User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Office-Based Aspirin Desensitization May Be Safe
SAN FRANCISCO – A small, retrospective study suggests that patients with aspirin-exacerbated respiratory disease may be safely desensitized to aspirin in an office setting rather than in a hospital.
Each of 15 patients who underwent a 1-day aspirin desensitization protocol in a clinic completed the protocol and ingested a cumulative total of 568 mg of aspirin on average by the end of the day. Each was then able to tolerate taking aspirin up to 650 mg b.i.d., Richard S. Dunn and Dr. Richard W. Hendershot reported in a poster presentation at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

In-hospital aspirin desensitization for patients with aspirin-exacerbated respiratory disease typically takes 2-3 days, and some clinicians recommend doing it in an ICU, said Mr. Dunn, a fourth-year medical student at the University of Utah, Salt Lake City. Dr. Hendershot is an allergy and immunology specialist with Intermountain Healthcare in Salt Lake City.
The outpatient protocol took 8-9 hours. The cost to desensitize a patient averaged $2,678 in the outpatient clinic, compared with an average daily cost for ICU care of $13,347 reported in the literature.
Desensitization started with application of intranasal ketorolac three times over half-hour intervals. Patients then ingested 81 mg of aspirin and increased the dose by 81 mg every 2 hours to a final dose of 325 mg.
They were closely monitored during the desensitization. No complications were seen in 56% of patients. FEV1 (forced expiratory volume in 1 second) decreased by more than 20% in 19% of patients; 13% of patients developed flushing, and dyspnea or urticaria was each seen in 6% of patients.
Approximately 21% of people with asthma and 40% of patients with asthma who are dependent on glucocorticoids have aspirin-exacerbated respiratory disease. These patients often present with asthma, chronic rhinosinusitis, and nasal polyps. If they ingest a cyclooxygenase-1 inhibitor, they develop asthma symptoms, rhinorrhea, periorbital edema, urticaria, pruritus, angioedema, anaphylaxis, or other symptoms.
The design of the desensitization protocol was borrowed from a similar protocol that was tested in a controlled study of 100 patients (Ann. Allergy Asthma Immunol. 2010;105:130-5).
A patient who could not afford desensitization in the hospital inspired the development of the outpatient protocol that was used in the study.
The results suggest that aspirin desensitization for the treatment of aspirin-exacerbated respiratory disease can be done safely and efficaciously in the outpatient setting in less time and with less cost, compared with inpatient treatment protocols, the investigators concluded.
The investigators reported having no conflicts of interest.
SAN FRANCISCO – A small, retrospective study suggests that patients with aspirin-exacerbated respiratory disease may be safely desensitized to aspirin in an office setting rather than in a hospital.
Each of 15 patients who underwent a 1-day aspirin desensitization protocol in a clinic completed the protocol and ingested a cumulative total of 568 mg of aspirin on average by the end of the day. Each was then able to tolerate taking aspirin up to 650 mg b.i.d., Richard S. Dunn and Dr. Richard W. Hendershot reported in a poster presentation at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In-hospital aspirin desensitization for patients with aspirin-exacerbated respiratory disease typically takes 2-3 days, and some clinicians recommend doing it in an ICU, said Mr. Dunn, a fourth-year medical student at the University of Utah, Salt Lake City. Dr. Hendershot is an allergy and immunology specialist with Intermountain Healthcare in Salt Lake City.
The outpatient protocol took 8-9 hours. The cost to desensitize a patient averaged $2,678 in the outpatient clinic, compared with an average daily cost for ICU care of $13,347 reported in the literature.
Desensitization started with application of intranasal ketorolac three times over half-hour intervals. Patients then ingested 81 mg of aspirin and increased the dose by 81 mg every 2 hours to a final dose of 325 mg.
They were closely monitored during the desensitization. No complications were seen in 56% of patients. FEV1 (forced expiratory volume in 1 second) decreased by more than 20% in 19% of patients; 13% of patients developed flushing, and dyspnea or urticaria was each seen in 6% of patients.
Approximately 21% of people with asthma and 40% of patients with asthma who are dependent on glucocorticoids have aspirin-exacerbated respiratory disease. These patients often present with asthma, chronic rhinosinusitis, and nasal polyps. If they ingest a cyclooxygenase-1 inhibitor, they develop asthma symptoms, rhinorrhea, periorbital edema, urticaria, pruritus, angioedema, anaphylaxis, or other symptoms.
The design of the desensitization protocol was borrowed from a similar protocol that was tested in a controlled study of 100 patients (Ann. Allergy Asthma Immunol. 2010;105:130-5).
A patient who could not afford desensitization in the hospital inspired the development of the outpatient protocol that was used in the study.
The results suggest that aspirin desensitization for the treatment of aspirin-exacerbated respiratory disease can be done safely and efficaciously in the outpatient setting in less time and with less cost, compared with inpatient treatment protocols, the investigators concluded.
The investigators reported having no conflicts of interest.
SAN FRANCISCO – A small, retrospective study suggests that patients with aspirin-exacerbated respiratory disease may be safely desensitized to aspirin in an office setting rather than in a hospital.
Each of 15 patients who underwent a 1-day aspirin desensitization protocol in a clinic completed the protocol and ingested a cumulative total of 568 mg of aspirin on average by the end of the day. Each was then able to tolerate taking aspirin up to 650 mg b.i.d., Richard S. Dunn and Dr. Richard W. Hendershot reported in a poster presentation at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In-hospital aspirin desensitization for patients with aspirin-exacerbated respiratory disease typically takes 2-3 days, and some clinicians recommend doing it in an ICU, said Mr. Dunn, a fourth-year medical student at the University of Utah, Salt Lake City. Dr. Hendershot is an allergy and immunology specialist with Intermountain Healthcare in Salt Lake City.
The outpatient protocol took 8-9 hours. The cost to desensitize a patient averaged $2,678 in the outpatient clinic, compared with an average daily cost for ICU care of $13,347 reported in the literature.
