User login
Extensive Tumoral Calcinosis in a Patient With Systemic Sclerosis
Rash Around a New Tatoo...
The way to a man's heart is through his liver
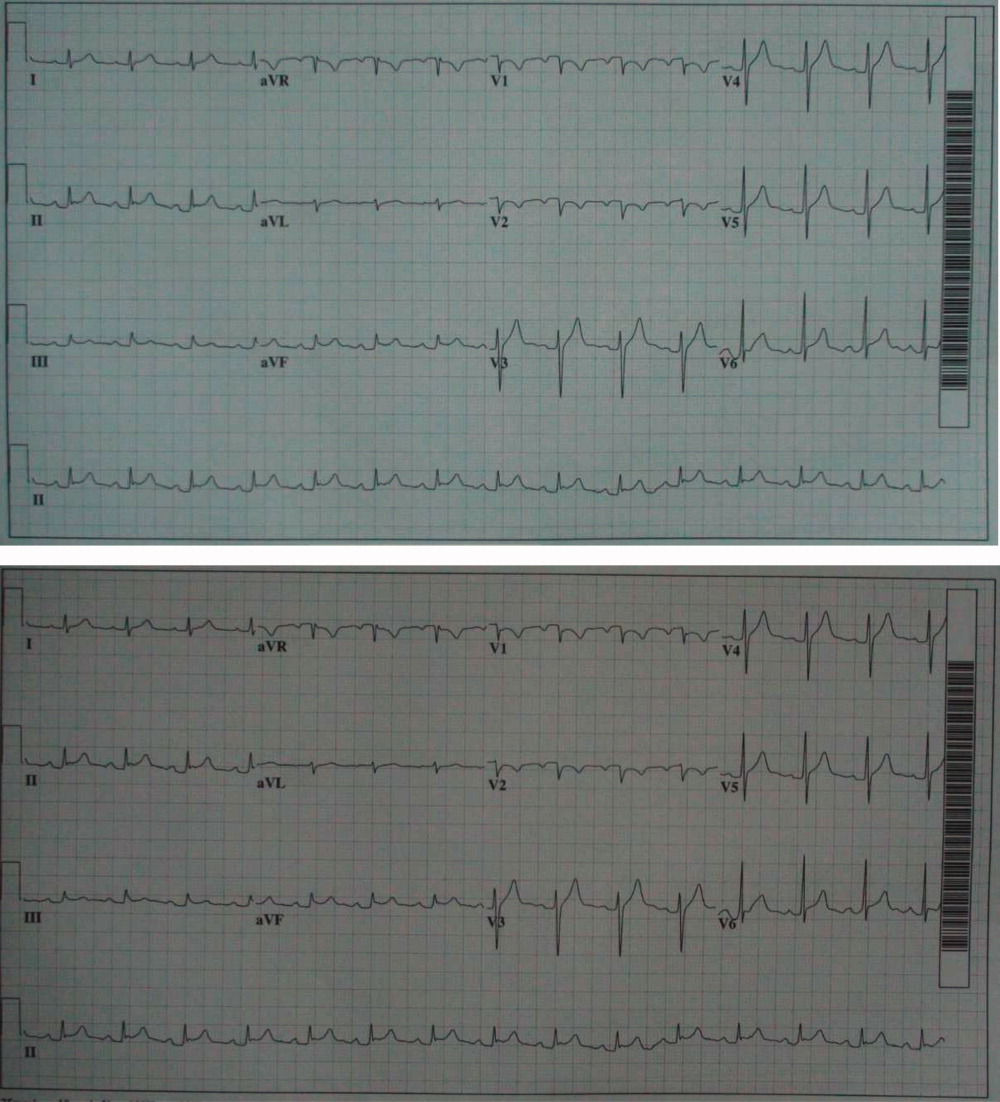
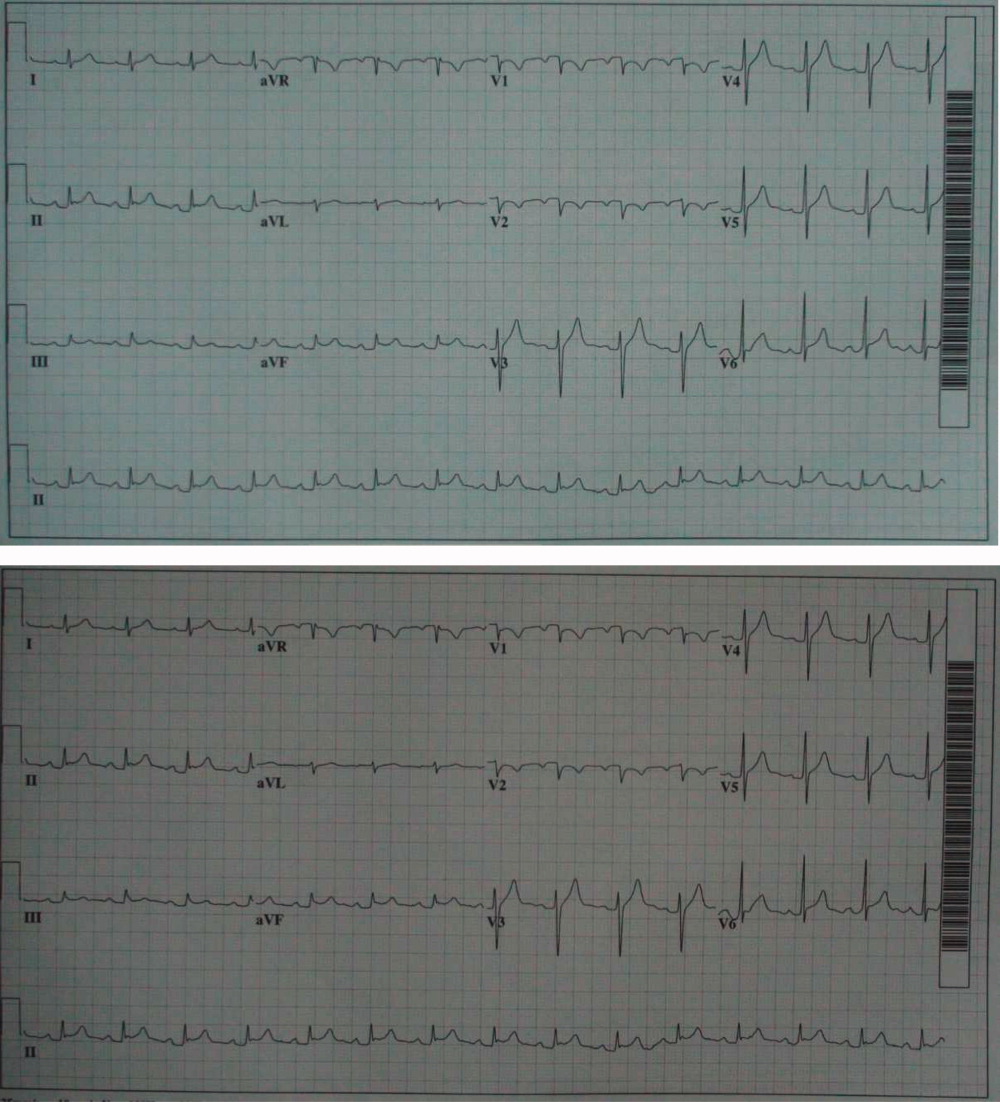
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0

Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0
Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0
Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.
The renal failure that vanished
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
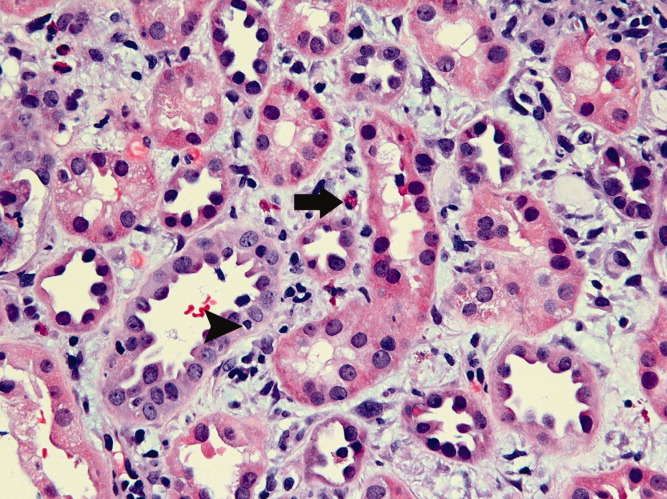
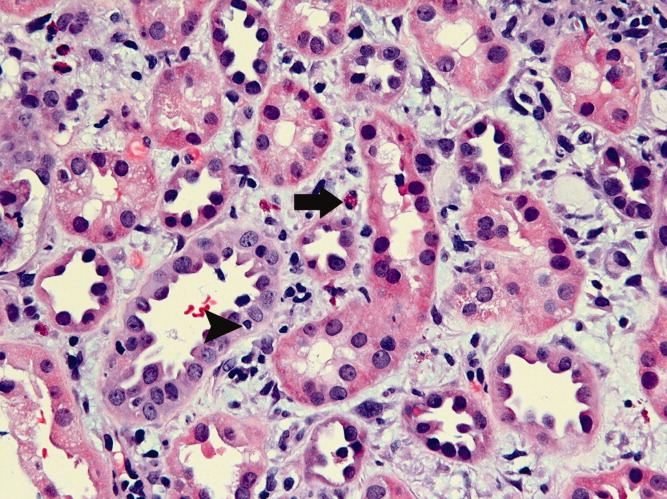
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
Diabetic Ketoacidosis as a Presentation of Hemochromatosis
Lesion on Scrotum
Hypotension and Seizure in a Healthy Young Woman
Florid Reactive Periostitis of the Hand
Combined Traumatic Occiput-C1 and C1-C2 Dissociation: 2 Case Reports
IHE Presenting as Chest Pain
Intramural hematoma of the esophagus (IHE) is a rare clinical entity. The majority of cases occur following esophageal instrumentation; however, other causes have been described.14 Rarely, IHE may develop spontaneously. We report a case of apparent spontaneous IHE (SIHE) in a patient presenting with acute‐onset chest pain and dysphagia who was taking low‐dose aspirin, bisphosphonate, and iron supplementation therapy. We highlight the evaluation of chest pain in these patients and the importance of considering the association between esophageal pathology and less commonly implicated medications which may increase the risk of esophageal injury.
