User login
Fever, wet cough, rash—Dx?
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
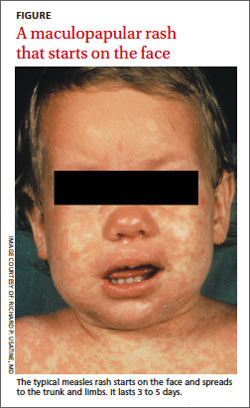
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
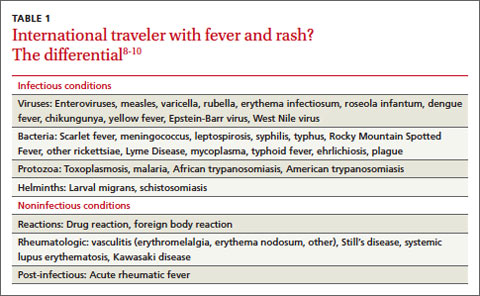
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness

Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
Displaced Ischial Stress Fracture Following Revision Total Hip Arthroplasty

Snapping Popliteus Tendon Within an Osteochondritis Dissecans Lesion: An Unusual Case of Lateral Knee Pain

Lateral Femoral Cutaneous Nerve Palsy Following Shoulder Surgery in the Beach Chair Position: A Report of 4 Cases

Timing of Forearm Deformity Correction in a Child With Multiple Hereditary Exostosis
Eikenella corrodens Septic Hip Arthritis in a Healthy Adult Treated With Arthroscopic Irrigation and Debridement

Meniscal Root Entrapment of an Osteochondritis Dissecans Loose Body
Acute small bowel obstruction owing to undiagnosed lung cancer
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Gout exacerbation, weakness, hypotension—Dx?
THE CASE
A 58-year-old female came to the emergency department (ED) because she had progressive weakness, hypotension, and altered mental status. In the ED she had a heart rate of 107 beats per minute; blood pressure, 96/68 mm Hg; respiratory rate, 20 breaths per minute; oxygen saturation, 96%; and a 96.7°F temperature that spiked to 101.6°F. The absolute neutrophil count (ANC) was 1500 cells/mm3, hemoglobin was 13 g/dL, and platelet count was 95 × 109/L. Her serum creatinine was 2.5 mg/dL (baseline of 1.0) and cyclosporine concentration was <25 ng/mL.
Our patient had a history of renal transplant, gout, and chronic kidney disease. Her medications included bumetanide, clonazepam, colchicine .6 mg BID, a therapeutic dose of cyclosporine, flurazepam, gabapentin, levothyroxine, mirtazapine, oxycodone, prednisone, and premarin. Three days before she came to the ED, she experienced a gout exacerbation and took six .6 mg doses (3.6 mg total) of colchicine that resulted in severe diarrhea. The next day, she took 3 mg of colchicine and had more severe diarrhea and a fever. Our patient took another 1.2 mg of colchicine the next day and developed the progressive weakness, hypotension, and altered mental status that led her to seek care in the ED.
THE DIAGNOSIS
Our patient was admitted to the hospital with a diagnosis of pancytopenia and presumed sepsis and intravenous broad-spectrum antibiotics were administered. Blood, urine, and sputum cultures, stool studies, and chest x-ray were negative for pneumonia. A peripheral blood smear revealed dysplastic-appearing neutrophils with vacuolization, which is characteristic of colchicine toxicity, myelodysplastic syndromes, or acute leukemia. However, the absence of blast cells in the peripheral blood smear and the normal appearance of the liver and spleen on a subsequent abdominal ultrasound refuted a primary hematologic disorder. Thus, based on the patient’s recent colchicine use and subsequent progressive pancytopenia and sepsis, we diagnosed colchicine toxicity in this patient.
DISCUSSION
Colchicine is a potent anti-inflammatory drug that has a narrow therapeutic index. Indicated for treating gout and familial Mediterranean fever, it inhibits mitosis by interfering with microtubule formation and arresting cell division. Colchicine is rapidly absorbed in the gastrointestinal (GI) tract and undergoes first-pass hepatic metabolism with enterohepatic recirculation of metabolites prior to excretion via the biliary tract.1 Ten percent to 20% of colchicine is excreted by the kidneys.2
Colchicine toxicity begins with GI symptoms, such as diarrhea, is followed by falling peripheral blood cell counts and altered mental status. A late sign of colchicine toxicity is alopecia. If the toxicity is left unchecked, multi-organ dysfunction that mimics severe sepsis will occur, resulting in death.3
Toxicity typically occurs at doses of .5 mg/kg/d. Fatal overdose from colchicine has been described in patients taking as little as 7 mg; however, survival from a 60-mg overdose has been reported.1 In a review of 150 patients who overdosed on colchicine, a single dose of .8 mg/kg was universally fatal.4 Therapeutic doses of colchicine have resulted in severe toxicity in patients with hepatic or renal dysfunction.5,6
Toxicity risk is increased in patients taking immunosuppressants
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs, particularly cyclosporine. In case series, patients taking stable doses of cyclosporine and prophylactic doses of colchicine exhibited toxicity when they took therapeutic doses of colchicine for gout exacerbations.7,8 Another case series described 2 post-renal transplant patients, immunosuppressed with azathioprine and prednisone, who had comorbid familial Mediterranean fever and were maintained on colchicine prophylaxis.9 When they converted to cyclosporine for immunosuppression, each patient began to demonstrate GI and muscular symptoms of colchicine toxicity. Upon discontinuing cyclosporine, the GI and muscular symptoms rapidly resolved.9
How cyclosporine interacts with colchicine. Cyclosporine is a potent CYP3A4 and P-glycoprotein inhibitor, and colchicine is a CYP3A4 and P-glycoprotein substrate. In vivo studies have demonstrated that cyclosporine inhibits hepatic and renal clearance of colchicine, thus increasing serum colchicine levels, further lowering the toxic colchicine dose.10,11
Our patient. The prophylactic dosage of colchicine our patient had been taking before her recent gout flare (.6 mg BID) was higher than the adjusted dose recommended to treat gout flares for patients taking cyclosporine (a single .6 mg dose to be repeated no earlier than 3 days).4 The dosages she took to treat her flare far exceeded this recommendation.
