User login
Diabetes Mellitus: Diagnosis and Management in the Emergency Department
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
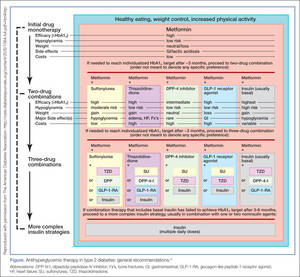
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
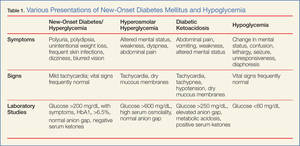
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
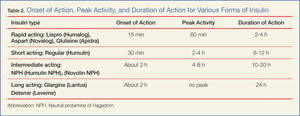
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.

Bladder Tear During Revision Total Hip Arthroplasty

Disseminated Coccidioidomycosis of the Spine in an Immunocompetent Patient

Snapping Knee Caused by Symptomatic Fabella in a Native Knee
Nonaccidental Traumatic Dislocation of the Hip in a 3-Year-Old Child: A Report of a Rare Pediatric Injury

Microprocessor Knee and Power Foot Combination in a Transfemoral Amputee
Rapid advances in technology have brought improvements in prosthetic components. In particular, prosthetic knees and ankle/foot complexes have made substantial advancements with the incorporation of computer technology. For example, microprocessor knees are relatively new; the X2 knee from Ottobock (Minneapolis, Minnesota) represents one of the latest and most advanced units and has just been upgraded.
Until recently, there have been no similarly functioning ankle/foot components except for the Proprio Foot from Össur (Foothill Ranch, California), which also provides powered dorsiflexion.
Also, recently BiOM introduced the BiOM T2 foot and ankle system with the added technology of powered plantarflexion to further normalize amputee prosthetic gait. Active patients who have successfully used a microprocessor knee, such as the X2, have generally paired that technology with a variety of foot/ankle components, ranging from passive-elastic units to advanced-energy storing units.
To normalize gait and improve biomechanics even further in select above-knee amputees, experts in the field have suggested combining a microprocessor knee with a powered foot/ankle complex. One potential obstacle to this combination, however, concerns the possible conflict between the active components of the individual units, such as over- or underengagement of component sensors. This situation, theoretically, could compromise patient safety. BiOM, however, provides training to prosthetic providers to address possible component integration issues, including microprocessor conflict and methods to safely use the components together. Once the prosthetist received this training, the patient in this study was fitted with the T2 foot and the X2 knee with excellent results and no perceived disadvantages.
Case Presentation
The patient was a 32-year-old man with a right transfemoral amputation due to trauma from a blast injury, which occurred during Marine service in Iraq. He also had a gunshot wound to his left leg, which resulted in severe injury, but this limb was salvaged and now has good residual function. Before the trauma, the patient was very athletic and involved in long-distance running and bicycling. Once he recovered from his acute injuries, the patient expressed a desire to return to his previous high level of activity and sport participation.

The experiences of these limitations pushed him to look for other prosthetic options that would offer better performance in these situations. Ultimately, he received the T2 ankle/foot with the X2 microprocessor knee after using a different combination for 2 years. He felt substantial improvements in all the aforementioned limitations and has been using the X2 and T2 combination ever since. The prosthetist provided training in both instances. For distance running, the patient uses the Flex-Run (Össur) Foot.
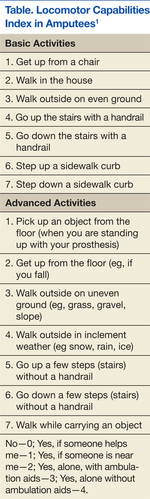
The Trinity Amputation and Prosthesis Experience Scale (TAPES) and the Locomotor Capabilities Index in Amputees (LCI) were used to assess his adjustment to the prosthetic and performance, respectively, before and after use of the aforementioned combination.
The LCI is a validated measure of lower-extremity amputees’ ability to perform activities with a prosthesis.1 The patient scored the maximum of 7 for all parameters of the LCI (a total of 28 parameters) while using his baseline prosthetic configuration of the X2 knee and the Triton foot (Ottobock). This score did not change when he used the X2/T2 combination (Figure 1; Table).
The TAPES Index is a validated measure of psychological adjustment to prosthetic integration.2 The measure consists of 12 items, rated 1 to 3 (1 = limited a lot; 2 = limited a little; and 3 = not limited at all). His total score was 25 using the X2 alone without the T2 but with the Triton foot. The patient reported that he was “limited a lot” on 2 activity measures (climbing several flights of stairs and running to catch a bus). This measure was reapplied after the patient used the T2 ankle/foot and X2 knee for several weeks. His new sum score was 36, the highest possible for this measure, indicating no functional, social, or athletic restrictions.
Furthermore, the patient reported other improvements, including an almost complete elimination of long-standing back pain, present since amputation. He reported he was able to climb hills with increased speed and less fatigue. The patient also reported he could stand more comfortably and don his shoes more easily, because the T2 would “bend.” Other subjective activity improvements included the ability to easily pick an object off the floor, step up curbs, walk on uneven ground, perform a mountain-climber exercise, and go through small spaces. He reported he was able to do all these activities previously, but the X2/T2 combination made these tasks easier than before to accomplish (Figures 2A and 2B).
Discussion
The subject of this case report is a physically active traumatic transfemoral amputee who had previous experience with several prosthetic components with the ultimate preference and use of the X2 microprocessor knee. Because of the patient’s desire for the most natural and energy-sparing gait he could achieve, a T2 foot and ankle system was added. Though objective measures of locomotion (LCI) did not change, he reported significant improvement in subjective measures of function and prosthetic acceptance (TAPES).
Reported objective advantages favoring the use of microprocessor prosthetic components most often refer to the decrease in energy consumption during locomotion. Several small studies have compared powered with nonpowered, energy-storing, or passive-elastic components and demonstrated at least modest energy savings. In a study of transtibial amputees, researchers compared oxygen consumption during locomotion in patients fitted with a passive-elastic ankle/foot with patients fitted with the powered T2.3 The researchers reported an average decrease in overall energy consumption of 8.4%. Plantarflexion and p
eak ankle-power production at push-off were both increased. The authors of this study conclude that the T2 ankle/foot allows achievement of greater biological realism.
A 2010 review by Highsmith and colleagues concluded that the microprocessor knee C-Leg demonstrated increased efficacy in safety and energy efficiency compared with other prosthetic knees for transfemoral amputees.4
Subjectively, the study patient reported less fatigue when using the X2/T2 combination than when using the X2 knee without the T2 ankle/foot. It is currently unknown whether the combination provided additive energy savings, and this area would be a good course for future investigation.

The study patient reported several subjective improvements, including reduced back pain, a more natural gait, and improved mobility. Hammarlund and colleagues found a significant prevalence of postamputation lower-extremity back pain compared with preamputation symptoms.5 This pain resulted in at least moderate disability in all subjects during prosthetic use. Morgenroth and colleagues went on to speculate that abnormal lumbar spinal kinematics could be a contributing factor for back pain in transfemoral amputees.6
Though not specifically causative, the study found that those transfemoral amputees with increased lumbar spine transverse plane motion experienced significantly more back pain than did similar amputees without lumbar spine transverse plane motion. An abnormal gait would promote more transverse plane motion than that seen in a normal gait. Normalizing prosthetic gait to best simulate the patient’s preamputation biomechanical baseline could reduce transverse lumbar spine motion, reduce back and other mechanical pain, and ultimately, reduce overall disability.

Similarly, the patient in this study also reported increased ease with hills and stairs. Many studies exist that attest to the advantages of microprocessor knees in providing improvements such as decreased stumbles, increased ability to multitask, increased satisfaction with the prosthesis, and improved stair and stance functions, such as with the Genium (Ottobock).7,8 Whether the combination of a microprocessor knee with a powered ankle/foot would further improve these aspects is yet to be objectively investigated. The report of this study patient who used the combination suggests these types of advantages but certainly as a single case report does not provide definitive answers.
The patient achieved the highest possible score on the LCI before using the X2/T2 combination and thus demonstrated a ceiling effect that has been discussed in several studies.9 Furthermore, Larsson and colleagues noted that because of the ceiling effect, the LCI was more useful for amputees of low to moderate activity levels.10 The TAPES, however, showed an improvement in before and after measurements, and assessment with it was not hindered by a ceiling effect.
Conclusion
The patient in this case report noted substantial subjective functional improvements when using the X2 compared with prior mechanical prosthetic knees paired with the T2 foot/ankle. The functional gains were further verified by significant improvement in the TAPES Index score, a validated measure of prosthetic integration. Specific subjective advantages included energy savings, almost complete resolution of back pain, and improved facility with hills, stairs, and crawl spaces. No perceived disadvantages were reported.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Franchignoni F, Orlandini D, Ferriero G, Moscato TA. Reliability, validity, and responsiveness of the locomotor capabilities index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehabil. 2004;85(5):743-748.
2. Gallagher P, MacLachlan M. Positive meaning in amputation and thoughts about the amputated limb. Prosthet Orthot Int. 2000;24(3):196-204.
3. Mancinelli C, Patritti BL, Tropea P, et al. Comparing a passive-elastic and a powered prosthesis in transtibial amputees. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:8255-8258.
4. Highsmith MJ, Kahle JT, Bongiorni DR, Sutton BS, Groer S, Kaufman KR. Safety, energy efficiency, and cost efficacy of the C-Leg for transfemoral amputees: A review of the literature. Prosthet Orthot Int. 2010;34(4):362-377.
5. Hammarlund CS, Carlström M, Melchior R, Persson BM. Prevalence of back pain, its effect on functional ability and health-related quality of life in lower limb amputees secondary to trauma or tumour: A comparison across three levels of amputation. Prosthet Orthot Int. 2011;35(1):97-105.
6. Morgenroth DC, Orendurff MS, Shakir A, Segal A, Shofer J, Czerniecki JM. The relationship between lumbar spine kinematics during gait and low-back pain in transfemoral amputees. Am J Phys Med Rehabil. 2010;89(8):635-643.
7. Hafner BJ, Willingham LL, Buell NC, Allyn KJ, Smith DG. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. 2007;88(2):207-217.
8. Bellmann M, Schmalz T, Ludwigs E, Blumentritt S. Immediate effects of a new microprocessor-controlled prosthetic knee joint: A comparative biomechanical evaluation. Arch Phys Med Rehabil. 2012;93(3):541-549.
9. Gailey RS, Scoville C, Raya M, et al. The comprehensive high level mobility predictor (CHAMP): A performance-based measure of functional ability of people with lower limb loss. Paper presented at: American Academy of Orthotists & Prosthetists 37th Academy Annual Meeting and Scientific Symposium; March 16-19, 2011; Orlando, FL.
10. Larsson B, Johannesson A, Andersson IH, Atroshi I. The Locomotor Capabilities Index; validity and reliability of the Swedish version in adults with lower limb amputation. Health Qual Life Outcomes. 2009;7:44.
Rapid advances in technology have brought improvements in prosthetic components. In particular, prosthetic knees and ankle/foot complexes have made substantial advancements with the incorporation of computer technology. For example, microprocessor knees are relatively new; the X2 knee from Ottobock (Minneapolis, Minnesota) represents one of the latest and most advanced units and has just been upgraded.
Until recently, there have been no similarly functioning ankle/foot components except for the Proprio Foot from Össur (Foothill Ranch, California), which also provides powered dorsiflexion.
Also, recently BiOM introduced the BiOM T2 foot and ankle system with the added technology of powered plantarflexion to further normalize amputee prosthetic gait. Active patients who have successfully used a microprocessor knee, such as the X2, have generally paired that technology with a variety of foot/ankle components, ranging from passive-elastic units to advanced-energy storing units.
To normalize gait and improve biomechanics even further in select above-knee amputees, experts in the field have suggested combining a microprocessor knee with a powered foot/ankle complex. One potential obstacle to this combination, however, concerns the possible conflict between the active components of the individual units, such as over- or underengagement of component sensors. This situation, theoretically, could compromise patient safety. BiOM, however, provides training to prosthetic providers to address possible component integration issues, including microprocessor conflict and methods to safely use the components together. Once the prosthetist received this training, the patient in this study was fitted with the T2 foot and the X2 knee with excellent results and no perceived disadvantages.
Case Presentation
The patient was a 32-year-old man with a right transfemoral amputation due to trauma from a blast injury, which occurred during Marine service in Iraq. He also had a gunshot wound to his left leg, which resulted in severe injury, but this limb was salvaged and now has good residual function. Before the trauma, the patient was very athletic and involved in long-distance running and bicycling. Once he recovered from his acute injuries, the patient expressed a desire to return to his previous high level of activity and sport participation.
The experiences of these limitations pushed him to look for other prosthetic options that would offer better performance in these situations. Ultimately, he received the T2 ankle/foot with the X2 microprocessor knee after using a different combination for 2 years. He felt substantial improvements in all the aforementioned limitations and has been using the X2 and T2 combination ever since. The prosthetist provided training in both instances. For distance running, the patient uses the Flex-Run (Össur) Foot.
The Trinity Amputation and Prosthesis Experience Scale (TAPES) and the Locomotor Capabilities Index in Amputees (LCI) were used to assess his adjustment to the prosthetic and performance, respectively, before and after use of the aforementioned combination.
The LCI is a validated measure of lower-extremity amputees’ ability to perform activities with a prosthesis.1 The patient scored the maximum of 7 for all parameters of the LCI (a total of 28 parameters) while using his baseline prosthetic configuration of the X2 knee and the Triton foot (Ottobock). This score did not change when he used the X2/T2 combination (Figure 1; Table).
The TAPES Index is a validated measure of psychological adjustment to prosthetic integration.2 The measure consists of 12 items, rated 1 to 3 (1 = limited a lot; 2 = limited a little; and 3 = not limited at all). His total score was 25 using the X2 alone without the T2 but with the Triton foot. The patient reported that he was “limited a lot” on 2 activity measures (climbing several flights of stairs and running to catch a bus). This measure was reapplied after the patient used the T2 ankle/foot and X2 knee for several weeks. His new sum score was 36, the highest possible for this measure, indicating no functional, social, or athletic restrictions.
Furthermore, the patient reported other improvements, including an almost complete elimination of long-standing back pain, present since amputation. He reported he was able to climb hills with increased speed and less fatigue. The patient also reported he could stand more comfortably and don his shoes more easily, because the T2 would “bend.” Other subjective activity improvements included the ability to easily pick an object off the floor, step up curbs, walk on uneven ground, perform a mountain-climber exercise, and go through small spaces. He reported he was able to do all these activities previously, but the X2/T2 combination made these tasks easier than before to accomplish (Figures 2A and 2B).