Desensitization started with application of intranasal ketorolac three times over half-hour intervals. Patients then ingested 81 mg of aspirin and increased the dose by 81 mg every 2 hours to a final dose of 325 mg.
They were closely monitored during the desensitization. No complications were seen in 56% of patients. FEV1 (forced expiratory volume in 1 second) decreased by more than 20% in 19% of patients; 13% of patients developed flushing, and dyspnea or urticaria was each seen in 6% of patients.
Approximately 21% of people with asthma and 40% of patients with asthma who are dependent on glucocorticoids have aspirin-exacerbated respiratory disease. These patients often present with asthma, chronic rhinosinusitis, and nasal polyps. If they ingest a cyclooxygenase-1 inhibitor, they develop asthma symptoms, rhinorrhea, periorbital edema, urticaria, pruritus, angioedema, anaphylaxis, or other symptoms.
The design of the desensitization protocol was borrowed from a similar protocol that was tested in a controlled study of 100 patients (Ann. Allergy Asthma Immunol. 2010;105:130-5).
A patient who could not afford desensitization in the hospital inspired the development of the outpatient protocol that was used in the study.
The results suggest that aspirin desensitization for the treatment of aspirin-exacerbated respiratory disease can be done safely and efficaciously in the outpatient setting in less time and with less cost, compared with inpatient treatment protocols, the investigators concluded.
The investigators reported having no conflicts of interest.
FROM A POSTER PRESENTATION AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Fifteen patients with aspirin-exacerbated respiratory disease tolerated desensitization to aspirin in an outpatient setting.
Data Source: Retrospective chart review of patients desensitized to aspirin using a 1-day protocol in a clinic.
Disclosures: The investigators reported having no conflicts of interest.
Montelukast May Lessen Pediatric Exercise-Induced Bronchospasm
SAN FRANCISCO – Compared with placebo, a single dose of montelukast attenuated exercise-induced bronchoconstriction in children within 2 hours and lasted through 24 hours post dose, results from a small study found.
Although this treatment effect of montelukast has been observed in previously published studies of adults with exercise-induced bronchoconstriction, this is the first analysis of its kind in children with the condition.

"The ability to take a single tablet and have it last for 24 hours is probably more meaningful for children than for adults, because children often engage in unplanned physical activities more than adults do," Dr. George Philip said in an interview during a poster session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a multicenter study, Dr. Philip, senior director of clinical research at Merck Research Laboratories, North Wales, Pa., and his associates enrolled 66 children aged 6-14 years with pre-exercise forced expiratory volume in 1 second (FEV1) of 70% predicted or greater and a maximum fall in FEV1 of 20% or greater at two screening exercise challenges performed on a treadmill. Study participants were randomized to receive single-dose montelukast (4 or 5 mg) or placebo before the exercise challenges were performed at 2 and 24 hours post dose.
The primary end point was maximum percent fall in FEV1 after exercise challenge 2 hours post dose. Secondary end points included maximum percent fall in FEV1 after the 24-hour postdose challenge and each of the following end points at 2 and 24 hours post dose: maximum percent fall in FEV1 categorized as less than 10%, 10%-20%, and greater than 20%; area under the curve during the 60 minutes post challenge; and time to recovery to within 5% of pre-exercise baseline.
The mean age of patients was 11 years, and 56% were male. About three-quarters (74.2%) were white, 16.7% were black, and 9.1% were from other ethnic groups.
Dr. Philip reported that the mean percent fall in FEV1 was significantly better after the 2-hour postdose exercise challenge in the montelukast treatment group, compared with the placebo group (15.3% vs. 20%, respectively). Patients in the montelukast group also fared significantly better, compared with their counterparts in the placebo group, in maximum percent fall in FEV1 after the 24-hour postdose exercise challenge (12.92% vs. 17.25%, respectively); the categorized maximum percent fall at 2 hours (P = .034) though not at 24 hours (P = .061); and area under the curve at 2 hours (P = .022) and 24 hours (P = .013).
There were few clinical adverse events and no serious drug-related adverse events.
Dr. Philip acknowledged that the controlled laboratory setting in which the exercise challenge took place is a limitation of the study. "Natural exercise may be different from what we did in the laboratory, where all the kids had to run on a treadmill and reach a certain heart rate so we could define a clear and reproducible exercise-induced response," he explained. "Based on that response to challenge, we showed a benefit. But the kind of exercise that’s done in a laboratory may or may not match what’s done in other settings. Also, because the use of a single dose of montelukast to prevent exercise-induced bronchoconstriction in children less than age 15 years is not currently approved by the FDA, this use is considered investigational."
Merck funded the study. Dr. Philip is a full-time employee of the company.
SAN FRANCISCO – Compared with placebo, a single dose of montelukast attenuated exercise-induced bronchoconstriction in children within 2 hours and lasted through 24 hours post dose, results from a small study found.
Although this treatment effect of montelukast has been observed in previously published studies of adults with exercise-induced bronchoconstriction, this is the first analysis of its kind in children with the condition.
"The ability to take a single tablet and have it last for 24 hours is probably more meaningful for children than for adults, because children often engage in unplanned physical activities more than adults do," Dr. George Philip said in an interview during a poster session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a multicenter study, Dr. Philip, senior director of clinical research at Merck Research Laboratories, North Wales, Pa., and his associates enrolled 66 children aged 6-14 years with pre-exercise forced expiratory volume in 1 second (FEV1) of 70% predicted or greater and a maximum fall in FEV1 of 20% or greater at two screening exercise challenges performed on a treadmill. Study participants were randomized to receive single-dose montelukast (4 or 5 mg) or placebo before the exercise challenges were performed at 2 and 24 hours post dose.
The primary end point was maximum percent fall in FEV1 after exercise challenge 2 hours post dose. Secondary end points included maximum percent fall in FEV1 after the 24-hour postdose challenge and each of the following end points at 2 and 24 hours post dose: maximum percent fall in FEV1 categorized as less than 10%, 10%-20%, and greater than 20%; area under the curve during the 60 minutes post challenge; and time to recovery to within 5% of pre-exercise baseline.