As a result, our patient developed severe colchicine toxicity. During her hospitalization, our patient’s cell counts continued to fall, requiring blood and platelet transfusions; her ANC nadir was 14 cells/mm3. She continued to have progressive multi-organ failure and developed alopecia. Management revolved around supportive measures for all of the end-organ effects.
Our patient died on hospital Day 7. Contributing factors included premorbid immunosuppression, renal insufficiency, and concomitant P-glycoprotein and CYP3A4 inhibition.
THE TAKEAWAY
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs. Physicians who prescribe colchicine should be aware of these additional risks and adjust dosages accordingly. Activated charcoal can be given for acute overdose.
1. Maxwell MJ, Muthu P, Pritty PE. Accidental colchicine overdose. A case report and literature review. Emerg Med J. 2002;19:265-267.
2. Gruberg L, Har-Zahav Y, Agranat O, et al. Acute myopathy induced by colchicine in a cyclosporine treated heart transplant recipient: possible role of the multidrug resistance transporter. Transplant Proc. 1999;31:2157-2158.
3. Colchicine: serious interactions. Prescrire Int. 2008;17:151-153.
4. Colcrys [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2012.
5. Dickinson M, Juneja S. Haematological toxicity of colchicine. Br J Haematol. 2009;146:465.
6. Lee KY, Kim do Y, Chang JY, et al. Two cases of acute leukopenia induced by colchicine with concurrent immunosuppressants use in Behçet’s disease. Yonsei Med J. 2008;49:171-173.
7. Rieger EH, Halasz NA, Wahlstrom HE. Colchicine neuromyopathy after renal transplantation. Transplantation. 1990;49:1196-1198.
8. Minetti E, Minetti L. Multiple organ failure in a kidney transplant patient receiving both colchicine and cyclosporine. J Nephrol. 2003;16:421-425.
9. Yussim A, Bar-Nathan N, Lustig S, et al. Gastrointestinal, hepatorenal, and neuromuscular toxicity caused by cyclosporine-colchicine interaction in renal transplantation. Transplant Proc. 1994;26:2825-2826.
10. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by the kidney multidrug transporter studied in vivo. J Pharmacol Exp Ther. 1992;261:50-55.
11. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by a liver canalicular transporter studied in vivo. Hepatology. 1992;15:899-903.
THE CASE
A 58-year-old female came to the emergency department (ED) because she had progressive weakness, hypotension, and altered mental status. In the ED she had a heart rate of 107 beats per minute; blood pressure, 96/68 mm Hg; respiratory rate, 20 breaths per minute; oxygen saturation, 96%; and a 96.7°F temperature that spiked to 101.6°F. The absolute neutrophil count (ANC) was 1500 cells/mm3, hemoglobin was 13 g/dL, and platelet count was 95 × 109/L. Her serum creatinine was 2.5 mg/dL (baseline of 1.0) and cyclosporine concentration was <25 ng/mL.
Our patient had a history of renal transplant, gout, and chronic kidney disease. Her medications included bumetanide, clonazepam, colchicine .6 mg BID, a therapeutic dose of cyclosporine, flurazepam, gabapentin, levothyroxine, mirtazapine, oxycodone, prednisone, and premarin. Three days before she came to the ED, she experienced a gout exacerbation and took six .6 mg doses (3.6 mg total) of colchicine that resulted in severe diarrhea. The next day, she took 3 mg of colchicine and had more severe diarrhea and a fever. Our patient took another 1.2 mg of colchicine the next day and developed the progressive weakness, hypotension, and altered mental status that led her to seek care in the ED.
THE DIAGNOSIS
Our patient was admitted to the hospital with a diagnosis of pancytopenia and presumed sepsis and intravenous broad-spectrum antibiotics were administered. Blood, urine, and sputum cultures, stool studies, and chest x-ray were negative for pneumonia. A peripheral blood smear revealed dysplastic-appearing neutrophils with vacuolization, which is characteristic of colchicine toxicity, myelodysplastic syndromes, or acute leukemia. However, the absence of blast cells in the peripheral blood smear and the normal appearance of the liver and spleen on a subsequent abdominal ultrasound refuted a primary hematologic disorder. Thus, based on the patient’s recent colchicine use and subsequent progressive pancytopenia and sepsis, we diagnosed colchicine toxicity in this patient.
DISCUSSION
Colchicine is a potent anti-inflammatory drug that has a narrow therapeutic index. Indicated for treating gout and familial Mediterranean fever, it inhibits mitosis by interfering with microtubule formation and arresting cell division. Colchicine is rapidly absorbed in the gastrointestinal (GI) tract and undergoes first-pass hepatic metabolism with enterohepatic recirculation of metabolites prior to excretion via the biliary tract.1 Ten percent to 20% of colchicine is excreted by the kidneys.2
Colchicine toxicity begins with GI symptoms, such as diarrhea, is followed by falling peripheral blood cell counts and altered mental status. A late sign of colchicine toxicity is alopecia. If the toxicity is left unchecked, multi-organ dysfunction that mimics severe sepsis will occur, resulting in death.3
Toxicity typically occurs at doses of .5 mg/kg/d. Fatal overdose from colchicine has been described in patients taking as little as 7 mg; however, survival from a 60-mg overdose has been reported.1 In a review of 150 patients who overdosed on colchicine, a single dose of .8 mg/kg was universally fatal.4 Therapeutic doses of colchicine have resulted in severe toxicity in patients with hepatic or renal dysfunction.5,6
Toxicity risk is increased in patients taking immunosuppressants
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs, particularly cyclosporine. In case series, patients taking stable doses of cyclosporine and prophylactic doses of colchicine exhibited toxicity when they took therapeutic doses of colchicine for gout exacerbations.7,8 Another case series described 2 post-renal transplant patients, immunosuppressed with azathioprine and prednisone, who had comorbid familial Mediterranean fever and were maintained on colchicine prophylaxis.9 When they converted to cyclosporine for immunosuppression, each patient began to demonstrate GI and muscular symptoms of colchicine toxicity. Upon discontinuing cyclosporine, the GI and muscular symptoms rapidly resolved.9
How cyclosporine interacts with colchicine. Cyclosporine is a potent CYP3A4 and P-glycoprotein inhibitor, and colchicine is a CYP3A4 and P-glycoprotein substrate. In vivo studies have demonstrated that cyclosporine inhibits hepatic and renal clearance of colchicine, thus increasing serum colchicine levels, further lowering the toxic colchicine dose.10,11
Our patient. The prophylactic dosage of colchicine our patient had been taking before her recent gout flare (.6 mg BID) was higher than the adjusted dose recommended to treat gout flares for patients taking cyclosporine (a single .6 mg dose to be repeated no earlier than 3 days).4 The dosages she took to treat her flare far exceeded this recommendation.