Discussion
The subject of this case report is a physically active traumatic transfemoral amputee who had previous experience with several prosthetic components with the ultimate preference and use of the X2 microprocessor knee. Because of the patient’s desire for the most natural and energy-sparing gait he could achieve, a T2 foot and ankle system was added. Though objective measures of locomotion (LCI) did not change, he reported significant improvement in subjective measures of function and prosthetic acceptance (TAPES).
Reported objective advantages favoring the use of microprocessor prosthetic components most often refer to the decrease in energy consumption during locomotion. Several small studies have compared powered with nonpowered, energy-storing, or passive-elastic components and demonstrated at least modest energy savings. In a study of transtibial amputees, researchers compared oxygen consumption during locomotion in patients fitted with a passive-elastic ankle/foot with patients fitted with the powered T2.3 The researchers reported an average decrease in overall energy consumption of 8.4%. Plantarflexion and p
eak ankle-power production at push-off were both increased. The authors of this study conclude that the T2 ankle/foot allows achievement of greater biological realism.
A 2010 review by Highsmith and colleagues concluded that the microprocessor knee C-Leg demonstrated increased efficacy in safety and energy efficiency compared with other prosthetic knees for transfemoral amputees.4
Subjectively, the study patient reported less fatigue when using the X2/T2 combination than when using the X2 knee without the T2 ankle/foot. It is currently unknown whether the combination provided additive energy savings, and this area would be a good course for future investigation.
The study patient reported several subjective improvements, including reduced back pain, a more natural gait, and improved mobility. Hammarlund and colleagues found a significant prevalence of postamputation lower-extremity back pain compared with preamputation symptoms.5 This pain resulted in at least moderate disability in all subjects during prosthetic use. Morgenroth and colleagues went on to speculate that abnormal lumbar spinal kinematics could be a contributing factor for back pain in transfemoral amputees.6
Though not specifically causative, the study found that those transfemoral amputees with increased lumbar spine transverse plane motion experienced significantly more back pain than did similar amputees without lumbar spine transverse plane motion. An abnormal gait would promote more transverse plane motion than that seen in a normal gait. Normalizing prosthetic gait to best simulate the patient’s preamputation biomechanical baseline could reduce transverse lumbar spine motion, reduce back and other mechanical pain, and ultimately, reduce overall disability.
Similarly, the patient in this study also reported increased ease with hills and stairs. Many studies exist that attest to the advantages of microprocessor knees in providing improvements such as decreased stumbles, increased ability to multitask, increased satisfaction with the prosthesis, and improved stair and stance functions, such as with the Genium (Ottobock).7,8 Whether the combination of a microprocessor knee with a powered ankle/foot would further improve these aspects is yet to be objectively investigated. The report of this study patient who used the combination suggests these types of advantages but certainly as a single case report does not provide definitive answers.
The patient achieved the highest possible score on the LCI before using the X2/T2 combination and thus demonstrated a ceiling effect that has been discussed in several studies.9 Furthermore, Larsson and colleagues noted that because of the ceiling effect, the LCI was more useful for amputees of low to moderate activity levels.10 The TAPES, however, showed an improvement in before and after measurements, and assessment with it was not hindered by a ceiling effect.
Conclusion
The patient in this case report noted substantial subjective functional improvements when using the X2 compared with prior mechanical prosthetic knees paired with the T2 foot/ankle. The functional gains were further verified by significant improvement in the TAPES Index score, a validated measure of prosthetic integration. Specific subjective advantages included energy savings, almost complete resolution of back pain, and improved facility with hills, stairs, and crawl spaces. No perceived disadvantages were reported.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Rapid advances in technology have brought improvements in prosthetic components. In particular, prosthetic knees and ankle/foot complexes have made substantial advancements with the incorporation of computer technology. For example, microprocessor knees are relatively new; the X2 knee from Ottobock (Minneapolis, Minnesota) represents one of the latest and most advanced units and has just been upgraded.
Until recently, there have been no similarly functioning ankle/foot components except for the Proprio Foot from Össur (Foothill Ranch, California), which also provides powered dorsiflexion.
Also, recently BiOM introduced the BiOM T2 foot and ankle system with the added technology of powered plantarflexion to further normalize amputee prosthetic gait. Active patients who have successfully used a microprocessor knee, such as the X2, have generally paired that technology with a variety of foot/ankle components, ranging from passive-elastic units to advanced-energy storing units.
To normalize gait and improve biomechanics even further in select above-knee amputees, experts in the field have suggested combining a microprocessor knee with a powered foot/ankle complex. One potential obstacle to this combination, however, concerns the possible conflict between the active components of the individual units, such as over- or underengagement of component sensors. This situation, theoretically, could compromise patient safety. BiOM, however, provides training to prosthetic providers to address possible component integration issues, including microprocessor conflict and methods to safely use the components together. Once the prosthetist received this training, the patient in this study was fitted with the T2 foot and the X2 knee with excellent results and no perceived disadvantages.
Case Presentation
The patient was a 32-year-old man with a right transfemoral amputation due to trauma from a blast injury, which occurred during Marine service in Iraq. He also had a gunshot wound to his left leg, which resulted in severe injury, but this limb was salvaged and now has good residual function. Before the trauma, the patient was very athletic and involved in long-distance running and bicycling. Once he recovered from his acute injuries, the patient expressed a desire to return to his previous high level of activity and sport participation.
The experiences of these limitations pushed him to look for other prosthetic options that would offer better performance in these situations. Ultimately, he received the T2 ankle/foot with the X2 microprocessor knee after using a different combination for 2 years. He felt substantial improvements in all the aforementioned limitations and has been using the X2 and T2 combination ever since. The prosthetist provided training in both instances. For distance running, the patient uses the Flex-Run (Össur) Foot.
The Trinity Amputation and Prosthesis Experience Scale (TAPES) and the Locomotor Capabilities Index in Amputees (LCI) were used to assess his adjustment to the prosthetic and performance, respectively, before and after use of the aforementioned combination.
The LCI is a validated measure of lower-extremity amputees’ ability to perform activities with a prosthesis.1 The patient scored the maximum of 7 for all parameters of the LCI (a total of 28 parameters) while using his baseline prosthetic configuration of the X2 knee and the Triton foot (Ottobock). This score did not change when he used the X2/T2 combination (Figure 1; Table).
The TAPES Index is a validated measure of psychological adjustment to prosthetic integration.2 The measure consists of 12 items, rated 1 to 3 (1 = limited a lot; 2 = limited a little; and 3 = not limited at all). His total score was 25 using the X2 alone without the T2 but with the Triton foot. The patient reported that he was “limited a lot” on 2 activity measures (climbing several flights of stairs and running to catch a bus). This measure was reapplied after the patient used the T2 ankle/foot and X2 knee for several weeks. His new sum score was 36, the highest possible for this measure, indicating no functional, social, or athletic restrictions.
Furthermore, the patient reported other improvements, including an almost complete elimination of long-standing back pain, present since amputation. He reported he was able to climb hills with increased speed and less fatigue. The patient also reported he could stand more comfortably and don his shoes more easily, because the T2 would “bend.” Other subjective activity improvements included the ability to easily pick an object off the floor, step up curbs, walk on uneven ground, perform a mountain-climber exercise, and go through small spaces. He reported he was able to do all these activities previously, but the X2/T2 combination made these tasks easier than before to accomplish (Figures 2A and 2B).
Discussion
The subject of this case report is a physically active traumatic transfemoral amputee who had previous experience with several prosthetic components with the ultimate preference and use of the X2 microprocessor knee. Because of the patient’s desire for the most natural and energy-sparing gait he could achieve, a T2 foot and ankle system was added. Though objective measures of locomotion (LCI) did not change, he reported significant improvement in subjective measures of function and prosthetic acceptance (TAPES).
Reported objective advantages favoring the use of microprocessor prosthetic components most often refer to the decrease in energy consumption during locomotion. Several small studies have compared powered with nonpowered, energy-storing, or passive-elastic components and demonstrated at least modest energy savings. In a study of transtibial amputees, researchers compared oxygen consumption during locomotion in patients fitted with a passive-elastic ankle/foot with patients fitted with the powered T2.3 The researchers reported an average decrease in overall energy consumption of 8.4%. Plantarflexion and p
eak ankle-power production at push-off were both increased. The authors of this study conclude that the T2 ankle/foot allows achievement of greater biological realism.
A 2010 review by Highsmith and colleagues concluded that the microprocessor knee C-Leg demonstrated increased efficacy in safety and energy efficiency compared with other prosthetic knees for transfemoral amputees.4
Subjectively, the study patient reported less fatigue when using the X2/T2 combination than when using the X2 knee without the T2 ankle/foot. It is currently unknown whether the combination provided additive energy savings, and this area would be a good course for future investigation.
The study patient reported several subjective improvements, including reduced back pain, a more natural gait, and improved mobility. Hammarlund and colleagues found a significant prevalence of postamputation lower-extremity back pain compared with preamputation symptoms.5 This pain resulted in at least moderate disability in all subjects during prosthetic use. Morgenroth and colleagues went on to speculate that abnormal lumbar spinal kinematics could be a contributing factor for back pain in transfemoral amputees.6
Though not specifically causative, the study found that those transfemoral amputees with increased lumbar spine transverse plane motion experienced significantly more back pain than did similar amputees without lumbar spine transverse plane motion. An abnormal gait would promote more transverse plane motion than that seen in a normal gait. Normalizing prosthetic gait to best simulate the patient’s preamputation biomechanical baseline could reduce transverse lumbar spine motion, reduce back and other mechanical pain, and ultimately, reduce overall disability.
Similarly, the patient in this study also reported increased ease with hills and stairs. Many studies exist that attest to the advantages of microprocessor knees in providing improvements such as decreased stumbles, increased ability to multitask, increased satisfaction with the prosthesis, and improved stair and stance functions, such as with the Genium (Ottobock).7,8 Whether the combination of a microprocessor knee with a powered ankle/foot would further improve these aspects is yet to be objectively investigated. The report of this study patient who used the combination suggests these types of advantages but certainly as a single case report does not provide definitive answers.
The patient achieved the highest possible score on the LCI before using the X2/T2 combination and thus demonstrated a ceiling effect that has been discussed in several studies.9 Furthermore, Larsson and colleagues noted that because of the ceiling effect, the LCI was more useful for amputees of low to moderate activity levels.10 The TAPES, however, showed an improvement in before and after measurements, and assessment with it was not hindered by a ceiling effect.
Conclusion
The patient in this case report noted substantial subjective functional improvements when using the X2 compared with prior mechanical prosthetic knees paired with the T2 foot/ankle. The functional gains were further verified by significant improvement in the TAPES Index score, a validated measure of prosthetic integration. Specific subjective advantages included energy savings, almost complete resolution of back pain, and improved facility with hills, stairs, and crawl spaces. No perceived disadvantages were reported.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Franchignoni F, Orlandini D, Ferriero G, Moscato TA. Reliability, validity, and responsiveness of the locomotor capabilities index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehabil. 2004;85(5):743-748.
2. Gallagher P, MacLachlan M. Positive meaning in amputation and thoughts about the amputated limb. Prosthet Orthot Int. 2000;24(3):196-204.
3. Mancinelli C, Patritti BL, Tropea P, et al. Comparing a passive-elastic and a powered prosthesis in transtibial amputees. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:8255-8258.
4. Highsmith MJ, Kahle JT, Bongiorni DR, Sutton BS, Groer S, Kaufman KR. Safety, energy efficiency, and cost efficacy of the C-Leg for transfemoral amputees: A review of the literature. Prosthet Orthot Int. 2010;34(4):362-377.
5. Hammarlund CS, Carlström M, Melchior R, Persson BM. Prevalence of back pain, its effect on functional ability and health-related quality of life in lower limb amputees secondary to trauma or tumour: A comparison across three levels of amputation. Prosthet Orthot Int. 2011;35(1):97-105.
6. Morgenroth DC, Orendurff MS, Shakir A, Segal A, Shofer J, Czerniecki JM. The relationship between lumbar spine kinematics during gait and low-back pain in transfemoral amputees. Am J Phys Med Rehabil. 2010;89(8):635-643.
7. Hafner BJ, Willingham LL, Buell NC, Allyn KJ, Smith DG. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. 2007;88(2):207-217.
8. Bellmann M, Schmalz T, Ludwigs E, Blumentritt S. Immediate effects of a new microprocessor-controlled prosthetic knee joint: A comparative biomechanical evaluation. Arch Phys Med Rehabil. 2012;93(3):541-549.
9. Gailey RS, Scoville C, Raya M, et al. The comprehensive high level mobility predictor (CHAMP): A performance-based measure of functional ability of people with lower limb loss. Paper presented at: American Academy of Orthotists & Prosthetists 37th Academy Annual Meeting and Scientific Symposium; March 16-19, 2011; Orlando, FL.
10. Larsson B, Johannesson A, Andersson IH, Atroshi I. The Locomotor Capabilities Index; validity and reliability of the Swedish version in adults with lower limb amputation. Health Qual Life Outcomes. 2009;7:44.
1. Franchignoni F, Orlandini D, Ferriero G, Moscato TA. Reliability, validity, and responsiveness of the locomotor capabilities index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehabil. 2004;85(5):743-748.
2. Gallagher P, MacLachlan M. Positive meaning in amputation and thoughts about the amputated limb. Prosthet Orthot Int. 2000;24(3):196-204.
3. Mancinelli C, Patritti BL, Tropea P, et al. Comparing a passive-elastic and a powered prosthesis in transtibial amputees. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:8255-8258.
4. Highsmith MJ, Kahle JT, Bongiorni DR, Sutton BS, Groer S, Kaufman KR. Safety, energy efficiency, and cost efficacy of the C-Leg for transfemoral amputees: A review of the literature. Prosthet Orthot Int. 2010;34(4):362-377.
5. Hammarlund CS, Carlström M, Melchior R, Persson BM. Prevalence of back pain, its effect on functional ability and health-related quality of life in lower limb amputees secondary to trauma or tumour: A comparison across three levels of amputation. Prosthet Orthot Int. 2011;35(1):97-105.
6. Morgenroth DC, Orendurff MS, Shakir A, Segal A, Shofer J, Czerniecki JM. The relationship between lumbar spine kinematics during gait and low-back pain in transfemoral amputees. Am J Phys Med Rehabil. 2010;89(8):635-643.
7. Hafner BJ, Willingham LL, Buell NC, Allyn KJ, Smith DG. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. 2007;88(2):207-217.
8. Bellmann M, Schmalz T, Ludwigs E, Blumentritt S. Immediate effects of a new microprocessor-controlled prosthetic knee joint: A comparative biomechanical evaluation. Arch Phys Med Rehabil. 2012;93(3):541-549.
