User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
For COPD Inpatients, Focus on Preventing Future Exacerbations
ATLANTA – Data suggest that only about a third of patients hospitalized for chronic obstructive pulmonary disease receive appropriate care, but a number of steps – beginning with decisions about when to admit and ending with proper discharge management – can be taken to improve outcomes, according to Dr. Darcy Marciniuk.
Although scientific guidance on when patients should be admitted is lacking, guidelines and consensus statements suggest that patients with an exacerbation should be admitted:

• If they experience a marked increase in dyspnea.
• If they have severe underlying COPD with little reserve, "such that there’s no room for error."
• If they fail to respond to initial management.
• If they have comorbidities, including heart failure, arrhythmias, or renal impairment.
• If they have advanced age.
• If they experience frequent severe exacerbations.
• If they have insufficient home support.
Once a patient is admitted, controlled appropriate supplemental oxygen should be administered as directed by Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, noninvasive ventilation should be used when indicated, aggressive therapies should be used at the outset, and use of antibiotics or systemic corticosteroids should be considered, said Dr. Marciniuk, AACP president, and head of the division of respirology, critical care, and sleep medicine at the University of Saskatchewan, Saskatoon, Canada.
An effort should also be made to identify the precipitating factor, to recognize and optimize, or prevent comorbid conditions, to prevent complications, and to address depressions and anxiety, he said.
With respect to supplemental oxygen, the GOLD guidelines will help ensure there is "always enough, but never too much," Dr. Marciniuk said.
"Now, with saturation monitors, life is good; it’s very easy to make sure patients receive appropriate therapy," he added.
He also spotlighted noninvasive ventilation. It has revolutionized in-hospital COPD management, lowering intubation rates by 60% and substantially decreasing in-hospital mortality, he said.
"Noninvasive ventilation has been incredible for our patients," he said.
Although it was first used in the 1980s, it is now "really the treatment of choice for acute hypercapnic respiratory failure in this setting," he added.
Contrary to some beliefs about outcomes with COPD in the intensive care unit, mortality is actually much lower than for many other conditions. For example, mortality in COPD patients in the ICU is about half that of patients with sepsis or acute respiratory distress syndrome.
"So, even though a patient may look short of breath, and someone may think they have a poor quality of life, it is the patients who should be judging that," he said, adding: "There needs to be that comfort, that back-up, of the ICU, because data would suggest the outcomes are pretty good."
There is significant evidence of benefit with the use of noninvasive ventilation, particularly with respiratory acidosis of pH less than 7.35, PCO2 greater than 45, and significant dyspnea, which is easily detected by clinical means, he added.
Depression in COPD patients is also particularly important to address.
Studies show that patients with depression have longer hospital stays (twice as long, according to one observational study), more frequent exacerbations in the year following discharge, and higher mortality rates, he said, acknowledging that "our understanding of the co-presence of depression and anxiety (in COPD patients) is growing, but our understanding that it appears to [have an impact] in this setting is also growing."
As for discharge planning, appropriate methods and practices must be put in place for reducing the future risk of acute exacerbations, he said.
Dr. Marciniuk reported having no financial disclosures, with the exception of research funding directed to and managed by his institution.
ATLANTA – Data suggest that only about a third of patients hospitalized for chronic obstructive pulmonary disease receive appropriate care, but a number of steps – beginning with decisions about when to admit and ending with proper discharge management – can be taken to improve outcomes, according to Dr. Darcy Marciniuk.
Although scientific guidance on when patients should be admitted is lacking, guidelines and consensus statements suggest that patients with an exacerbation should be admitted:
• If they experience a marked increase in dyspnea.
• If they have severe underlying COPD with little reserve, "such that there’s no room for error."
• If they fail to respond to initial management.
• If they have comorbidities, including heart failure, arrhythmias, or renal impairment.
• If they have advanced age.
• If they experience frequent severe exacerbations.
• If they have insufficient home support.
Once a patient is admitted, controlled appropriate supplemental oxygen should be administered as directed by Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, noninvasive ventilation should be used when indicated, aggressive therapies should be used at the outset, and use of antibiotics or systemic corticosteroids should be considered, said Dr. Marciniuk, AACP president, and head of the division of respirology, critical care, and sleep medicine at the University of Saskatchewan, Saskatoon, Canada.
An effort should also be made to identify the precipitating factor, to recognize and optimize, or prevent comorbid conditions, to prevent complications, and to address depressions and anxiety, he said.
With respect to supplemental oxygen, the GOLD guidelines will help ensure there is "always enough, but never too much," Dr. Marciniuk said.
"Now, with saturation monitors, life is good; it’s very easy to make sure patients receive appropriate therapy," he added.
He also spotlighted noninvasive ventilation. It has revolutionized in-hospital COPD management, lowering intubation rates by 60% and substantially decreasing in-hospital mortality, he said.
"Noninvasive ventilation has been incredible for our patients," he said.
Although it was first used in the 1980s, it is now "really the treatment of choice for acute hypercapnic respiratory failure in this setting," he added.
Contrary to some beliefs about outcomes with COPD in the intensive care unit, mortality is actually much lower than for many other conditions. For example, mortality in COPD patients in the ICU is about half that of patients with sepsis or acute respiratory distress syndrome.
"So, even though a patient may look short of breath, and someone may think they have a poor quality of life, it is the patients who should be judging that," he said, adding: "There needs to be that comfort, that back-up, of the ICU, because data would suggest the outcomes are pretty good."
There is significant evidence of benefit with the use of noninvasive ventilation, particularly with respiratory acidosis of pH less than 7.35, PCO2 greater than 45, and significant dyspnea, which is easily detected by clinical means, he added.
Depression in COPD patients is also particularly important to address.
Studies show that patients with depression have longer hospital stays (twice as long, according to one observational study), more frequent exacerbations in the year following discharge, and higher mortality rates, he said, acknowledging that "our understanding of the co-presence of depression and anxiety (in COPD patients) is growing, but our understanding that it appears to [have an impact] in this setting is also growing."
As for discharge planning, appropriate methods and practices must be put in place for reducing the future risk of acute exacerbations, he said.
Dr. Marciniuk reported having no financial disclosures, with the exception of research funding directed to and managed by his institution.
ATLANTA – Data suggest that only about a third of patients hospitalized for chronic obstructive pulmonary disease receive appropriate care, but a number of steps – beginning with decisions about when to admit and ending with proper discharge management – can be taken to improve outcomes, according to Dr. Darcy Marciniuk.
Although scientific guidance on when patients should be admitted is lacking, guidelines and consensus statements suggest that patients with an exacerbation should be admitted:
• If they experience a marked increase in dyspnea.
• If they have severe underlying COPD with little reserve, "such that there’s no room for error."
• If they fail to respond to initial management.
• If they have comorbidities, including heart failure, arrhythmias, or renal impairment.
• If they have advanced age.
• If they experience frequent severe exacerbations.
• If they have insufficient home support.
Once a patient is admitted, controlled appropriate supplemental oxygen should be administered as directed by Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, noninvasive ventilation should be used when indicated, aggressive therapies should be used at the outset, and use of antibiotics or systemic corticosteroids should be considered, said Dr. Marciniuk, AACP president, and head of the division of respirology, critical care, and sleep medicine at the University of Saskatchewan, Saskatoon, Canada.
An effort should also be made to identify the precipitating factor, to recognize and optimize, or prevent comorbid conditions, to prevent complications, and to address depressions and anxiety, he said.
With respect to supplemental oxygen, the GOLD guidelines will help ensure there is "always enough, but never too much," Dr. Marciniuk said.
"Now, with saturation monitors, life is good; it’s very easy to make sure patients receive appropriate therapy," he added.
He also spotlighted noninvasive ventilation. It has revolutionized in-hospital COPD management, lowering intubation rates by 60% and substantially decreasing in-hospital mortality, he said.
"Noninvasive ventilation has been incredible for our patients," he said.
Although it was first used in the 1980s, it is now "really the treatment of choice for acute hypercapnic respiratory failure in this setting," he added.
Contrary to some beliefs about outcomes with COPD in the intensive care unit, mortality is actually much lower than for many other conditions. For example, mortality in COPD patients in the ICU is about half that of patients with sepsis or acute respiratory distress syndrome.
"So, even though a patient may look short of breath, and someone may think they have a poor quality of life, it is the patients who should be judging that," he said, adding: "There needs to be that comfort, that back-up, of the ICU, because data would suggest the outcomes are pretty good."
There is significant evidence of benefit with the use of noninvasive ventilation, particularly with respiratory acidosis of pH less than 7.35, PCO2 greater than 45, and significant dyspnea, which is easily detected by clinical means, he added.
Depression in COPD patients is also particularly important to address.
Studies show that patients with depression have longer hospital stays (twice as long, according to one observational study), more frequent exacerbations in the year following discharge, and higher mortality rates, he said, acknowledging that "our understanding of the co-presence of depression and anxiety (in COPD patients) is growing, but our understanding that it appears to [have an impact] in this setting is also growing."
As for discharge planning, appropriate methods and practices must be put in place for reducing the future risk of acute exacerbations, he said.
Dr. Marciniuk reported having no financial disclosures, with the exception of research funding directed to and managed by his institution.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS

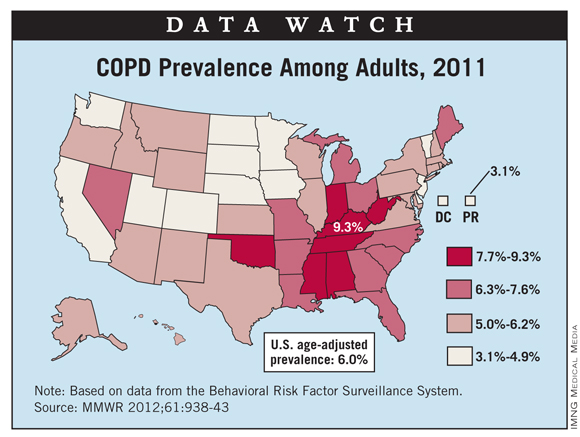
Kentucky Leads U.S. in Adult COPD Prevalence
Kentucky had the highest prevalence of chronic obstructive pulmonary disease in adults, 9.3%, in 2011, according to a study in Morbidity and Mortality Weekly Report.
The data for the first-ever report of state-specific prevalence of COPD among adults in all 50 states, the District of Columbia, and Puerto Rico come from the Behavioral Risk Factor Surveillance System. Among the 498,225 respondents to the survey, 39,038 reported that they had been told by a physician that they had COPD, for an overall prevalence of 6.3% (age-adjusted to 6%).
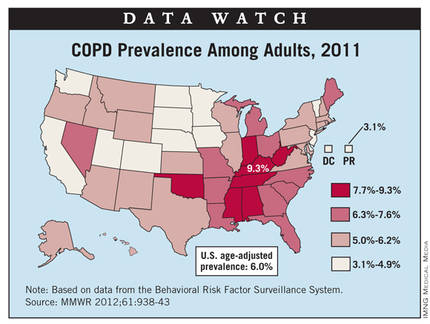
At 3.1%, Puerto Rico had the lowest COPD prevalence in the United States in 2011. The states with the lowest prevalence were Minnesota and Washington, both at 3.9%, according to the report.
Kentucky had the highest prevalence of chronic obstructive pulmonary disease in adults, 9.3%, in 2011, according to a study in Morbidity and Mortality Weekly Report.
The data for the first-ever report of state-specific prevalence of COPD among adults in all 50 states, the District of Columbia, and Puerto Rico come from the Behavioral Risk Factor Surveillance System. Among the 498,225 respondents to the survey, 39,038 reported that they had been told by a physician that they had COPD, for an overall prevalence of 6.3% (age-adjusted to 6%).
At 3.1%, Puerto Rico had the lowest COPD prevalence in the United States in 2011. The states with the lowest prevalence were Minnesota and Washington, both at 3.9%, according to the report.
Kentucky had the highest prevalence of chronic obstructive pulmonary disease in adults, 9.3%, in 2011, according to a study in Morbidity and Mortality Weekly Report.
The data for the first-ever report of state-specific prevalence of COPD among adults in all 50 states, the District of Columbia, and Puerto Rico come from the Behavioral Risk Factor Surveillance System. Among the 498,225 respondents to the survey, 39,038 reported that they had been told by a physician that they had COPD, for an overall prevalence of 6.3% (age-adjusted to 6%).
At 3.1%, Puerto Rico had the lowest COPD prevalence in the United States in 2011. The states with the lowest prevalence were Minnesota and Washington, both at 3.9%, according to the report.
Advanced Pleuroscopy Technique Is Biopsy Option for Unknown DPLDs
ATLANTA – Medical thoracoscopy is safe and feasible for performing lung biopsy in patients with diffuse parenchymal lung disease of unknown etiology on high-resolution computed tomography. And the approach could serve as an alternative to surgical biopsy in some patients, findings from a prospective study suggest.
In 10 patients who underwent medical thoracoscopic lung biopsies as part of the study, good biopsy specimens, with an average size of 0.5 x 0.4 cm were obtained, Dr. Mohamed Elnady said at the annual meeting of the American College of Chest Physicians.
