User login
IRIS Presenting as Acute Pericarditis
Although antiretroviral therapy for human immunodeficiency virus (HIV)‐infected patients reduces viral load dramatically and improves immune function, some patients experience a clinical deterioration within the first few months of therapy because of an exuberant and dysregulated immune responsethe immune reconstitution inflammatory syndrome (IRIS). The exaggerated immune response associated with this syndrome can be stimulated by either antigens from infectious agents (typically a mycobacterium or cryptococcus) or from autoantigens, giving rise to a heterogeneous range of clinical manifestations.1 IRIS may present as an inflammatory reaction that unmasks a previously untreated infection or as a paradoxical worsening of an infection that is being treated appropriately. Although most cases of IRIS are mild and self‐limited, some patients require aggressive treatment.1
Case Report
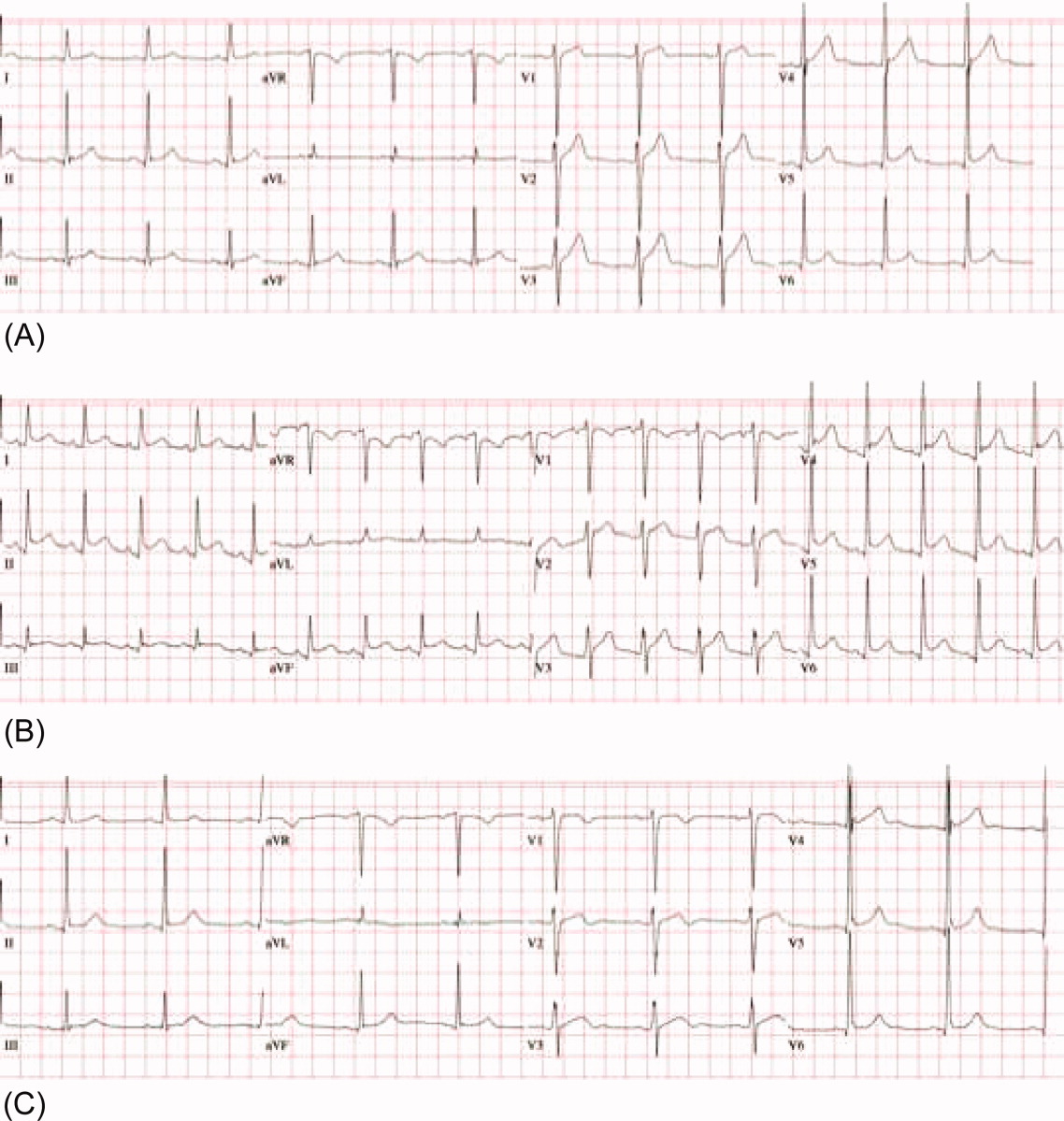
A 53‐year‐old man was evaluated for a 5‐day history of intermittent chest pain. He had been diagnosed with HIV/acquired immune deficiency syndrome (AIDS) 11 years ago but he had not been compliant with therapy. Seven years earlier he had been treated for 9 months with isoniazid for a positive tuberculin skin test. Three months before admission, he developed methicillin‐resistant Staphylococcus aureus skin abscesses and was found to have a CD4 count of 1/L and a HIV viral load of over 400,000 copies/mL. He finished a course of vancomycin, and was started on lopinavir, ritonavir, abacavir, lamivudine, and zidovudine. Five days before admission, he was evaluated in the emergency department for intermittent chest pain and described using cocaine. There was only J‐point elevation on the electrocardiogram (Figure 1A), serial cardiac enzymes were negative, and he was discharged home. However, despite discontinuation of cocaine use, his chest pain worsened, became pleuritic, and was associated with dyspnea, which prompted this admission. Physical examination was remarkable only for tachycardia, although the electrocardiogram now revealed diffuse ST segment (ST) elevation and PR segment (PR) depression, consistent with acute pericarditis (Figure 1B). Serial cardiac enzymes, viral studies, and bacterial, fungal, and mycobacterial blood cultures were negative. His CD4 count was 16/L, and the HIV viral load was 870 copies/mL.
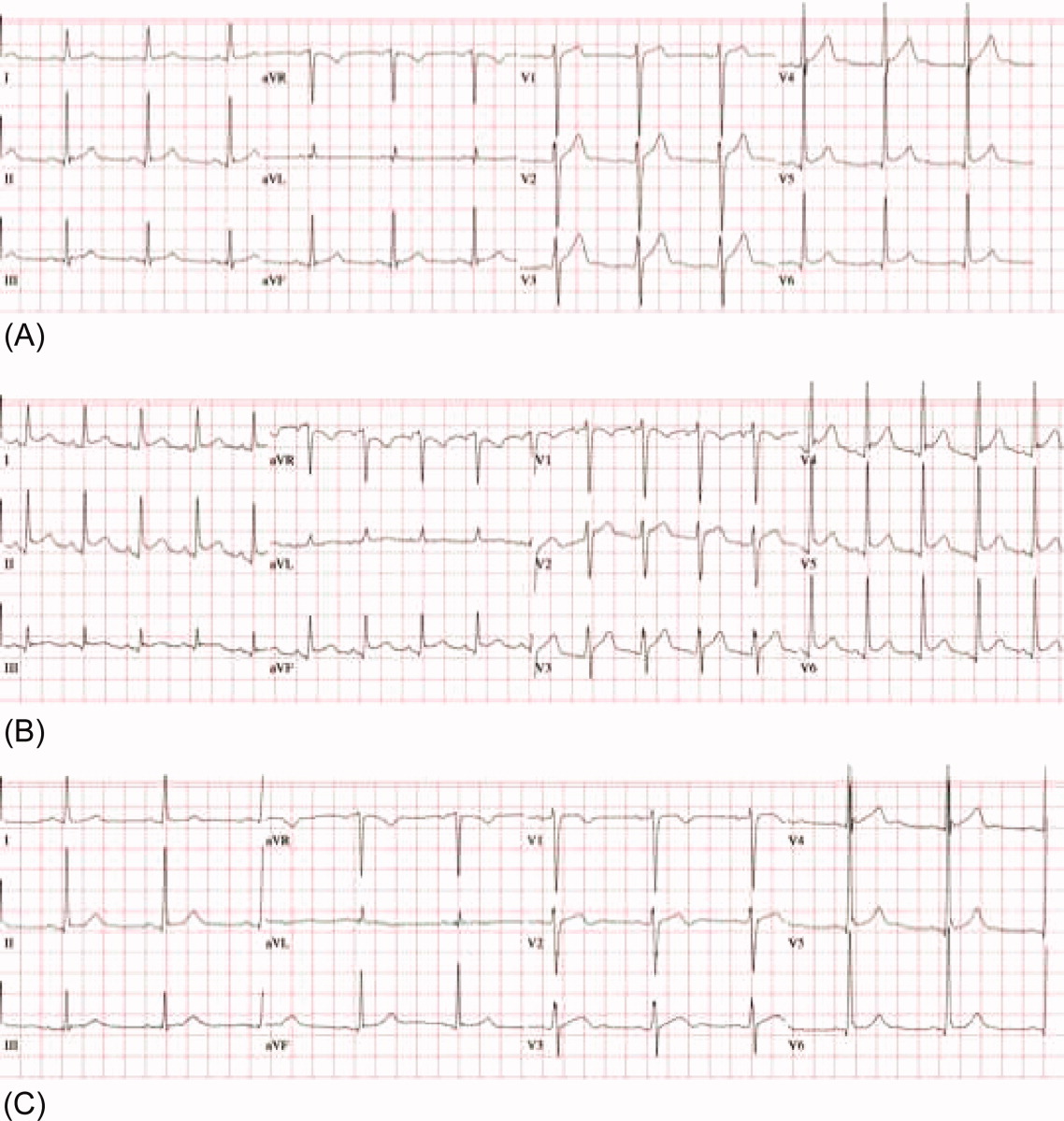
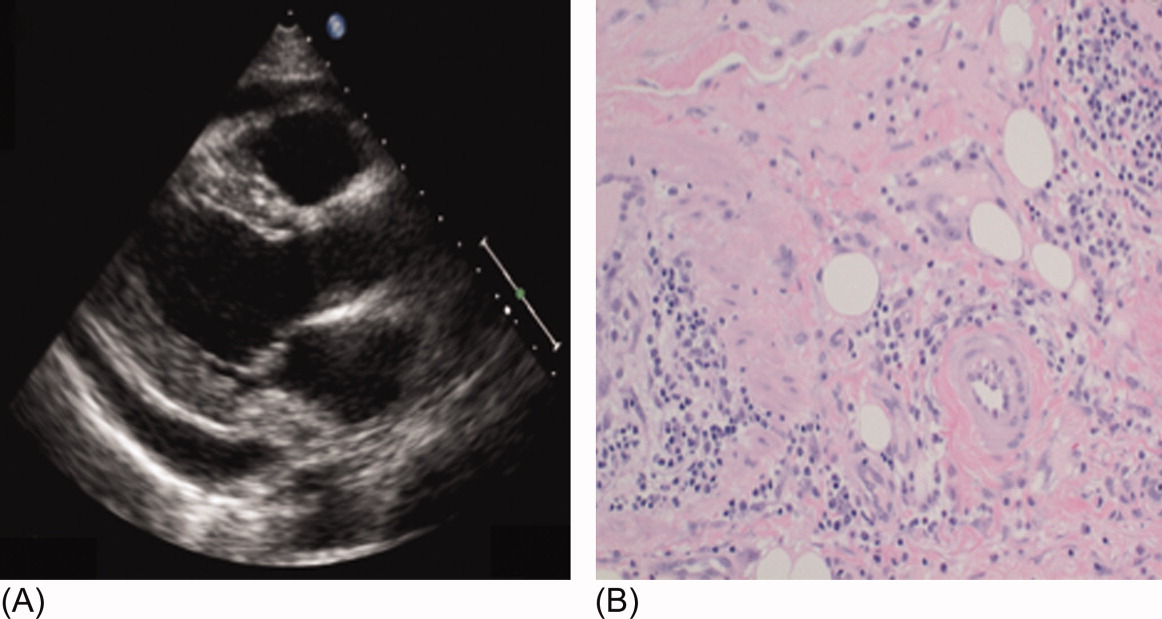
The patient was treated with high‐dose ibuprofen and colchicine, but mild chest pain and electrocardiogram changes persisted, and he developed a friction rub. A chest computed tomography (CT) scan was negative for pulmonary embolism and revealed no significant intra‐thoracic pathology, except for a moderate pericardial effusion that was confirmed by transthoracic echocardiogram (Figure 2A). There was no echocardiographic evidence of tamponade. He underwent thoracoscopic pericardial and mediastinal lymph node biopsy, along with drainage of the pericardial effusion. Pericardial biopsy showed acute on chronic inflammation consistent with pericarditis (Figure 2B) and culture was positive for Mycobacterium Avium Complex (MAC). He was treated with clarithromycin, ethambutol, and prednisone, and his antiretroviral medications were continued. At 2, 6, and 12 months follow‐up, he was asymptomatic, the electrocardiogram had normalized (Figure 1C), and the echocardiogram showed no effusion or evidence of pericardial constriction.
Discussion
This case demonstrates a unique manifestation of the IRIS associated with MAC infection, which more typically presents as peripheral, pulmonary, or intra‐abdominal lymphadenopathy.2, 3 It usually responds to MAC therapy, although intra‐abdominal disease portends a poor prognosis.3, 4 This patient has two significant risk factors for the development of IRIS: low CD4 count at the time of antiretroviral therapy and rapid viral clearance.5, 6 While his CD4 count response is lower than expected for IRIS, previous studies have shown that functional immune recovery usually precedes quantitative CD4 count recovery, and that IRIS could happen at low CD4 count.1, 7 Finally, we believe that the use of corticosteroids accounted for his rapid clinical improvement and favorable long‐term outcome, consistent with previous experience of corticosteroid use in MAC‐associated IRIS.3, 4 To our knowledge, this is the first reported case of MAC‐associated IRIS presenting as isolated acute pericarditis and pericardial effusion. In conclusion, our case illustrates that IRIS can present as an abnormal immune response to an opportunistic infection in an unusual location. Clinicians must be aware that after starting antiretroviral therapy, new symptoms, including chest pain, might represent 1 of the IRISs, and that corticosteroids might be beneficial when inflammation is severe.