Case Report
An 80‐year‐old Hispanic female with a history of osteoporosis, hypertension, and anemia presumed secondary to long‐standing noninsulin‐dependent diabetes mellitus presented with severe, abrupt‐onset, epigastric and retrosternal chest pain following ingestion of a banana. Home medications included aspirin (81 mg daily), alendronate (70 mg weekly), and ferrous sulfate (300 mg 3 times daily). She experienced nausea and minimal vomiting without hematemesis following the onset of pain. She admitted to several weeks of progressive dysphagia leading up to this event, but denied persistent vomiting, straining, foreign body ingestion, or trauma. At admission, the patient was afebrile with heart rate (HR) = 88, blood pressure (BP) = 172/88, pulse oximetry = 99% on room air, hemoglobin = 9.0 g/dL, hematocrit = 26.5%, platelets = 191,000, and international normalized ratio (INR) = 1.04. Electrocardiogram and cardiac enzymes were negative for myocardial infarction. Chest radiograph did not show a widened mediastinum. A computed tomography (CT) scan of the chest demonstrated diffuse thickening of the esophageal wall. Upper endoscopy demonstrated a large, purple, nonpulsatile submucosal mass protruding into and nearly occluding the esophageal lumen (Figure 1A). This mass extended 22 cm along the esophagus and terminated at the esophagogastric junction. There was suggestion of a potential distal mucosal tear and visible clot (Figure 1B, C). An endoscopy performed 6 years prior was unremarkable for esophagitis, stricture, mass, or hemorrhage.

The patient remained nil‐per‐os and was managed conservatively with intravenous fluids, antiemetics, and acid‐suppression therapy. Due to persistent odynophagia, the patient did not tolerate per‐os nutrition, and a percutaneous gastrostomy tube was placed nonendoscopically for temporary nutritional support. The patient's hospital stay was complicated by deep vein thrombosis of the right peroneal vein, for which she underwent inferior vena cava filter placement. She was discharged 18 days following admission. Alendronate and aspirin were discontinued and not reinitiated, and a follow‐up CT scan 6 weeks posthospitalization demonstrated complete resolution of the hematoma.
Discussion
Esophageal injuries include lacerations (Mallory‐Weiss syndrome), perforations (Boerhaave's syndrome), and hematomas (ie, IHE). IHE is by far the least common of these 3 pathologies and, despite increasing reports, it remains a rare clinical entity. Criblez et al.,4 in a review of 91 cases, found that only 35% of patients present with the classic triad of retrosternal chest pain, dysphagia/odynophagia, and hematemesis, while 99% present with at least 1 of these.5 Presentations mimic other cardiothoracic emergencies including myocardial infarction,6 pulmonary embolism,2 aortic dissection,6 and aortoesophageal fistula. Misdiagnosis of IHE and treatment with anticoagulant or thrombolytic therapy can have disastrous consequences, including death.5 Electrocardiograms, chest radiographs, and cardiac enzymes are often normal, as in this case. Endoscopy, performed cautiously, typically reveals a nonpulsatile, purple, submucosal mass. CT, which is rapid, noninvasive, and capable of differentiating between esophageal and life‐threatening thoracomediastinal pathology, frequently demonstrates thickening of the posterior wall of the esophagus with a long, smooth filling‐defect and luminal narrowing.7 Conservative management is the mainstay of treatment with most patients receiving acid suppression and antiemetic therapy. Surgical treatment and antibiotics (in cases of suspected infection) are required infrequently and should be used conservatively when necessary. The vast majority of patients recover spontaneously. Long‐term complications are rare.
IHE most frequently results from esophageal instrumentation, but other antecedent causes have been described. In contrast, SIHE occurs without warning, frequently developing in the absence of vomiting or hematemesis. Since SIHE was first reported in 1970,8 many authors have postulated potential mechanisms of hematoma formation. Controversy remains as to the precise etiology, but recent reports emphasize the association between SIHE and antiplatelet therapy, including low‐dose aspirin,9, 10 aspirin plus dipyridamole,11 and clopidogrel.12 Few studies have identified mechanisms for why the hemorrhage remains in the esophagus and why other parts of the gastrointestinal tract or other organ systems are not involved.
We report a case of apparent SIHE in a patient taking low‐dose aspirin, alendronate, and ferrous sulfate. While a subclinical traumatic event cannot be completely excluded, this patient lacked any apparent antecedent symptoms or other etiologic explanation. Alendronate and ferrous sulfate have been implicated in upper gastrointestinal irritation, but have not previously been associated with SIHE. Park et al.13 estimated a 3.0% incidence of esophageal or gastric events in alendronate users. Recently, esophagitis dissecans superficialis,3 esophageal dissection,14 and even fatal esophageal perforation16 have been reported in patients taking alendronate. Iron supplementation is also a recognized cause of esophageal injury. High local iron saturation may lead to concentration‐dependent absorption and thereby the formation of reactive oxygen metabolites and mucosal injury.16
We hypothesize that alendronate in combination with ferrous sulfate therapy resulted in subclinical esophageal injury predisposing our patient to SIHE. The patient reported 2 weeks of dysphagia prior to admission, suggesting a period of esophageal irritation. On endoscopy, a potential distal esophageal mucosal tear and clot were observed, which may represent a focus of injury. The interaction between this alendronate‐induced injury and chronic antiplatelet therapy may have resulted in hematoma expansion 22 cm along the esophagus. We are aware of one other report of IHE in a patient taking aspirin and alendronate published as an abstract in the Iranian Govaresh Journal.17
A spectrum of less‐commonly‐implicated medications may exert local toxicity on the esophagus and lead to de novo esophageal damage, predisposing patients to a broad spectrum of esophageal pathology, ranging from focal esophageal damage to large hematoma or perforation. Numerous medications are known to be associated with esophageal pathology through a variety of mechanisms (Table 1). Anatomic and motility disorders, as well as pill‐specific factors including contact time, coating materials, and sustained release formulations, may influence toxicity and predispose to injury.18 Elderly patients may be especially susceptible to the combined interactions between antiplatelet therapy and these commonly prescribed or over‐the‐counter medications.
