma, cryptococcal antigen Epstein‐Barr virus, cytomegalovirus (CMV), herpes simplex virus, human T‐lymphotropic virus, and JC virus was negative. Neurophysiological studies confirmed the presence of severe multilevel radiculopathy. The MRI scan of her head and spine showed multiple intraparenchymal cerebral tuberculomata and cavitation at T 911 that enhanced postgadolinium (see Fig. 1). She was commenced on highly active antiretroviral therapy (HAART) and steroids. Ten weeks later her HIV‐1 RNA VL became undetectable in the ultrasensitive assay (cutoff 50 copies/mL), and she regained sensation in both legs and was able to stand with support. Posttreatment MRI appearances demonstrated improvement, and 14 months after treatment the MRI brain was normal (see Fig. 1).
DISCUSSION
Tuberculous myeloradiculitis is a rarely reported manifestation of tuberculosis, and there are no accurate figures for its incidence.13 It may arise as a primary manifestation of the infection, by downward extension of tuberculous meningitis, or by spread from a vertebral osteomyelitis.3 It is not uncommon for it to develop during treatment for a primary infection elsewhere.4 The clinical features of this patient were those of radiculitis followed by rapid flaccid paraparesis. The acute onset of the paraplegia with a normal CSF could be mistakenly interpreted as purely peripheral HIV‐related conditions such as CMV or PML. The extensor plantars and acute development of a paraplegia and sensory level (a combination of radiculopathy, myelopathy, and spinal shock) betrayed the central involvement of the thoracolumbar region.2 In many cases there is a copious leptomeningeal exudate, which helps to explain the fairly typical clinical presentation. This case was unusual in that there was no visible imaging evidence of exudate. The presentation should be differentiated from the vacuolar myelopathy seen with HIV infection alone.1, 5 A further unusual and unique feature was the normality of the CSF examination. Although in cases of tuberculous abscess, the CSF may be normal until rupture occurs into the subarachnoid space, a lymhocytosis, raised protein and possibly hypoglycorrachia would have been expected even in a treated and sterile CSF.3 A normal CSF examination was reported in a previous study.6 This case strongly emphasizes that the diagnosis of opportunistic tuberculosis in the setting of HIV infection can be elusive. Immune reconstruction inflammatory syndrome is an unlikely cause of her neurological symptoms, as she developed these symptoms before HAART. Antituberculous medications and antimycobacterial treatment must be modified to take into account the altered pharmacokinetics as a result of HAART and steroids. There are no published guidelines on how long steroids should be maintained despite their efficacy as an adjunct in TB meningitis.7 There is no evidence to guide their use in patients with coexistent HIV. Treatment until significant improvement or a 6‐month tailed trial of steroids (in the absence of other contraindications) is probably acceptable. Even though the consequences of a well‐placed mycobacterial lesion may be devastating, appropriate treatment may lead to partial and clinically important reversal of disability.
- ,,, et al.Spectrum of myelopathies in HIV seropositive South African patients.Neurology.2001;57:348–351.
- ,.Diagnosis and management of tuberculous paraplegia with special reference to tuberculous radiculomyelitis.J Neurol Neurosurg Psychiatry.1979;42:12–18.
- ,,, et al.Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review.Clin Infect Dis.2000;30:915–921.
- ,,.Symptomatic intracranial tuberculoma developing during treatment of tuberculosis: a report of 10 patients and review of the literature.Q J Med.1987;63:449–460.
- ,.Infectious myelopathies.Semin Neurol.2002;22:133–141.
- ,,,,,, et al.Tuberculous meningitis in patients infected with the human immunodeficiency virus.New Engl J Med.1992;326:668–672.
- ,,, et al.Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults.N Engl J Med.2004;351:1741–1751.
A 35‐year‐old Zimbabwean woman living in London, England, presented to the local accident and emergency department with a history of cough, shortness of breath, nausea, vomiting, diarrhea, and weight loss of 3 months' duration. Her chest X‐ray showed miliary shadowing. She was admitted to the hospital and commenced on antituberculous medications and offered an HIV test. Two weeks later, her sputum grew acid‐fast bacilli (AFB) and her HIV‐1 test came back positive. Her baseline T‐lymphocyte CD4 cell count was 6 cells/mm3 (reference range 4551320), and her HIV‐1 RNA viral load (VL) was 4,760,000 copies/mL. However, because of her multiple symptoms, her antiretroviral therapy was postponed. Four weeks later the patient's general condition improved, but she started to experience pain in her right thigh, followed by progressive right leg weakness without sensory loss. This new change affected her mobility, and she fell while walking. Within a week the patient developed progressive flaccid paraparesis with radicular sensory disturbance. This was followed by acute onset of flaccid paraplegia, extensor plantars, sensory loss to T10, and urinary incontinence. Her cerebrospinal fluid (CSF) examination revealed normal protein, glucose, and white cell count and no AFB or malignant cells, A second CSF after 3 weeks was abnormal, with protein of 0.79 g/L, normal glucose, 7 white cells (no malignant cells), and positive oligoclonal bands. The CSF screening for AFB‐PCR, treponemes, toxoplasma, cryptococcal antigen Epstein‐Barr virus, cytomegalovirus (CMV), herpes simplex virus, human T‐lymphotropic virus, and JC virus was negative. Neurophysiological studies confirmed the presence of severe multilevel radiculopathy. The MRI scan of her head and spine showed multiple intraparenchymal cerebral tuberculomata and cavitation at T 911 that enhanced postgadolinium (see Fig. 1). She was commenced on highly active antiretroviral therapy (HAART) and steroids. Ten weeks later her HIV‐1 RNA VL became undetectable in the ultrasensitive assay (cutoff 50 copies/mL), and she regained sensation in both legs and was able to stand with support. Posttreatment MRI appearances demonstrated improvement, and 14 months after treatment the MRI brain was normal (see Fig. 1).
DISCUSSION
Tuberculous myeloradiculitis is a rarely reported manifestation of tuberculosis, and there are no accurate figures for its incidence.13 It may arise as a primary manifestation of the infection, by downward extension of tuberculous meningitis, or by spread from a vertebral osteomyelitis.3 It is not uncommon for it to develop during treatment for a primary infection elsewhere.4 The clinical features of this patient were those of radiculitis followed by rapid flaccid paraparesis. The acute onset of the paraplegia with a normal CSF could be mistakenly interpreted as purely peripheral HIV‐related conditions such as CMV or PML. The extensor plantars and acute development of a paraplegia and sensory level (a combination of radiculopathy, myelopathy, and spinal shock) betrayed the central involvement of the thoracolumbar region.2 In many cases there is a copious leptomeningeal exudate, which helps to explain the fairly typical clinical presentation. This case was unusual in that there was no visible imaging evidence of exudate. The presentation should be differentiated from the vacuolar myelopathy seen with HIV infection alone.1, 5 A further unusual and unique feature was the normality of the CSF examination. Although in cases of tuberculous abscess, the CSF may be normal until rupture occurs into the subarachnoid space, a lymhocytosis, raised protein and possibly hypoglycorrachia would have been expected even in a treated and sterile CSF.3 A normal CSF examination was reported in a previous study.6 This case strongly emphasizes that the diagnosis of opportunistic tuberculosis in the setting of HIV infection can be elusive. Immune reconstruction inflammatory syndrome is an unlikely cause of her neurological symptoms, as she developed these symptoms before HAART. Antituberculous medications and antimycobacterial treatment must be modified to take into account the altered pharmacokinetics as a result of HAART and steroids. There are no published guidelines on how long steroids should be maintained despite their efficacy as an adjunct in TB meningitis.7 There is no evidence to guide their use in patients with coexistent HIV. Treatment until significant improvement or a 6‐month tailed trial of steroids (in the absence of other contraindications) is probably acceptable. Even though the consequences of a well‐placed mycobacterial lesion may be devastating, appropriate treatment may lead to partial and clinically important reversal of disability.
