User login
Special Operations Training: An Atypical Presentation of Aspiration Pneumonia
Empyema is a well-known sequela resulting from the extension of bacterial pneumonia or pulmonary abscess to the pleural space. This case highlights the organism Streptococcus intermedius (S intermedius), an uncommon cause of pulmonary empyema.1Streptococcus intermedius is endogenous among oral flora and is notorious for its abscess-forming capabilities when spread to alternative sites.
The patient was a healthy, active-duty male who presented in sepsis after months of worsening dyspnea and subacute hemoptysis following 2 near-drowning episodes during Special Operations training. Eight weeks after urgent surgical decortication and intensive antibiotic therapy, the patient experienced a complete resolution of his symptoms. A brief discussion follows concerning the pathogenesis and relevant literature regarding S intermedius infections.
Case History
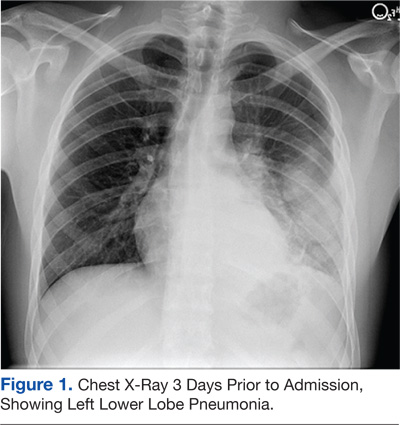
A 21-year-old Air Force Tactical Air Control Party (TACP) trainee with no significant past medical history presented with worsening dyspnea, pleuritic chest pain, and hemoptysis after failed outpatient therapy with levofloxacin for presumed community-acquired pneumonia (CAP) 3 days prior. The chest X-ray at that time demonstrated a left lower lobe consolidation with no evidence of pleural effusion or pulmonary abscess on the lateral view (Figure 1).
The patient stated that his symptoms started about 3 months prior with fever, chills, and night sweats. His symptoms occurred episodically every few weeks, but he had no knowledge of any significant events preceding the illness. The patient developed intermittent hemoptysis 2 weeks later. This included blood-streaked mucus with productive cough and bright-red blood, ranging between a teaspoon and a tablespoon, according to the patient. The patient gradually developed increased dyspnea, which began to impact his performance during Special Operations physical training. His symptoms gradually progressed to worsening dyspnea, which began to affect daily living activities, and new-onset left-sided rib pain. The patient reported no relevant travel history and tested negative for purified protein derivatives 3 months before the initial presentation.
On further questioning, the patient disclosed 2 near-drowning incidents within the preceding year. The first occurred 10 months before presentation, when the patient was performing a 1-minute underwater swim in preparation for the TACP training. The patient stated that he came to the surface to take a breath and lost consciousness. He was immediately brought to the edge of the pool and quickly recovered with no apparent residual symptoms. The second episode occurred during an underwater buddy-breathing training exercise 4 months before presentation and just 3 weeks before symptom onset. The patient reported that he knew he was not getting enough air but remained underwater, concerned that he might fail the exercise. He had a transient syncopal episode shortly after aspirating and was brought to the surface. Afterward, the patient refused to receive medical attention following this event, fearing risk of medical disqualification from training. He reportedly did not experience symptoms after this second episode.
The patient’s past medical history included seasonal allergic rhinitis, and his past surgical history was unremarkable. The patient was not taking medication other than levofloxacin, prescribed for the suspected CAP. The patient was allergic to penicillin, did not use tobacco, and reported drinking about 5 alcoholic beverages per week. His family history included a sister with asthma and a mother with factor V Leiden deficiency and pulmonary embolism related to hormone replacement therapy.
The patient’s vital signs revealed a temperature of 103.2°F, 114 beats per minute pulse, 24 breaths per minute respiratory rate, and oxygen saturation of 89% on room air. On physical examination, the patient was noted to be in moderate respiratory distress with accessory muscle use and was diaphoretic. Breath sounds were diminished in the left upper and lower lung fields with significant egophony.
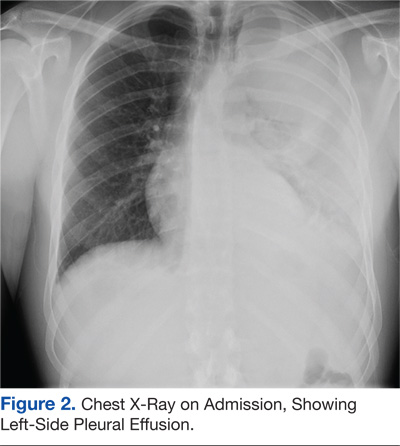
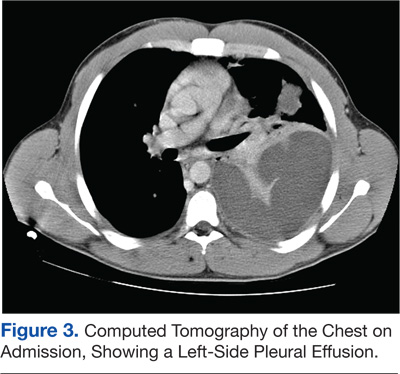
Tests revealed a white blood cell count of 23,300/mm3 with 30% bandemia. A chest radiograph showed an infiltrate/effusion of the entire left hemithorax (Figure 2). A computed tomography (CT) scan of the chest showed a large multiloculated left-side pleural effusion (Figure 3).
The patient was started on broad-spectrum antibiotics, including intravenous (IV) ceftriaxone, azithromycin, and clindamycin. He underwent thoracentesis on admission, yielding only 300 mL of purulent fluid, confirming its loculated status.
Serum total protein was 7.1 g/dL, and no serum lactic acid dehydrogenase (LDH) was obtained at the time of thoracentesis. Pleural fluid analysis revealed a protein of 5.2 g/dL, and an LDH of 5,176 units/L, meeting Light’s criteria for exudate based on a pleural fluid protein to serum protein ratio of > 0.5 (0.69) and pleural fluid LDH level > two-thirds of the upper limit of normal for serum LDH.
General surgery placed 2 thoracostomy tubes in the left hemithorax without significant drainage. On the first hospital day the patient seemed toxic and underwent a minithoracotomy with decortication. The Gram stain of the blood and blood cultures were negative over 72 hours. Another Gram stain of pleural fluid showed Gram-positive cocci in pairs. Pleural fluid cultures obtained during the procedure revealed S intermedius consistent with the patient’s history of aspiration and abscess formation. Antibiotic susceptibility tests were not performed on the sample.
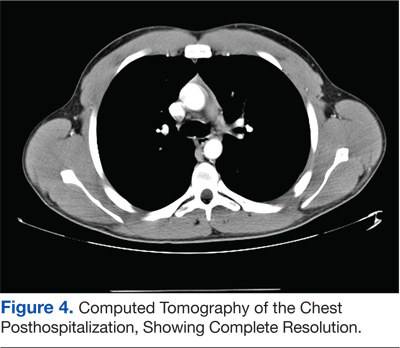
A peripherally inserted central catheter line was placed for daily IV ceftriaxone infusions to be continued with oral clindamycin for the subsequent 4 weeks. A CT scan of the chest at 8 weeks posthospitalization revealed minimal postoperative scarring, and pulmonary function tests showed normal flow volume loop and maximum voluntary ventilation (Figure 4). The patient reported full recovery and was returned to full activity, including further Special Operations training.
