User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
FDA issues CV safety update for smoking cessation drug
The rate of major adverse cardiovascular events was higher among patients treated with varenicline than those on placebo in a meta-analysis, but the difference was not statistically significant, according to the latest Food and Drug Administration statement on the cardiovascular safety of the smoking cessation drug.
In the study, conducted by the manufacturer at the request of the FDA, major adverse cardiovascular events (MACEs), a composite endpoint of cardiovascular-related death, nonfatal MI, and nonfatal stroke, "were uncommon in both the Chantix and placebo groups, and the increased risk was not statistically significant, which means it is uncertain whether the excess risk for the Chantix group was due to the drug or due to chance," the FDA statement said. Varenicline, a nicotinic receptor partial agonist marketed as Chantix by Pfizer, was approved in 2006.

The first notice issued by the FDA about the drug’s possible cardiac risks was in June 2011. That notice reported the increased risk in a smoking cessation trial of patients with stable cardiovascular disease, prompting the FDA to require the company to conduct the meta-analysis. The FDA statement, dated Dec. 12, says the findings of the meta-analysis are similar to the findings of the smoking cessation study.
The meta-analysis compared the MACE incidence of patients treated for at least 12 weeks, in 15 randomized, double-blind, placebo-controlled studies conducted by Pfizer. Within 30 days of stopping the drug, the incidence of MACE was 0.31% (13 cases among 4,190 patients) in those on the drug, compared with 0.21% (6 cases among 2,812 on placebo). This is comparable to an increase of 6.3 MACE cases per 1,000 patient years of exposure, the FDA said.
In the study, the rates of composite outcomes were higher among those on varenicline "across different time frames and prespecified sensitivity analyses, including various study groupings and cardiovascular endpoints," and while not significantly different, they were consistent, the statement said.
The FDA also points out that cardiovascular mortality and all-cause mortality, components of the MACE endpoint, were lower among the patients on varenicline, although the differences were not significant. The rate of cardiovascular mortality was 0.05% (two cases) among those on varenicline, compared with 0.07% (two cases) among those on placebo. The rate of all-cause mortality was 0.14% among those on varenicline (6 cases), compared with 0.25% (7 cases) among those on placebo.
In the statement, the FDA advises that when weighing the risks and benefits of varenicline, health care professionals should consider the "immediate and substantial" health benefits of quitting smoking, and that "Chantix is effective in helping patients to quit smoking and abstain from it for as long as one year," the FDA advised in the statement. Patients should also be counseled to seek medical help if they develop new or worsening cardiovascular disease symptoms during treatment with varenicline, the statement added.
The results of the meta-analysis have been added to the warnings and precautions section of the drug’s label.
About 2.3 million varenicline prescriptions were dispensed and about 1.26 million patients received prescriptions for the drug from outpatient retail pharmacies in the United States, during the 12-month period ending in September 2012, according to the FDA.
The safety communication is available here. Serious adverse events associated with varenicline should be reported to the FDA at 800-332-1088 or here.
The rate of major adverse cardiovascular events was higher among patients treated with varenicline than those on placebo in a meta-analysis, but the difference was not statistically significant, according to the latest Food and Drug Administration statement on the cardiovascular safety of the smoking cessation drug.
In the study, conducted by the manufacturer at the request of the FDA, major adverse cardiovascular events (MACEs), a composite endpoint of cardiovascular-related death, nonfatal MI, and nonfatal stroke, "were uncommon in both the Chantix and placebo groups, and the increased risk was not statistically significant, which means it is uncertain whether the excess risk for the Chantix group was due to the drug or due to chance," the FDA statement said. Varenicline, a nicotinic receptor partial agonist marketed as Chantix by Pfizer, was approved in 2006.
The first notice issued by the FDA about the drug’s possible cardiac risks was in June 2011. That notice reported the increased risk in a smoking cessation trial of patients with stable cardiovascular disease, prompting the FDA to require the company to conduct the meta-analysis. The FDA statement, dated Dec. 12, says the findings of the meta-analysis are similar to the findings of the smoking cessation study.
The meta-analysis compared the MACE incidence of patients treated for at least 12 weeks, in 15 randomized, double-blind, placebo-controlled studies conducted by Pfizer. Within 30 days of stopping the drug, the incidence of MACE was 0.31% (13 cases among 4,190 patients) in those on the drug, compared with 0.21% (6 cases among 2,812 on placebo). This is comparable to an increase of 6.3 MACE cases per 1,000 patient years of exposure, the FDA said.
In the study, the rates of composite outcomes were higher among those on varenicline "across different time frames and prespecified sensitivity analyses, including various study groupings and cardiovascular endpoints," and while not significantly different, they were consistent, the statement said.
The FDA also points out that cardiovascular mortality and all-cause mortality, components of the MACE endpoint, were lower among the patients on varenicline, although the differences were not significant. The rate of cardiovascular mortality was 0.05% (two cases) among those on varenicline, compared with 0.07% (two cases) among those on placebo. The rate of all-cause mortality was 0.14% among those on varenicline (6 cases), compared with 0.25% (7 cases) among those on placebo.
In the statement, the FDA advises that when weighing the risks and benefits of varenicline, health care professionals should consider the "immediate and substantial" health benefits of quitting smoking, and that "Chantix is effective in helping patients to quit smoking and abstain from it for as long as one year," the FDA advised in the statement. Patients should also be counseled to seek medical help if they develop new or worsening cardiovascular disease symptoms during treatment with varenicline, the statement added.
The results of the meta-analysis have been added to the warnings and precautions section of the drug’s label.
About 2.3 million varenicline prescriptions were dispensed and about 1.26 million patients received prescriptions for the drug from outpatient retail pharmacies in the United States, during the 12-month period ending in September 2012, according to the FDA.
The safety communication is available here. Serious adverse events associated with varenicline should be reported to the FDA at 800-332-1088 or here.
The rate of major adverse cardiovascular events was higher among patients treated with varenicline than those on placebo in a meta-analysis, but the difference was not statistically significant, according to the latest Food and Drug Administration statement on the cardiovascular safety of the smoking cessation drug.
In the study, conducted by the manufacturer at the request of the FDA, major adverse cardiovascular events (MACEs), a composite endpoint of cardiovascular-related death, nonfatal MI, and nonfatal stroke, "were uncommon in both the Chantix and placebo groups, and the increased risk was not statistically significant, which means it is uncertain whether the excess risk for the Chantix group was due to the drug or due to chance," the FDA statement said. Varenicline, a nicotinic receptor partial agonist marketed as Chantix by Pfizer, was approved in 2006.
The first notice issued by the FDA about the drug’s possible cardiac risks was in June 2011. That notice reported the increased risk in a smoking cessation trial of patients with stable cardiovascular disease, prompting the FDA to require the company to conduct the meta-analysis. The FDA statement, dated Dec. 12, says the findings of the meta-analysis are similar to the findings of the smoking cessation study.
The meta-analysis compared the MACE incidence of patients treated for at least 12 weeks, in 15 randomized, double-blind, placebo-controlled studies conducted by Pfizer. Within 30 days of stopping the drug, the incidence of MACE was 0.31% (13 cases among 4,190 patients) in those on the drug, compared with 0.21% (6 cases among 2,812 on placebo). This is comparable to an increase of 6.3 MACE cases per 1,000 patient years of exposure, the FDA said.
In the study, the rates of composite outcomes were higher among those on varenicline "across different time frames and prespecified sensitivity analyses, including various study groupings and cardiovascular endpoints," and while not significantly different, they were consistent, the statement said.
The FDA also points out that cardiovascular mortality and all-cause mortality, components of the MACE endpoint, were lower among the patients on varenicline, although the differences were not significant. The rate of cardiovascular mortality was 0.05% (two cases) among those on varenicline, compared with 0.07% (two cases) among those on placebo. The rate of all-cause mortality was 0.14% among those on varenicline (6 cases), compared with 0.25% (7 cases) among those on placebo.
In the statement, the FDA advises that when weighing the risks and benefits of varenicline, health care professionals should consider the "immediate and substantial" health benefits of quitting smoking, and that "Chantix is effective in helping patients to quit smoking and abstain from it for as long as one year," the FDA advised in the statement. Patients should also be counseled to seek medical help if they develop new or worsening cardiovascular disease symptoms during treatment with varenicline, the statement added.
The results of the meta-analysis have been added to the warnings and precautions section of the drug’s label.
About 2.3 million varenicline prescriptions were dispensed and about 1.26 million patients received prescriptions for the drug from outpatient retail pharmacies in the United States, during the 12-month period ending in September 2012, according to the FDA.
The safety communication is available here. Serious adverse events associated with varenicline should be reported to the FDA at 800-332-1088 or here.

Beriplex outperforms plasma for rapid warfarin reversal
DENVER – A four-factor prothrombin complex concentrate bettered plasma for urgent reversal of warfarin and other vitamin K antagonists in patients experiencing major bleeding.
Marketed as Beriplex, the product had a higher rate of INR reversal than did plasma at 30 minutes after the start of infusion, based on results from a phase IIIb prospective, multicenter, randomized clinical trial.

The prothrombin complex concentrate (PCC) also proved more successful than plasma at early replacement of depleted coagulation factors and was noninferior to plasma in terms of blinded investigator–rated hemostatic efficacy in the first 24 hours, Dr. Joshua N. Goldstein said at the annual meeting of the American College of Emergency Physicians.
The study included 202 adults on warfarin or another vitamin K antagonist who presented with acute major bleeding. The objectives were to correct their INR as quickly as possible and thereby reduce their blood loss. Participants were randomized to INR- and weight-based dosing of the PCC or to plasma on top of background vitamin K given by slow intravenous infusion in all cases.
Thirty minutes after the start of the infusion, the mean INR was significantly lower in patients on the PCC than in those given plasma. The higher the baseline INR, the greater the benefit of the PCC. For example, in 58 patients with a baseline INR above 6, the mean INR dropped from 10.6 preinfusion to 1.5 at 30 minutes in the PCC group and to 3.7 in the plasma recipients, reported Dr. Goldstein of the University of Rochester (N.Y.).
In 44 patients with a baseline INR of 4-6, the INR fell from a mean of 4.6 preinfusion to 1.4 at 30 minutes in the PCC group and to 3.2 in patients on plasma. And in patients with a baseline INR of 2 to less than 4, mean INR fell from 2.9 preinfusion to 1.6 in the PCC group and to 2.2 in the plasma recipients.
One hour after the start of infusion, roughly 70% of PCC recipients had corrected their INR as defined by an INR of 1.3 or less, compared with less than 5% of plasma recipients.
Median factor levels were below 50% at baseline. Levels increased significantly more within 30 minutes of starting PCC infusion than with plasma. This wasn’t particularly surprising, since the PCC contains factors II, VII, IX, and X, along with proteins C and S, Dr. Goldstein observed.
Blinded investigators rated hemostatic efficacy in the first 24 hours as good or excellent in 72% of the PCC group and in 65% of patients on plasma, a nonsignificant difference.
