User login
Four Steps to Diagnosing Drug Overdose
Misconceptions About Opioid Dosing
Use of C1 Lateral Mass and C2 Intralaminar Fixation to Stabilize a 30-Year-Old Odontoid Fracture That Was Causing Myelopathy
Ankle Clonus and Wakeup Tests During Posterior Spinal Fusion: Correlation With Bispectral Index
Closed-Reduction Percutaneous Pinning of a Complex Divergent Carpometacarpal Fracture-Dislocation Involving the 4 Ulnar Carpometacarpal Joints
Takotsubo Cardiomyopathy
Takotsubo cardiomyopathy, also known as transient left ventricular apical ballooning, stress cardiomyopathy, and broken heart syndrome, is a condition that mimics acute myocardial infarction. Patients typically present with chest pain, electrocardiographic changes consistent with acute ischemia or infarct, and elevated cardiac enzymes in the absence of significant coronary artery disease. Left ventriculography demonstrates a characteristic pattern of dysfunction: dyskinesis of the cardiac apex and hyperkinesis of the base. This resulting appearance of apical ballooning is reminiscent of the takotsubo, a Japanese octopus pot with a wide base and narrow top. The syndrome occurs almost exclusively in postmenopausal women and demonstrates a distinct temporal association with extreme emotional or physiological stress. The pathophysiology is poorly understood, but one theory suggests that the transient cardiomyopathy reflects myocardial stunning due to excessive sympathetic output.1 Treatment is supportive, and most patients rapidly recover normal systolic function.
A 57‐year‐old African American female with a past medical history significant only for chronic obstructive pulmonary disease presented with severe dyspnea that was progressive over several hours following the unexpected death of her son. She denied chest pain, palpitations, cough, or fever. On examination, she was afebrile with a blood pressure of 145/82 mm Hg, a pulse of 90 beats per minute, and a respiratory rate of 24 breaths per minute with oxygen saturations of 88% on room air. Lung examination revealed coarse breath sounds with a slightly prolonged expiration phase, but it was otherwise clear. Cardiac examination was unremarkable. Chest radiograph showed only emphysematous changes. Initial electrocardiogram and serial cardiac enzymes were negative. A computed tomography pulmonary angiogram showed no evidence of pulmonary embolism. The patient was admitted with the diagnosis of chronic obstructive pulmonary disease exacerbation and treated with supplemental oxygen, bronchodilators, and corticosteroids.
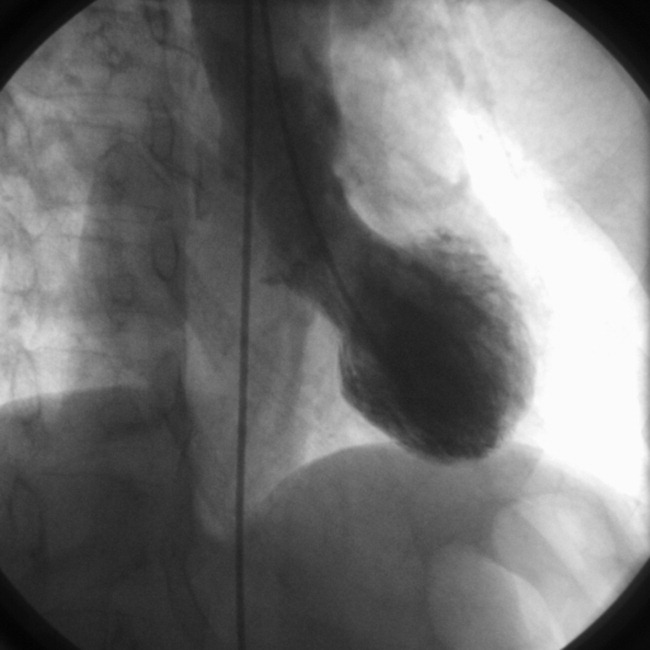
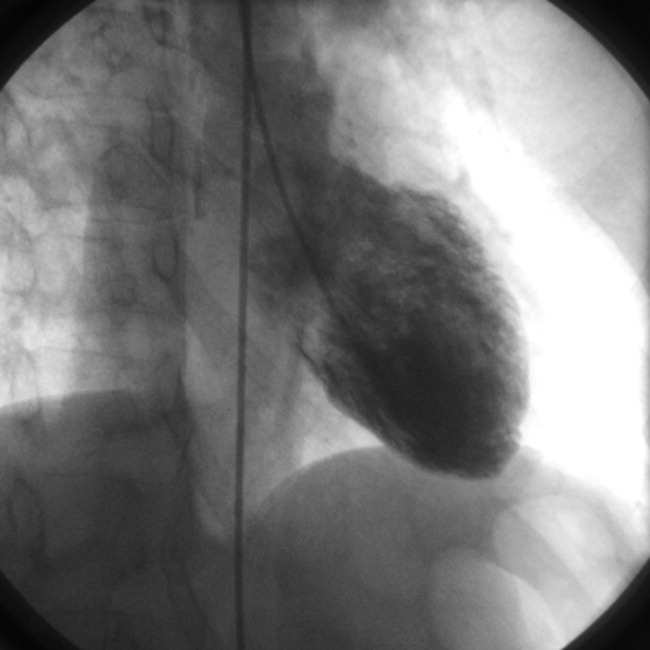
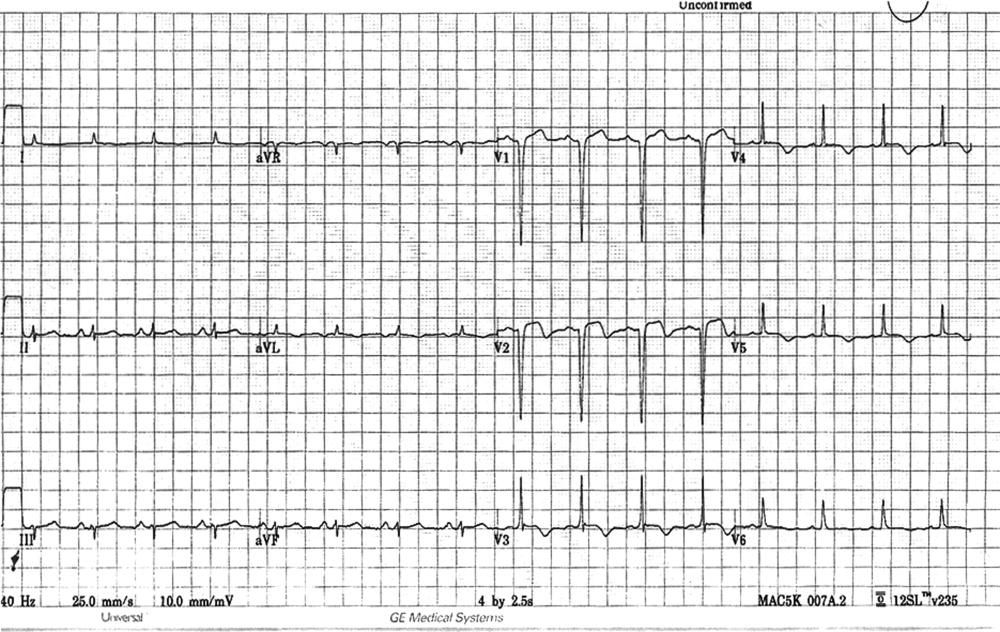
