User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
CHEST-1 Study: Riociguat Shows Efficacy in CTEPH
ATLANTA – Riociguat, a novel first-in-class soluble guanylate cyclase stimulator, significantly improved 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension in the randomized, placebo-controlled phase III CHEST-1 study.
The overall 46-m improvement in 6-minute walk distance at 16 weeks in the study population was largely attributable to improvements in the 173 patients randomized to receive riociguat treatment, as opposed to improvements in 88 patients who received placebo, Dr. Hossein A. Ghofrani reported at the annual meeting of the American College of Chest Physicians.
The improvement in the treatment group was progressive and had not reached a plateau at 16 weeks after treatment initiation. Meanwhile, an initial improvement in the placebo group was followed by a constant decline in the placebo group, said Dr. Ghofrani of University Hospital Giessen and Marburg in Germany.
Treatment also was associated with consistent, significant improvements in a number of secondary end points, including change in pulmonary vascular resistance (PVR), change in World Health Organization functional class, time to clinical worsening, change in Borg dyspnea score, and quality of life assessments, he said.
Hemodynamics were robustly improved, he added, noting that treatment was associated with a 32% reduction in PVR, which translated into a highly significant 246-dyne reduction.
Patients enrolled in the multicenter CHEST-1 study – the largest placebo-controlled study to date of chronic thromboembolic pulmonary hypertension (CTEPH), for which there are currently no approved medical treatments – were aged 18-80 years with either inoperable disease or persistent or recurrent pulmonary hypertension after pulmonary endarterectomy. They had a mean PVR of greater than 480 dyn.s/cm5.
Treatment with riociguat was initiated at an oral dose of 1 mg three times daily titrated up to a maximum of 2.5 mg three times daily as tolerated according to systolic blood pressure; 90% achieved the highest dose, attesting to the tolerability of the drug, Dr. Ghofrani said.
In fact, the adverse event rate was very low, and side effects were similar to those seen in the PATENT-1 trial of riociguat for pulmonary arterial hypertension (PAH), which also was reported at the meeting.
These included headache, dizziness, peripheral edema (which occurred more often in the placebo group), cough, dyspnea, nasopharyngitis, nausea, diarrhea, and vomiting.
The findings are encouraging given the lack of medical treatments for CETPH patients who either are ineligible for surgical treatment or have persistent pulmonary hypertension after surgery, Dr. Ghofrani said.
The study of riociguat for CETPH is ongoing. CHEST-1 completers were allowed to enroll in a long-term extension study (CHEST-2), and results of that study will be reported next year, Dr. Ghofrani said.
As for how it is that a single molecule appears to have efficacy for two distinct pulmonary hypertension subgroups (PAH and CETPH), which are believed to have differing pathophysiological mechanisms, he explained that the disease might have some "common denominators."
"After a certain level of severity, they have a lot of commonalities, and the progressive component, for instance for pulmonary vascular remodeling beyond a certain point of no return, becomes very much alike in the different disease entities. The lack of the endogenous [nitric oxide] signaling pathway has been proven for many of these diseases. ... I think there may be a common denominator for the disease, even if the underlying pathophysiology may be different," he explained.
This is not to say riociguat is a "magic bullet" for all pulmonary hypertension subgroups, he added.
The drug’s efficacy "has to be proven in each single indication with a proper randomized controlled trial," he said.
In addition to the PATENT-1 and CHEST-1 studies showing efficacy in PAH and CETPH, respectively, studies of other pulmonary hypertension disease subgroups are underway, including one involving patients with left heart systolic disorders and PAH; phase II data from that study will be presented at an upcoming meeting of the American Heart Association, he said.
The PATENT and CHEST trials are supported by Bayer, the maker of riociguat. Dr. Ghofrani disclosed that he has received grants from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and German Ministry for Education and Research; and from Bayer HealthCare, Aires, and other companies. He also has received payment for consulting and serving on speakers bureaus or advisory committees of several pharmaceutical companies.
ATLANTA – Riociguat, a novel first-in-class soluble guanylate cyclase stimulator, significantly improved 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension in the randomized, placebo-controlled phase III CHEST-1 study.
The overall 46-m improvement in 6-minute walk distance at 16 weeks in the study population was largely attributable to improvements in the 173 patients randomized to receive riociguat treatment, as opposed to improvements in 88 patients who received placebo, Dr. Hossein A. Ghofrani reported at the annual meeting of the American College of Chest Physicians.
The improvement in the treatment group was progressive and had not reached a plateau at 16 weeks after treatment initiation. Meanwhile, an initial improvement in the placebo group was followed by a constant decline in the placebo group, said Dr. Ghofrani of University Hospital Giessen and Marburg in Germany.
Treatment also was associated with consistent, significant improvements in a number of secondary end points, including change in pulmonary vascular resistance (PVR), change in World Health Organization functional class, time to clinical worsening, change in Borg dyspnea score, and quality of life assessments, he said.
Hemodynamics were robustly improved, he added, noting that treatment was associated with a 32% reduction in PVR, which translated into a highly significant 246-dyne reduction.
Patients enrolled in the multicenter CHEST-1 study – the largest placebo-controlled study to date of chronic thromboembolic pulmonary hypertension (CTEPH), for which there are currently no approved medical treatments – were aged 18-80 years with either inoperable disease or persistent or recurrent pulmonary hypertension after pulmonary endarterectomy. They had a mean PVR of greater than 480 dyn.s/cm5.
Treatment with riociguat was initiated at an oral dose of 1 mg three times daily titrated up to a maximum of 2.5 mg three times daily as tolerated according to systolic blood pressure; 90% achieved the highest dose, attesting to the tolerability of the drug, Dr. Ghofrani said.
In fact, the adverse event rate was very low, and side effects were similar to those seen in the PATENT-1 trial of riociguat for pulmonary arterial hypertension (PAH), which also was reported at the meeting.
These included headache, dizziness, peripheral edema (which occurred more often in the placebo group), cough, dyspnea, nasopharyngitis, nausea, diarrhea, and vomiting.
The findings are encouraging given the lack of medical treatments for CETPH patients who either are ineligible for surgical treatment or have persistent pulmonary hypertension after surgery, Dr. Ghofrani said.
The study of riociguat for CETPH is ongoing. CHEST-1 completers were allowed to enroll in a long-term extension study (CHEST-2), and results of that study will be reported next year, Dr. Ghofrani said.
As for how it is that a single molecule appears to have efficacy for two distinct pulmonary hypertension subgroups (PAH and CETPH), which are believed to have differing pathophysiological mechanisms, he explained that the disease might have some "common denominators."
"After a certain level of severity, they have a lot of commonalities, and the progressive component, for instance for pulmonary vascular remodeling beyond a certain point of no return, becomes very much alike in the different disease entities. The lack of the endogenous [nitric oxide] signaling pathway has been proven for many of these diseases. ... I think there may be a common denominator for the disease, even if the underlying pathophysiology may be different," he explained.
This is not to say riociguat is a "magic bullet" for all pulmonary hypertension subgroups, he added.
The drug’s efficacy "has to be proven in each single indication with a proper randomized controlled trial," he said.
In addition to the PATENT-1 and CHEST-1 studies showing efficacy in PAH and CETPH, respectively, studies of other pulmonary hypertension disease subgroups are underway, including one involving patients with left heart systolic disorders and PAH; phase II data from that study will be presented at an upcoming meeting of the American Heart Association, he said.
The PATENT and CHEST trials are supported by Bayer, the maker of riociguat. Dr. Ghofrani disclosed that he has received grants from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and German Ministry for Education and Research; and from Bayer HealthCare, Aires, and other companies. He also has received payment for consulting and serving on speakers bureaus or advisory committees of several pharmaceutical companies.
ATLANTA – Riociguat, a novel first-in-class soluble guanylate cyclase stimulator, significantly improved 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension in the randomized, placebo-controlled phase III CHEST-1 study.
The overall 46-m improvement in 6-minute walk distance at 16 weeks in the study population was largely attributable to improvements in the 173 patients randomized to receive riociguat treatment, as opposed to improvements in 88 patients who received placebo, Dr. Hossein A. Ghofrani reported at the annual meeting of the American College of Chest Physicians.
The improvement in the treatment group was progressive and had not reached a plateau at 16 weeks after treatment initiation. Meanwhile, an initial improvement in the placebo group was followed by a constant decline in the placebo group, said Dr. Ghofrani of University Hospital Giessen and Marburg in Germany.
Treatment also was associated with consistent, significant improvements in a number of secondary end points, including change in pulmonary vascular resistance (PVR), change in World Health Organization functional class, time to clinical worsening, change in Borg dyspnea score, and quality of life assessments, he said.
Hemodynamics were robustly improved, he added, noting that treatment was associated with a 32% reduction in PVR, which translated into a highly significant 246-dyne reduction.
Patients enrolled in the multicenter CHEST-1 study – the largest placebo-controlled study to date of chronic thromboembolic pulmonary hypertension (CTEPH), for which there are currently no approved medical treatments – were aged 18-80 years with either inoperable disease or persistent or recurrent pulmonary hypertension after pulmonary endarterectomy. They had a mean PVR of greater than 480 dyn.s/cm5.
Treatment with riociguat was initiated at an oral dose of 1 mg three times daily titrated up to a maximum of 2.5 mg three times daily as tolerated according to systolic blood pressure; 90% achieved the highest dose, attesting to the tolerability of the drug, Dr. Ghofrani said.
In fact, the adverse event rate was very low, and side effects were similar to those seen in the PATENT-1 trial of riociguat for pulmonary arterial hypertension (PAH), which also was reported at the meeting.
These included headache, dizziness, peripheral edema (which occurred more often in the placebo group), cough, dyspnea, nasopharyngitis, nausea, diarrhea, and vomiting.
The findings are encouraging given the lack of medical treatments for CETPH patients who either are ineligible for surgical treatment or have persistent pulmonary hypertension after surgery, Dr. Ghofrani said.
The study of riociguat for CETPH is ongoing. CHEST-1 completers were allowed to enroll in a long-term extension study (CHEST-2), and results of that study will be reported next year, Dr. Ghofrani said.
As for how it is that a single molecule appears to have efficacy for two distinct pulmonary hypertension subgroups (PAH and CETPH), which are believed to have differing pathophysiological mechanisms, he explained that the disease might have some "common denominators."
"After a certain level of severity, they have a lot of commonalities, and the progressive component, for instance for pulmonary vascular remodeling beyond a certain point of no return, becomes very much alike in the different disease entities. The lack of the endogenous [nitric oxide] signaling pathway has been proven for many of these diseases. ... I think there may be a common denominator for the disease, even if the underlying pathophysiology may be different," he explained.