The mean age of patients was 11 years, and 56% were male. About three-quarters (74.2%) were white, 16.7% were black, and 9.1% were from other ethnic groups.
Dr. Philip reported that the mean percent fall in FEV1 was significantly better after the 2-hour postdose exercise challenge in the montelukast treatment group, compared with the placebo group (15.3% vs. 20%, respectively). Patients in the montelukast group also fared significantly better, compared with their counterparts in the placebo group, in maximum percent fall in FEV1 after the 24-hour postdose exercise challenge (12.92% vs. 17.25%, respectively); the categorized maximum percent fall at 2 hours (P = .034) though not at 24 hours (P = .061); and area under the curve at 2 hours (P = .022) and 24 hours (P = .013).
There were few clinical adverse events and no serious drug-related adverse events.
Dr. Philip acknowledged that the controlled laboratory setting in which the exercise challenge took place is a limitation of the study. "Natural exercise may be different from what we did in the laboratory, where all the kids had to run on a treadmill and reach a certain heart rate so we could define a clear and reproducible exercise-induced response," he explained. "Based on that response to challenge, we showed a benefit. But the kind of exercise that’s done in a laboratory may or may not match what’s done in other settings. Also, because the use of a single dose of montelukast to prevent exercise-induced bronchoconstriction in children less than age 15 years is not currently approved by the FDA, this use is considered investigational."
Merck funded the study. Dr. Philip is a full-time employee of the company.
SAN FRANCISCO – Compared with placebo, a single dose of montelukast attenuated exercise-induced bronchoconstriction in children within 2 hours and lasted through 24 hours post dose, results from a small study found.
Although this treatment effect of montelukast has been observed in previously published studies of adults with exercise-induced bronchoconstriction, this is the first analysis of its kind in children with the condition.
"The ability to take a single tablet and have it last for 24 hours is probably more meaningful for children than for adults, because children often engage in unplanned physical activities more than adults do," Dr. George Philip said in an interview during a poster session at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
In a multicenter study, Dr. Philip, senior director of clinical research at Merck Research Laboratories, North Wales, Pa., and his associates enrolled 66 children aged 6-14 years with pre-exercise forced expiratory volume in 1 second (FEV1) of 70% predicted or greater and a maximum fall in FEV1 of 20% or greater at two screening exercise challenges performed on a treadmill. Study participants were randomized to receive single-dose montelukast (4 or 5 mg) or placebo before the exercise challenges were performed at 2 and 24 hours post dose.
The primary end point was maximum percent fall in FEV1 after exercise challenge 2 hours post dose. Secondary end points included maximum percent fall in FEV1 after the 24-hour postdose challenge and each of the following end points at 2 and 24 hours post dose: maximum percent fall in FEV1 categorized as less than 10%, 10%-20%, and greater than 20%; area under the curve during the 60 minutes post challenge; and time to recovery to within 5% of pre-exercise baseline.
The mean age of patients was 11 years, and 56% were male. About three-quarters (74.2%) were white, 16.7% were black, and 9.1% were from other ethnic groups.
Dr. Philip reported that the mean percent fall in FEV1 was significantly better after the 2-hour postdose exercise challenge in the montelukast treatment group, compared with the placebo group (15.3% vs. 20%, respectively). Patients in the montelukast group also fared significantly better, compared with their counterparts in the placebo group, in maximum percent fall in FEV1 after the 24-hour postdose exercise challenge (12.92% vs. 17.25%, respectively); the categorized maximum percent fall at 2 hours (P = .034) though not at 24 hours (P = .061); and area under the curve at 2 hours (P = .022) and 24 hours (P = .013).
There were few clinical adverse events and no serious drug-related adverse events.
Dr. Philip acknowledged that the controlled laboratory setting in which the exercise challenge took place is a limitation of the study. "Natural exercise may be different from what we did in the laboratory, where all the kids had to run on a treadmill and reach a certain heart rate so we could define a clear and reproducible exercise-induced response," he explained. "Based on that response to challenge, we showed a benefit. But the kind of exercise that’s done in a laboratory may or may not match what’s done in other settings. Also, because the use of a single dose of montelukast to prevent exercise-induced bronchoconstriction in children less than age 15 years is not currently approved by the FDA, this use is considered investigational."
Merck funded the study. Dr. Philip is a full-time employee of the company.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: After an exercise challenge 2 hours post dose, the mean percent fall in FEV1 was significantly better in children who took a single dose of montelukast than in those who took placebo (15.3% vs. 20%, respectively). A similar association was observed after an exercise challenge 24 hours post dose (12.92% vs. 17.25%).
Data Source: A randomized trial of 66 children aged 6-14 years who had a history of exercise-induced bronchoconstriction or wheeze/shortness of breath with exercise.
Disclosures: Merck funded the study. Dr. Philip is a full-time employee of the company.
Study Supports Nonrigid Fixation for Chest Wall Reconstruction
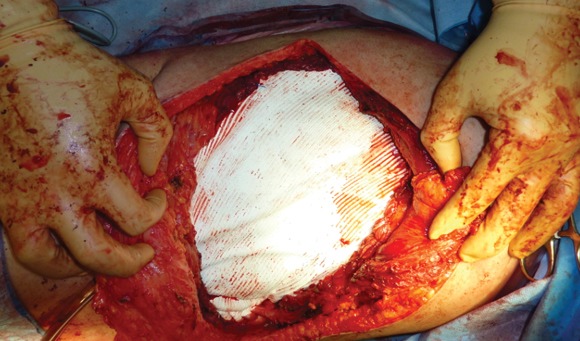
DETROIT – Chest wall reconstruction that uses nonrigid mesh or autologous tissue without rigid fixation was safe and provided excellent respiratory outcomes in one of the largest series to date.
"Our recommendations are to reconstruct with autologous tissue alone whenever possible," Dr. Waël Hanna said. "If you have to use mesh because you cannot reapproximate the chest wall or there’s not enough muscle to construct a flap, then nonrigid mesh should be favored over rigid fixation."