On the following day, the patient developed worsening dyspnea, hypoxia, and diffuse crackles on examination. Electrocardiogram at that time demonstrated ST‐segment elevations in leads V1 and V2 as well as T‐wave inversions in all precordial leads (Figure 1). The troponin‐I concentration was 1.92 ng/mL (0.05 nL), and the brain natriuretic peptide concentration was 1425 pg/mL. The patient underwent urgent cardiac catheterization with no evidence of coronary artery obstruction. Left ventriculogram revealed a hyperdynamic base and akinetic apex extending into the mid‐heart (Figure 2). Left ventricular systolic function was severely reduced, with an estimated ejection fraction of 10% to 15%. The normal diastolic ventriculogram image is shown for comparison (Figure 3). These findings were felt to be consistent with takotsubo syndrome. The patient required inotropic support briefly but experienced full clinical recovery by the sixth hospital day.

DISCUSSION
Takotsubo cardiomyopathy was first described in Japan in 1991.2 Although the condition made a relatively recent debut in the United States, with the first case series published in 2003, subsequent reports have suggested that the condition is not rare.3 Recent analyses of Western populations estimate the prevalence to be approximately 2% among patients with acute coronary syndrome.1, 4, 5 Because women compose the majority of patients with takotsubo cardiomyopathy, the prevalence among women as a subset of patients with acute coronary syndrome is likely much higher. The syndrome has been described as a clinical entity in Japanese, European, Caucasian, and African American patients.2, 3 Interesting differences appear to exist among different ethnic groups. For example, evidence suggests that the condition is more likely to be precipitated by emotional stress in Caucasians, whereas physiological stress is a more frequent trigger in Asians.6
Although chest pain is described as a cardinal feature in takotsubo cardiomyopathy, existing data suggest that African American patients may lack this typical symptom. The first African American female reported with takotsubo syndrome presented with heart failure and hypotension in the absence of chest pain.1 Subsequently, Patel et al.7 reported 5 African American women with takotsubo syndrome. Three patients presented with dyspnea, and 2 presented with nausea: none of the patients experienced chest pain. Our case adds to this evidence by describing an African American woman with takotsubo syndrome whose presenting symptom was severe dyspnea without chest pain. Unlike the majority of reported cases, electrocardiographic and biomarker abnormalities were not present in our patient at admission. As with our patient, the diagnosis of takotsubo cardiomyopathy may initially be overlooked in African Americans because of the atypical presentation. As takotsubo syndrome becomes increasingly recognized in the United States, clinicians are encouraged to consider the diagnosis in African American women who present with severe dyspnea in the setting of extreme emotional or physiological stress. Further research on the pathophysiology of takotsubo cardiomyopathy is needed to explain why such differences in presenting symptoms may exist.