Discussion
Pulmonary infections associated with near-drowning events are caused by a host of organisms that must be considered in the differential diagnosis. The most common include Aeromonas species, Burkholderia pseudomallei, Pseudallescheria boydii, Streptococcus pneumoniae, and Pseudomonas aeruginosa.2 However, the causative organism in this case was endogenous. Streptococcus intermedius is an anaerobic, Gram-positive cocci, a member of the Streptococcus milleri group, and is considered normal flora of the oral mucosa, upper respiratory tract, vagina, and gastrointestinal tract.3,4 This organism is innocuous in its normal habitat but may result in considerable mortality and morbidity if spread to alternative sites due to its ability to form abscesses and cause systemic infections.5
Although uncommon, respiratory infections caused by S intermedius typically result from aspiration of gastric or oral contents and may lead to pulmonary abscesses or empyema.1,6,7 It may present as a primary empyema.8 Current literature suggests a mortality rate between 2% and 14% with higher rates in older populations.9 A retrospective study looking at 72 cases of Streptococci viridans pulmonary infection from 1984 to 1996 found only 2 documented cases where S intermedius was identified as the cause of concomitant empyema and lung abscesses. This study also indicated a strong male predominance with only 7% of lung abscesses occurring in females.10,11
This patient developed a pulmonary abscess and empyema as a probable consequence of aspiration during underwater training exercises. The diagnosis was complicated, because the patient did not initially disclose the pertinent history, and he ignored his symptoms so that he could continue training. His actions delayed aggressive antibiotic therapy and likely led to the rapid progression of pneumonia and his complicated clinical course, because S intermedius has shown intermediate susceptibility or resistance to fluoroquinolone monotherapy.12
This case was also unusual given the subacute presentation and 3-month history of hemoptysis. On review of the available medical literature, hemoptysis is an unusual symptom of pulmonary infections caused by S intermedius but can likely be attributed to necrosis of the pulmonary tissue.8,13
Most patients with S intermedius pulmonary infection rapidly progress due to the virulence of this organism and predisposing comorbidities.14,15 However, this patient had a relatively indolent progression for 3 months, which speaks to the increased respiratory reserve of a healthy, young male in excellent cardiovascular condition.
Conclusion
This case highlights the potential for normal oral flora to cause advanced pulmonary disease in patients with no significant comorbidities. Streptococcus intermedius infections can be subacute in presentation but may rapidly progress to severe disease once seeded in the pleural cavity. Whereas early pleural space drainage remains fundamental, urgent surgical intervention may be required for loculated disease. Although infections with this organism may lead to irreversible pulmonary complications, complete resolution with full recovery is possible in young, healthy patients.
Primary care physicians must take a careful history to ensure optimal patient outcomes. This concept is particularly important to consider in aviators and Special Operations personnel who may be reluctant to seek medical care. Establishing a sense of trust among active-duty military is essential for mission accomplishment.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Weightman NC, Barnham MRD, Dove M. Streptococcus milleri group bacteraemia in North Yorkshire, England (1989-2000). Indian J Med Res. 2004;119(suppl):164-167.
2. Ender PT, Dolan MJ. Pneumonia associated with near-drowning. Clin Infect Dis. 1997;1(4):896-907.
3. Porta G, Rodriguez-Carballeira M, Gómez L, et al. Thoracic infection caused by Streptococcus milleri. Eur Respir J. 1998;12(2):357-362.
4. Van der Auwera P. Clinical significance of Streptococcus milleri. Eur J Clin Microbiol.1985;4(4):386-390.
5. Murray HW, Gross KC, Masur H, Roberts RB. Serious infections caused by Streptococcus milleri. Am J Med. 1978;64(5):759-764.
6. Shinzato T, Saito A. The Streptococcus milleri group as a cause of pulmonary infections. Clin Infect Dis. 1995;21(suppl 3):S238-S243.
7. Frankish PD, Kolbe J. Thoracic empyema due to Streptococcus milleri: Four cases. N Z Med J. 1984;97(769):849-851.
8. Iskandar SB, Al Hasan MA, Roy TM, Byrd RP Jr. Streptococcus intermedius: An unusual cause of a primary empyema. Tenn Med. 2006;99(2):37-39.
9. de Hoyos A, Sundaresan S. Thoracic empyema. Surg Clin North Am. 2002;82(3):643-671.
10. Jerng JS, Hsueh PR, Teng LJ, Lee LN, Yang PC, Luh KT. Empyema thoracis and lung abscess caused by viridans streptococci. Am J Respir Crit Care Med. 1997;156(5):1508-1514.
11. Wargo KA, McConnell VJ, Higginbotham SA. A case of Streptococcus intermedius empyema. Ann Pharmacother. 2006;40(6):1208-1210.
12. Limia A, Jiménez ML, Alarcón T, López-Brea M. Five-year analysis of antimicrobial susceptibility of the Streptococcus milleri group. Eur J Clin Microbiol Infect Dis. 1999;18(6):440-444.
13. Wong CA, Donal F, Macfarlane JT. Streptococcus milleri pulmonary disease: A review and clinical description of 25 patients. Thorax. 1995;50(10):1093-1096.
14. Shlaes DM, Lerner PI, Wolinsky E, Gopalakrishna KV. Infections due to Lancefield F and related Streptococci (S milleri, S anginosus). Medicine (Baltimore). 1981;60(3):197-207.
15. Roy WJ Jr, Roy TM, Davis GJ. Thoracic empyema due to Streptococcus intermedius. J Ky Med Assoc. 1991;89(11):558-562.
Empyema is a well-known sequela resulting from the extension of bacterial pneumonia or pulmonary abscess to the pleural space. This case highlights the organism Streptococcus intermedius (S intermedius), an uncommon cause of pulmonary empyema.1Streptococcus intermedius is endogenous among oral flora and is notorious for its abscess-forming capabilities when spread to alternative sites.
The patient was a healthy, active-duty male who presented in sepsis after months of worsening dyspnea and subacute hemoptysis following 2 near-drowning episodes during Special Operations training. Eight weeks after urgent surgical decortication and intensive antibiotic therapy, the patient experienced a complete resolution of his symptoms. A brief discussion follows concerning the pathogenesis and relevant literature regarding S intermedius infections.
Case History
A 21-year-old Air Force Tactical Air Control Party (TACP) trainee with no significant past medical history presented with worsening dyspnea, pleuritic chest pain, and hemoptysis after failed outpatient therapy with levofloxacin for presumed community-acquired pneumonia (CAP) 3 days prior. The chest X-ray at that time demonstrated a left lower lobe consolidation with no evidence of pleural effusion or pulmonary abscess on the lateral view (Figure 1).
The patient stated that his symptoms started about 3 months prior with fever, chills, and night sweats. His symptoms occurred episodically every few weeks, but he had no knowledge of any significant events preceding the illness. The patient developed intermittent hemoptysis 2 weeks later. This included blood-streaked mucus with productive cough and bright-red blood, ranging between a teaspoon and a tablespoon, according to the patient. The patient gradually developed increased dyspnea, which began to impact his performance during Special Operations physical training. His symptoms gradually progressed to worsening dyspnea, which began to affect daily living activities, and new-onset left-sided rib pain. The patient reported no relevant travel history and tested negative for purified protein derivatives 3 months before the initial presentation.
On further questioning, the patient disclosed 2 near-drowning incidents within the preceding year. The first occurred 10 months before presentation, when the patient was performing a 1-minute underwater swim in preparation for the TACP training. The patient stated that he came to the surface to take a breath and lost consciousness. He was immediately brought to the edge of the pool and quickly recovered with no apparent residual symptoms. The second episode occurred during an underwater buddy-breathing training exercise 4 months before presentation and just 3 weeks before symptom onset. The patient reported that he knew he was not getting enough air but remained underwater, concerned that he might fail the exercise. He had a transient syncopal episode shortly after aspirating and was brought to the surface. Afterward, the patient refused to receive medical attention following this event, fearing risk of medical disqualification from training. He reportedly did not experience symptoms after this second episode.
The patient’s past medical history included seasonal allergic rhinitis, and his past surgical history was unremarkable. The patient was not taking medication other than levofloxacin, prescribed for the suspected CAP. The patient was allergic to penicillin, did not use tobacco, and reported drinking about 5 alcoholic beverages per week. His family history included a sister with asthma and a mother with factor V Leiden deficiency and pulmonary embolism related to hormone replacement therapy.