A 35‐year‐old Zimbabwean woman living in London, England, presented to the local accident and emergency department with a history of cough, shortness of breath, nausea, vomiting, diarrhea, and weight loss of 3 months' duration. Her chest X‐ray showed miliary shadowing. She was admitted to the hospital and commenced on antituberculous medications and offered an HIV test. Two weeks later, her sputum grew acid‐fast bacilli (AFB) and her HIV‐1 test came back positive. Her baseline T‐lymphocyte CD4 cell count was 6 cells/mm3 (reference range 4551320), and her HIV‐1 RNA viral load (VL) was 4,760,000 copies/mL. However, because of her multiple symptoms, her antiretroviral therapy was postponed. Four weeks later the patient's general condition improved, but she started to experience pain in her right thigh, followed by progressive right leg weakness without sensory loss. This new change affected her mobility, and she fell while walking. Within a week the patient developed progressive flaccid paraparesis with radicular sensory disturbance. This was followed by acute onset of flaccid paraplegia, extensor plantars, sensory loss to T10, and urinary incontinence. Her cerebrospinal fluid (CSF) examination revealed normal protein, glucose, and white cell count and no AFB or malignant cells, A second CSF after 3 weeks was abnormal, with protein of 0.79 g/L, normal glucose, 7 white cells (no malignant cells), and positive oligoclonal bands. The CSF screening for AFB‐PCR, treponemes, toxoplasma, cryptococcal antigen Epstein‐Barr virus, cytomegalovirus (CMV), herpes simplex virus, human T‐lymphotropic virus, and JC virus was negative. Neurophysiological studies confirmed the presence of severe multilevel radiculopathy. The MRI scan of her head and spine showed multiple intraparenchymal cerebral tuberculomata and cavitation at T 911 that enhanced postgadolinium (see Fig. 1). She was commenced on highly active antiretroviral therapy (HAART) and steroids. Ten weeks later her HIV‐1 RNA VL became undetectable in the ultrasensitive assay (cutoff 50 copies/mL), and she regained sensation in both legs and was able to stand with support. Posttreatment MRI appearances demonstrated improvement, and 14 months after treatment the MRI brain was normal (see Fig. 1).
DISCUSSION
Tuberculous myeloradiculitis is a rarely reported manifestation of tuberculosis, and there are no accurate figures for its incidence.13 It may arise as a primary manifestation of the infection, by downward extension of tuberculous meningitis, or by spread from a vertebral osteomyelitis.3 It is not uncommon for it to develop during treatment for a primary infection elsewhere.4 The clinical features of this patient were those of radiculitis followed by rapid flaccid paraparesis. The acute onset of the paraplegia with a normal CSF could be mistakenly interpreted as purely peripheral HIV‐related conditions such as CMV or PML. The extensor plantars and acute development of a paraplegia and sensory level (a combination of radiculopathy, myelopathy, and spinal shock) betrayed the central involvement of the thoracolumbar region.2 In many cases there is a copious leptomeningeal exudate, which helps to explain the fairly typical clinical presentation. This case was unusual in that there was no visible imaging evidence of exudate. The presentation should be differentiated from the vacuolar myelopathy seen with HIV infection alone.1, 5 A further unusual and unique feature was the normality of the CSF examination. Although in cases of tuberculous abscess, the CSF may be normal until rupture occurs into the subarachnoid space, a lymhocytosis, raised protein and possibly hypoglycorrachia would have been expected even in a treated and sterile CSF.3 A normal CSF examination was reported in a previous study.6 This case strongly emphasizes that the diagnosis of opportunistic tuberculosis in the setting of HIV infection can be elusive. Immune reconstruction inflammatory syndrome is an unlikely cause of her neurological symptoms, as she developed these symptoms before HAART. Antituberculous medications and antimycobacterial treatment must be modified to take into account the altered pharmacokinetics as a result of HAART and steroids. There are no published guidelines on how long steroids should be maintained despite their efficacy as an adjunct in TB meningitis.7 There is no evidence to guide their use in patients with coexistent HIV. Treatment until significant improvement or a 6‐month tailed trial of steroids (in the absence of other contraindications) is probably acceptable. Even though the consequences of a well‐placed mycobacterial lesion may be devastating, appropriate treatment may lead to partial and clinically important reversal of disability.
- ,,, et al.Spectrum of myelopathies in HIV seropositive South African patients.Neurology.2001;57:348–351.
- ,.Diagnosis and management of tuberculous paraplegia with special reference to tuberculous radiculomyelitis.J Neurol Neurosurg Psychiatry.1979;42:12–18.
- ,,, et al.Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review.Clin Infect Dis.2000;30:915–921.
- ,,.Symptomatic intracranial tuberculoma developing during treatment of tuberculosis: a report of 10 patients and review of the literature.Q J Med.1987;63:449–460.
- ,.Infectious myelopathies.Semin Neurol.2002;22:133–141.
- ,,,,,, et al.Tuberculous meningitis in patients infected with the human immunodeficiency virus.New Engl J Med.1992;326:668–672.
- ,,, et al.Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults.N Engl J Med.2004;351:1741–1751.
- ,,, et al.Spectrum of myelopathies in HIV seropositive South African patients.Neurology.2001;57:348–351.
- ,.Diagnosis and management of tuberculous paraplegia with special reference to tuberculous radiculomyelitis.J Neurol Neurosurg Psychiatry.1979;42:12–18.
- ,,, et al.Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review.Clin Infect Dis.2000;30:915–921.
- ,,.Symptomatic intracranial tuberculoma developing during treatment of tuberculosis: a report of 10 patients and review of the literature.Q J Med.1987;63:449–460.
- ,.Infectious myelopathies.Semin Neurol.2002;22:133–141.
- ,,,,,, et al.Tuberculous meningitis in patients infected with the human immunodeficiency virus.New Engl J Med.1992;326:668–672.
- ,,, et al.Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults.N Engl J Med.2004;351:1741–1751.