This is not to say riociguat is a "magic bullet" for all pulmonary hypertension subgroups, he added.
The drug’s efficacy "has to be proven in each single indication with a proper randomized controlled trial," he said.
In addition to the PATENT-1 and CHEST-1 studies showing efficacy in PAH and CETPH, respectively, studies of other pulmonary hypertension disease subgroups are underway, including one involving patients with left heart systolic disorders and PAH; phase II data from that study will be presented at an upcoming meeting of the American Heart Association, he said.
The PATENT and CHEST trials are supported by Bayer, the maker of riociguat. Dr. Ghofrani disclosed that he has received grants from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and German Ministry for Education and Research; and from Bayer HealthCare, Aires, and other companies. He also has received payment for consulting and serving on speakers bureaus or advisory committees of several pharmaceutical companies.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: An overall 46-m improvement in 6-minute walk distance at 16 weeks in the study population was largely attributable to improvements in the 173 patients randomized to receive riociguat treatment, as opposed to fleeting improvements in 88 patients who received placebo.
Data Source: Data are from the randomized, controlled, phase III CHEST-1 trial.
Disclosures: The PATENT and CHEST trials are supported by Bayer, the maker of riociguat. Dr. Ghofrani disclosed that he has received grants from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and German Ministry for Education and Research; and from Bayer HealthCare, Aires, and other companies. He also has received payment for consulting and serving on speakers bureaus or advisory committees of several pharmaceutical companies.
Riociguat Improved Walk Distance and More in PAH Patients
ATLANTA – The investigational drug riociguat significantly improved 6-minute walk distance in patients with symptomatic pulmonary arterial hypertension in the phase III PATENT-1 trial.
Of 443 patients who participated in the randomized, double-blind trial, those who received active treatment with the novel oral soluble guanylate cyclase (sCG) stimulator experienced a 36-m improvement in 6-minute walk distance, compared with those who received placebo, after 12 weeks. This "clinically meaningful as well as highly statistically significant" improvement was evident in both treatment-naive patients and pretreated patients, who each comprised about 50% of the study population, Dr. Hossein Ghofrani reported at the annual meeting of the American College of Chest Physicians.
Treatment also resulted in "significant and robust" improvements on several secondary endpoints, including pulmonary vascular resistance, N-terminal prohormone brain natriuretic peptide, World Health Organization functional class, time to clinical worsening, and Borg dyspnea score, said Dr. Ghofrani of University Hospital Giessen and Marburg in Giessen, Germany.
For pulmonary vascular resistance, for example, a 29% reduction was noted in the treatment group, compared with the placebo group. This translated into a 226-dyne reduction, with more than a half liter increase in cardiac output and a highly statistically significant reduction of 432 ng/L in the serum biomarker, he said.
The findings suggest that riociguat – the first of the new sGC-stimulator class of drugs – represents a new treatment option for patients with PAH.
Riociguat has a dual mode of action, as it synergizes with endogenous nitric oxide and directly stimulates sGC independent of nitric oxide availability. Therefore, it may restore the NO-sGC-cGMP pathway, Dr. Ghofrani explained.
"I think it is well appreciated that, despite the major achievement over the past two decades in the field of the treatment of PAH, there is still a high mortality in this devastating progressive disease, which welcomes this representative of a new class of drug to the therapeutic armamentarium of this very special disease form," he said, noting that study of riociguat is ongoing.
Patients who participated in the multicenter, multinational PATENT-1 trial (Pulmonary Arterial Hypertension sGC-Stimulator Trial) were adults aged 18-80 years (with an average of about 50 years), including both treatment naive patients and patients pretreated with endothelin receptor antagonists or prostanoids. They were randomized to receive placebo or treatment with riociguat at a starting dose of 1 mg three times daily titrated over 8 weeks in 0.5-mg increments up to 2.5 mg three times daily.
The completion rate among participants was high, at about 93% for the treatment group and 88% for the placebo group, with 90% in the treatment group achieving the maximum dose, which reflected the tolerability of the drug, Dr. Ghofrani said.
The drug was also safe, with only 1.2% of patients experiencing an adverse event, although it is important to note that the observation period was relatively short, he added.
The 10 most frequently reported treatment-emergent adverse events occurring more often in the treatment group were headache, dyspepsia, peripheral edema, nausea, dizziness, diarrhea, nasopharyngitis, dyspnea, cough, and vomiting, he said.
When combined with phase II study data, PATENT-1 now has 5 years of follow-up, and it appears that the treatment effect is preserved for up to 12 months. Those who completed phase III had the option of continuing in an open-label phase, and results from that study are expected to be reported next year.
Additionally, riociguat was found in the phase III CHEST-1 trial to improve 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension. Thus, riociguat appears to be the first-ever drug to demonstrate robust efficacy in two distinct pulmonary hypertension groups, Dr. Ghofrani said.
The PATENT and CHEST trials are supported by Bayer, the maker of riocigualt. Dr. Ghofrani disclosed that he has received sponsored grants over the past 3 years from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and the Germany Ministry for Education and Research. He has also received industry-sponsored grants over the last 3 years from Bayer HealthCare AG, Aires, Encysive/Pfizer, and Novartis, and has received payment for consulting and serving on speaker bureaus and/or advisory committees for Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Novartis, and GlaxoSmithKline.
ATLANTA – The investigational drug riociguat significantly improved 6-minute walk distance in patients with symptomatic pulmonary arterial hypertension in the phase III PATENT-1 trial.
Of 443 patients who participated in the randomized, double-blind trial, those who received active treatment with the novel oral soluble guanylate cyclase (sCG) stimulator experienced a 36-m improvement in 6-minute walk distance, compared with those who received placebo, after 12 weeks. This "clinically meaningful as well as highly statistically significant" improvement was evident in both treatment-naive patients and pretreated patients, who each comprised about 50% of the study population, Dr. Hossein Ghofrani reported at the annual meeting of the American College of Chest Physicians.
Treatment also resulted in "significant and robust" improvements on several secondary endpoints, including pulmonary vascular resistance, N-terminal prohormone brain natriuretic peptide, World Health Organization functional class, time to clinical worsening, and Borg dyspnea score, said Dr. Ghofrani of University Hospital Giessen and Marburg in Giessen, Germany.
For pulmonary vascular resistance, for example, a 29% reduction was noted in the treatment group, compared with the placebo group. This translated into a 226-dyne reduction, with more than a half liter increase in cardiac output and a highly statistically significant reduction of 432 ng/L in the serum biomarker, he said.
The findings suggest that riociguat – the first of the new sGC-stimulator class of drugs – represents a new treatment option for patients with PAH.
Riociguat has a dual mode of action, as it synergizes with endogenous nitric oxide and directly stimulates sGC independent of nitric oxide availability. Therefore, it may restore the NO-sGC-cGMP pathway, Dr. Ghofrani explained.
"I think it is well appreciated that, despite the major achievement over the past two decades in the field of the treatment of PAH, there is still a high mortality in this devastating progressive disease, which welcomes this representative of a new class of drug to the therapeutic armamentarium of this very special disease form," he said, noting that study of riociguat is ongoing.
Patients who participated in the multicenter, multinational PATENT-1 trial (Pulmonary Arterial Hypertension sGC-Stimulator Trial) were adults aged 18-80 years (with an average of about 50 years), including both treatment naive patients and patients pretreated with endothelin receptor antagonists or prostanoids. They were randomized to receive placebo or treatment with riociguat at a starting dose of 1 mg three times daily titrated over 8 weeks in 0.5-mg increments up to 2.5 mg three times daily.
The completion rate among participants was high, at about 93% for the treatment group and 88% for the placebo group, with 90% in the treatment group achieving the maximum dose, which reflected the tolerability of the drug, Dr. Ghofrani said.
The drug was also safe, with only 1.2% of patients experiencing an adverse event, although it is important to note that the observation period was relatively short, he added.
The 10 most frequently reported treatment-emergent adverse events occurring more often in the treatment group were headache, dyspepsia, peripheral edema, nausea, dizziness, diarrhea, nasopharyngitis, dyspnea, cough, and vomiting, he said.
When combined with phase II study data, PATENT-1 now has 5 years of follow-up, and it appears that the treatment effect is preserved for up to 12 months. Those who completed phase III had the option of continuing in an open-label phase, and results from that study are expected to be reported next year.
Additionally, riociguat was found in the phase III CHEST-1 trial to improve 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension. Thus, riociguat appears to be the first-ever drug to demonstrate robust efficacy in two distinct pulmonary hypertension groups, Dr. Ghofrani said.
The PATENT and CHEST trials are supported by Bayer, the maker of riocigualt. Dr. Ghofrani disclosed that he has received sponsored grants over the past 3 years from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and the Germany Ministry for Education and Research. He has also received industry-sponsored grants over the last 3 years from Bayer HealthCare AG, Aires, Encysive/Pfizer, and Novartis, and has received payment for consulting and serving on speaker bureaus and/or advisory committees for Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Novartis, and GlaxoSmithKline.
ATLANTA – The investigational drug riociguat significantly improved 6-minute walk distance in patients with symptomatic pulmonary arterial hypertension in the phase III PATENT-1 trial.
Of 443 patients who participated in the randomized, double-blind trial, those who received active treatment with the novel oral soluble guanylate cyclase (sCG) stimulator experienced a 36-m improvement in 6-minute walk distance, compared with those who received placebo, after 12 weeks. This "clinically meaningful as well as highly statistically significant" improvement was evident in both treatment-naive patients and pretreated patients, who each comprised about 50% of the study population, Dr. Hossein Ghofrani reported at the annual meeting of the American College of Chest Physicians.
Treatment also resulted in "significant and robust" improvements on several secondary endpoints, including pulmonary vascular resistance, N-terminal prohormone brain natriuretic peptide, World Health Organization functional class, time to clinical worsening, and Borg dyspnea score, said Dr. Ghofrani of University Hospital Giessen and Marburg in Giessen, Germany.
For pulmonary vascular resistance, for example, a 29% reduction was noted in the treatment group, compared with the placebo group. This translated into a 226-dyne reduction, with more than a half liter increase in cardiac output and a highly statistically significant reduction of 432 ng/L in the serum biomarker, he said.
The findings suggest that riociguat – the first of the new sGC-stimulator class of drugs – represents a new treatment option for patients with PAH.
