User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Inhalation therapy: Help patients avoid these mistakes
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
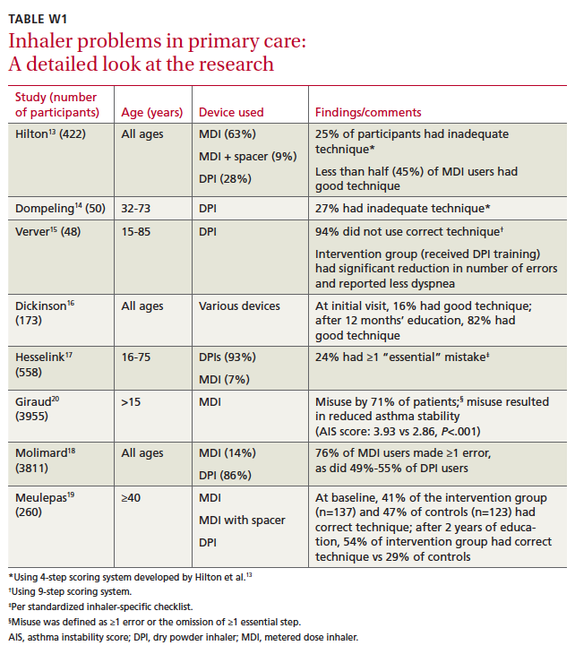
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; tself@uthsc.edu
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; tself@uthsc.edu
• Stress the importance of exhaling gently for a few seconds before inhaling (deeply and slowly for a metered dose inhaler, and deeply and rapidly for most dry powder inhalers). C
• Observe the inhaler technique of every patient receiving inhalation therapy on more than one occasion. C
• Don’t rely on self-reports regarding inhaler technique; despite claims of proficiency, most patients make at least one mistake. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
For patients with asthma or chronic obstructive pulmonary disease (COPD), inhalation therapy is the foundation of treatment. Yet all too often, patients don’t get the full value of their inhaled medications because they use their inhaler incorrectly. When technique is markedly flawed, suboptimal outcomes typically result.
Given the number of Americans with asthma (at least 22 million)1 and COPD (more than 13 million adults),2 faulty inhaler technique is a major public health problem. In fact, the number of people suffering from COPD may be even larger: Close to 24 million US adults are believed to have impaired lung function.3,4 For patients with asthma or COPD—many of whom are treated by family physicians—comprehensive education with a focus on correct use of an inhaler is essential.
In this review, we present evidence of frequent inhaler errors (from clinical studies) and highlight some of the more common mistakes (based on our clinical experience [TABLE]5). Finally, we offer ‘‘time-efficient’’ solutions to inhaler problems—steps that physicians in busy primary care practices can take to ensure that patients with asthma or COPD get the maximum benefit from inhalation therapy.
TABLE
Caution patients about these device-specific mistakes*
| Metered dose inhaler |
|---|
|
| Metered dose inhaler plus spacer/VHC |
|
| Dry powder inhaler |
|
| *These are examples based on the experience of the authors; other errors are possible. †Timing is not as crucial as it is for an MDI without a spacer, but the drug is still lost if inhalation is delayed. ‡Correct use varies by type of product (see product literature for specifics). DPI, dry powder inhaler; MDI, metered dose inhaler; VHC, valved holding chamber. Source: Adapted with permission from Self TH, et al. Consultant. 2003.5 |
Inhaler error is well documented
Since 1965, when it was first reported that many patients used metered dose inhalers (MDIs) incorrectly,6 evidence has accumulated supporting the magnitude of the problem.7-12 (Studies conducted in family practice settings are described in “Researchers look at inhaler problems in primary care” and in TABLE W1.13-20)
A number of studies of various sizes (from 41 to 3955 patients) have assessed inhaler technique in patients being treated by clinicians in primary care. The researchers used a variety of scoring methods, as well. Among them were a simple 4-step (0-4) rating system, a 9-step system, a standardized inhaler-specific checklist, and a system that tracked the number of omissions patients made.13-20 All found significant problems with inhaler technique. (You’ll find a detailed look at the studies in TABLE W1 at jfponline.com.)
In one study of 422 patients,13 including young children, adolescents, and adults, participants received one point for correctly performing each of the following steps:
- Adequate preparation (shaking well for those using a metered dose inhaler [MDI]; loading correctly for patients using a dry powder inhaler [DPI])
- Adequate expiration, correct head position
- Adequate inspiratory technique
- Holding breath afterwards.
The researchers found that 25% of the patients had inadequate technique (≤2 on a 0-4 point scale). In this study, as in others that included patients using various types of devices, use of an MDI was associated with a higher rate of incorrect technique.
Another much-smaller study14 used the same 4-step system to assess the technique of 50 patients, all of whom had the same type of DPI and had received extensive training in the correct use of the device. Despite the training, 27% of the patients received scores of ≤2 (inadequate technique). Sixty-eight percent received a score of 3 (adequate); only 5% received a score of 4 (good).
The 2 largest studies—one including 3955 patients using MDIs20 and the other looking at 3811 patients using various kinds of devices18—found high levels of errors, as well. In the latter study, 76% of patients with MDIs made at least one error vs 49% to 55% of patients using DPIs.18 The results convinced a large majority of the physicians caring for these patients of the need to check inhaler technique more frequently. In the study of MDI users alone, 71% of the patients made at least one mistake.20 inhaler misuse was associated with higher asthma instability scores, this study showed.
More recently, a researcher assessed the effects of an integrated primary care model on the management of asthma and/or COPD in middle-aged and elderly patients, in a study of 260 patients in 44 family practices.19 The study included an evaluation of inhaler technique.
Participants were divided into an intervention group—137 patients who received education regarding inhaler use from a nurse—and a usual care group (123 patients). After 2 years, correct inhaler technique among those in the intervention group went from 41% at baseline to 54%. At the same time, the proportion of those in the usual care group with correct technique fell from 47% to 29%.19
Error rates vary widely from one clinical trial to another, depending on study criteria, type of device, and extent of patient education, among other factors. Nonetheless, several studies (spanning 3 decades) found the error rate to be close to, or greater than, 90%.7,10,21
The most recent of these, published in 2009,21 was based on observation of the inhaler technique used by patients with asthma or COPD directly following appointments in an outpatient clinic. The authors found that, although >98% of the study participants claimed to know how to use their inhalers, 94% committed at least one error. In this study and a number of others, user error was more likely in patients using MDIs.13,18,21,22
Adding a spacer (eg, a valved holding chamber such as the AeroChamber) can be helpful, as the spacer affords the patient more time to inhale the medication. But patients who use an MDI with a spacer often make mistakes, too, and patient education is essential.23-26
Breath-activated dry powder inhalers (DPIs)—such as the Flexhaler, HandiHaler, Aerolizer, and Diskus—also reduce the likelihood of error. DPIs eliminate a step that MDI users often struggle with: the need to simultaneously press down on the canister and begin a slow, deep inhalation.
What’s more, DPIs do not have to be shaken before use. Nonetheless, using a DPI still involves a series of actions. For the HandiHaler and Aerolizer, patients must load the dose, and some patients fail to read the directions and swallow the capsule instead of loading it into the device. Patients must remember to exhale away from the device (ie, not into the dry powder) before inhaling, then hold their breath for approximately 10 seconds. There is potential for error at each step.
Stress the need to exhale before using the inhaler
Forgetting to exhale before inhaling is a common, and significant, mistake regardless of the type of device. It is paramount to stress the need to exhale gently for a few seconds before inhaling (slowly and deeply for patients using an MDI, rapidly and deeply with most DPIs). For MDI users, poor timing, described earlier, is another common and serious mistake. Patients using an MDI with a valved holding chamber sometimes inhale for too long before pressing down on the inhaler, then are unable to continue inhaling although the aerosol is still in the chamber. A common error made by patients using multidose DPIs is simply to forget to load the dose.
Physicians need to brush up on their skills, too
It’s not just patients who lack proficiency in inhaler technique. Numerous studies have demonstrated poor skill among physicians and other health care professionals.27-34 Evidence also shows that targeted education results in substantial improvement.32,35
In one study undertaken to evaluate family medicine residents’ proficiency in using asthma inhalers, participants (an intervention group at one clinic and a control group at another) all were given a pretest. The intervention group then received educational materials and a tutorial, as well as the opportunity for hands-on practice, after which both groups were given a post-test. The residents who received the training had a 170% jump, on average, in proficiency score, vs a 55% increase for the control group (P<.001).35
Inhaled Medication Instructional Videos
Courtesy of: National Jewish Health
Go to http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos
Another study—this one involving first-year interns—looked at level of improvement based on the type of education provided. Initially, only 5% of the interns could use an MDI without error. After a lecture and demonstration, 13% had an error-free technique. But when each intern participated in an intensive one-on-one session, the error-free rate reached 73%. The researchers’ conclusion: Lectures are relatively ineffective in teaching interns inhaler technique compared with a one-on-one approach.32
The Chicago Breathe Project,36 a new program aimed at improving education in the use of asthma inhalers for physicians and minority patients, provides further evidence of the value of clinician education. After a series of workshops for residents at 5 academic institutions, the physicians’ knowledge of proper use of inhalers rose dramatically—from just 5% preprogram to 91% postprogram (P<.001). Six months after the educational activity, the residents (n=161) were more likely (44% vs 11% preprogram) to assess patients’ inhaler technique.36
Teaching patients when time is tight
National and international guidelines stress the need to teach patients correct use of asthma and COPD inhalers.1,37,38 Providing the requisite education includes observation of each patient’s inhaler technique with proper use demonstrated, as needed.
The problem, of course, is how to provide that level of patient education within the time constraints of a busy family practice. We recommend these time-efficient solutions:
Enlist the help of other clinicians. While it is important that someone in your office be well trained and able to instruct patients in the proper use of inhalers, that individual need not be you. The National Institutes of Health recommends that the “principal clinician” introduce key educational messages, which can be reinforced and expanded on by other members of the health care team.1
After you advise patients that it is crucial for them to be trained in and adhere to proper inhaler technique, another health care professional—often a clinic nurse or pharmacist who has had special training—can provide the hands-on education. Studies have shown that when pharmacists who are competent in asthma management, including inhaler technique, work with physicians to optimize the education and overall management of patients with asthma, better outcomes often result, including a reduction in both emergency department visits and hospitalizations.1,39,40
Use videos to demonstrate correct technique. Videos are an effective teaching tool,9 and many of them are device-specific. National Jewish Health, which is world renowned for its asthma care, has a set of instructional videos posted on You-Tube and accessible from its Web site (http://www.nationaljewish.org/healthinfo/medications/lung-diseases/devices/instructional-videos). In addition to videos that demonstrate the use of an MDI alone and an MDI plus a valved holding chamber, the site has links to 6 DPI videos, each covering a different device.
Use intermittent observation. After the patient views the appropriate video, you or a member of your staff will still need to observe the patient’s inhaler technique to ensure correct use. Ideally, this should occur at every visit.1,37 When that’s not possible, use intermittent observation, starting with the first 2 or 3 visits after the introduction of inhalation therapy and then switching to periodic observation to ensure that the patient is maintaining good technique.
In determining how often observation is necessary, keep in mind that simply asking patients whether they are having inhaler problems is not sufficient.1 Patients tend to say they have little or no trouble when, in fact, most struggle, at times, with the devices. What’s more, good technique tends to decrease over time, and repetitive education is important.
To motivate patients, try this communication technique
Motivational interviewing, a technique that has been used to help patients battle obesity, quit smoking, and control hypertension,41-43 among other health problems, can help you identify inhaler problems that need to be addressed. It involves the use of open-ended questions (eg, “What worries you most about your asthma?”), affirmations (“You’ve done a great job testing your peak flow level every morning”), reflective listening (“You’re tired of taking medicine every day”), and summary statements (“You know you should take your medicine every day but you’re having trouble remembering it. Is that right?”).
A pilot study44 showed that when this technique was incorporated into an asthma education session, patient motivation increased. The ratio of perceived advantages vs disadvantages of taking asthma medication correctly improved, as well. Another study45 found that when motivational interviewing was used during home visits to inner-city African American adolescents for asthma care, the patients’ motivation, readiness to adhere to treatment, and asthma-related quality of life improved, although self-reported adherence to asthma medication did not. Further studies involving patients with asthma are under way (www.clinicaltrials.gov/ct2/results?term=asthma).
It is important to note that the use of motivational interviewing does not require a lengthy visit. One study found that on average, visits in which primary care physicians used this communication technique lasted less than 10 minutes.46
CORRESPONDENCE Timothy H. Self, PharmD, University of Tennessee Health Science Center, 881 Madison Avenue, Room 235, Memphis, TN 38163; tself@uthsc.edu
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
1. National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007.
2. Centers for Disease Control and Prevention. National Center for Health Statistics: National health interview survey raw data, 2008. Analysis performed by American Lung Association Research and Program Services.
3. American Lung Association. COPD—Helping the missing millions. February 24, 2010. Available at: http://www.lungusa.org/about-us/our-impact/top-stories/copd-helping-the-missing.html. Accessed November 9, 2011.
4. Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
5. Self TH, Kilgore KE, Shelton V. MDIs, spacers, and dry powder inhalers: what patients are likely to do wrong. Consultant. 2003;49:702-705.
6. Saunders KB. Misuse of inhaled bronchodilator agents. Br Med J. 1965;1:1037-1038.
7. Epstein SW, Manning CPR, Ashley MJ, et al. Survey of the clinical uses of pressurized aerosol inhalers. Can Med Assoc J. 1979;120:813-816.