Complications with this advanced technique included persistent air leak for 5-7 days in two patients, pneumothorax after removal of the intercostals tube in two patients, pain in six patients, and minor bleeding in one patient. The air leaks resolved spontaneously, and the pneumothoraces resolved with administration of high flow oxygen, said Dr. Elnady of Cairo (Egypt) University Hospitals.
The mean duration of intercostal tube placement was 3.1 days, with a range of 1-7 days; no infection, respiratory failure requiring intensive care unit admission, or mortality occurred within 30 days after the procedure, he noted.
Patients in the study included four women and six men with a mean age of 42 years. The lung biopsies obtained via medical thoracoscopy were sent for histopathologic examination, and patients underwent follow-up by chest x-ray for confirmation of lung expansion, as well as observation of the intercostal tube to detect complications. Among the ultimate diagnoses were metastatic adenocarcinoma, interstitial lung disease, and lymphangioleiomyomatosis.
"Thoracosopic lung biopsy by medical thoracoscopy is useful in the diagnosis of patient with diffuse pulmonary infiltrates of unknown etiology when lung biopsy is needed for an accurate diagnosis," Dr. Elnady concluded, noting that while the procedure does carry a risk of certain non–life-threatening complications, these can be minimized with good patient selection.
Commenting on the findings, Dr. Muthiah P. Muthiah, who moderated the session, said this novel approach to obtaining a lung biopsy is of interest, but also "something we still have to get comfortable with."
"I’m not ready to do this yet, but this is something to consider ... you will want to certainly do this with a surgeon’s back-up in your institution," said Dr. Muthiah of the University of Tennessee Health Science Center, Memphis.
Neither Dr. Muthiah nor Dr. Elnady had disclosures to report.
Dr. Lary Robinson, FCCP, comments: Medical thoracoscopy, commonly termed pleuroscopy, has been practiced for decades in some centers by pulmonary medicine specialists primarily to evaluate and treat pleural diseases, usually performed under conscious sedation.
Dr. Elmady from Cairo University Hospitals describes his experience in ten patients where a lung biopsy was performed. Their complication rate was significant (20% persistent air leak, 10% bleeding, 60% significant pain, etc.) for this awake procedure compared to the usual, minimal morbidity from VATS surgical thoracoscopy for lung biopsy. And the 5-mm x 4-mm diameter tissue specimen they obtained would be considered marginal at best for a definitive pathological diagnosis.
A VATS lung biopsy is a safe, quick 20-30 minute procedure under general anesthesia, with chest tube removal the following day, followed by discharge home in a very comfortable patient. Finally, most patients requiring this procedure have significantly compromised lung function (the reason for the biopsy) so that an awake, spontaneously-breathing patient can easily get into significant respiratory distress with the higher risk, medical thoracoscopic lung biopsy.
Lary Robinson, M.D., is a thoracic surgeon at the Moffitt Cancer Center in Tampa, Fla.
Dr. Lary Robinson, FCCP, comments: Medical thoracoscopy, commonly termed pleuroscopy, has been practiced for decades in some centers by pulmonary medicine specialists primarily to evaluate and treat pleural diseases, usually performed under conscious sedation.
Dr. Elmady from Cairo University Hospitals describes his experience in ten patients where a lung biopsy was performed. Their complication rate was significant (20% persistent air leak, 10% bleeding, 60% significant pain, etc.) for this awake procedure compared to the usual, minimal morbidity from VATS surgical thoracoscopy for lung biopsy. And the 5-mm x 4-mm diameter tissue specimen they obtained would be considered marginal at best for a definitive pathological diagnosis.
A VATS lung biopsy is a safe, quick 20-30 minute procedure under general anesthesia, with chest tube removal the following day, followed by discharge home in a very comfortable patient. Finally, most patients requiring this procedure have significantly compromised lung function (the reason for the biopsy) so that an awake, spontaneously-breathing patient can easily get into significant respiratory distress with the higher risk, medical thoracoscopic lung biopsy.
Lary Robinson, M.D., is a thoracic surgeon at the Moffitt Cancer Center in Tampa, Fla.
Dr. Lary Robinson, FCCP, comments: Medical thoracoscopy, commonly termed pleuroscopy, has been practiced for decades in some centers by pulmonary medicine specialists primarily to evaluate and treat pleural diseases, usually performed under conscious sedation.
Dr. Elmady from Cairo University Hospitals describes his experience in ten patients where a lung biopsy was performed. Their complication rate was significant (20% persistent air leak, 10% bleeding, 60% significant pain, etc.) for this awake procedure compared to the usual, minimal morbidity from VATS surgical thoracoscopy for lung biopsy. And the 5-mm x 4-mm diameter tissue specimen they obtained would be considered marginal at best for a definitive pathological diagnosis.
A VATS lung biopsy is a safe, quick 20-30 minute procedure under general anesthesia, with chest tube removal the following day, followed by discharge home in a very comfortable patient. Finally, most patients requiring this procedure have significantly compromised lung function (the reason for the biopsy) so that an awake, spontaneously-breathing patient can easily get into significant respiratory distress with the higher risk, medical thoracoscopic lung biopsy.
Lary Robinson, M.D., is a thoracic surgeon at the Moffitt Cancer Center in Tampa, Fla.
ATLANTA – Medical thoracoscopy is safe and feasible for performing lung biopsy in patients with diffuse parenchymal lung disease of unknown etiology on high-resolution computed tomography. And the approach could serve as an alternative to surgical biopsy in some patients, findings from a prospective study suggest.
In 10 patients who underwent medical thoracoscopic lung biopsies as part of the study, good biopsy specimens, with an average size of 0.5 x 0.4 cm were obtained, Dr. Mohamed Elnady said at the annual meeting of the American College of Chest Physicians.
Complications with this advanced technique included persistent air leak for 5-7 days in two patients, pneumothorax after removal of the intercostals tube in two patients, pain in six patients, and minor bleeding in one patient. The air leaks resolved spontaneously, and the pneumothoraces resolved with administration of high flow oxygen, said Dr. Elnady of Cairo (Egypt) University Hospitals.
The mean duration of intercostal tube placement was 3.1 days, with a range of 1-7 days; no infection, respiratory failure requiring intensive care unit admission, or mortality occurred within 30 days after the procedure, he noted.
Patients in the study included four women and six men with a mean age of 42 years. The lung biopsies obtained via medical thoracoscopy were sent for histopathologic examination, and patients underwent follow-up by chest x-ray for confirmation of lung expansion, as well as observation of the intercostal tube to detect complications. Among the ultimate diagnoses were metastatic adenocarcinoma, interstitial lung disease, and lymphangioleiomyomatosis.
"Thoracosopic lung biopsy by medical thoracoscopy is useful in the diagnosis of patient with diffuse pulmonary infiltrates of unknown etiology when lung biopsy is needed for an accurate diagnosis," Dr. Elnady concluded, noting that while the procedure does carry a risk of certain non–life-threatening complications, these can be minimized with good patient selection.
Commenting on the findings, Dr. Muthiah P. Muthiah, who moderated the session, said this novel approach to obtaining a lung biopsy is of interest, but also "something we still have to get comfortable with."
"I’m not ready to do this yet, but this is something to consider ... you will want to certainly do this with a surgeon’s back-up in your institution," said Dr. Muthiah of the University of Tennessee Health Science Center, Memphis.
Neither Dr. Muthiah nor Dr. Elnady had disclosures to report.
ATLANTA – Medical thoracoscopy is safe and feasible for performing lung biopsy in patients with diffuse parenchymal lung disease of unknown etiology on high-resolution computed tomography. And the approach could serve as an alternative to surgical biopsy in some patients, findings from a prospective study suggest.
In 10 patients who underwent medical thoracoscopic lung biopsies as part of the study, good biopsy specimens, with an average size of 0.5 x 0.4 cm were obtained, Dr. Mohamed Elnady said at the annual meeting of the American College of Chest Physicians.
Complications with this advanced technique included persistent air leak for 5-7 days in two patients, pneumothorax after removal of the intercostals tube in two patients, pain in six patients, and minor bleeding in one patient. The air leaks resolved spontaneously, and the pneumothoraces resolved with administration of high flow oxygen, said Dr. Elnady of Cairo (Egypt) University Hospitals.
The mean duration of intercostal tube placement was 3.1 days, with a range of 1-7 days; no infection, respiratory failure requiring intensive care unit admission, or mortality occurred within 30 days after the procedure, he noted.
Patients in the study included four women and six men with a mean age of 42 years. The lung biopsies obtained via medical thoracoscopy were sent for histopathologic examination, and patients underwent follow-up by chest x-ray for confirmation of lung expansion, as well as observation of the intercostal tube to detect complications. Among the ultimate diagnoses were metastatic adenocarcinoma, interstitial lung disease, and lymphangioleiomyomatosis.
"Thoracosopic lung biopsy by medical thoracoscopy is useful in the diagnosis of patient with diffuse pulmonary infiltrates of unknown etiology when lung biopsy is needed for an accurate diagnosis," Dr. Elnady concluded, noting that while the procedure does carry a risk of certain non–life-threatening complications, these can be minimized with good patient selection.
Commenting on the findings, Dr. Muthiah P. Muthiah, who moderated the session, said this novel approach to obtaining a lung biopsy is of interest, but also "something we still have to get comfortable with."
"I’m not ready to do this yet, but this is something to consider ... you will want to certainly do this with a surgeon’s back-up in your institution," said Dr. Muthiah of the University of Tennessee Health Science Center, Memphis.
Neither Dr. Muthiah nor Dr. Elnady had disclosures to report.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Good biopsy specimens (average size of 0.5 x 0.4 cm) were obtained and no life-threatening complications occurred in patients who underwent medical thorascopic lung biopsies.
Data Source: A prospective study in 10 patients was conducted.
Disclosures: Neither Dr. Muthiah nor Dr. Elnady had disclosures to report.
Pertussis Immunity Drop Linked to Whole Cell Vaccine Withdrawal
SAN DIEGO – The declining herd immunity to pertussis seen in the United States community may be related to withdrawal of the whole cell vaccine from the market about a decade ago, a study of more than 450,000 vaccinated patients from Kaiser Permanente Medical Center has shown.
Compared with their peers who had received at least one dose of whole cell vaccine, patients who had received only acellular vaccine had at least a tripling of the risk of acquiring the disease, lead author Maxwell Witt reported at IDWeek. The association was still present but weaker among patients who had received a total of six doses versus five.
"Acellular pertussis vaccine offered significantly less protection when compared with the whole cell vaccine," commented Mr. Witt of Kaiser Permanente in San Rafael, Calif. "The risk of pertussis was mitigated, but not eliminated, by a sixth dose of pertussis vaccine, the Tdap [tetanus, diphtheria, and acellular pertussis] vaccine.
"The current generation of children is the first to have been vaccinated solely with the acellular pertussis vaccine," Mr. Witt said. "Our findings would predict a significant population of underprotected children in this group." Recent outbreaks of pertussis in the United States "had peak attack rates among those who are exactly in the same age group," he noted.
"The waning immunity associated with these outbreaks is clearly a call for development of more effective and durable pertussis vaccines," Mr. Witt said. "In the shorter term, strategies to prevent these outbreaks of pertussis could include either earlier or additional booster doses, and targeted vaccination programs to address insufficient immunity in outbreak situations."
The field of pertussis vaccination has undergone transition, with the introduction of the acellular vaccine in 1991 and retirement of the whole cell vaccine in 2001. "In 2010, we saw the largest epidemic of Bordatella pertussis in California in more than 50 years, and that epidemic subsequently spread across the United States," he said at IDWeek, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In a previous study, the investigators noted waning pertussis immunity among preadolescents (with a peak attack rate among 8- to 12-year-olds) but also robust immunity among adolescents (with a sharply lower attack rate among 13-year-olds) (Clin. Infect. Dis. 2010;54:1730-35), suggesting a possible role for the vaccine transition.

In the new study, the investigators used electronic health records to identify vaccines administered and cases of laboratory-confirmed pertussis among Kaiser Permanente members aged 8-20 years in Northern California.
This age range was chosen to include patients who were old enough to have received whole cell vaccine and young enough to have received acellular vaccine, explained Mr. Witt. The search identified 465,059 patients, among whom there were 1,424 cases of pertussis.
A total of 253,005 patients had received all of their vaccine doses at Kaiser Permanente. Analyses restricted to this group showed that among patients who had received five total doses of vaccine, the pertussis attack rate was 786/100,000 for those who had received only acellular vaccine, compared with 92/100,000 for those who had received at least one dose of whole cell vaccine. The difference corresponded to an 8.57-fold higher risk for the former group (P less than .0001).
Similarly, among patients who had received six total doses of vaccine, the attack rate was 378 vs. 106/100,000 for those who received only acellular vaccine compared with those who had received at least one dose of whole cell vaccine. Here, the difference amounted to a smaller but still significant 3.55-fold higher risk.
The study findings were essentially the same when analyses were based on all patients, including those who had received at least some doses of vaccine outside of Kaiser Permanente, with respective 6.76- and 2.46-fold higher risks for patients given only acellular vaccine, depending on the total number of doses.
Mr. Witt disclosed no relevant financial conflicts.