The patient’s vital signs revealed a temperature of 103.2°F, 114 beats per minute pulse, 24 breaths per minute respiratory rate, and oxygen saturation of 89% on room air. On physical examination, the patient was noted to be in moderate respiratory distress with accessory muscle use and was diaphoretic. Breath sounds were diminished in the left upper and lower lung fields with significant egophony.
Tests revealed a white blood cell count of 23,300/mm3 with 30% bandemia. A chest radiograph showed an infiltrate/effusion of the entire left hemithorax (Figure 2). A computed tomography (CT) scan of the chest showed a large multiloculated left-side pleural effusion (Figure 3).
The patient was started on broad-spectrum antibiotics, including intravenous (IV) ceftriaxone, azithromycin, and clindamycin. He underwent thoracentesis on admission, yielding only 300 mL of purulent fluid, confirming its loculated status.
Serum total protein was 7.1 g/dL, and no serum lactic acid dehydrogenase (LDH) was obtained at the time of thoracentesis. Pleural fluid analysis revealed a protein of 5.2 g/dL, and an LDH of 5,176 units/L, meeting Light’s criteria for exudate based on a pleural fluid protein to serum protein ratio of > 0.5 (0.69) and pleural fluid LDH level > two-thirds of the upper limit of normal for serum LDH.
General surgery placed 2 thoracostomy tubes in the left hemithorax without significant drainage. On the first hospital day the patient seemed toxic and underwent a minithoracotomy with decortication. The Gram stain of the blood and blood cultures were negative over 72 hours. Another Gram stain of pleural fluid showed Gram-positive cocci in pairs. Pleural fluid cultures obtained during the procedure revealed S intermedius consistent with the patient’s history of aspiration and abscess formation. Antibiotic susceptibility tests were not performed on the sample.
A peripherally inserted central catheter line was placed for daily IV ceftriaxone infusions to be continued with oral clindamycin for the subsequent 4 weeks. A CT scan of the chest at 8 weeks posthospitalization revealed minimal postoperative scarring, and pulmonary function tests showed normal flow volume loop and maximum voluntary ventilation (Figure 4). The patient reported full recovery and was returned to full activity, including further Special Operations training.
Discussion
Pulmonary infections associated with near-drowning events are caused by a host of organisms that must be considered in the differential diagnosis. The most common include Aeromonas species, Burkholderia pseudomallei, Pseudallescheria boydii, Streptococcus pneumoniae, and Pseudomonas aeruginosa.2 However, the causative organism in this case was endogenous. Streptococcus intermedius is an anaerobic, Gram-positive cocci, a member of the Streptococcus milleri group, and is considered normal flora of the oral mucosa, upper respiratory tract, vagina, and gastrointestinal tract.3,4 This organism is innocuous in its normal habitat but may result in considerable mortality and morbidity if spread to alternative sites due to its ability to form abscesses and cause systemic infections.5
Although uncommon, respiratory infections caused by S intermedius typically result from aspiration of gastric or oral contents and may lead to pulmonary abscesses or empyema.1,6,7 It may present as a primary empyema.8 Current literature suggests a mortality rate between 2% and 14% with higher rates in older populations.9 A retrospective study looking at 72 cases of Streptococci viridans pulmonary infection from 1984 to 1996 found only 2 documented cases where S intermedius was identified as the cause of concomitant empyema and lung abscesses. This study also indicated a strong male predominance with only 7% of lung abscesses occurring in females.10,11
This patient developed a pulmonary abscess and empyema as a probable consequence of aspiration during underwater training exercises. The diagnosis was complicated, because the patient did not initially disclose the pertinent history, and he ignored his symptoms so that he could continue training. His actions delayed aggressive antibiotic therapy and likely led to the rapid progression of pneumonia and his complicated clinical course, because S intermedius has shown intermediate susceptibility or resistance to fluoroquinolone monotherapy.12
This case was also unusual given the subacute presentation and 3-month history of hemoptysis. On review of the available medical literature, hemoptysis is an unusual symptom of pulmonary infections caused by S intermedius but can likely be attributed to necrosis of the pulmonary tissue.8,13
Most patients with S intermedius pulmonary infection rapidly progress due to the virulence of this organism and predisposing comorbidities.14,15 However, this patient had a relatively indolent progression for 3 months, which speaks to the increased respiratory reserve of a healthy, young male in excellent cardiovascular condition.
Conclusion
This case highlights the potential for normal oral flora to cause advanced pulmonary disease in patients with no significant comorbidities. Streptococcus intermedius infections can be subacute in presentation but may rapidly progress to severe disease once seeded in the pleural cavity. Whereas early pleural space drainage remains fundamental, urgent surgical intervention may be required for loculated disease. Although infections with this organism may lead to irreversible pulmonary complications, complete resolution with full recovery is possible in young, healthy patients.
Primary care physicians must take a careful history to ensure optimal patient outcomes. This concept is particularly important to consider in aviators and Special Operations personnel who may be reluctant to seek medical care. Establishing a sense of trust among active-duty military is essential for mission accomplishment.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Empyema is a well-known sequela resulting from the extension of bacterial pneumonia or pulmonary abscess to the pleural space. This case highlights the organism Streptococcus intermedius (S intermedius), an uncommon cause of pulmonary empyema.1Streptococcus intermedius is endogenous among oral flora and is notorious for its abscess-forming capabilities when spread to alternative sites.
The patient was a healthy, active-duty male who presented in sepsis after months of worsening dyspnea and subacute hemoptysis following 2 near-drowning episodes during Special Operations training. Eight weeks after urgent surgical decortication and intensive antibiotic therapy, the patient experienced a complete resolution of his symptoms. A brief discussion follows concerning the pathogenesis and relevant literature regarding S intermedius infections.
Case History
A 21-year-old Air Force Tactical Air Control Party (TACP) trainee with no significant past medical history presented with worsening dyspnea, pleuritic chest pain, and hemoptysis after failed outpatient therapy with levofloxacin for presumed community-acquired pneumonia (CAP) 3 days prior. The chest X-ray at that time demonstrated a left lower lobe consolidation with no evidence of pleural effusion or pulmonary abscess on the lateral view (Figure 1).
The patient stated that his symptoms started about 3 months prior with fever, chills, and night sweats. His symptoms occurred episodically every few weeks, but he had no knowledge of any significant events preceding the illness. The patient developed intermittent hemoptysis 2 weeks later. This included blood-streaked mucus with productive cough and bright-red blood, ranging between a teaspoon and a tablespoon, according to the patient. The patient gradually developed increased dyspnea, which began to impact his performance during Special Operations physical training. His symptoms gradually progressed to worsening dyspnea, which began to affect daily living activities, and new-onset left-sided rib pain. The patient reported no relevant travel history and tested negative for purified protein derivatives 3 months before the initial presentation.
On further questioning, the patient disclosed 2 near-drowning incidents within the preceding year. The first occurred 10 months before presentation, when the patient was performing a 1-minute underwater swim in preparation for the TACP training. The patient stated that he came to the surface to take a breath and lost consciousness. He was immediately brought to the edge of the pool and quickly recovered with no apparent residual symptoms. The second episode occurred during an underwater buddy-breathing training exercise 4 months before presentation and just 3 weeks before symptom onset. The patient reported that he knew he was not getting enough air but remained underwater, concerned that he might fail the exercise. He had a transient syncopal episode shortly after aspirating and was brought to the surface. Afterward, the patient refused to receive medical attention following this event, fearing risk of medical disqualification from training. He reportedly did not experience symptoms after this second episode.
The patient’s past medical history included seasonal allergic rhinitis, and his past surgical history was unremarkable. The patient was not taking medication other than levofloxacin, prescribed for the suspected CAP. The patient was allergic to penicillin, did not use tobacco, and reported drinking about 5 alcoholic beverages per week. His family history included a sister with asthma and a mother with factor V Leiden deficiency and pulmonary embolism related to hormone replacement therapy.
