User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Incidence, Risks for Thoracic Aneurysm in AAA Defined
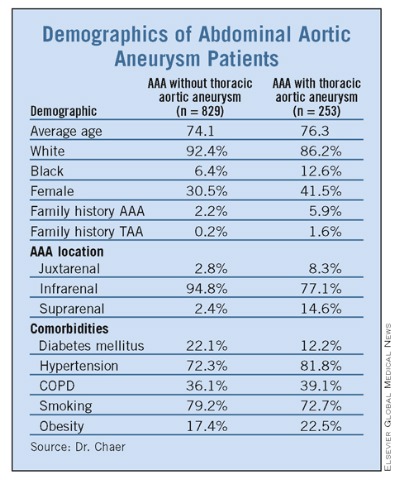
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
Demographics of Abdominal Aortic Aneurysm Patients
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
Demographics of Abdominal Aortic Aneurysm Patients
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
Demographics of Abdominal Aortic Aneurysm Patients
FROM THE ANNUAL MEETING OF THE EASTERN VASCULAR SOCIETY
Expect 2 Months of Sleep Disturbance After Stopping Hormone Therapy
CHICAGO – Almost 40% of women report sleep problems in midlife, and since hormone therapy benefits sleep, cessation of that therapy might have the opposite effect. A study of 1,704 women from the Group Health Research Institute of Seattle confirms that it does.

“Sleep problems were related to the suspension of hormone therapy for 1 or 2 months,” investigator Sarah E. Tom, Ph.D., formerly of the institute, said of the study’s findings. “Women who are discontinuing hormone therapy may benefit from alternative sleep management strategies immediately following discontinuation.” Dr. Tom presented her data at the annual meeting of the North American Menopause Society.
This was a secondary analysis of data from the READ study (Radiological Evaluation and Breast Density), a trial designed to test whether short-term suspension of hormone therapy resulted in better screening mammography performance. The trial recruited women aged 45-80 years from Group Health, a nonprofit health care system based in Washington state. The recruits were due for a screening mammography, and reported on use of hormone therapy for 2 years. They were randomized to continue hormone therapy or to suspend it for either 1 or 2 months prior to mammography.
The survey used a questionnaire that asked about the number of days subjects had various sleep complaints, including trouble falling asleep and waking while sleeping.
Various confounding variables, including alcohol consumption, body mass index, age, race, and ethnicity were considered, Dr. Tom said.
Of the 1,704 women, 1,405 had complete information on all variables. Of this group, 518 were randomized to continue hormone therapy, 452 to suspend therapy for 1 month, and 435 to suspend it for 2 months.
Demographic profiles were similar across all randomization groups. In the group continuing hormone therapy, for example, the median age was 58, more than 90% were white, and more than 50% used estrogen only. Sleep problems were comparable in the groups suspending therapy for 1 month or 2 months.
“For the group randomized to a 2-month suspension, they had an increase of about 0.7 days with trouble with their sleep, compared to women who were randomized to continue hormone therapy,” Dr. Tom said. Waking while sleeping was one of the most frequently reported problems, she said, and about 35% of women in the two sleep cessation groups reported using sleep aids in the previous week.
The study concluded that sleep problems were related to suspension of hormone therapy for 1 or 2 months. Dr. Tom said differences were modest but persistent across sleep items, and were similar for the 1- and 2-month suspension groups.
Dr. Tom disclosed no significant financial relationships. This study was sponsored by the Department of Defense, the National Institute on Aging, and the Group Health Research Institute.
CHICAGO – Almost 40% of women report sleep problems in midlife, and since hormone therapy benefits sleep, cessation of that therapy might have the opposite effect. A study of 1,704 women from the Group Health Research Institute of Seattle confirms that it does.
“Sleep problems were related to the suspension of hormone therapy for 1 or 2 months,” investigator Sarah E. Tom, Ph.D., formerly of the institute, said of the study’s findings. “Women who are discontinuing hormone therapy may benefit from alternative sleep management strategies immediately following discontinuation.” Dr. Tom presented her data at the annual meeting of the North American Menopause Society.
This was a secondary analysis of data from the READ study (Radiological Evaluation and Breast Density), a trial designed to test whether short-term suspension of hormone therapy resulted in better screening mammography performance. The trial recruited women aged 45-80 years from Group Health, a nonprofit health care system based in Washington state. The recruits were due for a screening mammography, and reported on use of hormone therapy for 2 years. They were randomized to continue hormone therapy or to suspend it for either 1 or 2 months prior to mammography.
The survey used a questionnaire that asked about the number of days subjects had various sleep complaints, including trouble falling asleep and waking while sleeping.
Various confounding variables, including alcohol consumption, body mass index, age, race, and ethnicity were considered, Dr. Tom said.
Of the 1,704 women, 1,405 had complete information on all variables. Of this group, 518 were randomized to continue hormone therapy, 452 to suspend therapy for 1 month, and 435 to suspend it for 2 months.
Demographic profiles were similar across all randomization groups. In the group continuing hormone therapy, for example, the median age was 58, more than 90% were white, and more than 50% used estrogen only. Sleep problems were comparable in the groups suspending therapy for 1 month or 2 months.
“For the group randomized to a 2-month suspension, they had an increase of about 0.7 days with trouble with their sleep, compared to women who were randomized to continue hormone therapy,” Dr. Tom said. Waking while sleeping was one of the most frequently reported problems, she said, and about 35% of women in the two sleep cessation groups reported using sleep aids in the previous week.
The study concluded that sleep problems were related to suspension of hormone therapy for 1 or 2 months. Dr. Tom said differences were modest but persistent across sleep items, and were similar for the 1- and 2-month suspension groups.
Dr. Tom disclosed no significant financial relationships. This study was sponsored by the Department of Defense, the National Institute on Aging, and the Group Health Research Institute.
CHICAGO – Almost 40% of women report sleep problems in midlife, and since hormone therapy benefits sleep, cessation of that therapy might have the opposite effect. A study of 1,704 women from the Group Health Research Institute of Seattle confirms that it does.
“Sleep problems were related to the suspension of hormone therapy for 1 or 2 months,” investigator Sarah E. Tom, Ph.D., formerly of the institute, said of the study’s findings. “Women who are discontinuing hormone therapy may benefit from alternative sleep management strategies immediately following discontinuation.” Dr. Tom presented her data at the annual meeting of the North American Menopause Society.
This was a secondary analysis of data from the READ study (Radiological Evaluation and Breast Density), a trial designed to test whether short-term suspension of hormone therapy resulted in better screening mammography performance. The trial recruited women aged 45-80 years from Group Health, a nonprofit health care system based in Washington state. The recruits were due for a screening mammography, and reported on use of hormone therapy for 2 years. They were randomized to continue hormone therapy or to suspend it for either 1 or 2 months prior to mammography.
The survey used a questionnaire that asked about the number of days subjects had various sleep complaints, including trouble falling asleep and waking while sleeping.
Various confounding variables, including alcohol consumption, body mass index, age, race, and ethnicity were considered, Dr. Tom said.
Of the 1,704 women, 1,405 had complete information on all variables. Of this group, 518 were randomized to continue hormone therapy, 452 to suspend therapy for 1 month, and 435 to suspend it for 2 months.
Demographic profiles were similar across all randomization groups. In the group continuing hormone therapy, for example, the median age was 58, more than 90% were white, and more than 50% used estrogen only. Sleep problems were comparable in the groups suspending therapy for 1 month or 2 months.
“For the group randomized to a 2-month suspension, they had an increase of about 0.7 days with trouble with their sleep, compared to women who were randomized to continue hormone therapy,” Dr. Tom said. Waking while sleeping was one of the most frequently reported problems, she said, and about 35% of women in the two sleep cessation groups reported using sleep aids in the previous week.
The study concluded that sleep problems were related to suspension of hormone therapy for 1 or 2 months. Dr. Tom said differences were modest but persistent across sleep items, and were similar for the 1- and 2-month suspension groups.
Dr. Tom disclosed no significant financial relationships. This study was sponsored by the Department of Defense, the National Institute on Aging, and the Group Health Research Institute.
FROM THE ANNUAL MEETING OF THE NORTH AMERICAN MENOPAUSE SOCIETY
Major Finding: Radiological Evaluation and Breast Density (READ) trial analysis predicts 2 months of disturbed sleep after stopping hormone therapy.
Data Source: Sample size of 1,405 from the READ Trial database randomized to three arms: HT (518), 1-month cessation (452), 2-month cessation (435).
Disclosures: None. The trial was sponsored by the Department of Defense, the National Institute on Aging, and the nonprofit Group Health Research Institute.
Back pain, then sudden death...Increase in morphine dose has fatal results...more
Back pain, then sudden death
BACK AND CHEST PAIN prompted a 42-year-old man to see a doctor. The family physician took the man’s blood pressure, which was 184/130, but performed no other testing. He prescribed pain medication and sent the patient home. The man died 3 days later of an aortic dissection.
PLAINTIFF’S CLAIM The physician was negligent because he did not try to lower the patient’s blood pressure or order a radiograph before sending him home.
THE DEFENSE There was no reason to suspect aortic dissection; the rupture was sudden and catastrophic.
VERDICT Alabama defense verdict.
COMMENT Although the defense prevailed, this case reminds us to always consider less common causes of low back pain.
Increase in morphine dose has fatal results
BREATHING DIFFICULTIES associated with chronic obstructive pulmonary disease led to the hospitalization of a 79-year-old woman. While there, she suffered respiratory arrest and a code was called. The pulmonologist on duty and the attending physician responded. After the patient was bagged, she started breathing on her own.
The attending physician subsequently discussed the patient’s treatment plan and prognosis with her daughter, who agreed to a do-not-resuscitate order. He ordered 2 mg morphine as needed for comfort.
Minutes later, the pulmonologist overrode the order and ordered 20 mg morphine by IV push. After it was given, the patient lost consciousness while talking to her daughter and granddaughter. She died about 3 hours later without regaining consciousness.
PLAINTIFF’S CLAIM The patient was improving until the night before her arrest, when she failed to get her scheduled breathing treatment. The pulmonologist was negligent in ordering 20 mg morphine, and the hospital nurses were negligent in administering it.
THE DEFENSE No negligence occurred. The patient would have died sooner than 3 hours after the morphine dose if morphine was, indeed, the cause of death.
VERDICT $3 million Georgia verdict.
