User login
Autoimmune Thyroid Dysfunction: A Possible Effect of Mangosteen
Hypopigmented Patches...
Open Fracture as a Rare Complication of Olecranon Enthesophyte in a Patient With Gout
Proximal Humerus Osteolysis After Revision Rotator Cuff Repair With Bioabsorbable Suture Anchors
Alendronate Therapy in Polyostotic Fibrous Dysplasia Presenting With Pathologic Fracture
Diffuse abdominal pain, vomiting
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission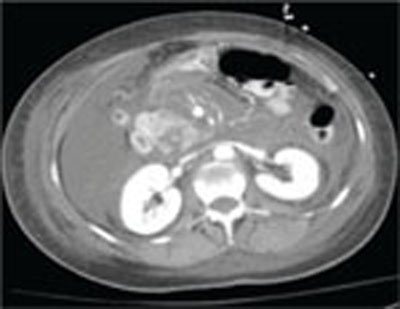
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
• Use the APACHE-II scoring system early on to help predict the severity of pancreatitis.
• Consider early enteral nutrition in patients with severe disease; taking this step has been linked to lower infection rates and shorter lengths of stay.
• Consider patient factors and the risk of severe infection when deciding whether or not to use prophylactic antibiotics in cases of severe necrotizing pancreatitis.
CASE A 57-year-old Caucasian woman sought care at our emergency department (ED) for diffuse abdominal pain and nausea. She said that the pain began after eating lunch earlier that day, and localized periumbilically, with radiation to the back. She had several episodes of nonbilious, nonbloody vomiting, but denied fever, chills, or diarrhea.
Her past medical history was notable only for an episode of gallstone pancreatitis 11 years earlier, after which she underwent a cholecystectomy. Her only medications were ibandronate sodium (Boniva) taken for osteoporosis (diagnosed 2 years earlier), a multivitamin, calcium, magnesium, and vitamin E supplements. Her family history was notable for a brother who had pancreatic cancer in his 50s. The patient reported infrequent alcohol use.
The abdominal exam was notable for diffuse tenderness to palpation, most prominent in the epigastric region. The patient exhibited voluntary guarding, without rebound, and positive bowel sounds throughout.
The patient’s laboratory studies on admission included leukocytosis of 21,300 cells/mcL and hemoglobin and hematocrit of 17.3 g/dL and 52.1%, respectively. She had an amylase of 1733 U/L and lipase of 4288 U/L. Lactate and lactic dehydrogenase were 1.83 mg/dL and 265 U/L, respectively. Liver function tests and a basic metabolic panel were within normal limits. A noncontrast computed tomography (CT) scan of the abdomen and pelvis was notable for an enlarged pancreas with peripancreatic edema and free fluid in the abdomen.
The patient underwent aggressive fluid resuscitation throughout the first 6 hours of her hospital stay. Urine output was noted to be incongruent with fluid intake, at just over 60 cc/h. Over the next 4 hours, she became progressively tachycardic, tachypneic, and somnolent, with increasing abdominal tenderness. Her serum potassium level rose to 4.9 mEq/L, while serum bicarbonate declined to 13 mEq/L and serum calcium, to 6.2 mg/dL. Arterial blood gas revealed metabolic acidosis with a pH of 7.22.
Our patient was subsequently transferred to the medical intensive care unit, where she required endotracheal intubation.
WHAT IS THE MOST LIKELY EXPLANATION FOR HER CONDITION?
Acute necrotizing pancreatitis
A repeat CT scan of the abdomen and pelvis with IV contrast taken on the second day of admission revealed extensive pancreatitis with complete disintegration of the pancreatic tissue and absence of pancreatic enhancement (FIGURE), as well as a large amount of abdominal ascites.