Cullen's sign associated with metastatic esophageal carcinoma
Examination of the abdomen is an important element of the physical examination, especially in patients with known or suspected cancer. Patients with intraabdominal malignancy occasionally manifest unusual ominous findings on abdominal examination that may portend a poor prognosis: periumbilical adenopathy (Sister Mary Joseph sign),1 hepatic pulsations,2 or a hepatic friction rub or bruit.3 An uncommonly reported, and likely under‐appreciated, sign of intraabdominal cancer is periumbilical ecchymosis, also known as Cullen's sign.4 Reported below is a case of Cullen's sign associated with metastatic esophageal carcinoma.
CASE REPORT
An 80‐year‐old man with recently diagnosed esophageal adenocarcinoma presented with fever, cough, lassitude, and abdominal distention. Several weeks earlier, the patient underwent esophagogastroduodenoscopy for dysphagia and weight loss and was found to have a partially obstructing, ulcerated distal esophageal mass. Biopsy revealed poorly differentiated adenocarcinoma. At that time, computed tomography showed mediastinal adenopathy Subsequently, the patient developed increasing dysphagia with a cough, painful abdominal distention, and profound weight loss and was admitted to the hospital for further evaluation.
The patient was tachycardic and hypotensive. Physical examination revealed muscle wasting, anasarca, and abdominal distention with diffuse tenderness. An area of periumbilical ecchymosis measuring approximately 10 cm in diameter was noted. The patient had not sustained any obvious abdominal trauma or received any injections in the periumbilical area. There were no other significant ecchymoses on the abdominal wall, including the flanks. Computed tomography revealed pulmonary infiltrates compatible with pneumonia, mediastinal adenopathy, thickening of the distal esophagus, and ascites; there were no obvious liver lesions, pancreatic or retroperitoneal hemorrhage, or evidence of pancreatitis. Liver enzymes, bilirubin, and alkaline phosphatase were normal, but anemia and leukocytosis were noted. Prothombin time and partial thromboplastin time were 20 and 28 seconds, respectively. Platelet count was normal. Broad‐spectrum antimicrobials were administered for pneumonia. Because of abdominal discomfort, paracentesis was performed. Approximately 2000 cc of opaque yellow fluid was removed. The ascitic fluid was positive for erythrocytes and adenocarcinoma cells, consistent with his known diagnosis of esophageal carcinoma. The patient developed acute renal failure, and his condition continue to decline. He subsequently was discharged to hospice care and died several days later; an autopsy was not performed.
DISCUSSION
Cullen's signecchymosis surrounding the umbilicusis classically associated with hemorrhagic pancreatitis, often occurring in conjunction with ecchymosis of the flank (Grey‐Turner sign).4 Cullen's sign, however, has been reported with other abdominal pathologies such as ruptured ectopic pregnancy, leaking aortic aneurysm, splenic rupture, and retroperitoneal hemorrhage.4, 5 Hemoperitoneum from any of these processes leads to diffusion of blood along fascial planes, resulting in flank staining (Grey‐Turner sign) or periumbilical staining (Cullen's sign). Cullen's sign, however, is traditionally not attributed to malignant disease in standard medical and surgical texts.6, 7 However, the results of a Medline literature search, which revealed only a handful of case reports, suggests an association between advanced malignancy and Cullen's sign (Table 1). All previous reports oc‐curred in patients with advanced terminal malignancy, although no firm conclusions regarding specific malignancies or other risk factors can be surmised from such a small number of cases.5, 8, 9
| Reference | Sex | Age | Cancer | Outcome |
|---|---|---|---|---|
| Present study | M | 80 | Esophageal | Died |
| 5 | M | 55 | Thyroid | Died |
| 8 | M | 62 | Lymphoma | Died |
| 9 | M | 32 | Hepatoma | Died |
| 9 | M | 64 | Hepatoma | Died |
Our patient had stage IV esophageal carcinoma with malignant ascites associated with periumbilical ecchymosis. Unfortunately, serum amylase and lipase were not obtained, but acute pancreatitis‐induced Cullen's sign is unlikely because the patient did not have symptoms of pancreatitis and computed tomography did not reveal pancreatic inflammation or hemorrhage. It is well known that patients with disseminated visceral adenocarcinoma can develop coagulopathy, and that cannot be excluded in our patient. The likely mechanism of periumbilical blood collection is unclear but could relate to subclinical hemoperitoneum from mesenteric and peritoneal carcinomatosus, abdominal wall trauma, or coagulopathy from cancer and acute renal failure. Nonetheless, it is evident from this and previously reported cases that Cullen's sign complicating cancer has a dismal prognosis and is a premorbid sign. Clinicians should consider occult or metastatic visceral malignancy in patients with unexplained abdominal wall ecchymosis.
- ,.Gastric cancer. In:Clinical Hematology and Oncology: Presentation, Diagnosis, and Treatment.Philadelphia:Churchill‐Livingstone,2003;887–898.
- ,.Hepatic pulsations in a patient with cholangiocarcinoma.Arch Intern Med.1996;157:133–134.
- The Abdomen. In:.The Art and Science of Bedside Diagnosis.Baltimore, MD:Williams and Wilkins,1990;371–390.
- .Cullen's sign.Hosp Physician.1999;35:35–36.
- .Cullen's sign associated with metastatic thyroid cancer.N Engl J Med.1999;340:149–150.
- Acute Pancreatitis. In:.Cope's Early Diagnosis of the Acute Abdomen.18th ed.New York:Oxford University Press;1991:123–131.
- ,.Acute and chronic pancreatitis. In:Braunwald E,Fauci AS,Kasper EL, et al., eds.Harrison's Principles of Internal Medicine.15th ed.New York:McGraw‐Hill;2001:1792–1804.
- ,,, et al.Cullen's sign secondary to intraabdominal non‐Hodgkin's lymphoma.Am J Gastroenterol.1996;91:1040–1041.
- ,.Cullen's sign, a feature in liver disease.BMJ.1974;1:493–494.
Examination of the abdomen is an important element of the physical examination, especially in patients with known or suspected cancer. Patients with intraabdominal malignancy occasionally manifest unusual ominous findings on abdominal examination that may portend a poor prognosis: periumbilical adenopathy (Sister Mary Joseph sign),1 hepatic pulsations,2 or a hepatic friction rub or bruit.3 An uncommonly reported, and likely under‐appreciated, sign of intraabdominal cancer is periumbilical ecchymosis, also known as Cullen's sign.4 Reported below is a case of Cullen's sign associated with metastatic esophageal carcinoma.
CASE REPORT
An 80‐year‐old man with recently diagnosed esophageal adenocarcinoma presented with fever, cough, lassitude, and abdominal distention. Several weeks earlier, the patient underwent esophagogastroduodenoscopy for dysphagia and weight loss and was found to have a partially obstructing, ulcerated distal esophageal mass. Biopsy revealed poorly differentiated adenocarcinoma. At that time, computed tomography showed mediastinal adenopathy Subsequently, the patient developed increasing dysphagia with a cough, painful abdominal distention, and profound weight loss and was admitted to the hospital for further evaluation.