SAN DIEGO – The declining herd immunity to pertussis seen in the United States community may be related to withdrawal of the whole cell vaccine from the market about a decade ago, a study of more than 450,000 vaccinated patients from Kaiser Permanente Medical Center has shown.
Compared with their peers who had received at least one dose of whole cell vaccine, patients who had received only acellular vaccine had at least a tripling of the risk of acquiring the disease, lead author Maxwell Witt reported at IDWeek. The association was still present but weaker among patients who had received a total of six doses versus five.
"Acellular pertussis vaccine offered significantly less protection when compared with the whole cell vaccine," commented Mr. Witt of Kaiser Permanente in San Rafael, Calif. "The risk of pertussis was mitigated, but not eliminated, by a sixth dose of pertussis vaccine, the Tdap [tetanus, diphtheria, and acellular pertussis] vaccine.
"The current generation of children is the first to have been vaccinated solely with the acellular pertussis vaccine," Mr. Witt said. "Our findings would predict a significant population of underprotected children in this group." Recent outbreaks of pertussis in the United States "had peak attack rates among those who are exactly in the same age group," he noted.
"The waning immunity associated with these outbreaks is clearly a call for development of more effective and durable pertussis vaccines," Mr. Witt said. "In the shorter term, strategies to prevent these outbreaks of pertussis could include either earlier or additional booster doses, and targeted vaccination programs to address insufficient immunity in outbreak situations."
The field of pertussis vaccination has undergone transition, with the introduction of the acellular vaccine in 1991 and retirement of the whole cell vaccine in 2001. "In 2010, we saw the largest epidemic of Bordatella pertussis in California in more than 50 years, and that epidemic subsequently spread across the United States," he said at IDWeek, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In a previous study, the investigators noted waning pertussis immunity among preadolescents (with a peak attack rate among 8- to 12-year-olds) but also robust immunity among adolescents (with a sharply lower attack rate among 13-year-olds) (Clin. Infect. Dis. 2010;54:1730-35), suggesting a possible role for the vaccine transition.
In the new study, the investigators used electronic health records to identify vaccines administered and cases of laboratory-confirmed pertussis among Kaiser Permanente members aged 8-20 years in Northern California.
This age range was chosen to include patients who were old enough to have received whole cell vaccine and young enough to have received acellular vaccine, explained Mr. Witt. The search identified 465,059 patients, among whom there were 1,424 cases of pertussis.
A total of 253,005 patients had received all of their vaccine doses at Kaiser Permanente. Analyses restricted to this group showed that among patients who had received five total doses of vaccine, the pertussis attack rate was 786/100,000 for those who had received only acellular vaccine, compared with 92/100,000 for those who had received at least one dose of whole cell vaccine. The difference corresponded to an 8.57-fold higher risk for the former group (P less than .0001).
Similarly, among patients who had received six total doses of vaccine, the attack rate was 378 vs. 106/100,000 for those who received only acellular vaccine compared with those who had received at least one dose of whole cell vaccine. Here, the difference amounted to a smaller but still significant 3.55-fold higher risk.
The study findings were essentially the same when analyses were based on all patients, including those who had received at least some doses of vaccine outside of Kaiser Permanente, with respective 6.76- and 2.46-fold higher risks for patients given only acellular vaccine, depending on the total number of doses.
Mr. Witt disclosed no relevant financial conflicts.
SAN DIEGO – The declining herd immunity to pertussis seen in the United States community may be related to withdrawal of the whole cell vaccine from the market about a decade ago, a study of more than 450,000 vaccinated patients from Kaiser Permanente Medical Center has shown.
Compared with their peers who had received at least one dose of whole cell vaccine, patients who had received only acellular vaccine had at least a tripling of the risk of acquiring the disease, lead author Maxwell Witt reported at IDWeek. The association was still present but weaker among patients who had received a total of six doses versus five.
"Acellular pertussis vaccine offered significantly less protection when compared with the whole cell vaccine," commented Mr. Witt of Kaiser Permanente in San Rafael, Calif. "The risk of pertussis was mitigated, but not eliminated, by a sixth dose of pertussis vaccine, the Tdap [tetanus, diphtheria, and acellular pertussis] vaccine.
"The current generation of children is the first to have been vaccinated solely with the acellular pertussis vaccine," Mr. Witt said. "Our findings would predict a significant population of underprotected children in this group." Recent outbreaks of pertussis in the United States "had peak attack rates among those who are exactly in the same age group," he noted.
"The waning immunity associated with these outbreaks is clearly a call for development of more effective and durable pertussis vaccines," Mr. Witt said. "In the shorter term, strategies to prevent these outbreaks of pertussis could include either earlier or additional booster doses, and targeted vaccination programs to address insufficient immunity in outbreak situations."
The field of pertussis vaccination has undergone transition, with the introduction of the acellular vaccine in 1991 and retirement of the whole cell vaccine in 2001. "In 2010, we saw the largest epidemic of Bordatella pertussis in California in more than 50 years, and that epidemic subsequently spread across the United States," he said at IDWeek, the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
In a previous study, the investigators noted waning pertussis immunity among preadolescents (with a peak attack rate among 8- to 12-year-olds) but also robust immunity among adolescents (with a sharply lower attack rate among 13-year-olds) (Clin. Infect. Dis. 2010;54:1730-35), suggesting a possible role for the vaccine transition.
In the new study, the investigators used electronic health records to identify vaccines administered and cases of laboratory-confirmed pertussis among Kaiser Permanente members aged 8-20 years in Northern California.
This age range was chosen to include patients who were old enough to have received whole cell vaccine and young enough to have received acellular vaccine, explained Mr. Witt. The search identified 465,059 patients, among whom there were 1,424 cases of pertussis.
A total of 253,005 patients had received all of their vaccine doses at Kaiser Permanente. Analyses restricted to this group showed that among patients who had received five total doses of vaccine, the pertussis attack rate was 786/100,000 for those who had received only acellular vaccine, compared with 92/100,000 for those who had received at least one dose of whole cell vaccine. The difference corresponded to an 8.57-fold higher risk for the former group (P less than .0001).
Similarly, among patients who had received six total doses of vaccine, the attack rate was 378 vs. 106/100,000 for those who received only acellular vaccine compared with those who had received at least one dose of whole cell vaccine. Here, the difference amounted to a smaller but still significant 3.55-fold higher risk.
The study findings were essentially the same when analyses were based on all patients, including those who had received at least some doses of vaccine outside of Kaiser Permanente, with respective 6.76- and 2.46-fold higher risks for patients given only acellular vaccine, depending on the total number of doses.
Mr. Witt disclosed no relevant financial conflicts.
AT IDWEEK
Major Finding: Compared with their peers who had received at least one dose of whole cell vaccine, patients who had received only acellular vaccine had a 3.55- to 8.57-fold higher risk of pertussis.
Data Source: A cross-sectional study of 465,059 vaccinated patients aged 8-20 years from a single health care system
Disclosures: Mr. Witt disclosed no relevant financial conflicts.

NIPPV Benefits Seen in Severe Stable COPD
ATLANTA – Long-term nocturnal use of noninvasive positive pressure ventilation significantly reduced the likelihood of intensive care unit admission in patients with severe stable chronic obstructive pulmonary disease, according to findings from a systematic review of 582 patients in 13 randomized, controlled clinical trials.
After 1 year, noninvasive positive pressure ventilation (NIPPV) was associated with a significant decrease in ICU admissions (odds ratio, 0.41) compared with standard medical therapy. Patients using NIPPV for more than 3 months also had improvements in oxygenation (mean difference of -2.43 mm Hg), reduction in PCO2 (mean difference, -2.96 mm Hg), and an improvement in 6-minute walk distance (mean difference 45.15 m), Dr. Monali Patil reported at the annual meeting of the American College of Chest Physicians.
A trend toward improved mortality at 1 year did not reach statistical significance, and no significant improvements in lung function were noted, said Dr. Patil of the University at Buffalo (N.Y.).
Dr. Patil selected the 13 trials from a review of more than 700 studies conducted between 1991 and 2011. The analysis included only randomized, controlled trials of COPD patients who had an FEV1 less than 50% of predicted and a PCO2 greater than 45 mm Hg and were receiving bilevel positive airway pressure (BIPAP). The patients in the studies were aged 18-75 years, and had no COPD exacerbations within 2 weeks prior to study enrollment.
The long-term use of NIPPV in patients with severe stable COPD has been controversial, but these findings demonstrate significant benefits.
"So NIPPV can be used as adjuvant treatment for management of severe stable COPD patients," she concluded.
Dr Patil reported having no financial disclosures.
ATLANTA – Long-term nocturnal use of noninvasive positive pressure ventilation significantly reduced the likelihood of intensive care unit admission in patients with severe stable chronic obstructive pulmonary disease, according to findings from a systematic review of 582 patients in 13 randomized, controlled clinical trials.
After 1 year, noninvasive positive pressure ventilation (NIPPV) was associated with a significant decrease in ICU admissions (odds ratio, 0.41) compared with standard medical therapy. Patients using NIPPV for more than 3 months also had improvements in oxygenation (mean difference of -2.43 mm Hg), reduction in PCO2 (mean difference, -2.96 mm Hg), and an improvement in 6-minute walk distance (mean difference 45.15 m), Dr. Monali Patil reported at the annual meeting of the American College of Chest Physicians.
A trend toward improved mortality at 1 year did not reach statistical significance, and no significant improvements in lung function were noted, said Dr. Patil of the University at Buffalo (N.Y.).
Dr. Patil selected the 13 trials from a review of more than 700 studies conducted between 1991 and 2011. The analysis included only randomized, controlled trials of COPD patients who had an FEV1 less than 50% of predicted and a PCO2 greater than 45 mm Hg and were receiving bilevel positive airway pressure (BIPAP). The patients in the studies were aged 18-75 years, and had no COPD exacerbations within 2 weeks prior to study enrollment.
The long-term use of NIPPV in patients with severe stable COPD has been controversial, but these findings demonstrate significant benefits.
"So NIPPV can be used as adjuvant treatment for management of severe stable COPD patients," she concluded.
Dr Patil reported having no financial disclosures.
ATLANTA – Long-term nocturnal use of noninvasive positive pressure ventilation significantly reduced the likelihood of intensive care unit admission in patients with severe stable chronic obstructive pulmonary disease, according to findings from a systematic review of 582 patients in 13 randomized, controlled clinical trials.
After 1 year, noninvasive positive pressure ventilation (NIPPV) was associated with a significant decrease in ICU admissions (odds ratio, 0.41) compared with standard medical therapy. Patients using NIPPV for more than 3 months also had improvements in oxygenation (mean difference of -2.43 mm Hg), reduction in PCO2 (mean difference, -2.96 mm Hg), and an improvement in 6-minute walk distance (mean difference 45.15 m), Dr. Monali Patil reported at the annual meeting of the American College of Chest Physicians.
A trend toward improved mortality at 1 year did not reach statistical significance, and no significant improvements in lung function were noted, said Dr. Patil of the University at Buffalo (N.Y.).
Dr. Patil selected the 13 trials from a review of more than 700 studies conducted between 1991 and 2011. The analysis included only randomized, controlled trials of COPD patients who had an FEV1 less than 50% of predicted and a PCO2 greater than 45 mm Hg and were receiving bilevel positive airway pressure (BIPAP). The patients in the studies were aged 18-75 years, and had no COPD exacerbations within 2 weeks prior to study enrollment.
The long-term use of NIPPV in patients with severe stable COPD has been controversial, but these findings demonstrate significant benefits.
"So NIPPV can be used as adjuvant treatment for management of severe stable COPD patients," she concluded.
Dr Patil reported having no financial disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Noninvasive positive pressure ventilation (NIPPV) was associated with a significant decrease in ICU admissions at 1 year (odds ratio, 0.41).
Data Source: Findings were based on a review of 582 patients in 13 randomized, controlled clinical trials.
Disclosures: Dr. Patil reported having no disclosures.
Aspirin Reduces Recurrence of Vascular Events and VTEs
A 100-mg daily dose of aspirin reduced by one-third the rate of recurrent major vascular events for patients who had one acute unprovoked venous thromboembolism and were switched from anticoagulant therapy to either aspirin or placebo after 3 months of anticoagulant therapy.*
Patients with one episode of unprovoked VTE often discontinue anticoagulant therapy due to inconvenience and the risk of bleeding, said Dr. Timothy A. Brighton of the University of Sydney, Australia, and his colleagues. For those patients, 100 mg of aspirin per day appears to be a safe alternative.
Dr. Brighton and his colleagues reported the findings based on combined data from the ASPIRE (Aspirin to Prevent Recurrent Venous Thromboembolism) study and the WARFASA (Warfarin and Aspirin) study. The findings of ASPIRE were simultaneously published in the New England Journal of Medicine and presented at the annual meeting of the American Heart Association in Los Angeles. The findings of WARFASA were previously published in the same journal.
ASPIRE examined the effect of a 100-mg daily dose of aspirin in patients who had a history of a first-ever unprovoked VTE and had completed initial anticoagulation therapy. The study population included 822 adults who were randomized to a placebo or aspirin at 56 sites in five countries from May 2003 and August 2011. Roughly half of the patients were men; 56% had a proximal deep-vein thrombosis as an index event; 29% had a pulmonary embolism as an index event, and 14% had both conditions as an index event (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMoa1210384]).