Thromboembolic event rates through 51 days of follow-up were 7.8% with the PCC and 5.5% with plasma.
Dr. Goldstein reported that he serves as a consultant to and advisory board member for CSL Behring, which markets Beriplex and sponsored the study.
DENVER – A four-factor prothrombin complex concentrate bettered plasma for urgent reversal of warfarin and other vitamin K antagonists in patients experiencing major bleeding.
Marketed as Beriplex, the product had a higher rate of INR reversal than did plasma at 30 minutes after the start of infusion, based on results from a phase IIIb prospective, multicenter, randomized clinical trial.
The prothrombin complex concentrate (PCC) also proved more successful than plasma at early replacement of depleted coagulation factors and was noninferior to plasma in terms of blinded investigator–rated hemostatic efficacy in the first 24 hours, Dr. Joshua N. Goldstein said at the annual meeting of the American College of Emergency Physicians.
The study included 202 adults on warfarin or another vitamin K antagonist who presented with acute major bleeding. The objectives were to correct their INR as quickly as possible and thereby reduce their blood loss. Participants were randomized to INR- and weight-based dosing of the PCC or to plasma on top of background vitamin K given by slow intravenous infusion in all cases.
Thirty minutes after the start of the infusion, the mean INR was significantly lower in patients on the PCC than in those given plasma. The higher the baseline INR, the greater the benefit of the PCC. For example, in 58 patients with a baseline INR above 6, the mean INR dropped from 10.6 preinfusion to 1.5 at 30 minutes in the PCC group and to 3.7 in the plasma recipients, reported Dr. Goldstein of the University of Rochester (N.Y.).
In 44 patients with a baseline INR of 4-6, the INR fell from a mean of 4.6 preinfusion to 1.4 at 30 minutes in the PCC group and to 3.2 in patients on plasma. And in patients with a baseline INR of 2 to less than 4, mean INR fell from 2.9 preinfusion to 1.6 in the PCC group and to 2.2 in the plasma recipients.
One hour after the start of infusion, roughly 70% of PCC recipients had corrected their INR as defined by an INR of 1.3 or less, compared with less than 5% of plasma recipients.
Median factor levels were below 50% at baseline. Levels increased significantly more within 30 minutes of starting PCC infusion than with plasma. This wasn’t particularly surprising, since the PCC contains factors II, VII, IX, and X, along with proteins C and S, Dr. Goldstein observed.
Blinded investigators rated hemostatic efficacy in the first 24 hours as good or excellent in 72% of the PCC group and in 65% of patients on plasma, a nonsignificant difference.
Thromboembolic event rates through 51 days of follow-up were 7.8% with the PCC and 5.5% with plasma.
Dr. Goldstein reported that he serves as a consultant to and advisory board member for CSL Behring, which markets Beriplex and sponsored the study.
DENVER – A four-factor prothrombin complex concentrate bettered plasma for urgent reversal of warfarin and other vitamin K antagonists in patients experiencing major bleeding.
Marketed as Beriplex, the product had a higher rate of INR reversal than did plasma at 30 minutes after the start of infusion, based on results from a phase IIIb prospective, multicenter, randomized clinical trial.
The prothrombin complex concentrate (PCC) also proved more successful than plasma at early replacement of depleted coagulation factors and was noninferior to plasma in terms of blinded investigator–rated hemostatic efficacy in the first 24 hours, Dr. Joshua N. Goldstein said at the annual meeting of the American College of Emergency Physicians.
The study included 202 adults on warfarin or another vitamin K antagonist who presented with acute major bleeding. The objectives were to correct their INR as quickly as possible and thereby reduce their blood loss. Participants were randomized to INR- and weight-based dosing of the PCC or to plasma on top of background vitamin K given by slow intravenous infusion in all cases.
Thirty minutes after the start of the infusion, the mean INR was significantly lower in patients on the PCC than in those given plasma. The higher the baseline INR, the greater the benefit of the PCC. For example, in 58 patients with a baseline INR above 6, the mean INR dropped from 10.6 preinfusion to 1.5 at 30 minutes in the PCC group and to 3.7 in the plasma recipients, reported Dr. Goldstein of the University of Rochester (N.Y.).
In 44 patients with a baseline INR of 4-6, the INR fell from a mean of 4.6 preinfusion to 1.4 at 30 minutes in the PCC group and to 3.2 in patients on plasma. And in patients with a baseline INR of 2 to less than 4, mean INR fell from 2.9 preinfusion to 1.6 in the PCC group and to 2.2 in the plasma recipients.
One hour after the start of infusion, roughly 70% of PCC recipients had corrected their INR as defined by an INR of 1.3 or less, compared with less than 5% of plasma recipients.
Median factor levels were below 50% at baseline. Levels increased significantly more within 30 minutes of starting PCC infusion than with plasma. This wasn’t particularly surprising, since the PCC contains factors II, VII, IX, and X, along with proteins C and S, Dr. Goldstein observed.
Blinded investigators rated hemostatic efficacy in the first 24 hours as good or excellent in 72% of the PCC group and in 65% of patients on plasma, a nonsignificant difference.
Thromboembolic event rates through 51 days of follow-up were 7.8% with the PCC and 5.5% with plasma.
Dr. Goldstein reported that he serves as a consultant to and advisory board member for CSL Behring, which markets Beriplex and sponsored the study.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Major Finding: One hour after the start of infusion, roughly 70% of prothrombin complex concentrate recipients and less than 5% of plasma recipients had an INR of 1.3 or less.
Data Source: This was a randomized, multicenter, prospective phase IIIb clinical trial involving 202 patients.
Disclosures: Dr. Goldstein reported that he serves as a consultant to and advisory board member for CSL Behring, which markets Beriplex and sponsored the study.

Antibodies May Link to Lung Disease in RA
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.

To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.
To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
WASHINGTON – Specific anticitrullinated peptide antibody levels were significantly higher in rheumatoid arthritis patients with interstitial lung disease than in those without lung disease, based on data from 177 patients.
Complications and death are common in rheumatoid arthritis (RA) patients with interstitial lung disease (ILD), and the findings "may implicate the lung as a site in which protein citrullination initiates epitope spreading and propagation of RA," said Dr. Jon T. Giles of Columbia University in New York.
To determine the association of anticitrullinated peptide antibodies (ACPA) with ILD, Dr. Giles and his colleagues reviewed data from multidetector computed tomography images and concurrent serum samples for 177 RA patients. The mean age of the patients was 59 years, 60% were women, and 11% were smokers.
A total of 57 patients (32%) showed some evidence of ILD on imaging, and 32 (18%) had ILD scores of 3 U or higher, Dr. Giles said at the meeting. Overall, levels of anticyclic citrullinated peptide (anti-CCP) and 17 specific ACPAs ranged from 46% to 273% higher in patients with ILD than in those without ILD. Patients with ILD were more likely to be male, to smoke, and to have a history of prednisone and leflunomide use as well as rheumatoid factor and anti-CCP seropositivity compared with patients without ILD, said Dr. Giles.
Anti-CCP seropositivity was significantly more common among patients with any ILD vs. those without ILD (89% vs. 69%), and the seropositivity was even more common (94%) in patients with ILD scores of 3 U or higher.
Higher levels of seven or more ACPAs were significantly more common in patients with reticulation, honeycombing, or traction bronchiectasis than in those with no ILD (40% vs. 18%).
In addition, higher levels of seven or more ACPAs were significantly more common in patients with evidence of restriction on a pulmonary function test and/or decreased results on a diffusing capacity of the lungs for carbon monoxide test compared with those without ILD (39% vs. 20%). The differences were significant after adjustment for age, sex, smoking status, disease activity score (using DAS28), and current prednisone and leflunomide use.
Levels of antibodies targeting noncitrullinated proteins were not significantly higher in patients with ILD, which "suggests a specificity for ACPA in the association," Dr. Giles said.
"Another mechanistic possibility is that ACPA[s] targeting citrullinated synovial antigens are generated and mediate remote pathogenic effects upon circulating to the lungs, where their cognate citrullinated proteins may also be present," he said.
The findings were limited in part by the use of multidetector computed tomography, which differs in slice thickness from high-resolution CT, Dr. Giles noted. But the strengths of the research include the multiple measures of pulmonary disease, he said.
Dr. Giles said he had no financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Levels of anticyclic citrullinated peptide and 17 specific anticitrullinated peptide antibodies ranged from 46% to 273% higher in rheumatoid arthritis patients with interstitial lung disease than in those without.
Data Source: The data come from chest imaging and serum samples from 177 adults with RA.
Disclosures: Dr. Giles said he had no relevant financial conflicts to disclose. The study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the American College of Rheumatology’s Within Our Reach Campaign.

Indacaterol Proves Safe, Effective Across COPD Patients
ATLANTA – Indacaterol significantly improves bronchodilation and health status in patients with chronic obstructive pulmonary disease, and is safe and well tolerated, according to findings from studies presented at the annual meeting of the American College of Chest Physicians.
In a pooled analysis of efficacy and safety data from two randomized controlled studies, the inhaled long-acting beta2-agonist bronchodilator given at the approved dose of 75 mcg daily was found to be of benefit regardless of age, sex, smoking status, or severity of airflow limitation. In another analysis of pooled data, treatment was shown to have an acceptable cardiovascular and cerebrovascular safety profile.

The efficacy analysis included 640 patients from two identically designed studies who were randomized to receive indacaterol or placebo for 12 weeks. Trough (24 hours post dose) forced expiratory volume in 1 second (FEV1) improved by least-squares mean differences of 150 and 110 mL among men and women, respectively; by 110 and 150 mL among those under age 65 and those aged 65 or older; by 150 and 110 mL among those with moderate and severe airflow limitation; and by 140 and 130 mL in ex-smokers and current smokers, Dr. Thomas Siler of Midwest Chest Consultants in St. Charles, Mo., reported.
Health status scores, as measured using the St. George’s Respiratory Questionnaire, improved similarly in men and women (by 3.8 and 3.7 units, respectively), and also improved in all of the other groups. Improvement was greater, however, in those aged 65 years and older (by 4.5 units vs. 3.3 units in those under age 65), those with severe airflow limitation (by 4.6 units vs. 3.3 units in those with moderate airflow limitation), and in ex-smokers (by 4.1 vs. 3.5 units in current smokers).
Adverse events occurred in 44%-57% of patients receiving indacaterol and in 40%-48% of patients receiving placebo. More adverse events in both groups occurred in older patients, women, those with moderate disease, and ex-smokers.
Patients in this study had a mean age of 63 years, and a mean post-albuterol FEV1 of 54% predicted. About 40% were receiving inhaled corticosteroids.
The findings suggest that indacaterol can be successfully used to treat a range of COPD patients, Dr. Siler concluded. Treatment can be expected to lead to "substantial and worthwhile improvements in bronchodilation and health status," he added.
According to findings from a separate analysis of pooled data from nearly 2,500 patients, these improvements come without an increase in the risk of cerebro- and cardiovascular adverse events (CCV AEs).