The patient was tachycardic and hypotensive. Physical examination revealed muscle wasting, anasarca, and abdominal distention with diffuse tenderness. An area of periumbilical ecchymosis measuring approximately 10 cm in diameter was noted. The patient had not sustained any obvious abdominal trauma or received any injections in the periumbilical area. There were no other significant ecchymoses on the abdominal wall, including the flanks. Computed tomography revealed pulmonary infiltrates compatible with pneumonia, mediastinal adenopathy, thickening of the distal esophagus, and ascites; there were no obvious liver lesions, pancreatic or retroperitoneal hemorrhage, or evidence of pancreatitis. Liver enzymes, bilirubin, and alkaline phosphatase were normal, but anemia and leukocytosis were noted. Prothombin time and partial thromboplastin time were 20 and 28 seconds, respectively. Platelet count was normal. Broad‐spectrum antimicrobials were administered for pneumonia. Because of abdominal discomfort, paracentesis was performed. Approximately 2000 cc of opaque yellow fluid was removed. The ascitic fluid was positive for erythrocytes and adenocarcinoma cells, consistent with his known diagnosis of esophageal carcinoma. The patient developed acute renal failure, and his condition continue to decline. He subsequently was discharged to hospice care and died several days later; an autopsy was not performed.
DISCUSSION
Cullen's signecchymosis surrounding the umbilicusis classically associated with hemorrhagic pancreatitis, often occurring in conjunction with ecchymosis of the flank (Grey‐Turner sign).4 Cullen's sign, however, has been reported with other abdominal pathologies such as ruptured ectopic pregnancy, leaking aortic aneurysm, splenic rupture, and retroperitoneal hemorrhage.4, 5 Hemoperitoneum from any of these processes leads to diffusion of blood along fascial planes, resulting in flank staining (Grey‐Turner sign) or periumbilical staining (Cullen's sign). Cullen's sign, however, is traditionally not attributed to malignant disease in standard medical and surgical texts.6, 7 However, the results of a Medline literature search, which revealed only a handful of case reports, suggests an association between advanced malignancy and Cullen's sign (Table 1). All previous reports oc‐curred in patients with advanced terminal malignancy, although no firm conclusions regarding specific malignancies or other risk factors can be surmised from such a small number of cases.5, 8, 9
| Reference | Sex | Age | Cancer | Outcome |
|---|---|---|---|---|
| Present study | M | 80 | Esophageal | Died |
| 5 | M | 55 | Thyroid | Died |
| 8 | M | 62 | Lymphoma | Died |
| 9 | M | 32 | Hepatoma | Died |
| 9 | M | 64 | Hepatoma | Died |
Our patient had stage IV esophageal carcinoma with malignant ascites associated with periumbilical ecchymosis. Unfortunately, serum amylase and lipase were not obtained, but acute pancreatitis‐induced Cullen's sign is unlikely because the patient did not have symptoms of pancreatitis and computed tomography did not reveal pancreatic inflammation or hemorrhage. It is well known that patients with disseminated visceral adenocarcinoma can develop coagulopathy, and that cannot be excluded in our patient. The likely mechanism of periumbilical blood collection is unclear but could relate to subclinical hemoperitoneum from mesenteric and peritoneal carcinomatosus, abdominal wall trauma, or coagulopathy from cancer and acute renal failure. Nonetheless, it is evident from this and previously reported cases that Cullen's sign complicating cancer has a dismal prognosis and is a premorbid sign. Clinicians should consider occult or metastatic visceral malignancy in patients with unexplained abdominal wall ecchymosis.
Examination of the abdomen is an important element of the physical examination, especially in patients with known or suspected cancer. Patients with intraabdominal malignancy occasionally manifest unusual ominous findings on abdominal examination that may portend a poor prognosis: periumbilical adenopathy (Sister Mary Joseph sign),1 hepatic pulsations,2 or a hepatic friction rub or bruit.3 An uncommonly reported, and likely under‐appreciated, sign of intraabdominal cancer is periumbilical ecchymosis, also known as Cullen's sign.4 Reported below is a case of Cullen's sign associated with metastatic esophageal carcinoma.
CASE REPORT
An 80‐year‐old man with recently diagnosed esophageal adenocarcinoma presented with fever, cough, lassitude, and abdominal distention. Several weeks earlier, the patient underwent esophagogastroduodenoscopy for dysphagia and weight loss and was found to have a partially obstructing, ulcerated distal esophageal mass. Biopsy revealed poorly differentiated adenocarcinoma. At that time, computed tomography showed mediastinal adenopathy Subsequently, the patient developed increasing dysphagia with a cough, painful abdominal distention, and profound weight loss and was admitted to the hospital for further evaluation.
The patient was tachycardic and hypotensive. Physical examination revealed muscle wasting, anasarca, and abdominal distention with diffuse tenderness. An area of periumbilical ecchymosis measuring approximately 10 cm in diameter was noted. The patient had not sustained any obvious abdominal trauma or received any injections in the periumbilical area. There were no other significant ecchymoses on the abdominal wall, including the flanks. Computed tomography revealed pulmonary infiltrates compatible with pneumonia, mediastinal adenopathy, thickening of the distal esophagus, and ascites; there were no obvious liver lesions, pancreatic or retroperitoneal hemorrhage, or evidence of pancreatitis. Liver enzymes, bilirubin, and alkaline phosphatase were normal, but anemia and leukocytosis were noted. Prothombin time and partial thromboplastin time were 20 and 28 seconds, respectively. Platelet count was normal. Broad‐spectrum antimicrobials were administered for pneumonia. Because of abdominal discomfort, paracentesis was performed. Approximately 2000 cc of opaque yellow fluid was removed. The ascitic fluid was positive for erythrocytes and adenocarcinoma cells, consistent with his known diagnosis of esophageal carcinoma. The patient developed acute renal failure, and his condition continue to decline. He subsequently was discharged to hospice care and died several days later; an autopsy was not performed.
DISCUSSION
Cullen's signecchymosis surrounding the umbilicusis classically associated with hemorrhagic pancreatitis, often occurring in conjunction with ecchymosis of the flank (Grey‐Turner sign).4 Cullen's sign, however, has been reported with other abdominal pathologies such as ruptured ectopic pregnancy, leaking aortic aneurysm, splenic rupture, and retroperitoneal hemorrhage.4, 5 Hemoperitoneum from any of these processes leads to diffusion of blood along fascial planes, resulting in flank staining (Grey‐Turner sign) or periumbilical staining (Cullen's sign). Cullen's sign, however, is traditionally not attributed to malignant disease in standard medical and surgical texts.6, 7 However, the results of a Medline literature search, which revealed only a handful of case reports, suggests an association between advanced malignancy and Cullen's sign (Table 1). All previous reports oc‐curred in patients with advanced terminal malignancy, although no firm conclusions regarding specific malignancies or other risk factors can be surmised from such a small number of cases.5, 8, 9
| Reference | Sex | Age | Cancer | Outcome |
|---|---|---|---|---|
| Present study | M | 80 | Esophageal | Died |
| 5 | M | 55 | Thyroid | Died |
| 8 | M | 62 | Lymphoma | Died |
| 9 | M | 32 | Hepatoma | Died |
| 9 | M | 64 | Hepatoma | Died |
Our patient had stage IV esophageal carcinoma with malignant ascites associated with periumbilical ecchymosis. Unfortunately, serum amylase and lipase were not obtained, but acute pancreatitis‐induced Cullen's sign is unlikely because the patient did not have symptoms of pancreatitis and computed tomography did not reveal pancreatic inflammation or hemorrhage. It is well known that patients with disseminated visceral adenocarcinoma can develop coagulopathy, and that cannot be excluded in our patient. The likely mechanism of periumbilical blood collection is unclear but could relate to subclinical hemoperitoneum from mesenteric and peritoneal carcinomatosus, abdominal wall trauma, or coagulopathy from cancer and acute renal failure. Nonetheless, it is evident from this and previously reported cases that Cullen's sign complicating cancer has a dismal prognosis and is a premorbid sign. Clinicians should consider occult or metastatic visceral malignancy in patients with unexplained abdominal wall ecchymosis.
