User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Delivering Asthma Meds at School Improved Outcomes
Major Finding: The number of symptom-free days increased from an average of 8 days per 2-week period for all children at baseline to 11.9 days with the intervention vs. 11.2 days with usual care.
Data Source: School-Based Asthma Therapy trial in 530 children with asthma.
Disclosures: SBAT was supported by grants from the National Heart, Lung, and Blood Institute and the Halcyon Hill Foundation. Ms. Fagnano and Dr. Halterman disclosed no financial conflicts.
VANCOUVER, B.C. — A school-based intervention that focused on medication adherence and reducing exposure to tobacco smoke significantly improved outcomes among inner-city children with asthma in a randomized trial.
Children receiving the intervention had almost 1 additional symptom-free day per 2-week period during the peak winter asthma season of November to February.
The number of symptom-free days increased from an average of 8 days for all children at baseline to 11.9 days per 2-week period with the intervention vs. 11.2 days with usual care. “This difference is larger than what has been seen with more intensive and costly interventions,” said Maria Fagnano, M.P.H., of the University of Rochester (N.Y.) Medical Center.
The children receiving the intervention were significantly more likely than controls to have fewer nights with symptoms (mean 1.5 nights vs. 2.0 nights), fewer days with limited activity (1.2 vs. 1.6), and fewer days with rescue medication use (1.59 vs. 2.61), Ms. Fagnano reported at the annual meeting of the Pediatric Academic Societies.
The intervention group also was significantly less likely than controls to have any acute visit for asthma (12% vs. 18%). In addition, the intervention group had fewer days absent from school due to asthma (0.3 days vs. 0.4 days).
Although additional efforts are needed to evaluate costs of the intervention and to develop dissemination strategies, collaborations with schools provide a unique opportunity to reach high-risk children and target those at greatest need for assistance, Ms. Fagnano said.
“This type of intervention is widely applicable for asthma care in the community nationwide, as well as for management of other chronic diseases, and could potentially reduce disparities between poor and nonpoor children,” she said.
The School-Based Asthma Therapy (SBAT) trial, led by colleague Dr. Jill Halterman, was implemented in 2006 in 54 schools and preschools in Rochester, N.Y., to reduce morbidity in poor children aged 3–10 years with physician-diagnosed asthma.
The school nurse was given a canister of preventive medication (fluticasone propionate or fluticasone propionate with salmeterol), with a spacer and mask as appropriate, and asked to give one dose to the child each school day. A supply of preventive asthma medications also was delivered to parents, who were instructed to use the medications on days the child did not attend school.
The intervention also used motivational interviewing to counsel the primary caregiver about how to reduce environmental tobacco smoke (ETS) in the home for smoke-exposed children, Ms. Fagnano said. Overall, 54% of children lived with one or more smokers at baseline. A home-based counseling session was delivered by a trained nurse, with two follow-up telephone calls made at 1 and 3 months after the 30-minute session.
In the usual care group, parents and physicians were notified of the child's asthma severity and encouraged to start on appropriate preventive treatments, but no medication was provided, she said.
At baseline, 69% of children were on preventive medications, 73% received Medicaid, 58% were male, 63% were black, and 28% were Hispanic. Their mean age was 7 years. There were 265 children in each arm.
In a regression analysis, the intervention was associated with 0.92 days per 2 weeks more symptom-free days (P less than .001), Ms. Fagnano said.
A stratified analysis showed a significant intervention effect on the primary outcome of symptom-free days for children with and without ETS exposure in the home. The mean number of symptom-free days among non-ETS exposed children was 11.6 days in the treatment group vs. 10.9 days in the control group; and was 11.6 days vs. 10.0 days, respectively, in smoke-exposed children, she said.
An audience member remarked on the improvement observed, even among controls. Ms. Fagnano said that monthly follow-up calls could have “clued parents in to what the child was experiencing,” and that asthma calendars given to these families may have helped them notice more symptoms.
Major Finding: The number of symptom-free days increased from an average of 8 days per 2-week period for all children at baseline to 11.9 days with the intervention vs. 11.2 days with usual care.
Data Source: School-Based Asthma Therapy trial in 530 children with asthma.
Disclosures: SBAT was supported by grants from the National Heart, Lung, and Blood Institute and the Halcyon Hill Foundation. Ms. Fagnano and Dr. Halterman disclosed no financial conflicts.
VANCOUVER, B.C. — A school-based intervention that focused on medication adherence and reducing exposure to tobacco smoke significantly improved outcomes among inner-city children with asthma in a randomized trial.
Children receiving the intervention had almost 1 additional symptom-free day per 2-week period during the peak winter asthma season of November to February.
The number of symptom-free days increased from an average of 8 days for all children at baseline to 11.9 days per 2-week period with the intervention vs. 11.2 days with usual care. “This difference is larger than what has been seen with more intensive and costly interventions,” said Maria Fagnano, M.P.H., of the University of Rochester (N.Y.) Medical Center.
The children receiving the intervention were significantly more likely than controls to have fewer nights with symptoms (mean 1.5 nights vs. 2.0 nights), fewer days with limited activity (1.2 vs. 1.6), and fewer days with rescue medication use (1.59 vs. 2.61), Ms. Fagnano reported at the annual meeting of the Pediatric Academic Societies.
The intervention group also was significantly less likely than controls to have any acute visit for asthma (12% vs. 18%). In addition, the intervention group had fewer days absent from school due to asthma (0.3 days vs. 0.4 days).
Although additional efforts are needed to evaluate costs of the intervention and to develop dissemination strategies, collaborations with schools provide a unique opportunity to reach high-risk children and target those at greatest need for assistance, Ms. Fagnano said.
“This type of intervention is widely applicable for asthma care in the community nationwide, as well as for management of other chronic diseases, and could potentially reduce disparities between poor and nonpoor children,” she said.
The School-Based Asthma Therapy (SBAT) trial, led by colleague Dr. Jill Halterman, was implemented in 2006 in 54 schools and preschools in Rochester, N.Y., to reduce morbidity in poor children aged 3–10 years with physician-diagnosed asthma.
The school nurse was given a canister of preventive medication (fluticasone propionate or fluticasone propionate with salmeterol), with a spacer and mask as appropriate, and asked to give one dose to the child each school day. A supply of preventive asthma medications also was delivered to parents, who were instructed to use the medications on days the child did not attend school.
The intervention also used motivational interviewing to counsel the primary caregiver about how to reduce environmental tobacco smoke (ETS) in the home for smoke-exposed children, Ms. Fagnano said. Overall, 54% of children lived with one or more smokers at baseline. A home-based counseling session was delivered by a trained nurse, with two follow-up telephone calls made at 1 and 3 months after the 30-minute session.
In the usual care group, parents and physicians were notified of the child's asthma severity and encouraged to start on appropriate preventive treatments, but no medication was provided, she said.
At baseline, 69% of children were on preventive medications, 73% received Medicaid, 58% were male, 63% were black, and 28% were Hispanic. Their mean age was 7 years. There were 265 children in each arm.
In a regression analysis, the intervention was associated with 0.92 days per 2 weeks more symptom-free days (P less than .001), Ms. Fagnano said.
A stratified analysis showed a significant intervention effect on the primary outcome of symptom-free days for children with and without ETS exposure in the home. The mean number of symptom-free days among non-ETS exposed children was 11.6 days in the treatment group vs. 10.9 days in the control group; and was 11.6 days vs. 10.0 days, respectively, in smoke-exposed children, she said.
An audience member remarked on the improvement observed, even among controls. Ms. Fagnano said that monthly follow-up calls could have “clued parents in to what the child was experiencing,” and that asthma calendars given to these families may have helped them notice more symptoms.
Major Finding: The number of symptom-free days increased from an average of 8 days per 2-week period for all children at baseline to 11.9 days with the intervention vs. 11.2 days with usual care.
Data Source: School-Based Asthma Therapy trial in 530 children with asthma.
Disclosures: SBAT was supported by grants from the National Heart, Lung, and Blood Institute and the Halcyon Hill Foundation. Ms. Fagnano and Dr. Halterman disclosed no financial conflicts.
VANCOUVER, B.C. — A school-based intervention that focused on medication adherence and reducing exposure to tobacco smoke significantly improved outcomes among inner-city children with asthma in a randomized trial.
Children receiving the intervention had almost 1 additional symptom-free day per 2-week period during the peak winter asthma season of November to February.
The number of symptom-free days increased from an average of 8 days for all children at baseline to 11.9 days per 2-week period with the intervention vs. 11.2 days with usual care. “This difference is larger than what has been seen with more intensive and costly interventions,” said Maria Fagnano, M.P.H., of the University of Rochester (N.Y.) Medical Center.
The children receiving the intervention were significantly more likely than controls to have fewer nights with symptoms (mean 1.5 nights vs. 2.0 nights), fewer days with limited activity (1.2 vs. 1.6), and fewer days with rescue medication use (1.59 vs. 2.61), Ms. Fagnano reported at the annual meeting of the Pediatric Academic Societies.
The intervention group also was significantly less likely than controls to have any acute visit for asthma (12% vs. 18%). In addition, the intervention group had fewer days absent from school due to asthma (0.3 days vs. 0.4 days).
Although additional efforts are needed to evaluate costs of the intervention and to develop dissemination strategies, collaborations with schools provide a unique opportunity to reach high-risk children and target those at greatest need for assistance, Ms. Fagnano said.
“This type of intervention is widely applicable for asthma care in the community nationwide, as well as for management of other chronic diseases, and could potentially reduce disparities between poor and nonpoor children,” she said.
The School-Based Asthma Therapy (SBAT) trial, led by colleague Dr. Jill Halterman, was implemented in 2006 in 54 schools and preschools in Rochester, N.Y., to reduce morbidity in poor children aged 3–10 years with physician-diagnosed asthma.
The school nurse was given a canister of preventive medication (fluticasone propionate or fluticasone propionate with salmeterol), with a spacer and mask as appropriate, and asked to give one dose to the child each school day. A supply of preventive asthma medications also was delivered to parents, who were instructed to use the medications on days the child did not attend school.
The intervention also used motivational interviewing to counsel the primary caregiver about how to reduce environmental tobacco smoke (ETS) in the home for smoke-exposed children, Ms. Fagnano said. Overall, 54% of children lived with one or more smokers at baseline. A home-based counseling session was delivered by a trained nurse, with two follow-up telephone calls made at 1 and 3 months after the 30-minute session.
In the usual care group, parents and physicians were notified of the child's asthma severity and encouraged to start on appropriate preventive treatments, but no medication was provided, she said.
At baseline, 69% of children were on preventive medications, 73% received Medicaid, 58% were male, 63% were black, and 28% were Hispanic. Their mean age was 7 years. There were 265 children in each arm.
In a regression analysis, the intervention was associated with 0.92 days per 2 weeks more symptom-free days (P less than .001), Ms. Fagnano said.
A stratified analysis showed a significant intervention effect on the primary outcome of symptom-free days for children with and without ETS exposure in the home. The mean number of symptom-free days among non-ETS exposed children was 11.6 days in the treatment group vs. 10.9 days in the control group; and was 11.6 days vs. 10.0 days, respectively, in smoke-exposed children, she said.
An audience member remarked on the improvement observed, even among controls. Ms. Fagnano said that monthly follow-up calls could have “clued parents in to what the child was experiencing,” and that asthma calendars given to these families may have helped them notice more symptoms.
COPD Phenotype Tied to More Exacerbations
Major Finding: A COPD patient's frequency of exacerbations remains stable over time, and the subgroup of patients with frequent exacerbations appears to have a particular phenotype of the disease.
Data Source: A secondary analysis of data collected in the multinational, prospective, observational, 3-year ECLIPSE study of 2,138 patients with mild, moderate, or severe COPD.
Disclosures: The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study — the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) — to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40–75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128–38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations in the third year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient's susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
View on the News
What Is the Mechanism?
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype, because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Major Finding: A COPD patient's frequency of exacerbations remains stable over time, and the subgroup of patients with frequent exacerbations appears to have a particular phenotype of the disease.
Data Source: A secondary analysis of data collected in the multinational, prospective, observational, 3-year ECLIPSE study of 2,138 patients with mild, moderate, or severe COPD.
Disclosures: The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study — the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) — to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40–75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128–38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations in the third year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient's susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
View on the News
What Is the Mechanism?
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype, because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Major Finding: A COPD patient's frequency of exacerbations remains stable over time, and the subgroup of patients with frequent exacerbations appears to have a particular phenotype of the disease.
Data Source: A secondary analysis of data collected in the multinational, prospective, observational, 3-year ECLIPSE study of 2,138 patients with mild, moderate, or severe COPD.
Disclosures: The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study — the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) — to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40–75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128–38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations in the third year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient's susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
View on the News
What Is the Mechanism?
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype, because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Endobronchial Valves Improve Emphysema 'Modestly'
Unilateral lobar treatment with endobronchial valves produces modest improvements in lung function, exercise tolerance, and symptoms in patients with advanced, heterogenous, hyperinflated emphysema, according to a report in the Sept. 23 issue of the New England Journal of Medicine.
However, these benefits come with substantial costs in the months following implantation: more frequent exacerbations of chronic obstructive pulmonary disease (COPD), pneumonia distal to the valves in more than 4% of cases, hemoptysis related to oozing from granulation tissue, and pneumothorax, said Dr. Frank C. Sciurba of the University of Pittsburgh and his associates.