Acknowledgements
The authors thank Dr. Arthur Evans for his comments.
- ,,,,.Immune reconstitution inflammatory syndrome in HIV‐infected patients receiving antiretroviral therapy.Drugs.2008;68:191–208.
- ,,,,.The imaging features of nontuberculous mycobacterial immune reconstitution syndrome.J Comput Assist Tomogr.2009;33:242–246.
- ,,, et al.Nontuberculous mycobacterial immune reconstitution syndrome in HIV‐infected patients: spectrum of disease and long‐term follow‐up.Clin Infect Dis.2005;41:1483–1497.
- ,,,,,.Mycobacterium avium complex immune reconstitution inflammatory syndrome: long term outcomes.J Transl Med.2007;5:50–56.
- ,,, et al.Incidence and risk factors for immune reconstitution inflammatory syndrome during highly active antiretroviral therapy.AIDS.2005;19:399–406.
- ,,,.Incidence and risk factors for immune reconstitution inflammatory syndrome in an ethnically diverse HIV type 1‐infected cohort.Clin Infect Dis.2006;42:418–427.
- ,,.Immune reconstitution disease associated with mycobacterial infections in HIV‐infected individuals receiving antiretrovirals.Lancet Infect Dis.2005;5:361–373.
Although antiretroviral therapy for human immunodeficiency virus (HIV)‐infected patients reduces viral load dramatically and improves immune function, some patients experience a clinical deterioration within the first few months of therapy because of an exuberant and dysregulated immune responsethe immune reconstitution inflammatory syndrome (IRIS). The exaggerated immune response associated with this syndrome can be stimulated by either antigens from infectious agents (typically a mycobacterium or cryptococcus) or from autoantigens, giving rise to a heterogeneous range of clinical manifestations.1 IRIS may present as an inflammatory reaction that unmasks a previously untreated infection or as a paradoxical worsening of an infection that is being treated appropriately. Although most cases of IRIS are mild and self‐limited, some patients require aggressive treatment.1
Case Report
A 53‐year‐old man was evaluated for a 5‐day history of intermittent chest pain. He had been diagnosed with HIV/acquired immune deficiency syndrome (AIDS) 11 years ago but he had not been compliant with therapy. Seven years earlier he had been treated for 9 months with isoniazid for a positive tuberculin skin test. Three months before admission, he developed methicillin‐resistant Staphylococcus aureus skin abscesses and was found to have a CD4 count of 1/L and a HIV viral load of over 400,000 copies/mL. He finished a course of vancomycin, and was started on lopinavir, ritonavir, abacavir, lamivudine, and zidovudine. Five days before admission, he was evaluated in the emergency department for intermittent chest pain and described using cocaine. There was only J‐point elevation on the electrocardiogram (Figure 1A), serial cardiac enzymes were negative, and he was discharged home. However, despite discontinuation of cocaine use, his chest pain worsened, became pleuritic, and was associated with dyspnea, which prompted this admission. Physical examination was remarkable only for tachycardia, although the electrocardiogram now revealed diffuse ST segment (ST) elevation and PR segment (PR) depression, consistent with acute pericarditis (Figure 1B). Serial cardiac enzymes, viral studies, and bacterial, fungal, and mycobacterial blood cultures were negative. His CD4 count was 16/L, and the HIV viral load was 870 copies/mL.
The patient was treated with high‐dose ibuprofen and colchicine, but mild chest pain and electrocardiogram changes persisted, and he developed a friction rub. A chest computed tomography (CT) scan was negative for pulmonary embolism and revealed no significant intra‐thoracic pathology, except for a moderate pericardial effusion that was confirmed by transthoracic echocardiogram (Figure 2A). There was no echocardiographic evidence of tamponade. He underwent thoracoscopic pericardial and mediastinal lymph node biopsy, along with drainage of the pericardial effusion. Pericardial biopsy showed acute on chronic inflammation consistent with pericarditis (Figure 2B) and culture was positive for Mycobacterium Avium Complex (MAC). He was treated with clarithromycin, ethambutol, and prednisone, and his antiretroviral medications were continued. At 2, 6, and 12 months follow‐up, he was asymptomatic, the electrocardiogram had normalized (Figure 1C), and the echocardiogram showed no effusion or evidence of pericardial constriction.
Discussion
This case demonstrates a unique manifestation of the IRIS associated with MAC infection, which more typically presents as peripheral, pulmonary, or intra‐abdominal lymphadenopathy.2, 3 It usually responds to MAC therapy, although intra‐abdominal disease portends a poor prognosis.3, 4 This patient has two significant risk factors for the development of IRIS: low CD4 count at the time of antiretroviral therapy and rapid viral clearance.5, 6 While his CD4 count response is lower than expected for IRIS, previous studies have shown that functional immune recovery usually precedes quantitative CD4 count recovery, and that IRIS could happen at low CD4 count.1, 7 Finally, we believe that the use of corticosteroids accounted for his rapid clinical improvement and favorable long‐term outcome, consistent with previous experience of corticosteroid use in MAC‐associated IRIS.3, 4 To our knowledge, this is the first reported case of MAC‐associated IRIS presenting as isolated acute pericarditis and pericardial effusion. In conclusion, our case illustrates that IRIS can present as an abnormal immune response to an opportunistic infection in an unusual location. Clinicians must be aware that after starting antiretroviral therapy, new symptoms, including chest pain, might represent 1 of the IRISs, and that corticosteroids might be beneficial when inflammation is severe.
Acknowledgements
The authors thank Dr. Arthur Evans for his comments.
Although antiretroviral therapy for human immunodeficiency virus (HIV)‐infected patients reduces viral load dramatically and improves immune function, some patients experience a clinical deterioration within the first few months of therapy because of an exuberant and dysregulated immune responsethe immune reconstitution inflammatory syndrome (IRIS). The exaggerated immune response associated with this syndrome can be stimulated by either antigens from infectious agents (typically a mycobacterium or cryptococcus) or from autoantigens, giving rise to a heterogeneous range of clinical manifestations.1 IRIS may present as an inflammatory reaction that unmasks a previously untreated infection or as a paradoxical worsening of an infection that is being treated appropriately. Although most cases of IRIS are mild and self‐limited, some patients require aggressive treatment.1
Case Report
A 53‐year‐old man was evaluated for a 5‐day history of intermittent chest pain. He had been diagnosed with HIV/acquired immune deficiency syndrome (AIDS) 11 years ago but he had not been compliant with therapy. Seven years earlier he had been treated for 9 months with isoniazid for a positive tuberculin skin test. Three months before admission, he developed methicillin‐resistant Staphylococcus aureus skin abscesses and was found to have a CD4 count of 1/L and a HIV viral load of over 400,000 copies/mL. He finished a course of vancomycin, and was started on lopinavir, ritonavir, abacavir, lamivudine, and zidovudine. Five days before admission, he was evaluated in the emergency department for intermittent chest pain and described using cocaine. There was only J‐point elevation on the electrocardiogram (Figure 1A), serial cardiac enzymes were negative, and he was discharged home. However, despite discontinuation of cocaine use, his chest pain worsened, became pleuritic, and was associated with dyspnea, which prompted this admission. Physical examination was remarkable only for tachycardia, although the electrocardiogram now revealed diffuse ST segment (ST) elevation and PR segment (PR) depression, consistent with acute pericarditis (Figure 1B). Serial cardiac enzymes, viral studies, and bacterial, fungal, and mycobacterial blood cultures were negative. His CD4 count was 16/L, and the HIV viral load was 870 copies/mL.
The patient was treated with high‐dose ibuprofen and colchicine, but mild chest pain and electrocardiogram changes persisted, and he developed a friction rub. A chest computed tomography (CT) scan was negative for pulmonary embolism and revealed no significant intra‐thoracic pathology, except for a moderate pericardial effusion that was confirmed by transthoracic echocardiogram (Figure 2A). There was no echocardiographic evidence of tamponade. He underwent thoracoscopic pericardial and mediastinal lymph node biopsy, along with drainage of the pericardial effusion. Pericardial biopsy showed acute on chronic inflammation consistent with pericarditis (Figure 2B) and culture was positive for Mycobacterium Avium Complex (MAC). He was treated with clarithromycin, ethambutol, and prednisone, and his antiretroviral medications were continued. At 2, 6, and 12 months follow‐up, he was asymptomatic, the electrocardiogram had normalized (Figure 1C), and the echocardiogram showed no effusion or evidence of pericardial constriction.
Discussion
This case demonstrates a unique manifestation of the IRIS associated with MAC infection, which more typically presents as peripheral, pulmonary, or intra‐abdominal lymphadenopathy.2, 3 It usually responds to MAC therapy, although intra‐abdominal disease portends a poor prognosis.3, 4 This patient has two significant risk factors for the development of IRIS: low CD4 count at the time of antiretroviral therapy and rapid viral clearance.5, 6 While his CD4 count response is lower than expected for IRIS, previous studies have shown that functional immune recovery usually precedes quantitative CD4 count recovery, and that IRIS could happen at low CD4 count.1, 7 Finally, we believe that the use of corticosteroids accounted for his rapid clinical improvement and favorable long‐term outcome, consistent with previous experience of corticosteroid use in MAC‐associated IRIS.3, 4 To our knowledge, this is the first reported case of MAC‐associated IRIS presenting as isolated acute pericarditis and pericardial effusion. In conclusion, our case illustrates that IRIS can present as an abnormal immune response to an opportunistic infection in an unusual location. Clinicians must be aware that after starting antiretroviral therapy, new symptoms, including chest pain, might represent 1 of the IRISs, and that corticosteroids might be beneficial when inflammation is severe.
Acknowledgements
The authors thank Dr. Arthur Evans for his comments.
- ,,,,.Immune reconstitution inflammatory syndrome in HIV‐infected patients receiving antiretroviral therapy.Drugs.2008;68:191–208.
- ,,,,.The imaging features of nontuberculous mycobacterial immune reconstitution syndrome.J Comput Assist Tomogr.2009;33:242–246.
- ,,, et al.Nontuberculous mycobacterial immune reconstitution syndrome in HIV‐infected patients: spectrum of disease and long‐term follow‐up.Clin Infect Dis.2005;41:1483–1497.
- ,,,,,.Mycobacterium avium complex immune reconstitution inflammatory syndrome: long term outcomes.J Transl Med.2007;5:50–56.
- ,,, et al.Incidence and risk factors for immune reconstitution inflammatory syndrome during highly active antiretroviral therapy.AIDS.2005;19:399–406.
- ,,,.Incidence and risk factors for immune reconstitution inflammatory syndrome in an ethnically diverse HIV type 1‐infected cohort.Clin Infect Dis.2006;42:418–427.
- ,,.Immune reconstitution disease associated with mycobacterial infections in HIV‐infected individuals receiving antiretrovirals.Lancet Infect Dis.2005;5:361–373.
- ,,,,.Immune reconstitution inflammatory syndrome in HIV‐infected patients receiving antiretroviral therapy.Drugs.2008;68:191–208.
- ,,,,.The imaging features of nontuberculous mycobacterial immune reconstitution syndrome.J Comput Assist Tomogr.2009;33:242–246.
- ,,, et al.Nontuberculous mycobacterial immune reconstitution syndrome in HIV‐infected patients: spectrum of disease and long‐term follow‐up.Clin Infect Dis.2005;41:1483–1497.
- ,,,,,.Mycobacterium avium complex immune reconstitution inflammatory syndrome: long term outcomes.J Transl Med.2007;5:50–56.
- ,,, et al.Incidence and risk factors for immune reconstitution inflammatory syndrome during highly active antiretroviral therapy.AIDS.2005;19:399–406.
- ,,,.Incidence and risk factors for immune reconstitution inflammatory syndrome in an ethnically diverse HIV type 1‐infected cohort.Clin Infect Dis.2006;42:418–427.
- ,,.Immune reconstitution disease associated with mycobacterial infections in HIV‐infected individuals receiving antiretrovirals.Lancet Infect Dis.2005;5:361–373.