9. Gailey RS, Scoville C, Raya M, et al. The comprehensive high level mobility predictor (CHAMP): A performance-based measure of functional ability of people with lower limb loss. Paper presented at: American Academy of Orthotists & Prosthetists 37th Academy Annual Meeting and Scientific Symposium; March 16-19, 2011; Orlando, FL.
10. Larsson B, Johannesson A, Andersson IH, Atroshi I. The Locomotor Capabilities Index; validity and reliability of the Swedish version in adults with lower limb amputation. Health Qual Life Outcomes. 2009;7:44.

Bacteremia From an Unlikely Source
The most common microbes causing postoperative wound infection are Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, Staphylococcus epidermidis, and Enterococcus faecalis.1 Pasteurella multocida (P multocida) is an uncommon organism causing surgical-site infections.2 This article reports a case of a patient who developed a postoperative wound infection due to P multocida complicated by a bloodstream infection.
CASE REPORT
A 54-year-old man presented with pain and discharge surrounding his recent surgical site and a 1-day history of fever and chills. Four weeks prior to the presentation, he underwent nodal dissection and reconstructive surgery with a muscle flap on his right leg for a superficial spreading melanoma. The patient noticed wound dehiscence the previous 2 to 3 days and a white-yellowish discharge from the wound.
Six years previously, the patient was diagnosed with a superficial spreading melanoma on his right thigh. At that time, he underwent wide excision for the localized disease. The patient was doing well until 3 months prior to the admission when he noticed a nodule in his right groin area, which had enlarged to a lump. Fine needle aspiration of the lump and immunohistochemistry showed the presence of malignant cells, positive for S100 and MART-1.These markers are useful for a diagnosis of metastatic melanoma.3,4
A positron emission tomography (PET) scan revealed localized disease with increased uptake only in the groin region. Superficial nodal dissection and sartorius muscle flap placement were performed, and the patient was discharged to his home with drains in place.
Two weeks after his node dissection, the patient was seen in the surgery clinic, and his drains were removed. Three days after his clinic visit, he noticed erythema around the suture line and discharge from the wound, followed by increasing pain, high fever, and chills. The patient reported no history of nausea, vomiting, diarrhea, painful urination, cough, shortness of breath, chest pain, or abdominal pain. His medical history was also significant for hypertension and multiple lipomas on his back and extremities, which were removed surgically 15 years previously. He had been a chronic smoker and occasionally used alcohol but did not use illicit drugs. The patient was unmarried and lived alone with his domestic cats.
The patient was febrile on admission (38.9°C); heart rate 110 bpm. His blood pressure and respiratory rate were normal. An examination of the right groin revealed an incision mark of about 20 cm in length from his right anterior superior iliac spine travelling inferomedially into his groin with breakdown at the infero-medial aspect, extending one-half to one-third the wound distance. The wound had clean borders with minimal amount of purulent drainage. Induration was noted, extending down the thigh to above the knee level. Sutures remained in place along the superior aspect of the incision site. No other abnormalities were found.
Laboratory studies revealed leucocytosis (white blood cell count, 12,200/mm3). Blood glucose, blood urea nitrogen, serum creatinine, and electrolytes were within normal range. Computerized tomography (CT) scans of the pelvis and thighs with IV contrast revealed normal right common femoral artery and vein with postsurgical changes and thickening of the skin and small air lucencies in the right groin. The patient was started on empiric treatment with IV vancomycin and piperacillin/tazobactam.
Due to initial worsening of erythema, piperacillin/tazobactam were stopped and ertapenem was initiated. Blood cultures sets and the culture of the surgical wound were positive for P multocida. Vancomycin was discontinued, and the patient rapidly improved. He was discharged on oral moxifloxacin for 2 weeks. After 10 months of follow-up, the patient was doing well and the surgical site wound had healed.
DISCUSSION
Pasteurella multocida is a small, Gram-negative, nonmotile, non–spore-forming coccobacillus with bipolar staining features.5 It often exists as a commensal in the upper respiratory tracts of domestic pet species, especially cats and dogs, and may cause hemorrhagic septicemia in cattle, fowl cholera in chickens, and atrophic rhinitis in pigs.6,7Pasteurella multocida infection in humans is often associated with an animal bite, scratch, or lick, but infection without epidemiologic evidence of animal contact may occur.8
The majority of animal bites involve dogs (85%-90%), followed by cats (5%-10%). Infectious complications occur in about 15% to 20% of dog-related bites and > 50% of cat-related bites. The sharp and long teeth of cats can easily penetrate human skin, create a deep puncture wound, and even inoculate the periosteal component of bones. Cat-related wounds more commonly progress to serious and deeper tissue infections, including osteomyelitis and meningitis.9 Human-to-human transmission is rare, but there are reported cases of respiratory transmission and maternal-to-fetal transmission.10,11
The most common presentation of P multocida infection in humans is soft-tissue infection, appearing as purulent wounds (48%), cellulitis (36%), or abscesses (16%).12 The infection is characterized by the development of soft-tissue inflammation at the site of contact, which may progress to diffuse, localized cellulitis. High leukocyte and neutrophil counts are typically observed.13 Complications of localized infection include rapidly progressive cellulitis, abscesses, tenosynovitis, osteomyelitis, and septic arthritis. The localized infection can also lead to septicemia, which carries a high mortality rate (31%).12,14
Pasteurella multocida septicemia commonly occurs in patients with an immune-compromised status, but septicemia in healthy individuals has also been reported.15,16 Apart from local skin and soft-tissue infections, P multocida can cause upper respiratory tract infections, lower respiratory tract infections leading to pneumonia, trachea-bronchitis, lung abscess, and empyema, usually in individuals with underlying pulmonary disease. Pasteurella multocida meningitis has been associated with cat licks and bites occurring on the face in both the young and the elderly.17-19
Gram stains of purulent material or other fluid specimens, including blood, sputum, and cerebrospinal fluid, may show small, Gram-negative, nonmotile, non–spore-forming pleomorphic coccobacilli. Wright, Giemsa, and Wayson stains enhance bipolar staining. The quickest and most accurate method for confirming an active P multocida infection is molecular detection using polymerase chain reaction.20 Evaluations of tenosynovitis, septic arthritis, osteomyelitis, and meningeal enhancement, when appropriate, should be done with CT scans or MRIs.
In < 10% of cases, localized infection by P multocida may lead to bacteremia. The most common predisposing factors associated with bacteremia identified in a review of cases over 20 years at an urban medical center included old age and chronic medical conditions.21 Chronic medical conditions involved most commonly were diabetes mellitus, hypertension, and congestive heart failure. Liver dysfunction has also been reported as a significant risk factor in cases of P multocida bacteremia. The most common antibiotics used to treat the patients with bacteremia were ampicillin/sulbactam, cephalosporins, and fluoroquinolones.
A brief review of the literature of 21 cases of bacteremia showed that the most common antibiotics used for treatment were penicillins (ampicillin, amoxicillin, and piperacillin) in 11 of 21 cases. After penicillin, ciprofloxacin was the most commonly used antibiotic to treat bacteremia secondary to P multocida. The review also identified chronic medical conditions, such as diabetes mellitus, hypertension, congestive heart failure, and chronic obstructive pulmonary disease, as the most common risk factors associated in these cases with bacteremia.
In 17 of 20 cases, patients reported being present in an environment with pets, mostly cats and dogs. Twelve out of 17 patients reported having contact with pet cats and dogs, mostly in the form of bites or pets licking their wounds, and 3 of these were postoperative patients with external wounds.22-24
This patient reported that after discharge from the hospital following surgery for his spreading melanoma, domestic cats at his home repeatedly licked the postoperative wound. This almost certainly was the source of the infection and bacteremia in this patient. These findings stress the importance of educating patients about proper postoperative wound care and precautions needed if there is potential exposure to domestic animals, such as cats and dogs.
CONCLUSIONS
Pasteurella multocida is an unusual cause of postoperative wound infection. The most common method of acquiring a P multocida infection is through contact with pet animals, mostly cats and dogs. Infection can occur not only with animal bites and scratches, but also with licking of open wounds. The rate of infections can be decreased significantly by educating patients about the mode of transmission of infection, its complications, and safety measures needed if they have pets at home.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Giacometti A, Cirioni O, Schimizzi AM, et al. Epidemiology and microbiology of surgical wound infection. J Clin Microbiol. 2000;38(2):918-919.
2. Cook PP. Persistent postoperative wound infection with Pasteurella multocida: Case report and literature review. Infection. 1995;23(4):252.
3. Hodi FS. Well-defined melanoma antigens as progression markers for melanoma: Insights into differential expression and host response based on stage. Clin Cancer Res. 2006;12(3, pt 1):673-678.
4. Zubovits J, Buzney E, Yu L, Duncan LM. HMB-45, S-100, NK1/C3, and MART-1 in metastatic melanoma. Hum Pathol. 2004;35(2):217-223.
5. Zurlo JJ. Pasteurella species. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2005:2687-2691.
6. Waghorn DJ, Robson M. Occupational risk of Pasteurella multocida septicaemia and premature labor in a pregnant vet. BJOG. 2003;110(8):780-781.
7. Francis DP, Holmes MA, Brandon G. Pasteurella multocida infections after domestic animal bites and scratches. JAMA. 1975;233(1):42-45.
8. Cordoba A, Bueno I, Monterrubio J, Corcho G. Surgical wound infection due to Pasteurella multocida [article in Spanish]. Enferm Infecc Microbiol Clin. 2002;20(10):536-537.
9. Kopita JM, Handshoe D, Kussin PS, Kelemen M. Cat germs! Pleuropulmonary pasteurella infection in an old man. N C Med J. 1993;54(7):308-311.
10. Hubert WT, Rosen MN. Pasteurella multocida infections. II. Pasteurella multocida infection in man unrelated to animal bite. Am J Pub Health Nations Health. 1970;60(6):1109-1117.
11. Escande F, Borde M, Pateyron F. Infection maternelle et néonatale à Pasteurella multocida. Arch Pediatr. 1997;4(11):1116-1118.
12. Luchansky M, Bergman M, Djaldetti R, Salman H. Cat bite in an old patient: Is it a simple injury? Eur J Emerg Med. 2003;10(2):130-132.
13. Ryan KJ, Ray CG, eds. Sherris Medical Microbiology. 4th ed. New York, NY: McGraw Hill; 2000.
14. Weber DJ, Wolfson JS, Swartz MN, Hooper DC. Pasteurella multocida infections. Report of 34 cases and review of the literature. Medicine (Baltimore). 1984;63(3):133-154.
15. Kimura R, Hayashi Y, Takeuchi T, Shimizu M, et al. Pasteurella multocida septicemia caused by close contact with a domestic cat: Case report and literature review. J Infect Chemother. 2004;10(4):250-252.
16. Albert TJ, Stevens DL. The first case of Pasteurella canis bacteremia: A cirrhotic patient with an open leg wound. Infection. 2010;38(6):483-485.
17. Lion C, Lozniewski A, Rosner V, Weber M. Lung abscess due to beta-lactamase-producing Pasteurella multocida. Clin Infect Dis. 1999;29(5):1345-1346.
18. Fernández-Esparrach G, Mascaró J, Rota R, Valerio L. Septicemia, peritonitis, and empyema due to Pasteurella multocida in a cirrhotic patient. Clin Infect Dis. 1994;18(3):486.
19. Wade T, Booy R, Teare EL, Kroll S. Pasteurella multocida meningitis in infancy—(a lick may be as bad as a bite). Eur J Pediatr. 1999;158(11):875-878.
20. Miflin JK, Balckall PJ. Development of a 23S rRNA-based PCR assay for the identification of Pasteurella multocida. Lett Appl Microbiol. 2001;33(3):216-221.
21. Ebright J, Frey AB, Fairfax MR. Pasteurella multocida infections and bacteremia: A twenty-year experience at an urban medical center. Infect Dis Clin Pract. 2009;17(2):102-104.
22. Baillot R, Voisine P, Côté LM, Longtin Y. Deep sternal wound infection due to Pasteurella multocida: The first case report and review of literature. Infection. 2011;39(6):575-578.
23. Baskar B, Desai SP, Parsons MA. Postoperative endophthalmitis due to Pasteurella multocida. Br J Ophthalmol. 1997;81(2):172-173.
24. Chun ML, Buekers TE, Sood AK, Sorosky JI. Postoperative wound infection with Pasteurella multocida from a pet cat. Am J Obstet Gynecol. 2003;188(4):1115-1116.
The most common microbes causing postoperative wound infection are Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, Staphylococcus epidermidis, and Enterococcus faecalis.1 Pasteurella multocida (P multocida) is an uncommon organism causing surgical-site infections.2 This article reports a case of a patient who developed a postoperative wound infection due to P multocida complicated by a bloodstream infection.
CASE REPORT
A 54-year-old man presented with pain and discharge surrounding his recent surgical site and a 1-day history of fever and chills. Four weeks prior to the presentation, he underwent nodal dissection and reconstructive surgery with a muscle flap on his right leg for a superficial spreading melanoma. The patient noticed wound dehiscence the previous 2 to 3 days and a white-yellowish discharge from the wound.
Six years previously, the patient was diagnosed with a superficial spreading melanoma on his right thigh. At that time, he underwent wide excision for the localized disease. The patient was doing well until 3 months prior to the admission when he noticed a nodule in his right groin area, which had enlarged to a lump. Fine needle aspiration of the lump and immunohistochemistry showed the presence of malignant cells, positive for S100 and MART-1.These markers are useful for a diagnosis of metastatic melanoma.3,4
A positron emission tomography (PET) scan revealed localized disease with increased uptake only in the groin region. Superficial nodal dissection and sartorius muscle flap placement were performed, and the patient was discharged to his home with drains in place.
Two weeks after his node dissection, the patient was seen in the surgery clinic, and his drains were removed. Three days after his clinic visit, he noticed erythema around the suture line and discharge from the wound, followed by increasing pain, high fever, and chills. The patient reported no history of nausea, vomiting, diarrhea, painful urination, cough, shortness of breath, chest pain, or abdominal pain. His medical history was also significant for hypertension and multiple lipomas on his back and extremities, which were removed surgically 15 years previously. He had been a chronic smoker and occasionally used alcohol but did not use illicit drugs. The patient was unmarried and lived alone with his domestic cats.
The patient was febrile on admission (38.9°C); heart rate 110 bpm. His blood pressure and respiratory rate were normal. An examination of the right groin revealed an incision mark of about 20 cm in length from his right anterior superior iliac spine travelling inferomedially into his groin with breakdown at the infero-medial aspect, extending one-half to one-third the wound distance. The wound had clean borders with minimal amount of purulent drainage. Induration was noted, extending down the thigh to above the knee level. Sutures remained in place along the superior aspect of the incision site. No other abnormalities were found.