The overall frequency of CCV AEs was similar in 449 patients treated for up to 3 months and 2,012 control patients who received placebo (2.0% and 2.58%, respectively), and no type of CCV AE occurred in more than 2 patients in the active treatment group, Dr. James Donohue reported.
Serious CCV AEs occurred in 2 patients in the treatment group and 13 in the placebo group, and an Antiplatelet Trialists’ Collaboration (APTC) event (a cerebrovascular accident not believed to be related to study treatment) occurred in 1 patient in the treatment group, compared with 8 patients in the control group, said Dr. Donohue of the University of North Carolina, Chapel Hill.
The overall frequency of patients with CCV AEs in a 6-month study population ranged from 3.3% to 5.8%, and no dose-response relationship was seen between the 75-mcg dose and up to 600 mcg daily for CCV AEs.
No deaths were reported in those receiving indacaterol 75.
These findings, which used pooled data from previous studies and a database of U.S. and Canadian patients, indicate that indacaterol given at the 75-mcg dose has an acceptable CCV safety profile in patients with moderate to severe COPD, Dr. Donohue said.
When considered in the context of the efficacy data, the findings should be very reassuring to clinicians, he concluded.
The studies included in the safety analysis were sponsored by Novartis. Dr. Donohue and Dr. Siler reported financial relationships with Novartis, which makes indacaterol, as well as with other industry companies. Dr. Donohue reported receiving fees for consulting and/or serving on speakers bureaus or advisory committees for Novartis, GSK, Boehringer-Ingelheim, and other companies. Dr. Siler reported receiving grant monies from GSK, Novartis, Boehringer-Ingelheim, and other companies. He also reported receiving fees for consulting, serving on speakers bureaus, and/or serving on advisory committees for Boehringer-Ingelheim, AstraZeneca, and Forest Research Institute.
ATLANTA – Indacaterol significantly improves bronchodilation and health status in patients with chronic obstructive pulmonary disease, and is safe and well tolerated, according to findings from studies presented at the annual meeting of the American College of Chest Physicians.
In a pooled analysis of efficacy and safety data from two randomized controlled studies, the inhaled long-acting beta2-agonist bronchodilator given at the approved dose of 75 mcg daily was found to be of benefit regardless of age, sex, smoking status, or severity of airflow limitation. In another analysis of pooled data, treatment was shown to have an acceptable cardiovascular and cerebrovascular safety profile.
The efficacy analysis included 640 patients from two identically designed studies who were randomized to receive indacaterol or placebo for 12 weeks. Trough (24 hours post dose) forced expiratory volume in 1 second (FEV1) improved by least-squares mean differences of 150 and 110 mL among men and women, respectively; by 110 and 150 mL among those under age 65 and those aged 65 or older; by 150 and 110 mL among those with moderate and severe airflow limitation; and by 140 and 130 mL in ex-smokers and current smokers, Dr. Thomas Siler of Midwest Chest Consultants in St. Charles, Mo., reported.
Health status scores, as measured using the St. George’s Respiratory Questionnaire, improved similarly in men and women (by 3.8 and 3.7 units, respectively), and also improved in all of the other groups. Improvement was greater, however, in those aged 65 years and older (by 4.5 units vs. 3.3 units in those under age 65), those with severe airflow limitation (by 4.6 units vs. 3.3 units in those with moderate airflow limitation), and in ex-smokers (by 4.1 vs. 3.5 units in current smokers).
Adverse events occurred in 44%-57% of patients receiving indacaterol and in 40%-48% of patients receiving placebo. More adverse events in both groups occurred in older patients, women, those with moderate disease, and ex-smokers.
Patients in this study had a mean age of 63 years, and a mean post-albuterol FEV1 of 54% predicted. About 40% were receiving inhaled corticosteroids.
The findings suggest that indacaterol can be successfully used to treat a range of COPD patients, Dr. Siler concluded. Treatment can be expected to lead to "substantial and worthwhile improvements in bronchodilation and health status," he added.
According to findings from a separate analysis of pooled data from nearly 2,500 patients, these improvements come without an increase in the risk of cerebro- and cardiovascular adverse events (CCV AEs).
The overall frequency of CCV AEs was similar in 449 patients treated for up to 3 months and 2,012 control patients who received placebo (2.0% and 2.58%, respectively), and no type of CCV AE occurred in more than 2 patients in the active treatment group, Dr. James Donohue reported.
Serious CCV AEs occurred in 2 patients in the treatment group and 13 in the placebo group, and an Antiplatelet Trialists’ Collaboration (APTC) event (a cerebrovascular accident not believed to be related to study treatment) occurred in 1 patient in the treatment group, compared with 8 patients in the control group, said Dr. Donohue of the University of North Carolina, Chapel Hill.
The overall frequency of patients with CCV AEs in a 6-month study population ranged from 3.3% to 5.8%, and no dose-response relationship was seen between the 75-mcg dose and up to 600 mcg daily for CCV AEs.
No deaths were reported in those receiving indacaterol 75.
These findings, which used pooled data from previous studies and a database of U.S. and Canadian patients, indicate that indacaterol given at the 75-mcg dose has an acceptable CCV safety profile in patients with moderate to severe COPD, Dr. Donohue said.
When considered in the context of the efficacy data, the findings should be very reassuring to clinicians, he concluded.
The studies included in the safety analysis were sponsored by Novartis. Dr. Donohue and Dr. Siler reported financial relationships with Novartis, which makes indacaterol, as well as with other industry companies. Dr. Donohue reported receiving fees for consulting and/or serving on speakers bureaus or advisory committees for Novartis, GSK, Boehringer-Ingelheim, and other companies. Dr. Siler reported receiving grant monies from GSK, Novartis, Boehringer-Ingelheim, and other companies. He also reported receiving fees for consulting, serving on speakers bureaus, and/or serving on advisory committees for Boehringer-Ingelheim, AstraZeneca, and Forest Research Institute.
ATLANTA – Indacaterol significantly improves bronchodilation and health status in patients with chronic obstructive pulmonary disease, and is safe and well tolerated, according to findings from studies presented at the annual meeting of the American College of Chest Physicians.
In a pooled analysis of efficacy and safety data from two randomized controlled studies, the inhaled long-acting beta2-agonist bronchodilator given at the approved dose of 75 mcg daily was found to be of benefit regardless of age, sex, smoking status, or severity of airflow limitation. In another analysis of pooled data, treatment was shown to have an acceptable cardiovascular and cerebrovascular safety profile.
The efficacy analysis included 640 patients from two identically designed studies who were randomized to receive indacaterol or placebo for 12 weeks. Trough (24 hours post dose) forced expiratory volume in 1 second (FEV1) improved by least-squares mean differences of 150 and 110 mL among men and women, respectively; by 110 and 150 mL among those under age 65 and those aged 65 or older; by 150 and 110 mL among those with moderate and severe airflow limitation; and by 140 and 130 mL in ex-smokers and current smokers, Dr. Thomas Siler of Midwest Chest Consultants in St. Charles, Mo., reported.
Health status scores, as measured using the St. George’s Respiratory Questionnaire, improved similarly in men and women (by 3.8 and 3.7 units, respectively), and also improved in all of the other groups. Improvement was greater, however, in those aged 65 years and older (by 4.5 units vs. 3.3 units in those under age 65), those with severe airflow limitation (by 4.6 units vs. 3.3 units in those with moderate airflow limitation), and in ex-smokers (by 4.1 vs. 3.5 units in current smokers).
Adverse events occurred in 44%-57% of patients receiving indacaterol and in 40%-48% of patients receiving placebo. More adverse events in both groups occurred in older patients, women, those with moderate disease, and ex-smokers.
Patients in this study had a mean age of 63 years, and a mean post-albuterol FEV1 of 54% predicted. About 40% were receiving inhaled corticosteroids.
The findings suggest that indacaterol can be successfully used to treat a range of COPD patients, Dr. Siler concluded. Treatment can be expected to lead to "substantial and worthwhile improvements in bronchodilation and health status," he added.
According to findings from a separate analysis of pooled data from nearly 2,500 patients, these improvements come without an increase in the risk of cerebro- and cardiovascular adverse events (CCV AEs).
The overall frequency of CCV AEs was similar in 449 patients treated for up to 3 months and 2,012 control patients who received placebo (2.0% and 2.58%, respectively), and no type of CCV AE occurred in more than 2 patients in the active treatment group, Dr. James Donohue reported.
Serious CCV AEs occurred in 2 patients in the treatment group and 13 in the placebo group, and an Antiplatelet Trialists’ Collaboration (APTC) event (a cerebrovascular accident not believed to be related to study treatment) occurred in 1 patient in the treatment group, compared with 8 patients in the control group, said Dr. Donohue of the University of North Carolina, Chapel Hill.
The overall frequency of patients with CCV AEs in a 6-month study population ranged from 3.3% to 5.8%, and no dose-response relationship was seen between the 75-mcg dose and up to 600 mcg daily for CCV AEs.
No deaths were reported in those receiving indacaterol 75.
These findings, which used pooled data from previous studies and a database of U.S. and Canadian patients, indicate that indacaterol given at the 75-mcg dose has an acceptable CCV safety profile in patients with moderate to severe COPD, Dr. Donohue said.
When considered in the context of the efficacy data, the findings should be very reassuring to clinicians, he concluded.
The studies included in the safety analysis were sponsored by Novartis. Dr. Donohue and Dr. Siler reported financial relationships with Novartis, which makes indacaterol, as well as with other industry companies. Dr. Donohue reported receiving fees for consulting and/or serving on speakers bureaus or advisory committees for Novartis, GSK, Boehringer-Ingelheim, and other companies. Dr. Siler reported receiving grant monies from GSK, Novartis, Boehringer-Ingelheim, and other companies. He also reported receiving fees for consulting, serving on speakers bureaus, and/or serving on advisory committees for Boehringer-Ingelheim, AstraZeneca, and Forest Research Institute.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Indacaterol at 75 mcg improved lung function and health status in patients with COPD, regardless of age, sex, smoking status, or severity of airflow limitation, and without an increase in the risk of cerebrovascular or cardiovascular adverse events.
Data Source: Results are from pooled data analyses.
Disclosures: The studies included in the safety analysis were sponsored by Novartis. Dr. Donohue and Dr. Siler reported financial relationships with Novartis, which makes indacaterol, as well as with other industry companies. Dr. Donohue reported receiving fees for consulting and/or serving on speakers bureaus or advisory committees for Novartis, GSK, and other companies. Dr. Siler reported receiving grant monies from GSK, Novartis, and other companies. He also reported receiving fees for consulting, serving on speakers bureaus, and/or serving on advisory committees for Boehringer-Ingelheim, AstraZeneca, and Forest Research Institute.

Grand Rounds: Woman, 38, With Pulseless Electrical Activity
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
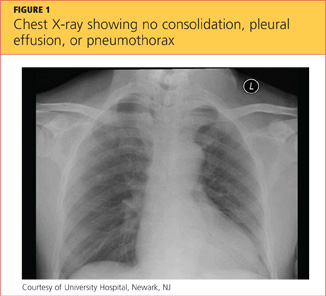
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.

Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
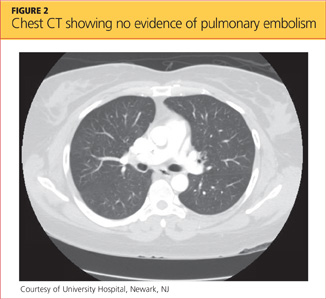
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.
Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
On an autumn day, a 38-year-old woman with a history of asthma presented to the emergency department (ED) with the chief complaint of shortness of breath (SOB). The patient described her SOB as sudden in onset and not relieved by use of her albuterol inhaler; hence the ED visit.
She denied any chest pain, palpitations, dizziness, orthopnea, upper respiratory tract infection, cough, wheezing, fever or chills, headache, vision changes, body aches, sick contacts, or pets at home. She said she uses her albuterol inhaler as needed, and that she had used it that day for the first time in “a few months.” She denied any history of intubation or steroid use. Additionally, she had not been seen by a primary care provider in years.
The woman, a native of Ghana, had been living in the United States for many years. She denied any recent travel or exposure to toxic chemicals; any use of tobacco, alcohol, or illicit drugs; or any history of sexually transmitted disease.
The patient was afebrile (temperature, 98.6°F), with a respiratory rate of 20 breaths/min; blood pressure, 144/69 mm Hg; and ventricular rate, 125 beats/min. On physical examination, her extraocular movements were intact; pupils were equal, round, reactive to light and accommodation; and sclera were nonicteric. The patient’s head was normocephalic and atraumatic, and the neck was supple with normal range of motion and no jugular venous distension or lymphadenopathy. Her mucous membranes were moist with no pharyngeal erythema or exudates. Cardiovascular examination, including ECG, revealed tachycardia but no murmurs or gallops.
While being evaluated in the ED, the patient became tachypneic and began to experience respiratory distress. She was intubated for airway protection, at which time she developed pulseless electrical activity (PEA), with 30 beats/min. She responded to atropine and epinephrine injections. A repeat ECG showed sinus tachycardia and right atrial enlargement with right-axis deviation. Chest x-ray (see Figure 1) showed no consolidation, pleural effusion, or pneumothorax.
Results from the patient’s lab work are shown in the table, above. Negative results were reported for a urine pregnancy test.
Since there was no clear etiology for the patient’s PEA, she underwent pan-culturing, with the following tests ordered: HIV antibody testing, immunovirology for influenza A and B viruses, and urine toxicology. Doppler ultrasound of the bilateral lower extremities was also ordered, in addition to chest CT and transthoracic and transesophageal echocardiography (TTE and TEE, respectively). The patient was intubated and transferred to the medical ICU for further management.
The differential diagnosis included cardiac tamponade, acute MI, acute pulmonary embolus (PE), tension pneumothorax, hypovolemia, and asthma exacerbated by viral or bacterial infection.1,2 Although the case patient presented with PEA, she did not have the presenting signs of cardiac tamponade known as Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds.3 TTE showed an ejection fraction of 65% and grade 2 diastolic dysfunction but no pericardial effusions (which accumulate rapidly in the patient with cardiac tamponade, resulting from fluid buildup in the pericardial layers),4 and TEE showed no atrial thrombi (which can masquerade as cardiac tamponade5). The patient had no signs of trauma and denied any history of malignancy (both potential causes of cardiac tamponade). Chest x-ray showed normal heart size and no pneumothorax, consolidations, or pleural effusions.4,6-8 Thus, the diagnosis of cardiac tamponade was ruled out.
Common presenting symptoms of acute MI include sudden-onset chest pain, SOB, palpitations, dizziness, nausea, and/or vomiting. Women may experience less dramatic symptoms—often little more than SOB and fatigue.9 According to a 2000 consensus document from a joint European Society of Cardiology/American College of Cardiology committee10 in which MI was redefined, the diagnosis of MI relies on a rise in cardiac troponin levels, typical MI symptoms, and changes in ECG showing pathological Q waves or ST elevation or depression. The case patient’s troponin I level was less than 0.02 ng/mL, and ECG did not reveal Q waves or ST-T wave changes; additionally, since the patient had no chest pain, palpitations, diaphoresis, nausea, or vomiting, acute MI was ruled out.
Blood clots capable of blocking the pulmonary artery usually originate in the deep veins of the lower extremities.11 Three main factors, called Virchow’s triad, are known to contribute to these deep vein thromboses (DVTs): venous stasis, endothelial injury, and a hypercoagulability state.12,13 The patient had denied any trauma, recent travel, history of malignancy, or use of tobacco or oral contraceptives, and the result of her urine pregnancy test was negative. Even though the patient presented with tachypnea and acute SOB, with ECG showing right-axis deviation and tachycardia (common presenting signs and symptoms for PE), her chest CT showed no evidence of PE (see Figure 2); additionally, Doppler ultrasound of the bilateral lower extremities revealed no DVTs. Thus, PE was also excluded.
Tension pneumothorax was also ruled out, as chest x-ray showed neither mediastinal shift nor tracheal deviation, and the patient had denied any trauma. Laboratory analyses did not indicate hyponatremia, and the patient’s hemoglobin and hematocrit were satisfactory. She was tachycardic on admission, but her blood pressure was stable. As the patient denied any use of vasodilators or diuretics, hypovolemia was ruled out.
Patients experiencing asthma exacerbation can present with acute SOB, which usually resolves following use of IV steroids, nebulizer therapy, and inhaler treatments. Despite being administered IV methylprednisolone and magnesium sulfate in the ED, the patient experienced PEA and respiratory distress and required intubation for airway protection.
The HIV test was nonreactive, and blood and urine cultures did not show any growth. Results of tests for Legionella urinary antigen and Streptococcus pneumoniae antigen were negative. Sputum culture showed normal flora. Immunovirology testing, however, was positive for both influenza A and B antigens.
Chest X-ray showed no acute pulmonary pathology, nor did chest CT show any central, interlobar, or segmental embolism or mediastinal lymphadenopathy. It was determined that the patient’s acute SOB might represent asthma exacerbation secondary to influenza viral infection. Her PEA was attributed to possible acute pericarditis secondary to concomitant influenza A and B viral infection.
DISCUSSION
Currently, the CDC recognizes three types of influenza virus: A, B, and C.14 Only influenza A viruses are further classified into subtypes, based on the presence of surface proteins called hemagglutinin (HA) or neuraminidase (NA) glycoproteins. Humans can be infected by influenza A subtypes H1N1 and H3N2.14 Influenza B viruses, found mostly in humans, are associated with significant morbidity and mortality.
Influenza A and B viruses are further classified into strains that change with each flu season—thus, the need to update vaccinations against influenza A and B each year. No vaccination exists against influenza C virus, which is known to cause only mild illness in humans.15
In patients with asthma (as in the case patient), chronic bronchitis, or emphysema, infection with the influenza virus can manifest with SOB, in addition to the more common symptoms of fever, sore throat, headache, rhinorrhea, chills, muscle aches, and general discomfort.16 Patients with coronary artery disease, congestive heart failure (CHF), and/or a history of smoking may experience more severe symptoms and increased risk for influenza-associated mortality than do other patients.17,18
Rare cardiac complications of influenza infections are myocarditis and benign acute pericarditis; myocarditis can progress to CHF and death.19,20 A case of acute myopericarditis was reported by Proby et al21 in a patient with acute influenza A infection who developed pericardial effusions, myositis, tamponade, and pleurisy. That patient recovered after pericardiocentesis and administration of inotropic drugs.
In the literature, a few cases of acute pericarditis have been reported in association with administration of the influenza vaccination.22,23
In the case patient, the diagnosis of influenza A and B was made following testing of nasal and nasopharyngeal swabs with an immunochromatographic assay that uses highly sensitive monoclonal antibodies to detect influenza A and B nucleoprotein antigens.24,25
According to reports in the literature, two-thirds of cases of acute pericarditis are caused by infection, most commonly viral infection (including influenza virus, adenovirus, enterovirus, cytomegalovirus, hepatitis B virus, and herpes simplex virus).26,27 Other etiologies for acute pericarditis are autoimmune (accounting for less than 10% of cases) and neoplastic conditions (5% to 7% of cases).26
PATIENT OUTCOME
Consultation with an infectious disease specialist was obtained. The patient was placed under droplet isolation precautions and was started on a nebulizer, IV steroid treatments, and oseltamivir 75 mg by mouth every 12 hours. She was transferred to a medical floor, where she completed a five-day course of oseltamivir.
As a result of timely intervention, the patient was discharged in stable condition on a therapeutic regimen that included albuterol, fluticasone, and salmeterol inhalation, in addition to tapered-dose steroids. She was advised to follow up with her primary care provider and at the pulmonary clinic.
CONCLUSION
To our knowledge, this is the first reported case of acute pericarditis in a patient with concomitant acute infections with influenza A and B. According to conclusions reached in recent literature, further research is needed to explain the pathophysiology of influenza viral infections, associated cardiovascular morbidity and mortality, and the degree to which these can be prevented by influenza vaccination.1,28 Also to be pursued through research is a better understanding of the morbidity and mortality associated with influenza viruses, especially in children and in adults affected by asthma, cardiac disease, and/or obesity.
REFERENCES
1. Finelli L, Chaves SS. Influenza and acute myocardial infarction. J Infect Dis. 2011;203(12):
1701-1704.
2. Steiger HV, Rimbach K, Müller E, Breitkreutz R. Focused emergency echocardiography: lifesaving tool for a 14-year-old girl suffering out-of-hospital pulseless electrical activity arrest because of cardiac tamponade. Eur J Emerg Med. 2009;16(2): 103-105.
3. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade.
J Emerg Trauma Shock. 2012;5(1):72-75.
4. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27(6):1595-1610.
5. Papanagnou D, Stone MB. Massive right atrial thrombus masquerading as cardiac tamponade. Acad Emerg Med. 2010;17(2):E11.
6. Saito Y, Donohue A, Attai S, et al. The syndrome of cardiac tamponade with “small” pericardial effusion. Echocardiography. 2008;25(3): 321-327.
7. Lin E, Boire A, Hemmige V, et al. Cardiac tamponade mimicking tuberculous pericarditis as the initial presentation of chronic lymphocytic leukemia in a 58-year-old woman: a case report. J Med Case Rep. 2010;4:246.
8. Meniconi A, Attenhofer Jost CH, Jenni R. How to survive myocardial rupture after myocardial infarction. Heart. 2000;84(5):552.
9. Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction. Circ J. 2006;70(3):222-226.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined: a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-969.
11. Goldhaber SZ. Deep venous thrombosis and pulmonary thromboembolism. In: Fauci AS, Braunwald E, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Medical; 2008:1651–1657.
12. Brooks EG, Trotman W, Wadsworth MP, et al. Valves of the deep venous system: an overlooked risk factor. Blood. 2009;114(6):1276-1279.