TEN Associated with Herbal Medication Use
A 49‐year‐old woman with history of rheumatic fever necessitating mechanical mitral valve replacement and a cerebrovascular accident of presumed embolic etiology presented with several months of progressive fatigue, weakness, arthralgias, and myalgias. After an extensive workup, a rheumatologist in the community diagnosed her with systemic lupus erythematosus and dermatomyositis. The patient refused therapy with corticosteroids and disease‐modifying agents, citing concerns of adverse effects. She consulted a naturopathic clinician, who gave her Rejuvenator Pills, Super Booster pill, Genesis Juice, and alkaline water (Table 1).
| Rejuvenator Pill |
| Slippery elm 45 mg (Ulmus rubra) |
| Capsicum 40 mg (Capsicum spp.) |
| Fennel seeds 35 mg (Foeniculum vulgare) |
| Chickweed 35 mg (Stellaria media) |
| Hawthorn berry 30 mg (Crataegus oxyacantha) |
| Mullein 30 mg (Verbascum thapsus) |
| Scullcap 25 mg (Scutellaria spp.) |
| Rosehip 25 mg (Rosa spp.) |
| Barberry 20 mg (Berberis vulgaris) |
| Pau d'arco 20 mg (Tabebuia spp.) |
| Comfrey leaf 20 mg (Symphytum officinale) |
| Alfalfa 20 mg (Medicago sativa) |
| Kelp 20 mg (Laminaria spp.) |
| Papaya leaf 15 mg (Carica papaya) |
| Bee pollen 15 mg |
| Black cohosh 15 mg (Cimicifuga racemosa) |
| Chaparral 10 mg (Larrea tridentata) |
| Ginger 10 mg (Zingiber officinale) |
| Dandelion 5 mg (Taraxacum officinale) |
| Sunflower 5 mg (Helianthus annuus) |
| Licorice root 5 mg (Glycyrrhiza glabra) |
| Cascara sagrada 25 mg |
| Super Booster pill |
| Cascara sagrada |
| Psyllium (Plantago spp.) |
| Fennel (Foeniculum vulgare) |
| Genesis Juice |
| Apple (Malus domestica) |
| Pomegranate (Punica granatum) |
| Aloe vera juice (reconstituted) |
| Whole fruit grape extract (Vitis vinifera spp.) |
| Barley grass (Hordeum vulgare) |
| Cinnamon bark (Cinnamomum spp.) |
| Coriander leaf (Coriandrum sativum) |
| Coriander seed (Coriandrum sativum) |
| Cucumber (Cucumis sativus) |
| Fig fruit (Ficus carica) |
| Garlic bulb (Allium sativum) |
| Juniper berry (Juniperus spp.) |
| Leek (Allium ampeloprasum) |
| Lentil (Lens culinaris) |
| Mulberry fruit (Morus spp.) |
| Olive leaf (Olea europaea) |
| Onion bulb (Allium cepa) |
| Sweet almond (Prunus amygdalus dulcis) |
| Wheat grass (Triticum aestivum) |
| Alkaline water |
Several weeks later, the patient developed dusky erythematous plaques on her anterior and posterior trunk, face, and proximal extremities. Over the next several weeks, she became progressively weak until she was ultimately bedbound. The plaques over her back began to denude. Upon admission to an outside hospital, she was diagnosed with warfarin‐related skin necrosis, superinfected decubitus ulcers, and severe anemia. She refused blood transfusion, and was discharged home with clindamycin and iron. After her clinical status deteriorated over the subsequent week, she arrived at our hospital by ambulance.
In addition to the herbal medications she had recently started, she had been taking warfarin, furosemide, nitroglycerin via skin patch, and aspirin for over 10 years. On exam, she was febrile, tachycardic, hypotensive, and toxic‐appearing. Conjunctivitis was absent. Her mucous membranes were dry, with easily removable white and yellowish deposits on the buccal mucosa. No lesions or ulcerations were present. Dermatologic exam demonstrated confluent scaly, violaceous erythematous patches and plaques covering 60% of the total body surface area with focal areas that were denuded. Large areas of denuded skin were present over the back, inframammary folds, and underneath her abdominal pannus (Figures 1 and 2). Nikolsky's sign was present. She was oriented to person only.


Initial laboratory studies were significant for the following: white blood cell count = 12,800 cells/mm3, hemoglobin = 7.3 g/dL, creatinine = 11.2 mg/dL, blood urea nitrogen = 136 mg/dL, and bicarbonate level = 15 mmol/L. She was admitted to the medical intensive care unit for presumed sepsis. Aggressive resuscitation and broad spectrum antibiotics were administered. A thorough workup for infection, including blood and urine cultures, chest radiography, and lumbar puncture, was unremarkable. Antinuclear antibodies (ANAs) were present in a 1:2560 titer; with a nucleolar and speckled pattern and cytoplasmic antibodies. Additional rheumatologic workup revealed positive anti‐Smith antibody and weakly positive antiribonuclear protein antibody. Pathology from a punch biopsy performed by a dermatology consultant on hospital day 2 demonstrated full‐thickness skin necrosis with scant perivascular infiltrate. While the patient's family had disposed of the pill containers, they had kept several pills. These were sent for analysis, which did not reveal contamination with heavy metals or allopathic medications.
The patient was ultimately diagnosed with TEN and systemic lupus erythematosus with overlap syndrome, and intravenous methylprednisolone was administered. Broad‐spectrum antibiotics were administered for 48 hours, but stopped after workup for infection proved unrevealing. Wound care was mupirocin ointment with petrolatum dressings twice daily as per the hospital's TEN protocol. The patient's course was complicated by acidosis requiring hemodialysis and several tonic‐clonic seizures, a result of presumed lupus cerebritis due to rapidly progressive lesions on serial magnetic resonance images (MRIs) with a negative lumbar puncture. Renal biopsy demonstrated acute tubular necrosis and collapsing glomerulopathy. The patient ultimately recovered, and was discharged to a rehabilitation facility. In follow‐up several months later, she had healing skin with residual dyspigmentation and normal renal function. She was ambulatory and fully oriented, but complained of persistent memory difficulties.
Discussion
While use of complementary or alternative medicine (CAM) is widespread, physicians often underestimate the prevalence of CAM use in their patients. Only one‐half of primary care practitioners are aware of the risk for serious adverse reactions from CAMs.1 This case demonstrates the need for hospitalists to obtain a thorough medication history, including probing for CAM use, when evaluating a new patient. The delayed diagnosis of TEN, whether due to failure to elicit CAM use or recognize the clinical presentation, delayed appropriate treatment by a week and this patient developed potentially lethal complications.
Stevens‐Johnson syndrome (SJS) and TEN lie on a spectrum of disorders involving separation of the epidermis from the dermis when tension is applied to the skin, associated with mucositis, conjunctivitis, and generalized toxicity. The rash is dusky and erythematous, and Nikolsky's sign (separation of the epidermis from the dermis with tension applied to the skin) is present. These entities most commonly develop secondary to medications or infections. Most reactions occur within 60 days of drug initiation. The rash progressives over 1 to 15 days, and the rate of healing is variable. The overall mortality is 30% and is predicted by the SCORTEN system, which incorporates laboratory data, patient history, and the extent of skin breakdown.2 Treatment is primarily supportive; the use of corticosteroids, nonsteroidal immunosuppressive agents, intravenous immunoglobulin (IVIG), or plasmapheresis remains controversial.3
Case reports have described the development of SJS or TEN with CAM use. For example, 1 patient repeatedly developed SJS, with each episode occurring after exposure to an herbal medication containing red clover, burdock, queen's delight, poke root, prickly ash, sassafras bark, and passion flower.4 Similar to our case, identifying the exact agent responsible for TEN was impossible due to large numbers of herbal medications combined into a single pill. SJS and TEN are not limited to Western herbal medicines. Traditional Chinese medications are one of the most common causes of SJS and TEN in East Asia,5 although adulteration with allopathic medications is common in this setting. Ayurvedic medications,6 an ophiopogonis‐containing health drink,7 ginseng,8 and Gingko biloba9, 10 have also been implicated.
Conclusions
This case demonstrates the difficulty in making a diagnosis of CAM‐induced toxicity and identifying the likely agent responsible. Hospitalists must have a high index of suspicion of CAM‐associated toxicity to make this diagnosis, especially when admitting patients who may not volunteer CAM use without direct questioning.
Acknowledgements
This case was initially presented at the Midwest Society of General Internal Medicine regional meeting on September 2526, 2008. Figures 1 and 2 are courtesy of Dr. Robert Chen. The authors thank Dr. James Rhee from the Section of Emergency Medicine at the University of Chicago, who provided toxicology consultation and assisted with toxicology analysis. The authors also acknowledge Meryl Prochaska for manuscript preparation and the patient and her family for their courage and tenacity during the recovery process.
- ,,,.A survey of primary care physicians' perceptions of their patients' use of complementary medicine.Complement Ther Med.2003;11(4):254–260.
- ,,,,,.SCORTEN: a severity‐of‐illness score for toxic epidermal necrolysis.J Invest Dermatol.2000;115(2):149–153.
- ,,.Toxic epidermal necrolysis.J Am Acad Dermatol.2007;56(2):181–200.
- .Severe cutaneous reactions to alternative remedies.Br Med J.1986;293(6548):665–666.
- ,.Toxic epidermal necrolysis in a burns centre: a 6‐year review.Burns.1996;22(4):275–258.
- ,,,,.Herbal medicine induced Stevens‐Johnson syndrome: a case report.Int J Paediatr Dent.2004;14(3):204–207.
- ,,,,.Stevens‐Johnson syndrome caused by a health drink (Eberu) containing ophiopogonis tuber.J Dermatol.1998;25(10):662–665.
- ,,,,.Ginseng as a cause for Stevens‐Johnson syndrome?Lancet.1996;347:1344.
- ,.Stevens‐Johnson syndrome with Ginkgo biloba.J Herbal Pharmacother.2001;1(3):65–69.
- ,,, et al.[Stevens‐Johnson syndrome/toxic epidermal necrolysis treated with intravenous immunoglobulins].Actas Dermosifiliogr.2005;96(9):589–592. [Spanish].
A 49‐year‐old woman with history of rheumatic fever necessitating mechanical mitral valve replacement and a cerebrovascular accident of presumed embolic etiology presented with several months of progressive fatigue, weakness, arthralgias, and myalgias. After an extensive workup, a rheumatologist in the community diagnosed her with systemic lupus erythematosus and dermatomyositis. The patient refused therapy with corticosteroids and disease‐modifying agents, citing concerns of adverse effects. She consulted a naturopathic clinician, who gave her Rejuvenator Pills, Super Booster pill, Genesis Juice, and alkaline water (Table 1).
| Rejuvenator Pill |
| Slippery elm 45 mg (Ulmus rubra) |
| Capsicum 40 mg (Capsicum spp.) |
| Fennel seeds 35 mg (Foeniculum vulgare) |
| Chickweed 35 mg (Stellaria media) |
| Hawthorn berry 30 mg (Crataegus oxyacantha) |
| Mullein 30 mg (Verbascum thapsus) |
| Scullcap 25 mg (Scutellaria spp.) |
| Rosehip 25 mg (Rosa spp.) |
| Barberry 20 mg (Berberis vulgaris) |
| Pau d'arco 20 mg (Tabebuia spp.) |
| Comfrey leaf 20 mg (Symphytum officinale) |
| Alfalfa 20 mg (Medicago sativa) |
| Kelp 20 mg (Laminaria spp.) |
| Papaya leaf 15 mg (Carica papaya) |
| Bee pollen 15 mg |
| Black cohosh 15 mg (Cimicifuga racemosa) |
| Chaparral 10 mg (Larrea tridentata) |
| Ginger 10 mg (Zingiber officinale) |
| Dandelion 5 mg (Taraxacum officinale) |
| Sunflower 5 mg (Helianthus annuus) |
| Licorice root 5 mg (Glycyrrhiza glabra) |
| Cascara sagrada 25 mg |
| Super Booster pill |
| Cascara sagrada |
| Psyllium (Plantago spp.) |
| Fennel (Foeniculum vulgare) |
| Genesis Juice |
| Apple (Malus domestica) |
| Pomegranate (Punica granatum) |
| Aloe vera juice (reconstituted) |
| Whole fruit grape extract (Vitis vinifera spp.) |
| Barley grass (Hordeum vulgare) |
| Cinnamon bark (Cinnamomum spp.) |
| Coriander leaf (Coriandrum sativum) |
| Coriander seed (Coriandrum sativum) |
| Cucumber (Cucumis sativus) |
| Fig fruit (Ficus carica) |
| Garlic bulb (Allium sativum) |
| Juniper berry (Juniperus spp.) |
| Leek (Allium ampeloprasum) |
| Lentil (Lens culinaris) |
| Mulberry fruit (Morus spp.) |
| Olive leaf (Olea europaea) |
| Onion bulb (Allium cepa) |
| Sweet almond (Prunus amygdalus dulcis) |
| Wheat grass (Triticum aestivum) |
| Alkaline water |
Several weeks later, the patient developed dusky erythematous plaques on her anterior and posterior trunk, face, and proximal extremities. Over the next several weeks, she became progressively weak until she was ultimately bedbound. The plaques over her back began to denude. Upon admission to an outside hospital, she was diagnosed with warfarin‐related skin necrosis, superinfected decubitus ulcers, and severe anemia. She refused blood transfusion, and was discharged home with clindamycin and iron. After her clinical status deteriorated over the subsequent week, she arrived at our hospital by ambulance.
In addition to the herbal medications she had recently started, she had been taking warfarin, furosemide, nitroglycerin via skin patch, and aspirin for over 10 years. On exam, she was febrile, tachycardic, hypotensive, and toxic‐appearing. Conjunctivitis was absent. Her mucous membranes were dry, with easily removable white and yellowish deposits on the buccal mucosa. No lesions or ulcerations were present. Dermatologic exam demonstrated confluent scaly, violaceous erythematous patches and plaques covering 60% of the total body surface area with focal areas that were denuded. Large areas of denuded skin were present over the back, inframammary folds, and underneath her abdominal pannus (Figures 1 and 2). Nikolsky's sign was present. She was oriented to person only.
Initial laboratory studies were significant for the following: white blood cell count = 12,800 cells/mm3, hemoglobin = 7.3 g/dL, creatinine = 11.2 mg/dL, blood urea nitrogen = 136 mg/dL, and bicarbonate level = 15 mmol/L. She was admitted to the medical intensive care unit for presumed sepsis. Aggressive resuscitation and broad spectrum antibiotics were administered. A thorough workup for infection, including blood and urine cultures, chest radiography, and lumbar puncture, was unremarkable. Antinuclear antibodies (ANAs) were present in a 1:2560 titer; with a nucleolar and speckled pattern and cytoplasmic antibodies. Additional rheumatologic workup revealed positive anti‐Smith antibody and weakly positive antiribonuclear protein antibody. Pathology from a punch biopsy performed by a dermatology consultant on hospital day 2 demonstrated full‐thickness skin necrosis with scant perivascular infiltrate. While the patient's family had disposed of the pill containers, they had kept several pills. These were sent for analysis, which did not reveal contamination with heavy metals or allopathic medications.