Overall, VTE recurred in 57 patients (14%) in the aspirin group, compared with 73 patients (18%) in the placebo group (rates of 5% and 7% per year, respectively, a nonsignificant difference).
However, the rates of two secondary composite outcomes were significantly reduced in patients who took aspirin compared with those on placebo, the researchers noted. The rate of a composite outcome including VTE, myocardial infarction, stroke, or cardiovascular death was reduced by 34% in aspirin patients (5% per year for aspirin vs. 8% per year for placebo).
The rate of a composite outcome including VTE, myocardial infarction, stroke, major bleeding, or death from any cause was reduce by 33% in aspirin patients (6% per year for aspirin vs. 9% per year for placebo).
No significant differences in serious adverse events or in the rates of major or clinically relevant nonmajor bleeding were observed between the aspirin and placebo groups, the researchers noted.
The findings were limited by the low number of patients in the study, however. The ASPIRE data alone were not adequately powered to show a significant reduction in the recurrence of VTE.
To address the issue, researchers combined the ASPIRE data with data from a similar population of 402 patients in the WARFASA (Warfarin and Aspirin) study (N. Engl. J. Med. 2012; 366:1959-67). In this multicenter, double-blind study, patients with first-ever unprovoked venous thromboembolism completed 6-18 months of oral anticoagulant treatment and were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years.
VTE recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 – 0.93). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups.
Using the combined data from both studies, the researchers found “a highly significant reduction of 32% in the rate of recurrence of venous thromboembolism and a reduction of 34% in the rate of major vascular events with no excess of bleeding.”
Therefore, the combined results of the two studies support the use of low-dose aspirin to prevent both recurrent VTE and major vascular events in patients who have had a first episode of unprovoked VTE, the researchers said.
Lead author Dr. Brighton disclosed serving as a consultant for Pfizer, GlaxoSmithKline, and other companies. The study was supported by grants from the National Health and Medical Research Council (Australia), the Health Research Council (New Zealand), the National Heart Foundation of Australia, Bayer HealthCare (Germany), and the Australasian Society of Haematology and Thrombosis
* This story was updated on 11/7/12.
Anticoagulants may trump aspirin in efficacy for preventing VTE after surgery, but the findings from the ASPIRE and WARFASA studies support a clinical role for aspirin in preventing VTE, Dr. Theodore Warkentin wrote.
Dr. Warkentin noted the long-term risk of a recurrence of VTE in patients who have had a first unprovoked VTE.
“Could aspirin represent a reasonable intermediate option between the extremes of indefinite anticoagulation and no ongoing anticoagulation, particularly from the additional perspective of concomitant prevention of arterial thrombosis?” he asked.
The combined data from the WARFASA and ASPIRE studies suggest that aspirin has the double benefit of significantly reducing not only the rate of VTE recurrence, but also the rate of a composite of major vascular events, Dr. Warkentin said.
On the basis of the findings, Dr. Warkentin explained how aspirin could fit into clinical practice.
“Before physicians consider prescribing aspirin for patients who have had acute unprovoked venous thromboembolism, it is important that they treat the patients with effective anticoagulation for at least 3 months, to avoid the high risk of early recurrence,” he said.
“For patients who then wish to stop anticoagulation, a switch to aspirin at a dose of 100 mg daily will reduce by one-third the risk of recurrent venous thromboembolism, as well as of arterial cardiovascular events, and may also attenuate the early burst of thrombosis recurrence after cessation of oral anticoagulation,” he said.
Aspirin has the added benefits of being cost-effective, requiring no monitoring, and not accumulating in patients with renal insufficiency, Dr. Warkentin added.
Dr. Warkentin is a professor of pathology and molecular medicine at McMaster University in Hamilton, Ont. He also has served as a consultant for GlaxoSmithKline and as a speaker for Pfizer Canada, and he has received grants from Bayer. These remarks were taken from his accompanying editorial (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMe1211480]).
Anticoagulants may trump aspirin in efficacy for preventing VTE after surgery, but the findings from the ASPIRE and WARFASA studies support a clinical role for aspirin in preventing VTE, Dr. Theodore Warkentin wrote.
Dr. Warkentin noted the long-term risk of a recurrence of VTE in patients who have had a first unprovoked VTE.
“Could aspirin represent a reasonable intermediate option between the extremes of indefinite anticoagulation and no ongoing anticoagulation, particularly from the additional perspective of concomitant prevention of arterial thrombosis?” he asked.
The combined data from the WARFASA and ASPIRE studies suggest that aspirin has the double benefit of significantly reducing not only the rate of VTE recurrence, but also the rate of a composite of major vascular events, Dr. Warkentin said.
On the basis of the findings, Dr. Warkentin explained how aspirin could fit into clinical practice.
“Before physicians consider prescribing aspirin for patients who have had acute unprovoked venous thromboembolism, it is important that they treat the patients with effective anticoagulation for at least 3 months, to avoid the high risk of early recurrence,” he said.
“For patients who then wish to stop anticoagulation, a switch to aspirin at a dose of 100 mg daily will reduce by one-third the risk of recurrent venous thromboembolism, as well as of arterial cardiovascular events, and may also attenuate the early burst of thrombosis recurrence after cessation of oral anticoagulation,” he said.
Aspirin has the added benefits of being cost-effective, requiring no monitoring, and not accumulating in patients with renal insufficiency, Dr. Warkentin added.
Dr. Warkentin is a professor of pathology and molecular medicine at McMaster University in Hamilton, Ont. He also has served as a consultant for GlaxoSmithKline and as a speaker for Pfizer Canada, and he has received grants from Bayer. These remarks were taken from his accompanying editorial (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMe1211480]).
Anticoagulants may trump aspirin in efficacy for preventing VTE after surgery, but the findings from the ASPIRE and WARFASA studies support a clinical role for aspirin in preventing VTE, Dr. Theodore Warkentin wrote.
Dr. Warkentin noted the long-term risk of a recurrence of VTE in patients who have had a first unprovoked VTE.
“Could aspirin represent a reasonable intermediate option between the extremes of indefinite anticoagulation and no ongoing anticoagulation, particularly from the additional perspective of concomitant prevention of arterial thrombosis?” he asked.
The combined data from the WARFASA and ASPIRE studies suggest that aspirin has the double benefit of significantly reducing not only the rate of VTE recurrence, but also the rate of a composite of major vascular events, Dr. Warkentin said.
On the basis of the findings, Dr. Warkentin explained how aspirin could fit into clinical practice.
“Before physicians consider prescribing aspirin for patients who have had acute unprovoked venous thromboembolism, it is important that they treat the patients with effective anticoagulation for at least 3 months, to avoid the high risk of early recurrence,” he said.
“For patients who then wish to stop anticoagulation, a switch to aspirin at a dose of 100 mg daily will reduce by one-third the risk of recurrent venous thromboembolism, as well as of arterial cardiovascular events, and may also attenuate the early burst of thrombosis recurrence after cessation of oral anticoagulation,” he said.
Aspirin has the added benefits of being cost-effective, requiring no monitoring, and not accumulating in patients with renal insufficiency, Dr. Warkentin added.
Dr. Warkentin is a professor of pathology and molecular medicine at McMaster University in Hamilton, Ont. He also has served as a consultant for GlaxoSmithKline and as a speaker for Pfizer Canada, and he has received grants from Bayer. These remarks were taken from his accompanying editorial (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMe1211480]).
A 100-mg daily dose of aspirin reduced by one-third the rate of recurrent major vascular events for patients who had one acute unprovoked venous thromboembolism and were switched from anticoagulant therapy to either aspirin or placebo after 3 months of anticoagulant therapy.*
Patients with one episode of unprovoked VTE often discontinue anticoagulant therapy due to inconvenience and the risk of bleeding, said Dr. Timothy A. Brighton of the University of Sydney, Australia, and his colleagues. For those patients, 100 mg of aspirin per day appears to be a safe alternative.
Dr. Brighton and his colleagues reported the findings based on combined data from the ASPIRE (Aspirin to Prevent Recurrent Venous Thromboembolism) study and the WARFASA (Warfarin and Aspirin) study. The findings of ASPIRE were simultaneously published in the New England Journal of Medicine and presented at the annual meeting of the American Heart Association in Los Angeles. The findings of WARFASA were previously published in the same journal.
ASPIRE examined the effect of a 100-mg daily dose of aspirin in patients who had a history of a first-ever unprovoked VTE and had completed initial anticoagulation therapy. The study population included 822 adults who were randomized to a placebo or aspirin at 56 sites in five countries from May 2003 and August 2011. Roughly half of the patients were men; 56% had a proximal deep-vein thrombosis as an index event; 29% had a pulmonary embolism as an index event, and 14% had both conditions as an index event (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMoa1210384]).
Overall, VTE recurred in 57 patients (14%) in the aspirin group, compared with 73 patients (18%) in the placebo group (rates of 5% and 7% per year, respectively, a nonsignificant difference).
However, the rates of two secondary composite outcomes were significantly reduced in patients who took aspirin compared with those on placebo, the researchers noted. The rate of a composite outcome including VTE, myocardial infarction, stroke, or cardiovascular death was reduced by 34% in aspirin patients (5% per year for aspirin vs. 8% per year for placebo).
The rate of a composite outcome including VTE, myocardial infarction, stroke, major bleeding, or death from any cause was reduce by 33% in aspirin patients (6% per year for aspirin vs. 9% per year for placebo).
No significant differences in serious adverse events or in the rates of major or clinically relevant nonmajor bleeding were observed between the aspirin and placebo groups, the researchers noted.
The findings were limited by the low number of patients in the study, however. The ASPIRE data alone were not adequately powered to show a significant reduction in the recurrence of VTE.
To address the issue, researchers combined the ASPIRE data with data from a similar population of 402 patients in the WARFASA (Warfarin and Aspirin) study (N. Engl. J. Med. 2012; 366:1959-67). In this multicenter, double-blind study, patients with first-ever unprovoked venous thromboembolism completed 6-18 months of oral anticoagulant treatment and were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years.
VTE recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 – 0.93). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups.
Using the combined data from both studies, the researchers found “a highly significant reduction of 32% in the rate of recurrence of venous thromboembolism and a reduction of 34% in the rate of major vascular events with no excess of bleeding.”
Therefore, the combined results of the two studies support the use of low-dose aspirin to prevent both recurrent VTE and major vascular events in patients who have had a first episode of unprovoked VTE, the researchers said.
Lead author Dr. Brighton disclosed serving as a consultant for Pfizer, GlaxoSmithKline, and other companies. The study was supported by grants from the National Health and Medical Research Council (Australia), the Health Research Council (New Zealand), the National Heart Foundation of Australia, Bayer HealthCare (Germany), and the Australasian Society of Haematology and Thrombosis
* This story was updated on 11/7/12.
A 100-mg daily dose of aspirin reduced by one-third the rate of recurrent major vascular events for patients who had one acute unprovoked venous thromboembolism and were switched from anticoagulant therapy to either aspirin or placebo after 3 months of anticoagulant therapy.*
Patients with one episode of unprovoked VTE often discontinue anticoagulant therapy due to inconvenience and the risk of bleeding, said Dr. Timothy A. Brighton of the University of Sydney, Australia, and his colleagues. For those patients, 100 mg of aspirin per day appears to be a safe alternative.
Dr. Brighton and his colleagues reported the findings based on combined data from the ASPIRE (Aspirin to Prevent Recurrent Venous Thromboembolism) study and the WARFASA (Warfarin and Aspirin) study. The findings of ASPIRE were simultaneously published in the New England Journal of Medicine and presented at the annual meeting of the American Heart Association in Los Angeles. The findings of WARFASA were previously published in the same journal.
ASPIRE examined the effect of a 100-mg daily dose of aspirin in patients who had a history of a first-ever unprovoked VTE and had completed initial anticoagulation therapy. The study population included 822 adults who were randomized to a placebo or aspirin at 56 sites in five countries from May 2003 and August 2011. Roughly half of the patients were men; 56% had a proximal deep-vein thrombosis as an index event; 29% had a pulmonary embolism as an index event, and 14% had both conditions as an index event (N. Engl. J. Med. 2012 Nov. 4 [doi: 10.1056/NEJMoa1210384]).
Overall, VTE recurred in 57 patients (14%) in the aspirin group, compared with 73 patients (18%) in the placebo group (rates of 5% and 7% per year, respectively, a nonsignificant difference).
However, the rates of two secondary composite outcomes were significantly reduced in patients who took aspirin compared with those on placebo, the researchers noted. The rate of a composite outcome including VTE, myocardial infarction, stroke, or cardiovascular death was reduced by 34% in aspirin patients (5% per year for aspirin vs. 8% per year for placebo).
The rate of a composite outcome including VTE, myocardial infarction, stroke, major bleeding, or death from any cause was reduce by 33% in aspirin patients (6% per year for aspirin vs. 9% per year for placebo).
No significant differences in serious adverse events or in the rates of major or clinically relevant nonmajor bleeding were observed between the aspirin and placebo groups, the researchers noted.