COMMENT Do not resuscitate does not mean negligible risk of malpractice. Orders for 20 mg (!) of morphine will always be difficult to defend—even in a terminally ill patient.
Breast cancer diagnosis falls through the cracks
AFTER NOTICING A LUMP IN HER LEFT BREAST, a woman in her 40s underwent a screening mammogram rather than a diagnostic mammogram at a local facility. The mammogram showed no abnormalities, but an ultrasound examination the following year was abnormal. The report was faxed to her physician, who reportedly didn’t receive it. No follow-up occurred.
A year later, the patient made a follow-up appointment on her own and underwent diagnostic mammography and surgical biopsy, which revealed advanced breast cancer. A vacuum-assisted core biopsy and clip localization the following month revealed infiltrating ductal carcinoma. Neoadjuvant chemotherapy resulted in complications and hospitalization. The patient subsequently underwent additional chemotherapy and radiation treatments.
PLAINTIFF’S CLAIM The defendant health care facility didn’t properly evaluate the patient for breast cancer.
THE DEFENSE The defendant denied liability and asserted that its personnel acted within the standard of care.
VERDICT $575,000 South Carolina settlement.
COMMENT Follow-up and tracking of results remain key in preventing malpractice.
| End-of-life care: How to reduce malpractice risk |
COMMENTARY PROVIDED BY
Jeffrey L. Susman, MD
Editor-in-Chief
| End-of-life care: How to reduce malpractice risk |
COMMENTARY PROVIDED BY
Jeffrey L. Susman, MD
Editor-in-Chief
| End-of-life care: How to reduce malpractice risk |
COMMENTARY PROVIDED BY
Jeffrey L. Susman, MD
Editor-in-Chief
Back pain, then sudden death
BACK AND CHEST PAIN prompted a 42-year-old man to see a doctor. The family physician took the man’s blood pressure, which was 184/130, but performed no other testing. He prescribed pain medication and sent the patient home. The man died 3 days later of an aortic dissection.
PLAINTIFF’S CLAIM The physician was negligent because he did not try to lower the patient’s blood pressure or order a radiograph before sending him home.
THE DEFENSE There was no reason to suspect aortic dissection; the rupture was sudden and catastrophic.
VERDICT Alabama defense verdict.
COMMENT Although the defense prevailed, this case reminds us to always consider less common causes of low back pain.
Increase in morphine dose has fatal results
BREATHING DIFFICULTIES associated with chronic obstructive pulmonary disease led to the hospitalization of a 79-year-old woman. While there, she suffered respiratory arrest and a code was called. The pulmonologist on duty and the attending physician responded. After the patient was bagged, she started breathing on her own.
The attending physician subsequently discussed the patient’s treatment plan and prognosis with her daughter, who agreed to a do-not-resuscitate order. He ordered 2 mg morphine as needed for comfort.
Minutes later, the pulmonologist overrode the order and ordered 20 mg morphine by IV push. After it was given, the patient lost consciousness while talking to her daughter and granddaughter. She died about 3 hours later without regaining consciousness.
PLAINTIFF’S CLAIM The patient was improving until the night before her arrest, when she failed to get her scheduled breathing treatment. The pulmonologist was negligent in ordering 20 mg morphine, and the hospital nurses were negligent in administering it.
THE DEFENSE No negligence occurred. The patient would have died sooner than 3 hours after the morphine dose if morphine was, indeed, the cause of death.
VERDICT $3 million Georgia verdict.
COMMENT Do not resuscitate does not mean negligible risk of malpractice. Orders for 20 mg (!) of morphine will always be difficult to defend—even in a terminally ill patient.
Breast cancer diagnosis falls through the cracks
AFTER NOTICING A LUMP IN HER LEFT BREAST, a woman in her 40s underwent a screening mammogram rather than a diagnostic mammogram at a local facility. The mammogram showed no abnormalities, but an ultrasound examination the following year was abnormal. The report was faxed to her physician, who reportedly didn’t receive it. No follow-up occurred.
A year later, the patient made a follow-up appointment on her own and underwent diagnostic mammography and surgical biopsy, which revealed advanced breast cancer. A vacuum-assisted core biopsy and clip localization the following month revealed infiltrating ductal carcinoma. Neoadjuvant chemotherapy resulted in complications and hospitalization. The patient subsequently underwent additional chemotherapy and radiation treatments.
PLAINTIFF’S CLAIM The defendant health care facility didn’t properly evaluate the patient for breast cancer.
THE DEFENSE The defendant denied liability and asserted that its personnel acted within the standard of care.
VERDICT $575,000 South Carolina settlement.
COMMENT Follow-up and tracking of results remain key in preventing malpractice.
Back pain, then sudden death
BACK AND CHEST PAIN prompted a 42-year-old man to see a doctor. The family physician took the man’s blood pressure, which was 184/130, but performed no other testing. He prescribed pain medication and sent the patient home. The man died 3 days later of an aortic dissection.
PLAINTIFF’S CLAIM The physician was negligent because he did not try to lower the patient’s blood pressure or order a radiograph before sending him home.
THE DEFENSE There was no reason to suspect aortic dissection; the rupture was sudden and catastrophic.
VERDICT Alabama defense verdict.
COMMENT Although the defense prevailed, this case reminds us to always consider less common causes of low back pain.
Increase in morphine dose has fatal results
BREATHING DIFFICULTIES associated with chronic obstructive pulmonary disease led to the hospitalization of a 79-year-old woman. While there, she suffered respiratory arrest and a code was called. The pulmonologist on duty and the attending physician responded. After the patient was bagged, she started breathing on her own.
The attending physician subsequently discussed the patient’s treatment plan and prognosis with her daughter, who agreed to a do-not-resuscitate order. He ordered 2 mg morphine as needed for comfort.
Minutes later, the pulmonologist overrode the order and ordered 20 mg morphine by IV push. After it was given, the patient lost consciousness while talking to her daughter and granddaughter. She died about 3 hours later without regaining consciousness.
PLAINTIFF’S CLAIM The patient was improving until the night before her arrest, when she failed to get her scheduled breathing treatment. The pulmonologist was negligent in ordering 20 mg morphine, and the hospital nurses were negligent in administering it.
THE DEFENSE No negligence occurred. The patient would have died sooner than 3 hours after the morphine dose if morphine was, indeed, the cause of death.
VERDICT $3 million Georgia verdict.
COMMENT Do not resuscitate does not mean negligible risk of malpractice. Orders for 20 mg (!) of morphine will always be difficult to defend—even in a terminally ill patient.
Breast cancer diagnosis falls through the cracks
AFTER NOTICING A LUMP IN HER LEFT BREAST, a woman in her 40s underwent a screening mammogram rather than a diagnostic mammogram at a local facility. The mammogram showed no abnormalities, but an ultrasound examination the following year was abnormal. The report was faxed to her physician, who reportedly didn’t receive it. No follow-up occurred.
A year later, the patient made a follow-up appointment on her own and underwent diagnostic mammography and surgical biopsy, which revealed advanced breast cancer. A vacuum-assisted core biopsy and clip localization the following month revealed infiltrating ductal carcinoma. Neoadjuvant chemotherapy resulted in complications and hospitalization. The patient subsequently underwent additional chemotherapy and radiation treatments.
PLAINTIFF’S CLAIM The defendant health care facility didn’t properly evaluate the patient for breast cancer.
THE DEFENSE The defendant denied liability and asserted that its personnel acted within the standard of care.
VERDICT $575,000 South Carolina settlement.
COMMENT Follow-up and tracking of results remain key in preventing malpractice.
Does office spirometry improve quit rates in smokers?
IT DEPENDS. Simply performing spirometry and offering cessation advice doesn’t improve quit rates in patients who smoke (strength of recommendation [SOR]: A, systematic review of randomized controlled trials [RCTs]). However, when the spirometry results are communicated in terms of “lung age,” smokers are more likely to quit (SOR: B, large RCT). Patients with abnormal spirometry results may be more likely to quit than patients with normal results (SOR: B, cohort studies).
Evidence summary
A systematic review of 3 RCTs with a total of 649 participants evaluated office spirometry as a motivational tool to improve quit rates by comparing spirometry plus cessation advice with cessation advice alone. All participants were men and women 19 to 75 years of age recruited from outpatient clinics.1
In 1 trial, the intervention group received repeated counseling at 4 visits and underwent spirometry; the control group had 1 counseling session and was given a brochure. In the other 2 trials, the intervention group had both carbon monoxide measurements and spirometry, and all participants received more extensive counseling, including cessation skills training.
At 9 to 12 months’ follow-up, quit rates ranged from 6% to 24% in the intervention groups vs 5% to 14% in the control groups (not significantly different).1
A subsequent study randomized 221 smokers to receive either spirometry plus brief cessation advice or advice alone. Researchers recruited patients 15 to 80 years of age who were willing to quit smoking from 16 general practice clinics in Belgium. Fifty-one percent of patients in both groups used nicotine replacement therapy (a larger percentage than is typical in studies done in the United States). At 6, 12, and 24 months, 5%, 2%, and 5% more smokers, respectively, from the spirometry group quit smoking compared with the control group, but this difference was not significant.2
Reporting spirometry results in terms of lung age may spur quitting
One RCT found significantly improved quit rates when patients who smoked were given their office spirometry results in terms of “lung age” (the age of an average healthy person with similar spirometry results) rather than as forced expiratory volume in 1 second (FEV1). Investigators performed office spirometry and gave smoking cessation advice to 561 smokers older than 35 years who were recruited from 5 general practices. They randomized patients to receive their spirometry results as either lung age or FEV1 and recorded quit rates at 12 months (smoking cessation was verified by measuring blood levels of carbon monoxide).
Patients whose spirometry results were reported as lung age were significantly more likely to quit than smokers whose results were given as FEV1 (13.6% vs 6.4%; P=.005; number needed to treat [NNT]=14 smokers counseled using lung age to cause 1 more patient to quit). Smokers with normal lung ages were no more likely to quit than smokers with abnormal results.3
Abnormal results also may be a motivator
However, 3 prospective cohort studies demonstrated that patients with abnormal spirometry results were more likely to quit than patients with normal spirometry. In the first study, 4494 patients with at least 10 pack-years of smoking from 10 outpatient chest clinics in Poland underwent spirometry and were counseled to quit smoking; 1177 had abnormal spirometry results.