13. Kyrle PA, Eichinger S. Is Virchow’s triad complete? Blood. 2009;114(6):1138-1139.
14. CDC. Seasonal influenza (flu): types of influenza viruses (2012). www.cdc.gov/flu/about/viruses/types.htm. Accessed October 24, 2012.
15. CDC. Seasonal influenza (flu)(2012). www.cdc .gov/flu. Accessed October 24, 2012.
16. Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718-725.
17. Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM. Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A. Conn Med. 2004;68(4):199-205.
18. Murin S, Bilello K. Respiratory tract infections: another reason not to smoke. Cleve Clin J Med. 2005;72(10):916-920.
19. Ray CG, Icenogle TB, Minnich LL, et al. The use of intravenous ribavirin to treat influenza virus–associated acute myocarditis. J Infect Dis. 1989; 159(5):829-836.
20. Fairley CK, Ryan M, Wall PG, Weinberg J. The organism reported to cause infective myocarditis and pericarditis in England and Wales. J Infect. 1996;32(3):223-225.
21. Proby CM, Hackett D, Gupta S, Cox TM. Acute myopericarditis in influenza A infection. Q J Med. 1986;60(233):887-892.
22. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed). 1981; 283(6290):526-527.
23. Desson JF, Leprévost M, Vabret F, Davy A. Acute benign pericarditis after anti-influenza vaccination [in French]. Presse Med. 1997;26 (9):415.
24. BinaxNOW® Influenza A&B Test Kit (product instructions). www.diagnosticsdirect2u.com/images/PDF/Binax%20Now%20416-022%20PPI .pdf. Accessed October 24, 2012.
25. 510(k) Substantial Equivalence Determination Decision Summary [BinaxNow® Influenza A & B Test] (2009). www.accessdata.fda.gov/cdrh_docs/reviews/K062109.pdf. Accessed October 24, 2012.
26. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121(7):916-928.
27. Maisch B, Seferovic PM, Ristic AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases: executive summary. Eur Heart J. 2004;25(7):587-610.
28. McCullers JA, Hayden FG. Fatal influenza B infections: time to reexamine influenza research priorities. J Infect Dis. 2012;205(6):870-872.
Rethinking antibiotics for sinusitis—again
Practice Changer
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than OTC remedies alone.1
Strength of recommendation
B: Based on a single high-quality randomized controlled trial.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after experiencing fatigue, purulent nasal discharge, and unilateral facial pain for nearly
10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his
recovery.
Each year, more than 30 million Americans—about one in seven adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
CDC guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last seven or more days, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than seven days are unlikely to have a bacterial infection. But the nonspecific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology–Head and Neck Surgery (AAO–HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within two weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
A previous PURL that was based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO–HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY
Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to receive amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1
To be eligible for the study, patients had to be between the ages of 18 and 70, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of seven- to-28-day duration and worsening or not improving, or of < 7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past four weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1,500 mg/d, divided into three doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0 = no problem; 3 = severe problem), with a clinically important difference of ≥ 0.5 on the mean score. The test was administered at enrollment and at days 3, 7, and 10. The disease-specific quality of life at day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on days 3 and 10. On day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥ 0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a six-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control groups at days 3 and 10. On day 7, 74% of patients treated with amoxicillin self-
reported significant improvement in symptoms since the start of the study, versus 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3 to 34; P = .02) for a reduction in symptoms at day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (< 10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW
Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on day 7 of 0.19 points, but no clinically meaningful difference (≥ 0.5) based on the SNOT-16 mean score.
CAVEATS
Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION
Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be
difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Clinicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhinosinusitis, as well as by offering symptomatic treatments.
REFERENCES
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007:137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al; American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Sys Rev. 2008(2):CD000243.
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009(4):CD005149.
9. Schumann A, Hickner, J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no.” J Fam Pract. 2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008; 47:735-743.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2012;61(10):610-612.
Practice Changer
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than OTC remedies alone.1
Strength of recommendation
B: Based on a single high-quality randomized controlled trial.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after experiencing fatigue, purulent nasal discharge, and unilateral facial pain for nearly
10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his
recovery.
Each year, more than 30 million Americans—about one in seven adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
CDC guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last seven or more days, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than seven days are unlikely to have a bacterial infection. But the nonspecific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology–Head and Neck Surgery (AAO–HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within two weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
A previous PURL that was based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO–HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY
Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to receive amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1
To be eligible for the study, patients had to be between the ages of 18 and 70, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of seven- to-28-day duration and worsening or not improving, or of < 7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past four weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1,500 mg/d, divided into three doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0 = no problem; 3 = severe problem), with a clinically important difference of ≥ 0.5 on the mean score. The test was administered at enrollment and at days 3, 7, and 10. The disease-specific quality of life at day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on days 3 and 10. On day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥ 0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a six-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control groups at days 3 and 10. On day 7, 74% of patients treated with amoxicillin self-
reported significant improvement in symptoms since the start of the study, versus 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3 to 34; P = .02) for a reduction in symptoms at day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (< 10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW
Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on day 7 of 0.19 points, but no clinically meaningful difference (≥ 0.5) based on the SNOT-16 mean score.
CAVEATS
Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION
Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be
difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Clinicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhinosinusitis, as well as by offering symptomatic treatments.
REFERENCES
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007:137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al; American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Sys Rev. 2008(2):CD000243.
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009(4):CD005149.
9. Schumann A, Hickner, J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no.” J Fam Pract. 2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008; 47:735-743.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2012;61(10):610-612.
Practice Changer
Stop prescribing amoxicillin for acute rhinosinusitis. It’s unlikely to provide a speedier recovery than OTC remedies alone.1
Strength of recommendation
B: Based on a single high-quality randomized controlled trial.
ILLUSTRATIVE CASE
A 28-year-old man comes to your clinic after experiencing fatigue, purulent nasal discharge, and unilateral facial pain for nearly
10 days. Overall, he appears healthy, and you diagnose acute rhinosinusitis. You suggest OTC remedies for supportive care and wonder if a course of amoxicillin would speed his
recovery.
Each year, more than 30 million Americans—about one in seven adults—are diagnosed with sinusitis.2 No more than 2% of these cases are thought to be bacterial.3
CDC guidelines for the diagnosis of acute bacterial rhinosinusitis include symptoms that last seven or more days, with maxillary pain or tenderness in the face or teeth and purulent nasal secretions.4 Patients with symptoms lasting less than seven days are unlikely to have a bacterial infection. But the nonspecific signs and symptoms included in the CDC guidelines limit their usefulness in determining whether the cause of the sinusitis is bacterial or viral on clinical grounds alone.
Most cases of sinusitis spontaneously resolve
In patients with acute bacterial sinusitis, the American Academy of Otolaryngology–Head and Neck Surgery (AAO–HNS) guidelines advocate watchful waiting and symptom relief with nasal oxymetazoline, pseudoephedrine, and saline nasal irrigation.3 The rate of spontaneous resolution is high: 80% of patients with clinically diagnosed sinusitis improve without treatment within two weeks.1,5
Traditional decongestants and mucolytics have not demonstrated efficacy in resolving sinusitis, although rigorous evaluation is lacking. Other treatments, such as saline irrigation and intranasal corticosteroids, are of unclear benefit and need further study.6-8
Lack of evidence has done little to curtail antibiotic use
A previous PURL that was based on a meta-analysis of antibiotic treatment trials for sinusitis recommended that we stop prescribing antibiotics for adults with acute sinusitis unless their symptoms are severe.9,10 Yet antibiotics remain the mainstay of treatment.
Despite the AAO–HNS guidelines, evidence of spontaneous resolution, and accumulating data on the lack of efficacy of antimicrobials for sinusitis, 81% of patients diagnosed with acute sinusitis were given prescriptions for antibiotics, a study of primary care practices showed.11 Frequent use of antibiotics contributes to high rates of drug resistance, and adverse events related to antibiotic use account for an estimated 142,500 emergency department visits annually.12
STUDY SUMMARY
Little benefit from amoxicillin, even for severe cases
Garbutt and colleagues revisited the issue, randomizing 166 patients from 10 primary care practices to receive amoxicillin plus symptomatic treatment or placebo plus symptomatic treatment for acute rhinosinusitis.1
To be eligible for the study, patients had to be between the ages of 18 and 70, meet CDC diagnostic criteria for acute rhinosinusitis, and have moderate to very severe symptoms that were of seven- to-28-day duration and worsening or not improving, or of < 7-day duration but had worsened after an initial improvement. Exclusion criteria included complications from sinusitis, a history of allergy to penicillin or amoxicillin, antibiotic use in the past four weeks, comorbidities that impair immune function, cystic fibrosis, pregnancy, and mild symptoms.
Both groups had similar baseline characteristics, with participants who were predominantly white (79%) and female (64%). All the participants received a supply of symptomatic treatments: acetaminophen, guaifenesin, dextromethorphan, and sustained-release pseudoephedrine. The treatment group also received amoxicillin 1,500 mg/d, divided into three doses; the placebo group received identical-looking placebo pills.
Patients were assessed with the Sino-nasal Outcome Test-16 (SNOT-16), a validated measure that asks patients to assess both the severity and frequency of 16 sinus symptoms. SNOT-16 uses a 0-to-3 rating scale (0 = no problem; 3 = severe problem), with a clinically important difference of ≥ 0.5 on the mean score. The test was administered at enrollment and at days 3, 7, and 10. The disease-specific quality of life at day 3 was the primary outcome.
There was no statistically significantly difference in SNOT-16 scores between the amoxicillin and placebo groups on days 3 and 10. On day 7, there was a small statistically significant improvement in the amoxicillin group, but it did not reach the level of clinical importance (≥ 0.5) based on SNOT-16’s mean score.
The authors also asked participants to retrospectively assess symptom change since enrollment on a six-point scale. Those who reported that their symptoms were “a lot better” or “absent” were characterized as significantly improved. The results correlated with the data from the SNOT-16, showing no difference between the amoxicillin and control groups at days 3 and 10. On day 7, 74% of patients treated with amoxicillin self-
reported significant improvement in symptoms since the start of the study, versus 56% in the control group. The number needed to treat was 6 (95% confidence interval, 3 to 34; P = .02) for a reduction in symptoms at day 7.
Patients in both groups had similar rates of absenteeism, inability to perform usual activities, relapse and recurrence, and use of additional health care. Satisfaction with treatment was similar, as well.
No serious adverse effects occurred. Both groups reported similar frequencies (< 10%) of nausea, diarrhea, abdominal pain, or vaginitis.
WHAT’S NEW
Even severe sinusitis resolves without antibiotics
Previous studies recommended foregoing antibiotics for acute sinusitis, except when symptoms are severe. This study—in which more than half (52%) of patients in each group had symptoms rated severe or very severe—found no benefit to adding amoxicillin to supportive treatments.1 Antibiotics did not shorten the duration of illness, prevent relapse and recurrence, or improve satisfaction with treatment. The researchers found a statistically significant difference between groups on day 7 of 0.19 points, but no clinically meaningful difference (≥ 0.5) based on the SNOT-16 mean score.