They assessed the safety and efficacy of endobronchial valves, compared with standard medical care, in what they described as the first randomized, prospective, multicenter study of the devices, the Endobronchial Valve for Emphysema Palliation Trial (VENT).
The study involved 321 patients (aged 40-75 years) who were randomly assigned to receive either the unidirectional valves (220 subjects), which block regional inflation while allowing exhalation, or standard medical therapy (101 controls).
The valves are designed to reduce the volume (hyperinflation) of the most severely damaged lobe, allowing expansion of the more viable adjacent lobe.
A mean of 3.8 valves was placed in each patient via bronchoscopy. The valves were placed in only one lung (in the lobar, segmental, or subsegmental bronchi, depending on the patient’s anatomy) to completely isolate the targeted lobe. Moderate sedation was used in 71% of patients and general anesthesia in 29%. The mean duration of the procedure was 34 minutes.
The composite efficacy end point was the percent change in FEV1 and distance achieved in the 6-minute walk test at the 6-month follow-up. The primary safety end point was a composite of six major complications arising within 6 months: death, empyema, massive hemoptysis, pneumonia distal to the valves, pneumothorax or air leak of more than 7 days’ duration, or ventilator-dependent respiratory failure of more than 24 hours’ duration.
Quality of life, exercise capacity, dyspnea, and daily oxygen use also were assessed as secondary end points.
At 6 months, FEV1 increased by 4.3% in the valve group and decreased by 2.5% in control group, for a mean between-group difference of 6.8%. Similarly, distance traveled in the 6-minute walk test increased by 2.5% in the valve group and decreased by 3.2% in the control group, for a mean between-group difference of 5.8%, Dr. Sciurba and his colleagues reported (N. Engl. J. Med. 2010;363:1233-44).
Patients who received the valves also showed modest changes in all secondary end points.
However, the 6-month rate of composite complications was 6.1% in the valve group, compared with 1.2% in the control group. This included six deaths in the valve group and none in the control group. At 1 year, the complication rates were 10.3% and 4.6%, respectively.
The most common adverse event related to valve placement was pneumonia distal to the valve, which developed in 4.2% of patients within 1 year of the procedure. Hemoptysis requiring bronchoscopic inspection was significantly more common in the valve group (approximately 12%) than in controls (0%). Similarly, pneumothorax developed more often in the valve group (5.2%) than in controls (2.4%), as did COPD exacerbations requiring hospitalization (7.9% and 1.1%, respectively).
“In 12 months of follow-up, valves were removed in 31 patients for reasons including retrieval of a migrated valve (in 8 patients), the patient’s request for an unspecified reason (in 7), pneumonia management (in 3), COPD exacerbations (in 2), hemoptysis (in 1), and other reasons (in 7),” the researchers said. In addition, further bronchoscopies were required in 23% of the valve group, compared with only 1% of the control group.
After the trial was completed in 2007, an additional eight patients underwent elective removal of the valves because of adverse events, and three others experienced spontaneous expectoration of a valve, the investigators said.
The VENT study was funded by Emphasys Medical (now Pulmonx) and a grant to Dr. Sciurba from the National Institutes of Health. Dr. Sciurba and several associates reported ties to numerous drug and device manufacturers.
It would be premature to recommend the routine use of endobronchial valves in patients with COPD based on the results of this study, which had several limitations, said Dr. Antonio Anzueto.
First, concomitant medical therapy was not standardized in the two study groups, and “in my opinion, the patients with severe or very severe COPD received suboptimal medical therapy,” Dr. Anzueto said. For example, fewer than 60% were taking the recommended bronchodilators at baseline.
Second, patients were given prophylactic antibiotics for 1 week following implantation, but the investigators did not cite any rationale for doing so, and did not describe any preliminary microbiologic data to guide the antibiotic therapy. The antibiotics did nothing to prevent pneumonia, which developed several weeks later.
“I believe that exhaustive microbiologic assessments should have been made in these patients with severe lung disease, because they are at high risk for lung infection by resistant pathogens,” Dr. Anzueto said.
Finally, lung volumes (as measured by body plethysmography) did not change significantly in either group. “Thus, changes in lung function seen in patients with endobronchial valves may not be due to decreased hyperinflation but to other unknown mechanisms,” he noted.
Antonio Anzueto, M.D., is at the University of Texas Health Science Center and the South Texas Veterans Health Care Center, both in San Antonio. He is cochair of the U.S. COPD Coalition and a member of the executive and scientific committee of the Global Initiative for Chronic Obstructive Lung Disease (GOLD), which issues disease management guidelines. He reported serving on boards and speakers bureaus for a number of pharmaceutical companies. His comments here were taken from an editorial (N. Engl. J. Med. 2010;363:1280-1) that accompanied the report by Dr. Sciurba and colleagues.
It would be premature to recommend the routine use of endobronchial valves in patients with COPD based on the results of this study, which had several limitations, said Dr. Antonio Anzueto.
First, concomitant medical therapy was not standardized in the two study groups, and “in my opinion, the patients with severe or very severe COPD received suboptimal medical therapy,” Dr. Anzueto said. For example, fewer than 60% were taking the recommended bronchodilators at baseline.
Second, patients were given prophylactic antibiotics for 1 week following implantation, but the investigators did not cite any rationale for doing so, and did not describe any preliminary microbiologic data to guide the antibiotic therapy. The antibiotics did nothing to prevent pneumonia, which developed several weeks later.
“I believe that exhaustive microbiologic assessments should have been made in these patients with severe lung disease, because they are at high risk for lung infection by resistant pathogens,” Dr. Anzueto said.
Finally, lung volumes (as measured by body plethysmography) did not change significantly in either group. “Thus, changes in lung function seen in patients with endobronchial valves may not be due to decreased hyperinflation but to other unknown mechanisms,” he noted.
Antonio Anzueto, M.D., is at the University of Texas Health Science Center and the South Texas Veterans Health Care Center, both in San Antonio. He is cochair of the U.S. COPD Coalition and a member of the executive and scientific committee of the Global Initiative for Chronic Obstructive Lung Disease (GOLD), which issues disease management guidelines. He reported serving on boards and speakers bureaus for a number of pharmaceutical companies. His comments here were taken from an editorial (N. Engl. J. Med. 2010;363:1280-1) that accompanied the report by Dr. Sciurba and colleagues.
It would be premature to recommend the routine use of endobronchial valves in patients with COPD based on the results of this study, which had several limitations, said Dr. Antonio Anzueto.
First, concomitant medical therapy was not standardized in the two study groups, and “in my opinion, the patients with severe or very severe COPD received suboptimal medical therapy,” Dr. Anzueto said. For example, fewer than 60% were taking the recommended bronchodilators at baseline.
Second, patients were given prophylactic antibiotics for 1 week following implantation, but the investigators did not cite any rationale for doing so, and did not describe any preliminary microbiologic data to guide the antibiotic therapy. The antibiotics did nothing to prevent pneumonia, which developed several weeks later.
“I believe that exhaustive microbiologic assessments should have been made in these patients with severe lung disease, because they are at high risk for lung infection by resistant pathogens,” Dr. Anzueto said.
Finally, lung volumes (as measured by body plethysmography) did not change significantly in either group. “Thus, changes in lung function seen in patients with endobronchial valves may not be due to decreased hyperinflation but to other unknown mechanisms,” he noted.
Antonio Anzueto, M.D., is at the University of Texas Health Science Center and the South Texas Veterans Health Care Center, both in San Antonio. He is cochair of the U.S. COPD Coalition and a member of the executive and scientific committee of the Global Initiative for Chronic Obstructive Lung Disease (GOLD), which issues disease management guidelines. He reported serving on boards and speakers bureaus for a number of pharmaceutical companies. His comments here were taken from an editorial (N. Engl. J. Med. 2010;363:1280-1) that accompanied the report by Dr. Sciurba and colleagues.
Unilateral lobar treatment with endobronchial valves produces modest improvements in lung function, exercise tolerance, and symptoms in patients with advanced, heterogenous, hyperinflated emphysema, according to a report in the Sept. 23 issue of the New England Journal of Medicine.
However, these benefits come with substantial costs in the months following implantation: more frequent exacerbations of chronic obstructive pulmonary disease (COPD), pneumonia distal to the valves in more than 4% of cases, hemoptysis related to oozing from granulation tissue, and pneumothorax, said Dr. Frank C. Sciurba of the University of Pittsburgh and his associates.
They assessed the safety and efficacy of endobronchial valves, compared with standard medical care, in what they described as the first randomized, prospective, multicenter study of the devices, the Endobronchial Valve for Emphysema Palliation Trial (VENT).
The study involved 321 patients (aged 40-75 years) who were randomly assigned to receive either the unidirectional valves (220 subjects), which block regional inflation while allowing exhalation, or standard medical therapy (101 controls).
The valves are designed to reduce the volume (hyperinflation) of the most severely damaged lobe, allowing expansion of the more viable adjacent lobe.
A mean of 3.8 valves was placed in each patient via bronchoscopy. The valves were placed in only one lung (in the lobar, segmental, or subsegmental bronchi, depending on the patient’s anatomy) to completely isolate the targeted lobe. Moderate sedation was used in 71% of patients and general anesthesia in 29%. The mean duration of the procedure was 34 minutes.
The composite efficacy end point was the percent change in FEV1 and distance achieved in the 6-minute walk test at the 6-month follow-up. The primary safety end point was a composite of six major complications arising within 6 months: death, empyema, massive hemoptysis, pneumonia distal to the valves, pneumothorax or air leak of more than 7 days’ duration, or ventilator-dependent respiratory failure of more than 24 hours’ duration.
Quality of life, exercise capacity, dyspnea, and daily oxygen use also were assessed as secondary end points.
At 6 months, FEV1 increased by 4.3% in the valve group and decreased by 2.5% in control group, for a mean between-group difference of 6.8%. Similarly, distance traveled in the 6-minute walk test increased by 2.5% in the valve group and decreased by 3.2% in the control group, for a mean between-group difference of 5.8%, Dr. Sciurba and his colleagues reported (N. Engl. J. Med. 2010;363:1233-44).
Patients who received the valves also showed modest changes in all secondary end points.
However, the 6-month rate of composite complications was 6.1% in the valve group, compared with 1.2% in the control group. This included six deaths in the valve group and none in the control group. At 1 year, the complication rates were 10.3% and 4.6%, respectively.
The most common adverse event related to valve placement was pneumonia distal to the valve, which developed in 4.2% of patients within 1 year of the procedure. Hemoptysis requiring bronchoscopic inspection was significantly more common in the valve group (approximately 12%) than in controls (0%). Similarly, pneumothorax developed more often in the valve group (5.2%) than in controls (2.4%), as did COPD exacerbations requiring hospitalization (7.9% and 1.1%, respectively).
“In 12 months of follow-up, valves were removed in 31 patients for reasons including retrieval of a migrated valve (in 8 patients), the patient’s request for an unspecified reason (in 7), pneumonia management (in 3), COPD exacerbations (in 2), hemoptysis (in 1), and other reasons (in 7),” the researchers said. In addition, further bronchoscopies were required in 23% of the valve group, compared with only 1% of the control group.
After the trial was completed in 2007, an additional eight patients underwent elective removal of the valves because of adverse events, and three others experienced spontaneous expectoration of a valve, the investigators said.
The VENT study was funded by Emphasys Medical (now Pulmonx) and a grant to Dr. Sciurba from the National Institutes of Health. Dr. Sciurba and several associates reported ties to numerous drug and device manufacturers.
Unilateral lobar treatment with endobronchial valves produces modest improvements in lung function, exercise tolerance, and symptoms in patients with advanced, heterogenous, hyperinflated emphysema, according to a report in the Sept. 23 issue of the New England Journal of Medicine.
However, these benefits come with substantial costs in the months following implantation: more frequent exacerbations of chronic obstructive pulmonary disease (COPD), pneumonia distal to the valves in more than 4% of cases, hemoptysis related to oozing from granulation tissue, and pneumothorax, said Dr. Frank C. Sciurba of the University of Pittsburgh and his associates.
They assessed the safety and efficacy of endobronchial valves, compared with standard medical care, in what they described as the first randomized, prospective, multicenter study of the devices, the Endobronchial Valve for Emphysema Palliation Trial (VENT).
The study involved 321 patients (aged 40-75 years) who were randomly assigned to receive either the unidirectional valves (220 subjects), which block regional inflation while allowing exhalation, or standard medical therapy (101 controls).
The valves are designed to reduce the volume (hyperinflation) of the most severely damaged lobe, allowing expansion of the more viable adjacent lobe.
A mean of 3.8 valves was placed in each patient via bronchoscopy. The valves were placed in only one lung (in the lobar, segmental, or subsegmental bronchi, depending on the patient’s anatomy) to completely isolate the targeted lobe. Moderate sedation was used in 71% of patients and general anesthesia in 29%. The mean duration of the procedure was 34 minutes.
The composite efficacy end point was the percent change in FEV1 and distance achieved in the 6-minute walk test at the 6-month follow-up. The primary safety end point was a composite of six major complications arising within 6 months: death, empyema, massive hemoptysis, pneumonia distal to the valves, pneumothorax or air leak of more than 7 days’ duration, or ventilator-dependent respiratory failure of more than 24 hours’ duration.