Laboratory studies revealed leucocytosis (white blood cell count, 12,200/mm3). Blood glucose, blood urea nitrogen, serum creatinine, and electrolytes were within normal range. Computerized tomography (CT) scans of the pelvis and thighs with IV contrast revealed normal right common femoral artery and vein with postsurgical changes and thickening of the skin and small air lucencies in the right groin. The patient was started on empiric treatment with IV vancomycin and piperacillin/tazobactam.
Due to initial worsening of erythema, piperacillin/tazobactam were stopped and ertapenem was initiated. Blood cultures sets and the culture of the surgical wound were positive for P multocida. Vancomycin was discontinued, and the patient rapidly improved. He was discharged on oral moxifloxacin for 2 weeks. After 10 months of follow-up, the patient was doing well and the surgical site wound had healed.
DISCUSSION
Pasteurella multocida is a small, Gram-negative, nonmotile, non–spore-forming coccobacillus with bipolar staining features.5 It often exists as a commensal in the upper respiratory tracts of domestic pet species, especially cats and dogs, and may cause hemorrhagic septicemia in cattle, fowl cholera in chickens, and atrophic rhinitis in pigs.6,7Pasteurella multocida infection in humans is often associated with an animal bite, scratch, or lick, but infection without epidemiologic evidence of animal contact may occur.8
The majority of animal bites involve dogs (85%-90%), followed by cats (5%-10%). Infectious complications occur in about 15% to 20% of dog-related bites and > 50% of cat-related bites. The sharp and long teeth of cats can easily penetrate human skin, create a deep puncture wound, and even inoculate the periosteal component of bones. Cat-related wounds more commonly progress to serious and deeper tissue infections, including osteomyelitis and meningitis.9 Human-to-human transmission is rare, but there are reported cases of respiratory transmission and maternal-to-fetal transmission.10,11
The most common presentation of P multocida infection in humans is soft-tissue infection, appearing as purulent wounds (48%), cellulitis (36%), or abscesses (16%).12 The infection is characterized by the development of soft-tissue inflammation at the site of contact, which may progress to diffuse, localized cellulitis. High leukocyte and neutrophil counts are typically observed.13 Complications of localized infection include rapidly progressive cellulitis, abscesses, tenosynovitis, osteomyelitis, and septic arthritis. The localized infection can also lead to septicemia, which carries a high mortality rate (31%).12,14
Pasteurella multocida septicemia commonly occurs in patients with an immune-compromised status, but septicemia in healthy individuals has also been reported.15,16 Apart from local skin and soft-tissue infections, P multocida can cause upper respiratory tract infections, lower respiratory tract infections leading to pneumonia, trachea-bronchitis, lung abscess, and empyema, usually in individuals with underlying pulmonary disease. Pasteurella multocida meningitis has been associated with cat licks and bites occurring on the face in both the young and the elderly.17-19
Gram stains of purulent material or other fluid specimens, including blood, sputum, and cerebrospinal fluid, may show small, Gram-negative, nonmotile, non–spore-forming pleomorphic coccobacilli. Wright, Giemsa, and Wayson stains enhance bipolar staining. The quickest and most accurate method for confirming an active P multocida infection is molecular detection using polymerase chain reaction.20 Evaluations of tenosynovitis, septic arthritis, osteomyelitis, and meningeal enhancement, when appropriate, should be done with CT scans or MRIs.
In < 10% of cases, localized infection by P multocida may lead to bacteremia. The most common predisposing factors associated with bacteremia identified in a review of cases over 20 years at an urban medical center included old age and chronic medical conditions.21 Chronic medical conditions involved most commonly were diabetes mellitus, hypertension, and congestive heart failure. Liver dysfunction has also been reported as a significant risk factor in cases of P multocida bacteremia. The most common antibiotics used to treat the patients with bacteremia were ampicillin/sulbactam, cephalosporins, and fluoroquinolones.
A brief review of the literature of 21 cases of bacteremia showed that the most common antibiotics used for treatment were penicillins (ampicillin, amoxicillin, and piperacillin) in 11 of 21 cases. After penicillin, ciprofloxacin was the most commonly used antibiotic to treat bacteremia secondary to P multocida. The review also identified chronic medical conditions, such as diabetes mellitus, hypertension, congestive heart failure, and chronic obstructive pulmonary disease, as the most common risk factors associated in these cases with bacteremia.
In 17 of 20 cases, patients reported being present in an environment with pets, mostly cats and dogs. Twelve out of 17 patients reported having contact with pet cats and dogs, mostly in the form of bites or pets licking their wounds, and 3 of these were postoperative patients with external wounds.22-24
This patient reported that after discharge from the hospital following surgery for his spreading melanoma, domestic cats at his home repeatedly licked the postoperative wound. This almost certainly was the source of the infection and bacteremia in this patient. These findings stress the importance of educating patients about proper postoperative wound care and precautions needed if there is potential exposure to domestic animals, such as cats and dogs.
CONCLUSIONS
Pasteurella multocida is an unusual cause of postoperative wound infection. The most common method of acquiring a P multocida infection is through contact with pet animals, mostly cats and dogs. Infection can occur not only with animal bites and scratches, but also with licking of open wounds. The rate of infections can be decreased significantly by educating patients about the mode of transmission of infection, its complications, and safety measures needed if they have pets at home.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The most common microbes causing postoperative wound infection are Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, Staphylococcus epidermidis, and Enterococcus faecalis.1 Pasteurella multocida (P multocida) is an uncommon organism causing surgical-site infections.2 This article reports a case of a patient who developed a postoperative wound infection due to P multocida complicated by a bloodstream infection.
CASE REPORT
A 54-year-old man presented with pain and discharge surrounding his recent surgical site and a 1-day history of fever and chills. Four weeks prior to the presentation, he underwent nodal dissection and reconstructive surgery with a muscle flap on his right leg for a superficial spreading melanoma. The patient noticed wound dehiscence the previous 2 to 3 days and a white-yellowish discharge from the wound.
Six years previously, the patient was diagnosed with a superficial spreading melanoma on his right thigh. At that time, he underwent wide excision for the localized disease. The patient was doing well until 3 months prior to the admission when he noticed a nodule in his right groin area, which had enlarged to a lump. Fine needle aspiration of the lump and immunohistochemistry showed the presence of malignant cells, positive for S100 and MART-1.These markers are useful for a diagnosis of metastatic melanoma.3,4
A positron emission tomography (PET) scan revealed localized disease with increased uptake only in the groin region. Superficial nodal dissection and sartorius muscle flap placement were performed, and the patient was discharged to his home with drains in place.
Two weeks after his node dissection, the patient was seen in the surgery clinic, and his drains were removed. Three days after his clinic visit, he noticed erythema around the suture line and discharge from the wound, followed by increasing pain, high fever, and chills. The patient reported no history of nausea, vomiting, diarrhea, painful urination, cough, shortness of breath, chest pain, or abdominal pain. His medical history was also significant for hypertension and multiple lipomas on his back and extremities, which were removed surgically 15 years previously. He had been a chronic smoker and occasionally used alcohol but did not use illicit drugs. The patient was unmarried and lived alone with his domestic cats.
The patient was febrile on admission (38.9°C); heart rate 110 bpm. His blood pressure and respiratory rate were normal. An examination of the right groin revealed an incision mark of about 20 cm in length from his right anterior superior iliac spine travelling inferomedially into his groin with breakdown at the infero-medial aspect, extending one-half to one-third the wound distance. The wound had clean borders with minimal amount of purulent drainage. Induration was noted, extending down the thigh to above the knee level. Sutures remained in place along the superior aspect of the incision site. No other abnormalities were found.
Laboratory studies revealed leucocytosis (white blood cell count, 12,200/mm3). Blood glucose, blood urea nitrogen, serum creatinine, and electrolytes were within normal range. Computerized tomography (CT) scans of the pelvis and thighs with IV contrast revealed normal right common femoral artery and vein with postsurgical changes and thickening of the skin and small air lucencies in the right groin. The patient was started on empiric treatment with IV vancomycin and piperacillin/tazobactam.
Due to initial worsening of erythema, piperacillin/tazobactam were stopped and ertapenem was initiated. Blood cultures sets and the culture of the surgical wound were positive for P multocida. Vancomycin was discontinued, and the patient rapidly improved. He was discharged on oral moxifloxacin for 2 weeks. After 10 months of follow-up, the patient was doing well and the surgical site wound had healed.
DISCUSSION
Pasteurella multocida is a small, Gram-negative, nonmotile, non–spore-forming coccobacillus with bipolar staining features.5 It often exists as a commensal in the upper respiratory tracts of domestic pet species, especially cats and dogs, and may cause hemorrhagic septicemia in cattle, fowl cholera in chickens, and atrophic rhinitis in pigs.6,7Pasteurella multocida infection in humans is often associated with an animal bite, scratch, or lick, but infection without epidemiologic evidence of animal contact may occur.8
The majority of animal bites involve dogs (85%-90%), followed by cats (5%-10%). Infectious complications occur in about 15% to 20% of dog-related bites and > 50% of cat-related bites. The sharp and long teeth of cats can easily penetrate human skin, create a deep puncture wound, and even inoculate the periosteal component of bones. Cat-related wounds more commonly progress to serious and deeper tissue infections, including osteomyelitis and meningitis.9 Human-to-human transmission is rare, but there are reported cases of respiratory transmission and maternal-to-fetal transmission.10,11
The most common presentation of P multocida infection in humans is soft-tissue infection, appearing as purulent wounds (48%), cellulitis (36%), or abscesses (16%).12 The infection is characterized by the development of soft-tissue inflammation at the site of contact, which may progress to diffuse, localized cellulitis. High leukocyte and neutrophil counts are typically observed.13 Complications of localized infection include rapidly progressive cellulitis, abscesses, tenosynovitis, osteomyelitis, and septic arthritis. The localized infection can also lead to septicemia, which carries a high mortality rate (31%).12,14
Pasteurella multocida septicemia commonly occurs in patients with an immune-compromised status, but septicemia in healthy individuals has also been reported.15,16 Apart from local skin and soft-tissue infections, P multocida can cause upper respiratory tract infections, lower respiratory tract infections leading to pneumonia, trachea-bronchitis, lung abscess, and empyema, usually in individuals with underlying pulmonary disease. Pasteurella multocida meningitis has been associated with cat licks and bites occurring on the face in both the young and the elderly.17-19
Gram stains of purulent material or other fluid specimens, including blood, sputum, and cerebrospinal fluid, may show small, Gram-negative, nonmotile, non–spore-forming pleomorphic coccobacilli. Wright, Giemsa, and Wayson stains enhance bipolar staining. The quickest and most accurate method for confirming an active P multocida infection is molecular detection using polymerase chain reaction.20 Evaluations of tenosynovitis, septic arthritis, osteomyelitis, and meningeal enhancement, when appropriate, should be done with CT scans or MRIs.
In < 10% of cases, localized infection by P multocida may lead to bacteremia. The most common predisposing factors associated with bacteremia identified in a review of cases over 20 years at an urban medical center included old age and chronic medical conditions.21 Chronic medical conditions involved most commonly were diabetes mellitus, hypertension, and congestive heart failure. Liver dysfunction has also been reported as a significant risk factor in cases of P multocida bacteremia. The most common antibiotics used to treat the patients with bacteremia were ampicillin/sulbactam, cephalosporins, and fluoroquinolones.
A brief review of the literature of 21 cases of bacteremia showed that the most common antibiotics used for treatment were penicillins (ampicillin, amoxicillin, and piperacillin) in 11 of 21 cases. After penicillin, ciprofloxacin was the most commonly used antibiotic to treat bacteremia secondary to P multocida. The review also identified chronic medical conditions, such as diabetes mellitus, hypertension, congestive heart failure, and chronic obstructive pulmonary disease, as the most common risk factors associated in these cases with bacteremia.
In 17 of 20 cases, patients reported being present in an environment with pets, mostly cats and dogs. Twelve out of 17 patients reported having contact with pet cats and dogs, mostly in the form of bites or pets licking their wounds, and 3 of these were postoperative patients with external wounds.22-24
This patient reported that after discharge from the hospital following surgery for his spreading melanoma, domestic cats at his home repeatedly licked the postoperative wound. This almost certainly was the source of the infection and bacteremia in this patient. These findings stress the importance of educating patients about proper postoperative wound care and precautions needed if there is potential exposure to domestic animals, such as cats and dogs.
CONCLUSIONS
Pasteurella multocida is an unusual cause of postoperative wound infection. The most common method of acquiring a P multocida infection is through contact with pet animals, mostly cats and dogs. Infection can occur not only with animal bites and scratches, but also with licking of open wounds. The rate of infections can be decreased significantly by educating patients about the mode of transmission of infection, its complications, and safety measures needed if they have pets at home.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Giacometti A, Cirioni O, Schimizzi AM, et al. Epidemiology and microbiology of surgical wound infection. J Clin Microbiol. 2000;38(2):918-919.
2. Cook PP. Persistent postoperative wound infection with Pasteurella multocida: Case report and literature review. Infection. 1995;23(4):252.
3. Hodi FS. Well-defined melanoma antigens as progression markers for melanoma: Insights into differential expression and host response based on stage. Clin Cancer Res. 2006;12(3, pt 1):673-678.
4. Zubovits J, Buzney E, Yu L, Duncan LM. HMB-45, S-100, NK1/C3, and MART-1 in metastatic melanoma. Hum Pathol. 2004;35(2):217-223.
5. Zurlo JJ. Pasteurella species. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2005:2687-2691.
6. Waghorn DJ, Robson M. Occupational risk of Pasteurella multocida septicaemia and premature labor in a pregnant vet. BJOG. 2003;110(8):780-781.
7. Francis DP, Holmes MA, Brandon G. Pasteurella multocida infections after domestic animal bites and scratches. JAMA. 1975;233(1):42-45.
8. Cordoba A, Bueno I, Monterrubio J, Corcho G. Surgical wound infection due to Pasteurella multocida [article in Spanish]. Enferm Infecc Microbiol Clin. 2002;20(10):536-537.
9. Kopita JM, Handshoe D, Kussin PS, Kelemen M. Cat germs! Pleuropulmonary pasteurella infection in an old man. N C Med J. 1993;54(7):308-311.
10. Hubert WT, Rosen MN. Pasteurella multocida infections. II. Pasteurella multocida infection in man unrelated to animal bite. Am J Pub Health Nations Health. 1970;60(6):1109-1117.