CAVEATS
Guidelines, risk of complications may give reason to pause
The 2012 Infectious Diseases Society of America guidelines recommend amoxicillin with clavulanic acid as empiric therapy for acute bacterial rhinosinusitis.7 The findings of the study by Garbutt et al—conducted at a time when the incidence of beta-lactamase-producing organisms was low and amoxicillin was the treatment of choice—suggest otherwise.
Serious complications of sinusitis, such as brain abscess, periorbital cellulitis, and meningitis, can occur, however. Patients who deteriorate clinically or develop high fever or severe headache require close follow-up, which may include further diagnostic evaluation or consultation with an otolaryngologist. Evidence is lacking as to whether antibiotics prevent such complications.5
CHALLENGES TO IMPLEMENTATION
Managing patient expectations
Many patients with symptoms of acute rhinosinusitis think they need an antibiotic. Managing their expectations and providing instructions about supportive treatments are time consuming and may be
difficult.
Nonetheless, we’re optimistic: We think that most patients today are aware of the problems associated with antibiotic resistance and wary of “superbugs,” and will therefore be receptive to this practice change. Clinicians can help by reminding patients of the adverse effects of antibiotics and the natural course of rhinosinusitis, as well as by offering symptomatic treatments.
REFERENCES
1. Garbutt J, Banister C, Spitznagel E, et al. Amoxicillin for acute rhinosinusitis: a randomized controlled trial. JAMA. 2012;307:685-692.
2. Centers for Disease Control and Prevention. Summary health statistics for US adults: National Health Interview Survey 2010. January 2012. www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf. Accessed July 9, 2012.
3. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007:137(3 suppl):S1-S31.
4. Hickner JM, Bartlett JG, Besser RE, et al; American Academy of Family Physians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control; Infectious Disease Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults; background. Ann Intern Med. 2001;134:498-505.
5. Ahovuo-Saloranta A, Borisenk OV, Kovanen N, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Sys Rev. 2008(2):CD000243.
6. Allen G, Kelsberg G, Jankowski TA. Do nasal decongestants relieve symptoms? J Fam Pract. 2003;52:714-724.
7. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112.
8. Zalmanovici A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2009(4):CD005149.
9. Schumann A, Hickner, J. Patients insist on antibiotics for sinusitis? Here is a good reason to say “no.” J Fam Pract. 2008;57:464-468.
10. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
11. Gill JM, Fleischut P, Haas S. Use of antibiotics for adult upper respiratory infections in outpatient settings: a national ambulatory network study. Fam Med. 2006;38:349-354.
12. Shehab N, Patel PR, Srinivasan A, et al. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008; 47:735-743.
ACKNOWLEDGEMENT
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2012;61(10):610-612.
COPD Varies By State, Peaks Above 9%
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
The prevalence of chronic obstructive pulmonary disease is 6% nationwide, but varies from less than 4% in Washington and Minnesota to more than 9% in Alabama and Kentucky, according to data from the Centers for Disease Control and Prevention. The findings were published in the CDC’s Morbidity and Mortality Weekly Report on Nov. 23.
A total of 13,306 adults who reported having chronic obstructive pulmonary disease (COPD) in the national survey also responded to the COPD module. Of these, 76% reported undergoing a diagnostic breathing test, 64% reported that COPD symptoms (specifically shortness of breath) had an adverse effect on their quality of life, and 51% reported taking at least one COPD medication (MMWR 2012; 61:938-43).
In age-adjusted comparisons, women were more likely to report COPD compared with men (7% vs. 5%, respectively). COPD prevalence decreased from an average of 10% among individuals making less than $25,000 per year to 3% in those making more than $75,000 per year, and the prevalence was lower among employed individuals, homemakers, and students compared with those who were unemployed, retired, or otherwise unable to work. The prevalence of COPD was highest in current smokers (13%) compared with former smokers (7%) and never smokers (3%).
Data were taken from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey. Additional COPD data were collected in an optional COPD module about COPD diagnosis and quality of life. This module was part of the BRFSS in 21 states, the District of Columbia, and Puerto Rico.
The 2011 BRFSS was conducted via telephone, either landline or mobile. The survey population included adults aged 18 years and older throughout the United States.
The findings were limited by several factors including the absence of data on individuals in institutions or nursing homes and by the use of self-reports for COPD diagnosis, the researchers said. However, the report is the first to analyze data on COPD prevalence in all 50 states, the District of Columbia, and Puerto Rico, they noted. State-level health officials should focus surveillance efforts, educational campaigns, and interventions on areas of highest COPD prevalence, they added.
The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION'S MORBIDITY AND MORTALITY WEEKLY REPORT
Major Finding: The overall prevalence of chronic obstructive pulmonary disease in the United States is approximately 6%.
Data Source: The data come from the 2011 Behavioral Risk Factor Surveillance System (BRFSS) survey.
Disclosures: The study was supported by the CDC and the National Heart, Lung, and Blood Institute of the National Institutes of Health.
FDA Panel Wants Limited Nosocomial Pneumonia Indication for Telavancin
SILVER SPRING, MD. – The approval of the antibacterial drug telavancin should be expanded to include patients with nosocomial pneumonia, but only in limited situations, according to the majority of a Food and Drug Administration advisory panel.
At a meeting Nov. 29, the FDA’s Anti-Infective Drugs Advisory Committee voted 13-2 that the available data on telavancin provided substantial evidence that it was safe and effective for treating nosocomial pneumonia, "when other alternatives are not suitable." Panelists agreed that telavancin should be reserved to treat patients with nosocomial pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) not methicillin-sensitive S. aureus (MSSA) or Streptococcus pneumoniae, because there are many other treatments available for those infections.
Most panelists did not support approval of the broader indication requested by the manufacturer: treatment of patients with nosocomial pneumonia, including ventilator-associated pneumonia (VAP), caused by susceptible isolates of the Gram-positive microorganisms, S. aureus (including methicillin-susceptible and methicillin-resistant isolates) or S. pneumoniae. The panel voted 9-6 that the data from the two studies did not provide substantial evidence that the drug was safe and effective for this indication.
Telavancin is a lipoglycopeptide antibacterial administered intravenously, with bactericidal activity that results from inhibition of cell wall synthesis and disruption of bacterial plasma membrane function, according to Theravance, the drug’s manufacturer. It was approved in 2009 for the treatment of adults with complicated skin and skin structure infections caused by susceptible Gram-positive bacteria and is marketed as Vibativ.
The current labeling for telavancin includes warnings and precautions in the prescribing information about the increased risk of nephrotoxicity associated with treatment, based on experience in patients treated for the skin infection indication. A boxed warning cites the potential fetal risks.
Among the other points made by panelists were that labeling should include statements about use in patients with reduced creatinine clearance and renal failure and that the company should aggressively collect postmarketing safety and efficacy data.
The panel considered data that included analyses of clinical cure and 28-day all-cause mortality from two non-inferiority studies. These studies comprised 1,503 patients with nosocomial pneumonia and compared telavancin for 7-21 days (10 mg/kg every 24 hours administered intravenously in patients with normal renal function and mild renal impairment or an adjusted dose for patients with moderate or severe renal insufficiency) with vancomycin (1 g IV every 12 hours).
Theravance first submitted an application for approval of the broad nosocomial pneumonia indication in 2009. That application included results of the two studies, which used clinical cure rate as the primary endpoint. Since then, the FDA has requested more data from the company, including a post hoc analysis of mortality, but subsequently declined to approve telavancin after deciding that the trials did not provide adequate evidence of non-inferiority to vancomycin. In response, the company filed a formal dispute, which was rejected by the FDA, but the agency encouraged the company to resubmit the application and held the panel meeting Nov. 29 to review the data.
Telavancin has been approved in the European Union for the treatment of nosocomial pneumonia caused by MRSA, similar to the indication backed by the FDA panel.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The approval of the antibacterial drug telavancin should be expanded to include patients with nosocomial pneumonia, but only in limited situations, according to the majority of a Food and Drug Administration advisory panel.
At a meeting Nov. 29, the FDA’s Anti-Infective Drugs Advisory Committee voted 13-2 that the available data on telavancin provided substantial evidence that it was safe and effective for treating nosocomial pneumonia, "when other alternatives are not suitable." Panelists agreed that telavancin should be reserved to treat patients with nosocomial pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) not methicillin-sensitive S. aureus (MSSA) or Streptococcus pneumoniae, because there are many other treatments available for those infections.
Most panelists did not support approval of the broader indication requested by the manufacturer: treatment of patients with nosocomial pneumonia, including ventilator-associated pneumonia (VAP), caused by susceptible isolates of the Gram-positive microorganisms, S. aureus (including methicillin-susceptible and methicillin-resistant isolates) or S. pneumoniae. The panel voted 9-6 that the data from the two studies did not provide substantial evidence that the drug was safe and effective for this indication.
Telavancin is a lipoglycopeptide antibacterial administered intravenously, with bactericidal activity that results from inhibition of cell wall synthesis and disruption of bacterial plasma membrane function, according to Theravance, the drug’s manufacturer. It was approved in 2009 for the treatment of adults with complicated skin and skin structure infections caused by susceptible Gram-positive bacteria and is marketed as Vibativ.
The current labeling for telavancin includes warnings and precautions in the prescribing information about the increased risk of nephrotoxicity associated with treatment, based on experience in patients treated for the skin infection indication. A boxed warning cites the potential fetal risks.
Among the other points made by panelists were that labeling should include statements about use in patients with reduced creatinine clearance and renal failure and that the company should aggressively collect postmarketing safety and efficacy data.
The panel considered data that included analyses of clinical cure and 28-day all-cause mortality from two non-inferiority studies. These studies comprised 1,503 patients with nosocomial pneumonia and compared telavancin for 7-21 days (10 mg/kg every 24 hours administered intravenously in patients with normal renal function and mild renal impairment or an adjusted dose for patients with moderate or severe renal insufficiency) with vancomycin (1 g IV every 12 hours).
Theravance first submitted an application for approval of the broad nosocomial pneumonia indication in 2009. That application included results of the two studies, which used clinical cure rate as the primary endpoint. Since then, the FDA has requested more data from the company, including a post hoc analysis of mortality, but subsequently declined to approve telavancin after deciding that the trials did not provide adequate evidence of non-inferiority to vancomycin. In response, the company filed a formal dispute, which was rejected by the FDA, but the agency encouraged the company to resubmit the application and held the panel meeting Nov. 29 to review the data.
Telavancin has been approved in the European Union for the treatment of nosocomial pneumonia caused by MRSA, similar to the indication backed by the FDA panel.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver, but not at this meeting.
SILVER SPRING, MD. – The approval of the antibacterial drug telavancin should be expanded to include patients with nosocomial pneumonia, but only in limited situations, according to the majority of a Food and Drug Administration advisory panel.