8. Shim C, Williams MH. The adequacy of inhalation of aerosol from canister nebulizers. Am J Med. 1980;69:891-894.
9. Self TH, Brooks JB, Lieberman P, et al. The value of demonstration and role of the pharmacist in teaching the correct use of pressurized bronchodilators. Can Med Assoc J. 1983;128:129-131.
10. Hartert TV, Windom HH, Peeples RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386-394.
11. Goodman DE, Israel E, Rosenberg M, et al. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150:1256-1261.
12. Newman SP, Pavia D, Clarke SW. How should a pressurized beta-adrenergic bronchodilator be inhaled? Eur J Respir Dis. 1981;62:3-21.
13. Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. Br J Gen Pract. 1990;40:505-506.
14. Dompeling E, Van Grunsven PM, Van Schayck GP, et al. Treatment with inhaled steroids in asthma and chronic bronchitis: long-term compliance and inhaler technique. Fam Pract. 1992;9:161-166.
15. Verver S, Poelman M, Bogels A, et al. Effects of instruction by practice assistants on inhaler technique and respiratory symptoms of patients. A controlled randomized videotaped intervention study. Fam Pract. 1996;13:35-40.
16. Dickinson J, Hutton S, Atkin A, et al. Reducing asthma morbidity in the community: the effect of a targeted nurse-run asthma clinic in an English general practice. Respir Med. 1997;91:634-640.
17. Hesselink AE, Penninx BW, Wijnhoven HA, et al. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001;19:255-260.
18. Molimard M, Raherison C, Lignot S, et al. Assessment of handling of inhaler devices in real life: An observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249-254.
19. Meulepas MA, Jacobs JE, Smeenk FW, et al. Effect of an integrated primary care model on the management of middle-aged and old patients with obstructive lung diseases. Scand J Prim Health Care. 2007;25:186-192.
20. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246-251.
21. Souza ML, Meneghini AC, Ferraz E, et al. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824-831.
22. Rootmensen GN, van Keimpema AR, Jansen HM, et al. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23:323-328.
23. Rachelefsky GS, Rohr AS, Wo J, et al. Use of a tube spacer to improve the efficacy of a metered dose inhaler in asthmatic children. Am J Dis Child. 1986;140:1191-1193.
24. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration by metered-dose inhaler alone vs metered-dose inhaler plus valved holding chamber. Chest. 2000;117:1314-1318.
25. Pedersen S, Ostergaard PA. Nasal inhalation as a cause of inefficient pulmonal aerosol inhalation technique in children. Allergy. 1983;38:191-194.
26. Dolovich MD, Ahrens RS, Hess DR, et al. Device selection an outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127:335-371.
27. Interiano B, Guntupalli KK. Metered-dose inhalers: do health care providers know what to teach? Arch Intern Med. 1993;153:81-85.
28. Hanania NA, Wittman R, Kesten S, et al. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105:111-116.
29. Amirav I, Goren A, Pawlowski NA. What do pediatricians in training know about the correct use of inhalers and spacer devices? J Allergy Clin Immunol. 1994;94:669-675.
30. Chopra N, Oprescu N, Fask A, et al. Does introduction of new “easy to use” inhalational devices improve medical personnel’s knowledge of their proper use? Ann Allergy Asthma Immunol. 2002;88:395-400.
31. Self TH, Arnold LB, Czosnowski LM, et al. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44:593-598.
32. Lee-Wong M, Mayo PH. Results of a programme to improve house staff use of metered dose inhalers and spacers. Postgrad Med J. 2003;79:221-225.
33. Muchao FP, Pern SL, Rodriques JC, et al. Evaluation of the knowledge of health professionals at a pediatric hospital regarding the use of metered dose inhalers. J Bras Pneumol. 2008;34:4-12.
34. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46:944-950.
35. Kelcher S, Brownoff R. Teaching residents to use asthma devices. Assessing family residents’ skill and a brief intervention. Can Fam Physician. 1994;40:2090-2095.
36. Press VG, Pincayage AT, Pappalardo AA, et al. The Chicago Breathe Project: a regional approach to improving education on asthma inhalers for resident physicians and minority patients. J Natl Med Assoc. 2010;102:548-555.
37. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2010. Available at: www.ginasthma.org. Accessed November 9, 2011.
38. Executive Summary: global strategy on the diagnosis and management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Workshop Report, 2009. Available at: www.goldcopd.com. Accessed November 9, 2011.
39. Self TH, Chrisman CR, Mason DL, et al. Reducing emergency department visits and hospitalizations in African American and Hispanic patients: a 15-year review. J Asthma. 2005;42:807-812.
40. Armour C, Bosnic-Anticevich S, Brillant M, et al. Pharmacy asthma care program (PACP) improves outcomes for patients in the community. Thorax. 2007;62:496-502.
41. DiLillo V, Nicole J, West DS. Incorporating motivational interviewing into behavioral obesity treatment. Cogn Behav Pract. 2003;10:120-130.
42. Borrelli B, Novak S, Hecht J, et al. Home health care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Prev Med. 2005;41:815-821.
43. Woollard L, Beilin L, Lord T, et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol. 1995;22:466-468.
44. Schmaling K, Blume A, Afari N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J Clin Psych Med Settings. 2001;8:167-172.
45. Riekert KA, Borrelli B, Bilderback A, et al. The development of a motivational interviewing intervention to promote medication adherence among inner-city, African-American adolescents with asthma. Patient Educ Couns. 2011;82:117-122.
46. Butler C, Rollnick S, Cohen D, et al. Motivational consulting versus brief advice for smokers in general practice: a randomized trial. Br J Gen Pract. 1999;49:611-616.
New COPD Treatments Needed, Expert Says
HONOLULU – Current interventions for chronic obstructive pulmonary disease leave many patients with unmet needs, according to Dr. Nicola A. Hanania.
"We know from large clinical trials that current pharmacotherapies do not change the natural history of COPD, and many patients remain symptomatic with current therapies," Dr. Hanania, director of the asthma clinical research center at Baylor College of Medicine, Houston, said at the annual meeting of the American College of Chest Physicians.

Inadequate adherence to therapy "is a major cause of poor clinical outcomes in the treatment of COPD," he said. The cost, compliance, and safety of certain agents are issues "that we cannot ignore."
When considering a therapy for COPD, clinicians should factor in components of COPD beyond bronchoconstriction, he advised, including mucociliary dysfunction, structural changes in the airway and the lung, systemic components, and airway inflammation. "We also have to look at outcomes other than lung function including exacerbations, activity limitation, and symptoms of dyspnea," he said. "We are no more satisfied with just a drug that improves lung function but does nothing for the patient-reported outcomes."
Dr. Hanania’s "wish list" for an ideal COPD therapeutic option in the future is one that addresses the multiple components and phenotypes of COPD. He said he would like to see drugs that blunt proinflammatory cells and molecules known to be involved in COPD. "We’d also like to see drugs that could modify the disease progression and comorbid conditions," he said. Such drugs, he continued, should be well tolerated and compatible with other therapies for COPD and comorbid conditions, be simple to administer, and have the potential to improve patient adherence, he added.
Treatment approaches being studied include novel formulations of existing medications, such as the combination of ultralong-acting beta-2 agonists and long-acting antimuscarinics. Among the agents that are the most promising on this front, he said, are indacaterol plus glycopyrronium (QVA-149) and vilanterol plus GSK-573719.
Other agents in development include bifunctional muscarinic antagonist–beta-2 agonists such as GSK-961081 and THRX-200495 as well as combinations of once-daily long-acting beta-2 agonists and inhaled corticosteroids, including formoterol and mometasone (MFF258) and vilanterol and fluticasone (Relovair).
However, perhaps the most promising pharmacotherapies will be novel agents aimed at reducing local and systemic inflammation. "We know that COPD is an inflammatory disease, so we need drugs that can target inflammation right from the very beginning," Dr. Hanania explained. "Inhaled steroids are important, but they’re not as effective in COPD as they are in asthma."
Phosphodiesterase type 4 inhibitors are currently being studied in COPD. These agents reduce the activity of neutrophils, macrophages, and CD8-positive T-lymphocytes, as well as the expression of cytokines and other inflammatory mediators. Currently, the only phosphodiesterase type 4 inhibitor approved in the United States for use in patients with COPD is roflumilast (Daliresp). Several others are in development.
"We know from large clinical trials that current pharmaco-therapies do not change the natural history of COPD."
Because they target airway inflammation, p38 mitogen-activated protein kinase inhibitors are also being studied in COPD patients. However, so far clinical trials have found potential problems related to systemic side effects and toxicity, "indicating that it is probably necessary to deliver these drugs by inhalation to reduce systemic exposure," Dr. Hanania said.
He concluded his presentation by noting that certain medications used to treat comorbidities in COPD may have beneficial effects on COPD outcomes. These include statins, ACE inhibitors, beta-blockers, peroxisome proliferator–activated receptor agonists, and macrolides. The National Heart, Lung, and Blood Institute COPD Clinical Research Network is currently conducting a prospective randomized controlled trial in 1,126 patients with severe COPD randomized to daily simvastatin (40 mg) vs. placebo for at least 1 year. The primary outcome is exacerbation of COPD. The secondary outcomes include change in forced expiratory volume in 1 second (FEV1), St. George’s Respiratory Questionnaire responses, 6-minute walk test results, BODE Index score, a combined cardiovascular end point, and serum inflammatory biomarker levels. Furthermore, a recent study showed that daily azithromycin significantly reduced exacerbations in high-risk patients.
Dr. Hanania disclosed that he has received grant support from the National Institutes of Health, the American Lung Association, GlaxoSmithKline (GSK), Boehringer Ingelheim (BI), Sunovion, Novartis, Pfizer, and Forest Pharmaceuticals. He also serves as a consultant for GSK, Dey Pharmaceuticals, Sunovion, Pfizer, and Forest, and is a member of the speakers bureau for GSK, BI, AstraZeneca, and Forest.
HONOLULU – Current interventions for chronic obstructive pulmonary disease leave many patients with unmet needs, according to Dr. Nicola A. Hanania.
"We know from large clinical trials that current pharmacotherapies do not change the natural history of COPD, and many patients remain symptomatic with current therapies," Dr. Hanania, director of the asthma clinical research center at Baylor College of Medicine, Houston, said at the annual meeting of the American College of Chest Physicians.
Inadequate adherence to therapy "is a major cause of poor clinical outcomes in the treatment of COPD," he said. The cost, compliance, and safety of certain agents are issues "that we cannot ignore."
When considering a therapy for COPD, clinicians should factor in components of COPD beyond bronchoconstriction, he advised, including mucociliary dysfunction, structural changes in the airway and the lung, systemic components, and airway inflammation. "We also have to look at outcomes other than lung function including exacerbations, activity limitation, and symptoms of dyspnea," he said. "We are no more satisfied with just a drug that improves lung function but does nothing for the patient-reported outcomes."
Dr. Hanania’s "wish list" for an ideal COPD therapeutic option in the future is one that addresses the multiple components and phenotypes of COPD. He said he would like to see drugs that blunt proinflammatory cells and molecules known to be involved in COPD. "We’d also like to see drugs that could modify the disease progression and comorbid conditions," he said. Such drugs, he continued, should be well tolerated and compatible with other therapies for COPD and comorbid conditions, be simple to administer, and have the potential to improve patient adherence, he added.
Treatment approaches being studied include novel formulations of existing medications, such as the combination of ultralong-acting beta-2 agonists and long-acting antimuscarinics. Among the agents that are the most promising on this front, he said, are indacaterol plus glycopyrronium (QVA-149) and vilanterol plus GSK-573719.
Other agents in development include bifunctional muscarinic antagonist–beta-2 agonists such as GSK-961081 and THRX-200495 as well as combinations of once-daily long-acting beta-2 agonists and inhaled corticosteroids, including formoterol and mometasone (MFF258) and vilanterol and fluticasone (Relovair).
However, perhaps the most promising pharmacotherapies will be novel agents aimed at reducing local and systemic inflammation. "We know that COPD is an inflammatory disease, so we need drugs that can target inflammation right from the very beginning," Dr. Hanania explained. "Inhaled steroids are important, but they’re not as effective in COPD as they are in asthma."
Phosphodiesterase type 4 inhibitors are currently being studied in COPD. These agents reduce the activity of neutrophils, macrophages, and CD8-positive T-lymphocytes, as well as the expression of cytokines and other inflammatory mediators. Currently, the only phosphodiesterase type 4 inhibitor approved in the United States for use in patients with COPD is roflumilast (Daliresp). Several others are in development.
"We know from large clinical trials that current pharmaco-therapies do not change the natural history of COPD."
Because they target airway inflammation, p38 mitogen-activated protein kinase inhibitors are also being studied in COPD patients. However, so far clinical trials have found potential problems related to systemic side effects and toxicity, "indicating that it is probably necessary to deliver these drugs by inhalation to reduce systemic exposure," Dr. Hanania said.
He concluded his presentation by noting that certain medications used to treat comorbidities in COPD may have beneficial effects on COPD outcomes. These include statins, ACE inhibitors, beta-blockers, peroxisome proliferator–activated receptor agonists, and macrolides. The National Heart, Lung, and Blood Institute COPD Clinical Research Network is currently conducting a prospective randomized controlled trial in 1,126 patients with severe COPD randomized to daily simvastatin (40 mg) vs. placebo for at least 1 year. The primary outcome is exacerbation of COPD. The secondary outcomes include change in forced expiratory volume in 1 second (FEV1), St. George’s Respiratory Questionnaire responses, 6-minute walk test results, BODE Index score, a combined cardiovascular end point, and serum inflammatory biomarker levels. Furthermore, a recent study showed that daily azithromycin significantly reduced exacerbations in high-risk patients.