The patient’s vital signs revealed a temperature of 103.2°F, 114 beats per minute pulse, 24 breaths per minute respiratory rate, and oxygen saturation of 89% on room air. On physical examination, the patient was noted to be in moderate respiratory distress with accessory muscle use and was diaphoretic. Breath sounds were diminished in the left upper and lower lung fields with significant egophony.
Tests revealed a white blood cell count of 23,300/mm3 with 30% bandemia. A chest radiograph showed an infiltrate/effusion of the entire left hemithorax (Figure 2). A computed tomography (CT) scan of the chest showed a large multiloculated left-side pleural effusion (Figure 3).
The patient was started on broad-spectrum antibiotics, including intravenous (IV) ceftriaxone, azithromycin, and clindamycin. He underwent thoracentesis on admission, yielding only 300 mL of purulent fluid, confirming its loculated status.
Serum total protein was 7.1 g/dL, and no serum lactic acid dehydrogenase (LDH) was obtained at the time of thoracentesis. Pleural fluid analysis revealed a protein of 5.2 g/dL, and an LDH of 5,176 units/L, meeting Light’s criteria for exudate based on a pleural fluid protein to serum protein ratio of > 0.5 (0.69) and pleural fluid LDH level > two-thirds of the upper limit of normal for serum LDH.
General surgery placed 2 thoracostomy tubes in the left hemithorax without significant drainage. On the first hospital day the patient seemed toxic and underwent a minithoracotomy with decortication. The Gram stain of the blood and blood cultures were negative over 72 hours. Another Gram stain of pleural fluid showed Gram-positive cocci in pairs. Pleural fluid cultures obtained during the procedure revealed S intermedius consistent with the patient’s history of aspiration and abscess formation. Antibiotic susceptibility tests were not performed on the sample.
A peripherally inserted central catheter line was placed for daily IV ceftriaxone infusions to be continued with oral clindamycin for the subsequent 4 weeks. A CT scan of the chest at 8 weeks posthospitalization revealed minimal postoperative scarring, and pulmonary function tests showed normal flow volume loop and maximum voluntary ventilation (Figure 4). The patient reported full recovery and was returned to full activity, including further Special Operations training.
Discussion
Pulmonary infections associated with near-drowning events are caused by a host of organisms that must be considered in the differential diagnosis. The most common include Aeromonas species, Burkholderia pseudomallei, Pseudallescheria boydii, Streptococcus pneumoniae, and Pseudomonas aeruginosa.2 However, the causative organism in this case was endogenous. Streptococcus intermedius is an anaerobic, Gram-positive cocci, a member of the Streptococcus milleri group, and is considered normal flora of the oral mucosa, upper respiratory tract, vagina, and gastrointestinal tract.3,4 This organism is innocuous in its normal habitat but may result in considerable mortality and morbidity if spread to alternative sites due to its ability to form abscesses and cause systemic infections.5
Although uncommon, respiratory infections caused by S intermedius typically result from aspiration of gastric or oral contents and may lead to pulmonary abscesses or empyema.1,6,7 It may present as a primary empyema.8 Current literature suggests a mortality rate between 2% and 14% with higher rates in older populations.9 A retrospective study looking at 72 cases of Streptococci viridans pulmonary infection from 1984 to 1996 found only 2 documented cases where S intermedius was identified as the cause of concomitant empyema and lung abscesses. This study also indicated a strong male predominance with only 7% of lung abscesses occurring in females.10,11
This patient developed a pulmonary abscess and empyema as a probable consequence of aspiration during underwater training exercises. The diagnosis was complicated, because the patient did not initially disclose the pertinent history, and he ignored his symptoms so that he could continue training. His actions delayed aggressive antibiotic therapy and likely led to the rapid progression of pneumonia and his complicated clinical course, because S intermedius has shown intermediate susceptibility or resistance to fluoroquinolone monotherapy.12
This case was also unusual given the subacute presentation and 3-month history of hemoptysis. On review of the available medical literature, hemoptysis is an unusual symptom of pulmonary infections caused by S intermedius but can likely be attributed to necrosis of the pulmonary tissue.8,13
Most patients with S intermedius pulmonary infection rapidly progress due to the virulence of this organism and predisposing comorbidities.14,15 However, this patient had a relatively indolent progression for 3 months, which speaks to the increased respiratory reserve of a healthy, young male in excellent cardiovascular condition.
Conclusion
This case highlights the potential for normal oral flora to cause advanced pulmonary disease in patients with no significant comorbidities. Streptococcus intermedius infections can be subacute in presentation but may rapidly progress to severe disease once seeded in the pleural cavity. Whereas early pleural space drainage remains fundamental, urgent surgical intervention may be required for loculated disease. Although infections with this organism may lead to irreversible pulmonary complications, complete resolution with full recovery is possible in young, healthy patients.
Primary care physicians must take a careful history to ensure optimal patient outcomes. This concept is particularly important to consider in aviators and Special Operations personnel who may be reluctant to seek medical care. Establishing a sense of trust among active-duty military is essential for mission accomplishment.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Weightman NC, Barnham MRD, Dove M. Streptococcus milleri group bacteraemia in North Yorkshire, England (1989-2000). Indian J Med Res. 2004;119(suppl):164-167.
2. Ender PT, Dolan MJ. Pneumonia associated with near-drowning. Clin Infect Dis. 1997;1(4):896-907.
3. Porta G, Rodriguez-Carballeira M, Gómez L, et al. Thoracic infection caused by Streptococcus milleri. Eur Respir J. 1998;12(2):357-362.
4. Van der Auwera P. Clinical significance of Streptococcus milleri. Eur J Clin Microbiol.1985;4(4):386-390.
5. Murray HW, Gross KC, Masur H, Roberts RB. Serious infections caused by Streptococcus milleri. Am J Med. 1978;64(5):759-764.
6. Shinzato T, Saito A. The Streptococcus milleri group as a cause of pulmonary infections. Clin Infect Dis. 1995;21(suppl 3):S238-S243.
7. Frankish PD, Kolbe J. Thoracic empyema due to Streptococcus milleri: Four cases. N Z Med J. 1984;97(769):849-851.
8. Iskandar SB, Al Hasan MA, Roy TM, Byrd RP Jr. Streptococcus intermedius: An unusual cause of a primary empyema. Tenn Med. 2006;99(2):37-39.
9. de Hoyos A, Sundaresan S. Thoracic empyema. Surg Clin North Am. 2002;82(3):643-671.
10. Jerng JS, Hsueh PR, Teng LJ, Lee LN, Yang PC, Luh KT. Empyema thoracis and lung abscess caused by viridans streptococci. Am J Respir Crit Care Med. 1997;156(5):1508-1514.
11. Wargo KA, McConnell VJ, Higginbotham SA. A case of Streptococcus intermedius empyema. Ann Pharmacother. 2006;40(6):1208-1210.
12. Limia A, Jiménez ML, Alarcón T, López-Brea M. Five-year analysis of antimicrobial susceptibility of the Streptococcus milleri group. Eur J Clin Microbiol Infect Dis. 1999;18(6):440-444.
13. Wong CA, Donal F, Macfarlane JT. Streptococcus milleri pulmonary disease: A review and clinical description of 25 patients. Thorax. 1995;50(10):1093-1096.
14. Shlaes DM, Lerner PI, Wolinsky E, Gopalakrishna KV. Infections due to Lancefield F and related Streptococci (S milleri, S anginosus). Medicine (Baltimore). 1981;60(3):197-207.
15. Roy WJ Jr, Roy TM, Davis GJ. Thoracic empyema due to Streptococcus intermedius. J Ky Med Assoc. 1991;89(11):558-562.
1. Weightman NC, Barnham MRD, Dove M. Streptococcus milleri group bacteraemia in North Yorkshire, England (1989-2000). Indian J Med Res. 2004;119(suppl):164-167.
