User login
Concomitant Fractures of Capitellum and Radial Neck in an Adolescent
A refractory case of community-acquired pneumonia
CASE: A 26-year-old woman came to our emergency department with shortness of breath—a symptom that had begun 2 weeks earlier and was getting steadily worse. She had a history of severe, persistent asthma, and had been admitted to the ICU—but not intubated—9 months earlier. Now, she reported dyspnea with even mild exertion, which inhalers failed to relieve.
The patient also had a cough and had recently begun producing thick, green sputum, but said she’d had no chest pain, fever, or lower extremity swelling. The young woman lived with her parents, both of whom smoked heavily, but denied tobacco or alcohol use herself. She had not taken antibiotics in the past 6 months.
On physical examination, the patient was afebrile, mildly tachypneic, and had a heart rate of 125 bpm. She was saturating 80% on ambient air and 95% on 2 liters per minute via nasal cannula; her lung exam was significant for diffuse wheezes and rhonchi, but the remainder of the physical exam was normal.
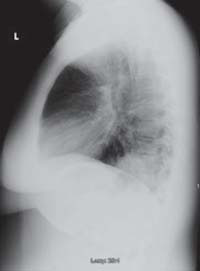
Lab tests revealed a white blood cell count of 25,200/mcL, with 81% neutrophils. Blood and urine cultures were preliminarily negative. We sent a sputum sample to be cultured and took chest x-rays. Posterior-anterior (PA) (FIGURE 1) and lateral (FIGURE 2) radiographs showed a dense right lower lobe inflltrate.
We diagnosed community-acquired pneumonia (CAP), coupled with an acute exacerbation of asthma, and admitted the patient to the hospital. We started her on intravenous (IV) moxifloxacin, parenteral steroids, and nebulized albuterol and ipratropium. But by the patient’s third day in the hospital, her white blood cell count had climbed to 34,500/mcL, and she still required oxygen by nasal cannula.
FIGURE 1 PA x-ray shows right lower lobe infiltrate
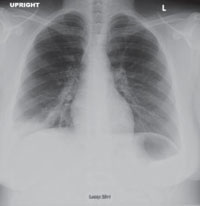
FIGURE 2 Dense infiltrate on lateral view
WHY DIDN’T THIS PATIENT RESPOND TO DRUG THERAPY?
CAP complicated by CA-MRSA
Initially, this appeared to be a rather straightforward case of CAP and asthma. The return of the sputum cultures on day 4, showing positive results for methicillin-resistant Staphylococcus aureus (MRSA), indicated that this was not the case. Sensitivity analysis revealed intermediate susceptibility to moxifloxacin and sensitivity to trimethoprim-sulfamethoxazole (TMP-SMX), vancomycin, and linezolid.
We switched the patient’s antibiotic from moxifloxacin to parenteral linezolid. She responded rapidly. On day 5, the patient was successfully weaned from O2 and converted to oral linezolid; the following day, she was discharged, with orders to complete an 8-day course of linezolid and an appointment with her family physician for the following week. At follow-up, she was doing well.
Cultures are crucial if results would alter Tx
In 2007, the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) published guidelines on the management of CAP1—a clinical diagnosis based on the presence of select features, including cough, fever, sputum production, and pleuritic chest pain. (Imaging of the chest may be used to support the diagnosis, but is not required.)
Following a site-of-care decision, ideally made with the help of a severity-of-illness scoring system such as the CURB-65 (Confusion, Urea nitrogen, Respiratory rate, Blood pressure, 65 years of age and older) or Pneumonia Severity Index, the guidelines recommend cultures whenever the result is likely to significantly alter standard empiric treatment.1
Pretreatment blood samples for culture should be obtained (strength of recommendation: A, well-conducted randomized controlled trials). The IDSA/ATS CAP guidelines also recommend an expectorated sputum sample for stain and culture for patients admitted to the ICU, as well as for those with a presentation suggestive of CAP who:
- have failed outpatient treatment;
- abuse alcohol;
- have severe structural or obstructive lung disease;
- or have pleural effusion.1
In our patient’s case, we obtained a sputum culture on admission because of her severe asthma. She was persistently hypoxic during her initial days in the hospital, and when the sputum culture returned positive for MRSA, her regimen of antibiotics was adjusted.
Suspect CA-MRSA when CAP is severe
Although MRSA has traditionally been thought of as a nosocomial pathogen, infections caused by distinct CA-MRSA strains are on the rise. An estimated 1% to 10% of CAP cases are caused by S aureus, but the percentage of those strains that are resistant to methicillin is not known.2
Clinical risk factors for S aureus CAP include end-stage renal disease, injection drug use, prior influenza, and prior antibiotic therapy, especially with fluoroquinolones.1 How-ever, CA-MRSA CAP often affects children and healthy young adults without any risk factors.3,4
Additionally, CAP that is caused by CA-MRSA is typically severe, often involving empyema, acute respiratory distress syndrome (ARDS), cavitary pneumonia, or severe sepsis.5 Consider a diagnosis of CA-MRSA CAP in patients who present with cavitary infiltrates without risk factors for anaerobic aspiration, such as syncope, seizures, alcohol abuse, or esophageal motility disorders.1
Start treatment without delay in patients at risk
Standard empiric treatment options for hospitalized patients with CAP (with the exception of those in the ICU) include either a beta-lactam and azithromycin or a respiratory fluoroquinolone (neither of which is active against MRSA).1 All patients who are hospitalized for CAP should be started on this regimen without delay. If gram-positive cocci in clusters suggestive of S aureus are isolated from sputum, this standard empiric regimen should be adequate until further microbiologic identification is available.1 While most cases of S aureus CAP are not MRSA, the increased mortality rate associated with inappropriate antibiotic selection led the IDSA/ATS to recommend broader empiric coverage for MRSA for patients with risk factors for S aureus.1
CA-MRSA strains are distinct from their nosocomial counterpart, and the optimal therapy for confirmed CA-MRSA CAP has not been determined. Frequently, CA-MRSA isolates are sensitive to TMP-SMX, clindamycin, and fluoroquinolones. But neither fluoroquinolones nor TMP-SMX have a clear effect on toxin production, and bacterial resistance frequently emerges during therapy with clindamycin.1
The IDSA/ATS guidelines recommend either vancomycin or linezolid for CAP due to CA-MRSA, and these are the most widely used drugs for invasive CA-MRSA infections. Linezolid has been recognized as having a theoretical advantage in treating pneumonia, as it achieves higher lung epithelial concentrations than vancomycin.6 Particularly in cases of necrotizing CA-MRSA pneumonia, vancomycin has not been found to decrease toxin production, and linezolid is therefore the preferred treatment.1 Because of the limitations of vancomycin, we chose linezolid for our patient.
Treatment duration is not evidence-based
Although most patients with CAP are treated for 7 to 10 days, there are few well-designed studies evaluating the optimal time frame. Guidelines for the duration of antibiotics for CAP recommend a minimum of 5 days of therapy, presuming the patient is clinically stable.1,7 Short-duration therapy for patients with bacteremic S aureus CAP infection has been associated with an increased risk of endocarditis, and the presence of pulmonary cavities may warrant prolonged therapy.1 Our patient had an isolate of S aureus with intermediate susceptibility to moxifloxacin, which likely explains her rapid response to linezolid. She remained on linezolid for 8 days.
• Consider CA-MRSA as a cause of CAP, especially in cases in which the presentation is severe, as the guidelines for empiric treatment of CAP feature antibiotics that are not active against the CA-MRSA pathogen.
• Order sputum cultures for all patients admitted to the ICU, as well as for patients with a clinical presentation suggestive of CAP who abuse alcohol, have severe asthma or other lung disease, or have a pleural effusion.
• Start patients with CA-MRSA CAP on linezolid without delay.
The author reported no potential conflict of interest relevant to this article.
1. Mandell LA, Wunderink RG, Anzueto A, et al. IDSA/ATS Guidelines for CAP in adults. Clin Infect Dis. 2007;44(suppl 2):S27-S72.
2. Hidron AI, Low CE, Honig EG, et al. Emergence of community-acquired methicillin-resistant Staphylococcus aureus strain USA300 as a cause of necrotizing community-onset pneumonia. Lancet Infect Dis. 2009;9:384-392.
3. Torell E, Molin D, Tano E, et al. CAP and bacteraemia in a healthy young woman caused by methicillin-resistant Staphylococcus aureus (MRSA) carrying the genes encoding Panton-Valentine leukocidin (PVL). Scandinavian J Inf Dis. 2005;37:902-904.
4. Soderquist B, Berglund C, Stralin K. CAP and bacteremia caused by an unusual methicillin-resistant Staphylococcus aureus (MRSA) strain with sequence type 36, staphylococcal cassette chromosome mec type IV and Panton-Valentine leukocidin genes. Eur J Clin Microbiol Infec Dis. 2006;25:604-606.
5. Mizell KN, Patterson KV, Carter JE. Empyema necessitatis due to methicillin-resistant Staphylococcus aureus: case report and review of the literature. J Clin Microbiol. 2008;46:3534-3536.
6. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for CAP: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
7. Martino JL, McMillian WD, Polish LB, et al. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Resp Med. 2008;102:932-943.
CORRESPONDENCE Jeffrey D. Schlaudecker, MD, The Christ Hospital/University of Cincinnati, Family Medicine Residency, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; schlaj@fammed.uc.edu
CASE: A 26-year-old woman came to our emergency department with shortness of breath—a symptom that had begun 2 weeks earlier and was getting steadily worse. She had a history of severe, persistent asthma, and had been admitted to the ICU—but not intubated—9 months earlier. Now, she reported dyspnea with even mild exertion, which inhalers failed to relieve.
The patient also had a cough and had recently begun producing thick, green sputum, but said she’d had no chest pain, fever, or lower extremity swelling. The young woman lived with her parents, both of whom smoked heavily, but denied tobacco or alcohol use herself. She had not taken antibiotics in the past 6 months.
On physical examination, the patient was afebrile, mildly tachypneic, and had a heart rate of 125 bpm. She was saturating 80% on ambient air and 95% on 2 liters per minute via nasal cannula; her lung exam was significant for diffuse wheezes and rhonchi, but the remainder of the physical exam was normal.
Lab tests revealed a white blood cell count of 25,200/mcL, with 81% neutrophils. Blood and urine cultures were preliminarily negative. We sent a sputum sample to be cultured and took chest x-rays. Posterior-anterior (PA) (FIGURE 1) and lateral (FIGURE 2) radiographs showed a dense right lower lobe inflltrate.