The patient was ultimately diagnosed with TEN and systemic lupus erythematosus with overlap syndrome, and intravenous methylprednisolone was administered. Broad‐spectrum antibiotics were administered for 48 hours, but stopped after workup for infection proved unrevealing. Wound care was mupirocin ointment with petrolatum dressings twice daily as per the hospital's TEN protocol. The patient's course was complicated by acidosis requiring hemodialysis and several tonic‐clonic seizures, a result of presumed lupus cerebritis due to rapidly progressive lesions on serial magnetic resonance images (MRIs) with a negative lumbar puncture. Renal biopsy demonstrated acute tubular necrosis and collapsing glomerulopathy. The patient ultimately recovered, and was discharged to a rehabilitation facility. In follow‐up several months later, she had healing skin with residual dyspigmentation and normal renal function. She was ambulatory and fully oriented, but complained of persistent memory difficulties.
Discussion
While use of complementary or alternative medicine (CAM) is widespread, physicians often underestimate the prevalence of CAM use in their patients. Only one‐half of primary care practitioners are aware of the risk for serious adverse reactions from CAMs.1 This case demonstrates the need for hospitalists to obtain a thorough medication history, including probing for CAM use, when evaluating a new patient. The delayed diagnosis of TEN, whether due to failure to elicit CAM use or recognize the clinical presentation, delayed appropriate treatment by a week and this patient developed potentially lethal complications.
Stevens‐Johnson syndrome (SJS) and TEN lie on a spectrum of disorders involving separation of the epidermis from the dermis when tension is applied to the skin, associated with mucositis, conjunctivitis, and generalized toxicity. The rash is dusky and erythematous, and Nikolsky's sign (separation of the epidermis from the dermis with tension applied to the skin) is present. These entities most commonly develop secondary to medications or infections. Most reactions occur within 60 days of drug initiation. The rash progressives over 1 to 15 days, and the rate of healing is variable. The overall mortality is 30% and is predicted by the SCORTEN system, which incorporates laboratory data, patient history, and the extent of skin breakdown.2 Treatment is primarily supportive; the use of corticosteroids, nonsteroidal immunosuppressive agents, intravenous immunoglobulin (IVIG), or plasmapheresis remains controversial.3
Case reports have described the development of SJS or TEN with CAM use. For example, 1 patient repeatedly developed SJS, with each episode occurring after exposure to an herbal medication containing red clover, burdock, queen's delight, poke root, prickly ash, sassafras bark, and passion flower.4 Similar to our case, identifying the exact agent responsible for TEN was impossible due to large numbers of herbal medications combined into a single pill. SJS and TEN are not limited to Western herbal medicines. Traditional Chinese medications are one of the most common causes of SJS and TEN in East Asia,5 although adulteration with allopathic medications is common in this setting. Ayurvedic medications,6 an ophiopogonis‐containing health drink,7 ginseng,8 and Gingko biloba9, 10 have also been implicated.
Conclusions
This case demonstrates the difficulty in making a diagnosis of CAM‐induced toxicity and identifying the likely agent responsible. Hospitalists must have a high index of suspicion of CAM‐associated toxicity to make this diagnosis, especially when admitting patients who may not volunteer CAM use without direct questioning.
Acknowledgements
This case was initially presented at the Midwest Society of General Internal Medicine regional meeting on September 2526, 2008. Figures 1 and 2 are courtesy of Dr. Robert Chen. The authors thank Dr. James Rhee from the Section of Emergency Medicine at the University of Chicago, who provided toxicology consultation and assisted with toxicology analysis. The authors also acknowledge Meryl Prochaska for manuscript preparation and the patient and her family for their courage and tenacity during the recovery process.
A 49‐year‐old woman with history of rheumatic fever necessitating mechanical mitral valve replacement and a cerebrovascular accident of presumed embolic etiology presented with several months of progressive fatigue, weakness, arthralgias, and myalgias. After an extensive workup, a rheumatologist in the community diagnosed her with systemic lupus erythematosus and dermatomyositis. The patient refused therapy with corticosteroids and disease‐modifying agents, citing concerns of adverse effects. She consulted a naturopathic clinician, who gave her Rejuvenator Pills, Super Booster pill, Genesis Juice, and alkaline water (Table 1).
| Rejuvenator Pill |
| Slippery elm 45 mg (Ulmus rubra) |
| Capsicum 40 mg (Capsicum spp.) |
| Fennel seeds 35 mg (Foeniculum vulgare) |
| Chickweed 35 mg (Stellaria media) |
| Hawthorn berry 30 mg (Crataegus oxyacantha) |
| Mullein 30 mg (Verbascum thapsus) |
| Scullcap 25 mg (Scutellaria spp.) |
| Rosehip 25 mg (Rosa spp.) |
| Barberry 20 mg (Berberis vulgaris) |
| Pau d'arco 20 mg (Tabebuia spp.) |
| Comfrey leaf 20 mg (Symphytum officinale) |
| Alfalfa 20 mg (Medicago sativa) |
| Kelp 20 mg (Laminaria spp.) |
| Papaya leaf 15 mg (Carica papaya) |
| Bee pollen 15 mg |
| Black cohosh 15 mg (Cimicifuga racemosa) |
| Chaparral 10 mg (Larrea tridentata) |
| Ginger 10 mg (Zingiber officinale) |
| Dandelion 5 mg (Taraxacum officinale) |
| Sunflower 5 mg (Helianthus annuus) |
| Licorice root 5 mg (Glycyrrhiza glabra) |
| Cascara sagrada 25 mg |
| Super Booster pill |
| Cascara sagrada |
| Psyllium (Plantago spp.) |
| Fennel (Foeniculum vulgare) |
| Genesis Juice |
| Apple (Malus domestica) |
| Pomegranate (Punica granatum) |
| Aloe vera juice (reconstituted) |
| Whole fruit grape extract (Vitis vinifera spp.) |
| Barley grass (Hordeum vulgare) |
| Cinnamon bark (Cinnamomum spp.) |
| Coriander leaf (Coriandrum sativum) |
| Coriander seed (Coriandrum sativum) |
| Cucumber (Cucumis sativus) |
| Fig fruit (Ficus carica) |
| Garlic bulb (Allium sativum) |
| Juniper berry (Juniperus spp.) |
| Leek (Allium ampeloprasum) |
| Lentil (Lens culinaris) |
| Mulberry fruit (Morus spp.) |
| Olive leaf (Olea europaea) |
| Onion bulb (Allium cepa) |
| Sweet almond (Prunus amygdalus dulcis) |
| Wheat grass (Triticum aestivum) |
| Alkaline water |
Several weeks later, the patient developed dusky erythematous plaques on her anterior and posterior trunk, face, and proximal extremities. Over the next several weeks, she became progressively weak until she was ultimately bedbound. The plaques over her back began to denude. Upon admission to an outside hospital, she was diagnosed with warfarin‐related skin necrosis, superinfected decubitus ulcers, and severe anemia. She refused blood transfusion, and was discharged home with clindamycin and iron. After her clinical status deteriorated over the subsequent week, she arrived at our hospital by ambulance.
In addition to the herbal medications she had recently started, she had been taking warfarin, furosemide, nitroglycerin via skin patch, and aspirin for over 10 years. On exam, she was febrile, tachycardic, hypotensive, and toxic‐appearing. Conjunctivitis was absent. Her mucous membranes were dry, with easily removable white and yellowish deposits on the buccal mucosa. No lesions or ulcerations were present. Dermatologic exam demonstrated confluent scaly, violaceous erythematous patches and plaques covering 60% of the total body surface area with focal areas that were denuded. Large areas of denuded skin were present over the back, inframammary folds, and underneath her abdominal pannus (Figures 1 and 2). Nikolsky's sign was present. She was oriented to person only.
Initial laboratory studies were significant for the following: white blood cell count = 12,800 cells/mm3, hemoglobin = 7.3 g/dL, creatinine = 11.2 mg/dL, blood urea nitrogen = 136 mg/dL, and bicarbonate level = 15 mmol/L. She was admitted to the medical intensive care unit for presumed sepsis. Aggressive resuscitation and broad spectrum antibiotics were administered. A thorough workup for infection, including blood and urine cultures, chest radiography, and lumbar puncture, was unremarkable. Antinuclear antibodies (ANAs) were present in a 1:2560 titer; with a nucleolar and speckled pattern and cytoplasmic antibodies. Additional rheumatologic workup revealed positive anti‐Smith antibody and weakly positive antiribonuclear protein antibody. Pathology from a punch biopsy performed by a dermatology consultant on hospital day 2 demonstrated full‐thickness skin necrosis with scant perivascular infiltrate. While the patient's family had disposed of the pill containers, they had kept several pills. These were sent for analysis, which did not reveal contamination with heavy metals or allopathic medications.
The patient was ultimately diagnosed with TEN and systemic lupus erythematosus with overlap syndrome, and intravenous methylprednisolone was administered. Broad‐spectrum antibiotics were administered for 48 hours, but stopped after workup for infection proved unrevealing. Wound care was mupirocin ointment with petrolatum dressings twice daily as per the hospital's TEN protocol. The patient's course was complicated by acidosis requiring hemodialysis and several tonic‐clonic seizures, a result of presumed lupus cerebritis due to rapidly progressive lesions on serial magnetic resonance images (MRIs) with a negative lumbar puncture. Renal biopsy demonstrated acute tubular necrosis and collapsing glomerulopathy. The patient ultimately recovered, and was discharged to a rehabilitation facility. In follow‐up several months later, she had healing skin with residual dyspigmentation and normal renal function. She was ambulatory and fully oriented, but complained of persistent memory difficulties.
Discussion
While use of complementary or alternative medicine (CAM) is widespread, physicians often underestimate the prevalence of CAM use in their patients. Only one‐half of primary care practitioners are aware of the risk for serious adverse reactions from CAMs.1 This case demonstrates the need for hospitalists to obtain a thorough medication history, including probing for CAM use, when evaluating a new patient. The delayed diagnosis of TEN, whether due to failure to elicit CAM use or recognize the clinical presentation, delayed appropriate treatment by a week and this patient developed potentially lethal complications.
Stevens‐Johnson syndrome (SJS) and TEN lie on a spectrum of disorders involving separation of the epidermis from the dermis when tension is applied to the skin, associated with mucositis, conjunctivitis, and generalized toxicity. The rash is dusky and erythematous, and Nikolsky's sign (separation of the epidermis from the dermis with tension applied to the skin) is present. These entities most commonly develop secondary to medications or infections. Most reactions occur within 60 days of drug initiation. The rash progressives over 1 to 15 days, and the rate of healing is variable. The overall mortality is 30% and is predicted by the SCORTEN system, which incorporates laboratory data, patient history, and the extent of skin breakdown.2 Treatment is primarily supportive; the use of corticosteroids, nonsteroidal immunosuppressive agents, intravenous immunoglobulin (IVIG), or plasmapheresis remains controversial.3
Case reports have described the development of SJS or TEN with CAM use. For example, 1 patient repeatedly developed SJS, with each episode occurring after exposure to an herbal medication containing red clover, burdock, queen's delight, poke root, prickly ash, sassafras bark, and passion flower.4 Similar to our case, identifying the exact agent responsible for TEN was impossible due to large numbers of herbal medications combined into a single pill. SJS and TEN are not limited to Western herbal medicines. Traditional Chinese medications are one of the most common causes of SJS and TEN in East Asia,5 although adulteration with allopathic medications is common in this setting. Ayurvedic medications,6 an ophiopogonis‐containing health drink,7 ginseng,8 and Gingko biloba9, 10 have also been implicated.
Conclusions
This case demonstrates the difficulty in making a diagnosis of CAM‐induced toxicity and identifying the likely agent responsible. Hospitalists must have a high index of suspicion of CAM‐associated toxicity to make this diagnosis, especially when admitting patients who may not volunteer CAM use without direct questioning.
Acknowledgements
This case was initially presented at the Midwest Society of General Internal Medicine regional meeting on September 2526, 2008. Figures 1 and 2 are courtesy of Dr. Robert Chen. The authors thank Dr. James Rhee from the Section of Emergency Medicine at the University of Chicago, who provided toxicology consultation and assisted with toxicology analysis. The authors also acknowledge Meryl Prochaska for manuscript preparation and the patient and her family for their courage and tenacity during the recovery process.
- ,,,.A survey of primary care physicians' perceptions of their patients' use of complementary medicine.Complement Ther Med.2003;11(4):254–260.
- ,,,,,.SCORTEN: a severity‐of‐illness score for toxic epidermal necrolysis.J Invest Dermatol.2000;115(2):149–153.
- ,,.Toxic epidermal necrolysis.J Am Acad Dermatol.2007;56(2):181–200.
- .Severe cutaneous reactions to alternative remedies.Br Med J.1986;293(6548):665–666.
- ,.Toxic epidermal necrolysis in a burns centre: a 6‐year review.Burns.1996;22(4):275–258.
- ,,,,.Herbal medicine induced Stevens‐Johnson syndrome: a case report.Int J Paediatr Dent.2004;14(3):204–207.
- ,,,,.Stevens‐Johnson syndrome caused by a health drink (Eberu) containing ophiopogonis tuber.J Dermatol.1998;25(10):662–665.
- ,,,,.Ginseng as a cause for Stevens‐Johnson syndrome?Lancet.1996;347:1344.
- ,.Stevens‐Johnson syndrome with Ginkgo biloba.J Herbal Pharmacother.2001;1(3):65–69.
- ,,, et al.[Stevens‐Johnson syndrome/toxic epidermal necrolysis treated with intravenous immunoglobulins].Actas Dermosifiliogr.2005;96(9):589–592. [Spanish].
- ,,,.A survey of primary care physicians' perceptions of their patients' use of complementary medicine.Complement Ther Med.2003;11(4):254–260.
- ,,,,,.SCORTEN: a severity‐of‐illness score for toxic epidermal necrolysis.J Invest Dermatol.2000;115(2):149–153.
- ,,.Toxic epidermal necrolysis.J Am Acad Dermatol.2007;56(2):181–200.