2. Ender PT, Dolan MJ. Pneumonia associated with near-drowning. Clin Infect Dis. 1997;1(4):896-907.
3. Porta G, Rodriguez-Carballeira M, Gómez L, et al. Thoracic infection caused by Streptococcus milleri. Eur Respir J. 1998;12(2):357-362.
4. Van der Auwera P. Clinical significance of Streptococcus milleri. Eur J Clin Microbiol.1985;4(4):386-390.
5. Murray HW, Gross KC, Masur H, Roberts RB. Serious infections caused by Streptococcus milleri. Am J Med. 1978;64(5):759-764.
6. Shinzato T, Saito A. The Streptococcus milleri group as a cause of pulmonary infections. Clin Infect Dis. 1995;21(suppl 3):S238-S243.
7. Frankish PD, Kolbe J. Thoracic empyema due to Streptococcus milleri: Four cases. N Z Med J. 1984;97(769):849-851.
8. Iskandar SB, Al Hasan MA, Roy TM, Byrd RP Jr. Streptococcus intermedius: An unusual cause of a primary empyema. Tenn Med. 2006;99(2):37-39.
9. de Hoyos A, Sundaresan S. Thoracic empyema. Surg Clin North Am. 2002;82(3):643-671.
10. Jerng JS, Hsueh PR, Teng LJ, Lee LN, Yang PC, Luh KT. Empyema thoracis and lung abscess caused by viridans streptococci. Am J Respir Crit Care Med. 1997;156(5):1508-1514.
11. Wargo KA, McConnell VJ, Higginbotham SA. A case of Streptococcus intermedius empyema. Ann Pharmacother. 2006;40(6):1208-1210.
12. Limia A, Jiménez ML, Alarcón T, López-Brea M. Five-year analysis of antimicrobial susceptibility of the Streptococcus milleri group. Eur J Clin Microbiol Infect Dis. 1999;18(6):440-444.
13. Wong CA, Donal F, Macfarlane JT. Streptococcus milleri pulmonary disease: A review and clinical description of 25 patients. Thorax. 1995;50(10):1093-1096.
14. Shlaes DM, Lerner PI, Wolinsky E, Gopalakrishna KV. Infections due to Lancefield F and related Streptococci (S milleri, S anginosus). Medicine (Baltimore). 1981;60(3):197-207.
15. Roy WJ Jr, Roy TM, Davis GJ. Thoracic empyema due to Streptococcus intermedius. J Ky Med Assoc. 1991;89(11):558-562.

Persistent fever, left-sided neck pain, night sweats—Dx?
THE CASE
A previously healthy 35-year-old man with a one-week history of left-sided neck pain and fever as high as 104°F sought care at our emergency department. He was given a diagnosis of viral pharyngitis and discharged. He returned the next day and indicated that he was now experiencing drenching night sweats and weakness.
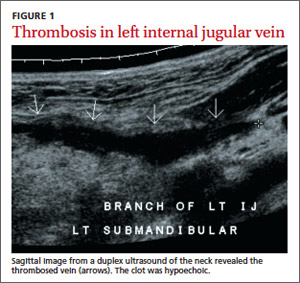
The patient was anxious, but not distressed. His temperature was 100.1°F; blood pressure, 113/65 mm Hg; heart rate, 150 beats per minute; respiratory rate, 18 breaths per minute; and oxygen saturation, 95% on room air. Head and neck examination revealed bilateral cervical lymphadenopathy with pronounced tenderness on the left side of his neck. Oral exam revealed dry mucous membranes, halitosis, and bilateral tonsillar enlargement without exudate. The cardiopulmonary exam was within normal limits. Lab tests showed a white blood cell (WBC) count of 5.9 x 109/L. An ultrasound of the neck revealed thrombosis in the left submandibular branch of the left internal jugular vein (IJV) (FIGURE 1).
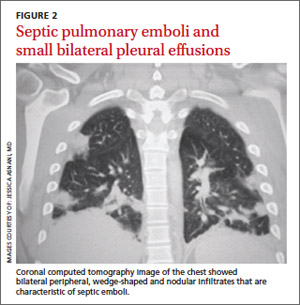
The next day, the patient remained febrile (102.8°F) and developed rigors, diarrhea, pleuritic chest pain, and an elevated WBC count (14.5). A blood culture grew gramnegative rods. The patient was started on piperacillin/tazobactam, and doxycycline was added to treat possible tick-borne infections. Computed tomography (CT) scans of the chest showed the presence of septic pulmonary emboli and small bilateral pleural effusions (FIGURE 2).
THE DIAGNOSIS
We made a diagnosis of Lemierre’s syndrome because our patient met all 4 criteria for the condition:1,2
• a recent oropharyngeal infection
• clinical or radiological evidence of IJV thrombosis
• isolation of anaerobic pathogens (mainly Fusobacterium necrophorum)
• evidence of at least one septic focus, most commonly in the lungs.
We changed the patient’s antibiotic therapy to intravenous (IV) meropenem. His WBC and fever improved, and on Day 10 he was discharged to complete a 28-day course of IV meropenem via a peripherally inserted central catheter.
DISCUSSION
Lemierre’s—A “forgotten” condition that’s making a comeback
In 1936, French microbiologist Andrew Lemierre formally characterized the syndrome in a review of 20 patients who had sepsis, metastatic pulmonary lesions, and isolation of Bacillus funduliformis (now known as F necrophorum).1,2 Other organisms that have been identified in this syndrome include Fusobacterium nucleatum, Candida, Staphylococcus, and Streptococcus.2
Before the antibiotic era, Lemierre’s syndrome was common and often fatal. But with the introduction of penicillin in the 1940s, the incidence of the syndrome dropped, and it eventually became known as “the forgotten disease.”2 Since the 1990s, however, there has been a marked resurgence of Lemierre’s syndrome.3 The incidence of Lemierre’s syndrome today is 0.6 to 2.3 cases per 1 million people per year, with a mortality rate of up to 18%.3,4
This resurgence of Lemierre’s syndrome has been linked to the restricted use of antibiotics for throat infections.3 (One study found the number of prescriptions written for antibiotics decreased by 23% from 1992 to 2000.5) Other factors cited for the increased incidence of Lemierre’s syndrome include improved identification of anaerobic organisms, more effective blood culture methods, and an increased awareness of this syndrome among clinical microbiologists.6
Diagnosis requires a high degree of suspicion
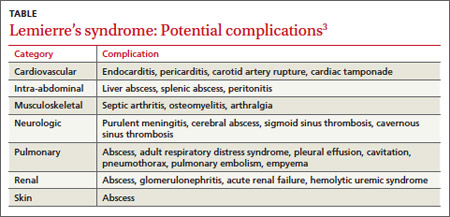
Lemierre’s syndrome typically occurs in healthy young adults. Pharyngitis is the most common initial symptom, occurring in 87% of patients.2 This is followed by a fever (102.2°F - 105.8°F) usually 4 to 5 days after the onset of sore throat.3 Other common symptoms include chills, dysphagia, dyspnea, chest pain, hemoptysis, cervical neck discomfort, arthralgia, malaise, and night sweats.2 Following suppurative thrombophlebitis of the IJV, infection spreads to other organ systems. Pulmonary involvement is the most common site (97% of cases).3 Other complications of this syndrome are listed in the TABLE.3
The differential includes mononucleosis
The differential diagnosis encompasses several common illnesses, including mononucleosis, Group A streptococcal pharyngitis, and peritonsillar abscess. However, while patients with these conditions might have a fever and an elevated WBC count, they typically would not have the pleuritic chest pain that is characteristic of Lemierre’s syndrome. In addition, while patients with peritonsillar abscess would have tonsillar exudates, patients with Lemierre’s syndrome would not likely have them.
Influenza is also part of the differential, although focal neck pain usually isn’t a finding in patients who have the flu.