| |
| Nonsteroidal antiinflammatory drugs | Aspirin, naproxen, ibuprofen |
| Bisphosphonates | Alendronate, etidronate, pamidronate |
| Antibiotics | Tetracycline, doxycycline, clindamycin, penicillin |
| Antiviral agents | Zalcitibine, zidovudine, nelfanavir |
| Chemotherapeutic agents | Dactinomycin, bleomycin, cytarabine, daunorubicin, 5‐fluorouracil, methotrexate, vincristine |
| Others | Ferrous sulfate, potassium chloride, ascorbic acid, multivitamins, quinidine, theophylline |
Conclusions
We report a case of apparent SIHE in an elderly woman taking low‐dose aspirin, iron, and alendronate therapy who presented with acute‐onset retrosternal chest pain and dysphagia. We emphasize the importance of including esophageal pathology in the evaluation of chest pain in these patients, particularly elderly women. We encourage a thorough examination of symptoms, including dysphagia/odynophagia, and an exhaustive medication history to identify medications less‐commonly implicated with esophageal pathology. In patients with chest pain taking these medications, clinicians must remain vigilant in their diagnostic approach to prevent misdiagnosis and inappropriate treatment.
Acknowledgements
The authors acknowledge and thank Dr. Sonal Singh for his assistance in helping to analyze the potential drug interactions involved in this case presentation.
- ,,.Post‐sclerotherapy intramural esophageal hematoma: endoscopic and radiologic findings.Gastrointest Endosc.1992;38:102–103.
- ,,.Esophageal hematoma. Four new cases, a review, and proposed etiology.Dig Dis Sci.1981;26:1019–1024.
- ,,.Spontaneous dissecting intramural hematoma of the oesophagus: a rare cause of haematemesis and dysphagia.Endoscopy.1981;13:128–130.
- ,,,,.Intramural rupture and intramural hematoma of the esophagus: 3 case reports and literature review.Schweiz Med Wochenschr.1992;122:416–423.
- ,.Dissecting intramural hematoma of the esophagus.Eur J Gastroenterol Hepatol.2000;12:1151–1161.
- ,,.Spontaneous intramural hematoma of the oesophagus: a report of three cases and review of the literature.Aust N Z J Surg.1994;64:190–193.
- ,,,,.Intramural hematoma of the esophagus: a pictorial essay.Emerg Radiol.2008;15(1):13–22.
- ,.Spontaneous cervico‐mediastinal haematoma.J Ir Med Assoc.1970;63:298.
- ,,,,,.Giant esophageal hematoma: possible association with low‐dose aspirin.Gastroenterol Hepatol.2004;27(8):460–463.
- ,,,.Intramural esophageal hematoma. Clinical and endoscopic evolution.Med Clin.2004;123(1):39.
- ,.Spontaneous intramural esophageal hematoma. Diagnosis by CT scanning.J Clin Gastroenterol.1987;9(5):546–548.
- ,,,.Intramural hematoma of the esophagus: a rare cause of chest pain.Am J Emerg Med.2008;26(7):843.e1–e2.
- ,,,.Incidence of adverse oesophageal and gastric events in alendronate users.Pharmacoepidemiol Drug Saf.2000;9(5):371–376.
- ,,.An elderly man with excruciating retrosternal pain and dysphagia.CMAJ.2005;172:1556.
- ,.Fatal esophageal perforation with alendronate.Am J Gastroenterol.2001;96:3212–3213.
- ,,.Erosive injury to the upper gastrointestinal tract in patients receiving iron medication: an underrecognized entitiy.Am J Surg Pathol.1999;23:1241–1247.
- ,.[A case report of esophageal intramural hematoma.] [English abstract on p.4 of the pdf].Govaresh J.2006;11(1):39–41. [Farsi] Available at: http://www.iagh.org/Portals/44fa7561‐56f7‐47e4‐a228‐477ca071e439/Volume%2011,%20Number%201,%20Spring%202006/(1)Dr_bagheri‐11‐1‐7.pdf. Accessed October 2009.
- .Esophageal disorders caused by medications, trauma, and infection. In:Feldman M, Friedman L, Brandt L, eds.Sleisenger and Fordtran's Gastrointestinal and Liver Disease.8th ed.Philadelphia:Saunders;2006:937–948.
Intramural hematoma of the esophagus (IHE) is a rare clinical entity. The majority of cases occur following esophageal instrumentation; however, other causes have been described.14 Rarely, IHE may develop spontaneously. We report a case of apparent spontaneous IHE (SIHE) in a patient presenting with acute‐onset chest pain and dysphagia who was taking low‐dose aspirin, bisphosphonate, and iron supplementation therapy. We highlight the evaluation of chest pain in these patients and the importance of considering the association between esophageal pathology and less commonly implicated medications which may increase the risk of esophageal injury.