We diagnosed community-acquired pneumonia (CAP), coupled with an acute exacerbation of asthma, and admitted the patient to the hospital. We started her on intravenous (IV) moxifloxacin, parenteral steroids, and nebulized albuterol and ipratropium. But by the patient’s third day in the hospital, her white blood cell count had climbed to 34,500/mcL, and she still required oxygen by nasal cannula.
FIGURE 1 PA x-ray shows right lower lobe infiltrate
FIGURE 2 Dense infiltrate on lateral view
WHY DIDN’T THIS PATIENT RESPOND TO DRUG THERAPY?
CAP complicated by CA-MRSA
Initially, this appeared to be a rather straightforward case of CAP and asthma. The return of the sputum cultures on day 4, showing positive results for methicillin-resistant Staphylococcus aureus (MRSA), indicated that this was not the case. Sensitivity analysis revealed intermediate susceptibility to moxifloxacin and sensitivity to trimethoprim-sulfamethoxazole (TMP-SMX), vancomycin, and linezolid.
We switched the patient’s antibiotic from moxifloxacin to parenteral linezolid. She responded rapidly. On day 5, the patient was successfully weaned from O2 and converted to oral linezolid; the following day, she was discharged, with orders to complete an 8-day course of linezolid and an appointment with her family physician for the following week. At follow-up, she was doing well.
Cultures are crucial if results would alter Tx
In 2007, the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) published guidelines on the management of CAP1—a clinical diagnosis based on the presence of select features, including cough, fever, sputum production, and pleuritic chest pain. (Imaging of the chest may be used to support the diagnosis, but is not required.)
Following a site-of-care decision, ideally made with the help of a severity-of-illness scoring system such as the CURB-65 (Confusion, Urea nitrogen, Respiratory rate, Blood pressure, 65 years of age and older) or Pneumonia Severity Index, the guidelines recommend cultures whenever the result is likely to significantly alter standard empiric treatment.1
Pretreatment blood samples for culture should be obtained (strength of recommendation: A, well-conducted randomized controlled trials). The IDSA/ATS CAP guidelines also recommend an expectorated sputum sample for stain and culture for patients admitted to the ICU, as well as for those with a presentation suggestive of CAP who:
- have failed outpatient treatment;
- abuse alcohol;
- have severe structural or obstructive lung disease;
- or have pleural effusion.1
In our patient’s case, we obtained a sputum culture on admission because of her severe asthma. She was persistently hypoxic during her initial days in the hospital, and when the sputum culture returned positive for MRSA, her regimen of antibiotics was adjusted.
Suspect CA-MRSA when CAP is severe
Although MRSA has traditionally been thought of as a nosocomial pathogen, infections caused by distinct CA-MRSA strains are on the rise. An estimated 1% to 10% of CAP cases are caused by S aureus, but the percentage of those strains that are resistant to methicillin is not known.2
Clinical risk factors for S aureus CAP include end-stage renal disease, injection drug use, prior influenza, and prior antibiotic therapy, especially with fluoroquinolones.1 How-ever, CA-MRSA CAP often affects children and healthy young adults without any risk factors.3,4
Additionally, CAP that is caused by CA-MRSA is typically severe, often involving empyema, acute respiratory distress syndrome (ARDS), cavitary pneumonia, or severe sepsis.5 Consider a diagnosis of CA-MRSA CAP in patients who present with cavitary infiltrates without risk factors for anaerobic aspiration, such as syncope, seizures, alcohol abuse, or esophageal motility disorders.1
Start treatment without delay in patients at risk
Standard empiric treatment options for hospitalized patients with CAP (with the exception of those in the ICU) include either a beta-lactam and azithromycin or a respiratory fluoroquinolone (neither of which is active against MRSA).1 All patients who are hospitalized for CAP should be started on this regimen without delay. If gram-positive cocci in clusters suggestive of S aureus are isolated from sputum, this standard empiric regimen should be adequate until further microbiologic identification is available.1 While most cases of S aureus CAP are not MRSA, the increased mortality rate associated with inappropriate antibiotic selection led the IDSA/ATS to recommend broader empiric coverage for MRSA for patients with risk factors for S aureus.1
CA-MRSA strains are distinct from their nosocomial counterpart, and the optimal therapy for confirmed CA-MRSA CAP has not been determined. Frequently, CA-MRSA isolates are sensitive to TMP-SMX, clindamycin, and fluoroquinolones. But neither fluoroquinolones nor TMP-SMX have a clear effect on toxin production, and bacterial resistance frequently emerges during therapy with clindamycin.1
The IDSA/ATS guidelines recommend either vancomycin or linezolid for CAP due to CA-MRSA, and these are the most widely used drugs for invasive CA-MRSA infections. Linezolid has been recognized as having a theoretical advantage in treating pneumonia, as it achieves higher lung epithelial concentrations than vancomycin.6 Particularly in cases of necrotizing CA-MRSA pneumonia, vancomycin has not been found to decrease toxin production, and linezolid is therefore the preferred treatment.1 Because of the limitations of vancomycin, we chose linezolid for our patient.
Treatment duration is not evidence-based
Although most patients with CAP are treated for 7 to 10 days, there are few well-designed studies evaluating the optimal time frame. Guidelines for the duration of antibiotics for CAP recommend a minimum of 5 days of therapy, presuming the patient is clinically stable.1,7 Short-duration therapy for patients with bacteremic S aureus CAP infection has been associated with an increased risk of endocarditis, and the presence of pulmonary cavities may warrant prolonged therapy.1 Our patient had an isolate of S aureus with intermediate susceptibility to moxifloxacin, which likely explains her rapid response to linezolid. She remained on linezolid for 8 days.
• Consider CA-MRSA as a cause of CAP, especially in cases in which the presentation is severe, as the guidelines for empiric treatment of CAP feature antibiotics that are not active against the CA-MRSA pathogen.
• Order sputum cultures for all patients admitted to the ICU, as well as for patients with a clinical presentation suggestive of CAP who abuse alcohol, have severe asthma or other lung disease, or have a pleural effusion.
• Start patients with CA-MRSA CAP on linezolid without delay.
The author reported no potential conflict of interest relevant to this article.
CASE: A 26-year-old woman came to our emergency department with shortness of breath—a symptom that had begun 2 weeks earlier and was getting steadily worse. She had a history of severe, persistent asthma, and had been admitted to the ICU—but not intubated—9 months earlier. Now, she reported dyspnea with even mild exertion, which inhalers failed to relieve.
The patient also had a cough and had recently begun producing thick, green sputum, but said she’d had no chest pain, fever, or lower extremity swelling. The young woman lived with her parents, both of whom smoked heavily, but denied tobacco or alcohol use herself. She had not taken antibiotics in the past 6 months.
On physical examination, the patient was afebrile, mildly tachypneic, and had a heart rate of 125 bpm. She was saturating 80% on ambient air and 95% on 2 liters per minute via nasal cannula; her lung exam was significant for diffuse wheezes and rhonchi, but the remainder of the physical exam was normal.
Lab tests revealed a white blood cell count of 25,200/mcL, with 81% neutrophils. Blood and urine cultures were preliminarily negative. We sent a sputum sample to be cultured and took chest x-rays. Posterior-anterior (PA) (FIGURE 1) and lateral (FIGURE 2) radiographs showed a dense right lower lobe inflltrate.
We diagnosed community-acquired pneumonia (CAP), coupled with an acute exacerbation of asthma, and admitted the patient to the hospital. We started her on intravenous (IV) moxifloxacin, parenteral steroids, and nebulized albuterol and ipratropium. But by the patient’s third day in the hospital, her white blood cell count had climbed to 34,500/mcL, and she still required oxygen by nasal cannula.
FIGURE 1 PA x-ray shows right lower lobe infiltrate
FIGURE 2 Dense infiltrate on lateral view
WHY DIDN’T THIS PATIENT RESPOND TO DRUG THERAPY?
CAP complicated by CA-MRSA
Initially, this appeared to be a rather straightforward case of CAP and asthma. The return of the sputum cultures on day 4, showing positive results for methicillin-resistant Staphylococcus aureus (MRSA), indicated that this was not the case. Sensitivity analysis revealed intermediate susceptibility to moxifloxacin and sensitivity to trimethoprim-sulfamethoxazole (TMP-SMX), vancomycin, and linezolid.
We switched the patient’s antibiotic from moxifloxacin to parenteral linezolid. She responded rapidly. On day 5, the patient was successfully weaned from O2 and converted to oral linezolid; the following day, she was discharged, with orders to complete an 8-day course of linezolid and an appointment with her family physician for the following week. At follow-up, she was doing well.
Cultures are crucial if results would alter Tx
In 2007, the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) published guidelines on the management of CAP1—a clinical diagnosis based on the presence of select features, including cough, fever, sputum production, and pleuritic chest pain. (Imaging of the chest may be used to support the diagnosis, but is not required.)
Following a site-of-care decision, ideally made with the help of a severity-of-illness scoring system such as the CURB-65 (Confusion, Urea nitrogen, Respiratory rate, Blood pressure, 65 years of age and older) or Pneumonia Severity Index, the guidelines recommend cultures whenever the result is likely to significantly alter standard empiric treatment.1
Pretreatment blood samples for culture should be obtained (strength of recommendation: A, well-conducted randomized controlled trials). The IDSA/ATS CAP guidelines also recommend an expectorated sputum sample for stain and culture for patients admitted to the ICU, as well as for those with a presentation suggestive of CAP who:
- have failed outpatient treatment;
- abuse alcohol;
- have severe structural or obstructive lung disease;
- or have pleural effusion.1
In our patient’s case, we obtained a sputum culture on admission because of her severe asthma. She was persistently hypoxic during her initial days in the hospital, and when the sputum culture returned positive for MRSA, her regimen of antibiotics was adjusted.