11. Escande F, Borde M, Pateyron F. Infection maternelle et néonatale à Pasteurella multocida. Arch Pediatr. 1997;4(11):1116-1118.
12. Luchansky M, Bergman M, Djaldetti R, Salman H. Cat bite in an old patient: Is it a simple injury? Eur J Emerg Med. 2003;10(2):130-132.
13. Ryan KJ, Ray CG, eds. Sherris Medical Microbiology. 4th ed. New York, NY: McGraw Hill; 2000.
14. Weber DJ, Wolfson JS, Swartz MN, Hooper DC. Pasteurella multocida infections. Report of 34 cases and review of the literature. Medicine (Baltimore). 1984;63(3):133-154.
15. Kimura R, Hayashi Y, Takeuchi T, Shimizu M, et al. Pasteurella multocida septicemia caused by close contact with a domestic cat: Case report and literature review. J Infect Chemother. 2004;10(4):250-252.
16. Albert TJ, Stevens DL. The first case of Pasteurella canis bacteremia: A cirrhotic patient with an open leg wound. Infection. 2010;38(6):483-485.
17. Lion C, Lozniewski A, Rosner V, Weber M. Lung abscess due to beta-lactamase-producing Pasteurella multocida. Clin Infect Dis. 1999;29(5):1345-1346.
18. Fernández-Esparrach G, Mascaró J, Rota R, Valerio L. Septicemia, peritonitis, and empyema due to Pasteurella multocida in a cirrhotic patient. Clin Infect Dis. 1994;18(3):486.
19. Wade T, Booy R, Teare EL, Kroll S. Pasteurella multocida meningitis in infancy—(a lick may be as bad as a bite). Eur J Pediatr. 1999;158(11):875-878.
20. Miflin JK, Balckall PJ. Development of a 23S rRNA-based PCR assay for the identification of Pasteurella multocida. Lett Appl Microbiol. 2001;33(3):216-221.
21. Ebright J, Frey AB, Fairfax MR. Pasteurella multocida infections and bacteremia: A twenty-year experience at an urban medical center. Infect Dis Clin Pract. 2009;17(2):102-104.
22. Baillot R, Voisine P, Côté LM, Longtin Y. Deep sternal wound infection due to Pasteurella multocida: The first case report and review of literature. Infection. 2011;39(6):575-578.
23. Baskar B, Desai SP, Parsons MA. Postoperative endophthalmitis due to Pasteurella multocida. Br J Ophthalmol. 1997;81(2):172-173.
24. Chun ML, Buekers TE, Sood AK, Sorosky JI. Postoperative wound infection with Pasteurella multocida from a pet cat. Am J Obstet Gynecol. 2003;188(4):1115-1116.
1. Giacometti A, Cirioni O, Schimizzi AM, et al. Epidemiology and microbiology of surgical wound infection. J Clin Microbiol. 2000;38(2):918-919.
2. Cook PP. Persistent postoperative wound infection with Pasteurella multocida: Case report and literature review. Infection. 1995;23(4):252.
3. Hodi FS. Well-defined melanoma antigens as progression markers for melanoma: Insights into differential expression and host response based on stage. Clin Cancer Res. 2006;12(3, pt 1):673-678.
4. Zubovits J, Buzney E, Yu L, Duncan LM. HMB-45, S-100, NK1/C3, and MART-1 in metastatic melanoma. Hum Pathol. 2004;35(2):217-223.
5. Zurlo JJ. Pasteurella species. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2005:2687-2691.
6. Waghorn DJ, Robson M. Occupational risk of Pasteurella multocida septicaemia and premature labor in a pregnant vet. BJOG. 2003;110(8):780-781.
7. Francis DP, Holmes MA, Brandon G. Pasteurella multocida infections after domestic animal bites and scratches. JAMA. 1975;233(1):42-45.
8. Cordoba A, Bueno I, Monterrubio J, Corcho G. Surgical wound infection due to Pasteurella multocida [article in Spanish]. Enferm Infecc Microbiol Clin. 2002;20(10):536-537.
9. Kopita JM, Handshoe D, Kussin PS, Kelemen M. Cat germs! Pleuropulmonary pasteurella infection in an old man. N C Med J. 1993;54(7):308-311.
10. Hubert WT, Rosen MN. Pasteurella multocida infections. II. Pasteurella multocida infection in man unrelated to animal bite. Am J Pub Health Nations Health. 1970;60(6):1109-1117.
11. Escande F, Borde M, Pateyron F. Infection maternelle et néonatale à Pasteurella multocida. Arch Pediatr. 1997;4(11):1116-1118.
12. Luchansky M, Bergman M, Djaldetti R, Salman H. Cat bite in an old patient: Is it a simple injury? Eur J Emerg Med. 2003;10(2):130-132.
13. Ryan KJ, Ray CG, eds. Sherris Medical Microbiology. 4th ed. New York, NY: McGraw Hill; 2000.
14. Weber DJ, Wolfson JS, Swartz MN, Hooper DC. Pasteurella multocida infections. Report of 34 cases and review of the literature. Medicine (Baltimore). 1984;63(3):133-154.
15. Kimura R, Hayashi Y, Takeuchi T, Shimizu M, et al. Pasteurella multocida septicemia caused by close contact with a domestic cat: Case report and literature review. J Infect Chemother. 2004;10(4):250-252.
16. Albert TJ, Stevens DL. The first case of Pasteurella canis bacteremia: A cirrhotic patient with an open leg wound. Infection. 2010;38(6):483-485.
17. Lion C, Lozniewski A, Rosner V, Weber M. Lung abscess due to beta-lactamase-producing Pasteurella multocida. Clin Infect Dis. 1999;29(5):1345-1346.
18. Fernández-Esparrach G, Mascaró J, Rota R, Valerio L. Septicemia, peritonitis, and empyema due to Pasteurella multocida in a cirrhotic patient. Clin Infect Dis. 1994;18(3):486.
19. Wade T, Booy R, Teare EL, Kroll S. Pasteurella multocida meningitis in infancy—(a lick may be as bad as a bite). Eur J Pediatr. 1999;158(11):875-878.
20. Miflin JK, Balckall PJ. Development of a 23S rRNA-based PCR assay for the identification of Pasteurella multocida. Lett Appl Microbiol. 2001;33(3):216-221.
21. Ebright J, Frey AB, Fairfax MR. Pasteurella multocida infections and bacteremia: A twenty-year experience at an urban medical center. Infect Dis Clin Pract. 2009;17(2):102-104.
22. Baillot R, Voisine P, Côté LM, Longtin Y. Deep sternal wound infection due to Pasteurella multocida: The first case report and review of literature. Infection. 2011;39(6):575-578.
23. Baskar B, Desai SP, Parsons MA. Postoperative endophthalmitis due to Pasteurella multocida. Br J Ophthalmol. 1997;81(2):172-173.
24. Chun ML, Buekers TE, Sood AK, Sorosky JI. Postoperative wound infection with Pasteurella multocida from a pet cat. Am J Obstet Gynecol. 2003;188(4):1115-1116.
Recurrent Multidrug Resistant Urinary Tract Infections in Geriatric Patients
Urinary tract infections (UTIs) account for 8.3 million doctor visits, 1 million emergency department (ED) visits, and 100,000 hospitalizations annually, with an estimated cost of $1 billion annually in the U.S.1 Urnary tract infections are the most common bacterial infections found in nursing home residents, accounting for 50% of reported infections in Norwegian nursing homes, 30% to 50% in U.S. nursing homes, and 25% of all infections in the noninstitutionalized elderly in the U.S.2-4 In the geriatric population, UTIs are often found incidentally at the time of hospitalization for other admitting diagnoses, such as mentation changes or falls.5 Asymptomatic pyuria was found in 14.8% of community residents aged ≥ 80 years.6 Woodford and colleague found that 37% of geriatric patients admitted through an ED diagnosed with UTIs had no dysuria or urinary frequency.7
The incidence of UTIs is higher in the elderly due to genitourinary abnormalities, urolithiasis, dehydration, and diabetes, among other causes. These are considered complicated UTIs, defined as those in the presence of factors that predispose to persistent or relapsing infection, such as foreign bodies (calculi, indwelling catheters), obstruction, renal failure, and urinary retention.8
In elderly men, prostate enlargement causes bladder outlet obstruction predisposing them to urinary stasis and UTIs.2 Urinary tract infections are prone to recur when urinary tract abnormalities persist or treatment ineffectively eradicates resistant bacteria. Urinary tract infections are considered recurrent when ≥ 3 occur within 1 year or ≥ 2 occur in a 6-month period. The anticipated recurrence rate of complicated UTIs at 4 to 6 weeks following completion of therapy is 40% to 60%.4
Current practice standards recommend not treating asymptomatic UTIs to avoid contributing to bacterial antibiotic resistance.9 The frequent use of antibiotics, such as quinolones, which are increasingly inactive against these organisms, contributes to the overgrowth of bacteria in the gastrointestinal tract and their appearance in the genitourinary tract.10,11
As UTI-causing bacteria become more resistant to available antibiotics, the need to explore new strategies for managing UTIs is clear.12 The spread of extended spectrum beta-lactamase (ESBL), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (VRE), among other emerging bacterial resistance factors, present increasing treatment cost and poor patient outcomes. This challenge is occurring at a time when the discovery and development of new anti-infective agents is slowing down.13
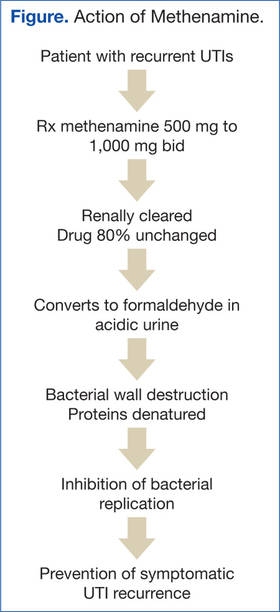
The European Commission Scientific Committee on Health and Environmental Risk reported that in patients receiving up to 4,000 mg/d methenamine for preventive long-term treatment of UTIs, no adverse effects (AEs) were noted (Figure).17
Complicated UTIs in the elderly are difficult to treat due to bacterial resistance. The off-label use of methenamine hippurate for treatment/prophylaxis of MDR-recurrent UTIs is a compelling option, explored further in the following case studies. Four case studies using methenamine for treatment and prevention of recurrent MDR UTIs in geriatric patients are presented.
Treating UTI Patients
Case Study 1
A man aged > 89 years, symptomatic with nocturia due to benign prostatic hypertrophy (BPH) with bladder outlet obstruction had 8 symptomatic UTIs over 15 months. His urine culture tested positive for MDR Providencia stuartia (resistant to ampicillin, chephazolin, gentamycin, tigecycline, tobramycin and sulfamethizole) and Staphylococcus haemolyticus (resistant to ciprofloxacin, levofloxacin, and nitrofurantoin). Postvoid residual urine was identified as the cause for his recurrent UTIs. Self-catheterization was recommended, but the patient declined. Due to his advanced age and preference, surgical intervention was not pursued. His renal function was within normal limits.
Treatment with methenamine hippurate 500 mg bid with 1,000 mg ascorbic acid to acidify the urine was initiated. This reduced dose of 500 mg bid (rather than 1,000 mg bid) was prescribed due to his advanced age and a choice to “err on the side of caution.” Two months later, urinalysis was negative for leukocyte esterase and nitrates, and the growth culture tested negative. Three- and 6-month urinalyses also showed no growth. The patient’s renal function remained stable. He experienced no AEs from the methenamine.
Due to his urinary retention, formaldehyde was able to collect in his bladder for longer than 2 hours, achieving bactericidal levels and effectively preventing recurrence of MDR UTIs.
Case Study 2
A man aged > 89 years with BPH and urinary incontinence managed with an external urinary device worn continuously had a history of 4 UTIs within a 6-month period. His renal function was normal with a creatinine clearance of 37 mg/dL. He was diagnosed with a symptomatic UTI culturing > 100,000 CFU Proteus mirabilis (resistant to ciprofloxacin, nitrofurantoin, and septra).
Due to resistance of the organism to available oral antibiotics, the patient’s desire to avoid hospitalization, and his caregiver’s inability to learn to administer IV antibiotics in the home, methenamine hippurate 500 mg bid was initiated. Within 21 days, the patient’s urinalysis was negative, indicating no bacterial growth. He was treated for 4 months with no recurrence of a UTI. No symptomatic UTIs recurred during the ongoing methenamine treatment.
Case Study 3
A man aged > 89 years with end-stage renal disease and a history of bladder cancer declined dialysis, indicating that his goals for care were palliative. He was followed at home by a hospice team. He had 3 recurrent symptomatic MRSA UTIs in a 9-month period (resistant to ciprofloxacin, levofloxin, penicillin, and oxacillin). The antibiotics the bacteria was sensitive to, nitrofurantoin and septra, could not be given because his creatinine clearance was merely 8 mg/dL. He was prescribed 500 mg methenamine with 1,000 mg ascorbic acid bid. Within 4 weeks, his urinalysis had changed from > 100,000 CFU to > 50,000 CFU (< 100,000 CFU). One month later with the only treatment the methenamine and ascorbic acid, there was no bacterial growth in the patient’s urine culture. He had no recurrence of a symptomatic UTI while receiving methenamine.
Case Study 4
An 89-year-old man with BPH and recurrent MRSA UTIs had 3 hospitalizations within 1 year. He had stage 3 chronic kidney disease with a creatinine clearance of 43 mg/dL. The patient had a symptomatic UTI > 100,000 CFU MRSA. He was treated with 500 mg methenamine and 1,000 mg ascorbic acid bid. Urinalysis results 2 months later revealed the bacterial count had dropped to the colonization range (< 50,000 CFU). His urinalysis was positive for leukocyte esterase with high white blood cell (WBC) counts, but it was negative for nitrites. He continued without recurrent UTIs while receiving the medication.
Discussion
Patients with similar profiles to those discussed in this report were treated with less dramatic results. Several remained free of symptomatic UTIs with urine cultures showing bacterial counts in the colonization range of < 50,000 CFU, as noted in case 4. Frequently, patients treated with methenamine have urinalyses with negative nitrites, positive leukocyte esterase, high WBCs, and few bacteria, but cultures show no growth. Some patients who did not reliably take medications as prescribed had recurrent symptomatic UTIs. Some had a subsequent UTI culturing a different organism or a change in the sensitivity profile of the same organism. This phenomenon suggests that formaldehyde disrupts the manufacture and transmission of the proteins and enzymes responsible for bacterial resistance factors.