- .Severe cutaneous reactions to alternative remedies.Br Med J.1986;293(6548):665–666.
- ,.Toxic epidermal necrolysis in a burns centre: a 6‐year review.Burns.1996;22(4):275–258.
- ,,,,.Herbal medicine induced Stevens‐Johnson syndrome: a case report.Int J Paediatr Dent.2004;14(3):204–207.
- ,,,,.Stevens‐Johnson syndrome caused by a health drink (Eberu) containing ophiopogonis tuber.J Dermatol.1998;25(10):662–665.
- ,,,,.Ginseng as a cause for Stevens‐Johnson syndrome?Lancet.1996;347:1344.
- ,.Stevens‐Johnson syndrome with Ginkgo biloba.J Herbal Pharmacother.2001;1(3):65–69.
- ,,, et al.[Stevens‐Johnson syndrome/toxic epidermal necrolysis treated with intravenous immunoglobulins].Actas Dermosifiliogr.2005;96(9):589–592. [Spanish].

A Multiple Choice Answer?
A 49‐year‐old man with a history of hypertension presented to our hospital with a 2‐week history of sharp pain in the right upper abdomen and right lower chest radiating to the back. The patient reported a few days of fevers, chills, drenching night sweats, shortness of breath, malaise, and fatigue. He denied recent travel. Vital signs were temperature 38.4C, blood pressure 119/74 mmHg, heart rate 95 beats/minutes, respiratory rate 16 breaths/minutes, and oxygen saturation 96% on 5 L nasal cannula. Physical examination revealed poor dentition, right upper abdominal quadrant tenderness, and dullness to percussion over the right lung base.
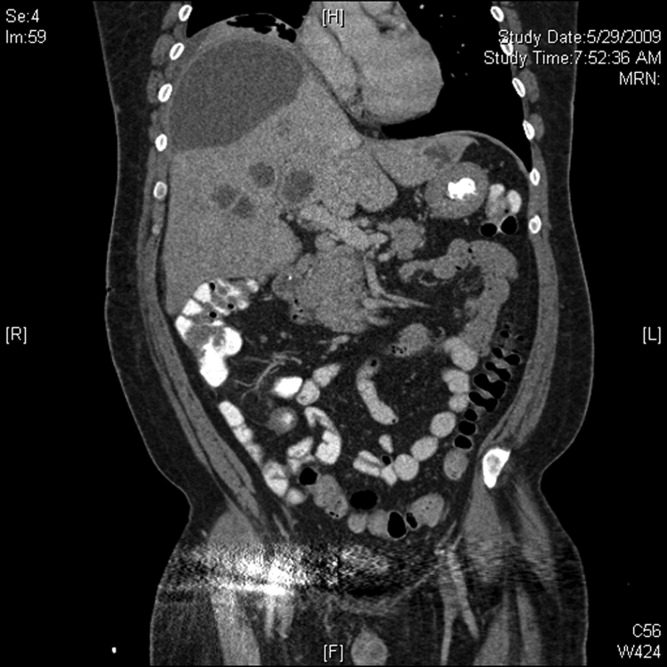
Initial labs showed white blood count (WBC) 22,540/mm3, alkaline phosphatase 280 units/L, bilirubin 1.1 mg/dL, aspartate aminotransferase (AST) 28 units/L, alanine aminotransferase (ALT) 33 units/L. Blood cultures were negative. An human immunodeficiency virus (HIV)1/HIV2 antibody screen was negative. Computed tomography (CT) of the chest demonstrated a large cystic lesion in the diaphragmatic dome of the liver with multiple lesions in the right lobe of the liver. Elevation of the right hemidiaphragm and moderate right pleural effusion were noted. CT abdomen showed multiple areas of fluid collection within the liver suspicious for liver abscesses (see Figure 1). Multiple gallstones were seen within gallbladder with a large stone in the region of the gallbladder neck vs. cystic duct without evidence of extrahepatic biliary dilatation. There was mild distention of the appendix with minimal soft tissue stranding.
The patient underwent ultrasound‐guided drainage of the largest liver abscess. Cultures from the aspiration grew Fusobacterium nucleatum. The patient's stool studies for ova and parasites were negative. The patient was started on piperacillin/tazobactam and metronidazole, then switched to ertapenem. A hepatobiliary iminodiacetic acid (HIDA) scan confirmed cholecystitis, and the patient underwent open cholecystectomy. Pathology on the gallbladder returned as chronic cholecystitis with cholelithiasis. A full dental examination revealed possible periapical abscesses of teeth #12 and #30 and stringent daily oral hygiene was recommended. Tooth extraction was initially recommended but ultimately postponed. Plans were made for dental follow‐up.
With continued antibiotic treatment, the patient's fevers resolved and leukocytosis improved. A follow‐up CT abdomen/pelvis obtained on hospital day 10 showed a reduction in size of the multiple liver abscesses. There was also increased prominence of the appendix with mild stranding. The patient was taken for appendectomy. Pathology was consistent with acute appendicitis with focal fat necrosis. The patient was ultimately discharged with the plan being to continue ertapenem until radiographic resolution of all the abscesses was demonstrated.
Discussion
Pyogenic liver abscesses are infrequently encountered in the western population, but when present, result in significant morbidity and mortality.1 Mortality rates range from 6% to 31%, decreased from 100% mortality in the preantibiotic era.1 The leading cause of pyogenic liver abscesses has been in the past ascribed to ruptured appendicitis.2 However, biliary tract pathology is now the leading cause, accounting for 43% to 60% of cases.2 In addition, hematogenous seeding of infection from the oral cavity has been recognized in the literature as a potential source of infection in the development of pyogenic liver abscesses.2
The empiric treatment of pyogenic liver abscesses is intravenous broad‐spectrum antibiotics, most commonly metronidazole in combination with quinolones, aminoglycosides, third generation cephalosporins, carbapenems, piperacillin/tazobactam, ampicillin‐sulbactam, or amoxicillin/clavulanate.1 The optimal treatment course is controversial but suggested to include 2 weeks to 3 weeks of intravenous antibiotics followed by at least 3 weeks to 4 weeks of oral antibiotics.1
According to a study of 84 patients hospitalized with pyogenic liver abscesses of which 70 cases were cultured, the most typical organisms isolated from liver abscesses are Streptococcus spp. (40.5%), Escherichia coli (27.4%), Klebsiella spp. (14.3%), and anaerobic organisms (17.9%).1 The anaerobic Gram‐negative bacterium Fusobacterium nucleatum, known to play a role in periodontal disease, is an uncommon cause of liver abscesses: a review of the literature revealed only 14 cases of liver abscesses caused by Fusobacterium nucleatum, five cases of which occurred in patients with known immunodeficiency, and a retrospective study of 70 cases of liver abscesses revealed only 2 cases linked to this bacterium.1, 2 Though accounting for a minority of cases of pyogenic liver abscesses, it is commonly cited as a cause of liver abscesses resulting from spread of infection from the oral cavity. Four case reports have implicated severe dental disease or recent dental work in the development of pyogenic liver abscesses involving Fusobacterium nucleatum.2 For example, a literature search revealed a case report of a patient with a liver abscess due to Fusobacterium nucleatum resulting from hematogenous spread of infection from the oral cavity.2
Although Fusobacterium has rarely been reported in biliary culture from patients with cholangitis or gangrenous cholecystitis,3 this organism has been identified as a causative organism in appendicitis. In two separate studies of 41 children with appendicitis and 30 patients older than 12 years with gangrenous or perforated appendicitis, Fusobacterium nucleatum or Fusobacterium spp. were isolated in 44% and 33% of cases, respectively.4, 5 Nevertheless, the mechanism of appendicitis causing liver abscesses is thought to be by direct spread via the peritoneum after perforation.2 Thus, despite the isolation of this bacterium from appendectomy specimens, appendicitis is less likely the source of infection in this patient given that there is no evidence that appendiceal perforation occurred in this case.
Our patient was found to have dental abscesses, cholecystitis requiring cholecystectomy, and appendicitis requiring appendectomyall of which, to varying degrees, were plausible sources of infection by virtue of their known role in the development of pyogenic liver abscesses. Although periodontal disease was the likely source of Fusobacterium nucleatum infection, we could not exclude the leading causes of pyogenic liver abscesses, appendicitis and/or biliary tract disease. As a result, the patient underwent 2 surgeries and was counseled to maintain good oral hygiene in order to eliminate all persisting sources of infection.
This was an unusual case in which the question What is the source of infection? appears to have had multiple correct answers. We theorize that leaving any 1 of the 3 possible sources of infection in place could have led to treatment failure. This patient is a humbling reminder that not every clinical problem will have one clear solution. In such cases, all possible underlying conditions need to be managed appropriately to achieve the desired outcome.
- ,,,,,.Pyogenic liver abscesses: mortality‐related factors.Eur J Gastroenterol Hepatol.2007;19:853–858.
- ,,, et al.Pyogenic liver abscess related to dental disease in an immunocompetent host.Intern Med.2008;47:675–678.
- ,,,.Gangrenous cholecystitis and acute cholangitis associated with anaerobic bacteria in bile.Eur J Clin Microbiol.1986;5:35–39.
- ,,,,.Bacteriology of histopathologically defined appendicitis in children.Ped Infect Dis J.2000;19:1078–1083.
- ,,, et al.The bacteriology of gangrenous and perforated appendicitis—revisited.Ann Surg.1990;211:165–171.
A 49‐year‐old man with a history of hypertension presented to our hospital with a 2‐week history of sharp pain in the right upper abdomen and right lower chest radiating to the back. The patient reported a few days of fevers, chills, drenching night sweats, shortness of breath, malaise, and fatigue. He denied recent travel. Vital signs were temperature 38.4C, blood pressure 119/74 mmHg, heart rate 95 beats/minutes, respiratory rate 16 breaths/minutes, and oxygen saturation 96% on 5 L nasal cannula. Physical examination revealed poor dentition, right upper abdominal quadrant tenderness, and dullness to percussion over the right lung base.
Initial labs showed white blood count (WBC) 22,540/mm3, alkaline phosphatase 280 units/L, bilirubin 1.1 mg/dL, aspartate aminotransferase (AST) 28 units/L, alanine aminotransferase (ALT) 33 units/L. Blood cultures were negative. An human immunodeficiency virus (HIV)1/HIV2 antibody screen was negative. Computed tomography (CT) of the chest demonstrated a large cystic lesion in the diaphragmatic dome of the liver with multiple lesions in the right lobe of the liver. Elevation of the right hemidiaphragm and moderate right pleural effusion were noted. CT abdomen showed multiple areas of fluid collection within the liver suspicious for liver abscesses (see Figure 1). Multiple gallstones were seen within gallbladder with a large stone in the region of the gallbladder neck vs. cystic duct without evidence of extrahepatic biliary dilatation. There was mild distention of the appendix with minimal soft tissue stranding.
The patient underwent ultrasound‐guided drainage of the largest liver abscess. Cultures from the aspiration grew Fusobacterium nucleatum. The patient's stool studies for ova and parasites were negative. The patient was started on piperacillin/tazobactam and metronidazole, then switched to ertapenem. A hepatobiliary iminodiacetic acid (HIDA) scan confirmed cholecystitis, and the patient underwent open cholecystectomy. Pathology on the gallbladder returned as chronic cholecystitis with cholelithiasis. A full dental examination revealed possible periapical abscesses of teeth #12 and #30 and stringent daily oral hygiene was recommended. Tooth extraction was initially recommended but ultimately postponed. Plans were made for dental follow‐up.
With continued antibiotic treatment, the patient's fevers resolved and leukocytosis improved. A follow‐up CT abdomen/pelvis obtained on hospital day 10 showed a reduction in size of the multiple liver abscesses. There was also increased prominence of the appendix with mild stranding. The patient was taken for appendectomy. Pathology was consistent with acute appendicitis with focal fat necrosis. The patient was ultimately discharged with the plan being to continue ertapenem until radiographic resolution of all the abscesses was demonstrated.
Discussion
Pyogenic liver abscesses are infrequently encountered in the western population, but when present, result in significant morbidity and mortality.1 Mortality rates range from 6% to 31%, decreased from 100% mortality in the preantibiotic era.1 The leading cause of pyogenic liver abscesses has been in the past ascribed to ruptured appendicitis.2 However, biliary tract pathology is now the leading cause, accounting for 43% to 60% of cases.2 In addition, hematogenous seeding of infection from the oral cavity has been recognized in the literature as a potential source of infection in the development of pyogenic liver abscesses.2
The empiric treatment of pyogenic liver abscesses is intravenous broad‐spectrum antibiotics, most commonly metronidazole in combination with quinolones, aminoglycosides, third generation cephalosporins, carbapenems, piperacillin/tazobactam, ampicillin‐sulbactam, or amoxicillin/clavulanate.1 The optimal treatment course is controversial but suggested to include 2 weeks to 3 weeks of intravenous antibiotics followed by at least 3 weeks to 4 weeks of oral antibiotics.1
According to a study of 84 patients hospitalized with pyogenic liver abscesses of which 70 cases were cultured, the most typical organisms isolated from liver abscesses are Streptococcus spp. (40.5%), Escherichia coli (27.4%), Klebsiella spp. (14.3%), and anaerobic organisms (17.9%).1 The anaerobic Gram‐negative bacterium Fusobacterium nucleatum, known to play a role in periodontal disease, is an uncommon cause of liver abscesses: a review of the literature revealed only 14 cases of liver abscesses caused by Fusobacterium nucleatum, five cases of which occurred in patients with known immunodeficiency, and a retrospective study of 70 cases of liver abscesses revealed only 2 cases linked to this bacterium.1, 2 Though accounting for a minority of cases of pyogenic liver abscesses, it is commonly cited as a cause of liver abscesses resulting from spread of infection from the oral cavity. Four case reports have implicated severe dental disease or recent dental work in the development of pyogenic liver abscesses involving Fusobacterium nucleatum.2 For example, a literature search revealed a case report of a patient with a liver abscess due to Fusobacterium nucleatum resulting from hematogenous spread of infection from the oral cavity.2
Although Fusobacterium has rarely been reported in biliary culture from patients with cholangitis or gangrenous cholecystitis,3 this organism has been identified as a causative organism in appendicitis. In two separate studies of 41 children with appendicitis and 30 patients older than 12 years with gangrenous or perforated appendicitis, Fusobacterium nucleatum or Fusobacterium spp. were isolated in 44% and 33% of cases, respectively.4, 5 Nevertheless, the mechanism of appendicitis causing liver abscesses is thought to be by direct spread via the peritoneum after perforation.2 Thus, despite the isolation of this bacterium from appendectomy specimens, appendicitis is less likely the source of infection in this patient given that there is no evidence that appendiceal perforation occurred in this case.