- ,,, et al.Neurohormonal features of myocardial stunning due to sudden emotional stress.N Engl J Med.2005;352:540–548.
- ,,, et al.Myocardial stunning due to simultaneous multivessel coronary spasm: a review of 5 cases.J Cardiol.1991;21:203–214.
- ,,, et al.A syndrome of transient left ventricular apical wall motion abnormality in the absence of coronary disease: a perspective from the United States.Cardiology.2003;100:61–66.
- ,,, et al.Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular ballooning syndrome.Am J Cardiol.2004;94:343–346.
- ,,, et al.Left ventricular apical ballooning: not an uncommon variant of acute myocardial infarction in women.Clin Cardiol.2006;29:9–12.
- ,.Clinical characteristics, demographics and prognosis of transient left ventricular apical ballooning syndrome.Heart Fail Rev.2005;10:311–316.
- ,,, et al.Takotsubo syndrome in African‐American women with atypical presentations: a single‐center experience.Clin Cardiol2007;30:14–18.
Takotsubo cardiomyopathy, also known as transient left ventricular apical ballooning, stress cardiomyopathy, and broken heart syndrome, is a condition that mimics acute myocardial infarction. Patients typically present with chest pain, electrocardiographic changes consistent with acute ischemia or infarct, and elevated cardiac enzymes in the absence of significant coronary artery disease. Left ventriculography demonstrates a characteristic pattern of dysfunction: dyskinesis of the cardiac apex and hyperkinesis of the base. This resulting appearance of apical ballooning is reminiscent of the takotsubo, a Japanese octopus pot with a wide base and narrow top. The syndrome occurs almost exclusively in postmenopausal women and demonstrates a distinct temporal association with extreme emotional or physiological stress. The pathophysiology is poorly understood, but one theory suggests that the transient cardiomyopathy reflects myocardial stunning due to excessive sympathetic output.1 Treatment is supportive, and most patients rapidly recover normal systolic function.
A 57‐year‐old African American female with a past medical history significant only for chronic obstructive pulmonary disease presented with severe dyspnea that was progressive over several hours following the unexpected death of her son. She denied chest pain, palpitations, cough, or fever. On examination, she was afebrile with a blood pressure of 145/82 mm Hg, a pulse of 90 beats per minute, and a respiratory rate of 24 breaths per minute with oxygen saturations of 88% on room air. Lung examination revealed coarse breath sounds with a slightly prolonged expiration phase, but it was otherwise clear. Cardiac examination was unremarkable. Chest radiograph showed only emphysematous changes. Initial electrocardiogram and serial cardiac enzymes were negative. A computed tomography pulmonary angiogram showed no evidence of pulmonary embolism. The patient was admitted with the diagnosis of chronic obstructive pulmonary disease exacerbation and treated with supplemental oxygen, bronchodilators, and corticosteroids.
On the following day, the patient developed worsening dyspnea, hypoxia, and diffuse crackles on examination. Electrocardiogram at that time demonstrated ST‐segment elevations in leads V1 and V2 as well as T‐wave inversions in all precordial leads (Figure 1). The troponin‐I concentration was 1.92 ng/mL (0.05 nL), and the brain natriuretic peptide concentration was 1425 pg/mL. The patient underwent urgent cardiac catheterization with no evidence of coronary artery obstruction. Left ventriculogram revealed a hyperdynamic base and akinetic apex extending into the mid‐heart (Figure 2). Left ventricular systolic function was severely reduced, with an estimated ejection fraction of 10% to 15%. The normal diastolic ventriculogram image is shown for comparison (Figure 3). These findings were felt to be consistent with takotsubo syndrome. The patient required inotropic support briefly but experienced full clinical recovery by the sixth hospital day.
DISCUSSION
Takotsubo cardiomyopathy was first described in Japan in 1991.2 Although the condition made a relatively recent debut in the United States, with the first case series published in 2003, subsequent reports have suggested that the condition is not rare.3 Recent analyses of Western populations estimate the prevalence to be approximately 2% among patients with acute coronary syndrome.1, 4, 5 Because women compose the majority of patients with takotsubo cardiomyopathy, the prevalence among women as a subset of patients with acute coronary syndrome is likely much higher. The syndrome has been described as a clinical entity in Japanese, European, Caucasian, and African American patients.2, 3 Interesting differences appear to exist among different ethnic groups. For example, evidence suggests that the condition is more likely to be precipitated by emotional stress in Caucasians, whereas physiological stress is a more frequent trigger in Asians.6
Although chest pain is described as a cardinal feature in takotsubo cardiomyopathy, existing data suggest that African American patients may lack this typical symptom. The first African American female reported with takotsubo syndrome presented with heart failure and hypotension in the absence of chest pain.1 Subsequently, Patel et al.7 reported 5 African American women with takotsubo syndrome. Three patients presented with dyspnea, and 2 presented with nausea: none of the patients experienced chest pain. Our case adds to this evidence by describing an African American woman with takotsubo syndrome whose presenting symptom was severe dyspnea without chest pain. Unlike the majority of reported cases, electrocardiographic and biomarker abnormalities were not present in our patient at admission. As with our patient, the diagnosis of takotsubo cardiomyopathy may initially be overlooked in African Americans because of the atypical presentation. As takotsubo syndrome becomes increasingly recognized in the United States, clinicians are encouraged to consider the diagnosis in African American women who present with severe dyspnea in the setting of extreme emotional or physiological stress. Further research on the pathophysiology of takotsubo cardiomyopathy is needed to explain why such differences in presenting symptoms may exist.