Suspect CA-MRSA when CAP is severe
Although MRSA has traditionally been thought of as a nosocomial pathogen, infections caused by distinct CA-MRSA strains are on the rise. An estimated 1% to 10% of CAP cases are caused by S aureus, but the percentage of those strains that are resistant to methicillin is not known.2
Clinical risk factors for S aureus CAP include end-stage renal disease, injection drug use, prior influenza, and prior antibiotic therapy, especially with fluoroquinolones.1 How-ever, CA-MRSA CAP often affects children and healthy young adults without any risk factors.3,4
Additionally, CAP that is caused by CA-MRSA is typically severe, often involving empyema, acute respiratory distress syndrome (ARDS), cavitary pneumonia, or severe sepsis.5 Consider a diagnosis of CA-MRSA CAP in patients who present with cavitary infiltrates without risk factors for anaerobic aspiration, such as syncope, seizures, alcohol abuse, or esophageal motility disorders.1
Start treatment without delay in patients at risk
Standard empiric treatment options for hospitalized patients with CAP (with the exception of those in the ICU) include either a beta-lactam and azithromycin or a respiratory fluoroquinolone (neither of which is active against MRSA).1 All patients who are hospitalized for CAP should be started on this regimen without delay. If gram-positive cocci in clusters suggestive of S aureus are isolated from sputum, this standard empiric regimen should be adequate until further microbiologic identification is available.1 While most cases of S aureus CAP are not MRSA, the increased mortality rate associated with inappropriate antibiotic selection led the IDSA/ATS to recommend broader empiric coverage for MRSA for patients with risk factors for S aureus.1
CA-MRSA strains are distinct from their nosocomial counterpart, and the optimal therapy for confirmed CA-MRSA CAP has not been determined. Frequently, CA-MRSA isolates are sensitive to TMP-SMX, clindamycin, and fluoroquinolones. But neither fluoroquinolones nor TMP-SMX have a clear effect on toxin production, and bacterial resistance frequently emerges during therapy with clindamycin.1
The IDSA/ATS guidelines recommend either vancomycin or linezolid for CAP due to CA-MRSA, and these are the most widely used drugs for invasive CA-MRSA infections. Linezolid has been recognized as having a theoretical advantage in treating pneumonia, as it achieves higher lung epithelial concentrations than vancomycin.6 Particularly in cases of necrotizing CA-MRSA pneumonia, vancomycin has not been found to decrease toxin production, and linezolid is therefore the preferred treatment.1 Because of the limitations of vancomycin, we chose linezolid for our patient.
Treatment duration is not evidence-based
Although most patients with CAP are treated for 7 to 10 days, there are few well-designed studies evaluating the optimal time frame. Guidelines for the duration of antibiotics for CAP recommend a minimum of 5 days of therapy, presuming the patient is clinically stable.1,7 Short-duration therapy for patients with bacteremic S aureus CAP infection has been associated with an increased risk of endocarditis, and the presence of pulmonary cavities may warrant prolonged therapy.1 Our patient had an isolate of S aureus with intermediate susceptibility to moxifloxacin, which likely explains her rapid response to linezolid. She remained on linezolid for 8 days.
• Consider CA-MRSA as a cause of CAP, especially in cases in which the presentation is severe, as the guidelines for empiric treatment of CAP feature antibiotics that are not active against the CA-MRSA pathogen.
• Order sputum cultures for all patients admitted to the ICU, as well as for patients with a clinical presentation suggestive of CAP who abuse alcohol, have severe asthma or other lung disease, or have a pleural effusion.
• Start patients with CA-MRSA CAP on linezolid without delay.
The author reported no potential conflict of interest relevant to this article.
1. Mandell LA, Wunderink RG, Anzueto A, et al. IDSA/ATS Guidelines for CAP in adults. Clin Infect Dis. 2007;44(suppl 2):S27-S72.
2. Hidron AI, Low CE, Honig EG, et al. Emergence of community-acquired methicillin-resistant Staphylococcus aureus strain USA300 as a cause of necrotizing community-onset pneumonia. Lancet Infect Dis. 2009;9:384-392.
3. Torell E, Molin D, Tano E, et al. CAP and bacteraemia in a healthy young woman caused by methicillin-resistant Staphylococcus aureus (MRSA) carrying the genes encoding Panton-Valentine leukocidin (PVL). Scandinavian J Inf Dis. 2005;37:902-904.
4. Soderquist B, Berglund C, Stralin K. CAP and bacteremia caused by an unusual methicillin-resistant Staphylococcus aureus (MRSA) strain with sequence type 36, staphylococcal cassette chromosome mec type IV and Panton-Valentine leukocidin genes. Eur J Clin Microbiol Infec Dis. 2006;25:604-606.
5. Mizell KN, Patterson KV, Carter JE. Empyema necessitatis due to methicillin-resistant Staphylococcus aureus: case report and review of the literature. J Clin Microbiol. 2008;46:3534-3536.
6. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for CAP: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
7. Martino JL, McMillian WD, Polish LB, et al. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Resp Med. 2008;102:932-943.
CORRESPONDENCE Jeffrey D. Schlaudecker, MD, The Christ Hospital/University of Cincinnati, Family Medicine Residency, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; schlaj@fammed.uc.edu
1. Mandell LA, Wunderink RG, Anzueto A, et al. IDSA/ATS Guidelines for CAP in adults. Clin Infect Dis. 2007;44(suppl 2):S27-S72.
2. Hidron AI, Low CE, Honig EG, et al. Emergence of community-acquired methicillin-resistant Staphylococcus aureus strain USA300 as a cause of necrotizing community-onset pneumonia. Lancet Infect Dis. 2009;9:384-392.
3. Torell E, Molin D, Tano E, et al. CAP and bacteraemia in a healthy young woman caused by methicillin-resistant Staphylococcus aureus (MRSA) carrying the genes encoding Panton-Valentine leukocidin (PVL). Scandinavian J Inf Dis. 2005;37:902-904.
4. Soderquist B, Berglund C, Stralin K. CAP and bacteremia caused by an unusual methicillin-resistant Staphylococcus aureus (MRSA) strain with sequence type 36, staphylococcal cassette chromosome mec type IV and Panton-Valentine leukocidin genes. Eur J Clin Microbiol Infec Dis. 2006;25:604-606.
5. Mizell KN, Patterson KV, Carter JE. Empyema necessitatis due to methicillin-resistant Staphylococcus aureus: case report and review of the literature. J Clin Microbiol. 2008;46:3534-3536.
6. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for CAP: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
7. Martino JL, McMillian WD, Polish LB, et al. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Resp Med. 2008;102:932-943.
CORRESPONDENCE Jeffrey D. Schlaudecker, MD, The Christ Hospital/University of Cincinnati, Family Medicine Residency, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; schlaj@fammed.uc.edu
Hospital-Acquired and Community-Acquired MRSA: Two Distinct Infections
Cocaine-Associated Chest Pain
Darkening of Tongue Surface
Spondylodiscitis After Vertebral Fracture in the Thoracic Spine
Traumatic Thoracic Spondyloptosis Without Neurologic Deficit, and Treatment With In Situ Fusion
Clinical Use of Porous Tantalum in Complex Primary Total Knee Arthroplasty
Closed Reduction of a Dislocated Total Hip Athroplasty With a Constrained Acetabular Component
Failure to thrive
A 13-month-old girl arrives at your clinic, referred by the staff at the Women, Infants, and Children (WIC) nutritional center where her parents—recent immigrants from Africa—go for food supplements. The baby is bundled up in layers of clothing, even though it’s a relatively mild winter day. The father carries her into the examining room and undresses her. The child is tiny and dark-skinned, with curly hair painstakingly divided into little bunches. The parents seem caring, loving, and not particularly worried. They tell you the nurse at the WIC center thought their baby was not gaining enough weight and advised them to bring the baby to you. The referral note from WIC says hemoglobin levels found on routine blood test were low. You list the presenting complaint as anemia.
Q: What are some of the etiologies for anemia in a child this age? What strategies would you use to narrow down the cause?
Additional medical history
- The birth history is unremarkable, with neither antepartum nor postpartum complications.
- At her 6-month well-child checkup, neither the child’s physician nor her parents expressed any concerns about her development. Her parents received the routine anticipatory guidance at that visit, including advice on breastfeeding, vitamin supplementation, vaccination, and care of minor illnesses.
- She hasn’t been in for a well-child visit since then, but she has been seen for an upper respiratory infection and a bout of gastroenteritis. Her parents have not been worried about her health.
- The parents tell you the baby doesn’t sleep soundly, scratches her skin in her sleep, and cries a lot.
Family and social history
- The parents speak very little English.
- The patient is an only child, and no extended family live in the area.
- Her mother works nights and her father works days, with the parent who is not working caring for her at home.
- Her parents tell you she takes small sips of juice or water, and an occasional bite of noodles. She won’t drink milk at all and refuses any other foods they offer.
Physical examination
- The child is in no acute distress. She is afebrile, and her vital signs are appropriate for her age.
- Height is 27½ inches, weight 15 lb, 15 oz, placing her at less than the 5th percentile for height and weight for her age—a regression from the 50th percentile she showed at earlier visits.
- Head and neck exam reveals mild frontal bossing and prominent sternoclavicular joints. There is no adenopathy or thyromegaly.
- Heart and lung exam are normal.
- Abdomen is soft, nontender, nondistended, with bowel sounds present.
- There is slight bowing of the lower extremities and puffiness around the wrists and ankles. When you ask her father to have her stand on the examining table, you see that she needs support to do so (FIGURE 1).
Q: What is your clinical diagnosis, and what tests will you order?
FIGURE 1
The patient, not weight-bearing
The 13-month-old patient has slight bowing of the lower extremities and puffiness around the wrists and ankles. She needs support to stand.
Laboratory results
- Hemoglobin, 9.9 mg/dL
(normal: 10.4-12.4 mg/dL) - Mean corpuscular volume (MCV), 74 fL
(normal: 70-86 fL) - Alkaline phosphatase, 3417 U/L
(normal: 115-460 U/L) - Vitamin D (calcidiol), <7 nmol/L
(normal: 60-108 nmol/L) - Calcium, 9.1 mg/dL
(normal: 8.8-10.8 mg/dL) - Comprehensive metabolic panel, liver transaminases, and thyroid-stimulating hormone levels are all normal
- Parathyroid hormone level, 101 pg/mL
(normal: 10-55 pg/mL).
Radiologic findings
- X-ray shows slight saber deformity of the femurs and broadening of the epiphyses of the forearm (FIGURE 2).
FIGURE 2
Forearm x-ray
The patient’s x-ray shows a widening of the epiphyses (black arrow) and pseudofracture (white arrow).
Can this be rickets?
Here is a child with a history of poor growth and peculiar eating habits. Her legs are bowed and her wrists seem swollen. She does not stand or walk, and refuses to bear weight on her legs. She is anemic, and the lab tests you’ve ordered show abnormal vitamin D, alkaline phosphatase, and parathyroid hormone levels. All of this suggests a diagnosis of rickets.