Case Report
An 80‐year‐old Hispanic female with a history of osteoporosis, hypertension, and anemia presumed secondary to long‐standing noninsulin‐dependent diabetes mellitus presented with severe, abrupt‐onset, epigastric and retrosternal chest pain following ingestion of a banana. Home medications included aspirin (81 mg daily), alendronate (70 mg weekly), and ferrous sulfate (300 mg 3 times daily). She experienced nausea and minimal vomiting without hematemesis following the onset of pain. She admitted to several weeks of progressive dysphagia leading up to this event, but denied persistent vomiting, straining, foreign body ingestion, or trauma. At admission, the patient was afebrile with heart rate (HR) = 88, blood pressure (BP) = 172/88, pulse oximetry = 99% on room air, hemoglobin = 9.0 g/dL, hematocrit = 26.5%, platelets = 191,000, and international normalized ratio (INR) = 1.04. Electrocardiogram and cardiac enzymes were negative for myocardial infarction. Chest radiograph did not show a widened mediastinum. A computed tomography (CT) scan of the chest demonstrated diffuse thickening of the esophageal wall. Upper endoscopy demonstrated a large, purple, nonpulsatile submucosal mass protruding into and nearly occluding the esophageal lumen (Figure 1A). This mass extended 22 cm along the esophagus and terminated at the esophagogastric junction. There was suggestion of a potential distal mucosal tear and visible clot (Figure 1B, C). An endoscopy performed 6 years prior was unremarkable for esophagitis, stricture, mass, or hemorrhage.
The patient remained nil‐per‐os and was managed conservatively with intravenous fluids, antiemetics, and acid‐suppression therapy. Due to persistent odynophagia, the patient did not tolerate per‐os nutrition, and a percutaneous gastrostomy tube was placed nonendoscopically for temporary nutritional support. The patient's hospital stay was complicated by deep vein thrombosis of the right peroneal vein, for which she underwent inferior vena cava filter placement. She was discharged 18 days following admission. Alendronate and aspirin were discontinued and not reinitiated, and a follow‐up CT scan 6 weeks posthospitalization demonstrated complete resolution of the hematoma.
Discussion
Esophageal injuries include lacerations (Mallory‐Weiss syndrome), perforations (Boerhaave's syndrome), and hematomas (ie, IHE). IHE is by far the least common of these 3 pathologies and, despite increasing reports, it remains a rare clinical entity. Criblez et al.,4 in a review of 91 cases, found that only 35% of patients present with the classic triad of retrosternal chest pain, dysphagia/odynophagia, and hematemesis, while 99% present with at least 1 of these.5 Presentations mimic other cardiothoracic emergencies including myocardial infarction,6 pulmonary embolism,2 aortic dissection,6 and aortoesophageal fistula. Misdiagnosis of IHE and treatment with anticoagulant or thrombolytic therapy can have disastrous consequences, including death.5 Electrocardiograms, chest radiographs, and cardiac enzymes are often normal, as in this case. Endoscopy, performed cautiously, typically reveals a nonpulsatile, purple, submucosal mass. CT, which is rapid, noninvasive, and capable of differentiating between esophageal and life‐threatening thoracomediastinal pathology, frequently demonstrates thickening of the posterior wall of the esophagus with a long, smooth filling‐defect and luminal narrowing.7 Conservative management is the mainstay of treatment with most patients receiving acid suppression and antiemetic therapy. Surgical treatment and antibiotics (in cases of suspected infection) are required infrequently and should be used conservatively when necessary. The vast majority of patients recover spontaneously. Long‐term complications are rare.
IHE most frequently results from esophageal instrumentation, but other antecedent causes have been described. In contrast, SIHE occurs without warning, frequently developing in the absence of vomiting or hematemesis. Since SIHE was first reported in 1970,8 many authors have postulated potential mechanisms of hematoma formation. Controversy remains as to the precise etiology, but recent reports emphasize the association between SIHE and antiplatelet therapy, including low‐dose aspirin,9, 10 aspirin plus dipyridamole,11 and clopidogrel.12 Few studies have identified mechanisms for why the hemorrhage remains in the esophagus and why other parts of the gastrointestinal tract or other organ systems are not involved.
We report a case of apparent SIHE in a patient taking low‐dose aspirin, alendronate, and ferrous sulfate. While a subclinical traumatic event cannot be completely excluded, this patient lacked any apparent antecedent symptoms or other etiologic explanation. Alendronate and ferrous sulfate have been implicated in upper gastrointestinal irritation, but have not previously been associated with SIHE. Park et al.13 estimated a 3.0% incidence of esophageal or gastric events in alendronate users. Recently, esophagitis dissecans superficialis,3 esophageal dissection,14 and even fatal esophageal perforation16 have been reported in patients taking alendronate. Iron supplementation is also a recognized cause of esophageal injury. High local iron saturation may lead to concentration‐dependent absorption and thereby the formation of reactive oxygen metabolites and mucosal injury.16
We hypothesize that alendronate in combination with ferrous sulfate therapy resulted in subclinical esophageal injury predisposing our patient to SIHE. The patient reported 2 weeks of dysphagia prior to admission, suggesting a period of esophageal irritation. On endoscopy, a potential distal esophageal mucosal tear and clot were observed, which may represent a focus of injury. The interaction between this alendronate‐induced injury and chronic antiplatelet therapy may have resulted in hematoma expansion 22 cm along the esophagus. We are aware of one other report of IHE in a patient taking aspirin and alendronate published as an abstract in the Iranian Govaresh Journal.17
A spectrum of less‐commonly‐implicated medications may exert local toxicity on the esophagus and lead to de novo esophageal damage, predisposing patients to a broad spectrum of esophageal pathology, ranging from focal esophageal damage to large hematoma or perforation. Numerous medications are known to be associated with esophageal pathology through a variety of mechanisms (Table 1). Anatomic and motility disorders, as well as pill‐specific factors including contact time, coating materials, and sustained release formulations, may influence toxicity and predispose to injury.18 Elderly patients may be especially susceptible to the combined interactions between antiplatelet therapy and these commonly prescribed or over‐the‐counter medications.