Takotsubo cardiomyopathy, also known as transient left ventricular apical ballooning, stress cardiomyopathy, and broken heart syndrome, is a condition that mimics acute myocardial infarction. Patients typically present with chest pain, electrocardiographic changes consistent with acute ischemia or infarct, and elevated cardiac enzymes in the absence of significant coronary artery disease. Left ventriculography demonstrates a characteristic pattern of dysfunction: dyskinesis of the cardiac apex and hyperkinesis of the base. This resulting appearance of apical ballooning is reminiscent of the takotsubo, a Japanese octopus pot with a wide base and narrow top. The syndrome occurs almost exclusively in postmenopausal women and demonstrates a distinct temporal association with extreme emotional or physiological stress. The pathophysiology is poorly understood, but one theory suggests that the transient cardiomyopathy reflects myocardial stunning due to excessive sympathetic output.1 Treatment is supportive, and most patients rapidly recover normal systolic function.
A 57‐year‐old African American female with a past medical history significant only for chronic obstructive pulmonary disease presented with severe dyspnea that was progressive over several hours following the unexpected death of her son. She denied chest pain, palpitations, cough, or fever. On examination, she was afebrile with a blood pressure of 145/82 mm Hg, a pulse of 90 beats per minute, and a respiratory rate of 24 breaths per minute with oxygen saturations of 88% on room air. Lung examination revealed coarse breath sounds with a slightly prolonged expiration phase, but it was otherwise clear. Cardiac examination was unremarkable. Chest radiograph showed only emphysematous changes. Initial electrocardiogram and serial cardiac enzymes were negative. A computed tomography pulmonary angiogram showed no evidence of pulmonary embolism. The patient was admitted with the diagnosis of chronic obstructive pulmonary disease exacerbation and treated with supplemental oxygen, bronchodilators, and corticosteroids.
On the following day, the patient developed worsening dyspnea, hypoxia, and diffuse crackles on examination. Electrocardiogram at that time demonstrated ST‐segment elevations in leads V1 and V2 as well as T‐wave inversions in all precordial leads (Figure 1). The troponin‐I concentration was 1.92 ng/mL (0.05 nL), and the brain natriuretic peptide concentration was 1425 pg/mL. The patient underwent urgent cardiac catheterization with no evidence of coronary artery obstruction. Left ventriculogram revealed a hyperdynamic base and akinetic apex extending into the mid‐heart (Figure 2). Left ventricular systolic function was severely reduced, with an estimated ejection fraction of 10% to 15%. The normal diastolic ventriculogram image is shown for comparison (Figure 3). These findings were felt to be consistent with takotsubo syndrome. The patient required inotropic support briefly but experienced full clinical recovery by the sixth hospital day.
DISCUSSION
Takotsubo cardiomyopathy was first described in Japan in 1991.2 Although the condition made a relatively recent debut in the United States, with the first case series published in 2003, subsequent reports have suggested that the condition is not rare.3 Recent analyses of Western populations estimate the prevalence to be approximately 2% among patients with acute coronary syndrome.1, 4, 5 Because women compose the majority of patients with takotsubo cardiomyopathy, the prevalence among women as a subset of patients with acute coronary syndrome is likely much higher. The syndrome has been described as a clinical entity in Japanese, European, Caucasian, and African American patients.2, 3 Interesting differences appear to exist among different ethnic groups. For example, evidence suggests that the condition is more likely to be precipitated by emotional stress in Caucasians, whereas physiological stress is a more frequent trigger in Asians.6
Although chest pain is described as a cardinal feature in takotsubo cardiomyopathy, existing data suggest that African American patients may lack this typical symptom. The first African American female reported with takotsubo syndrome presented with heart failure and hypotension in the absence of chest pain.1 Subsequently, Patel et al.7 reported 5 African American women with takotsubo syndrome. Three patients presented with dyspnea, and 2 presented with nausea: none of the patients experienced chest pain. Our case adds to this evidence by describing an African American woman with takotsubo syndrome whose presenting symptom was severe dyspnea without chest pain. Unlike the majority of reported cases, electrocardiographic and biomarker abnormalities were not present in our patient at admission. As with our patient, the diagnosis of takotsubo cardiomyopathy may initially be overlooked in African Americans because of the atypical presentation. As takotsubo syndrome becomes increasingly recognized in the United States, clinicians are encouraged to consider the diagnosis in African American women who present with severe dyspnea in the setting of extreme emotional or physiological stress. Further research on the pathophysiology of takotsubo cardiomyopathy is needed to explain why such differences in presenting symptoms may exist.
- ,,, et al.Neurohormonal features of myocardial stunning due to sudden emotional stress.N Engl J Med.2005;352:540–548.