Causes of rickets
Rickets is the result of abnormal mineralization of bone and cartilage in growing children. The analogous condition in adults whose epiphyseal plates have closed is osteomalacia. Clinical rickets typically presents with the constellation of signs and symptoms listed in the box and depicted in FIGURES 1, 2, and 3.
Clinical findings
- Apathy, listlessness, and poor growth
- Muscle cramps, weakness, hypotonia, numbness, paresthesias, tetany, and seizures
- Pot belly and waddling gait
- Soft, misshapen head with widened sutures and frontal bossing
- Delayed eruption of teeth
- Rachitic rosary (see below)
- Harrison’s groove (indentation at point of insertion of diaphragm, due to the pull of the diaphragm against the softened lower ribs)
- Bowed limbs and swollen joints
Radiologic findings
- Epiphyses widened and flared with irregular, “cupped” epiphyseal-metaphyseal junctions; involvement of the costrochondral junctions produces a row of beadlike prominences often called the “rachitic rosary”
- Long bones bowed (“saber shaped”), with indistinct cortices
- Pseudofractures (also called Looser’s zone or Milkman’s fractures), often found on the concave side of femoral neck, pubic rami, ribs, clavicles, and lateral aspect of scapulae
- Pathologic fractures
Laboratory findings
- Creatinine: Normal value excludes renal insufficiency as etiology
- Liver enzymes: Normal value excludes liver disease as etiology
- Phosphorus: Normal phosphorus and parathyroid hormone make a diagnosis of rickets unlikely
- Parathyroid hormone: Elevated in hypocalcemic rickets (>55 pg/mL)
- Calcium, total and ionized with albumin: May be normal in rickets
- Alkaline phosphatase: Usually markedly increased over the age-specific reference range in rickets
- Urinary calcium level: Usually decreased in rickets (<50 mg/d, depending on calcium content of diet)
- Calcidiol level: May be low in rickets (<50 nmol/L [20 ng/mL])
- Calcitriol level: Usually normal in rickets, because of its short-half life (60-108 nmol/L [25-45 pg/mL])
FIGURE 3
Rachitic rosary
The patient had a developing rosary, most pronounced at the sternoclavicular joint (white arrow) and early saber deformity of the shin (black arrows). Frontal bossing and swollen wrists and ankles may also be seen in patients with rickets.
Not enough vitamin D
The most common cause of rickets is a deficiency of vitamin D, a substance physiologically necessary to produce concentrations of calcium and phosphate adequate for proper bone mineralization. Vitamin D is produced in the skin in the presence of sunlight and can also be ingested in supplements and certain foods.
Vitamin D deficiency may result from reduced sunlight exposure, inadequate dietary intake, malabsorption, or a combination of these factors.1 Rickets may also be caused by medications that alter absorption or secretion of phosphate and calcium, including antacids, anticonvulsants, corticosteroids, and loop diuretics. Various disease states, such as Crohn’s disease, pancreatic disease, biliary disease, gastrointestinal loops and fistulae, cirrhosis, chronic renal disease, and mesenchymal tumors, may also alter absorption and metabolism of these ions.
How much sunshine does a baby need?
It doesn’t take a great deal of sunlight exposure to provide adequate supplies of vitamin D. An infant wearing only a diaper will get enough vitamin D from half an hour per week of sun exposure. A fully clothed infant needs 3 hours. But children with dark skin, like this African baby, need more time in the sun. And if parents follow current anticipatory guidance about protecting children from overexposure to the sun and slather on the sunscreen, vitamin D synthesis decreases by more than 95%.2
Vitamin D in the diet
Consuming adequate quantities of vitamin D is difficult, unless the diet includes fortified foods or vitamin supplements. Current recommendations for daily intake are 400 IU per day for all infants, children, and adolescents.3 But the average daily intake by adults in North America from sources such as fish, eggs, and butter or margarine is only 50 to 100 IU.3
Infants born to vitamin-D replete women have an 8- to 12-week store of vitamin D at birth, but breastfeeding does not ensure the baby is getting adequate amounts of vitamin D, even if the mother’s vitamin D status is adequate. Human milk from vitamin D-replete women has a vitamin D concentration of only 25 IU per liter, far below the recommended daily intake of 400 IU.3
How deficient is this baby?
Vitamin D deficiency may be categorized as mild, moderate, or severe. Calcidiol is the next-to-last step in the metabolism of vitamin D and is used as a marker because it is easier to measure than the concentration of calcitriol, the final step. Mild vitamin D deficiency is defined as serum calcidiol concentration of 25 to 50 nmol/L. A serum calcidiol concentration of 12.5 to 25 nmol/L indicates a moderate vitamin D deficiency, and at those levels the incidence of hypocalcemia and rickets increases. Serum calcidiol concentration of less than 12.5 nmol/L, as in the case of the patient presented here, indicates a severe deficiency.4
Not enough calcium
In addition to calcium malabsorption due to inadequate vitamin D levels, hypocalcemia may result from inadequate intake of calcium or from vitamin D-dependent metabolic disorders, of which there are 2 types.
Type I, sometimes known as pseudo-vitamin D-deficiency rickets, is due to defective production of 25(OH)D3-1-α-hydroxylase, an enzyme necessary for the conversion of calcidiol to calcitriol in the kidneys.
Type II, also called hereditary rickets, is rare. It is caused by mutations in vitamin D receptors and the inability of the ligand to bind or stimulate the proper physiologic response. In this condition, laboratory tests may show high levels of calcitriol.
Not enough phosphorus
Vitamin D-resistant rickets, or familial hypophosphatemic rickets, refers to a clinical presentation of rickets that is caused by a hereditary renal wasting of phosphorus at the proximal tubule level. Laboratory evaluation of a child with this condition will show low phosphate levels, normal calcitriol levels, and hypercalciuria. The specific defect that causes this condition is not known. A family history of short stature, orthopedic abnormalities, poor dentition, alopecia, or parental consanguinity may be suggestive of vitamin D-dependent or vitamin D-resistant forms of inherited rickets.
Other causes of hypophosphatemia include inadequate nutritional intake, X-linked hypophosphatemia, generalized tubular disorders such as renal tubular acidosis, Fanconi syndrome, and Dent disease. These disorders may also lead to rickets.
Q: What are the available treatments for rickets? What about prevention?
Replenishing vitamin D
Vitamin D deficiency may be remedied by supplementing anywhere along the metabolic pathway. Dihydrotachysterol (DHT, or D1), the substance in the skin that responds to sunlight, is given as 60,000 IU once, then 6000 IU daily until the rickets are clinically and radiologically resolved. Further downstream, ergocalciferol (D2) may be given as 1000 to 5000 IU daily for 6 to 12 weeks. The dosage is calibrated by age: 1000 IU/d if age <1 month, 3000 IU/d for ages 1 to 12 months, and 5000 IU/d for children older than 12 months. The final form of vitamin D is cholecalciferol (D3). This is typically administered as either 5000 to 10,000 IU daily for 2 to 3 months, or as 600,000 IU in 1 day, divided into 4 to 6 doses.5,6 All of these supplements taste bad and children are often resistant to swallowing them.
When follow-up and multiple dosing are impractical—because the family finds repeated clinic visits too difficult, or because the child will not comply with the regimen—you can use stosstherapy.7 This is a bolus of cholecalciferol (D3) or ergocalciferol (D2), 150,000 to 600,000 IU, given as a single dose or divided over several days. For example, you would give 300,000 IU over 1 to 7 days in children 1 to 12 months of age. With this therapy, onset of action is less than a day and maximal effects are seen in 4 weeks. Some preparations contain propylene glycol, which is limited in food additives to <25 mg/kg of body weight because of potential toxicity.
When supplementation doesn’t work. Vitamin D is not effective in treatment of familial hypophosphatemic rickets, Type II vitamin D-dependent rickets, or disorders of phosphate metabolism.
Monitoring therapeutic success
When possible, treatment should be monitored by checking serum calcium and alkaline phosphatase at 1 month, and calcium, magnesium, phosphate, alkaline phosphatase, calcidiol, parathyroid hormone, and wrist x-ray at 3 months from initiation of treatment, to ensure that they are normalizing.
Preventing rickets
In the developed world, public health efforts to prevent rickets have been largely successful. Rickets was prevalent worldwide in the early decades of the 20th century, but after milk began to be routinely fortified with vitamin D in the 1920s, cases of nutritional rickets almost disappeared in industrialized nations.
In 1963, the American Academy of Pediatrics (AAP) began recommending vitamin D supplementation to prevent rickets. Although the recommendation remains controversial because of concerns about the possibility of hypervitaminosis and the resultant hypercalcemia and hypercalciuria, there has been renewed emphasis on this recommendation in light of a rise in the number of cases of rickets in the United States in recent years.8-14 Current AAP recommendations for vitamin D supplementation are daily supplementation of 400 IU vitamin D for the following groups:3
- Breastfed infants, beginning with the first few days of life and continued until they are weaned to at least 1000 mL per day of vitamin D-fortified formula or milk.
- Nonbreastfed infants who are ingesting less than 1000 mL per day of vitamin D-fortified formula or milk. Most commercial baby formulas contain 400 IU/L, which means that an intake of 500 mL of formula per day provides 200 IU.15 Additionally, special milk supplemented with vitamin D3 up to 200 IU per 250 mL has recently become available in Europe.16
- Children and adolescents who do not get regular sunlight exposure, do not ingest at least 32 ounces per day of vitamin D-fortified milk, or do not take a daily multivitamin supplement containing at least 400 IU of vitamin D.
Others have suggested a bolus dosing 150,000 IU each autumn for those in northern climates.17
Most over-the-counter vitamin formulations now contain D3 (cholecalciferol), as recent studies show this form is more potent than D2 (ergocalciferol).18 Calcium supplements are available in combination with vitamin D. Calcitriol, the most active form of vitamin D, is available only by prescription. Because it does not require activation in the kidneys, it is the drug of choice for renally impaired patients.
Q: How would you treat this child?
Bad taste is a big hurdle
The child in this case was prescribed 150,000 U oral cholecalciferol. She spit it out at the clinic, and the dose was sent home for her parents to administer. She was also started on a multivitamin (Poly-Vi-Sol). On the return visit a few days later, the parents reported that she only took three-quarters of the vitamin D dose, spitting out the remainder.