Freeman and colleagues conducted a prospective study of 249 men with bacteruria followed for up to 10 years.18 Continuous therapy with methenamine delayed recurrence of bacteruria. Nilsson found that recurrent UTIs were reduced by 25% with long-term treatment (> 3 months) with methenamine.19
Bacteria do not develop resistance to methenamine.20 Reports of AEs are low, and drug interactions are limited to sulfamethizole, which can cause crystallization in the urine. Daily dosing used in studies ranged from 1 g to 4 g daily.21 Nilsson conducted research over 16 months with geriatric patients and found no changes in renal function or crystallization in urine.19
Severe hepatic impairment is also a contraindication, as methenamine can be hydrolyzed to ammonia. Studies have shown a reduced effectiveness with lower urinary tract abnormalities, although those studies administered the medication for short periods of time.21 Because the action of the medication relies on ≥ 2 hours of exposure to urine in the bladder, patients with indwelling catheters or patients who urinate frequently experience little benefit.22 Ideal candidates for methenamine are those with urinary retention and recurrent UTIs.
Although the use of methenamine has increased in Norway and Sweden by 24% since 2000, the use of methenamine in the U.S. remains low, perhaps because of conflicting reports in the literature regarding effectiveness and use with limited populations (ie, noncatheterized patients, those able to retain urine for ≥ 2 hours, and a creatinine clearance > 50 mg/dL).3
Some health care providers use methenamine for UTI prophylaxis, but this practice is less common in the U.S. than it is in Scandinavian countries.3 However, no published studies have explored the action of methenamine on MRSA, ESBL, and VRE bacteria or on the enzymes and proteins that enable and transmit bacterial resistance factors.
Elderly patients with complicated recurrent UTIs due to resistant bacteria are often left with no oral antibiotic options. Costs escalate rapidly when IV antibiotics are given. Administration generally requires hospitalization with close monitoring of renal function and drug levels and the placement of a PICC or midline IV access. If there is no caregiver, then hospitalization followed by an admission to a skilled nursing facility is required.
Lee and colleagues concluded that there is a need for further studies to explore long-duration therapy with methenamine.21 No studies have addressed its use in the geriatric population for long-term use of prevention of recurrent UTIs. No studies have been done on its use for primary treatment of MDR UTIs. The benefits of this drug with a low AE profile and low cost ($60/month for 1 g bid), which has been proven to reduce the incidence and/or delay recurrence of UTIs, is well worth further examination.
Conclusion
Multiple studies over 60 years have shown methenamine hippurate to be a well-tolerated and safe medication. Little data are available about the use of this medication in the elderly in the U.S., despite its wide use in Scandinavian countries. Use of methenamine for MDR UTIs in the geriatric population has been shown to be safe and effective, as presented in these case studies. Substantial cost savings were realized with the use of methenamine in these geriatric patients by reducing hospitalizations and complications due to recurrent MDR UTIs. The use of methenamine for treating MDR UTIs and the prevention of recurrent UTIs in the geriatric population warrants further clinical use and research.
The very interesting changes noted in sensitivity of the same bacteria in subsequent UTIs in patients treated with methenamine raises questions about the action of formaldehyde in the bladder on bacterial resistance factors. Given the worldwide increase in bacterial resistance to currently available antibiotics, this is a most compelling action that demands further study.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med. 2002;113(suppl 1A):5S-13S.
2. Kamel HK. Managing urinary tract infections: Guide for nursing home practitioners. Ann of Long Term Care. 2005;13(9):21-28.
3. Blix HS, Røed J, Sti MO. Large variation in antibacterial use among Norwegian nursing homes. Scand J Infect Dis. 2007;39(6-7):536-541.
4. Nicolle LE. Asymptomatic bacteruria in diabetic women. Diabetes Care. 2000;23(6):722-723.
5. Rhoads J, Clayman A, Nelson S. The relationship of urinary tract infections and falls in a nursing home. Director. 2007;15(1):22-26.
6. Rodhe N, Mølstad S, Englund L, Svärdsudd K. Asymptomatic bacteriuria in a population of elderly residents living in a community setting: Prevalence, characteristics and associated factors. Fam Pract. 2006;23(3):303-307.
7. Woodford HJ, George J. Diagnosis and management of urinary tract infection in hospitalized older people. J Am Geriatr Soc. 2009;57(1):107-114.
8. Levison ME, Kaye D. Treatment of complicated urinary tract infections with an emphasis on drug-resistant gram-negative uropathogens. Curr Infect Dis Rep. 2013;15(2):109-115.
9. Miller LG, Tang AW. Treatment of uncomplicated urinary tract infections in an era of increasing antimicrobial resistance. Mayo Clin Proc. 2004;79(8):1048-1053.
10. Nicoletti J, Kuster SP, Sulser T, et al. Risk factors for urinary tract infections due to ciprofloxacin-resistant Escherichia coli in a tertiary care urology department in Switzerland. Swiss Med Wkly. 2010;140:w13059.
11. Nicolle LE. Urinary tract infection in geriatric and institutionalized patients. Curr Opin Urol. 2002;12(1):51-55.
12. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660.
13. Spellberg B, Guidos R, Gilbert D, et al; Infectious Diseases Society of America. The epidemic of antibiotic-resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(2):155-164.
14. Dagley S, Dawes EA, Morrison GA. Inhibition of growth of Aerobacter aerogenes: The mode of action of phenols, alcohols, acetone, and ethyl acetate.
J Bacteriol. 1950;60(4):369-379.
15. Neely WB. Action of formaldehyde on microorganisms I. Correlation of activity with formaldehyde metabolism. J Bacteriol. 1963;85(5):1028-1031.
16. Musher DM, Griffith DP. Generation of formaldehyde from methenamine: Effect of pH and concentration, and antibacterial effect. Antimicrob Agents Chemother. 1974;6(6):708-711.
17. Scientific Committee on Health and Environmental Risks. Risk Assessment Report on Methenamine. Brussels, Belgium: European Commission; 2007. CAS 100-97-0.
18. Freeman RB, Smith WM, Richardson JA, et al. Long-term therapy for chronic bacteriuria in men. U.S. Public Health Service cooperative study. Ann Intern Med. 1975;83(2):133-147.
19. Nilsson S. Long-term treatment with methenamine hippurate in recurrent urinary tract infection. Acta Med Scand. 1975;198(1-2):81-85.
20. Drugs.com. Methenamine (systemic). http://www.drugs.com/mmx/methenamine-hippurate.html?printable=1. Updated March 28, 2000. Accessed June 17, 2014.
21. Lee BSB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;10:CD003265.
22. Lee BB, Haran MJ, Hunt LM, et al. Spinal-injured neuropathic bladder antisepsis (SINBA) trial. Spinal Cord. 2007;45(8):542-550.
Urinary tract infections (UTIs) account for 8.3 million doctor visits, 1 million emergency department (ED) visits, and 100,000 hospitalizations annually, with an estimated cost of $1 billion annually in the U.S.1 Urnary tract infections are the most common bacterial infections found in nursing home residents, accounting for 50% of reported infections in Norwegian nursing homes, 30% to 50% in U.S. nursing homes, and 25% of all infections in the noninstitutionalized elderly in the U.S.2-4 In the geriatric population, UTIs are often found incidentally at the time of hospitalization for other admitting diagnoses, such as mentation changes or falls.5 Asymptomatic pyuria was found in 14.8% of community residents aged ≥ 80 years.6 Woodford and colleague found that 37% of geriatric patients admitted through an ED diagnosed with UTIs had no dysuria or urinary frequency.7
The incidence of UTIs is higher in the elderly due to genitourinary abnormalities, urolithiasis, dehydration, and diabetes, among other causes. These are considered complicated UTIs, defined as those in the presence of factors that predispose to persistent or relapsing infection, such as foreign bodies (calculi, indwelling catheters), obstruction, renal failure, and urinary retention.8
In elderly men, prostate enlargement causes bladder outlet obstruction predisposing them to urinary stasis and UTIs.2 Urinary tract infections are prone to recur when urinary tract abnormalities persist or treatment ineffectively eradicates resistant bacteria. Urinary tract infections are considered recurrent when ≥ 3 occur within 1 year or ≥ 2 occur in a 6-month period. The anticipated recurrence rate of complicated UTIs at 4 to 6 weeks following completion of therapy is 40% to 60%.4
Current practice standards recommend not treating asymptomatic UTIs to avoid contributing to bacterial antibiotic resistance.9 The frequent use of antibiotics, such as quinolones, which are increasingly inactive against these organisms, contributes to the overgrowth of bacteria in the gastrointestinal tract and their appearance in the genitourinary tract.10,11
As UTI-causing bacteria become more resistant to available antibiotics, the need to explore new strategies for managing UTIs is clear.12 The spread of extended spectrum beta-lactamase (ESBL), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (VRE), among other emerging bacterial resistance factors, present increasing treatment cost and poor patient outcomes. This challenge is occurring at a time when the discovery and development of new anti-infective agents is slowing down.13
The European Commission Scientific Committee on Health and Environmental Risk reported that in patients receiving up to 4,000 mg/d methenamine for preventive long-term treatment of UTIs, no adverse effects (AEs) were noted (Figure).17
Complicated UTIs in the elderly are difficult to treat due to bacterial resistance. The off-label use of methenamine hippurate for treatment/prophylaxis of MDR-recurrent UTIs is a compelling option, explored further in the following case studies. Four case studies using methenamine for treatment and prevention of recurrent MDR UTIs in geriatric patients are presented.
Treating UTI Patients
Case Study 1
A man aged > 89 years, symptomatic with nocturia due to benign prostatic hypertrophy (BPH) with bladder outlet obstruction had 8 symptomatic UTIs over 15 months. His urine culture tested positive for MDR Providencia stuartia (resistant to ampicillin, chephazolin, gentamycin, tigecycline, tobramycin and sulfamethizole) and Staphylococcus haemolyticus (resistant to ciprofloxacin, levofloxacin, and nitrofurantoin). Postvoid residual urine was identified as the cause for his recurrent UTIs. Self-catheterization was recommended, but the patient declined. Due to his advanced age and preference, surgical intervention was not pursued. His renal function was within normal limits.
Treatment with methenamine hippurate 500 mg bid with 1,000 mg ascorbic acid to acidify the urine was initiated. This reduced dose of 500 mg bid (rather than 1,000 mg bid) was prescribed due to his advanced age and a choice to “err on the side of caution.” Two months later, urinalysis was negative for leukocyte esterase and nitrates, and the growth culture tested negative. Three- and 6-month urinalyses also showed no growth. The patient’s renal function remained stable. He experienced no AEs from the methenamine.
Due to his urinary retention, formaldehyde was able to collect in his bladder for longer than 2 hours, achieving bactericidal levels and effectively preventing recurrence of MDR UTIs.
Case Study 2
A man aged > 89 years with BPH and urinary incontinence managed with an external urinary device worn continuously had a history of 4 UTIs within a 6-month period. His renal function was normal with a creatinine clearance of 37 mg/dL. He was diagnosed with a symptomatic UTI culturing > 100,000 CFU Proteus mirabilis (resistant to ciprofloxacin, nitrofurantoin, and septra).
Due to resistance of the organism to available oral antibiotics, the patient’s desire to avoid hospitalization, and his caregiver’s inability to learn to administer IV antibiotics in the home, methenamine hippurate 500 mg bid was initiated. Within 21 days, the patient’s urinalysis was negative, indicating no bacterial growth. He was treated for 4 months with no recurrence of a UTI. No symptomatic UTIs recurred during the ongoing methenamine treatment.
Case Study 3
A man aged > 89 years with end-stage renal disease and a history of bladder cancer declined dialysis, indicating that his goals for care were palliative. He was followed at home by a hospice team. He had 3 recurrent symptomatic MRSA UTIs in a 9-month period (resistant to ciprofloxacin, levofloxin, penicillin, and oxacillin). The antibiotics the bacteria was sensitive to, nitrofurantoin and septra, could not be given because his creatinine clearance was merely 8 mg/dL. He was prescribed 500 mg methenamine with 1,000 mg ascorbic acid bid. Within 4 weeks, his urinalysis had changed from > 100,000 CFU to > 50,000 CFU (< 100,000 CFU). One month later with the only treatment the methenamine and ascorbic acid, there was no bacterial growth in the patient’s urine culture. He had no recurrence of a symptomatic UTI while receiving methenamine.
Case Study 4
An 89-year-old man with BPH and recurrent MRSA UTIs had 3 hospitalizations within 1 year. He had stage 3 chronic kidney disease with a creatinine clearance of 43 mg/dL. The patient had a symptomatic UTI > 100,000 CFU MRSA. He was treated with 500 mg methenamine and 1,000 mg ascorbic acid bid. Urinalysis results 2 months later revealed the bacterial count had dropped to the colonization range (< 50,000 CFU). His urinalysis was positive for leukocyte esterase with high white blood cell (WBC) counts, but it was negative for nitrites. He continued without recurrent UTIs while receiving the medication.
Discussion
Patients with similar profiles to those discussed in this report were treated with less dramatic results. Several remained free of symptomatic UTIs with urine cultures showing bacterial counts in the colonization range of < 50,000 CFU, as noted in case 4. Frequently, patients treated with methenamine have urinalyses with negative nitrites, positive leukocyte esterase, high WBCs, and few bacteria, but cultures show no growth. Some patients who did not reliably take medications as prescribed had recurrent symptomatic UTIs. Some had a subsequent UTI culturing a different organism or a change in the sensitivity profile of the same organism. This phenomenon suggests that formaldehyde disrupts the manufacture and transmission of the proteins and enzymes responsible for bacterial resistance factors.
Freeman and colleagues conducted a prospective study of 249 men with bacteruria followed for up to 10 years.18 Continuous therapy with methenamine delayed recurrence of bacteruria. Nilsson found that recurrent UTIs were reduced by 25% with long-term treatment (> 3 months) with methenamine.19
Bacteria do not develop resistance to methenamine.20 Reports of AEs are low, and drug interactions are limited to sulfamethizole, which can cause crystallization in the urine. Daily dosing used in studies ranged from 1 g to 4 g daily.21 Nilsson conducted research over 16 months with geriatric patients and found no changes in renal function or crystallization in urine.19
Severe hepatic impairment is also a contraindication, as methenamine can be hydrolyzed to ammonia. Studies have shown a reduced effectiveness with lower urinary tract abnormalities, although those studies administered the medication for short periods of time.21 Because the action of the medication relies on ≥ 2 hours of exposure to urine in the bladder, patients with indwelling catheters or patients who urinate frequently experience little benefit.22 Ideal candidates for methenamine are those with urinary retention and recurrent UTIs.