Once other common illnesses have been ruled out, it’s important to have a high index of suspicion for Lemierre’s syndrome because the oropharyngeal infection may resolve by the time of presentation, and there may be few findings on physical exam.7 Therefore, suspect Lemierre’s if a patient comes in with neck pain and/or pleuritic chest pain and has a recent history of oropharyngeal infection and fever.
CT scan of the neck and chest with contrast is the optimal diagnostic modality because it allows physicians to visualize the IJV8 and detect pulmonary emboli.9 Doppler ultrasound also can be used to diagnose IJV thrombosis. Ultrasound findings would reveal an echogenic focus within a dilated IJV or a complex mass of cystic and solid components.10
Prompt antibiotic treatment is essential
Patients with Lemierre’s syndrome require prompt and appropriate antimicrobial therapy. Researchers have reported mortality rates of 25% among patients who received delayed antibiotic therapy, compared with rates of up to 18% with prompt therapy.3 Metronidazole is the most commonly prescribed antibiotic.8 When combined with ceftriaxone, it provides coverage for both F necrophorum and streptococci, a common copathogen. Monotherapy with a carbapenem antibiotic, clindamycin, ampicillin/sulbactam, or antipseudomonal penicillin also are appropriate options.5 Antimicrobial treatment for 3 to 6 weeks is recommended because relapses have been noted in patients treated for less than 2 weeks.11
Anticoagulation is controversial.2 Proponents of anticoagulation to treat Lemierre’s syndrome believe it may prevent formation of septic emboli and could expedite recovery.4,12 Others believe that clots associated with Lemierre’s syndrome dissolve on their own and that anticoagulation may increase the likelihood of septic emboli.13 Many case reports, including this one, have demonstrated that complete recovery is possible without anticoagulation.10,13-15 Anticoagulation therapy can be considered for patients with Lemierre’s syndrome in the absence of any contraindications such as gastrointestinal or intracranial bleeding.
THE TAKEAWAY
Suspect Lemierre’s syndrome when a patient complains of neck pain, high fever, rigors, dry cough, and pleuritic chest pain and mentions a sore throat that he or she had in the pretceding 7 days. Diagnosis can be confirmed by radiological findings and blood cultures positive for F. necrophorum. Patients with Lemierre’s syndrome should be promptly treated with antibiotics; evidence for anticoagulation is inconclusive.
1. Golpe R, Marin B, Alonso M. Lemierre’s syndrome (necrobacillosis). Postgrad Med J. 1999;75:141-144.
2. Wright WF, Shiner CN, Ribes JA. Lemierre syndrome. South Med J. 2012;105:283-288.
3. Riordan T, Wilson M. Lemierre’s syndrome: more than a historical curiosa. Postgrad Med J. 2004;80:328-334.
4. Ridgway JM, Parikh DA, Wright R, et al. Lemierre syndrome: a pediatric case series and review of literature. Am J Otolaryngol. 2010;31:38-45.
5. McCaig LF, Besser RE, Hughes JM. Antimicrobial drug prescription in ambulatory care settings, United States, 1992–2000. Emerg Infect Dis. 2003;9:432-437.
6. Hagelskjaer Kristensen L, Prag J. Human necrobacillosis, with emphasis on Lemierre’s syndrome. Clin Infect Dis. 2000;31:524-532.
7. Kupalli K, Livorsi D, Talati N, et al. Lemierre’s syndrome due to fusobacterium necrophorum. Lancet Infect Dis. 2012;12:808-815.
8. Armstrong AW, Spooner K, Sanders JW. Lemierre’s syndrome. Curr Infect Dis Rep. 2000;2:168-173.
9. Screaton NJ, Ravenel JG, Lehner PJ, et al. Lemierre syndrome: forgotten but not extinct--report of four cases. Radiology. 1999;213:369-374.
10. Chirinos JA, Lichtstein DM, Garcia J, et al. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine (Baltimore). 2002;81:458-465.
11. Karkos PD, Asrani S, Karkos CD, et al. Lemierre syndrome: a systematic review. Laryngoscope. 2009;119:1552-1559.
12. Phan T, So TY. Use of anticoagulation therapy for jugular vein thrombus in pediatric patients with Lemierre’s syndrome. Int J Clin Pharm. 2012;34:818-821.
13. O’Brien WT, Cohen RA. Lemierre’ syndrome. Applied Radiology. 2011;40:37-38.
14. Vandenberg SJ, Hartig GK. Lemierre’s syndrome. Otolaryngol Head Neck Surg. 1998;119:516-518.
15. Goldhagen J, Alford BA, Prewitt LH, et al. Suppurative thrombophlebitis of the internal jugular vein: report of three cases and review of the pediatric literature. Pediatr Infect Dis J. 1988;7:410-414.
THE CASE
A previously healthy 35-year-old man with a one-week history of left-sided neck pain and fever as high as 104°F sought care at our emergency department. He was given a diagnosis of viral pharyngitis and discharged. He returned the next day and indicated that he was now experiencing drenching night sweats and weakness.
The patient was anxious, but not distressed. His temperature was 100.1°F; blood pressure, 113/65 mm Hg; heart rate, 150 beats per minute; respiratory rate, 18 breaths per minute; and oxygen saturation, 95% on room air. Head and neck examination revealed bilateral cervical lymphadenopathy with pronounced tenderness on the left side of his neck. Oral exam revealed dry mucous membranes, halitosis, and bilateral tonsillar enlargement without exudate. The cardiopulmonary exam was within normal limits. Lab tests showed a white blood cell (WBC) count of 5.9 x 109/L. An ultrasound of the neck revealed thrombosis in the left submandibular branch of the left internal jugular vein (IJV) (FIGURE 1).
The next day, the patient remained febrile (102.8°F) and developed rigors, diarrhea, pleuritic chest pain, and an elevated WBC count (14.5). A blood culture grew gramnegative rods. The patient was started on piperacillin/tazobactam, and doxycycline was added to treat possible tick-borne infections. Computed tomography (CT) scans of the chest showed the presence of septic pulmonary emboli and small bilateral pleural effusions (FIGURE 2).
THE DIAGNOSIS
We made a diagnosis of Lemierre’s syndrome because our patient met all 4 criteria for the condition:1,2
• a recent oropharyngeal infection
• clinical or radiological evidence of IJV thrombosis
• isolation of anaerobic pathogens (mainly Fusobacterium necrophorum)
• evidence of at least one septic focus, most commonly in the lungs.
We changed the patient’s antibiotic therapy to intravenous (IV) meropenem. His WBC and fever improved, and on Day 10 he was discharged to complete a 28-day course of IV meropenem via a peripherally inserted central catheter.
DISCUSSION
Lemierre’s—A “forgotten” condition that’s making a comeback
In 1936, French microbiologist Andrew Lemierre formally characterized the syndrome in a review of 20 patients who had sepsis, metastatic pulmonary lesions, and isolation of Bacillus funduliformis (now known as F necrophorum).1,2 Other organisms that have been identified in this syndrome include Fusobacterium nucleatum, Candida, Staphylococcus, and Streptococcus.2
Before the antibiotic era, Lemierre’s syndrome was common and often fatal. But with the introduction of penicillin in the 1940s, the incidence of the syndrome dropped, and it eventually became known as “the forgotten disease.”2 Since the 1990s, however, there has been a marked resurgence of Lemierre’s syndrome.3 The incidence of Lemierre’s syndrome today is 0.6 to 2.3 cases per 1 million people per year, with a mortality rate of up to 18%.3,4
This resurgence of Lemierre’s syndrome has been linked to the restricted use of antibiotics for throat infections.3 (One study found the number of prescriptions written for antibiotics decreased by 23% from 1992 to 2000.5) Other factors cited for the increased incidence of Lemierre’s syndrome include improved identification of anaerobic organisms, more effective blood culture methods, and an increased awareness of this syndrome among clinical microbiologists.6
Diagnosis requires a high degree of suspicion
Lemierre’s syndrome typically occurs in healthy young adults. Pharyngitis is the most common initial symptom, occurring in 87% of patients.2 This is followed by a fever (102.2°F - 105.8°F) usually 4 to 5 days after the onset of sore throat.3 Other common symptoms include chills, dysphagia, dyspnea, chest pain, hemoptysis, cervical neck discomfort, arthralgia, malaise, and night sweats.2 Following suppurative thrombophlebitis of the IJV, infection spreads to other organ systems. Pulmonary involvement is the most common site (97% of cases).3 Other complications of this syndrome are listed in the TABLE.3
The differential includes mononucleosis
The differential diagnosis encompasses several common illnesses, including mononucleosis, Group A streptococcal pharyngitis, and peritonsillar abscess. However, while patients with these conditions might have a fever and an elevated WBC count, they typically would not have the pleuritic chest pain that is characteristic of Lemierre’s syndrome. In addition, while patients with peritonsillar abscess would have tonsillar exudates, patients with Lemierre’s syndrome would not likely have them.