Quality of life, exercise capacity, dyspnea, and daily oxygen use also were assessed as secondary end points.
At 6 months, FEV1 increased by 4.3% in the valve group and decreased by 2.5% in control group, for a mean between-group difference of 6.8%. Similarly, distance traveled in the 6-minute walk test increased by 2.5% in the valve group and decreased by 3.2% in the control group, for a mean between-group difference of 5.8%, Dr. Sciurba and his colleagues reported (N. Engl. J. Med. 2010;363:1233-44).
Patients who received the valves also showed modest changes in all secondary end points.
However, the 6-month rate of composite complications was 6.1% in the valve group, compared with 1.2% in the control group. This included six deaths in the valve group and none in the control group. At 1 year, the complication rates were 10.3% and 4.6%, respectively.
The most common adverse event related to valve placement was pneumonia distal to the valve, which developed in 4.2% of patients within 1 year of the procedure. Hemoptysis requiring bronchoscopic inspection was significantly more common in the valve group (approximately 12%) than in controls (0%). Similarly, pneumothorax developed more often in the valve group (5.2%) than in controls (2.4%), as did COPD exacerbations requiring hospitalization (7.9% and 1.1%, respectively).
“In 12 months of follow-up, valves were removed in 31 patients for reasons including retrieval of a migrated valve (in 8 patients), the patient’s request for an unspecified reason (in 7), pneumonia management (in 3), COPD exacerbations (in 2), hemoptysis (in 1), and other reasons (in 7),” the researchers said. In addition, further bronchoscopies were required in 23% of the valve group, compared with only 1% of the control group.
After the trial was completed in 2007, an additional eight patients underwent elective removal of the valves because of adverse events, and three others experienced spontaneous expectoration of a valve, the investigators said.
The VENT study was funded by Emphasys Medical (now Pulmonx) and a grant to Dr. Sciurba from the National Institutes of Health. Dr. Sciurba and several associates reported ties to numerous drug and device manufacturers.
Major Finding: At 6 months, FEV1 increased by 4.3% in patients who received endobronchial valves, but decreased by 2.5% in the control subjects; timed walking distance increased by 2.5% in the valve group, but decreased by 3.2% in the control group. However, adverse events including pneumonia, exacerbations of COPD, hemoptysis, and pneumothorax were significantly more common in the valve group.
Data Source: A randomized, prospective, multicenter clinical trial involving 321 patients with advanced, heterogenous emphysema who were followed for 1 year.
Disclosures: The VENT study was funded by Emphasys Medical (now Pulmonx) and an NIH grant to Dr. Sciurba. Dr. Sciurba and several associates reported ties to numerous drug and device manufacturers.
Large Population-Based Study Confirms Increased Risk of VTE With Antipsychotics
Antipsychotic drugs are associated with an almost one-third (32%) greater risk of venous thromboembolism, according to results of a nested case-control study of more than 100,000 primary care patients in the United Kingdom. The study was published online Sept. 21 in the British Medical Journal.
Previous research has suggested that these drugs – also commonly used for nausea, vomiting, and vertigo – might be linked with an increased risk of venous thromboembolism (VTE). However, the results have been inconsistent.
In the current study, the association was even greater for new users of antipsychotics. Those with any antipsychotic use in last 3 months had a 56% increased risk of VTE. Patients who started taking an antipsychotic in the past 3 months had a 97% increased risk. However, the absolute risks were low, with an excess of four extra cases of VTE per 10,000 patients treated over 1 year in patients of all ages and 10 for patients aged 65 years and older.
“Our study adds to the accumulating evidence of adverse health events associated with antipsychotic drugs,” the researchers wrote (BMJ 2010 Sept. 21[doi:10.1136/bmj.c4245]). “If other studies replicate these findings, antipsychotic drugs should be used more cautiously for nausea and agitation, etc., especially among patients at high risk of thromboembolism.”
The researchers used data from the QResearch database, which includes primary care clinical records for more than 11 million people registered in the past 16 years at more than 500 U.K. general practices. The study population was an open cohort of patients aged 16-100 years, who were registered with participating practices between January 1996 and July 2007. Case patients had a first-ever record of VTE – either deep vein thrombosis or pulmonary embolism – during the study period (including postmortem diagnoses).
Incidence density sampling was used to identify up to four control patients for each case patient. Control patients were matched by age, calendar time, sex, and practice. Control patients had no diagnoses of VTE prior to the date of the first recorded diagnosis of VTE in their matched case patient (index date).
Both case and control patients had to have at least 24 months of data before the index date. Control patients were excluded if they had any prescriptions for warfarin prior to the index date. Case patients with any use of warfarin earlier than 6 weeks prior to VTE diagnosis were also excluded, according to Chris Parker, a medical statistician at Hucknall Health Centre in Nottingham, England, and colleagues.
Each patient was classified for exposure to antipsychotics as a current user (one or more prescriptions within 3 months before the index date), a recent user (prescriptions within 4-12 months before the index date), a past user (prescriptions within 13-24 months before the index date), or not exposed within the previous 24 months.
Current users were subclassified as new users (a prescription for antipsychotic within 3 months of the index date, after at least 12 months with no prescription for that antipsychotic) or as continuing users. Exposure during the previous 24 months also was classified according by type (conventional, atypical, or both) and potency (high potency, low potency, or both). High potency was defined as equivalent dose of more than 100 mg chlorpromazine.
Patients with more than one mental health indication were categorized according to a hierarchy: schizophrenia, bipolar disorder without schizophrenia, and dementia without schizophrenia or bipolar disorder.
The analyses were adjusted for socioeconomic status, comorbidities (coronary heart disease, cardiac failure, stroke, cancer, inflammatory bowel disease, liver disease, varicose veins, gastrointestinal bleed, Parkinson’s disease, renal disease, asthma, diabetes, hypertension, hyperlipidemia), drug variables, and the number of complete months of data before the index date.
In addition, data were extracted for 6 months prior to the index date for several events that are associated with increased risk in the short term (hip surgery, hip or lower limb fractures, acute infections, pregnancy). The researchers also looked for whether there was any computer-recorded evidence of a hospital admission in the preceding 31-183 days.
In all, 25,532 eligible case patients – 15,975 with DVT and 9,557 with pulmonary embolism – and 89,491 control patients were included in the study. In terms of mental health disorders, the overall prevalence was 0.4% for schizophrenia, 0.3% for bipolar disorder, and 1.0% for dementia. Eight case patients and 31 control patients had more than one disorder. In all, 8.3% of case patients and 5.3% of control patients had received an antipsychotic in the previous 24 months.
Overall, antipsychotic users had a 32% greater risk of VTE than did nonusers. Among those on antipsychotics, 38% were current users and their increase in risk was 56% compared with 36% for recent users. The risk was not significantly increased for past users. Among current antipsychotic users, 15% had started a new drug within the 3 months prior to the index date. This group of new users showed a greater increase in risk (97%) than did continuing users (29%).
Patients who were prescribed atypical antipsychotic drugs had a greater risk of VTE than did those who were prescribed conventional antipsychotics – 73% compared with 28%. Patients who had received only one prescription in the previous 12 months had a significantly greater risk (32%) than did those receiving none. In addition, those who were prescribed two or more different antipsychotics had a greater risk (99%) than did those who received only one (29%).
The most commonly prescribed drug was prochlorperazine – a high-potency phenothiazine – which also is commonly prescribed for nausea, vomiting, and vertigo. Prochlorperazine was prescribed for 75% of the total number of those on antipsychotics. The other most commonly prescribed drugs were (in order) risperidone, haloperidol, olanzapine, chlorpromazine, trifluoperazine, and quetiapine. Separate odds ratios were estimated for exposure to these drugs, with highest risks for those patients who were prescribed quetiapine, chlorpromazine, and haloperidol, with adjusted odds ratios of 2.81, 1.77, and 2.17, respectively.
Individuals with a diagnosis of dementia were at higher risk than were those with diagnoses of schizophrenia, bipolar disorder, or none of these conditions. There was a more than threefold increase associated with cancer and a roughly 13-fold increase associated with recent surgery or fractures. “Individuals prescribed statins or aspirin in the past 24 months had a lower risk of venous thromboembolism, and those prescribed NSAIDs, oral contraceptives, hormone replacement therapy, tamoxifen, or antimanics had a higher risk,” the authors noted.
The number needed for harm for any antipsychotic use in the past 24 months for patients aged 65 years and older was 1,044; for new users in the past 3 months this number was 344; and for continuing users it was 1,152. The corresponding numbers of excess cases of VTE per 10,000 treated patients were 10, 29, and 9, respectively.
The study authors reported that they have no relevant financial relationships.
The validity of the findings is strengthened by the large sample size and the low potential for exposure and outcome misclassification because of the detailed source of data and adjustment for a large number of confounders, according to Dr. Rosa Liperoti and Dr. Giovanni Gambassi.
It’s been demonstrated that “patients with schizophrenia have an increased risk of venous thromboembolism (VTE), and this might be associated with the use of antipsychotics, especially low-potency drugs such as chlorpromazine and thioridazine. So far, however, the possibility that the underlying psychiatric disorders themselves – and not the antipsychotics – are associated with VTE has never been excluded. This could occur, for example, by the increased concentrations of adrenaline seen during psychotic excitation increasing blood coagulation,” they noted.
In this study, in almost all cases the reason for prescription of antipsychotics could not be ascertained. Most of the antipsychotics used were conventional agents, with prochlorperazine – probably given for nausea and vomiting – accounting for almost 80% of all prescriptions, they wrote. “These findings indicate that VTE is directly linked to the use of an antipsychotic, and that the risk of VTE increases early after starting the drug.”
The implications are potentially far reaching. “Despite their association with serious risks and few data to support their efficacy, antipsychotics are widely used, and in 2008 they became the top selling drug class in the United States. Despite efforts to improve non–drug based interventions, antipsychotics are often used, especially for the treatment of agitation in people with dementia,” they wrote.
The findings suggest that physicians “need to be able to identify the best candidates for antipsychotic treatment, such as those people with the lowest vascular risk profile who may respond to short-term and low-dose treatment with antipsychotics because of individual pharmacogenetic characteristics, and those who may be more susceptible to developing side effects as a result of individual vascular risk factors possibly interacting with antipsychotics.”
Dr. Rosa Liperoti is a specialist in geriatrics and Dr. Giovanni Gambassi is a professor of geriatrics at Universit? Cattolica del Sacro Cuore in Rome. Both Dr. Liperoti and Dr. Gambassi reported that they have no relevant financial relationships. These comments were taken from a commentary that accompanied the study (BMJ 2010 Sept. 21[doi: 10.1136/bmj.c4216]).
The validity of the findings is strengthened by the large sample size and the low potential for exposure and outcome misclassification because of the detailed source of data and adjustment for a large number of confounders, according to Dr. Rosa Liperoti and Dr. Giovanni Gambassi.
It’s been demonstrated that “patients with schizophrenia have an increased risk of venous thromboembolism (VTE), and this might be associated with the use of antipsychotics, especially low-potency drugs such as chlorpromazine and thioridazine. So far, however, the possibility that the underlying psychiatric disorders themselves – and not the antipsychotics – are associated with VTE has never been excluded. This could occur, for example, by the increased concentrations of adrenaline seen during psychotic excitation increasing blood coagulation,” they noted.
In this study, in almost all cases the reason for prescription of antipsychotics could not be ascertained. Most of the antipsychotics used were conventional agents, with prochlorperazine – probably given for nausea and vomiting – accounting for almost 80% of all prescriptions, they wrote. “These findings indicate that VTE is directly linked to the use of an antipsychotic, and that the risk of VTE increases early after starting the drug.”
The implications are potentially far reaching. “Despite their association with serious risks and few data to support their efficacy, antipsychotics are widely used, and in 2008 they became the top selling drug class in the United States. Despite efforts to improve non–drug based interventions, antipsychotics are often used, especially for the treatment of agitation in people with dementia,” they wrote.
The findings suggest that physicians “need to be able to identify the best candidates for antipsychotic treatment, such as those people with the lowest vascular risk profile who may respond to short-term and low-dose treatment with antipsychotics because of individual pharmacogenetic characteristics, and those who may be more susceptible to developing side effects as a result of individual vascular risk factors possibly interacting with antipsychotics.”
Dr. Rosa Liperoti is a specialist in geriatrics and Dr. Giovanni Gambassi is a professor of geriatrics at Universit? Cattolica del Sacro Cuore in Rome. Both Dr. Liperoti and Dr. Gambassi reported that they have no relevant financial relationships. These comments were taken from a commentary that accompanied the study (BMJ 2010 Sept. 21[doi: 10.1136/bmj.c4216]).
The validity of the findings is strengthened by the large sample size and the low potential for exposure and outcome misclassification because of the detailed source of data and adjustment for a large number of confounders, according to Dr. Rosa Liperoti and Dr. Giovanni Gambassi.
It’s been demonstrated that “patients with schizophrenia have an increased risk of venous thromboembolism (VTE), and this might be associated with the use of antipsychotics, especially low-potency drugs such as chlorpromazine and thioridazine. So far, however, the possibility that the underlying psychiatric disorders themselves – and not the antipsychotics – are associated with VTE has never been excluded. This could occur, for example, by the increased concentrations of adrenaline seen during psychotic excitation increasing blood coagulation,” they noted.