Although the use of methenamine has increased in Norway and Sweden by 24% since 2000, the use of methenamine in the U.S. remains low, perhaps because of conflicting reports in the literature regarding effectiveness and use with limited populations (ie, noncatheterized patients, those able to retain urine for ≥ 2 hours, and a creatinine clearance > 50 mg/dL).3
Some health care providers use methenamine for UTI prophylaxis, but this practice is less common in the U.S. than it is in Scandinavian countries.3 However, no published studies have explored the action of methenamine on MRSA, ESBL, and VRE bacteria or on the enzymes and proteins that enable and transmit bacterial resistance factors.
Elderly patients with complicated recurrent UTIs due to resistant bacteria are often left with no oral antibiotic options. Costs escalate rapidly when IV antibiotics are given. Administration generally requires hospitalization with close monitoring of renal function and drug levels and the placement of a PICC or midline IV access. If there is no caregiver, then hospitalization followed by an admission to a skilled nursing facility is required.
Lee and colleagues concluded that there is a need for further studies to explore long-duration therapy with methenamine.21 No studies have addressed its use in the geriatric population for long-term use of prevention of recurrent UTIs. No studies have been done on its use for primary treatment of MDR UTIs. The benefits of this drug with a low AE profile and low cost ($60/month for 1 g bid), which has been proven to reduce the incidence and/or delay recurrence of UTIs, is well worth further examination.
Conclusion
Multiple studies over 60 years have shown methenamine hippurate to be a well-tolerated and safe medication. Little data are available about the use of this medication in the elderly in the U.S., despite its wide use in Scandinavian countries. Use of methenamine for MDR UTIs in the geriatric population has been shown to be safe and effective, as presented in these case studies. Substantial cost savings were realized with the use of methenamine in these geriatric patients by reducing hospitalizations and complications due to recurrent MDR UTIs. The use of methenamine for treating MDR UTIs and the prevention of recurrent UTIs in the geriatric population warrants further clinical use and research.
The very interesting changes noted in sensitivity of the same bacteria in subsequent UTIs in patients treated with methenamine raises questions about the action of formaldehyde in the bladder on bacterial resistance factors. Given the worldwide increase in bacterial resistance to currently available antibiotics, this is a most compelling action that demands further study.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Urinary tract infections (UTIs) account for 8.3 million doctor visits, 1 million emergency department (ED) visits, and 100,000 hospitalizations annually, with an estimated cost of $1 billion annually in the U.S.1 Urnary tract infections are the most common bacterial infections found in nursing home residents, accounting for 50% of reported infections in Norwegian nursing homes, 30% to 50% in U.S. nursing homes, and 25% of all infections in the noninstitutionalized elderly in the U.S.2-4 In the geriatric population, UTIs are often found incidentally at the time of hospitalization for other admitting diagnoses, such as mentation changes or falls.5 Asymptomatic pyuria was found in 14.8% of community residents aged ≥ 80 years.6 Woodford and colleague found that 37% of geriatric patients admitted through an ED diagnosed with UTIs had no dysuria or urinary frequency.7
The incidence of UTIs is higher in the elderly due to genitourinary abnormalities, urolithiasis, dehydration, and diabetes, among other causes. These are considered complicated UTIs, defined as those in the presence of factors that predispose to persistent or relapsing infection, such as foreign bodies (calculi, indwelling catheters), obstruction, renal failure, and urinary retention.8
In elderly men, prostate enlargement causes bladder outlet obstruction predisposing them to urinary stasis and UTIs.2 Urinary tract infections are prone to recur when urinary tract abnormalities persist or treatment ineffectively eradicates resistant bacteria. Urinary tract infections are considered recurrent when ≥ 3 occur within 1 year or ≥ 2 occur in a 6-month period. The anticipated recurrence rate of complicated UTIs at 4 to 6 weeks following completion of therapy is 40% to 60%.4
Current practice standards recommend not treating asymptomatic UTIs to avoid contributing to bacterial antibiotic resistance.9 The frequent use of antibiotics, such as quinolones, which are increasingly inactive against these organisms, contributes to the overgrowth of bacteria in the gastrointestinal tract and their appearance in the genitourinary tract.10,11
As UTI-causing bacteria become more resistant to available antibiotics, the need to explore new strategies for managing UTIs is clear.12 The spread of extended spectrum beta-lactamase (ESBL), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (VRE), among other emerging bacterial resistance factors, present increasing treatment cost and poor patient outcomes. This challenge is occurring at a time when the discovery and development of new anti-infective agents is slowing down.13
The European Commission Scientific Committee on Health and Environmental Risk reported that in patients receiving up to 4,000 mg/d methenamine for preventive long-term treatment of UTIs, no adverse effects (AEs) were noted (Figure).17
Complicated UTIs in the elderly are difficult to treat due to bacterial resistance. The off-label use of methenamine hippurate for treatment/prophylaxis of MDR-recurrent UTIs is a compelling option, explored further in the following case studies. Four case studies using methenamine for treatment and prevention of recurrent MDR UTIs in geriatric patients are presented.
Treating UTI Patients
Case Study 1
A man aged > 89 years, symptomatic with nocturia due to benign prostatic hypertrophy (BPH) with bladder outlet obstruction had 8 symptomatic UTIs over 15 months. His urine culture tested positive for MDR Providencia stuartia (resistant to ampicillin, chephazolin, gentamycin, tigecycline, tobramycin and sulfamethizole) and Staphylococcus haemolyticus (resistant to ciprofloxacin, levofloxacin, and nitrofurantoin). Postvoid residual urine was identified as the cause for his recurrent UTIs. Self-catheterization was recommended, but the patient declined. Due to his advanced age and preference, surgical intervention was not pursued. His renal function was within normal limits.
Treatment with methenamine hippurate 500 mg bid with 1,000 mg ascorbic acid to acidify the urine was initiated. This reduced dose of 500 mg bid (rather than 1,000 mg bid) was prescribed due to his advanced age and a choice to “err on the side of caution.” Two months later, urinalysis was negative for leukocyte esterase and nitrates, and the growth culture tested negative. Three- and 6-month urinalyses also showed no growth. The patient’s renal function remained stable. He experienced no AEs from the methenamine.
Due to his urinary retention, formaldehyde was able to collect in his bladder for longer than 2 hours, achieving bactericidal levels and effectively preventing recurrence of MDR UTIs.
Case Study 2
A man aged > 89 years with BPH and urinary incontinence managed with an external urinary device worn continuously had a history of 4 UTIs within a 6-month period. His renal function was normal with a creatinine clearance of 37 mg/dL. He was diagnosed with a symptomatic UTI culturing > 100,000 CFU Proteus mirabilis (resistant to ciprofloxacin, nitrofurantoin, and septra).
Due to resistance of the organism to available oral antibiotics, the patient’s desire to avoid hospitalization, and his caregiver’s inability to learn to administer IV antibiotics in the home, methenamine hippurate 500 mg bid was initiated. Within 21 days, the patient’s urinalysis was negative, indicating no bacterial growth. He was treated for 4 months with no recurrence of a UTI. No symptomatic UTIs recurred during the ongoing methenamine treatment.
Case Study 3
A man aged > 89 years with end-stage renal disease and a history of bladder cancer declined dialysis, indicating that his goals for care were palliative. He was followed at home by a hospice team. He had 3 recurrent symptomatic MRSA UTIs in a 9-month period (resistant to ciprofloxacin, levofloxin, penicillin, and oxacillin). The antibiotics the bacteria was sensitive to, nitrofurantoin and septra, could not be given because his creatinine clearance was merely 8 mg/dL. He was prescribed 500 mg methenamine with 1,000 mg ascorbic acid bid. Within 4 weeks, his urinalysis had changed from > 100,000 CFU to > 50,000 CFU (< 100,000 CFU). One month later with the only treatment the methenamine and ascorbic acid, there was no bacterial growth in the patient’s urine culture. He had no recurrence of a symptomatic UTI while receiving methenamine.
Case Study 4
An 89-year-old man with BPH and recurrent MRSA UTIs had 3 hospitalizations within 1 year. He had stage 3 chronic kidney disease with a creatinine clearance of 43 mg/dL. The patient had a symptomatic UTI > 100,000 CFU MRSA. He was treated with 500 mg methenamine and 1,000 mg ascorbic acid bid. Urinalysis results 2 months later revealed the bacterial count had dropped to the colonization range (< 50,000 CFU). His urinalysis was positive for leukocyte esterase with high white blood cell (WBC) counts, but it was negative for nitrites. He continued without recurrent UTIs while receiving the medication.
Discussion
Patients with similar profiles to those discussed in this report were treated with less dramatic results. Several remained free of symptomatic UTIs with urine cultures showing bacterial counts in the colonization range of < 50,000 CFU, as noted in case 4. Frequently, patients treated with methenamine have urinalyses with negative nitrites, positive leukocyte esterase, high WBCs, and few bacteria, but cultures show no growth. Some patients who did not reliably take medications as prescribed had recurrent symptomatic UTIs. Some had a subsequent UTI culturing a different organism or a change in the sensitivity profile of the same organism. This phenomenon suggests that formaldehyde disrupts the manufacture and transmission of the proteins and enzymes responsible for bacterial resistance factors.
Freeman and colleagues conducted a prospective study of 249 men with bacteruria followed for up to 10 years.18 Continuous therapy with methenamine delayed recurrence of bacteruria. Nilsson found that recurrent UTIs were reduced by 25% with long-term treatment (> 3 months) with methenamine.19
Bacteria do not develop resistance to methenamine.20 Reports of AEs are low, and drug interactions are limited to sulfamethizole, which can cause crystallization in the urine. Daily dosing used in studies ranged from 1 g to 4 g daily.21 Nilsson conducted research over 16 months with geriatric patients and found no changes in renal function or crystallization in urine.19
Severe hepatic impairment is also a contraindication, as methenamine can be hydrolyzed to ammonia. Studies have shown a reduced effectiveness with lower urinary tract abnormalities, although those studies administered the medication for short periods of time.21 Because the action of the medication relies on ≥ 2 hours of exposure to urine in the bladder, patients with indwelling catheters or patients who urinate frequently experience little benefit.22 Ideal candidates for methenamine are those with urinary retention and recurrent UTIs.
Although the use of methenamine has increased in Norway and Sweden by 24% since 2000, the use of methenamine in the U.S. remains low, perhaps because of conflicting reports in the literature regarding effectiveness and use with limited populations (ie, noncatheterized patients, those able to retain urine for ≥ 2 hours, and a creatinine clearance > 50 mg/dL).3
Some health care providers use methenamine for UTI prophylaxis, but this practice is less common in the U.S. than it is in Scandinavian countries.3 However, no published studies have explored the action of methenamine on MRSA, ESBL, and VRE bacteria or on the enzymes and proteins that enable and transmit bacterial resistance factors.
Elderly patients with complicated recurrent UTIs due to resistant bacteria are often left with no oral antibiotic options. Costs escalate rapidly when IV antibiotics are given. Administration generally requires hospitalization with close monitoring of renal function and drug levels and the placement of a PICC or midline IV access. If there is no caregiver, then hospitalization followed by an admission to a skilled nursing facility is required.
Lee and colleagues concluded that there is a need for further studies to explore long-duration therapy with methenamine.21 No studies have addressed its use in the geriatric population for long-term use of prevention of recurrent UTIs. No studies have been done on its use for primary treatment of MDR UTIs. The benefits of this drug with a low AE profile and low cost ($60/month for 1 g bid), which has been proven to reduce the incidence and/or delay recurrence of UTIs, is well worth further examination.
Conclusion
Multiple studies over 60 years have shown methenamine hippurate to be a well-tolerated and safe medication. Little data are available about the use of this medication in the elderly in the U.S., despite its wide use in Scandinavian countries. Use of methenamine for MDR UTIs in the geriatric population has been shown to be safe and effective, as presented in these case studies. Substantial cost savings were realized with the use of methenamine in these geriatric patients by reducing hospitalizations and complications due to recurrent MDR UTIs. The use of methenamine for treating MDR UTIs and the prevention of recurrent UTIs in the geriatric population warrants further clinical use and research.
The very interesting changes noted in sensitivity of the same bacteria in subsequent UTIs in patients treated with methenamine raises questions about the action of formaldehyde in the bladder on bacterial resistance factors. Given the worldwide increase in bacterial resistance to currently available antibiotics, this is a most compelling action that demands further study.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med. 2002;113(suppl 1A):5S-13S.
2. Kamel HK. Managing urinary tract infections: Guide for nursing home practitioners. Ann of Long Term Care. 2005;13(9):21-28.
3. Blix HS, Røed J, Sti MO. Large variation in antibacterial use among Norwegian nursing homes. Scand J Infect Dis. 2007;39(6-7):536-541.
4. Nicolle LE. Asymptomatic bacteruria in diabetic women. Diabetes Care. 2000;23(6):722-723.
5. Rhoads J, Clayman A, Nelson S. The relationship of urinary tract infections and falls in a nursing home. Director. 2007;15(1):22-26.
6. Rodhe N, Mølstad S, Englund L, Svärdsudd K. Asymptomatic bacteriuria in a population of elderly residents living in a community setting: Prevalence, characteristics and associated factors. Fam Pract. 2006;23(3):303-307.
7. Woodford HJ, George J. Diagnosis and management of urinary tract infection in hospitalized older people. J Am Geriatr Soc. 2009;57(1):107-114.
8. Levison ME, Kaye D. Treatment of complicated urinary tract infections with an emphasis on drug-resistant gram-negative uropathogens. Curr Infect Dis Rep. 2013;15(2):109-115.
9. Miller LG, Tang AW. Treatment of uncomplicated urinary tract infections in an era of increasing antimicrobial resistance. Mayo Clin Proc. 2004;79(8):1048-1053.
10. Nicoletti J, Kuster SP, Sulser T, et al. Risk factors for urinary tract infections due to ciprofloxacin-resistant Escherichia coli in a tertiary care urology department in Switzerland. Swiss Med Wkly. 2010;140:w13059.
11. Nicolle LE. Urinary tract infection in geriatric and institutionalized patients. Curr Opin Urol. 2002;12(1):51-55.
12. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660.
13. Spellberg B, Guidos R, Gilbert D, et al; Infectious Diseases Society of America. The epidemic of antibiotic-resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(2):155-164.
14. Dagley S, Dawes EA, Morrison GA. Inhibition of growth of Aerobacter aerogenes: The mode of action of phenols, alcohols, acetone, and ethyl acetate.
J Bacteriol. 1950;60(4):369-379.
15. Neely WB. Action of formaldehyde on microorganisms I. Correlation of activity with formaldehyde metabolism. J Bacteriol. 1963;85(5):1028-1031.
16. Musher DM, Griffith DP. Generation of formaldehyde from methenamine: Effect of pH and concentration, and antibacterial effect. Antimicrob Agents Chemother. 1974;6(6):708-711.