The findings were limited by the low number of patients in the study, however. The ASPIRE data alone were not adequately powered to show a significant reduction in the recurrence of VTE.
To address the issue, researchers combined the ASPIRE data with data from a similar population of 402 patients in the WARFASA (Warfarin and Aspirin) study (N. Engl. J. Med. 2012; 366:1959-67). In this multicenter, double-blind study, patients with first-ever unprovoked venous thromboembolism completed 6-18 months of oral anticoagulant treatment and were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years.
VTE recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 – 0.93). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups.
Using the combined data from both studies, the researchers found “a highly significant reduction of 32% in the rate of recurrence of venous thromboembolism and a reduction of 34% in the rate of major vascular events with no excess of bleeding.”
Therefore, the combined results of the two studies support the use of low-dose aspirin to prevent both recurrent VTE and major vascular events in patients who have had a first episode of unprovoked VTE, the researchers said.
Lead author Dr. Brighton disclosed serving as a consultant for Pfizer, GlaxoSmithKline, and other companies. The study was supported by grants from the National Health and Medical Research Council (Australia), the Health Research Council (New Zealand), the National Heart Foundation of Australia, Bayer HealthCare (Germany), and the Australasian Society of Haematology and Thrombosis
* This story was updated on 11/7/12.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: The combined results of the ASPIRE and WARFASA trials showed significant reductions of 32% in the rate of recurrence of venous thromboembolism and 34% in the rate of major vascular events among patients given 100 mg of aspirin daily compared with a placebo.
Data Source: The data come from 822 adults in the ASPIRE trial and 402 adults in the WARFASA trial.
Disclosures: Dr. Brighton disclosed serving as a consultant for Pfizer, GlaxoSmithKline, and other companies. The study was supported by grants from the National Health and Medical Research Council (Australia), the Health Research Council (New Zealand), the National Heart Foundation of Australia, Bayer HealthCare (Germany), and the Australasian Society of Haematology and Thrombosis. Dr. Warkentin has served as a consultant for GlaxoSmithKline and as a speaker for Pfizer Canada, and he has received grants from Bayer.

Macitentan Promising for Long-Term Outcomes in PAH
ATLANTA – Macitentan, a novel dual endothelin receptor antagonist with enhanced tissue penetration, significantly improves morbidity and mortality in patients with pulmonary arterial hypertension, according to findings from an industry-sponsored, randomized controlled phase III SERAPHIN study.
Macitentan treatment reduced the risk of occurrence of combined morbidity and mortality events by 30% in 250 patients randomized to receive 3 mg once daily and by 45% in 242 patients randomized to receive 10 mg once daily, compared with 250 patients who received placebo, Dr. Lewis Rubin reported at the annual meeting of the American College of Chest Physicians.

The differences were highly significant for both macitentan doses, and the effect of treatment on this novel primary end point was observed irrespective of background therapy, which consisted mainly of phosphodiesterase type-5 (PDE-5) inhibitors.
Among patients using background therapy, risk was reduced by 17% and 38% for the 3 mg and 10 mg groups, respectively; in treatment-naive patients, the risk was reduced by 47% and 55% in the dosage groups, respectively, said Dr. Rubin of the University of California, San Diego.
The findings hold promise for improved long-term outcomes in patients with pulmonary arterial hypertension (PAH), Dr. Rubin said. "This primary morbidity/mortality end point captures clinically relevant events that reflect true disease progression," he noted, explaining that the end point included time to death, atrial septostomy, lung transplantation, initiation of intravenous/subcutaneous prostanoids, or worsening of PAH.
To meet the criteria for PAH worsening, participants had to experience a confirmed 15% or greater decrease in 6-minute walk distance and worsening of symptoms as defined by either a worsening in functional class, worsening symptoms of right heart failure, need for a new PAH treatment, or need for an intravenous diuretic. The majority of events contributing to achievement of the primary end point were associated with worsening of PAH, rather than death, he noted.
In addition to improvements with respect to the primary end point, macitentan treatment also was associated with improvement on the secondary end point of the composite of mortality or hospitalization due to PAH, with risk reduction of 33% and 50% in the 3-mg and 10-mg groups, respectively, compared with placebo, Dr. Rubin said.
Macitentan was well tolerated, with both the treatment group and the placebo group experiencing similar incidences of elevated liver aminotransferases and peripheral edema, although headache, nasopharyngitis, and anemia all occurred more frequently in the treatment groups.
Participants in the double-blind, event-driven SERAPHIN study (Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome) were individuals aged 12 years or older with PAH. Randomization began in May of 2008, and study end was predefined as the occurrence of 285 morbidity/mortality events, which occurred as of March 2012.
The findings are notable because existing PAH therapies, including bosentan and ambrisentan, have been approved based only on short-term trials with exercise capacity as the primary end point, and have potential for adverse events that can limit tolerability, Dr. Rubin said.
"So an endothelin receptor antagonist that has a better tolerability profile would be potentially desirable," he said.
Indeed, macitentan, which is a product of a tailored discovery program, has not only been shown to have enhanced tissue penetration and "superior in vivo efficacy in a number of animal models," but also to have no effect on bile salts. It, therefore, has diminished adverse effects on the rate of hepatic dysfunction that is seen, with varying degrees, as a manifestation of endothelin receptor antagonism, he explained.
"In addition, it has demonstrated unique sustained receptor binding, which also may be beneficial in long-term therapy," he said.
The SERAPHIN study was sponsored by Actelion, the maker of macitentan. Dr. Rubin disclosed that he has received payment for consulting and/or serving on speaker bureaus or advisory committees for Actelion, Pfizer, United Therapeutics, Lung LLC, Gilead, GlaxoSmithKline, Bayer, and GeNo.
ATLANTA – Macitentan, a novel dual endothelin receptor antagonist with enhanced tissue penetration, significantly improves morbidity and mortality in patients with pulmonary arterial hypertension, according to findings from an industry-sponsored, randomized controlled phase III SERAPHIN study.
Macitentan treatment reduced the risk of occurrence of combined morbidity and mortality events by 30% in 250 patients randomized to receive 3 mg once daily and by 45% in 242 patients randomized to receive 10 mg once daily, compared with 250 patients who received placebo, Dr. Lewis Rubin reported at the annual meeting of the American College of Chest Physicians.
The differences were highly significant for both macitentan doses, and the effect of treatment on this novel primary end point was observed irrespective of background therapy, which consisted mainly of phosphodiesterase type-5 (PDE-5) inhibitors.
Among patients using background therapy, risk was reduced by 17% and 38% for the 3 mg and 10 mg groups, respectively; in treatment-naive patients, the risk was reduced by 47% and 55% in the dosage groups, respectively, said Dr. Rubin of the University of California, San Diego.
The findings hold promise for improved long-term outcomes in patients with pulmonary arterial hypertension (PAH), Dr. Rubin said. "This primary morbidity/mortality end point captures clinically relevant events that reflect true disease progression," he noted, explaining that the end point included time to death, atrial septostomy, lung transplantation, initiation of intravenous/subcutaneous prostanoids, or worsening of PAH.
To meet the criteria for PAH worsening, participants had to experience a confirmed 15% or greater decrease in 6-minute walk distance and worsening of symptoms as defined by either a worsening in functional class, worsening symptoms of right heart failure, need for a new PAH treatment, or need for an intravenous diuretic. The majority of events contributing to achievement of the primary end point were associated with worsening of PAH, rather than death, he noted.
In addition to improvements with respect to the primary end point, macitentan treatment also was associated with improvement on the secondary end point of the composite of mortality or hospitalization due to PAH, with risk reduction of 33% and 50% in the 3-mg and 10-mg groups, respectively, compared with placebo, Dr. Rubin said.
Macitentan was well tolerated, with both the treatment group and the placebo group experiencing similar incidences of elevated liver aminotransferases and peripheral edema, although headache, nasopharyngitis, and anemia all occurred more frequently in the treatment groups.
Participants in the double-blind, event-driven SERAPHIN study (Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome) were individuals aged 12 years or older with PAH. Randomization began in May of 2008, and study end was predefined as the occurrence of 285 morbidity/mortality events, which occurred as of March 2012.
The findings are notable because existing PAH therapies, including bosentan and ambrisentan, have been approved based only on short-term trials with exercise capacity as the primary end point, and have potential for adverse events that can limit tolerability, Dr. Rubin said.
"So an endothelin receptor antagonist that has a better tolerability profile would be potentially desirable," he said.
Indeed, macitentan, which is a product of a tailored discovery program, has not only been shown to have enhanced tissue penetration and "superior in vivo efficacy in a number of animal models," but also to have no effect on bile salts. It, therefore, has diminished adverse effects on the rate of hepatic dysfunction that is seen, with varying degrees, as a manifestation of endothelin receptor antagonism, he explained.
"In addition, it has demonstrated unique sustained receptor binding, which also may be beneficial in long-term therapy," he said.
The SERAPHIN study was sponsored by Actelion, the maker of macitentan. Dr. Rubin disclosed that he has received payment for consulting and/or serving on speaker bureaus or advisory committees for Actelion, Pfizer, United Therapeutics, Lung LLC, Gilead, GlaxoSmithKline, Bayer, and GeNo.
ATLANTA – Macitentan, a novel dual endothelin receptor antagonist with enhanced tissue penetration, significantly improves morbidity and mortality in patients with pulmonary arterial hypertension, according to findings from an industry-sponsored, randomized controlled phase III SERAPHIN study.
Macitentan treatment reduced the risk of occurrence of combined morbidity and mortality events by 30% in 250 patients randomized to receive 3 mg once daily and by 45% in 242 patients randomized to receive 10 mg once daily, compared with 250 patients who received placebo, Dr. Lewis Rubin reported at the annual meeting of the American College of Chest Physicians.
The differences were highly significant for both macitentan doses, and the effect of treatment on this novel primary end point was observed irrespective of background therapy, which consisted mainly of phosphodiesterase type-5 (PDE-5) inhibitors.
Among patients using background therapy, risk was reduced by 17% and 38% for the 3 mg and 10 mg groups, respectively; in treatment-naive patients, the risk was reduced by 47% and 55% in the dosage groups, respectively, said Dr. Rubin of the University of California, San Diego.
The findings hold promise for improved long-term outcomes in patients with pulmonary arterial hypertension (PAH), Dr. Rubin said. "This primary morbidity/mortality end point captures clinically relevant events that reflect true disease progression," he noted, explaining that the end point included time to death, atrial septostomy, lung transplantation, initiation of intravenous/subcutaneous prostanoids, or worsening of PAH.
To meet the criteria for PAH worsening, participants had to experience a confirmed 15% or greater decrease in 6-minute walk distance and worsening of symptoms as defined by either a worsening in functional class, worsening symptoms of right heart failure, need for a new PAH treatment, or need for an intravenous diuretic. The majority of events contributing to achievement of the primary end point were associated with worsening of PAH, rather than death, he noted.
In addition to improvements with respect to the primary end point, macitentan treatment also was associated with improvement on the secondary end point of the composite of mortality or hospitalization due to PAH, with risk reduction of 33% and 50% in the 3-mg and 10-mg groups, respectively, compared with placebo, Dr. Rubin said.
Macitentan was well tolerated, with both the treatment group and the placebo group experiencing similar incidences of elevated liver aminotransferases and peripheral edema, although headache, nasopharyngitis, and anemia all occurred more frequently in the treatment groups.
Participants in the double-blind, event-driven SERAPHIN study (Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome) were individuals aged 12 years or older with PAH. Randomization began in May of 2008, and study end was predefined as the occurrence of 285 morbidity/mortality events, which occurred as of March 2012.
The findings are notable because existing PAH therapies, including bosentan and ambrisentan, have been approved based only on short-term trials with exercise capacity as the primary end point, and have potential for adverse events that can limit tolerability, Dr. Rubin said.
"So an endothelin receptor antagonist that has a better tolerability profile would be potentially desirable," he said.
Indeed, macitentan, which is a product of a tailored discovery program, has not only been shown to have enhanced tissue penetration and "superior in vivo efficacy in a number of animal models," but also to have no effect on bile salts. It, therefore, has diminished adverse effects on the rate of hepatic dysfunction that is seen, with varying degrees, as a manifestation of endothelin receptor antagonism, he explained.
"In addition, it has demonstrated unique sustained receptor binding, which also may be beneficial in long-term therapy," he said.
The SERAPHIN study was sponsored by Actelion, the maker of macitentan. Dr. Rubin disclosed that he has received payment for consulting and/or serving on speaker bureaus or advisory committees for Actelion, Pfizer, United Therapeutics, Lung LLC, Gilead, GlaxoSmithKline, Bayer, and GeNo.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Macitentan treatment reduced the risk of morbidity and mortality by 30% in patients who received 3 mg once daily and by 45% in those who received 10 mg once daily, compared patients who received placebo.
Data Source: The randomized controlled phase III SERAPHIN study included 250 and 242 patients in the 3-mg and 10-mg treatment groups, respectively, and 250 patients in the placebo group.