- ,.Gastric cancer. In:Clinical Hematology and Oncology: Presentation, Diagnosis, and Treatment.Philadelphia:Churchill‐Livingstone,2003;887–898.
- ,.Hepatic pulsations in a patient with cholangiocarcinoma.Arch Intern Med.1996;157:133–134.
- The Abdomen. In:.The Art and Science of Bedside Diagnosis.Baltimore, MD:Williams and Wilkins,1990;371–390.
- .Cullen's sign.Hosp Physician.1999;35:35–36.
- .Cullen's sign associated with metastatic thyroid cancer.N Engl J Med.1999;340:149–150.
- Acute Pancreatitis. In:.Cope's Early Diagnosis of the Acute Abdomen.18th ed.New York:Oxford University Press;1991:123–131.
- ,.Acute and chronic pancreatitis. In:Braunwald E,Fauci AS,Kasper EL, et al., eds.Harrison's Principles of Internal Medicine.15th ed.New York:McGraw‐Hill;2001:1792–1804.
- ,,, et al.Cullen's sign secondary to intraabdominal non‐Hodgkin's lymphoma.Am J Gastroenterol.1996;91:1040–1041.
- ,.Cullen's sign, a feature in liver disease.BMJ.1974;1:493–494.
- ,.Gastric cancer. In:Clinical Hematology and Oncology: Presentation, Diagnosis, and Treatment.Philadelphia:Churchill‐Livingstone,2003;887–898.
- ,.Hepatic pulsations in a patient with cholangiocarcinoma.Arch Intern Med.1996;157:133–134.
- The Abdomen. In:.The Art and Science of Bedside Diagnosis.Baltimore, MD:Williams and Wilkins,1990;371–390.
- .Cullen's sign.Hosp Physician.1999;35:35–36.
- .Cullen's sign associated with metastatic thyroid cancer.N Engl J Med.1999;340:149–150.
- Acute Pancreatitis. In:.Cope's Early Diagnosis of the Acute Abdomen.18th ed.New York:Oxford University Press;1991:123–131.
- ,.Acute and chronic pancreatitis. In:Braunwald E,Fauci AS,Kasper EL, et al., eds.Harrison's Principles of Internal Medicine.15th ed.New York:McGraw‐Hill;2001:1792–1804.
- ,,, et al.Cullen's sign secondary to intraabdominal non‐Hodgkin's lymphoma.Am J Gastroenterol.1996;91:1040–1041.
- ,.Cullen's sign, a feature in liver disease.BMJ.1974;1:493–494.
Case Report
A 26‐year‐old woman presented with a 1‐week history of epigastric and left upper quadrant pain associated with nausea and vomiting. She also described 3 weeks of constant substernal chest pain, dyspnea, and decreased exercise tolerance.
Her medical history was significant for a pituitary macroadenoma diagnosed 6 years previously that had been treated with cabergoline. She had a miscarriage 7 years ago but gave birth to a healthy child 5 months prior to admission. She had smoked 2 cigarettes per day for the last 7 years. She denied alcohol or illicit drug use. Her mother had sickle cell trait.
On admission, her heart rate was 112 beats/minute, blood pressure was 110/80 mm Hg, and respiratory rate was 26 per minute. Jugular venous distension was not appreciated. She had decreased breath sounds over the right lung base. The apical impulse was palpated in the left sixth intercostal space 1 cm lateral to the midclavicular line, and a 2/6 holosystolic murmur was auscultated at the left lower sternal border. No other murmurs or S3 or S4 gallop could be appreciated. There were no vascular or immunological phenomena suggestive of infective endocarditis. She had abdominal tenderness in the epigastrium and bilateral upper quadrants. There was no lower extremity edema, and the extremities were well perfused.
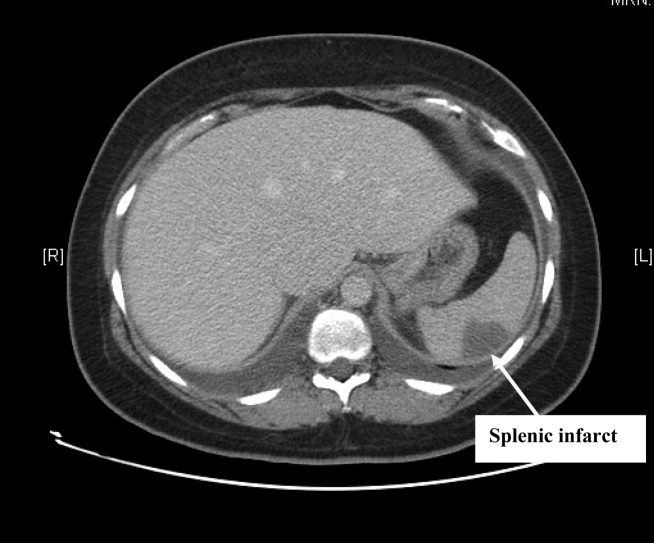
Complete blood count, electrolytes, and liver, renal, and coagulation profiles were normal. Her chest x‐ray revealed cardiomegaly and bilateral pleural effusions. EKG showed sinus tachycardia and nonspecific T‐wave changes. To further evaluate her abdominal pain, a CT scan of the abdomen and pelvis (Fig. 1) was ordered. This revealed a 3 by 1.8 cm splenic infarct. Because of her respiratory symptoms and tachycardia, a pulmonary embolism was suspected but was ruled out with a CT angiogram of the chest.