Riociguat has a dual mode of action, as it synergizes with endogenous nitric oxide and directly stimulates sGC independent of nitric oxide availability. Therefore, it may restore the NO-sGC-cGMP pathway, Dr. Ghofrani explained.
"I think it is well appreciated that, despite the major achievement over the past two decades in the field of the treatment of PAH, there is still a high mortality in this devastating progressive disease, which welcomes this representative of a new class of drug to the therapeutic armamentarium of this very special disease form," he said, noting that study of riociguat is ongoing.
Patients who participated in the multicenter, multinational PATENT-1 trial (Pulmonary Arterial Hypertension sGC-Stimulator Trial) were adults aged 18-80 years (with an average of about 50 years), including both treatment naive patients and patients pretreated with endothelin receptor antagonists or prostanoids. They were randomized to receive placebo or treatment with riociguat at a starting dose of 1 mg three times daily titrated over 8 weeks in 0.5-mg increments up to 2.5 mg three times daily.
The completion rate among participants was high, at about 93% for the treatment group and 88% for the placebo group, with 90% in the treatment group achieving the maximum dose, which reflected the tolerability of the drug, Dr. Ghofrani said.
The drug was also safe, with only 1.2% of patients experiencing an adverse event, although it is important to note that the observation period was relatively short, he added.
The 10 most frequently reported treatment-emergent adverse events occurring more often in the treatment group were headache, dyspepsia, peripheral edema, nausea, dizziness, diarrhea, nasopharyngitis, dyspnea, cough, and vomiting, he said.
When combined with phase II study data, PATENT-1 now has 5 years of follow-up, and it appears that the treatment effect is preserved for up to 12 months. Those who completed phase III had the option of continuing in an open-label phase, and results from that study are expected to be reported next year.
Additionally, riociguat was found in the phase III CHEST-1 trial to improve 6-minute walk distance in patients with inoperable chronic thromboembolic pulmonary hypertension. Thus, riociguat appears to be the first-ever drug to demonstrate robust efficacy in two distinct pulmonary hypertension groups, Dr. Ghofrani said.
The PATENT and CHEST trials are supported by Bayer, the maker of riocigualt. Dr. Ghofrani disclosed that he has received sponsored grants over the past 3 years from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and the Germany Ministry for Education and Research. He has also received industry-sponsored grants over the last 3 years from Bayer HealthCare AG, Aires, Encysive/Pfizer, and Novartis, and has received payment for consulting and serving on speaker bureaus and/or advisory committees for Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Novartis, and GlaxoSmithKline.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Pulmonary arterial hypertension patients who received active treatment with the novel oral soluble guanylate cyclase (sCG) stimulator experienced a 36-m improvement in 6-minute walk distance, compared with those who received placebo, after 12 weeks.
Data Source: The randomized, controlled, double-blind PATENT-1 trial involved 443 patients.
Disclosures: The PATENT and CHEST trials are supported by Bayer, the maker of riociguat. Dr. Ghofrani disclosed that he has received sponsored grants over the past 3 years from the German Research Foundation, Excellence Cluster Cardiopulmonary Research, and the Germany Ministry for Education and Research. He has also received industry-sponsored grants over the last 3 years from Bayer HealthCare AG, Aires, Encysive/Pfizer, and Novartis, and has received payment for consulting and serving on speaker bureaus and/or advisory committees for Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Novartis, and GlaxoSmithKline.
Perceived Dyspnea Affects COPD Quality of Life Outcomes
ATLANTA – The perception of dyspnea among patients with chronic obstructive pulmonary disorder plays a bigger role in quality of life, functional status, and depression than do objective measures of disease severity, according to findings from cross-sectional study involving 158 patients.
The findings suggest that assessing and addressing dyspnea in COPD patients could play an important role in improving quality of life outcomes, Dr. Sandra Adams reported at the annual meeting of the American College of Chest Physicians.
The patients included in this analysis are part of the CASCADE study, a 2-year longitudinal observational study of genes and depression in COPD. They completed spirometry, the modified Medical Research Council (mMRC) dyspnea scale, questions related to exacerbation risk within the last year, the Chronic Respiratory Questionnaire (CRQ), a nine-item depression interview, the Personal Health Questionnaire (PHQ-9), and a 6-minute walk test at baseline.
Study participants had a mean age of about 67 years, about 25% were women, 40% were on supplemental oxygen, and the mean forced expiratory volume in 1 second (FEV1) percent predicted was 43%. Exacerbations were self-reported.
More than 60% had a self-reported physician diagnosis of depression.
About 20% of the patients were found to be grade A patients, based on the revised Global Initiative for Chronic Obstructive Lung Disease (GOLD) released in December 2011, about 10% were grade B patients, about 20% were grade C patients, and about 50% were grade D patients, said Dr. Adams of the University of Texas Health Science Center, San Antonio.
Patients with grade A disease have mild disease severity, airflow limitation, and few exacerbations; those with grade B disease are similar to those with grade A, except they have more symptoms (in this study, the grade B patients had no exacerbations). Those with grade C disease have minimal symptoms, severe airflow limitation, and/or two or more exacerbations each year; those with grade D disease are similar to those with grade C disease, except they have more symptoms.
"One thing we were actually really surprised to find is that the group of A and C with minimal symptoms may be a lot more similar than we think, whereas D and B with the severe symptoms – even though they have significant differences in exacerbations and/or airflow limitation, may be very similar," she said.
Indeed, no differences on the various measures used in this study were seen between the A and C patients, and between the B and D patients. But when the A and C patients were combined and compared with the combined group of B and D patients, significant differences emerged for every measure.
"Again, the big difference is symptoms; A and C have minimal symptoms and B and D have severe symptoms," Dr. Adams said.
As it turned out, grades A and C patients had significantly higher CRQ scores (higher scores are better) than did grades B and D patients (mean of 105 and 98 for A and C vs. 80 and 84 for B and D, respectively). Grades A and C also had statistically and clinically significantly greater 6-minute walk test distances, Dr. Adams noted.
On a physical function measure of steps walked in a day, the A and C patients averaged 7,900, and the B and D patients averaged only 4,800, she added.
That’s 3,900 fewer steps despite inclusion of B-group patient (10% of the total study population) in the B/D combined group, Dr. Adams noted.
"Again ... grade B had relatively normal lung function and no exacerbations, but yet they’re severely dyspneic," she noted.
As for depression, the history was similar across all grades, although more grade B and D patients than A and C patients had PHQ-9 scores of 10 or greater, which indicates significant depression. On linear regression, an mMRC dyspnea scale score of 2 or higher was associated with a significant increase in depression (odds ratio, 2.8).
"So the bottom line to this is grades A and C have similar levels of depression, quality of life, physical function, and physical activity despite significant differences in FEV1 percent predicted and and/or the number of exacerbations," she said, explaining that it appears that the perception of dyspnea is the main factor associated with these outcomes.
"And, in fact, those who report severe dyspnea may be even more limited than those with frequent exacerbations," she said.
What are the clinical implications of the findings?
"We ask our patients, ‘How are you doing? How is your shortness of breath?’ but actually getting an assessment and also trying to really address the dyspnea in addition to the exacerbations is going to be really key in this population," Dr. Adams concluded.
Dr. Adams disclosed that she has received grant money for research from the Chest Foundation, the NIH, the Veterans Affairs Cooperative Studies Program, Bayer, Boehringer Ingelheim, Centocor, GlaxoSmithKline, Novartis, Pfizer, and Schering-Plough. She also has received honoraria for speaking from ABCam, Altana, AstraZeneca, Aventis, Bayer, Boehringer Ingelheim, GSK, Novartis, AG, Mycomed, Pfizer, and Schering-Plough.
ATLANTA – The perception of dyspnea among patients with chronic obstructive pulmonary disorder plays a bigger role in quality of life, functional status, and depression than do objective measures of disease severity, according to findings from cross-sectional study involving 158 patients.
The findings suggest that assessing and addressing dyspnea in COPD patients could play an important role in improving quality of life outcomes, Dr. Sandra Adams reported at the annual meeting of the American College of Chest Physicians.
The patients included in this analysis are part of the CASCADE study, a 2-year longitudinal observational study of genes and depression in COPD. They completed spirometry, the modified Medical Research Council (mMRC) dyspnea scale, questions related to exacerbation risk within the last year, the Chronic Respiratory Questionnaire (CRQ), a nine-item depression interview, the Personal Health Questionnaire (PHQ-9), and a 6-minute walk test at baseline.
Study participants had a mean age of about 67 years, about 25% were women, 40% were on supplemental oxygen, and the mean forced expiratory volume in 1 second (FEV1) percent predicted was 43%. Exacerbations were self-reported.
More than 60% had a self-reported physician diagnosis of depression.
About 20% of the patients were found to be grade A patients, based on the revised Global Initiative for Chronic Obstructive Lung Disease (GOLD) released in December 2011, about 10% were grade B patients, about 20% were grade C patients, and about 50% were grade D patients, said Dr. Adams of the University of Texas Health Science Center, San Antonio.
Patients with grade A disease have mild disease severity, airflow limitation, and few exacerbations; those with grade B disease are similar to those with grade A, except they have more symptoms (in this study, the grade B patients had no exacerbations). Those with grade C disease have minimal symptoms, severe airflow limitation, and/or two or more exacerbations each year; those with grade D disease are similar to those with grade C disease, except they have more symptoms.
"One thing we were actually really surprised to find is that the group of A and C with minimal symptoms may be a lot more similar than we think, whereas D and B with the severe symptoms – even though they have significant differences in exacerbations and/or airflow limitation, may be very similar," she said.
Indeed, no differences on the various measures used in this study were seen between the A and C patients, and between the B and D patients. But when the A and C patients were combined and compared with the combined group of B and D patients, significant differences emerged for every measure.
"Again, the big difference is symptoms; A and C have minimal symptoms and B and D have severe symptoms," Dr. Adams said.
As it turned out, grades A and C patients had significantly higher CRQ scores (higher scores are better) than did grades B and D patients (mean of 105 and 98 for A and C vs. 80 and 84 for B and D, respectively). Grades A and C also had statistically and clinically significantly greater 6-minute walk test distances, Dr. Adams noted.
On a physical function measure of steps walked in a day, the A and C patients averaged 7,900, and the B and D patients averaged only 4,800, she added.
That’s 3,900 fewer steps despite inclusion of B-group patient (10% of the total study population) in the B/D combined group, Dr. Adams noted.
"Again ... grade B had relatively normal lung function and no exacerbations, but yet they’re severely dyspneic," she noted.