Dr. Hanania disclosed that he has received grant support from the National Institutes of Health, the American Lung Association, GlaxoSmithKline (GSK), Boehringer Ingelheim (BI), Sunovion, Novartis, Pfizer, and Forest Pharmaceuticals. He also serves as a consultant for GSK, Dey Pharmaceuticals, Sunovion, Pfizer, and Forest, and is a member of the speakers bureau for GSK, BI, AstraZeneca, and Forest.
HONOLULU – Current interventions for chronic obstructive pulmonary disease leave many patients with unmet needs, according to Dr. Nicola A. Hanania.
"We know from large clinical trials that current pharmacotherapies do not change the natural history of COPD, and many patients remain symptomatic with current therapies," Dr. Hanania, director of the asthma clinical research center at Baylor College of Medicine, Houston, said at the annual meeting of the American College of Chest Physicians.
Inadequate adherence to therapy "is a major cause of poor clinical outcomes in the treatment of COPD," he said. The cost, compliance, and safety of certain agents are issues "that we cannot ignore."
When considering a therapy for COPD, clinicians should factor in components of COPD beyond bronchoconstriction, he advised, including mucociliary dysfunction, structural changes in the airway and the lung, systemic components, and airway inflammation. "We also have to look at outcomes other than lung function including exacerbations, activity limitation, and symptoms of dyspnea," he said. "We are no more satisfied with just a drug that improves lung function but does nothing for the patient-reported outcomes."
Dr. Hanania’s "wish list" for an ideal COPD therapeutic option in the future is one that addresses the multiple components and phenotypes of COPD. He said he would like to see drugs that blunt proinflammatory cells and molecules known to be involved in COPD. "We’d also like to see drugs that could modify the disease progression and comorbid conditions," he said. Such drugs, he continued, should be well tolerated and compatible with other therapies for COPD and comorbid conditions, be simple to administer, and have the potential to improve patient adherence, he added.
Treatment approaches being studied include novel formulations of existing medications, such as the combination of ultralong-acting beta-2 agonists and long-acting antimuscarinics. Among the agents that are the most promising on this front, he said, are indacaterol plus glycopyrronium (QVA-149) and vilanterol plus GSK-573719.
Other agents in development include bifunctional muscarinic antagonist–beta-2 agonists such as GSK-961081 and THRX-200495 as well as combinations of once-daily long-acting beta-2 agonists and inhaled corticosteroids, including formoterol and mometasone (MFF258) and vilanterol and fluticasone (Relovair).
However, perhaps the most promising pharmacotherapies will be novel agents aimed at reducing local and systemic inflammation. "We know that COPD is an inflammatory disease, so we need drugs that can target inflammation right from the very beginning," Dr. Hanania explained. "Inhaled steroids are important, but they’re not as effective in COPD as they are in asthma."
Phosphodiesterase type 4 inhibitors are currently being studied in COPD. These agents reduce the activity of neutrophils, macrophages, and CD8-positive T-lymphocytes, as well as the expression of cytokines and other inflammatory mediators. Currently, the only phosphodiesterase type 4 inhibitor approved in the United States for use in patients with COPD is roflumilast (Daliresp). Several others are in development.
"We know from large clinical trials that current pharmaco-therapies do not change the natural history of COPD."
Because they target airway inflammation, p38 mitogen-activated protein kinase inhibitors are also being studied in COPD patients. However, so far clinical trials have found potential problems related to systemic side effects and toxicity, "indicating that it is probably necessary to deliver these drugs by inhalation to reduce systemic exposure," Dr. Hanania said.
He concluded his presentation by noting that certain medications used to treat comorbidities in COPD may have beneficial effects on COPD outcomes. These include statins, ACE inhibitors, beta-blockers, peroxisome proliferator–activated receptor agonists, and macrolides. The National Heart, Lung, and Blood Institute COPD Clinical Research Network is currently conducting a prospective randomized controlled trial in 1,126 patients with severe COPD randomized to daily simvastatin (40 mg) vs. placebo for at least 1 year. The primary outcome is exacerbation of COPD. The secondary outcomes include change in forced expiratory volume in 1 second (FEV1), St. George’s Respiratory Questionnaire responses, 6-minute walk test results, BODE Index score, a combined cardiovascular end point, and serum inflammatory biomarker levels. Furthermore, a recent study showed that daily azithromycin significantly reduced exacerbations in high-risk patients.
Dr. Hanania disclosed that he has received grant support from the National Institutes of Health, the American Lung Association, GlaxoSmithKline (GSK), Boehringer Ingelheim (BI), Sunovion, Novartis, Pfizer, and Forest Pharmaceuticals. He also serves as a consultant for GSK, Dey Pharmaceuticals, Sunovion, Pfizer, and Forest, and is a member of the speakers bureau for GSK, BI, AstraZeneca, and Forest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Roots of Acute Worsening in ILD Elusive
HONOLULU – Acute worsening is an important part of the natural history of many interstitial lung diseases, especially idiopathic pulmonary fibrosis.
But the roots of acute worsening in interstitial lung disease (ILD) are not fully understood, Dr. Harold R. Collard said at the annual meeting of the American College of Chest Physicians.
"A lot of what’s known in the medical literature comes from patients with idiopathic pulmonary fibrosis [IPF]," said Dr. Collard, who directs the interstitial lung disease program at the University of California, San Francisco. "I think it’s an open question whether that can be extrapolated to patients with other forms of ILD or not. The course of many ILDs – certainly IPF – is unpredictable; it’s not always a linear decline," he continued. "This is an important shift in how we think about the disease – to recognize that this is the case for many patients."

According to a survey of academic pulmonologists, 88% of respondents reported that acute exacerbations in ILD patients occur "sometimes" or "frequently," while 92% of respondents reported that exacerbations were "sometimes" or "frequently" fatal (Respir. Med. 2007;101:2011-6).
If these are not fatal, they often leave patients significantly worse than they were before, unlike exacerbations in other forms of lung disease, said Dr. Collard, who was the survey’s lead investigator.
Potential causes of acute worsening include infection, aspiration, myocardial infarction, pulmonary embolism, pneumothorax, and heart failure, as well as idiopathic causes. Acute worsening has not been studied in all ILDs, but it has been most closely studied in IPF. In Dr. Collard’s opinion, the best data on acute worsening in IPF come from a Korean cohort study of 461 patients with IPF who were followed longitudinally (Eur. Resp. J. 2011;37:356-63). The researchers divided patients into two groups: those with respiratory deterioration (defined as acute worsening with radiographic abnormalities) and those with acute exacerbation (defined as acute worsening in the absence of an identifiable etiology).
The researchers found that the 1-year incidence of respiratory deterioration was 23%, "which is higher than a lot of us have taken from clinical trials," Dr. Collard said. Of these cases, 55% were idiopathic, while the remainder had known causes that included infection and heart failure.
"These idiopathic acute worsenings, as defined in this study, are what we call acute exacerbation," Dr. Collard noted. "In IPF, acute exacerbation has a specific connotation compared with asthma or [chronic obstructive pulmonary disease]. It’s an idiopathic acute worsening."
The median survival among patients with acute exacerbation of IPF was 2.2 months from the onset of exacerbation. "This is a highly morbid and fatal condition," he said.
Dr. Collard led a panel of experts that established criteria for acute exacerbations of IPF (Am. J. Respir. Crit. Care Med. 2007;176:636-43). The criteria include previous or concurrent diagnosis of IPF, unexplained worsening or development of dyspnea over a period of 30 days or less, new bilateral ground glass and/or consolidation superimposed on a usual interstitial pneumonitis pattern on high-resolution CT, no microbiologic evidence of respiratory infection by endotracheal aspirate or bronchoalveolar lavage, and exclusion of other known causes of acute worsening.
According to the Korean IPF cohort study, significant risk factors for acute exacerbation include never having smoked tobacco and having a low forced vital capacity (FVC). "The higher your FVC, the lower your risk of acute exacerbation," Dr. Collard said. "That makes sense, [but] the protective effect of smoking is hard to explain."
He acknowledged that certain aspects of acute exacerbation remain elusive. "Does exacerbation actually represent an abrupt acceleration of the underlying disease process, or is it a manifestation of an occult secondary complication such as an infection that we’re missing because of the limitations of our clinical assessment?" he asked.
Researchers who conducted a test of gene expression profiling in this patient population found no differences in the global expression pattern between patients with stable IPF and those with acute exacerbation (Am. J. Respir. Crit. Care Med. 2009;180:167-75). "They did find evidence of enhanced alveolar epithelial cell activity," Dr. Collard said. "That was the main predominant pattern."
A study of biomarkers conducted by Dr. Collard and his associates yielded similar findings (Am. J. Physiol. Lung Cell Mol. Physiol. 2010;299:L3-7).
Dr. Collard hypothesized that acute exacerbation of IPF represents a primary acceleration of IPF in the setting of acute lung stress. "This stress may be minor, at a level that would not cause clinical disease in a normal lung," he said. Potential sources of stress include infection, occult aspiration, interventions, and drugs.
Dr. Collard disclosed that he receives research funding from the National Institutes of Health, the University of California, Boehringer Ingelheim, and Genentech. He also receives consulting fees from Fibrogen, Gilead, InterMune, and Onyx.
HONOLULU – Acute worsening is an important part of the natural history of many interstitial lung diseases, especially idiopathic pulmonary fibrosis.
But the roots of acute worsening in interstitial lung disease (ILD) are not fully understood, Dr. Harold R. Collard said at the annual meeting of the American College of Chest Physicians.
"A lot of what’s known in the medical literature comes from patients with idiopathic pulmonary fibrosis [IPF]," said Dr. Collard, who directs the interstitial lung disease program at the University of California, San Francisco. "I think it’s an open question whether that can be extrapolated to patients with other forms of ILD or not. The course of many ILDs – certainly IPF – is unpredictable; it’s not always a linear decline," he continued. "This is an important shift in how we think about the disease – to recognize that this is the case for many patients."
According to a survey of academic pulmonologists, 88% of respondents reported that acute exacerbations in ILD patients occur "sometimes" or "frequently," while 92% of respondents reported that exacerbations were "sometimes" or "frequently" fatal (Respir. Med. 2007;101:2011-6).
If these are not fatal, they often leave patients significantly worse than they were before, unlike exacerbations in other forms of lung disease, said Dr. Collard, who was the survey’s lead investigator.
Potential causes of acute worsening include infection, aspiration, myocardial infarction, pulmonary embolism, pneumothorax, and heart failure, as well as idiopathic causes. Acute worsening has not been studied in all ILDs, but it has been most closely studied in IPF. In Dr. Collard’s opinion, the best data on acute worsening in IPF come from a Korean cohort study of 461 patients with IPF who were followed longitudinally (Eur. Resp. J. 2011;37:356-63). The researchers divided patients into two groups: those with respiratory deterioration (defined as acute worsening with radiographic abnormalities) and those with acute exacerbation (defined as acute worsening in the absence of an identifiable etiology).
The researchers found that the 1-year incidence of respiratory deterioration was 23%, "which is higher than a lot of us have taken from clinical trials," Dr. Collard said. Of these cases, 55% were idiopathic, while the remainder had known causes that included infection and heart failure.
"These idiopathic acute worsenings, as defined in this study, are what we call acute exacerbation," Dr. Collard noted. "In IPF, acute exacerbation has a specific connotation compared with asthma or [chronic obstructive pulmonary disease]. It’s an idiopathic acute worsening."
The median survival among patients with acute exacerbation of IPF was 2.2 months from the onset of exacerbation. "This is a highly morbid and fatal condition," he said.
Dr. Collard led a panel of experts that established criteria for acute exacerbations of IPF (Am. J. Respir. Crit. Care Med. 2007;176:636-43). The criteria include previous or concurrent diagnosis of IPF, unexplained worsening or development of dyspnea over a period of 30 days or less, new bilateral ground glass and/or consolidation superimposed on a usual interstitial pneumonitis pattern on high-resolution CT, no microbiologic evidence of respiratory infection by endotracheal aspirate or bronchoalveolar lavage, and exclusion of other known causes of acute worsening.
According to the Korean IPF cohort study, significant risk factors for acute exacerbation include never having smoked tobacco and having a low forced vital capacity (FVC). "The higher your FVC, the lower your risk of acute exacerbation," Dr. Collard said. "That makes sense, [but] the protective effect of smoking is hard to explain."
He acknowledged that certain aspects of acute exacerbation remain elusive. "Does exacerbation actually represent an abrupt acceleration of the underlying disease process, or is it a manifestation of an occult secondary complication such as an infection that we’re missing because of the limitations of our clinical assessment?" he asked.
Researchers who conducted a test of gene expression profiling in this patient population found no differences in the global expression pattern between patients with stable IPF and those with acute exacerbation (Am. J. Respir. Crit. Care Med. 2009;180:167-75). "They did find evidence of enhanced alveolar epithelial cell activity," Dr. Collard said. "That was the main predominant pattern."
A study of biomarkers conducted by Dr. Collard and his associates yielded similar findings (Am. J. Physiol. Lung Cell Mol. Physiol. 2010;299:L3-7).
Dr. Collard hypothesized that acute exacerbation of IPF represents a primary acceleration of IPF in the setting of acute lung stress. "This stress may be minor, at a level that would not cause clinical disease in a normal lung," he said. Potential sources of stress include infection, occult aspiration, interventions, and drugs.
Dr. Collard disclosed that he receives research funding from the National Institutes of Health, the University of California, Boehringer Ingelheim, and Genentech. He also receives consulting fees from Fibrogen, Gilead, InterMune, and Onyx.