17. Scientific Committee on Health and Environmental Risks. Risk Assessment Report on Methenamine. Brussels, Belgium: European Commission; 2007. CAS 100-97-0.
18. Freeman RB, Smith WM, Richardson JA, et al. Long-term therapy for chronic bacteriuria in men. U.S. Public Health Service cooperative study. Ann Intern Med. 1975;83(2):133-147.
19. Nilsson S. Long-term treatment with methenamine hippurate in recurrent urinary tract infection. Acta Med Scand. 1975;198(1-2):81-85.
20. Drugs.com. Methenamine (systemic). http://www.drugs.com/mmx/methenamine-hippurate.html?printable=1. Updated March 28, 2000. Accessed June 17, 2014.
21. Lee BSB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;10:CD003265.
22. Lee BB, Haran MJ, Hunt LM, et al. Spinal-injured neuropathic bladder antisepsis (SINBA) trial. Spinal Cord. 2007;45(8):542-550.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med. 2002;113(suppl 1A):5S-13S.
2. Kamel HK. Managing urinary tract infections: Guide for nursing home practitioners. Ann of Long Term Care. 2005;13(9):21-28.
3. Blix HS, Røed J, Sti MO. Large variation in antibacterial use among Norwegian nursing homes. Scand J Infect Dis. 2007;39(6-7):536-541.
4. Nicolle LE. Asymptomatic bacteruria in diabetic women. Diabetes Care. 2000;23(6):722-723.
5. Rhoads J, Clayman A, Nelson S. The relationship of urinary tract infections and falls in a nursing home. Director. 2007;15(1):22-26.
6. Rodhe N, Mølstad S, Englund L, Svärdsudd K. Asymptomatic bacteriuria in a population of elderly residents living in a community setting: Prevalence, characteristics and associated factors. Fam Pract. 2006;23(3):303-307.
7. Woodford HJ, George J. Diagnosis and management of urinary tract infection in hospitalized older people. J Am Geriatr Soc. 2009;57(1):107-114.
8. Levison ME, Kaye D. Treatment of complicated urinary tract infections with an emphasis on drug-resistant gram-negative uropathogens. Curr Infect Dis Rep. 2013;15(2):109-115.
9. Miller LG, Tang AW. Treatment of uncomplicated urinary tract infections in an era of increasing antimicrobial resistance. Mayo Clin Proc. 2004;79(8):1048-1053.
10. Nicoletti J, Kuster SP, Sulser T, et al. Risk factors for urinary tract infections due to ciprofloxacin-resistant Escherichia coli in a tertiary care urology department in Switzerland. Swiss Med Wkly. 2010;140:w13059.
11. Nicolle LE. Urinary tract infection in geriatric and institutionalized patients. Curr Opin Urol. 2002;12(1):51-55.
12. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653-660.
13. Spellberg B, Guidos R, Gilbert D, et al; Infectious Diseases Society of America. The epidemic of antibiotic-resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(2):155-164.
14. Dagley S, Dawes EA, Morrison GA. Inhibition of growth of Aerobacter aerogenes: The mode of action of phenols, alcohols, acetone, and ethyl acetate.
J Bacteriol. 1950;60(4):369-379.
15. Neely WB. Action of formaldehyde on microorganisms I. Correlation of activity with formaldehyde metabolism. J Bacteriol. 1963;85(5):1028-1031.
16. Musher DM, Griffith DP. Generation of formaldehyde from methenamine: Effect of pH and concentration, and antibacterial effect. Antimicrob Agents Chemother. 1974;6(6):708-711.
17. Scientific Committee on Health and Environmental Risks. Risk Assessment Report on Methenamine. Brussels, Belgium: European Commission; 2007. CAS 100-97-0.
18. Freeman RB, Smith WM, Richardson JA, et al. Long-term therapy for chronic bacteriuria in men. U.S. Public Health Service cooperative study. Ann Intern Med. 1975;83(2):133-147.
19. Nilsson S. Long-term treatment with methenamine hippurate in recurrent urinary tract infection. Acta Med Scand. 1975;198(1-2):81-85.
20. Drugs.com. Methenamine (systemic). http://www.drugs.com/mmx/methenamine-hippurate.html?printable=1. Updated March 28, 2000. Accessed June 17, 2014.
21. Lee BSB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;10:CD003265.
22. Lee BB, Haran MJ, Hunt LM, et al. Spinal-injured neuropathic bladder antisepsis (SINBA) trial. Spinal Cord. 2007;45(8):542-550.
23-year-old woman being treated for opioid dependence, unexpected weight gain
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
THE CASE
We were treating a 23-year-old woman in our clinic for opioid dependence. She had begun using hydrocodone/acetaminophen, oxycodone, and heroin at age 17. Her parents and relatives had a history of alcohol and drug addiction and her brother had died from a heroin overdose.
The patient was taking buprenorphine/naloxone 12 mg/3 mg daily. She attended weekly counseling sessions at a community outreach center. We explained to her the potentially dangerous effects of buprenorphine/naloxone. Urine toxicology was negative for substances other than buprenorphine/naloxone.
Over 8 months, our patient gained 33 pounds and began wearing loose clothing to her appointments. When we asked her about it, she said that she had been “eating more bagels” lately.
What the patient wasn’t telling us was that she was pregnant. (We learned of her pregnancy only after she delivered.) In addition, she didn’t disclose to her obstetrician (OB) that she was taking buprenorphine/naloxone until she was nearly full term. At that point, the OB consulted maternal fetal medicine, and the buprenorphine/naloxone was continued through delivery. The patient had an uncomplicated spontaneous vaginal delivery of an 8.19 lb girl with an APGAR score of 8 at 1 minute and 8 again at 5 minutes.
Concerned about neonatal abstinence syndrome (NAS), which is characterized by tremors, increased body tone, feeding intolerance, vomiting, sweating, and fever, the healthcare team used the NAS scoring system to assess the newborn’s need for pharmacologic therapy. The newborn’s score at birth was 16/45. It then dropped to 11/45 indicating that she was experiencing mild withdrawal, but her symptoms—grunting, tachycardia, increased tone, tremors, irritability, and sweating—suggested she was experiencing severe withdrawal. The infant remained hospitalized for 29 days and received oral morphine titrated to her NAS score. The drug regimen for treatment/tapering was oral morphine given at 0.1 mg/kg/dose every 4 hours. This dose was lowered by 10% each time her NAS score was <8. At discharge, the infant’s NAS score had decreased to 3/45.
After discharge, the mother admitted to us that she concealed her pregnancy because she was afraid of being placed on methadone. She said she didn’t want to have to go to a clinic to receive the medication.
Continued good health. The child has since reached all of her developmental milestones appropriately and has normal height and weight.
DISCUSSION
Opioid abuse is an increasing cause of morbidity and mortality. In the United States, the number of deaths from opioid overdose is approaching that of motor vehicle accidents: approximately 100 deaths a day.1
The use of opioids by a pregnant woman can cause intrauterine growth retardation and preterm delivery.2 It also can result in withdrawal symptoms in the newborn,3 necessitating treatment guided by the NAS score. This score takes into consideration the metabolic, respiratory, central nervous system, and gastrointestinal symptoms of the infant at specified time intervals.4
Treatment options. For nonpregnant patients, opioid dependence typically is treated with methadone, an opioid agonist or buprenorphine, a partial opioid agonist; buprenorphine usually is prescribed as a combination medication that also contains naloxone, an opioid antagonist.
While methadone must be prescribed through licensed clinics, physicians meeting specific qualifications can prescribe buprenorphine or buprenorphine/naloxone in the office setting.5 Studies have supported the effectiveness of buprenorphine, alone or in combination with naloxone, in discouraging illicit opioid use.6-8
When the patient is pregnant… Methadone is the current standard of care for opioid-dependent patients who become pregnant.9 Buprenorphine/naloxone is currently a US Food and Drug Administration category C drug. However, recent studies have demonstrated the safety of buprenorphine without naloxone during pregnancy.10,11
The incidence and severity of NAS following treatment with buprenorphine is less than or comparable to methadone maintenance.10,11 The NAS score of 11 recorded in our patient’s case was comparable to those reported by Jones et al,9 who found neonates of women on buprenorphine had an average maximum NAS score of 11 and those on methadone had a maximum of 12.8.
Higher birth weights have been found for infants in the buprenorphine group. One study noted a mean birth weight of 6.48 lb in a methadone group vs 7.17 lb in a buprenorphine group, a statistically significant difference.11 The birth weight of our patient’s daughter (8.19 lb) was higher than those reported in studies of women receiving buprenorphine and methadone.11,12
Hospital stays were shorter for neonates exposed to buprenorphine when compared to methadone.12 When methadone was used as maintenance therapy their hospital stays were between 8.1 and 19.7 days. On average, buprenorphine-exposed neonates were hospitalized between 6.8 and 10 days.9,11,12
THE TAKEAWAY
Physicians who prescribe or care for women who receive buprenorphine need to remain alert for the possibility of pregnancy. Assess your patient’s weight at each appointment. If you suspect she has become pregnant, address the issue with the patient and obtain consent for a pregnancy test. Although buprenorphine is a category C drug, patients who become pregnant should be made aware that several studies have found that buprenorphine can be used safely and effectively during pregnancy9-12 and it may be an option to continue the medication through delivery.
Because naloxone can trigger withdrawal symptoms in a fetus if a mother uses illicit opioids while pregnant, we recommend that naloxone be discontinued once pregnancy is discovered.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
1. Centers for Disease Control and Prevention (CDC). Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Moral Wkly Rep. 2011;60:1487-1492.
2. Dattel BJ. Substance abuse in pregnancy. Semin Perinatol. 1990;14:179-187.
3. Kassim Z, Greenough A. Neonatal abstinence syndrome: Identification and management. Curr Paediatrics. 2006;16:172-175.
4. Finnegan LP, Kandall SR. Maternal and neonatal effects of drug dependence in pregnancy. In: Lowinson J, Ruiz P, Millman RB, et al, eds. Substance Abuse: A Comprehensive Textbook. 2nd ed. Baltimore, MD: Williams & Wilkins; 1992.
5. US Department of Health and Human Services. Drug Addiction Treatment Act of 2000. US Department of Health and Human Services Web site. Available at: http://buprenorphine.samhsa.gov/fulllaw.html. Accessed June 4, 2014.
6. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med. 2003;349:949-958.
7. Bell J, Byron G, Gibson A, et al. A pilot study of buprenorphine-naloxone combination tablet (Suboxone) in treatment of opioid dependence. Drug and Alcohol Rev. 2004;23:311-317.
8. Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend. 2010;106:56-60.
9. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320-2331.
10. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003;70(2 suppl):S87-S101.
11. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008;96:69-78.
12. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79:1-10.
Young girl with lower leg rash
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
An 8-year-old girl was brought into our clinic for evaluation of a leg rash on her right lower leg that had been bothering her for 2 months. Another physician had performed a biopsy and diagnosed subacute spongiotic dermatitis, but the rash did not respond to treatment with triamcinolone cream 0.1% twice daily.
The rash was mildly tender and markedly pruritic. The girl had no history of trauma, prior skin conditions, or other areas with a similar rash. Physical examination revealed concentric annular lesions on the right lower leg (FIGURE). The central areas demonstrated a bruised appearance that did not resolve with diascopy.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: tinea corporis
A potassium hydroxide (KOH) preparation was performed. It showed septate hyphae and confirmed a diagnosis of tinea corporis. We ordered a periodic acid-Schiff (PAS) stain on the previous biopsy specimen, and it revealed septate hyphae in the stratum corneum that were not apparent on the original hematoxylin and eosin (H&E) stained sections.
Dermatophyte infections of the skin are known as tinea corporis or “ringworm.” Ringworm fungi belong to 3 genera, Microsporum, Trichophyton, and Epidermophyton. These infections occur at any age and are more common in warmer climates.1 The classic lesion is an annular scaly patch, sometimes with the concentric rings, as seen in our patient (FIGURE). The bruising was almost certainly caused by rubbing and scratching.
We suspected tinea coporis based on the physical characteristics of the rash and the fact that it did not respond promptly to topical steroids. Our suspicions were confirmed by the KOH prep. Inked KOH using chlorazol black E stain turns fungal hyphae black, which makes them easier to distinguish from keratinocyte cell walls.2
Differential of a nonspecific rash should include infections
The initial misdiagnosis was based on the histopathologic diagnosis of spongiotic dermatitis. Subacute spongiotic dermatitis is associated with intracellular and intercellular edema of the keratinocytes in the epidermis. This is a nonspecific finding seen in eczematous dermatitis and can be etiologically associated with a wide variety of clinical conditions, including allergic contact dermatitis, atopic dermatitis, nummular eczema, and, in this case, dermatophytosis.3
If a biopsy is performed for a nonspecific rash, the pathologist should be advised of the possibility of superficial fungal infection. Providing a history and the physical characteristics of the rash or a differential diagnosis will prompt the performance of a PAS stain. Otherwise, the diagnosis can be missed because fungal elements are often not visible on routine H&E stains.
Proper treatment
provides speedy relief
Tinea corporis on a non-hair-bearing area is readily cleared with a topical azole antifungal agent, such as ketoconazole cream 2% twice daily for 2 weeks or a topical allylamine, such as terbinafine cream 1%, twice daily for 2 weeks. Topical allylamines may be more effective than topical azoles for tinea corporis4 (strength of recommendation [SOR]: A). Hair-bearing areas such as the scalp, fingers, and toes are unlikely to respond to topically applied medications and require an oral anti-fungal medication, such as griseofulvin 15 to 20 mg/kg/d.5
Relief for our patient
Our patient’s rash was treated with griseofulvin oral suspension 20 mg/kg/d (with milk to enhance absorption) for 6 weeks. There was complete clearing and the condition did not recur.
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.
1. Shrum JP, Millikan LE, Bataineh O. Superficial fungal infections in the tropics. Dermatol Clin. 1994;12:687-693.
2. Burke WA, Jones BE. A simple stain for rapid office diagnosis of fungus infections of the skin. Arch Dermatol. 1984;120:1519-1520.
3. Alsaad KO, Ghazarian D. My approach to superficial inflammatory dermatoses. J Clin Pathol. 2005;58:1233-1241.
4. Rotta I, Otuki MF, Sanches AC, et al. Efficacy of topical antifungal drugs in different dermatomycoses: a systematic review with meta-analysis. Rev Assoc Med Bras. 2012;58:308-318.
5. Noble SL, Forbes RC, Stamm PL. Diagnosis and management of common tinea infections. Am Fam Physician. 1998;58:163-174,177-178.