Pancreatitis is a common inpatient diagnosis, with approximately 200,000 hospitalizations yearly.1 Most cases are mild and self-limiting, requiring minimal intervention including parenteral fluid resuscitation, pain control, and restriction of oral intake. Most cases can be attributed to gallstones or excessive alcohol use, but approximately 25% of cases are idiopathic.1 Other causes include hypertriglyceridemia, infection, hypercalcemia, and medications such as azathioprine, 6-mercaptopurine, trimethoprim sulfa-methoxazole, and furosemide. Severe necrotizing pancreatitis represents about 20% of all cases, but carries a mortality rate of between 10% and 30%.1
Diagnosis is based on clinical features in conjunction with biochemical markers. Amylase is nonspecific, but levels 3 times the upper limit of normal are usually diagnostic of acute pancreatitis. Lipase is 85% to 100% sensitive for pancreatitis, and is more specific than amylase. Alanine aminotransferase >150 IU/L is 96% specific for gallstone pancreatitis.2 Of note: there is no evidence to support daily monitoring of these enzyme levels as predictors of clinical improvement or disease severity.
FIGURE
CT scan of abdomen taken on second day of admission
Predicting severity at time of presentation can be difficult
As was true with our patient, predicting the severity of acute pancreatitis at the time of presentation can be difficult. Scoring systems that are commonly used to evaluate disease severity include Ranson’s score, APACHE-II (Acute Physiology and Chronic Health Evaluation-II), and CT severity index, among others (TABLE). Of these, the APACHE-II score has been found to be most predictive of progression to severe disease, with accuracy of up to 75%.3
Recent studies have shown that a body mass index >30 kg/m2 is an independent risk factor for progression to severe pancreatitis.4 Other clinical predictors include poor urine output, rising hematocrit, agitation or confusion, and lack of improvement in symptoms within 48 hours.1
Though our patient came in with symptoms that were initially mild, she quickly manifested several clinical predictors for severe pancreatitis, including poor urine output and increasing confusion, as well as an APACHE-II score of 12 at 6 hours after presentation (values ≥8 indicate high risk for progression to severe disease).
TABLE
Predictors for progression to severe pancreatitis1
| Ranson score ≥3 |
| APACHE-II score ≥8 |
| CT severity index (CT grade + necrosis score) >6 |
| Body mass index >30 kg/m2 |
| Hematocrit >44% (clearly increases risk for pancreatic necrosis) |
Clinical findings:
|
| Lack of improvement in symptoms within the first 48 hours |
| APACHE, Acute Physiology and Chronic Health Evaluation; CT, computed tomography. |
Role of antibiotics? A source of debate
Infection represents the leading cause of morbidity and mortality in patients with pancreatic necrosis. Approximately 40% of patients with necrosis develop infection, with a 20% mortality rate.5 Signs of infection usually develop relatively late in the clinical course and rates increase drastically each week a patient remains hospitalized (71% of patients have signs of infection at 3 weeks).5
Interestingly, the role for antibiotics in such patients has been a source of debate in practice, as well as in the medical literature. Two recent large meta-analyses came to different conclusions regarding the use of antibiotics. A 2006 study by Heinrich et al concluded that patients with pancreatic necrosis demonstrated by contrast-enhanced CT scans should receive antibiotic prophylaxis with imipenem or meropenem for 14 days, and that prophylactic antibiotics do not increase rates of subsequent fungal infection.6 Conversely, as noted in a 2008 study published in the American Journal of Gastroenterology, “prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in patients with acute necrotizing pancreatitis.”7
Two leading professional groups have similarly contradictory recommendations on the topic, with the American Gastroenterological Association (AGA) supporting antibiotic use for patients with >30% pancreatic necrosis noted on CT and the American College of Gastroenterology (ACG) recommending against the use of prophylactic antibiotics.8
As with any clinical dilemma, it seems prudent to make the decision for or against prophylactic antibiotics based on available clinical information and the particular patient’s risk factors. Clearly, in the most high-risk patients, it would be difficult to justify withholding antibiotic therapy.
Complete bowel rest—or not?