- ,,, et al.Myocardial stunning due to simultaneous multivessel coronary spasm: a review of 5 cases.J Cardiol.1991;21:203–214.
- ,,, et al.A syndrome of transient left ventricular apical wall motion abnormality in the absence of coronary disease: a perspective from the United States.Cardiology.2003;100:61–66.
- ,,, et al.Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular ballooning syndrome.Am J Cardiol.2004;94:343–346.
- ,,, et al.Left ventricular apical ballooning: not an uncommon variant of acute myocardial infarction in women.Clin Cardiol.2006;29:9–12.
- ,.Clinical characteristics, demographics and prognosis of transient left ventricular apical ballooning syndrome.Heart Fail Rev.2005;10:311–316.
- ,,, et al.Takotsubo syndrome in African‐American women with atypical presentations: a single‐center experience.Clin Cardiol2007;30:14–18.
- ,,, et al.Neurohormonal features of myocardial stunning due to sudden emotional stress.N Engl J Med.2005;352:540–548.
- ,,, et al.Myocardial stunning due to simultaneous multivessel coronary spasm: a review of 5 cases.J Cardiol.1991;21:203–214.
- ,,, et al.A syndrome of transient left ventricular apical wall motion abnormality in the absence of coronary disease: a perspective from the United States.Cardiology.2003;100:61–66.
- ,,, et al.Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular ballooning syndrome.Am J Cardiol.2004;94:343–346.
- ,,, et al.Left ventricular apical ballooning: not an uncommon variant of acute myocardial infarction in women.Clin Cardiol.2006;29:9–12.
- ,.Clinical characteristics, demographics and prognosis of transient left ventricular apical ballooning syndrome.Heart Fail Rev.2005;10:311–316.
- ,,, et al.Takotsubo syndrome in African‐American women with atypical presentations: a single‐center experience.Clin Cardiol2007;30:14–18.
Legionella pneumonia and use of the Legionella urinary antigen test
A 33‐year‐old Caucasian woman presented to an outside hospital with a 10‐day history of fever, cough, and progressive dyspnea on exertion. Ten days prior to the onset of symptoms, she had traveled to Calgary, Alberta, Canada. Her niece and nephew had recently suffered upper respiratory symptoms. Additional review of systems was negative for joint pain, rash, diarrhea, or bloody stools. She had a history of ulcerative colitis, primary sclerosing cholangitis, and juvenile rheumatoid arthritis. Her outpatient medications included prednisone 10 mg daily, methotrexate 7.5 mg weekly, and ursodiol 200 mg 3 times daily. She was employed at a local hospital and her annual purified protein derivative (PPD) test had been negative. Computed tomography angiography demonstrated bilateral patchy consolidation. Vancomycin, levofloxacin, piperacillin/tazobactam, and fluconazole were initiated and she was transferred to our hospital for further evaluation.
On arrival, her vital signs were within normal limits. She was breathing comfortably but on auscultation had crackles at the right‐mid lung field. A complete blood cell count demonstrated a white blood cell count of 7000/L with left shift, hemoglobin 10.7 g/dL, and platelet count 156,000/L. Liver function tests showed albumin 2.6 g/dL, total bilirubin 9.0 mg/dL with conjugated fraction 6.6 mg/dL, alkaline phosphatase 586 U/L, aspartate aminotransferase 104 U/L, and alanine aminotransferase 72 U/L; these were all near her baseline. The basic metabolic panel was within normal limits. A chest X‐ray showed dense areas of consolidation in the lingula and left upper lobe. All antibiotics from the outside hospital were discontinued and empiric moxifloxacin was initiated.
On hospital day 1, she underwent bronchoscopy, which yielded cloudy fluid from the bronchoalveolar lavage (BAL). Initial BAL gram stain showed moderate white blood cells but no organisms; fungal smears and stains for acid fast bacilli were negative. Blood cultures and Legionella and Streptococcus urinary antigen tests were negative. The remainder of her hospital course was uneventful. Her shortness of breath improved and she remained afebrile. She was discharged home on a 10‐day course of moxifloxacin with close follow‐up. Six days after the BAL specimen was collected, the culture grew Legionella micdadei. Repeat chest film 2 weeks later demonstrated resolution of the original findings.
DISCUSSION
Legionella is responsible for 8000 to 18,000 hospitalizations for pneumonia annually.1 It is associated with community‐acquired, hospital‐acquired, and travel‐associated pneumonia. Twenty‐five Legionella species have been identified and 8 species are associated with pneumonia in humans.2 Community‐acquired and travel‐acquired Legionella pneumonia is most commonly caused by Legionella pneumophila; the second most common cause is L. micdadei.2, 3 It was initially identified in 1977 at the University of Pittsburgh in renal transplant patients with acute pneumonitis and is known as the Pittsburgh pneumonia agent. Similar cases were identified in a group of immunocompromised patients in Virginia, all of whom were receiving steroids and cytotoxic chemotherapy. It is unclear why L. micdadei predominates in this population, but is likely related to its decreased virulence compared to L. pneumophila. The definitive mode of transmission of L. micdadei is not known; it may be from contaminated water supplies but infections from inhalation of respiratory secretions have also been documented.2 While L. micdadei is not commonly seen in travel‐associated Legionella pneumonia, the patient's immunocompromised status secondary to the treatment of her underlying medical conditions made her particularly vulnerable. Given the temporal association with her trip, she was most likely exposed during her travels but her hospital employment should also be considered.