As a result, our patient developed severe colchicine toxicity. During her hospitalization, our patient’s cell counts continued to fall, requiring blood and platelet transfusions; her ANC nadir was 14 cells/mm3. She continued to have progressive multi-organ failure and developed alopecia. Management revolved around supportive measures for all of the end-organ effects.
Our patient died on hospital Day 7. Contributing factors included premorbid immunosuppression, renal insufficiency, and concomitant P-glycoprotein and CYP3A4 inhibition.
THE TAKEAWAY
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs. Physicians who prescribe colchicine should be aware of these additional risks and adjust dosages accordingly. Activated charcoal can be given for acute overdose.
THE CASE
A 58-year-old female came to the emergency department (ED) because she had progressive weakness, hypotension, and altered mental status. In the ED she had a heart rate of 107 beats per minute; blood pressure, 96/68 mm Hg; respiratory rate, 20 breaths per minute; oxygen saturation, 96%; and a 96.7°F temperature that spiked to 101.6°F. The absolute neutrophil count (ANC) was 1500 cells/mm3, hemoglobin was 13 g/dL, and platelet count was 95 × 109/L. Her serum creatinine was 2.5 mg/dL (baseline of 1.0) and cyclosporine concentration was <25 ng/mL.
Our patient had a history of renal transplant, gout, and chronic kidney disease. Her medications included bumetanide, clonazepam, colchicine .6 mg BID, a therapeutic dose of cyclosporine, flurazepam, gabapentin, levothyroxine, mirtazapine, oxycodone, prednisone, and premarin. Three days before she came to the ED, she experienced a gout exacerbation and took six .6 mg doses (3.6 mg total) of colchicine that resulted in severe diarrhea. The next day, she took 3 mg of colchicine and had more severe diarrhea and a fever. Our patient took another 1.2 mg of colchicine the next day and developed the progressive weakness, hypotension, and altered mental status that led her to seek care in the ED.
THE DIAGNOSIS
Our patient was admitted to the hospital with a diagnosis of pancytopenia and presumed sepsis and intravenous broad-spectrum antibiotics were administered. Blood, urine, and sputum cultures, stool studies, and chest x-ray were negative for pneumonia. A peripheral blood smear revealed dysplastic-appearing neutrophils with vacuolization, which is characteristic of colchicine toxicity, myelodysplastic syndromes, or acute leukemia. However, the absence of blast cells in the peripheral blood smear and the normal appearance of the liver and spleen on a subsequent abdominal ultrasound refuted a primary hematologic disorder. Thus, based on the patient’s recent colchicine use and subsequent progressive pancytopenia and sepsis, we diagnosed colchicine toxicity in this patient.
DISCUSSION
Colchicine is a potent anti-inflammatory drug that has a narrow therapeutic index. Indicated for treating gout and familial Mediterranean fever, it inhibits mitosis by interfering with microtubule formation and arresting cell division. Colchicine is rapidly absorbed in the gastrointestinal (GI) tract and undergoes first-pass hepatic metabolism with enterohepatic recirculation of metabolites prior to excretion via the biliary tract.1 Ten percent to 20% of colchicine is excreted by the kidneys.2
Colchicine toxicity begins with GI symptoms, such as diarrhea, is followed by falling peripheral blood cell counts and altered mental status. A late sign of colchicine toxicity is alopecia. If the toxicity is left unchecked, multi-organ dysfunction that mimics severe sepsis will occur, resulting in death.3
Toxicity typically occurs at doses of .5 mg/kg/d. Fatal overdose from colchicine has been described in patients taking as little as 7 mg; however, survival from a 60-mg overdose has been reported.1 In a review of 150 patients who overdosed on colchicine, a single dose of .8 mg/kg was universally fatal.4 Therapeutic doses of colchicine have resulted in severe toxicity in patients with hepatic or renal dysfunction.5,6
Toxicity risk is increased in patients taking immunosuppressants
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs, particularly cyclosporine. In case series, patients taking stable doses of cyclosporine and prophylactic doses of colchicine exhibited toxicity when they took therapeutic doses of colchicine for gout exacerbations.7,8 Another case series described 2 post-renal transplant patients, immunosuppressed with azathioprine and prednisone, who had comorbid familial Mediterranean fever and were maintained on colchicine prophylaxis.9 When they converted to cyclosporine for immunosuppression, each patient began to demonstrate GI and muscular symptoms of colchicine toxicity. Upon discontinuing cyclosporine, the GI and muscular symptoms rapidly resolved.9
How cyclosporine interacts with colchicine. Cyclosporine is a potent CYP3A4 and P-glycoprotein inhibitor, and colchicine is a CYP3A4 and P-glycoprotein substrate. In vivo studies have demonstrated that cyclosporine inhibits hepatic and renal clearance of colchicine, thus increasing serum colchicine levels, further lowering the toxic colchicine dose.10,11
Our patient. The prophylactic dosage of colchicine our patient had been taking before her recent gout flare (.6 mg BID) was higher than the adjusted dose recommended to treat gout flares for patients taking cyclosporine (a single .6 mg dose to be repeated no earlier than 3 days).4 The dosages she took to treat her flare far exceeded this recommendation.