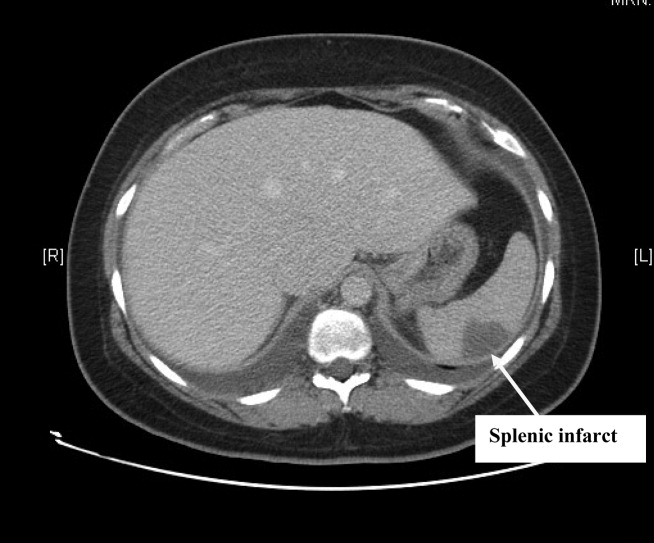
She was diagnosed with new‐onset heart failure and a splenic infarct. However, it was unclear if the 2 problems were linked. Possible etiologies of the splenic infarct included thrombus from hypercoagulable state (given her prior miscarriage, postpartum state), infarct from hemoglobinopathy (given her family history), septic emboli from infective endocarditis, and peripartum cardiomyopathy associated with embolism to the spleen.
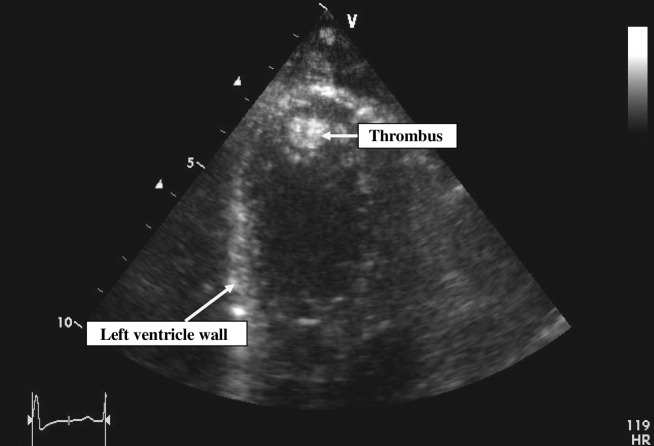
Pain control, empiric antibiotics, and intravenous diuretics were started. Twelve hours later, the patient's dyspnea and chest pain resolved. Her blood culture results were negative, and hemoglobin electrophoresis was normal. Results of a hypercoagulable workup for an arterial thrombus that included lupus anticoagulant, anticardiolipin antibodies, and antibodies to 2‐glycoprotein‐I were negative. The echocardiogram (Fig. 2) showed a dilated left ventricle with an ejection fraction (EF) of 10%15%, normal valvular morphology without vegetations, moderate mitral and tricuspid regurgitation, and a 1‐cm left ventricular thrombus and 3 small adjacent thrombi.
Based on the echocardiographic data, recent pregnancy, and absence of other risk factors for heart failure, a diagnosis was made of peripartum cardiomyopathy with left ventricular thrombi and subsequent embolization to the spleen.
Standard heart failure therapy including diuretics, beta‐blockers, and angiotensin‐converting enzyme inhibitors and anticoagulation with warfarin were started. Within 24 hours, the patient was asymptomatic except for minimal abdominal pain. The patient was discharged home in a stable condition the following day. At her outpatient follow‐up 3 months later, she was well compensated and asymptomatic.
DISCUSSION
Using the search terms peripartum cardiomyopathy, cardiomyopathy, thromboembolism, and postpartum period, we performed a MEDLINE search of the English literature from 1950 to 2007. We did not find any reported cases of splenic infarction complicating peripartum cardiomyopathy.
Peripartum cardiomyopathy (PPCM) is a form of dilated cardiomyopathy that occurs as a complication of pregnancy. It can present with heart failure in the last month of pregnancy or within 5 months after delivery.1, 2 The incidence of PPCM is unknown but has been estimated at 1 in 30004000 live births.3
Our patient met the criteria for PPCM as set forth by the National Heart, Lung, and Blood Institute (NHLBI), in conjunction with the Office of Rare Disease of the National Institutes of Health in April 1997.3 To establish a diagnosis of PPCM, 4 criteria have to be met:
-
Development of heart failure in the last month of pregnancy or within 5 months after delivery;
-
Absence of an identifiable cause of heart failure;
-
Absence of recognizable heart disease prior to the last month of pregnancy; and
-
Left ventricular systolic dysfunction demonstrated by echocardiographic variables such as depressed shortening fraction or left ventricular ejection fraction 45%.
Thromboembolism has been reported with an incidence of 4% to 30% in peripartum cardiomyopathy.4 In our literature review, we found several case reports of thromboembolic phenomena complicating peripartum cardiomyopathy. These included lower extremity arterial thromboembolism with compromised circulation,5 cerebral embolism,6 and acute myocardial infarction secondary to coronary artery embolism.7 This is the first reported case of splenic artery embolization leading to splenic infarct as a complication of peripartum cardiomyopathy.
Because of the high risk of thromboembolism, the NHLBI recommends that anticoagulation be added to the standard heart failure treatment of PPCM patients with an ejection fraction of less than 35%,3 although there are no prospective randomized clinical trial data to support this recommendation. For anticoagulation, heparin is generally used in the antepartum period and warfarin in the postpartum period. It has been recommended that anticoagulation be continued for as long as the cardiomegaly persists.1
In addition to anticoagulation for PPCM patients with an EF 35%, standard heart failure therapy includes salt restriction, diuretics, and beta‐blockers. Angiotensin‐converting enzyme inhibitors can be teratogenic during pregnancy but can be used after delivery. Hydralazine can be used safely during pregnancy as an alternative to angiotensin‐converting enzyme inhibitors. Patients failing maximal medical management may be candidates for cardiac transplantation.
Recommendations regarding subsequent pregnancies seem related to the return of ventricular size and function. Patients whose heart size does not return to normal should be strongly advised to avoid future pregnancies.2, 3 Patients who recover ventricular function may have deterioration of left ventricular function with future pregnancies.8 They should be counseled about the risk and closely monitored for development of heart failure if they become pregnant again.
- ,.Peripartum cardiomyopathy.Circulation.1971;44:964–968.
- ,,, et al.Natural course of peripartum cardiomyopathy.Circulation.1971;44:1053–1061.
- ,,, et al.Peripartum Cardiomyopathy. National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) Workshop Recommendations and Review.JAMA.2000;283:1183–1188.
- .Peripartum cardiomyopathy.N Engl J Med.1985;312:1432–1437.
- ,,, et al.Peripartum cardiomyopathy presenting as lower extremity arterial thromboembolism.J Reprod Med.2000;45:351–353.
- ,,, et al.Cerebral embolism as the initial manifestation of peripartum cardiomyopathy.Neurology.1982;32:668–671.
- ,,, et al.Peripartum cardiomyopathy presenting as an acute myocardial infarction.Mayo Clin Proc.2002;77:500–501.
- ,,, et al.Recurrent peripartum cardiomyopathy.Eur J Obstet Gynecol Reprod Biol.1998;76:29–30.