As for depression, the history was similar across all grades, although more grade B and D patients than A and C patients had PHQ-9 scores of 10 or greater, which indicates significant depression. On linear regression, an mMRC dyspnea scale score of 2 or higher was associated with a significant increase in depression (odds ratio, 2.8).
"So the bottom line to this is grades A and C have similar levels of depression, quality of life, physical function, and physical activity despite significant differences in FEV1 percent predicted and and/or the number of exacerbations," she said, explaining that it appears that the perception of dyspnea is the main factor associated with these outcomes.
"And, in fact, those who report severe dyspnea may be even more limited than those with frequent exacerbations," she said.
What are the clinical implications of the findings?
"We ask our patients, ‘How are you doing? How is your shortness of breath?’ but actually getting an assessment and also trying to really address the dyspnea in addition to the exacerbations is going to be really key in this population," Dr. Adams concluded.
Dr. Adams disclosed that she has received grant money for research from the Chest Foundation, the NIH, the Veterans Affairs Cooperative Studies Program, Bayer, Boehringer Ingelheim, Centocor, GlaxoSmithKline, Novartis, Pfizer, and Schering-Plough. She also has received honoraria for speaking from ABCam, Altana, AstraZeneca, Aventis, Bayer, Boehringer Ingelheim, GSK, Novartis, AG, Mycomed, Pfizer, and Schering-Plough.
ATLANTA – The perception of dyspnea among patients with chronic obstructive pulmonary disorder plays a bigger role in quality of life, functional status, and depression than do objective measures of disease severity, according to findings from cross-sectional study involving 158 patients.
The findings suggest that assessing and addressing dyspnea in COPD patients could play an important role in improving quality of life outcomes, Dr. Sandra Adams reported at the annual meeting of the American College of Chest Physicians.
The patients included in this analysis are part of the CASCADE study, a 2-year longitudinal observational study of genes and depression in COPD. They completed spirometry, the modified Medical Research Council (mMRC) dyspnea scale, questions related to exacerbation risk within the last year, the Chronic Respiratory Questionnaire (CRQ), a nine-item depression interview, the Personal Health Questionnaire (PHQ-9), and a 6-minute walk test at baseline.
Study participants had a mean age of about 67 years, about 25% were women, 40% were on supplemental oxygen, and the mean forced expiratory volume in 1 second (FEV1) percent predicted was 43%. Exacerbations were self-reported.
More than 60% had a self-reported physician diagnosis of depression.
About 20% of the patients were found to be grade A patients, based on the revised Global Initiative for Chronic Obstructive Lung Disease (GOLD) released in December 2011, about 10% were grade B patients, about 20% were grade C patients, and about 50% were grade D patients, said Dr. Adams of the University of Texas Health Science Center, San Antonio.
Patients with grade A disease have mild disease severity, airflow limitation, and few exacerbations; those with grade B disease are similar to those with grade A, except they have more symptoms (in this study, the grade B patients had no exacerbations). Those with grade C disease have minimal symptoms, severe airflow limitation, and/or two or more exacerbations each year; those with grade D disease are similar to those with grade C disease, except they have more symptoms.
"One thing we were actually really surprised to find is that the group of A and C with minimal symptoms may be a lot more similar than we think, whereas D and B with the severe symptoms – even though they have significant differences in exacerbations and/or airflow limitation, may be very similar," she said.
Indeed, no differences on the various measures used in this study were seen between the A and C patients, and between the B and D patients. But when the A and C patients were combined and compared with the combined group of B and D patients, significant differences emerged for every measure.
"Again, the big difference is symptoms; A and C have minimal symptoms and B and D have severe symptoms," Dr. Adams said.
As it turned out, grades A and C patients had significantly higher CRQ scores (higher scores are better) than did grades B and D patients (mean of 105 and 98 for A and C vs. 80 and 84 for B and D, respectively). Grades A and C also had statistically and clinically significantly greater 6-minute walk test distances, Dr. Adams noted.
On a physical function measure of steps walked in a day, the A and C patients averaged 7,900, and the B and D patients averaged only 4,800, she added.
That’s 3,900 fewer steps despite inclusion of B-group patient (10% of the total study population) in the B/D combined group, Dr. Adams noted.
"Again ... grade B had relatively normal lung function and no exacerbations, but yet they’re severely dyspneic," she noted.
As for depression, the history was similar across all grades, although more grade B and D patients than A and C patients had PHQ-9 scores of 10 or greater, which indicates significant depression. On linear regression, an mMRC dyspnea scale score of 2 or higher was associated with a significant increase in depression (odds ratio, 2.8).
"So the bottom line to this is grades A and C have similar levels of depression, quality of life, physical function, and physical activity despite significant differences in FEV1 percent predicted and and/or the number of exacerbations," she said, explaining that it appears that the perception of dyspnea is the main factor associated with these outcomes.
"And, in fact, those who report severe dyspnea may be even more limited than those with frequent exacerbations," she said.
What are the clinical implications of the findings?
"We ask our patients, ‘How are you doing? How is your shortness of breath?’ but actually getting an assessment and also trying to really address the dyspnea in addition to the exacerbations is going to be really key in this population," Dr. Adams concluded.
Dr. Adams disclosed that she has received grant money for research from the Chest Foundation, the NIH, the Veterans Affairs Cooperative Studies Program, Bayer, Boehringer Ingelheim, Centocor, GlaxoSmithKline, Novartis, Pfizer, and Schering-Plough. She also has received honoraria for speaking from ABCam, Altana, AstraZeneca, Aventis, Bayer, Boehringer Ingelheim, GSK, Novartis, AG, Mycomed, Pfizer, and Schering-Plough.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Patients with more perceived dyspnea had poorer outcomes on measures of quality of life, functional status, and depression.
Data Source: Results were taken from a cross-sectional study of 158 patients from the CASCADE trial.
Disclosures: Dr. Adams disclosed that she has received grant money for research from the Chest Foundation, the NIH, the VA Cooperative Studies Program, Bayer, Boehringer Ingelheim, Centocor, GlaxoSmithKline, Novartis, Pfizer, and Schering-Plough. She also has received honoraria for speaking from ABCam, Altana, AstraZeneca, Aventis, Bayer, Boehringer Ingelheim, GSK, Novartis Pharmaceuticals, AG, Mycomed, Pfizer, and Schering-Plough.
Shades of SARS? New Virus Took Root in Pneumonia Patient
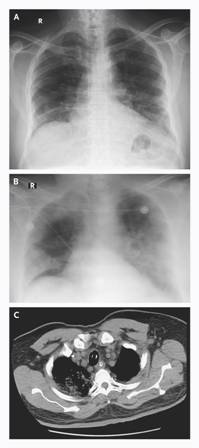
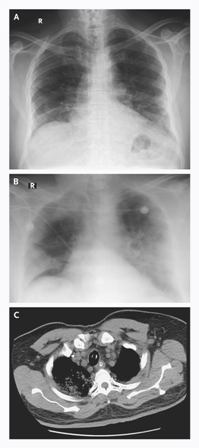
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
FDA Approves Abraxane for Non-Small Cell Lung Cancer
The Food and Drug Administration has approved the albumin-bound formulation of paclitaxel for injectible suspension as first-line treatment of locally advanced or metastatic non–small cell lung cancer, the agency announced on Oct. 12.
Marketed as Abraxane, nanoparticle albumin-bound (nab)-paclitaxel was developed as an alternative to Taxol, which delivers paclitaxel in a highly toxic cremophor solvent. The FDA said it based the new approval on the previous approval of Taxol for this indication and a supportive study.
Abraxis Bioscience, a subsidiary of Celgene Corp., markets Abraxane. Nab-paclitaxel was initially approved in 2005 as a treatment for breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy.
The new indication is for use in combination with carboplatin for the initial treatment of patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) who are not candidates for curative surgery or radiation therapy. The recommended dose and schedule is 100 mg/m2 administered as an intravenous infusion over 30 minutes on days 1, 8, and 15 of each 21-day cycle. The recommended dose of carboplatin is AUC = 6 mg/min per mL on day 1 of each 21-day cycle after the Abraxane infusion is completed.
Approval was based on the previous approval of Taxol injection for the same indication, plus a randomized open-label, multinational study "establishing that Abraxane was as at least as active (as determined by overall response rate) as paclitaxel when both agents are used in combination with carboplatin," the FDA said.
In the study – the CA-031 trial – 521 patients with locally advanced or metastatic NSCLC were treated with Abraxane (at a dose of 100 mg/m2 as a weekly infusion) and 531 were treated with paclitaxel injection (at a dose of 200 mg/m2 as an IV infusion 3 three weeks). All patients received the same dose and schedule of carboplatin every 3 weeks.
Premedication with corticosteroids and an antihistamine was used in all patients receiving paclitaxel, but use was discretionary in the Abraxane arm.
The primary end point of the study, the overall response rate (the proportion of patients who achieved a durable complete or partial response, as determined by blinded radiological reviewers), was 33% among those in the Abraxane arm, compared with 25% of those in the paclitaxel arm, a statistically significant difference.
Among the responders in both groups, the durability of the responses was statistically similar, with median response duration reaching 6.9 months among those on Abraxane and 6.0 months among those on paclitaxel. There was no significant difference in overall survival between the two groups.
Celgene noted in a written statement that Abraxane demonstrated a higher overall response rate for squamous cell carcinoma (41% vs. 24%) and large cell carcinoma (33% vs. 15%) but was similar in patients with carcinoma/adenocarcinoma (26% vs. 27%).
The rate of serious adverse reactions was 18% in both groups: anemia (4%) and thrombocytopenia (3%) were the most common serious adverse reactions reported among those on Abraxane, according to the FDA. The safety evaluation was based on 1,038 patients who received at least one dose of their planned treatments.
The Abraxane label carries a neutropenia warning that it should not be administered in patients with baseline neutrophil counts of less than 1,500 cells/mm3, and that frequent peripheral blood cell counts should be performed to monitor occurrence of bone marrow suppression. The agency also warns that Abraxane should not be substituted "for or with other paclitaxel formulations."
Abraxane is currently being studied for the treatment of pancreatic, metastatic melanoma, bladder, and ovarian cancers, and for expanded applications for breast cancer, according to Celgene.
The Food and Drug Administration has approved the albumin-bound formulation of paclitaxel for injectible suspension as first-line treatment of locally advanced or metastatic non–small cell lung cancer, the agency announced on Oct. 12.
Marketed as Abraxane, nanoparticle albumin-bound (nab)-paclitaxel was developed as an alternative to Taxol, which delivers paclitaxel in a highly toxic cremophor solvent. The FDA said it based the new approval on the previous approval of Taxol for this indication and a supportive study.