Disclosures: The SERAPHIN study was sponsored by Actelion, the maker of macitentan. Dr. Rubin has received payment for consulting and/or serving on speaker bureaus or advisory committees for Actelion, Pfizer, United Therapeutics, Lung LLC, Gilead, GlaxoSmithKline, Bayer, and GeNo.

New Gene-Expression Test Improves Diagnostic Yield of Bronchoscopy
ATLANTA – The combined use of a novel bronchial airway gene-expression test and bronchoscopy improves the ability to rule out lung cancer in patients with benign disease, compared with bronchoscopy alone, according to findings from the prospective case-controlled AEGIS-1 trial.
Because bronchoscopy, which plays a central role in lung cancer diagnosis, has varying diagnostic yield based on factors such as the size and location of the lesion, the method used to collect cells, and pathological processing methods, the findings suggest that the test (BronchoGen) could minimize the need for additional invasive procedures in these patients, Duncan Whitney, Ph.D., said at the annual meeting of the American College of Chest Physicians.
The AEGIS-1 (Airway Epithelium Gene Expression in the Diagnosis of Lung Cancer 1) trial included more than 700 current or former smokers undergoing bronchoscopy for suspicion of lung cancer. It was designed to evaluate the diagnostic accuracy of the genomic test, which detects gene expression of cytologically normal bronchial airway epithelial cells.
The investigators collected mainstem bronchial airway brushings from 330 patients, including 240 with confirmed primary lung cancer and 90 controls, and performed microarray analysis. The sample set was then split into an independent training sample of 220 cases and a test set of 110 cases, and the gene-expression prediction model was optimized.
Next, reverse transcription polymerase chain reaction (RT-PCR) assays were developed for candidate biomarker genes, and a multivariate test algorithm was reoptimized using the RT-PCR data generated by a reanalysis of 153 of the samples from cancer patients and 64 of the samples from controls, explained Dr. Whitney.
The test, which ultimately focused on 30 genes, yielded a sensitivity of 77%, compared with 74% for bronchoscopy alone. The combined use of the test and bronchoscopy yielded a sensitivity of 96% and a specificity of 73%.
The negative predictive value of the combined test also was better than that of bronchoscopy alone (0.85 vs. 0.65, respectively), said Dr. Whitney.
"So in essence, we’re reducing the false negative rate from 26% down to 4%," he said.
The BronchoGen test was developed based on the airway "field of injury" principle, which refers to the common molecular response that occurs throughout the respiratory tract in current and former smokers with lung cancer, Dr. Whitney explained.
These changes are detected in a gene-expression signature from normal airway cells, even decades after smoking cessation, he noted.
Despite tremendous work done in this area, which has dramatically improved the diagnostic yield and sensitivity of bronchoscopy in the past few years, the procedure is either inconclusive or not diagnostic in up to 50% of cases, he said.
Thus, a "fairly large need" exists in the medical community, given that about 300,000 bronchoscopy procedures are performed each year for suspicion of lung cancer, he added.
Complete results from AEGIS-1, as well as clinical validation of the BronchoGen test, are expected to be released later this year. An additional 1,300 patients have been enrolled in the ongoing AEGIS-II trial.
Allegro Diagnostics, which developed the BronchoGen test, reports that it plans to commercialize it for use with bronchoscopy beginning in 2013.
This study was sponsored by Allegro Diagnostics. Dr. Whitney is an employee of the company, and had no other disclosures to report.
ATLANTA – The combined use of a novel bronchial airway gene-expression test and bronchoscopy improves the ability to rule out lung cancer in patients with benign disease, compared with bronchoscopy alone, according to findings from the prospective case-controlled AEGIS-1 trial.
Because bronchoscopy, which plays a central role in lung cancer diagnosis, has varying diagnostic yield based on factors such as the size and location of the lesion, the method used to collect cells, and pathological processing methods, the findings suggest that the test (BronchoGen) could minimize the need for additional invasive procedures in these patients, Duncan Whitney, Ph.D., said at the annual meeting of the American College of Chest Physicians.
The AEGIS-1 (Airway Epithelium Gene Expression in the Diagnosis of Lung Cancer 1) trial included more than 700 current or former smokers undergoing bronchoscopy for suspicion of lung cancer. It was designed to evaluate the diagnostic accuracy of the genomic test, which detects gene expression of cytologically normal bronchial airway epithelial cells.
The investigators collected mainstem bronchial airway brushings from 330 patients, including 240 with confirmed primary lung cancer and 90 controls, and performed microarray analysis. The sample set was then split into an independent training sample of 220 cases and a test set of 110 cases, and the gene-expression prediction model was optimized.
Next, reverse transcription polymerase chain reaction (RT-PCR) assays were developed for candidate biomarker genes, and a multivariate test algorithm was reoptimized using the RT-PCR data generated by a reanalysis of 153 of the samples from cancer patients and 64 of the samples from controls, explained Dr. Whitney.
The test, which ultimately focused on 30 genes, yielded a sensitivity of 77%, compared with 74% for bronchoscopy alone. The combined use of the test and bronchoscopy yielded a sensitivity of 96% and a specificity of 73%.
The negative predictive value of the combined test also was better than that of bronchoscopy alone (0.85 vs. 0.65, respectively), said Dr. Whitney.
"So in essence, we’re reducing the false negative rate from 26% down to 4%," he said.
The BronchoGen test was developed based on the airway "field of injury" principle, which refers to the common molecular response that occurs throughout the respiratory tract in current and former smokers with lung cancer, Dr. Whitney explained.
These changes are detected in a gene-expression signature from normal airway cells, even decades after smoking cessation, he noted.
Despite tremendous work done in this area, which has dramatically improved the diagnostic yield and sensitivity of bronchoscopy in the past few years, the procedure is either inconclusive or not diagnostic in up to 50% of cases, he said.
Thus, a "fairly large need" exists in the medical community, given that about 300,000 bronchoscopy procedures are performed each year for suspicion of lung cancer, he added.
Complete results from AEGIS-1, as well as clinical validation of the BronchoGen test, are expected to be released later this year. An additional 1,300 patients have been enrolled in the ongoing AEGIS-II trial.
Allegro Diagnostics, which developed the BronchoGen test, reports that it plans to commercialize it for use with bronchoscopy beginning in 2013.
This study was sponsored by Allegro Diagnostics. Dr. Whitney is an employee of the company, and had no other disclosures to report.
ATLANTA – The combined use of a novel bronchial airway gene-expression test and bronchoscopy improves the ability to rule out lung cancer in patients with benign disease, compared with bronchoscopy alone, according to findings from the prospective case-controlled AEGIS-1 trial.
Because bronchoscopy, which plays a central role in lung cancer diagnosis, has varying diagnostic yield based on factors such as the size and location of the lesion, the method used to collect cells, and pathological processing methods, the findings suggest that the test (BronchoGen) could minimize the need for additional invasive procedures in these patients, Duncan Whitney, Ph.D., said at the annual meeting of the American College of Chest Physicians.
The AEGIS-1 (Airway Epithelium Gene Expression in the Diagnosis of Lung Cancer 1) trial included more than 700 current or former smokers undergoing bronchoscopy for suspicion of lung cancer. It was designed to evaluate the diagnostic accuracy of the genomic test, which detects gene expression of cytologically normal bronchial airway epithelial cells.
The investigators collected mainstem bronchial airway brushings from 330 patients, including 240 with confirmed primary lung cancer and 90 controls, and performed microarray analysis. The sample set was then split into an independent training sample of 220 cases and a test set of 110 cases, and the gene-expression prediction model was optimized.
Next, reverse transcription polymerase chain reaction (RT-PCR) assays were developed for candidate biomarker genes, and a multivariate test algorithm was reoptimized using the RT-PCR data generated by a reanalysis of 153 of the samples from cancer patients and 64 of the samples from controls, explained Dr. Whitney.
The test, which ultimately focused on 30 genes, yielded a sensitivity of 77%, compared with 74% for bronchoscopy alone. The combined use of the test and bronchoscopy yielded a sensitivity of 96% and a specificity of 73%.
The negative predictive value of the combined test also was better than that of bronchoscopy alone (0.85 vs. 0.65, respectively), said Dr. Whitney.
"So in essence, we’re reducing the false negative rate from 26% down to 4%," he said.
The BronchoGen test was developed based on the airway "field of injury" principle, which refers to the common molecular response that occurs throughout the respiratory tract in current and former smokers with lung cancer, Dr. Whitney explained.
These changes are detected in a gene-expression signature from normal airway cells, even decades after smoking cessation, he noted.
Despite tremendous work done in this area, which has dramatically improved the diagnostic yield and sensitivity of bronchoscopy in the past few years, the procedure is either inconclusive or not diagnostic in up to 50% of cases, he said.
Thus, a "fairly large need" exists in the medical community, given that about 300,000 bronchoscopy procedures are performed each year for suspicion of lung cancer, he added.
Complete results from AEGIS-1, as well as clinical validation of the BronchoGen test, are expected to be released later this year. An additional 1,300 patients have been enrolled in the ongoing AEGIS-II trial.
Allegro Diagnostics, which developed the BronchoGen test, reports that it plans to commercialize it for use with bronchoscopy beginning in 2013.
This study was sponsored by Allegro Diagnostics. Dr. Whitney is an employee of the company, and had no other disclosures to report.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: The test, which focused on 30 genes, yielded a sensitivity of 77% for lung cancer, compared with 74% for bronchoscopy alone. The combined use of the test and bronchoscopy yielded a sensitivity of 96% and a specificity of 73%.
Data Source: This was a prospective case-controlled trial (AEGIS-1).
Disclosures: This study was sponsored by Allegro Diagnostics. Dr. Whitney is an employee of the company, and had no other disclosures to report.
Don't Quit on a Quitter: Helping Your Patient Stop Smoking
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
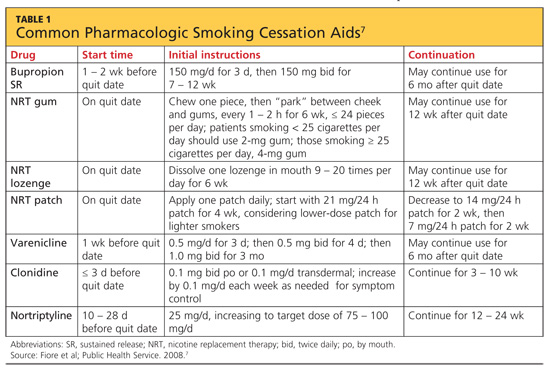
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
Although smoking prevalence among US adults declined by about 42% between 1965 and 2011, this reduction has slowed in recent years. According to 2010 figures from the CDC, 19.3% of US adults (nearly one in five) remain current smokers,1 despite all the evidence of negative effects that tobacco use and smoke exposure exert on good health.2 Each year, 443,000 premature deaths in the US are attributed to cigarette smoking.3
In the face of these discouraging data, and in ongoing efforts to minimize the deadly effects of cigarette smoking, the US Department of Health and Human Services’ program, Healthy People 2020,4 restated its 10-year goals pertaining to tobacco use as put forth in Healthy People 2010.5 These are to reduce the proportion of Americans who currently smoke to 12%, and to increase the proportion of current smokers who have attempted cessation to 80%.4
Though trained to encourage smoking cessation in their patients, health care providers often lack the knowledge, skills, or resources to support patients through the difficulties of discontinuing tobacco use. Whatever barriers clinicians may face in accessing smoking cessation services, the barriers faced by underserved patients are often greater.6 A heightened awareness of these barriers and improved understanding of common smoking cessation methods will help providers better support their patients who are trying to quit.
ASSESSING READINESS AND MOTIVATING PATIENTS
In 2008, the Public Health Service, US Department of Health and Human Services, updated its clinical practice guidelines for clinicians who manage tobacco-dependent patients.7 According to evidence from randomized controlled trials, even brief interventions on the health care provider’s part (such as raising the issue of smoking cessation at each patient visit to determine whether the patient is ready to quit) can prompt the patient to seriously consider smoking abstinence.3,8 Being asked repeatedly can advance a patient’s readiness, and any attempts patients make to quit must be robustly supported.9
The Public Health Service’s five A’s3,7 outline the recommended conversation with patients:
Ask about tobacco use;
Advise tobacco users to quit in strong, clear terms;
Assess readiness for tobacco cessation;
Assist in developing a plan to stop tobacco use; and
Arrange a follow-up consultation to review the patient’s success or to reassess cessation readiness.
Whenever a patient expresses any interest in smoking cessation, it is essential for the clinician to respond with motivation. To help the patient prepare to stop, the clinician must address the five R’s7:
Relevance—the importance of smoking cessation to the patient;
Risks of continuing to smoke, particularly health concerns;
Rewards of smoking cessation, especially alleviation of health complaints;
Roadblocks that contribute to the threat of relapse—but which can be overcome with sufficient motivation; and
Repetition of support and reinforcement for this healthy lifestyle choice, be it from family, friends, coworkers, or the clinician. To prepare for times when support seems to wane, patients should be encouraged to phone 1-800-QUITNOW, a number that will connect the caller to his or her state’s quit line.