HONOLULU – Acute worsening is an important part of the natural history of many interstitial lung diseases, especially idiopathic pulmonary fibrosis.
But the roots of acute worsening in interstitial lung disease (ILD) are not fully understood, Dr. Harold R. Collard said at the annual meeting of the American College of Chest Physicians.
"A lot of what’s known in the medical literature comes from patients with idiopathic pulmonary fibrosis [IPF]," said Dr. Collard, who directs the interstitial lung disease program at the University of California, San Francisco. "I think it’s an open question whether that can be extrapolated to patients with other forms of ILD or not. The course of many ILDs – certainly IPF – is unpredictable; it’s not always a linear decline," he continued. "This is an important shift in how we think about the disease – to recognize that this is the case for many patients."
According to a survey of academic pulmonologists, 88% of respondents reported that acute exacerbations in ILD patients occur "sometimes" or "frequently," while 92% of respondents reported that exacerbations were "sometimes" or "frequently" fatal (Respir. Med. 2007;101:2011-6).
If these are not fatal, they often leave patients significantly worse than they were before, unlike exacerbations in other forms of lung disease, said Dr. Collard, who was the survey’s lead investigator.
Potential causes of acute worsening include infection, aspiration, myocardial infarction, pulmonary embolism, pneumothorax, and heart failure, as well as idiopathic causes. Acute worsening has not been studied in all ILDs, but it has been most closely studied in IPF. In Dr. Collard’s opinion, the best data on acute worsening in IPF come from a Korean cohort study of 461 patients with IPF who were followed longitudinally (Eur. Resp. J. 2011;37:356-63). The researchers divided patients into two groups: those with respiratory deterioration (defined as acute worsening with radiographic abnormalities) and those with acute exacerbation (defined as acute worsening in the absence of an identifiable etiology).
The researchers found that the 1-year incidence of respiratory deterioration was 23%, "which is higher than a lot of us have taken from clinical trials," Dr. Collard said. Of these cases, 55% were idiopathic, while the remainder had known causes that included infection and heart failure.
"These idiopathic acute worsenings, as defined in this study, are what we call acute exacerbation," Dr. Collard noted. "In IPF, acute exacerbation has a specific connotation compared with asthma or [chronic obstructive pulmonary disease]. It’s an idiopathic acute worsening."
The median survival among patients with acute exacerbation of IPF was 2.2 months from the onset of exacerbation. "This is a highly morbid and fatal condition," he said.
Dr. Collard led a panel of experts that established criteria for acute exacerbations of IPF (Am. J. Respir. Crit. Care Med. 2007;176:636-43). The criteria include previous or concurrent diagnosis of IPF, unexplained worsening or development of dyspnea over a period of 30 days or less, new bilateral ground glass and/or consolidation superimposed on a usual interstitial pneumonitis pattern on high-resolution CT, no microbiologic evidence of respiratory infection by endotracheal aspirate or bronchoalveolar lavage, and exclusion of other known causes of acute worsening.
According to the Korean IPF cohort study, significant risk factors for acute exacerbation include never having smoked tobacco and having a low forced vital capacity (FVC). "The higher your FVC, the lower your risk of acute exacerbation," Dr. Collard said. "That makes sense, [but] the protective effect of smoking is hard to explain."
He acknowledged that certain aspects of acute exacerbation remain elusive. "Does exacerbation actually represent an abrupt acceleration of the underlying disease process, or is it a manifestation of an occult secondary complication such as an infection that we’re missing because of the limitations of our clinical assessment?" he asked.
Researchers who conducted a test of gene expression profiling in this patient population found no differences in the global expression pattern between patients with stable IPF and those with acute exacerbation (Am. J. Respir. Crit. Care Med. 2009;180:167-75). "They did find evidence of enhanced alveolar epithelial cell activity," Dr. Collard said. "That was the main predominant pattern."
A study of biomarkers conducted by Dr. Collard and his associates yielded similar findings (Am. J. Physiol. Lung Cell Mol. Physiol. 2010;299:L3-7).
Dr. Collard hypothesized that acute exacerbation of IPF represents a primary acceleration of IPF in the setting of acute lung stress. "This stress may be minor, at a level that would not cause clinical disease in a normal lung," he said. Potential sources of stress include infection, occult aspiration, interventions, and drugs.
Dr. Collard disclosed that he receives research funding from the National Institutes of Health, the University of California, Boehringer Ingelheim, and Genentech. He also receives consulting fees from Fibrogen, Gilead, InterMune, and Onyx.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Beta2 Agonists for Asthma in Pregnancy
Asthma continues to be one of the most common chronic conditions complicating pregnancy; approximately 8% of pregnant women in the United States report a current diagnosis. Asthmatic women are at increased risk of adverse birth outcomes and perinatal complications, including spontaneous abortion, preterm delivery, reduced birth weight, preeclampsia, and in selected studies, congenital anomalies. In some cases, these increased risks have been linked to specific medications (for example, oral corticosteroid use is linked with orofacial clefts). But much of the current evidence is also consistent with the interpretation that at least some of the excess risk can be attributed to the underlying severity/inadequate control of maternal asthma.

However, two recently published studies suggest that beta2-agonists – mainstays of treatment and control of asthma symptoms – may be associated with increased risks of congenital anomalies.
The first, an analysis conducted with data from the National Birth Defects Prevention Study, focused specifically on orofacial clefts as the outcome and bronchodilators as the exposure. Using a case control design, researchers interviewd 2,711 mothers of infants with oral clefts and 6,482 mothers of infants with no malformations in 10 states between 1997 and 2005 about bronchodilator use for asthma during and just before pregnancy. The authors separately evaluated risks for cleft lip alone, cleft lip with cleft palate, and cleft palate alone, as each of these defect categories may have distinct etiologies. Almost 3% (247 women) reported exposure to any bronchodilator in the periconceptional period, with nearly 90% of those exposures limited to the widely used short-acting beta2-agonist, albuterol.
Significantly increased risks were noted for any bronchodilator use (without an additional anti-inflammatory drug) and cleft lip alone (adjusted odds ratio, 1.77; 95% confidence interval, 1.08-2.88); however, with the addition of an anti-inflammatory drug (four cases), the odds were attenuated and no longer statistically significant. Limiting the analysis to only those reporting use of albuterol, the estimated risks for cleft lip alone (adjusted OR, 1.79; 95% CI, 1.07-2.99) and cleft palate alone (adjusted OR, 1.65; 95% CI, 1.06-2.58) were both significantly elevated. No increased risks were noted for use of any bronchodilator and cleft lip with cleft palate. If these findings represent a causal association, the estimated odds ratios would translate to less than one excess case each of cleft lip alone and cleft palate alone for every 1,000 women using albuterol in the first trimester (Hum. Reprod. 2011;26:3147-54).
Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, with possible unintended risks for both mother and baby.
As the authors pointed out, there was no mechanism in the study to adjust for the contribution of underlying disease severity/asthma symptom control in these mothers. However, the lack of an association between orofacial clefts and bronchodilators among those women who also used an anti-inflammatory drug suggests that perhaps women on polytherapy had more optimum treatment and therefore better control.
The second study used a retrospective cohort design drawing on administrative data collected between 1990 and 2002 in Quebec. The 13,117 pregnancies selected for the analysis were limited to those with a coded diagnosis of asthma and excluded women who received multiple prescriptions for oral corticosteroids in the year before pregnancy. The exposures evaluated were any prescription in the periconceptional period for a short-acting beta2-agonist rescue medication (such as albuterol), and any prescription in the periconceptional period for a long-acting beta2-agonist controller medication (such as salmeterol, available during the years of this study as a single active ingredient medication). In all, 17 categories of major congenital malformations were evaluated as outcomes, including orofacial clefts. More than 50% of pregnant women in the study filled a prescription for a short-acting drug in the first trimester, while only 1.3% received a prescription for one of the long-acting medications.
The authors found no significant associations with short-acting beta2-agonists for any of the congenital defect categories. Cases of cleft lip and cleft palate were combined, and the odds ratio after considering adjustment factors, was 1.50 (95% CI, 0.72-3.14). However, the authors did report that first trimester prescription for long-acting beta2-agonists was associated with significantly increased risks for major cardiac malformations (adjusted OR, 2.30; 95% CI, 1.11-5.10) based on seven infants exposed and "other or unspecified major malformations" (adjusted OR, 3.97; 95% CI, 1.29-12.20) based on three infants exposed (Birth Defects Res. Clin. Molec. Teratol. 2011;91:937-47).
In this study, the authors attempted to control for underlying disease severity using Canadian treatment guidelines as well as emergency room and other hospital admissions for asthma. However, no direct measure of disease severity or symptom control was collected, and unfortunately, the "lumping" of orofacial clefts (likely due to the small number of affected infants) makes comparison to the above-described study difficult. The findings with long-acting beta2-agonists, as the authors point out, could be influenced by the higher rate of more severe and less well-controlled asthma among these women, the expected higher rate of preterm delivery with associated prematurity-related defects, and/or multiple testing/chance. Finally, it has been suggested that some asthmatic women will reduce or discontinue medication in the first trimester of pregnancy based on fear of fetal exposure, not on remission of symptoms. If in fact this is the case, prescriptions filled may not reflect true usage of the drug.
With respect to previously published studies, an increased risk for congenital anomalies in general or orofacial clefts in particular, has not been suggested for albuterol. There is a lack of published data on long-acting beta2-agonists and pregnancy outcome. Thus, although neither of the two new studies reviewed above will likely change clinical practice, they both point out the need for further study of commonly-used asthma medications, and specifically, studies that incorporate direct measures of disease severity/symptom control. Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, which in turn may result in unintended risks for both mother and baby.
Dr. Chambers is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she had no relevant financial disclosures.
Asthma continues to be one of the most common chronic conditions complicating pregnancy; approximately 8% of pregnant women in the United States report a current diagnosis. Asthmatic women are at increased risk of adverse birth outcomes and perinatal complications, including spontaneous abortion, preterm delivery, reduced birth weight, preeclampsia, and in selected studies, congenital anomalies. In some cases, these increased risks have been linked to specific medications (for example, oral corticosteroid use is linked with orofacial clefts). But much of the current evidence is also consistent with the interpretation that at least some of the excess risk can be attributed to the underlying severity/inadequate control of maternal asthma.
However, two recently published studies suggest that beta2-agonists – mainstays of treatment and control of asthma symptoms – may be associated with increased risks of congenital anomalies.
The first, an analysis conducted with data from the National Birth Defects Prevention Study, focused specifically on orofacial clefts as the outcome and bronchodilators as the exposure. Using a case control design, researchers interviewd 2,711 mothers of infants with oral clefts and 6,482 mothers of infants with no malformations in 10 states between 1997 and 2005 about bronchodilator use for asthma during and just before pregnancy. The authors separately evaluated risks for cleft lip alone, cleft lip with cleft palate, and cleft palate alone, as each of these defect categories may have distinct etiologies. Almost 3% (247 women) reported exposure to any bronchodilator in the periconceptional period, with nearly 90% of those exposures limited to the widely used short-acting beta2-agonist, albuterol.
Significantly increased risks were noted for any bronchodilator use (without an additional anti-inflammatory drug) and cleft lip alone (adjusted odds ratio, 1.77; 95% confidence interval, 1.08-2.88); however, with the addition of an anti-inflammatory drug (four cases), the odds were attenuated and no longer statistically significant. Limiting the analysis to only those reporting use of albuterol, the estimated risks for cleft lip alone (adjusted OR, 1.79; 95% CI, 1.07-2.99) and cleft palate alone (adjusted OR, 1.65; 95% CI, 1.06-2.58) were both significantly elevated. No increased risks were noted for use of any bronchodilator and cleft lip with cleft palate. If these findings represent a causal association, the estimated odds ratios would translate to less than one excess case each of cleft lip alone and cleft palate alone for every 1,000 women using albuterol in the first trimester (Hum. Reprod. 2011;26:3147-54).
Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, with possible unintended risks for both mother and baby.
As the authors pointed out, there was no mechanism in the study to adjust for the contribution of underlying disease severity/asthma symptom control in these mothers. However, the lack of an association between orofacial clefts and bronchodilators among those women who also used an anti-inflammatory drug suggests that perhaps women on polytherapy had more optimum treatment and therefore better control.
The second study used a retrospective cohort design drawing on administrative data collected between 1990 and 2002 in Quebec. The 13,117 pregnancies selected for the analysis were limited to those with a coded diagnosis of asthma and excluded women who received multiple prescriptions for oral corticosteroids in the year before pregnancy. The exposures evaluated were any prescription in the periconceptional period for a short-acting beta2-agonist rescue medication (such as albuterol), and any prescription in the periconceptional period for a long-acting beta2-agonist controller medication (such as salmeterol, available during the years of this study as a single active ingredient medication). In all, 17 categories of major congenital malformations were evaluated as outcomes, including orofacial clefts. More than 50% of pregnant women in the study filled a prescription for a short-acting drug in the first trimester, while only 1.3% received a prescription for one of the long-acting medications.
The authors found no significant associations with short-acting beta2-agonists for any of the congenital defect categories. Cases of cleft lip and cleft palate were combined, and the odds ratio after considering adjustment factors, was 1.50 (95% CI, 0.72-3.14). However, the authors did report that first trimester prescription for long-acting beta2-agonists was associated with significantly increased risks for major cardiac malformations (adjusted OR, 2.30; 95% CI, 1.11-5.10) based on seven infants exposed and "other or unspecified major malformations" (adjusted OR, 3.97; 95% CI, 1.29-12.20) based on three infants exposed (Birth Defects Res. Clin. Molec. Teratol. 2011;91:937-47).