Rigid fixation with methacrylate or metallic plates and screws has conventionally been advocated as the best method to achieve chest wall stability and to maintain respiratory integrity following resection of chest wall tumors. However, these approaches are frequently complicated by motion deformities of the shoulder girdle, long-term cosmetic deformities, pain that limits daily activities, and a high morbidity of infection, Dr. Hanna explained at the annual meeting of the Central Surgical Association.
He reported on 37 patients who underwent major chest wall reconstruction in 2003-2010 with autologous tissue alone or with a soft prosthetic mesh. No patient underwent rigid fixation with methacrylate or plates and screws. The study excluded patients with concomitant lung or pleural resection to avoid confounding the respiratory outcomes.
Nine patients had a small defect (less than 60 cm2) and 28 patients had a large defect (greater than 60 cm2); no defect measured exactly 60 cm2, according to Dr. Hanna. The large-defect group was further divided into a subgroup of 16 patients who were reconstructed with soft mesh alone and a subgroup of 12 patients whose reconstruction was with autologous tissue alone and no mesh. Soft mesh was used in only one small-defect patient.
"We have turned away from using rigid prosthetics or methacrylate at our institution," said Dr. Hanna, a fifth-year resident with McGill University in Montreal.
Sarcoma was the most common indication for resection, followed by metastases to the chest wall, neurofibromas, and desmoid tumors. Reconstruction parameters were similar between the small- and large-defect cohorts, except for the mean size of the defect that was created in the chest wall (51 cm2 vs. 149 cm2), the dissection of three or more ribs (0% vs. 50%), and the use of soft mesh only (11% vs. 61%). A muscle flap to cover the prosthesis was used equally in both cohorts (56% vs. 75%).
The rate of immediate postoperative extubation was similar, at 100% in the small-defect cohort and 89% in the large-defect cohort, Dr. Hanna said. Only one patient was reintubated on postop day 1 and remained intubated for 3 days in the ICU.
None of the small-defect group went to the ICU for ventilation or flap monitoring, whereas 11% and 18% of the large-defect cohort did (P = .006 for both subgroups).
Pneumonia developed in three patients with large defects and in none with small defects (11% vs. 0%). One patient had to be re-extubated postoperatively, he said.
Secondary outcomes were also similar between the small- and large-defect groups, including site infection (0% vs. 7%) and reoperation rates (0% vs. 11%).
A subgroup analysis comparing patients with and without mesh revealed no significant differences in the primary outcomes of immediate extubation (100% vs. 75%), ICU stay for ventilation (6% vs. 25%), ICU stay for flap monitoring (13% vs. 17%), or pneumonia (6% vs. 8%).
The mesh and no-mesh subgroups were also nonsignificantly different with regard to site infection (13% vs. 0%) and reoperation (19% vs. 0%).
After a mean follow-up of 42 months (range, 36-84 months), there were no reports of infections beyond 30 postoperative days, long-term pain, restriction of mobility, or cosmetic disturbances. Patients were seen every 3 months for the first 2 years and every 6 months thereafter.
"For chest wall defects smaller than 60 cm2, reconstruction without a prosthesis has excellent outcomes," Dr. Hanna concluded. "For [defects] larger than 60 cm2, there does not seem to be any major difference between autologous tissue alone vs. nonrigid prosthesis reconstruction.
"Finally, nonrigid mesh seems to offer better short-term and long-term outcomes," compared with the historical data on rigid fixation, he said.
Invited discussant Dr. Fred Luchette, professor of surgery at Loyola University Medical Center in Chicago asked how the surgeons manage the often catastrophic event of mesh infection, and whether any long-term pulmonary function data were available, as the defects would likely prompt the development of some degree of paradoxical chest wall motion, even with the soft mesh.
Dr. Hanna replied that the retrospective nature of the series did not allow pulmonary function testing, and that the thoracic surgery community views such testing as less than ideal after reconstruction of the chest wall. A better measure is home oxygen use or limitation of daily activities, neither of which were observed in the cohort.
Dr. Hanna agreed that mesh infection is a highly morbid situation, especially with methacrylate or metallic prostheses, and that one of the benefits of soft prostheses like Vicryl or Gore-Tex is that they are able to respond to antibiotics.
Dr. Gerald Larson of University Surgical Associates in Louisville, Ky., who was also invited to discuss the study, asked how closure was achieved when mesh and a flap were not used, and why mesh and a muscle flap weren’t used for all patients.
Dr. Hanna responded that the risk of surgical site infection kept them from closing all patients with mesh and a muscle flap. The ideal method for closure is to mobilize enough local muscle that is present in the chest wall to reapproximate the muscle, and to close with skin without having to rotate a pedicle flap. When this is impossible, the defect has to be filled, and most surgeons at his institution elect to use soft mesh for the larger defects.
"In 75% of the time, on top of the mesh, we still mobilize a subcutaneous flap to cover the mesh because of the theoretical perception that a flap on top of the mesh would provide a good oxygenated environment and would decrease the rate of infection," Dr. Hanna said. The risk of surgical site infection kept them from closing all patients with mesh and a muscle flap, he added.
Dr. Hanna and his coauthors reported no relevant conflicts of interest.
DETROIT – Chest wall reconstruction that uses nonrigid mesh or autologous tissue without rigid fixation was safe and provided excellent respiratory outcomes in one of the largest series to date.
"Our recommendations are to reconstruct with autologous tissue alone whenever possible," Dr. Waël Hanna said. "If you have to use mesh because you cannot reapproximate the chest wall or there’s not enough muscle to construct a flap, then nonrigid mesh should be favored over rigid fixation."
Rigid fixation with methacrylate or metallic plates and screws has conventionally been advocated as the best method to achieve chest wall stability and to maintain respiratory integrity following resection of chest wall tumors. However, these approaches are frequently complicated by motion deformities of the shoulder girdle, long-term cosmetic deformities, pain that limits daily activities, and a high morbidity of infection, Dr. Hanna explained at the annual meeting of the Central Surgical Association.