As a result, our patient developed severe colchicine toxicity. During her hospitalization, our patient’s cell counts continued to fall, requiring blood and platelet transfusions; her ANC nadir was 14 cells/mm3. She continued to have progressive multi-organ failure and developed alopecia. Management revolved around supportive measures for all of the end-organ effects.
Our patient died on hospital Day 7. Contributing factors included premorbid immunosuppression, renal insufficiency, and concomitant P-glycoprotein and CYP3A4 inhibition.
THE TAKEAWAY
Colchicine toxicity from therapeutic doses may occur in patients taking concomitant immunosuppressive drugs. Physicians who prescribe colchicine should be aware of these additional risks and adjust dosages accordingly. Activated charcoal can be given for acute overdose.
1. Maxwell MJ, Muthu P, Pritty PE. Accidental colchicine overdose. A case report and literature review. Emerg Med J. 2002;19:265-267.
2. Gruberg L, Har-Zahav Y, Agranat O, et al. Acute myopathy induced by colchicine in a cyclosporine treated heart transplant recipient: possible role of the multidrug resistance transporter. Transplant Proc. 1999;31:2157-2158.
3. Colchicine: serious interactions. Prescrire Int. 2008;17:151-153.
4. Colcrys [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2012.
5. Dickinson M, Juneja S. Haematological toxicity of colchicine. Br J Haematol. 2009;146:465.
6. Lee KY, Kim do Y, Chang JY, et al. Two cases of acute leukopenia induced by colchicine with concurrent immunosuppressants use in Behçet’s disease. Yonsei Med J. 2008;49:171-173.
7. Rieger EH, Halasz NA, Wahlstrom HE. Colchicine neuromyopathy after renal transplantation. Transplantation. 1990;49:1196-1198.
8. Minetti E, Minetti L. Multiple organ failure in a kidney transplant patient receiving both colchicine and cyclosporine. J Nephrol. 2003;16:421-425.
9. Yussim A, Bar-Nathan N, Lustig S, et al. Gastrointestinal, hepatorenal, and neuromuscular toxicity caused by cyclosporine-colchicine interaction in renal transplantation. Transplant Proc. 1994;26:2825-2826.
10. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by the kidney multidrug transporter studied in vivo. J Pharmacol Exp Ther. 1992;261:50-55.
11. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by a liver canalicular transporter studied in vivo. Hepatology. 1992;15:899-903.
1. Maxwell MJ, Muthu P, Pritty PE. Accidental colchicine overdose. A case report and literature review. Emerg Med J. 2002;19:265-267.
2. Gruberg L, Har-Zahav Y, Agranat O, et al. Acute myopathy induced by colchicine in a cyclosporine treated heart transplant recipient: possible role of the multidrug resistance transporter. Transplant Proc. 1999;31:2157-2158.
3. Colchicine: serious interactions. Prescrire Int. 2008;17:151-153.
4. Colcrys [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2012.
5. Dickinson M, Juneja S. Haematological toxicity of colchicine. Br J Haematol. 2009;146:465.
6. Lee KY, Kim do Y, Chang JY, et al. Two cases of acute leukopenia induced by colchicine with concurrent immunosuppressants use in Behçet’s disease. Yonsei Med J. 2008;49:171-173.
7. Rieger EH, Halasz NA, Wahlstrom HE. Colchicine neuromyopathy after renal transplantation. Transplantation. 1990;49:1196-1198.
8. Minetti E, Minetti L. Multiple organ failure in a kidney transplant patient receiving both colchicine and cyclosporine. J Nephrol. 2003;16:421-425.
9. Yussim A, Bar-Nathan N, Lustig S, et al. Gastrointestinal, hepatorenal, and neuromuscular toxicity caused by cyclosporine-colchicine interaction in renal transplantation. Transplant Proc. 1994;26:2825-2826.
10. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by the kidney multidrug transporter studied in vivo. J Pharmacol Exp Ther. 1992;261:50-55.
11. Speeg KV, Maldonado AL, Liaci J, et al. Effect of cyclosporine on colchicine secretion by a liver canalicular transporter studied in vivo. Hepatology. 1992;15:899-903.
Case Studies in Toxicology: Hot as a Hare and Red as a Beet
A previously healthy 11-month-old boy was brought to the ED after his parents discovered him with an open bottle of nonprescription diphenhydramine. On initial presentation, the child was irritable with diffuse skin redness and dry mucous membranes. He was tremulous and making nonpurposeful reaching movements with his arms. He had roving eye movements and markedly dilated pupils that were minimally reactive. Initial vital signs were: blood pressure, 140/95 mm Hg; heart rate, 220 beats/minute; respiratory rate, 30 breaths/minute; temperature, 100.6ºF. Capillary glucose was 120 mg/dL, and oxygen saturation was 100% on room air. An electrocardiogram (ECG) revealed sinus tachycardia with normal QRS and QTc intervals.
What is the toxicological differential diagnosis?
Toxicity from several different classes of drugs may cause an altered level of consciousness, tachycardia, and hyperthermia. Serotonin agonists, such as selective serotonin reuptake inhibitors, may result in serotonin toxicity—a syndrome that includes altered cognition, autonomic changes (eg, tachycardia, hyperthermia), and neuromuscular effects (eg, rigidity, clonus), along with mydriasis and diaphoresis. Neuroleptic malignant syndrome (NMS) occurs following exposure to dopamine antagonists, such as antipsychotic medications.
Neuroleptic malignant syndrome presents in a similar manner to serotonin toxicity but tends to have a more indolent course compared with the abrupt onset and resolution of serotonin toxicity. Sympathomimetic medications (eg, methylphenidate) or drugs of abuse (eg, cocaine, methamphetamines) result in catecholamine effects including tachycardia, hypertension, diaphoresis, and mydriasis. Acetylsalicylic-acid (aspirin) toxicity (salicylism) often causes tinnitus, hyperpnea, and gastrointestinal (GI) effects following exposure. Severe toxicity may cause altered level of consciousness and hyperthermia; however, these are ominous and late findings. Mydriasis is not common.