Our patient was found to have dental abscesses, cholecystitis requiring cholecystectomy, and appendicitis requiring appendectomyall of which, to varying degrees, were plausible sources of infection by virtue of their known role in the development of pyogenic liver abscesses. Although periodontal disease was the likely source of Fusobacterium nucleatum infection, we could not exclude the leading causes of pyogenic liver abscesses, appendicitis and/or biliary tract disease. As a result, the patient underwent 2 surgeries and was counseled to maintain good oral hygiene in order to eliminate all persisting sources of infection.
This was an unusual case in which the question What is the source of infection? appears to have had multiple correct answers. We theorize that leaving any 1 of the 3 possible sources of infection in place could have led to treatment failure. This patient is a humbling reminder that not every clinical problem will have one clear solution. In such cases, all possible underlying conditions need to be managed appropriately to achieve the desired outcome.
A 49‐year‐old man with a history of hypertension presented to our hospital with a 2‐week history of sharp pain in the right upper abdomen and right lower chest radiating to the back. The patient reported a few days of fevers, chills, drenching night sweats, shortness of breath, malaise, and fatigue. He denied recent travel. Vital signs were temperature 38.4C, blood pressure 119/74 mmHg, heart rate 95 beats/minutes, respiratory rate 16 breaths/minutes, and oxygen saturation 96% on 5 L nasal cannula. Physical examination revealed poor dentition, right upper abdominal quadrant tenderness, and dullness to percussion over the right lung base.
Initial labs showed white blood count (WBC) 22,540/mm3, alkaline phosphatase 280 units/L, bilirubin 1.1 mg/dL, aspartate aminotransferase (AST) 28 units/L, alanine aminotransferase (ALT) 33 units/L. Blood cultures were negative. An human immunodeficiency virus (HIV)1/HIV2 antibody screen was negative. Computed tomography (CT) of the chest demonstrated a large cystic lesion in the diaphragmatic dome of the liver with multiple lesions in the right lobe of the liver. Elevation of the right hemidiaphragm and moderate right pleural effusion were noted. CT abdomen showed multiple areas of fluid collection within the liver suspicious for liver abscesses (see Figure 1). Multiple gallstones were seen within gallbladder with a large stone in the region of the gallbladder neck vs. cystic duct without evidence of extrahepatic biliary dilatation. There was mild distention of the appendix with minimal soft tissue stranding.
The patient underwent ultrasound‐guided drainage of the largest liver abscess. Cultures from the aspiration grew Fusobacterium nucleatum. The patient's stool studies for ova and parasites were negative. The patient was started on piperacillin/tazobactam and metronidazole, then switched to ertapenem. A hepatobiliary iminodiacetic acid (HIDA) scan confirmed cholecystitis, and the patient underwent open cholecystectomy. Pathology on the gallbladder returned as chronic cholecystitis with cholelithiasis. A full dental examination revealed possible periapical abscesses of teeth #12 and #30 and stringent daily oral hygiene was recommended. Tooth extraction was initially recommended but ultimately postponed. Plans were made for dental follow‐up.
With continued antibiotic treatment, the patient's fevers resolved and leukocytosis improved. A follow‐up CT abdomen/pelvis obtained on hospital day 10 showed a reduction in size of the multiple liver abscesses. There was also increased prominence of the appendix with mild stranding. The patient was taken for appendectomy. Pathology was consistent with acute appendicitis with focal fat necrosis. The patient was ultimately discharged with the plan being to continue ertapenem until radiographic resolution of all the abscesses was demonstrated.
Discussion
Pyogenic liver abscesses are infrequently encountered in the western population, but when present, result in significant morbidity and mortality.1 Mortality rates range from 6% to 31%, decreased from 100% mortality in the preantibiotic era.1 The leading cause of pyogenic liver abscesses has been in the past ascribed to ruptured appendicitis.2 However, biliary tract pathology is now the leading cause, accounting for 43% to 60% of cases.2 In addition, hematogenous seeding of infection from the oral cavity has been recognized in the literature as a potential source of infection in the development of pyogenic liver abscesses.2
The empiric treatment of pyogenic liver abscesses is intravenous broad‐spectrum antibiotics, most commonly metronidazole in combination with quinolones, aminoglycosides, third generation cephalosporins, carbapenems, piperacillin/tazobactam, ampicillin‐sulbactam, or amoxicillin/clavulanate.1 The optimal treatment course is controversial but suggested to include 2 weeks to 3 weeks of intravenous antibiotics followed by at least 3 weeks to 4 weeks of oral antibiotics.1
According to a study of 84 patients hospitalized with pyogenic liver abscesses of which 70 cases were cultured, the most typical organisms isolated from liver abscesses are Streptococcus spp. (40.5%), Escherichia coli (27.4%), Klebsiella spp. (14.3%), and anaerobic organisms (17.9%).1 The anaerobic Gram‐negative bacterium Fusobacterium nucleatum, known to play a role in periodontal disease, is an uncommon cause of liver abscesses: a review of the literature revealed only 14 cases of liver abscesses caused by Fusobacterium nucleatum, five cases of which occurred in patients with known immunodeficiency, and a retrospective study of 70 cases of liver abscesses revealed only 2 cases linked to this bacterium.1, 2 Though accounting for a minority of cases of pyogenic liver abscesses, it is commonly cited as a cause of liver abscesses resulting from spread of infection from the oral cavity. Four case reports have implicated severe dental disease or recent dental work in the development of pyogenic liver abscesses involving Fusobacterium nucleatum.2 For example, a literature search revealed a case report of a patient with a liver abscess due to Fusobacterium nucleatum resulting from hematogenous spread of infection from the oral cavity.2
Although Fusobacterium has rarely been reported in biliary culture from patients with cholangitis or gangrenous cholecystitis,3 this organism has been identified as a causative organism in appendicitis. In two separate studies of 41 children with appendicitis and 30 patients older than 12 years with gangrenous or perforated appendicitis, Fusobacterium nucleatum or Fusobacterium spp. were isolated in 44% and 33% of cases, respectively.4, 5 Nevertheless, the mechanism of appendicitis causing liver abscesses is thought to be by direct spread via the peritoneum after perforation.2 Thus, despite the isolation of this bacterium from appendectomy specimens, appendicitis is less likely the source of infection in this patient given that there is no evidence that appendiceal perforation occurred in this case.
Our patient was found to have dental abscesses, cholecystitis requiring cholecystectomy, and appendicitis requiring appendectomyall of which, to varying degrees, were plausible sources of infection by virtue of their known role in the development of pyogenic liver abscesses. Although periodontal disease was the likely source of Fusobacterium nucleatum infection, we could not exclude the leading causes of pyogenic liver abscesses, appendicitis and/or biliary tract disease. As a result, the patient underwent 2 surgeries and was counseled to maintain good oral hygiene in order to eliminate all persisting sources of infection.
This was an unusual case in which the question What is the source of infection? appears to have had multiple correct answers. We theorize that leaving any 1 of the 3 possible sources of infection in place could have led to treatment failure. This patient is a humbling reminder that not every clinical problem will have one clear solution. In such cases, all possible underlying conditions need to be managed appropriately to achieve the desired outcome.
- ,,,,,.Pyogenic liver abscesses: mortality‐related factors.Eur J Gastroenterol Hepatol.2007;19:853–858.
- ,,, et al.Pyogenic liver abscess related to dental disease in an immunocompetent host.Intern Med.2008;47:675–678.
- ,,,.Gangrenous cholecystitis and acute cholangitis associated with anaerobic bacteria in bile.Eur J Clin Microbiol.1986;5:35–39.
- ,,,,.Bacteriology of histopathologically defined appendicitis in children.Ped Infect Dis J.2000;19:1078–1083.
- ,,, et al.The bacteriology of gangrenous and perforated appendicitis—revisited.Ann Surg.1990;211:165–171.
- ,,,,,.Pyogenic liver abscesses: mortality‐related factors.Eur J Gastroenterol Hepatol.2007;19:853–858.
- ,,, et al.Pyogenic liver abscess related to dental disease in an immunocompetent host.Intern Med.2008;47:675–678.
- ,,,.Gangrenous cholecystitis and acute cholangitis associated with anaerobic bacteria in bile.Eur J Clin Microbiol.1986;5:35–39.
- ,,,,.Bacteriology of histopathologically defined appendicitis in children.Ped Infect Dis J.2000;19:1078–1083.
- ,,, et al.The bacteriology of gangrenous and perforated appendicitis—revisited.Ann Surg.1990;211:165–171.

Malignant Otitis Externa
Malignant Otitis Externa (MOE) is a necrotizing infection of the external auditory canal characterized by extension into nearby soft tissue and bony structures that can potentially lead to mastoiditis, skull base osteomyelitis, cranial nerve palsies, and rarely, intracranial complications. MOE has been classically described as a disease affecting elderly diabetics1 and has been reported in immunocompromised patients with acquired immune deficiency syndrome (AIDS), malignancy, patients receiving chemotherapy, and neutropenic children.24 The incidence of MOE in the general population is estimated to be quite low and difficult to determine.5 However, over the past decades, the number of reported cases has been increasing, suggesting increased awareness of this syndrome by primary care physicians.6
Case Report
A 56‐year‐old white male was brought to the emergency department with altered mental status including decreased level of consciousness, bizarre behavior, headaches, and nausea for several weeks. He had a history of alcohol and cocaine abuse. He was homeless and a smoker. On examination, the patient was lethargic, disoriented with respect to time, place and person. Blood pressure was 107/72 mm Hg, heart rate 85 beats per minute; respirations were 16 per minute and temperature was 97.9F. Neurological examination was significant for loss of vision of the left eye and left facial peripheral nerve palsy. Examination of the left eye showed yellowish‐greenish discharge, a lower lid ectropium with upper lid ptosis, conjunctival erythema, and an 8 mm 6 mm abrasion in the medial half of the cornea. He had purulent drainage from the left ear with small vesicular lesions on the auricle, and a 3 cm 4 cm abscess on the right forearm. The remainder of the physical examination was unremarkable.
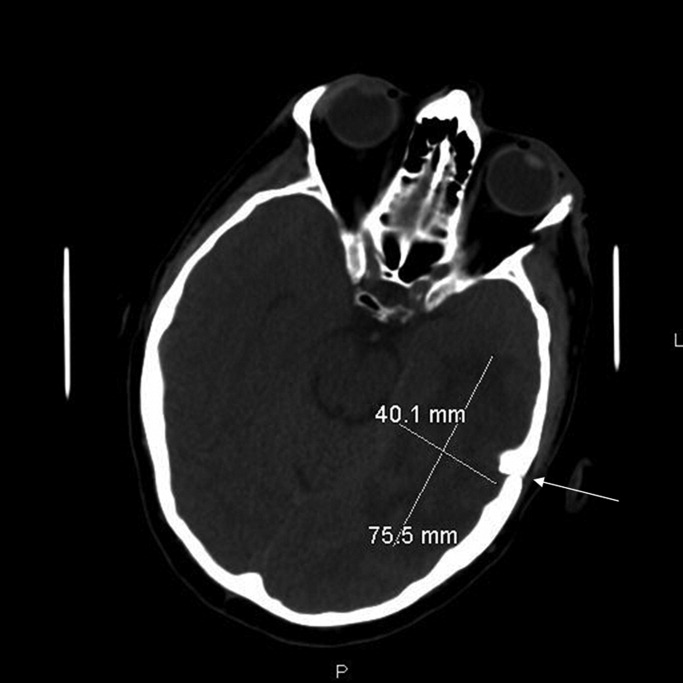
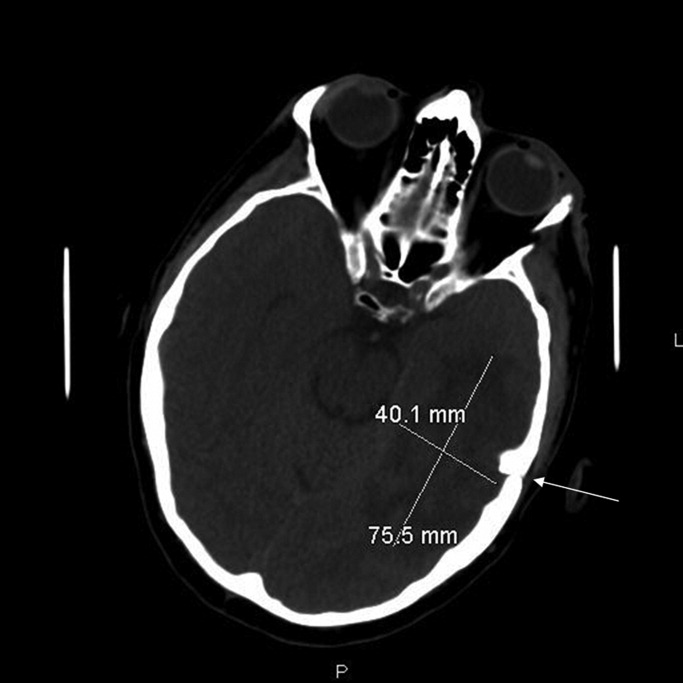
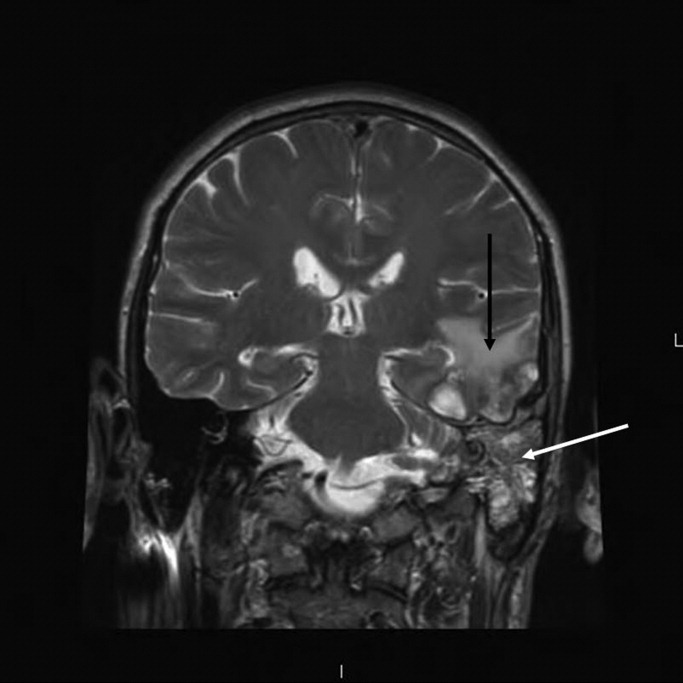
Laboratory‐test results showed white blood cell (WBC) count; 11.27 109 cells/L with 76.6% neutrophils. A complete metabolic panel was within normal limits. Human immunodeficiency virus (HIV) and RPR testing were negative. Cerebrospinal fluid (CSF) studies demonstrated a WBC 39 cells/mm3 with lymphocytes predominance (85%), Red blood cell (RBC) 6 cells/mm3, protein 48 mg/dL, and glucose; 63 mg/dL. Computed tomographic scan of the head revealed an area of low attenuation with surrounding edema of the left temporal lobe and fracture of the temporal bone on the superior margin of the mastoid air cells extending into the left mastoid air cells (Figure 1). The fluid draining from the patient's left ear grew 2 different strains of Pseudomonas aeruginosa. Magnetic resonance imaging (MRI) of the brain demonstrated a 2.5 cm to 3.0 cm region of multiple loculations and edema in the left temporal lobe representing cerebritis with abscess and complete opacification of left mastoid air cell suggestive of mastoiditis (Figure 2). Piperacillin/tazobactam and tobramycin were initiated for suspected MOE with brain involvement. CSF and blood cultures were negative.