Legionella pneumonia is underdiagnosed because of difficulty distinguishing it from other types of pneumonia, failure to order diagnostic tests, and variable sensitivity of available diagnostic tests.4 Culture is considered the gold standard and is ideally performed from lower respiratory secretions, but variable sensitivity due to interlaboratory variation (range, 10%‐80%) limits its use.3, 4 Direct immunofluorescence assay (DFA) testing of respiratory secretions is available but also limited by poor sensitivity. Both culture and DFA have specificities approaching 100%. A newer test, the Legionella urinary antigen test, is an immunochromatographic assay. It is less technically difficult and results are available in less than 1 hour. The assay can detect the antigen in the urine starting 1 day after the onset of symptoms, and can remain positive for days or weeks following treatment.4
With the introduction and wide availability of the Legionella urinary antigen test, it is important to consider its limitations. While the test carries a high specificity, it detects only the soluble antigen of Legionella pneumophila serogroup 1. Thus, as in this case, the urinary test can be negative when infection is caused by other species such as L. micdadei. In the literature, the urine assay's sensitivity is variously reported at 45% to 100% with lower sensitivities in circumstances such as hospital‐acquired disease, where the association with other species is higher than in the community setting.3, 4 For instance, in nosocomial infections, the reported sensitivity is 45%.3 False‐positive results have also been seen in patients with serum sickness.4
The Legionella urinary antigen test has improved detection of Legionella pneumonia. Given its limitations, it is likely to be most accurate in community‐acquired and travel‐acquired cases.3 The Centers for Disease Control and Prevention recommend testing for Legionella in pneumonia patients requiring admission to the intensive care unit (ICU), immunocompromised patients, patients who traveled within 2 weeks of presentation, and those who have failed treatment with beta‐lactams or cephalosporins. A negative test does not rule out Legionella infection and additional testing with bronchoscopy may be indicated, especially in immunocompromised hosts.4
- Centers for Disease Control. Legionellosis Resource Site (Legionnaires' Disease and Pontiac Fever). Top 10 Things Every Clinician Needs to Know About Legionellosis. Available at http://www.cdc.gov/legionella/top10.htm. Accessed February2009.
- ,,.Disease due to the legionellaceae (other than Legionella pneumophila): historical, microbiological, clinical, and epidemiological review.Medicine.1989;68:116–132.
- ,,, et al.Clinical utility of urinary antigen detection for diagnosis of community‐acquired, travel‐associated, and nosocomial legionnaire's disease.J Clin Microbiol.2003;41(2):838–840.
- .Diagnosis of Legionella infection.Clin Infect Dis.2003;36:64–69.
A 33‐year‐old Caucasian woman presented to an outside hospital with a 10‐day history of fever, cough, and progressive dyspnea on exertion. Ten days prior to the onset of symptoms, she had traveled to Calgary, Alberta, Canada. Her niece and nephew had recently suffered upper respiratory symptoms. Additional review of systems was negative for joint pain, rash, diarrhea, or bloody stools. She had a history of ulcerative colitis, primary sclerosing cholangitis, and juvenile rheumatoid arthritis. Her outpatient medications included prednisone 10 mg daily, methotrexate 7.5 mg weekly, and ursodiol 200 mg 3 times daily. She was employed at a local hospital and her annual purified protein derivative (PPD) test had been negative. Computed tomography angiography demonstrated bilateral patchy consolidation. Vancomycin, levofloxacin, piperacillin/tazobactam, and fluconazole were initiated and she was transferred to our hospital for further evaluation.
On arrival, her vital signs were within normal limits. She was breathing comfortably but on auscultation had crackles at the right‐mid lung field. A complete blood cell count demonstrated a white blood cell count of 7000/L with left shift, hemoglobin 10.7 g/dL, and platelet count 156,000/L. Liver function tests showed albumin 2.6 g/dL, total bilirubin 9.0 mg/dL with conjugated fraction 6.6 mg/dL, alkaline phosphatase 586 U/L, aspartate aminotransferase 104 U/L, and alanine aminotransferase 72 U/L; these were all near her baseline. The basic metabolic panel was within normal limits. A chest X‐ray showed dense areas of consolidation in the lingula and left upper lobe. All antibiotics from the outside hospital were discontinued and empiric moxifloxacin was initiated.
On hospital day 1, she underwent bronchoscopy, which yielded cloudy fluid from the bronchoalveolar lavage (BAL). Initial BAL gram stain showed moderate white blood cells but no organisms; fungal smears and stains for acid fast bacilli were negative. Blood cultures and Legionella and Streptococcus urinary antigen tests were negative. The remainder of her hospital course was uneventful. Her shortness of breath improved and she remained afebrile. She was discharged home on a 10‐day course of moxifloxacin with close follow‐up. Six days after the BAL specimen was collected, the culture grew Legionella micdadei. Repeat chest film 2 weeks later demonstrated resolution of the original findings.