When that didn’t work…
The child was then admitted to the hospital for administration of vitamin D and to allow for dietary and social work evaluations of factors contributing to her malnutrition.
Social services evaluation ruled out an economic etiology for the child’s failure to thrive. The family was able to afford a nutritionally adequate diet for the child. They were enrolled in Medicaid and WIC. Willful neglect was not an issue: A very loving and appropriate relationship was evident between the child and her parents. Child care was shared equally by the young parents, but they simply didn’t know what foods were appropriate for a child of her age.
Turning things around
The hospital dietician observed one of the child’s meals. The child ate some of everything on the plate: mashed potatoes and gravy, chicken strips, vegetables, bananas, yogurt, and milk. She was willing to try a variety of foods, and ate most of them. Both the physician and the dietician spent a lot of time with the parents reviewing feeding techniques and healthy food choices. Language was a problem, solved for the most part with the assistance of a dial-up language translation service to ensure clear understanding of the instructions. The health care professionals prepared a list of healthy foods to buy at the grocery store, with pictures illustrating healthy food items. In addition, appropriate exposure to sunlight was explained and encouraged.
Parent education is the key
The child’s father expressed gratitude several times for the instruction on healthy food choices for the daughter, while the mother smiled in shy agreement. He said they did not know what to feed her, and when she refused most things they offered, they fed her the noodles and juice she seemed to prefer. He was grateful to the nutritionist, social worker, nursing staff, and physicians for taking care of his daughter. He was eager to go to the grocery store and to start feeding her the “right foods.”
Ready to go home
By discharge, the child had received the full dose of vitamin D and was eating a variety of foods, including 1 to 4 ounces of milk daily, supplemented with Poly-Vi-Sol, 1 mL orally twice daily, and calcium carbonate (OsCal) with vitamin D, 1 crushed tablet orally twice daily. Home health nursing provided follow-up twice a week, and weekly appointments in the clinic with the physician were also scheduled. Compliance with the discharge plan was impeccable. Both laboratory and clinical signs of rickets resolved over the subsequent weeks.
1. Thacher TD. Determining the nutritional cause of rickets in children. Am Fam Physician. 2007;75:470, 472.-
2. Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79:362-371.
3. Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142-1152.
4. Stroud ML, Stilgoe S, Stott VE, et al. Vitamin D-A review. Aust Fam Physician. 2008;37:1002-1005.
5. Misra M, Pacaud D, Petryk A, et al. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398-417.
6. Shah BR, Finberg L. Single-day therapy for nutritional vitamin D-deficiency rickets: a preferred method. J Pediatr. 1994;125:487-490.
7. Cesur Y, Caksen H, Gundem A, et al. Comparison of low and high dose of vitamin D treatment in nutritional vitamin D deficiency rickets. J Pediatr Endocrinol Metab. 2003;16:1105-1109.
8. Centers for Disease Control and Prevention. Severe malnutrition among young children—Georgia, January 1997-June 1999. MMWR Morb Mortal Wkly Rep. 2001;50:224-227.
9. Rajakumar K, Thomas SB. Reemerging nutritional rickets: a historical perspective. Arch Pediatr Adolesc Med. 2005;159:335-341.
10. Tomashek KM, Nesby S, Scanlon KS, et al. Nutritional rickets in Georgia. Pediatrics. 2001;107:E45.-
11. Weisberg P, Scanlon KS, Li R, et al. Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004;80(suppl 6):S1697-S1705S.
12. Alouf B, Grigalonis M. Incidental finding of vitamin-D deficient rickets in an otherwise healthy infant—a reappraisal of current vitamin-D supplementation guidelines. J Natl Med Assoc. 2005;97:1170-1173.
13. Nield LS, Mahajan P, Joshi A, et al. Rickets: not a disease of the past. Am Fam Physician. 2006;74:619-626.
14. Wagner C. Rickets: emerging from obscurity. Am Fam Physician. 2006;74:561-562.
15. Calvo MS, Whiting SJ, Barton CN. Vitamin D fortification in the United States and Canada: current status and data needs. Am J Clin Nutr. 2004;80(suppl 6):S1710-S1716.
16. Avonmore Super Milk. Glanbia Consumer Foods, Dublin, Ireland. Available at: www.sendmorefamilies.com/super-milk.aspx. Accessed August 23, 2009.
17. Oliveri B, Cassinelli H, Mautalen C, et al. Vitamin D prophylaxis in children with a single dose of 150,000 IU of vitamin D. Eur J Clin Nutr. 1996;50:807-810.
18. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab. 2004;89:5387-5391.
Correspondence Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; mark.huntington@usd.edu
A 13-month-old girl arrives at your clinic, referred by the staff at the Women, Infants, and Children (WIC) nutritional center where her parents—recent immigrants from Africa—go for food supplements. The baby is bundled up in layers of clothing, even though it’s a relatively mild winter day. The father carries her into the examining room and undresses her. The child is tiny and dark-skinned, with curly hair painstakingly divided into little bunches. The parents seem caring, loving, and not particularly worried. They tell you the nurse at the WIC center thought their baby was not gaining enough weight and advised them to bring the baby to you. The referral note from WIC says hemoglobin levels found on routine blood test were low. You list the presenting complaint as anemia.
Q: What are some of the etiologies for anemia in a child this age? What strategies would you use to narrow down the cause?
Additional medical history
- The birth history is unremarkable, with neither antepartum nor postpartum complications.
- At her 6-month well-child checkup, neither the child’s physician nor her parents expressed any concerns about her development. Her parents received the routine anticipatory guidance at that visit, including advice on breastfeeding, vitamin supplementation, vaccination, and care of minor illnesses.
- She hasn’t been in for a well-child visit since then, but she has been seen for an upper respiratory infection and a bout of gastroenteritis. Her parents have not been worried about her health.
- The parents tell you the baby doesn’t sleep soundly, scratches her skin in her sleep, and cries a lot.
Family and social history
- The parents speak very little English.
- The patient is an only child, and no extended family live in the area.
- Her mother works nights and her father works days, with the parent who is not working caring for her at home.
- Her parents tell you she takes small sips of juice or water, and an occasional bite of noodles. She won’t drink milk at all and refuses any other foods they offer.
Physical examination
- The child is in no acute distress. She is afebrile, and her vital signs are appropriate for her age.
- Height is 27½ inches, weight 15 lb, 15 oz, placing her at less than the 5th percentile for height and weight for her age—a regression from the 50th percentile she showed at earlier visits.
- Head and neck exam reveals mild frontal bossing and prominent sternoclavicular joints. There is no adenopathy or thyromegaly.
- Heart and lung exam are normal.
- Abdomen is soft, nontender, nondistended, with bowel sounds present.
- There is slight bowing of the lower extremities and puffiness around the wrists and ankles. When you ask her father to have her stand on the examining table, you see that she needs support to do so (FIGURE 1).
Q: What is your clinical diagnosis, and what tests will you order?
FIGURE 1
The patient, not weight-bearing
The 13-month-old patient has slight bowing of the lower extremities and puffiness around the wrists and ankles. She needs support to stand.
Laboratory results
- Hemoglobin, 9.9 mg/dL
(normal: 10.4-12.4 mg/dL) - Mean corpuscular volume (MCV), 74 fL
(normal: 70-86 fL) - Alkaline phosphatase, 3417 U/L
(normal: 115-460 U/L) - Vitamin D (calcidiol), <7 nmol/L
(normal: 60-108 nmol/L) - Calcium, 9.1 mg/dL
(normal: 8.8-10.8 mg/dL) - Comprehensive metabolic panel, liver transaminases, and thyroid-stimulating hormone levels are all normal
- Parathyroid hormone level, 101 pg/mL
(normal: 10-55 pg/mL).
Radiologic findings
- X-ray shows slight saber deformity of the femurs and broadening of the epiphyses of the forearm (FIGURE 2).
FIGURE 2
Forearm x-ray
The patient’s x-ray shows a widening of the epiphyses (black arrow) and pseudofracture (white arrow).
Can this be rickets?
Here is a child with a history of poor growth and peculiar eating habits. Her legs are bowed and her wrists seem swollen. She does not stand or walk, and refuses to bear weight on her legs. She is anemic, and the lab tests you’ve ordered show abnormal vitamin D, alkaline phosphatase, and parathyroid hormone levels. All of this suggests a diagnosis of rickets.
Causes of rickets
Rickets is the result of abnormal mineralization of bone and cartilage in growing children. The analogous condition in adults whose epiphyseal plates have closed is osteomalacia. Clinical rickets typically presents with the constellation of signs and symptoms listed in the box and depicted in FIGURES 1, 2, and 3.
Clinical findings
- Apathy, listlessness, and poor growth
- Muscle cramps, weakness, hypotonia, numbness, paresthesias, tetany, and seizures
- Pot belly and waddling gait
- Soft, misshapen head with widened sutures and frontal bossing
- Delayed eruption of teeth
- Rachitic rosary (see below)
- Harrison’s groove (indentation at point of insertion of diaphragm, due to the pull of the diaphragm against the softened lower ribs)
- Bowed limbs and swollen joints
Radiologic findings
- Epiphyses widened and flared with irregular, “cupped” epiphyseal-metaphyseal junctions; involvement of the costrochondral junctions produces a row of beadlike prominences often called the “rachitic rosary”
- Long bones bowed (“saber shaped”), with indistinct cortices
- Pseudofractures (also called Looser’s zone or Milkman’s fractures), often found on the concave side of femoral neck, pubic rami, ribs, clavicles, and lateral aspect of scapulae
- Pathologic fractures
Laboratory findings
- Creatinine: Normal value excludes renal insufficiency as etiology
- Liver enzymes: Normal value excludes liver disease as etiology
- Phosphorus: Normal phosphorus and parathyroid hormone make a diagnosis of rickets unlikely
- Parathyroid hormone: Elevated in hypocalcemic rickets (>55 pg/mL)
- Calcium, total and ionized with albumin: May be normal in rickets
- Alkaline phosphatase: Usually markedly increased over the age-specific reference range in rickets
- Urinary calcium level: Usually decreased in rickets (<50 mg/d, depending on calcium content of diet)
- Calcidiol level: May be low in rickets (<50 nmol/L [20 ng/mL])
- Calcitriol level: Usually normal in rickets, because of its short-half life (60-108 nmol/L [25-45 pg/mL])
FIGURE 3
Rachitic rosary
The patient had a developing rosary, most pronounced at the sternoclavicular joint (white arrow) and early saber deformity of the shin (black arrows). Frontal bossing and swollen wrists and ankles may also be seen in patients with rickets.