He reported on 37 patients who underwent major chest wall reconstruction in 2003-2010 with autologous tissue alone or with a soft prosthetic mesh. No patient underwent rigid fixation with methacrylate or plates and screws. The study excluded patients with concomitant lung or pleural resection to avoid confounding the respiratory outcomes.
Nine patients had a small defect (less than 60 cm2) and 28 patients had a large defect (greater than 60 cm2); no defect measured exactly 60 cm2, according to Dr. Hanna. The large-defect group was further divided into a subgroup of 16 patients who were reconstructed with soft mesh alone and a subgroup of 12 patients whose reconstruction was with autologous tissue alone and no mesh. Soft mesh was used in only one small-defect patient.
"We have turned away from using rigid prosthetics or methacrylate at our institution," said Dr. Hanna, a fifth-year resident with McGill University in Montreal.
Sarcoma was the most common indication for resection, followed by metastases to the chest wall, neurofibromas, and desmoid tumors. Reconstruction parameters were similar between the small- and large-defect cohorts, except for the mean size of the defect that was created in the chest wall (51 cm2 vs. 149 cm2), the dissection of three or more ribs (0% vs. 50%), and the use of soft mesh only (11% vs. 61%). A muscle flap to cover the prosthesis was used equally in both cohorts (56% vs. 75%).
The rate of immediate postoperative extubation was similar, at 100% in the small-defect cohort and 89% in the large-defect cohort, Dr. Hanna said. Only one patient was reintubated on postop day 1 and remained intubated for 3 days in the ICU.
None of the small-defect group went to the ICU for ventilation or flap monitoring, whereas 11% and 18% of the large-defect cohort did (P = .006 for both subgroups).
Pneumonia developed in three patients with large defects and in none with small defects (11% vs. 0%). One patient had to be re-extubated postoperatively, he said.
Secondary outcomes were also similar between the small- and large-defect groups, including site infection (0% vs. 7%) and reoperation rates (0% vs. 11%).
A subgroup analysis comparing patients with and without mesh revealed no significant differences in the primary outcomes of immediate extubation (100% vs. 75%), ICU stay for ventilation (6% vs. 25%), ICU stay for flap monitoring (13% vs. 17%), or pneumonia (6% vs. 8%).
The mesh and no-mesh subgroups were also nonsignificantly different with regard to site infection (13% vs. 0%) and reoperation (19% vs. 0%).
After a mean follow-up of 42 months (range, 36-84 months), there were no reports of infections beyond 30 postoperative days, long-term pain, restriction of mobility, or cosmetic disturbances. Patients were seen every 3 months for the first 2 years and every 6 months thereafter.
"For chest wall defects smaller than 60 cm2, reconstruction without a prosthesis has excellent outcomes," Dr. Hanna concluded. "For [defects] larger than 60 cm2, there does not seem to be any major difference between autologous tissue alone vs. nonrigid prosthesis reconstruction.
"Finally, nonrigid mesh seems to offer better short-term and long-term outcomes," compared with the historical data on rigid fixation, he said.
Invited discussant Dr. Fred Luchette, professor of surgery at Loyola University Medical Center in Chicago asked how the surgeons manage the often catastrophic event of mesh infection, and whether any long-term pulmonary function data were available, as the defects would likely prompt the development of some degree of paradoxical chest wall motion, even with the soft mesh.
Dr. Hanna replied that the retrospective nature of the series did not allow pulmonary function testing, and that the thoracic surgery community views such testing as less than ideal after reconstruction of the chest wall. A better measure is home oxygen use or limitation of daily activities, neither of which were observed in the cohort.
Dr. Hanna agreed that mesh infection is a highly morbid situation, especially with methacrylate or metallic prostheses, and that one of the benefits of soft prostheses like Vicryl or Gore-Tex is that they are able to respond to antibiotics.
Dr. Gerald Larson of University Surgical Associates in Louisville, Ky., who was also invited to discuss the study, asked how closure was achieved when mesh and a flap were not used, and why mesh and a muscle flap weren’t used for all patients.
Dr. Hanna responded that the risk of surgical site infection kept them from closing all patients with mesh and a muscle flap. The ideal method for closure is to mobilize enough local muscle that is present in the chest wall to reapproximate the muscle, and to close with skin without having to rotate a pedicle flap. When this is impossible, the defect has to be filled, and most surgeons at his institution elect to use soft mesh for the larger defects.
"In 75% of the time, on top of the mesh, we still mobilize a subcutaneous flap to cover the mesh because of the theoretical perception that a flap on top of the mesh would provide a good oxygenated environment and would decrease the rate of infection," Dr. Hanna said. The risk of surgical site infection kept them from closing all patients with mesh and a muscle flap, he added.
Dr. Hanna and his coauthors reported no relevant conflicts of interest.
DETROIT – Chest wall reconstruction that uses nonrigid mesh or autologous tissue without rigid fixation was safe and provided excellent respiratory outcomes in one of the largest series to date.
"Our recommendations are to reconstruct with autologous tissue alone whenever possible," Dr. Waël Hanna said. "If you have to use mesh because you cannot reapproximate the chest wall or there’s not enough muscle to construct a flap, then nonrigid mesh should be favored over rigid fixation."
Rigid fixation with methacrylate or metallic plates and screws has conventionally been advocated as the best method to achieve chest wall stability and to maintain respiratory integrity following resection of chest wall tumors. However, these approaches are frequently complicated by motion deformities of the shoulder girdle, long-term cosmetic deformities, pain that limits daily activities, and a high morbidity of infection, Dr. Hanna explained at the annual meeting of the Central Surgical Association.
He reported on 37 patients who underwent major chest wall reconstruction in 2003-2010 with autologous tissue alone or with a soft prosthetic mesh. No patient underwent rigid fixation with methacrylate or plates and screws. The study excluded patients with concomitant lung or pleural resection to avoid confounding the respiratory outcomes.
Nine patients had a small defect (less than 60 cm2) and 28 patients had a large defect (greater than 60 cm2); no defect measured exactly 60 cm2, according to Dr. Hanna. The large-defect group was further divided into a subgroup of 16 patients who were reconstructed with soft mesh alone and a subgroup of 12 patients whose reconstruction was with autologous tissue alone and no mesh. Soft mesh was used in only one small-defect patient.
"We have turned away from using rigid prosthetics or methacrylate at our institution," said Dr. Hanna, a fifth-year resident with McGill University in Montreal.
Sarcoma was the most common indication for resection, followed by metastases to the chest wall, neurofibromas, and desmoid tumors. Reconstruction parameters were similar between the small- and large-defect cohorts, except for the mean size of the defect that was created in the chest wall (51 cm2 vs. 149 cm2), the dissection of three or more ribs (0% vs. 50%), and the use of soft mesh only (11% vs. 61%). A muscle flap to cover the prosthesis was used equally in both cohorts (56% vs. 75%).
The rate of immediate postoperative extubation was similar, at 100% in the small-defect cohort and 89% in the large-defect cohort, Dr. Hanna said. Only one patient was reintubated on postop day 1 and remained intubated for 3 days in the ICU.
None of the small-defect group went to the ICU for ventilation or flap monitoring, whereas 11% and 18% of the large-defect cohort did (P = .006 for both subgroups).
Pneumonia developed in three patients with large defects and in none with small defects (11% vs. 0%). One patient had to be re-extubated postoperatively, he said.
Secondary outcomes were also similar between the small- and large-defect groups, including site infection (0% vs. 7%) and reoperation rates (0% vs. 11%).
A subgroup analysis comparing patients with and without mesh revealed no significant differences in the primary outcomes of immediate extubation (100% vs. 75%), ICU stay for ventilation (6% vs. 25%), ICU stay for flap monitoring (13% vs. 17%), or pneumonia (6% vs. 8%).
The mesh and no-mesh subgroups were also nonsignificantly different with regard to site infection (13% vs. 0%) and reoperation (19% vs. 0%).
After a mean follow-up of 42 months (range, 36-84 months), there were no reports of infections beyond 30 postoperative days, long-term pain, restriction of mobility, or cosmetic disturbances. Patients were seen every 3 months for the first 2 years and every 6 months thereafter.
"For chest wall defects smaller than 60 cm2, reconstruction without a prosthesis has excellent outcomes," Dr. Hanna concluded. "For [defects] larger than 60 cm2, there does not seem to be any major difference between autologous tissue alone vs. nonrigid prosthesis reconstruction.
"Finally, nonrigid mesh seems to offer better short-term and long-term outcomes," compared with the historical data on rigid fixation, he said.
Invited discussant Dr. Fred Luchette, professor of surgery at Loyola University Medical Center in Chicago asked how the surgeons manage the often catastrophic event of mesh infection, and whether any long-term pulmonary function data were available, as the defects would likely prompt the development of some degree of paradoxical chest wall motion, even with the soft mesh.
Dr. Hanna replied that the retrospective nature of the series did not allow pulmonary function testing, and that the thoracic surgery community views such testing as less than ideal after reconstruction of the chest wall. A better measure is home oxygen use or limitation of daily activities, neither of which were observed in the cohort.
Dr. Hanna agreed that mesh infection is a highly morbid situation, especially with methacrylate or metallic prostheses, and that one of the benefits of soft prostheses like Vicryl or Gore-Tex is that they are able to respond to antibiotics.
Dr. Gerald Larson of University Surgical Associates in Louisville, Ky., who was also invited to discuss the study, asked how closure was achieved when mesh and a flap were not used, and why mesh and a muscle flap weren’t used for all patients.
Dr. Hanna responded that the risk of surgical site infection kept them from closing all patients with mesh and a muscle flap. The ideal method for closure is to mobilize enough local muscle that is present in the chest wall to reapproximate the muscle, and to close with skin without having to rotate a pedicle flap. When this is impossible, the defect has to be filled, and most surgeons at his institution elect to use soft mesh for the larger defects.
"In 75% of the time, on top of the mesh, we still mobilize a subcutaneous flap to cover the mesh because of the theoretical perception that a flap on top of the mesh would provide a good oxygenated environment and would decrease the rate of infection," Dr. Hanna said. The risk of surgical site infection kept them from closing all patients with mesh and a muscle flap, he added.
Dr. Hanna and his coauthors reported no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE CENTRAL SURGICAL ASSOCIATION
Major Finding: For chest wall defects smaller than 60 cm2, reconstruction without prosthesis was recommended. For larger defects, no major differences were seen between autologous tissue alone vs. nonrigid prosthesis reconstruction. Nonrigid mesh showed better short- and long-term outcomes, compared with historical data on rigid fixation.
Data Source: Retrospective analysis of 37 patients who underwent complex chest wall reconstruction.
Disclosures: Dr. Hanna and his coauthors reported no relevant conflicts of interest.
Genetic Link Found to Pulmonary Fibrosis, Familial Pneumonia
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
FROM THE NEW ENGLAND JOURNAL OF
MEDICINE
Major Finding: The rs35705950 SNP on the MUC5B gene that encodes for mucin formation in the lungs is associated with both IPF and FIP.
Data Source: A genomewide linkage scan, fine mapping study, and other genetic analyses to identify mutations associated with IPF and FIP.
Disclosures: This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources.
Genetic Link Found to Pulmonary Fibrosis, Familial Pneumonia
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
Like many successful genomewide linkage studies, the report by Dr. Seibold and colleagues "provides a provocative stimulus for broadening our understanding of the pathogenesis of pulmonary fibrosis," said Dr. Richard C. Boucher.
The study also "dictates that we broaden our vision of pulmonary fibrosis therapeutics, particularly given the absence of satisfactory clinical responses to immunosuppressants and corticosteroids. Thus, agents in clinical development that may regulate the unfolded-protein response may be worthy of early trials in pulmonary fibrosis.
"Similarly, agents that reduce MUC5B transcriptional activity in vitro should be tested for activity in vivo, including in subjects expressing the variant genotype," he said.
The study by Dr. Seibold and colleagues "may have ‘unstuck’ our thought processes with respect to a disease that has frustrated both patients and their physicians."
Richard C. Boucher, M.D., is at the University of North Carolina at Chapel Hill. He reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix. These remarks were taken from his editorial accompanying Dr. Seibold’s report (N. Engl. J. Med. 2011;364:1560-1).
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
A genetic variant in the MUC5B gene appears to be associated with both idiopathic pulmonary fibrosis and familial interstitial pneumonia, according to a report in the April 21 issue of the New England Journal of Medicine.
The MUC5B gene encodes mucin 5B, a gel-forming protein that is usually found in the lungs and is overexpressed in pulmonary diseases such as asthma, bronchitis, chronic obstructive pulmonary disorder, and cystic fibrosis. "In the aggregate, our findings suggest that dysregulated MUC5B expression in the lung may be involved in the pathogenesis of pulmonary fibrosis," said Max A. Seibold, Ph.D., of National Jewish Health, Denver, and his associates.
In addition, the link with familial interstitial pneumonia "could provide insight into the particular clinical manifestations of this complex disease process and consequently lead to earlier detection, more predictable prognosis, and personalized therapeutic strategies," they said.
Until now, the genetic mutations that have been implicated in both idiopathic pulmonary fibrosis (IPF) and familial interstitial pneumonia (FIP) have accounted for only a small proportion of the population risk for the disorders. The investigators searched further for other related mutations, beginning with a genomewide linkage scan in 82 families with FIP.
The results led the researchers to assess genetic variation in particular regions of three gel-forming mucin genes, using blood samples from a separate cohort of 83 subjects who had FIP, 492 subjects who had IPF, and 322 controls. One single-nucleotide polymorphism (SNP) in the putative promoter of the MUC5B gene was particularly strongly associated with both disorders. The minor allele of this SNP (rs35705950) was found at a frequency of 34% among subjects with FIP and 38% among those with IPF, compared with only 9% among controls.
A subsequent analysis demonstrated that rs35705950 exerted an effect in both disorders that was strongly independent of that of other, known mucin variants.
Next, the investigators evaluated the effect of rs35705950 on MUC5B expression in lung tissue from 33 subjects with IPF and 47 control subjects. They found that MUC5B expression was 14 times higher in samples from affected patients than in those from control subjects.
Finally, immunohistochemical staining of the lung tissue from IPF patients showed regions of dense accumulation of MUC5B in areas of microscopic honeycombing that are characteristic of IPF lesions. There was patchy staining of the metaplastic epithelia lining the honeycomb cysts, and of the mucous plugs within the cysts, the investigators said (N. Engl. J. Med. 2011;364:1503-12).
"The prevailing opinion is that IPF develops as a result of excessive, sequential lung injury or aberrant wound healing." The mechanisms by which this genetic variant interacts with excessive lung injury or aberrant repair is not yet known, they added.
"Our results could potentially alter the clinical approach to interstitial pneumonia," Dr. Seibold and his colleagues said.
"The implication of secreted airway mucins in the pathogenesis of [pulmonary fibrosis] suggests that the air space plays a role in the development of idiopathic [interstitial pneumonia]. Although identification of rs35705950 ... can be used to target persons at risk for the development of idiopathic [interstitial pneumonia] (especially those who are members of families subject to idiopathic [interstitial pneumonia]), our observations that the biologic features of mucins may be important etiologic factors in this disease could reorient the focus of pathogenic and therapeutic studies in interstitial lung disease to lung mucins, the air space, and the bronchoalveolar unit," they noted.
This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources. Dr. Boucher reported ties to Parion Sciences, Inspire Pharmaceuticals, and Pulmatrix.
FROM THE NEW ENGLAND JOURNAL OF
MEDICINE
Major Finding: The rs35705950 SNP on the MUC5B gene that encodes for mucin formation in the lungs is associated with both IPF and FIP.
Data Source: A genomewide linkage scan, fine mapping study, and other genetic analyses to identify mutations associated with IPF and FIP.
Disclosures: This study was supported by the National Institute of Environmental Health Sciences, the National Cancer Institute, the American Lung Association, the Cystic Fibrosis Foundation, the Chapman Foundation, InterMune, and the National Heart, Lung, and Blood Institute. Dr. Seibold’s associates reported ties to numerous academic, government, and industry sources.
No Bad Eye Effects Found With Long-Term Inhaled Corticosteroid
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Children with chronic asthma who used daily inhaled budesonide for an average of 16 years showed no increased risk of cataracts, intraocular pressure, or vision problems.
Data Source: Prospective longitudinal study of 300 treated children with chronic asthma and 163 healthy sibling controls.
Disclosures: AstraZeneca, which markets budesonide, funded the study. Dr. Pederson said he had no other relevant financial disclosures.
No Bad Eye Effects Found With Long-Term Inhaled Corticosteroid
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
SAN FRANCISCO – Using inhaled budesonide daily for chronic asthma for a mean of 16 years from childhood into adulthood didn’t cause more cataracts or significantly change intraocular pressure or vision in a prospective, longitudinal, placebo-controlled study.
Among 300 Danish patients taking inhaled budesonide for chronic asthma, 148 underwent eye examinations 15-20 years after the start of the study, as did 53 of 163 healthy siblings in the control group. The exams detected two posterior subcapsular cataracts that were outside the central 3-mm zone, but both were in the control group and none in the budesonide group, Dr. Søren Pedersen and his associates reported at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
Nineteen cataracts in the budesonide group would have been needed to demonstrate a statistically significant 5% increased risk for cataracts, a poststudy power analysis found.
Average vision measurements were identical between groups (1.04 in each eye), said Dr. Pedersen of the University of Southern Denmark, Kolding. Intraocular pressures did not differ significantly between groups, with average measurements of 13.8 mm Hg in each eye of the asthma patients, and averages of 14.5 mm Hg in the right eyes and 14.2 mm Hg in the left eyes of the control group.
“This is a very strong finding” of safety with long-term inhaled budesonide, he said in an interview.