Abraxis Bioscience, a subsidiary of Celgene Corp., markets Abraxane. Nab-paclitaxel was initially approved in 2005 as a treatment for breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy.
The new indication is for use in combination with carboplatin for the initial treatment of patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) who are not candidates for curative surgery or radiation therapy. The recommended dose and schedule is 100 mg/m2 administered as an intravenous infusion over 30 minutes on days 1, 8, and 15 of each 21-day cycle. The recommended dose of carboplatin is AUC = 6 mg/min per mL on day 1 of each 21-day cycle after the Abraxane infusion is completed.
Approval was based on the previous approval of Taxol injection for the same indication, plus a randomized open-label, multinational study "establishing that Abraxane was as at least as active (as determined by overall response rate) as paclitaxel when both agents are used in combination with carboplatin," the FDA said.
In the study – the CA-031 trial – 521 patients with locally advanced or metastatic NSCLC were treated with Abraxane (at a dose of 100 mg/m2 as a weekly infusion) and 531 were treated with paclitaxel injection (at a dose of 200 mg/m2 as an IV infusion 3 three weeks). All patients received the same dose and schedule of carboplatin every 3 weeks.
Premedication with corticosteroids and an antihistamine was used in all patients receiving paclitaxel, but use was discretionary in the Abraxane arm.
The primary end point of the study, the overall response rate (the proportion of patients who achieved a durable complete or partial response, as determined by blinded radiological reviewers), was 33% among those in the Abraxane arm, compared with 25% of those in the paclitaxel arm, a statistically significant difference.
Among the responders in both groups, the durability of the responses was statistically similar, with median response duration reaching 6.9 months among those on Abraxane and 6.0 months among those on paclitaxel. There was no significant difference in overall survival between the two groups.
Celgene noted in a written statement that Abraxane demonstrated a higher overall response rate for squamous cell carcinoma (41% vs. 24%) and large cell carcinoma (33% vs. 15%) but was similar in patients with carcinoma/adenocarcinoma (26% vs. 27%).
The rate of serious adverse reactions was 18% in both groups: anemia (4%) and thrombocytopenia (3%) were the most common serious adverse reactions reported among those on Abraxane, according to the FDA. The safety evaluation was based on 1,038 patients who received at least one dose of their planned treatments.
The Abraxane label carries a neutropenia warning that it should not be administered in patients with baseline neutrophil counts of less than 1,500 cells/mm3, and that frequent peripheral blood cell counts should be performed to monitor occurrence of bone marrow suppression. The agency also warns that Abraxane should not be substituted "for or with other paclitaxel formulations."
Abraxane is currently being studied for the treatment of pancreatic, metastatic melanoma, bladder, and ovarian cancers, and for expanded applications for breast cancer, according to Celgene.
The Food and Drug Administration has approved the albumin-bound formulation of paclitaxel for injectible suspension as first-line treatment of locally advanced or metastatic non–small cell lung cancer, the agency announced on Oct. 12.
Marketed as Abraxane, nanoparticle albumin-bound (nab)-paclitaxel was developed as an alternative to Taxol, which delivers paclitaxel in a highly toxic cremophor solvent. The FDA said it based the new approval on the previous approval of Taxol for this indication and a supportive study.
Abraxis Bioscience, a subsidiary of Celgene Corp., markets Abraxane. Nab-paclitaxel was initially approved in 2005 as a treatment for breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy.
The new indication is for use in combination with carboplatin for the initial treatment of patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) who are not candidates for curative surgery or radiation therapy. The recommended dose and schedule is 100 mg/m2 administered as an intravenous infusion over 30 minutes on days 1, 8, and 15 of each 21-day cycle. The recommended dose of carboplatin is AUC = 6 mg/min per mL on day 1 of each 21-day cycle after the Abraxane infusion is completed.
Approval was based on the previous approval of Taxol injection for the same indication, plus a randomized open-label, multinational study "establishing that Abraxane was as at least as active (as determined by overall response rate) as paclitaxel when both agents are used in combination with carboplatin," the FDA said.
In the study – the CA-031 trial – 521 patients with locally advanced or metastatic NSCLC were treated with Abraxane (at a dose of 100 mg/m2 as a weekly infusion) and 531 were treated with paclitaxel injection (at a dose of 200 mg/m2 as an IV infusion 3 three weeks). All patients received the same dose and schedule of carboplatin every 3 weeks.
Premedication with corticosteroids and an antihistamine was used in all patients receiving paclitaxel, but use was discretionary in the Abraxane arm.
The primary end point of the study, the overall response rate (the proportion of patients who achieved a durable complete or partial response, as determined by blinded radiological reviewers), was 33% among those in the Abraxane arm, compared with 25% of those in the paclitaxel arm, a statistically significant difference.
Among the responders in both groups, the durability of the responses was statistically similar, with median response duration reaching 6.9 months among those on Abraxane and 6.0 months among those on paclitaxel. There was no significant difference in overall survival between the two groups.
Celgene noted in a written statement that Abraxane demonstrated a higher overall response rate for squamous cell carcinoma (41% vs. 24%) and large cell carcinoma (33% vs. 15%) but was similar in patients with carcinoma/adenocarcinoma (26% vs. 27%).
The rate of serious adverse reactions was 18% in both groups: anemia (4%) and thrombocytopenia (3%) were the most common serious adverse reactions reported among those on Abraxane, according to the FDA. The safety evaluation was based on 1,038 patients who received at least one dose of their planned treatments.
The Abraxane label carries a neutropenia warning that it should not be administered in patients with baseline neutrophil counts of less than 1,500 cells/mm3, and that frequent peripheral blood cell counts should be performed to monitor occurrence of bone marrow suppression. The agency also warns that Abraxane should not be substituted "for or with other paclitaxel formulations."
Abraxane is currently being studied for the treatment of pancreatic, metastatic melanoma, bladder, and ovarian cancers, and for expanded applications for breast cancer, according to Celgene.
CDC Issues First Report for 2012-2013 Flu Season
The Centers for Disease Control and Prevention has released the influenza season's first activity report. The FluView report, which notes that influenza activity has been low thus far, now includes web-based interactive applications that will allow for customized, visual interpretations and comparisons of data. It can be viewed weekly on the CDC's website.
The Centers for Disease Control and Prevention has released the influenza season's first activity report. The FluView report, which notes that influenza activity has been low thus far, now includes web-based interactive applications that will allow for customized, visual interpretations and comparisons of data. It can be viewed weekly on the CDC's website.
The Centers for Disease Control and Prevention has released the influenza season's first activity report. The FluView report, which notes that influenza activity has been low thus far, now includes web-based interactive applications that will allow for customized, visual interpretations and comparisons of data. It can be viewed weekly on the CDC's website.
Adenotonsillectomy Dries Up Some Bed-Wetting
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY - HEAD AND NECK SURGERY FOUNDATION
Major Finding: Adenotonsillectomy reduced bed-wetting and obstructive sleep apnea in 51% of children with both conditions.
Data Source: The data come from a prospective study of 35 children with nighttime enuresis and obstructive sleep apnea.
Disclosures: Dr. Thottam had no financial conflicts to disclose.
Epic Progress Seen in Reducing Pneumococcal Infections
VAIL, COLO. - American medicine emphatically surpassed the Healthy People 2010 goal for reduction of invasive Streptococcus pneumoniae infections well ahead of schedule in both of the highest-risk target groups: children under age 5 years and seniors. And the tougher Healthy People 2020 objectives are already well within striking distance.
"We get an A+ on this," Dr. Mary P. Glodé commented at the annual pediatric infectious diseases conference sponsored by Children’s Hospital Colorado.

The Healthy People 2010 objective was to reduce the incidence of invasive S. pneumoniae infections to 46 cases per 100,000 among children under age 5 years and to 42 per 100,000 persons age 65 or older. The actual 2010 rates were 19 and 36 per 100,000, respectively.
Between 1999 and 2010, the annual rate of invasive pneumococcal disease in children younger age 5 plummeted by 86% as a consequence of the licensure in 2000 of the pneumococcal conjugate vaccine 7 (PCV 7) vaccine.
Most impressively, the rate also fell by 50% during that period among seniors, even though they didn’t receive the vaccine. This is ascribed to herd immunity. The presumed mechanism is that once immunized, young children were far less likely to become colonized by virulent pneumococcal serotypes, with resultant diminished opportunity for transmission of the pathogens to older children and adults, explained Dr. Glodé, professor of pediatrics and head of the section of pediatric infectious disease at the University of Colorado, Denver, and Children’s Hospital Colorado.
The Healthy People 2020 goal is to further reduce the incidence of invasive pneumococcal infections in children under age 5 from the 2010 rate of 19 down to 12 per 100,000, and in seniors from the 2010 figure of 36 per 100,000 to 31 per 100,000.
The expectation is that the target in children will be handily reached, and early on, as a consequence of the spring 2010 recommendation by the American Academy of Pediatrics and the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) that all children aged 2-59 months be routinely vaccinated with the PCV 13 vaccine, which contains the PCV 7 serotypes plus six others causing invasive disease. Early unpublished CDC data suggest there has already been some decline in disease in children as a result of the added serotypes included in PCV 13, especially in cases involving serotypes 19A and 7F, according to Dr. Glodé.
The difficult unanswered question concerns the best way to get the nation’s seniors to the Healthy People 2020 target. The rate of invasive pneumococcal disease is higher in persons aged 65 and older than in any other age group, as is the associated mortality. Indeed, of an estimated 44,000 cases of invasive pneumococcal disease in the United States during 2009, 37,000 were in adults, including 15,000 cases in individuals age 65 or more.
Late last year the Food and Drug Administration licensed the PCV 13 vaccine for use in people aged 50 and up. But that doesn’t necessarily mean it will see widespread use. There has been no official recommendation from the ACIP that the vaccine be routinely used in this population. The expert panel has noted that to date there are no data showing that the PCV 13 vaccine is effective in preventing pneumococcal pneumonia in adults, although a Dutch trial in 85,000 people over age 65 is underway.
The committee also noted that one-quarter of all cases of invasive pneumococcal disease in seniors are caused by 11 serotypes in the PPSV 23 vaccine that are not included in the PCV 13 vaccine, which further complicates the situation. The PPSV 23 vaccine has been approved since 1983 and is recommended for use in all adults over age 65 and in younger adults with certain underlying medical conditions, including diabetes and chronic lung disease.