DISCUSSION
Legionella is responsible for 8000 to 18,000 hospitalizations for pneumonia annually.1 It is associated with community‐acquired, hospital‐acquired, and travel‐associated pneumonia. Twenty‐five Legionella species have been identified and 8 species are associated with pneumonia in humans.2 Community‐acquired and travel‐acquired Legionella pneumonia is most commonly caused by Legionella pneumophila; the second most common cause is L. micdadei.2, 3 It was initially identified in 1977 at the University of Pittsburgh in renal transplant patients with acute pneumonitis and is known as the Pittsburgh pneumonia agent. Similar cases were identified in a group of immunocompromised patients in Virginia, all of whom were receiving steroids and cytotoxic chemotherapy. It is unclear why L. micdadei predominates in this population, but is likely related to its decreased virulence compared to L. pneumophila. The definitive mode of transmission of L. micdadei is not known; it may be from contaminated water supplies but infections from inhalation of respiratory secretions have also been documented.2 While L. micdadei is not commonly seen in travel‐associated Legionella pneumonia, the patient's immunocompromised status secondary to the treatment of her underlying medical conditions made her particularly vulnerable. Given the temporal association with her trip, she was most likely exposed during her travels but her hospital employment should also be considered.
Legionella pneumonia is underdiagnosed because of difficulty distinguishing it from other types of pneumonia, failure to order diagnostic tests, and variable sensitivity of available diagnostic tests.4 Culture is considered the gold standard and is ideally performed from lower respiratory secretions, but variable sensitivity due to interlaboratory variation (range, 10%‐80%) limits its use.3, 4 Direct immunofluorescence assay (DFA) testing of respiratory secretions is available but also limited by poor sensitivity. Both culture and DFA have specificities approaching 100%. A newer test, the Legionella urinary antigen test, is an immunochromatographic assay. It is less technically difficult and results are available in less than 1 hour. The assay can detect the antigen in the urine starting 1 day after the onset of symptoms, and can remain positive for days or weeks following treatment.4
With the introduction and wide availability of the Legionella urinary antigen test, it is important to consider its limitations. While the test carries a high specificity, it detects only the soluble antigen of Legionella pneumophila serogroup 1. Thus, as in this case, the urinary test can be negative when infection is caused by other species such as L. micdadei. In the literature, the urine assay's sensitivity is variously reported at 45% to 100% with lower sensitivities in circumstances such as hospital‐acquired disease, where the association with other species is higher than in the community setting.3, 4 For instance, in nosocomial infections, the reported sensitivity is 45%.3 False‐positive results have also been seen in patients with serum sickness.4
The Legionella urinary antigen test has improved detection of Legionella pneumonia. Given its limitations, it is likely to be most accurate in community‐acquired and travel‐acquired cases.3 The Centers for Disease Control and Prevention recommend testing for Legionella in pneumonia patients requiring admission to the intensive care unit (ICU), immunocompromised patients, patients who traveled within 2 weeks of presentation, and those who have failed treatment with beta‐lactams or cephalosporins. A negative test does not rule out Legionella infection and additional testing with bronchoscopy may be indicated, especially in immunocompromised hosts.4
A 33‐year‐old Caucasian woman presented to an outside hospital with a 10‐day history of fever, cough, and progressive dyspnea on exertion. Ten days prior to the onset of symptoms, she had traveled to Calgary, Alberta, Canada. Her niece and nephew had recently suffered upper respiratory symptoms. Additional review of systems was negative for joint pain, rash, diarrhea, or bloody stools. She had a history of ulcerative colitis, primary sclerosing cholangitis, and juvenile rheumatoid arthritis. Her outpatient medications included prednisone 10 mg daily, methotrexate 7.5 mg weekly, and ursodiol 200 mg 3 times daily. She was employed at a local hospital and her annual purified protein derivative (PPD) test had been negative. Computed tomography angiography demonstrated bilateral patchy consolidation. Vancomycin, levofloxacin, piperacillin/tazobactam, and fluconazole were initiated and she was transferred to our hospital for further evaluation.
On arrival, her vital signs were within normal limits. She was breathing comfortably but on auscultation had crackles at the right‐mid lung field. A complete blood cell count demonstrated a white blood cell count of 7000/L with left shift, hemoglobin 10.7 g/dL, and platelet count 156,000/L. Liver function tests showed albumin 2.6 g/dL, total bilirubin 9.0 mg/dL with conjugated fraction 6.6 mg/dL, alkaline phosphatase 586 U/L, aspartate aminotransferase 104 U/L, and alanine aminotransferase 72 U/L; these were all near her baseline. The basic metabolic panel was within normal limits. A chest X‐ray showed dense areas of consolidation in the lingula and left upper lobe. All antibiotics from the outside hospital were discontinued and empiric moxifloxacin was initiated.
On hospital day 1, she underwent bronchoscopy, which yielded cloudy fluid from the bronchoalveolar lavage (BAL). Initial BAL gram stain showed moderate white blood cells but no organisms; fungal smears and stains for acid fast bacilli were negative. Blood cultures and Legionella and Streptococcus urinary antigen tests were negative. The remainder of her hospital course was uneventful. Her shortness of breath improved and she remained afebrile. She was discharged home on a 10‐day course of moxifloxacin with close follow‐up. Six days after the BAL specimen was collected, the culture grew Legionella micdadei. Repeat chest film 2 weeks later demonstrated resolution of the original findings.
DISCUSSION
Legionella is responsible for 8000 to 18,000 hospitalizations for pneumonia annually.1 It is associated with community‐acquired, hospital‐acquired, and travel‐associated pneumonia. Twenty‐five Legionella species have been identified and 8 species are associated with pneumonia in humans.2 Community‐acquired and travel‐acquired Legionella pneumonia is most commonly caused by Legionella pneumophila; the second most common cause is L. micdadei.2, 3 It was initially identified in 1977 at the University of Pittsburgh in renal transplant patients with acute pneumonitis and is known as the Pittsburgh pneumonia agent. Similar cases were identified in a group of immunocompromised patients in Virginia, all of whom were receiving steroids and cytotoxic chemotherapy. It is unclear why L. micdadei predominates in this population, but is likely related to its decreased virulence compared to L. pneumophila. The definitive mode of transmission of L. micdadei is not known; it may be from contaminated water supplies but infections from inhalation of respiratory secretions have also been documented.2 While L. micdadei is not commonly seen in travel‐associated Legionella pneumonia, the patient's immunocompromised status secondary to the treatment of her underlying medical conditions made her particularly vulnerable. Given the temporal association with her trip, she was most likely exposed during her travels but her hospital employment should also be considered.
Legionella pneumonia is underdiagnosed because of difficulty distinguishing it from other types of pneumonia, failure to order diagnostic tests, and variable sensitivity of available diagnostic tests.4 Culture is considered the gold standard and is ideally performed from lower respiratory secretions, but variable sensitivity due to interlaboratory variation (range, 10%‐80%) limits its use.3, 4 Direct immunofluorescence assay (DFA) testing of respiratory secretions is available but also limited by poor sensitivity. Both culture and DFA have specificities approaching 100%. A newer test, the Legionella urinary antigen test, is an immunochromatographic assay. It is less technically difficult and results are available in less than 1 hour. The assay can detect the antigen in the urine starting 1 day after the onset of symptoms, and can remain positive for days or weeks following treatment.4
With the introduction and wide availability of the Legionella urinary antigen test, it is important to consider its limitations. While the test carries a high specificity, it detects only the soluble antigen of Legionella pneumophila serogroup 1. Thus, as in this case, the urinary test can be negative when infection is caused by other species such as L. micdadei. In the literature, the urine assay's sensitivity is variously reported at 45% to 100% with lower sensitivities in circumstances such as hospital‐acquired disease, where the association with other species is higher than in the community setting.3, 4 For instance, in nosocomial infections, the reported sensitivity is 45%.3 False‐positive results have also been seen in patients with serum sickness.4
The Legionella urinary antigen test has improved detection of Legionella pneumonia. Given its limitations, it is likely to be most accurate in community‐acquired and travel‐acquired cases.3 The Centers for Disease Control and Prevention recommend testing for Legionella in pneumonia patients requiring admission to the intensive care unit (ICU), immunocompromised patients, patients who traveled within 2 weeks of presentation, and those who have failed treatment with beta‐lactams or cephalosporins. A negative test does not rule out Legionella infection and additional testing with bronchoscopy may be indicated, especially in immunocompromised hosts.4
- Centers for Disease Control. Legionellosis Resource Site (Legionnaires' Disease and Pontiac Fever). Top 10 Things Every Clinician Needs to Know About Legionellosis. Available at http://www.cdc.gov/legionella/top10.htm. Accessed February2009.
- ,,.Disease due to the legionellaceae (other than Legionella pneumophila): historical, microbiological, clinical, and epidemiological review.Medicine.1989;68:116–132.
- ,,, et al.Clinical utility of urinary antigen detection for diagnosis of community‐acquired, travel‐associated, and nosocomial legionnaire's disease.J Clin Microbiol.2003;41(2):838–840.
- .Diagnosis of Legionella infection.Clin Infect Dis.2003;36:64–69.
- Centers for Disease Control. Legionellosis Resource Site (Legionnaires' Disease and Pontiac Fever). Top 10 Things Every Clinician Needs to Know About Legionellosis. Available at http://www.cdc.gov/legionella/top10.htm. Accessed February2009.
- ,,.Disease due to the legionellaceae (other than Legionella pneumophila): historical, microbiological, clinical, and epidemiological review.Medicine.1989;68:116–132.
- ,,, et al.Clinical utility of urinary antigen detection for diagnosis of community‐acquired, travel‐associated, and nosocomial legionnaire's disease.J Clin Microbiol.2003;41(2):838–840.
- .Diagnosis of Legionella infection.Clin Infect Dis.2003;36:64–69.