Not enough vitamin D
The most common cause of rickets is a deficiency of vitamin D, a substance physiologically necessary to produce concentrations of calcium and phosphate adequate for proper bone mineralization. Vitamin D is produced in the skin in the presence of sunlight and can also be ingested in supplements and certain foods.
Vitamin D deficiency may result from reduced sunlight exposure, inadequate dietary intake, malabsorption, or a combination of these factors.1 Rickets may also be caused by medications that alter absorption or secretion of phosphate and calcium, including antacids, anticonvulsants, corticosteroids, and loop diuretics. Various disease states, such as Crohn’s disease, pancreatic disease, biliary disease, gastrointestinal loops and fistulae, cirrhosis, chronic renal disease, and mesenchymal tumors, may also alter absorption and metabolism of these ions.
How much sunshine does a baby need?
It doesn’t take a great deal of sunlight exposure to provide adequate supplies of vitamin D. An infant wearing only a diaper will get enough vitamin D from half an hour per week of sun exposure. A fully clothed infant needs 3 hours. But children with dark skin, like this African baby, need more time in the sun. And if parents follow current anticipatory guidance about protecting children from overexposure to the sun and slather on the sunscreen, vitamin D synthesis decreases by more than 95%.2
Vitamin D in the diet
Consuming adequate quantities of vitamin D is difficult, unless the diet includes fortified foods or vitamin supplements. Current recommendations for daily intake are 400 IU per day for all infants, children, and adolescents.3 But the average daily intake by adults in North America from sources such as fish, eggs, and butter or margarine is only 50 to 100 IU.3
Infants born to vitamin-D replete women have an 8- to 12-week store of vitamin D at birth, but breastfeeding does not ensure the baby is getting adequate amounts of vitamin D, even if the mother’s vitamin D status is adequate. Human milk from vitamin D-replete women has a vitamin D concentration of only 25 IU per liter, far below the recommended daily intake of 400 IU.3
How deficient is this baby?
Vitamin D deficiency may be categorized as mild, moderate, or severe. Calcidiol is the next-to-last step in the metabolism of vitamin D and is used as a marker because it is easier to measure than the concentration of calcitriol, the final step. Mild vitamin D deficiency is defined as serum calcidiol concentration of 25 to 50 nmol/L. A serum calcidiol concentration of 12.5 to 25 nmol/L indicates a moderate vitamin D deficiency, and at those levels the incidence of hypocalcemia and rickets increases. Serum calcidiol concentration of less than 12.5 nmol/L, as in the case of the patient presented here, indicates a severe deficiency.4
Not enough calcium
In addition to calcium malabsorption due to inadequate vitamin D levels, hypocalcemia may result from inadequate intake of calcium or from vitamin D-dependent metabolic disorders, of which there are 2 types.
Type I, sometimes known as pseudo-vitamin D-deficiency rickets, is due to defective production of 25(OH)D3-1-α-hydroxylase, an enzyme necessary for the conversion of calcidiol to calcitriol in the kidneys.
Type II, also called hereditary rickets, is rare. It is caused by mutations in vitamin D receptors and the inability of the ligand to bind or stimulate the proper physiologic response. In this condition, laboratory tests may show high levels of calcitriol.
Not enough phosphorus
Vitamin D-resistant rickets, or familial hypophosphatemic rickets, refers to a clinical presentation of rickets that is caused by a hereditary renal wasting of phosphorus at the proximal tubule level. Laboratory evaluation of a child with this condition will show low phosphate levels, normal calcitriol levels, and hypercalciuria. The specific defect that causes this condition is not known. A family history of short stature, orthopedic abnormalities, poor dentition, alopecia, or parental consanguinity may be suggestive of vitamin D-dependent or vitamin D-resistant forms of inherited rickets.
Other causes of hypophosphatemia include inadequate nutritional intake, X-linked hypophosphatemia, generalized tubular disorders such as renal tubular acidosis, Fanconi syndrome, and Dent disease. These disorders may also lead to rickets.
Q: What are the available treatments for rickets? What about prevention?
Replenishing vitamin D
Vitamin D deficiency may be remedied by supplementing anywhere along the metabolic pathway. Dihydrotachysterol (DHT, or D1), the substance in the skin that responds to sunlight, is given as 60,000 IU once, then 6000 IU daily until the rickets are clinically and radiologically resolved. Further downstream, ergocalciferol (D2) may be given as 1000 to 5000 IU daily for 6 to 12 weeks. The dosage is calibrated by age: 1000 IU/d if age <1 month, 3000 IU/d for ages 1 to 12 months, and 5000 IU/d for children older than 12 months. The final form of vitamin D is cholecalciferol (D3). This is typically administered as either 5000 to 10,000 IU daily for 2 to 3 months, or as 600,000 IU in 1 day, divided into 4 to 6 doses.5,6 All of these supplements taste bad and children are often resistant to swallowing them.
When follow-up and multiple dosing are impractical—because the family finds repeated clinic visits too difficult, or because the child will not comply with the regimen—you can use stosstherapy.7 This is a bolus of cholecalciferol (D3) or ergocalciferol (D2), 150,000 to 600,000 IU, given as a single dose or divided over several days. For example, you would give 300,000 IU over 1 to 7 days in children 1 to 12 months of age. With this therapy, onset of action is less than a day and maximal effects are seen in 4 weeks. Some preparations contain propylene glycol, which is limited in food additives to <25 mg/kg of body weight because of potential toxicity.
When supplementation doesn’t work. Vitamin D is not effective in treatment of familial hypophosphatemic rickets, Type II vitamin D-dependent rickets, or disorders of phosphate metabolism.
Monitoring therapeutic success
When possible, treatment should be monitored by checking serum calcium and alkaline phosphatase at 1 month, and calcium, magnesium, phosphate, alkaline phosphatase, calcidiol, parathyroid hormone, and wrist x-ray at 3 months from initiation of treatment, to ensure that they are normalizing.
Preventing rickets
In the developed world, public health efforts to prevent rickets have been largely successful. Rickets was prevalent worldwide in the early decades of the 20th century, but after milk began to be routinely fortified with vitamin D in the 1920s, cases of nutritional rickets almost disappeared in industrialized nations.
In 1963, the American Academy of Pediatrics (AAP) began recommending vitamin D supplementation to prevent rickets. Although the recommendation remains controversial because of concerns about the possibility of hypervitaminosis and the resultant hypercalcemia and hypercalciuria, there has been renewed emphasis on this recommendation in light of a rise in the number of cases of rickets in the United States in recent years.8-14 Current AAP recommendations for vitamin D supplementation are daily supplementation of 400 IU vitamin D for the following groups:3
- Breastfed infants, beginning with the first few days of life and continued until they are weaned to at least 1000 mL per day of vitamin D-fortified formula or milk.
- Nonbreastfed infants who are ingesting less than 1000 mL per day of vitamin D-fortified formula or milk. Most commercial baby formulas contain 400 IU/L, which means that an intake of 500 mL of formula per day provides 200 IU.15 Additionally, special milk supplemented with vitamin D3 up to 200 IU per 250 mL has recently become available in Europe.16
- Children and adolescents who do not get regular sunlight exposure, do not ingest at least 32 ounces per day of vitamin D-fortified milk, or do not take a daily multivitamin supplement containing at least 400 IU of vitamin D.
Others have suggested a bolus dosing 150,000 IU each autumn for those in northern climates.17
Most over-the-counter vitamin formulations now contain D3 (cholecalciferol), as recent studies show this form is more potent than D2 (ergocalciferol).18 Calcium supplements are available in combination with vitamin D. Calcitriol, the most active form of vitamin D, is available only by prescription. Because it does not require activation in the kidneys, it is the drug of choice for renally impaired patients.
Q: How would you treat this child?
Bad taste is a big hurdle
The child in this case was prescribed 150,000 U oral cholecalciferol. She spit it out at the clinic, and the dose was sent home for her parents to administer. She was also started on a multivitamin (Poly-Vi-Sol). On the return visit a few days later, the parents reported that she only took three-quarters of the vitamin D dose, spitting out the remainder.
When that didn’t work…
The child was then admitted to the hospital for administration of vitamin D and to allow for dietary and social work evaluations of factors contributing to her malnutrition.
Social services evaluation ruled out an economic etiology for the child’s failure to thrive. The family was able to afford a nutritionally adequate diet for the child. They were enrolled in Medicaid and WIC. Willful neglect was not an issue: A very loving and appropriate relationship was evident between the child and her parents. Child care was shared equally by the young parents, but they simply didn’t know what foods were appropriate for a child of her age.
Turning things around
The hospital dietician observed one of the child’s meals. The child ate some of everything on the plate: mashed potatoes and gravy, chicken strips, vegetables, bananas, yogurt, and milk. She was willing to try a variety of foods, and ate most of them. Both the physician and the dietician spent a lot of time with the parents reviewing feeding techniques and healthy food choices. Language was a problem, solved for the most part with the assistance of a dial-up language translation service to ensure clear understanding of the instructions. The health care professionals prepared a list of healthy foods to buy at the grocery store, with pictures illustrating healthy food items. In addition, appropriate exposure to sunlight was explained and encouraged.
Parent education is the key
The child’s father expressed gratitude several times for the instruction on healthy food choices for the daughter, while the mother smiled in shy agreement. He said they did not know what to feed her, and when she refused most things they offered, they fed her the noodles and juice she seemed to prefer. He was grateful to the nutritionist, social worker, nursing staff, and physicians for taking care of his daughter. He was eager to go to the grocery store and to start feeding her the “right foods.”
Ready to go home
By discharge, the child had received the full dose of vitamin D and was eating a variety of foods, including 1 to 4 ounces of milk daily, supplemented with Poly-Vi-Sol, 1 mL orally twice daily, and calcium carbonate (OsCal) with vitamin D, 1 crushed tablet orally twice daily. Home health nursing provided follow-up twice a week, and weekly appointments in the clinic with the physician were also scheduled. Compliance with the discharge plan was impeccable. Both laboratory and clinical signs of rickets resolved over the subsequent weeks.