Repetition may also imply repeated cessation attempts if the first (or most recent) was unsuccessful. According to findings from a literature review, the reasons smokers relapse are numerous, including cravings (the most common) and withdrawal symptoms, weight gain, stress, and exposure to other smokers.10,11 Interventions based on patients’ given reasons for relapse have no apparent impact on the rate of return to smoking.12 Nevertheless, clinicians must take responsibility to motivate patients and reinforce their successes at every encounter.
UNAIDED CESSATION
In a culture demanding quick results and in the context of ongoing pharmaceutical advertisements and aisles lined with quit-smoking products, it may be easy to dismiss unaided cessation. Options range from gradual cutting down to the abrupt discontinuation of tobacco—going cold turkey. Although little research has been devoted to these strategies,13 unaided cessation is the method patients most often cite in their attempts to quit—and the method successful quitters report as most effective.14,15 The patients most likely to succeed at quitting are those who do not ask for help.
ASSISTED CESSATION
Patients with a significant dependence on nicotine are likely to request assistance with cessation.15 Identifying those who struggle to quit smoking and offering appropriate support may represent the difference between their success and failure.9
Several available tools to support patients’ “quit smoking” efforts, including pharmacologic options (see table7), are described here.
Nicotine Replacement Therapy
Nicotine replacement therapy (NRT) is used to reduce nicotine withdrawal symptoms by replacing smoking-produced nicotine with an alternate source of delivery. NRT is currently available in several forms: a transdermal patch, gum, lozenge, or the electronic cigarette. The chance of successful quitting is increased 50% to 70% when NRT is used, compared with patients using placebo.16 While the various forms of NRT share the same goal, they are not equally effective.17
Nicotine transdermal patches have been used in the US since 1991. The patches are used in a stepwise fashion; each patch delivers nicotine at a consistent quantity per hour, and over time, patches with increasingly lower doses of nicotine are substituted. There is some evidence that the patch is more efficacious for maintenance after smoking cessation than for the initial effort to quit.18
Nicotine gum and lozenges, orally absorbed forms of NRT, are used as needed, depending on patients’ withdrawal symptoms. Japuntich et al18 found that these products alone are not beneficial. However, combining bupropion with gum or lozenge therapy was found more effective for patients attempting to stop smoking than either agent alone.18 Lozenges have also been described as increasingly beneficial when combined with a longer-acting NRT, such as a transdermal patch, when cravings increase and rapid delivery of nicotine is required.16
The electronic cigarette (e-cigarette) is a battery-operated device that aerosolizes liquid nicotine, which is then orally absorbed. In a 2011 study, Siegel et al19 found that more than two-thirds of smokers reduced the number of cigarettes smoked after using an e-cigarette. Six months after subjects first purchased e-cigarettes, 31% remained tobacco-abstinent.
Since e-cigarettes are flameless, their use has been suggested in areas where smoking was previously prohibited. This short-acting NRT may benefit a patient when craving is provoked by forced denial of nicotine.
Current research is under way to examine two newer potential NRT tools: a nicotine mouth spray and a nicotine vaccine.20,21 In a randomized, double-blind, placebo-controlled study, Tønnesen et al20 found that use of a nicotine mouth spray was associated with significantly higher rates of tobacco abstinence at six, 24, and 52 weeks, compared with patients receiving placebo; however, rates of adverse effects were high in both groups (88% and 71%, respectively).
NRT is inexpensive and easily accessible to patients. Since its forms are all available OTC, consultation with health care providers is unnecessary. For patients who have tried to quit smoking unaided and who need short-term or immediate assistance to prevent a smoking relapse, NRT can be a helpful resource.
Bupropion
For smokers who want to quit without using a nicotine-based intervention, the antidepressant bupropion can be a promising smoking cessation aid. It is not clear what mechanism of action helps smokers who take bupropion to stop, although its chemical structure resembles that of diethylpropion, a drug used as an appetite suppressant.22 Bupropion does hinder norepinephrine and dopamine reuptake in the nervous system—opposing an effect of nicotine withdrawal.
Bupropion’s effects as an antidepressant and as a smoking cessation aid do not appear to be related.22 For this reason, even a patient who has not responded to bupropion for treatment of depression may benefit from using it as a smoking cessation aid.
Bupropion may be used alone or with other agents to stop nicotine use. Many study groups report that a combination of medications is more effective than monotherapy, and this is true for combinations that include bupropion.23-26 When used with nicotine lozenges, bupropion has been found effective in preventing a return to tobacco after previous lapses in smoking abstinence. Aside from a nicotine patch, no other monotherapy or combination was effective at achieving this goal.18 Thus, bupropion may be best utilized as a component in combination therapy.
Varenicline
Approved for use in the US in 2006, varenicline is the newest pharmaceutical therapy for smoking cessation. As a partial nicotinic receptor agonist,7 varenicline prevents nicotine from activating the mesolimbic dopamine system, which is associated with pleasure and reward (among other functions). By stimulating the nervous system’s dopamine (though to a lesser extent than nicotine), this agent reduces cravings for tobacco and symptoms of nicotine withdrawal—which are among the greatest barriers to smoking cessation.10 Because of its mechanism of action, varenicline is not often used in combination with NRT.
Varenicline has been shown to be as effective as the combination therapy of bupropion with nicotine lozenges.7,27 UK investigators Hajek et al27 found that using varenicline for four weeks before attempting to stop smoking had minimal effect on smoking urges and withdrawal symptoms, compared with using varenicline for just one week before attempting to quit. However, those who used varenicline for four weeks before stopping smoking were more likely to be smoke-free at 12 weeks than those who had used it for just one week before quitting.27
Other Pharmaceutical Options
Clonidine, long recognized as an effective antihypertensive medication, was determined by Gourlay et al9 in a 2004 review to have potential for use in supporting smoking cessation. Because significant adverse events (including drowsiness, sedation, and postural hypotension) have been associated with clonidine use7,28 and the FDA has not yet approved it for the indication of smoking cessation, its use may be most appropriate as a second-line treatment option, in combination with bupropion or nortriptyline, or for specialists’ use.28 Clonidine should not be discontinued suddenly.
Like bupropion, the tricyclic antidepressant nortriptyline has been investigated for its potential in tobacco cessation therapy. While a significant amount is known about plasma concentrations of nortriptyline needed to treat depression, levels required for effective tobacco cessation are less clear. Mooney et al29 found that therapeutic plasma concentrations of nortriptyline varied among subjects by race and smoking habits; although a lower concentration was usually required to assist smoking cessation than to treat depression, adverse effects were common even at lower concentrations. Thus, it was recommended that nortriptyline be reserved for second-line treatment.
This summer, researchers for the Cochrane Tobacco Addiction Review Group published a review of the literature (including phase II and phase III trials conducted by pharmaceutical companies—making the risk for bias “high or unclear”) pertaining to two nicotine vaccines in development.21 In two studies, the level of development of nicotine antibodies was associated with commensurate cessation rates; in two others, the outcome measure (12 months’ abstinence from smoking) was met in 11% of subjects, whether they received the vaccine or placebo. Thus, no strong evidence yet exists that nicotine vaccination supports smoking cessation in the long term; further research is needed.
NONPHARMACEUTICAL
INTERVENTIONS
Acupuncture
Variations and modifications of the traditional Chinese therapy of acupuncture, including acupressure and electrostimulation, have been examined in a number of clinical trials. Despite the supporting rhetoric, objective research of good quality in this area is limited. However, one systematic literature review showed acupuncture to be only slightly more effective than sham interventions and less effective than NRT.30 Insufficient evidence was reported on acupressure and laser stimulation, and acupressure was no more effective than psychological treatments. Considering questionable study quality and other limitations in the currently available research, practitioners should not consider acupuncture or related interventions as first-line options—nor should their potential be dismissed altogether.
Hypnotherapy
Conclusive research findings regarding hypnotherapy as an effective treatment for tobacco dependence are also limited. In 2010, Barnes at al31 reviewed 11 studies comparing hypnotherapy with various alternate methods and found little difference in effectiveness among hypnotherapy, psychological counseling, and rapid smoking therapy. Despite the limitations in these data, however, hypnotherapy may be appropriate for some patients.
CONCLUSION
Tobacco dependence is not the same for any two patients. Just as health care providers do not use the same treatment option for every patient with hypertension or diabetes, treatment for tobacco-dependent patients must also be individualized.
Our professional goal is to care for the health of patients. We clinicians must recommend cessation to our patients who smoke at every encounter—and offer support often. When we miss an opportunity to counsel a patient on the importance of quitting, the patient may interpret our silence as condoning the behavior. Empowering patients with an understanding of the options can contribute to their success—a significant move toward better health.
The authors of Healthy People 2020 hope that 80% of current smokers will have tried to stop smoking by that year. Have 80% of your patients been counseled and offered assistance to stop?
REFERENCES
1. CDC. Current cigarette smoking prevalence among working adults—United States, 2004-2010. MMWR Morb Mortal Wkly Rep. 2011;60(38):1305-1309.
2. CDC. Vital signs: current cigarette smoking among adults aged ≥ 18 years—United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1135-1140.
3. Jamal A, Dube SR, Malarcher AM, et al; CDC. Tobacco use screening and counseling during physician office visits among adults—National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61 suppl: 38-45.
4. US Department of Health and Human Services. Healthy People 2020 summary of objectives: tobacco use. http://healthypeople.gov/2020/topicsobjectives2020/pdfs/TobaccoUse.pdf. Accessed October 18, 2012.
5. US Department of Health and Human Services. Healthy People 2010 archives. www.healthypeople.gov/2010. Accessed October 18, 2012.
6. Blumenthal DS. Barriers to the provision of smoking cessation services reported by clinicians in underserved communities. J Am Board Fam Med. 2007;20(3):272-279.
7. Fiore MC, Jaén CR, Baker TB, et al; Public Health Service, US Department of Health and Human Services. Clinical practice guideline: treating tobacco use and dependence: 2008 update. www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf. Accessed October 18, 2012.
8. Carson KV, Verbiest ME, Crone MR, et al. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2012 May 16; 5:CD000214.
9. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
10. Guirguis AB, Ray SM, Zingone MM, et al. Smoking cessation: barriers to success and readiness to change. Tenn Med. 2010;103(9):45-49.
11. Nørregaard J, Tønnesen P, Petersen L. Predictors and reasons for relapse in smoking cessation with nicotine and placebo patches. Prev Med. 1993;22(2):261-271.
12. Lancaster T, Hajek P, Stead LF, et al. Prevention of relapse after quitting smoking: a systematic review of trials. Arch Intern Med. 2006;166(8): 828-835.
13. Chapman S, MacKenzie R. The global research neglect of unassisted smoking cessation: causes and consequences. PLoS Med. 2010;7(2):e1000216.
14. Hung WT, Dunlop SM, Perez D, Cotter T. Use and perceived helpfulness of smoking cessation methods: results from a population survey of recent quitters. BMC Public Health. 2011;11:592.
15. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34(2):102-111.
16. Stead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD000146.
17. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations. Clin Ther. 2008;30(5):800-812.
18. Japuntich SJ, Piper ME, Leventhal AM, et al. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. J Consult Clin Psychol. 2011;79(1):34-42.
19. Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation tool: results from an online survey. Am J Prev Med. 2011;40 (4):472-475.
20. Tønnesen P, Lauri H, Perfekt R, et al. Efficacy of a nicotine mouth spray in smoking cessation: a randomised, double-blind trial. Eur Respir J. 2012;40(3):548-554.
21. Hartmann-Boyce J, Cahill K, Hatsukami D, Cornuz J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012 Aug 15;8:CD007072.
22. Roddy E. Bupropion and other non-nicotine pharmacotherapies. BMJ. 2004;328(7438):
509-511.
23. Loh WY, Piper ME, Schlam TR, et al. Should all smokers use combination smoking cessation pharmacotherapy? Using novel analytic methods to detect differential treatment effects over 8 weeks of pharmacotherapy. Nicotine Tob Res. 2012;14(2):131-141.
24. Bolt DM, Piper ME, Theobald WE, Baker TB. Why two smoking cessation agents work better than one: role of craving suppression. J Consult Clin Psychol. 2012;80(1):44-65.
25. McNeil JJ, Piccenna L, Ioannides-Demos LL. Smoking cessation: recent advances. Cardiovasc Drugs Ther. 2010;24(4):359-367.
26. Ebbert JO, Hays JT, Hurt RD. Combination pharmacotherapy for stopping smoking: what advantages does it offer? Drugs. 2010;70(6):643-650.
27. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171 (8):770-777.
28. Bentz CJ. Review: clonidine is more effective than placebo for long-term smoking cessation, but has side effects. ACP J Club. 2005;142(1):12.
29. Mooney ME, Reus VI, Gorecki J, et al. Therapeutic drug monitoring of nortriptyline in smoking cessation: a multistudy analysis. Clin Pharmacol Ther. 2008;83(3):436-442.
30. White AR, Rampes H, Liu JP, et al. Acupuncture and related interventions for smoking cessation. Cochrane Database Syst Rev. 2011;(1): CD000009.
31. Barnes J, Dong CY, McRobbie H, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev. 2010;(10):CD001008.
MI Rate Declines After Smoke-Free Laws Enacted in Olmsted County
The rate of myocardial infarction dropped by one-third after laws prohibiting smoking in public places and workplaces were enacted in Olmsted County, Minnesota, according to a report published online Oct. 29 in Archives of Internal Medicine.