A 26‐year‐old woman presented with a 1‐week history of epigastric and left upper quadrant pain associated with nausea and vomiting. She also described 3 weeks of constant substernal chest pain, dyspnea, and decreased exercise tolerance.
Her medical history was significant for a pituitary macroadenoma diagnosed 6 years previously that had been treated with cabergoline. She had a miscarriage 7 years ago but gave birth to a healthy child 5 months prior to admission. She had smoked 2 cigarettes per day for the last 7 years. She denied alcohol or illicit drug use. Her mother had sickle cell trait.
On admission, her heart rate was 112 beats/minute, blood pressure was 110/80 mm Hg, and respiratory rate was 26 per minute. Jugular venous distension was not appreciated. She had decreased breath sounds over the right lung base. The apical impulse was palpated in the left sixth intercostal space 1 cm lateral to the midclavicular line, and a 2/6 holosystolic murmur was auscultated at the left lower sternal border. No other murmurs or S3 or S4 gallop could be appreciated. There were no vascular or immunological phenomena suggestive of infective endocarditis. She had abdominal tenderness in the epigastrium and bilateral upper quadrants. There was no lower extremity edema, and the extremities were well perfused.
Complete blood count, electrolytes, and liver, renal, and coagulation profiles were normal. Her chest x‐ray revealed cardiomegaly and bilateral pleural effusions. EKG showed sinus tachycardia and nonspecific T‐wave changes. To further evaluate her abdominal pain, a CT scan of the abdomen and pelvis (Fig. 1) was ordered. This revealed a 3 by 1.8 cm splenic infarct. Because of her respiratory symptoms and tachycardia, a pulmonary embolism was suspected but was ruled out with a CT angiogram of the chest.
She was diagnosed with new‐onset heart failure and a splenic infarct. However, it was unclear if the 2 problems were linked. Possible etiologies of the splenic infarct included thrombus from hypercoagulable state (given her prior miscarriage, postpartum state), infarct from hemoglobinopathy (given her family history), septic emboli from infective endocarditis, and peripartum cardiomyopathy associated with embolism to the spleen.
Pain control, empiric antibiotics, and intravenous diuretics were started. Twelve hours later, the patient's dyspnea and chest pain resolved. Her blood culture results were negative, and hemoglobin electrophoresis was normal. Results of a hypercoagulable workup for an arterial thrombus that included lupus anticoagulant, anticardiolipin antibodies, and antibodies to 2‐glycoprotein‐I were negative. The echocardiogram (Fig. 2) showed a dilated left ventricle with an ejection fraction (EF) of 10%15%, normal valvular morphology without vegetations, moderate mitral and tricuspid regurgitation, and a 1‐cm left ventricular thrombus and 3 small adjacent thrombi.
Based on the echocardiographic data, recent pregnancy, and absence of other risk factors for heart failure, a diagnosis was made of peripartum cardiomyopathy with left ventricular thrombi and subsequent embolization to the spleen.
Standard heart failure therapy including diuretics, beta‐blockers, and angiotensin‐converting enzyme inhibitors and anticoagulation with warfarin were started. Within 24 hours, the patient was asymptomatic except for minimal abdominal pain. The patient was discharged home in a stable condition the following day. At her outpatient follow‐up 3 months later, she was well compensated and asymptomatic.
DISCUSSION
Using the search terms peripartum cardiomyopathy, cardiomyopathy, thromboembolism, and postpartum period, we performed a MEDLINE search of the English literature from 1950 to 2007. We did not find any reported cases of splenic infarction complicating peripartum cardiomyopathy.
Peripartum cardiomyopathy (PPCM) is a form of dilated cardiomyopathy that occurs as a complication of pregnancy. It can present with heart failure in the last month of pregnancy or within 5 months after delivery.1, 2 The incidence of PPCM is unknown but has been estimated at 1 in 30004000 live births.3
Our patient met the criteria for PPCM as set forth by the National Heart, Lung, and Blood Institute (NHLBI), in conjunction with the Office of Rare Disease of the National Institutes of Health in April 1997.3 To establish a diagnosis of PPCM, 4 criteria have to be met:
-
Development of heart failure in the last month of pregnancy or within 5 months after delivery;
-
Absence of an identifiable cause of heart failure;
-
Absence of recognizable heart disease prior to the last month of pregnancy; and
-
Left ventricular systolic dysfunction demonstrated by echocardiographic variables such as depressed shortening fraction or left ventricular ejection fraction 45%.
Thromboembolism has been reported with an incidence of 4% to 30% in peripartum cardiomyopathy.4 In our literature review, we found several case reports of thromboembolic phenomena complicating peripartum cardiomyopathy. These included lower extremity arterial thromboembolism with compromised circulation,5 cerebral embolism,6 and acute myocardial infarction secondary to coronary artery embolism.7 This is the first reported case of splenic artery embolization leading to splenic infarct as a complication of peripartum cardiomyopathy.
Because of the high risk of thromboembolism, the NHLBI recommends that anticoagulation be added to the standard heart failure treatment of PPCM patients with an ejection fraction of less than 35%,3 although there are no prospective randomized clinical trial data to support this recommendation. For anticoagulation, heparin is generally used in the antepartum period and warfarin in the postpartum period. It has been recommended that anticoagulation be continued for as long as the cardiomegaly persists.1
In addition to anticoagulation for PPCM patients with an EF 35%, standard heart failure therapy includes salt restriction, diuretics, and beta‐blockers. Angiotensin‐converting enzyme inhibitors can be teratogenic during pregnancy but can be used after delivery. Hydralazine can be used safely during pregnancy as an alternative to angiotensin‐converting enzyme inhibitors. Patients failing maximal medical management may be candidates for cardiac transplantation.
Recommendations regarding subsequent pregnancies seem related to the return of ventricular size and function. Patients whose heart size does not return to normal should be strongly advised to avoid future pregnancies.2, 3 Patients who recover ventricular function may have deterioration of left ventricular function with future pregnancies.8 They should be counseled about the risk and closely monitored for development of heart failure if they become pregnant again.
A 26‐year‐old woman presented with a 1‐week history of epigastric and left upper quadrant pain associated with nausea and vomiting. She also described 3 weeks of constant substernal chest pain, dyspnea, and decreased exercise tolerance.
Her medical history was significant for a pituitary macroadenoma diagnosed 6 years previously that had been treated with cabergoline. She had a miscarriage 7 years ago but gave birth to a healthy child 5 months prior to admission. She had smoked 2 cigarettes per day for the last 7 years. She denied alcohol or illicit drug use. Her mother had sickle cell trait.
On admission, her heart rate was 112 beats/minute, blood pressure was 110/80 mm Hg, and respiratory rate was 26 per minute. Jugular venous distension was not appreciated. She had decreased breath sounds over the right lung base. The apical impulse was palpated in the left sixth intercostal space 1 cm lateral to the midclavicular line, and a 2/6 holosystolic murmur was auscultated at the left lower sternal border. No other murmurs or S3 or S4 gallop could be appreciated. There were no vascular or immunological phenomena suggestive of infective endocarditis. She had abdominal tenderness in the epigastrium and bilateral upper quadrants. There was no lower extremity edema, and the extremities were well perfused.