In this study, the authors attempted to control for underlying disease severity using Canadian treatment guidelines as well as emergency room and other hospital admissions for asthma. However, no direct measure of disease severity or symptom control was collected, and unfortunately, the "lumping" of orofacial clefts (likely due to the small number of affected infants) makes comparison to the above-described study difficult. The findings with long-acting beta2-agonists, as the authors point out, could be influenced by the higher rate of more severe and less well-controlled asthma among these women, the expected higher rate of preterm delivery with associated prematurity-related defects, and/or multiple testing/chance. Finally, it has been suggested that some asthmatic women will reduce or discontinue medication in the first trimester of pregnancy based on fear of fetal exposure, not on remission of symptoms. If in fact this is the case, prescriptions filled may not reflect true usage of the drug.
With respect to previously published studies, an increased risk for congenital anomalies in general or orofacial clefts in particular, has not been suggested for albuterol. There is a lack of published data on long-acting beta2-agonists and pregnancy outcome. Thus, although neither of the two new studies reviewed above will likely change clinical practice, they both point out the need for further study of commonly-used asthma medications, and specifically, studies that incorporate direct measures of disease severity/symptom control. Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, which in turn may result in unintended risks for both mother and baby.
Dr. Chambers is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she had no relevant financial disclosures.
Asthma continues to be one of the most common chronic conditions complicating pregnancy; approximately 8% of pregnant women in the United States report a current diagnosis. Asthmatic women are at increased risk of adverse birth outcomes and perinatal complications, including spontaneous abortion, preterm delivery, reduced birth weight, preeclampsia, and in selected studies, congenital anomalies. In some cases, these increased risks have been linked to specific medications (for example, oral corticosteroid use is linked with orofacial clefts). But much of the current evidence is also consistent with the interpretation that at least some of the excess risk can be attributed to the underlying severity/inadequate control of maternal asthma.
However, two recently published studies suggest that beta2-agonists – mainstays of treatment and control of asthma symptoms – may be associated with increased risks of congenital anomalies.
The first, an analysis conducted with data from the National Birth Defects Prevention Study, focused specifically on orofacial clefts as the outcome and bronchodilators as the exposure. Using a case control design, researchers interviewd 2,711 mothers of infants with oral clefts and 6,482 mothers of infants with no malformations in 10 states between 1997 and 2005 about bronchodilator use for asthma during and just before pregnancy. The authors separately evaluated risks for cleft lip alone, cleft lip with cleft palate, and cleft palate alone, as each of these defect categories may have distinct etiologies. Almost 3% (247 women) reported exposure to any bronchodilator in the periconceptional period, with nearly 90% of those exposures limited to the widely used short-acting beta2-agonist, albuterol.
Significantly increased risks were noted for any bronchodilator use (without an additional anti-inflammatory drug) and cleft lip alone (adjusted odds ratio, 1.77; 95% confidence interval, 1.08-2.88); however, with the addition of an anti-inflammatory drug (four cases), the odds were attenuated and no longer statistically significant. Limiting the analysis to only those reporting use of albuterol, the estimated risks for cleft lip alone (adjusted OR, 1.79; 95% CI, 1.07-2.99) and cleft palate alone (adjusted OR, 1.65; 95% CI, 1.06-2.58) were both significantly elevated. No increased risks were noted for use of any bronchodilator and cleft lip with cleft palate. If these findings represent a causal association, the estimated odds ratios would translate to less than one excess case each of cleft lip alone and cleft palate alone for every 1,000 women using albuterol in the first trimester (Hum. Reprod. 2011;26:3147-54).
Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, with possible unintended risks for both mother and baby.
As the authors pointed out, there was no mechanism in the study to adjust for the contribution of underlying disease severity/asthma symptom control in these mothers. However, the lack of an association between orofacial clefts and bronchodilators among those women who also used an anti-inflammatory drug suggests that perhaps women on polytherapy had more optimum treatment and therefore better control.
The second study used a retrospective cohort design drawing on administrative data collected between 1990 and 2002 in Quebec. The 13,117 pregnancies selected for the analysis were limited to those with a coded diagnosis of asthma and excluded women who received multiple prescriptions for oral corticosteroids in the year before pregnancy. The exposures evaluated were any prescription in the periconceptional period for a short-acting beta2-agonist rescue medication (such as albuterol), and any prescription in the periconceptional period for a long-acting beta2-agonist controller medication (such as salmeterol, available during the years of this study as a single active ingredient medication). In all, 17 categories of major congenital malformations were evaluated as outcomes, including orofacial clefts. More than 50% of pregnant women in the study filled a prescription for a short-acting drug in the first trimester, while only 1.3% received a prescription for one of the long-acting medications.
The authors found no significant associations with short-acting beta2-agonists for any of the congenital defect categories. Cases of cleft lip and cleft palate were combined, and the odds ratio after considering adjustment factors, was 1.50 (95% CI, 0.72-3.14). However, the authors did report that first trimester prescription for long-acting beta2-agonists was associated with significantly increased risks for major cardiac malformations (adjusted OR, 2.30; 95% CI, 1.11-5.10) based on seven infants exposed and "other or unspecified major malformations" (adjusted OR, 3.97; 95% CI, 1.29-12.20) based on three infants exposed (Birth Defects Res. Clin. Molec. Teratol. 2011;91:937-47).
In this study, the authors attempted to control for underlying disease severity using Canadian treatment guidelines as well as emergency room and other hospital admissions for asthma. However, no direct measure of disease severity or symptom control was collected, and unfortunately, the "lumping" of orofacial clefts (likely due to the small number of affected infants) makes comparison to the above-described study difficult. The findings with long-acting beta2-agonists, as the authors point out, could be influenced by the higher rate of more severe and less well-controlled asthma among these women, the expected higher rate of preterm delivery with associated prematurity-related defects, and/or multiple testing/chance. Finally, it has been suggested that some asthmatic women will reduce or discontinue medication in the first trimester of pregnancy based on fear of fetal exposure, not on remission of symptoms. If in fact this is the case, prescriptions filled may not reflect true usage of the drug.
With respect to previously published studies, an increased risk for congenital anomalies in general or orofacial clefts in particular, has not been suggested for albuterol. There is a lack of published data on long-acting beta2-agonists and pregnancy outcome. Thus, although neither of the two new studies reviewed above will likely change clinical practice, they both point out the need for further study of commonly-used asthma medications, and specifically, studies that incorporate direct measures of disease severity/symptom control. Reports of even small increased risks for asthma medications during pregnancy can further deter women from appropriate treatment, which in turn may result in unintended risks for both mother and baby.
Dr. Chambers is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she had no relevant financial disclosures.
FDA Approves Low-Dose Zolpidem for Night Awakening
A low-dose sublingual formulation of zolpidem tartrate is the first agent to be approved to treat insomnia characterized by middle-of-the-night waking followed by difficulty returning to sleep, the Food and Drug Administration announced Nov. 23.
Zolpidem tartrate was first approved in the United States in 1992 as the higher-dose formulation known as Ambien.
"For people whose insomnia causes them to wake in the middle of the night with difficulty returning to sleep, this new medication offers a safer choice than taking a higher dose of zolpidem upon waking," said Dr. Robert Temple, deputy center director for clinical science in the FDA’s Center for Drug Evaluation and Research, in a statement. "With this lower dose there is less risk of a person having too much drug in the body upon waking, which can cause dangerous drowsiness and impair driving."
Intermezzo (Transcept Pharmaceuticals Inc.) should only be used when a person has at least 4 hours of bedtime remaining. It should not be taken if alcohol has been consumed or with any other sleep aid.
The recommended and maximum dose of Intermezzo is 1.75 mg for women and 3.5 mg for men, taken once per night. The recommended dose for women is lower because women clear zolpidem from the body at a lower rate than men.
Intermezzo was studied in two clinical trials involving more than 370 patients. In the studies, patients taking the drug fell back to sleep faster after awakening as compared to people taking a placebo. The most commonly reported adverse reactions in the clinical trials were headache, nausea, and fatigue.
Potential side effects include getting out of bed while not fully awake and undertaking activities that are not remembered. Reported and not remembered activities have included driving a car, making and eating food, having sex, talking on the phone, and sleepwalking. Risks of such activities increase with use of alcohol or sedating drugs.
Intermezzo is a federally controlled substance.
A low-dose sublingual formulation of zolpidem tartrate is the first agent to be approved to treat insomnia characterized by middle-of-the-night waking followed by difficulty returning to sleep, the Food and Drug Administration announced Nov. 23.
Zolpidem tartrate was first approved in the United States in 1992 as the higher-dose formulation known as Ambien.
"For people whose insomnia causes them to wake in the middle of the night with difficulty returning to sleep, this new medication offers a safer choice than taking a higher dose of zolpidem upon waking," said Dr. Robert Temple, deputy center director for clinical science in the FDA’s Center for Drug Evaluation and Research, in a statement. "With this lower dose there is less risk of a person having too much drug in the body upon waking, which can cause dangerous drowsiness and impair driving."
Intermezzo (Transcept Pharmaceuticals Inc.) should only be used when a person has at least 4 hours of bedtime remaining. It should not be taken if alcohol has been consumed or with any other sleep aid.
The recommended and maximum dose of Intermezzo is 1.75 mg for women and 3.5 mg for men, taken once per night. The recommended dose for women is lower because women clear zolpidem from the body at a lower rate than men.
Intermezzo was studied in two clinical trials involving more than 370 patients. In the studies, patients taking the drug fell back to sleep faster after awakening as compared to people taking a placebo. The most commonly reported adverse reactions in the clinical trials were headache, nausea, and fatigue.
Potential side effects include getting out of bed while not fully awake and undertaking activities that are not remembered. Reported and not remembered activities have included driving a car, making and eating food, having sex, talking on the phone, and sleepwalking. Risks of such activities increase with use of alcohol or sedating drugs.
Intermezzo is a federally controlled substance.
A low-dose sublingual formulation of zolpidem tartrate is the first agent to be approved to treat insomnia characterized by middle-of-the-night waking followed by difficulty returning to sleep, the Food and Drug Administration announced Nov. 23.
Zolpidem tartrate was first approved in the United States in 1992 as the higher-dose formulation known as Ambien.
"For people whose insomnia causes them to wake in the middle of the night with difficulty returning to sleep, this new medication offers a safer choice than taking a higher dose of zolpidem upon waking," said Dr. Robert Temple, deputy center director for clinical science in the FDA’s Center for Drug Evaluation and Research, in a statement. "With this lower dose there is less risk of a person having too much drug in the body upon waking, which can cause dangerous drowsiness and impair driving."
Intermezzo (Transcept Pharmaceuticals Inc.) should only be used when a person has at least 4 hours of bedtime remaining. It should not be taken if alcohol has been consumed or with any other sleep aid.
The recommended and maximum dose of Intermezzo is 1.75 mg for women and 3.5 mg for men, taken once per night. The recommended dose for women is lower because women clear zolpidem from the body at a lower rate than men.
Intermezzo was studied in two clinical trials involving more than 370 patients. In the studies, patients taking the drug fell back to sleep faster after awakening as compared to people taking a placebo. The most commonly reported adverse reactions in the clinical trials were headache, nausea, and fatigue.
Potential side effects include getting out of bed while not fully awake and undertaking activities that are not remembered. Reported and not remembered activities have included driving a car, making and eating food, having sex, talking on the phone, and sleepwalking. Risks of such activities increase with use of alcohol or sedating drugs.
Intermezzo is a federally controlled substance.
Discussing End-of-Life Planning with Patients
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Additions Grow the Environmental Risk List
PHILADELPHIA – When it comes to environmental health hazards, children are canaries in the coal shaft.
That’s because children are not just scaled-down adults. "Children are a lot more vulnerable to environmental hazards than adults," Dr. Jerome A. Paulson said at a conference sponsored by the Mid-Atlantic Center for Children's Health and the Environment. Factors behind the increased vulnerability include their small mass for a given dose of food or water contamination, increased transdermal absorption due to thinner skin and increased surface-area-to-mass ratio, more hand-to-mouth activity, more time spent on the ground, higher relative minute ventilation, and a longer window of exposure due to their longer life expectancy compared with adults, said Dr. Paulson, a pediatrician at George Washington University and director of the Mid-Atlantic Center for Children’s Health and the Environment in Washington, D.C.

Children, like adults, face an ever-growing list of potential environmental hazards. Here are some of the newer additions to Dr. Paulson’s list of concerns:
• Organophosphates. This pesticide class that includes malathion has been implicated in causing adverse neurodevelopmental effects. A 2004 report linked infant exposure to decrements in memory, attention, motor tasks, and behavior (Environ. Health Perspect. 2004;112:46-51). A report last year linked detectable levels of organophosphates in children aged 8-15 years with an increased risk for attention-deficit/hyperactivity disorder (Pediatrics 2010;125:e1270-7).
• Pyrethrins. This pesticide class has grown more popular as health concerns cut sales of other pesticides. Since 2000, calls to poison control centers and visits to health facilities due to exposure to pyrethrins and the related pyrethroids steadily increased (J. Med. Toxicol. 2007;3:94-9). Pyrethrins are commonly accepted as safe for children, and are in head lice products, but their long-term neurologic effects have not been thoroughly evaluated.
• Bisphenol A (BPA). Until recently, BPA was widely used as a hardener agent in plastics, although originally it was developed as a synthetic estrogen. This led to concerns about its impact on endocrinologic function and reproduction, as well as effects on metabolism and neurodevelopment (Environ. Health Perspect. 2009;117:1945-52; Curr. Opin. Pediatr. 2011;23:233-9).