Also, if the serotypes contained in the PCV 13 vaccine are going to largely go away in the senior population as a consequence of universal pediatric immunization, which could happen based upon the earlier herd immunity experience noted with the PCV 7 vaccine, then it may not be reasonable to give PCV 13 to all older adults, Dr. Glodé noted.
She reported serving on the data safety monitoring board for trials of an unrelated Pfizer vaccine.
VAIL, COLO. - American medicine emphatically surpassed the Healthy People 2010 goal for reduction of invasive Streptococcus pneumoniae infections well ahead of schedule in both of the highest-risk target groups: children under age 5 years and seniors. And the tougher Healthy People 2020 objectives are already well within striking distance.
"We get an A+ on this," Dr. Mary P. Glodé commented at the annual pediatric infectious diseases conference sponsored by Children’s Hospital Colorado.
The Healthy People 2010 objective was to reduce the incidence of invasive S. pneumoniae infections to 46 cases per 100,000 among children under age 5 years and to 42 per 100,000 persons age 65 or older. The actual 2010 rates were 19 and 36 per 100,000, respectively.
Between 1999 and 2010, the annual rate of invasive pneumococcal disease in children younger age 5 plummeted by 86% as a consequence of the licensure in 2000 of the pneumococcal conjugate vaccine 7 (PCV 7) vaccine.
Most impressively, the rate also fell by 50% during that period among seniors, even though they didn’t receive the vaccine. This is ascribed to herd immunity. The presumed mechanism is that once immunized, young children were far less likely to become colonized by virulent pneumococcal serotypes, with resultant diminished opportunity for transmission of the pathogens to older children and adults, explained Dr. Glodé, professor of pediatrics and head of the section of pediatric infectious disease at the University of Colorado, Denver, and Children’s Hospital Colorado.
The Healthy People 2020 goal is to further reduce the incidence of invasive pneumococcal infections in children under age 5 from the 2010 rate of 19 down to 12 per 100,000, and in seniors from the 2010 figure of 36 per 100,000 to 31 per 100,000.
The expectation is that the target in children will be handily reached, and early on, as a consequence of the spring 2010 recommendation by the American Academy of Pediatrics and the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) that all children aged 2-59 months be routinely vaccinated with the PCV 13 vaccine, which contains the PCV 7 serotypes plus six others causing invasive disease. Early unpublished CDC data suggest there has already been some decline in disease in children as a result of the added serotypes included in PCV 13, especially in cases involving serotypes 19A and 7F, according to Dr. Glodé.
The difficult unanswered question concerns the best way to get the nation’s seniors to the Healthy People 2020 target. The rate of invasive pneumococcal disease is higher in persons aged 65 and older than in any other age group, as is the associated mortality. Indeed, of an estimated 44,000 cases of invasive pneumococcal disease in the United States during 2009, 37,000 were in adults, including 15,000 cases in individuals age 65 or more.
Late last year the Food and Drug Administration licensed the PCV 13 vaccine for use in people aged 50 and up. But that doesn’t necessarily mean it will see widespread use. There has been no official recommendation from the ACIP that the vaccine be routinely used in this population. The expert panel has noted that to date there are no data showing that the PCV 13 vaccine is effective in preventing pneumococcal pneumonia in adults, although a Dutch trial in 85,000 people over age 65 is underway.
The committee also noted that one-quarter of all cases of invasive pneumococcal disease in seniors are caused by 11 serotypes in the PPSV 23 vaccine that are not included in the PCV 13 vaccine, which further complicates the situation. The PPSV 23 vaccine has been approved since 1983 and is recommended for use in all adults over age 65 and in younger adults with certain underlying medical conditions, including diabetes and chronic lung disease.
Also, if the serotypes contained in the PCV 13 vaccine are going to largely go away in the senior population as a consequence of universal pediatric immunization, which could happen based upon the earlier herd immunity experience noted with the PCV 7 vaccine, then it may not be reasonable to give PCV 13 to all older adults, Dr. Glodé noted.
She reported serving on the data safety monitoring board for trials of an unrelated Pfizer vaccine.
VAIL, COLO. - American medicine emphatically surpassed the Healthy People 2010 goal for reduction of invasive Streptococcus pneumoniae infections well ahead of schedule in both of the highest-risk target groups: children under age 5 years and seniors. And the tougher Healthy People 2020 objectives are already well within striking distance.
"We get an A+ on this," Dr. Mary P. Glodé commented at the annual pediatric infectious diseases conference sponsored by Children’s Hospital Colorado.
The Healthy People 2010 objective was to reduce the incidence of invasive S. pneumoniae infections to 46 cases per 100,000 among children under age 5 years and to 42 per 100,000 persons age 65 or older. The actual 2010 rates were 19 and 36 per 100,000, respectively.
Between 1999 and 2010, the annual rate of invasive pneumococcal disease in children younger age 5 plummeted by 86% as a consequence of the licensure in 2000 of the pneumococcal conjugate vaccine 7 (PCV 7) vaccine.
Most impressively, the rate also fell by 50% during that period among seniors, even though they didn’t receive the vaccine. This is ascribed to herd immunity. The presumed mechanism is that once immunized, young children were far less likely to become colonized by virulent pneumococcal serotypes, with resultant diminished opportunity for transmission of the pathogens to older children and adults, explained Dr. Glodé, professor of pediatrics and head of the section of pediatric infectious disease at the University of Colorado, Denver, and Children’s Hospital Colorado.
The Healthy People 2020 goal is to further reduce the incidence of invasive pneumococcal infections in children under age 5 from the 2010 rate of 19 down to 12 per 100,000, and in seniors from the 2010 figure of 36 per 100,000 to 31 per 100,000.
The expectation is that the target in children will be handily reached, and early on, as a consequence of the spring 2010 recommendation by the American Academy of Pediatrics and the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) that all children aged 2-59 months be routinely vaccinated with the PCV 13 vaccine, which contains the PCV 7 serotypes plus six others causing invasive disease. Early unpublished CDC data suggest there has already been some decline in disease in children as a result of the added serotypes included in PCV 13, especially in cases involving serotypes 19A and 7F, according to Dr. Glodé.
The difficult unanswered question concerns the best way to get the nation’s seniors to the Healthy People 2020 target. The rate of invasive pneumococcal disease is higher in persons aged 65 and older than in any other age group, as is the associated mortality. Indeed, of an estimated 44,000 cases of invasive pneumococcal disease in the United States during 2009, 37,000 were in adults, including 15,000 cases in individuals age 65 or more.
Late last year the Food and Drug Administration licensed the PCV 13 vaccine for use in people aged 50 and up. But that doesn’t necessarily mean it will see widespread use. There has been no official recommendation from the ACIP that the vaccine be routinely used in this population. The expert panel has noted that to date there are no data showing that the PCV 13 vaccine is effective in preventing pneumococcal pneumonia in adults, although a Dutch trial in 85,000 people over age 65 is underway.
The committee also noted that one-quarter of all cases of invasive pneumococcal disease in seniors are caused by 11 serotypes in the PPSV 23 vaccine that are not included in the PCV 13 vaccine, which further complicates the situation. The PPSV 23 vaccine has been approved since 1983 and is recommended for use in all adults over age 65 and in younger adults with certain underlying medical conditions, including diabetes and chronic lung disease.
Also, if the serotypes contained in the PCV 13 vaccine are going to largely go away in the senior population as a consequence of universal pediatric immunization, which could happen based upon the earlier herd immunity experience noted with the PCV 7 vaccine, then it may not be reasonable to give PCV 13 to all older adults, Dr. Glodé noted.
She reported serving on the data safety monitoring board for trials of an unrelated Pfizer vaccine.
EXPERT ANALYSIS FROM THE ANNUAL PEDIATRIC INFECTIOUS DISEASES CONFERENCE SPONSORED BY CHILDREN'S HOSPITAL COLORADO
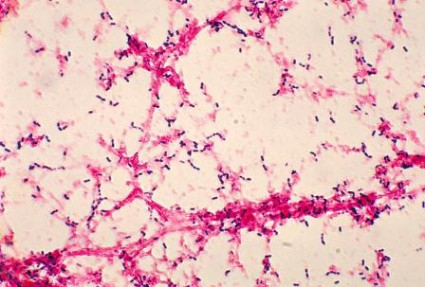
Antibiotics fail to head off sepsis … Failure to address persistent symptoms proves disastrous… more
Antibiotics fail to head off sepsis
SHORTNESS OF BREATH AND RIGHT-SIDED CHEST PAIN prompted a 45-year-old woman to go to the emergency department (ED) early one morning. She had a history of chronic lung problems with multiple diagnoses of pneumonia, pneumothorax, blebs, and bronchiectasis. The ED doctor diagnosed community-acquired pneumonia and admitted her for intravenous antibiotic treatment.
Late that afternoon the patient’s condition deteriorated rapidly. She was transferred to the intensive care unit, where she died of septic shock caused by Pseudomonas aeruginosa 22 hours after she had arrived at the ED.
PLAINTIFF’S CLAIM The patient should have received broader-spectrum antibiotics.
THE DEFENSE The hospitalist who treated the woman as an inpatient claimed that the treatment she received was appropriate and that she probably would have died even if other antibiotics had been prescribed. The hospitalist also claimed that the nursing staff failed to notify her of the patient’s low blood pressure readings until 10 hours after the initial evaluation. A nurse denied this claim, asserting that the hospitalist had been paged several times during the day. The discharge summary and nursing notes on the patient were missing.
VERDICT $5.28 million arbitration award.
COMMENT It surprises me how often key portions of medical records go missing! Here, the absence of a discharge summary and nursing notes may well have contributed to a $5 million award.
Change, and not for the better
AN ATYPICAL MOLE ON THE LEFT CALF was brought to the attention of a primary care physician by a 36-year-old man during a full physical. The mole was 1 3 1 cm; the patient reported that it had been changing. The mole’s appearance didn’t worry the physician, who described it in his notes as either a hemangioma or dermatofibroma. The doctor advised the patient to return in 6 months if he wanted the mole removed for cosmetic reasons.
Over the next 5 months, the patient noticed further changes in the mole and called the doctor’s office. He was seen by a colleague of his physician, who immediately sent the patient for a biopsy and surgical consultation. The mole was removed and diagnosed as an ulcerating melanoma with downward growth.
Shortly thereafter, the patient underwent wide excision and lymph node dissection, which showed clear margins and no lymph node involvement. Twenty months later, a mass was found in the patient’s liver. Biopsy diagnosed metastatic spread of the melanoma. The patient died 2 months later.