What is the anticholinergic toxidrome?
Acetylcholine is a neurotransmitter present both in the central and peripheral nervous systems. In the periphery, acetylcholine acts at both the sympathetic and parasympathetic components of the autonomic nervous system and at somatic motor fibers. Acetylcholine acts at two classes of receptors, namely, nicotinic and muscarinic types. Muscarinic receptors are found in the central nervous system (CNS) (specifically the brain) and peripherally on effector cells of the parasympathetic nervous system and on sympathetically innervated sweat glands.1 Anticholinergic toxicity results from antagonism of muscarinic receptors and is more appropriately referred to as antimuscarinic poisoning, though the terms are used interchangeably. Nicotinic receptor antagonists are used primarily for neuromuscular blockade and do not cause this syndrome.
- “Hot as a hare” (anhidrosis with temperature elevation);
- “Red as a beet” (vasodilation with skin hyperemia);
- “Blind as a bat” (pupillary dilation with loss of accommodation);
- “Dry as a bone” (drying of mucosal surfaces and skin);
- “Full as a flask” (urinary retention); “Stuffed as a pepper” (constipation); and
- “Mad as a hatter” (describing the central anticholinergic effects that are often present—eg, altered mental status manifested as agitation, delirium, hallucinations, abnormal picking movements, rarely seizures).
Elderly patients and those with underlying medical illness or psychiatric disorders may be more prone to the CNS manifestations of anticholinergic medications. Anticholinergic effects can occur through ingestion, smoking, inhalation, and topical absorption (including transdermal or ophthalmic routes). Delayed or prolonged effects may occur due to slow gastric emptying and prolonged GI absorption. The duration of effects is variable and central anticholinergic manifestations of confusion or agitation may be present for several days, even after peripheral manifestations have resolved (termed the central anticholinergic syndrome).
What are common causes of anticholinergic toxicity?
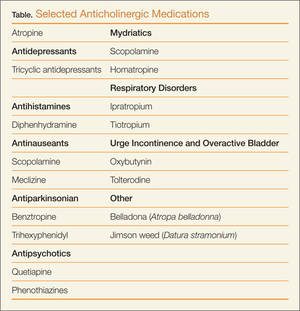
Although anticholinergic effects are often described in terms of “toxicity,” these effects are often used for therapeutic benefit. Such roles of anticholinergic agents include the following:
- Atropine to treat bradycardia;
- Ipratropium bromide to manage asthma;
- Antinauseants (eg, scopolamine, meclizine) for symptom relief;
- Tolterodine to treat urge incontinence and overactive bladder; and
- Ophthalmologic medications (eg, scopolamine, homatropine) to inhibit ciliary spasm in patients with iritis.
Although the above medications are being used for a specific anticholinergic property, other unintended and troublesome anticholinergic effects are often seen. Similarly, many other medications often have unintended anticholinergic effects (see Table). Anticholinergic “toxicity” is simply an extension of the effects that occur with therapeutic use.
What is the treatment for patients with anticholinergic toxicity?
Most patients with anticholinergic toxicity do well with supportive management. Benzodiazepines are the treatment of choice for agitation. Haloperidol and other antipsychotics are relatively contraindicated for treatment of agitation as they may impair temperature regulation and lead to hyperthermia. Although likely of limited overall benefit, oral activated charcoal may reduce the amount of drug absorbed.
Antidotal therapy with physostigmine should be considered for select patients presenting with altered mental status due to an anticholinergic. Physostigmine is an acetylcholinesterase inhibitor that prevents the breakdown of acetylcholine in the synaptic cleft, thus antagonizing the effects of anticholinergic drugs. A retrospective study noted a lower incidence of complications and shorter time to recovery with the use of physostigmine compared with benzodiazepines in patients with anticholinergic toxicity.2 The use of physostigmine in select patients may obviate the need for a further delirium workup, which often includes computed tomography or lumbar puncture.
When administering physostigmine, atropine should be present at the bedside with airway equipment readily available as cholinergic effects may develop (specifically bronchospasm, bronchorrhea, or bradycardia). Dosing of physostigmine in adult patients is 1 to 2 mg via slow intravenous (IV) push, in aliquots of 0.2 to 0.3 mg each, over 5 minutes; pediatric dosing is 20 mcg/kg to maximum 0.5 mg. Onset of effects can be expected within minutes of administration.3 Since the duration of physostigmine is less than that of many anticholinergic drugs, recurrence of anticholinergic effects should be anticipated.
Historically, physostigmine was included in the “coma cocktail,” along with thiamine, dextrose, and naloxone for treating undifferentiated patients with altered level of consciousness. Concern for its ubiquitous use arose following reports of asystole in two patients who presented with tricyclic antidepressant (TCA) overdose, although these patients actually had more complicated multidrug overdoses.4 Nevertheless, an ECG should be performed in all patients for whom physostigmine is being considered, and it should not be administered (or perhaps only extremely cautiously) if the ECG demonstrates a QRS complex duration >100 ms.3 Relative contraindications include reactive airways disease, peripheral vascular disease, or intestinal or bladder-outlet obstruction.
Prolongation of the QRS interval is not always indicative of TCA ingestion as certain other antimuscarinic drugs, such as diphenhydramine, may cause sodium-channel blockade. Based on extrapolation from TCA literature,5 if the QRS >100 ms, a bolus of 1 to 2 mEq/kg sodium bicarbonate should be given with monitoring of the QRS interval for narrowing.
Case conclusion
The clinicians at the bedside felt that the infant’s presentation was consistent with anticholinergic toxicity. Physostigmine was administered by slow IV push for a total dose of 1.5 mg. The patient had immediate improvement of symptoms, including decreased skin redness, decreased agitation, and improved vital signs (BP, 118/80 mm Hg and HR, 160 beats/minute). He was admitted to the pediatric intensive care unit for monitoring and was subsequently discharged home with complete symptom resolution 2 days later.