At a meeting Nov. 29, the FDA’s Anti-Infective Drugs Advisory Committee voted 13-2 that the available data on telavancin provided substantial evidence that it was safe and effective for treating nosocomial pneumonia, "when other alternatives are not suitable." Panelists agreed that telavancin should be reserved to treat patients with nosocomial pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) not methicillin-sensitive S. aureus (MSSA) or Streptococcus pneumoniae, because there are many other treatments available for those infections.
Most panelists did not support approval of the broader indication requested by the manufacturer: treatment of patients with nosocomial pneumonia, including ventilator-associated pneumonia (VAP), caused by susceptible isolates of the Gram-positive microorganisms, S. aureus (including methicillin-susceptible and methicillin-resistant isolates) or S. pneumoniae. The panel voted 9-6 that the data from the two studies did not provide substantial evidence that the drug was safe and effective for this indication.
Telavancin is a lipoglycopeptide antibacterial administered intravenously, with bactericidal activity that results from inhibition of cell wall synthesis and disruption of bacterial plasma membrane function, according to Theravance, the drug’s manufacturer. It was approved in 2009 for the treatment of adults with complicated skin and skin structure infections caused by susceptible Gram-positive bacteria and is marketed as Vibativ.
The current labeling for telavancin includes warnings and precautions in the prescribing information about the increased risk of nephrotoxicity associated with treatment, based on experience in patients treated for the skin infection indication. A boxed warning cites the potential fetal risks.
Among the other points made by panelists were that labeling should include statements about use in patients with reduced creatinine clearance and renal failure and that the company should aggressively collect postmarketing safety and efficacy data.
The panel considered data that included analyses of clinical cure and 28-day all-cause mortality from two non-inferiority studies. These studies comprised 1,503 patients with nosocomial pneumonia and compared telavancin for 7-21 days (10 mg/kg every 24 hours administered intravenously in patients with normal renal function and mild renal impairment or an adjusted dose for patients with moderate or severe renal insufficiency) with vancomycin (1 g IV every 12 hours).
Theravance first submitted an application for approval of the broad nosocomial pneumonia indication in 2009. That application included results of the two studies, which used clinical cure rate as the primary endpoint. Since then, the FDA has requested more data from the company, including a post hoc analysis of mortality, but subsequently declined to approve telavancin after deciding that the trials did not provide adequate evidence of non-inferiority to vancomycin. In response, the company filed a formal dispute, which was rejected by the FDA, but the agency encouraged the company to resubmit the application and held the panel meeting Nov. 29 to review the data.
Telavancin has been approved in the European Union for the treatment of nosocomial pneumonia caused by MRSA, similar to the indication backed by the FDA panel.
The FDA usually follows the recommendations of its advisory panels, which are not binding. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver, but not at this meeting.
AT A MEETING OF THE FDA'S ANTI-INFECTIVE DRUGS ADVISORY COMMITTEE
FDA Panel Gives Nod to Drug for Multidrug-Resistant TB
SILVER SPRING, MD. – Bedaquiline, an oral antimycobacterial drug with a novel mechanism of action, received an 18 to 0 vote for approval for the treatment of multidrug-resistant pulmonary tuberculosis by a Food and Drug Administration advisory panel.
At a meeting on Nov. 28, the FDA’s Anti-Infective Drugs Advisory Committee concluded that phase II clinical data indicated the drug increased the time to sputum culture conversion, a surrogate marker for clinical effectiveness, when added to standard background treatment in adults with multidrug-resistant (MDR) TB. Sputum culture conversion was defined as two consecutive negative cultures collected at least 25 days apart that were not followed by a confirmed positive culture.
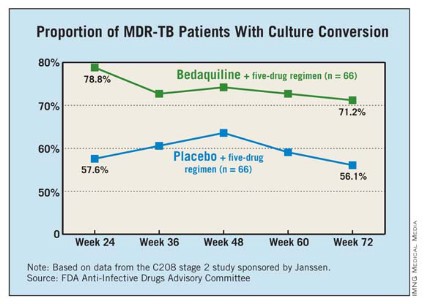
The panel voted 11 to 7 that the data provided substantial evidence that the drug was safe for this indication. There were 10 deaths among 79 patients on bedaquiline, compared with 2 deaths in 81 patients on placebo. The FDA reviewers and the company could not identify any pattern or cause that could explain the imbalance in the death rate. All but one of the deaths in the bedaquiline-treated patients occurred after treatment with the drug was completed.
The FDA is reviewing the drug as an accelerated approval, because bedaquiline addresses the unmet need for an effective therapy for MDR TB. In such cases, recommendation for approval can be based on surrogate clinical end points, with the requirement that clinical effectiveness be confirmed in a postmarketing study with hard clinical end points before full approval is granted. Panelists recommended that full approval require concrete evidence of increased cure rates with treatment in a confirmatory study. Further, more data on the drug are needed in HIV-positive and black populations, and studies also are needed to address the implications of the drug’s long half-life.
Bedaquiline, a diarylquinolone discovered at Janssen Therapeutics, a division of Janssen Products, inhibits mycobacterial adenosine triphosphate (ATP) synthetase. The drug kills both replicating and nonreplicating TB bacilli, and is active against drug-sensitive and MDR TB, according to the company.
If approved by the FDA, bedaquiline will be the first antituberculosis drug with a novel mechanism of action approved in the United States since rifampin’s approval in 1970, and the first drug approved for TB since rifapentine was approved in 1998.
"The fact that this drug is able to shorten the period the organism is in the sputum has public health implications for [reducing]transmission," said Dr. Peter Katona, of the University of California, Los Angeles.
In 2011, 98 cases of MDR TB were reported in the United States, but the condition is a far greater problem globally, with an estimated incidence in 2011 of 310,000 cases, according to the Centers for Disease Control and Prevention.
The panel reviewed two phase II studies of almost 400 patients with pulmonary MDR TB.
One study enrolled 160 nonwhite patients, most of them men from South Africa with a mean age of 35 years. All were newly diagnosed with pulmonary MDR TB; a small proportion were HIV positive. They were treated with a standard five-drug regimen that included ethionamide, pyrazinamide, ofloxacin, kanamycin, and 400 mg once daily of bedaquiline for 2 weeks, followed by 200 mg three times a week for 22 weeks, or placebo. After 24 weeks, patients continued background treatment for 12-18 months.
At 24 weeks, 79% of those treated with bedaquiline had a culture conversion, compared with 58% of those on placebo, a significant difference.
The second study was an open-label trial of 233 previously treated patients with sputum smear–positive pulmonary MDR TB. They received the same dosing regimen of bedaquiline combined with an individualized background regimen for MDR TB. At 24 weeks, the culture conversion rate was 80%, and sputum cultures became negative in a mean of 57 days. The faster conversion rate likely reflected the fact that most patients were already on treatment when enrolled in the trial.
The incidence of serious adverse events was higher among those on bedaquiline (6.9% vs. 1.9%). Treatment was associated with elevated transaminases in 4 cases, compared with 0 in placebo-treated patients. There was a modest increase in QT prolongation, although there were no cases of torsades de pointes or evidence that this caused any deaths.
The FDA’s deadline for making a decision on bedaquiline is by the end of December. The agency usually follows the recommendations of its advisory panels, which are not binding. Panelists were cleared of potential conflicts of interest related to the topic of the meeting.
SILVER SPRING, MD. – Bedaquiline, an oral antimycobacterial drug with a novel mechanism of action, received an 18 to 0 vote for approval for the treatment of multidrug-resistant pulmonary tuberculosis by a Food and Drug Administration advisory panel.
At a meeting on Nov. 28, the FDA’s Anti-Infective Drugs Advisory Committee concluded that phase II clinical data indicated the drug increased the time to sputum culture conversion, a surrogate marker for clinical effectiveness, when added to standard background treatment in adults with multidrug-resistant (MDR) TB. Sputum culture conversion was defined as two consecutive negative cultures collected at least 25 days apart that were not followed by a confirmed positive culture.
The panel voted 11 to 7 that the data provided substantial evidence that the drug was safe for this indication. There were 10 deaths among 79 patients on bedaquiline, compared with 2 deaths in 81 patients on placebo. The FDA reviewers and the company could not identify any pattern or cause that could explain the imbalance in the death rate. All but one of the deaths in the bedaquiline-treated patients occurred after treatment with the drug was completed.
The FDA is reviewing the drug as an accelerated approval, because bedaquiline addresses the unmet need for an effective therapy for MDR TB. In such cases, recommendation for approval can be based on surrogate clinical end points, with the requirement that clinical effectiveness be confirmed in a postmarketing study with hard clinical end points before full approval is granted. Panelists recommended that full approval require concrete evidence of increased cure rates with treatment in a confirmatory study. Further, more data on the drug are needed in HIV-positive and black populations, and studies also are needed to address the implications of the drug’s long half-life.
Bedaquiline, a diarylquinolone discovered at Janssen Therapeutics, a division of Janssen Products, inhibits mycobacterial adenosine triphosphate (ATP) synthetase. The drug kills both replicating and nonreplicating TB bacilli, and is active against drug-sensitive and MDR TB, according to the company.
If approved by the FDA, bedaquiline will be the first antituberculosis drug with a novel mechanism of action approved in the United States since rifampin’s approval in 1970, and the first drug approved for TB since rifapentine was approved in 1998.
"The fact that this drug is able to shorten the period the organism is in the sputum has public health implications for [reducing]transmission," said Dr. Peter Katona, of the University of California, Los Angeles.
In 2011, 98 cases of MDR TB were reported in the United States, but the condition is a far greater problem globally, with an estimated incidence in 2011 of 310,000 cases, according to the Centers for Disease Control and Prevention.
The panel reviewed two phase II studies of almost 400 patients with pulmonary MDR TB.
One study enrolled 160 nonwhite patients, most of them men from South Africa with a mean age of 35 years. All were newly diagnosed with pulmonary MDR TB; a small proportion were HIV positive. They were treated with a standard five-drug regimen that included ethionamide, pyrazinamide, ofloxacin, kanamycin, and 400 mg once daily of bedaquiline for 2 weeks, followed by 200 mg three times a week for 22 weeks, or placebo. After 24 weeks, patients continued background treatment for 12-18 months.
At 24 weeks, 79% of those treated with bedaquiline had a culture conversion, compared with 58% of those on placebo, a significant difference.
The second study was an open-label trial of 233 previously treated patients with sputum smear–positive pulmonary MDR TB. They received the same dosing regimen of bedaquiline combined with an individualized background regimen for MDR TB. At 24 weeks, the culture conversion rate was 80%, and sputum cultures became negative in a mean of 57 days. The faster conversion rate likely reflected the fact that most patients were already on treatment when enrolled in the trial.
The incidence of serious adverse events was higher among those on bedaquiline (6.9% vs. 1.9%). Treatment was associated with elevated transaminases in 4 cases, compared with 0 in placebo-treated patients. There was a modest increase in QT prolongation, although there were no cases of torsades de pointes or evidence that this caused any deaths.
The FDA’s deadline for making a decision on bedaquiline is by the end of December. The agency usually follows the recommendations of its advisory panels, which are not binding. Panelists were cleared of potential conflicts of interest related to the topic of the meeting.