PLAINTIFF’S CLAIM The patient should have had a biopsy and received a surgical referral at the time of the physical examination when he first reported the mole.
THE DEFENSE Waiting for 6 months was appropriate because the mole didn’t look like a melanoma when the patient first called it to the physician’s attention. The melanoma had already metastasized at the time of the physical examination and the diagnostic delay didn’t affect the outcome.
VERDICT $1 million Massachusetts settlement.
COMMENT A changing mole should always raise concern. Biopsy, excision, or a referral could have avoided a million-dollar settlement.
Failure to address persistent symptoms proves disastrous
PAIN IN THE BACK AND CHEST along with respiratory difficulty prompted a 49-year-old man to visit his physician. The physician told him to go to a hospital. The doctor who examined the patient at the hospital diagnosed muscle strain and prescribed muscle relaxants.
The following day, the patient returned to his physician complaining of continuing symptoms. The doctor sent him home. He died the next day of an aortic rupture caused by an undiagnosed dissection.
PLAINTIFF’S CLAIM The 2 physicians should have diagnosed the dissection, which would have permitted treatment and prevented death. The patient had been treated previously at the hospital, and his records should have raised suspicion of an aortic aneurysm. The hospital physician was a new hire and hadn’t received proper training in the hospital’s electronic records system. He should have ordered a computed tomography scan or cardiology consult. The patient’s physician failed to address the ongoing symptoms. He should have hospitalized the patient at the time of the second visit.
THE DEFENSE The hospital physician claimed he had intended to contact the cardiologist who had treated the patient, but the patient couldn’t remember the cardiologist’s name. The patient’s symptoms didn’t suggest an aortic dissection, and the dissection occurred after the patient was discharged from the hospital.
VERDICT $3.4 million New York verdict against the hospital physician only.
COMMENT Although the hoofbeats are usually horses, always remember the zebras (or should it be lions?), particularly when a patient returns repeatedly with ongoing symptoms.
Controlled substances out of control
A WOMAN WITH CHRONIC MIGRAINES, anxiety problems, and nausea also had cardiomyopathy and chronic atrial fibrillation, which could be triggered by pain from her other ailments. She came under the care of a physician who prescribed a number of drugs, including meperidine, hydrocodone, tizanidine, diazepam, promethazine, alprazolam, and oxcarbazepine. The doctor prescribed injectable forms of certain medications after the patient told him her next-door neighbor was a nurse and could help administer the drugs.
Four years after coming under the doctor’s care, the patient signed a Controlled Substance Agreement specifying that the physician would discontinue her as a patient if she got controlled substances from another doctor. (Evidence was later found that the patient was receiving prescriptions from other physicians.)
While under treatment by her doctor, the patient was hospitalized a number of times for medication overdoses. The record from one hospitalization reported that she had made angry, profanity-laced requests for meperidine and promethazine.
About 2 years after signing the Controlled Substance Agreement, the patient received prescriptions from her doctor for 210 doses of meperidine, 100 doses of promethazine, and 60 pills each of diazepam, alprazolam, and acetaminophen and hydrocodone. She filled the prescriptions at 2 pharmacies without objections from the pharmacists. She died of an accidental drug overdose the following month.
Postmortem blood testing showed high levels of meperidine and promethazine. The patient had apparently taken the equivalent of 11 “shots” of meperidine (5 times the maximum prescribed amount), probably by injecting herself through a peripherally inserted central catheter rather than by intramuscular injection, as prescribed.
PLAINTIFF’S CLAIM The patient’s doctor was negligent in prescribing large amounts of controlled substances when he should have known that she was a drug seeker with a drug abuse problem. The pharmacies were negligent for filling the prescriptions without question.
THE DEFENSE The patient was solely responsible for her own death because she gave herself a large overdose.
VERDICT $500,000 Alabama verdict. The case against the pharmacies was dismissed.
COMMENT Increasingly it is expected that physicians (and pharmacists) perform due diligence when prescribing opioids, including taking reasonable precautions against the drug-seeking patient.
Antibiotics fail to head off sepsis
SHORTNESS OF BREATH AND RIGHT-SIDED CHEST PAIN prompted a 45-year-old woman to go to the emergency department (ED) early one morning. She had a history of chronic lung problems with multiple diagnoses of pneumonia, pneumothorax, blebs, and bronchiectasis. The ED doctor diagnosed community-acquired pneumonia and admitted her for intravenous antibiotic treatment.
Late that afternoon the patient’s condition deteriorated rapidly. She was transferred to the intensive care unit, where she died of septic shock caused by Pseudomonas aeruginosa 22 hours after she had arrived at the ED.
PLAINTIFF’S CLAIM The patient should have received broader-spectrum antibiotics.
THE DEFENSE The hospitalist who treated the woman as an inpatient claimed that the treatment she received was appropriate and that she probably would have died even if other antibiotics had been prescribed. The hospitalist also claimed that the nursing staff failed to notify her of the patient’s low blood pressure readings until 10 hours after the initial evaluation. A nurse denied this claim, asserting that the hospitalist had been paged several times during the day. The discharge summary and nursing notes on the patient were missing.
VERDICT $5.28 million arbitration award.
COMMENT It surprises me how often key portions of medical records go missing! Here, the absence of a discharge summary and nursing notes may well have contributed to a $5 million award.
Change, and not for the better
AN ATYPICAL MOLE ON THE LEFT CALF was brought to the attention of a primary care physician by a 36-year-old man during a full physical. The mole was 1 3 1 cm; the patient reported that it had been changing. The mole’s appearance didn’t worry the physician, who described it in his notes as either a hemangioma or dermatofibroma. The doctor advised the patient to return in 6 months if he wanted the mole removed for cosmetic reasons.
Over the next 5 months, the patient noticed further changes in the mole and called the doctor’s office. He was seen by a colleague of his physician, who immediately sent the patient for a biopsy and surgical consultation. The mole was removed and diagnosed as an ulcerating melanoma with downward growth.
Shortly thereafter, the patient underwent wide excision and lymph node dissection, which showed clear margins and no lymph node involvement. Twenty months later, a mass was found in the patient’s liver. Biopsy diagnosed metastatic spread of the melanoma. The patient died 2 months later.
PLAINTIFF’S CLAIM The patient should have had a biopsy and received a surgical referral at the time of the physical examination when he first reported the mole.
THE DEFENSE Waiting for 6 months was appropriate because the mole didn’t look like a melanoma when the patient first called it to the physician’s attention. The melanoma had already metastasized at the time of the physical examination and the diagnostic delay didn’t affect the outcome.
VERDICT $1 million Massachusetts settlement.
COMMENT A changing mole should always raise concern. Biopsy, excision, or a referral could have avoided a million-dollar settlement.
Failure to address persistent symptoms proves disastrous
PAIN IN THE BACK AND CHEST along with respiratory difficulty prompted a 49-year-old man to visit his physician. The physician told him to go to a hospital. The doctor who examined the patient at the hospital diagnosed muscle strain and prescribed muscle relaxants.
The following day, the patient returned to his physician complaining of continuing symptoms. The doctor sent him home. He died the next day of an aortic rupture caused by an undiagnosed dissection.
PLAINTIFF’S CLAIM The 2 physicians should have diagnosed the dissection, which would have permitted treatment and prevented death. The patient had been treated previously at the hospital, and his records should have raised suspicion of an aortic aneurysm. The hospital physician was a new hire and hadn’t received proper training in the hospital’s electronic records system. He should have ordered a computed tomography scan or cardiology consult. The patient’s physician failed to address the ongoing symptoms. He should have hospitalized the patient at the time of the second visit.
THE DEFENSE The hospital physician claimed he had intended to contact the cardiologist who had treated the patient, but the patient couldn’t remember the cardiologist’s name. The patient’s symptoms didn’t suggest an aortic dissection, and the dissection occurred after the patient was discharged from the hospital.
VERDICT $3.4 million New York verdict against the hospital physician only.
COMMENT Although the hoofbeats are usually horses, always remember the zebras (or should it be lions?), particularly when a patient returns repeatedly with ongoing symptoms.
Controlled substances out of control
A WOMAN WITH CHRONIC MIGRAINES, anxiety problems, and nausea also had cardiomyopathy and chronic atrial fibrillation, which could be triggered by pain from her other ailments. She came under the care of a physician who prescribed a number of drugs, including meperidine, hydrocodone, tizanidine, diazepam, promethazine, alprazolam, and oxcarbazepine. The doctor prescribed injectable forms of certain medications after the patient told him her next-door neighbor was a nurse and could help administer the drugs.
Four years after coming under the doctor’s care, the patient signed a Controlled Substance Agreement specifying that the physician would discontinue her as a patient if she got controlled substances from another doctor. (Evidence was later found that the patient was receiving prescriptions from other physicians.)
While under treatment by her doctor, the patient was hospitalized a number of times for medication overdoses. The record from one hospitalization reported that she had made angry, profanity-laced requests for meperidine and promethazine.
About 2 years after signing the Controlled Substance Agreement, the patient received prescriptions from her doctor for 210 doses of meperidine, 100 doses of promethazine, and 60 pills each of diazepam, alprazolam, and acetaminophen and hydrocodone. She filled the prescriptions at 2 pharmacies without objections from the pharmacists. She died of an accidental drug overdose the following month.
Postmortem blood testing showed high levels of meperidine and promethazine. The patient had apparently taken the equivalent of 11 “shots” of meperidine (5 times the maximum prescribed amount), probably by injecting herself through a peripherally inserted central catheter rather than by intramuscular injection, as prescribed.
PLAINTIFF’S CLAIM The patient’s doctor was negligent in prescribing large amounts of controlled substances when he should have known that she was a drug seeker with a drug abuse problem. The pharmacies were negligent for filling the prescriptions without question.
THE DEFENSE The patient was solely responsible for her own death because she gave herself a large overdose.
VERDICT $500,000 Alabama verdict. The case against the pharmacies was dismissed.
COMMENT Increasingly it is expected that physicians (and pharmacists) perform due diligence when prescribing opioids, including taking reasonable precautions against the drug-seeking patient.
Antibiotics fail to head off sepsis
SHORTNESS OF BREATH AND RIGHT-SIDED CHEST PAIN prompted a 45-year-old woman to go to the emergency department (ED) early one morning. She had a history of chronic lung problems with multiple diagnoses of pneumonia, pneumothorax, blebs, and bronchiectasis. The ED doctor diagnosed community-acquired pneumonia and admitted her for intravenous antibiotic treatment.