- Gerretsen P, Pollock BG. Drugs with anticholinergic properties: a current perspective on use and safety. Expert Opin Drug Saf. 2011;10(5):751-765.
- Burns MJ, Linden CH, Graudins A, Brown RM, Fletcher KE. A comparison of physostigmine and benzodiazepines for the treatment of anticholinergic poisoning. Ann Emerg Med. 2000;35(4):374-381.
- Howland MA. Physostigmine salicylate. In: Nelson LS, Lewin NA, Howland MA, Hoffman RS, Goldfrank LR, Flomenbaum NE, eds. Goldfrank’s Toxicologic Emergencies. 9th ed. New York, NY: McGraw Hill; 2011:759-762.
- Pentel P, Peterson CD. Asystole complicating physostigmine treatment of tricyclic antidepressant overdose. Ann Emerg Med. 1980;9(11):588-590.
- Boehnert MT, Lovejoy FH, Jr. Value of the QRS duration versus the serum drug level in predicting seizures and ventricular arrhythmias after an acute overdose of tricyclic antidepressants. N Engl J Med. 1985;313(8):474-479.
A previously healthy 11-month-old boy was brought to the ED after his parents discovered him with an open bottle of nonprescription diphenhydramine. On initial presentation, the child was irritable with diffuse skin redness and dry mucous membranes. He was tremulous and making nonpurposeful reaching movements with his arms. He had roving eye movements and markedly dilated pupils that were minimally reactive. Initial vital signs were: blood pressure, 140/95 mm Hg; heart rate, 220 beats/minute; respiratory rate, 30 breaths/minute; temperature, 100.6ºF. Capillary glucose was 120 mg/dL, and oxygen saturation was 100% on room air. An electrocardiogram (ECG) revealed sinus tachycardia with normal QRS and QTc intervals.
What is the toxicological differential diagnosis?
Toxicity from several different classes of drugs may cause an altered level of consciousness, tachycardia, and hyperthermia. Serotonin agonists, such as selective serotonin reuptake inhibitors, may result in serotonin toxicity—a syndrome that includes altered cognition, autonomic changes (eg, tachycardia, hyperthermia), and neuromuscular effects (eg, rigidity, clonus), along with mydriasis and diaphoresis. Neuroleptic malignant syndrome (NMS) occurs following exposure to dopamine antagonists, such as antipsychotic medications.
Neuroleptic malignant syndrome presents in a similar manner to serotonin toxicity but tends to have a more indolent course compared with the abrupt onset and resolution of serotonin toxicity. Sympathomimetic medications (eg, methylphenidate) or drugs of abuse (eg, cocaine, methamphetamines) result in catecholamine effects including tachycardia, hypertension, diaphoresis, and mydriasis. Acetylsalicylic-acid (aspirin) toxicity (salicylism) often causes tinnitus, hyperpnea, and gastrointestinal (GI) effects following exposure. Severe toxicity may cause altered level of consciousness and hyperthermia; however, these are ominous and late findings. Mydriasis is not common.
What is the anticholinergic toxidrome?
Acetylcholine is a neurotransmitter present both in the central and peripheral nervous systems. In the periphery, acetylcholine acts at both the sympathetic and parasympathetic components of the autonomic nervous system and at somatic motor fibers. Acetylcholine acts at two classes of receptors, namely, nicotinic and muscarinic types. Muscarinic receptors are found in the central nervous system (CNS) (specifically the brain) and peripherally on effector cells of the parasympathetic nervous system and on sympathetically innervated sweat glands.1 Anticholinergic toxicity results from antagonism of muscarinic receptors and is more appropriately referred to as antimuscarinic poisoning, though the terms are used interchangeably. Nicotinic receptor antagonists are used primarily for neuromuscular blockade and do not cause this syndrome.
- “Hot as a hare” (anhidrosis with temperature elevation);
- “Red as a beet” (vasodilation with skin hyperemia);
- “Blind as a bat” (pupillary dilation with loss of accommodation);
- “Dry as a bone” (drying of mucosal surfaces and skin);
- “Full as a flask” (urinary retention); “Stuffed as a pepper” (constipation); and
- “Mad as a hatter” (describing the central anticholinergic effects that are often present—eg, altered mental status manifested as agitation, delirium, hallucinations, abnormal picking movements, rarely seizures).
Elderly patients and those with underlying medical illness or psychiatric disorders may be more prone to the CNS manifestations of anticholinergic medications. Anticholinergic effects can occur through ingestion, smoking, inhalation, and topical absorption (including transdermal or ophthalmic routes). Delayed or prolonged effects may occur due to slow gastric emptying and prolonged GI absorption. The duration of effects is variable and central anticholinergic manifestations of confusion or agitation may be present for several days, even after peripheral manifestations have resolved (termed the central anticholinergic syndrome).
What are common causes of anticholinergic toxicity?
Although anticholinergic effects are often described in terms of “toxicity,” these effects are often used for therapeutic benefit. Such roles of anticholinergic agents include the following:
- Atropine to treat bradycardia;
- Ipratropium bromide to manage asthma;
- Antinauseants (eg, scopolamine, meclizine) for symptom relief;
- Tolterodine to treat urge incontinence and overactive bladder; and
- Ophthalmologic medications (eg, scopolamine, homatropine) to inhibit ciliary spasm in patients with iritis.
Although the above medications are being used for a specific anticholinergic property, other unintended and troublesome anticholinergic effects are often seen. Similarly, many other medications often have unintended anticholinergic effects (see Table). Anticholinergic “toxicity” is simply an extension of the effects that occur with therapeutic use.
What is the treatment for patients with anticholinergic toxicity?
Most patients with anticholinergic toxicity do well with supportive management. Benzodiazepines are the treatment of choice for agitation. Haloperidol and other antipsychotics are relatively contraindicated for treatment of agitation as they may impair temperature regulation and lead to hyperthermia. Although likely of limited overall benefit, oral activated charcoal may reduce the amount of drug absorbed.