| |
| Nonsteroidal antiinflammatory drugs | Aspirin, naproxen, ibuprofen |
| Bisphosphonates | Alendronate, etidronate, pamidronate |
| Antibiotics | Tetracycline, doxycycline, clindamycin, penicillin |
| Antiviral agents | Zalcitibine, zidovudine, nelfanavir |
| Chemotherapeutic agents | Dactinomycin, bleomycin, cytarabine, daunorubicin, 5‐fluorouracil, methotrexate, vincristine |
| Others | Ferrous sulfate, potassium chloride, ascorbic acid, multivitamins, quinidine, theophylline |
Conclusions
We report a case of apparent SIHE in an elderly woman taking low‐dose aspirin, iron, and alendronate therapy who presented with acute‐onset retrosternal chest pain and dysphagia. We emphasize the importance of including esophageal pathology in the evaluation of chest pain in these patients, particularly elderly women. We encourage a thorough examination of symptoms, including dysphagia/odynophagia, and an exhaustive medication history to identify medications less‐commonly implicated with esophageal pathology. In patients with chest pain taking these medications, clinicians must remain vigilant in their diagnostic approach to prevent misdiagnosis and inappropriate treatment.
Acknowledgements
The authors acknowledge and thank Dr. Sonal Singh for his assistance in helping to analyze the potential drug interactions involved in this case presentation.
Intramural hematoma of the esophagus (IHE) is a rare clinical entity. The majority of cases occur following esophageal instrumentation; however, other causes have been described.14 Rarely, IHE may develop spontaneously. We report a case of apparent spontaneous IHE (SIHE) in a patient presenting with acute‐onset chest pain and dysphagia who was taking low‐dose aspirin, bisphosphonate, and iron supplementation therapy. We highlight the evaluation of chest pain in these patients and the importance of considering the association between esophageal pathology and less commonly implicated medications which may increase the risk of esophageal injury.
Case Report
An 80‐year‐old Hispanic female with a history of osteoporosis, hypertension, and anemia presumed secondary to long‐standing noninsulin‐dependent diabetes mellitus presented with severe, abrupt‐onset, epigastric and retrosternal chest pain following ingestion of a banana. Home medications included aspirin (81 mg daily), alendronate (70 mg weekly), and ferrous sulfate (300 mg 3 times daily). She experienced nausea and minimal vomiting without hematemesis following the onset of pain. She admitted to several weeks of progressive dysphagia leading up to this event, but denied persistent vomiting, straining, foreign body ingestion, or trauma. At admission, the patient was afebrile with heart rate (HR) = 88, blood pressure (BP) = 172/88, pulse oximetry = 99% on room air, hemoglobin = 9.0 g/dL, hematocrit = 26.5%, platelets = 191,000, and international normalized ratio (INR) = 1.04. Electrocardiogram and cardiac enzymes were negative for myocardial infarction. Chest radiograph did not show a widened mediastinum. A computed tomography (CT) scan of the chest demonstrated diffuse thickening of the esophageal wall. Upper endoscopy demonstrated a large, purple, nonpulsatile submucosal mass protruding into and nearly occluding the esophageal lumen (Figure 1A). This mass extended 22 cm along the esophagus and terminated at the esophagogastric junction. There was suggestion of a potential distal mucosal tear and visible clot (Figure 1B, C). An endoscopy performed 6 years prior was unremarkable for esophagitis, stricture, mass, or hemorrhage.
The patient remained nil‐per‐os and was managed conservatively with intravenous fluids, antiemetics, and acid‐suppression therapy. Due to persistent odynophagia, the patient did not tolerate per‐os nutrition, and a percutaneous gastrostomy tube was placed nonendoscopically for temporary nutritional support. The patient's hospital stay was complicated by deep vein thrombosis of the right peroneal vein, for which she underwent inferior vena cava filter placement. She was discharged 18 days following admission. Alendronate and aspirin were discontinued and not reinitiated, and a follow‐up CT scan 6 weeks posthospitalization demonstrated complete resolution of the hematoma.