A repeat MRI at 3 weeks of therapy demonstrated interval improvement in the temporal lobe abscess and the edema surrounding the infection. At the time of discharge, after 6 weeks of antimicrobial therapy, the patient was alert and oriented with respect to person, place, and time.
Discussion
Pseudomonas aeruginosa is the most common organism cultured from MOE.4, 5 Other organisms such as Staphylococcus aureus,6 Proteus mirabilis, Klebsiella oxytocea,7 and Aspergillus species8 have been reported as well.
While the exact pathogenesis of MOE is poorly understood, accidental trauma from cotton swabs, exposure to lake water, swimming pool water, and repeated aural lavage have all been implicated as inciting factors.9 The current literature suggests that Pseudomonal otitis externa occurs due to abnormal host defense mechanisms rather than enhanced pathogen colonization.10
MOE typically presents with severe otalgia, headache, auricular tenderness, mastoid tenderness, or persistent otorrhea. The pain of MOE is usually severe, and the classic signs of infection such as fever, leukocytosis and neutrophil predominance (left shift) may not be present.5 The diagnosis can be confirmed by otoscopic exam which will demonstrate granulation tissue at the junction between the bony and cartilaginous tissues in the external auditory canal. MOE can produce certain physical findings that should raise red flags for local extension. Temporomandibular joint pain in the susceptible patient with otalgia could indicate MOE with joint invasion. Cranial nerve involvement, most commonly involves the seventh cranial nerve which results in a facial palsy. Other cranial neuropathies have been reported in MOE such as the glossopharyngeal, vagal, spinal accessory, and hypoglossal nerves.11 Confusion and nuchal rigidity should arouse suspicion of intracranial extension of the infection.
The diagnosis of MOE is usually made by a constellation of clinical, microbiological and radiological features. The first attempt at defining diagnostic criteria for MOE was in 1987, when Cohen and Friedman named several obligatory signs such as pain, exudate, edema, granulation tissue in the external ear canal, the presence of microabscesses if surgery is performed, and either a positive Tc‐99m bone scan or failure of local treatment for 1 week.12
Recent literature reviews emphasize that a positive bacterial or fungal culture of the external ear canal can help make the diagnosis of MOE.4 A recent study looking at diagnostic criteria noted that MOE may be present even without meeting all of these major criteria (clinical, microbiological, and radiological features).13 Some authors suggest that ear biopsy be considered if malignancy is a reasonable possibility.9
Other laboratory data can be within normal limits, such as a WBC count or differential and metabolic profiles.4 Erythrocyte sedimentation rate (ESR), while non‐specific, has been reported to be markedly increased in the setting of MOE.5 It is recommended that a baseline ESR be obtained, and then used to follow the response to treatment.14
Computed tomography (CT) scanning is considered the appropriate initial imaging study, however, there are mixed reports about whether a CT scan alone is enough to evaluate disease severity and its complications.15 While CT scan is quite sensitive for demonstrating bony destruction associated with MOE, MRI is better at detecting the soft tissue changes associated with MOE and more useful for following disease resolution after treatment.16
The treatment of MOE has evolved over time. Before the introduction of effective anti‐pseudomonal antibiotics, MOE had an associated mortality near 50%, and surgery was the recommended therapy.17 Currently, given the availability of effective anti‐pseudomonal therapy, there is usually no indication for surgery as a primary treatment in MOE. For sensitive pseudomonal species, oral Ciprofloxacin therapy for 6 to 8 weeks is considered the treatment of choice for MOE.18 Clinicians should be aware of the emergence of quinolone resistance in P. Aeruginosa,19 and antibiotic sensitivities should be performed on the culture to guide further treatment. In the setting of resistant or multi‐species infection, one should obtain external ear canal biopsy with wound debridement and begin long‐term intravenous therapy with an antipseudomonal beta‐lactam plus an aminoglycoside.18 In the setting of extension into the cranium causing cerebritis or abscess, it is recommended that a neurosurgeon be consulted immediately to determine whether the lesion is amenable to aspiration, excision, or watchful waiting with imaging follow up.
This case illustrates a serious complication from MOE, with ipsilateral facial nerve palsy, opthalmitis, mastoiditis, and cerebral abscess that was successfully treated with conservative medical management.
- .Malignant external otitis.Laryngoscope.1968;78:1257.
- ,,, et al.Necrotizing external otitis in patients with AIDS.Laryngoscope.1997;107:456.
- ,,,.Malignant external otitis in an infant.J Laryngol Otol.1990;104(6):488–490.
- ,,.The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations.Lancet Infect Dis.2004;4:34.
- ,.Malignant external otitis: insights into pathogenesis, clinical manifestations, diagnosis, and therapy.Am J Med.1988;85:391.
- ,,Staphylococcal malignant external otitis.Can Med Assoc J.1982;126:155.
- ,,, et al.A case of malignant external otitis involving Klebsiella oxytoca.Eur J Clin Microbiol Infect Dis.1992;11:75.
- ,.Invasive otitis externa due to Aspergillus species: case report and review.Clin Infect Dis.1994;19:866.
- ,.Necrotizing (malignant) external otitis.Am Fam Physician.2003;68(2):309–312.
- ,,,.Bacterial flora of the external canal in diabetics and non‐diabetics.Laryngoscope.1982;92:672.
- ,,.Neurologic complications of malignant external otitis.Neurology.1971;21:1077–1084.
- ,.The diagnostic criteria of malignant external otitis.J Laryngol Otol.1987;101:216–221.
- ,,,,.Stratification for malignant external otitis.Otolaryngol Head Neck Surg.2007;137(2):301–305.
- ,,,,,.Efficacy of oral ciprofloxacin plus rifampin for treatment of malignant external otitis.Arch Otolaryngol Head Neck Surg.1989;115:1063–1069.
- ,,,,,.Usefulness of CT scans in malignant external otitis: effective tool for the diagnosis, but of limited value in predicting outcome.Eur Arch Otorhinolaryngol.2008;265(1):53–56.
- ,,.Use of magnetic resonance imaging as the primary imaging modality in the diagnosis and follow‐up of malignant external otitis.J Laryngol Otol.2004;118:576.
- ,.Skull base osteomyelitis. Malignant external otitis.Otolaryngol Clin North Am.1996;29(5):795–806.
- .Ciprofloxacin: an oral quinolone for the treatment of infections with gram‐negative pathogens. Committee on Antimicrobial Agents. Canadian Infectious Disease Society.Can Med Assoc J.1994;150(5):669–676.
- ,,,.Resistance of Pseudomonas to ciprofloxacin: implications for the treatment of malignant otitis externa.J Laryngol Otol.2007;121:118–123.
Malignant Otitis Externa (MOE) is a necrotizing infection of the external auditory canal characterized by extension into nearby soft tissue and bony structures that can potentially lead to mastoiditis, skull base osteomyelitis, cranial nerve palsies, and rarely, intracranial complications. MOE has been classically described as a disease affecting elderly diabetics1 and has been reported in immunocompromised patients with acquired immune deficiency syndrome (AIDS), malignancy, patients receiving chemotherapy, and neutropenic children.24 The incidence of MOE in the general population is estimated to be quite low and difficult to determine.5 However, over the past decades, the number of reported cases has been increasing, suggesting increased awareness of this syndrome by primary care physicians.6
Case Report
A 56‐year‐old white male was brought to the emergency department with altered mental status including decreased level of consciousness, bizarre behavior, headaches, and nausea for several weeks. He had a history of alcohol and cocaine abuse. He was homeless and a smoker. On examination, the patient was lethargic, disoriented with respect to time, place and person. Blood pressure was 107/72 mm Hg, heart rate 85 beats per minute; respirations were 16 per minute and temperature was 97.9F. Neurological examination was significant for loss of vision of the left eye and left facial peripheral nerve palsy. Examination of the left eye showed yellowish‐greenish discharge, a lower lid ectropium with upper lid ptosis, conjunctival erythema, and an 8 mm 6 mm abrasion in the medial half of the cornea. He had purulent drainage from the left ear with small vesicular lesions on the auricle, and a 3 cm 4 cm abscess on the right forearm. The remainder of the physical examination was unremarkable.
Laboratory‐test results showed white blood cell (WBC) count; 11.27 109 cells/L with 76.6% neutrophils. A complete metabolic panel was within normal limits. Human immunodeficiency virus (HIV) and RPR testing were negative. Cerebrospinal fluid (CSF) studies demonstrated a WBC 39 cells/mm3 with lymphocytes predominance (85%), Red blood cell (RBC) 6 cells/mm3, protein 48 mg/dL, and glucose; 63 mg/dL. Computed tomographic scan of the head revealed an area of low attenuation with surrounding edema of the left temporal lobe and fracture of the temporal bone on the superior margin of the mastoid air cells extending into the left mastoid air cells (Figure 1). The fluid draining from the patient's left ear grew 2 different strains of Pseudomonas aeruginosa. Magnetic resonance imaging (MRI) of the brain demonstrated a 2.5 cm to 3.0 cm region of multiple loculations and edema in the left temporal lobe representing cerebritis with abscess and complete opacification of left mastoid air cell suggestive of mastoiditis (Figure 2). Piperacillin/tazobactam and tobramycin were initiated for suspected MOE with brain involvement. CSF and blood cultures were negative.
A repeat MRI at 3 weeks of therapy demonstrated interval improvement in the temporal lobe abscess and the edema surrounding the infection. At the time of discharge, after 6 weeks of antimicrobial therapy, the patient was alert and oriented with respect to person, place, and time.
Discussion
Pseudomonas aeruginosa is the most common organism cultured from MOE.4, 5 Other organisms such as Staphylococcus aureus,6 Proteus mirabilis, Klebsiella oxytocea,7 and Aspergillus species8 have been reported as well.
While the exact pathogenesis of MOE is poorly understood, accidental trauma from cotton swabs, exposure to lake water, swimming pool water, and repeated aural lavage have all been implicated as inciting factors.9 The current literature suggests that Pseudomonal otitis externa occurs due to abnormal host defense mechanisms rather than enhanced pathogen colonization.10
MOE typically presents with severe otalgia, headache, auricular tenderness, mastoid tenderness, or persistent otorrhea. The pain of MOE is usually severe, and the classic signs of infection such as fever, leukocytosis and neutrophil predominance (left shift) may not be present.5 The diagnosis can be confirmed by otoscopic exam which will demonstrate granulation tissue at the junction between the bony and cartilaginous tissues in the external auditory canal. MOE can produce certain physical findings that should raise red flags for local extension. Temporomandibular joint pain in the susceptible patient with otalgia could indicate MOE with joint invasion. Cranial nerve involvement, most commonly involves the seventh cranial nerve which results in a facial palsy. Other cranial neuropathies have been reported in MOE such as the glossopharyngeal, vagal, spinal accessory, and hypoglossal nerves.11 Confusion and nuchal rigidity should arouse suspicion of intracranial extension of the infection.