Antidotal therapy with physostigmine should be considered for select patients presenting with altered mental status due to an anticholinergic. Physostigmine is an acetylcholinesterase inhibitor that prevents the breakdown of acetylcholine in the synaptic cleft, thus antagonizing the effects of anticholinergic drugs. A retrospective study noted a lower incidence of complications and shorter time to recovery with the use of physostigmine compared with benzodiazepines in patients with anticholinergic toxicity.2 The use of physostigmine in select patients may obviate the need for a further delirium workup, which often includes computed tomography or lumbar puncture.
When administering physostigmine, atropine should be present at the bedside with airway equipment readily available as cholinergic effects may develop (specifically bronchospasm, bronchorrhea, or bradycardia). Dosing of physostigmine in adult patients is 1 to 2 mg via slow intravenous (IV) push, in aliquots of 0.2 to 0.3 mg each, over 5 minutes; pediatric dosing is 20 mcg/kg to maximum 0.5 mg. Onset of effects can be expected within minutes of administration.3 Since the duration of physostigmine is less than that of many anticholinergic drugs, recurrence of anticholinergic effects should be anticipated.
Historically, physostigmine was included in the “coma cocktail,” along with thiamine, dextrose, and naloxone for treating undifferentiated patients with altered level of consciousness. Concern for its ubiquitous use arose following reports of asystole in two patients who presented with tricyclic antidepressant (TCA) overdose, although these patients actually had more complicated multidrug overdoses.4 Nevertheless, an ECG should be performed in all patients for whom physostigmine is being considered, and it should not be administered (or perhaps only extremely cautiously) if the ECG demonstrates a QRS complex duration >100 ms.3 Relative contraindications include reactive airways disease, peripheral vascular disease, or intestinal or bladder-outlet obstruction.
Prolongation of the QRS interval is not always indicative of TCA ingestion as certain other antimuscarinic drugs, such as diphenhydramine, may cause sodium-channel blockade. Based on extrapolation from TCA literature,5 if the QRS >100 ms, a bolus of 1 to 2 mEq/kg sodium bicarbonate should be given with monitoring of the QRS interval for narrowing.
Case conclusion
The clinicians at the bedside felt that the infant’s presentation was consistent with anticholinergic toxicity. Physostigmine was administered by slow IV push for a total dose of 1.5 mg. The patient had immediate improvement of symptoms, including decreased skin redness, decreased agitation, and improved vital signs (BP, 118/80 mm Hg and HR, 160 beats/minute). He was admitted to the pediatric intensive care unit for monitoring and was subsequently discharged home with complete symptom resolution 2 days later.
A previously healthy 11-month-old boy was brought to the ED after his parents discovered him with an open bottle of nonprescription diphenhydramine. On initial presentation, the child was irritable with diffuse skin redness and dry mucous membranes. He was tremulous and making nonpurposeful reaching movements with his arms. He had roving eye movements and markedly dilated pupils that were minimally reactive. Initial vital signs were: blood pressure, 140/95 mm Hg; heart rate, 220 beats/minute; respiratory rate, 30 breaths/minute; temperature, 100.6ºF. Capillary glucose was 120 mg/dL, and oxygen saturation was 100% on room air. An electrocardiogram (ECG) revealed sinus tachycardia with normal QRS and QTc intervals.
What is the toxicological differential diagnosis?
Toxicity from several different classes of drugs may cause an altered level of consciousness, tachycardia, and hyperthermia. Serotonin agonists, such as selective serotonin reuptake inhibitors, may result in serotonin toxicity—a syndrome that includes altered cognition, autonomic changes (eg, tachycardia, hyperthermia), and neuromuscular effects (eg, rigidity, clonus), along with mydriasis and diaphoresis. Neuroleptic malignant syndrome (NMS) occurs following exposure to dopamine antagonists, such as antipsychotic medications.
Neuroleptic malignant syndrome presents in a similar manner to serotonin toxicity but tends to have a more indolent course compared with the abrupt onset and resolution of serotonin toxicity. Sympathomimetic medications (eg, methylphenidate) or drugs of abuse (eg, cocaine, methamphetamines) result in catecholamine effects including tachycardia, hypertension, diaphoresis, and mydriasis. Acetylsalicylic-acid (aspirin) toxicity (salicylism) often causes tinnitus, hyperpnea, and gastrointestinal (GI) effects following exposure. Severe toxicity may cause altered level of consciousness and hyperthermia; however, these are ominous and late findings. Mydriasis is not common.
What is the anticholinergic toxidrome?
Acetylcholine is a neurotransmitter present both in the central and peripheral nervous systems. In the periphery, acetylcholine acts at both the sympathetic and parasympathetic components of the autonomic nervous system and at somatic motor fibers. Acetylcholine acts at two classes of receptors, namely, nicotinic and muscarinic types. Muscarinic receptors are found in the central nervous system (CNS) (specifically the brain) and peripherally on effector cells of the parasympathetic nervous system and on sympathetically innervated sweat glands.1 Anticholinergic toxicity results from antagonism of muscarinic receptors and is more appropriately referred to as antimuscarinic poisoning, though the terms are used interchangeably. Nicotinic receptor antagonists are used primarily for neuromuscular blockade and do not cause this syndrome.
- “Hot as a hare” (anhidrosis with temperature elevation);
- “Red as a beet” (vasodilation with skin hyperemia);
- “Blind as a bat” (pupillary dilation with loss of accommodation);
- “Dry as a bone” (drying of mucosal surfaces and skin);
- “Full as a flask” (urinary retention); “Stuffed as a pepper” (constipation); and
- “Mad as a hatter” (describing the central anticholinergic effects that are often present—eg, altered mental status manifested as agitation, delirium, hallucinations, abnormal picking movements, rarely seizures).
Elderly patients and those with underlying medical illness or psychiatric disorders may be more prone to the CNS manifestations of anticholinergic medications. Anticholinergic effects can occur through ingestion, smoking, inhalation, and topical absorption (including transdermal or ophthalmic routes). Delayed or prolonged effects may occur due to slow gastric emptying and prolonged GI absorption. The duration of effects is variable and central anticholinergic manifestations of confusion or agitation may be present for several days, even after peripheral manifestations have resolved (termed the central anticholinergic syndrome).