Complete blood count, electrolytes, and liver, renal, and coagulation profiles were normal. Her chest x‐ray revealed cardiomegaly and bilateral pleural effusions. EKG showed sinus tachycardia and nonspecific T‐wave changes. To further evaluate her abdominal pain, a CT scan of the abdomen and pelvis (Fig. 1) was ordered. This revealed a 3 by 1.8 cm splenic infarct. Because of her respiratory symptoms and tachycardia, a pulmonary embolism was suspected but was ruled out with a CT angiogram of the chest.
She was diagnosed with new‐onset heart failure and a splenic infarct. However, it was unclear if the 2 problems were linked. Possible etiologies of the splenic infarct included thrombus from hypercoagulable state (given her prior miscarriage, postpartum state), infarct from hemoglobinopathy (given her family history), septic emboli from infective endocarditis, and peripartum cardiomyopathy associated with embolism to the spleen.
Pain control, empiric antibiotics, and intravenous diuretics were started. Twelve hours later, the patient's dyspnea and chest pain resolved. Her blood culture results were negative, and hemoglobin electrophoresis was normal. Results of a hypercoagulable workup for an arterial thrombus that included lupus anticoagulant, anticardiolipin antibodies, and antibodies to 2‐glycoprotein‐I were negative. The echocardiogram (Fig. 2) showed a dilated left ventricle with an ejection fraction (EF) of 10%15%, normal valvular morphology without vegetations, moderate mitral and tricuspid regurgitation, and a 1‐cm left ventricular thrombus and 3 small adjacent thrombi.
Based on the echocardiographic data, recent pregnancy, and absence of other risk factors for heart failure, a diagnosis was made of peripartum cardiomyopathy with left ventricular thrombi and subsequent embolization to the spleen.
Standard heart failure therapy including diuretics, beta‐blockers, and angiotensin‐converting enzyme inhibitors and anticoagulation with warfarin were started. Within 24 hours, the patient was asymptomatic except for minimal abdominal pain. The patient was discharged home in a stable condition the following day. At her outpatient follow‐up 3 months later, she was well compensated and asymptomatic.
DISCUSSION
Using the search terms peripartum cardiomyopathy, cardiomyopathy, thromboembolism, and postpartum period, we performed a MEDLINE search of the English literature from 1950 to 2007. We did not find any reported cases of splenic infarction complicating peripartum cardiomyopathy.
Peripartum cardiomyopathy (PPCM) is a form of dilated cardiomyopathy that occurs as a complication of pregnancy. It can present with heart failure in the last month of pregnancy or within 5 months after delivery.1, 2 The incidence of PPCM is unknown but has been estimated at 1 in 30004000 live births.3
Our patient met the criteria for PPCM as set forth by the National Heart, Lung, and Blood Institute (NHLBI), in conjunction with the Office of Rare Disease of the National Institutes of Health in April 1997.3 To establish a diagnosis of PPCM, 4 criteria have to be met:
-
Development of heart failure in the last month of pregnancy or within 5 months after delivery;
-
Absence of an identifiable cause of heart failure;
-
Absence of recognizable heart disease prior to the last month of pregnancy; and
-
Left ventricular systolic dysfunction demonstrated by echocardiographic variables such as depressed shortening fraction or left ventricular ejection fraction 45%.
Thromboembolism has been reported with an incidence of 4% to 30% in peripartum cardiomyopathy.4 In our literature review, we found several case reports of thromboembolic phenomena complicating peripartum cardiomyopathy. These included lower extremity arterial thromboembolism with compromised circulation,5 cerebral embolism,6 and acute myocardial infarction secondary to coronary artery embolism.7 This is the first reported case of splenic artery embolization leading to splenic infarct as a complication of peripartum cardiomyopathy.
Because of the high risk of thromboembolism, the NHLBI recommends that anticoagulation be added to the standard heart failure treatment of PPCM patients with an ejection fraction of less than 35%,3 although there are no prospective randomized clinical trial data to support this recommendation. For anticoagulation, heparin is generally used in the antepartum period and warfarin in the postpartum period. It has been recommended that anticoagulation be continued for as long as the cardiomegaly persists.1
In addition to anticoagulation for PPCM patients with an EF 35%, standard heart failure therapy includes salt restriction, diuretics, and beta‐blockers. Angiotensin‐converting enzyme inhibitors can be teratogenic during pregnancy but can be used after delivery. Hydralazine can be used safely during pregnancy as an alternative to angiotensin‐converting enzyme inhibitors. Patients failing maximal medical management may be candidates for cardiac transplantation.
Recommendations regarding subsequent pregnancies seem related to the return of ventricular size and function. Patients whose heart size does not return to normal should be strongly advised to avoid future pregnancies.2, 3 Patients who recover ventricular function may have deterioration of left ventricular function with future pregnancies.8 They should be counseled about the risk and closely monitored for development of heart failure if they become pregnant again.
- ,.Peripartum cardiomyopathy.Circulation.1971;44:964–968.
- ,,, et al.Natural course of peripartum cardiomyopathy.Circulation.1971;44:1053–1061.
- ,,, et al.Peripartum Cardiomyopathy. National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) Workshop Recommendations and Review.JAMA.2000;283:1183–1188.
- .Peripartum cardiomyopathy.N Engl J Med.1985;312:1432–1437.
- ,,, et al.Peripartum cardiomyopathy presenting as lower extremity arterial thromboembolism.J Reprod Med.2000;45:351–353.
- ,,, et al.Cerebral embolism as the initial manifestation of peripartum cardiomyopathy.Neurology.1982;32:668–671.
- ,,, et al.Peripartum cardiomyopathy presenting as an acute myocardial infarction.Mayo Clin Proc.2002;77:500–501.
- ,,, et al.Recurrent peripartum cardiomyopathy.Eur J Obstet Gynecol Reprod Biol.1998;76:29–30.
- ,.Peripartum cardiomyopathy.Circulation.1971;44:964–968.
- ,,, et al.Natural course of peripartum cardiomyopathy.Circulation.1971;44:1053–1061.
- ,,, et al.Peripartum Cardiomyopathy. National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) Workshop Recommendations and Review.JAMA.2000;283:1183–1188.
- .Peripartum cardiomyopathy.N Engl J Med.1985;312:1432–1437.
- ,,, et al.Peripartum cardiomyopathy presenting as lower extremity arterial thromboembolism.J Reprod Med.2000;45:351–353.
- ,,, et al.Cerebral embolism as the initial manifestation of peripartum cardiomyopathy.Neurology.1982;32:668–671.
- ,,, et al.Peripartum cardiomyopathy presenting as an acute myocardial infarction.Mayo Clin Proc.2002;77:500–501.
- ,,, et al.Recurrent peripartum cardiomyopathy.Eur J Obstet Gynecol Reprod Biol.1998;76:29–30.