The diagnosis of MOE is usually made by a constellation of clinical, microbiological and radiological features. The first attempt at defining diagnostic criteria for MOE was in 1987, when Cohen and Friedman named several obligatory signs such as pain, exudate, edema, granulation tissue in the external ear canal, the presence of microabscesses if surgery is performed, and either a positive Tc‐99m bone scan or failure of local treatment for 1 week.12
Recent literature reviews emphasize that a positive bacterial or fungal culture of the external ear canal can help make the diagnosis of MOE.4 A recent study looking at diagnostic criteria noted that MOE may be present even without meeting all of these major criteria (clinical, microbiological, and radiological features).13 Some authors suggest that ear biopsy be considered if malignancy is a reasonable possibility.9
Other laboratory data can be within normal limits, such as a WBC count or differential and metabolic profiles.4 Erythrocyte sedimentation rate (ESR), while non‐specific, has been reported to be markedly increased in the setting of MOE.5 It is recommended that a baseline ESR be obtained, and then used to follow the response to treatment.14
Computed tomography (CT) scanning is considered the appropriate initial imaging study, however, there are mixed reports about whether a CT scan alone is enough to evaluate disease severity and its complications.15 While CT scan is quite sensitive for demonstrating bony destruction associated with MOE, MRI is better at detecting the soft tissue changes associated with MOE and more useful for following disease resolution after treatment.16
The treatment of MOE has evolved over time. Before the introduction of effective anti‐pseudomonal antibiotics, MOE had an associated mortality near 50%, and surgery was the recommended therapy.17 Currently, given the availability of effective anti‐pseudomonal therapy, there is usually no indication for surgery as a primary treatment in MOE. For sensitive pseudomonal species, oral Ciprofloxacin therapy for 6 to 8 weeks is considered the treatment of choice for MOE.18 Clinicians should be aware of the emergence of quinolone resistance in P. Aeruginosa,19 and antibiotic sensitivities should be performed on the culture to guide further treatment. In the setting of resistant or multi‐species infection, one should obtain external ear canal biopsy with wound debridement and begin long‐term intravenous therapy with an antipseudomonal beta‐lactam plus an aminoglycoside.18 In the setting of extension into the cranium causing cerebritis or abscess, it is recommended that a neurosurgeon be consulted immediately to determine whether the lesion is amenable to aspiration, excision, or watchful waiting with imaging follow up.
This case illustrates a serious complication from MOE, with ipsilateral facial nerve palsy, opthalmitis, mastoiditis, and cerebral abscess that was successfully treated with conservative medical management.
Malignant Otitis Externa (MOE) is a necrotizing infection of the external auditory canal characterized by extension into nearby soft tissue and bony structures that can potentially lead to mastoiditis, skull base osteomyelitis, cranial nerve palsies, and rarely, intracranial complications. MOE has been classically described as a disease affecting elderly diabetics1 and has been reported in immunocompromised patients with acquired immune deficiency syndrome (AIDS), malignancy, patients receiving chemotherapy, and neutropenic children.24 The incidence of MOE in the general population is estimated to be quite low and difficult to determine.5 However, over the past decades, the number of reported cases has been increasing, suggesting increased awareness of this syndrome by primary care physicians.6
Case Report
A 56‐year‐old white male was brought to the emergency department with altered mental status including decreased level of consciousness, bizarre behavior, headaches, and nausea for several weeks. He had a history of alcohol and cocaine abuse. He was homeless and a smoker. On examination, the patient was lethargic, disoriented with respect to time, place and person. Blood pressure was 107/72 mm Hg, heart rate 85 beats per minute; respirations were 16 per minute and temperature was 97.9F. Neurological examination was significant for loss of vision of the left eye and left facial peripheral nerve palsy. Examination of the left eye showed yellowish‐greenish discharge, a lower lid ectropium with upper lid ptosis, conjunctival erythema, and an 8 mm 6 mm abrasion in the medial half of the cornea. He had purulent drainage from the left ear with small vesicular lesions on the auricle, and a 3 cm 4 cm abscess on the right forearm. The remainder of the physical examination was unremarkable.
Laboratory‐test results showed white blood cell (WBC) count; 11.27 109 cells/L with 76.6% neutrophils. A complete metabolic panel was within normal limits. Human immunodeficiency virus (HIV) and RPR testing were negative. Cerebrospinal fluid (CSF) studies demonstrated a WBC 39 cells/mm3 with lymphocytes predominance (85%), Red blood cell (RBC) 6 cells/mm3, protein 48 mg/dL, and glucose; 63 mg/dL. Computed tomographic scan of the head revealed an area of low attenuation with surrounding edema of the left temporal lobe and fracture of the temporal bone on the superior margin of the mastoid air cells extending into the left mastoid air cells (Figure 1). The fluid draining from the patient's left ear grew 2 different strains of Pseudomonas aeruginosa. Magnetic resonance imaging (MRI) of the brain demonstrated a 2.5 cm to 3.0 cm region of multiple loculations and edema in the left temporal lobe representing cerebritis with abscess and complete opacification of left mastoid air cell suggestive of mastoiditis (Figure 2). Piperacillin/tazobactam and tobramycin were initiated for suspected MOE with brain involvement. CSF and blood cultures were negative.
A repeat MRI at 3 weeks of therapy demonstrated interval improvement in the temporal lobe abscess and the edema surrounding the infection. At the time of discharge, after 6 weeks of antimicrobial therapy, the patient was alert and oriented with respect to person, place, and time.
Discussion
Pseudomonas aeruginosa is the most common organism cultured from MOE.4, 5 Other organisms such as Staphylococcus aureus,6 Proteus mirabilis, Klebsiella oxytocea,7 and Aspergillus species8 have been reported as well.
While the exact pathogenesis of MOE is poorly understood, accidental trauma from cotton swabs, exposure to lake water, swimming pool water, and repeated aural lavage have all been implicated as inciting factors.9 The current literature suggests that Pseudomonal otitis externa occurs due to abnormal host defense mechanisms rather than enhanced pathogen colonization.10
MOE typically presents with severe otalgia, headache, auricular tenderness, mastoid tenderness, or persistent otorrhea. The pain of MOE is usually severe, and the classic signs of infection such as fever, leukocytosis and neutrophil predominance (left shift) may not be present.5 The diagnosis can be confirmed by otoscopic exam which will demonstrate granulation tissue at the junction between the bony and cartilaginous tissues in the external auditory canal. MOE can produce certain physical findings that should raise red flags for local extension. Temporomandibular joint pain in the susceptible patient with otalgia could indicate MOE with joint invasion. Cranial nerve involvement, most commonly involves the seventh cranial nerve which results in a facial palsy. Other cranial neuropathies have been reported in MOE such as the glossopharyngeal, vagal, spinal accessory, and hypoglossal nerves.11 Confusion and nuchal rigidity should arouse suspicion of intracranial extension of the infection.
The diagnosis of MOE is usually made by a constellation of clinical, microbiological and radiological features. The first attempt at defining diagnostic criteria for MOE was in 1987, when Cohen and Friedman named several obligatory signs such as pain, exudate, edema, granulation tissue in the external ear canal, the presence of microabscesses if surgery is performed, and either a positive Tc‐99m bone scan or failure of local treatment for 1 week.12
Recent literature reviews emphasize that a positive bacterial or fungal culture of the external ear canal can help make the diagnosis of MOE.4 A recent study looking at diagnostic criteria noted that MOE may be present even without meeting all of these major criteria (clinical, microbiological, and radiological features).13 Some authors suggest that ear biopsy be considered if malignancy is a reasonable possibility.9
Other laboratory data can be within normal limits, such as a WBC count or differential and metabolic profiles.4 Erythrocyte sedimentation rate (ESR), while non‐specific, has been reported to be markedly increased in the setting of MOE.5 It is recommended that a baseline ESR be obtained, and then used to follow the response to treatment.14
Computed tomography (CT) scanning is considered the appropriate initial imaging study, however, there are mixed reports about whether a CT scan alone is enough to evaluate disease severity and its complications.15 While CT scan is quite sensitive for demonstrating bony destruction associated with MOE, MRI is better at detecting the soft tissue changes associated with MOE and more useful for following disease resolution after treatment.16
The treatment of MOE has evolved over time. Before the introduction of effective anti‐pseudomonal antibiotics, MOE had an associated mortality near 50%, and surgery was the recommended therapy.17 Currently, given the availability of effective anti‐pseudomonal therapy, there is usually no indication for surgery as a primary treatment in MOE. For sensitive pseudomonal species, oral Ciprofloxacin therapy for 6 to 8 weeks is considered the treatment of choice for MOE.18 Clinicians should be aware of the emergence of quinolone resistance in P. Aeruginosa,19 and antibiotic sensitivities should be performed on the culture to guide further treatment. In the setting of resistant or multi‐species infection, one should obtain external ear canal biopsy with wound debridement and begin long‐term intravenous therapy with an antipseudomonal beta‐lactam plus an aminoglycoside.18 In the setting of extension into the cranium causing cerebritis or abscess, it is recommended that a neurosurgeon be consulted immediately to determine whether the lesion is amenable to aspiration, excision, or watchful waiting with imaging follow up.
This case illustrates a serious complication from MOE, with ipsilateral facial nerve palsy, opthalmitis, mastoiditis, and cerebral abscess that was successfully treated with conservative medical management.
- .Malignant external otitis.Laryngoscope.1968;78:1257.
- ,,, et al.Necrotizing external otitis in patients with AIDS.Laryngoscope.1997;107:456.
- ,,,.Malignant external otitis in an infant.J Laryngol Otol.1990;104(6):488–490.
- ,,.The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations.Lancet Infect Dis.2004;4:34.
- ,.Malignant external otitis: insights into pathogenesis, clinical manifestations, diagnosis, and therapy.Am J Med.1988;85:391.
- ,,Staphylococcal malignant external otitis.Can Med Assoc J.1982;126:155.
- ,,, et al.A case of malignant external otitis involving Klebsiella oxytoca.Eur J Clin Microbiol Infect Dis.1992;11:75.
- ,.Invasive otitis externa due to Aspergillus species: case report and review.Clin Infect Dis.1994;19:866.
- ,.Necrotizing (malignant) external otitis.Am Fam Physician.2003;68(2):309–312.
- ,,,.Bacterial flora of the external canal in diabetics and non‐diabetics.Laryngoscope.1982;92:672.
- ,,.Neurologic complications of malignant external otitis.Neurology.1971;21:1077–1084.
- ,.The diagnostic criteria of malignant external otitis.J Laryngol Otol.1987;101:216–221.
- ,,,,.Stratification for malignant external otitis.Otolaryngol Head Neck Surg.2007;137(2):301–305.
- ,,,,,.Efficacy of oral ciprofloxacin plus rifampin for treatment of malignant external otitis.Arch Otolaryngol Head Neck Surg.1989;115:1063–1069.
- ,,,,,.Usefulness of CT scans in malignant external otitis: effective tool for the diagnosis, but of limited value in predicting outcome.Eur Arch Otorhinolaryngol.2008;265(1):53–56.
- ,,.Use of magnetic resonance imaging as the primary imaging modality in the diagnosis and follow‐up of malignant external otitis.J Laryngol Otol.2004;118:576.
- ,.Skull base osteomyelitis. Malignant external otitis.Otolaryngol Clin North Am.1996;29(5):795–806.
- .Ciprofloxacin: an oral quinolone for the treatment of infections with gram‐negative pathogens. Committee on Antimicrobial Agents. Canadian Infectious Disease Society.Can Med Assoc J.1994;150(5):669–676.
- ,,,.Resistance of Pseudomonas to ciprofloxacin: implications for the treatment of malignant otitis externa.J Laryngol Otol.2007;121:118–123.
- .Malignant external otitis.Laryngoscope.1968;78:1257.
- ,,, et al.Necrotizing external otitis in patients with AIDS.Laryngoscope.1997;107:456.
- ,,,.Malignant external otitis in an infant.J Laryngol Otol.1990;104(6):488–490.
- ,,.The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations.Lancet Infect Dis.2004;4:34.
- ,.Malignant external otitis: insights into pathogenesis, clinical manifestations, diagnosis, and therapy.Am J Med.1988;85:391.
- ,,Staphylococcal malignant external otitis.Can Med Assoc J.1982;126:155.
- ,,, et al.A case of malignant external otitis involving Klebsiella oxytoca.Eur J Clin Microbiol Infect Dis.1992;11:75.
- ,.Invasive otitis externa due to Aspergillus species: case report and review.Clin Infect Dis.1994;19:866.
- ,.Necrotizing (malignant) external otitis.Am Fam Physician.2003;68(2):309–312.
- ,,,.Bacterial flora of the external canal in diabetics and non‐diabetics.Laryngoscope.1982;92:672.
- ,,.Neurologic complications of malignant external otitis.Neurology.1971;21:1077–1084.
- ,.The diagnostic criteria of malignant external otitis.J Laryngol Otol.1987;101:216–221.
- ,,,,.Stratification for malignant external otitis.Otolaryngol Head Neck Surg.2007;137(2):301–305.
- ,,,,,.Efficacy of oral ciprofloxacin plus rifampin for treatment of malignant external otitis.Arch Otolaryngol Head Neck Surg.1989;115:1063–1069.
- ,,,,,.Usefulness of CT scans in malignant external otitis: effective tool for the diagnosis, but of limited value in predicting outcome.Eur Arch Otorhinolaryngol.2008;265(1):53–56.
- ,,.Use of magnetic resonance imaging as the primary imaging modality in the diagnosis and follow‐up of malignant external otitis.J Laryngol Otol.2004;118:576.
- ,.Skull base osteomyelitis. Malignant external otitis.Otolaryngol Clin North Am.1996;29(5):795–806.
- .Ciprofloxacin: an oral quinolone for the treatment of infections with gram‐negative pathogens. Committee on Antimicrobial Agents. Canadian Infectious Disease Society.Can Med Assoc J.1994;150(5):669–676.
- ,,,.Resistance of Pseudomonas to ciprofloxacin: implications for the treatment of malignant otitis externa.J Laryngol Otol.2007;121:118–123.