What are common causes of anticholinergic toxicity?
Although anticholinergic effects are often described in terms of “toxicity,” these effects are often used for therapeutic benefit. Such roles of anticholinergic agents include the following:
- Atropine to treat bradycardia;
- Ipratropium bromide to manage asthma;
- Antinauseants (eg, scopolamine, meclizine) for symptom relief;
- Tolterodine to treat urge incontinence and overactive bladder; and
- Ophthalmologic medications (eg, scopolamine, homatropine) to inhibit ciliary spasm in patients with iritis.
Although the above medications are being used for a specific anticholinergic property, other unintended and troublesome anticholinergic effects are often seen. Similarly, many other medications often have unintended anticholinergic effects (see Table). Anticholinergic “toxicity” is simply an extension of the effects that occur with therapeutic use.
What is the treatment for patients with anticholinergic toxicity?
Most patients with anticholinergic toxicity do well with supportive management. Benzodiazepines are the treatment of choice for agitation. Haloperidol and other antipsychotics are relatively contraindicated for treatment of agitation as they may impair temperature regulation and lead to hyperthermia. Although likely of limited overall benefit, oral activated charcoal may reduce the amount of drug absorbed.
Antidotal therapy with physostigmine should be considered for select patients presenting with altered mental status due to an anticholinergic. Physostigmine is an acetylcholinesterase inhibitor that prevents the breakdown of acetylcholine in the synaptic cleft, thus antagonizing the effects of anticholinergic drugs. A retrospective study noted a lower incidence of complications and shorter time to recovery with the use of physostigmine compared with benzodiazepines in patients with anticholinergic toxicity.2 The use of physostigmine in select patients may obviate the need for a further delirium workup, which often includes computed tomography or lumbar puncture.
When administering physostigmine, atropine should be present at the bedside with airway equipment readily available as cholinergic effects may develop (specifically bronchospasm, bronchorrhea, or bradycardia). Dosing of physostigmine in adult patients is 1 to 2 mg via slow intravenous (IV) push, in aliquots of 0.2 to 0.3 mg each, over 5 minutes; pediatric dosing is 20 mcg/kg to maximum 0.5 mg. Onset of effects can be expected within minutes of administration.3 Since the duration of physostigmine is less than that of many anticholinergic drugs, recurrence of anticholinergic effects should be anticipated.
Historically, physostigmine was included in the “coma cocktail,” along with thiamine, dextrose, and naloxone for treating undifferentiated patients with altered level of consciousness. Concern for its ubiquitous use arose following reports of asystole in two patients who presented with tricyclic antidepressant (TCA) overdose, although these patients actually had more complicated multidrug overdoses.4 Nevertheless, an ECG should be performed in all patients for whom physostigmine is being considered, and it should not be administered (or perhaps only extremely cautiously) if the ECG demonstrates a QRS complex duration >100 ms.3 Relative contraindications include reactive airways disease, peripheral vascular disease, or intestinal or bladder-outlet obstruction.
Prolongation of the QRS interval is not always indicative of TCA ingestion as certain other antimuscarinic drugs, such as diphenhydramine, may cause sodium-channel blockade. Based on extrapolation from TCA literature,5 if the QRS >100 ms, a bolus of 1 to 2 mEq/kg sodium bicarbonate should be given with monitoring of the QRS interval for narrowing.
Case conclusion
The clinicians at the bedside felt that the infant’s presentation was consistent with anticholinergic toxicity. Physostigmine was administered by slow IV push for a total dose of 1.5 mg. The patient had immediate improvement of symptoms, including decreased skin redness, decreased agitation, and improved vital signs (BP, 118/80 mm Hg and HR, 160 beats/minute). He was admitted to the pediatric intensive care unit for monitoring and was subsequently discharged home with complete symptom resolution 2 days later.
- Gerretsen P, Pollock BG. Drugs with anticholinergic properties: a current perspective on use and safety. Expert Opin Drug Saf. 2011;10(5):751-765.
- Burns MJ, Linden CH, Graudins A, Brown RM, Fletcher KE. A comparison of physostigmine and benzodiazepines for the treatment of anticholinergic poisoning. Ann Emerg Med. 2000;35(4):374-381.
- Howland MA. Physostigmine salicylate. In: Nelson LS, Lewin NA, Howland MA, Hoffman RS, Goldfrank LR, Flomenbaum NE, eds. Goldfrank’s Toxicologic Emergencies. 9th ed. New York, NY: McGraw Hill; 2011:759-762.
- Pentel P, Peterson CD. Asystole complicating physostigmine treatment of tricyclic antidepressant overdose. Ann Emerg Med. 1980;9(11):588-590.
- Boehnert MT, Lovejoy FH, Jr. Value of the QRS duration versus the serum drug level in predicting seizures and ventricular arrhythmias after an acute overdose of tricyclic antidepressants. N Engl J Med. 1985;313(8):474-479.
- Gerretsen P, Pollock BG. Drugs with anticholinergic properties: a current perspective on use and safety. Expert Opin Drug Saf. 2011;10(5):751-765.
- Burns MJ, Linden CH, Graudins A, Brown RM, Fletcher KE. A comparison of physostigmine and benzodiazepines for the treatment of anticholinergic poisoning. Ann Emerg Med. 2000;35(4):374-381.
- Howland MA. Physostigmine salicylate. In: Nelson LS, Lewin NA, Howland MA, Hoffman RS, Goldfrank LR, Flomenbaum NE, eds. Goldfrank’s Toxicologic Emergencies. 9th ed. New York, NY: McGraw Hill; 2011:759-762.
- Pentel P, Peterson CD. Asystole complicating physostigmine treatment of tricyclic antidepressant overdose. Ann Emerg Med. 1980;9(11):588-590.
- Boehnert MT, Lovejoy FH, Jr. Value of the QRS duration versus the serum drug level in predicting seizures and ventricular arrhythmias after an acute overdose of tricyclic antidepressants. N Engl J Med. 1985;313(8):474-479.