Influenza is also part of the differential, although focal neck pain usually isn’t a finding in patients who have the flu.
Once other common illnesses have been ruled out, it’s important to have a high index of suspicion for Lemierre’s syndrome because the oropharyngeal infection may resolve by the time of presentation, and there may be few findings on physical exam.7 Therefore, suspect Lemierre’s if a patient comes in with neck pain and/or pleuritic chest pain and has a recent history of oropharyngeal infection and fever.
CT scan of the neck and chest with contrast is the optimal diagnostic modality because it allows physicians to visualize the IJV8 and detect pulmonary emboli.9 Doppler ultrasound also can be used to diagnose IJV thrombosis. Ultrasound findings would reveal an echogenic focus within a dilated IJV or a complex mass of cystic and solid components.10
Prompt antibiotic treatment is essential
Patients with Lemierre’s syndrome require prompt and appropriate antimicrobial therapy. Researchers have reported mortality rates of 25% among patients who received delayed antibiotic therapy, compared with rates of up to 18% with prompt therapy.3 Metronidazole is the most commonly prescribed antibiotic.8 When combined with ceftriaxone, it provides coverage for both F necrophorum and streptococci, a common copathogen. Monotherapy with a carbapenem antibiotic, clindamycin, ampicillin/sulbactam, or antipseudomonal penicillin also are appropriate options.5 Antimicrobial treatment for 3 to 6 weeks is recommended because relapses have been noted in patients treated for less than 2 weeks.11
Anticoagulation is controversial.2 Proponents of anticoagulation to treat Lemierre’s syndrome believe it may prevent formation of septic emboli and could expedite recovery.4,12 Others believe that clots associated with Lemierre’s syndrome dissolve on their own and that anticoagulation may increase the likelihood of septic emboli.13 Many case reports, including this one, have demonstrated that complete recovery is possible without anticoagulation.10,13-15 Anticoagulation therapy can be considered for patients with Lemierre’s syndrome in the absence of any contraindications such as gastrointestinal or intracranial bleeding.
THE TAKEAWAY
Suspect Lemierre’s syndrome when a patient complains of neck pain, high fever, rigors, dry cough, and pleuritic chest pain and mentions a sore throat that he or she had in the pretceding 7 days. Diagnosis can be confirmed by radiological findings and blood cultures positive for F. necrophorum. Patients with Lemierre’s syndrome should be promptly treated with antibiotics; evidence for anticoagulation is inconclusive.
THE CASE
A previously healthy 35-year-old man with a one-week history of left-sided neck pain and fever as high as 104°F sought care at our emergency department. He was given a diagnosis of viral pharyngitis and discharged. He returned the next day and indicated that he was now experiencing drenching night sweats and weakness.
The patient was anxious, but not distressed. His temperature was 100.1°F; blood pressure, 113/65 mm Hg; heart rate, 150 beats per minute; respiratory rate, 18 breaths per minute; and oxygen saturation, 95% on room air. Head and neck examination revealed bilateral cervical lymphadenopathy with pronounced tenderness on the left side of his neck. Oral exam revealed dry mucous membranes, halitosis, and bilateral tonsillar enlargement without exudate. The cardiopulmonary exam was within normal limits. Lab tests showed a white blood cell (WBC) count of 5.9 x 109/L. An ultrasound of the neck revealed thrombosis in the left submandibular branch of the left internal jugular vein (IJV) (FIGURE 1).
The next day, the patient remained febrile (102.8°F) and developed rigors, diarrhea, pleuritic chest pain, and an elevated WBC count (14.5). A blood culture grew gramnegative rods. The patient was started on piperacillin/tazobactam, and doxycycline was added to treat possible tick-borne infections. Computed tomography (CT) scans of the chest showed the presence of septic pulmonary emboli and small bilateral pleural effusions (FIGURE 2).
THE DIAGNOSIS
We made a diagnosis of Lemierre’s syndrome because our patient met all 4 criteria for the condition:1,2
• a recent oropharyngeal infection
• clinical or radiological evidence of IJV thrombosis
• isolation of anaerobic pathogens (mainly Fusobacterium necrophorum)
• evidence of at least one septic focus, most commonly in the lungs.
We changed the patient’s antibiotic therapy to intravenous (IV) meropenem. His WBC and fever improved, and on Day 10 he was discharged to complete a 28-day course of IV meropenem via a peripherally inserted central catheter.
DISCUSSION
Lemierre’s—A “forgotten” condition that’s making a comeback
In 1936, French microbiologist Andrew Lemierre formally characterized the syndrome in a review of 20 patients who had sepsis, metastatic pulmonary lesions, and isolation of Bacillus funduliformis (now known as F necrophorum).1,2 Other organisms that have been identified in this syndrome include Fusobacterium nucleatum, Candida, Staphylococcus, and Streptococcus.2
Before the antibiotic era, Lemierre’s syndrome was common and often fatal. But with the introduction of penicillin in the 1940s, the incidence of the syndrome dropped, and it eventually became known as “the forgotten disease.”2 Since the 1990s, however, there has been a marked resurgence of Lemierre’s syndrome.3 The incidence of Lemierre’s syndrome today is 0.6 to 2.3 cases per 1 million people per year, with a mortality rate of up to 18%.3,4
This resurgence of Lemierre’s syndrome has been linked to the restricted use of antibiotics for throat infections.3 (One study found the number of prescriptions written for antibiotics decreased by 23% from 1992 to 2000.5) Other factors cited for the increased incidence of Lemierre’s syndrome include improved identification of anaerobic organisms, more effective blood culture methods, and an increased awareness of this syndrome among clinical microbiologists.6
Diagnosis requires a high degree of suspicion
Lemierre’s syndrome typically occurs in healthy young adults. Pharyngitis is the most common initial symptom, occurring in 87% of patients.2 This is followed by a fever (102.2°F - 105.8°F) usually 4 to 5 days after the onset of sore throat.3 Other common symptoms include chills, dysphagia, dyspnea, chest pain, hemoptysis, cervical neck discomfort, arthralgia, malaise, and night sweats.2 Following suppurative thrombophlebitis of the IJV, infection spreads to other organ systems. Pulmonary involvement is the most common site (97% of cases).3 Other complications of this syndrome are listed in the TABLE.3
The differential includes mononucleosis
The differential diagnosis encompasses several common illnesses, including mononucleosis, Group A streptococcal pharyngitis, and peritonsillar abscess. However, while patients with these conditions might have a fever and an elevated WBC count, they typically would not have the pleuritic chest pain that is characteristic of Lemierre’s syndrome. In addition, while patients with peritonsillar abscess would have tonsillar exudates, patients with Lemierre’s syndrome would not likely have them.
Influenza is also part of the differential, although focal neck pain usually isn’t a finding in patients who have the flu.