Although this epidemiologic study could not establish causality, no other interventions during the study period could plausibly explain this community-wide reduction in the MI rate. And the only major MI risk factor that declined concurrently was the prevalence of smoking; rates of hypertension and hypercholesterolemia remained steady, and rates of diabetes and obesity increased, said Dr. Richard D. Hurt of the Nicotine Dependence Center and the department of internal medicine at the Mayo Clinic in Rochester, Minn., and his associates.

"We believe that secondhand smoke should be considered a major risk factor for MI, joining family history, hypertension, hyperlipidemia, diabetes mellitus, and low physical activity. Hence, all clinicians should ascertain secondhand smoke exposure and promote the elimination of secondhand smoke exposure as part of their lifestyle recommendations," they noted.
"All people should avoid secondhand smoke exposure as much as possible, and those with [coronary heart disease] should have no exposure to secondhand smoke," the investigators added.
Several studies have documented declines in hospital admissions for MI after the implementation of smoke-free laws, and the Institute of Medicine has concluded that there is a causal relationship between smoking bans and reductions in acute coronary events. To more closely examine the magnitude of that risk reduction, Dr. Hurt and his colleagues analyzed data from the Rochester Epidemiology Project, in which all cases of MI and sudden cardiac death in a well-defined community were validated using rigorous epidemiologic criteria. This project "has a long track record (more than 50 years) of robust epidemiologic studies," they said.
In Olmsted County, restaurants were required to be smoke free as of Jan. 1, 2002; bars and workplaces were required to follow suit on Oct. 1, 2007. The researchers examined rates of MI and sudden cardiac death during the 18 months before and the 18 months following implementation of each ordinance.
During the entire study period, there were 717 incident MIs and 514 cases of sudden cardiac death.
The age- and sex-adjusted rate of MI dropped from 150.8/100,000 people before the laws were implemented to 100.7/100,000 afterward – a 34% decline, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.46]).
Similarly, there was a 17% decline in the incidence of sudden cardiac death during this period, which indicates a trend but does not constitute a statistically significant reduction.
Smoke-free legislation is effective not only because it decreases the amount of secondhand smoke to which nonsmokers are exposed, but also because it reduces the intensity of smoking among smokers, increases quit rates, and reduces the rate of taking up smoking in the first place, Dr. Hurt and his associates said.
Other research has demonstrated that as little as 30 minutes of exposure to secondhand smoke causes an abrupt and dramatic decrease in coronary artery flow velocity reserves and vascular injury that inhibits endothelial function. Exposure also has been associated with low HDL cholesterol levels, increased markers of inflammation, increased serum levels of fibrinogen and homocysteine, decreased antioxidant levels, and increased insulin resistance, they wrote.
Taken together, these findings indicate that physicians should "become advocates for effective tobacco control policies, such as increased taxes, graphic labeling, smoke-free workplaces, and marketing and advertising restrictions," the researchers said.
One limitation of this study was that the population of Olmsted County is predominantly white. Further studies are needed "in communities of more diverse racial and ethnic composition," Dr. Hurt and his colleagues said.
This study was supported by ClearWay Minnesota; the National Heart, Lung, and Blood Institute; and the National Institute on Aging. No financial conflicts of interest were reported.
The evidence documenting positive health outcomes from smoking bans continues to grow, as more areas adopt smoke-free legislation.
Clinicians should now work on closing the loopholes in existing smoke-free policies and expanding those policies to include bans in multiunit housing, motor vehicles, casinos, and outdoor locations. Studies have shown that smoking bans enacted in multiunit housing not only reduce exposure to second-hand smoke, but also increase quit attempts in persons who generally have higher smoking prevalences, such as those with low socioeconomic status.
Sara Kalkhoran, M.D., is in the department of internal medicine; Pamela M. Ling, M.D., is at the Center for Tobacco Control Research and Education within the department of internal medicine at the University of California, San Francisco. These remarks were taken from their invited commentary accompanying Dr. Hurt’s report (Arch. Intern. Med. 2012 [doi10.1001/2013.jamainternmed.269]). They reported no financial conflicts of interest.
The evidence documenting positive health outcomes from smoking bans continues to grow, as more areas adopt smoke-free legislation.
Clinicians should now work on closing the loopholes in existing smoke-free policies and expanding those policies to include bans in multiunit housing, motor vehicles, casinos, and outdoor locations. Studies have shown that smoking bans enacted in multiunit housing not only reduce exposure to second-hand smoke, but also increase quit attempts in persons who generally have higher smoking prevalences, such as those with low socioeconomic status.
Sara Kalkhoran, M.D., is in the department of internal medicine; Pamela M. Ling, M.D., is at the Center for Tobacco Control Research and Education within the department of internal medicine at the University of California, San Francisco. These remarks were taken from their invited commentary accompanying Dr. Hurt’s report (Arch. Intern. Med. 2012 [doi10.1001/2013.jamainternmed.269]). They reported no financial conflicts of interest.
The evidence documenting positive health outcomes from smoking bans continues to grow, as more areas adopt smoke-free legislation.
Clinicians should now work on closing the loopholes in existing smoke-free policies and expanding those policies to include bans in multiunit housing, motor vehicles, casinos, and outdoor locations. Studies have shown that smoking bans enacted in multiunit housing not only reduce exposure to second-hand smoke, but also increase quit attempts in persons who generally have higher smoking prevalences, such as those with low socioeconomic status.
Sara Kalkhoran, M.D., is in the department of internal medicine; Pamela M. Ling, M.D., is at the Center for Tobacco Control Research and Education within the department of internal medicine at the University of California, San Francisco. These remarks were taken from their invited commentary accompanying Dr. Hurt’s report (Arch. Intern. Med. 2012 [doi10.1001/2013.jamainternmed.269]). They reported no financial conflicts of interest.
The rate of myocardial infarction dropped by one-third after laws prohibiting smoking in public places and workplaces were enacted in Olmsted County, Minnesota, according to a report published online Oct. 29 in Archives of Internal Medicine.
Although this epidemiologic study could not establish causality, no other interventions during the study period could plausibly explain this community-wide reduction in the MI rate. And the only major MI risk factor that declined concurrently was the prevalence of smoking; rates of hypertension and hypercholesterolemia remained steady, and rates of diabetes and obesity increased, said Dr. Richard D. Hurt of the Nicotine Dependence Center and the department of internal medicine at the Mayo Clinic in Rochester, Minn., and his associates.
"We believe that secondhand smoke should be considered a major risk factor for MI, joining family history, hypertension, hyperlipidemia, diabetes mellitus, and low physical activity. Hence, all clinicians should ascertain secondhand smoke exposure and promote the elimination of secondhand smoke exposure as part of their lifestyle recommendations," they noted.
"All people should avoid secondhand smoke exposure as much as possible, and those with [coronary heart disease] should have no exposure to secondhand smoke," the investigators added.
Several studies have documented declines in hospital admissions for MI after the implementation of smoke-free laws, and the Institute of Medicine has concluded that there is a causal relationship between smoking bans and reductions in acute coronary events. To more closely examine the magnitude of that risk reduction, Dr. Hurt and his colleagues analyzed data from the Rochester Epidemiology Project, in which all cases of MI and sudden cardiac death in a well-defined community were validated using rigorous epidemiologic criteria. This project "has a long track record (more than 50 years) of robust epidemiologic studies," they said.
In Olmsted County, restaurants were required to be smoke free as of Jan. 1, 2002; bars and workplaces were required to follow suit on Oct. 1, 2007. The researchers examined rates of MI and sudden cardiac death during the 18 months before and the 18 months following implementation of each ordinance.
During the entire study period, there were 717 incident MIs and 514 cases of sudden cardiac death.
The age- and sex-adjusted rate of MI dropped from 150.8/100,000 people before the laws were implemented to 100.7/100,000 afterward – a 34% decline, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.46]).
Similarly, there was a 17% decline in the incidence of sudden cardiac death during this period, which indicates a trend but does not constitute a statistically significant reduction.
Smoke-free legislation is effective not only because it decreases the amount of secondhand smoke to which nonsmokers are exposed, but also because it reduces the intensity of smoking among smokers, increases quit rates, and reduces the rate of taking up smoking in the first place, Dr. Hurt and his associates said.
Other research has demonstrated that as little as 30 minutes of exposure to secondhand smoke causes an abrupt and dramatic decrease in coronary artery flow velocity reserves and vascular injury that inhibits endothelial function. Exposure also has been associated with low HDL cholesterol levels, increased markers of inflammation, increased serum levels of fibrinogen and homocysteine, decreased antioxidant levels, and increased insulin resistance, they wrote.
Taken together, these findings indicate that physicians should "become advocates for effective tobacco control policies, such as increased taxes, graphic labeling, smoke-free workplaces, and marketing and advertising restrictions," the researchers said.
One limitation of this study was that the population of Olmsted County is predominantly white. Further studies are needed "in communities of more diverse racial and ethnic composition," Dr. Hurt and his colleagues said.
This study was supported by ClearWay Minnesota; the National Heart, Lung, and Blood Institute; and the National Institute on Aging. No financial conflicts of interest were reported.
The rate of myocardial infarction dropped by one-third after laws prohibiting smoking in public places and workplaces were enacted in Olmsted County, Minnesota, according to a report published online Oct. 29 in Archives of Internal Medicine.
Although this epidemiologic study could not establish causality, no other interventions during the study period could plausibly explain this community-wide reduction in the MI rate. And the only major MI risk factor that declined concurrently was the prevalence of smoking; rates of hypertension and hypercholesterolemia remained steady, and rates of diabetes and obesity increased, said Dr. Richard D. Hurt of the Nicotine Dependence Center and the department of internal medicine at the Mayo Clinic in Rochester, Minn., and his associates.
"We believe that secondhand smoke should be considered a major risk factor for MI, joining family history, hypertension, hyperlipidemia, diabetes mellitus, and low physical activity. Hence, all clinicians should ascertain secondhand smoke exposure and promote the elimination of secondhand smoke exposure as part of their lifestyle recommendations," they noted.
"All people should avoid secondhand smoke exposure as much as possible, and those with [coronary heart disease] should have no exposure to secondhand smoke," the investigators added.
Several studies have documented declines in hospital admissions for MI after the implementation of smoke-free laws, and the Institute of Medicine has concluded that there is a causal relationship between smoking bans and reductions in acute coronary events. To more closely examine the magnitude of that risk reduction, Dr. Hurt and his colleagues analyzed data from the Rochester Epidemiology Project, in which all cases of MI and sudden cardiac death in a well-defined community were validated using rigorous epidemiologic criteria. This project "has a long track record (more than 50 years) of robust epidemiologic studies," they said.
In Olmsted County, restaurants were required to be smoke free as of Jan. 1, 2002; bars and workplaces were required to follow suit on Oct. 1, 2007. The researchers examined rates of MI and sudden cardiac death during the 18 months before and the 18 months following implementation of each ordinance.
During the entire study period, there were 717 incident MIs and 514 cases of sudden cardiac death.
The age- and sex-adjusted rate of MI dropped from 150.8/100,000 people before the laws were implemented to 100.7/100,000 afterward – a 34% decline, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.46]).
Similarly, there was a 17% decline in the incidence of sudden cardiac death during this period, which indicates a trend but does not constitute a statistically significant reduction.
Smoke-free legislation is effective not only because it decreases the amount of secondhand smoke to which nonsmokers are exposed, but also because it reduces the intensity of smoking among smokers, increases quit rates, and reduces the rate of taking up smoking in the first place, Dr. Hurt and his associates said.
Other research has demonstrated that as little as 30 minutes of exposure to secondhand smoke causes an abrupt and dramatic decrease in coronary artery flow velocity reserves and vascular injury that inhibits endothelial function. Exposure also has been associated with low HDL cholesterol levels, increased markers of inflammation, increased serum levels of fibrinogen and homocysteine, decreased antioxidant levels, and increased insulin resistance, they wrote.
Taken together, these findings indicate that physicians should "become advocates for effective tobacco control policies, such as increased taxes, graphic labeling, smoke-free workplaces, and marketing and advertising restrictions," the researchers said.
One limitation of this study was that the population of Olmsted County is predominantly white. Further studies are needed "in communities of more diverse racial and ethnic composition," Dr. Hurt and his colleagues said.
This study was supported by ClearWay Minnesota; the National Heart, Lung, and Blood Institute; and the National Institute on Aging. No financial conflicts of interest were reported.
FROM ARCHIVES OF INTERNAL MEDICINE
Major Finding: The rate of incident MI dropped 34%, from 150.8/100,000 people to 100.7/100,000, after laws prohibiting smoking in public places and workplaces were enacted.
Data Source: An analysis of data in the Rochester Epidemiology Project concerning the incidence of MI and sudden cardiac death in Olmsted County, Minn., during the 18 months before and the 18 months after smoke-free legislation was enacted.
Disclosures: This study was supported by ClearWay Minnesota; the National Heart, Lung, and Blood Institute; and the National Institute on Aging. No financial conflicts of interest were reported.