SILVER SPRING, MD. – Bedaquiline, an oral antimycobacterial drug with a novel mechanism of action, received an 18 to 0 vote for approval for the treatment of multidrug-resistant pulmonary tuberculosis by a Food and Drug Administration advisory panel.
At a meeting on Nov. 28, the FDA’s Anti-Infective Drugs Advisory Committee concluded that phase II clinical data indicated the drug increased the time to sputum culture conversion, a surrogate marker for clinical effectiveness, when added to standard background treatment in adults with multidrug-resistant (MDR) TB. Sputum culture conversion was defined as two consecutive negative cultures collected at least 25 days apart that were not followed by a confirmed positive culture.
The panel voted 11 to 7 that the data provided substantial evidence that the drug was safe for this indication. There were 10 deaths among 79 patients on bedaquiline, compared with 2 deaths in 81 patients on placebo. The FDA reviewers and the company could not identify any pattern or cause that could explain the imbalance in the death rate. All but one of the deaths in the bedaquiline-treated patients occurred after treatment with the drug was completed.
The FDA is reviewing the drug as an accelerated approval, because bedaquiline addresses the unmet need for an effective therapy for MDR TB. In such cases, recommendation for approval can be based on surrogate clinical end points, with the requirement that clinical effectiveness be confirmed in a postmarketing study with hard clinical end points before full approval is granted. Panelists recommended that full approval require concrete evidence of increased cure rates with treatment in a confirmatory study. Further, more data on the drug are needed in HIV-positive and black populations, and studies also are needed to address the implications of the drug’s long half-life.
Bedaquiline, a diarylquinolone discovered at Janssen Therapeutics, a division of Janssen Products, inhibits mycobacterial adenosine triphosphate (ATP) synthetase. The drug kills both replicating and nonreplicating TB bacilli, and is active against drug-sensitive and MDR TB, according to the company.
If approved by the FDA, bedaquiline will be the first antituberculosis drug with a novel mechanism of action approved in the United States since rifampin’s approval in 1970, and the first drug approved for TB since rifapentine was approved in 1998.
"The fact that this drug is able to shorten the period the organism is in the sputum has public health implications for [reducing]transmission," said Dr. Peter Katona, of the University of California, Los Angeles.
In 2011, 98 cases of MDR TB were reported in the United States, but the condition is a far greater problem globally, with an estimated incidence in 2011 of 310,000 cases, according to the Centers for Disease Control and Prevention.
The panel reviewed two phase II studies of almost 400 patients with pulmonary MDR TB.
One study enrolled 160 nonwhite patients, most of them men from South Africa with a mean age of 35 years. All were newly diagnosed with pulmonary MDR TB; a small proportion were HIV positive. They were treated with a standard five-drug regimen that included ethionamide, pyrazinamide, ofloxacin, kanamycin, and 400 mg once daily of bedaquiline for 2 weeks, followed by 200 mg three times a week for 22 weeks, or placebo. After 24 weeks, patients continued background treatment for 12-18 months.
At 24 weeks, 79% of those treated with bedaquiline had a culture conversion, compared with 58% of those on placebo, a significant difference.
The second study was an open-label trial of 233 previously treated patients with sputum smear–positive pulmonary MDR TB. They received the same dosing regimen of bedaquiline combined with an individualized background regimen for MDR TB. At 24 weeks, the culture conversion rate was 80%, and sputum cultures became negative in a mean of 57 days. The faster conversion rate likely reflected the fact that most patients were already on treatment when enrolled in the trial.
The incidence of serious adverse events was higher among those on bedaquiline (6.9% vs. 1.9%). Treatment was associated with elevated transaminases in 4 cases, compared with 0 in placebo-treated patients. There was a modest increase in QT prolongation, although there were no cases of torsades de pointes or evidence that this caused any deaths.
The FDA’s deadline for making a decision on bedaquiline is by the end of December. The agency usually follows the recommendations of its advisory panels, which are not binding. Panelists were cleared of potential conflicts of interest related to the topic of the meeting.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S ANTI-INFECTIVE DRUGS ADVISORY COMMITTEE
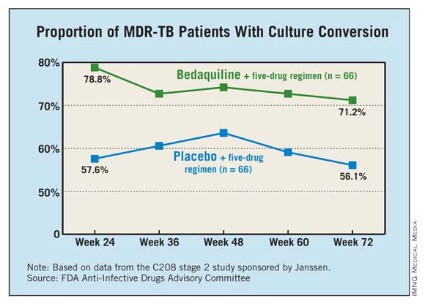
COPD Guidelines Found Underutilized
ATLANTA – Regardless of disease severity, guideline-concordant treatment is not provided to nearly half of all patients who have stable chronic obstructive pulmonary disease and are treated in the ambulatory care setting, findings from an observational study suggest.
The study also indicated that guideline-concordant treatment was more likely to be provided when patients were comanaged by a pulmonologist and a primary care physician.
Of 450 patients, 56% received guideline-concordant care as outlined by the 2010 Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage-specific recommendations, Dr. Gulshan Sharma reported at the annual meeting of the American College of Chest Physicians.
No differences were found in treatment level with respect to age, gender, race, disease severity, or comorbidities on multivariate analysis, but patients comanaged by a primary care physician and a pulmonologist were more likely to receive an appropriate level of care, as compared to patients treated by a primary care physician (odds ratio, 4.6), said Dr. Sharma of the University of Texas Medical Branch, Galveston.
Clinical practice guidelines for the treatment of patients with COPD in the ambulatory care setting are issued and updated regularly. Previous studies have demonstrated the value of these guidelines for improving the quality of care of patients with COPD and for reducing exacerbations and hospitalizations.
However, the degree to which these guidelines are implemented in clinical practice has been unclear, Dr. Sharma said. The study findings suggest that they are underutilized, particularly by primary care physicians.
Patients included in the study were adults with a clinical diagnosis of COPD and at least one outpatient visit between January and December 2010. The mean age of participants was 67 years, 46% were women, 20% had no comorbidities, and 75% had one or two comorbidities.
About 7% had GOLD stage I disease, almost half (more than 46%) had GOLD stage II disease, 33% had stage III disease, and 13% had stage IV disease.
Additionally, 47% were managed by a primary care physician alone, 41% were comanaged by a primary care physician and a pulmonologist, 10% did not have a primary care physician and received care mainly from a specialist, and about 2% had no regular care provider.
The findings indicate a need for efforts to increase awareness of clinical practice guidelines and the importance of adherence to the guidelines in patients with COPD, particularly among primary care physicians, Dr. Sharma concluded.
Dr. Sharma reported having no disclosures.
ATLANTA – Regardless of disease severity, guideline-concordant treatment is not provided to nearly half of all patients who have stable chronic obstructive pulmonary disease and are treated in the ambulatory care setting, findings from an observational study suggest.
The study also indicated that guideline-concordant treatment was more likely to be provided when patients were comanaged by a pulmonologist and a primary care physician.
Of 450 patients, 56% received guideline-concordant care as outlined by the 2010 Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage-specific recommendations, Dr. Gulshan Sharma reported at the annual meeting of the American College of Chest Physicians.
No differences were found in treatment level with respect to age, gender, race, disease severity, or comorbidities on multivariate analysis, but patients comanaged by a primary care physician and a pulmonologist were more likely to receive an appropriate level of care, as compared to patients treated by a primary care physician (odds ratio, 4.6), said Dr. Sharma of the University of Texas Medical Branch, Galveston.
Clinical practice guidelines for the treatment of patients with COPD in the ambulatory care setting are issued and updated regularly. Previous studies have demonstrated the value of these guidelines for improving the quality of care of patients with COPD and for reducing exacerbations and hospitalizations.
However, the degree to which these guidelines are implemented in clinical practice has been unclear, Dr. Sharma said. The study findings suggest that they are underutilized, particularly by primary care physicians.
Patients included in the study were adults with a clinical diagnosis of COPD and at least one outpatient visit between January and December 2010. The mean age of participants was 67 years, 46% were women, 20% had no comorbidities, and 75% had one or two comorbidities.
About 7% had GOLD stage I disease, almost half (more than 46%) had GOLD stage II disease, 33% had stage III disease, and 13% had stage IV disease.
Additionally, 47% were managed by a primary care physician alone, 41% were comanaged by a primary care physician and a pulmonologist, 10% did not have a primary care physician and received care mainly from a specialist, and about 2% had no regular care provider.
The findings indicate a need for efforts to increase awareness of clinical practice guidelines and the importance of adherence to the guidelines in patients with COPD, particularly among primary care physicians, Dr. Sharma concluded.
Dr. Sharma reported having no disclosures.
ATLANTA – Regardless of disease severity, guideline-concordant treatment is not provided to nearly half of all patients who have stable chronic obstructive pulmonary disease and are treated in the ambulatory care setting, findings from an observational study suggest.
The study also indicated that guideline-concordant treatment was more likely to be provided when patients were comanaged by a pulmonologist and a primary care physician.
Of 450 patients, 56% received guideline-concordant care as outlined by the 2010 Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage-specific recommendations, Dr. Gulshan Sharma reported at the annual meeting of the American College of Chest Physicians.
No differences were found in treatment level with respect to age, gender, race, disease severity, or comorbidities on multivariate analysis, but patients comanaged by a primary care physician and a pulmonologist were more likely to receive an appropriate level of care, as compared to patients treated by a primary care physician (odds ratio, 4.6), said Dr. Sharma of the University of Texas Medical Branch, Galveston.
Clinical practice guidelines for the treatment of patients with COPD in the ambulatory care setting are issued and updated regularly. Previous studies have demonstrated the value of these guidelines for improving the quality of care of patients with COPD and for reducing exacerbations and hospitalizations.
However, the degree to which these guidelines are implemented in clinical practice has been unclear, Dr. Sharma said. The study findings suggest that they are underutilized, particularly by primary care physicians.
Patients included in the study were adults with a clinical diagnosis of COPD and at least one outpatient visit between January and December 2010. The mean age of participants was 67 years, 46% were women, 20% had no comorbidities, and 75% had one or two comorbidities.
About 7% had GOLD stage I disease, almost half (more than 46%) had GOLD stage II disease, 33% had stage III disease, and 13% had stage IV disease.
Additionally, 47% were managed by a primary care physician alone, 41% were comanaged by a primary care physician and a pulmonologist, 10% did not have a primary care physician and received care mainly from a specialist, and about 2% had no regular care provider.
The findings indicate a need for efforts to increase awareness of clinical practice guidelines and the importance of adherence to the guidelines in patients with COPD, particularly among primary care physicians, Dr. Sharma concluded.
Dr. Sharma reported having no disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Major Finding: Patients comanaged by a primary care physician and a pulmonologist were 4.6 times more likely to receive an appropriate level of care, as compared to patients treated by a primary care physician alone.
Data Source: An observational study of 450 COPD patients seen in outpatient clinics.
Disclosures: Dr. Sharma reported having no disclosures.