In the past, it was thought necessary to allow for complete bowel rest and suppression of pancreatic exocrine secretion during acute pancreatitis by providing total parenteral nutrition.6,9 More recently, though, the use of early nasojejunal enteral feeding (which was initiated for our patient) has been advocated by several large meta-analyses,6 as well as by the AGA and ACG.2
The use of enteral feeding has been associated with improved outcomes, including lower infection rates (due to maintenance of the intestinal barrier and prevention of bacterial translocation), decreased length of stay, reduced rates of organ failure, and fewer deaths among patients who require surgical intervention.6
A lengthy road to recovery for our patient
After 7 days of mechanical ventilation, our patient was extubated. However, she developed significant bilateral pleural effusions as a result of fluid third spacing, and required thoracentesis.
She completed a 14-day course of imipenem, followed by an additional 10-day course due to hypotension and a suspected infected pseudocyst. Subsequent imaging studies confirmed our suspicions: She had developed a large pseudocyst (>13 cm), which remained under observation by both a gastroenterologist and general surgeon. Six weeks after admission, our patient was discharged to home with family.
But what was the cause? Although we were unable to clearly delineate an inciting cause for her pancreatitis during the admission, she was to undergo further investigation as an outpatient. There were also plans to drain the pseudocyst 6 weeks after discharge.
A learning opportunity. This patient’s case provided an excellent opportunity for our team to review the important clinical predictors for progression to severe pancreatitis, and the rapid nature of clinical decline in such patients. In hindsight, the predictors of severity in our patient were few, but included the rapid onset and clinical progression of her symptoms, as well as her elevated hematocrit on presentation and poor urine output over the first 6 hours of admission.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
1. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142-2150.
2. Vege SS, Whitcomb DC, Ginsburg CH. Clinical manifestations and diagnosis of acute pancreatitis. In: Basow DS. ed. UpTo-Date [online database]. Version 18.2. Waltham, Mass: UpTo-Date; 2010.
3. Vege SS, Whitcomb DC, Ginsburg CH. Predicting severity of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
4. Skipworth JRA, Pereira SP. Acute pancreatitis. Curr Opin Crit Care. 2008;14:172-178.
5. Windsor JA, Schweder P. Complications of acute pancreatitis (including pseudocysts). In: Zinner MJ, Ashley SW, eds. Main-got’s Abdominal Operations. 11th ed. New York: McGraw-Hill; 2007:chap 37. Available at: http://www.accesssurgery.com/content.aspx?filename="6003JFP_HospitalRounds" aid=130125. Accessed November 30, 2010.
6. Heinrich S, Shafer M, Rousson V, et al. Evidenced-based treatment of acute pancreatitis: a look at established paradigms. Ann Surg. 2006;243:154-168.
7. Bai Y, Gao J, Zou DW, et al. Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2008;103:104-110.
8. Vege SS, Whitcomb DC, Ginsburg CH. Treatment of acute pancreatitis. In: Basow DS, ed. UpToDate [online database]. Version 18.2. Waltham, Mass: UpToDate; 2010.
9. Haney JC, Pappas TN. Necrotizing pancreatitis: diagnosis and management. Surg Clin North Am. 2007;87:1431-1446.
Pregabalin‐induced trismus in a leukemia patient
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
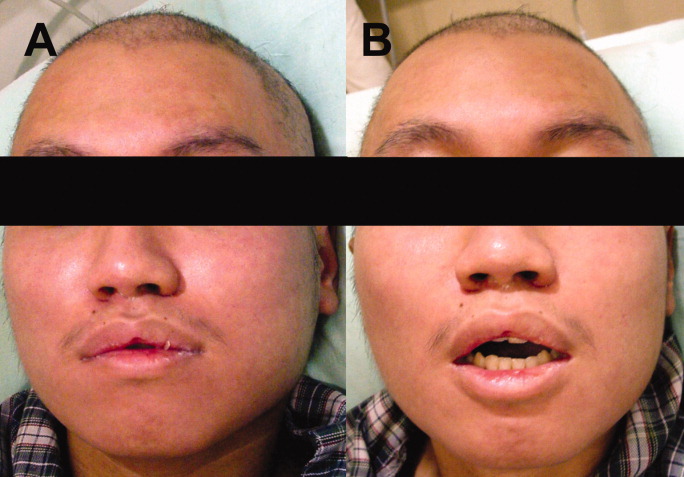
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