One year later, 16.3% of smokers with abnormal results had quit smoking, compared with 12% in the group with normal spirometry (P=.0003; NNT=23).4
The second study, also at outpatient chest clinics in Poland, evaluated spirometry plus cessation advice among 558 smokers, 297 of whom had abnormal spirometry results. At 1 year, 10.6% of patients with abnormal results had quit, compared with 8.4% of patients with normal lung function. A subgroup of 109 patients with moderate to severe airflow limitation showed significantly higher quit rates when compared with patients with mildly abnormal spirometry (16.5% vs 6.4%; P<.0001; NNT=10).5
In the third study, 6 primary care sites in Sweden provided spirometry and brief cessation advice to 445 smokers, 119 of whom were found to have abnormal lung function. At 3-year follow-up, 29% of patients with abnormal lung function had quit smoking, compared with 14% of patients with normal lung function (P=.001; NNT=7). Forty-five smokers with mildly abnormal lung function were recruited from this study to participate in another study, which may have biased the results toward higher quit rates among smokers with worse spirometry results.6
Recommendations
The US Preventive Services Task Force recommends against using spirometry to screen for chronic obstructive pulmonary disease, but advocates screening all adults for tobacco use and encouraging cessation.7
The authors of a Cochrane review found insufficient evidence to recommend using biomedical risk assessment (carbon monoxide blood levels, spirometry, genetic testing for alpha-1 antitrypsin deficiency) as a smoking cessation aid.8
1. Wilt TJ, Niewoehner D, Kane RL, et al. Spirometry as a motivational tool to improve smoking cessation rates: a systematic review of the literature. Nicotine Tob Res. 2007;9:21-32.
2. Buffels J, Degryse J, Decramer M, et al. Spirometry and smoking cessation advice in general practice: a randomised clinical trial. Respir Med. 2006;100:2012-2017.
3. Parkes G, Greenhalgh T, Griffin M, et al. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
4. Bednarek M, Gorecka D, Wielgomas J, et al. Smokers with airway obstruction are more likely to quit smoking. Thorax. 2006;61:869-873.
5. Gorecka D, Bednarek M, Nowinski A, et al. Diagnosis of airflow limitation combined with smoking cessation advice increases stop-smoking rate. Chest. 2003;123:1916-1923.
6. Stratelis G, Molstad S, Jakobsson P, et al. The impact of repeated spirometry and smoking cessation advice on smokers with mild COPD. Scand J Prim Health Care. 2006;24:133-139.
7. Task force recommends against screening for chronic obstructive pulmonary disease using spirometry [press release] Rockville, Md: Agency for Healthcare Research and Quality; March 3, 2008. Available at: www.ahrq.gov/news/press/pr2008/tfcopdpr.htm. Accessed September 4, 2008.
8. Bize R, Burnand B, Mueller Y, et al. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2009;(2):CD004705.-
IT DEPENDS. Simply performing spirometry and offering cessation advice doesn’t improve quit rates in patients who smoke (strength of recommendation [SOR]: A, systematic review of randomized controlled trials [RCTs]). However, when the spirometry results are communicated in terms of “lung age,” smokers are more likely to quit (SOR: B, large RCT). Patients with abnormal spirometry results may be more likely to quit than patients with normal results (SOR: B, cohort studies).
Evidence summary
A systematic review of 3 RCTs with a total of 649 participants evaluated office spirometry as a motivational tool to improve quit rates by comparing spirometry plus cessation advice with cessation advice alone. All participants were men and women 19 to 75 years of age recruited from outpatient clinics.1
In 1 trial, the intervention group received repeated counseling at 4 visits and underwent spirometry; the control group had 1 counseling session and was given a brochure. In the other 2 trials, the intervention group had both carbon monoxide measurements and spirometry, and all participants received more extensive counseling, including cessation skills training.
At 9 to 12 months’ follow-up, quit rates ranged from 6% to 24% in the intervention groups vs 5% to 14% in the control groups (not significantly different).1
A subsequent study randomized 221 smokers to receive either spirometry plus brief cessation advice or advice alone. Researchers recruited patients 15 to 80 years of age who were willing to quit smoking from 16 general practice clinics in Belgium. Fifty-one percent of patients in both groups used nicotine replacement therapy (a larger percentage than is typical in studies done in the United States). At 6, 12, and 24 months, 5%, 2%, and 5% more smokers, respectively, from the spirometry group quit smoking compared with the control group, but this difference was not significant.2
Reporting spirometry results in terms of lung age may spur quitting
One RCT found significantly improved quit rates when patients who smoked were given their office spirometry results in terms of “lung age” (the age of an average healthy person with similar spirometry results) rather than as forced expiratory volume in 1 second (FEV1). Investigators performed office spirometry and gave smoking cessation advice to 561 smokers older than 35 years who were recruited from 5 general practices. They randomized patients to receive their spirometry results as either lung age or FEV1 and recorded quit rates at 12 months (smoking cessation was verified by measuring blood levels of carbon monoxide).
Patients whose spirometry results were reported as lung age were significantly more likely to quit than smokers whose results were given as FEV1 (13.6% vs 6.4%; P=.005; number needed to treat [NNT]=14 smokers counseled using lung age to cause 1 more patient to quit). Smokers with normal lung ages were no more likely to quit than smokers with abnormal results.3
Abnormal results also may be a motivator
However, 3 prospective cohort studies demonstrated that patients with abnormal spirometry results were more likely to quit than patients with normal spirometry. In the first study, 4494 patients with at least 10 pack-years of smoking from 10 outpatient chest clinics in Poland underwent spirometry and were counseled to quit smoking; 1177 had abnormal spirometry results.
One year later, 16.3% of smokers with abnormal results had quit smoking, compared with 12% in the group with normal spirometry (P=.0003; NNT=23).4
The second study, also at outpatient chest clinics in Poland, evaluated spirometry plus cessation advice among 558 smokers, 297 of whom had abnormal spirometry results. At 1 year, 10.6% of patients with abnormal results had quit, compared with 8.4% of patients with normal lung function. A subgroup of 109 patients with moderate to severe airflow limitation showed significantly higher quit rates when compared with patients with mildly abnormal spirometry (16.5% vs 6.4%; P<.0001; NNT=10).5
In the third study, 6 primary care sites in Sweden provided spirometry and brief cessation advice to 445 smokers, 119 of whom were found to have abnormal lung function. At 3-year follow-up, 29% of patients with abnormal lung function had quit smoking, compared with 14% of patients with normal lung function (P=.001; NNT=7). Forty-five smokers with mildly abnormal lung function were recruited from this study to participate in another study, which may have biased the results toward higher quit rates among smokers with worse spirometry results.6
Recommendations
The US Preventive Services Task Force recommends against using spirometry to screen for chronic obstructive pulmonary disease, but advocates screening all adults for tobacco use and encouraging cessation.7
The authors of a Cochrane review found insufficient evidence to recommend using biomedical risk assessment (carbon monoxide blood levels, spirometry, genetic testing for alpha-1 antitrypsin deficiency) as a smoking cessation aid.8
IT DEPENDS. Simply performing spirometry and offering cessation advice doesn’t improve quit rates in patients who smoke (strength of recommendation [SOR]: A, systematic review of randomized controlled trials [RCTs]). However, when the spirometry results are communicated in terms of “lung age,” smokers are more likely to quit (SOR: B, large RCT). Patients with abnormal spirometry results may be more likely to quit than patients with normal results (SOR: B, cohort studies).
Evidence summary
A systematic review of 3 RCTs with a total of 649 participants evaluated office spirometry as a motivational tool to improve quit rates by comparing spirometry plus cessation advice with cessation advice alone. All participants were men and women 19 to 75 years of age recruited from outpatient clinics.1
In 1 trial, the intervention group received repeated counseling at 4 visits and underwent spirometry; the control group had 1 counseling session and was given a brochure. In the other 2 trials, the intervention group had both carbon monoxide measurements and spirometry, and all participants received more extensive counseling, including cessation skills training.
At 9 to 12 months’ follow-up, quit rates ranged from 6% to 24% in the intervention groups vs 5% to 14% in the control groups (not significantly different).1
A subsequent study randomized 221 smokers to receive either spirometry plus brief cessation advice or advice alone. Researchers recruited patients 15 to 80 years of age who were willing to quit smoking from 16 general practice clinics in Belgium. Fifty-one percent of patients in both groups used nicotine replacement therapy (a larger percentage than is typical in studies done in the United States). At 6, 12, and 24 months, 5%, 2%, and 5% more smokers, respectively, from the spirometry group quit smoking compared with the control group, but this difference was not significant.2
Reporting spirometry results in terms of lung age may spur quitting
One RCT found significantly improved quit rates when patients who smoked were given their office spirometry results in terms of “lung age” (the age of an average healthy person with similar spirometry results) rather than as forced expiratory volume in 1 second (FEV1). Investigators performed office spirometry and gave smoking cessation advice to 561 smokers older than 35 years who were recruited from 5 general practices. They randomized patients to receive their spirometry results as either lung age or FEV1 and recorded quit rates at 12 months (smoking cessation was verified by measuring blood levels of carbon monoxide).
Patients whose spirometry results were reported as lung age were significantly more likely to quit than smokers whose results were given as FEV1 (13.6% vs 6.4%; P=.005; number needed to treat [NNT]=14 smokers counseled using lung age to cause 1 more patient to quit). Smokers with normal lung ages were no more likely to quit than smokers with abnormal results.3
Abnormal results also may be a motivator
However, 3 prospective cohort studies demonstrated that patients with abnormal spirometry results were more likely to quit than patients with normal spirometry. In the first study, 4494 patients with at least 10 pack-years of smoking from 10 outpatient chest clinics in Poland underwent spirometry and were counseled to quit smoking; 1177 had abnormal spirometry results.
One year later, 16.3% of smokers with abnormal results had quit smoking, compared with 12% in the group with normal spirometry (P=.0003; NNT=23).4
The second study, also at outpatient chest clinics in Poland, evaluated spirometry plus cessation advice among 558 smokers, 297 of whom had abnormal spirometry results. At 1 year, 10.6% of patients with abnormal results had quit, compared with 8.4% of patients with normal lung function. A subgroup of 109 patients with moderate to severe airflow limitation showed significantly higher quit rates when compared with patients with mildly abnormal spirometry (16.5% vs 6.4%; P<.0001; NNT=10).5
In the third study, 6 primary care sites in Sweden provided spirometry and brief cessation advice to 445 smokers, 119 of whom were found to have abnormal lung function. At 3-year follow-up, 29% of patients with abnormal lung function had quit smoking, compared with 14% of patients with normal lung function (P=.001; NNT=7). Forty-five smokers with mildly abnormal lung function were recruited from this study to participate in another study, which may have biased the results toward higher quit rates among smokers with worse spirometry results.6
Recommendations
The US Preventive Services Task Force recommends against using spirometry to screen for chronic obstructive pulmonary disease, but advocates screening all adults for tobacco use and encouraging cessation.7
The authors of a Cochrane review found insufficient evidence to recommend using biomedical risk assessment (carbon monoxide blood levels, spirometry, genetic testing for alpha-1 antitrypsin deficiency) as a smoking cessation aid.8
1. Wilt TJ, Niewoehner D, Kane RL, et al. Spirometry as a motivational tool to improve smoking cessation rates: a systematic review of the literature. Nicotine Tob Res. 2007;9:21-32.
2. Buffels J, Degryse J, Decramer M, et al. Spirometry and smoking cessation advice in general practice: a randomised clinical trial. Respir Med. 2006;100:2012-2017.
3. Parkes G, Greenhalgh T, Griffin M, et al. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
4. Bednarek M, Gorecka D, Wielgomas J, et al. Smokers with airway obstruction are more likely to quit smoking. Thorax. 2006;61:869-873.
5. Gorecka D, Bednarek M, Nowinski A, et al. Diagnosis of airflow limitation combined with smoking cessation advice increases stop-smoking rate. Chest. 2003;123:1916-1923.
6. Stratelis G, Molstad S, Jakobsson P, et al. The impact of repeated spirometry and smoking cessation advice on smokers with mild COPD. Scand J Prim Health Care. 2006;24:133-139.
7. Task force recommends against screening for chronic obstructive pulmonary disease using spirometry [press release] Rockville, Md: Agency for Healthcare Research and Quality; March 3, 2008. Available at: www.ahrq.gov/news/press/pr2008/tfcopdpr.htm. Accessed September 4, 2008.
8. Bize R, Burnand B, Mueller Y, et al. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2009;(2):CD004705.-
1. Wilt TJ, Niewoehner D, Kane RL, et al. Spirometry as a motivational tool to improve smoking cessation rates: a systematic review of the literature. Nicotine Tob Res. 2007;9:21-32.
2. Buffels J, Degryse J, Decramer M, et al. Spirometry and smoking cessation advice in general practice: a randomised clinical trial. Respir Med. 2006;100:2012-2017.
3. Parkes G, Greenhalgh T, Griffin M, et al. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
4. Bednarek M, Gorecka D, Wielgomas J, et al. Smokers with airway obstruction are more likely to quit smoking. Thorax. 2006;61:869-873.
5. Gorecka D, Bednarek M, Nowinski A, et al. Diagnosis of airflow limitation combined with smoking cessation advice increases stop-smoking rate. Chest. 2003;123:1916-1923.
6. Stratelis G, Molstad S, Jakobsson P, et al. The impact of repeated spirometry and smoking cessation advice on smokers with mild COPD. Scand J Prim Health Care. 2006;24:133-139.
7. Task force recommends against screening for chronic obstructive pulmonary disease using spirometry [press release] Rockville, Md: Agency for Healthcare Research and Quality; March 3, 2008. Available at: www.ahrq.gov/news/press/pr2008/tfcopdpr.htm. Accessed September 4, 2008.
8. Bize R, Burnand B, Mueller Y, et al. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2009;(2):CD004705.-
Evidence-based answers from the Family Physicians Inquiries Network
Children With Sleep Apnea Had Lower Grades in School : Sleep-disordered breathing may be linked to a higher risk of learning and behavioral problems.
SAN ANTONIO — Children with obstructive sleep apnea get worse grades in school than do their classmates without sleep-disordered breathing, a study shows.
These 10- to 16-year-olds with even mild obstructive sleep apnea (OSA) were also independently rated both by parents and by teachers as more likely to have attention and learning problems, Dean W. Beebe, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies.
“There was an impressive impact of sleep-disordered breathing on academic grades. That leaves the subjects with moderate to severe sleep apnea at a serious disadvantage,” said Dr. Beebe of Cincinnati Children's Hospital Medical Center.
The study included 163 overweight youths aged 10–16 years, who were recruited from sleep or weight management clinics. Investigators rated 42 of them as having moderate to severe OSA based on an apnea-hypopnea index in excess of 5 events/hr. Another 58 had mild OSA, defined by an apnea-hypopnea index of 1–5 events/hr. Twenty-six participants were classified as snorers, while 37 were free of sleep-disordered breathing (SDB).
Subjects without SDB maintained a collective B average at school. Snorers trended toward lower grades, although the difference was not significant. But participants with OSA, whether mild or more severe, averaged half a grade point lower than did those without SDB. The difference—a B–/C+ average rather than a solid B—could have implications down the road in terms of college and career opportunities, Dr. Beebe noted.
Thirty percent of students with moderate to severe OSA had a C average or less, compared with just 15% of those without SDB. And while 15% of subjects with no SDB had an A average academically, that was the case for only a single student with moderate to severe OSA.
On the validated Behavior Assessment System for Children (BASC), teachers rated the students with mild or more severe OSA as having significantly more attention and learning problems than those without SDB. Teachers also rated the non-SDB youths significantly higher in terms of the BASC adaptive functioning domains of leadership, social skills, and study skills.
Parents of students with SDB rated them on the BASC as having more attention, anxiety, depression, aggression, and hyperactivity problems.
Given the worsening obesity epidemic and the fact that obesity is a major risk factor for SDB in middle childhood, the evidence that SDB has adverse academic, behavioral, and cognitive consequences suggests a major public health concern, according to Dr. Beebe.
He said the next stage of his research will be to see whether the academic and learning deficits associated with SDB in middle childhood and adolescence are remediable when the respiratory condition is treated.
The study was funded by the American Sleep Medicine Foundation and the National Institutes of Health. Dr. Beebe reported having no financial conflicts.
SAN ANTONIO — Children with obstructive sleep apnea get worse grades in school than do their classmates without sleep-disordered breathing, a study shows.
These 10- to 16-year-olds with even mild obstructive sleep apnea (OSA) were also independently rated both by parents and by teachers as more likely to have attention and learning problems, Dean W. Beebe, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies.
“There was an impressive impact of sleep-disordered breathing on academic grades. That leaves the subjects with moderate to severe sleep apnea at a serious disadvantage,” said Dr. Beebe of Cincinnati Children's Hospital Medical Center.
The study included 163 overweight youths aged 10–16 years, who were recruited from sleep or weight management clinics. Investigators rated 42 of them as having moderate to severe OSA based on an apnea-hypopnea index in excess of 5 events/hr. Another 58 had mild OSA, defined by an apnea-hypopnea index of 1–5 events/hr. Twenty-six participants were classified as snorers, while 37 were free of sleep-disordered breathing (SDB).
Subjects without SDB maintained a collective B average at school. Snorers trended toward lower grades, although the difference was not significant. But participants with OSA, whether mild or more severe, averaged half a grade point lower than did those without SDB. The difference—a B–/C+ average rather than a solid B—could have implications down the road in terms of college and career opportunities, Dr. Beebe noted.
Thirty percent of students with moderate to severe OSA had a C average or less, compared with just 15% of those without SDB. And while 15% of subjects with no SDB had an A average academically, that was the case for only a single student with moderate to severe OSA.
On the validated Behavior Assessment System for Children (BASC), teachers rated the students with mild or more severe OSA as having significantly more attention and learning problems than those without SDB. Teachers also rated the non-SDB youths significantly higher in terms of the BASC adaptive functioning domains of leadership, social skills, and study skills.
Parents of students with SDB rated them on the BASC as having more attention, anxiety, depression, aggression, and hyperactivity problems.
Given the worsening obesity epidemic and the fact that obesity is a major risk factor for SDB in middle childhood, the evidence that SDB has adverse academic, behavioral, and cognitive consequences suggests a major public health concern, according to Dr. Beebe.
He said the next stage of his research will be to see whether the academic and learning deficits associated with SDB in middle childhood and adolescence are remediable when the respiratory condition is treated.
The study was funded by the American Sleep Medicine Foundation and the National Institutes of Health. Dr. Beebe reported having no financial conflicts.
SAN ANTONIO — Children with obstructive sleep apnea get worse grades in school than do their classmates without sleep-disordered breathing, a study shows.
These 10- to 16-year-olds with even mild obstructive sleep apnea (OSA) were also independently rated both by parents and by teachers as more likely to have attention and learning problems, Dean W. Beebe, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies.
“There was an impressive impact of sleep-disordered breathing on academic grades. That leaves the subjects with moderate to severe sleep apnea at a serious disadvantage,” said Dr. Beebe of Cincinnati Children's Hospital Medical Center.
The study included 163 overweight youths aged 10–16 years, who were recruited from sleep or weight management clinics. Investigators rated 42 of them as having moderate to severe OSA based on an apnea-hypopnea index in excess of 5 events/hr. Another 58 had mild OSA, defined by an apnea-hypopnea index of 1–5 events/hr. Twenty-six participants were classified as snorers, while 37 were free of sleep-disordered breathing (SDB).
Subjects without SDB maintained a collective B average at school. Snorers trended toward lower grades, although the difference was not significant. But participants with OSA, whether mild or more severe, averaged half a grade point lower than did those without SDB. The difference—a B–/C+ average rather than a solid B—could have implications down the road in terms of college and career opportunities, Dr. Beebe noted.
Thirty percent of students with moderate to severe OSA had a C average or less, compared with just 15% of those without SDB. And while 15% of subjects with no SDB had an A average academically, that was the case for only a single student with moderate to severe OSA.
On the validated Behavior Assessment System for Children (BASC), teachers rated the students with mild or more severe OSA as having significantly more attention and learning problems than those without SDB. Teachers also rated the non-SDB youths significantly higher in terms of the BASC adaptive functioning domains of leadership, social skills, and study skills.
Parents of students with SDB rated them on the BASC as having more attention, anxiety, depression, aggression, and hyperactivity problems.
Given the worsening obesity epidemic and the fact that obesity is a major risk factor for SDB in middle childhood, the evidence that SDB has adverse academic, behavioral, and cognitive consequences suggests a major public health concern, according to Dr. Beebe.
He said the next stage of his research will be to see whether the academic and learning deficits associated with SDB in middle childhood and adolescence are remediable when the respiratory condition is treated.
The study was funded by the American Sleep Medicine Foundation and the National Institutes of Health. Dr. Beebe reported having no financial conflicts.
Tolerance Not Seen With Sublingual Zolpidem
Major Finding: Persons who received a new formulation of low-dose sublingual zolpidem for middle-of-the-night insomnia showed no potential for abuse of the drug in the form of dependency, tolerance, or rebound potential, compared with placebo recipients.
Data Source: A 4-week outpatient study of 146 subjects.
Disclosures: Dr. Roth has served as a consultant to Transept Pharmaceuticals Inc., the manufacturer of the sublingual formulation of zolpidem tartrate. He has also received research support from and had other relationships with numerous pharmaceutical companies.
AMSTERDAM — A sublingual 3.5-mg formulation of zolpidem tartrate is effective for middle-of-the-night insomnia, producing no tolerance, rebound, or increase in use over a 4-week period, a study has shown.
“Awakening during the night with difficulty falling back to sleep is a prevalent condition, and a PRN treatment for this is needed as it may decrease overall drug exposure,” said the study's coinvestigator, Thomas Roth, Ph.D., of Henry Ford Hospital, Detroit.
Zolpidem sublingual tablets 3.5 mg and 1.75 mg were developed for the treatment of insomnia that is characterized by difficulty returning to sleep after middle-of-the-night (MOTN) awakening.
The compound is formulated with binary buffers to promote buccal absorption of a portion of the drug. This facilitates bioavailability, resulting in a rapid return to sleep.
Previous studies have found that sublingual zolpidem significantly reduces sleep latency after MOTN dosing.
In a sleep laboratory study, sleep latency time was approximately 28 minutes with placebo but just 10 minutes with zolpidem 3.5 mg (Sleep 2008;31:1277–84).
“This is a reduced dose of zolpidem, and importantly it is a sublingual formulation so you achieve much faster blood levels to help you fall back asleep but you reduce the total blood level as compared to taking it prophylactically. The concern is that over time, people take more and more of the medication,” Dr. Roth said at the meeting.
The drug is currently under review by the Food and Drug Administration for MOTN awakening.
In a study designed to address possible abuse liability associated with PRN use of the drug, 75 outpatients received zolpidem and 71 patients received placebo; all were assessed for latency to sleep onset after MOTN dosing across a 4-week treatment period.
To address rebound potential, outcomes also were observed on the first night of nondosing after 1 or more nights of medication use. Dependence and tolerance also were examined.
The study found no evidence of residual sleepiness after MOTN dosing with zolpidem. Patients who received the drug actually reported greater alertness, compared with baseline. On a scale of 1–9 (with 9 being most alert), the mean score was 4.9 at baseline, increasing to 5.7 after zolpidem dosing. Scores in the placebo arm were 4.7 and 5.2, respectively.
Sleep quality also improved significantly. Mean scores were 4.7 at baseline and 5.8 after treatment with zolpidem, compared with 4.5 and 5.2, respectively, with placebo.
The study found no evidence for the development of tolerance to zolpidem's efficacy.
Latency to sleep onset improved over the first 2 weeks, and apparently stabilized by week 3, for both the active-treatment and placebo groups, suggesting a nonspecific trend toward improvement in outcome over time.
The response to the medication did not change across the entire treatment period, and drug use was not different between treatment and placebo groups, Dr. Roth reported.
In fact, weekly medication use showed a decline for both the active and placebo groups, with medication use during week 4 being significantly lower than during week 1 in both arms.
The mean number of tablets taken during weeks 1 and 4 were 4.9 and 4.0, respectively, for the zolpidem group and 4.9 and 4.3, respectively, for the placebo group. There was no evidence of rebound effects on sleep initiation or total sleep time on nondosing nights, regardless of the number of nights of continuous use.
On average, for nights during which zolpidem was not dosed, total sleep time was similar for the active and placebo groups.
Dr. Roth noted that the improvement over placebo of about 20 minutes is clinically meaningful.
“It doesn't sound impressive, but try sleeping 20 minutes less every night for 3 months — you'll be in a coma. The effect is cumulative. It's about 2 hours a week.”
{kind=link}
Middle-of-the-night awakening with difficulty falling back to sleep is a prevalent condition.
Source ©iStockphoto/redmonkey8
Major Finding: Persons who received a new formulation of low-dose sublingual zolpidem for middle-of-the-night insomnia showed no potential for abuse of the drug in the form of dependency, tolerance, or rebound potential, compared with placebo recipients.
Data Source: A 4-week outpatient study of 146 subjects.
Disclosures: Dr. Roth has served as a consultant to Transept Pharmaceuticals Inc., the manufacturer of the sublingual formulation of zolpidem tartrate. He has also received research support from and had other relationships with numerous pharmaceutical companies.
AMSTERDAM — A sublingual 3.5-mg formulation of zolpidem tartrate is effective for middle-of-the-night insomnia, producing no tolerance, rebound, or increase in use over a 4-week period, a study has shown.
“Awakening during the night with difficulty falling back to sleep is a prevalent condition, and a PRN treatment for this is needed as it may decrease overall drug exposure,” said the study's coinvestigator, Thomas Roth, Ph.D., of Henry Ford Hospital, Detroit.
Zolpidem sublingual tablets 3.5 mg and 1.75 mg were developed for the treatment of insomnia that is characterized by difficulty returning to sleep after middle-of-the-night (MOTN) awakening.
The compound is formulated with binary buffers to promote buccal absorption of a portion of the drug. This facilitates bioavailability, resulting in a rapid return to sleep.
Previous studies have found that sublingual zolpidem significantly reduces sleep latency after MOTN dosing.
In a sleep laboratory study, sleep latency time was approximately 28 minutes with placebo but just 10 minutes with zolpidem 3.5 mg (Sleep 2008;31:1277–84).
“This is a reduced dose of zolpidem, and importantly it is a sublingual formulation so you achieve much faster blood levels to help you fall back asleep but you reduce the total blood level as compared to taking it prophylactically. The concern is that over time, people take more and more of the medication,” Dr. Roth said at the meeting.
The drug is currently under review by the Food and Drug Administration for MOTN awakening.
In a study designed to address possible abuse liability associated with PRN use of the drug, 75 outpatients received zolpidem and 71 patients received placebo; all were assessed for latency to sleep onset after MOTN dosing across a 4-week treatment period.
To address rebound potential, outcomes also were observed on the first night of nondosing after 1 or more nights of medication use. Dependence and tolerance also were examined.
The study found no evidence of residual sleepiness after MOTN dosing with zolpidem. Patients who received the drug actually reported greater alertness, compared with baseline. On a scale of 1–9 (with 9 being most alert), the mean score was 4.9 at baseline, increasing to 5.7 after zolpidem dosing. Scores in the placebo arm were 4.7 and 5.2, respectively.
Sleep quality also improved significantly. Mean scores were 4.7 at baseline and 5.8 after treatment with zolpidem, compared with 4.5 and 5.2, respectively, with placebo.
The study found no evidence for the development of tolerance to zolpidem's efficacy.
Latency to sleep onset improved over the first 2 weeks, and apparently stabilized by week 3, for both the active-treatment and placebo groups, suggesting a nonspecific trend toward improvement in outcome over time.
The response to the medication did not change across the entire treatment period, and drug use was not different between treatment and placebo groups, Dr. Roth reported.
In fact, weekly medication use showed a decline for both the active and placebo groups, with medication use during week 4 being significantly lower than during week 1 in both arms.
The mean number of tablets taken during weeks 1 and 4 were 4.9 and 4.0, respectively, for the zolpidem group and 4.9 and 4.3, respectively, for the placebo group. There was no evidence of rebound effects on sleep initiation or total sleep time on nondosing nights, regardless of the number of nights of continuous use.
On average, for nights during which zolpidem was not dosed, total sleep time was similar for the active and placebo groups.
Dr. Roth noted that the improvement over placebo of about 20 minutes is clinically meaningful.
“It doesn't sound impressive, but try sleeping 20 minutes less every night for 3 months — you'll be in a coma. The effect is cumulative. It's about 2 hours a week.”
Middle-of-the-night awakening with difficulty falling back to sleep is a prevalent condition.
Source ©iStockphoto/redmonkey8
Major Finding: Persons who received a new formulation of low-dose sublingual zolpidem for middle-of-the-night insomnia showed no potential for abuse of the drug in the form of dependency, tolerance, or rebound potential, compared with placebo recipients.
Data Source: A 4-week outpatient study of 146 subjects.
Disclosures: Dr. Roth has served as a consultant to Transept Pharmaceuticals Inc., the manufacturer of the sublingual formulation of zolpidem tartrate. He has also received research support from and had other relationships with numerous pharmaceutical companies.
AMSTERDAM — A sublingual 3.5-mg formulation of zolpidem tartrate is effective for middle-of-the-night insomnia, producing no tolerance, rebound, or increase in use over a 4-week period, a study has shown.
“Awakening during the night with difficulty falling back to sleep is a prevalent condition, and a PRN treatment for this is needed as it may decrease overall drug exposure,” said the study's coinvestigator, Thomas Roth, Ph.D., of Henry Ford Hospital, Detroit.
Zolpidem sublingual tablets 3.5 mg and 1.75 mg were developed for the treatment of insomnia that is characterized by difficulty returning to sleep after middle-of-the-night (MOTN) awakening.
The compound is formulated with binary buffers to promote buccal absorption of a portion of the drug. This facilitates bioavailability, resulting in a rapid return to sleep.
Previous studies have found that sublingual zolpidem significantly reduces sleep latency after MOTN dosing.
In a sleep laboratory study, sleep latency time was approximately 28 minutes with placebo but just 10 minutes with zolpidem 3.5 mg (Sleep 2008;31:1277–84).
“This is a reduced dose of zolpidem, and importantly it is a sublingual formulation so you achieve much faster blood levels to help you fall back asleep but you reduce the total blood level as compared to taking it prophylactically. The concern is that over time, people take more and more of the medication,” Dr. Roth said at the meeting.
The drug is currently under review by the Food and Drug Administration for MOTN awakening.
In a study designed to address possible abuse liability associated with PRN use of the drug, 75 outpatients received zolpidem and 71 patients received placebo; all were assessed for latency to sleep onset after MOTN dosing across a 4-week treatment period.
To address rebound potential, outcomes also were observed on the first night of nondosing after 1 or more nights of medication use. Dependence and tolerance also were examined.
The study found no evidence of residual sleepiness after MOTN dosing with zolpidem. Patients who received the drug actually reported greater alertness, compared with baseline. On a scale of 1–9 (with 9 being most alert), the mean score was 4.9 at baseline, increasing to 5.7 after zolpidem dosing. Scores in the placebo arm were 4.7 and 5.2, respectively.
Sleep quality also improved significantly. Mean scores were 4.7 at baseline and 5.8 after treatment with zolpidem, compared with 4.5 and 5.2, respectively, with placebo.
The study found no evidence for the development of tolerance to zolpidem's efficacy.
Latency to sleep onset improved over the first 2 weeks, and apparently stabilized by week 3, for both the active-treatment and placebo groups, suggesting a nonspecific trend toward improvement in outcome over time.
The response to the medication did not change across the entire treatment period, and drug use was not different between treatment and placebo groups, Dr. Roth reported.
In fact, weekly medication use showed a decline for both the active and placebo groups, with medication use during week 4 being significantly lower than during week 1 in both arms.
The mean number of tablets taken during weeks 1 and 4 were 4.9 and 4.0, respectively, for the zolpidem group and 4.9 and 4.3, respectively, for the placebo group. There was no evidence of rebound effects on sleep initiation or total sleep time on nondosing nights, regardless of the number of nights of continuous use.
On average, for nights during which zolpidem was not dosed, total sleep time was similar for the active and placebo groups.
Dr. Roth noted that the improvement over placebo of about 20 minutes is clinically meaningful.
“It doesn't sound impressive, but try sleeping 20 minutes less every night for 3 months — you'll be in a coma. The effect is cumulative. It's about 2 hours a week.”
Middle-of-the-night awakening with difficulty falling back to sleep is a prevalent condition.
Source ©iStockphoto/redmonkey8
Sleep Disturbances May Be Target in PTSD Treatment
BOSTON — Sleep disturbances may be an important target for treating posttraumatic stress disorder, according to Dr. R. Bruce Lydiard of the Medical University of South Carolina in Charleston.
Persistent, severe posttraumatic nightmares, REM sleep fragmentation, insomnia, excessive nocturnal periodic limb movements, and sleep-disordered breathing are frequently experienced by individuals with PTSD, Dr. Lydiard said. Although these sleep problems are often viewed as secondary symptoms of PTSD, “the evidence suggests that after a traumatic event, sleep disruption appears before the onset of PTSD and may be a risk factor for it,” he proposed.
Polysomnographic data from 21 individuals with traumatic injuries showed that the number of REM periods and the (shorter) duration of REM periods within 1 month after the traumatic event were predictive of PTSD symptom severity 6 weeks later (Am. J. Psychiatry. 2002;159:1696–701).
Neurobiologically, the association makes sense, Dr. Lydiard said. “Sleep is regulated in part by brain areas in which PTSD-related changes occur,” which suggests that the stress response in PTSD and sleep dysfunction may be biologically linked.
Imaging studies suggest that exposure to trauma-related stimuli leads to hyperactivation in the amygdala and decreased activation in the medial prefrontal cortex/anterior cingulate cortex and hippocampus, with the magnitude of the activation correlating with the clinical severity of PTSD symptoms.
Polysomnographic investigations in patients with PTSD and sleep disturbances have revealed increased REM density, reduced REM duration, and increased motor activity, Dr. Lydiard said.
Together with clinical reports, “these data provide the basis for REM sleep dysregulation as a core feature in PTSD,” whereby increased activity in the amygdala and decreased inhibitory input from the medial prefrontal cortex lead to a persistently overactive noradrenergic system. “As a result, the usual rhythm of REM-NREM sleep is disrupted, and REM sleep is fragmented,” he said.
Based on this model, investigators have hypothesized that targeting noradrenergic signaling during or near REM episodes may normalize REM sleep, which in turn might improve PTSD sleep disturbances and, potentially, other PTSD symptoms, Dr. Lydiard said.
The alpha adrenergic antagonist prazosin has shown promise in multiple case and chart reviews, open-label trials, and placebo-controlled studies.
In one trial of 40 veterans with PTSD sleep disturbance, patients who were randomized to receive a nightly dose of prazosin — originally marketed as an antihypertensive agent — reported significant improvements in sleep quality and significant reductions in trauma nightmares, as well a better overall sense of well-being and improved daily functioning (Biol. Psychiatry 2007;61:928–34).
In another study, investigators evaluated the effect of prazosin vs. placebo on objective sleep parameters in 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance. The prazosin group experienced significantly increased total sleep time as well as increased REM sleep time and mean REM period duration (Biol. Psychiatry 2008;63:629–32).
In the various studies, the therapeutic benefit of prazosin was achieved within 1–2 weeks “with doses as low as 1 mg nightly,” Dr. Lydiard said.
In addition to improving sleep measures, prazosin may be useful for other trauma-related symptoms. In a small study of PTSD subjects whose nightmares were well controlled with the drug, the addition of small daytime doses lessened patients' reactivity to trauma cues during the day, he said (Biol. Psychiatry 2006;59:577–81). This finding “adds to the growing body of evidence that targeting sleep in PTSD is clinically relevant.”
Although some evidence exists to support the use of other antiadrenergic agents such as clonidine and guanfacine—as well as the anticonvulsant gabapentin—in PTSD, “large, randomized controlled trials are needed to clarify the role” of all of these agents, Dr. Lydiard said.
Additional studies also are warranted, he said, to investigate nonpharmacologic approaches to improving PTSD sleep disturbance, such as the use of imagery rehearsal therapy, which has demonstrated efficacy in small studies (J. Trauma. Stress 2009;22:236–9).
Dr. Lydiard disclosed receiving honoraria from Reed Medical Education, the logistics collaborator for the Massachusetts General Hospital Psychiatry Academy.
BOSTON — Sleep disturbances may be an important target for treating posttraumatic stress disorder, according to Dr. R. Bruce Lydiard of the Medical University of South Carolina in Charleston.
Persistent, severe posttraumatic nightmares, REM sleep fragmentation, insomnia, excessive nocturnal periodic limb movements, and sleep-disordered breathing are frequently experienced by individuals with PTSD, Dr. Lydiard said. Although these sleep problems are often viewed as secondary symptoms of PTSD, “the evidence suggests that after a traumatic event, sleep disruption appears before the onset of PTSD and may be a risk factor for it,” he proposed.
Polysomnographic data from 21 individuals with traumatic injuries showed that the number of REM periods and the (shorter) duration of REM periods within 1 month after the traumatic event were predictive of PTSD symptom severity 6 weeks later (Am. J. Psychiatry. 2002;159:1696–701).
Neurobiologically, the association makes sense, Dr. Lydiard said. “Sleep is regulated in part by brain areas in which PTSD-related changes occur,” which suggests that the stress response in PTSD and sleep dysfunction may be biologically linked.
Imaging studies suggest that exposure to trauma-related stimuli leads to hyperactivation in the amygdala and decreased activation in the medial prefrontal cortex/anterior cingulate cortex and hippocampus, with the magnitude of the activation correlating with the clinical severity of PTSD symptoms.
Polysomnographic investigations in patients with PTSD and sleep disturbances have revealed increased REM density, reduced REM duration, and increased motor activity, Dr. Lydiard said.
Together with clinical reports, “these data provide the basis for REM sleep dysregulation as a core feature in PTSD,” whereby increased activity in the amygdala and decreased inhibitory input from the medial prefrontal cortex lead to a persistently overactive noradrenergic system. “As a result, the usual rhythm of REM-NREM sleep is disrupted, and REM sleep is fragmented,” he said.
Based on this model, investigators have hypothesized that targeting noradrenergic signaling during or near REM episodes may normalize REM sleep, which in turn might improve PTSD sleep disturbances and, potentially, other PTSD symptoms, Dr. Lydiard said.
The alpha adrenergic antagonist prazosin has shown promise in multiple case and chart reviews, open-label trials, and placebo-controlled studies.
In one trial of 40 veterans with PTSD sleep disturbance, patients who were randomized to receive a nightly dose of prazosin — originally marketed as an antihypertensive agent — reported significant improvements in sleep quality and significant reductions in trauma nightmares, as well a better overall sense of well-being and improved daily functioning (Biol. Psychiatry 2007;61:928–34).
In another study, investigators evaluated the effect of prazosin vs. placebo on objective sleep parameters in 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance. The prazosin group experienced significantly increased total sleep time as well as increased REM sleep time and mean REM period duration (Biol. Psychiatry 2008;63:629–32).
In the various studies, the therapeutic benefit of prazosin was achieved within 1–2 weeks “with doses as low as 1 mg nightly,” Dr. Lydiard said.
In addition to improving sleep measures, prazosin may be useful for other trauma-related symptoms. In a small study of PTSD subjects whose nightmares were well controlled with the drug, the addition of small daytime doses lessened patients' reactivity to trauma cues during the day, he said (Biol. Psychiatry 2006;59:577–81). This finding “adds to the growing body of evidence that targeting sleep in PTSD is clinically relevant.”
Although some evidence exists to support the use of other antiadrenergic agents such as clonidine and guanfacine—as well as the anticonvulsant gabapentin—in PTSD, “large, randomized controlled trials are needed to clarify the role” of all of these agents, Dr. Lydiard said.
Additional studies also are warranted, he said, to investigate nonpharmacologic approaches to improving PTSD sleep disturbance, such as the use of imagery rehearsal therapy, which has demonstrated efficacy in small studies (J. Trauma. Stress 2009;22:236–9).
Dr. Lydiard disclosed receiving honoraria from Reed Medical Education, the logistics collaborator for the Massachusetts General Hospital Psychiatry Academy.
BOSTON — Sleep disturbances may be an important target for treating posttraumatic stress disorder, according to Dr. R. Bruce Lydiard of the Medical University of South Carolina in Charleston.
Persistent, severe posttraumatic nightmares, REM sleep fragmentation, insomnia, excessive nocturnal periodic limb movements, and sleep-disordered breathing are frequently experienced by individuals with PTSD, Dr. Lydiard said. Although these sleep problems are often viewed as secondary symptoms of PTSD, “the evidence suggests that after a traumatic event, sleep disruption appears before the onset of PTSD and may be a risk factor for it,” he proposed.
Polysomnographic data from 21 individuals with traumatic injuries showed that the number of REM periods and the (shorter) duration of REM periods within 1 month after the traumatic event were predictive of PTSD symptom severity 6 weeks later (Am. J. Psychiatry. 2002;159:1696–701).
Neurobiologically, the association makes sense, Dr. Lydiard said. “Sleep is regulated in part by brain areas in which PTSD-related changes occur,” which suggests that the stress response in PTSD and sleep dysfunction may be biologically linked.
Imaging studies suggest that exposure to trauma-related stimuli leads to hyperactivation in the amygdala and decreased activation in the medial prefrontal cortex/anterior cingulate cortex and hippocampus, with the magnitude of the activation correlating with the clinical severity of PTSD symptoms.
Polysomnographic investigations in patients with PTSD and sleep disturbances have revealed increased REM density, reduced REM duration, and increased motor activity, Dr. Lydiard said.
Together with clinical reports, “these data provide the basis for REM sleep dysregulation as a core feature in PTSD,” whereby increased activity in the amygdala and decreased inhibitory input from the medial prefrontal cortex lead to a persistently overactive noradrenergic system. “As a result, the usual rhythm of REM-NREM sleep is disrupted, and REM sleep is fragmented,” he said.
Based on this model, investigators have hypothesized that targeting noradrenergic signaling during or near REM episodes may normalize REM sleep, which in turn might improve PTSD sleep disturbances and, potentially, other PTSD symptoms, Dr. Lydiard said.
The alpha adrenergic antagonist prazosin has shown promise in multiple case and chart reviews, open-label trials, and placebo-controlled studies.
In one trial of 40 veterans with PTSD sleep disturbance, patients who were randomized to receive a nightly dose of prazosin — originally marketed as an antihypertensive agent — reported significant improvements in sleep quality and significant reductions in trauma nightmares, as well a better overall sense of well-being and improved daily functioning (Biol. Psychiatry 2007;61:928–34).
In another study, investigators evaluated the effect of prazosin vs. placebo on objective sleep parameters in 13 outpatients with chronic civilian trauma PTSD, frequent nightmares, and sleep disturbance. The prazosin group experienced significantly increased total sleep time as well as increased REM sleep time and mean REM period duration (Biol. Psychiatry 2008;63:629–32).
In the various studies, the therapeutic benefit of prazosin was achieved within 1–2 weeks “with doses as low as 1 mg nightly,” Dr. Lydiard said.
In addition to improving sleep measures, prazosin may be useful for other trauma-related symptoms. In a small study of PTSD subjects whose nightmares were well controlled with the drug, the addition of small daytime doses lessened patients' reactivity to trauma cues during the day, he said (Biol. Psychiatry 2006;59:577–81). This finding “adds to the growing body of evidence that targeting sleep in PTSD is clinically relevant.”
Although some evidence exists to support the use of other antiadrenergic agents such as clonidine and guanfacine—as well as the anticonvulsant gabapentin—in PTSD, “large, randomized controlled trials are needed to clarify the role” of all of these agents, Dr. Lydiard said.
Additional studies also are warranted, he said, to investigate nonpharmacologic approaches to improving PTSD sleep disturbance, such as the use of imagery rehearsal therapy, which has demonstrated efficacy in small studies (J. Trauma. Stress 2009;22:236–9).
Dr. Lydiard disclosed receiving honoraria from Reed Medical Education, the logistics collaborator for the Massachusetts General Hospital Psychiatry Academy.
Lack of Sleep Is Linked To Psychological Distress
Major Finding: A 14% increased likelihood of high psychological distress was linked with each hour fewer than 8 slept, on average, per night among young adults.
Data Source: Prospective cohort study of responses from 19,648 young adults surveyed at baseline and from 2,937 resurveyed 12–18 months later.
Disclosures: There was no industry support for the study. Dr. Nicholas Glozier is on the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Coauthor Dr. Ian Hickie formerly served as CEO and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects funded by drug industry partners. The others reported no conflicts.
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation — a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night — after they controlled for possible confounders. Sleeping 8–9 hours per night is recommended.
A total of 19,648 Australians (aged 17–24 years) reported their sleep hours for the previous month in a survey of registered drivers.
Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine.
Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7–8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139–45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12–18 months later.
They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline.
In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). The risk was most pronounced among those who reported an average 5 hours or fewer of sleep (RR, 3.25), compared with the other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted.
Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new-onset psychological distress by asking about sleep duration.
Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use).
Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration.
Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97–106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%).
The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm.
The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation.
In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
Major Finding: A 14% increased likelihood of high psychological distress was linked with each hour fewer than 8 slept, on average, per night among young adults.
Data Source: Prospective cohort study of responses from 19,648 young adults surveyed at baseline and from 2,937 resurveyed 12–18 months later.
Disclosures: There was no industry support for the study. Dr. Nicholas Glozier is on the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Coauthor Dr. Ian Hickie formerly served as CEO and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects funded by drug industry partners. The others reported no conflicts.
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation — a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night — after they controlled for possible confounders. Sleeping 8–9 hours per night is recommended.
A total of 19,648 Australians (aged 17–24 years) reported their sleep hours for the previous month in a survey of registered drivers.
Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine.
Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7–8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139–45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12–18 months later.
They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline.
In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). The risk was most pronounced among those who reported an average 5 hours or fewer of sleep (RR, 3.25), compared with the other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted.
Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new-onset psychological distress by asking about sleep duration.
Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use).
Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration.
Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97–106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%).
The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm.
The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation.
In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
Major Finding: A 14% increased likelihood of high psychological distress was linked with each hour fewer than 8 slept, on average, per night among young adults.
Data Source: Prospective cohort study of responses from 19,648 young adults surveyed at baseline and from 2,937 resurveyed 12–18 months later.
Disclosures: There was no industry support for the study. Dr. Nicholas Glozier is on the Sanofi-Aventis advisory board and is a speaker for CSL Laboratories. Coauthor Dr. Ian Hickie formerly served as CEO and clinical adviser for Beyondblue, the Australian National Depression Initiative, and has led projects funded by drug industry partners. The others reported no conflicts.
Young adults who report sleeping fewer hours per night on average than do their counterparts are at elevated risk for persistent or new-onset psychological distress, according to results of a large, prospective cohort study.
Researchers found a linear correlation — a 14% greater risk for higher psychological distress for each hour slept fewer than 8, on average, per night — after they controlled for possible confounders. Sleeping 8–9 hours per night is recommended.
A total of 19,648 Australians (aged 17–24 years) reported their sleep hours for the previous month in a survey of registered drivers.
Researchers found almost one-third (32.5%) had high baseline levels of psychological distress (defined as a score greater than 21 on the K10 (Kessler Psychological Distress Scale), a 10-item instrument that screens for feeling “tired out for no reason,” nervous, hopeless, restless, or depressed during the previous 4 weeks.
Psychological distress was most acute among the fewer than 2% of young adults who reported sleeping an average 5 hours or fewer per night, representing a group that might benefit the most from an intervention to improve their sleep routine.
Another 18% reported sleeping an average 7 hours or fewer per night, and 30% reported sleeping 7–8 hours each night.
The full findings of the study were published in the September issue of the journal Sleep (2010;33:1139–45).
Lead researcher Dr. Nicholas Glozier and his associates also resurveyed a random sample of 2,937 respondents 12–18 months later.
They found that high levels of distress persisted for 32% of the 945 who were initially distressed at baseline.
In addition, 12% of those with no initial elevated distress (239 of 1992 respondents) had new-onset distress 1 year later, reported Dr. Glozier, who is on the psychological medicine faculty at the Brain and Mind Research Institute at the University of Sydney.
Again, a linear association was found between shorter sleep duration and likelihood for onset of psychological distress (relative risk, 1.12). The risk was most pronounced among those who reported an average 5 hours or fewer of sleep (RR, 3.25), compared with the other participants.
This is the first prospective study to link shorter sleep duration in young adults with increased psychological distress, the researchers noted.
Interestingly, there was no increased risk of psychological distress at any time in the study among those who reported sleeping an average 9 hours or more per night.
Based on these findings, clinicians could potentially identify young adults who are at elevated risk for persistent or new-onset psychological distress by asking about sleep duration.
Also, because young adulthood is a time when elevated psychological distress could develop into depression and many other psychiatric conditions, short sleep duration could be an important marker for early intervention, the authors wrote.
The authors acknowledged the difficulty associated with any populationwide effort to improve sleep (such as reducing late-night television viewing, computer gaming, and Internet use).
Instead, they recommend that clinicians identify and focus their efforts on young adults who are at highest risk: those who report current distress or extremely short sleep duration.
Other researchers demonstrated an association between short sleep duration and later bedtimes with depressed mood and suicidal ideation among adolescents (Sleep 2010;33:97–106).
High psychological distress was more common among females (40%, compared with 28% of males). It was also higher among those who reported unemployment (33% vs. 28% of those employed); drug use (45% vs. 32%); harmful alcohol use (38% vs. 32%); high sensation-seeking behavior (44% vs. 22%), and recent deliberate self-harm (70% vs. 31%).
The researchers controlled for these potential confounders in the study.
Predictors of persistent distress included initial symptom severity, older age, and recent attempts at self-harm.
The authors termed presence of elevated distress at baseline and follow-up as “persistent,” but said that taking measurements at only two time points is a potential limitation.
In addition, the cohort was derived from driving registration records and might not be representative of the entire population of 17- to 24-year-olds.
Smoking More Harmful Than Sedentary Lifestyle
CRYSTAL CITY, VA. — The combination of smoking and an active lifestyle was associated with significantly worse lung function than was the combination of nonsmoking and a sedentary lifestyle in blacks, on the basis of data from more than 3,000 participants in the Jackson Heart Study.
Previous studies have shown that the poor lung function associated with a sedentary lifestyle can significantly predict cardiovascular problems, said Brenda Campbell Jenkins, Ph.D., and her colleagues at Jackson (Miss.) State University. Additional research suggests that blacks might be especially vulnerable to lung damage from smoking, they noted.
But no study has examined the combined effects of smoking and sedentary lifestyle and their effects on lung function, Dr. Campbell Jenkins said in an interview.
“We know that among African Americans there is a low prevalence of smoking and a high prevalence of sedentary lifestyle,” she said.
In this study, the researchers examined the joint effect of smoking and sedentary lifestyle on heart health in blacks, using data from the Jackson Heart Study, a population-based observational study including black adults aged 21–94 years living in the area of Jackson, Miss.
The researchers measured pulmonary function using forced vital capacity (FVC) and forced expiratory volume per second (FEV1). The study findings were presented in a poster at the meeting.
The participants were divided into four groups: nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary. Sedentary lifestyle was defined as the lowest quartile of physical activity.
The mean percentages of predicted FEV1 values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups were 95%, 94%, 89%, and 85%. The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after controlling for multiple variables.
The mean percentages of predicted FVC values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups was 94%, 92%, 89%, and 88%, respectively.
The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after adjustment for multiple variables.
For men, the mean percentages of predicted FEV1 values in the four groups were 93%, 89%, 88%, 76%, respectively, but these differences were not significant. In addition, the mean percentages of predicted FVC values in each group were 91%, 88%, 91%, and 80%, respectively, and these differences were not significant.
However, after controlling for multiple variables, the mean FEV1 to FVC ratio was significantly higher among men in the nonsmoking sedentary group, compared with the smoking nonsedentary group (78.8 vs. 77.5).
Based on these findings, smoking and sedentary lifestyle were both negatively associated with lung function, but smoking tended to have more harmful effects, which was consistent with the literature, noted Dr. Sarpong, director, co—principal investigator, and senior biostatistician of the Jackson Heart Study.
However, more research is needed to determine the clinical implications of the findings.
Study participants were enrolled during 2000–2004. The current study included 1,191 men and 2,065 women aged 21–93 years (average, 54 years). Participants with prevalent cardiovascular disease, asthma, and incomplete measures of smoking or lung function were excluded.
The researchers had no financial conflicts to disclose. The study was supported by grants from the National Heart, Lung, and Blood Institute and the National Center for Minority Health and Health Disparities.
CRYSTAL CITY, VA. — The combination of smoking and an active lifestyle was associated with significantly worse lung function than was the combination of nonsmoking and a sedentary lifestyle in blacks, on the basis of data from more than 3,000 participants in the Jackson Heart Study.
Previous studies have shown that the poor lung function associated with a sedentary lifestyle can significantly predict cardiovascular problems, said Brenda Campbell Jenkins, Ph.D., and her colleagues at Jackson (Miss.) State University. Additional research suggests that blacks might be especially vulnerable to lung damage from smoking, they noted.
But no study has examined the combined effects of smoking and sedentary lifestyle and their effects on lung function, Dr. Campbell Jenkins said in an interview.
“We know that among African Americans there is a low prevalence of smoking and a high prevalence of sedentary lifestyle,” she said.
In this study, the researchers examined the joint effect of smoking and sedentary lifestyle on heart health in blacks, using data from the Jackson Heart Study, a population-based observational study including black adults aged 21–94 years living in the area of Jackson, Miss.
The researchers measured pulmonary function using forced vital capacity (FVC) and forced expiratory volume per second (FEV1). The study findings were presented in a poster at the meeting.
The participants were divided into four groups: nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary. Sedentary lifestyle was defined as the lowest quartile of physical activity.
The mean percentages of predicted FEV1 values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups were 95%, 94%, 89%, and 85%. The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after controlling for multiple variables.
The mean percentages of predicted FVC values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups was 94%, 92%, 89%, and 88%, respectively.
The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after adjustment for multiple variables.
For men, the mean percentages of predicted FEV1 values in the four groups were 93%, 89%, 88%, 76%, respectively, but these differences were not significant. In addition, the mean percentages of predicted FVC values in each group were 91%, 88%, 91%, and 80%, respectively, and these differences were not significant.
However, after controlling for multiple variables, the mean FEV1 to FVC ratio was significantly higher among men in the nonsmoking sedentary group, compared with the smoking nonsedentary group (78.8 vs. 77.5).
Based on these findings, smoking and sedentary lifestyle were both negatively associated with lung function, but smoking tended to have more harmful effects, which was consistent with the literature, noted Dr. Sarpong, director, co—principal investigator, and senior biostatistician of the Jackson Heart Study.
However, more research is needed to determine the clinical implications of the findings.
Study participants were enrolled during 2000–2004. The current study included 1,191 men and 2,065 women aged 21–93 years (average, 54 years). Participants with prevalent cardiovascular disease, asthma, and incomplete measures of smoking or lung function were excluded.
The researchers had no financial conflicts to disclose. The study was supported by grants from the National Heart, Lung, and Blood Institute and the National Center for Minority Health and Health Disparities.
CRYSTAL CITY, VA. — The combination of smoking and an active lifestyle was associated with significantly worse lung function than was the combination of nonsmoking and a sedentary lifestyle in blacks, on the basis of data from more than 3,000 participants in the Jackson Heart Study.
Previous studies have shown that the poor lung function associated with a sedentary lifestyle can significantly predict cardiovascular problems, said Brenda Campbell Jenkins, Ph.D., and her colleagues at Jackson (Miss.) State University. Additional research suggests that blacks might be especially vulnerable to lung damage from smoking, they noted.
But no study has examined the combined effects of smoking and sedentary lifestyle and their effects on lung function, Dr. Campbell Jenkins said in an interview.
“We know that among African Americans there is a low prevalence of smoking and a high prevalence of sedentary lifestyle,” she said.
In this study, the researchers examined the joint effect of smoking and sedentary lifestyle on heart health in blacks, using data from the Jackson Heart Study, a population-based observational study including black adults aged 21–94 years living in the area of Jackson, Miss.
The researchers measured pulmonary function using forced vital capacity (FVC) and forced expiratory volume per second (FEV1). The study findings were presented in a poster at the meeting.
The participants were divided into four groups: nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary. Sedentary lifestyle was defined as the lowest quartile of physical activity.
The mean percentages of predicted FEV1 values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups were 95%, 94%, 89%, and 85%. The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after controlling for multiple variables.
The mean percentages of predicted FVC values in women in the nonsmoking nonsedentary, nonsmoking sedentary, smoking nonsedentary, and smoking sedentary groups was 94%, 92%, 89%, and 88%, respectively.
The differences between women in the nonsmoking sedentary and in the smoking nonsedentary groups were significant after adjustment for multiple variables.
For men, the mean percentages of predicted FEV1 values in the four groups were 93%, 89%, 88%, 76%, respectively, but these differences were not significant. In addition, the mean percentages of predicted FVC values in each group were 91%, 88%, 91%, and 80%, respectively, and these differences were not significant.
However, after controlling for multiple variables, the mean FEV1 to FVC ratio was significantly higher among men in the nonsmoking sedentary group, compared with the smoking nonsedentary group (78.8 vs. 77.5).
Based on these findings, smoking and sedentary lifestyle were both negatively associated with lung function, but smoking tended to have more harmful effects, which was consistent with the literature, noted Dr. Sarpong, director, co—principal investigator, and senior biostatistician of the Jackson Heart Study.
However, more research is needed to determine the clinical implications of the findings.
Study participants were enrolled during 2000–2004. The current study included 1,191 men and 2,065 women aged 21–93 years (average, 54 years). Participants with prevalent cardiovascular disease, asthma, and incomplete measures of smoking or lung function were excluded.
The researchers had no financial conflicts to disclose. The study was supported by grants from the National Heart, Lung, and Blood Institute and the National Center for Minority Health and Health Disparities.
Asthma Admissions Drop After Smoking Ban
Pediatric asthma hospitalizations decreased by about 20% per year after a ban on smoking in enclosed public spaces was enacted in Scotland, said Daniel Mackay, Ph.D., of the University of Glasgow and his associates.
Before the legislation was implemented, there was concern that people might transfer their smoking from public areas to their homes, “leading paradoxically to an increase in exposure … among children,” they said (N. Engl. J. Med. 2010;363:1139–45).
Such displacement of smoking activity has not occurred. Instead, the results support the conclusion of another study that found that the public ban on smoking was followed by an increase in voluntary smoking restrictions in homes as well, the investigators said.
They used government databases to identify all 21,415 asthma admissions across Scotland from January 2000 through October 2009 for children younger than 15 years.
In the period from 2000 until implementation of the smoking ban in 2006, hospital admissions for asthma rose an adjusted average of 4.4% per year.
In the period after the smoking ban was enacted, the risk-adjusted annual rate of pediatric asthma admissions declined 19.5%, a statistically significant difference. The rate of asthma hospitalizations decreased both in preschool and school-age children, Dr. Mackay and his colleagues said.
NHS Health Scotland funded the study. The investigators had no relevant conflicts of interest.
Pediatric asthma hospitalizations decreased by about 20% per year after a ban on smoking in enclosed public spaces was enacted in Scotland, said Daniel Mackay, Ph.D., of the University of Glasgow and his associates.
Before the legislation was implemented, there was concern that people might transfer their smoking from public areas to their homes, “leading paradoxically to an increase in exposure … among children,” they said (N. Engl. J. Med. 2010;363:1139–45).
Such displacement of smoking activity has not occurred. Instead, the results support the conclusion of another study that found that the public ban on smoking was followed by an increase in voluntary smoking restrictions in homes as well, the investigators said.
They used government databases to identify all 21,415 asthma admissions across Scotland from January 2000 through October 2009 for children younger than 15 years.
In the period from 2000 until implementation of the smoking ban in 2006, hospital admissions for asthma rose an adjusted average of 4.4% per year.
In the period after the smoking ban was enacted, the risk-adjusted annual rate of pediatric asthma admissions declined 19.5%, a statistically significant difference. The rate of asthma hospitalizations decreased both in preschool and school-age children, Dr. Mackay and his colleagues said.
NHS Health Scotland funded the study. The investigators had no relevant conflicts of interest.
Pediatric asthma hospitalizations decreased by about 20% per year after a ban on smoking in enclosed public spaces was enacted in Scotland, said Daniel Mackay, Ph.D., of the University of Glasgow and his associates.
Before the legislation was implemented, there was concern that people might transfer their smoking from public areas to their homes, “leading paradoxically to an increase in exposure … among children,” they said (N. Engl. J. Med. 2010;363:1139–45).
Such displacement of smoking activity has not occurred. Instead, the results support the conclusion of another study that found that the public ban on smoking was followed by an increase in voluntary smoking restrictions in homes as well, the investigators said.
They used government databases to identify all 21,415 asthma admissions across Scotland from January 2000 through October 2009 for children younger than 15 years.
In the period from 2000 until implementation of the smoking ban in 2006, hospital admissions for asthma rose an adjusted average of 4.4% per year.
In the period after the smoking ban was enacted, the risk-adjusted annual rate of pediatric asthma admissions declined 19.5%, a statistically significant difference. The rate of asthma hospitalizations decreased both in preschool and school-age children, Dr. Mackay and his colleagues said.
NHS Health Scotland funded the study. The investigators had no relevant conflicts of interest.