In this study, in almost all cases the reason for prescription of antipsychotics could not be ascertained. Most of the antipsychotics used were conventional agents, with prochlorperazine – probably given for nausea and vomiting – accounting for almost 80% of all prescriptions, they wrote. “These findings indicate that VTE is directly linked to the use of an antipsychotic, and that the risk of VTE increases early after starting the drug.”
The implications are potentially far reaching. “Despite their association with serious risks and few data to support their efficacy, antipsychotics are widely used, and in 2008 they became the top selling drug class in the United States. Despite efforts to improve non–drug based interventions, antipsychotics are often used, especially for the treatment of agitation in people with dementia,” they wrote.
The findings suggest that physicians “need to be able to identify the best candidates for antipsychotic treatment, such as those people with the lowest vascular risk profile who may respond to short-term and low-dose treatment with antipsychotics because of individual pharmacogenetic characteristics, and those who may be more susceptible to developing side effects as a result of individual vascular risk factors possibly interacting with antipsychotics.”
Dr. Rosa Liperoti is a specialist in geriatrics and Dr. Giovanni Gambassi is a professor of geriatrics at Universit? Cattolica del Sacro Cuore in Rome. Both Dr. Liperoti and Dr. Gambassi reported that they have no relevant financial relationships. These comments were taken from a commentary that accompanied the study (BMJ 2010 Sept. 21[doi: 10.1136/bmj.c4216]).
Antipsychotic drugs are associated with an almost one-third (32%) greater risk of venous thromboembolism, according to results of a nested case-control study of more than 100,000 primary care patients in the United Kingdom. The study was published online Sept. 21 in the British Medical Journal.
Previous research has suggested that these drugs – also commonly used for nausea, vomiting, and vertigo – might be linked with an increased risk of venous thromboembolism (VTE). However, the results have been inconsistent.
In the current study, the association was even greater for new users of antipsychotics. Those with any antipsychotic use in last 3 months had a 56% increased risk of VTE. Patients who started taking an antipsychotic in the past 3 months had a 97% increased risk. However, the absolute risks were low, with an excess of four extra cases of VTE per 10,000 patients treated over 1 year in patients of all ages and 10 for patients aged 65 years and older.
“Our study adds to the accumulating evidence of adverse health events associated with antipsychotic drugs,” the researchers wrote (BMJ 2010 Sept. 21[doi:10.1136/bmj.c4245]). “If other studies replicate these findings, antipsychotic drugs should be used more cautiously for nausea and agitation, etc., especially among patients at high risk of thromboembolism.”
The researchers used data from the QResearch database, which includes primary care clinical records for more than 11 million people registered in the past 16 years at more than 500 U.K. general practices. The study population was an open cohort of patients aged 16-100 years, who were registered with participating practices between January 1996 and July 2007. Case patients had a first-ever record of VTE – either deep vein thrombosis or pulmonary embolism – during the study period (including postmortem diagnoses).
Incidence density sampling was used to identify up to four control patients for each case patient. Control patients were matched by age, calendar time, sex, and practice. Control patients had no diagnoses of VTE prior to the date of the first recorded diagnosis of VTE in their matched case patient (index date).
Both case and control patients had to have at least 24 months of data before the index date. Control patients were excluded if they had any prescriptions for warfarin prior to the index date. Case patients with any use of warfarin earlier than 6 weeks prior to VTE diagnosis were also excluded, according to Chris Parker, a medical statistician at Hucknall Health Centre in Nottingham, England, and colleagues.
Each patient was classified for exposure to antipsychotics as a current user (one or more prescriptions within 3 months before the index date), a recent user (prescriptions within 4-12 months before the index date), a past user (prescriptions within 13-24 months before the index date), or not exposed within the previous 24 months.
Current users were subclassified as new users (a prescription for antipsychotic within 3 months of the index date, after at least 12 months with no prescription for that antipsychotic) or as continuing users. Exposure during the previous 24 months also was classified according by type (conventional, atypical, or both) and potency (high potency, low potency, or both). High potency was defined as equivalent dose of more than 100 mg chlorpromazine.
Patients with more than one mental health indication were categorized according to a hierarchy: schizophrenia, bipolar disorder without schizophrenia, and dementia without schizophrenia or bipolar disorder.
The analyses were adjusted for socioeconomic status, comorbidities (coronary heart disease, cardiac failure, stroke, cancer, inflammatory bowel disease, liver disease, varicose veins, gastrointestinal bleed, Parkinson’s disease, renal disease, asthma, diabetes, hypertension, hyperlipidemia), drug variables, and the number of complete months of data before the index date.
In addition, data were extracted for 6 months prior to the index date for several events that are associated with increased risk in the short term (hip surgery, hip or lower limb fractures, acute infections, pregnancy). The researchers also looked for whether there was any computer-recorded evidence of a hospital admission in the preceding 31-183 days.
In all, 25,532 eligible case patients – 15,975 with DVT and 9,557 with pulmonary embolism – and 89,491 control patients were included in the study. In terms of mental health disorders, the overall prevalence was 0.4% for schizophrenia, 0.3% for bipolar disorder, and 1.0% for dementia. Eight case patients and 31 control patients had more than one disorder. In all, 8.3% of case patients and 5.3% of control patients had received an antipsychotic in the previous 24 months.
Overall, antipsychotic users had a 32% greater risk of VTE than did nonusers. Among those on antipsychotics, 38% were current users and their increase in risk was 56% compared with 36% for recent users. The risk was not significantly increased for past users. Among current antipsychotic users, 15% had started a new drug within the 3 months prior to the index date. This group of new users showed a greater increase in risk (97%) than did continuing users (29%).
Patients who were prescribed atypical antipsychotic drugs had a greater risk of VTE than did those who were prescribed conventional antipsychotics – 73% compared with 28%. Patients who had received only one prescription in the previous 12 months had a significantly greater risk (32%) than did those receiving none. In addition, those who were prescribed two or more different antipsychotics had a greater risk (99%) than did those who received only one (29%).
The most commonly prescribed drug was prochlorperazine – a high-potency phenothiazine – which also is commonly prescribed for nausea, vomiting, and vertigo. Prochlorperazine was prescribed for 75% of the total number of those on antipsychotics. The other most commonly prescribed drugs were (in order) risperidone, haloperidol, olanzapine, chlorpromazine, trifluoperazine, and quetiapine. Separate odds ratios were estimated for exposure to these drugs, with highest risks for those patients who were prescribed quetiapine, chlorpromazine, and haloperidol, with adjusted odds ratios of 2.81, 1.77, and 2.17, respectively.
Individuals with a diagnosis of dementia were at higher risk than were those with diagnoses of schizophrenia, bipolar disorder, or none of these conditions. There was a more than threefold increase associated with cancer and a roughly 13-fold increase associated with recent surgery or fractures. “Individuals prescribed statins or aspirin in the past 24 months had a lower risk of venous thromboembolism, and those prescribed NSAIDs, oral contraceptives, hormone replacement therapy, tamoxifen, or antimanics had a higher risk,” the authors noted.
The number needed for harm for any antipsychotic use in the past 24 months for patients aged 65 years and older was 1,044; for new users in the past 3 months this number was 344; and for continuing users it was 1,152. The corresponding numbers of excess cases of VTE per 10,000 treated patients were 10, 29, and 9, respectively.
The study authors reported that they have no relevant financial relationships.
Antipsychotic drugs are associated with an almost one-third (32%) greater risk of venous thromboembolism, according to results of a nested case-control study of more than 100,000 primary care patients in the United Kingdom. The study was published online Sept. 21 in the British Medical Journal.
Previous research has suggested that these drugs – also commonly used for nausea, vomiting, and vertigo – might be linked with an increased risk of venous thromboembolism (VTE). However, the results have been inconsistent.
In the current study, the association was even greater for new users of antipsychotics. Those with any antipsychotic use in last 3 months had a 56% increased risk of VTE. Patients who started taking an antipsychotic in the past 3 months had a 97% increased risk. However, the absolute risks were low, with an excess of four extra cases of VTE per 10,000 patients treated over 1 year in patients of all ages and 10 for patients aged 65 years and older.
“Our study adds to the accumulating evidence of adverse health events associated with antipsychotic drugs,” the researchers wrote (BMJ 2010 Sept. 21[doi:10.1136/bmj.c4245]). “If other studies replicate these findings, antipsychotic drugs should be used more cautiously for nausea and agitation, etc., especially among patients at high risk of thromboembolism.”
The researchers used data from the QResearch database, which includes primary care clinical records for more than 11 million people registered in the past 16 years at more than 500 U.K. general practices. The study population was an open cohort of patients aged 16-100 years, who were registered with participating practices between January 1996 and July 2007. Case patients had a first-ever record of VTE – either deep vein thrombosis or pulmonary embolism – during the study period (including postmortem diagnoses).
Incidence density sampling was used to identify up to four control patients for each case patient. Control patients were matched by age, calendar time, sex, and practice. Control patients had no diagnoses of VTE prior to the date of the first recorded diagnosis of VTE in their matched case patient (index date).
Both case and control patients had to have at least 24 months of data before the index date. Control patients were excluded if they had any prescriptions for warfarin prior to the index date. Case patients with any use of warfarin earlier than 6 weeks prior to VTE diagnosis were also excluded, according to Chris Parker, a medical statistician at Hucknall Health Centre in Nottingham, England, and colleagues.
Each patient was classified for exposure to antipsychotics as a current user (one or more prescriptions within 3 months before the index date), a recent user (prescriptions within 4-12 months before the index date), a past user (prescriptions within 13-24 months before the index date), or not exposed within the previous 24 months.
Current users were subclassified as new users (a prescription for antipsychotic within 3 months of the index date, after at least 12 months with no prescription for that antipsychotic) or as continuing users. Exposure during the previous 24 months also was classified according by type (conventional, atypical, or both) and potency (high potency, low potency, or both). High potency was defined as equivalent dose of more than 100 mg chlorpromazine.
Patients with more than one mental health indication were categorized according to a hierarchy: schizophrenia, bipolar disorder without schizophrenia, and dementia without schizophrenia or bipolar disorder.
The analyses were adjusted for socioeconomic status, comorbidities (coronary heart disease, cardiac failure, stroke, cancer, inflammatory bowel disease, liver disease, varicose veins, gastrointestinal bleed, Parkinson’s disease, renal disease, asthma, diabetes, hypertension, hyperlipidemia), drug variables, and the number of complete months of data before the index date.
In addition, data were extracted for 6 months prior to the index date for several events that are associated with increased risk in the short term (hip surgery, hip or lower limb fractures, acute infections, pregnancy). The researchers also looked for whether there was any computer-recorded evidence of a hospital admission in the preceding 31-183 days.
In all, 25,532 eligible case patients – 15,975 with DVT and 9,557 with pulmonary embolism – and 89,491 control patients were included in the study. In terms of mental health disorders, the overall prevalence was 0.4% for schizophrenia, 0.3% for bipolar disorder, and 1.0% for dementia. Eight case patients and 31 control patients had more than one disorder. In all, 8.3% of case patients and 5.3% of control patients had received an antipsychotic in the previous 24 months.
Overall, antipsychotic users had a 32% greater risk of VTE than did nonusers. Among those on antipsychotics, 38% were current users and their increase in risk was 56% compared with 36% for recent users. The risk was not significantly increased for past users. Among current antipsychotic users, 15% had started a new drug within the 3 months prior to the index date. This group of new users showed a greater increase in risk (97%) than did continuing users (29%).
Patients who were prescribed atypical antipsychotic drugs had a greater risk of VTE than did those who were prescribed conventional antipsychotics – 73% compared with 28%. Patients who had received only one prescription in the previous 12 months had a significantly greater risk (32%) than did those receiving none. In addition, those who were prescribed two or more different antipsychotics had a greater risk (99%) than did those who received only one (29%).
The most commonly prescribed drug was prochlorperazine – a high-potency phenothiazine – which also is commonly prescribed for nausea, vomiting, and vertigo. Prochlorperazine was prescribed for 75% of the total number of those on antipsychotics. The other most commonly prescribed drugs were (in order) risperidone, haloperidol, olanzapine, chlorpromazine, trifluoperazine, and quetiapine. Separate odds ratios were estimated for exposure to these drugs, with highest risks for those patients who were prescribed quetiapine, chlorpromazine, and haloperidol, with adjusted odds ratios of 2.81, 1.77, and 2.17, respectively.
Individuals with a diagnosis of dementia were at higher risk than were those with diagnoses of schizophrenia, bipolar disorder, or none of these conditions. There was a more than threefold increase associated with cancer and a roughly 13-fold increase associated with recent surgery or fractures. “Individuals prescribed statins or aspirin in the past 24 months had a lower risk of venous thromboembolism, and those prescribed NSAIDs, oral contraceptives, hormone replacement therapy, tamoxifen, or antimanics had a higher risk,” the authors noted.
The number needed for harm for any antipsychotic use in the past 24 months for patients aged 65 years and older was 1,044; for new users in the past 3 months this number was 344; and for continuing users it was 1,152. The corresponding numbers of excess cases of VTE per 10,000 treated patients were 10, 29, and 9, respectively.
The study authors reported that they have no relevant financial relationships.
FROM THE BRITISH MEDICAL JOURNAL
Major Finding: Patients taking antipsychotics had a 32% greater risk of venous thromboembolism, compared with those not on the drugs.
Data Source: A nested case-control study of 115,023 primary care patients in the United Kingdom.
Disclosures: The authors reported that they have no relevant financial relationships.
Timing, Type of anti-TNFa Therapy Linked to L. Pneumophila
BOSTON – The risk of Legionnaires’ disease associated with tumor necrosis factor-alpha antagonist therapy is greatest during the first year of treatment and is significantly higher for patients receiving adalimumab or infliximab, compared with etanercept, according to a study reported Sept. 15 at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
Using data from the prospective French RATIO (Research Axed on Tolerance of Biotherapies) registry, which was designed to collect information on opportunistic and severe bacterial infections and lymphoma in patients treated with anti–tumor necrosis factor–alpha (anti-TNF-alpha) agents, Dr. Fanny Lanternier of the Necker Hospital for Sick Children in Paris and colleagues conducted an incidence and risk factor study to investigate the relationship between the three drugs included in the registry – adalimumab, infliximab, and etanercept – and Legionella pneumophila infection, which they previously reported in patients receiving anti-TNF–alpha treatment. The researchers used the French population as the reference for the incidence analysis and they conducted a case control study – with four anti-TNF-alpha–treated controls per case – to investigate the risk of newly diagnosed cases of L. pneumophila infection. The mean patient age was 53 years.
From Feb. 1, 2004, to Jan.1, 2007, the RATIO registry received reports of 27 cases of laboratory-confirmed L. pneumophila infection. “The overall annual incidence rate of infection for patients on anti-TNF–alpha therapy, adjusted for age and sex, was 47/100,000 patients per year, which represents a 13-fold increased risk, compared with the reference population,” Dr. Lanternier reported. When evaluated by agent, the standardized incidence risk was significantly higher, at 22.3, for patients taking infliximab or adalimumab – both anti-TNF-alpha monoclonal antibody agents – compared with 3.0 for patients taking etanercept, which is a soluble TNF-alpha receptor therapy, she said at the meeting, sponsored by the American Society for Microbiology.
Similarly, in the case-control analysis, exposure to adalimumab or infliximab vs. etanercept was an independent risk factor for L. pneumophila infection, as was the first year of anti-TNF-alpha treatment, Dr. Lanternier said.
Compared with patients with L. pneumophila infection in the French population, anti-TNF-alpha–treated patients with the infection were younger and had a markedly lower infection-related mortality rate at 3.7% vs. the 10%-20% observed in the population not treated with anti-TNF-alpha drugs, said Dr. Lanternier, attributing the difference to the probability that the immunosuppressed patients are more closely monitored.
In a separate study also presented today, Dr. Alfred F. Sorbello, medical officer for the Food and Drug Administration reported an association between L. pneumophila infection-related mortality and onset of the infection within 90 days of initiating anti-TNF-alpha therapy in patients of younger mean age receiving concomitant steroids or methotrexate. This finding was based on a review of post-marketing adverse event reports for 21 of 80 patients from the FDA Adverse Event Reporting System between 1999 and 2010. Although the results are limited by the small number of patients included in the analysis because of missing data, lack of randomization, and underreporting, they do suggest a key role for TNF-alpha in host defense against L. pneumophila, and they point to the need for clinical vigilance with appropriate diagnostic testing and treatment in these patients, he stressed.
Dr. Lanternier disclosed no conflicts of interests. One of her co-investigators, Dr. Dominique Salmon, disclosed research relationships with Schering, Wyeth, and Abbott. Dr. Sorbello had no financial conflicts. The investigators did not give information on who funded the study.
BOSTON – The risk of Legionnaires’ disease associated with tumor necrosis factor-alpha antagonist therapy is greatest during the first year of treatment and is significantly higher for patients receiving adalimumab or infliximab, compared with etanercept, according to a study reported Sept. 15 at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
Using data from the prospective French RATIO (Research Axed on Tolerance of Biotherapies) registry, which was designed to collect information on opportunistic and severe bacterial infections and lymphoma in patients treated with anti–tumor necrosis factor–alpha (anti-TNF-alpha) agents, Dr. Fanny Lanternier of the Necker Hospital for Sick Children in Paris and colleagues conducted an incidence and risk factor study to investigate the relationship between the three drugs included in the registry – adalimumab, infliximab, and etanercept – and Legionella pneumophila infection, which they previously reported in patients receiving anti-TNF–alpha treatment. The researchers used the French population as the reference for the incidence analysis and they conducted a case control study – with four anti-TNF-alpha–treated controls per case – to investigate the risk of newly diagnosed cases of L. pneumophila infection. The mean patient age was 53 years.
From Feb. 1, 2004, to Jan.1, 2007, the RATIO registry received reports of 27 cases of laboratory-confirmed L. pneumophila infection. “The overall annual incidence rate of infection for patients on anti-TNF–alpha therapy, adjusted for age and sex, was 47/100,000 patients per year, which represents a 13-fold increased risk, compared with the reference population,” Dr. Lanternier reported. When evaluated by agent, the standardized incidence risk was significantly higher, at 22.3, for patients taking infliximab or adalimumab – both anti-TNF-alpha monoclonal antibody agents – compared with 3.0 for patients taking etanercept, which is a soluble TNF-alpha receptor therapy, she said at the meeting, sponsored by the American Society for Microbiology.
Similarly, in the case-control analysis, exposure to adalimumab or infliximab vs. etanercept was an independent risk factor for L. pneumophila infection, as was the first year of anti-TNF-alpha treatment, Dr. Lanternier said.
Compared with patients with L. pneumophila infection in the French population, anti-TNF-alpha–treated patients with the infection were younger and had a markedly lower infection-related mortality rate at 3.7% vs. the 10%-20% observed in the population not treated with anti-TNF-alpha drugs, said Dr. Lanternier, attributing the difference to the probability that the immunosuppressed patients are more closely monitored.
In a separate study also presented today, Dr. Alfred F. Sorbello, medical officer for the Food and Drug Administration reported an association between L. pneumophila infection-related mortality and onset of the infection within 90 days of initiating anti-TNF-alpha therapy in patients of younger mean age receiving concomitant steroids or methotrexate. This finding was based on a review of post-marketing adverse event reports for 21 of 80 patients from the FDA Adverse Event Reporting System between 1999 and 2010. Although the results are limited by the small number of patients included in the analysis because of missing data, lack of randomization, and underreporting, they do suggest a key role for TNF-alpha in host defense against L. pneumophila, and they point to the need for clinical vigilance with appropriate diagnostic testing and treatment in these patients, he stressed.
Dr. Lanternier disclosed no conflicts of interests. One of her co-investigators, Dr. Dominique Salmon, disclosed research relationships with Schering, Wyeth, and Abbott. Dr. Sorbello had no financial conflicts. The investigators did not give information on who funded the study.
BOSTON – The risk of Legionnaires’ disease associated with tumor necrosis factor-alpha antagonist therapy is greatest during the first year of treatment and is significantly higher for patients receiving adalimumab or infliximab, compared with etanercept, according to a study reported Sept. 15 at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
Using data from the prospective French RATIO (Research Axed on Tolerance of Biotherapies) registry, which was designed to collect information on opportunistic and severe bacterial infections and lymphoma in patients treated with anti–tumor necrosis factor–alpha (anti-TNF-alpha) agents, Dr. Fanny Lanternier of the Necker Hospital for Sick Children in Paris and colleagues conducted an incidence and risk factor study to investigate the relationship between the three drugs included in the registry – adalimumab, infliximab, and etanercept – and Legionella pneumophila infection, which they previously reported in patients receiving anti-TNF–alpha treatment. The researchers used the French population as the reference for the incidence analysis and they conducted a case control study – with four anti-TNF-alpha–treated controls per case – to investigate the risk of newly diagnosed cases of L. pneumophila infection. The mean patient age was 53 years.
From Feb. 1, 2004, to Jan.1, 2007, the RATIO registry received reports of 27 cases of laboratory-confirmed L. pneumophila infection. “The overall annual incidence rate of infection for patients on anti-TNF–alpha therapy, adjusted for age and sex, was 47/100,000 patients per year, which represents a 13-fold increased risk, compared with the reference population,” Dr. Lanternier reported. When evaluated by agent, the standardized incidence risk was significantly higher, at 22.3, for patients taking infliximab or adalimumab – both anti-TNF-alpha monoclonal antibody agents – compared with 3.0 for patients taking etanercept, which is a soluble TNF-alpha receptor therapy, she said at the meeting, sponsored by the American Society for Microbiology.
Similarly, in the case-control analysis, exposure to adalimumab or infliximab vs. etanercept was an independent risk factor for L. pneumophila infection, as was the first year of anti-TNF-alpha treatment, Dr. Lanternier said.
Compared with patients with L. pneumophila infection in the French population, anti-TNF-alpha–treated patients with the infection were younger and had a markedly lower infection-related mortality rate at 3.7% vs. the 10%-20% observed in the population not treated with anti-TNF-alpha drugs, said Dr. Lanternier, attributing the difference to the probability that the immunosuppressed patients are more closely monitored.
In a separate study also presented today, Dr. Alfred F. Sorbello, medical officer for the Food and Drug Administration reported an association between L. pneumophila infection-related mortality and onset of the infection within 90 days of initiating anti-TNF-alpha therapy in patients of younger mean age receiving concomitant steroids or methotrexate. This finding was based on a review of post-marketing adverse event reports for 21 of 80 patients from the FDA Adverse Event Reporting System between 1999 and 2010. Although the results are limited by the small number of patients included in the analysis because of missing data, lack of randomization, and underreporting, they do suggest a key role for TNF-alpha in host defense against L. pneumophila, and they point to the need for clinical vigilance with appropriate diagnostic testing and treatment in these patients, he stressed.
Dr. Lanternier disclosed no conflicts of interests. One of her co-investigators, Dr. Dominique Salmon, disclosed research relationships with Schering, Wyeth, and Abbott. Dr. Sorbello had no financial conflicts. The investigators did not give information on who funded the study.
Major Finding: Treatment with some anti–tumor necrosis factor agents increase the risk of L. pneumophila infection as much as 22-fold.
Data Source: Incidence and risk analysis of data from a prospective French database on L. pneumophila associated with tumor necrosis factor–alpha antagonists; Analysis of post-marketing adverse events from FDA Adverse Event Reporting System.
Disclosures: Dr. Lanternier disclosed no conflicts of interests. Co-investigators Dr. Dominique Salmon disclosed research relationships with Schering, Wyeth, and Abbott. Dr. Sorbello disclosed no financial conflicts.
COPD With Frequent Exacerbations May Constitute a Distinct Phenotype
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis reported in the Sept. 16 issue of the New England Journal of Medicine.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study – the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) – to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40-75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128-38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations during the third study year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient’s susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
A full 22% of the patients with moderate COPD were found to have frequent exacerbations, which is “an important observation, considering that such patients, who have relatively mild disease according to FEV1 criteria, may not at present be identified for interventions to reduce exacerbations,” they noted.
Conversely, 29% of the subjects who had very severe COPD appeared to have some resistance to exacerbations, since they experienced none or very few exacerbations during the study.
The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Dr. Tashkin is at the University of California, Los Angeles. These comments were taken from his editorial accompanying Dr. Hurst’s report (N. Engl. J. Med. 2010;363:1183-4).
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Dr. Tashkin is at the University of California, Los Angeles. These comments were taken from his editorial accompanying Dr. Hurst’s report (N. Engl. J. Med. 2010;363:1183-4).
The finding of a distinct phenotype of chronic obstructive pulmonary disease implies that some underlying genetic, biologic, or behavioral mechanism determines either susceptibility or resistance to recurrent exacerbations, independent of disease severity, according to Dr. Donald P. Tashkin.
“Such a mechanism could include greater or lesser susceptibility to respiratory tract infection (the principal trigger of exacerbations); microaspiration from gastroesophageal reflux; psychological factors such as perception of dyspnea (the major symptom of exacerbation); and medication adherence.
“Understanding the mechanistic basis for frequent exacerbations might lead to more effective preventive therapy,” he wrote.
It is important for clinicians to identify which patients fit the phenotype because effective therapies are already available to curb the frequency of exacerbations.
In addition, “a better understanding of the underlying mechanisms that predispose a patient to exacerbations could lead to the development of more targeted preventive strategies,” which in turn would favorably affect the overall course of COPD, he added.
Dr. Tashkin is at the University of California, Los Angeles. These comments were taken from his editorial accompanying Dr. Hurst’s report (N. Engl. J. Med. 2010;363:1183-4).
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis reported in the Sept. 16 issue of the New England Journal of Medicine.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study – the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) – to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40-75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128-38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations during the third study year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient’s susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
A full 22% of the patients with moderate COPD were found to have frequent exacerbations, which is “an important observation, considering that such patients, who have relatively mild disease according to FEV1 criteria, may not at present be identified for interventions to reduce exacerbations,” they noted.
Conversely, 29% of the subjects who had very severe COPD appeared to have some resistance to exacerbations, since they experienced none or very few exacerbations during the study.
The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
It appears that chronic obstructive pulmonary disease with frequent exacerbations constitutes a distinct phenotype of the disease that can occur at mild, moderate, or severe levels of illness, according to results from a data analysis reported in the Sept. 16 issue of the New England Journal of Medicine.
The frequency of COPD exacerbations appears to be relatively stable over time, and a distinct subgroup of patients appears to be prone to frequent (two or more times per year) exacerbations year after year, said Dr. John R. Hurst of University College London Medical School and his associates.
“Despite the importance of exacerbations, we know relatively little about their incidence, their determinants, and their effects in patients with COPD at various levels of severity,” the investigators noted. They used data from a large observational study – the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) – to examine exacerbation frequency.
The international ECLIPSE study included 2,138 patients aged 40-75 years with a history of 10 or more pack-years of smoking, a forced expiratory volume in 1 second (FEV1) of less than 80% of predicted value, and an FEV1-to-forced vital capacity ratio of 0.7 or less after use of a bronchodilator. The subjects had a wide range of COPD severity, and were evaluated at baseline, 3 months, and 6 months, and at 6-month intervals thereafter for 3 years.
Although exacerbations tended to increase with increasing disease severity, patients also tended to fall into and remain in one of two groups: those with infrequent exacerbations (0 or 1 per year) or those with more frequent exacerbations.
For example, 1,187 patients had infrequent exacerbations in the first year of the study, and 987 (83%) of them also had infrequent exacerbations in the second year. Another 492 patients had frequent exacerbations in year 1, and 296 of them (60%) had frequent exacerbations in year 2 as well. “Thus, exacerbation frequency in the first year had a sensitivity of 60% and a specificity of 83%” for predicting the frequency in the second year, Dr. Hurst and his colleagues said (N. Engl. J. Med. 2010;363:1128-38).
Similarly, 994 (84%) of the 1,187 patients with infrequent exacerbations also had infrequent exacerbations during the third study year, while 276 (56%) of the 496 with frequent exacerbations also had frequent exacerbations during the third study year.
And 210 (71%) of those with frequent exacerbations during years 1 and 2 went on to have frequent exacerbations in year 3, while 388 (74%) of those who had no exacerbations during years 1 and 2 also had no exacerbations in year 3.
The easiest and most accurate way of predicting a patient’s susceptibility to exacerbations was simply to ask that patient how many exacerbations they had had the preceding year, the researchers said.
A full 22% of the patients with moderate COPD were found to have frequent exacerbations, which is “an important observation, considering that such patients, who have relatively mild disease according to FEV1 criteria, may not at present be identified for interventions to reduce exacerbations,” they noted.
Conversely, 29% of the subjects who had very severe COPD appeared to have some resistance to exacerbations, since they experienced none or very few exacerbations during the study.
The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
From the New England Journal of Medicine
Major Finding: A COPD patient’s frequency of exacerbations remains stable over time, and the subgroup of patients with frequent exacerbations appears to have a particular phenotype of the disease.
Data Source: A secondary analysis of data collected in the multinational, prospective, observational, 3-year ECLIPSE study of 2,138 patients with mild, moderate, or severe COPD.
Disclosures: The ECLIPSE study was funded by GlaxoSmithKline. Dr. Hurst and his associates reported ties to numerous pharmaceutical companies.
Short Sleep Duration in Young Adults Linked to Prevalent, Persistent Psychological Distress
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation – a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night – after they controlled for possible confounders. Sleeping 8-9 hours per night is recommended.
A total of 19,648 Australians (aged 17-24 years) reported their sleep hours for the previous month in a survey of registered drivers. Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine. Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7-8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139-45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12-18 months later. They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline. In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). Risk was most pronounced among those reporting an average 5 hours or fewer of sleep (RR, 3.25), compared with other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted. Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new onset psychological distress by asking about sleep duration. Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use). Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration. Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97-106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%). The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm. The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation. In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
There was no industry support for the study. Dr. Glozier is a member of the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Dr. Ian Hickie, one of the investigators, formerly served as chief executive officer and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects supported by numerous drug industry partners. The other authors reported no relevant disclosures.
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation – a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night – after they controlled for possible confounders. Sleeping 8-9 hours per night is recommended.
A total of 19,648 Australians (aged 17-24 years) reported their sleep hours for the previous month in a survey of registered drivers. Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine. Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7-8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139-45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12-18 months later. They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline. In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). Risk was most pronounced among those reporting an average 5 hours or fewer of sleep (RR, 3.25), compared with other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted. Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new onset psychological distress by asking about sleep duration. Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use). Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration. Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97-106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%). The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm. The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation. In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
There was no industry support for the study. Dr. Glozier is a member of the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Dr. Ian Hickie, one of the investigators, formerly served as chief executive officer and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects supported by numerous drug industry partners. The other authors reported no relevant disclosures.
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation – a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night – after they controlled for possible confounders. Sleeping 8-9 hours per night is recommended.
A total of 19,648 Australians (aged 17-24 years) reported their sleep hours for the previous month in a survey of registered drivers. Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine. Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7-8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139-45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12-18 months later. They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline. In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). Risk was most pronounced among those reporting an average 5 hours or fewer of sleep (RR, 3.25), compared with other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted. Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new onset psychological distress by asking about sleep duration. Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use). Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration. Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97-106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%). The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm. The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation. In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
There was no industry support for the study. Dr. Glozier is a member of the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Dr. Ian Hickie, one of the investigators, formerly served as chief executive officer and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects supported by numerous drug industry partners. The other authors reported no relevant disclosures.
Major Finding: A 14% increased likelihood of high psychological distress was associated with each hour fewer than 8 slept, on average, per night among young adults.
Data Source: Prospective cohort study of responses from 19,648 young adults surveyed at baseline and from 2,937 resurveyed 12-18 months later.
Disclosures: Dr. Nicholas Glozier is a member of the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Coauthor Dr. Ian Hickie formerly served as CEO and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects supported by numerous drug industry partners. The other authors reported no relevant disclosures.
AHA: ‘Smokeless’ Tobacco Products Unsafe, Don’t Help Smokers Quit
Smokeless tobacco products are not safer alternatives to cigarette smoking, do not help smokers quit, and their long-term use can, in fact, increase the risk of fatal heart attack, fatal stroke and cancer, the American Heart Association warned in a scientific statement published online Sept. 13.

The researchers, led by Mariann R. Piano, Ph.D., examined several international studies to compare smokeless tobacco use and its health risks. Metaanalysis data involving male, Swedish smokers from 1976-2002 showed a significant decrease in cigarette smoking that corresponded with an increase in use of smokeless tobacco products, the investigators wrote in the AHA journal, Circulation. Despite the decline in cigarette use, concern is warranted, Dr. Piano, professor of biobehavioral science at the University of Illinois at Chicago, explained: “Smokeless tobacco products are harmful and addictive – that does not translate to a better alternative,” Dr. Piano, said in a written statement released by the AHA.
“Scientists and policy makers need to assess the effect of ‘reduced risk’ messages related to smokeless tobacco use on public perception, especially among smokers who might be trying to quit,” Dr. Piano and her colleagues wrote. Citing “inadequate evidence of smoking cessation efficacy and safety,” the researchers deemed as inappropriate the promotion of smokeless tobacco as a way to reduce smoking-related diseases.
The American Heart Association does recommend nicotine replacement therapy (nicotine gum or a nicotine-releasing patch placed on the skin) as a safer option for cigarette smokers wanting to quit. “Clinical studies have found no increased risk of heart attack or stroke with either type of nicotine replacement therapy,” the AHA statement said in the written statement.
Metaanalysis data in the AHA scientific statement indicated that smokeless tobacco use was associated with an increased risk of heart disease (relative risk 1.12, n=8 studies) (Int J Epidemiol. 2007;36:789–804). Additionally, a subanalysis of INTERHEART (a study of 15,152 cases of first myocardial infarction in 52 countries) showed that tobacco chewers had a significantly increased risk of first myocardial infarction (odds ratio 2.23) compared with those who never used tobacco. Two other metaanalyses indicated that smokeless tobacco use was also associated with an increased risk of fatal stroke (RR 1.42, n=5 studies, and RR 1.40, n=5 studies).
The researchers explained that, like cigarettes, smokeless tobacco (ST) products still contain nicotine of varying concentrations as well as a number of carcinogens that are just as harmful. Cigarettes and oral snuff have similar amounts of nicotine (milligrams per gram of tobacco), while chewing tobacco appears to have “somewhat lower” amounts compared with cigarettes, Dr. Piano and her colleagues wrote. “Even though certain manufacturing techniques are used to reduce the level of these compounds in some products, they remain present in substantial concentrations in ST products, including Swedish snus,” they said.
In a comparison of nicotine concentration between three types of smokeless tobacco products (chewing tobacco, dry snuff, and moist snuff) and cigarettes sold in the United States, all of the smokeless tobacco products had nicotine concentrations that were similar to cigarettes with the highest concentrations (see chart).
Dr. Piano and her colleagues found that unlike the aforementioned Swedish cohorts, there was no reduction in smoking rates among people in the United States using smokeless tobacco. (The sale of smokeless tobacco products such as moist snuff or snus is banned in most of the European Union with the exception of Sweden and Norway.)
In the United States about 8.1 million people are users of smokeless tobacco and its use is more prevalent in men than women, and people between the ages of 18-25 are the most likely to use smokeless tobacco, the researchers wrote. According to the study, educational background and socioeconomic status coincided with who tends to use smokeless tobacco the most. High prevalence was reported among people with a high-school diploma as their highest level of education, as well as people who live in southern states and rural areas. Blue-collar workers and service or labor workers, as well as the unemployed, were among the regular users of smokeless tobacco products. Native Americans have the highest prevalence of use (9%) followed by whites (5.8%), African Americans (1.9%), Hispanics (0.8%), and Asian Americans (0.6%).
It also appears that while U.S. chewing tobacco use has been on the decline since the 1980s, snuff consumption and production is increasing, the researchers said.
Dr. Piano reported that she received a grant from the National Institutes of Health. The researchers reported no relevant conflicts of interest.
Nicotine Concentrations in Smokeless Tobacco Products and Cigarettes Sold in the United States
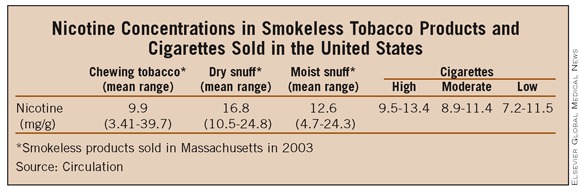
Smokeless Tobacco in the U.S.A.
In a scientific statement published in Circulation, the American Heart Association highlighted other trends related to smokeless tobacco (ST) use in the United States.
As smoke-free air laws become more commonplace in public areas, the AHA said, smokeless tobacco marketers have been promoting their products for use where cigarette smoking is prohibited. The researchers also pointed out a rise in smokeless tobacco use in teenage boys and reported that in 2008 1.4 million people aged 12 and older began using smokeless tobacco, up 47% from 2002 figures. In addition, and of concern, the researchers said, “less than half of the new initiates of ST product use were less than 18 years of age at first use and adolescent males.”
In response to these trends, the Food and Drug Administration issued a final regulation prohibiting the sale of tobacco products —smokeless and otherwise — to anyone under the age of 18. This regulation is a part of the Family Smoking Prevention and Tobacco Control Act. The act has specific requirements about the labeling of smokeless tobacco products and advertisements, which must include at least 1 of these 4 warnings:
WARNING: This product can cause mouth cancer.
WARNING: This product can cause gum disease and tooth loss.
WARNING: This product is not a safe alternative to cigarettes.
WARNING: Smokeless tobacco is addictive.
As of June 22, all tobacco products had to have these labels and follow the guidelines. Smokeless tobacco products had until July 22 to comply with the new laws regarding labeling.
Smokeless tobacco products are not safer alternatives to cigarette smoking, do not help smokers quit, and their long-term use can, in fact, increase the risk of fatal heart attack, fatal stroke and cancer, the American Heart Association warned in a scientific statement published online Sept. 13.
The researchers, led by Mariann R. Piano, Ph.D., examined several international studies to compare smokeless tobacco use and its health risks. Metaanalysis data involving male, Swedish smokers from 1976-2002 showed a significant decrease in cigarette smoking that corresponded with an increase in use of smokeless tobacco products, the investigators wrote in the AHA journal, Circulation. Despite the decline in cigarette use, concern is warranted, Dr. Piano, professor of biobehavioral science at the University of Illinois at Chicago, explained: “Smokeless tobacco products are harmful and addictive – that does not translate to a better alternative,” Dr. Piano, said in a written statement released by the AHA.
“Scientists and policy makers need to assess the effect of ‘reduced risk’ messages related to smokeless tobacco use on public perception, especially among smokers who might be trying to quit,” Dr. Piano and her colleagues wrote. Citing “inadequate evidence of smoking cessation efficacy and safety,” the researchers deemed as inappropriate the promotion of smokeless tobacco as a way to reduce smoking-related diseases.
The American Heart Association does recommend nicotine replacement therapy (nicotine gum or a nicotine-releasing patch placed on the skin) as a safer option for cigarette smokers wanting to quit. “Clinical studies have found no increased risk of heart attack or stroke with either type of nicotine replacement therapy,” the AHA statement said in the written statement.
Metaanalysis data in the AHA scientific statement indicated that smokeless tobacco use was associated with an increased risk of heart disease (relative risk 1.12, n=8 studies) (Int J Epidemiol. 2007;36:789–804). Additionally, a subanalysis of INTERHEART (a study of 15,152 cases of first myocardial infarction in 52 countries) showed that tobacco chewers had a significantly increased risk of first myocardial infarction (odds ratio 2.23) compared with those who never used tobacco. Two other metaanalyses indicated that smokeless tobacco use was also associated with an increased risk of fatal stroke (RR 1.42, n=5 studies, and RR 1.40, n=5 studies).
The researchers explained that, like cigarettes, smokeless tobacco (ST) products still contain nicotine of varying concentrations as well as a number of carcinogens that are just as harmful. Cigarettes and oral snuff have similar amounts of nicotine (milligrams per gram of tobacco), while chewing tobacco appears to have “somewhat lower” amounts compared with cigarettes, Dr. Piano and her colleagues wrote. “Even though certain manufacturing techniques are used to reduce the level of these compounds in some products, they remain present in substantial concentrations in ST products, including Swedish snus,” they said.
In a comparison of nicotine concentration between three types of smokeless tobacco products (chewing tobacco, dry snuff, and moist snuff) and cigarettes sold in the United States, all of the smokeless tobacco products had nicotine concentrations that were similar to cigarettes with the highest concentrations (see chart).
Dr. Piano and her colleagues found that unlike the aforementioned Swedish cohorts, there was no reduction in smoking rates among people in the United States using smokeless tobacco. (The sale of smokeless tobacco products such as moist snuff or snus is banned in most of the European Union with the exception of Sweden and Norway.)
In the United States about 8.1 million people are users of smokeless tobacco and its use is more prevalent in men than women, and people between the ages of 18-25 are the most likely to use smokeless tobacco, the researchers wrote. According to the study, educational background and socioeconomic status coincided with who tends to use smokeless tobacco the most. High prevalence was reported among people with a high-school diploma as their highest level of education, as well as people who live in southern states and rural areas. Blue-collar workers and service or labor workers, as well as the unemployed, were among the regular users of smokeless tobacco products. Native Americans have the highest prevalence of use (9%) followed by whites (5.8%), African Americans (1.9%), Hispanics (0.8%), and Asian Americans (0.6%).
It also appears that while U.S. chewing tobacco use has been on the decline since the 1980s, snuff consumption and production is increasing, the researchers said.
Dr. Piano reported that she received a grant from the National Institutes of Health. The researchers reported no relevant conflicts of interest.
Nicotine Concentrations in Smokeless Tobacco Products and Cigarettes Sold in the United States
Smokeless Tobacco in the U.S.A.
In a scientific statement published in Circulation, the American Heart Association highlighted other trends related to smokeless tobacco (ST) use in the United States.
As smoke-free air laws become more commonplace in public areas, the AHA said, smokeless tobacco marketers have been promoting their products for use where cigarette smoking is prohibited. The researchers also pointed out a rise in smokeless tobacco use in teenage boys and reported that in 2008 1.4 million people aged 12 and older began using smokeless tobacco, up 47% from 2002 figures. In addition, and of concern, the researchers said, “less than half of the new initiates of ST product use were less than 18 years of age at first use and adolescent males.”
In response to these trends, the Food and Drug Administration issued a final regulation prohibiting the sale of tobacco products —smokeless and otherwise — to anyone under the age of 18. This regulation is a part of the Family Smoking Prevention and Tobacco Control Act. The act has specific requirements about the labeling of smokeless tobacco products and advertisements, which must include at least 1 of these 4 warnings:
WARNING: This product can cause mouth cancer.
WARNING: This product can cause gum disease and tooth loss.
WARNING: This product is not a safe alternative to cigarettes.
WARNING: Smokeless tobacco is addictive.
As of June 22, all tobacco products had to have these labels and follow the guidelines. Smokeless tobacco products had until July 22 to comply with the new laws regarding labeling.
Smokeless tobacco products are not safer alternatives to cigarette smoking, do not help smokers quit, and their long-term use can, in fact, increase the risk of fatal heart attack, fatal stroke and cancer, the American Heart Association warned in a scientific statement published online Sept. 13.
The researchers, led by Mariann R. Piano, Ph.D., examined several international studies to compare smokeless tobacco use and its health risks. Metaanalysis data involving male, Swedish smokers from 1976-2002 showed a significant decrease in cigarette smoking that corresponded with an increase in use of smokeless tobacco products, the investigators wrote in the AHA journal, Circulation. Despite the decline in cigarette use, concern is warranted, Dr. Piano, professor of biobehavioral science at the University of Illinois at Chicago, explained: “Smokeless tobacco products are harmful and addictive – that does not translate to a better alternative,” Dr. Piano, said in a written statement released by the AHA.
“Scientists and policy makers need to assess the effect of ‘reduced risk’ messages related to smokeless tobacco use on public perception, especially among smokers who might be trying to quit,” Dr. Piano and her colleagues wrote. Citing “inadequate evidence of smoking cessation efficacy and safety,” the researchers deemed as inappropriate the promotion of smokeless tobacco as a way to reduce smoking-related diseases.
The American Heart Association does recommend nicotine replacement therapy (nicotine gum or a nicotine-releasing patch placed on the skin) as a safer option for cigarette smokers wanting to quit. “Clinical studies have found no increased risk of heart attack or stroke with either type of nicotine replacement therapy,” the AHA statement said in the written statement.
Metaanalysis data in the AHA scientific statement indicated that smokeless tobacco use was associated with an increased risk of heart disease (relative risk 1.12, n=8 studies) (Int J Epidemiol. 2007;36:789–804). Additionally, a subanalysis of INTERHEART (a study of 15,152 cases of first myocardial infarction in 52 countries) showed that tobacco chewers had a significantly increased risk of first myocardial infarction (odds ratio 2.23) compared with those who never used tobacco. Two other metaanalyses indicated that smokeless tobacco use was also associated with an increased risk of fatal stroke (RR 1.42, n=5 studies, and RR 1.40, n=5 studies).
The researchers explained that, like cigarettes, smokeless tobacco (ST) products still contain nicotine of varying concentrations as well as a number of carcinogens that are just as harmful. Cigarettes and oral snuff have similar amounts of nicotine (milligrams per gram of tobacco), while chewing tobacco appears to have “somewhat lower” amounts compared with cigarettes, Dr. Piano and her colleagues wrote. “Even though certain manufacturing techniques are used to reduce the level of these compounds in some products, they remain present in substantial concentrations in ST products, including Swedish snus,” they said.
In a comparison of nicotine concentration between three types of smokeless tobacco products (chewing tobacco, dry snuff, and moist snuff) and cigarettes sold in the United States, all of the smokeless tobacco products had nicotine concentrations that were similar to cigarettes with the highest concentrations (see chart).
Dr. Piano and her colleagues found that unlike the aforementioned Swedish cohorts, there was no reduction in smoking rates among people in the United States using smokeless tobacco. (The sale of smokeless tobacco products such as moist snuff or snus is banned in most of the European Union with the exception of Sweden and Norway.)
In the United States about 8.1 million people are users of smokeless tobacco and its use is more prevalent in men than women, and people between the ages of 18-25 are the most likely to use smokeless tobacco, the researchers wrote. According to the study, educational background and socioeconomic status coincided with who tends to use smokeless tobacco the most. High prevalence was reported among people with a high-school diploma as their highest level of education, as well as people who live in southern states and rural areas. Blue-collar workers and service or labor workers, as well as the unemployed, were among the regular users of smokeless tobacco products. Native Americans have the highest prevalence of use (9%) followed by whites (5.8%), African Americans (1.9%), Hispanics (0.8%), and Asian Americans (0.6%).
It also appears that while U.S. chewing tobacco use has been on the decline since the 1980s, snuff consumption and production is increasing, the researchers said.
Dr. Piano reported that she received a grant from the National Institutes of Health. The researchers reported no relevant conflicts of interest.
Nicotine Concentrations in Smokeless Tobacco Products and Cigarettes Sold in the United States
Smokeless Tobacco in the U.S.A.
In a scientific statement published in Circulation, the American Heart Association highlighted other trends related to smokeless tobacco (ST) use in the United States.
As smoke-free air laws become more commonplace in public areas, the AHA said, smokeless tobacco marketers have been promoting their products for use where cigarette smoking is prohibited. The researchers also pointed out a rise in smokeless tobacco use in teenage boys and reported that in 2008 1.4 million people aged 12 and older began using smokeless tobacco, up 47% from 2002 figures. In addition, and of concern, the researchers said, “less than half of the new initiates of ST product use were less than 18 years of age at first use and adolescent males.”
In response to these trends, the Food and Drug Administration issued a final regulation prohibiting the sale of tobacco products —smokeless and otherwise — to anyone under the age of 18. This regulation is a part of the Family Smoking Prevention and Tobacco Control Act. The act has specific requirements about the labeling of smokeless tobacco products and advertisements, which must include at least 1 of these 4 warnings:
WARNING: This product can cause mouth cancer.
WARNING: This product can cause gum disease and tooth loss.
WARNING: This product is not a safe alternative to cigarettes.
WARNING: Smokeless tobacco is addictive.
As of June 22, all tobacco products had to have these labels and follow the guidelines. Smokeless tobacco products had until July 22 to comply with the new laws regarding labeling.
From Circulation
Major Finding: Several meta-analyses indicate that smokeless tobacco use was associated with an increased risk of heart disease (relative risk 1.12,) and fatal stroke (RR 1.42 and RR 1.40).
Data Source: Nonsystematic review of meta-analyses, randomized clinical trials, cohort or case control, and comparative studies regarding CV risk and ST product use primarily conducted in Sweden and the United States.
Disclosures: None.
Decline in Tobacco Use Stalled, but Secondhand Smoke Exposure Down
Smoking rates, which declined precipitously in the United States from 1964 to 2004, have remained virtually unchanged since then, according to data from the 2009 National Health Interview Survey. In 2009, 20.6% of adult Americans smoked cigarettes, compared with 20.9% of Americans in 2005, a difference that was not statistically significant.

On the other hand, data from the 2007-2008 National Health and Nutrition Examination Survey (NHANES) demonstrated a significant drop in the proportion of nonsmoking Americans aged 3 years and above with detectable levels of serum cotinine, an indication of exposure to secondhand smoke. That rate fell from 52.5% in the 1999-2000 survey to 40.1% in the 2007-2008 survey.
Both studies appeared in the Sept. 7 issue of the Morbidity and Mortality Weekly Report, published by the Centers for Disease Control and Prevention (MMWR 2010;59:1-6 and 7-12).
In announcing the results at a press briefing today, Dr. Thomas R. Frieden, director of the CDC, said that both the tobacco industry and federal, state, and local governments bear the blame for the failure of smoking rates to decline. “The industry has gotten even better at sidestepping laws designed to get people to stop smoking,” he said. “They ensure that every cigarette they sell delivers nicotine quickly and efficiently to keep people addicted.”
In addition, the industry has found ways to sidestep regulations banning the sale of flavored cigarettes, which can encourage children to start smoking, Dr. Frieden said. And while tobacco companies are not permitted to market their products as having lower levels of tar and nicotine, “they continue to deceive smokers with color coding and other subtle and not-so-subtle ways of sending the message that some cigarettes are less deadly than others, when in fact all cigarettes kill equally,” he said.
Furthermore, “government is also not doing what it needs to reduce smoking,” he charged. “Comprehensive, evidence-based programs are not being widely implemented. Last year, states took in about $25 billion from tobacco taxes and the [Tobacco] Master Settlement Agreement but spent only about $700 million – about 3 cents on every dollar [on tobacco control]. By 2015, if all states funded tobacco control at the CDC recommended level – 15 cents on the dollar of tobacco revenue – there would be an estimated 5 million fewer smokers in this country and that would prevent at least 1 million deaths in the future.”
While the NHANES study did find significant overall declines in the proportion of nonsmokers with detectable levels of serum cotinine, that decline did not extend to children who live with a smoker. Virtually all such children – 98.3% – had detectable cotinine levels, compared with 39.9% of children not living with someone who smoked inside the home. For nonsmoking adults, the corresponding figures were 93.4% and 33.4%.
The first study used data collected in 2009 by the National Health Interview Survey, which involved telephone interviews with 27,603 Americans aged 18 years and older. The second study used NHANES data collected from a nationally representative sample of 30,451 nonsmoking Americans aged 3 years and older.
In answer to a reporter’s question, Dr. Frieden said, “There’s a lot that doctors can do. Doctors can ask every patient if they smoke, and they can advise every patient who does to quit and quit today, and, if not today, then to set a date when they can quit. [Physicians] should also know what services are available in their community to help smokers quit and refer people to quit [telephone] lines. With the Affordable Care Act, tobacco cessation medication will be free of charge, so it should be easier for people to quit smoking in the future.”
No disclosures were reported.
Smoking rates, which declined precipitously in the United States from 1964 to 2004, have remained virtually unchanged since then, according to data from the 2009 National Health Interview Survey. In 2009, 20.6% of adult Americans smoked cigarettes, compared with 20.9% of Americans in 2005, a difference that was not statistically significant.
On the other hand, data from the 2007-2008 National Health and Nutrition Examination Survey (NHANES) demonstrated a significant drop in the proportion of nonsmoking Americans aged 3 years and above with detectable levels of serum cotinine, an indication of exposure to secondhand smoke. That rate fell from 52.5% in the 1999-2000 survey to 40.1% in the 2007-2008 survey.
Both studies appeared in the Sept. 7 issue of the Morbidity and Mortality Weekly Report, published by the Centers for Disease Control and Prevention (MMWR 2010;59:1-6 and 7-12).
In announcing the results at a press briefing today, Dr. Thomas R. Frieden, director of the CDC, said that both the tobacco industry and federal, state, and local governments bear the blame for the failure of smoking rates to decline. “The industry has gotten even better at sidestepping laws designed to get people to stop smoking,” he said. “They ensure that every cigarette they sell delivers nicotine quickly and efficiently to keep people addicted.”
In addition, the industry has found ways to sidestep regulations banning the sale of flavored cigarettes, which can encourage children to start smoking, Dr. Frieden said. And while tobacco companies are not permitted to market their products as having lower levels of tar and nicotine, “they continue to deceive smokers with color coding and other subtle and not-so-subtle ways of sending the message that some cigarettes are less deadly than others, when in fact all cigarettes kill equally,” he said.
Furthermore, “government is also not doing what it needs to reduce smoking,” he charged. “Comprehensive, evidence-based programs are not being widely implemented. Last year, states took in about $25 billion from tobacco taxes and the [Tobacco] Master Settlement Agreement but spent only about $700 million – about 3 cents on every dollar [on tobacco control]. By 2015, if all states funded tobacco control at the CDC recommended level – 15 cents on the dollar of tobacco revenue – there would be an estimated 5 million fewer smokers in this country and that would prevent at least 1 million deaths in the future.”
While the NHANES study did find significant overall declines in the proportion of nonsmokers with detectable levels of serum cotinine, that decline did not extend to children who live with a smoker. Virtually all such children – 98.3% – had detectable cotinine levels, compared with 39.9% of children not living with someone who smoked inside the home. For nonsmoking adults, the corresponding figures were 93.4% and 33.4%.
The first study used data collected in 2009 by the National Health Interview Survey, which involved telephone interviews with 27,603 Americans aged 18 years and older. The second study used NHANES data collected from a nationally representative sample of 30,451 nonsmoking Americans aged 3 years and older.
In answer to a reporter’s question, Dr. Frieden said, “There’s a lot that doctors can do. Doctors can ask every patient if they smoke, and they can advise every patient who does to quit and quit today, and, if not today, then to set a date when they can quit. [Physicians] should also know what services are available in their community to help smokers quit and refer people to quit [telephone] lines. With the Affordable Care Act, tobacco cessation medication will be free of charge, so it should be easier for people to quit smoking in the future.”
No disclosures were reported.
Smoking rates, which declined precipitously in the United States from 1964 to 2004, have remained virtually unchanged since then, according to data from the 2009 National Health Interview Survey. In 2009, 20.6% of adult Americans smoked cigarettes, compared with 20.9% of Americans in 2005, a difference that was not statistically significant.
On the other hand, data from the 2007-2008 National Health and Nutrition Examination Survey (NHANES) demonstrated a significant drop in the proportion of nonsmoking Americans aged 3 years and above with detectable levels of serum cotinine, an indication of exposure to secondhand smoke. That rate fell from 52.5% in the 1999-2000 survey to 40.1% in the 2007-2008 survey.
Both studies appeared in the Sept. 7 issue of the Morbidity and Mortality Weekly Report, published by the Centers for Disease Control and Prevention (MMWR 2010;59:1-6 and 7-12).
In announcing the results at a press briefing today, Dr. Thomas R. Frieden, director of the CDC, said that both the tobacco industry and federal, state, and local governments bear the blame for the failure of smoking rates to decline. “The industry has gotten even better at sidestepping laws designed to get people to stop smoking,” he said. “They ensure that every cigarette they sell delivers nicotine quickly and efficiently to keep people addicted.”
In addition, the industry has found ways to sidestep regulations banning the sale of flavored cigarettes, which can encourage children to start smoking, Dr. Frieden said. And while tobacco companies are not permitted to market their products as having lower levels of tar and nicotine, “they continue to deceive smokers with color coding and other subtle and not-so-subtle ways of sending the message that some cigarettes are less deadly than others, when in fact all cigarettes kill equally,” he said.
Furthermore, “government is also not doing what it needs to reduce smoking,” he charged. “Comprehensive, evidence-based programs are not being widely implemented. Last year, states took in about $25 billion from tobacco taxes and the [Tobacco] Master Settlement Agreement but spent only about $700 million – about 3 cents on every dollar [on tobacco control]. By 2015, if all states funded tobacco control at the CDC recommended level – 15 cents on the dollar of tobacco revenue – there would be an estimated 5 million fewer smokers in this country and that would prevent at least 1 million deaths in the future.”
While the NHANES study did find significant overall declines in the proportion of nonsmokers with detectable levels of serum cotinine, that decline did not extend to children who live with a smoker. Virtually all such children – 98.3% – had detectable cotinine levels, compared with 39.9% of children not living with someone who smoked inside the home. For nonsmoking adults, the corresponding figures were 93.4% and 33.4%.
The first study used data collected in 2009 by the National Health Interview Survey, which involved telephone interviews with 27,603 Americans aged 18 years and older. The second study used NHANES data collected from a nationally representative sample of 30,451 nonsmoking Americans aged 3 years and older.
In answer to a reporter’s question, Dr. Frieden said, “There’s a lot that doctors can do. Doctors can ask every patient if they smoke, and they can advise every patient who does to quit and quit today, and, if not today, then to set a date when they can quit. [Physicians] should also know what services are available in their community to help smokers quit and refer people to quit [telephone] lines. With the Affordable Care Act, tobacco cessation medication will be free of charge, so it should be easier for people to quit smoking in the future.”
No disclosures were reported.
Major Finding: Among American adults, 20.6% smoked cigarettes in 2009, the fifth year in a row with no significant decline in the smoking rate. Among nonsmokers older than 3 years, 40.1% had measurable levels of serum cotinine in 2007-2008, a significant decline from 1999-2000, when 52.5% of the population had evidence of secondhand smoke exposure.
Data Source: Telephone survey of 27,603 adults from the 2009 National Health Interview Survey and data from 30,451 nonsmokers in the 2007-2008 National Health and Nutrition Examination Survey.
Disclosures: None reported.
FDA Advisory Panel Gives Nod to Ceftaroline for CABP
GAITHERSBURG, Md. – A Food and Drug Administration advisory panel voted 21 to 0 that the antimicrobial drug ceftaroline fosamil had been shown to be safe and effective for treating community-acquired bacterial pneumonia, based on the result of two clinical trials.
At a meeting of the FDA’s Anti-Infective Drugs Advisory Committee Sept. 7, panelists were enthusiastic about the drug, but had some concerns, including the lack of data in patients with methicillin-resistant Staphylococcus aureus (MRSA) since it’s likely the drug would be used to treat such infections. Another concern was the generalizability of the data, since the studies were done largely in Eastern European patients.
The manufacturer, Cerexa Inc., a subsidiary of Forest Laboratories Inc., has proposed that ceftaroline fosamil be approved for the treatment of adults with community-acquired bacterial pneumonia (CABP) or complicated skin and skin structure infections (cSSSI). The panel will discuss and vote on the cSSSI indication during the afternoon session of the meeting.
Ceftaroline, the active metabolite of ceftaroline fosamil, is a beta-lactam in the cephalosporin class of antimicrobials, with antibacterial activity against aerobic and anaerobic gram-positive and aerobic gram-negative bacteria, which are associated with skin and respiratory infections. The proposed dose for treating CABP is 600 mg administered intravenously every 12 hours, for 5-7 days, with a reduced dose for patients with moderate renal impairment.
In two international nearly identical phase III noninferiority studies of 1,240 patients with moderate to severe CABP, the effectiveness of treatment with ceftaroline at the proposed dose for 5-7 days was similar to treatment with the comparator, ceftriaxone (1 g IV every 24 hours). Effectiveness was based on the primary end point, clinical response at test of cure (TOC), 8-15 days after completing treatment. Clinical cure was defined as total resolution of all signs and symptoms of pneumonia or improvements to the extent that further antimicrobial treatment was not recommended. This end point was met by 84% and 81% of those treated with ceftaroline in the two studies, compared with 78% and 76% among those on the comparator, respectively. These results met the 10% noninferiority margin.
The safety profile of ceftaroline was similar to that expected for other cephalosporins, according to the company and FDA reviewers. The most common adverse reactions among those on ceftaroline were GI-related, such as diarrhea or nausea, followed by nervous system complaints such as headaches. The panelists also agreed that the safety profile was comparable to what would be expected with cephalosporins.
GAITHERSBURG, Md. – A Food and Drug Administration advisory panel voted 21 to 0 that the antimicrobial drug ceftaroline fosamil had been shown to be safe and effective for treating community-acquired bacterial pneumonia, based on the result of two clinical trials.
At a meeting of the FDA’s Anti-Infective Drugs Advisory Committee Sept. 7, panelists were enthusiastic about the drug, but had some concerns, including the lack of data in patients with methicillin-resistant Staphylococcus aureus (MRSA) since it’s likely the drug would be used to treat such infections. Another concern was the generalizability of the data, since the studies were done largely in Eastern European patients.
The manufacturer, Cerexa Inc., a subsidiary of Forest Laboratories Inc., has proposed that ceftaroline fosamil be approved for the treatment of adults with community-acquired bacterial pneumonia (CABP) or complicated skin and skin structure infections (cSSSI). The panel will discuss and vote on the cSSSI indication during the afternoon session of the meeting.
Ceftaroline, the active metabolite of ceftaroline fosamil, is a beta-lactam in the cephalosporin class of antimicrobials, with antibacterial activity against aerobic and anaerobic gram-positive and aerobic gram-negative bacteria, which are associated with skin and respiratory infections. The proposed dose for treating CABP is 600 mg administered intravenously every 12 hours, for 5-7 days, with a reduced dose for patients with moderate renal impairment.
In two international nearly identical phase III noninferiority studies of 1,240 patients with moderate to severe CABP, the effectiveness of treatment with ceftaroline at the proposed dose for 5-7 days was similar to treatment with the comparator, ceftriaxone (1 g IV every 24 hours). Effectiveness was based on the primary end point, clinical response at test of cure (TOC), 8-15 days after completing treatment. Clinical cure was defined as total resolution of all signs and symptoms of pneumonia or improvements to the extent that further antimicrobial treatment was not recommended. This end point was met by 84% and 81% of those treated with ceftaroline in the two studies, compared with 78% and 76% among those on the comparator, respectively. These results met the 10% noninferiority margin.
The safety profile of ceftaroline was similar to that expected for other cephalosporins, according to the company and FDA reviewers. The most common adverse reactions among those on ceftaroline were GI-related, such as diarrhea or nausea, followed by nervous system complaints such as headaches. The panelists also agreed that the safety profile was comparable to what would be expected with cephalosporins.
GAITHERSBURG, Md. – A Food and Drug Administration advisory panel voted 21 to 0 that the antimicrobial drug ceftaroline fosamil had been shown to be safe and effective for treating community-acquired bacterial pneumonia, based on the result of two clinical trials.
At a meeting of the FDA’s Anti-Infective Drugs Advisory Committee Sept. 7, panelists were enthusiastic about the drug, but had some concerns, including the lack of data in patients with methicillin-resistant Staphylococcus aureus (MRSA) since it’s likely the drug would be used to treat such infections. Another concern was the generalizability of the data, since the studies were done largely in Eastern European patients.
The manufacturer, Cerexa Inc., a subsidiary of Forest Laboratories Inc., has proposed that ceftaroline fosamil be approved for the treatment of adults with community-acquired bacterial pneumonia (CABP) or complicated skin and skin structure infections (cSSSI). The panel will discuss and vote on the cSSSI indication during the afternoon session of the meeting.
Ceftaroline, the active metabolite of ceftaroline fosamil, is a beta-lactam in the cephalosporin class of antimicrobials, with antibacterial activity against aerobic and anaerobic gram-positive and aerobic gram-negative bacteria, which are associated with skin and respiratory infections. The proposed dose for treating CABP is 600 mg administered intravenously every 12 hours, for 5-7 days, with a reduced dose for patients with moderate renal impairment.
In two international nearly identical phase III noninferiority studies of 1,240 patients with moderate to severe CABP, the effectiveness of treatment with ceftaroline at the proposed dose for 5-7 days was similar to treatment with the comparator, ceftriaxone (1 g IV every 24 hours). Effectiveness was based on the primary end point, clinical response at test of cure (TOC), 8-15 days after completing treatment. Clinical cure was defined as total resolution of all signs and symptoms of pneumonia or improvements to the extent that further antimicrobial treatment was not recommended. This end point was met by 84% and 81% of those treated with ceftaroline in the two studies, compared with 78% and 76% among those on the comparator, respectively. These results met the 10% noninferiority margin.
The safety profile of ceftaroline was similar to that expected for other cephalosporins, according to the company and FDA reviewers. The most common adverse reactions among those on ceftaroline were GI-related, such as diarrhea or nausea, followed by nervous system complaints such as headaches. The panelists also agreed that the safety profile was comparable to what would be expected with cephalosporins.