Discussion
Esophageal injuries include lacerations (Mallory‐Weiss syndrome), perforations (Boerhaave's syndrome), and hematomas (ie, IHE). IHE is by far the least common of these 3 pathologies and, despite increasing reports, it remains a rare clinical entity. Criblez et al.,4 in a review of 91 cases, found that only 35% of patients present with the classic triad of retrosternal chest pain, dysphagia/odynophagia, and hematemesis, while 99% present with at least 1 of these.5 Presentations mimic other cardiothoracic emergencies including myocardial infarction,6 pulmonary embolism,2 aortic dissection,6 and aortoesophageal fistula. Misdiagnosis of IHE and treatment with anticoagulant or thrombolytic therapy can have disastrous consequences, including death.5 Electrocardiograms, chest radiographs, and cardiac enzymes are often normal, as in this case. Endoscopy, performed cautiously, typically reveals a nonpulsatile, purple, submucosal mass. CT, which is rapid, noninvasive, and capable of differentiating between esophageal and life‐threatening thoracomediastinal pathology, frequently demonstrates thickening of the posterior wall of the esophagus with a long, smooth filling‐defect and luminal narrowing.7 Conservative management is the mainstay of treatment with most patients receiving acid suppression and antiemetic therapy. Surgical treatment and antibiotics (in cases of suspected infection) are required infrequently and should be used conservatively when necessary. The vast majority of patients recover spontaneously. Long‐term complications are rare.
IHE most frequently results from esophageal instrumentation, but other antecedent causes have been described. In contrast, SIHE occurs without warning, frequently developing in the absence of vomiting or hematemesis. Since SIHE was first reported in 1970,8 many authors have postulated potential mechanisms of hematoma formation. Controversy remains as to the precise etiology, but recent reports emphasize the association between SIHE and antiplatelet therapy, including low‐dose aspirin,9, 10 aspirin plus dipyridamole,11 and clopidogrel.12 Few studies have identified mechanisms for why the hemorrhage remains in the esophagus and why other parts of the gastrointestinal tract or other organ systems are not involved.
We report a case of apparent SIHE in a patient taking low‐dose aspirin, alendronate, and ferrous sulfate. While a subclinical traumatic event cannot be completely excluded, this patient lacked any apparent antecedent symptoms or other etiologic explanation. Alendronate and ferrous sulfate have been implicated in upper gastrointestinal irritation, but have not previously been associated with SIHE. Park et al.13 estimated a 3.0% incidence of esophageal or gastric events in alendronate users. Recently, esophagitis dissecans superficialis,3 esophageal dissection,14 and even fatal esophageal perforation16 have been reported in patients taking alendronate. Iron supplementation is also a recognized cause of esophageal injury. High local iron saturation may lead to concentration‐dependent absorption and thereby the formation of reactive oxygen metabolites and mucosal injury.16
We hypothesize that alendronate in combination with ferrous sulfate therapy resulted in subclinical esophageal injury predisposing our patient to SIHE. The patient reported 2 weeks of dysphagia prior to admission, suggesting a period of esophageal irritation. On endoscopy, a potential distal esophageal mucosal tear and clot were observed, which may represent a focus of injury. The interaction between this alendronate‐induced injury and chronic antiplatelet therapy may have resulted in hematoma expansion 22 cm along the esophagus. We are aware of one other report of IHE in a patient taking aspirin and alendronate published as an abstract in the Iranian Govaresh Journal.17
A spectrum of less‐commonly‐implicated medications may exert local toxicity on the esophagus and lead to de novo esophageal damage, predisposing patients to a broad spectrum of esophageal pathology, ranging from focal esophageal damage to large hematoma or perforation. Numerous medications are known to be associated with esophageal pathology through a variety of mechanisms (Table 1). Anatomic and motility disorders, as well as pill‐specific factors including contact time, coating materials, and sustained release formulations, may influence toxicity and predispose to injury.18 Elderly patients may be especially susceptible to the combined interactions between antiplatelet therapy and these commonly prescribed or over‐the‐counter medications.
| |
| Nonsteroidal antiinflammatory drugs | Aspirin, naproxen, ibuprofen |
| Bisphosphonates | Alendronate, etidronate, pamidronate |
| Antibiotics | Tetracycline, doxycycline, clindamycin, penicillin |
| Antiviral agents | Zalcitibine, zidovudine, nelfanavir |
| Chemotherapeutic agents | Dactinomycin, bleomycin, cytarabine, daunorubicin, 5‐fluorouracil, methotrexate, vincristine |
| Others | Ferrous sulfate, potassium chloride, ascorbic acid, multivitamins, quinidine, theophylline |
Conclusions
We report a case of apparent SIHE in an elderly woman taking low‐dose aspirin, iron, and alendronate therapy who presented with acute‐onset retrosternal chest pain and dysphagia. We emphasize the importance of including esophageal pathology in the evaluation of chest pain in these patients, particularly elderly women. We encourage a thorough examination of symptoms, including dysphagia/odynophagia, and an exhaustive medication history to identify medications less‐commonly implicated with esophageal pathology. In patients with chest pain taking these medications, clinicians must remain vigilant in their diagnostic approach to prevent misdiagnosis and inappropriate treatment.
Acknowledgements
The authors acknowledge and thank Dr. Sonal Singh for his assistance in helping to analyze the potential drug interactions involved in this case presentation.
- ,,.Post‐sclerotherapy intramural esophageal hematoma: endoscopic and radiologic findings.Gastrointest Endosc.1992;38:102–103.
- ,,.Esophageal hematoma. Four new cases, a review, and proposed etiology.Dig Dis Sci.1981;26:1019–1024.
- ,,.Spontaneous dissecting intramural hematoma of the oesophagus: a rare cause of haematemesis and dysphagia.Endoscopy.1981;13:128–130.
- ,,,,.Intramural rupture and intramural hematoma of the esophagus: 3 case reports and literature review.Schweiz Med Wochenschr.1992;122:416–423.
- ,.Dissecting intramural hematoma of the esophagus.Eur J Gastroenterol Hepatol.2000;12:1151–1161.
- ,,.Spontaneous intramural hematoma of the oesophagus: a report of three cases and review of the literature.Aust N Z J Surg.1994;64:190–193.
- ,,,,.Intramural hematoma of the esophagus: a pictorial essay.Emerg Radiol.2008;15(1):13–22.
- ,.Spontaneous cervico‐mediastinal haematoma.J Ir Med Assoc.1970;63:298.
- ,,,,,.Giant esophageal hematoma: possible association with low‐dose aspirin.Gastroenterol Hepatol.2004;27(8):460–463.
- ,,,.Intramural esophageal hematoma. Clinical and endoscopic evolution.Med Clin.2004;123(1):39.
- ,.Spontaneous intramural esophageal hematoma. Diagnosis by CT scanning.J Clin Gastroenterol.1987;9(5):546–548.
- ,,,.Intramural hematoma of the esophagus: a rare cause of chest pain.Am J Emerg Med.2008;26(7):843.e1–e2.
- ,,,.Incidence of adverse oesophageal and gastric events in alendronate users.Pharmacoepidemiol Drug Saf.2000;9(5):371–376.
- ,,.An elderly man with excruciating retrosternal pain and dysphagia.CMAJ.2005;172:1556.
- ,.Fatal esophageal perforation with alendronate.Am J Gastroenterol.2001;96:3212–3213.
- ,,.Erosive injury to the upper gastrointestinal tract in patients receiving iron medication: an underrecognized entitiy.Am J Surg Pathol.1999;23:1241–1247.
- ,.[A case report of esophageal intramural hematoma.] [English abstract on p.4 of the pdf].Govaresh J.2006;11(1):39–41. [Farsi] Available at: http://www.iagh.org/Portals/44fa7561‐56f7‐47e4‐a228‐477ca071e439/Volume%2011,%20Number%201,%20Spring%202006/(1)Dr_bagheri‐11‐1‐7.pdf. Accessed October 2009.
- .Esophageal disorders caused by medications, trauma, and infection. In:Feldman M, Friedman L, Brandt L, eds.Sleisenger and Fordtran's Gastrointestinal and Liver Disease.8th ed.Philadelphia:Saunders;2006:937–948.
- ,,.Post‐sclerotherapy intramural esophageal hematoma: endoscopic and radiologic findings.Gastrointest Endosc.1992;38:102–103.
- ,,.Esophageal hematoma. Four new cases, a review, and proposed etiology.Dig Dis Sci.1981;26:1019–1024.
- ,,.Spontaneous dissecting intramural hematoma of the oesophagus: a rare cause of haematemesis and dysphagia.Endoscopy.1981;13:128–130.
- ,,,,.Intramural rupture and intramural hematoma of the esophagus: 3 case reports and literature review.Schweiz Med Wochenschr.1992;122:416–423.
- ,.Dissecting intramural hematoma of the esophagus.Eur J Gastroenterol Hepatol.2000;12:1151–1161.
- ,,.Spontaneous intramural hematoma of the oesophagus: a report of three cases and review of the literature.Aust N Z J Surg.1994;64:190–193.
- ,,,,.Intramural hematoma of the esophagus: a pictorial essay.Emerg Radiol.2008;15(1):13–22.
- ,.Spontaneous cervico‐mediastinal haematoma.J Ir Med Assoc.1970;63:298.
- ,,,,,.Giant esophageal hematoma: possible association with low‐dose aspirin.Gastroenterol Hepatol.2004;27(8):460–463.
- ,,,.Intramural esophageal hematoma. Clinical and endoscopic evolution.Med Clin.2004;123(1):39.
- ,.Spontaneous intramural esophageal hematoma. Diagnosis by CT scanning.J Clin Gastroenterol.1987;9(5):546–548.
- ,,,.Intramural hematoma of the esophagus: a rare cause of chest pain.Am J Emerg Med.2008;26(7):843.e1–e2.
- ,,,.Incidence of adverse oesophageal and gastric events in alendronate users.Pharmacoepidemiol Drug Saf.2000;9(5):371–376.
- ,,.An elderly man with excruciating retrosternal pain and dysphagia.CMAJ.2005;172:1556.
- ,.Fatal esophageal perforation with alendronate.Am J Gastroenterol.2001;96:3212–3213.
- ,,.Erosive injury to the upper gastrointestinal tract in patients receiving iron medication: an underrecognized entitiy.Am J Surg Pathol.1999;23:1241–1247.
- ,.[A case report of esophageal intramural hematoma.] [English abstract on p.4 of the pdf].Govaresh J.2006;11(1):39–41. [Farsi] Available at: http://www.iagh.org/Portals/44fa7561‐56f7‐47e4‐a228‐477ca071e439/Volume%2011,%20Number%201,%20Spring%202006/(1)Dr_bagheri‐11‐1‐7.pdf. Accessed October 2009.
- .Esophageal disorders caused by medications, trauma, and infection. In:Feldman M, Friedman L, Brandt L, eds.Sleisenger and Fordtran's Gastrointestinal and Liver Disease.8th ed.Philadelphia:Saunders;2006:937–948.