Late that afternoon the patient’s condition deteriorated rapidly. She was transferred to the intensive care unit, where she died of septic shock caused by Pseudomonas aeruginosa 22 hours after she had arrived at the ED.
PLAINTIFF’S CLAIM The patient should have received broader-spectrum antibiotics.
THE DEFENSE The hospitalist who treated the woman as an inpatient claimed that the treatment she received was appropriate and that she probably would have died even if other antibiotics had been prescribed. The hospitalist also claimed that the nursing staff failed to notify her of the patient’s low blood pressure readings until 10 hours after the initial evaluation. A nurse denied this claim, asserting that the hospitalist had been paged several times during the day. The discharge summary and nursing notes on the patient were missing.
VERDICT $5.28 million arbitration award.
COMMENT It surprises me how often key portions of medical records go missing! Here, the absence of a discharge summary and nursing notes may well have contributed to a $5 million award.
Change, and not for the better
AN ATYPICAL MOLE ON THE LEFT CALF was brought to the attention of a primary care physician by a 36-year-old man during a full physical. The mole was 1 3 1 cm; the patient reported that it had been changing. The mole’s appearance didn’t worry the physician, who described it in his notes as either a hemangioma or dermatofibroma. The doctor advised the patient to return in 6 months if he wanted the mole removed for cosmetic reasons.
Over the next 5 months, the patient noticed further changes in the mole and called the doctor’s office. He was seen by a colleague of his physician, who immediately sent the patient for a biopsy and surgical consultation. The mole was removed and diagnosed as an ulcerating melanoma with downward growth.
Shortly thereafter, the patient underwent wide excision and lymph node dissection, which showed clear margins and no lymph node involvement. Twenty months later, a mass was found in the patient’s liver. Biopsy diagnosed metastatic spread of the melanoma. The patient died 2 months later.
PLAINTIFF’S CLAIM The patient should have had a biopsy and received a surgical referral at the time of the physical examination when he first reported the mole.
THE DEFENSE Waiting for 6 months was appropriate because the mole didn’t look like a melanoma when the patient first called it to the physician’s attention. The melanoma had already metastasized at the time of the physical examination and the diagnostic delay didn’t affect the outcome.
VERDICT $1 million Massachusetts settlement.
COMMENT A changing mole should always raise concern. Biopsy, excision, or a referral could have avoided a million-dollar settlement.
Failure to address persistent symptoms proves disastrous
PAIN IN THE BACK AND CHEST along with respiratory difficulty prompted a 49-year-old man to visit his physician. The physician told him to go to a hospital. The doctor who examined the patient at the hospital diagnosed muscle strain and prescribed muscle relaxants.
The following day, the patient returned to his physician complaining of continuing symptoms. The doctor sent him home. He died the next day of an aortic rupture caused by an undiagnosed dissection.
PLAINTIFF’S CLAIM The 2 physicians should have diagnosed the dissection, which would have permitted treatment and prevented death. The patient had been treated previously at the hospital, and his records should have raised suspicion of an aortic aneurysm. The hospital physician was a new hire and hadn’t received proper training in the hospital’s electronic records system. He should have ordered a computed tomography scan or cardiology consult. The patient’s physician failed to address the ongoing symptoms. He should have hospitalized the patient at the time of the second visit.
THE DEFENSE The hospital physician claimed he had intended to contact the cardiologist who had treated the patient, but the patient couldn’t remember the cardiologist’s name. The patient’s symptoms didn’t suggest an aortic dissection, and the dissection occurred after the patient was discharged from the hospital.
VERDICT $3.4 million New York verdict against the hospital physician only.
COMMENT Although the hoofbeats are usually horses, always remember the zebras (or should it be lions?), particularly when a patient returns repeatedly with ongoing symptoms.
Controlled substances out of control
A WOMAN WITH CHRONIC MIGRAINES, anxiety problems, and nausea also had cardiomyopathy and chronic atrial fibrillation, which could be triggered by pain from her other ailments. She came under the care of a physician who prescribed a number of drugs, including meperidine, hydrocodone, tizanidine, diazepam, promethazine, alprazolam, and oxcarbazepine. The doctor prescribed injectable forms of certain medications after the patient told him her next-door neighbor was a nurse and could help administer the drugs.
Four years after coming under the doctor’s care, the patient signed a Controlled Substance Agreement specifying that the physician would discontinue her as a patient if she got controlled substances from another doctor. (Evidence was later found that the patient was receiving prescriptions from other physicians.)
While under treatment by her doctor, the patient was hospitalized a number of times for medication overdoses. The record from one hospitalization reported that she had made angry, profanity-laced requests for meperidine and promethazine.
About 2 years after signing the Controlled Substance Agreement, the patient received prescriptions from her doctor for 210 doses of meperidine, 100 doses of promethazine, and 60 pills each of diazepam, alprazolam, and acetaminophen and hydrocodone. She filled the prescriptions at 2 pharmacies without objections from the pharmacists. She died of an accidental drug overdose the following month.
Postmortem blood testing showed high levels of meperidine and promethazine. The patient had apparently taken the equivalent of 11 “shots” of meperidine (5 times the maximum prescribed amount), probably by injecting herself through a peripherally inserted central catheter rather than by intramuscular injection, as prescribed.
PLAINTIFF’S CLAIM The patient’s doctor was negligent in prescribing large amounts of controlled substances when he should have known that she was a drug seeker with a drug abuse problem. The pharmacies were negligent for filling the prescriptions without question.
THE DEFENSE The patient was solely responsible for her own death because she gave herself a large overdose.
VERDICT $500,000 Alabama verdict. The case against the pharmacies was dismissed.
COMMENT Increasingly it is expected that physicians (and pharmacists) perform due diligence when prescribing opioids, including taking reasonable precautions against the drug-seeking patient.
Rethinking antibiotics for sinusitis—again
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than over-the-counter (OTC) remedies alone.1
STRENGTH OF RECOMMENDATION
B: Based on a single high-quality randomized controlled trial.
Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012 ;307:685-692.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after suffering from fatigue, purulent nasal discharge, and unilateral facial pain for nearly 10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his recovery.
Each year, more than 30 million Americans—about one in 7 adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
Centers for Disease Control and Prevention (CDC) guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last 7 days or more, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than 7 days are unlikely to have a bacterial infection. But the non-specific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within 2 weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
An earlier PURL based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO-HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY: Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1 To be eligible for the study, patients had to be between the ages of 18 and 70 years, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of 7- to-28-day duration and worsening or not improving or of <7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past 4 weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1500 mg/d, divided into 3 doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0=no problem; 3=severe problem), with a clinically important difference of ≥0.5 on the mean score. The test was administered at enrollment and at Days 3, 7, and 10. The disease-specific quality of life at Day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on Days 3 and 10. On Day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a 6-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control group at Days 3 and 10. On Day 7, 74% of patients treated with amoxicillin self- reported significant improvement in symptoms since the start of the study, vs 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3-34; P= .02) for a reduction in symptoms at Day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (<10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW: Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on Day 7 of 0.19 points, but no clinically meaningful difference (≥0.5) based on the SNOT-16 mean score.
CAVEATS: Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION: Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Physicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhino-sinusitis, as well as by offering symptomatic treatments.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. Available at: http://www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al. American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2008;(2):CD000243.-
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009;(4):CD005149.-
9. Schumann A, Hickner J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no”. J Fam Pract. Jul:2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008;47:735-743.
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than over-the-counter (OTC) remedies alone.1
STRENGTH OF RECOMMENDATION
B: Based on a single high-quality randomized controlled trial.
Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012 ;307:685-692.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after suffering from fatigue, purulent nasal discharge, and unilateral facial pain for nearly 10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his recovery.
Each year, more than 30 million Americans—about one in 7 adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
Centers for Disease Control and Prevention (CDC) guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last 7 days or more, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than 7 days are unlikely to have a bacterial infection. But the non-specific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within 2 weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
An earlier PURL based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO-HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY: Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1 To be eligible for the study, patients had to be between the ages of 18 and 70 years, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of 7- to-28-day duration and worsening or not improving or of <7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past 4 weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1500 mg/d, divided into 3 doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0=no problem; 3=severe problem), with a clinically important difference of ≥0.5 on the mean score. The test was administered at enrollment and at Days 3, 7, and 10. The disease-specific quality of life at Day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on Days 3 and 10. On Day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a 6-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control group at Days 3 and 10. On Day 7, 74% of patients treated with amoxicillin self- reported significant improvement in symptoms since the start of the study, vs 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3-34; P= .02) for a reduction in symptoms at Day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (<10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW: Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on Day 7 of 0.19 points, but no clinically meaningful difference (≥0.5) based on the SNOT-16 mean score.
CAVEATS: Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION: Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Physicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhino-sinusitis, as well as by offering symptomatic treatments.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than over-the-counter (OTC) remedies alone.1
STRENGTH OF RECOMMENDATION
B: Based on a single high-quality randomized controlled trial.
Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012 ;307:685-692.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after suffering from fatigue, purulent nasal discharge, and unilateral facial pain for nearly 10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his recovery.
Each year, more than 30 million Americans—about one in 7 adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
Centers for Disease Control and Prevention (CDC) guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last 7 days or more, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than 7 days are unlikely to have a bacterial infection. But the non-specific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within 2 weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
An earlier PURL based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO-HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY: Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1 To be eligible for the study, patients had to be between the ages of 18 and 70 years, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of 7- to-28-day duration and worsening or not improving or of <7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past 4 weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1500 mg/d, divided into 3 doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0=no problem; 3=severe problem), with a clinically important difference of ≥0.5 on the mean score. The test was administered at enrollment and at Days 3, 7, and 10. The disease-specific quality of life at Day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on Days 3 and 10. On Day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a 6-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control group at Days 3 and 10. On Day 7, 74% of patients treated with amoxicillin self- reported significant improvement in symptoms since the start of the study, vs 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3-34; P= .02) for a reduction in symptoms at Day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (<10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW: Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on Day 7 of 0.19 points, but no clinically meaningful difference (≥0.5) based on the SNOT-16 mean score.
CAVEATS: Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION: Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Physicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhino-sinusitis, as well as by offering symptomatic treatments.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. Available at: http://www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al. American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2008;(2):CD000243.-
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009;(4):CD005149.-
9. Schumann A, Hickner J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no”. J Fam Pract. Jul:2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008;47:735-743.
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. Available at: http://www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al. American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2008;(2):CD000243.-
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009;(4):CD005149.-
9. Schumann A, Hickner J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no”. J Fam Pract. Jul:2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008;47:735-743.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.