• Phthalates. This widely used plasticizer softens plastics, but also appears in a huge variety of other products including packaging, cosmetics, lotions, vinyl flooring, and fragrances. Classified as endocrine-disrupting chemicals, results from preliminary studies suggest possible effects on reproduction, a possible role as an allergen, and possible carcinogenic effects, but more study is needed (J. Med. Toxicol. 2006;2:126-35).
• Manganese. This metal in gasoline and industrial waste that can appear in air, water, and soil has been linked with impaired development in infants and toddlers and low IQ scores in children aged 11-13 years (Lancet 2006;368:2167-78).
• Arsenic. A classic heavy metal toxin that causes multi-organ system injury, it can cause neurotoxicity at chronic, low levels, producing impaired verbal IQ scores and memory (Neurotoxicology 2006;27:210-6).
• Global Climate Change. This was called by Dr. Paulson "the single most important environmental health threat to children today because it impacts every single child." It is a cause of air pollution, severe weather, vector-borne infectious diseases, floods, draughts, malnutrition, and so on.
Dr. Paulson said that he had no relevant financial disclosures.
PHILADELPHIA – When it comes to environmental health hazards, children are canaries in the coal shaft.
That’s because children are not just scaled-down adults. "Children are a lot more vulnerable to environmental hazards than adults," Dr. Jerome A. Paulson said at a conference sponsored by the Mid-Atlantic Center for Children's Health and the Environment. Factors behind the increased vulnerability include their small mass for a given dose of food or water contamination, increased transdermal absorption due to thinner skin and increased surface-area-to-mass ratio, more hand-to-mouth activity, more time spent on the ground, higher relative minute ventilation, and a longer window of exposure due to their longer life expectancy compared with adults, said Dr. Paulson, a pediatrician at George Washington University and director of the Mid-Atlantic Center for Children’s Health and the Environment in Washington, D.C.
Children, like adults, face an ever-growing list of potential environmental hazards. Here are some of the newer additions to Dr. Paulson’s list of concerns:
• Organophosphates. This pesticide class that includes malathion has been implicated in causing adverse neurodevelopmental effects. A 2004 report linked infant exposure to decrements in memory, attention, motor tasks, and behavior (Environ. Health Perspect. 2004;112:46-51). A report last year linked detectable levels of organophosphates in children aged 8-15 years with an increased risk for attention-deficit/hyperactivity disorder (Pediatrics 2010;125:e1270-7).
• Pyrethrins. This pesticide class has grown more popular as health concerns cut sales of other pesticides. Since 2000, calls to poison control centers and visits to health facilities due to exposure to pyrethrins and the related pyrethroids steadily increased (J. Med. Toxicol. 2007;3:94-9). Pyrethrins are commonly accepted as safe for children, and are in head lice products, but their long-term neurologic effects have not been thoroughly evaluated.
• Bisphenol A (BPA). Until recently, BPA was widely used as a hardener agent in plastics, although originally it was developed as a synthetic estrogen. This led to concerns about its impact on endocrinologic function and reproduction, as well as effects on metabolism and neurodevelopment (Environ. Health Perspect. 2009;117:1945-52; Curr. Opin. Pediatr. 2011;23:233-9).
• Phthalates. This widely used plasticizer softens plastics, but also appears in a huge variety of other products including packaging, cosmetics, lotions, vinyl flooring, and fragrances. Classified as endocrine-disrupting chemicals, results from preliminary studies suggest possible effects on reproduction, a possible role as an allergen, and possible carcinogenic effects, but more study is needed (J. Med. Toxicol. 2006;2:126-35).
• Manganese. This metal in gasoline and industrial waste that can appear in air, water, and soil has been linked with impaired development in infants and toddlers and low IQ scores in children aged 11-13 years (Lancet 2006;368:2167-78).
• Arsenic. A classic heavy metal toxin that causes multi-organ system injury, it can cause neurotoxicity at chronic, low levels, producing impaired verbal IQ scores and memory (Neurotoxicology 2006;27:210-6).
• Global Climate Change. This was called by Dr. Paulson "the single most important environmental health threat to children today because it impacts every single child." It is a cause of air pollution, severe weather, vector-borne infectious diseases, floods, draughts, malnutrition, and so on.
Dr. Paulson said that he had no relevant financial disclosures.
PHILADELPHIA – When it comes to environmental health hazards, children are canaries in the coal shaft.
That’s because children are not just scaled-down adults. "Children are a lot more vulnerable to environmental hazards than adults," Dr. Jerome A. Paulson said at a conference sponsored by the Mid-Atlantic Center for Children's Health and the Environment. Factors behind the increased vulnerability include their small mass for a given dose of food or water contamination, increased transdermal absorption due to thinner skin and increased surface-area-to-mass ratio, more hand-to-mouth activity, more time spent on the ground, higher relative minute ventilation, and a longer window of exposure due to their longer life expectancy compared with adults, said Dr. Paulson, a pediatrician at George Washington University and director of the Mid-Atlantic Center for Children’s Health and the Environment in Washington, D.C.
Children, like adults, face an ever-growing list of potential environmental hazards. Here are some of the newer additions to Dr. Paulson’s list of concerns:
• Organophosphates. This pesticide class that includes malathion has been implicated in causing adverse neurodevelopmental effects. A 2004 report linked infant exposure to decrements in memory, attention, motor tasks, and behavior (Environ. Health Perspect. 2004;112:46-51). A report last year linked detectable levels of organophosphates in children aged 8-15 years with an increased risk for attention-deficit/hyperactivity disorder (Pediatrics 2010;125:e1270-7).
• Pyrethrins. This pesticide class has grown more popular as health concerns cut sales of other pesticides. Since 2000, calls to poison control centers and visits to health facilities due to exposure to pyrethrins and the related pyrethroids steadily increased (J. Med. Toxicol. 2007;3:94-9). Pyrethrins are commonly accepted as safe for children, and are in head lice products, but their long-term neurologic effects have not been thoroughly evaluated.
• Bisphenol A (BPA). Until recently, BPA was widely used as a hardener agent in plastics, although originally it was developed as a synthetic estrogen. This led to concerns about its impact on endocrinologic function and reproduction, as well as effects on metabolism and neurodevelopment (Environ. Health Perspect. 2009;117:1945-52; Curr. Opin. Pediatr. 2011;23:233-9).
• Phthalates. This widely used plasticizer softens plastics, but also appears in a huge variety of other products including packaging, cosmetics, lotions, vinyl flooring, and fragrances. Classified as endocrine-disrupting chemicals, results from preliminary studies suggest possible effects on reproduction, a possible role as an allergen, and possible carcinogenic effects, but more study is needed (J. Med. Toxicol. 2006;2:126-35).
• Manganese. This metal in gasoline and industrial waste that can appear in air, water, and soil has been linked with impaired development in infants and toddlers and low IQ scores in children aged 11-13 years (Lancet 2006;368:2167-78).
• Arsenic. A classic heavy metal toxin that causes multi-organ system injury, it can cause neurotoxicity at chronic, low levels, producing impaired verbal IQ scores and memory (Neurotoxicology 2006;27:210-6).
• Global Climate Change. This was called by Dr. Paulson "the single most important environmental health threat to children today because it impacts every single child." It is a cause of air pollution, severe weather, vector-borne infectious diseases, floods, draughts, malnutrition, and so on.
Dr. Paulson said that he had no relevant financial disclosures.
EXPERT ANALYSIS FROM A CONFERENCE SPONSORED BY THE MID-ATLANTIC CENTER FOR CHILDREN'S HEALTH AND THE ENVIRONMENT
Long-Term Impairments Common in ALI/ARDS
HONOLULU – Although large numbers of patients are surviving acute lung injury/adult respiratory distress syndrome, long-term impairments are common and "striking for their relationship to neuropsychiatric dysfunction," Dr. Jesse Hall said at the annual meeting of the American College of Chest Physicians.
"The pace of recovery is protracted and likely incomplete in the current paradigm of care," said Dr. Hall, professor of medicine, anesthesia, and critical care at the University of Chicago. "Interventions including those begun at the onset of critical illness will hopefully improve these outcomes."

According to the best epidemiologic study on the topic, an estimated 191,000 cases of acute lung injury (ALI) and 141,500 cases of adult respiratory distress syndrome (ARDS) occur each year in the United States, causing a combined 133,500 deaths annually (N. Engl. J. Med 2005;353:1685-93). Implementation of low-tidal-volume ventilation over the past decade has led to an improvement in survival among this patient population, Dr. Hall said, but "we are just beginning to understand through descriptive studies what the path is for these patients down the road. We really lack many prospective trials in that arena."
One study of 109 ARDS patients who were followed for 1 year found that most developed a restrictive lung lesion that improved in the first 6-12 months (N. Engl. J. Med 2003;348:683-93). "The most consistent pulmonary function test abnormality tends to be low diffusion capacity that often resolves over time," Dr. Hall said. Some of their general functional limitation correlates to their pulmonary dysfunction, "but much of it does not," he said. "In fact, it’s not what the patients report. They start to have a very low functional status 6, 12, and more months out, and they don’t ascribe it primarily to their lung dysfunction."
Residual areas of fibrosis are not unusual on follow-up CT scans of ALI/ARDS patients, and many of these patients develop airway abnormalities such as bronchiectasis associated with their lung injury, said Dr. Hall, who is also section chief of pulmonary and critical care medicine at the University of Chicago.
The 2003 study of 109 ARDS patients found that all subjects reported poor function due to loss of muscle bulk, proximal weakness, and fatigue. Some (12%) reported persistent pain at the chest tube site, 7% reported entrapment neuropathies, 7% had tracheotomy site problems, 5% had large joint enlargement/immobility from heterotopic ossification, and 4% had immobility in the form of contracted fingers or frozen shoulders. "It can be up to a year before patients regain their body weight after this episode," Dr. Hall said.
Neuromuscular sequelae may include myopathy, peripheral neuropathy, or deconditioning. "Any given patient can have any combination of those," he said. "Some of these disorders are reasonably strongly associated with some of our therapies. Most of our patients have a combination of peripheral neuropathies and myopathies that may by themselves be modest but are attended by extreme deconditioning. The neuromuscular sequelae of critical illness are variable in terms of recovery over months and years, and some patients seem to never fully recover."
The impact of neuropsychiatric sequelae can be significant. One study of 55 ARDS patients found that 100% had cognitive and affective impairments at hospital discharge, and 30% had generalized cognitive decline 1 year later (Am. J. Respir. Crit. Care Med. 1999;160:50-6). In the 2003 study, only 49% of the ARDS patients who had been employed were back to work at 1 year. "This is an astounding economic and financial consequence for the patient and the family," Dr. Hall commented. "Scores on the Short Form-36 were below normal in all eight domains at 3-, 6-, and 12-month follow-up from ICU discharge. There were improvements in most SF-36 categories, but almost none were back to normal."
Dr. Hall said that changes in the current health care system are needed to improve outcomes for ALI/ARDS patients. Currently, "it’s difficult for those in our discipline to figure out how to become a change agent, or help our patients acquire what they need to optimize their recovery," he explained. "It’s not likely, in fact, to be done by critical care doctors down the road."
One study from the United Kingdom sought to determine if giving patients a self-help rehabilitation manual would affect their general functional status "and therefore their psychiatric axes as well, and maybe even make them more functional," Dr. Hall said. For the study, patients in the control group received ward visits, three telephone calls at home, and clinic appointments at 8 weeks and 6 months, whereas patients in the intervention group received the same plus a 6-week self-help rehabilitation manual. At the end of 6 weeks, patients in the intervention group had significantly better physical function scores, compared with controls (Crit. Care Med. 2003;31:2456-61). Unfortunately, such benefits were not seen in another recent prospective trial.
In a recent trial conducted by a group of researchers that included Dr. Hall, 104 critical care patients who required ventilation were randomized to either early physical and occupational therapy during periods of daily interruption of sedation, or to daily interruption of sedation with therapy as ordered by the primary care team (Lancet 2009;373:1874-82). Compared with controls, patients who received early physical and occupational therapy had better return to independent functional status at hospital discharge (59% vs. 35%, respectively) and less ICU delirium (2 days vs. 4 days).
Dr. Hall concluded by noting that the brain and the neurologic and musculoskeletal systems "are likely the last to recover after ALI/ARDS, and may not recover fully to the status patients had before. We don’t know what matters most for long-term recovery. It’s reasonable to think that shortening ICU and mechanical ventilation time would be beneficial."
Dr. Hall disclosed that he receives honoraria from the American College of Chest Physicians and the American Thoracic Society.
HONOLULU – Although large numbers of patients are surviving acute lung injury/adult respiratory distress syndrome, long-term impairments are common and "striking for their relationship to neuropsychiatric dysfunction," Dr. Jesse Hall said at the annual meeting of the American College of Chest Physicians.
"The pace of recovery is protracted and likely incomplete in the current paradigm of care," said Dr. Hall, professor of medicine, anesthesia, and critical care at the University of Chicago. "Interventions including those begun at the onset of critical illness will hopefully improve these outcomes."
According to the best epidemiologic study on the topic, an estimated 191,000 cases of acute lung injury (ALI) and 141,500 cases of adult respiratory distress syndrome (ARDS) occur each year in the United States, causing a combined 133,500 deaths annually (N. Engl. J. Med 2005;353:1685-93). Implementation of low-tidal-volume ventilation over the past decade has led to an improvement in survival among this patient population, Dr. Hall said, but "we are just beginning to understand through descriptive studies what the path is for these patients down the road. We really lack many prospective trials in that arena."