A 13-month-old girl arrives at your clinic, referred by the staff at the Women, Infants, and Children (WIC) nutritional center where her parents—recent immigrants from Africa—go for food supplements. The baby is bundled up in layers of clothing, even though it’s a relatively mild winter day. The father carries her into the examining room and undresses her. The child is tiny and dark-skinned, with curly hair painstakingly divided into little bunches. The parents seem caring, loving, and not particularly worried. They tell you the nurse at the WIC center thought their baby was not gaining enough weight and advised them to bring the baby to you. The referral note from WIC says hemoglobin levels found on routine blood test were low. You list the presenting complaint as anemia.
Q: What are some of the etiologies for anemia in a child this age? What strategies would you use to narrow down the cause?
Additional medical history
- The birth history is unremarkable, with neither antepartum nor postpartum complications.
- At her 6-month well-child checkup, neither the child’s physician nor her parents expressed any concerns about her development. Her parents received the routine anticipatory guidance at that visit, including advice on breastfeeding, vitamin supplementation, vaccination, and care of minor illnesses.
- She hasn’t been in for a well-child visit since then, but she has been seen for an upper respiratory infection and a bout of gastroenteritis. Her parents have not been worried about her health.
- The parents tell you the baby doesn’t sleep soundly, scratches her skin in her sleep, and cries a lot.
Family and social history
- The parents speak very little English.
- The patient is an only child, and no extended family live in the area.
- Her mother works nights and her father works days, with the parent who is not working caring for her at home.
- Her parents tell you she takes small sips of juice or water, and an occasional bite of noodles. She won’t drink milk at all and refuses any other foods they offer.
Physical examination
- The child is in no acute distress. She is afebrile, and her vital signs are appropriate for her age.
- Height is 27½ inches, weight 15 lb, 15 oz, placing her at less than the 5th percentile for height and weight for her age—a regression from the 50th percentile she showed at earlier visits.
- Head and neck exam reveals mild frontal bossing and prominent sternoclavicular joints. There is no adenopathy or thyromegaly.
- Heart and lung exam are normal.
- Abdomen is soft, nontender, nondistended, with bowel sounds present.
- There is slight bowing of the lower extremities and puffiness around the wrists and ankles. When you ask her father to have her stand on the examining table, you see that she needs support to do so (FIGURE 1).
Q: What is your clinical diagnosis, and what tests will you order?
FIGURE 1
The patient, not weight-bearing
The 13-month-old patient has slight bowing of the lower extremities and puffiness around the wrists and ankles. She needs support to stand.
Laboratory results
- Hemoglobin, 9.9 mg/dL
(normal: 10.4-12.4 mg/dL) - Mean corpuscular volume (MCV), 74 fL
(normal: 70-86 fL) - Alkaline phosphatase, 3417 U/L
(normal: 115-460 U/L) - Vitamin D (calcidiol), <7 nmol/L
(normal: 60-108 nmol/L) - Calcium, 9.1 mg/dL
(normal: 8.8-10.8 mg/dL) - Comprehensive metabolic panel, liver transaminases, and thyroid-stimulating hormone levels are all normal
- Parathyroid hormone level, 101 pg/mL
(normal: 10-55 pg/mL).
Radiologic findings
- X-ray shows slight saber deformity of the femurs and broadening of the epiphyses of the forearm (FIGURE 2).
FIGURE 2
Forearm x-ray
The patient’s x-ray shows a widening of the epiphyses (black arrow) and pseudofracture (white arrow).
Can this be rickets?
Here is a child with a history of poor growth and peculiar eating habits. Her legs are bowed and her wrists seem swollen. She does not stand or walk, and refuses to bear weight on her legs. She is anemic, and the lab tests you’ve ordered show abnormal vitamin D, alkaline phosphatase, and parathyroid hormone levels. All of this suggests a diagnosis of rickets.
Causes of rickets
Rickets is the result of abnormal mineralization of bone and cartilage in growing children. The analogous condition in adults whose epiphyseal plates have closed is osteomalacia. Clinical rickets typically presents with the constellation of signs and symptoms listed in the box and depicted in FIGURES 1, 2, and 3.
Clinical findings
- Apathy, listlessness, and poor growth
- Muscle cramps, weakness, hypotonia, numbness, paresthesias, tetany, and seizures
- Pot belly and waddling gait
- Soft, misshapen head with widened sutures and frontal bossing
- Delayed eruption of teeth
- Rachitic rosary (see below)
- Harrison’s groove (indentation at point of insertion of diaphragm, due to the pull of the diaphragm against the softened lower ribs)
- Bowed limbs and swollen joints
Radiologic findings
- Epiphyses widened and flared with irregular, “cupped” epiphyseal-metaphyseal junctions; involvement of the costrochondral junctions produces a row of beadlike prominences often called the “rachitic rosary”
- Long bones bowed (“saber shaped”), with indistinct cortices
- Pseudofractures (also called Looser’s zone or Milkman’s fractures), often found on the concave side of femoral neck, pubic rami, ribs, clavicles, and lateral aspect of scapulae
- Pathologic fractures
Laboratory findings
- Creatinine: Normal value excludes renal insufficiency as etiology
- Liver enzymes: Normal value excludes liver disease as etiology
- Phosphorus: Normal phosphorus and parathyroid hormone make a diagnosis of rickets unlikely
- Parathyroid hormone: Elevated in hypocalcemic rickets (>55 pg/mL)
- Calcium, total and ionized with albumin: May be normal in rickets
- Alkaline phosphatase: Usually markedly increased over the age-specific reference range in rickets
- Urinary calcium level: Usually decreased in rickets (<50 mg/d, depending on calcium content of diet)
- Calcidiol level: May be low in rickets (<50 nmol/L [20 ng/mL])
- Calcitriol level: Usually normal in rickets, because of its short-half life (60-108 nmol/L [25-45 pg/mL])
FIGURE 3
Rachitic rosary
The patient had a developing rosary, most pronounced at the sternoclavicular joint (white arrow) and early saber deformity of the shin (black arrows). Frontal bossing and swollen wrists and ankles may also be seen in patients with rickets.
Not enough vitamin D
The most common cause of rickets is a deficiency of vitamin D, a substance physiologically necessary to produce concentrations of calcium and phosphate adequate for proper bone mineralization. Vitamin D is produced in the skin in the presence of sunlight and can also be ingested in supplements and certain foods.
Vitamin D deficiency may result from reduced sunlight exposure, inadequate dietary intake, malabsorption, or a combination of these factors.1 Rickets may also be caused by medications that alter absorption or secretion of phosphate and calcium, including antacids, anticonvulsants, corticosteroids, and loop diuretics. Various disease states, such as Crohn’s disease, pancreatic disease, biliary disease, gastrointestinal loops and fistulae, cirrhosis, chronic renal disease, and mesenchymal tumors, may also alter absorption and metabolism of these ions.
How much sunshine does a baby need?
It doesn’t take a great deal of sunlight exposure to provide adequate supplies of vitamin D. An infant wearing only a diaper will get enough vitamin D from half an hour per week of sun exposure. A fully clothed infant needs 3 hours. But children with dark skin, like this African baby, need more time in the sun. And if parents follow current anticipatory guidance about protecting children from overexposure to the sun and slather on the sunscreen, vitamin D synthesis decreases by more than 95%.2
Vitamin D in the diet
Consuming adequate quantities of vitamin D is difficult, unless the diet includes fortified foods or vitamin supplements. Current recommendations for daily intake are 400 IU per day for all infants, children, and adolescents.3 But the average daily intake by adults in North America from sources such as fish, eggs, and butter or margarine is only 50 to 100 IU.3
Infants born to vitamin-D replete women have an 8- to 12-week store of vitamin D at birth, but breastfeeding does not ensure the baby is getting adequate amounts of vitamin D, even if the mother’s vitamin D status is adequate. Human milk from vitamin D-replete women has a vitamin D concentration of only 25 IU per liter, far below the recommended daily intake of 400 IU.3
How deficient is this baby?
Vitamin D deficiency may be categorized as mild, moderate, or severe. Calcidiol is the next-to-last step in the metabolism of vitamin D and is used as a marker because it is easier to measure than the concentration of calcitriol, the final step. Mild vitamin D deficiency is defined as serum calcidiol concentration of 25 to 50 nmol/L. A serum calcidiol concentration of 12.5 to 25 nmol/L indicates a moderate vitamin D deficiency, and at those levels the incidence of hypocalcemia and rickets increases. Serum calcidiol concentration of less than 12.5 nmol/L, as in the case of the patient presented here, indicates a severe deficiency.4
Not enough calcium
In addition to calcium malabsorption due to inadequate vitamin D levels, hypocalcemia may result from inadequate intake of calcium or from vitamin D-dependent metabolic disorders, of which there are 2 types.
Type I, sometimes known as pseudo-vitamin D-deficiency rickets, is due to defective production of 25(OH)D3-1-α-hydroxylase, an enzyme necessary for the conversion of calcidiol to calcitriol in the kidneys.
Type II, also called hereditary rickets, is rare. It is caused by mutations in vitamin D receptors and the inability of the ligand to bind or stimulate the proper physiologic response. In this condition, laboratory tests may show high levels of calcitriol.
Not enough phosphorus
Vitamin D-resistant rickets, or familial hypophosphatemic rickets, refers to a clinical presentation of rickets that is caused by a hereditary renal wasting of phosphorus at the proximal tubule level. Laboratory evaluation of a child with this condition will show low phosphate levels, normal calcitriol levels, and hypercalciuria. The specific defect that causes this condition is not known. A family history of short stature, orthopedic abnormalities, poor dentition, alopecia, or parental consanguinity may be suggestive of vitamin D-dependent or vitamin D-resistant forms of inherited rickets.
Other causes of hypophosphatemia include inadequate nutritional intake, X-linked hypophosphatemia, generalized tubular disorders such as renal tubular acidosis, Fanconi syndrome, and Dent disease. These disorders may also lead to rickets.
Q: What are the available treatments for rickets? What about prevention?
Replenishing vitamin D
Vitamin D deficiency may be remedied by supplementing anywhere along the metabolic pathway. Dihydrotachysterol (DHT, or D1), the substance in the skin that responds to sunlight, is given as 60,000 IU once, then 6000 IU daily until the rickets are clinically and radiologically resolved. Further downstream, ergocalciferol (D2) may be given as 1000 to 5000 IU daily for 6 to 12 weeks. The dosage is calibrated by age: 1000 IU/d if age <1 month, 3000 IU/d for ages 1 to 12 months, and 5000 IU/d for children older than 12 months. The final form of vitamin D is cholecalciferol (D3). This is typically administered as either 5000 to 10,000 IU daily for 2 to 3 months, or as 600,000 IU in 1 day, divided into 4 to 6 doses.5,6 All of these supplements taste bad and children are often resistant to swallowing them.
When follow-up and multiple dosing are impractical—because the family finds repeated clinic visits too difficult, or because the child will not comply with the regimen—you can use stosstherapy.7 This is a bolus of cholecalciferol (D3) or ergocalciferol (D2), 150,000 to 600,000 IU, given as a single dose or divided over several days. For example, you would give 300,000 IU over 1 to 7 days in children 1 to 12 months of age. With this therapy, onset of action is less than a day and maximal effects are seen in 4 weeks. Some preparations contain propylene glycol, which is limited in food additives to <25 mg/kg of body weight because of potential toxicity.
When supplementation doesn’t work. Vitamin D is not effective in treatment of familial hypophosphatemic rickets, Type II vitamin D-dependent rickets, or disorders of phosphate metabolism.
Monitoring therapeutic success
When possible, treatment should be monitored by checking serum calcium and alkaline phosphatase at 1 month, and calcium, magnesium, phosphate, alkaline phosphatase, calcidiol, parathyroid hormone, and wrist x-ray at 3 months from initiation of treatment, to ensure that they are normalizing.
Preventing rickets
In the developed world, public health efforts to prevent rickets have been largely successful. Rickets was prevalent worldwide in the early decades of the 20th century, but after milk began to be routinely fortified with vitamin D in the 1920s, cases of nutritional rickets almost disappeared in industrialized nations.
In 1963, the American Academy of Pediatrics (AAP) began recommending vitamin D supplementation to prevent rickets. Although the recommendation remains controversial because of concerns about the possibility of hypervitaminosis and the resultant hypercalcemia and hypercalciuria, there has been renewed emphasis on this recommendation in light of a rise in the number of cases of rickets in the United States in recent years.8-14 Current AAP recommendations for vitamin D supplementation are daily supplementation of 400 IU vitamin D for the following groups:3
- Breastfed infants, beginning with the first few days of life and continued until they are weaned to at least 1000 mL per day of vitamin D-fortified formula or milk.
- Nonbreastfed infants who are ingesting less than 1000 mL per day of vitamin D-fortified formula or milk. Most commercial baby formulas contain 400 IU/L, which means that an intake of 500 mL of formula per day provides 200 IU.15 Additionally, special milk supplemented with vitamin D3 up to 200 IU per 250 mL has recently become available in Europe.16
- Children and adolescents who do not get regular sunlight exposure, do not ingest at least 32 ounces per day of vitamin D-fortified milk, or do not take a daily multivitamin supplement containing at least 400 IU of vitamin D.
Others have suggested a bolus dosing 150,000 IU each autumn for those in northern climates.17
Most over-the-counter vitamin formulations now contain D3 (cholecalciferol), as recent studies show this form is more potent than D2 (ergocalciferol).18 Calcium supplements are available in combination with vitamin D. Calcitriol, the most active form of vitamin D, is available only by prescription. Because it does not require activation in the kidneys, it is the drug of choice for renally impaired patients.
Q: How would you treat this child?
Bad taste is a big hurdle
The child in this case was prescribed 150,000 U oral cholecalciferol. She spit it out at the clinic, and the dose was sent home for her parents to administer. She was also started on a multivitamin (Poly-Vi-Sol). On the return visit a few days later, the parents reported that she only took three-quarters of the vitamin D dose, spitting out the remainder.
When that didn’t work…
The child was then admitted to the hospital for administration of vitamin D and to allow for dietary and social work evaluations of factors contributing to her malnutrition.
Social services evaluation ruled out an economic etiology for the child’s failure to thrive. The family was able to afford a nutritionally adequate diet for the child. They were enrolled in Medicaid and WIC. Willful neglect was not an issue: A very loving and appropriate relationship was evident between the child and her parents. Child care was shared equally by the young parents, but they simply didn’t know what foods were appropriate for a child of her age.
Turning things around
The hospital dietician observed one of the child’s meals. The child ate some of everything on the plate: mashed potatoes and gravy, chicken strips, vegetables, bananas, yogurt, and milk. She was willing to try a variety of foods, and ate most of them. Both the physician and the dietician spent a lot of time with the parents reviewing feeding techniques and healthy food choices. Language was a problem, solved for the most part with the assistance of a dial-up language translation service to ensure clear understanding of the instructions. The health care professionals prepared a list of healthy foods to buy at the grocery store, with pictures illustrating healthy food items. In addition, appropriate exposure to sunlight was explained and encouraged.
Parent education is the key
The child’s father expressed gratitude several times for the instruction on healthy food choices for the daughter, while the mother smiled in shy agreement. He said they did not know what to feed her, and when she refused most things they offered, they fed her the noodles and juice she seemed to prefer. He was grateful to the nutritionist, social worker, nursing staff, and physicians for taking care of his daughter. He was eager to go to the grocery store and to start feeding her the “right foods.”
Ready to go home
By discharge, the child had received the full dose of vitamin D and was eating a variety of foods, including 1 to 4 ounces of milk daily, supplemented with Poly-Vi-Sol, 1 mL orally twice daily, and calcium carbonate (OsCal) with vitamin D, 1 crushed tablet orally twice daily. Home health nursing provided follow-up twice a week, and weekly appointments in the clinic with the physician were also scheduled. Compliance with the discharge plan was impeccable. Both laboratory and clinical signs of rickets resolved over the subsequent weeks.
1. Thacher TD. Determining the nutritional cause of rickets in children. Am Fam Physician. 2007;75:470, 472.-
2. Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79:362-371.
3. Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142-1152.
4. Stroud ML, Stilgoe S, Stott VE, et al. Vitamin D-A review. Aust Fam Physician. 2008;37:1002-1005.
5. Misra M, Pacaud D, Petryk A, et al. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398-417.
6. Shah BR, Finberg L. Single-day therapy for nutritional vitamin D-deficiency rickets: a preferred method. J Pediatr. 1994;125:487-490.
7. Cesur Y, Caksen H, Gundem A, et al. Comparison of low and high dose of vitamin D treatment in nutritional vitamin D deficiency rickets. J Pediatr Endocrinol Metab. 2003;16:1105-1109.
8. Centers for Disease Control and Prevention. Severe malnutrition among young children—Georgia, January 1997-June 1999. MMWR Morb Mortal Wkly Rep. 2001;50:224-227.
9. Rajakumar K, Thomas SB. Reemerging nutritional rickets: a historical perspective. Arch Pediatr Adolesc Med. 2005;159:335-341.
10. Tomashek KM, Nesby S, Scanlon KS, et al. Nutritional rickets in Georgia. Pediatrics. 2001;107:E45.-
11. Weisberg P, Scanlon KS, Li R, et al. Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004;80(suppl 6):S1697-S1705S.
12. Alouf B, Grigalonis M. Incidental finding of vitamin-D deficient rickets in an otherwise healthy infant—a reappraisal of current vitamin-D supplementation guidelines. J Natl Med Assoc. 2005;97:1170-1173.
13. Nield LS, Mahajan P, Joshi A, et al. Rickets: not a disease of the past. Am Fam Physician. 2006;74:619-626.
14. Wagner C. Rickets: emerging from obscurity. Am Fam Physician. 2006;74:561-562.
15. Calvo MS, Whiting SJ, Barton CN. Vitamin D fortification in the United States and Canada: current status and data needs. Am J Clin Nutr. 2004;80(suppl 6):S1710-S1716.
16. Avonmore Super Milk. Glanbia Consumer Foods, Dublin, Ireland. Available at: www.sendmorefamilies.com/super-milk.aspx. Accessed August 23, 2009.
17. Oliveri B, Cassinelli H, Mautalen C, et al. Vitamin D prophylaxis in children with a single dose of 150,000 IU of vitamin D. Eur J Clin Nutr. 1996;50:807-810.
18. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab. 2004;89:5387-5391.
Correspondence Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; mark.huntington@usd.edu
1. Thacher TD. Determining the nutritional cause of rickets in children. Am Fam Physician. 2007;75:470, 472.-
2. Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79:362-371.
3. Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142-1152.
4. Stroud ML, Stilgoe S, Stott VE, et al. Vitamin D-A review. Aust Fam Physician. 2008;37:1002-1005.
5. Misra M, Pacaud D, Petryk A, et al. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398-417.
6. Shah BR, Finberg L. Single-day therapy for nutritional vitamin D-deficiency rickets: a preferred method. J Pediatr. 1994;125:487-490.
7. Cesur Y, Caksen H, Gundem A, et al. Comparison of low and high dose of vitamin D treatment in nutritional vitamin D deficiency rickets. J Pediatr Endocrinol Metab. 2003;16:1105-1109.
8. Centers for Disease Control and Prevention. Severe malnutrition among young children—Georgia, January 1997-June 1999. MMWR Morb Mortal Wkly Rep. 2001;50:224-227.
9. Rajakumar K, Thomas SB. Reemerging nutritional rickets: a historical perspective. Arch Pediatr Adolesc Med. 2005;159:335-341.
10. Tomashek KM, Nesby S, Scanlon KS, et al. Nutritional rickets in Georgia. Pediatrics. 2001;107:E45.-
11. Weisberg P, Scanlon KS, Li R, et al. Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004;80(suppl 6):S1697-S1705S.
12. Alouf B, Grigalonis M. Incidental finding of vitamin-D deficient rickets in an otherwise healthy infant—a reappraisal of current vitamin-D supplementation guidelines. J Natl Med Assoc. 2005;97:1170-1173.
13. Nield LS, Mahajan P, Joshi A, et al. Rickets: not a disease of the past. Am Fam Physician. 2006;74:619-626.
14. Wagner C. Rickets: emerging from obscurity. Am Fam Physician. 2006;74:561-562.
15. Calvo MS, Whiting SJ, Barton CN. Vitamin D fortification in the United States and Canada: current status and data needs. Am J Clin Nutr. 2004;80(suppl 6):S1710-S1716.
16. Avonmore Super Milk. Glanbia Consumer Foods, Dublin, Ireland. Available at: www.sendmorefamilies.com/super-milk.aspx. Accessed August 23, 2009.
17. Oliveri B, Cassinelli H, Mautalen C, et al. Vitamin D prophylaxis in children with a single dose of 150,000 IU of vitamin D. Eur J Clin Nutr. 1996;50:807-810.
18. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab. 2004;89:5387-5391.
Correspondence Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; mark.huntington@usd.edu