Patients took a mean daily dose of 385 mcg of budesonide and accumulated a mean dose of 2.3 g. Increased intraocular pressures (higher than 21 mm Hg) were seen in five patients (3.4%) and in one sibling in the control group (1.9%), a nonsignificant difference between groups. The accumulated dose of budesonide was not significantly associated with intraocular pressure, Dr. Pedersen said.
The study is part of a larger study that began with 270 children, including 62 with asthma who did not use inhaled corticosteroids, all of whom were evaluated for cataracts, bruises, growth, bone mineral density, and clinical effects of inhaled budesonide 4-6 years after treatment started, with no adverse effects found. At that point, 32 children in the control group dropped out, the other 30 shifted to the budesonide group, and 163 healthy siblings became the new control group. Patients were followed with various evaluations every 1-2 years.
The mean age of those who had eye exams 15-20 years into the study was 26 years for patients and 28 years for siblings. A total of 68% of patients and 47% of controls were male. Treatment duration ranged from 3 to 22 years. Daily budesonide dose ranged from 50 to 1,220 mcg. The accumulated budesonide dose ranged from less than 1 g to 8.8 g.
The ophthalmologist who performed all of the eye exams did not know which subjects were patients and which were controls.
Previous studies of the risk of posterior subcapsular cataracts from oral or inhaled steroids were cross-sectional studies with little or no information on the dose of inhaled corticosteroid used, he said.
AstraZeneca, which markets budesonide, funded the study. Dr. Pedersen said there were no other conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Children with chronic asthma who used daily inhaled budesonide for an average of 16 years showed no increased risk of cataracts, intraocular pressure, or vision problems.
Data Source: Prospective longitudinal study of 300 treated children with chronic asthma and 163 healthy sibling controls.
Disclosures: AstraZeneca, which markets budesonide, funded the study. Dr. Pederson said he had no other relevant financial disclosures.
Pediatricians Lead the Way in Asthma Care

Dr. Peterson modeled the Children’s Healthcare Access Program in Grand Rapids after a similar program that was started at Denver Children’s Hospital. He told me that in all the initiatives like this that he’s aware of, the effort starts with the actions of a single pediatrician who gets the ball rolling.
It takes a village, but it starts with individuals. Hats off to the docs who find time to take care of patients and to address the systemic needs.
—Sherry Boschert (On Twitter @sherryboschert)
Dr. Peterson modeled the Children’s Healthcare Access Program in Grand Rapids after a similar program that was started at Denver Children’s Hospital. He told me that in all the initiatives like this that he’s aware of, the effort starts with the actions of a single pediatrician who gets the ball rolling.
It takes a village, but it starts with individuals. Hats off to the docs who find time to take care of patients and to address the systemic needs.
—Sherry Boschert (On Twitter @sherryboschert)
Dr. Peterson modeled the Children’s Healthcare Access Program in Grand Rapids after a similar program that was started at Denver Children’s Hospital. He told me that in all the initiatives like this that he’s aware of, the effort starts with the actions of a single pediatrician who gets the ball rolling.
It takes a village, but it starts with individuals. Hats off to the docs who find time to take care of patients and to address the systemic needs.
—Sherry Boschert (On Twitter @sherryboschert)
Perceived Uncontrolled Asthma in Overweight Teens May Be Deconditioning
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Overweight inner-city adolescents with nonobstructive asthma were more likely than their normal-weight peers to report uncontrolled asthma despite similar lung function between groups.
Data Source: Secondary analysis of data on 114 patients in a larger prospective study of using electronic technology to improve asthma control.
Disclosures: The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
Perceived Uncontrolled Asthma in Overweight Teens May Be Deconditioning
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
SAN FRANCISCO – Overweight inner-city teenagers with nonobstructive asthma were more likely than their normal-weight peers to report that their asthma was out of control even when spirometry results suggested they were having a relatively good day, a study of 114 teens found.
The study included 102 normal-weight adolescents and 112 overweight adolescents (defined as a body mass index greater than the 85th percentile) who completed the Asthma Control Test and spirometry measures. Observed lung function was similar between the two groups, Iwalola Awoyinka and her associates reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Overall, the overweight teenagers were more likely than the normal-weight teenagers to report uncontrolled asthma on the Asthma Control Test. When compared by asthma pattern, however, only teens with nonobstructive asthma were significantly more likely to report uncontrolled asthma (in more than 60%), compared with normal-weight teens with nonobstructive asthma, approximately 50% of whom reported uncontrolled asthma.
Among teens with an obstructive asthma pattern, reports of uncontrolled asthma were statistically similar between the overweight and normal-weight groups, hovering around 60%, said Ms. Awoyinka, a pulmonary function specialist and research coordinator at the University of Wisconsin, Madison.
What some overweight teens perceive as uncontrolled asthma may be a symptom of deconditioning, Ms. Awoyinka suggested. Misperceptions of uncontrolled asthma may lead to overuse of asthma medication. Perhaps prescriptions for overweight teens with asthma should include prescriptions to exercise, she added in an interview.
Uncontrolled asthma, defined as a score of 19 or less on the Asthma Control Test, was reported by 131 adolescents. Spirometry identified 99 teens as having nonobstructive asthma and 115 as having an obstructive asthma pattern, defined as less than 80% of predicted forced expiratory volume in 1 second (FEV1) or a ratio of FEV1 to forced vital capacity (FVC) of less than 0.85.
The analysis was part of a larger study of the use of electronic technology to improve asthma control in 218 inner-city teens on Medicaid, 4 of whom were excluded from the analysis because of a lack of acceptable spirometry results. Previous studies have shown that teens with low socioeconomic status are more likely to be overweight and to have asthma than are more affluent teens.
The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Overweight inner-city adolescents with nonobstructive asthma were more likely than their normal-weight peers to report uncontrolled asthma despite similar lung function between groups.
Data Source: Secondary analysis of data on 114 patients in a larger prospective study of using electronic technology to improve asthma control.
Disclosures: The National Institutes of Health funded the study. The investigators reported having no relevant conflicts of interest.