One study of 109 ARDS patients who were followed for 1 year found that most developed a restrictive lung lesion that improved in the first 6-12 months (N. Engl. J. Med 2003;348:683-93). "The most consistent pulmonary function test abnormality tends to be low diffusion capacity that often resolves over time," Dr. Hall said. Some of their general functional limitation correlates to their pulmonary dysfunction, "but much of it does not," he said. "In fact, it’s not what the patients report. They start to have a very low functional status 6, 12, and more months out, and they don’t ascribe it primarily to their lung dysfunction."
Residual areas of fibrosis are not unusual on follow-up CT scans of ALI/ARDS patients, and many of these patients develop airway abnormalities such as bronchiectasis associated with their lung injury, said Dr. Hall, who is also section chief of pulmonary and critical care medicine at the University of Chicago.
The 2003 study of 109 ARDS patients found that all subjects reported poor function due to loss of muscle bulk, proximal weakness, and fatigue. Some (12%) reported persistent pain at the chest tube site, 7% reported entrapment neuropathies, 7% had tracheotomy site problems, 5% had large joint enlargement/immobility from heterotopic ossification, and 4% had immobility in the form of contracted fingers or frozen shoulders. "It can be up to a year before patients regain their body weight after this episode," Dr. Hall said.
Neuromuscular sequelae may include myopathy, peripheral neuropathy, or deconditioning. "Any given patient can have any combination of those," he said. "Some of these disorders are reasonably strongly associated with some of our therapies. Most of our patients have a combination of peripheral neuropathies and myopathies that may by themselves be modest but are attended by extreme deconditioning. The neuromuscular sequelae of critical illness are variable in terms of recovery over months and years, and some patients seem to never fully recover."
The impact of neuropsychiatric sequelae can be significant. One study of 55 ARDS patients found that 100% had cognitive and affective impairments at hospital discharge, and 30% had generalized cognitive decline 1 year later (Am. J. Respir. Crit. Care Med. 1999;160:50-6). In the 2003 study, only 49% of the ARDS patients who had been employed were back to work at 1 year. "This is an astounding economic and financial consequence for the patient and the family," Dr. Hall commented. "Scores on the Short Form-36 were below normal in all eight domains at 3-, 6-, and 12-month follow-up from ICU discharge. There were improvements in most SF-36 categories, but almost none were back to normal."
Dr. Hall said that changes in the current health care system are needed to improve outcomes for ALI/ARDS patients. Currently, "it’s difficult for those in our discipline to figure out how to become a change agent, or help our patients acquire what they need to optimize their recovery," he explained. "It’s not likely, in fact, to be done by critical care doctors down the road."
One study from the United Kingdom sought to determine if giving patients a self-help rehabilitation manual would affect their general functional status "and therefore their psychiatric axes as well, and maybe even make them more functional," Dr. Hall said. For the study, patients in the control group received ward visits, three telephone calls at home, and clinic appointments at 8 weeks and 6 months, whereas patients in the intervention group received the same plus a 6-week self-help rehabilitation manual. At the end of 6 weeks, patients in the intervention group had significantly better physical function scores, compared with controls (Crit. Care Med. 2003;31:2456-61). Unfortunately, such benefits were not seen in another recent prospective trial.
In a recent trial conducted by a group of researchers that included Dr. Hall, 104 critical care patients who required ventilation were randomized to either early physical and occupational therapy during periods of daily interruption of sedation, or to daily interruption of sedation with therapy as ordered by the primary care team (Lancet 2009;373:1874-82). Compared with controls, patients who received early physical and occupational therapy had better return to independent functional status at hospital discharge (59% vs. 35%, respectively) and less ICU delirium (2 days vs. 4 days).
Dr. Hall concluded by noting that the brain and the neurologic and musculoskeletal systems "are likely the last to recover after ALI/ARDS, and may not recover fully to the status patients had before. We don’t know what matters most for long-term recovery. It’s reasonable to think that shortening ICU and mechanical ventilation time would be beneficial."
Dr. Hall disclosed that he receives honoraria from the American College of Chest Physicians and the American Thoracic Society.
HONOLULU – Although large numbers of patients are surviving acute lung injury/adult respiratory distress syndrome, long-term impairments are common and "striking for their relationship to neuropsychiatric dysfunction," Dr. Jesse Hall said at the annual meeting of the American College of Chest Physicians.
"The pace of recovery is protracted and likely incomplete in the current paradigm of care," said Dr. Hall, professor of medicine, anesthesia, and critical care at the University of Chicago. "Interventions including those begun at the onset of critical illness will hopefully improve these outcomes."
According to the best epidemiologic study on the topic, an estimated 191,000 cases of acute lung injury (ALI) and 141,500 cases of adult respiratory distress syndrome (ARDS) occur each year in the United States, causing a combined 133,500 deaths annually (N. Engl. J. Med 2005;353:1685-93). Implementation of low-tidal-volume ventilation over the past decade has led to an improvement in survival among this patient population, Dr. Hall said, but "we are just beginning to understand through descriptive studies what the path is for these patients down the road. We really lack many prospective trials in that arena."
One study of 109 ARDS patients who were followed for 1 year found that most developed a restrictive lung lesion that improved in the first 6-12 months (N. Engl. J. Med 2003;348:683-93). "The most consistent pulmonary function test abnormality tends to be low diffusion capacity that often resolves over time," Dr. Hall said. Some of their general functional limitation correlates to their pulmonary dysfunction, "but much of it does not," he said. "In fact, it’s not what the patients report. They start to have a very low functional status 6, 12, and more months out, and they don’t ascribe it primarily to their lung dysfunction."
Residual areas of fibrosis are not unusual on follow-up CT scans of ALI/ARDS patients, and many of these patients develop airway abnormalities such as bronchiectasis associated with their lung injury, said Dr. Hall, who is also section chief of pulmonary and critical care medicine at the University of Chicago.
The 2003 study of 109 ARDS patients found that all subjects reported poor function due to loss of muscle bulk, proximal weakness, and fatigue. Some (12%) reported persistent pain at the chest tube site, 7% reported entrapment neuropathies, 7% had tracheotomy site problems, 5% had large joint enlargement/immobility from heterotopic ossification, and 4% had immobility in the form of contracted fingers or frozen shoulders. "It can be up to a year before patients regain their body weight after this episode," Dr. Hall said.
Neuromuscular sequelae may include myopathy, peripheral neuropathy, or deconditioning. "Any given patient can have any combination of those," he said. "Some of these disorders are reasonably strongly associated with some of our therapies. Most of our patients have a combination of peripheral neuropathies and myopathies that may by themselves be modest but are attended by extreme deconditioning. The neuromuscular sequelae of critical illness are variable in terms of recovery over months and years, and some patients seem to never fully recover."
The impact of neuropsychiatric sequelae can be significant. One study of 55 ARDS patients found that 100% had cognitive and affective impairments at hospital discharge, and 30% had generalized cognitive decline 1 year later (Am. J. Respir. Crit. Care Med. 1999;160:50-6). In the 2003 study, only 49% of the ARDS patients who had been employed were back to work at 1 year. "This is an astounding economic and financial consequence for the patient and the family," Dr. Hall commented. "Scores on the Short Form-36 were below normal in all eight domains at 3-, 6-, and 12-month follow-up from ICU discharge. There were improvements in most SF-36 categories, but almost none were back to normal."
Dr. Hall said that changes in the current health care system are needed to improve outcomes for ALI/ARDS patients. Currently, "it’s difficult for those in our discipline to figure out how to become a change agent, or help our patients acquire what they need to optimize their recovery," he explained. "It’s not likely, in fact, to be done by critical care doctors down the road."
One study from the United Kingdom sought to determine if giving patients a self-help rehabilitation manual would affect their general functional status "and therefore their psychiatric axes as well, and maybe even make them more functional," Dr. Hall said. For the study, patients in the control group received ward visits, three telephone calls at home, and clinic appointments at 8 weeks and 6 months, whereas patients in the intervention group received the same plus a 6-week self-help rehabilitation manual. At the end of 6 weeks, patients in the intervention group had significantly better physical function scores, compared with controls (Crit. Care Med. 2003;31:2456-61). Unfortunately, such benefits were not seen in another recent prospective trial.
In a recent trial conducted by a group of researchers that included Dr. Hall, 104 critical care patients who required ventilation were randomized to either early physical and occupational therapy during periods of daily interruption of sedation, or to daily interruption of sedation with therapy as ordered by the primary care team (Lancet 2009;373:1874-82). Compared with controls, patients who received early physical and occupational therapy had better return to independent functional status at hospital discharge (59% vs. 35%, respectively) and less ICU delirium (2 days vs. 4 days).
Dr. Hall concluded by noting that the brain and the neurologic and musculoskeletal systems "are likely the last to recover after ALI/ARDS, and may not recover fully to the status patients had before. We don’t know what matters most for long-term recovery. It’s reasonable to think that shortening ICU and mechanical ventilation time would be beneficial."
Dr. Hall disclosed that he receives honoraria from the American College of Chest Physicians and the American Thoracic Society.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Overweight Patients Don't Have Higher Risk of Death After Surgery
HONOLULU – Having a higher body mass index is not significantly associated with hospital mortality among patients admitted to the surgical ICU.
While similar findings have been reported in medical ICUs, this is believed to be the largest study to investigate the relationship between BMI and mortality exclusively in a surgical ICU, Dr. Adam Khader said in an interview during a poster session at the annual meeting of the American College of Chest Physicians.

Dr. Khader, a resident in the department of surgery at Hofstra North Shore–Long Island Jewish Medical Center, Manhasset, N.Y., and his associates evaluated the records of 1,860 patients admitted to the medical center’s surgical ICU. Patients younger than age 18 years and those who did not undergo surgery were excluded from the analysis. The researchers used area under the receiver operating characteristic curves to assess the effect of BMI on mortality and categorized patients as underweight (BMI less than 20 kg/m2), normal weight (20-25 kg/m2), overweight (25-30 kg/m2), obese (30-35 kg/m2), severely obese (35-50 kg/m2), and super obese (greater than 50 kg/m2).
Overall 30-day hospital mortality was 10%. Hospital mortality was 15% for underweight patients, 11% for normal weight patients, 8% for overweight patients, 9% for obese patients, 13% for severely obese patients, and 22% for super obese patients. Area under the receiver operating characteristic curve analysis yielded no significant association between BMI and mortality, even after stratification of patients by elective vs. emergent surgery, and patients younger vs. older than age 75 years.
Dr. Khader and his associates observed a trend toward increased mortality for patients in the underweight, obese, and severely obese categories of BMI, "but nothing statistically significant," he said. "Still, there was a large number of patients [in this study]. You can’t really ignore the numbers."
Dr. Khader said that he had no relevant financial conflicts to disclose.
HONOLULU – Having a higher body mass index is not significantly associated with hospital mortality among patients admitted to the surgical ICU.
While similar findings have been reported in medical ICUs, this is believed to be the largest study to investigate the relationship between BMI and mortality exclusively in a surgical ICU, Dr. Adam Khader said in an interview during a poster session at the annual meeting of the American College of Chest Physicians.
Dr. Khader, a resident in the department of surgery at Hofstra North Shore–Long Island Jewish Medical Center, Manhasset, N.Y., and his associates evaluated the records of 1,860 patients admitted to the medical center’s surgical ICU. Patients younger than age 18 years and those who did not undergo surgery were excluded from the analysis. The researchers used area under the receiver operating characteristic curves to assess the effect of BMI on mortality and categorized patients as underweight (BMI less than 20 kg/m2), normal weight (20-25 kg/m2), overweight (25-30 kg/m2), obese (30-35 kg/m2), severely obese (35-50 kg/m2), and super obese (greater than 50 kg/m2).
Overall 30-day hospital mortality was 10%. Hospital mortality was 15% for underweight patients, 11% for normal weight patients, 8% for overweight patients, 9% for obese patients, 13% for severely obese patients, and 22% for super obese patients. Area under the receiver operating characteristic curve analysis yielded no significant association between BMI and mortality, even after stratification of patients by elective vs. emergent surgery, and patients younger vs. older than age 75 years.
Dr. Khader and his associates observed a trend toward increased mortality for patients in the underweight, obese, and severely obese categories of BMI, "but nothing statistically significant," he said. "Still, there was a large number of patients [in this study]. You can’t really ignore the numbers."
Dr. Khader said that he had no relevant financial conflicts to disclose.
HONOLULU – Having a higher body mass index is not significantly associated with hospital mortality among patients admitted to the surgical ICU.
While similar findings have been reported in medical ICUs, this is believed to be the largest study to investigate the relationship between BMI and mortality exclusively in a surgical ICU, Dr. Adam Khader said in an interview during a poster session at the annual meeting of the American College of Chest Physicians.
Dr. Khader, a resident in the department of surgery at Hofstra North Shore–Long Island Jewish Medical Center, Manhasset, N.Y., and his associates evaluated the records of 1,860 patients admitted to the medical center’s surgical ICU. Patients younger than age 18 years and those who did not undergo surgery were excluded from the analysis. The researchers used area under the receiver operating characteristic curves to assess the effect of BMI on mortality and categorized patients as underweight (BMI less than 20 kg/m2), normal weight (20-25 kg/m2), overweight (25-30 kg/m2), obese (30-35 kg/m2), severely obese (35-50 kg/m2), and super obese (greater than 50 kg/m2).
Overall 30-day hospital mortality was 10%. Hospital mortality was 15% for underweight patients, 11% for normal weight patients, 8% for overweight patients, 9% for obese patients, 13% for severely obese patients, and 22% for super obese patients. Area under the receiver operating characteristic curve analysis yielded no significant association between BMI and mortality, even after stratification of patients by elective vs. emergent surgery, and patients younger vs. older than age 75 years.