Once other common illnesses have been ruled out, it’s important to have a high index of suspicion for Lemierre’s syndrome because the oropharyngeal infection may resolve by the time of presentation, and there may be few findings on physical exam.7 Therefore, suspect Lemierre’s if a patient comes in with neck pain and/or pleuritic chest pain and has a recent history of oropharyngeal infection and fever.
CT scan of the neck and chest with contrast is the optimal diagnostic modality because it allows physicians to visualize the IJV8 and detect pulmonary emboli.9 Doppler ultrasound also can be used to diagnose IJV thrombosis. Ultrasound findings would reveal an echogenic focus within a dilated IJV or a complex mass of cystic and solid components.10
Prompt antibiotic treatment is essential
Patients with Lemierre’s syndrome require prompt and appropriate antimicrobial therapy. Researchers have reported mortality rates of 25% among patients who received delayed antibiotic therapy, compared with rates of up to 18% with prompt therapy.3 Metronidazole is the most commonly prescribed antibiotic.8 When combined with ceftriaxone, it provides coverage for both F necrophorum and streptococci, a common copathogen. Monotherapy with a carbapenem antibiotic, clindamycin, ampicillin/sulbactam, or antipseudomonal penicillin also are appropriate options.5 Antimicrobial treatment for 3 to 6 weeks is recommended because relapses have been noted in patients treated for less than 2 weeks.11
Anticoagulation is controversial.2 Proponents of anticoagulation to treat Lemierre’s syndrome believe it may prevent formation of septic emboli and could expedite recovery.4,12 Others believe that clots associated with Lemierre’s syndrome dissolve on their own and that anticoagulation may increase the likelihood of septic emboli.13 Many case reports, including this one, have demonstrated that complete recovery is possible without anticoagulation.10,13-15 Anticoagulation therapy can be considered for patients with Lemierre’s syndrome in the absence of any contraindications such as gastrointestinal or intracranial bleeding.
THE TAKEAWAY
Suspect Lemierre’s syndrome when a patient complains of neck pain, high fever, rigors, dry cough, and pleuritic chest pain and mentions a sore throat that he or she had in the pretceding 7 days. Diagnosis can be confirmed by radiological findings and blood cultures positive for F. necrophorum. Patients with Lemierre’s syndrome should be promptly treated with antibiotics; evidence for anticoagulation is inconclusive.
1. Golpe R, Marin B, Alonso M. Lemierre’s syndrome (necrobacillosis). Postgrad Med J. 1999;75:141-144.
2. Wright WF, Shiner CN, Ribes JA. Lemierre syndrome. South Med J. 2012;105:283-288.
3. Riordan T, Wilson M. Lemierre’s syndrome: more than a historical curiosa. Postgrad Med J. 2004;80:328-334.
4. Ridgway JM, Parikh DA, Wright R, et al. Lemierre syndrome: a pediatric case series and review of literature. Am J Otolaryngol. 2010;31:38-45.
5. McCaig LF, Besser RE, Hughes JM. Antimicrobial drug prescription in ambulatory care settings, United States, 1992–2000. Emerg Infect Dis. 2003;9:432-437.
6. Hagelskjaer Kristensen L, Prag J. Human necrobacillosis, with emphasis on Lemierre’s syndrome. Clin Infect Dis. 2000;31:524-532.
7. Kupalli K, Livorsi D, Talati N, et al. Lemierre’s syndrome due to fusobacterium necrophorum. Lancet Infect Dis. 2012;12:808-815.
8. Armstrong AW, Spooner K, Sanders JW. Lemierre’s syndrome. Curr Infect Dis Rep. 2000;2:168-173.
9. Screaton NJ, Ravenel JG, Lehner PJ, et al. Lemierre syndrome: forgotten but not extinct--report of four cases. Radiology. 1999;213:369-374.
10. Chirinos JA, Lichtstein DM, Garcia J, et al. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine (Baltimore). 2002;81:458-465.
11. Karkos PD, Asrani S, Karkos CD, et al. Lemierre syndrome: a systematic review. Laryngoscope. 2009;119:1552-1559.
12. Phan T, So TY. Use of anticoagulation therapy for jugular vein thrombus in pediatric patients with Lemierre’s syndrome. Int J Clin Pharm. 2012;34:818-821.
13. O’Brien WT, Cohen RA. Lemierre’ syndrome. Applied Radiology. 2011;40:37-38.
14. Vandenberg SJ, Hartig GK. Lemierre’s syndrome. Otolaryngol Head Neck Surg. 1998;119:516-518.
15. Goldhagen J, Alford BA, Prewitt LH, et al. Suppurative thrombophlebitis of the internal jugular vein: report of three cases and review of the pediatric literature. Pediatr Infect Dis J. 1988;7:410-414.
1. Golpe R, Marin B, Alonso M. Lemierre’s syndrome (necrobacillosis). Postgrad Med J. 1999;75:141-144.
2. Wright WF, Shiner CN, Ribes JA. Lemierre syndrome. South Med J. 2012;105:283-288.
3. Riordan T, Wilson M. Lemierre’s syndrome: more than a historical curiosa. Postgrad Med J. 2004;80:328-334.
4. Ridgway JM, Parikh DA, Wright R, et al. Lemierre syndrome: a pediatric case series and review of literature. Am J Otolaryngol. 2010;31:38-45.
5. McCaig LF, Besser RE, Hughes JM. Antimicrobial drug prescription in ambulatory care settings, United States, 1992–2000. Emerg Infect Dis. 2003;9:432-437.
6. Hagelskjaer Kristensen L, Prag J. Human necrobacillosis, with emphasis on Lemierre’s syndrome. Clin Infect Dis. 2000;31:524-532.
7. Kupalli K, Livorsi D, Talati N, et al. Lemierre’s syndrome due to fusobacterium necrophorum. Lancet Infect Dis. 2012;12:808-815.
8. Armstrong AW, Spooner K, Sanders JW. Lemierre’s syndrome. Curr Infect Dis Rep. 2000;2:168-173.
9. Screaton NJ, Ravenel JG, Lehner PJ, et al. Lemierre syndrome: forgotten but not extinct--report of four cases. Radiology. 1999;213:369-374.
10. Chirinos JA, Lichtstein DM, Garcia J, et al. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine (Baltimore). 2002;81:458-465.
11. Karkos PD, Asrani S, Karkos CD, et al. Lemierre syndrome: a systematic review. Laryngoscope. 2009;119:1552-1559.
12. Phan T, So TY. Use of anticoagulation therapy for jugular vein thrombus in pediatric patients with Lemierre’s syndrome. Int J Clin Pharm. 2012;34:818-821.
13. O’Brien WT, Cohen RA. Lemierre’ syndrome. Applied Radiology. 2011;40:37-38.
14. Vandenberg SJ, Hartig GK. Lemierre’s syndrome. Otolaryngol Head Neck Surg. 1998;119:516-518.
15. Goldhagen J, Alford BA, Prewitt LH, et al. Suppurative thrombophlebitis of the internal jugular vein: report of three cases and review of the pediatric literature. Pediatr Infect Dis J. 1988;7:410-414.

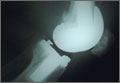
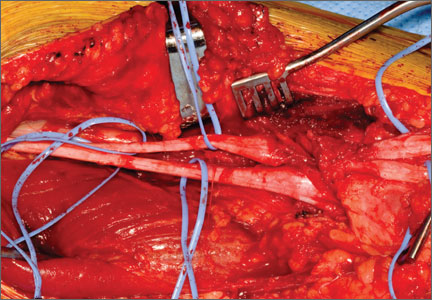
Failed First Metatarsophalangeal Arthroplasty Salvaged by Hamstring Interposition Arthroplasty: Metallic Debris From Grommets
joint, arthroplasty, implant, metallic debris, grommets, titanium, synovitis, foot
joint, arthroplasty, implant, metallic debris, grommets, titanium, synovitis, foot
joint, arthroplasty, implant, metallic debris, grommets, titanium, synovitis, foot