Dr. Khader and his associates observed a trend toward increased mortality for patients in the underweight, obese, and severely obese categories of BMI, "but nothing statistically significant," he said. "Still, there was a large number of patients [in this study]. You can’t really ignore the numbers."
Dr. Khader said that he had no relevant financial conflicts to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Body mass index is not an independent risk factor associated with hospital mortality in patients admitted to the surgical ICU.
Data Source: A study of 1,860 patients admitted to the surgical ICU at Hofstra North Shore–Long Island Jewish Medical Center.
Disclosures: Dr. Khader said that he had no relevant financial conflicts to disclose.
Criteria Shift for Lung Transplantation Candidacy
HONOLULU – Not long ago, patients older than 65 years were rarely considered candidates for lung transplantation. But that’s not quite true anymore.
Being elderly is still a relative contraindication, but according to data from the International Society for Heart and Lung Transplantation, an increasing proportion of people older than age 65 are receiving lung transplants, from about 2% in 1995-1999 to about 6% between 2000 and June of 2010.

Instead of age and the length of time spent on the list waiting for a transplant, candidacy for the procedure is now based on whether patients’ advanced respiratory disease has progressed despite medical therapy, and whether they have a 50% or less chance of survival in the next 2-3 years, Dr. Luis F. Angel explained at the annual meeting of the American College of Chest Physicians.
"Potential candidates must be capable of comprehending the procedure, undergoing the selection process, and waiting the time necessary on the waiting list," said Dr. Angel, director of lung transplantation for the University of Texas Health Science Center at San Antonio.
In a review of the latest criteria, he explained that patients "must also be free of significant medical comorbidities and be sufficiently fit to handle this major surgical procedure and multiple medications post procedure."
The list of absolute contraindications for lung transplantation is lengthy, and includes recent malignancy (other than nonmelanoma skin cancer); infection with HIV; infection with hepatitis B or C with histologic evidence of cirrhosis; active cigarette smoking or substance abuse; severe and untreated psychiatric illness; documented noncompliance with medical care; and absence of a reliable social network.
Relative contraindications, Dr. Angel said, include the clinical state at the moment of notification or referral, such as the presence of hemodynamic instability, excessive physical deterioration, or severe muscle atrophy that impedes performing outpatient rehabilitation. Also taken into account is the need for invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO) support.
"Colonization by multiresistant or panresistant bacteria, fungus, or mycobacteria is another contraindication," Dr. Angel said, "as are other medical conditions such as coronary artery disease, liver and renal disease, gastroesophageal reflux, or symptomatic osteoporosis, and having a body mass index higher than 30 kg/m2."
Regarding the following specific indication for transplantation, the success rates vary according to the condition:
• COPD/emphysema. In a select group of patients with COPD/emphysema, transplantation provides both survival and quality of life benefits.
Referral criteria include a BODE index of 7-10 points, or at least one of the following: a history of hospitalization for exacerbation associated with acute hypercapnia; pulmonary hypertension or cor pulmonale, or both, despite oxygen therapy; and an FEV1 (forced expiratory volume in 1 second) of less than 20% and either a DLCO (diffusing capacity of the lungs for carbon monoxide) finding of less than 20% or homogenous distribution of emphysema.
• Pulmonary fibrosis. "The natural history of the disease is more predictable, and there are major limitations in effective therapy for this diagnosis," said Dr. Angel of the department of pulmonary and critical care medicine at the university.
Referral criteria, he said, include histologic or radiographic evidence of interstitial pneumonia, and any of the following: a DLCO of less than 39% predicted; a 10% or greater decrement in forced vital capacity during 6 months of follow-up; a decrease in pulse oximetry less than 88% during a 6-minute walk test; honeycombing on high-resolution CT; or development of secondary pulmonary hypertension.
• Cystic fibrosis. Patients with this condition "can get the most significant benefit and prolonged survival with lung transplantation," Dr. Angel said. "Referrals are often delayed, as there is [a] high emotional aspect in the management of these patients and their families."
Referral criteria, he said, include a FEV1 of less than 30% of predicted, or rapidly declining lung function if FEV1 is greater than 30% of predicted, and/or any of the following: increasing oxygen requirements, hypercapnia, and pulmonary hypertension.
• Idiopathic PAH (pulmonary arterial hypertension). "This is one of the most difficult conditions [in which] to determine the right time for transplantation," Dr. Angel said. "Significant improvements with medical therapy and increased awareness of the disease have decreased the number of lung transplants for this indication."
Referral criteria, he said, include persistent New York Heart Association class III or IV on maximal medical therapy; low or declining 6-minute walk test findings; failing therapy with intravenous epoprostenol or equivalent; a cardiac index of less than 2 L/min per square meter, or a right atrial pressure exceeding 15 mm Hg.
Dr. Angel said that he had no relevant financial conflicts to disclose.
elderly, the International Society for Heart and Lung Transplantation, lung transplants, Dr. Luis F. Angel, the American College of Chest Physicians, contraindications for lung transplantation,
HONOLULU – Not long ago, patients older than 65 years were rarely considered candidates for lung transplantation. But that’s not quite true anymore.
Being elderly is still a relative contraindication, but according to data from the International Society for Heart and Lung Transplantation, an increasing proportion of people older than age 65 are receiving lung transplants, from about 2% in 1995-1999 to about 6% between 2000 and June of 2010.
Instead of age and the length of time spent on the list waiting for a transplant, candidacy for the procedure is now based on whether patients’ advanced respiratory disease has progressed despite medical therapy, and whether they have a 50% or less chance of survival in the next 2-3 years, Dr. Luis F. Angel explained at the annual meeting of the American College of Chest Physicians.
"Potential candidates must be capable of comprehending the procedure, undergoing the selection process, and waiting the time necessary on the waiting list," said Dr. Angel, director of lung transplantation for the University of Texas Health Science Center at San Antonio.
In a review of the latest criteria, he explained that patients "must also be free of significant medical comorbidities and be sufficiently fit to handle this major surgical procedure and multiple medications post procedure."
The list of absolute contraindications for lung transplantation is lengthy, and includes recent malignancy (other than nonmelanoma skin cancer); infection with HIV; infection with hepatitis B or C with histologic evidence of cirrhosis; active cigarette smoking or substance abuse; severe and untreated psychiatric illness; documented noncompliance with medical care; and absence of a reliable social network.
Relative contraindications, Dr. Angel said, include the clinical state at the moment of notification or referral, such as the presence of hemodynamic instability, excessive physical deterioration, or severe muscle atrophy that impedes performing outpatient rehabilitation. Also taken into account is the need for invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO) support.
"Colonization by multiresistant or panresistant bacteria, fungus, or mycobacteria is another contraindication," Dr. Angel said, "as are other medical conditions such as coronary artery disease, liver and renal disease, gastroesophageal reflux, or symptomatic osteoporosis, and having a body mass index higher than 30 kg/m2."
Regarding the following specific indication for transplantation, the success rates vary according to the condition:
• COPD/emphysema. In a select group of patients with COPD/emphysema, transplantation provides both survival and quality of life benefits.
Referral criteria include a BODE index of 7-10 points, or at least one of the following: a history of hospitalization for exacerbation associated with acute hypercapnia; pulmonary hypertension or cor pulmonale, or both, despite oxygen therapy; and an FEV1 (forced expiratory volume in 1 second) of less than 20% and either a DLCO (diffusing capacity of the lungs for carbon monoxide) finding of less than 20% or homogenous distribution of emphysema.
• Pulmonary fibrosis. "The natural history of the disease is more predictable, and there are major limitations in effective therapy for this diagnosis," said Dr. Angel of the department of pulmonary and critical care medicine at the university.
Referral criteria, he said, include histologic or radiographic evidence of interstitial pneumonia, and any of the following: a DLCO of less than 39% predicted; a 10% or greater decrement in forced vital capacity during 6 months of follow-up; a decrease in pulse oximetry less than 88% during a 6-minute walk test; honeycombing on high-resolution CT; or development of secondary pulmonary hypertension.
• Cystic fibrosis. Patients with this condition "can get the most significant benefit and prolonged survival with lung transplantation," Dr. Angel said. "Referrals are often delayed, as there is [a] high emotional aspect in the management of these patients and their families."
Referral criteria, he said, include a FEV1 of less than 30% of predicted, or rapidly declining lung function if FEV1 is greater than 30% of predicted, and/or any of the following: increasing oxygen requirements, hypercapnia, and pulmonary hypertension.
• Idiopathic PAH (pulmonary arterial hypertension). "This is one of the most difficult conditions [in which] to determine the right time for transplantation," Dr. Angel said. "Significant improvements with medical therapy and increased awareness of the disease have decreased the number of lung transplants for this indication."
Referral criteria, he said, include persistent New York Heart Association class III or IV on maximal medical therapy; low or declining 6-minute walk test findings; failing therapy with intravenous epoprostenol or equivalent; a cardiac index of less than 2 L/min per square meter, or a right atrial pressure exceeding 15 mm Hg.
Dr. Angel said that he had no relevant financial conflicts to disclose.
HONOLULU – Not long ago, patients older than 65 years were rarely considered candidates for lung transplantation. But that’s not quite true anymore.
Being elderly is still a relative contraindication, but according to data from the International Society for Heart and Lung Transplantation, an increasing proportion of people older than age 65 are receiving lung transplants, from about 2% in 1995-1999 to about 6% between 2000 and June of 2010.
Instead of age and the length of time spent on the list waiting for a transplant, candidacy for the procedure is now based on whether patients’ advanced respiratory disease has progressed despite medical therapy, and whether they have a 50% or less chance of survival in the next 2-3 years, Dr. Luis F. Angel explained at the annual meeting of the American College of Chest Physicians.
"Potential candidates must be capable of comprehending the procedure, undergoing the selection process, and waiting the time necessary on the waiting list," said Dr. Angel, director of lung transplantation for the University of Texas Health Science Center at San Antonio.
In a review of the latest criteria, he explained that patients "must also be free of significant medical comorbidities and be sufficiently fit to handle this major surgical procedure and multiple medications post procedure."
The list of absolute contraindications for lung transplantation is lengthy, and includes recent malignancy (other than nonmelanoma skin cancer); infection with HIV; infection with hepatitis B or C with histologic evidence of cirrhosis; active cigarette smoking or substance abuse; severe and untreated psychiatric illness; documented noncompliance with medical care; and absence of a reliable social network.
Relative contraindications, Dr. Angel said, include the clinical state at the moment of notification or referral, such as the presence of hemodynamic instability, excessive physical deterioration, or severe muscle atrophy that impedes performing outpatient rehabilitation. Also taken into account is the need for invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO) support.
"Colonization by multiresistant or panresistant bacteria, fungus, or mycobacteria is another contraindication," Dr. Angel said, "as are other medical conditions such as coronary artery disease, liver and renal disease, gastroesophageal reflux, or symptomatic osteoporosis, and having a body mass index higher than 30 kg/m2."
Regarding the following specific indication for transplantation, the success rates vary according to the condition:
• COPD/emphysema. In a select group of patients with COPD/emphysema, transplantation provides both survival and quality of life benefits.
Referral criteria include a BODE index of 7-10 points, or at least one of the following: a history of hospitalization for exacerbation associated with acute hypercapnia; pulmonary hypertension or cor pulmonale, or both, despite oxygen therapy; and an FEV1 (forced expiratory volume in 1 second) of less than 20% and either a DLCO (diffusing capacity of the lungs for carbon monoxide) finding of less than 20% or homogenous distribution of emphysema.
• Pulmonary fibrosis. "The natural history of the disease is more predictable, and there are major limitations in effective therapy for this diagnosis," said Dr. Angel of the department of pulmonary and critical care medicine at the university.
Referral criteria, he said, include histologic or radiographic evidence of interstitial pneumonia, and any of the following: a DLCO of less than 39% predicted; a 10% or greater decrement in forced vital capacity during 6 months of follow-up; a decrease in pulse oximetry less than 88% during a 6-minute walk test; honeycombing on high-resolution CT; or development of secondary pulmonary hypertension.
• Cystic fibrosis. Patients with this condition "can get the most significant benefit and prolonged survival with lung transplantation," Dr. Angel said. "Referrals are often delayed, as there is [a] high emotional aspect in the management of these patients and their families."
Referral criteria, he said, include a FEV1 of less than 30% of predicted, or rapidly declining lung function if FEV1 is greater than 30% of predicted, and/or any of the following: increasing oxygen requirements, hypercapnia, and pulmonary hypertension.
• Idiopathic PAH (pulmonary arterial hypertension). "This is one of the most difficult conditions [in which] to determine the right time for transplantation," Dr. Angel said. "Significant improvements with medical therapy and increased awareness of the disease have decreased the number of lung transplants for this indication."
Referral criteria, he said, include persistent New York Heart Association class III or IV on maximal medical therapy; low or declining 6-minute walk test findings; failing therapy with intravenous epoprostenol or equivalent; a cardiac index of less than 2 L/min per square meter, or a right atrial pressure exceeding 15 mm Hg.
Dr. Angel said that he had no relevant financial conflicts to disclose.
elderly, the International Society for Heart and Lung Transplantation, lung transplants, Dr. Luis F. Angel, the American College of Chest Physicians, contraindications for lung transplantation,
elderly, the International Society for Heart and Lung Transplantation, lung transplants, Dr. Luis F. Angel, the American College of Chest Physicians, contraindications for lung transplantation,
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS